








Dental News, Volume XXV, Number I, 2018
Bio f ilm Eraser
POWDER PRO CARE
ABOVE AND BELOW THE GUMS

ABOVE AND BELOW THE GUMS

Dentsply and Sirona have joined forces to become the world’s largest provider of professional dental solutions. Our trusted brands have empowered dental professionals to provide better, safer and faster care in all fields of dentistry for over 100 years. However, as advanced as dentistry is today, together we are committed to making it even better. Everything we do is about helping you deliver the best possible dental care, for the benefit of your patients and practice.
Find out more on dentsplysirona.com





• Universal application – for all bonding procedures and etching techniques
• Predictable results – high bond strength on wet or over-dried dentin
• Universal delivery – available in bottles and the convenient VivaPen®






12.
Enamel White Lesions (Part II): A report of three cases treated according to the new Classification (WSTC)
Drs. Fadwa Chtioui, Omar Marouane, Nabiha Douki

26.
Bleaching of Non-vital Discolored Teeth: Keys of Success
Dr Mayada Jemâa, Dr T. Ben Neji, Pr N. Zokkar, Dr H. Ouertani, Dr H. Jegham, Pr L. Bhouri, Pr MB. Khattech

48. Digital Smile Analysis: Replicating Nature with Two Ceramic Veneers
Dr. Ramy Chayah

58. Distortion Free Dental Photography
Dr. Mohamed Essam

60. Ormco 1st Saudi Symposium
December 1 - 2, 2017
Riyadh, Kingdom of Saudi Arabia
62. SIDC 2018 - Saudi Dental Society International Dental Conference
January 10 - 12, 2018
International Convention & Exhibition Center - KSA
66. LSOS 2018 - Lebanese Society of Oral Surgery International Convention
January 26 - 27, 2018
Hilton Beirut Metropolitan Palace - Beirut, Lebanon
68. AEEDC 2018 - International Dental Conference & Arab Dental Exhibition
February 6 - 8, 2018
Dubai International Convention & Exhibition Center, United Arab Emirates
3SHAPE 19
ACE SURGICAL 17
ACTEON 27, 80
A-DEC 9
BA INTERNATIONAL 35
BIEN AIR 7
BISCO 25
CARESTREAM 20
CAMLOG 6
COLTENE 15
DENTSPLY SIRONA C2, 21
DURR 33
EMOFORM 4, 5
FKG 65
GC 8
HENRY SCHEIN 23
HU FRIEDY 49
IVOCLAR 1, C4
MANI 52
MECTRON 59
MICRO MEGA 42
MORITA 39
NSK C1
ORMCO 31
ORTHO ORGANIZERS 55
PHILIPS 29
PLANMECA C3
PROMEDICA 24
SCHEU 42
SDI 43
ULTRADENT USA 14
VITA 13
VOCO 45
W&H 10, 37
ZHERMACK 2
PHILIPS 65




From its practical design to its seamless setup and operation, every aspect of the Optima was thought-out with simplicity in mind. Composed of a tabletop control unit and Bien-Air’s best-selling MCX brushless micromotor, this ingenious system gives dental professionals the option to upgrade their units with the latest electric technology at the most affordable price.
2-year standard warranty and 1-year optional warranty available through Bien-Air’s PlanCare extended warranty program.
Available colors :


1 shade, 3 strong options for all posterior indications


Fax. +32.16.40.48.32
info@gceurope.com
http://www.gceurope.com


The right composite viscosity for each clinical case


Introducing the new A-dec 300 LED light: Accurate. Economical. Reliable. With an innovative light distribution that creates a uniform pattern, a “stadium” effect to minimize shadowing, and a feathered edge light pattern that reduces eye fatigue, the A-dec 300 LED light offers 20+ years of illumination.
Contact international@a-dec.com for more information.



