



















A GLIMPSE INTO THE FUTURE #AEEDC2016 www.dentalnews.com NEW & IMPROVED www.dentalnews.com Volume XXIII, Number I, 2016 SDS/KSU 2016 FEATURING AEEDC 2016 KDAC 2016 ISSN 261 1026 X STAY CONNECTED DENTAL NEWS APP















































Dental News, Volume XXIII, Number I, 2016
















SYNERGY IN IMPLANTOLOGY



















Surgical Micromotor System Ultrasonic Bone Surgery System




OptiBond™ XTR
10:46 Pagina 1
AD_OptiBond_XTR_bullet 12.11.2010 10:46 Pagina 1
Unmatched power for all your direct and indirect restorations.
OptiBond™ XTR
OptiBond™ XTR
Unmatched
Unmatched power for all your direct and indirect restorations.
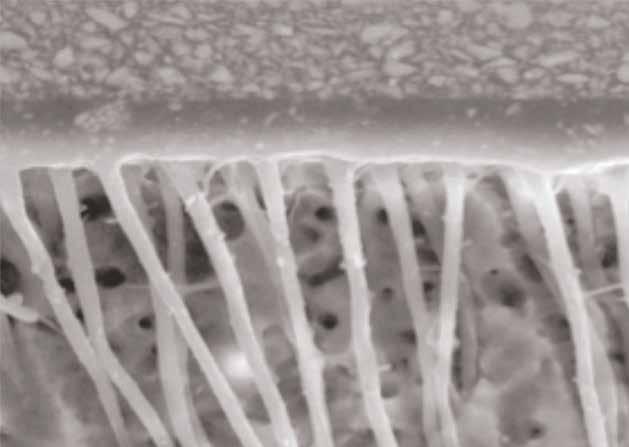
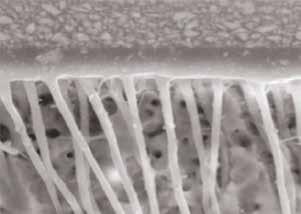
OptiBond XTR well-defined hybrid layer.

OptiBond XTR well-defined hybrid layer.
OptiBond XTR well-defined hybrid layer.
OptiBond XTR well-defined hybrid layer.

long
Clear, long resin tags with penetration into lateral dentin tubule branches (2,000x).
Clear, long resin tags with penetration into layer. penetration into branches (2,000x).
tags
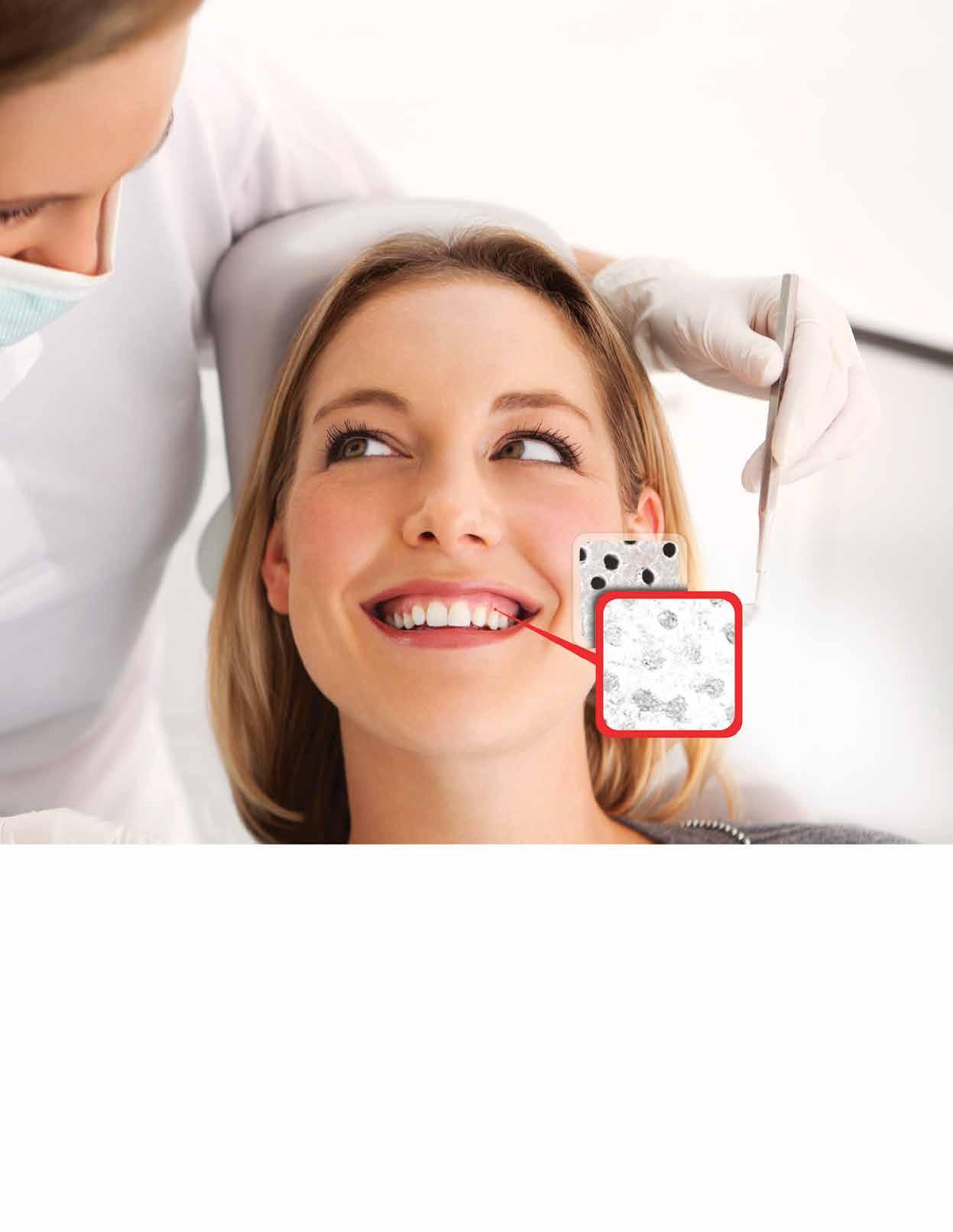
OptiBond XTR Self-Etch, Light-Cure Universal Adhesive.
Clear, long resin tags with penetration into lateral dentin tubule branches (2,000x).
•Outstanding bond strengths to dentin and enamel. Extraordinary performance for long-lasting restorations.
•Self-etch. Minimizes
•For
OptiBond XTR Self-Etch, Light-Cure Univesal Adhesive.
•Outstanding bond strengths to dentin and enamel. Extraordinary performance for long-lasting restorations.
patient comfort. and indirect restorations. A true universal adhesive.
performance and substrates. inspiration.™
•Self-etch. Minimizes post-operative sensitivity, maximizes patient comfort.
•For direct and indirect restorations. A true universal adhesive.

Dental News, Volume XXIII, Number I, 2016
OptiBond XTR Self-Etch, Light-Cure Univesal Adhesive.
sensitivity, maximizes patient
post-operative
comfort.
true universal adhesive.
direct and indirect restorations. A
For more
Your practice is our inspiration.™ KerrHawe SA P.O. Box 2686934 Bioggio Switzerland Freephone: 00800 41 05 05 05 Fax: ++41 91 610 05 14 www.kerrdental.eu
hybrid layer. Clear, long resin tags with penetration into
•Universal compatibility. Enables use with all cements, core build-up materials and substrates.
information visit: www.kerrdental.eu/optibondxtr
OptiBond XTR well-defined
power for all your direct indirect restorations.
post-operative sensitivity, maximizes
OptiBond XTR Self-Etch, Light-Cure Univesal Adhesive. •Outstanding bond strengths to dentin and enamel. Extraordinary performance long-lasting restorations. Minimizes
AD_OptiBond_XTR_bullet 12.11.2010
Clear,
resin
with penetration into lateral dentin tubule branches (2,000x).
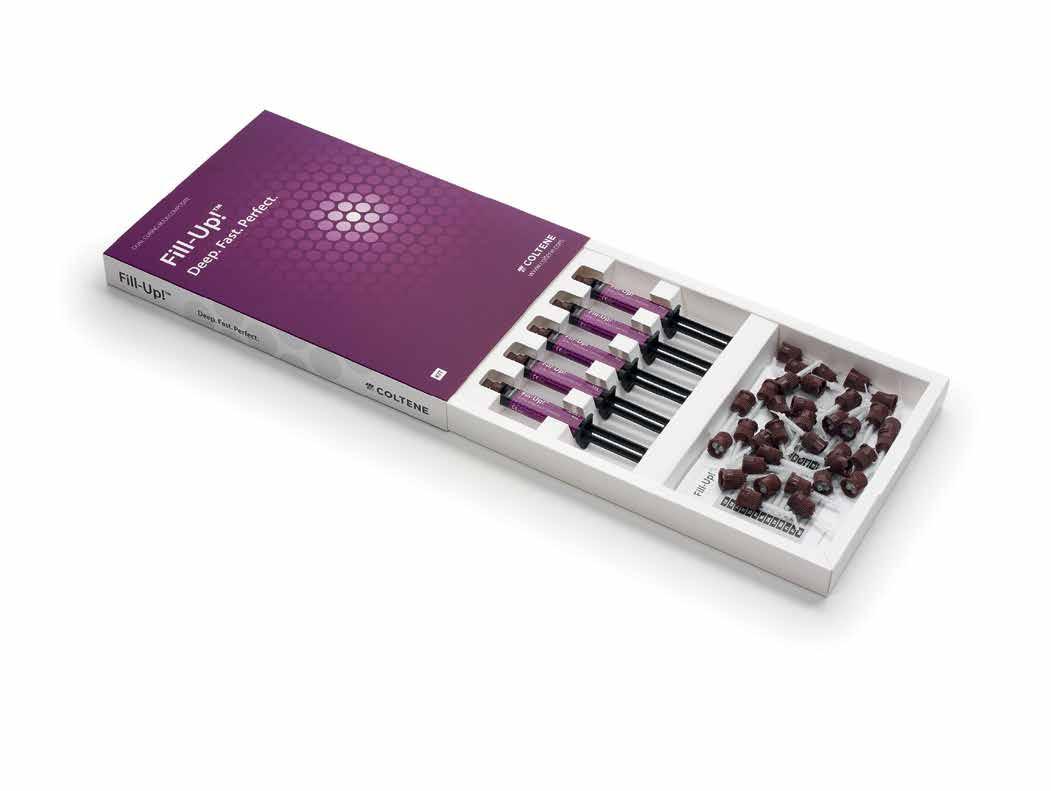
® N-Ceram Bulk Fill
The nano-optimized 4-mm composite
• Bulk filling is possible due to Ivocerin®, the patented light initiator
• Special filler technology ensures low shrinkage stress
• Esthetic results are achieved quickly and efficiently in the posterior region 4 mm to success
Discover the new time-saving composite www.ivoclarvivadent.com Ivoclar Vivadent AG Bendererstr. 2 | 9494 Schaan | Liechtenstein | Tel.: +423 235 35 35 | Fax: +423 235 33 60
Tetric
4 mm

Dental News, Volume XXIII, Number I, 2016
ARTICLES CONGRESSES
Tooth staining and discoloration: a review of literature. Part II: Management
Dr. Sawsan Nasreddine, Dr. Fida Sayah, Dr. Fady Kassir, Pr. Mounir Doumit. Lebanese University, School of Dentistry

The permanent maxillary second molar: Canal number and configurations in a Tunisian population
Dr. Soumaya Touzi, Dr. Rim Kallala, Dr. Faten Khanfir, Dr. Mohamed Romdhane, Dr. Khalfi Mohamed Salah, Dr. Faten Ben Amor




Orthodontic management of an impacted mandibular canine in a 14 years old Kuwaiti girl.
Dr. Saud A. Al-Anezi


SDS 2016
January 5 - 7, 2016
Riyadh International Convention & Exhibition Center, KSA
AEEDC 2016
February 2 - 4, 2016
Dubai International Convention & Exhibition Center,
UAE
KDAC 2016
February 13 - 15, 2016
Jumeirah Messilah Beach Hotel & Spa, Badriah Ballroom, KUWAIT

