ANISOCORIA ANISOCORIA
 EDITED BY MARINA ADDIS WALDMANN
EDITED BY MARINA ADDIS WALDMANN
ANISOCORIA
 EDITED BY MARINA ADDIS WALDMANN
EDITED BY MARINA ADDIS WALDMANN
ANISOCORIA
4 Introduction Introduzione 22 A diary of care, healing and courage Un diario di cura, guarigione e coraggio 30 Delirious Intensive Care Unit, a retroactive manifesto Delirio in Terapia Intensiva un manifesto retroattivo 36 Epidemiology of traumatic brain injury Epidemiologia del trauma cranico 40 Medical Imaging and its interpretations Imaging Medico e le sue interpretazioni 44 #healthcareheroes and work overload #eroidellasanità e sovraccarico di lavoro 48 Custom-Made cranial implants Impianti cranici su misura 54 Sensorial Aphasia Afasia sensoriale 58 Surgery as a performance La chirurgia come performance 62 Who Will Care for the Caregivers? Chi si prenderà Cura dei Caregivers? 70 Hogeweyk, the first dementia village Hogeweyk, il primo dementia village
Anisocoria è un termine medico usato per descrivere una diversa dilatazione delle due pupille in identiche condizioni di illuminazione. Spesso significa che nell’encefalo si sta verificando un danno imminente e che è necessario intervenire rapidamente con un intervento neurochirurgico. Anisocoria è un diario dei giorni e dei mesi successivi all’incidente d’auto di mia sorella. Attraverso l’imaging medico l’opera interroga i limiti e le frontiere dell’odierna percezione del corpo umano. Scansioni come RM (Risonanza Magnetica) e CT (tomografia computerizzata) diventano strumenti imprescindibili sia in fase analitica che operativa. Funzionano come mezzo introduttivo tra un corpo, quello del paziente, e un altro corpo, quello del chirurgo. Il primo esplorato visivamente, e messo a nudo, prima di entrare in sala operatoria, il secondo anch’esso spogliato di ogni possessione privata, per poi essere uniformato e igienizzato. Entrambi insieme per ore, esposti a raggi potenzialmente pericolosi, in condizioni fisiche estreme. È qui che la medicina contemporanea si lascia guidare da un’immagine. Il progetto fa parte di una più ampia ricerca volta a esplorare dove, da chi e come le procedure salvavita e le prestazioni sanitarie sono erogate nel mondo. Come le nozioni di cura e vulnerabilità possono essere integrate dal punto di vista progettuale. Infine la pubblicazione che accompagna il film s’ispira al “diario del lutto*” di Roland Barthes, dove a seguito della morte della madre annotò una frase al giorno, usando semplice inchiostro su foglietti di carta di cui teneva una scorta costante. Un frammento tra i frammenti.
*https://www.nytimes.com/2010/10/15/books/15book.html
6
Anisocoria is a medical term used to describe a different dilation of the two pupils under identical lighting conditions. It often means that there is imminent damage to the brain and rapid neurosurgical intervention is needed. Anisocoria is a diary of the days and months following my sister’s car accident. Through medical imaging, the work questions the limits and frontiers of today’s perception of the human body. Scans such as MRI (Magnetic Resonance Imaging) and CT (Computed Tomography) become essential tools both in the analytical and operational phases. They function as an introductory medium between one body, that of the patient, and another body, that of the surgeon. The first visually explored, and stripped, before entering the operating room, the second also stripped of any private possession, to then be standardized and sanitized. Both together for hours, exposed to potentially dangerous rays, in extreme physical conditions. This is where contemporary medicine lets itself be guided by an image. The project is part of a larger research focus aiming to explore where, by who, and how life saving procedures and healthcare are provided world wide, and how caring and vulnerability can be better understood from the designer’s perspective. Finally the publication that accompanies the film follows the lesson of Roland Barthes in “mourning diary*”, where after his mother’s death he noted one phrase every day, using simple ink on slips of paper (regular typing paper cut into quarters) of which he kept a constant supply. A fragment of fragments.
*https://www.nytimes.com/2010/10/15/books/15book.html
7
Ever wondered what the inside of a CT scanner looks like? #NationalTechnologyDay #MGH

8
9
10
Nacht in Venedig, workshop with Danilo Correale
11

12

13
Picture taken with an Iphone 12 mini, screenshot from photo library
https://emedicine.medscape.com/arti-
14
cle/1158571-clinical

15

16
Walter C. Mackenzie Health Sciences Centre and nearby West Edmonton Mall, Edmonton, Alberta, photographs by
Annmarie Adams
17
18
19 ImplantForCranioplastyR3DM_Model.3dm (66 MB) - Rhino 7 Not For Resale Lab


21
Detail from CT scan, courtesy Katharine Thomas Waldmann
22
Detail from CT scan, courtesy Katharine Thomas Waldmann
23
A hospital with a view on the sea, picture taken with an Iphone 12 mini

