















































Dental News, Volume XXIV, Number I, 2017





































Surgical Micromotor System Ultrasonic Bone Surgery System












Universal application – for all bonding procedures and etching techniques
Predictable results – high bond strength on wet or over-dried dentin delivery – available in bottles and the convenient VivaPen®











Molar Incisor Hypomineralization (MIH): Conservative Treatment Approach
Dr. Mayada Jemâa, Dr. H. Jegham, Dr. H. Ouertani, Pr. S. Marouane, Pr. L. Bhouri, Pr. MB. Khattech

Full mouth rehabilitation: a case report and review of the literature
Dr. Ali E Al-Kandari, Dr. Hassan Albakkar, Dr. Fatema N Alrayes, Dr. Abdulaziz

Interview with Dr. Patrick Hescot

Healthy teeth is Miss Universe advocacy

46.
SDA 2016
Sudanese Dental Association
9th International Dental conference & Exhibition
December 6 - 8, 2016
Friendship Hall - Khartoum, SUDAN
50.
60. SDS 2017
Saudi Dental Society
28th International Dental Conference
January 10 - 12, 2017
Riyadh International Convention & Exhibition Center, KSA
AEEDC 2017
February 7 - 9, 2017
Dubai International Convention & Exhibition Center, UAE
3SHAPE 51
ACTEON 37, 45
A-DEC 17
BA INTERNATIONAL 55
BEYOND 6
BIEN AIR 15
BISCO 9
CAMLOG 7
CARESTREAM 36
COLTENE 13
DENTAURUM 22
DENTSPLY SIRONA 41, 63
DURR 27
EMOFORM 4, 5
FKG 16
GC 31
GSK C3, 33, 39, 61
HENRY SCHEIN 57
ITENA 35
IVOCLAR 1, C4
KERR C2
MECTRON 30
MEDESY 67
MICRO MEGA 23
MORITA 53
NSK C1
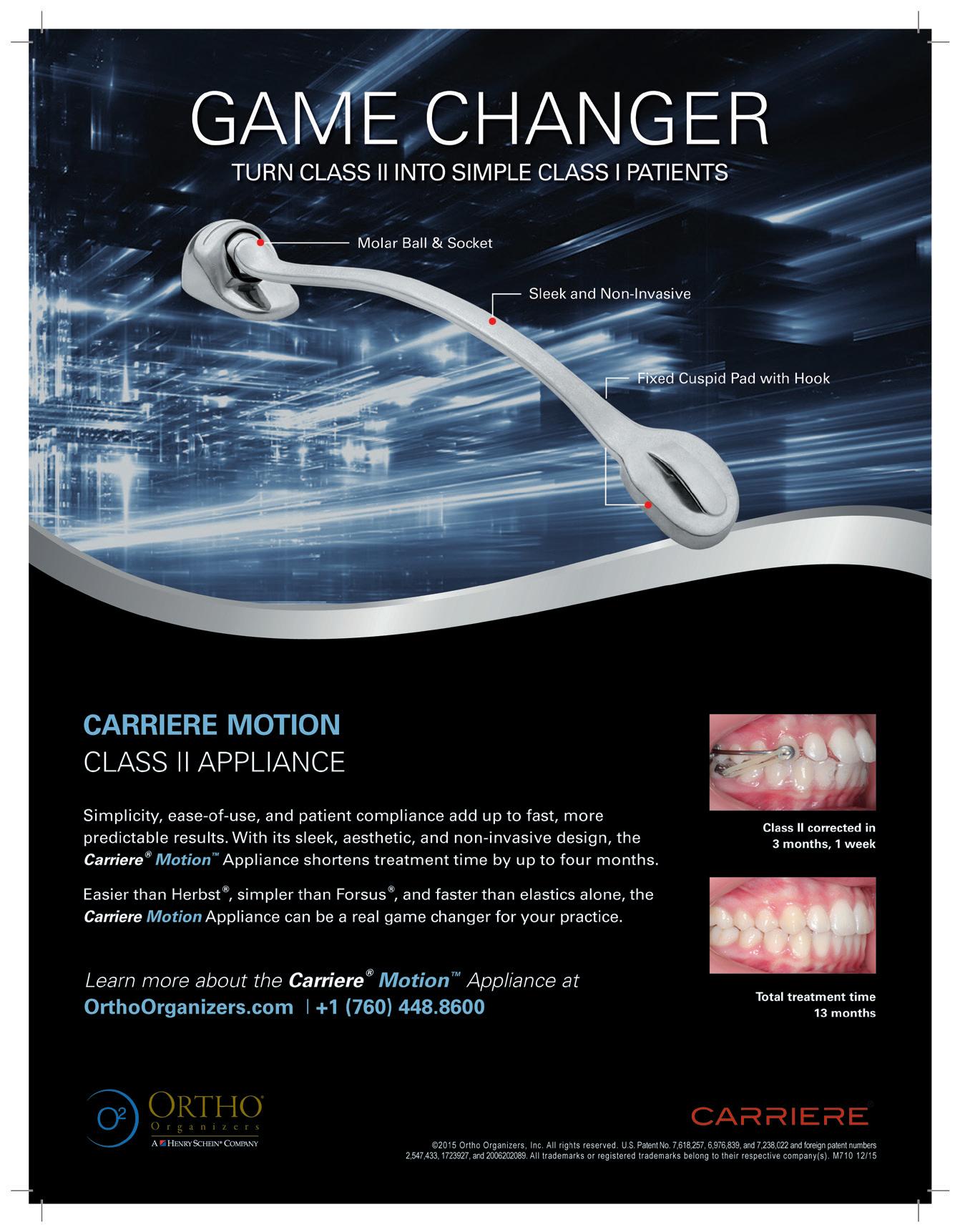
ORTHO ORGANIZERS 47
PLANMECA 29
PROMEDICA 26
RITTER 19
SCHEU 40
SDI 21
ULTRADENT GER 65
ULTRADENT USA 71
VOCO 59
W&H 10
ZHERMACK 2






The COMFOUR ™ Abutment System for occlusal screw-retainded restorations is an ideal addition to the CAMLOG ® and the CONELOG ® Implant System. With the COMFOUR™ System, you can offer your edentulous patients the option of an immediate, comfortable and permanent denture on four or six implants – and thus a considerable gain in quality of life. www.camlog.com


Angled bar abutment for the COMFOUR™ System, available in 17° and 30° angles

Anatomically shaped emergence pro le, lean design










Titanium bonding base for straight and angled bar abutments, Passive Fit
COMFOUR ™ offers you a range of options to overcome the challenges you face in your implant practice, making them easier while saving time.




 Prosthetic screw M 1.6
Prosthetic screw M 1.6



















Resin-Modi ed Calcium Silicate Pulp Protectant/Liner
TheraCal LC is a light-cured, resin-modified calcium silicate. Its unique apatite stimulating ability makes it ideal for direct and indirect pulp capping and as a protective base/liner.



























Light-Cured Dental Adhesive
Bisco’s ALL-BOND UNIVERSAL allows you to standardize clinical protocols for effective delivery of adhesion with a single-bottle.




Implantmed with W&H Osstell ISQ module for reliable treatment results.
Implant stability can be measured precisely with the W&H Osstell ISQ module, available as an accessory. In combination with the torque control it greatly increases the reliability of the treatment process. Upgrade at any time – for today and tomorrow!

TEAM COORDINATOR ART DEPARTMENT SUBSCRIPTION ADVERTISING PHOTOGRAPHY TRANSLATION DIRECTOR ISSN
Alfred Naaman, Nada Naaman, Jihad Fakhoury, Dona Raad, Antoine Saadé, Lina Chamseddine, Tarek Kotob, Mohammed Rifai, Bilal Koleilat, Mohammad H. Al-Jammaz
Suha Nader
Marc Salloum
Micheline Assaf, Nariman Nehmeh
Josiane Younes
Albert Saykali
Gisèle Wakim, Marielle Khoury
Tony Dib 1026-261X
DENTAL NEWS IS A QUARTERLY MAGAZINE DISTRIBUTED MAINLY IN THE MIDDLE EAST & NORTH AFRICA IN COLLABORATION WITH THE COUNCIL OF DENTAL SOCIETIES FOR THE GCC.
Statements and opinions expressed in the articles and communications herein are those of the author(s) and not necessarily those of the Editor(s) or publisher. No part of this magazine may be reproduced in any form, either electronic or mechanical, without the express written permission of the publisher.
DENTAL NEWS – Sami Solh Ave., G. Younis Bldg.
POB: 116-5515 Beirut, Lebanon.
Tel: 961-3-30 30 48
Fax: 961-1-38 46 57
Email: info@dentalnews.com Website: www.dentalnews.com
www.facebook.com/dentalnews1
www.instagram.com/dentalnews
twitter.com/dentalnews
Dental News App on both Appstore & Google play