ADVERTISING INDEX
3SHAPE 39
ACTEON 6, 15
A-DEC 8
BA INTERNATIONAL 63
BIEN AIR 7
BISCO 23
CAMLOG 33
CARESTREAM 36
COLGATE 17, 47
COLTENE 62
DENTAURUM 45
DENTSPLY 35
DURR 55
EMOFORM 4, 5
FKG 28
GC 59
GSK C3, 29, 49, 57
HENRY SCHEIN 43
ITENA 31
IVOCLAR 1, C4
KERR C2
MECTRON 21
MEDESY 13
MICRO MEGA 27
MORITA 51
NSK C1
ORTHO ORGANIZERS 37
PLANMECA 25
PROMEDICA 40
RITTER 10
SCHEU 20
SDI 41
SIRONA 19
ULTRADENT USA 30
VOCO 53
W&H 9
ZHERMACK 2
ZOOM PHILIPS 67
3
42. 50. 66.
22. 12. 34. Dental News, Volume XXIII, Number I, 2016
NEW INNOVATIVE PRODUCTS FROM
NEW INNOVATIVE PRODUCTS FROM
EMOFORM®-F DIAMOND and EMOFORM®-F PROTECT are the new generation of oral hygiene, developped from the leading Swiss oral care company Dr. Wild & Co. AG. Using only the best ingredients, EMOFORM®-F toothpastes are especially composed to be forward-looking, ecological and safe.
EMOFORM®-F DIAMOND
Diamonds polish all the parts of the tooth evenly, including ceramic-inlays, gold or fillings
Gentle tooth polishing even for patients with sensitive teeth, because it only has an RDA value of 30.
The formation of plaque is delayed on smooth surfaces, which impedes the development of caries, gingivitis, periodontitis and more.
Against:
• Caries
• Plaque
• Tooth discoloration
EMOFORM®-F DIAMOND is free from:
• Preservatives
• Artificial sweeteners
• Plastic particles
• Nanoparticles
• Sodium lauryl sulfate (SLS)
• Titanium dioxide
DR. WILD‘S DISTRIBUTORS
Dental News, Volume XXIII, Number I, 2016
Al

 Bahrain: Awal Pharmacy, East Riffa, Bahrain. Egypt: Sesic, Alexandria. Jordan: Areel for Cosmetics Trading, Amman. Kuwait: Al-Maseela Pharmaceutical Co., Safat. Lebanon: A.M.G. Medical.Jdeideh-Azur Center. Libya: Al Osra, Benghazi.
Oman: Ibn Sina Pharmacy L.L.C., Muscat. Qatar: Masar Medical, Doha. Saudi Arabia: Depot Pharmaceutique du Moyen Orient, Jeddah. United Arab Emirates: Al Hayat Pharmaceuticals, Sharjah. Yemen:
Rawdha Trading Group, Sana’a.
Bahrain: Awal Pharmacy, East Riffa, Bahrain. Egypt: Sesic, Alexandria. Jordan: Areel for Cosmetics Trading, Amman. Kuwait: Al-Maseela Pharmaceutical Co., Safat. Lebanon: A.M.G. Medical.Jdeideh-Azur Center. Libya: Al Osra, Benghazi.
Oman: Ibn Sina Pharmacy L.L.C., Muscat. Qatar: Masar Medical, Doha. Saudi Arabia: Depot Pharmaceutique du Moyen Orient, Jeddah. United Arab Emirates: Al Hayat Pharmaceuticals, Sharjah. Yemen:
Rawdha Trading Group, Sana’a.
SWITZERLAND Swiss professional oral care
INNOWAVAILABLE PHARMACIES
Against:
• Caries
• Erosions
Minimizes dental erosion and prevents root caries. EMOFORM®-F PROTECT
Protects against irritations of the gums and acts desensitizing through plugging of the dentin tubules.
Protects actively against caries with its combination of sodiumand stannous fluoride and xylitol (NSX formula).
EMOFORM®-F PROTECT is free from:
• Microbeads
• Sodium lauryl sulfate
• Colouring
• Preservatives
• Artificial sweeteners
• Nanoparticles
• Allergenic substances
Dr. Wild
& Co. AG | www.wild-pharma.com

YOUR WEAPONS
ACTEON® offers a complete solution to manage peri-implantitis from the prevention, to the treatment and maintenance.
The combination of in-depth implant cleaning with ImplantProtect ultrasonic tips in Pure Titanium and targeted polishing with AIR-N-GO® easy nozzles and powders represent a safe and effective solution to defeat peri-implantitis.


I AM A CLINICAL SOLUTION
NEWTRON






AIR-N-GO














Made of Pure Titanium, and driven by perfectly-controlled Newtron® technology, ImplantProtect micro-tips preserve implant surface.




Interchangeable and innovative design for gentle sub-gingival use in surgical and non-surgical treatments of teeth and implants.

Dental News, Volume XXIII, Number I, 2016
17 av. Gustave Eiffel • BP 30216 • 33708 MERIGNAC cedex • France • www.acteongroup.com • info@acteongroup.com
MIDDLE EAST • 247 Wasfi Al Tal str. • 401 AMMAN
ACTEON
EASY
BORA & PRESTIGE INNOVATION AND TECHNOLOGY.
Imagine incredibly light instruments, refined, efficient and rugged at the same time.
Inspired by the latest technological breakthroughs in the most demanding environments, the Bora and Prestige BLACKLINE incorporates a carbon fiber handle. These turbines are incredibly light and therefore easier to handle. Moreover, the carbon fiber offers improved resistance to wear, friction, torsion and impacts. The two Bien-Air monobloc optical glass rods provide ideal distribution of the LED intensity. There is virtually no shadow area. Diffusing a natural white light similar to daylight, the LED has a service life 10 times longer than that of a traditional light bulb.
Available with a metal or a carbon fiber handle, the powerful Bora and the miniature Prestige turbines set new standards in ergonomics, performance and durability.

UP TO 3 YEARS WARRANTY
2-year standard warranty and 1-year optional warranty available through Bien-Air’s PlanCare extended warranty program.
Bien-Air Dental SA Länggasse 60 Case postale 2500 Bienne 6 Switzerland Tél. +41 (0)32 344 64 64 Fax +41 (0)32 344 64 91 dental@bienair.com www.bienair.com

Not to mention everything else.
The ability to perform your job comfortably is essential. And the new feature-rich A-dec 500 stools have you covered. Based on a unique dynamic seating system design, individual performance zones work in unison to conform and move with your body. With an ultimate ergonomic solution like this, you can focus on what’s really important—your patients.
Discover your ultimate comfort at a-dec.com/500stools

Dental News, Volume XXIII, Number I, 2016 We’ve got your back.
© 2015 A-dec Inc. All rights reserved.
The A-dec Dynamic Seating System
Minimally invasive, maximally effective

The new force in bone surgery: The new Piezomed offers extremely high performance, yet is gentle on soft tissue. In addition, it includes automatic instrument recognition and LED handpiece illumination. The handpiece with the cable is thermo washer disinfectable and sterilizable!
Now available from your dental supplier or via wh.com
SR & Cameo: Aesthetics and individuality for the individual style of your clinic
made in germany
Henry Schein Dental, Dr. Ghassan Nasser Hussein , Sales and Marketing Director (Henry Schein) Middle East and North Africa, Mobile: +971 50 4813292, Tel: +971 6 5252842, Fax: +971 6 5531291 E-mail: ghassan.nasser@henryschein.com




Ritter Concept GmbH, Germany, Christian Findeisen Sales and Key Account Manager , Middle East/ Africa Ritter Concept GmbH, Mobile: +971 56 9578689
E-mail: christian.findeisen@ritterconcept.com www.ritterconcept.com






Individual design of glass surfaces: Choose your preferred colours, patterns or photos!
The treatment unit ARIA SR and the furniture line Cameo combine efficiency and userfriendly handling with pure aesthetics and individuality and improve the productivity in the dental office with simple and practical solutions. The careful selection of high-quality materials, a very attractive design and outstanding functionality guarantee fantastic results. In terms of design the products amaze with elegant glass elements in fresh colours that can be customized according to the all preferences, with personal images, motifs or clinic logos. Create your distinctive brand recognition!
Dental News, Volume XXIII, Number I, 2016
*** Exclusively distributed
by
***
Henry Schein Middle East
Ritter
ARIA
EDITORIAL TEAM
Alfred Naaman, Nada Naaman, Jihad Fakhoury, Dona Raad, Antoine Saadé, Lina Chamseddine, Tarek Kotob, Mohammed Rifai, Bilal Koleilat, Mohammad H. Al-Jammaz
INTERNATIONAL CALENDAR

COORDINATOR ART DEPARTMENT SUBSCRIPTION ADVERTISING PHOTOGRAPHY TRANSLATION DIRECTOR ISSN
Suha Nader
Elie Hajj
Micheline Assaf, Nariman Nehmeh
Josiane Younes
Albert Saykali
Gisèle Wakim, Marielle Khoury
Tony Dib 1026-261X
DENTAL NEWS IS A QUARTERLY MAGAZINE DISTRIBUTED MAINLY IN THE MIDDLE EAST & NORTH AFRICA IN COLLABORATION WITH THE COUNCIL OF DENTAL SOCIETIES FOR THE GCC.
Statements and opinions expressed in the articles and communications herein are those of the author(s) and not necessarily those of the Editor(s) or publisher. No part of this magazine may be reproduced in any form, either electronic or mechanical, without the express written permission of the publisher.
DENTAL NEWS – Sami Solh Ave., G. Younis Bldg. POB: 116-5515 Beirut, Lebanon.
Tel: 961-3-30 30 48
Fax: 961-1-38 46 57
Email: info@dentalnews.com Website: www.dentalnews.com
www.facebook.com/dentalnews1
www.instagram.com/dentalnews
twitter.com/dentalnews
Dental News App on both Appstore & Google play




OIDC 2016 - The 18th Oman International Dental Conference

JDA 2016 - The Jordanian Dental Association Meeting



The 8th Lebanese Dental Association - Tripoli International Meeting
The 11th CAD/CAM & Digital Dentistry International Conference
LDLS 2016 - The 9th Lebanese Dental Laboratories Show
BIDM 2016 - The 26th Lebanese Dental Association Congress
AIDC 2016 - The 20th Alexandria International Dental Congress
DFCIC 2016 - The 8th Dental-Facial Cosmetic International Conference
AEEDC 2017 - The 21st UAE International Dental Conference & Arab Dental Exhibition
March 31 - April 1, 2016 at the Grand Hyatt Muscat, OMAN Website: www.odsoman.org
April 6, 2015 JORDAN Website: www.jda.org.jo
April 21 - 23, 2016 at the University of Balamand, LEBANON Website: www.lda-tripoli.com
May 4 - 8, 2016 at the Jumeirah Beach Hotel, Dubai, UAE Website: www.cappmea.com
May 12 - 14, 2016 Le Royal Hotel Dbayeh, LEBANON Website: www.opdlb.org
October 13 - 15, 2016 at the BIEL, Beirut, LEBANON Website: www.bidm-lda.com
November 1 - 4, 2016 Alexandria, EGYPT Website: www.aidc2016.com
November 4 - 5, 2016 at the Jumeirah Beach Hotel, Dubai, UAE Website: www.cappmea.com/cadcam10
February 7 - 9, 2017 at the Dubai International Convention & Exhibition Center, Dubai, UAE Email: info@aeedc.com Website: www.aeedc.com
11
Volume XXIII, Number I, 2016 www.dentalnews.com This magazine is printed on FSC – certified paper.
Dental News, Volume XXIII, Number I, 2016
Restorative Dentistry
Tooth staining and discoloration: a review of literature. Part II: Management