24

25

26
27
Detail from CT scan, courtesy Katharine Thomas Waldmann
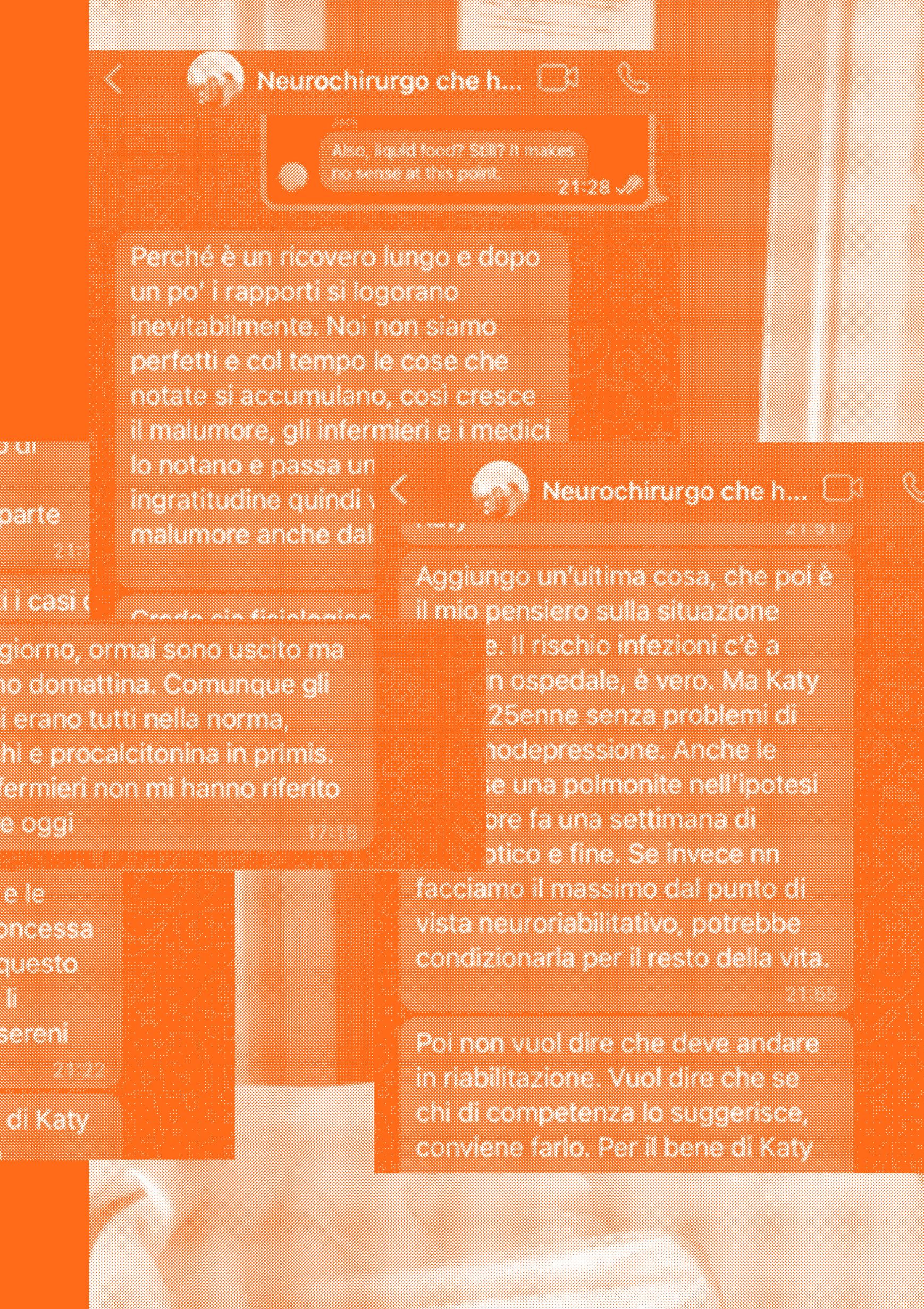
Good words make good worlds, screen shot from whatsapp, courtesy F.V.S
28
29
UN DIARIO DI CURA, GUARIGIONE E CORAGGIO
30
A DIARY OF CARE, HEALING AND COURAGE
31
[1]
La notte tra il 13 e il 14 Aprile 2022 con gli altri studenti del Master Movies - Moving Images Arts e Danilo Correale passeggiavamo tra le strade semi-oscure di Venezia, stavamo cercando di carpire l’anima della città di notte per il progetto che poi prenderà il nome di Nacht in Venedig. All’ora dell’appuntamento circa le 3 di notte mia sorella e il suo amico Ricky si trovavano su un traghetto che sarebbe sbarcato l’indomani mattina al porto di Olbia in Sardegna. Quando ho incontrato il resto della classe davanti al campiello della Maddalena, ho notato tre barche ambulanza, che con il loro fari multi colori illuminavano la notte Veneziana e soprattutto cercavano la persona da soccorrere. Notai subito che questa ricerca si stava svolgendo con non poca difficoltà rispetto a scenari simili, in altre città. Non ci sono ascensori a Venezia eppure portare un malato grave su vari piani di scale non è facile, ma non solo i soccorritori non riuscivano ad identificare con certezza e rapidità l’indirizzo esatto, passarono quasi dieci minuti di erratici andirivieni prima che sparissero in un sottopasso. Fu allora che mi avvicinai a Danilo per dirgli che secondo me questo era il nostro tema, che il fato aveva fatto in modo che ci trovassimo proprio lì con i soccorritori, pieni di equipaggiamento audiovisivo per filmare questo momento. La notte appartiene oltre che alle discoteche anche alla malattia. Per i malati gravi non c’è notte, non c’è Pasqua, o Natale, la malattia non conosce ferie. Quella notte non riprendemmo quella scena, ma una conversazione con un altro diverso e lontano da noi, seguimmo il copione e le riprese si diressero verso un essere incarcerato dentro uno smartphone che ci stava distraendo da quello che ci circondava. Dopo aver camminato ancora fino all’albergo “Agli artisti” ci separammo così come ci eravamo ritrovati e andammo a dormire.
32
On the night between 13 and 14 April 2022 with the other students of the Master Movies - Moving Images Arts and Danilo Correale we walked through the semi-dark streets of Venice, we were trying to capture the soul of the city at night for the project which will afterwards take the name of Nacht in Venedig. At the time of the appointment around 3 in the morning my sister and her friend Ricky were on a ferry that was to arrive the next morning at the port of Olbia in Sardinia. When I met the rest of the class in front of Campiello della Maddalena, I noticed three ambulance boats, which illuminated the Venetian night with their multicolored lights and they were looking for a person to be rescued. I immediately noticed that this research was quite complicated compared to similar scenarios in other cities. There are no elevators in Venice and yet carrying a seriously ill person up several floors of stairs is not easy. Furthermore the rescuers were unable to identify the exact street number, they spent almost ten minutes of erratic comings and goings before disappearing under a Calle. I then approached Danilo to tell him that in my opinion this was our theme, that fate had arranged that we were right there with the rescuers, full of audiovisual equipment to film this epic yet totally dystopian moment. In my opinion The nights are not only for night owls and day dreamers but also for illness and care. For the seriously ill there is no night, there are no holidays, serious illness know no spring break. That night we didn’t shoot the scene I was so mesmerized about, we followed the script and we directed our camera towards a distant human being “incarcerated” inside a smartphone who was of course distracting us from our surroundings. After stopping in front of the hotel “Agli Artisti ‘’ we parted by the same path we had reunited and went to sleep.
33
Quella notte non prestai molta attenzione ai vari messaggi che mandava mia sorella, “stiamo partendo da casa”, “siamo arrivati a Civitavecchia”, “siamo sulla nave”. Eppuro furono gli ultimi che ricevetti da parte sua per vari mesi. Fu mio Zio a chiamarmi, Kathy era in sala operatoria. Davanti al meraviglioso spettacolo della laguna Veneziana, ho ricollegato, la macchina, il viaggio per dimostrare a me la sorella maggiore che non dovevo più trattarla da bambina. Ora mia sorella sta bene, o almeno bene abbastanza. Ogni giorno cerchiamo di rendere omaggio alla grazia che ci é stata concessa. Poiché con quel viaggio per guadagnarsi l’indipendenza ha rischiato di perderla per sempre: é tornata bambina, piccola, fragile e spaventata. La dottoressa che le ha salvato la vita con l’elisoccorso mi disse come prima cosa “ci vuole un secondo a rompersi ma ci vuole molto di più ad aggiustarsi”. Abbiamo imparato ad essere pazienti, che poi è il termine con cui si indicano coloro che in ospedale ricevono le cure. Come se curarsi fosse prima di ogni cosa una questione di tempo. Per questo la sanità non può rispondere alle leggi tayloriane, forse si può migliorare l’efficienza ma non si possono accorciare i tempi, il corpo a volte guarisce ma piano, piano. Che poi è la frase che ho scritto di più in questi mesi “piano, piano”. Le barche ambulanza che vidi la Venezia mi sembrano oggi come un presagio. Era quella, la vita che occupava la mia notte. Penso che sia importante raccontare almeno una parte della nostra storia, non per narcisismo, ma perché credo che ognuno di noi abbia bisogno di ricongiungersi con la propria fragilità, che non va intesa necessariamente come un difetto. L’ambulanza non è il momento in cui il tempo della vita si interrompe ma piuttosto il momento in cui la vita incontra un altra vita, e un corpo si lascia aiutare da altri corpi disposti almeno temporaneamente a sostenerlo.
34
That night I didn’t pay much attention to the various messages my sister sent, “we are leaving home”, “we have arrived in Civitavecchia”, “we are on the ship”. I did not know then that they should be the last ones for several months. It was my Uncle who called me, Kathy was in the operation room. In front of the marvelous spectacle of the Venetian lagoon, I reconnected to the car. To her journey to demonstrate to me, the older sister that I no longer had to treat her as a child. Today my sister is fine, or at least fine enough, every day we try to be thankful for the grace that has been granted us. We were lucky, very lucky because in that journey for her independence she risked losing it forever: she turned suddenly into a child again, small, fragile and scared. The doctor who saved her life told me “it takes seconds to break but it takes much longer to fix”. We have learned to be patient, which is the term used to indicate those who receive treatment in a hospital. As if healing was above all a matter of time. This is why healthcare cannot respond to Taylorian laws, perhaps efficiency can be improved but times cannot be shortened, the body sometimes can and will heal itself but slowly very very slowly. Which is the phrase I’ve written the most in recent months “piano, piano”. The ambulance boats that I saw in Venice, as I return again to the lagoon, seem as an omen. That was it, the life that occupied my night, that is why I think it’s important to tell at least part of our story, not out of narcissism but because I believe that each of us needs to reunite with its own fragility, which shouldn’t necessarily be understood as a defect. The ambulance is not the moment in which the time of life is interrupted but rather a moment in which life meets another life, and a body lets itself be helped by other bodies willing at least temporarily to support others.