EDITORIAL TEAM COORDINATOR ART DEPARTMENT SUBSCRIPTION ADVERTISING PHOTOGRAPHY TRANSLATION
DIRECTOR ISSN
Alfred Naaman, Nada Naaman, Jihad Fakhoury, Dona Raad, Antoine Saadé, Lina Chamseddine, Tarek Kotob, Mohammed Rifai, Bilal Koleilat, Mohammad H. Al-Jammaz
Suha Nader
Marc Salloum
Micheline Assaf, Nariman Nehmeh
Josiane Younes
Albert Saykali
Gisèle Wakim
Tony Dib 1026-261X
DENTAL NEWS IS A QUARTERLY MAGAZINE DISTRIBUTED MAINLY IN THE MIDDLE EAST & NORTH AFRICA IN COLLABORATION WITH THE COUNCIL OF DENTAL SOCIETIES FOR THE GCC.
Statements and opinions expressed in the articles and communications herein are those of the author(s) and not necessarily those of the Editor(s) or publisher. No part of this magazine may be reproduced in any form, either electronic or mechanical, without the express written permission of the publisher.
DENTAL NEWS – Sami Solh Ave., G. Younis Bldg.
POB: 116-5515 Beirut, Lebanon.
Tel: 961-3-30 30 48
Fax: 961-1-38 46 57
Email: info@dentalnews.com Website: www.dentalnews.com
www.facebook.com/dentalnews1
www.instagram.com/dentalnews
twitter.com/dentalnews
Dental News App on both Appstore & Google play




St. Joseph University Dental Meeting

The 2nd Jordanian International Paediatric Dentistry Conference

CAD/CAM 2018

EXPODENTAL 2018 Dental Congress
IADH 2018 The 24th International Association for Disability & Oral Health Congress

FDI 2018 World Dental Congress
BIDM 2018 - Beirut International Dental Meeting

April 18 - 21, 2018
St. Joseph University Beirut, LEBANON Website: www.fmd.usj.edu.lb
April 25 - 26, 2018
LeRoyal hotel Amman, JORDAN Website: www.jda.org.jo
May 4 - 5, 2018 Dubai, UAE Website: www.cappmea.com/cadcam
May 17 - 19, 2018 Rimini, ITALY Website: www.expodental.it
August 31 - September 2, 2018 Intercontinental Festival City Dubai, UAE Website: www.iadh2018.com
September 5 - 8, 2018 Buenos Aires, ARGENTINA Website: www.world-dental-congress.org
October 4 - 6, 2018 BIEL - Beirut, LEBANON Website: www.bidm-lda.com
November 6 - 9,
Alexandria, EGYPT Website: www.aoiaegypt.com/starsmeeting

KDA 2018 Kuwait Dental Association Meeting
November 25 - 27, 2018 KUWAIT Website: www.kda.org.kw

