THE INTEGRATED DESIGN DEVELOPMENT PROCESS OF HEALTHCARE BUILDINGS
1.2.2 Focus Area
My work on healthcare buildings has given me an understanding of what has to be considered when designing hospitals. To me, quick visualisations and calculations of various performances can be of great use. BIM allows us to get a better picture of what we are planning and how all the building elements fit together. The use of BIM in practice inspired me to research how it might be best applied in the design development process (DDP) for healthcare buildings. The aim of the research is to find out or suggest starting points as to when, how much and why the utilisation of BIM is effective of all areas.
According to “buildingsmart” and “Pinnacle Infotech Inc”, two well-know institutions, “the design work and the decision making process shifts forward the design timeline, when utilising BIM”.
The figure below shows the DDP, established by “buildingsmart” and “Pinnacle Infotech Inc”:
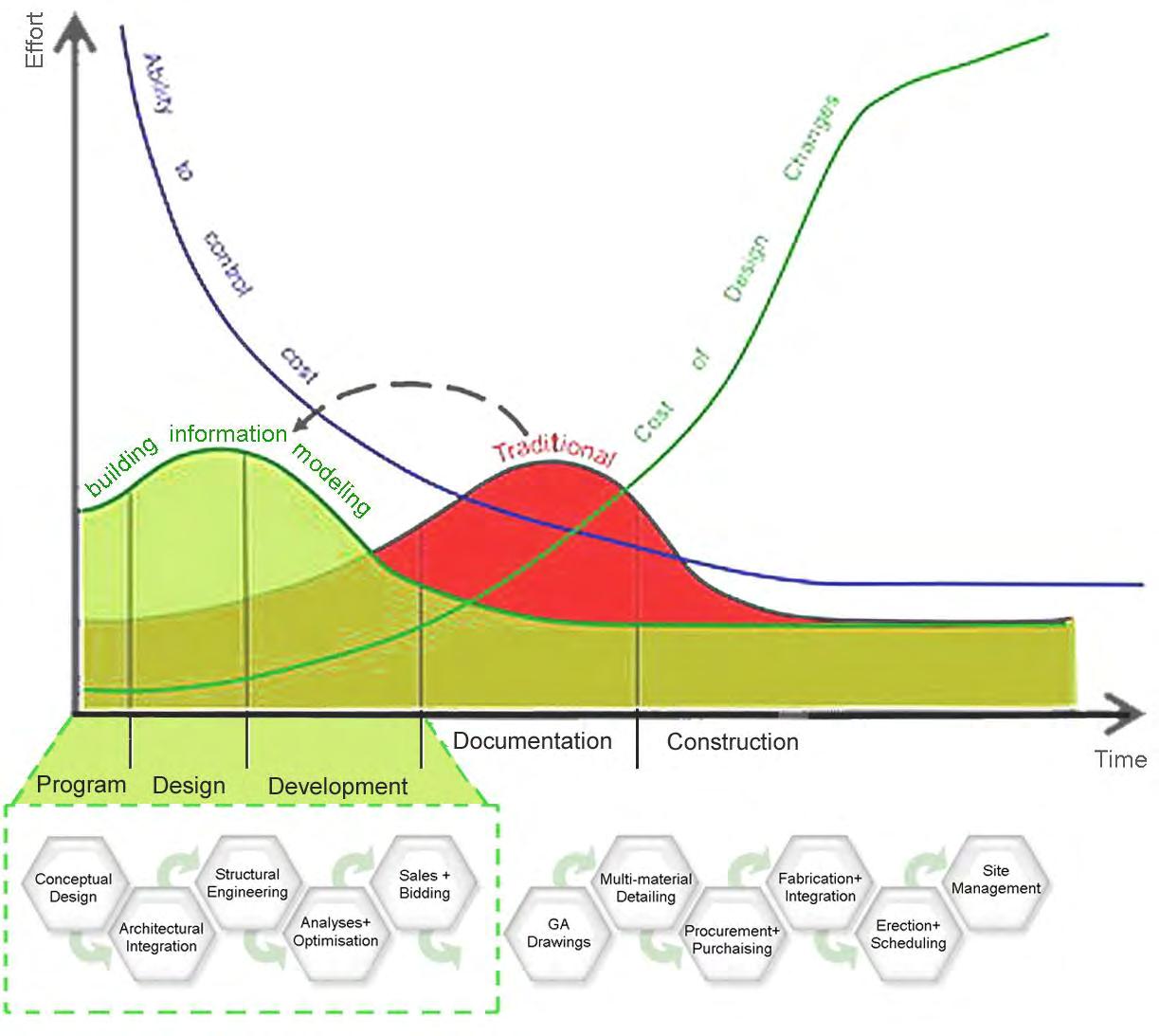
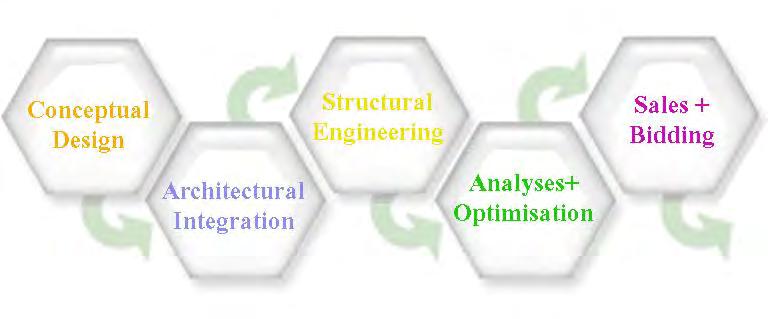
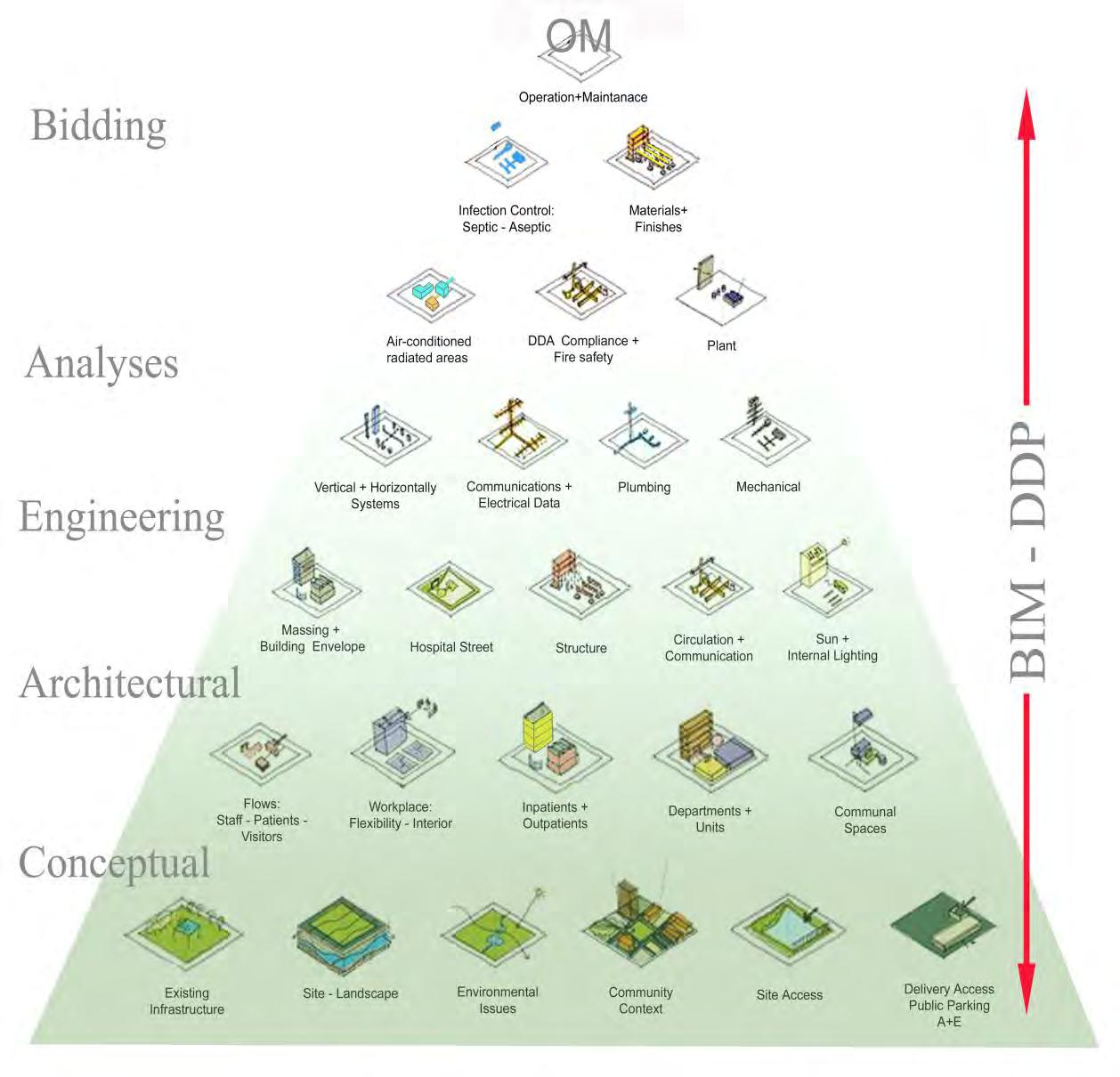
By translating the ‘System Approach’ (page 5) and ‘Design Timeline’ (page 9) to the tasks of designing a healthcare building, the figure below shows a potential design order. Within a given timeline or brief, the related functions of a hospitals are brought into an order to inform the separate BIM models.