35
Sicuramente non é un’esperienza facilmente dematerializzabile, e forse proprio per questo la teniamo a distanza. Come nota bene Annmarie Adams* sono gli ospedali ad assomigliare sempre di più a dei centri commerciali e non l’inverso. In quanto architetti, pensiamo all’ospedale come una tipologia priva di potenziale in cui lo spazio per la creazione è limitato dalle considerazioni funzionali. Un centro di trattamento di corpi senza storia e senza identità, dove ogni paziente ha un numero identificativo per ragioni di sicurezza. Un luogo in cui i pasti si consumano in solitudine e vengono serviti ad orari regolari. Un luogo in cui purtroppo è facile sentirsi intrappolati, in cui i giorni cominciano presto ad assomigliarsi uno all’altro, e a confondersi irrimediabilmente. Eppure nonostante ciò l’ospedale é vita: nel senso di proprietà o condizione di sistemi materiali (viventi, dagli organismi unicellulari a quelli pluricellulari più evoluti) caratterizzati da un alto grado di organizzazione e complessità. Dentro le quattro mura di una stanza o i corridoi di un reparto si incrociano storie di persone molto diverse eppure imparano a convivere. Storie di malattia, di fede, di guarigione ma anche storie personali degli operatori che fanno di quell’edificio la loro casa praticamente quanto i pazienti. L’ospedale non conosce il vuoto, ogni risorsa, ogni armadietto, ogni letto disponibile viene utilizzato e la città tutta entra con rispetto e commozione in questi luoghi che tutto hanno fuorché di astratto. Poiché é in questi luoghi che molti di noi siamo nati.
*https://www.e-flux.com/architecture/treatment/410336/deception-and-design-the-rise-of-the-dementia-village/
36
It is certainly not an easily de-materializable experience, and perhaps for this very reason we keep it at a distance. As Annmarie Adams well notes, it is hospitals that look more and more like shopping malls and not the other way around. As architects, we think of the hospital as a typology without interest where the potential for creation is limited by functional considerations. A treatment center for bodies with no history and no identity, where each patient has an identification number for security reasons. A place where meals are eaten in solitude and are served at regular times. Somewhere where it is very easy to feel trapped, where the days resemble one another, and to get hopelessly confusing. Yet despite this, the hospital is life: in the sense of a condition of material systems (living systems, from unicellular organisms to more evolved multicellular ones) characterized by a high degree of organization and complexity. Inside the four walls of a room or the corridors of a department, stories of very different people cross and learn to live together. Stories of illness, of faith, of healing but also personal stories of the operators who make that building their home practically as much as the patients. The hospital does not know the void, every resource, every locker, every available bed is used and the whole city enters such a place with a mixture of respect and reluctance. Yet it is in a hospital somewhere someday that most of us were born.
37
DELIRIUM DA TERAPIA INTENSIVA. UN MANIFESTO RETROATTIVO
38
39
[2]
DELIRIOUS ICU. A RETROACTIVE MANIFESTO
Delirious New York è un manifesto retroattivo dell’impresa architettonica di Manhattan: districa le teorie, le tattiche e le dissimulazioni che hanno permesso agli architetti di New York di fissare nella Griglia i desideri dell’inconscio collettivo di Manhattan. Il libro di Rem Koolhaas dimostra soprattutto che Manhattan è stata, sin dall’inizio, dedita alla ricerca più razionale, efficiente e utilitaristica dell’irrazionale*. Potremmo dire lo stesso delle Unità di Terapia Intensiva, tra i luoghi più tecnologici di un ospedale. Dove il tempo e le attività sono focalizzati su prestazioni cliniche straordinarie. Bolle spazio temporali in cui il personale e i pazienti sono immersi per quella che sembra essere una giornata interminabile caratterizzata da suoni straordinari, illuminazione artificiale e assistenza meccanica. I posti letto sono predisposti per poter vegliare il maggior numero di pazienti. Qui l’utilitarismo e l’efficienza servono al bisogno “irrazionale” dell’essere umano di sconfiggere la fragilità della propria carne. L’Unità di Terapia Intensiva è una terra di libertà dalla nostra mortalità e dalla dipendenza dalle risorse che non possiamo più provvedere a noi stessi. Un ambiente spesso inospitale per i pazienti stessi in quanto provoca nel 50-60% dei casi una condizione riconosciuta come Delirium da Terapia Intensiva.
*https://www.gsd.harvard.edu/publication/delirious-new-york-aretroactive-manifesto-for-manhattan-1/
40
Delirious New York is a retroactive manifesto of Manhattan’s architectural enterprise: it untangles the theories, tactics and dissimulations that allowed New York’s architects to establish the desires of Manhattan’s collective unconscious in the Grid. The book by Rem Koolhaas proves above all, that Manhattan has been, from the beginning, devoted to the most rational, efficient and utilitarian pursuit of the irrational*. We could say the same of the Intensive Care Units, one of the most technology-intensive places in a hospital. Where time and activities are focused on outstanding clinical performance. Staff and patients are plunged into an everlasting day characterized by noise overload, artificial lighting and machines assistance. The beds are arranged to be able to watch over the greatest number of patients. Here utilitarianism and efficiency serve the “irrational” need of human beings to defeat the fragility of their own flesh. The ICU is a land of freedom from our mortality and dependance from ressources we can no longer provide for ourselves. Often an unsuited environment for the patients themselve as it causes a condition recognized as Intensive Care Delirium in 50-60% of cases.
*https://www.gsd.harvard.edu/publication/delirious-new-york-aretroactive-manifesto-for-manhattan-1/
41
CURA*
s. f. [lat. cūra]. – 1. a. Interessamento solerte e premuroso per un oggetto, che impegna sia il nostro animo sia la nostra attività: dedicare ogni c. alla famiglia, all’educazione dei figli; avere c., prendersi c. di qualcuno o di qualche cosa, occuparsene attivamente, provvedere alle sue necessità, alla sua conservazione: avere c. della propria persona, dei proprî oggetti; non darsi c. di nulla, disinteressarsi di tutto, essere indolente. b. Riguardo, attenzione: conservare, custodire con c.; aversi c., avere riguardi per sé stesso, e soprattutto per la propria salute. Al plur., premure, vigile assistenza: c. pazienti, assidue, affettuose, materne, filiali; 2. a. Il complesso dei mezzi terapeutici e delle prescrizioni mediche che hanno il fine di guarire una malattia (sinon. di terapia, ma con significato e uso più ampî): la c. dei tumori, delle affezioni polmonari, delle nefropatie; c. dimagrante; prescrivere, adottare una c.; fare una c.; sottoporre (un malato), e sottoporsi a una c.; seguire scrupolosamente la c.; tutte le c. sono state vane; una c. efficace, miracolosa; c. preventiva, lo stesso che profilassi; casa di cura, clinica privata, sanatorio; 3. a. Attività di assistenza, nelle varie forme con cui essa viene esercitata da un curatore (con sign. meno specifico di curatela): la c. di un fallimento; più genericam., amministrazione: la c. degli affari, dell’azienda, del patrimonio.