Dr. Fadwa Chtioui DDS and Postgraduate Student Department of restorative Dentistry and Endodontics
University Hospital of Sahloul Sousse, Tunisia
cldfadwa@hotmail.com
Dr. Omar Marouane Assistant Doctor Department of restorative Dentistry and Endodontics
University Hospital of Sahloul Sousse, Tunisia
Dr. Nabiha Douki Head of the department of Odontology, Professor in Restorative Dentistry and Endodontics
University Hospital of Sahloul Sousse, Tunisia
Abstract
Conventional treatment options available to treat enamel Opacities include non-invasive and invasive approaches. Resin infiltration technique has been used in cases of enamel discoloration arising from developmental defects (hypocalcification, fluorosis, and molar-incisive hypomineralization) or white spot lesions (WSL) as a minimally invasive treatment that aims to mask enamel discolorations.
The present paper presents 3 case reports of young patients with white opacities on their incisors. The lesions were categorized according to the new classification of Enamel white lesions (WSTC) consecutively as superficial, mixed and deep enamel white lesions.
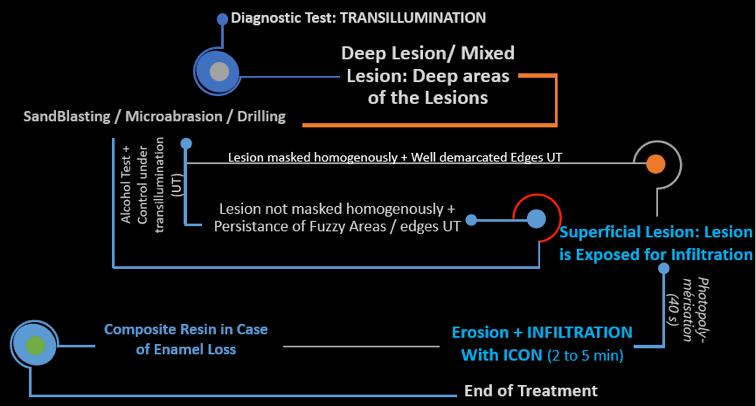
Apart from the superficial lesion which was infiltrated after surface erosion with Icon etch (DMG, Germany), deep and mixed lesions were eventually treated with a combined use of an average of 10 cycles of microabrasion followed by infiltration of the lesion using Icon (DMG, GER), during a 30-minute appointment to correct the aesthetic defect.
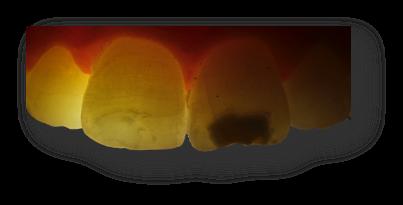
To overcome the difficulty in locating such enamel opacities, transillumination in this procedure was useful for a more predictable and conservative treatment.
The clinical cases illustrated in this work emphasize the major role of the new classification in insuring a more predictable treatment showing the importance of Transillumination in identifying the location but to significantly evaluate the opacity of the lesion.
Key words: Enamel White Lesions; Resin Infiltration Technique; ICON, Transillumination
Introduction
The most important aspect in diagnosis of the enamel demineralization involves accurate and reliable description of such lesions, rather than detection; which mainly requires reading certain topographic characteristics of the enamel opacity. However, the existing devices to directly assess its location within the enamel lesions are expensive and not well-suited for use by most of dental professionals and cannot be used in every practice.
And so, Simple, low cost, fast, chairside approach and accurate tools for a more accurate clinical inspection of white lesions by Dental professionals are always needed 1
This actually comes in response to the constant need of non-invasive management strategies of such lesions.
Analyzing the body and edges of the lesions examined under transillumination has provided interesting information regarding their depth and thickness and helped setting forth a new classification where Enamel lesion which maybe deep, superficial or mixed 1, 2
Studying these dark spots has brought our attention to adopt light-assisted methods towards a modified, non invasive, treatment approach 5, 6. The ‘resin infiltration technique’ was introduced with the development of highly-flowable resin material 7
The first hybrid ceramic with dual network structure for unsurpassed absorption of masticatory forces



• enormous load capacity since masticatory forces are absorbed
• reduction of wall thickness possible to achieve restorations that require minimal preparation
• highly precise and particularly accurate results
• tooth-like material properties
• fast and easy to process with no furnace required








*) In addition to a high degree of elasticity, this innovative hybrid ceramic guarantees outstanding load capacity after adhesive bonding.