IDS 2017 LSE 2017 12th International Congress
March 21 - 25, 2017 Cologne, GERMANY Website: www.english.ids-cologne.de
April 7 - 8, 2017 Beirut, LEBANON Website: www.lse-lebanon.org
CAD/CAM 2017
Lebanese University Dental Meeting
EXPODENTAL 2017 Dental Congress
AIO 2017 9th International Congress
FDI 2017 - Annual World Dental Congress
EDSIC 2017 Egyptian Dental Syndicate International Congress
BIDM 2017 27th Beirut International Dental Meeting
CADEX 2017 Central Asia Dental Expo
May 5 - 6, 2017 at the Intercontinental Hotel, Festival City Dubai, UAE Website: www.cappmea.com
May 10 - 13, 2017 at the Lebanese Univesity Campus, Hadath, LEBANON Website: www.ul.edu.lb
May 18 - 20, 2017 Rimini, ITALY Website: www.expodental.it
June 15 - 17, 2017 Chia Laguna Resort (Cagliari), Sardinia, ITALY Website: www.congress.aio.it
August 29 - September 1, 2017 Madrid, SPAIN Website: www.fdiworldental.org
September 13 - 15, 2017 at the Intercontinental City Stars, Cairo, EGYPT Website: www.edsic-eg.com
October 5 - 7, 2017 Biel, Beirut - LEBANON Website: www.lda.org.lb
October 19 - 21, 2017 Almaty, KAZAKHSTAN Website: www.cadex.kz

Dr Mayada Jemâa
Assistant Professor, Department of Dental Medicine, Military Principal Hospital of Instruction, Tunis, Tunisia dr.jemaamayada@gmail.com
Dr H. Jegham
Assistant Professor, Department of Dental Medicine, Military Principal Hospital of Instruction, Tunis, Tunisia
Dr H. Ouertani
Assistant Professor, Department of Dental Medicine, Military Principal Hospital of Instruction, Tunis, Tunisia
Pr S. Marouane
Professor, Department of Dental Medicine, Military Principal Hospital of Instruction, Tunis, Tunisia
Pr L. Bhouri
Professor, Department of Restorative Dentistry and Endodontics, Dental Clinic, Monastir, Tunisia
Pr MB. Khattech
Professor, Department of Dental Medicine, Military Principal Hospital of Instruction, Tunis, Tunisia
Abstract
Molar Incisor Hypomineralization (MIH) is defined as a hypomineralization of systemic origin of one to four permanent first molars, frequently associated with similarly affected permanent incisors. The affected molars are related to major clinical problems in severe cases. Clinically, MIH includes the presence of demarcated enamel opacities, post eruptive breakdown due to soft and porous enamel and atypical restoration. Early diagnosis is very important due to the risk of rapid breakdown of tooth structure.
The early intervention is essential; it includes monitoring, preventive treatment to help in remineralization of the hypomineralized enamel and in some cases restoration with resin composite.
The late or the improper diagnosis can result in mismanagement of the defect, tooth sensitivity to cold air and hot water, rapid development of dental caries, pulpal inflammation, enamel and restoration breakdown and early loss of affected first permanent molars. The high prevalence of MIH indicates the need for more research to clarify etiological factors.
The purpose of this article was to describe the diagnosis information, prevalence, etiological factors of the MIH for a better knowledge of this phenomenon and to illustrate its clinical management.
Key words:
Molar Incisor Hypomineralization (MIH), Enamel hypomineralization, Tooth abnormalities, Aetiology, Diagnosis, Clinical management
Introduction
In spite of dental caries is strongly influenced by social, economic, cultural, religious and environmental factors, its severity may be increased by
structural changes of enamel/dentin such those observed in cases of Molar Incisor Hypomineralization (MIH) (Márcia et al, 2012).
In the literature, MIH is also known as non-fluoride enamel opacities, internal enamel hypoplasia, nonendemic mottling of enamel, opaque spots, idiopathic enamel opacities and idiopathic enamel hypomineralization. 10, 17
This condition is due to disrupted ameloblastic function during the transitional and maturational stages of amelogenesis. 11, 13
MIH was defined in 2001 by Weerheijm; it describes the clinical picture of enamel hypomineralization of systemic origin. Affecting one to four permanent first molars and frequently associated with permanent incisors. 1, 2, 3, 4, 11, 12, 13, 16, 17, 21
Molars are always affected by this phenomenon and often we can find a combination of molars and demarcated opacities of the involved incisors. 12
Even though MIH is defined as a chronological and general disturbance, the number of permanent first molars and the degree of hypomineralization varies extensively. (Fagrell, 2011)
We should also notice that if the opacities are only on the incisors, it may indicate another origin of the defect different from MIH. 12
MIH is one of the forms of structural abnormalities during tooth development, also referred as tooth dysplasia. (Rossitza et al, 2012)
In the Netherlands, the term of “Cheese Molar” has been used to describe this enamel defect. 10
The main clinical characteristics of the MIH are: demarcated opacities, posteruptive breakdown and atypical restorations. 14
Referring to Fagrell in 2011, enamel in teeth affected by MIH exhibits disorganized enamel prisms, a porous structure and loosely packed crystallites.
The European Academy of Paediatric Dentistry
Reinforced composite bloc for permanent restoration

Ò High flexural strength – resistant restorations
Ò Tooth-like modulus of elasticity – shock absorbing
Ò Wear resistant and gentle to the antagonist
(EAPD) organized, in Helsinki in May 2009, an Interim Seminar and Workshop concerning the MIH. It was revealed that there are only a limited number of evidence based research papers on this subject. 7
The world prevalence of MIH ranges from 2.4% to 40% (Fragelli et al, 2015). Referring to the European Academy of Paediatric Dentistry (EAPD), the MIH is classified as mild or severe. This classification depends on the extension of the defect and on the complexity of the treatment required. 14
Treating the MIH has some challenges such as sensitivity, increased risk of plaque accumulation, unexpectedly rapid development and progression of caries, inability to anaesthetize, pulpal inflammation (due to the porosity of the enamel), difficult cooperation of the young patient (dental fear and anxiety), severe discomfort, repeated marginal breakdown of dental restorations and unpredictable behavior of apparently intact opacities. 1, 4, 5, 13, 14, 15, 17, 20
These co-morbidities (dentine hypersensitivity, aesthetic concerns, caries and oral hygiene) are capable of impacting negatively on the quality of life of the children. (Oyedele et al, 2015) Several aetiological factors are mentioned as the cause of MIH and they are frequently associated with childhood diseases or nutritional conditions during the first three years of life. (Márcia et al, 2012)
• Treatment approach of MIH depends on some factors: 5, 9
- Extension and severity of the defect
- Degree of tooth eruption
- Occlusion
- Child’s compliance
- Oral hygiene /Motivation
- Extent of treatment recommended
- Prognosis of the teeth affected
- Financial cost
- Diet habits …
• Management options of MIH: 8
- Early diagnosis +++
- Caries risk management,
- Remineralization therapy,
-Restorations (composite restorations, crowns…)
- Veneers for anterior teeth… Strategies for correct diagnosis, treatment plan and possible prevention attitude are recommended. 12
First of all, for an appropriate clinical evaluation, we should clean carefully the four first permanent molars and the eight erupted permanent incisors. They should be wet for an accurate examination (opacities…). 1, 5
The age of eight years is considered the appropriate age for diagnosing MIH because all permanent first molars and majority of permanent incisors are erupted at this age. 5, 11, 13, 19
To diagnose MIH, at least one first permanent molar has to be affected (Lygidakis et al, 2010).
Clinical characteristics of MIH are: demarcated opacities (altered enamel translucency, variable in degree) of different colour, post-eruption breakdown, atypical restorations, and extracted first permanent molars due to MIH. 1, 12, 14, 17 The porous opacity of the hypomineralized enamel can be white, yellow or even brown. 2, 4, 5, 12, 11, 17, 20, 22
The borders of opacity are well-defined and different from healthy and adjacent enamel. 2, 3, 6
Most of the time, opacities are limited to the incisal or cuspal one third than the cervical one third. 1 In general, the enamel defects in the incisors are milder than in molars due to the absence of chewing forces. 3, 10, 17 Frequently, in the affected molars restorations are extended to the buccal or palatal smooth surface. 12,17
Enamel opacities may occur adjacent to restoration margins. (William et al, 2006) The hypomineralized enamel looks soft, porous and has the appearance of discolored chalk or Old Dutch cheese. 3, 4, 11, 17, 21
The breakdown of teeth affected by MIH can occur just after eruption in case of significant porosity of the opacity 2, 3. The loss of porous and brittle enamel can be the result of masticatory forces. 3, 4
Consequences are dentin exposure, tooth sensitivity and an unexpectedly rapid caries development.2,5
Tooth hypersensitivity is a common problem resulting from MIH, leading to poor oral hygiene, eating difficulty and compromising the affected teeth. 9
The yellow and brown opacities present as microscopically porous, with a higher clinical risk of breakdown than that of the white opacities. (Fragelli et al, 2015)
The creamy-white opacities are present in the internal part of the enamel. 10
The severity of the defect can be clinically evaluated through the stained degree of MIH enamel. 5