For example, the early design of the hospital or the ‘building site’ (=Conceptual BIM) determines the number of bedrooms, en-suits, (=Architectural BIM) and the best structural method (=Engineering BIM). The arrangement of in- and outpatient departments (=Conceptual BIM) allows for different structural and organisational models (=Architectural BIM + Engineering BIM) as well as fire- and DDA safety measures (=Analysis BIM). Finally, the performance of the building (=Analysis BIM) determines the documentation and building cost (=Bidding BIM), and so on.
1.2.3
Research Aim and Objectives
For the purpose of this research, the spectrum of BIM for healthcare buildings was analysed. Based on a collection of BIM material, the objectives of this research are to investigate the design development process (DDP) with the utilisation of BIM:
Explore BIM as a design tool and find out how it might support the DDP as a vehicle of sustainable design and integrated design coordination for health buildings planning.
Examine front end design service of DDP and determine the suitability of BIM into this process for health buildings
Survey and interviews of key design leaders with 3 case studies whom have used BIM in the DDP process in the UK
Set out findings with recommendations for the use of BIM in the DDP of health buildings planning with key design principles for project coordination for the use for the project team.
The aim of this research was to develop a design guideline for the use of BIM in the DDP for healthcare buildings.
The literature review and the individual research were organised in 5 main BIM themes to meet the complexity of BIM and the DDP. By using...
Case Studies (BIM comparison with different level of BIM expertise)
Online Survey (achieving a sample size that allows for statistical calculations)
Interview (direct and personal data collection)
...this research feeds back with various reasoning whether BIM utilisation supports the DDP of Healthcare buildings:
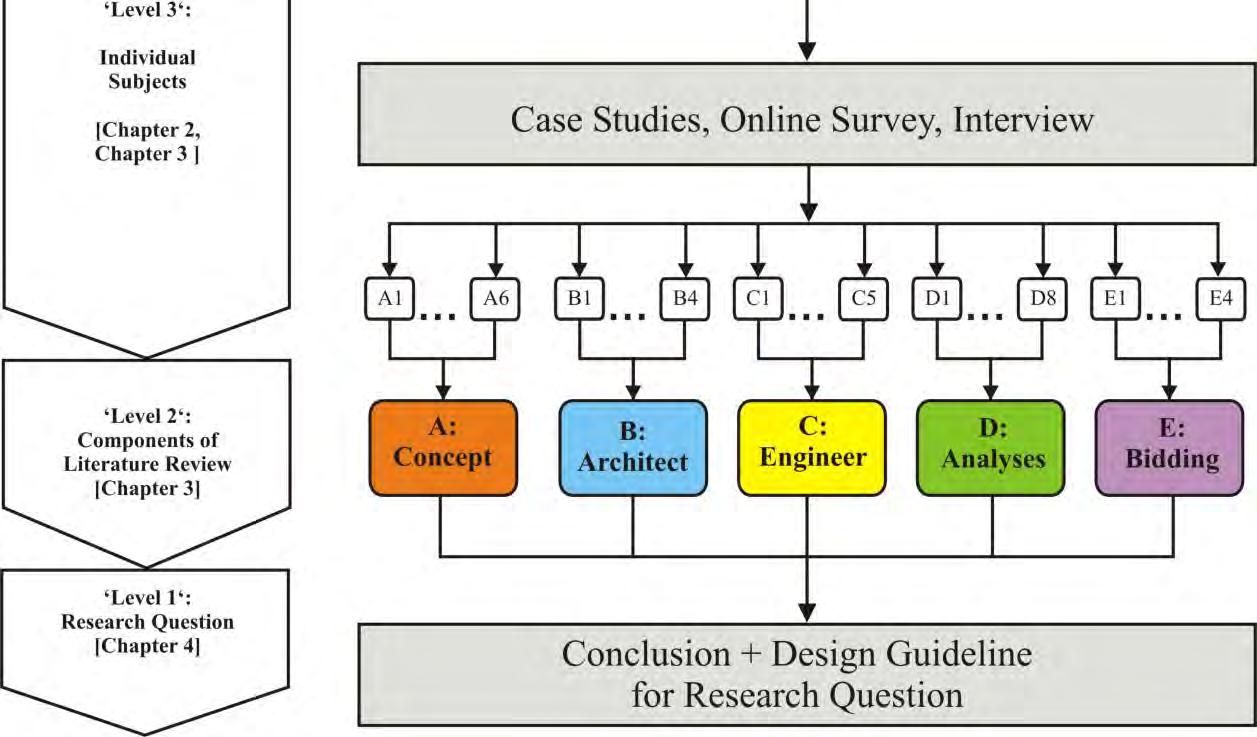
Thereby the research question, as shown below, is the highest of three ‘Levels’ of analysis that will enable a component based approach, as presented in Figure 1 ‘Research Methodology and Data Collection.’
Does BIM support the DDP of Healthcare Buildings?
1.3ResearchMethodology+DataCollection
1.3.1
Methodology structure