To date, Icon (DMG, Hamburg, Germany) remains the most efficient product for the infiltration procedure 3. The main purpose of this therapeutic approach is to infiltrate the hypomineralized enamel with a low viscosity resin having the same optic properties as sound enamel. However, even by following the manufacturer’s instructions, the treatment outcome remains unpredictable, especially when it’s based merely on the lesion’s etiology 8
By describing a modified treatment approach adopted for 3 clinical cases of different topographies within the enamel, the aim of this paper is to emphasize the major role of the new classification in insuring a more predictable treatment and show the importance of Transillumination, not only in identifying the location and the degree of the opacity of the enamel hypomineralization but also in significantly assessing the treatment progress and defining the appropriate time to proceed with the different treatment steps.
A 19-year-old young patient consulted our department the university hospital of Sahloul, Sousse, Tunisia, to correct the white opacity on her Maxillary anterior tooth.
The clinical examination revealed a white lesion aspect on her upper right central incisor, the medical history arose suspicions of a traumatic etiology as the patient couldn’t recall any childhood dental injuries.
Regardless of the cause, the treatment was proceeded after assessing the depth of the lesion according to the new classification criteria 1
The lesion in this case was superficial and the treatment consisted on alternative minimal intervention, avoiding other treatments with more predictable results that would require greater tooth structure reduction, as in using micro abrasive procedures. To solely isolate the lesion, we initially intended to, first of all protect the sound enamel tissue and then the soft tissue surrounding the tooth by


From anterior restorations to mock-ups, the reusable Uveneer direct composite template system allows you to work smarter and faster with





High flexibility
Extreme resistance to fracture
Centred canal preparation
Regeneration by thermal treatment


Initial status showing white lesion on tooth #11
According to the new classification, it shows a thick Superficial Lesion on the enamel (bright white spot)
Visual examination after the erosive cycle, a mild lesion, slightly distinguishable from sound enamel becomes noticeable

covering sound tissues with a light-cured rubber dam instead of the conventional one. This step is called “lesion focalization” which also allows a more conservative and economic treatment 2, 9
The enamel infiltration technique with a resin infiltrant (Icon, DMG, Germany) was selected for this patient. The acid gel (ICON Etch), drying agent (ICON Dry), and resin infiltrant (ICON Infiltrant), which were all applied respecting the manufacturer’s instructions 7, 10
After cleaning the tooth surface with a rubber cup and a prophylaxis paste. The next step consisted of accessing the hypomineralized lesion. Therefore, the surface area of the lesion was eroded with a 15% hydrochloric acid (Icon-Etch DMG) for 120 seconds to expose the lesion’s body. Then, the etching gel was thoroughly washed away for 30 seconds using a water spray. To dessicate the lesions, ethanol was used (ICON-Dry; DMG) for 30 s followed by air drying 7, 10
The Icon infiltrant resin (ICON) was applied to the surface and its penetration within the porous enamel lesion was aided with a microbrush activated in a circular motion for 3 min per application 7 After light curing for 40 s, the application of the infiltrant resin was repeated once for 1 min and light cured for 40 s. Finally, the roughened enamel surface was polished using a composite resin polishing discs. An improvement in the esthetic appearance was achieved by adding a composite resin on the surface to repair the slight enamel loss.
In transillumination, the lesion appears opaque with homogeneous aspect showing sharply demarcated margins
During the Control Under Transillumination, the lesion shows a faint opacity allowing passage of light
Under transillumination right after the erosion and infiltration procedures are done, we may see the disappearance of most of the opaqueness which barely remains at the margins
In our first contribution describing superficial infiltration we limited the application of the erosion/infiltrationtechniquetocaseswithsuperficial lesions which required no dental preparation beforehand 11
In this case, a 27-year-old young patient was chiefly complaining of the aspect of the anterior spot affecting both maxillary central incisors.
Direct visual inspection showed a creamy appearance of the enamel lesion with hardly perceivable interface between sound and hypominerlized enamel areas, while the lesion appeared homogenously opaque with ill-demarcated and dull margins under transillumination. Thus, deep enamel lesion was diagnosed 1, 2
In cases of deep lesions, the lesion is covered with sound enamel tissue, thus the Infiltration takes place on the level of healthy enamel and therefore does not produce a favorable optical effect. Only a small part of the lesion is infiltrated and masking remains insufficient. This is why treating deep lesions by erosion/infiltration has been never, or almost never, successful and the results have never been satisfactory 11
To overcome this treatment failure, the concept of infiltrating deep lesions’ category involves a mild mutilation of the enamel through an average of 10 cycles of microabrasion, around 15 seconds each, should be performed before moving ahead with the erosion/infiltration of the lesion. This will eventually ensure that the infiltration can indeed reach the body of the lesion itself.
Allografts – Xenografts – Alloplasts
The cycles of microabrasion, erosion and application of alcohol will continue until the optical appearance is further improved whether under transillumination as the exposed lesion shows clearly demarcated edges 1, 9 or while the lesion is dried with alcohol (ICON Dry).
Alcohol changes the refractive index of the surface of the enamel 3. Both tests will assist in assessing whether the further microabrasion and surface erosion will be necessary to ultimately expose the lesion almost entirely.