*https://www.treccani.it/vocabolario/cura/
42
CARE*
noun US/ker/UK/keər/ the process of protecting someone or something and providing what that person or thing needs:
* mira’s going to be very weak for a long time after the operation, so she’ll need a lot of care. used as a combining form: *skincare/healthcare/childcare.
TAKE CARE verb US/UK to protect someone or something and provide the things that that person or thing needs:
*take good care of that girl of yours, Patrick - she’s very special.
IN CARE (also take/put into care) UK children who are in care or who have been put into care are not living with their natural parents but instead with a national or local government organization or another family:
*both children were taken into care when their parents died. care in the community UK a system in which people with mental illness or reduced mental ability are allowed to continue living in their own homes, with treatment and help, and are not kept in the hospital:
*these people are supposed to be getting care in the community, but it’s just not happening.
*https://dictionary.cambridge.org/dictionary/english/care
43
EPIDEMIOLOGIA DEL TRAUMA CRANICO
44
EPIDEMIOLOGY OF TRAUMATIC BRAIN INJURY
45
[3]
/I paesi a basso e medio reddito sperimentano quasi tre volte più casi di lesioni cerebrali traumatiche in proporzione rispetto ai paesi ad alto reddito.*
Le differenze di lesioni cerebrali traumatiche legate all’età dimostrano tre principali gruppi di età con la più alta prevalenza:
°Prima infanzia (le cadute sono la causa principale)
°Tarda adolescenza / prima età adulta (gli incidenti stradali sono la causa principale)
°Anziani (le cadute sono la causa principale)
Di tutti i tipi di lesione, quelli al cervello sono tra quelle che hanno maggiori probabilità di provocare morte o invalidità permanente. La proporzione di lesioni cerebrali traumatiche derivanti da incidenti stradali è maggiore in Africa e Sud-est asiatico (entrambi 56%) e più bassa in Nord America (25%), mentre Sud America, Caraibi e Africa subsahariana rappresentano la più alta incidenza mondiale di lesioni traumatiche cerebrali legate alla violenza.**\
*Hyder, Wunderlich, Puvanachandra, Gururaj, Kobusingye. The impact of traumatic brain injuries: a global perspective. NeuroRehabilitation. 2007;22(5):341-53.
**https://www.physio-pedia.com/Epidemiology_of_Traumatic_ Brain_Injury
46
/The low and medium-income countries experience nearly three times more cases of traumatic brain injury proportionally than high-income countries* .
Age-related traumatic brain injury differences demonstrate three main age groups with the highest prevalence:
°Early childhood (falls being the main cause)
°Late adolescence / early adulthood (road traffic (RTAs) being the main cause)
°Elderly (falls being the main cause)
Of all types of injury, those to the brain are among the most likely to result in death or permanent disability. The proportion of traumatic brain injury resulting from road traffic collisions is greatest in Africa and Southeast Asia (both 56%) and lowest in North America (25%), while South America, the Caribbean and Sub Saharan Africa represent the highest world incidence of traumatic brain injury-related to violence.**\
*Hyder, Wunderlich, Puvanachandra, Gururaj, Kobusingye. The impact of traumatic brain injuries: a global perspective. NeuroRehabilitation. 2007;22(5):341-53.
**https://www.physio-pedia.com/Epidemiology_of_Traumatic_ Brain_Injury
47
IMAGING MEDICO
48
E LE SUE INTERPRETAZIONI
MEDICAL IMAGING AND ITS INTERPRETATIONS
[4] 49
È difficile definire il ruolo delle «immagini» prodotte dai dispositivi tecnologici di imaging medico quali TAC (Tomografia assiale computerizzata) e RM (Risonanza magnetica). L’obiettivo di un progetto di ricerca a più ampio spettro potrebbe essere quello di interrogare lo status di tali sistemi operativi, che possono essere definiti al contempo cibernetici che cognitivi. In quanto da un lato elaborati principalmente dal macchinario, che ricrea in forma visiva informazioni captate inizialmente sotto forma di dati, al contempo cognitivi in quanto ancora ad oggi fortemente dipendenti dallo sguardo formato del radiologo. Evidenziare tale dualità intende sottolineare quanto ancora una volta il paradigma uomo-macchina si riveli spesso fragile e sussista la necessità di proporre ipotesi maggiormente trasversali e interconnesse dei fenomeni percettivi. Queste vere e proprie “immagini in movimento”, fungono da principali mediatori insostituibili, nella triade tra medico,paziente e macchina. Un’ “immagine” che fungendo da interfaccia tra queste presenze si trova ad essere tanto più complessa quanto soggetta a molteplici interpretazioni, per dirlo con i termini di James Elkins «queste immagini sono schemata, una combinazione di scrittura, immagini e notazioni»*. In altre parole spettri bi-dimensionali, dalle mille sfumature di bianco e di nero; macchie che appaiono all’occhio inesperto tanto enigmatiche ed equivocabili quanto le gocce d’olio da cui un tempo si era soliti cercare risposte.
*Elkins, J., Two conceptions of the human form: Bernard Siegfried Albinus and Adreas Vesalius in Artibus et historiae, 14, 1986.
50
It is difficult to define the role of “images” produced by medical imaging technology devices such as CT (Computerized Axial Tomography) and MRI (Magnetic Resonance). The goal of a broader research project could be to question the status of these operating systems, which can be defined as both cybernetic and cognitive. As on the one hand processed mainly by the machine, which recreates in visual form information initially captured in the form of data, at the same time cognitive as still today strongly dependent on the trained gaze of the radiologist. Highlighting this duality intends to underline how once again the manmachine paradigm often turns out to be fragile and there is a need to propose more transversal and interconnected hypotheses of perceptual phenomena. These real “moving images” act as the main irreplaceable mediators in the triad between doctor, patient and machine. An “image” which, acting as an interface between these presences, is all the more complex as it is subject to multiple interpretations, to put it in James Elkins’ terms «these images are schemata, a combination of writing, images and notations»*. In other words two-dimensional spectra, with a thousand shades of black and white; spots that appear to the inexperienced eye as enigmatic and equivocal as the drops of oil from which it was once customary to seek answers.
*Elkins, J., Two conceptions of the human form: Bernard Siegfried Albinus and Andreas Vesalius in Artibus et historiae, 14, 1986.
51
#EROIDELLASANITÀ SOVRACCARICO DI LAVORO
52
¿ ¿ ¿
53 #HEALTHCAREHEROES WORK OVERLOAD [5] ¿ ¿ ¿
/Durante la pandemia di COVID-19, i media hanno ripetutamente elogiato gli operatori sanitari per il loro lavoro “eroico”. Sebbene questa gratitudine sia indubbiamente apprezzata da molti, dobbiamo essere cauti sull’uso eccessivo del termine “eroe” in tali discussioni. Le sfide attualmente affrontate dagli operatori sanitari sono persino maggiori di quelle incontrate nel loro normale lavoro, ed è comprensibile che sia stato evocato il linguaggio dell’eroismo per lodarli per le loro azioni. È importante capire cos’è l’eroismo e perché viene applicato attualmente agli operatori sanitari, prima di delineare alcuni dei problemi associati alla narrativa dell’eroismo attualmente impiegata dai media. Gli operatori sanitari hanno un chiaro e limitato dovere di cura durante la pandemia di COVID-19, che può essere fondato su un ampio contratto sociale ed è fortemente associato a determinati doveri reciproci che la società ha nei confronti degli operatori sanitari. L’eroismo come narrazione può essere dannoso, in quanto non riconosce l’importanza della reciprocità.*\