Dr. Sawsan Nasreddine, BDS, DESS Pediatric Dentistry, DESS Public Health Dentistry, Department of Public Health Dentistry
Abstract
Dr. Fida Sayah, BDS, DESS Public Health Dentistry, Department of Public Health Dentistry
Dr. Dani Daou, DESS Public Health Dentistry, MPH, Department of Public Health Dentistry
Pr. Mounir Doumit, DCD, DSO, HDR, Expert WHO in Dental Health, Director FDI, CE Middle Orient, 1st vicepresident CIDCDF
Lebanese University, School of Dentistry sawsan-n25@hotmail.com
The management of tooth discoloration consists of implementing the required therapy. Scaling and polishing of the teeth using prophylactic paste applied with a rotating rubber cup may remove many extrinsic stains. For more stubborn extrinsic and intrinsic stain, various bleaching techniques may be attempted. Bleaching can be performed externally, termed night guard bleaching or vital tooth bleaching, or intra coronally in root-filled teeth, called non-vital tooth bleaching. Teeth discolored by dental caries or dental materials require the removal of the carious and/or restorative material, followed by adequate restoration of the tooth. Partial or full-coverage dental restorations may be used to treat generalized intrinsic tooth discoloration in which bleaching is not indicated or in which the esthetic results of bleaching fail to meet the patient’s expectations.
The purpose of this article is to review literature on the management of tooth staining and discoloration.
Keywords Management, extrinsic discoloration, intrinsic discoloration
Introduction
Tooth color changes may be the result of intrinsic or extrinsic factors. In the management of patients with discolored teeth, knowledge of the mechanisms and the etiology behind tooth discoloration is of relevance as it can influence the treatment plan. There are many factors that contribute to tooth staining. It is important to understand what staining is in order to be able to prevent it.1
In some instances, the mechanism of staining may have an effect on the outcome of treatment and can influence the treatment options offered by the dentist to the patients.2, 3
History
History is essential for establishing an accurate diagnosis of intrinsic tooth discoloration, as the choice of treatment it should cover the following aspects:
History of mother’s obstetric and the delivery; medical history including neo-natal or early childhood illness and drugs intake, dental history relating to primary teeth and about any trauma of primary and permanent teeth; family history of discolored or abnormal teeth; fluoride history including supplementation, residence in natural water areas, tooth brushing habits including the amount of paste used, the type of paste in childhood and any admitted swallowing of paste.4
Examination
Clinical
A standard extra-oral examination and full mouth intra-oral examination should be undertaken, with special emphasis on the presence and/or absence of both primary and permanent teeth.4
The scratch test is usually used to distinguish between extrinsic and intrinsic discoloration. Discolored tooth surfaces are scratched with care by using a dental explorer, scaler, or similar sharp instrument to assess surface texture.2
Light scratching with a dental instrument removes weakly adherent plaque that causes extrinsic discoloration. If the discoloration requires removal
Dental News, Volume XXIII, Number I, 2016
12
with a sharp dental scaler, the discoloration is considered to be tenacious. Intrinsic discoloration cannot be removed by using the scratch test. Extrinsic staining of a single tooth is unusual. The distribution is usually generalized. The stains are usually found on surfaces with poor tooth brush accessibility. In case of intrinsic discoloration, distribution is either generalized to all teeth or localized to certain teeth or tooth surfaces. An in trinsic etiology usually exists when a single tooth is discolored. Teeth with extrinsic tooth discoloration usually demonstrate no signs of pulp disease, usually associated with intrinsic discolor ation.2
Additional Investigations
Appropriate radiographs will show abnormalities of enamel and dentin structure, abnormal tooth morphology and the adequacy of root canal fillings in non-vital teeth. Sensibility testing will sug gest the presence or absence of a functioning nerve supply. Histological sectioning of exfoliated or extracted teeth may iden tify hereditary and environmental abnormalities.



MEDESY srl 33085 Maniago, PN - ITALY Viale dell’Industria, 1 - Industrial Area www.medesy.it - info@medesy.it
Restorative Dentistry
Diagnosis
Clinical examination and review of oral hygiene practices, dietary habits and history of exposure to chemicals, trauma, and infection are essential in making a final diagnosis of the cause of tooth discoloration.5
Management of stains (Table 1)
Proper diet and habits
Extrinsic staining caused by foods, beverages, or habits (smoking, chewing tobacco, coffee and tea) is treated with a thorough dental prophylaxis and cessation of dietary or other contributory habits to prevent further staining.6, 7
Management
Proper diet and habits
Tooth brushing
Professional tooth cleaning
• Ultrasonic scalers
• Air jet polishing
Prophylactic paste
Microabrasion
Non-vital bleaching
Hydrogen peroxide/sodium perborate
Vital bleaching
• Chairside: hydrogen peroxide + heat source
• Nightguard: carbamide peroxide gel
Composite resin restorations
Porcelain laminate veneers
Extraction
In case of
Foods / beverages
Smoking, coffee, tea and chewing tobacco
Prevent extrinsic staining
Prolonged used of chlorhexidine mouthwash - Calculus and persistent stains.
Stain due smoking, coffee, tea, chlorhexidine and heavily stained enamel
Cleaning and polishing with less abrasion to tooth dentin and enamel. Excellent stain and plaque removal
- Post orthodontic demineralization (white spot)
- Localized hypoplasia (infection or trauma)
- Idiopathic hypoplasia
- Minor fluorosis
Non vital, endodontically treated teeth (cause: deposition of blood degradation)
- Mild tetracycline staining without obvious banding
- Mild fluorosis
- Single tooth with sclerosed pulp chambers and root canals
- Moderate fluorosis
- Hypoplasia (caused moderate to severe fluorosis)
- Localized hypoplasia not responsive to microabrasion
- Tetracycline staining
- Discoloration due to loss of vitality not responsive to non vital bleaching
- Amelogenesis imperfect
- Dentinogenesis imperfect
- Hypolplasia and discoloration teeth in patients aged 16 years and over
- When techniques such as micro abrasion non vital bleaching and composite resins have failed to produce satisfactory clinical result
- Teeth that are non restorable
- Severe amelogenesis imperfect and dentinogenesis imperfect
- Teeth with large periodontal defects
Dental News, Volume XXIII, Number I, 2016 14
Table 1: Management of different types of stains


I AM demanding
The outstanding visualisation for the most demanding results
• Image definition of 75 µm.
• 4 selectable sizes of Field of View (from 40x40 mm to 110x80 mm).
• Dedicated metal artifact reduction filter.
• An optimal 3D solution for all specialties including Implantology, Orthodontics, Endodontics, Periodontology…
• A complete and exclusive service provided by Acteon: hot-line, on-site training, remote software assistance…
99 Gardens Str. Numan Center. 205. P.O.Box: 5746 Amman, 11953 Jordan, Amman, JORDAN Tel. +962 6 553 4401 • Fax + 962 6553 7833 • www.acteongroup.com
Restorative Dentistry
Tooth brushing
Effective tooth brushing twice a day with a dentifrice helps to prevent extrinsic staining. Most dentifrices contain an abrasive, a detergent and an anti-tartar agent. In addition, some dentifrices now contain tooth-whitening agents.6, 7
The patient’s use of a dentifrice can also contribute to dental stain removal and prevent recurrent discoloration.8 The dentifrice’s stain-removal property is firstly related to the abrasives present in its composition.9 It is important to point out that if, on one hand, increased dentifrice abrasiveness leads to improved stain removal efficacy, on the other hand it increases tooth wear. Thus, dentifrices containing active ingredients specifically designed for tooth stain removal are known as whitening dentifrices. These dentifrices usually have enzymes in their composition that help to break down the organic components of biological film and remove stains and bacterial plaque. Another common dentifrice component is detergent, especially Sodium Lauryl Sulfate. It acts by lowering the surface tension of stain producing molecules, thus disrupting their potential to bind to enamel. Some whitening dentifrices also contain low peroxide concentrations, with the aim of releasing free oxygen radicals. These radicals are responsible for an oxidation reaction, which is the principle of the bleaching technique used for extrinsic and intrinsic stain removal. 3, 8, 10, 11, 12
Professional tooth cleaning
Some extrinsic stains may be removed with ultrasonic cleaning, rotary polishing with an abrasive prophylactic paste, or air-jet polishing with an abrasive powder. However, these modalities can lead to enamel removal; therefore, their repeated use is undesirable.6, 7

Ultrasonic and sonic scalers are referred to as power-driven scalers. The small, quick vibrations in combination with a water flow provide a whole new level of effectiveness in removal of deposits on the tooth surface. The benefits of ultrasonic scaling include increased efficiency of calculus removal and less need for hand scaling (fig.1). Microvibration crushes and removes calculus under cooling water. Sonic scalers are air-turbine units that operate at low frequencies ranging between 3000 and 8000 cycles per sec (cps).7, 13
Prophylactic paste
Prophylactic pastes contain abrasive, water, humectants, binder, sweetener, flavoring and coloring agents. Prophylaxis polishing agents are available in two basic forms: dry powders, also referred to as flours that must be mixed with a liquid (fig.2) (water, fluoride, or mouth rinse) and commercially prepared polishing pastes that are available in bulk or individual unit doses.10
Therefore, the use of dry abrasives or powder on a dry polishing cup is contraindicated due to the potential for thermal injury to natural teeth.7, 10 However, it is general knowledge that pumice and glycerin are the most commonly used ingredients in commercially prepared polishing pastes.7, 10

Microabrasion
Microabrasion involves the removal of a small amount of surface enamel and classically incorporates both “abrasion” with dental instruments and “erosion” with an acid mixture.4 Microabrasion is indicated for fluorosis, postorthodontic demineralization (white spot), localized hypoplasia due to infection or trauma and idiopathic hypoplasia where the discoloration is limited to the outer layer.4, 14, 15
Dental News, Volume XXIII, Number I, 2016
16
Fig 1: Calculus removal with ultrasonic scaling
Fig 2: Stain removal with prophylactic paste
Fig 1
Fig 2
COLGATE TOTAL® PROVIDES
PROTECTION* TO 100% OF THE MOUTH’S SURFACES1

O Regular toothpastes† only protect the hard tissue, which is 20% of the mouth2
O The remaining 80% of the mouth is the tongue, cheeks, and gums, which can provide a bacteria reservoir for plaque biofilm recolonization
WHY SETTLE FOR 20% WHEN YOU CAN OFFER PATIENTS PROTECTION TO 100% OF THE MOUTH’S SURFACES?
*In addition to fluoride for cavity protection, Colgate Total® provides 12-hour antibacterial protection for teeth, tongue, cheeks, and gums.
†Defined as non-antibacterial fluoride toothpaste.
References: 1. Fine DH, Sreenivasan PK, McKiernan M, et al. J Clin Periodontol. 2012;39:1056-1064. 2. Collins LMC, Dawes C. J Dent Res. 1987;66:1300-1302.
18
Restorative Dentistry
Non-vital bleaching
Non-vital bleaching is indicated for non vital, endodontically treated teeth which have become discolored due to the deposition of blood degradation products in the dentinal tubules. Most techniques utilize hydrogen peroxide or sodium perborate.4
Vital bleaching
Vital bleaching involves the external application of hydrogen peroxide to the surface of the tooth followed by its activation with a heat source. An alternative source of hydrogen peroxide is sodium per carbonate and this has been used in a silicone polymer containing product that is painted onto the teeth forming a durable film for overnight bleaching procedures 16, 17. It is indicated for mild tetracycline staining without obvious banding, mild fluorosis and single teeth with scleroses pulp chambers and root canals.4, 18
Composite resin restorations
Teeth discolored by dental caries or dental materials require the removal of the caries or restorative materials, followed by proper restoration of the tooth. Partial or full-coverage dental restorations may be used to treat generalized intrinsic tooth discoloration in which bleaching is not indicated or in which the esthetic results of bleaching fail to meet the patient’s expectations.2 Composite resin restorations are indicated in cases of hypoplasia caused by moderate to severe fluorosis, localized hypoplasia not responsive to micro abrasion, tetracycline staining, and discoloration due to loss of vitality not responsive to non vital bleaching, amelogenesis and dentinogenesis imperfect and idiopathic hypoplasia.4, 19
Porcelain laminate veneers
They are indicated for hypoplastic and discolored teeth in patients aged 16 years and over, when techniques such as microabrasion, non vital bleaching and composite resins have failed to produce a satisfactory clinical results.4
Tetracycline/minocycline-induced discoloration cannot be removed. The staining of the permanent teeth creates an esthetic and psychological concern for which patients may look for advice and treatment to improve their appearance.18
Treatment may include vital or non vital teeth bleaching, which will lighten the discoloration but will leave a translucent appearance. As tetracycline staining is intrinsic, the bleaching technique is most often partially successful. Other options include placing composite resins or porcelain laminate veneers or full-coverage porcelain crowns to physically cover the teeth.18
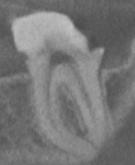
Dental extractions may be required for severely carious teeth that are non restorable (fig.3) or for teeth with large periodontal defects that are refractory to periodontal rehabilitation. Previously endodontically treated teeth that develop further dentoalveolar infections require intracanal endodontic retreatments, endodontic surgery of the tooth apex, or extraction20 severely involved teeth with amelogenesis imperfect or dentinogenesis imperfect also may require extraction.20


Dental News, Volume XXIII, Number I, 2016
Fig 3: Extraction of carious teeth that are non restorable
Fig 3
ORTHOPHOS XG