The infiltration can only begin if the optical change concerns the lesion in totality, the latter is now superficial more accessible by the infiltrant 3, 9
A slight loss of the enamel is inevitable in deep lesions due to the surface micro-preparation; however it can be corrected with composite 7
The choice of composite shade may differ according to the amount of tissue loss. The latter can be perceived and evaluated clinically as a concavity in the enamel will be more or less obvious with regard to the importance of enamel preparation 10, 11

Initial status showing white lesion on both teeth #21 & 11 according to the new classification, the Lesion is located deep within the enamel (an ivory-white aspect with blurry edges)
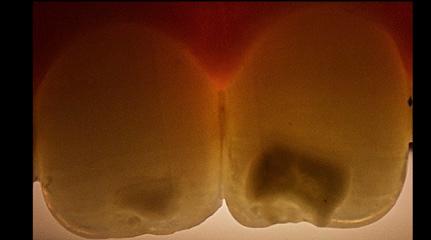
In transillumination, the lesion appears opaque with ill-demarcated and dull margins. The body of the lesion is smooth, showing a heterogeneous opaqueness
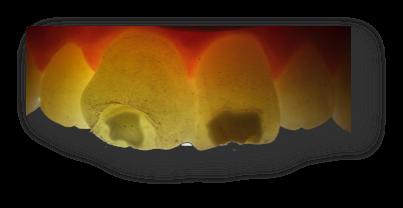
Visual examination after Ten cycles of microabrasion applied to the lesion for 15 secnds each (activated with a micro brush) : hypomineralized enamel became intensely white

Under transillumination, well-demarcated limits are seen between sound and hypominerilized enamel after abrasive & erosive cycles


Post-operative clinical view and under transillumination just after the erosion and infiltration procedure shows the disappearance of most of the opaqueness
Excite patients and advance case acceptance






Carestream Dental makes it easy for you to elevate your practice above the rest with the CS 3600 intraoral scanner. High-speed continuous scanning captures dual arches quickly and easily, while full HD 3D scans simplify communication with patients, referrals and labs. With open system files and no hidden click fees, Carestream Dental has designed the CS 3600 to rise to the challenge of making digital impressions fast, accurate, easy and open. Visit us at www.carestreamdental.com
A 16-year old male patient consulted for an unpleasant aspect of his maxillary Central Incisors. Intra oral examination revealed the presence of a huge hypomineralized lesion occupying almost 2 thirds of both central incisors.
The lesion was defined as mixed according to the new classification 1. Therefore, microabrasion will be focused on deep areas to expose them to the surface and thus assuring the efficacy of the infiltration step.
Added to the alcohol test, inspecting the lesion under transillumination also plays a major role in guiding us towards initiating 1,3,9,12. The enamel loss was repaired with composite resin. We only showed the treatment results of the right incisor in this case.