*Cox CL. ‘Healthcare Heroes’: problems with media focus on heroism from healthcare workers during the COVID-19 pandemic. J Med Ethics. 2020 Aug;46(8):510-513. doi: 10.1136/medethics-2020-106398. Epub 2020 Jun 16. PMID: 32546658; PMCID: PMC7316119.
54
/During the COVID-19 pandemic, the media have repeatedly praised healthcare workers for their ‘heroic’ work. Although this gratitude is undoubtedly appreciated by many, we must be cautious about overuse of the term ‘hero’ in such discussions. The challenges currently faced by healthcare workers are even greater than those encountered in their normal work, and it is understandable that the language of heroism has been evoked to praise them for their actions. It is important to understand what heroism is and why it is being applied to the healthcare workers currently, before outlining some of the problems associated with the heroism narrative currently being employed by the media. Healthcare workers have a clear and limited duty to treat during the COVID-19 pandemic, which can be grounded in a broad social contract and is strongly associated with certain reciprocal duties that society has towards healthcare workers. Heroism as a narrative can be damaging, as it fails to acknowledge the importance of reciprocity.*\
*Cox CL. ‘Healthcare Heroes’: problems with media focus on heroism from healthcare workers during the COVID-19 pandemic. J Med Ethics. 2020 Aug;46(8):510-513. doi: 10.1136/medethics-2020-106398. Epub 2020 Jun 16. PMID: 32546658; PMCID: PMC7316119.
55
IMPIANTI CRANICI SU MISURA
56
CUSTOM-MADE CRANIAL IMPLANTS
[6] 57
/Le protesi craniche custom-made specifiche per il paziente, sono progettate sul modello anatomico del paziente che viene ricreato dalle immagini della scansione TC. Pertanto, gli opercoli si adattano perfettamente all’anatomia del paziente, riempiono completamente un difetto, assicurano una fissazione stabile e ripristinano la simmetria estetica del cranio. Rispetto ad altre soluzioni di riempimento di difetti cranici, hanno una migliore funzionalità; riducono il rischio di complicanze, prevengono gli effetti collaterali e riducono la durata dell’intervento chirurgico e il periodo di riabilitazione. Gli impianti cranici specifici per il paziente sono fabbricati utilizzando la tecnologia di produzione additiva dalla lega di titanio di grado medico Ti6Al4V.*\
*http://balticimplants.eu/patient-specific-medical-devices/cranialimplants/
58
/Custom-made patient-specific cranial implants are designed on the patient’s anatomical model that is recreated from CT scan images. Thus, the implants adapt perfectly to the patient’s anatomy, completely fill a defect, ensure stable fixation and restore the aesthetic symmetry of the skull. Compared with other cranial defect filling solutions, they have better functionality; they reduce the risk of complications, prevent side effects and shorten the duration of surgery and the rehabilitation period. The patientspecific cranial implants are manufactured using additive manufacturing technology from the medical grade titanium alloy Ti6Al4V.*\
*http://balticimplants.eu/patient-specific-medical-devices/cranialimplants/
59
Nel caso di mia sorella l’impianto è stato prodotto dalle immagini TC del cranio fratturato, un modello CAD costruito digitalmente. Dal momento dell’ordine effettuato con cura e precisione l’opercolo personale é arrivato circa tre settimane dopo. Il pezzo unico riporta le iniziali del cognome Waldmann ovvero WAL che si possono intravedere nelle RX. In quanto familiari non sappiamo chi é stato precisamente l’operatore o l’impresa che hanno prodotto il pezzo ma a loro va tutta la nostra gratitudine. Lavoratori dell’ombra hanno dato anche loro un importante contributo. In quanto designer è affascinante pensare che questi pezzi vengono creati usando il software Rhino Medical che funziona in modo molto simile a quello utilizzato per creare numerosi pezzi di design in 3D. Infine la strada che ha portato ogni singola particella di titanio a far parte integrante del corpo di mia sorella ha probabilmente avuto origine nei siti di estrazione in Australia, Sierra Leone, Sud Africa, Russia e Giappone**, da una parte generosa ed consumata della crosta terrestre.
**Shunyu Liu,Yung C. Shin, Additive manufacturing of Ti6Al4V alloy: A review, Materials & Design, Elsevier, 15 February 2019.
60
In my sister’s case the implant was produced from CT images of the fractured skull, a digitally constructed CAD model. From the moment of the order, placed with care and precision, the personal operculum arrived about three weeks later. The unique piece bears the initials of the surname Waldmann or WAL which can be glimpsed in the RXs. As family members we do not know who exactly was the CADoperator or the company that produced the piece but all our gratitude goes to them. Workers outside the frontline that also make important contributions. As a designer it is fascinating to think that these pieces are created using the Rhino Medical software which works very similarly to that used to create 3D models for buildings and everyday objects. Finally, the path that led every single particle of titanium to become an integral part of my sibling’s body probably originated in the extraction sites in Australia, Sierra Leone, South Africa, Russia and Japan.*
*Shunyu Liu,Yung C. Shin, Additive manufacturing of Ti6Al4V alloy: A review, Materials & Design, Elsevier, 15 February 2019.
61
AFASIA SENSORIALE
62
SENSORIAL APHASIA
[7] 63
/L’afasia è una compromissione della comprensione o della formulazione del linguaggio causata da un danno al centro corticale del linguaggio. L’area linguistica del cervello si trova tipicamente nell’emisfero dominante. Le Sindromi specifiche dell’afasia dipendono dalla posizione della lesione nel cervello. Nell’afasia fluente, il paziente può pronunciare frasi che suonano come un discorso normale, ma alcune delle parole sono parole inventate o hanno alcuni suoni che non sono corretti.* Recenti studi clinici hanno evidenziato che i pazienti bilingue affetti da afasia riacquistano in modo relativamente veloce la capacità di parlare e di comunicare con la loro lingua madre; la seconda lingua, invece, è più difficilmente recuperata.** Comprendere la natura del recupero del linguaggio nell’afasia è una delle questioni fondamentali e importanti in quanto influisce sulla diagnosi, sul trattamento e sulla prognosi dei pazienti con afasia. Un corpus significativo di ricerche ha enumerato la natura del recupero del linguaggio nelle fasi acuta, subacuta e cronica; ad esempio, Kiran e Thompson (2019) hanno esaminato i meccanismi neuroplastici sottostanti che supportano i cambiamenti cerebrali correlati al trattamento.***\
*Le H, Lui Y. Aphasia. 2022 Apr 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 32644741.
**https://www.my-personaltrainer.it/benessere/afasia-terapia.html
***Neuroplasticity in Aphasia: A Proposed Framework of Language
Recovery Swathi Kiran, Erin L. Meier and Jeffrey P. Johnson. Journal of Speech, Language and Hearing research. November 2019.
64
