CLINICAL LEARNING & DEVELOPMENT Contracted Staff Hospice Aide Orientation Agency_HA_01/24/22

2
OUR PURPOSE Reimagining care, together. OUR VISION We imagine a world where: • Patients and Clients receive the understanding, empathy, and excellence they deserve. • Families experience compassionate support from a trusted guide at each step. • Team Members grow, thrive, and find inspiration in a supportive work environment. • Communities and Strategic Partners succeed with the help of a comprehensive and responsive partner. OUR VALUES Act with integrity. Be Commitcompassionate.toexcellence. 3
This is used to communicate visits to other team members.
1. Review to see comments from other disciplines.
2. Complete the next available section with a brief summary of your visit.
SH 106 1 (11 08 16)
D scip ine: RN LPN SW CHAP MT HCC PCL HA Hospice visit made today VOL AT S gn ficant findings or new orders: S gnature: Tit e: Da e: Note p aced n chart D scip ine: RN LPN SW CHAP MT HCC PCL HA Hospice visit made today VOL AT S gn ficant findings or new orders: S gnature: Tit e: Da e: Note p aced n chart
HOSPICE VISIT COMMUNICATION
ACES
3. Be sure to sign and date your note.
DOCUMENTATIONPAPER
HOSPICE VISIT COMMUNICATION www seasons org
4
Your site will provide you with a Steps for Success Document that will yourinformationnumbersimportantincludephoneandaboutteam.
Pa ient Name (Las First Midd e D # D scip ine: RN LPN SW CHAP MT HCC PCL HA Hospice visit made today VOL AT S gn ficant findings or new orders: S gnature: Tit e: Da e: Note p aced n chart
• Equipment-cleaning wipes are removed to clean all patient care items before replacing in bag.
5
Care of bag: Replace equipment/supplies as needed to maintain bag stock. Remove all equipment/supplies at least once yearly and thoroughly disinfect bag. Wash outside and inside of bag as needed and when visibly soiled.
• Patient’s right to privacy protected while hand washing & removing items from bag (patient kept covered until ready to provide care).
Inside of bag and contents are considered clean.
BAG TECHNIQUE
• Wash or gel hands before entering bag, and then each time prior to re-entering bag.
• Items removed from bag are placed on a clean dry surface (paper towel, newspaper, etc.). When the surface is not dry, a non-porous barrier is recommended.
Bag use.notwhenclosedisin
• Patient care instruments including computer are disinfected before they are returned to the bag.
Sharps containers are NOT carried inside supply bag. Bag transported in clean area of car and out of site (locked in trunk). Bag removed from car at end of day (extreme temperatures may cause damage to bag contents). Bag kept out of reach of children.
Keep Them Separate Multi-use items should be kept in a separate section of the bag from single-use items (such as alcohol swabs, barrier/paper towel/ chucks, gloves, etc.). Computer and personal items should be kept in a different area than these two. A Safe Space Bag is placed on protective surface in patient care areas or has wheels that keep it off the floor (bag may be suspended off floor by hanging on a door knob).



























































Professional BoundariesGait Belt Transfer Hoyer Lift Instruction Gait Belt Safety Watch The Gait Belt Safety Video Watch The BoundariesProfessionalVideoWatch The Gait Belt Transfer Video Watch The Hoyer Lift Instruction Video HA VIDEO RESOURCES Bag Technique Watch The Bag Technique Video Your site will provide you with a Steps for Success Document that will include important phone numbers and information about your team. 6
The RN will create the plan of care based on the patient assessment and the patient/family goals of care. RN will: • Review HA documentation, assess HA concerns and related patient needs, and direct the HA accordingly to allow completion of the visit.
• If it’s determined that the patient’s care is complicated, the nurse will make the initial visit with the hospice aide and instruct them on the care.
•
•
• Make a supervisory visit at least every 14 days to assess the quality of care and services provided. The hospice aide does not need to be present during the supervisory visit but is preferred.
• Help individualize and guide personal care for each patient by reporting changes or patient preferences to the RN. Report concerns or changes in condition to the RN or team director. If the Plan of Care cannot be followed: Contact RN, Team Director or RN Supervisor. Document that you were not able to complete this task, including the reason.
• No plan of care available to view.
• Review the plan of care before every visit, allowing it to guide the visit.