Celtra® Duo (ZLS) blocks, Prime&Bond universal™ Adhesive, and Calibra® Ceram Cement were designed to enhance and strengthen the individual benefits each of them provides, resulting in an easy-to-use system that streamlines the restoration process.
Celtra Duo (ZLS) blocks
• Restoration longevity of Celtra Duo (ZLS) is ensured when used with Prime&Bond universal Adhesive and Calibra Ceram Cement
• Firing is optional: choose either fire and seat or polish and seat
Prime&Bond universal Adhesive
• No need to use a self cure activator when used with Calibra Ceram Cement
• Low film thickness to allow passive seating of the crown
Calibra Ceram Cement
• One-step curing when used with Prime&Bond universal Adhesive
• 10-second tack cure window and 45-second gel phase ensures an easy, no-stress cleanup

Visual examination after abrasive and erosive cycles shows well-demarcated limits between sound and hypomineralized enamel, which became intensely white
enamel. As the complete infiltration of the lesion remains the key to assure the success of the technique, the present paper aimed to highlight the major role of this classification in aiding a more predictable treatment outcome thanks to the use of direct visual inspection and light-based observation under transillumination.

In a previous article, it was established a new classification for enamel white lesions showing a high reliability in categorizing those lesions according to their topography and depth within the
Thus, this topographic classification has a marked prognostic effect even in cases where the etiology was ill- or not even defined. The main difficulty with this technique is judging at what moment it is possible to perform the infiltration. Sometimes, the infiltration is performed after a large number of cycles of sandblasting or microabrasion cycles and erosion, but never before alcohol producing a clear optical effect and masking the lesion homogenously. The alcohol can also be the fine line between the moment where the body of the lesion is attained and the infiltration is allowed. In fact, the alcohol applied onto the surface of the lesion will change the refractive index of the surface of the enamel as it dries it out. This will assist in assessing whether the resin will make a difference in erasing the white lesion completely or further sand blasting and hydrochloric acid etching will be necessary.
However, transillumination can play a major role as well. Added to the Alcohol test already recommended by multiple authors, transillu-
Henry Schein Brand products are designed to be cost-effective with exceptional value. We offer you solutions to meet your dental procedure needs and make your practice more efficient. From gloves to curing lights, you will find many product options that help you achieve greater patient satisfaction, enhance your productivity, and increase your revenue. Our products have met high standards to earn the Henry Schein Seal of Excellence— your 100% guarantee of satisfaction.
Rely on us to provide a broad selection of cost-effective products and ultimately, to improve your bottom line.


mination also offered a good indicator in this present one to preview the edges resolution and the opacity of the lesion. Following microabrasion, if the lesion doesn’t show well-demarcated margins with a clear interface under transillumination, either chemical erosion should be repeated or further cycles of microabrasion should be performed, specifically in the zones where the lesion edges remain fuzzy and no optical modification is visible.
Infiltrating deep and superficial areas are complementary procedures in cases of mixed lesions. In return for a very slight mutilation of the tooth, deep infiltration makes it possible to treat all white spot lesions of the enamel, whatever their
etiology or depth once they were correctly identified according to the new classification. The dark hallow which might be seen around the lesion by the end of the treatment, marks areas where the infiltration wasn’t achieved, and may present the limitation of the infiltration technique in cases of deep and mixed lesions.
Adopting conservative treatment approaches remains a priority before having recourse to any substantial enamel preparation. The new classification of enamel white lesions allows a fast, easy and a more predictable and conservative treatment. We also tended to assure the lesion focalization during the treatment procedure in order to obtain a more conservative and economic treatment.
• high level of adhesion
• highly biocompatible, low acidity
• continuous fluoride release