BLE.
By choosing an or THoPHos XG you are investing in a secure future. This is because the units in the or THoPHos XG family offer you high quality, durability and the best image quality with the lowest dose and a perfect workflow. s o it‘s no surprise that more than 100,000 dentists all over the world have decided on an or THoPHos XG. Enjoy every day. With Sirona.
B-753-01-7600-V0 sirona.com
simPLY rELia
EVERY DAY.
Restorative Dentistry
Conclusion
In the management of patients with discolored tooth, an understanding of the mechanism behind the discoloration is of relevance to the dental practitioner as it can be valuable in the decision-making process when considering how to treat the condition. An understanding of the pathological process involved can assist in explaining the cause to anxious or concerned patients/ parents.2
References
1. Watt a, addy M. tooth discolouration and staining: a revieW of the literature. Bri dent J 2001;190(6):309-316.
2. Manuel st, aBhishek P, kundaBala M. etiology of tooth discoloration- a revieW nig dent J 2010;18(2):56-63.
3. cynthia k, Pierre k, tatiana Z, carina M. extrinsic tooth discoloration, an uPdated revieW dent triB 2015:7B-8B.
4. Wray a, WelBury r treatMent of intrinsic discoloration in PerManent anterior teeth in children and adolescents int J Paediatr denti 2001;11:309-315.
5. Bandon d, chaBane-leMBouB a les colorations dentaires noires exogènes cheZ l ’ enfant : Black-stains archives de Pédiatrie 2011;18(12):1343-1347.
6. Bussell rM, deery c case rePort: Blue chroMogenic dental staining in child With West syndroMe eur arch Paediatr denti 2010;11(6):298-300.
7. sruthy P, raJesh h, Boloor va, rao as extrinsic stains and ManageMent: a neW insight. J acad indus res 2013;1(8):435442.
8. liMa danl, silva alf, aguiar fhB, liPoroni Pcs, Munin e, aMBrosano gMB, lovadino Jr in vitro assessMent of the effectiveness of Whitening dentifrices for the reMoval of extrinsic tooth stains BraZ oral res 2008;22(2):106-11.
9. Meyers ia, McQueen MJ, harBroW d, seyMour gJ. the surface effect of dentifrices aust dent J 2000;45(2):118-124.
10. Pontes dg, correa kMl, cohen-carneiro f re-estaBlishing esthetics of fluorosis-stained teeth using enaMel MicroaBrasion and dental Bleaching techniQues eur J esthet denti 2012;7(2):130137.
11. Joiner a revieW of the extrinsic stain reMoval and enaMel/dentine aBrasion By a calciuM carBonate and Perlite containing Whitening toothPaste int dent J 2006; 56(4):175-80
12. BaZZi J, fraxino Bindo MJ, rached r, MaZur r the effect of at-hoMe Bleaching and tooth Brushing on reMoval of coffee and cigarette sMoke stains and color staBility of enaMel. J aM dent ass 2012;143:e1-e7.
13. iBiyeMi o, taiWo Jo, oke ga iMProvised source of Water coolant for ultrasonic scaler: an aPProPriate technology in underserved coMMunities rural and reMote health 2012:1-7.
14. MuñoZ Ma, arana-gordillo la, goMes gM, goMes oM, BoMBarda nhc, reis a, loguercio ad alternative esthetic ManageMent of fluorosis and hyPoPlasia stains: Blending effect oBtained With resin infiltration techniQues. J esthet restor dent 2013;25(1):32-39.
15. croll tP. enaMel MicroaBrasion: oBservations after 10 years. J aM dent assoc 1997;128:45s-50s
16. andreW J. the Bleaching of teeth: a revieW of the literature Jour of dent 2006;34:412-419.
17. date rf, yue J, BarloW aP, BellaMy Pg, Prendergast MJ, gerlach rW. delivery, suBstantivity and clinical resPonse of a direct aPPlication PercarBonate tooth Whitening filM aMer Jour of denti 2003;16:3B–8B.
18. sáncheZ ar, rogers rs, sheridan PJ. tetracycline and other tetracycline-derivative staining of the teeth and oral cavity inter J derMatol 2004;43:709-715.
19. Bidra as, uriBe f successful Bleaching of teeth With dentinogenesis iMPerfecta discoloration: a case rePort. J esthet restor dent 2011;23(1):3-11.
20. krastl g, allgayer n, lenherr P, filiPPi a, taneJa P, Weiger r tooth discoloration induced By endodontic Materials: a literature revieW dent trauMatol. 2013;29(1):2-7.
20











mectron s.p.a., via Loreto 15/A, 16042 Carasco (Ge), Italy, tel 0185 35361, fax 0185 351374, www.mectron.com, mectron@mectron.com Û BEST CUTTING EFFICIENCY AND MAXIMUM INTRAOPERATIVE CONTROL Û WHAT WAS YOUR REASON FOR NOT BUYING ONE? NEW PIEZOSURGERY® white Û FIND MORE ON WWW.MECTRON.COM NEW INSERTS Û SINUS LIFT BY CRESTAL APPROACH Û HIGH EFFECTIVENESS OSTEOTOMY Û PERIOSTEUM DETACHMENT
Endodontics
The permanent maxillary second molar: Canal number and configurations in a Tunisian population

Dr. Soumaya Touzi
Key words
Materials and Methods
Dr. Rim Kallala
Faten Khanfir
Dr. Mohamed Romdhane
Dr. Khalfi
2: Department of General Anatomy of the Dentistry Clinic of Monastir, Tunisia touzi.soumaya@gmail.com
Anatomy, maxillary second molar, morphology, root, canal
Introduction
One of the major causes of failure in endodontic treatment is the impossibility of locating and treating the entire root canal system, a result of the lack of knowledge regarding the dental, internal or external anatomy. 1
Maxillary molars are the teeth that contain the greatest number of roots, with diverse shapes and formations, which is why their internal canal system is so variable. 2
Any existing root canals that remain undetected by the operator during the entire course of endodontic treatment are a major threat to the failure of treatment. 3
The aim of the current research was to describe the variations in the root canal anatomy of maxillary first molar in a tunisian population using sectioning.
In this study, we used 98 maxillary second molars that have been extracted mainly for periodontal reasons. The teeth were stored in a sodium hypochlorite solution diluted to 5% during 3 days and then washed in running water and dried. Each tooth is macroscopically examined to determine the number of roots and grinded progressively at the root surface to highlight the path of the root canals.
Canal number and configurations are observed and analyzed using sections:
-Mesio buccal and disto buccal root: bucco-lingual sections
-Palatal root: mesio-distal sections.
Results
1- Number of roots by tooth (Table 1)
2- Number of canals by root (Table 2)
1: Department of Dental Anatomy of the Dentistry Clinic of Monastir, Tunisia
Dental News, Volume XXIII, Number I, 2016
1
1
1
2
Mohamed Salah 2 Dr. Faten Ben Amor 2
Dr.
1 canal 3 canals Mesio buccal root 97.5% 2.5% 0% Lingual root 100% 0% 0% 2 canals Disto buccal root 100% 0% 0% Table 2 % % effectif effectif % % 2 roots 4 roots effectif effectif 1 root 3 roots 1 1.1% 5 5.8% 80 93% 0 0%
Table 1
Number of roots by tooth
Number of canals by root
Endodontics
3- Canal configurations (Table 3)
Table 3
4- Different canal configurations observed at the mesio buccal root (Figures 1, 2)
5- Different canal configurations observed at the disto buccal root (Figure 3)
6- Different canal configurations observed at the lingual root (Figure 4)
Discussion : Number of roots
In the present study, 93 % of maxillary first molars were 3 rooted. Our results are similar to the findings of Libfeld 4 (90.6%), Neelakantan 5 (93.1%) and Sert 6 (91.27%).
We found 5.8% 2 rooted second maxillary molars. For consulted studies, the percentage was from 0% 5 to 21.86%. 7
We found 1.1% one rooted molars which is close to the majority of studies. 7,4,8,6 Gu Y 7 found larger percentage (14.11%).
We didn’t found 4 rooted second maxillary molars which is similar to the study of Neelakantan.5 Other studies found percentages that do not exceed 1.4% 8 (table 4).




Dental News, Volume XXIII, Number I, 2016 24
Root D-V M-V P VIII 0 IV 0 VII 0 III 0 VI 0 II 0 V 0 I 100 % canal configuration (class. Vertucci) 97.5 100 2.5 0 0 0 0 0 0 0 0 0 0 0 0 0
Authors Sert 6 Population Number of roots
et al. 8 Mixed population Chinese Tunisian Libfeld et al. 4 Gu Y 7 Touzi et al. Mixed population Turkish Neelakantan P. 5 Indian 4 1.4% 0.98% 0% 3 79.6% 63.05% 93% 2 15.9% 21.86% 5.8% Year 1996 2015 2015 1 3.1% 14.11% 1.1% 1989 2011 2010 3% 2.69% 0.9% 6% 6.75% 0% 90.6% 91.27% 93.1% 0.4% 0.57% 0%
Peikoff
Table 4: Number of roots per tooth
Fig 1: type I (Vertucci)
Fig 3: type I (Vertucci)
Fig 2: type II (Vertucci)
Fig 4: type I (Vertucci)
Fig 1 Fig 2
Fig 3 Fig 4


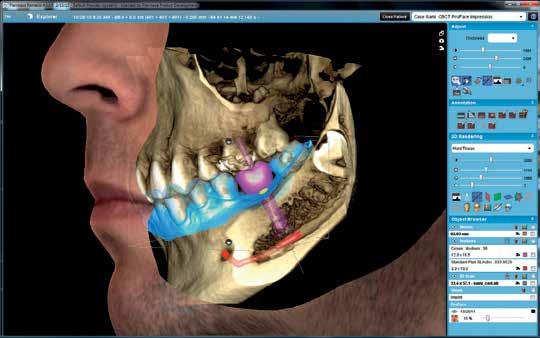
Planmeca Oy Asentajankatu 6, 00880 Helsinki, Finland Tel. +358 20 7795 500, fax +358 20 7795 555, sales@planmeca.com Find more info and your local dealer www.planmeca.com Planmeca Romexis ® is the only dental software platform in the world to combine CAD/CAM work and all imaging data. Take advantage the software’s advanced specialist tools and create a new standard of care for patients. The winning combination CAD/CAM and 3D in one software software
Endodontics
Internal morphology
• Mesio buccal root
- Number of canals:
We found in our study that 97.5 % of cases have a single canal and 2.4 % have 2 canals.
The frequencies of 2 canals varied from 19.7% according to Al-Fouzan 9 to 93.7% according to Kulild 10 ; these results are not consistent with ours. These differences may be due to the variety of the used techniques.
This root can have more than two canals according to Ozcan et al. 11 who reported a case of a maxillary second molar with 3 canals in the mesio buccal root and Caliskan et al. 12 who showed that 16% of second maxillary molars had 3 canals in this root (Table 5).
- Canals configurations:
Our study showed that 97.5 % have type I configuration and 2.5 % have type II configuration. We have not found the types III, IV and V. There is great variability in the results of literature; the percentage of type I varied from 34%14 to 86,9% 18 ; type II from 1, 8% 18 to 34% 14 and type III from 0% 14 to 15.6%. 19
For type IV, the results are divergent and span from 0% 19 to 40%. 20 Type V presents 0% for most studies 18, 19, 22, 14, 21 (table 6).
The differences in results may be explained by differences in the number of samples or by heterogeneous populations.
Dental News, Volume XXIII, Number I, 2016 26
Authors Stropoko 15 Study Kulild et al. 10 Sectionning Dye injection Cone Beam and Micro Computed Tomography Operating microscope Sectionning Weller et al. 13 Alavi et al. 16 Domark J D 17 Al-Fouzan 9 Touzi et al. Radiographs Clinical observations Singh et al. 14 Clearing % 2 canals 93.7% 65.4% 57% 19.7% 2.4% % 1 canal 6.3% 44.6% 43% 80.3% 97.5% Year 1990 2002 2013 2013 2015 Sample 32 65 14 162 80 1989 1999 1994 299 310 50 78.6% 40% 34% 21.4% 60% 66%
Study Yoshika et al. 22 Sert et al. 6 Population Canals configurations
Vertucci ) Caliskan et al. 21 Turkish Uagandiens Korean Chinese Tunisian Singh et al. 14 Rwenyonyi et al. 18 Kim et al. 20 Weng et al. 23 Touzi et al. Indian Non spécif. Turkish Ng et al. 19 Neelakantan et al. 5 Birman Indian V 0% 0% 2% 4% 0% IV 4.2% 3.2% 40% 6% 0% III 23.6% 1.8% 20.5% 8% 2.5% Year Number I 1995 100 2007 2012 221 775 2009 2015 50 80 II 27.1% 14.7% 86.9% 6.7% 36.4% 0.25% 82% 0% 97.5% 0% 1994 50 2005 2011 110 230 2001 2010 77 191 34% 0% 56.4% 0% 48.26% 7.39% 49.3% 15.6% 62% 0% 34% 29.1% 26.95% 18.2% 6.3% 4% 0.9% 10.86% 0% 24.4% 0% 0% 2.17% 0% 0%
Table 5: Number of canals in the mesio buccal root
(classification of
Table 6: Mesio buccal canal configurations according to some studies




Your single
root
shaping MICRO-MEGA 5-12 rue du Tunnel - 25006 Besançon Cedex - France - www.micro-mega.com ® Simplicity Efficiency 110 With You Years Discover One Shape® Procedure Pack Learn more on: micro-mega.com Your endo protocol ready for use in one single blister!
rotary file for
canal
STERILE
Endodontics
• Disto buccal root
- Number of canals:
In the present study, this root had in 100% of cases one canal whitch agree with the study of Médioni et al. 24
- Canals configurations: All studies confirmed that the type I is predominant with a percentage that varies from 84.9%5 to 100%. 24 Other configurations have a percentage not exceeding for the type II 2% 23, for the type III 2.4% 5, for the type IV 4.4% 5, and for the type V 6% 23 (table 7).