Producing the best instruments to simplify the work of practitioners and constantly improve patient comfort. This has been Bien-Air’s mission since its creation in 1959.
Ergonomics, precision and reliability are at the core of the development of every new product. Paying careful attention to professionals every day, Bien-Air has made numerous innovations, always setting the bar higher. A true culture of excellence sitting perfectly with the tradition of Swiss-Made products from the renowned Watch Valley.
The young patient history should be investigated to determine possible etiological factors. 1
There is a difference in the severity of the MIH between patients and even in the same mouth since not all the permanent first molars can be affected with the same degree of extension. 3
Within one patient, intact opacities can be found on one molar; while in another molar large parts of the enamel break down soon after eruption. (Weerheijm et al, 2004)
Where there are more molars and incisors affected the more severe is the defect. (Lygidakis et al, 2010) The risk of affected upper incisors is increased with more affected first permanent molars. 4, 10, 11, 17
The absence of first permanent molars in a healthy dentition associated to the presence of demarcated opacities on the incisors is suspected for MIH. 12, 17
Young patients may complain about the unesthetic appearance of their affected incisors. 5
The bonding to enamel is difficult and risky in such case, because of the prismatic morphology in the porous enamel is altered; as a result the loss of the
defective restoration and frequent re-treatments. 17, 20
There are two forms of severity of MIH that should be recorded by the clinician to help for the clinical management.In the mild form, we find demarcated enamel opacities, absence of enamel breakdown, presence of occasional tooth sensitivity and mild aesthetic concerns on discoloration of the incisors. 7, 14
The characteristics of the severe form are: demarcated enamel opacities with post-eruptive enamel or enamel and dentine breakdown, caries, persistent/spontaneous hypersensitivity, restorations with atypical shape, extension or even extractions and strong aesthetic concerns. 7, 14
It is imperative to identify the early diagnosis, associated problems to MIH and to explain them to the parents and the young patient. 3
There are different enamel abnormalities that can be confused with MIH.




- Enamel hypoplasia (EH): quantitative defect (deficient enamel matrix formation) due to disruption of the secretory phase during ameloblast function. In such case, the thickness of the enamel is reduced. 1,3 Referring to Márcia et al. in 2012, in case of enamel hypoplasia, the enamel can be partially present or totally absent, presence of white colored lesions that are symmetrical or isolated, presence of vertical or horizontal grooves and deep fissures, presence of smooth edges associated to adjacent normal enamel.
- Amelogenesis Imperfecta (AI):
AI is defined as clinically and genetically heterogeneous group of condition, affecting the appearance and the structure of the enamel of all or approximately all dentition. It is sometimes associated with other dental, oral and extraoral tissues. The degree of severity is different in the same mouth. 23 In case of AI, the pathology affects all dentition, the family history is usually involved and the radiographic examination can reveal taurodont teeth. 11 All teeth are affected with the generalized opacities. 5 The permanent first molars are equally affected and imitative of appearance of Amelogenesis imperfecta only in severe cases of MIH. 4, 11
- Fluorosis:
Dental fluorosis is a development disturbance of enamel that is characterized by increased porosity and lower mineral content. It is caused by the repeated exposure of the patient to important concentrations of fluoride during tooth development.24 The fluorosis is considered as caries resistant due to the structure of enamel and opacities are diffuse. However, in MIH opacities are well demarcated and caries prone. 4, 11
The number of teeth affected with fluorosis is related to the time of exposure. 11
- White spot lesions:
White spot lesions represent areas of demineralized dental enamel and it is usually due to prolonged plaque accumulation and colonization of aciduric bacteria. Any tooth surface can be involved especially when the microbial biofilm can develop and remain a long period such as during orthodontic therapy. 25 The absence of treatment of white spot lesions will lead to the development of cavitated caries. 25
Prevalence of Molar Incisor Hypomineralization (MIH)
Referring to the literature, the prevalence figures range from 3.6 % to 25%. 3, 4, 5, 6, 21
Márcia et al in 2012 indicated that according to the results of recent studies the prevalence of the defect is between 3.5 % and 40.2%.
Most of the epidemiological studies about MIH were conducted in European countries. 3, 5, 20, 21
In Jeddah, the prevalence of MIH in 8–12-year-old patients was 8.6%. 17
In Ankara Turkey, the prevalence of MIH in a group of 4,018 children was 7.7% and researchers also find that severity of lesions increased with age. 19
A study of Ahmadi et al in 2012, showed a prevalence of 12.7% for MIH in a group of Iranian children. 20
The prevalence of MIH was 20.4% among Brazilian schoolchildren aged 8 and 9 years. 18
It gives the impression to differ between countries, birth cohorts, criteria used in the diagnosis and methodological differences. 4, 18, 21
For the same patient, the number of affected first permanent molars varies from 1 to 4, involving especially 2 or more molars including the controlateral tooth. 1
The more first permanent molars affected, the higher risk of affected permanent incisors. 4, 10, 11, 17
Although MIH causes are still unclear and difficult to identify, some factors have been associated with this enamel defect.
The causative factors suggested by some authors are systemic conditions and environmental insults that influence natal and early post natal development. 1, 11
There is a relationship between health problems occurring during pregnancy, environmental factors and MIH. 2 During the perinatal period, factors that can contribute to MIH are hypoxia, hypocalcaemia and preterm birth. 15, 16
Children with poor general health in the first years of life are believed to be more likely to be affected by more severe MIH. 6, 19
When the young patient had more than one medical problem in his childhood, it would be very difficult to determine the etiological factors. 1
Referring to Allazzam et al. in 2014, higher percent-

Flow chart illustrated by the authors of clinical management of MIH Children with a history of putative aetiological factors in the first 3 years should be screening at risk for MIH (Alaluusua, 2010, Crombie et al., 2009, Fagrell et al., 2011, Márcia et al., 2012) 5
age of children with MIH had histories of illnesses during the first four years of their childhood. Referring to William et al. in 2006, conditions common in the first 3 years, such as upper respiratory diseases, asthma, otitis media, tonsillitis, chicken pox, measles, and rubella, appear to be associated with MIH. The use of antibiotic is also suggested to be involved in this disease. 1, 3, 4, 7, 10, 14, 16, 19, 20 There is about a 2-fold increase in risk of MIH if amoxicillin is used in the first year of life. (Lygidakis et al. 2010) Other possible causes suggested are: environmental conditions, premature birth, perinatal complications, exposure to dioxine by prolonged breastfeeding, respiratory diseases and oxygen shortage of the ameloblasts, calcium and phosphate metabolic troubles, oxygen starvation associated to low birth weight and febrile childhood diseases. 3, 4, 9, 10 Vaccines administrated in an early age can be a cause of MIH. 4 An underlying genetic predisposition is mentioned to contribute to MIH development. 6 Actually, there is no evidence of relationship between genetic component and MIH. 7 Knowledge on causative factors can contribute to the identification of children who are more prone to this pathology and facilitate to establish a preventive treatment plan.
The MIH may contribute to a large treatment need and the difference in treatment requirement is largely related to the affected teeth. 4 The treatment plan of MIH is composed of three levels (Preventive, Restorative and Rehabilitation) (Fig. 1)
The decision on which therapy should be used is difficult and is dependent upon on a number of factors such as the severity of the condition, patient’s dental age, the child/parent’s social background and expectation. 7
Dentist must explain the MIH pathology and the treatment options to the parent and child.
The prevention plan has a large importance in early post-eruptive stage when the affected tooth is further vulnerable to breakdown and caries attack. 7 When restorative treatment is indicated, the proper local anesthesia is obligatory and in some cases, it is difficult to obtain properly anaesthetized molars. 4 Cast restorations can be full coverage crown, toothcolored crown, porcelains or veneers. And they are not advisable in early post-eruptive stage (large pulp size, short crown height…). 5
Restorative options include glass ionomer cements (GIC), resin-modified glass ionomer cements (RMGIC), polyacid modified resin composites (PMRC), resin composites (RC), amalgam, stainless







steel crowns (SSCs), and indirect adhesive or cast onlays or crowns. (William et al, 2006) Concerning adhesive and fissure sealant for the posterior teeth that are important before breakdown occurs, Lygidakis et al. in 2010 suggested that higher retention rates could be achieved if a 5th generation bonding adhesive is applied prior to fissure sealant application. Composite restorations should be reviewed very frequently. Because more breakdown of the affected enamel can happen at the restoration margins. 9
In some cases, extraction of the severely affected molars with a poor long-term prospect, combined with orthodontic therapy, should be considered as an alternative treatment. 4
If the orthodontic condition were favorable, the ideal dental age for extracting the defective FPM would be 8.5-9 years of age so as to enable the second permanent molars to drift into the FPM position establishing an adequate occlusion. 7
The maintenance is very important. Dentist must monitor margins of restorations for post eruptive breakdown and should consider full coronal coverage restorations in the long term. 1
A twenty two year old patient, who was unsatisfied with the appearance of his anterior teeth, was examined at the service of Dental Medicine and diagnosed with Molar Incisor Hypomineralization. Defined white non-transparent spots on the vestibular surfaces of the maxillary and mandibular incisors were clearly visible. (Fig.2: a,b,c) The first permanent molars were restored with glass ionomer cements (GIC). (Fig.3: a,b,c)
The treatment plan was: Microabrasion and restoration with resin composites (RC) of the maxillary and mandibular incisors. Concerning the first permanent molars, full coverage crowns were programmed. (Fig.4, Fig.5, Fig.6, Fig.7, Fig.8, Fig.9)
The maintenance was also programmed.