/Aphasia is an impairment of comprehension or formulation of language caused by damage to the cortical center for language. The language area of the brain is typically located in the dominant hemisphere. Specific aphasia syndromes are dependent on the location of the lesion in the brain. In fluent aphasia, the patient can speak in sentences that sound like normal speech, but some of the words are madeup words or have some sounds that are not correct.* Recent clinical studies have shown that bilingual patients with aphasia regain the ability to speak and communicate in their native language relatively quickly; the second language, on the other hand, is only difficult to recover.**
Understanding the nature of language recovery in aphasia is one of the fundamental questions in aphasia research as it impacts the diagnosis, treatment, and prognosis of patients with aphasia (PWA). A significant body of research has enumerated the nature of language recovery in the acute, subacute, and chronic phases of aphasia; for instance, Kiran and Thompson (2019) have reviewed the underlying neuroplastic mechanisms supporting treatment-related changes in the brain.***\
*Le H, Lui Y. Aphasia. 2022 Apr 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 32644741.
**https://www.my-personaltrainer.it/benessere/afasia-terapia.html
***Neuroplasticity in Aphasia: A Proposed Framework of Language Recovery Swathi Kiran, Erin L. Meier and Jeffrey P. Johnson. Journal of Speech, Language and Hearing research. November 2019.
65
LA CHIRURGIA COME PERFORMANCE
66
SURGERY AS A PERFORMACE
[8] 67
L’apprendistato è stato da sempre alla base dell’insegnamento medico e chirurgico. Talora i professionisti della medicina considerano la loro pratica quasi un’arte - l’arte della guarigione. Fu il filosofo tedesco Hans-Georg Gadamer (1900 – 2002) trani più ferventi sostenitori che i medici non sono artisti, e che solo la natura può esserlo*. D’altro canto, facciamo appello ai medici per riposizionare e riparare gli artefatti danneggiati da un incidente o dalla semplice usura. Forse sarebbe più appropriato vedere i medici come degli artigiani. Eppure In termini di prestigio, esiste una gerarchia nella medicina contemporanea che pone la chirurgia al vertice. Questo potrebbe essere dovuto al fatto che, se è vero che si può sempre chiedere una seconda opinione per una terapia, ciò è meno facile nel caso di un’operazione durante la quale é solo ad un paio o massimo quattro mani che affidiamo tutta una vita. Lo facciamo in parte perché non abbiamo scelta, qualcuno dovrà farlo e non basterebbero tutti i tutorial del mondo perché serve oltre a tutto il resto anche e soprattutto la pratica in situ. Ci affidiamo anche perché qualcosa in noi ci dice che possiamo fidarci. Ma soprattutto perché crediamo che come ogni grande performer nel chirurgo risieda quell’insieme straordinario di talento, perfetta padronanza dello strumento e capacità di esibirsi quando necessario. La chirurgia è arte di prim’ordine e uno sport agonistico al contempo.
*Clark J. Philosophy, understanding and the consultation: a fusion of horizons. Br J Gen Pract. 2008 Jan;58(546):58-60. doi: 10.3399/bjgp08X263929. PMID: 18187004; PMCID: PMC2148246.
68
The apprenticeship has always been the basis of medical and surgical teaching. Sometimes medical professionals consider their practice almost an art - the art of healing. The German philosopher Hans-Georg Gadamer (1900 – 2002) was among the most fervent supporters that doctors are not artists, and that only nature can create*. On the other hand, we call doctors to reposition and repair artifacts damaged by an accident or simple weared out. Perhaps then it would be more appropriate to see doctors as artisans. Yet In terms of prestige, there is a hierarchy in contemporary medicine that places surgery at the top. This could be due to the fact that, if it is true that you can always ask for a second opinion for a therapy, this is less easy in the case of an operation during which it is only to a couple or at most four hands that we entrust life. We do it in part because we have no choice, someone will have to do it, knowing that all the tutorials in the world would not be enough because in addition to everything else we need also and above all the practice in situ. We entrust because something in us tells us we should and can. But above all because we believe that like any great performer, in the surgeon resides that extraordinary combination of talent, perfect command of the instrument and ability to perform when necessary. Surgery is art of the highest order and an olympic sport at the same time.
*Clark J. Philosophy, understanding and the consultation: a fusion of horizons. Br J Gen Pract. 2008 Jan;58(546):58-60. doi: 10.3399/bjgp08X263929. PMID: 18187004; PMCID: PMC2148246.
69
CHI SI PRENDERÀ CURA DEI CAREGIVERS?
70
WHO WILL CARE FOR THE CAREGIVERS?
[9] 71
/Avrei dovuto rimettergli i calzini. Il pensiero continuava a tormentarmi mentre finivo i miei appunti clinici. Il mio ultimo paziente della giornata - un uomo con demenza - è stato aggiunto in ritardo al programma, dopo che sua figlia, lei stessa una mia paziente, ha chiamato. L’abbiamo programmato per l’ultimo appuntamento, in modo che potesse unirsi dopo aver finito di lavorare. Ha raccontato i sottili cambiamenti che aveva notato. Mangiava di meno, dormiva di più, era meno stabile in piedi. Dalla sua borsetta, ha tirato fuori non meno di otto flaconi di pillole, ciascuno con una dose e una frequenza meticolosamente etichettate. Mi ha consegnato una trascrizione delle sue altre nomine recenti: un oftalmologo, un neurologo, un cardiologo. Mentre lo esaminavo, il suo telefono squillò. «Il nonno non si sente bene, tesoro» disse. «C’é della lasagna in frigo. Presto saremo a casa.» Riattaccò e si scusò per l’interruzione. Poi si sporse per infilargli i calzini sui piedi nudi, calzini che avevo tolto pochi istanti prima e lasciato sul lettino.
Avrei dovuto rimettergli i calzini.*\
*https://www.nytimes.com/2017/01/19/upshot/who-will-care-forthe-caregivers.html
72
/I should have put his socks back on.
The thought kept nagging me as I finished my clinic notes, replaying the afternoon in my head. My final patient of the day — a man with dementia — was a late addition to the schedule, after his daughter, herself a patient of mine, called to report he hadn’t been himself lately. We scheduled him for the last appointment, so she could join after finishing work across town. She recounted the subtle changes she’d noticed. He’d been eating less, sleeping more, he was less steady on his feet. From her purse, she pulled out no fewer than eight pill bottles — each with a dose, and frequency meticulously labeled. She handed me a transcript of his other recent appointments: an ophthalmologist, a neurologist, a cardiologist. As I examined him, her phone rang. “Grandpa isn’t feeling well, sweetie,” she said. “There’s macaroni in the fridge. We’ll be home soon.” She hung up and apologized for the interruption. Then she leaned over to pull his socks over his bare feet — socks I’d removed moments before and left on the exam table.
I should have put his socks back on.”*\
*https://www.nytimes.com/2017/01/19/upshot/who-will-care-forthe-caregivers.html
73
Sono più di 30 milioni i casi in america che ricordano questo. Sono casi di figure che aiutano a tutte le task del quotidiano da prepararsi da mangiare a lavarsi o badare alle medicine un membro della propria famiglia o un vicino di casa. Uno studio della National Alliance for Caregiving, ldipinge il ritratto del caregiver come di sesso femminile intorno alla cinquantina che si occupa di una persona più anziana di lei. Ciononostante ormai un quarto dei caregivers appartengono alla generazione millenial e sono di sesso sia maschile che femminile in equa misura. Purtroppo il fabbisogno in questo settore non smette di aumentare in parte grazie alla maggiore aspettativa di vita in parte perché la forza lavoro, anche volontaria va man mano riducendosi. Le famiglie hanno dimensioni minori e le distanze loro diventano sempre maggiori. Dieci anno fa c’erano 6/7 caregiver all’interno della famiglia, anche estesa, ogni persona over ottanta. Tra dieci anni questo numero dovrebbe aggirarsi tra 3/4 per ogni senior americano.