•
•
Examples of why care plan can’t be followed:
• Patient or family wants bed bath instead of shower. Patient or family wants less visits then ordered.
Seasons Protocol 2112: Aide Plan of Care: Coordination, Documentation & Supervision
• Ensure personal care services are provided under the supervision of the RN. Deliver care as directed by the plan of care
• The supervising nurse will assess an aide’s ability to demonstrate satisfactory performance including: - Following the patient’s plan of care - Creating successful interpersonal relationships with the patient and family Demonstrating competency with assigned tasks - Complying with infection control policies and procedures - Reporting changes in the patient’s condition
7
• Patient refused visit. Only part of care can be completed.
•
Responsibility of hospice aide:
• Make changes to the Aide POC in the EMR within 24 hours.
•
HA PLAN OF CARE
• Patient’s brother was yelling and jumping up and down in the living room. I notified the hospice nurse. Avoid labeling the patient/caregiver/family:
• Mary is different today.
Document what is observed/heard
• Susan sighed heavily and spoke to Martin in a loud tone of voice. • Martin shrugged his shoulders and said I will try harder. Avoid documenting your opinion
Document what is observed/heard/felt/smelled:
• Paul is coughing and says it is hard to breathe. I notified the hospice nurse. Avoid diagnosing the patient: • I think patient has a lung infection.
• Mr. Moore did not try to hit me today when I was helping with his shoes. Avoid vague statements • John is emotional.
HA
Be specific:
• Mr. Smith’s appetite is improved.
• Susan swore and spoke to Martin in a loud tone of voice.
Document why patient is improving & the impact of hospice interventions on quality of life:
DO DON’T
Document what is observed/heard/felt/smelled:
• Mr. Moore was good today.
• Susan was upset with Martin
Avoid statements that don’t include details or paint a picture
• Ms. Ely is doing great!
• Mary slept through my visit today. She didn’t say goodbye.
• Bobby was crying and shaking his head. He went into the bedroom and closed the door.
• Mr. Smith is eating 100% of his breakfast meal because I feed him slowly and it takes 45 minutes for him to eat.
BESTDOCUMENTATIONPRACTICES
• John cried when his son left to fly home. He stated “I know I won’t live to see him again.”
Describe patient’s actions, statements & behaviors:
• Bobby wanted to be alone.
• Mr. Jones found asleep in bed. I gave personal care. Patient left in dining room.
Document words/statements which are not contradictory to terminal status:
• Martin didn’t seem to care.
Describe the actual behavior and events:
• Ms. Ely reports pain is a 2 on 1-10 scale and she is sleeping better. Avoid words that do not accurately reflect the patient’s status:
• Mr. Jones found asleep in bed. Bed bath provided. He was unable to assist with bathing or transfer to wheelchair. I took him to the dining room and reported to the facility RN.
• His brother was acting crazy.
** Always notify the TD with changes in the patient’s status. If patient resides in a facility, also notify the facility RN. 8
Early stage Mild cognitive decline – recent memory loss, difficulty with word-finding, organizing, working. Some lack of judgment, depression. Middle stage Reduced memory of personal history, difficulty planning events and paying bills, may seem subdued or withdrawn, disoriented to place and time, depression.
Alzheimer’s Disease: Caused by damage to brain cells that lead to cell death. Fronto-temporal Dementia: Caused by degeneration of the frontal and temporal lobes.
• Irreversible loss of cognitive function. • Diagnosis is based on clinical tests and findings.
What is Dementia?
Dementia Stages
9
Lewy Body Dementia: Caused by abnormal deposits of protein (alpha-synuclein) inside the brain’s nerve cells.
NAMASTE
Late Stage Depression, patient can no longer speak, groaning, teeth clenching, withdrawn, Increased confusion and agitation.