Case completed with ScoutRace Scouting iRace, iRace plus Shaping XP-endo Finisher Finishing
TotalFill Obturation

Dr Ahmed Abdel Rahman Hashem, Egypt
28
Study Sert et al. 6 Population Canals configurations (classification of Vertucci) Weng et al. 23 Chinese Korean Turkish Médioni et al. 24 Kim et al. 20 Altunsoy et al. 25 French Turkish Neelakantan et al. 5 Touzi et al. Indian Tunisian V 6% 0.37% 0% IV 0% 0.37% 0.6% III 2% 0.37% 0% Year Sample I 2009 50 2012 775 2014 1305 II 92% 0% 98.8% 0.12% 99% 0% 1994 Not defined 2010 230 2010 2015 191 98 100% 0% 98.69% 0.43% 84.9% 2.4% 100% 0% 0% 0.86% 1.5% 0% 3.6% 0% 4.4% 0% 0% 0% 0% 0%
FKG Dentaire SA www.fkg.ch We love endo ! Pre-Op Post-Op Tooth 38 Dx : Acute pulpitis Tx : Root canal treatment Final preparation : 30/.04
Table 7: canals configurations in the disto buccal root
«The superb flexibility of ScoutRace enabled me to reach predictably to the working length in this extremely curved lower third molar. The excellent spacing between files and the 4% taper of iRaCe made it easy for me to prepare this case with confidence and ease to the end of the root canal.»




Maintain your patients’ confidence and satisfaction with their dentures by helping them overcome daily social, emotional and physical challenges. Help your patients eat, speak and smile with confidence with the Corega® denture care regime. For full information about the product, please refer to the product pack. For reporting any Adverse Event/Side Effect related to GSK product please contact us on contactus-me@gsk.com Date of preparation: June 2014, CHSAU/CHPLD/0008/14b We value your feedback Saudi Arabia: 8008447012 All Gulf and Near East countries: +973 16500404 Arenco Tower, Media City, Dubai, U.A.E. Tel: +971 4 3769555, Fax: +971 3928549 P.O.Box 23816.
Endodontics
• Palatal root
- Number of canals:
In the present study,the palatal root had in 100% of cases only one canal whitch agrees with the findings of Médioni et al. 24 and Sert et al. 6 Neelakantan et al 5 found only 87.7% of this root with one canal. According to all studies, types III and V did not exceed 6% 23, 20, 25 and type IV did not exceed 3.4% 5, 25 and type II was not found.
- Canals configurations: All studies confirmed that the type I is predominant with a percentage that varies from 87.8%5 to 100%. 24, 6 Other configurations have a percentage not exceeding for the type III 6% 20, 23 , for the type IV 3.4% 5, and for the type V 6%.23 the type II is absent for all studies 24, 23, 5, 6, 20, 25 (table 8).










Before

After 10 minutes
new HOME WHITENING TO GO
Opalescence GO, the professional alternative for home whitening:
• Simple, fast and great-tasting
• No impressions or custom trays necessary
• Ready to use
• 10% & 15%, 15 to 60 minutes wear for a 5 to 10 days treatment
• UltraFit tray adaptable to any smile
• 20% of water with Potassium Nitrate and Fluoride
30
Study Sert et al. 6 Population Canals configurations
Weng et al. 23 Chinese Korean Turkish Médioni et al. 24 Kim et al. 20 Altunsoy et al. 25 French Turkish Neelakantan et al. 5 Touzi et al. Indian Tunisian V 6% 0% 0% IV 0% 0% 0.1% III 0% 0% 0% Year Sample I 2009 50 2012 775 2014 1305 II 94% 6% 94% 6% 99.8% 0.1% 1994 Not defined 2010 230 2010 2015 191 98 100% 0% 100% 0% 87.8% 0% 100% 0% 0% 0% 0% 0% 0% 0% 3.4% 0% 0% 0% 0.9% 0%
(classification of Vertucci)
Table 8: canals configurations in the Palatal root
ULTRADENT PRODUCT INC. - 1 888 230 1420 - info@ultradent.com - www.ultradent.com
The absolute disinfection for Endodontics !

Irrigation
EFFICIENT ROOT CANAL CLEANING
PATENTED CONCEPT
Disinfection
Tip oscillation to allow perfect disinfection.





IRRIGATYS : the new two-in-one handpiece with dual functions
Two-in-one system provides and activates liquid for the perfect clean.
A removable tank allows the irrigation of the root canal with Hypochlorite and EDTA. The irrigation line leads the solution through the Irriga-Tip This patented technology, developed after 6 years of research, optimizes the result of the complex procedure of root canal irrigation.





Class IIa medical device. CE0120. For dental healthcare professional use only. Certifying body SGS United Kingdom LTD. Date of creation 02/02/15
Endodontics
Conclusion
The present study showed that most of maxillary first molars were 3 rooted (93%), 5.8% were 2 rooted and 1.1% presented one root. In the mesio buccal root, the most prevalent configuration was type I (97.5%), type II represented 2.5%. In the disto buccal root and in the palatal root, we found vertucci type I on 100% of cases.
References
1. Pécora Jd, Woelfel JB, sousa neto Md, issa eP. MorPhologic study of the Maxillary Molars. Part ii: internal anatoMy. BraZ dent J 1992; 3: 53-57.
2. Betancourt P, navarro P, cantín M, fuentes r cone-BeaM coMPuted toMograPhy study of Prevalence and location of MB2 canal in the MesioBuccal root of the Maxillary second Molar int J clinexP Med 2015; 8:9128-34.
3. alrahaB M, Zafar Ms evaluation of root canal MorPhology of Maxillary Molars using cone BeaM coMPuted toMograPhy. Pak J Medsci 2015; 31:426-30.
4. liBfeld h, rotsteini incidence of four-rootedMaxillary second Molars: literaturerevieW andradiograPhicsurvey of 1200 teeth. J endod 1989; 15: 129-31.
5. neelakantan.P,suBBarao c, Bds, ahuJa r, suBBarao c v, and gutMann.J.l cone-BeaM coMPuted toMograPhy study of root and canal MorPhology of Maxillary first and second Molars in an indian PoPulation, Journal of endodontic 2010; 36: 1622-07.
6. sert s, sahinkesen g,toPcu f t eroglu s e and oktaye a root canal configurations of third Molar teeth a coMParisonWith first and second Molars in the turkish PoPulation aust endod J 2011; 37: 109–17.
7. gu y ,Wang.W , ni l four-rooted PerManent Maxillary first and second Molars in a northWestern chinese PoPulation, archives of oral Biology 2015 ;60: 811–7.
8. Peikoff Md, christie Wh, fogelhM. the Maxillary second Molar: variations in the nuMBer of roots and canals int endod J 1996; 29: 365-9.
9. al-fouZan ks, ounis hf,Merdad k and al-heZaiMi k incidence of canal systeMs in the Mesio-Buccal roots of Maxillary first and second Molars in saudi araBian PoPulation aust endod J 2013; 39: 98–101.
10. kulild Jc, Peters dd incidence and configuration of canal systeMs in the MesioBuccal root of Maxillary first and second Molars. J endod 1990; 16:311-7.
11. oZcan e, aktan aM, ari h a case rePort: unusual anatoMy of Maxillary second Molar With 3MesioBuccal canals oral surg oral Med oral Pathol oral radiol endod 2009;107: 43-6.
12. holderrieth s, gernhardtcr. Maxillary Molars With MorPhologic variations of the Palatal root canals: a rePort of four cases. J endod 2009;35:1060-5.
13. Weller rn, hartWell gr the iMPact of iMProved access and searching techniQues on detection of the Mesiolingual canal in Maxillary Molars. J endod 1989; 15: 82–3.
14. singh c, sikri vk, arora r study of root canals and their configuration in Maxillary second PerManent Molar indian J dent res 1994; 5:3-8.
15. stroPko JJ. canal MorPhology of Maxillary Molars: clinical oBservations of canal configurations. J endod 1999; 25: 446-50.
16. alavi aM, oPasanon a, ng yl, gulaBivala k root and canal MorPhology of thai Maxillary Molars int endod J 2002; 35: 478–85
17. doMark Jd, hatton Jf, Benison rP, hildeBolt cf an ex vivo coMParison of digital radiograPhy and cone-BeaM and Micro coMPuted toMograPhy in the detection of the nuMBer of canals in the MesioBuccal roots of Maxillary Molars, J endod 2013 ;39:901-5.
18. rWenyonyi cM, kutesa aM, MuWaZi lM, BuWeMBoW. root and canal MorPhology of Maxillary first and second PerManent Molar teeth in a ugandan PoPulation int endod J 2007; 40: 679-83.
19. y-l ng, t h aung, a alavi& k gulaBivala. BlackWell science, ltd root and canal MorPhology of BurMese Maxillary Molars international endodontic Journal, 2001;34: 620–30.
20. kiM y, lee sJ, Woo J. MorPhology of Maxillary first and second Molars analyZed By cone-BeaM coMPuted toMograPhy in a korean PoPulation: variations in the nuMBer of roots and canals and the incidence of fusionJournal of endodontics2012;38: 1063-8.
21. caliskan Mk, Pehlivan y, sePetçioglu f, türkün M, tuncer ss root canal MorPhology of huMan PerManent teeth in a turkish PoPulation. J endod 1995; 21: 200-4.
22. yoshioka t, kikuchi i,fukuMoto y, koBayashi c&suda h detection of the second MesioBuccal canal in MesioBuccal roots of Maxillary Molar teeth ex vivo international endodontic Journal 2005; 38:124–8.
23. Weng x l,yu,s.B,Zhao sl,Wang hg,Mu t,tang ry,Zhou xd,root canal MorPhology of PerManent Maxillary teeth in the han nationality in chinese guanZhong area: a neW Modified root canal staining techniQue. Journal of endodontics 2009; 35: 651–6.
24. Médioni e, vené g anatoMie endodontiQue fondaMentale et cliniQue encycl Med chir (Paris, france), stoMatologie odontologie, 23-050-a-05, 1994, 10P
25. altunsoy M, et al root canal MorPhology analysis of Maxillary PerManent first and second Molars in a southeastern turkish PoPulation using cone-BeaM coMPuted toMograPhy, Journal of dental sciences 2014;20: 1-7.
Dental News, Volume XXIII, Number I, 2016
32


BENEFITS CONELOG® offers benefits!
The CONELOG®
offers a comprehensive prosthetic
The conical implant/abutment connection with its proven CAMLOG positioning
three grooves and
provides maximum precision
user-friendliness. More
CAMLOG® offers benefits! Millionfold proven SCREW-LINE outer geometry Simple abutment positioning through three grooves and cams Excellent conical connection Highly precise transfer without transfer aid High radial position precision 7 mm implants optionally available
www.camlog.com
Implant System
portfolio for all indications.
through
cams
and
infos: www.camlog.com
Orthodontic management of an impacted mandibular canine in a 14 years old Kuwaiti girl.

Dr. Saud A. Al-Anezi BDS (Liverpool, UK), MFD RCSI, Doctorate in Orthodontics (Bristol, UK), MOrth RCSEd saudalan@gmail.com
Department of Orthodontics, Bneid Al-Gar Specialty Dental Center, Ministry of Health, Kuwait.
Key words
Impacted canines, Orthodontic treatment, Surgical exposure.
Introduction
An impacted tooth can be defined as a tooth with a delayed in eruption time or that are not expected to erupt completely based on clinical and radiographic assessment. 1 An impacted tooth in children is a major problem with potentially damaging sequelae such as, damage to the adjacent teeth and cystic formation. The prevalence of impacted maxillary canine is reported to be 1.5% 2, however, the prevalence of impaction of the mandibular canine is much lower. 3,4 In one particular study, the incidence of mandibular canine impaction was shown to be 1.29% in 5022 individuals of a Turkish population sample. 5 Clinicians should suspect impaction if the canine is not palpable in the buccal sulcus by the age of 10–11 years, hence a full clinical examination and radiographic assessment are essential in order to locate the canines. 6 There are many etiological factors that can lead to the failure of eruption such as the presence of a supernumerary tooth that prevents the successful eruption of the canine. Early diagnosis of such problem will make the treatment simpler and in some cases shortens the treatment duration. The aim of this report is to illustrate a conventional orthodontic treatment of an impacted mandibular canine which was diagnosed late.
Clinical Presentation and Intervention
A 14 years old Kuwaiti girl attended the clinic complaining of “a gap between bottom teeth” (Fig 1). She was fit and well. She had a Class 1 skeletal pattern with average vertical proportions. In
the intra-oral examination, it was found that, her oral hygiene was fair and required improvement prior to the initiation of orthodontic treatment (Fig 2). Furthermore, there was mild crowding in the mandibular arch and well aligned maxillary arch. The overjet was increased with an average overbite and a mild central line discrepancy. The buccal segments were Class 1.