74
There are more than 30 million cases in America that recall this. These are cases of figures who help a member of one’s family or a neighbor with all the daily tasks from preparing food to washing or taking care of medicines. A study by the National Alliance for Caregiving paints the portrait of the caregiver as a female in her 50s caring for an older person. Nonetheless, now a quarter of caregivers belong to the millennial generation and are equally male and female. Unfortunately, the need in this sector continues to increase partly thanks to the higher life expectancy and partly because the workforce, even voluntary, is gradually decreasing. Families are smaller and their distances are getting bigger and bigger. Ten years ago there were 6/7 caregivers within the family, even extended ones, each person over eighty. Ten years from now, this number should be around 3/4 for every American senior.
75
/I caregiver familiari hanno maggiori probabilità di sperimentare effetti negativi sulla salute come ansia, depressione e malattie croniche. Uno studio ha rilevato che coloro che hanno sperimentato stress mentale o emotivo mentre si prendevano cura di un coniuge disabile avevano il 63% in più di probabilità di morire entro quattro anni rispetto ai non caregiver che sono stati anche monitorati. Un altro studio ha rilevato che i caregiver a lungo termine hanno interrotto il sistema immunitario anche tre anni dopo la fine del loro ruolo di caregiver. E caregiver di pazienti con lunga terapia intensiva. i ricoveri hanno alti livelli di sintomi depressivi che possono durare più di un anno. I sistemi sanitari, sotto pressione per ridurre i costi, fanno sempre più affidamento su di loro per gestire le malattie a casa.*\
*https://www.nytimes.com/2017/01/19/upshot/who-will-care-for-the-caregivers.html
76
/Family caregivers are more likely to experience negative health effects like anxiety, depression and chronic disease. One study found that those who experienced mental or emotional stress while caring for a disabled spouse were 63 percent more likely to die within four years than noncaregivers who were also tracked. Another study found that long-term caregivers have disrupted immune systems even three years after their caregiving roles have ended. And caregivers of patients with long I.C.U. stays have high levels of depressive symptoms that can last for more than a year. Health systems, under pressure to reduce costs, increasingly rely on them to manage illness at home.*”\
*https://www.nytimes.com/2017/01/19/upshot/who-will-care-for-the-caregivers.html
77
HOGEWEYK, IL PRIMO DEMENTIA VILLAGE
HOGEWEYK, THE FIRST DEMENTIA VILLAGE
[10]
/De Hogeweyk, nei Paesi Bassi, potrebbe sembrare stranamente familiare, anche se non ci sei mai stato. Inaugurato nel 2009, il primo villaggio per la demenza al mondo cerca di creare una nostalgia per un luogo in cui i residenti potrebbero non essere mai stati, ma che hanno sempre voluto chiamare casa. Basato sul potere dell’architettura di evocare ricordi forti, De Hogeweyk è stato progettato dagli architetti olandesi Molenaar&Bol&VanDillen per fornire un ambiente confortevole, sicuro e persino curativo per coloro che soffrono di perdita di memoria, cambiamenti di personalità e compromissione del ragionamento spesso associato a demenza avanzata. De Hogeweyk comprende appartamenti, case, ristoranti, negozi, un teatro e giardini. Da quando è stato aperto, 152 pazienti/ residenti affetti da demenza l’hanno chiamato casa e sono stati costruiti dozzine di villaggi di demenza seguendo il modello Hogeweyk. Il villaggio della demenza ci racconta molto della società occidentale. Ci dice che vediamo ancora il “villaggio” come un ambiente premuroso, nonostante il fatto che pochi di noi abbiano mai vissuto in un villaggio. Rivela anche la nostra profonda paura di malattie gravi sopratutto se interessano le facoltà cognitive.*\ più ampia nella progettazione ospedaliera degli ultimi quar
*https://www.e-flux.com/architecture/treatment/410336/deception-and-design-the-rise-of-the-dementia-village/
80
/De Hogeweyk in the Netherlands might look eerily familiar, even if you’ve never been there. Opened in 2009, the world’s first dementia village seeks to create a nostalgia for a place residents may never have been, but have always wanted to call home. Based on the power of architecture to evoke strong memories, De Hogeweyk was designed by Dutch architects Molenaar&Bol&VanDillen to provide a comfortable, safe and even healing environment for those suffering from memory loss, personality changes and impaired reasoning often associated with dementia advanced. De Hogeweyk comprises apartments, houses, restaurants, shops, a theater and gardens. Since it opened, 152 dementia patients/residents have called it home and dozens of dementia villages have been built following the Hogeweyk model. The village of dementia tells us a lot about Western society. It tells us that we still see the “village” as a caring environment, despite the fact that few of us have ever lived in a village. It also reveals our deep fear of serious diseases especially if they affect the cognitive faculties.*\
*https://www.e-flux.com/architecture/treatment/410336/deception-and-design-the-rise-of-the-dementia-village/
81
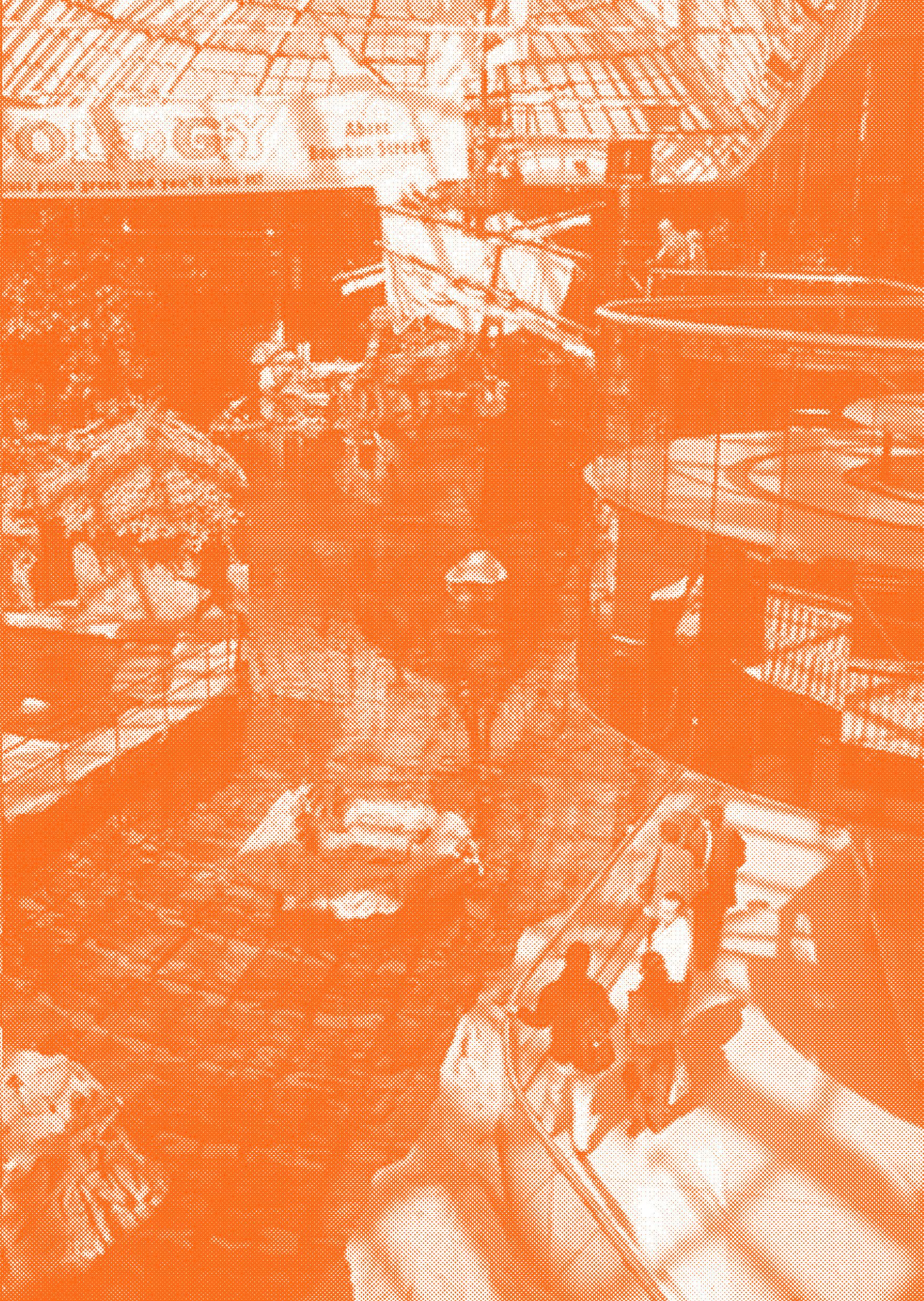
/Il villaggio della demenza mostra una tendenza più ampia nella progettazione ospedaliera degli ultimi quarant’anni: l’esigenza di camuffare malattie gravi realizzando ambienti sanitari che simulano altri tipi di edifici. Dagli anni ‘80, gli ospedali sono diventati sempre più simili a centri commerciali o aeroporti. Alcuni sembrano hotel di lusso o spa. Il Walter Mackenzie Hospital di Edmonton, Alberta, ad esempio, un antico ospedale ad atrio, sembra stranamente simile al vicino West Edmonton Mall, uno dei più grandi centri commerciali del Nord America. Mentre gli storici della medicina sottolineano l’influenza della cosiddetta cura centrata sul paziente e l’ascesa del design basato sull’evidenza per questa tendenza ospedaliera, l’ospedale come centro commerciale riguarda in realtà la normalizzazione della malattia.*\
*https://www.e-flux.com/architecture/treatment/410336/deceptionand-design-the-rise-of-the-dementia-village/
82
/The dementia village showcases a wider trend in hospital design over the past forty years: the urge to camouflage serious illness by making healthcare environments that simulate other building types. Since the 1980s, hospitals have come to look more and more like shopping malls or airports. Some look like luxury hotels or spas. The Walter Mackenzie Hospital in Edmonton, Alberta, for instance, an early atrium hospital, looks uncannily similar to the nearby West Edmonton Mall, one of the largest malls in North America. While medical historians point to the influence of so-called patient-centered care and the rise of evidence-based design for this hospital trend, the hospital-as-mall is really about normalizing illness.*\
*https://www.e-flux.com/architecture/treatment/410336/deceptionand-design-the-rise-of-the-dementia-village/
83
How can Care be a pathway towards more sustainable forms of production and consumption?