Safety 110 With You Years


Case Report N°1:





















ONLINE YEARLY SUBSCRIPTION
Price: 50 EURO + 14 EURO (shipment / free for the AMU)
2 yearly issues of the African Journal of Dentistry & Implantology + Access to all digital archives
Membership card to the African Society of Dentistry & Implantology + 20% discount on African Society of Dentistry & Implantology events

A twenty four year old patient, who presented as chief complaint the unaesthetic appearance of the 11 and 21, was examined at the service of Dental Medicine and diagnosed with Molar Incisor Hypomineralization.
Defined white stains on the vestibular surfaces of the 11 and 21 were clearly visible. (Fig.10) The first permanent molars presented yellow-

ish brown hypomineralized lesions, occlusal cavity with exposed dentin and amalgam restoration. (Fig. 11) The treatment plan was: Restoration with resin composites (RC) of the maxillary incisors (11, 21). Concerning the first permanent molars, full coverage crowns were programmed. (Fig.12, Fig.13, Fig.14, Fig.15) And a follow-up was also programmed.
Light-curing nano-ceram composite
• nano-reinforced ceramic particles
• special resin matrix
• significantly less free monomers
• highly esthetic

• universal for all cavity classes
• comfortable handling, easy modellation
• also available as a flowable version







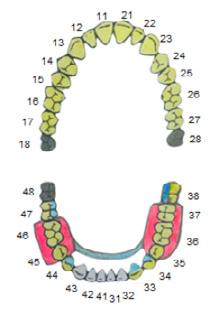
A nine year old patient attended the service of Dental Medicine with a chief complaint of the presence of stains in the 21 and the 32. After teeth prophylaxis and clinical examination we diagnosed that the stains were caused by Molar Incisor Hypomineralization. Teeth 21 and 32 showed yellow opacities at the buccal surfaces. (Fig.16, Fig.17) Teeth 16 and 26 were intact. (Fig.18) Tooth 46 presented a stainless steel crown and the tooth 36 presented a moderate dentinal carie. (Fig.19)

Fig. 20: Elimination of the yellow opacity of the tooth 21 by a Diamond Flame Burr.
Fig. 21:
Aspect of the tooth 21 after the preparation.

Fig. 22: Elimination of the yellow opacity of the tooth 32 with the same diamond bur.
Fig. 23:
Aspect of the tooth 32 after the preparation.
Fig. 24:
Final aspect after restoration of the teeth 21 and 32 with Nanohybrid resin composite.
Fig. 25: Restoration of the tooth 36 with glass ionomer cements (GIC).


The treatment plan was: Restoration with resin composites (RC) of the teeth 21 and 32. Restoration with glass ionomer cement (GIC) of the tooth 36. (Fig.20, Fig.21, Fig.22, Fig.23, Fig.24, Fig.25) The maintenance phase was programmed.






MIH is considered a challenge in dental practice both for the dentist and the patient. The keys for successful management of patients with MIH are early diagnosis, appropriate treatment plan and intensive Monitoring. More research studies are needed in order to help clarify the aetiology of MIH for better management options.



mectron s.p.a., Italy, tel +39 0185 35361, www.mectron.com, mectron@mectron.com







1. Molar IncIsor HypoMIneral zatIon: revIew and recoMMendatIons for clIn cal ManageMent vanessa wIllIaM, louIse B Messer, MIcHael f Burrow, pedIatr c dentIstry – 28:3 2006
2. Molar ncIsor HypoMIneral zatIon (MIH): conservatIve treatMent ManageMent to restore affected teetH caMIla MarIa BullIo fragellI, JulIana feltrIn de souza, faBIano JereMIas, rIta de cássIa loIola cordeIro, lourdes santos-pInto Braz oral res [onlIne]. 2015; 29(1):1-7
3. Molar IncIsor HypoMIneralIsatIon (MIH). K.l weerHeIJM european Journal of paedIatrIc dentIstry 3/2003
4. Molar IncIsor HypoMIneralIzat on (MIH): clInIcal presentat on, aetIology and ManageMent. K.l weerHeIJM dental update – January/feBruary 2004
5. MárcIa pereIra alves dos santos and lucIanne cople MaIa (2012). Molar Inc sor HypoMIneralIzatIon: MorpHologIcal, aetIologIcal, epIdeMIologIcal and clInIcal consIderatIons, conteMporary approacH to dental carIes, dr. MIng-yu lI (ed.), IsBn: 978-953-51-0305-9, IntecH, avaIlaBle froM: Http://www IntecHopen coM/BooKs/conteMporary-approacH-to-dental-carIes/Molar-IncIsor-HypoMIneralIzatIonep deMIologIcalMorpHologIcal-and-clInIcal-consIderatIons
6. Molar-IncIsor-HypoMIneralIsatIon (MIH). a retrospectIve clIn cal study In greeK cHIldren. II. possIBle MedIcal aetIologIcal factors n a lygIdaKIs, g dIMou, d. MarInou european arcHIves of paed atr c dentIstry // 9 (4). 2008
7. Best clInIcal pract ce guIdance for clInIcIans dealIng wItH cHIldren presentIng wItH Molar-IncIsor-HypoMIneralIsatIon (MIH) an eapd polIcy docuMent n a lygIdaKIs, f wong, B. JälevIK, a-M.v errou, s alaluusua, I. espelId european arcHIves of paedIatrIc dentIstry // 11 (Issue 2). 2010
8. clInIcal treatMent approacH of a cHIld wItH Molar Inc sor HypoMIneralIzatIon (MIH) coMBIned wItH MalocclusIon rossItza KaBaKtcHIeva, vladIMIr Bogdanov Journal of IMaB - annual proceedIng (scIentIfIc papers) 2012, vol. 18, BooK 2
9. Molar IncIsor HypoMIneralIsat on: clInIcal ManageMent of tHe young patIent dyMpna daly, JM waldron. Journal of tHe IrIsH dental assocIatIon 2009; 55 (2): 83 – 86. 10. factors Involved In tHe aet ology of Molar- ncIsor HypoMIneralIsat on (MIH) v e v.M. BeentJes, K.l weerHeIJM, H.J.groen european Journal of paed atr c dentIstry 1/2002
11. Molar IncIsor HypoMIneralIzatIon: a lIterature revIew sudHIr MIttal, avn nder Kaur, sunIla sHarMa, adItI Bector, reetu sIngH tHe offIcIal Journal of HIMacHal pradesH unIversIty, 2013 voluMe-I (Issue-I) 12. JudgeMent crIterIa for Molar IncIsor HypoMIneralIsatIon (MIH) In ep deMIologIc studIes: a suMMary of tHe european MeetIng on MIH Held In atHens, 2003 K.l weerHeIJM , M. duggal, I. MeJare, l papagIannoulIs, g. KocH, l c. Martens, a-l Hallonsten european Journal of paedIatrIc dentIstry 3/2003
13. estHetIc and functIonal reHaBIlItatIon of Molar IncIsor HypoMIneralIsatIon: report of two cases nagvenI nB, KatKade s, KotHarI s, poornIMa p (2014). oral Hyg HealtH 2: 130
14. Molar-IncIsor HypoMIneralIzatIon: a cHallenge In tHe dental pract ce neves aB, Jorge rc, MarIen Jv, sIMoes p, sovIero vM (2015). dentIstry 5: 307
15. Molar IncIsor HypoMIneralIzatIon MorpHologIcal and cHeMIcal aspects, onset and possIBle et ologIcal factors, toBIas fagrell swedIsH dental Journal suppleMent 216 gotHenBurg 2011
16. aetIology of Molar-IncIsor HypoMIneralIsatIon: a systeMat c revIew s alaluusua european arcHIves of paedIatrIc dentIstry // 11 (Issue 2). 2010
17. Molar IncIsor HypoMIneralIzatIon, prevalence, and etIology sulaIMan MoHaMMed allazzaM, suMerMadanI alaKI, oMar aBdel sadeK el MelIgy InternatIonal Journal of dent stry, voluMe 2014, artIcle Id 234508, 8 pages
18. assocIatIon Between Molar IncIsor HypoMIneralIzatIon n scHoolcHIldren and BotH prenatal and postnatal factors: a populatIon-Based study tourIno lfpg, corrêa-farIa p, ferre ra rc, Bendo cB, zarzar pM, vale Mp (2016) plos one 11(6): e0156332. doI:10.1371/Journal pone.0156332
19. tHe prevalence aand severIty of Molar IncIsor HypoMIneralIzatIon In a group of cHIldren lIvIng In anKara turKey. Hayr ye sönMez, gözde yIldIrIM, tuBa BezgIn clInIcal dentIstry aand researcH 2013; 37(1): 35-41
20. Molar IncIsor HypoMIneralIzatIon: a study of prevalence and et ology In a group of IranIan cHIldren raHIl aHMadI, naHId raMazanI, raHMatollaH nourInasaB Iran J pedIatr, Jun 2012; vol 22 (no 2), pp: 245-251
21. clInIcal ManageMent approacH of Molar IncIsor HypoMIneralIsatIon a case report sHaIKHa alraeesI, Manal al HalaBI dental trIBune MIddle east & afrIca edItIon | January-feBruary 2016
22. co-MorBIdItIes assocIated wItH Molar-IncIsor HypoMIneralIsatIon In 8 to 16 year old pupIls In Ile-Ife, nIgerIa oyedele et al. BMc oral HealtH (2015) 15:37
23. aMelogenesIs IMperfecta - lIterature revIew geMIMaa HeMagaran, arv nd. M Journal of dental and Med cal scIences (Iosr-JdMs), voluMe 13, Issue 1 ver. IX. (feB. 2014), pp 48-51
24. dental fluorosIs: eXposure, preventIon and ManageMent. Jenny aBanto alvarez, Karla Mayra p c rezende, susana María salazar MarocHo , faBIana B. t alves , paula celIBertI , ana lIdIa cIaMponI . J clIn eXp dent. 2009; 1(1):e14-18.
25. wHIte spot lesIons: preventIon and treatMent readers’ foruM aMerIcan Journal of ortHodontIcs and dentofacIal ortHopedIcs, voluMe 138, nuMBer 6