Dental News, Volume XXIII, Number I, 2016 22 Orthodontics
Figure 1. Pre-treatment Extra-oral photographs.
Figure 2. Pre-treatment Intra-oral photographs.
Fig 1
Fig 2


Surf the canal with confidence
WAIT IS OVER















CS 8100 3D 3D imaging is now available for everyone


Many have waited for a redefined 2D/3D multifunctional system that was more relevant to their everyday work, that was plug-and-play and that was a strong yet affordable investment for their practice. With the CS 8100 3D, that wait is over.
• Versatile programs and views (from 8 cm x 9 cm to 4 cm x 4 cm)
• New 4T CMOS sensor for detailed images with up to 75 μm resolution
• Intuitive patient placement, fast acquisition and low dose
• The new standard of care, now even more affordable
LET’S REDEFINE EXPERTISE
The CS 8100 3D is just one way we redefine imaging. Discover more at carestreamdental.com









All permanent dentition were present except for the lower right manbibular canine and the third molars. Further investigations revealed that the tooth was lingually displaced with no presence of any supernumerary or any other obstruction preventing its eruption (Figure 3). The treatment plan was to initiate a fixed orthodontic appliance therapy to create more space for the mandibular canine then carry on a surgical exposure procedure to uncover the tooth and enable its traction through the orthodontic appliance using an 0.22 inch slot, MBT prescription. Treatment started with leveling and alignment through 0.14 and 0.18 inch Nickel Titanium wires. Furthermore, the treatment continued through 0.19x0.25 NiTi and Stainless Steel archwires to achieve the treatment objectives (Figure 4). A retention regime was also planned which included a fixed retainer in the lower arch to minimize the risk of relapse of the impacted canine after alignment plus an upper and lower removable retainers.




Dental News, Volume XXIII, Number I, 2016 © Carestream Health, Inc. 2015.
THE
Figure 3. Pre-treatment radiographs.
Figure 4. During the surgical exposure procedure and photographs of following visits.
Fig 3
Fig 4




GAME
TURN CLASS II INTO SIMPLE CLASS I PATIENTS Class II corrected in 3 months, 1 week Total treatment time 13 months Simplicity, ease-of-use, and patient compliance add up to fast, more predictable results. With its sleek, aesthetic, and non-invasive design, the Carriere ® Motion™ Appliance shortens treatment time by up to four months. Easier than Herbst ®, simpler than Forsus ®, and faster than elastics alone, the Carriere Motion Appliance can be a real game changer for your practice. CARRIERE MOTION CLASS II APPLIANCE Learn more about the Carriere ® Motion™ Appliance at OrthoOrganizers.com l +1 (760) 448.8600 ©2015 Ortho Organizers, Inc. All rights reserved. U.S. Patent No. 7,618,257, 6,976,839, and 7,238,022 and foreign patent numbers 2,547,433, 1723927, and 2006202089. All trademarks or registered trademarks belong to their respective company(s). M710 12/15
CHANGER
Molar Ball & Socket
Sleek and Non-Invasive
Fixed Cuspid Pad with Hook
Discussion
Although the impaction of a mandibular canines is not frequently occurring episode compared to maxillary canines, those individuals with this problem may suffer potentially harmful effects if left untreated. The impacted maxillary canine is extensively discussed and mentioned in the dental literature unlike the mandibular canine. The key factor here is 7 the early diagnosis, because that will allow some simpler measures such as the removal of the deciduous tooth at the appropriate time. This would enable the permanent canine to follow its course and erupt normally. However, as children grow older (i.e. beyond the age of 12-13 years), the use of this simple “interceptive” measure is no longer feasible and more comprehensive treatment should be considered. 1 The treatment options then are categorically divided into two: 1) either to attempt to orthodontically align the tooth with or without surgical intervention, or 2) extraction of the tooth and replace it with a dental implant. The definitive treatment plan can be decided on several factors such as the age of the treatment 5, the age of the patient, the more likely orthodontic treatment will work and vice versa. Another factor is the position of the impacted tooth.4 If the tooth, as in this case report, was not far away from its original place, it is considered favorable to surgically expose it and align it orthodontically.8 This is decided after a careful clinical and radiographic examination. Another extremely useful tool that can be used is the use of a Cone Beam Computed Tomography (CBCT) scan 9 , however, this was not available to the author at the start of treatment. It can be stated that, if the tooth was positioned deep in the bone and the surgical removal of it bears many risks, as an alternative, the tooth can be left in situ providing regular monitoring of the tooth, in order to detect any changes that may occur.
Another treatment option is to auto-transplant the tooth (i.e. to extract it surgically and reimplant it in its place), nonetheless, that approach has very poor prognosis and very rarely considered as an option. 10,11 It must emphasized that for each treatment option, there are advantages and disadvantages. For instance, if orthodontic
treatment with surgical exposure plan was chosen, treatment duration may be long as opposed to the extraction and the implant option which takes shorter treatment duration to accomplish. However, the main advantage with the orthodontic treatment approach is that a prosthesis is not required and an ideal occlusion can be achieved (Figure 5).




Conclusion
Impacted maxillary canines are more common than mandibular canines. The treatment plan for such teeth will be based on several factors such as the age of the patient and the position of the tooth. Treatment options includes orthodontic treatment to align the tooth or removal of the tooth and replace it with a dental implant. This girl was treated successfully via surgical exposure and orthodontic alignment because the position of the impacted canine was favorable.
Informed consent:
Permission was granted by the patient and her father to use her clinical records in this case report.
Dental News, Volume XXIII, Number I, 2016 38 Orthodontics
Figure 5. Post-treatment Intra-oral photographs.
Fig 5

The award-winning TRIOS ® intraoral scanner gets your patients back up on the horse quickly. TRIOS ® 3 makes your work more efficient, more precise and your patients, more comfortable.
Three solutions in one:
• Intraoral scanner for fast, easy-to-do 3D real color digital impressions
• Digital shade measurement while you scan – for more accurate and predictable results

• Integrated intraoral camera included in the scanner

nothing but
Visit www.3shape.com/TRIOS for a full presentation
When
the best will do
Acknowledgments
I would like to thank Dr. Joju George from the Oral Surgery Department in Bneid Al-Gar Specialty Dental Center for his great contribution in the tooth exposure stage. I would also like to extend my appreciation to patient and her father for their remarkable cooperation throughout the course of treatment. A special thank for my assistance, Deepa for her immense help.
References
1. richardson g, russell ka a revieW of iMPacted PerManent Maxillary cusPids: diagnosis and Prevention. J can dent assoc 2000;66:497-501.
2. ericson s and kurol J. radiograPhic exaMination of ectoPically eruPting Maxillary canines aM J orthod 1987; 91: 483-492.
3. aydin u, yilMaZ hh, yildiriM d incidence of canine iMPaction and transMigration in a Patient PoPulation dentoMax radiol 2004; 33:164-9.
4. alaeJos-algarra c, Berini-aytes l, gay-escoda c transMigration of Man-diBular canines: rePort of six cases and revieW of the literature. Quint int. 1998; 29:395-398.
5. yavus Ms, aras Mh, Buyukkurt Mc, toZoglu s iMPacted MandiBular canines. J of conteMPorary dent Practice. 2007; 8(7):2-9.
6. the ManageMent of the Palatally ectoPic Maxillary canine national clinical guidelines the royal college of surgeons of england, WWW rcseng ac uk, March 2010.
www.promedica.de to see our upcoming exhibitions
Light-curing nano-ceram composite
• nano-reinforced ceramic particles
• special resin matrix

• significantly less free monomers
• highly esthetic
• universal for all cavity classes
• comfortable handling, easy modellation
• also available as a flowable version
7. ericson s and kurol J. radiograPhic assessMent of Maxillary canine eruPtion in children With clinical signs of eruPtion disturBances eur J orthod 1986; 8: 133-140.
8. Mcsherry Pf the ectoPic Maxillary canine: a revieW. Br J orthod 1998; 25: 209-216.
9. yh Jung, h liang, BW Benson, dJ flint, Bh cho the assessMent of iMPacted Maxillary canine Position With PanoraMic radiograPhy and cone BeaM ct dentoMaxillofac radiol 2012: 41(5): 356-360.
10. thoMas s, turner sr, sandy Jr autotransPlantation of teeth: is there a role? Br J orthod 1998;25: 275–82.
11. cZochroWska eM, stenvik a, BJercke B,Zachrisson Bu outcoMe of tooth transPlantation: survival and success rates 17-41 years PosttreatMent aM J orthod dentofacial orthoP 2002;121: 110–19.

Dental News, Volume XXIII, Number I, 2016 40
Orthodontics
phone: +49 4321 / 5 41 73 - fax: +49 4321 / 5 19 08 - Email: inf Dental Material GmbH PROMEDICA
self cure
self curing, tooth remineralising
glass
ionomer restorative material
• Strong dentine replacement
• BPA & HEMA free

• High fluoride releasing and recharging ability
• No shrinkage
• Great marginal adaptation
• High acid resistance
Also available in powder liquid


non-stick GIC riva


Authorised SDI Distributors: Also available in high viscosity
Algeria Expert Dental Industry 00 213 36 93 94 93 expert_dental_industry@yahoo.fr
Bahrain Gulf Pharmacy & Gen. Store 97317239387 orders@gctbahrain.com
Eqypt Zaident Dental Supply 202 3760 1582 Zaident@link.net
Iran Kazemeini Trading Co. 98-21-8884-9977 kazemeini3@hotmail.com
Iraq Himat Co. Ltd 964 7901 317209 (Mobile) marketing@himat.net
Jordan Khoury Dental Establishment 962-6-5827015 dental@khds.jo
Kenya Dentmed (K) Ltd 254 722 523697 infinity@iconnect.ko.ke
Kuwait Safwan Trading & Contracting CO. 965 22276888 blubbad@safwantrading.com
Lebanon ETA Assy Trading Dental Supply 961 381 371 denassy@cyberia.net.lb
Libya Al - Magd Co. 218 21 3610154 nasdent@yahoo.com
Mauritania Espace Dentaire 222 48 00 48 48 espacedentaire.mr@gmail.com
Morocco Medico Dentaire S.A.R.L. 212 522364482 medent1@menara.ma
Morocco Aire Dentaires
212 55 62 26 31 ouhazza@menara.ma
Oman Health City Projects LLC 968 2448 9319 mushtaq.ahmed@healthcityprojects.com
Palestine Al - Manara Distribution Center 972 2 295 3718 kshatara@p-ol.com
Palestine Solila Dental Center 972 8 282 8486 solila@palnet.com
Qatar Al Romani Trading Centre 974 5528743 romani63@qatar.net.qa
Saudi Arabia M/S Commercial & Maintenance Company 966-1-463-3361 najm.alhoda@comate.com
Sudan Zaident Dental Supply 202 3760 1582 Zaident@link.net
Syria Al Kurdi Store 963-11-222-2336 alkurdi@net.sy
Tunisia New Med 216 74 401 254 newmed@gnet.tn
UAE Al Sahab General Trading 971-6-7470260 kazemeini3@hotmail.com
Uganda The Medical Warehouse LTD 256 312 516 954 themedicalwarehouse@gmail.com
Yemen Dieda Corp For Drugs & Medical Appliances 967 1 278557 dieda@y.net.ye

Your Smile. Our Vision. www.sdi.com.au www.polawhite.com.au

SDS 2016
16th King Saud University International Dental Conference & 27th for the Saudi Dental Society
January 5 - 7, 2016
Riyadh International Convention & Exhibition Center - KSA


Opening ceremOny under the patrOnage Of hrh emir faisal Bin Bandar Bin aBdulaziz alsaud left tO right; prOf. thakiB alshalan, dr Badran alOmar, prince Of riyadh, dr. ahmed alaameri, dr mOhamed al OBeida


It is with great pleasure to welcome you to the 16th King Saud University International Dental Conference and the 27th for the Saudi Dental Society.
The theme for this year’s conference is “Regenerative Dentistry”, which is based on the natural ability of body cells and tissues to restore themselves under certain conditions. Owing to advances in modern science, we now know more about the mechanisms behind every tissue in the body to self-repair. Those mechanisms are being investigated further as we learn that living cell regeneration is dependent on many factors such as genetics, hormones and environmental influences.
The conference also allows for diversity of research covering other fields of Dentistry through oral presentations
and posters and it also offers full state exhibits which show the current trend in dental materials, instruments and equipment.
To all speakers, participants and exhibitors, my very best wishes for a successful meeting. I hope that you will enjoy the conference and that your interaction with your colleagues will stimulate a creative exchange of ideas and will be personally rewarding.
Prof. Thakib A. Al Shalan Dean, College of Dentistry Chairman, Organizing Committee
16th Saudi International Dental Meeting
27th for the Saudi Dental Society
Dental News, Volume XXIII, Number I, 2016 42
More Pictures Available On www.facebook.com/dentalnews1
eli chedid receiving the trOphy Of care the main spOnsOr
prOf. thakiB al shalan
Henry Schein is a name you can trust
Henry Schein is the largest global dental distributor of health care products and Services to general practitioners, specialists and laboratories throughout the world. Our network of exclusive Henry Schein Middle East Distributors offer dentists a complete portfolio from the following high-quality and value-priced consumable and equipment product manufacturers that you can rely on to fulfill your practice needs.