Specialized Hospice Care for Patients with Advanced Dementia Types of Dementia

Special Care Goals • Promotion of sensory stimulation to evoke feelings of comfort • Create a calm and relaxing environment • Person-centered approaches personalized for each patient • Teach loved ones’ ways to interact with the person with advanced dementia • Support caregivers by enhancing the support team Respect for Individuality Understanding them… • Lifestyle sensoryAppraisalPreferencesidentifiespreferences • Completed by caregivers with assistance from nurses, social workers, CNAs, and Volunteers • Basis for care planning of all disciplines Knowing them… • Family and work history • preferredNicknames/name • Hobbies • Leisure activities • Daily routine • Last wishes Providing Care • Everyone who visits a patient with dementia can and should provide Namaste Care. • Promoting comfort, relaxation, and gentle touch is all of our responsibilities. Namaste care is: BatheUnrushedinbed - Ensure comfortable positioning - Soaking Massaginghands/feetwithlavender lotion - Gentle hair combing - Gentle mouth care Make presenceyourknown. Greet patient – eye level, warm smile, soft voice. Close aroundcurtainsbedside and use lavender spray. Play calming music. Engage staff to understand patient's plan of care. 10




THE HOSPICE BELIEF
THE HOSPICE REQUEST
“Alzheimer’s From the