info@gceurope.com
http://www.gceurope.com

Dr. Ali E Al-Kandari 1
Dr. Hassan Albakkar 2
Dr. Fatema N Alrayes 3
Dr. Abdulaziz Alduwaisan 4 dr.bozeeez@gmail.com
Dr. Hamad Alyaseen 5
Dr. Abdulrahman B Alawadhi 6
Abstract
Background
Full mouth rehabilitation should be focused on restoring natural appearance. Achieving natural esthetics during full mouth rehabilitation is possible with modern all ceramic restorations. Choosing the right materials is of paramount importance to achieve good result.
Case presentation
We report a case of a full mouth rehabilitation of a 65 years old male, who had no medical problems and is not taking any medications. A clinical evaluation revealed a loss of the vertical dimension. Patient’s smile was restored to natural esthetic and function, by restoring the upper arch with lithium disilicate glass ceramic and the lower arch with partial telescope denture.
Conclusions
Full mouth rehabilitation should be achieved by restoring patient mouth back to its natural appearance and normal vertical dimension. Natural esthetic can be achieved using lithium disilicate glass ceramic. Postgraduate student, Department of Prosthodontics & Medical materials, University Hospital Tuebingen, Germany, ( Kuwait National Guard, Ministry of Interior, Ministry of Defense, State of Kuwait )
Specialist in department of Prosthodontics, dental center, (Ministry of health, Riyadh, KSA)
Specialist in department of Periodontology, dental center, (Ministry of health, State of Kuwait)


Keywords
Full mouth rehabilitation, lithium disilicate glass ceramic, partial telescope denture
Background
Full mouth rehabilitation should be focused on restoring natural appearance. Achieving natural esthetics during full mouth rehabilitation is possible with modern all ceramic restorations. Choosing the right materials is of paramount importance to achieve good result. The combination of different materials and techniques allows for restoring patient’s mouth back to normal esthetic and vertical dimension.
Case presentation
A healthy 65-year-old male presented to our clinic requesting to improve his esthetic appearance as well as his chewing ability. Clinical examination revealed multiple old restorations and crowns, multiple missing teeth, attrition of remaining anterior teeth as well as loss of vertical dimension (Fig 1- 4).



CHSAU/CHSENO/0079/16c – Jan 2017.



Radiographic evaluation (Fig 5) showed heavily restored dentition with multiple missing teeth. Bone and maxillary sinuses appeared to be within normal limits.
The aim of the treatment is to restore the patient mouth to full dentition with normal vertical dimension. Therefore, different treatment options were discussed with the patient.
The procedures of the chosen treatment plan were clarified to the patient. The chosen treatment plan aimed for increasing



Soothes all types of oral inflammations
Contributes to reducing inflammatory conditions like gingivitis, bleeding of the gums, receding gums, gingival pockets
Recommended for mucositis, ulceration, and following gingi val curettage
Chairside treatment can be continued at home by the patient
Patented gel, made in France with natural ingredients






Carestream Dental makes it easy for you to elevate your practice above the rest with the CS 3600 intraoral scanner. High-speed continuous scanning captures dual arches quickly and easily, while full HD 3D scans simplify communication with patients, referrals and labs. With open system files and no hidden click fees, Carestream Dental has designed the CS 3600 to rise to the challenge of making digital impressions fast, accurate, easy and open. Visit us at www.carestreamdental.com
the vertical dimension by 2 mm, through wearing a removable partial denture to allow adequate space for composite build up of the lower teeth.
Once the desired vertical dimension is achieved, the final restorations of the upper arch included ceramic bridges (zirconium) in teeth 17-15-13 and all ceramic crowns (Emax.press) in teeth 12-17. Whereas for the lower arch, telescopic crowns for teeth (hybrid crowns) 34, 33, 44, 47.
Porcelain fused to metal crown, for tooth 38 and a partial denture with an E-clasp and sublingual bar to replace missing teeth 37, 36, 35, 45 and 46 (Fig 6).
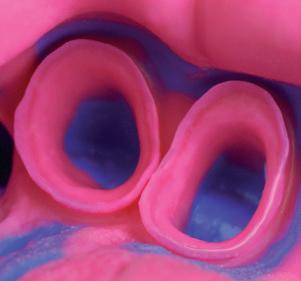
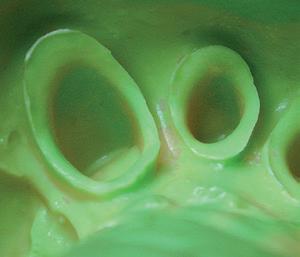
The treatment plan was initiated following the removal of the old bridge and crowns in upper and lower jaws; using Ti-core build up and new temporary bridge and crowns (ProtempTM4® ) (3M ESPE-Seefeld-Germany). This was followed by final preparation (Fig. 7-8) and final impression (Fig. 9-10) with polyether impression material (Impregum® and Permadyne®) (3M Espe-Seefeld-Germany) of the upper and lower arches. Newtemporary bridges were fabricated to maintain the new vertical dimension.
Metal crown 38 and telescopic crowns on 33, 34, 44 and 47 were tried in (Fig 11). Fixation Impression of the lower jaw with the primary telescopic crowns in mouth using polyether impression material (Impregum® and Permadyne® ) was done.
Following metal framework try-in and aesthetic check of the first porcelain bake of upper crowns, the finished final prostheses (Figure 12-14) were delivered. All-ceramic crowns of Emax press as well as the zirconium bridge of upper jaw were cemented using Multilink® (Ivoclar-Schaan-Liechtenstein), whereas the primary crowns were cemented using phosphate cement (Harvard cement).

Dynamic power responsiveness for superior osseous surgery





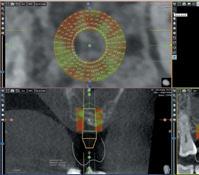

















The 3D technology that facilitates the implant planning with immediate volume measurement and bone density assessment













Discussion
The patient’s prime concern was the aesthetic appearance of upper teeth. He cannot freely laugh or show his teeth without feeling shame how ugly they are. After examination, the problem of the secondary reduction of the vertical dimension was found. It was caused by worn dentition in the lower front teeth, several restorations in upper front teeth and chipping in the secondary crowns of 33, 34 and 44. After explaining to the patient his situation, the patient refused the treatment with Porcelain Fused to Metal crowns, his argument was that he wants natural appearance and good esthetic teeth in the upper jaw. The high esthetic properties of the lithium disilicate glass ceramic meet the patient’s wish of having natural good esthetic appearance 1,2 Silicate ceramics has a high content of glass matrix in which crystalline particles are distributed. This microstructural composition makes them thefirst choice when the aesthetic needs to be restored 3, 4
Also the biocompatibility of the all-ceramic restoration is considered as an advantage of having such a restoration rather than Porcelain Fused to Metal crowns 5, 6. Besides that, zirconia veneered with ceramic is strong enough to be a good alternative of metal ceramic fixed dental prosthesis in the anterior and posterior dentition 7
Restoring the upper right side bridge by zirconium dioxide bridge does also make sense, in order to overcome the huge bite force in the posterior teeth. And restoring the lower jaw with partial telescope denture was the first treatment choice compared to fixed partial dentures.
Telescopic retained partial denture prosthesis is mainly used in Germany to replace multiple missing teeth instead of using the conventional removable partial denture. It is a good treatment option for patient with reduced dentition which provide good retention and the patient can maintain good oral hygiene 8, 9
Hybrid telescopic prosthesis is one type of this technique, which contains friction pins to increase the retention 10
Based on the finding of the speaking distance (4 mm), minimal increase of the occlusal vertical dimension by 2 mm at the incisal pin of the articulator could be done without using an occlusal splint pretreatment 11
The wax up casts was done with increasing the occlusal vertical dimension by 2 mm in the articulator pin. That helped in restoring the worn dentition in the front teeth and had no major effect on the posterior teeth. It was very important to finish the preparation in upper and lower teeth as soon as possible to let the patient get used to the raised occlusal vertical dimension when the provisional crowns were cemented.
We need to have the patients’ feedback after placing all the ceramic crowns, bridges and partial telescope denture. In the recall appointment one week after seating, the patient came with much confidence, he was more satisfied with the results. In the recall appointment after one and half year, the patient came for routine recall appointment. He was very happy without any complication.
The success of such treatment lies mainly on the patient. Keeping good oral hygiene, attendance in the routine recall appointment, and not ignoring any problems regarding his facial muscles and Temporomandibular joint are the important factors that will help in the success of such a treatment.

benefits of NovaMin® technology and sodium fluoride in a single formulation
With twice-daily brushing, it can:
• Create an even harder hydroxyapatite-like layer over exposed dentine and within exposed dentine tubules*1-7
• Continually protect your patients from dentine hypersensitivity,** with significant benefits in as little as 2 weeks8,9


Recommend Sensodyne Repair & Protect to help your patients live life more free from the impacts of dentine hypersensitivity**
Full mouth rehabilitation should be achieved by restoring patient’s mouth back to its natural appearance with normal vertical dimension. Natural esthetic can be achieved using lithium disilicate glass ceramic.
The authors declare that they have no competing interests.
Authors’ contributions
All authors read and approved the final manuscript.