Henry Schein Exclusive Partners Henry Schein Exclusive Supplier Partners Dubai, UAE Dubai, Business Bay, Churchill towers – Office tower, office 1115, contacts: Tel: +971 6 5252842 • Fax: +971 6 5531291 • Mobile: +971 50 4813292 www.scheinexport.com



 hrh emir faisal Bin Bandar Bin aBdulaziz cutting the riBBOn Of the exhiBitiOn flOOr
dr. patrick hescOt, president Of the fdi with prince faisal
left tO right: drs ahmed shamiah, alessandrO agnini, andrea mastrOrOsa, mOhamed shehri, faysal alshail, mOhamad alkatheri
left tO right: dr. tOny diB, dr. waseem radwan, dr. hassan halawani, mr Jamil asmar
hrh emir faisal Bin Bandar Bin aBdulaziz cutting the riBBOn Of the exhiBitiOn flOOr
dr. patrick hescOt, president Of the fdi with prince faisal
left tO right: drs ahmed shamiah, alessandrO agnini, andrea mastrOrOsa, mOhamed shehri, faysal alshail, mOhamad alkatheri
left tO right: dr. tOny diB, dr. waseem radwan, dr. hassan halawani, mr Jamil asmar

Turnstr. 31 I 75228 Ispringen I Germany I Phone + 49 72 31 / 803 - 0 I Fax + 49 72 31 / 803 - 295 www.dentaurum-implants.com I info@dentaurum-implants.com A Dentaurum Group company YES I WANT THE COMPLETE CAD/CAM SOLUTION. Innovation has a name: tioLogic® digital. Your step towards digital implantology. Say yes!

pr yOusef talic giving the certificate tO pr seBastian cianciO frOm BuffalO



pr saad al nazhan giving the certificate tO dr marcO martignOni frOm rOme

exhiBitiOn flOOr SDS 2016



BEFORE
Open tubules AFTER
Closed tubules in 60 SECONDS with Colgate® Sensitive Pro-Relief™ Toothpaste*
Extensive scientific research has shown that Colgate® Sensitive Pro-Relief™ protects against the triggers and causes of sensitivity, and is proven to occlude dentin tubules in 60 seconds.*
Finally, a way to quickly improve your patients’ satisfaction and comfort.

BRAND RECOMMENDED BY DENTISTS 1 # BRAND RECOMMENDED BY DENTISTS www.colgateprofessional.com YOUR PARTNER IN ORAL HEALTH www.colgateprofessional.com PATIENT SENSITIVITY CAN BE GONE IN SECONDS. COLGATE® SENSITIVE PRO-RELIEF
PRO-ARGIN™ TECHNOLOGY PROVIDES INSTANT AND LONG-LASTING RELIEF.
™ WITH
*When toothpaste is directly applied to each sensitive tooth for 60 seconds.
Ayad F, Ayad N, Delgado
E, et al. J Clin Dent. 2009;20(4):115-122.


exhiBitiOn flOOr SDS 2016




 left tO right: dr. essam haidary, dr patrick hescOt president Of the fdi, dr mOhamed al OBeida president Of the sds, dr nizar kadi, dr. tOny diB
left tO right: dr. essam haidary, dr patrick hescOt president Of the fdi, dr mOhamed al OBeida president Of the sds, dr nizar kadi, dr. tOny diB
Sensodyne Repair & Protect
Presenting a new layer of protection

Sensodyne Repair & Protect harnesses advanced NovaMin® technology to help build a robust hydroxyapatite-like layer over exposed dentine and within dentine tubules.1–5 With Sensodyne Repair & Protect, you can do more than treat the pain of dentine hypersensitivity – you can repair and protect your patients’ exposed dentine.



Think beyond
relief and recommend Sensodyne Repair & Protect
pain
For full information about the product, please refer to the product pack. For further information please contact your doctor/healthcare professional. For reporting any Adverse Event/Side Effect related to GSK product please contact us on contactus-me@gsk.com Date of Preparation: June 2014, CHSAU/CHSENO/0063/14 Arenco Tower, Media City, Dubai, U.A.E. Tel: +971 4 3769555, Fax: +971 3928549 P.O.Box 23816. We value your feedback Saudi Arabia: 8008447012 All Gulf and Near East countries: +973 16500404 References: 1. Burwell A et al. J Clin Dent 2010; 21(Spec Iss): 66–71. 2. LaTorre G, Greenspan DC. J Clin Dent 2010; 21(3): 72-76. 3. West NX et al. J Clin Dent 2011; 22(Spec Iss): 82-89. 4. Earl J et al. J Clin Dent 2011; 22(Spec Iss): 62-67. 5. Efflandt SE et al. J Mater Sci Mater Med 2002; 26(6): 557-565. Prepared December 2011, Z-11-516.

2 - 4,

More than 1,800 Exhibiting Companies & Over 40,000 Participants
Under the patronage of His Highness Sheikh Hamdan Bin Rashid Al Maktoum, His Excellency Humaid Mohammed Obaid Al Qatami, Chairman of the board of the Dubai Health Authority inaugurated the 20th edition of the AEEDC Dubai.
This year, AEEDC Dubai 2016 celebrated its 20th anniversary with the participation of regional and international officials, a number of delegations from 130 countries top-notch speakers and more than 1800 exhibitors His Excellency was delighted by hearing from the exhibitors about the latest technologies and accomplishments that the manufacturing companies had reached in the field of dentistry.
Dr. Abdul Salam Al Madani, Executive Chairman of AEEDC Dubai Conference and Exhibition and the Global Scientific Dental Alliance stated: “This is a very special edition for AEEDC as we are celebrating its 20th anniversary and 20 years of achievement and global recognition. We are also proud that AEEDC Dubai retains its number one position among the MENASA region and remains to be the 2nd largest dental conference and exhibition in the world.
Dr. Abdul Salam went on saying: “This year AEEDC Dubai features two new specialized conferences to enrich the Oral & Maxillofacial Surgery and Orthodontic fields. The scientific agenda for this year is tailored with excellence, a number of outstanding scientific activities took place during the three day event which makes AEEDC Dubai the best educational platform and a good source of attaining credit hours for specialists and dentists.”
AEEDC Dubai 2016 features a rich agenda that includes various scientific activities like the GCC Preventive Dentistry Conference, AEEDC Advanced Specialty Courses, 20 specialized courses & workshops, more than 100 Poster and Oral Poster Presentations, the 7th AEEDC Student Competition with the participation of 6 universities, the Global Scientific Dental Alliance Meeting, and the AEEDC Dubai Awards.
On the other hand, AEEDC Dubai exhibition spreads over more than 62,000 square meters of space with leading local and international companies and industry leaders showcasing medical and dental equipment and innovations. AEEDC 2016 Exhibition features also 16 national pavilions primarily from Brazil, China, Finland, France, Germany, Italy, Japan, Korea, Russia, Spain, Slovenia, Switzerland, Turkey, United Arab Emirates, United Kingdom, and United States of America.
Dental News, Volume XXIII, Number I, 2016
2016 Dubai International Convention & Exhibition Center, UAE 50 More Pictures Available On www.facebook.com/dentalnews1
February
picture frOm the Opening ceremOny

INAUGURATION




OF
THE EXHIBIT FLOOR

á«`≤«≤`M IQƒ`K


Admira Fusion
Iô°TÉÑŸG äGƒ°ûë∏d ⁄É©dG ‘ ∫h’G ±õÿG • √óMh ±õÿG ¤G óæà°ùJ ⁄É©dG ‘ º«eôJ IOÉe ∫hCG
¢ü∏≤àdG ó¡÷ ¢†Øîæe iƒà°ùeh (ºé◊G øe %1^25) ¢†Øîæe Iôª∏H ¢ü∏≤J
• á«fƒ∏dG äGÒ¨à∏d GóL ΩhÉ≤eh ‹ÉY …ƒ«M πÑ≤J hP ƒ¡a Gòd ,Éjhɪ«c πeÉN • á«Ø∏ÿGh á«eÉe’G ≥WÉæŸG ‘ äÉÑ∏£àŸG ≈∏YG »Ñ∏j
èFÉàf É¡∏c øª°†J í£°ù∏d á«dÉY IhÉ°ùbh π¡°S ™«ª∏J ,RÉà‡ Ò°†– ܃∏°SCG ióŸG á∏jƒW IRÉà‡ • ájó«∏≤àdG ≥°ü∏dG OGƒe πc ™e ∫ɪ©à°SÓd ídÉ°U
@ ójóL âjRƒÑeƒμdG øe ájó«∏≤àdG ƒ°û◊G OGƒe ™e áfQÉ≤ŸÉH
VOCO GmbH · Anton-Flettner-Straße 1-3 · 27472 Cuxhaven · Germany · Tel. +49 4721 719-0 · www.voco.com
•
@
•
ójóL G’B¿ S°ÉFπ°µπ




 dr aBdulsalam al madani with representatives frOm arOund the wOrld
with dr khalid el Badr president Of the saudi OrthO sOciety
with dr hussein lawati president Of the Oman dental sOciety
left tO right: drs khalid alBadr, aBdulwahaB alawadi, sami maneh, salah Bulushi
with dr fahad al shehri president Of the sds
dr aBdulsalam al madani with representatives frOm arOund the wOrld
with dr khalid el Badr president Of the saudi OrthO sOciety
with dr hussein lawati president Of the Oman dental sOciety
left tO right: drs khalid alBadr, aBdulwahaB alawadi, sami maneh, salah Bulushi
with dr fahad al shehri president Of the sds







56













Head Office Researchpark
Haasrode-Leuven 1240
Interleuvenlaan 33
B-3001 Leuven
Tel. +32.16.74.10.00 Fax. +32.16.40.48.32
info@gceurope.com http://www.gceurope.com
Essentia & G-Premio BOND from GC No
compromises, aesthetic restorations taken to the next level GC EUROPE N.V.