Inside Out” ~ Richard Taylor Extra Special Touches NATURAL SCENTS - EucalyptusLavender - Lemon - LilacOrange - Fresh cut grass - Evergreen (juniper) QUILTS OR CLOTHING FROM -MATERIALSSOFT/LIGHTHOME Bubbles, boas, stuffed animals -REMINISCENCEINDIVIDUAL Talking about life memories Other patients to include Late stage Parkinson’s Disease DepressedAgitatedEmphysemaresidentsresidents with other diseases or ChildrenFailureconditionstothrivewhohave sensory deficits Positive Outcomes PATIENT • qualityImprovedof life • Comfort • Relaxation FAMILY • communicationImproved • satisfactionImproved FACILITY STAFF • andCollaborationsupport • Calmer, patientsmanageablemore Watch NamasteTheVideo 11
We are born into a world of comfort, warmth and love and it is our belief that we should all leave the world in the same way.
“Please consider and reconsider these concerns of mine: Everyone living with Alzheimer’s disease is and will be until the moment of their death, a whole and complete human being. Every day of my life I will be, in my own mind Richard. I am neither half-full or half-empty. I am Richard. I am not fading away. Will you always treat me as Richard? Or will there come a time when I am seen as Richard’s shell? I want and need to give and receive love. Even when I can’t remember your name, will you please love me?”
“We promise to enhance the quality of time by ensuring that neither pain or declining symptoms will diminish the character of a patient’s remaining days, weeks or months.”
THE HOSPICE PROMISE