Due to the complex nature of the DDP and discovering, whether BIM utilisation makes sense inside the design development process, the research question was broken down into components and subcomponents which are then used to formulate questions for the survey. The results of the subcomponents were then combined into the components and subsequently into the conclusions for the research question. The structure of this methodology was presented below:
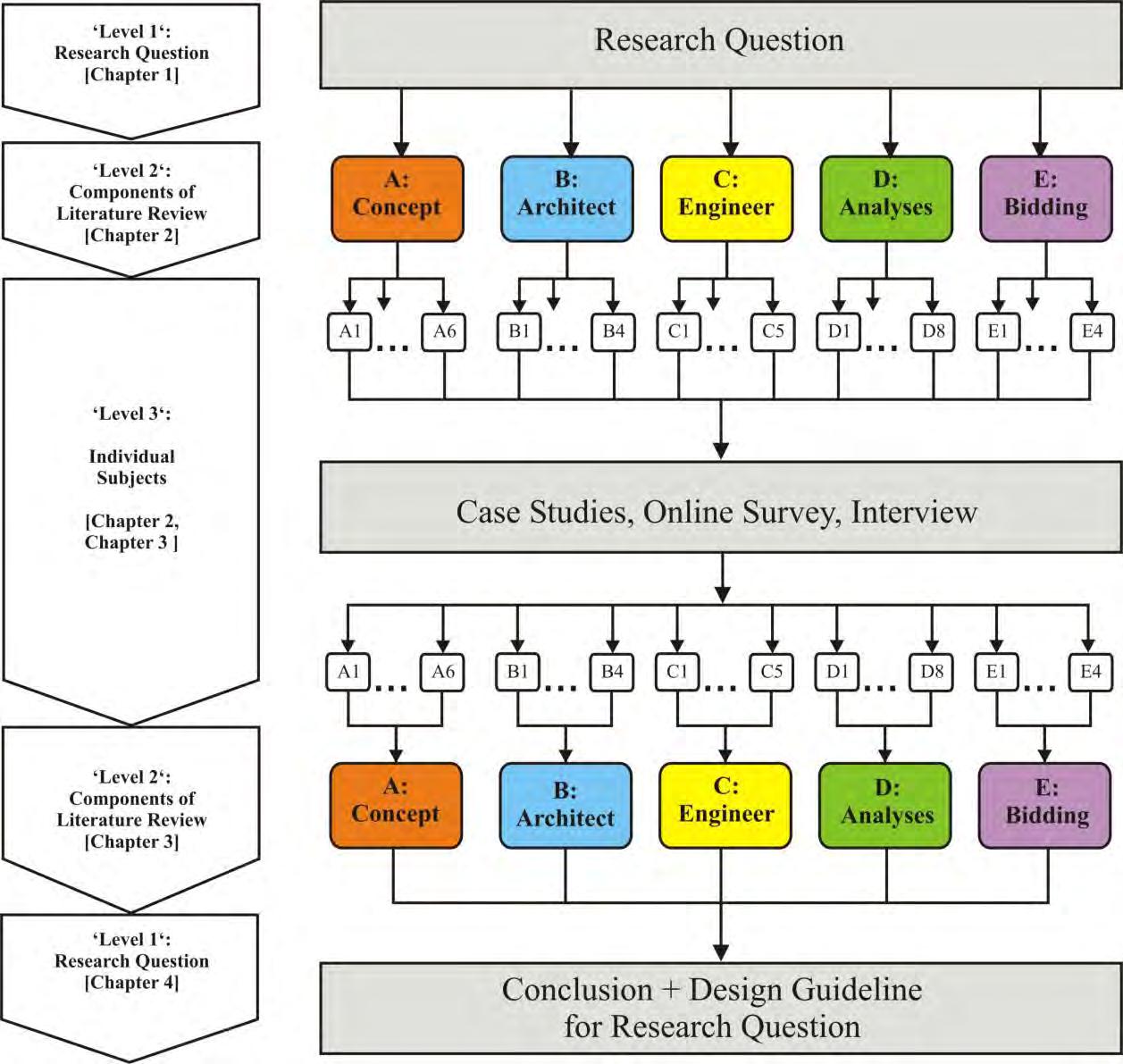
For the purpose of enabling a precise research approach to the research question, the same was broken down into three component questions (Level 2), eg asking what BIM does and how it can be utilised in healthcare and sustainable planning.
‘Level 2’ – Component Questions for the DDP
The above ‘Level 2’ sub-questions were further split into subject elements (Level 3) to formulate and support my individual research. The Case Study and Interview feed back to the initial research question and give additional reasoning.
‘Level 3’ – Component Questions for the DDP
‘Level 3’ sub-questions were parametric, space and component based modelling and performance analysed modelling with BIM.
Limitations: The study does not intend to compare, explain or appraise software packages. That is subject to each BIM vendor. Rather a general overview, a roadmap, a plan that examines, compares, clarifies the design process and helps architects decide whether BIM supports the process, as well as to move forward with BIM is the authors intention.
1.3.2 Data collection



The literature review was examined towards 5 separate BIMs Conceptual + Architectural + Engineering + Analysis + Bidding and tested on the following entities:
Space and Component based modelling, Parametric modelling
Design Coordination and Collaboration
Life-cycle related topics such as sustainability, standardisation, future change,
The selection of 3 Case Studies cover 2d, 3D, and 4D/5D scenarios:
Case Study 1 (Conceptual + Architectural BIM approach)
Case Study 2 (Architectural + Engineering’ BIM approach
Case Study 3 (Engineering + Analysis BIM approach)
The survey was an online- questionnaire which was sent out to 103 healthcare architects to find out what is there approach to the 5 BIM themes. A total of 20 offices responded. This was done to achieve a sample size that allows for statistical calculations.
The interview with a London based architectural office using BIM was carried out to find out about office resources, setting up skills, software, equipment and management. This was a direct and personal data collection.