7.–9. February Stand: 7E07
1. aBdou J. :safety of IncreasIng vertIcal dIMensIon of occlusIon: a systeMatIc rev ew. QuIntessence Int. 2012:43:s:369-380.
2. agustIn-panadero r et al., zIrconIa In fIXed prostHesIs a lIterature revIew, J clIn eXp dent. 2014;6(1):e66-73.
3. Kern, M., KoHal, r., MeHl, a., pospIecH, p., franKenBerger, r., reIss, B., KunzelMann, K. (2006). vollKeraMIK auf eInen BlIcK QuIntessenz zaHntecHnIK, 32(5),514.
4. struB, J. r. (1994). currIculuM protHetIK: QuIntessenz-verl
5. saIler, I., et al., asysteMatIc rev ew of tHe survIval and coMplIcat on rates of all-ceraMIc and Metal-ceraMIc reconstructIons after an oBservat on perIod of at least 3 years part II: fIXed dental prostHeses clIn oral IMplants res, 2007.18suppl 3:86-96.
6. p Jetursson, B. e., et al., a systeMatIc rev ew of tHe survIval and coMplIcatIon rates of all-ceraMIc and Metal-ceraMIc reconstruct ons after an oBservatIon perIod of at least 3 years part I: sIngle crowns clIn oral IMplants res, 2007.18 suppl 3:73-85.
7. raIgrodsKI, a. J., et al., survIval and coMplIcatIons of zIrconIaBased fIXed dental prostHeses: a systeMatIc revIew. J prostate dent, 2012.107(3):170-177.
8. groten, M., et al., HyBrIdtelesKope zur veranKerung von KoMBIn ert festsItzend
9. scHwIndl ng fs, dIttMann B, raMMelsBerg p, douBle-crownretaIned reMovaBle dental prostHeses: a retrospectIve study of surv val and coMplIcatIons J prostHet dent. 2014 sept;112(3):488-93
11. Harper rp. IndIcatIon for alterIng occlusal vertIcal dIMens on QuIntessence Int. 2000;31:s:275-280. CA ® CLEAR ALIGNER –3 aligner per step for accelerated treatment results. precision made in Germany clinically proven 3-splint-system for effective treatment treatment corrections are possible at any time more than 100.000 patients successfully treated
CA® CLEAR ALIGNER Seminar with Dr. Pablo Echarri, 11.02.2017, Dubai
10. BreItMan JB, naKaMura s, freedMan al, yalIsove Il, telescopIc retaIners: an old or new solutIon? a second cHance to Have norMal dental funct on J prostH 2012;21:79-83 HerausneHMBareM zaHnersatz.QuIntessenz zaHntecH 2009; 35(12):1568-1580.










Dr. Hescot, you are the president of the Federation Dentaire Internationale, what are the policies of the FDI regarding the promotion of the oral health globally?
For us, what is important is to have a new definition of Oral Health. As this definition was established, last year, during our world dental congress in Poznan, Poland. This definition is to explain to people that the dentist is responsible of the quality of life and the wellbeing of his patients. In fact, for long time, for many people, the dentist was only about the teeth, about the mouth. But that is not true. The dentist is responsible of your quality of life. How it is possible to speak, to eat, to drink, to socialize, to have love life without good oral health?
What about the relationship between the Oral Health and total wellbeing?
First example about the ageing population. For the elderly people, it is very important to keep good oral health. Because without good oral health, you have infections, you lose your self-esteem, you don’t speak, you don’t have social life and “Ils se referment sur eux mêmes” and after that, they lose their interest in life.
Second example: we have an established relation between general health and oral health. There may be a deterioration of the systemic diseases if the oral health is not checked. Relation exists between diabetes, cardiovascular diseases, malnutrition, and oral health.
The quality of life is at 2 levels: 1st level: physical. 2nd level: psychological.
And the oral health is important for the physical and psychological health. The dentist job is not only for treatment, his is essential for the promotion of your good oral and general health. It is very important to prevent and for that, what is important for me, for FDI today, is to promote prevention.
It is more important to change the image of the dentist. Today, the dentist is a technician. This is not enough, we have to promote the psychological approach. Dental studies have to evolve, because today the dentist is too much a super technician that he forgets the human approach. I don’t treat your teeth and your mouth only, I treat you as a person and what is important for the person is self-esteem.
I will expose the case of implants. Today, you have excellent treatments in implant dentistry. The dentist places the implants.
We have big companies, great technicians, and after that, for the majority, the role of the dentist is finished. But no, it is very dangerous. They have to come back. Because today, we have more than 30% of post implant diseases in the world.
The problem is when you treat and you forget to educate. For example, it is very important that you have a good toothbrush and oral care devices at each moment after implant placement. This is of utmost importance. More than before implant placement.
Regarding the role of the companies, how can they help in the prevention and the control of these problems?
The first level is clear: it is the good quality of the products. It is compulsory.
But the second level is very important. It is to promote. Because if you need to change the image of the dentist, it is a series of communication and lots of advertising.
And the responsibility of the companies, producing the oral care equipment, is more important than the dentist. Because for me, I’m a dentist and we want to work together on 2 levels. Ads on TV, campaigns and promotion during world health day, which is on the 20th of March and Philips is our partner and it is very important these days to do lots of campaigns in all the countries.
What would you say about the connected care solutions like the latest toothbrush connected to Bluetooth and to an application? How could that help in the personalization of prevention of oral health disease?
It is important in the sense that everybody likes that, especially the young generation, same as the smartphone today.
Philips organizes a new strategy about the toothbrush like the smartphone. This new approach is important because it is better but also because it is in the spirit of the time and life. We are witnessing interesting times with technological advances.
With these connected devices, the dentist can monitor your daily oral hygiene habits? what do you think about it?
For me, it is a very good tool to educate. That tool will be a communication between the dentist and his patient. The dentist can take a look on how good is the patient’s brushing pattern. It is like a physical trainer for his clients.

 Dr. Dominique Caron, Dr. Mohamed Darwish, Dr. Patrick Hescot president FDI
Dr. Angelo Putignano, Dr. Patrick Hescot, Mr. Paul Wilson, Dr. Tony Dib
Dr. Dominique Caron, Dr. Mohamed Darwish, Dr. Patrick Hescot president FDI
Dr. Angelo Putignano, Dr. Patrick Hescot, Mr. Paul Wilson, Dr. Tony Dib

Iris Mittenaere, aspiring dentist from Lille, north of France, was elected miss universe 2017 in Manila, the Philippines on January 30, 2017. Iris is the second from France to win the title since Christiane Martel in 1953.
At 23 years old, the newly crowned queen is pursuing a degree in dental surgery. Besides dental school, Iris is also fond of extreme sports, traveling the world and cooking French dishes, according to her profile at the Miss Universe website.
She said her primary advocacies are dental health and oral hygiene
As a dental student, she wants to continue her awareness campaign for dental and oral care, taking her campaign all around the world.


« She wants to continue her awareness campaign for dental and oral care »
The new Miss Universe Iris Mittenaere revealed the advocacy she would be pursuing now that she is the new queen – she would be fighting for healthy teeth.
We consider this a happy day for dentistry and to the promotion of optimal oral and general health for the whole world.
Iris Mittenaere is an inspiration to every dentist to get passionate and pursue the things they want to achieve in their lives.



Compact design and easy to access: the smallest imaging plate scanner on the market for your personal convenience.
Streamline workflow with images in seconds: drop your imaging plate in the PSPIX2 and let it do the rest.
Improved patient experience with various sizes of thin and flexible imaging plates.
Striking contrast for a more reliable diagnosis.