85
Dispositivi Protezione Individuale

86

87
Detail from neck XR, courtesy Katharine Thomas Waldmann

88

89
90
Anima sf anima, -ae; spiritus, -ūs sm ◊

91
92
BIBLIOGRAFIA / BIBLIOGRAPHY
93
https://www.nytimes.com/2010/10/15/books/15book.html
https://www.e-flux.com/architecture/treatment/410336/deception-anddesign-the-rise-of-the-dementia-village/
https://www.e-flux.com/architecture/treatment/410336/deception-anddesign-the-rise-of-the-dementia-village/
https://dictionary.cambridge.org/dictionary/english/care
https://www.gsd.harvard.edu/publication/delirious-new-york-aretroactive-manifesto-for-manhattan-1/
https://www.gsd.harvard.edu/publication/delirious-new-york-aretroactive-manifesto-for-manhattan-1/
Hyder, Wunderlich, Puvanachandra, Gururaj, Kobusingye. The impact of traumatic brain injuries: a global perspective. NeuroRehabilitation. 2007;22(5):341-53.
https://www.physio-pedia.com/Epidemiology_of_Traumatic_Brain_ Injury
Elkins, J., Two conceptions of the human form: Bernard Siegfried Albinus and Andreas Vesalius in Artibus et historiae, 14, 1986.
Cox CL. ‘Healthcare Heroes’: problems with media focus on heroism from healthcare workers during the COVID-19 pandemic. J Med Ethics. 2020 Aug;46(8):510-513. doi: 10.1136/medethics-2020-106398. Epub 2020 Jun 16. PMID: 32546658; PMCID: PMC7316119.
http://balticimplants.eu/patient-specific-medical-devices/cranialimplants/
Shunyu Liu,Yung C. Shin, Additive manufacturing of Ti6Al4V alloy: A review, Materials & Design, Elsevier, 15 February 2019.Le H, Lui Y. Aphasia. 2022 Apr 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 32644741.
https://www.my-personaltrainer.it/benessere/afasia-terapia.html
94
Neuroplasticity in Aphasia: A Proposed Framework of Language
Recovery Swathi Kiran, Erin L. Meier and Jeffrey P. Johnson. Journal of Speech, Language and Hearing research. November 2019.
Clark J. Philosophy, understanding and the consultation: a fusion of horizons. Br J Gen Pract. 2008 Jan;58(546):58-60. doi: 10.3399/ bjgp08X263929. PMID: 18187004; PMCID: PMC2148246.
https://www.nytimes.com/2017/01/19/upshot/who-will-care-for-thecaregivers.html
https://www.nytimes.com/2017/01/19/upshot/who-will-care-for-thecaregivers.html
https://www.e-flux.com/architecture/treatment/410336/deception-anddesign-the-rise-of-the-dementia-village/
https://www.e-flux.com/architecture/treatment/410336/deception-anddesign-the-rise-of-the-dementia-village/
95
The project was presented as part of the program MOVIES - Moving Images Arts www.mov-ies.eu
ANISOCORIA ANISOCORIA