If you feel your patient is thinking of harming themselves, ask them: “Are you thinking of killing yourself?” If they say yes, stay with the patient and call the RN or Team Director immediately. The more of these signs a person shows, the greater the risk. Warning signs are associated with suicide but may not be what causes a suicide.
Acting anxious, agitated or recklessly Sleeping too much or too little
Review Protocol 2111 Suicide Risk Assessment
Looking for a way to kill oneself
Talking about being a burden to others
Suicide Warning Signs
Talking about feeling hopeless or having no purpose
Displaying extreme mood swings
Talking about feeling trapped or in unbearable pain
12
SUICIDE ASSESSMENTRISK
If you recognize any of the following warning signs in your patient, report to your manager immediately:
Withdrawing or feeling isolated Showing rage or talking about seeking revenge
Talking about wanting to die
Presence of a gun or other dangerous weapon
Provided in hospice house or at nursing facility
Family/caregivers provide custodial care to patient
This higher level of care is utilized when a patient has an uncontrolled symptom or symptoms that was not manageable under routine level of care
95% of patients are on routine hospice care Patients are either at home, a nursing facility, or an assisted living facility (ALF)
GENERAL INPATIENT LEVEL OF CARE
Strict requirements-minimum coverage of 8 hours required for billing - Hospice staffing - Patient appropriateness - Cannot be used instead of custodial care Documentation should be at least hourly and should demonstrate the ongoing need for continuous care