• precision due to micro- fine film thickness
• translucency for an aesthetic result
If you are interested in our entire product range and detailed product information visit our website or contact us directly
1. Chtioui F, Marouane o, Douki n enaMel White lesions (Part i): a neW toPograPhiC ClassiFiCation (eWlC). Dent neWs (lonD). 2017;24(4):12–24.
2. Marouane o, Douki n, Chtioui F. alternative Conservative treatMent For enaMel White lesions: a Case rePort. J CosMet Dent 2017;33(3):48–54.
3. greenWall l. White lesion eraDiCation using resin inFiltration int Dent. 2013;3(4):54–62.
4. horuztePe sa, Baseren M. eFFeCt oF resin inFiltration on the Color anD MiCroharDness oF BleaCheD White-sPot lesions in Bovine enaMel (an in vitro stuDy). J esthet restor Dent. 2017;29(5):378–85.
5. Coelho Ms, CarD sJ, taWil Pz visualization enhanCeMent oF Dentinal DeFeCts By using light-eMitting DioDe transilluMination. J enDoD 2016;42(7):1110–3.
6. Park t-y, Choi h-s, ku h-W, kiM h-s, lee y-J, Min J-B. aPPliCation oF quantitative light-inDuCeD FluoresCenCe to DeterMine the DePth oF DeMineralization oF Dental Fluorosis in enaMel MiCroaBrasion: a Case rePort restor Dent enDoD. 2016;41(3):225–30.
7. DhaiMy s, hinD a, DhouM s, Benkiran i treatMent oF laBial enaMel White sPot lesions By resin MiCro-inFiltration eC Dent sCi 2016;4(5):1149–55.
8. ChaWla n, Messer e, silva M. CliniCal stuDies on Molar-inCisorineralisation Part 1: DistriBution anD Putative assoCiations eur Diatr Dent. 2008;9(4):180–90.

arouane o, Douki n traiteMent FoCal De l ’hyPoMinéralisation De l’éMail l’inForMation Dentaire. 2016;27(7):2–7. illarroel M, Fahl n, De sousa a De oo. DireCt esthetiC BaseD on transluCenCy anD oPaCity oF CoMPosite resins. J estor Dent. 2011;23(2):73–87.

JP, atlan a, Denis M, vennat e, tirlet g taChes BlanChes rotoCole De traiteMent Par inFiltration suPerFiCielle ou en Partie 2). int orthoD. 2014;12(1):1–31. a resin inFiltration May Be ConsiDereD as a ColorreatMent oPtion For enaMel DeveloPMent DeFeCts anD esions. J eviD BaseD Dent PraCt. 2017;17(2):113–5. , hur B, kiM h-C, Park J-k. ManageMent oF White sPots: iltration teChnique anD MiCroaBrasion. J korean aCaD Con. 2011;36(1):66.



Dr Mayada Jemâa, Assistant Professor, Department of Dental Medicine, Military Principal Hospital of Instruction, Tunis, Tunisia.
dr.jemaamayada@gmail.com
Dr T. Ben Neji, Resident in Restorative Dentistry and Endodontics, Military Principal Hospital of Instruction, Tunis, Tunisia.
Pr N. Zokkar, Professor, Department of Restorative Dentistry and Endodontics, Dental Clinic, Monastir, Tunisia.
Dr H. Ouertani, Assistant Professor, Department of Dental Medicine, Military Principal Hospital of Instruction, Tunis, Tunisia.
Dr H. Jegham, Assistant Professor, Department of Dental Medicine, Military Principal Hospital of Instruction, Tunis, Tunisia.
Pr L. Bhouri, Professor, Department of Restorative Dentistry and Endodontics, Dental Clinic, Monastir, Tunisia.
Pr MB. Khattech, Professor, Department of Dental Medicine, Military Principal Hospital of Instruction, Tunis, Tunisia
Abstract
Teeth discoloration is a fundamental aesthetic problem. It has a social impact on children, adolescents and adults. It is necessary for dentists to identify the etiology of teeth discoloration to establish an accurate and proper diagnosis. There are different options to treat discolored teeth such as restorative procedures, veneers, crowns… Actually, bleaching of non-vital teeth is a routine conservative approach to have a suitable esthetic result for endodontically treated teeth.
Various methods to bleach non-vital teeth have been proposed. Three techniques were described through the literature: the walking bleach technique, the inside/outside bleach technique and the in-office bleaching procedure. The most recommended one is the walking bleach technique since it is simple, safe, with lower risks and suitable for patients and dentists.
Different bleaching agents were used such as sodium perborate, hydrogen peroxide and carbamide peroxide with various concentrations. Some side effects were reported like external root resorption, diminution of tooth resistance (fracture…), morphological alteration of dental hard tissues and alteration of the characteristics of dental materials.
The objectives of this article:
- To describe the causes of discolored non-vital teeth,
- To explain the protocol of the different bleaching procedures and the agents used for,
- To report different clinical cases of discolored non-vital teeth treated in our service of Dental Medicine with internal bleaching procedures.
Key words
Non-vital teeth, Discoloration, Bleaching, Carbamide peroxide, Hydrogen peroxide, Sodium perborate, Cervical root resorption.
Introduction
In our daily dental practice, we observe the increasing demand for esthetics in all fields of dentistry. Esthetic procedures can vary from restorative techniques such as conventional crowns, veneers, or bonding to bleaching treatments. 26 Despite different methods that can improve esthetics; bleaching procedures are safe, minimally invasive, conservative, low cost and effective to treat discolored teeth. 11
Referring to Zarow et al. 2014, even the esthetic treatment plan is based on conservative or prosthodontic procedure; dentist should start with teeth bleaching.
Referring to Rona et al. 2009, the discolored teeth can have an incidence on the self-confidence, self-image, attractiveness and employability of every one. 6
Actually, bleaching of non-vital teeth is considered as a popular procedure because of the continuous need for white teeth and good looks. 1 The internal tooth-bleaching is used to lighten a discolored tooth that was endodontically treated and the procedure consists of the placement of a chemical oxidizing agent within the cavity access chamber to remove discoloration. 25
The first reports concerning bleaching of discolored non-vital teeth were published in the middle of the 19th century. 2, 3
Dynamic power responsiveness for superior osseous surgery