DENTAL NEWS WALL OF FAME

















ENDO POWER

HyFlex™ EDM THE NEW NITI FILE GENERATION








Extremely break resistant le for quick preparation























> Up to 700% higher fracture resistance
> Specially hardened surface











ORIFICE OPENER (optional) 25 / .12












Glidepath File 10 / .05
HyFlex™ OneFile 25 / ~




> Less lling required for treatment success







FINISHING FILES (optional)







40 / .04



50 / .03
60 / .02









































Dental News, Volume XXIII, Number I, 2016
www.coltene.com
CONTROLLED MEMORY

























LOOKING FOR THE HIGHEST QUALITY HANDPIECE AT THE LOWEST PRICE? YOU FOUND IT! For further information, contact your local dealer or B.A. International www.bainternational.com B.A. INTERNATIONAL Unit 9, Kingsthorpe Business Centre, Studland Road, Kingsthorpe, Northampton, NN2 6NE, United Kingdom. info@bainternational.com Available in 5 different fittings ULTIMATE POWER + ULTIMATE Thermodisinfectable Power Autoclavable Ceramic Bearings Fibre Optic Titanium Body 22w Thermodisinfectable Power Autoclavable Ceramic Bearings Fibre Optic “Smart Coat” 22w Longer Warranty! Available in the following fittings:
W&H Sirona Bien Air NSK Available in the
fittings:
KaVo
following
KaVo W&H Sirona Bien Air NSK





DENTAL NEWS WALL OF FAME









Dr Ghassan Naser Ditributing Trophies during the Henry Schein Dinner at the Grand Hyatt Hotel


 tO mr. paul daniel
tO mr. firas lellO
tO dr. mOhamad akar
tO mr. paul daniel
tO mr. firas lellO
tO dr. mOhamad akar

February 13 - 15, 2016


I would like to welcome each of you to the 4th Kuwait Dental Administration Conference, under the patronage of Kuwait Ministry of Health.
This is a biennial conference which goes with the mission of MOH, Kuwait to update and upgrade the knowledge and and skills of all involved with dentistry. The current conference is aptly themed as “Our Vision for a Better Tomorrow”. During this conference, a wide range of dental topics of interest will be deliberated. Selected topics range from Dental Marketing, different aspects of clinical dentistry, laboratory technology, Cone Beam Computed Technology, Behavior Management and Basic Life support techniques.
The organizing committee has left no stone unturned to ensure that this conference will be beneficial to all the personnel connected with dentistry. Hence we expect academicians, clinical dentists, students, nurses, technicians and researchers to be part of this exciting event.
On behalf of the Ministry of Health, Kuwait and the organizing committee, I welcome you all to be a part of this conference and take back some wonderful memories from here.
Dr. Sabiha Al Mutawa Chairperson, Director Dental Administration Ministry of Health - Kuwait
66
More Pictures Available On www.facebook.com/dentalnews1
Opening ceremOny under the patrOnage Of dr. ali al-OBaidi, minister Of health
Jumeirah Messilah Beach Hotel & Spa, Badriah Ballroom - KUWAIT
dr saBiha al mutawa chairpersOn Of the cOnference
95% said it was easy to use*
97% showed improved gum health** UP TO 99.9% plaque biofilm removal in the treated area*** UP TO


An FDI initiative
Proud Sponsor of





dr. yOusef al-dOueiry, the minister Of health, dr. saBiha al-mutawa mr ghassan mamlOuk, gOlden spOnsOr frOm atc h e dr ali al-OBaidi, minister Of health trOphy distriButiOn tO:
left tO right: dr. azhar naseeB, the minister Of health, dr. hashemy, dr. emady, dr. aisha sultan, dr. saBiha al-mutawa, dr. yOusef al-dueiry


dr. JOhn cassis lecturing On the geriatrics
dr. martin trOpe lecturing On BiOceramic technOlOgy

dr nawaf al-dOusary lecturing On restOring esthetics
dr. walter devOtO lecturing On indirect restOratiOns

 left tO right, drs.: ahmad asad, elhmeida, aBdullah al shammery, hashemy, salah Bulushi, tarek khOury, naser al malek
left tO right, drs.: maryam al-sharaf, hashemy, a. al-emady, saBiha al-mutawa, aisha sultan, azhar naseeB, tarek khOury, salahuddin Bulushi, yOusef dOueiry, tOny diB
left tO right, drs.: ahmad asad, elhmeida, aBdullah al shammery, hashemy, salah Bulushi, tarek khOury, naser al malek
left tO right, drs.: maryam al-sharaf, hashemy, a. al-emady, saBiha al-mutawa, aisha sultan, azhar naseeB, tarek khOury, salahuddin Bulushi, yOusef dOueiry, tOny diB


Lebanese Dental Association
Tripoli-Lebanon
8th International Meeting
April 21-22-23, 2016
Venue: University Of Balamand









 dr. sami maneh, president Of the kda in the middle, with dr. saud a. al-anezi
dr. sami maneh, president Of the kda in the middle, with dr. saud a. al-anezi

Dentsply Sirona: Merger Creates The Dental Solutions CompanyTM
YORK, PA (USA)/SALZBURG (AUSTRIA), February 29, 2016 – Dentsply Sirona Inc. (NASDAQ: XRAY) announced that it has successfully completed the merger of equals between DENTSPLY International Inc. (“Dentsply”) and Sirona Dental Systems, Inc. (“Sirona”). The merger of DENTSPLY, the market leader in dental consumables and Sirona, the market leader in dental technology and equipment, creates the world’s largest and most diversified manufacturer of professional dental products and technologies. Dentsply Sirona will have leading positions and some of the most well-established brands across consumables, equipment, technology, and specialty products to address the needs of dental professionals, specialists and dental labs. Each day, approximately 600,000 dental professionals will use a Dentsply Sirona product.With the largest R&D platform in the industry, Dentsply Sirona will develop and support innovative end-to-end clinical solutions that advance patient care.
Total Solution Provider
By combining DENTSPLY’s consumables platform with Sirona’s technology and equipment, the new company offers more products and integrated solutions than any other dental organization. Dentsply Sirona’s wide array of products for dental professionals and labs enable the treatment of general and specialty procedures including implantology, endodontics, and orthodontics. With the broadest clinical education platform in the industry, the company is driving the adoption of new and approved technology and integrated solutions for more efficient workflows. Customer service and satisfaction will remain a key value to the new company and will be supported by the industry largest sales and service infrastructure comprised of direct sales and leading distributors.

Two Innovation Drivers coming together
The merger unites the two leading innovators in dental, each with over 100 years of experience. Combined, Dentsply Sirona will have largest and strongest R&D platform with over 600 experienced scientists and engineers to foster the development of better, safer and faster dental care. With its enhanced commitment to innovation, the company will advance patient care, improve the patient experience and reduce chair time for procedures.
Jeffrey T. Slovin, Chief Executive Officer of Dentsply
Sirona comments: “With our merger complete, Dentsply Sirona can now focus its efforts on empowering dental professionals to provide better, safer and faster dental care. As The Dental Solutions CompanyTM, we will drive long-term growth by being uniquely positioned to deliver innovative solutions and support our customers with the broadest product portfolio and the largest sales and service infrastructure in the industry. Dentsply Sirona will continue to be at the forefront of the digitization of dentistry, single visit dentistry and improving clinical outcomes for patients around the world.”
Visit www.dentsplysirona.com for more information about Dentsply Sirona and its products.
Dental News, Volume XXIII, Number I, 2016 22








This new kit will suit you to realize quality root canal preparations thanks to the use of rotative single file for glide path One G and shaping One Shape® :
One Shape® Discovery Kit +:
2 One G blisters
3 One Shape® blisters
1 box Gutta Percha One Shape® Shaping
1 box Paper Points One Shape® Shaping
One Shape® Discovery Kit +, the simplicity and safety asset
• Simplicity: 1 only rotative single use instrument for glide path and shaping.
• Efficiency: time saving on the overall duration of treatment.
• Safety: controls risk of infections thanks to the sterile instrumentation.
Website: www.micro-mega.com
Medesy new periodontal micro-surgery kit
Nowadays periodontology has become extremely specialized, more complex and advanced thanks to the most recent developments in the treatment techniques and has created a demand for more sophisticated surgical instruments far more suitable for accurate dental interventions.
Medesy has replied to the precise needs of the professionals with a new specific kit created uniquely for periodontal micro surgery, a combination of instruments made in titanium, extremely light and purer than steel.
The kit is composed of the following items:
1. Titanium Scalpel Handle for micro blades
2. Molt Periosteal elevator and Periosteal HP3 both in titanium, they allow minimal traumatic detachment of the dental Papilla
3. Titanium Curved Micro tweezers excellent for meticulous suturing of the tissue.
4. Titanium Micro needle holder with smooth tips, for wires 8-0 /9-0, versatile instrument, ideal for use inside narrow interdental spaces.
5. Titanium curved micro scissors: like the needle-holder it has a very fine and precise tip for easy access in narrow areas.
Website: www.medesy.it


Dental News, Volume XXIII, Number I, 2016
its new
76
MICRO-MEGA® Presenting
One Shape® Discovery Kit +.
Aesthetic restorations from GC: More creativity, less complexity
GC is always striving to develop smart solutions for dentists’ daily challenges – which sometimes implies going against traditional concepts. In this respect, GC reveals a daring new approach to aesthetic dental restorations: Essentia. Essentia is developed together with a group of experts in aesthetics, does no longer rely on the traditional Vita® colours but on a very simple assortment of seven shades, created to mimic natural teeth at any patient’s age and offering dentists the maximum of creative freedom.

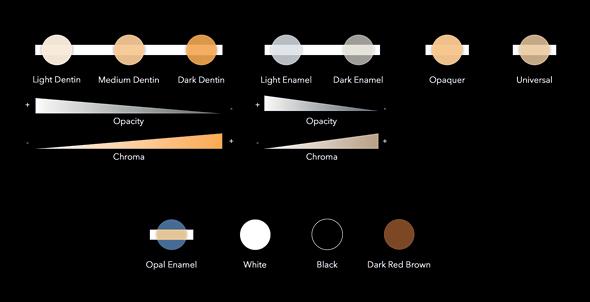
Improved plaque index and shallower pockets
Intensive oral care with Cervitec Gel improves the clinical treatment results of peri-implant mucositis.
Personal oral health care plays an important part in the long-term maintenance of implant-retained restorations. These measures are of particular importance in situations where mucositis has already developed, in other words, if the peri-implant soft tissue is inflamed. A successful treatment strategy for this type of case has been devised in the course of a clinical study conducted in Sweden.
Reduction in the bleeding on probing
The additional use of the oral care gel had a statistically significant effect on the reduction of the bleeding on probing (BOP) compared with the placebo gel. Moreover, the local plaque index in the test group improved and the periodontal pocket depth decreased.
High level of compliance
Throughout the study period, no staining of the teeth or disgeusia was observed or reported. The participants showed a high level of compliance for using the mild-tasting gel.
Website: www.ivoclarvivadent.com
By combining enamel and dentins, four main combinations following the patient’s age (Young, Junior, Adult & Senior) will make the shade selection become easier and will be sufficient to form the basis of any restoration – at any age.
On the other hand, knowing that the bonding is equally important, we accepted no compromises when developing our new universal bonding system.
G-Premio BOND is a one-bottle universal bonding compatible with all etching modes and which can be used not only for direct restorations, but also for repair cases & hypersensitivity treatment.
Its unique formula combining three functional monomers (4MET, MDP and MDTP) ensures excellent stability and bond strength not just to tooth tissue but to all indirect substrates, including composites, precious and non-precious metals, zirconia and alumina for all repair cases.
website: www.gceurope.com

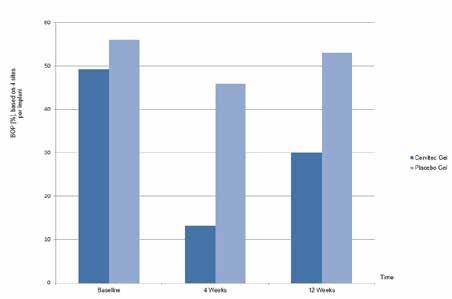

Dental News, Volume XXIII, Number I, 2016 78


Dentures contain surface pores in which microorganisms can colonise.1
Corega® cleanser is proven to penetrate the biofilm* and kill microorganisms within hard-to-reach surface pores.2


Help your patients eat, speak and smile with confidence with the Corega® denture care regime.

SEM images of denture surface. *In vitro single species biofilm after 5 minutes soak References: 1. Glass RT et al. J Prosthet Dent. 2010; 103(6): 384-389. 2. GSK Data on File, Lux R. 2012. For full information about the product, please refer to the product pack. For reporting any Adverse Event/Side Effect related to GSK product please contact us on contactus-me@gsk.com Date of preparation: June 2014, CHSAU/CHPLD/0008/14c We value your feedback Saudi Arabia: 8008447012 All Gulf and Near East countries: +973 16500404 Arenco Tower, Media City, Dubai, U.A.E. Tel: +971 4 3769555, Fax: +971 3928549 P.O.Box 23816.
Dry milling of zirconium oxide, acrylic resin, wax
• Wet-grinding capabilities for IPS e.max® CAD for Zenotec

• The IPS e.matrix multiholder maximizes productivity and flexibility




Dental News, Volume XXIII, Number I, 2016 all digital all options Manufacturer:
Wieland Dental+Technik GmbH & Co. KG Lindenstr. 2 75175 Pforzheim Germany Tel. +49 7231 3705 0 info@wieland-dental.de www.wieland-dental.de • Automated material changer for enhanced efficiency •
LEARN MORE: alldigitalalloptions.com The innovative milling system
IPS e.matrix with IPS e.max® CAD for Zenotec High precision and productivity The right milling option Distributor: www.ivoclarvivadent.com/distributors F U LL C O N TO U R ZIRCONIA ®
Zenostar® Telio® CAD for Zenotec