December 6 - 8, 2016 Friendship Hall - Khartoum, SUDAN

dr yAssEr AlgEndy, PrEsidEnt oF thE EgyPtiAn dEntAl soCiEty, AddrEssing dr AhmEd rizg, mr hAsBo ABdElrAhmAn, And ministEr oF hEAlth dr somAyA oKd

dr. AhmEd rizg, PrEsidEnt oF thE gEnErAl sudAnEsE dEntAl union

dr. AnwAr BAtAynEh lECturing ABout PAtiEnt’s PAin PErCEPtion

mr hAmmAdi gtAt From thE indEx ComPAny duBAi

mAguEEd Amin From EgyPt

dr. nAhAwAnd thABEt From thE EgyPtiAn dEntAl syndiCAtE

dr tony diB From lEBAnon

Pr tArEK ABBAs From EgyPt

dr hussEin lAwAti From omAn

dr iBrAhim ghAnnAm From PAlEstinE

dr hAlA ABBoud From lEBAnon

dr. KhAlil issA From thE sAudi dEntAl soCiEty

dr. mohAmEd JErrAr And dr. moulAy Ali From moroCCo

dr hAsAn nAtour From PAlEstinE

dr gEorgE KhAlil From lEBAnon

dr. AyA AsmAr From thE JordAn dEntAl AssoCiAtion

dr mohAmEd mustAFA From mAuritAniA

dr mohAmEd AlJishi From BAhrAin
 Photo From thE gAlA dinnEr
Photo From thE gAlA dinnEr

28th Saudi Dental Society International Dental Conference
January 10 - 12, 2017
Riyadh International Convention & Exhibition Center - KSA

lEFt to


It is with great pleasure to welcome you to participate in the 28th Saudi Dental Society International Dental Conference which is held on January 10 -12, 2017 at the Riyadh International Convention and Exhibition Center in Riyadh. Our conference is very unique this year!
This years’ conference will be joined by Twenty Seven international and Saudi renowned speakers, who excel in their field of specialties. This conference uniquely gathers many dental specialties, such as implant dentistry, orthodontics, endodontics, restorative and esthetic dentistry, pedodontics, periodontics, oral surgery, and dental photography, that all are centered on providing an excellent dental care to our patients.
This is an excellent opportunity to hear interesting recent developments, learn and develop new techniques, discuss
and share our ideas, and we can have a unique opportunity to generate international research networks.
The world is constantly changing, and it is particularly an exciting time to be involved as we are seeing rapid changes and advances in the field of Dentistry. I sincerely hope that by participating to this event, we will gain great benefits to all of us and to all of our partners in success.
I humbly thank the Saudi Dental Society members for the trust that they have given me to serve our colleagues and to somehow contribute and share my experiences with you. We look forward to your full support and participation in this important event.
Dr. Fahad A. AlShehri
President The Saudi Dental Society

A reliable, high-quality CAD/CAM solution is essential to secure and grow your business. The new 3Shape E scanners with optional 3Shape LabCare subscription are raising the bar for entry-level solutions -making CAD/CAM design accessible to everyone
Learn more at 3sha.pe/Escanners

dEnstPly sironA Booth gC Booth

drs. gEorgio romAnos, toni diB, mr. dArrEn BAylEy


ultrAdEnt gErmAny Booth

dr mEshAri Al otEiBy, dr mAnsour AsEry


gsK Booth ultrAdEnt usA Booth




l to r: drs. tArEq Khoury, nAsEr mAliK, ABdullAh shAmmEry, KhAlEd BAdEr, ABdulsAlAm Al mAdAni, tony diB














































 PlAnmECA Booth
Photo From thE ExhiBition
CAmlog Booth
PlAnmECA Booth
Photo From thE ExhiBition
CAmlog Booth
Henry Schein is a name you can trust
Henry Schein is the largest global dental distributor of health care products and Services to general practitioners, specialists and laboratories throughout the world. Our network of exclusive Henry Schein Middle East Distributors offer dentists a complete portfolio from the following high-quality and value-priced consumable and equipment product manufacturers that you can rely on to fulfill your practice needs.





dr. mohAmEd JErrAr From moroCCo

ProF. AhmEd rizg From sudAn

dr. Antonis ChAniotis From grEECE


troPhy distriBution

dr hAssAn hAlAwAny From riyAdh

ProF. CArlos KhAirAllAh From lEBAnon

dr. nizAr El KAdi From BEirut

dr. yAssEr AlgEndy From EgyPt




February 7 - 9, 2017




His Highness Sheikh Hamdan Bin Rashid Al Maktoum, Deputy Ruler of Dubai, Minister of Finance and President of the Dubai Health Authority inaugurated the 21st edition of the UAE International Dental Conference and Arab Dental Exhibition (AEEDC Dubai) which is held at the Dubai International Convention and Exhibition Centre. AEEDC Dubai, the largest dental conference & exhibition in the Middle East, North Africa, and South Asia and the second largest in the world, is organized by INDEX Conferences & Exhibitions.
Following the opening ceremony, His Highness, accompanied by a number of key officials toured the exhibition area, and he was introduced to the latest medical devices, technologies and equipment put on display by leading local and international companies in the dental field.
After the tour, His highness expressed his delight in the great development and growth that the exhibition is witnessing year after year, and he praised the increase in the number of participating companies this year that has reached to 4,700 companies representing more than 2000 global brands
From his side, Dr. Abdul Salam Al Madani, the Executive Chairman of AEEDC Dubai and the Global Scientific Dental Alliance said: “AEEDC Dubai has entered the most exciting phase in the events history of Dubai, as over the past 21 years, it had a
flourishing effect on the health, economy, trade and tourism sectors of the UAE which further reflect positively on maintaining sustainable development in addition to encouraging and developing the skills of human force working in the public and private sectors.”
“Throughout the years, AEEDC Dubai, has won the trust of all our exhibitors and partners.
We have partnered with the world’s most exclusive and prominent dental associations, which added more value and flavor to this international conference and exhibition. AEEDC Dubai represents an ultimate platform for top-notch speakers to share their knowledge, to exchange experience in the dental field, and to gain CME points.
The conference agenda includes more than 170 lectures delivered by 150 speakers covering various topics that include: Endodontics, Infection Control, Laser in Dentistry, Oral and Maxillofacial Surgery, Oral Implantology, Oral Pathology, Orthodontics, Pediatric Dentistry and Restorative Dentistry.
AEEDC Dubai 2017 features a number of new scientific activities that are happening for the first time and it includes Digital Dentistry Society Symposium, Oral / Dental Hygiene Symposium.
In addition to that, AEEDC Dubai 2017 features also the GCC Preventive Dentistry Conference. The 22nd AEEDC will be on 6-8 February 2018.
CHSAU/CHSENO/0079/16c – Jan 2017.




 dr. ABdulsAlAm Al mAdAni guiding his highnEss through thE ExhiBition Floor - vivAdEnt Booth
dEntsPly sironA Booth with dr dimA Al rEFAE
dr. ABdulsAlAm Al mAdAni guiding his highnEss through thE ExhiBition Floor - vivAdEnt Booth
dEntsPly sironA Booth with dr dimA Al rEFAE

Dentsply and Sirona have joined forces to become the world’s largest provider of professional dental solutions. Our trusted brands have empowered dental professionals to provide better, safer and faster care in all fields of dentistry for over 100 years. However, as advanced as dentistry is today, together we are committed to making it even better. Everything we do is about helping you deliver the best possible dental care, for the benefit of your patients and practice.
Find out more on dentsplysirona.com

thE gloBAl sCiEntiFiC dEntAl AlliAnCE BoArd: drs roBErt EdwAB, ABdulsAlAm AlmAdAni, ABdullAh AlshAmmEry, tArEK Khoury, nAsir mAliK, mohAmEd ABEdin

dr. ABdulghAni mirA, dEAn King ABdulAziz univErsity

dr. ABdEl rAhmAn AlAzri From omAn

dr. mAryAm JAFAr From thE duBAi hEAlth Authority
CErtiFiCAtE distriBution to: dr nAhAwAnd thABEt From thE EgyPtiAn dEntAl AssoCiAtion

dr. Ali tAJErniA, PrEsidEnt oF thE irAniAn dEntAl AssoCiAtion


Pr. tony zEinoun, dEAn oF thE dEntAl sChool, lu
Ent E r th E world of high E st Quality dE ntal u nits – mad E in gE rmany.
ULTRADENT – a leading German provider of high-class Dental Units – continually invests in the development of its products and always stays abreast of current and future challenges in dentistry. The broad spectrum of potential options reflects this expertise. Today, we present two of our latest ULRADENT Treatment Units:
u 6000 – Exclusive Premium u nit for highest d emands
The U 6000 offers everything you need when you make a superior strategic investment. It optionally comes with the revolutionary vision U multimedia system, which includes a 21.5 inch touchscreen monitor, digital intraoral camera and many innovative functions.

u 1303 – l atest technology and high d urability
The U 1303 makes it easy for you to combine dentalmedical convenience with German top standards. It is comprehensive and uncompromising for both your patients and you – ergonomic design, reliability, durability and perfect infection control included.