Hospice team members will make visits to patient according to their individualize plan of care
CONTINUOUS CARE LEVEL OF CARE
13
Family gets “time off” and break
ROUTINE LEVEL OF CARE
RESPITE LEVEL OF CARE
Typically provided at a Seasons Inpatient Unit (IPC), Hospice House, or in contract beds at hospitals or nursing homes Patient must need skilled nursing care and not simply custodial care No cap on number of days they can stay but must meet criteria daily
Level of care may be changed with a physician order at any time during patient’s hospice stay based upon their condition
LEVELS OF CARE
Provides custodial care to patients
Lasts until the symptoms are managed, typically less than a Providedweekathome or nursing home Hospice provides 24 hour help at home provided by HHA, LPN, and RN
Limits 5 days per stay
Patient does not meet requirement for GIP or continuous care
This higher level of care is utilized when a patient has an uncontrolled symptom or symptoms that cannot be managed in any other setting
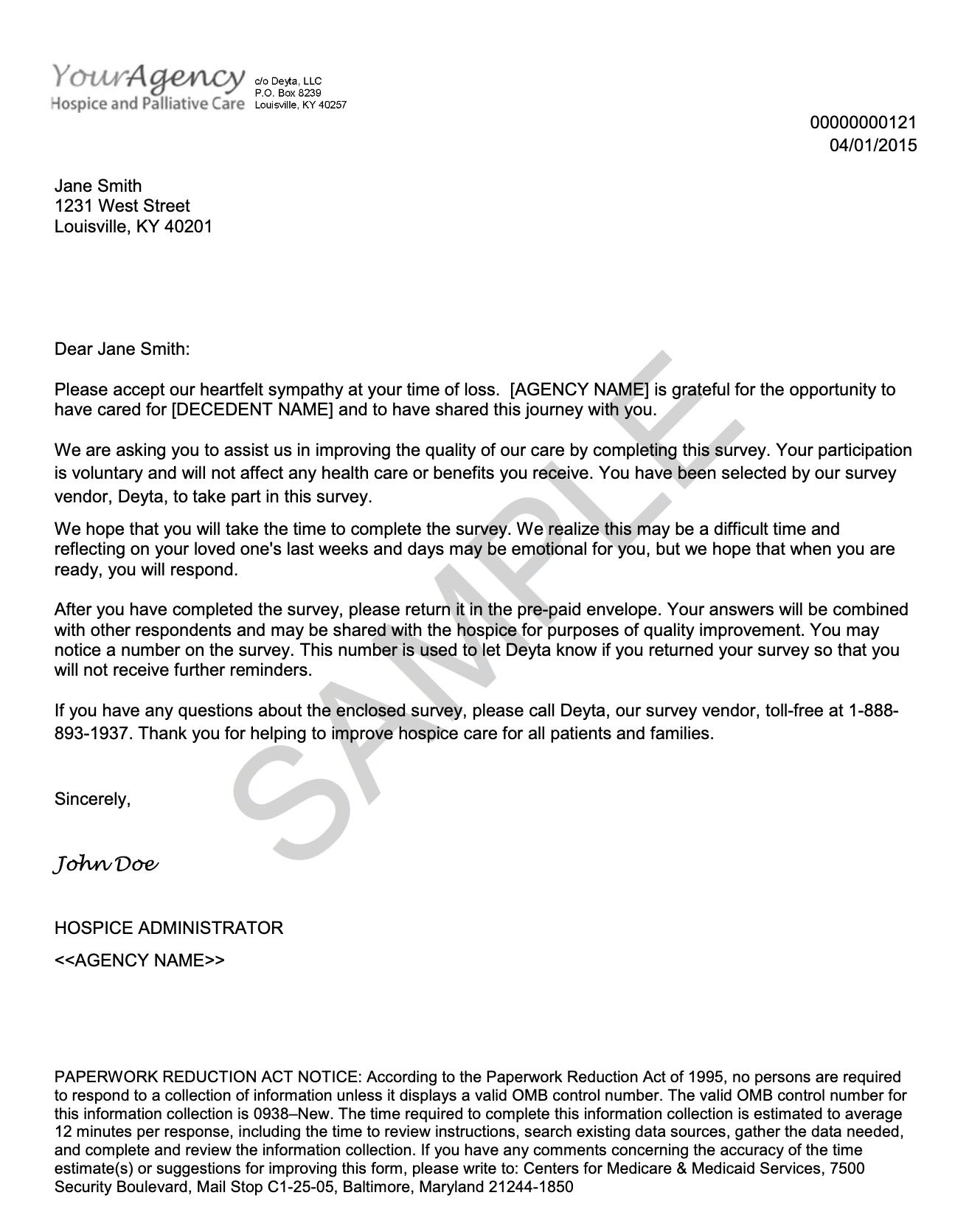
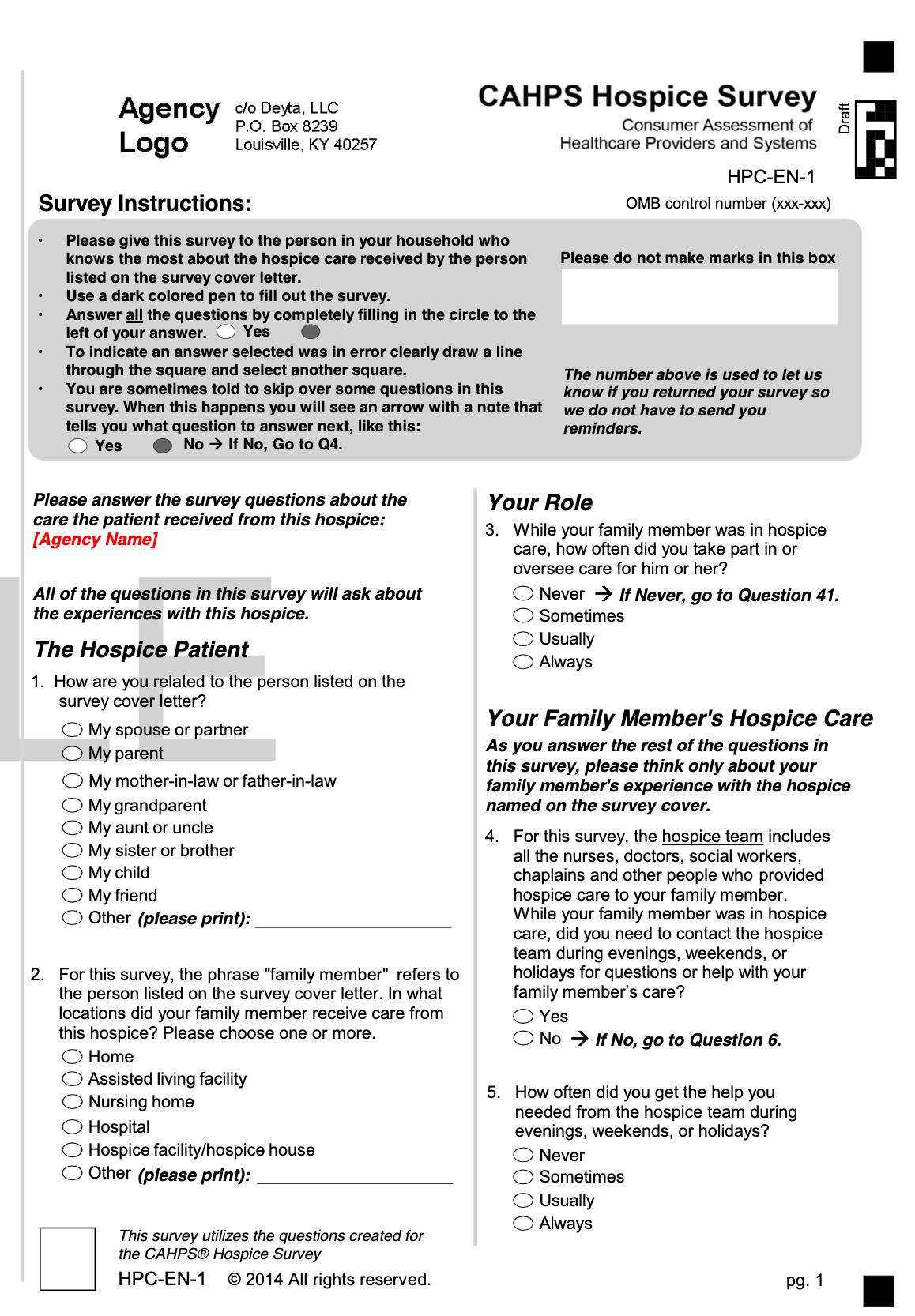
Consumer Assessment Of Healthcare Providers And Systems (Cahps) Hospice Survey
CAHPS SAMPLE LETTER
This is a survey used to gather feedback from a family member or caregiver regarding the quality of care that Seasons Hospice provided. The CAHPS survey is sent to the designated family member or caregiver approximately 6 weeks after the patient’s death. The surveys returned are reviewed for trends and may result in changes in policies, procedures, protocols and/or personnel to improve our performance. Centers for Medicare and Medicaid Services (CMS) publicly reports the survey results. Following is an example of the letter and survey:
14
15
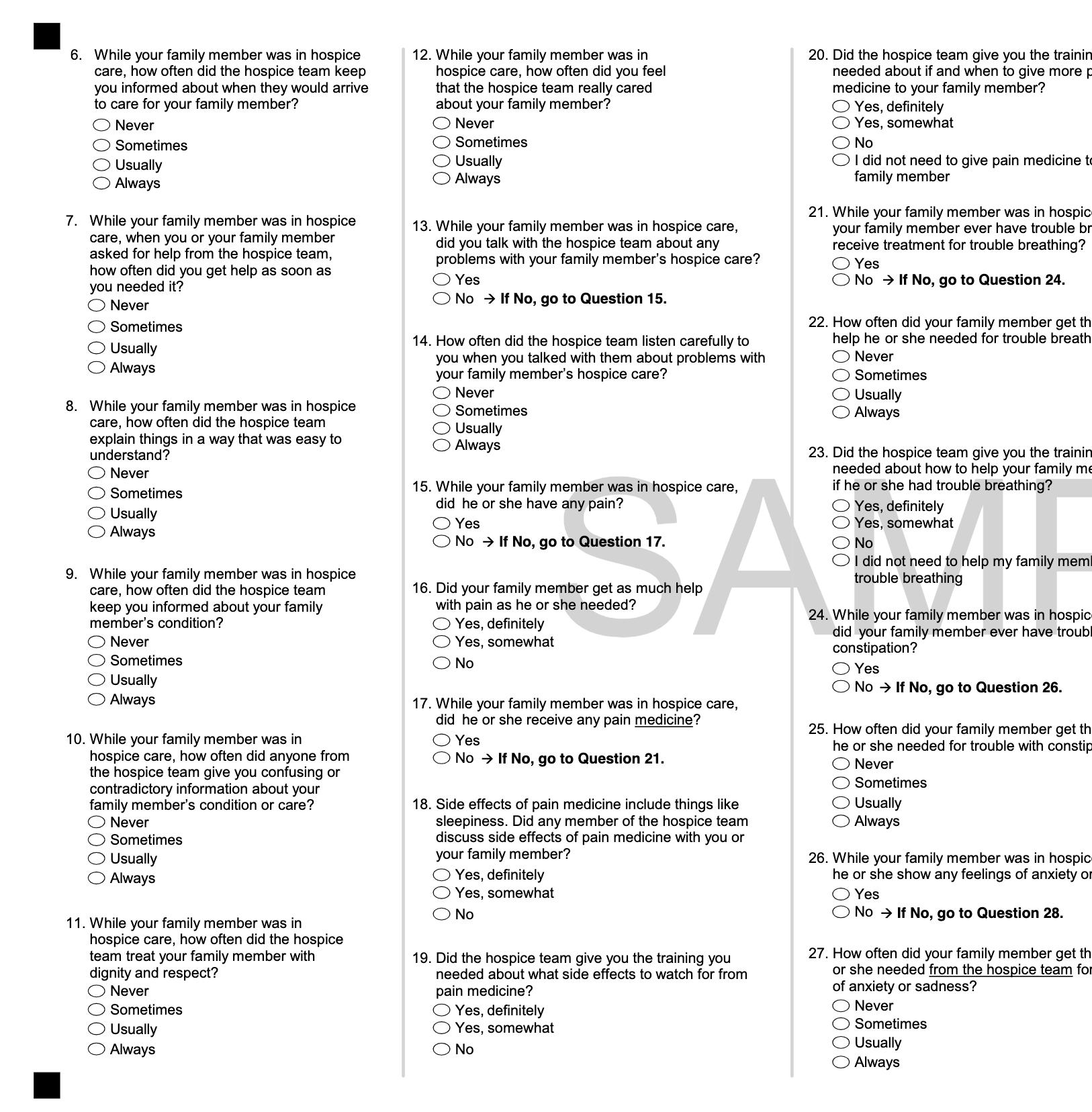
CAHPS Sample Letter, cont. 16
17
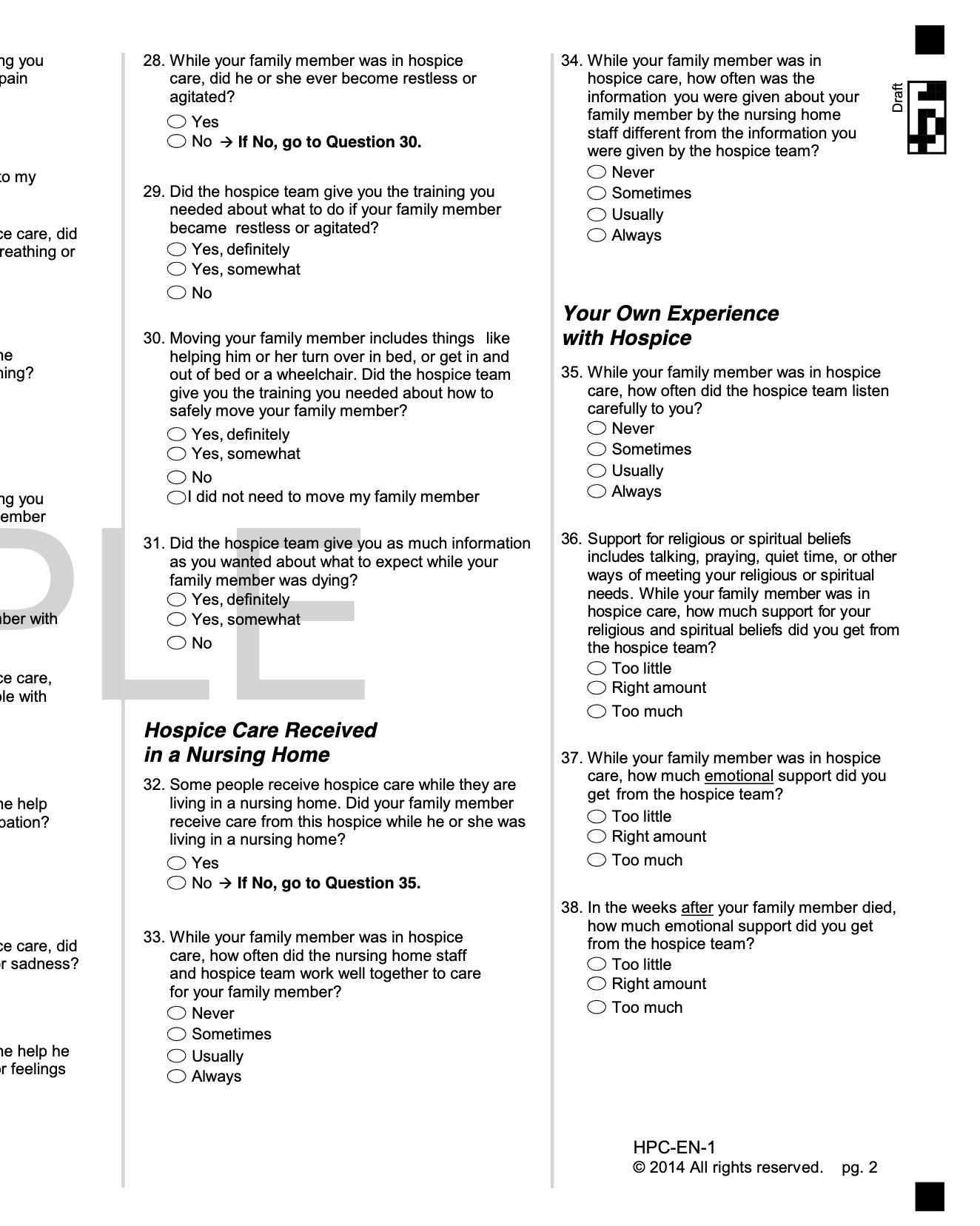
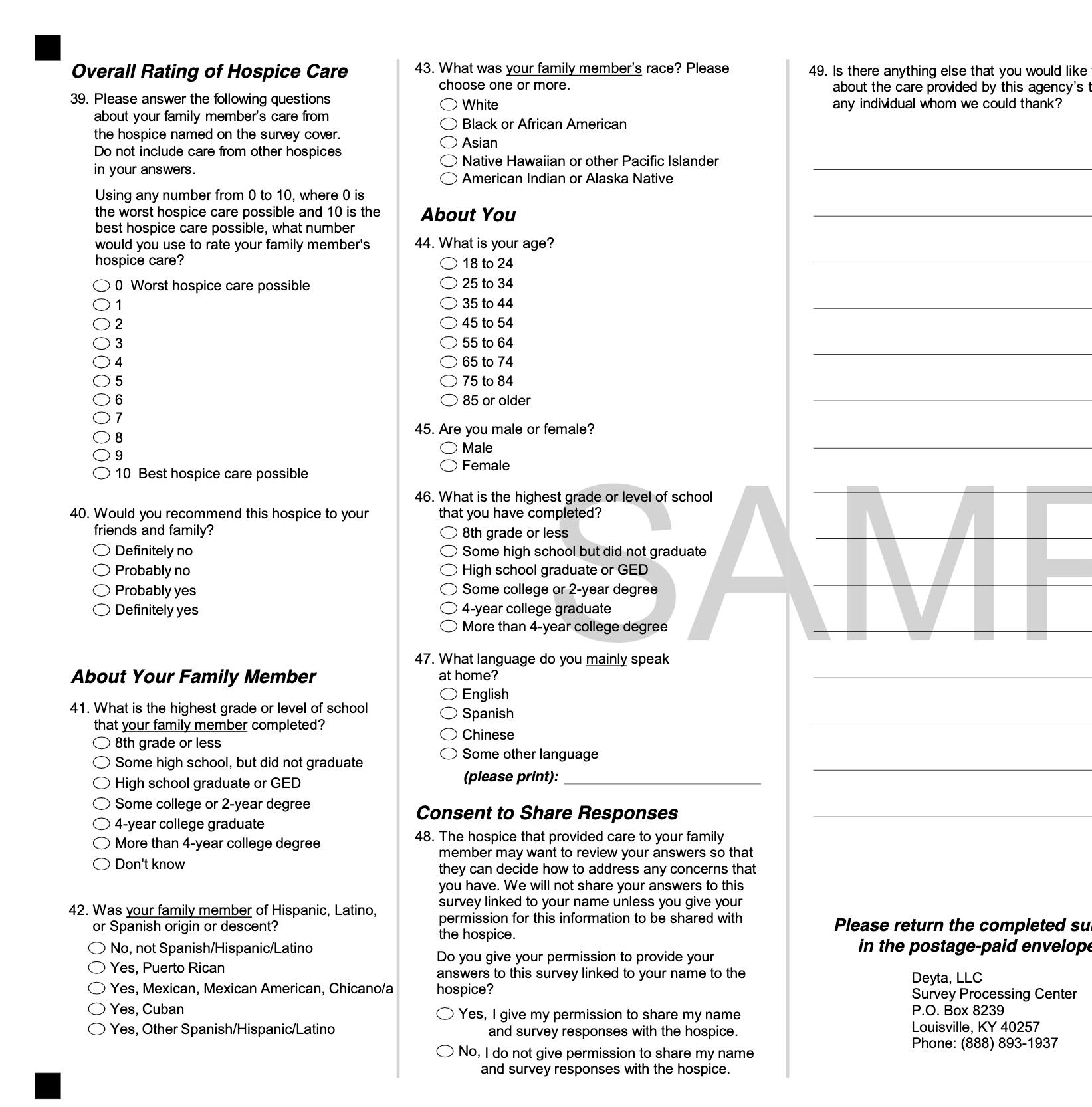
CAHPS Sample Letter, cont. 18
19
Last revised:
D= Direct
T
Recognizing emergencies and knowledge of emergency procedures Choose an item. Choose an item. Physical, emotional, and developmental needs of, and ways to work with, hospice patients, including the need for respect for the patient, her/his privacy and her/his property Choose an item. Choose an item. Adequate nutrition and fluid intake Choose an item. Choose an item. Appropriate/safe techniques in personal hygiene and grooming that include: Bed Bath Choose an item. D Sponge Choose an item. D Shower bath Choose an item. D Shampoo (bed) Choose an item. D Nail care Choose an item. D Skin care Choose an item. D Oral hygiene Choose an item. D Toileting and elimination Choose an item. D Safe transfer techniques and ambulation Choose an item. D Normal range of motion and positioning Choose an item. D Tub Bath; Shampoo (sink and tub) Choose an item. V Upon completion of orientation, you will go out in the field with the RN to complete patient visits. During these visits, your supervisor will be providing immediate and specific feedback to you. During this patient interaction time, the nurse will perform a competency on you using the form identified in this section. This completed form including your and the supervising nurse’s name, signature, credentials, and date will be stored in your agency/HR file on site.
Communication Skills Choose an item. D Observation, reporting, and documentation of patient status and the care or service furnished Choose an item. Choose an item. Reading and recording temperature Choose an item. D Reading and recording pulse Choose an item. D Reading and recording respiration Choose an item. D Basic infection control procedures Choose an item. Choose an item. Basic elements of body functioning and changes in body function that must be reported to an aide’s supervisor Choose an item. Choose an item. Maintenance of a clean, safe and healthy environment Choose an item. Choose an item.
HA COMPETENCY TOOL
This form is to be used when a RN is evaluating and completing an HHA competency. This form should only be used if/when the Back to the Bedside App is unavailable This form should be used when the information can be submitted through the Back to the Bedside App properly.
V=Verbal
Hospice Aide Performance Appraisal & Competency Evaluation
20
©Seasons Hospice & Palliative Care Hospice Aide (Full Name): Date of Evaluation: Click or tap to enter a date. RN Evaluator (Full Name and Title):
Competence Assessment Method Observation and De monstration of Skill on Patient Question and Answer Session =Written Test Skills (Met/NotCompetencyMet) Method(D,V,T) Comments