whether you favour the Premium unit u 6000 or the Compact unit u 1303 you can be sure to get best german quality for your dental practice.
The 7 inch dentist’s element is also available as a mobile cart The dentist‘s element is also available with swiveling arm Jaeger & Talente, Munich



 drs. : ABdullAh Fidhi, mEsAAd BAhAtEq, KhAlEd Al BAdEr
drs. : yAsin AlhusBAn, mAnsour AsEry, mohAmEd JErrAr, Aws rEJAE
Photo Booth From thE
drs. : ABdullAh Fidhi, mEsAAd BAhAtEq, KhAlEd Al BAdEr
drs. : yAsin AlhusBAn, mAnsour AsEry, mohAmEd JErrAr, Aws rEJAE
Photo Booth From thE




 lEFt to right; ProF tony zEinoun, Fou ziAd sAlAmEh, hAni ounsi
drs tony diB, ABdulsAlAm And AnAs mrs. JosiAnE diB
lEFt to right; ProF tony zEinoun, Fou ziAd sAlAmEh, hAni ounsi
drs tony diB, ABdulsAlAm And AnAs mrs. JosiAnE diB







 CArEstrEAm Booth
nsK Booth
A-dEC Booth
gC Booth
ACtEon Booth
w&h Booth
ExhiBition Floor
CArEstrEAm Booth
nsK Booth
A-dEC Booth
gC Booth
ACtEon Booth
w&h Booth
ExhiBition Floor


John Beumer (USA), Peter Moy (USA), Antonio Coppel (Spain), Axel Kirsch (Germany), Alessandro Pozzi (Italy), Monish Bhola (USA), Armin Nedjat (Germany), Emenulele Campagna (Switzerland), Nabil Barakat (Lebanon), Robert Fulkner (USA), Nadim Aboujouda (Lebanon), Ates Parlar (Turkey),), Abdel Salam El Askry (Egypt), Sudarat Kiat-amnuay (USA), Gurcan Eskitascioglu (Turkey), Muharam Erhan Comlekoglu (Turkey), Pravej Serichetaphongse (Thailand), Khaled Gaffar (Egypt) Mine Dundar Comlekoglu (Turkey), Hussein El Charkawi (Egypt), Jabbar Hassanov Azerbaijan, Cem Yaldiz (Turkey) and Many More!!
www.essdi.net
email: helcharkawi@gmail.com 01222150439
Prof. Hussein El Charkawi President
Prof. Hamdy Abou El Fetouh General Secretary
Prof. Mohamed Farouk Abdeallah Treasurer







 PlAnmECA Booth
BEyond int’l Booth
hEnry sChEin Booth
miCro mEgA Booth
ColtEnE Booth
sdi Booth
PlAnmECA Booth
BEyond int’l Booth
hEnry sChEin Booth
miCro mEgA Booth
ColtEnE Booth
sdi Booth




•
•
•
•
•
•







Three months to go until the opening of Expodental Meeting 2017! UNIDI – the Italian Dental Industries Association – that promotes and organizes the exhibition, is ready to introduce all the news of the next edition.
Expodental Meeting is the most relevant international tradeshow for the dental sector in Italy – the one dental Event set up over 45 years ago by the Italian industry.
In fact, Expodental Meeting is the showcase of the Italian dental industry, which has confirmed its position in the forefront of international markets on the strength of products that are appreciated throughout the world for the reliability of their components, their avant-garde technological solutions and pleasing design.
In 2016 the exhibition and the comprehensive cultural and scientific program has attracted a huge number of dental professionals and buyers (16.000 visitors from 72 Countries), which created an increasing number of business opportunities and returns for the 244 Exhibitors; the beautiful location of Rimini Fiera turned out to be perfectly appropriate to welcome both national and international visitors.
For 2017 the offer for exhibitors and visitors will be even more complete and appealing: not only a trade-show, but a comprehensive experience where producers, distributors, agents, professionals, press and university from all over the world will have the opportunity to meet, with a special consideration for education and updating.
In addition to the broad exhibition, there will be a comprehensive cultural and scientific program for dentists, dental technicians and maxillo-facial surgeons, in partnership with the most important dental associations. Furthermore, there will be training opportunities for dental hygienists and dental assistants. A panel of internationally renowed lecturers will hold their courses in the training rooms of Rimini Fiera from 18 to 20 May 2017.
However, what will really make the difference at the upcoming edition is the new pavilion called EXPO3D: an entire area, totally
dedicated to the digital workflow from dental practice to dental lab. The exposure of digital products and the intense scientific programme focused on digital technologies aim at a broader disclosure and knowledge of digital dentistry, in order to promote professional growth within the dental sector.
Besides the display of materials, equipment and machineries used within the digital workflow, a rich scientific program will take place, entirely focused on digital technologies, including events by professional Associations like the Digital Dentistry Society, scientific lectures by academic experts such us the Digital Group of S. Raffaele Institute and the Eastman Institute for Oral Health University of Rochester, and workshops by the Exhibiting Companies.
At last, our scientific partner together with UNIDI, will set up a theoretical journey through videos and infographics explaining the complete digital workflow in dentistry: starting from the image acquisition - through CBCT, Intraoral Scanner, Dental laboratory scanner - all the way through the use of CAD/CAM software to the final manufacturing phase (Milling, Prototyping, Additive Printing).
Finally, in 2017 the cooperation with ICE/ITA (Italian Trade Agency) will be even more intense, in order to make Expodental Meeting more and more international. In fact, last year the international participation has increased by 72%, with 563 new foreign visitors from 71 Countries and a large delegation with more than 60 buyers; next year no less than 100 delegates will meet the Italian companies in Rimini.
Besides, with its immense offer of beautiful landscapes, restaurants serving the best in local cuisine, culture, shopping, wellbeing and entertainment, Rimini is the place where business meets leisure, making your stay a truly unforgettable experience.
See you in Rimini from 18th to 20th May!




IPS e.max lithium disilicate: 500 MPa for even more confidence and new possibilities
Since the introduction of IPS e.max, dentists and dental technicians worldwide rely on the highly resistant and highly esthetic lithium disilicate glass ceramic IPS e.max. 11 years of consistent quality tests prove: This ceramic has an average biaxial flexural strength of 500 MPa. Ivoclar Vivadent have adapted their communication accordingly.
Since the introduction of IPS e.max (2005), this all-ceramic material has proven itself to users with excellent results and reliability. More than 100 million restorations and a survival rate of more than 96 percent speak for themselves. However, it’s more than just 11 years of success with patients. This is underlined by internal quality tests. Each individual material batch is tested for a large number of material properties to meet the required standards. More than a decade of continuous quality testing has shown that IPS e.max lithium disilicate has an average biaxial strength of 500 MPa, which confirms the high success rates.
Thanks to the clinical data, it is possible to reduce the required material thickness for IPS e.max lithium disilicate crowns. A thickness of only 1 millimetre is sufficient when the crowns are adhesively cemented. In addition, minimally invasive occlusal



veneers can now also be produced with IPS e.max CAD. This means conservative dentistry is supported. Dentists have even more options of using IPS e.max for minimally invasive restorations. Furthermore, dental technicians have the assurance that they have made a good choice with IPS e.max. They gain from even greater flexibility when producing highly esthetic restorations. Patients can be happy because the higher strength values mean more natural tooth substance can be preserved.
website: www.ivoclarvivadent.com

In the current digital age, everyday work in the dental office should proceed as smoothly as possible, with highly efficient procedures and fast communication channels. Especially when it comes to laboratory-made restorations, all parties concerned will ultimately benefit from technological process – the dentist and the dental team as much as the dental technician and of course the patient.
With the new Aadva IOS intraoral scanner, the Japanese company GC has developed a device that renders conventional impressions obsolete in many cases. The associated material costs, the many errors and re-takes and the unnecessary many physical shipments have become superfluous. The Aadva IOS can create a digital impression in less than 5 minutes, and this can be forwarded directly to the laboratory via the cloud.
Aadva IOS presents one of the smallest and lightest handpieces in its class. It is ergonomic to work with, which automatically increases patient comfort. Unlike the systems of many other manufacturers, Aadva IOS does not require any preparation with powder spray prior to scanning. This makes the entire scanning process far easier and faster.
GC’s Aadva IOS is an extremely cost-effective high-tech system and an attractive solution for any dentist, not least because it is an open system. The scanner will play an increasingly important role as an interface in computer-assisted restorative dentistry.
website: www.gceurope.com







































































26-29
Octobre Marrakech Mansour Eddahbi
Marrakech 2017









benefits of NovaMin® technology and sodium fluoride in a single formulation
With twice-daily brushing, it can:
• Create an even harder hydroxyapatite-like layer over exposed dentine and within exposed dentine tubules*1-7
• Continually protect your patients from dentine hypersensitivity,** with significant benefits in as little as 2 weeks8,9

Recommend Sensodyne Repair & Protect to help your patients live life more free from the impacts of dentine hypersensitivity**


More and more dentists and dental lab technicians rely on IPS e.max, the clinically proven all-ceramic system that offers high esthetics and dependable strength. 100 million restorations placed attest to this. From crowns, inlays, onlays, thin veneers and abutments to bridges – make the choice more dental professionals make... MAKE IT e.max! THE WORLD ’ S MOST USED * ALL-CERAMIC