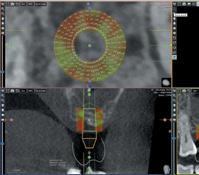















The 3D technology that facilitates the implant planning with immediate volume measurement and bone density assessment










Different chemical agents were used to bleach discolored teeth such as chlorinated lime, oxalic acid, acetic acid, chlorine compounds and solutions, sodium peroxide, sodium hypochlorite, different concentrations of hydrogen peroxide, carbamide peroxide and sodium perborate. 1, 2, 3, 4, 23
The mechanism of action of the different bleaching products is the same. The hydrogen peroxide will decompose into oxygen and water. Then, the oxygen will cause the oxidation and reduction of the organic pigments that are mainly concentrated in the dentin structure. As a result, we obtain the bleaching impact. 7 Referring to literature, we can use light, heat and even electric currents to activate the bleaching agents and to have a rapid result. 2
Clinical examination and radiographic exploration are important before establishing the treatment plan of bleaching. In case of discolored tooth, a periapical radiograph is necessary to evaluate the quality of endodontic filling, the periapex region and a possible alteration of a resorption process. 24 Dentist must define the etiology of the dental discoloration that will have a deep impact on the success of the bleaching treatment. 3
Various procedures are available for non-vital tooth bleaching: In-office bleach technique, Inside/outside bleach technique and Walking bleach technique. Some side effects have been reported in non-vital tooth bleaching including external root resorption, alteration of morphology of dental tissues, modification of the properties of restorative materials and reduction of tooth resistance and adhesion. 7
It is important that clinicians understand the etiology of tooth discoloration to establish the appropriate diagnosis and to define which treatment to apply. 2, 3
Referring to Zimmerli et al. 2010, the intrinsic discoloration is a discoloration that originates from the pulp chamber. Dental trauma or removal of the pulp tissue are the most common causes of intrinsic discoloration. 19
The optical properties and interaction with light of both enamel and dentin help to define the intrinsic color. 2
The modifications of enamel or dentine structures and the induction of different chromatogenic materials into the dental tissues during odontogenesis or in post eruption lead to the intrinsic tooth discoloration. 2, 5
The intrinsic discoloration can be brown, grey, red or yellow. 5 The regular prophylactic techniques cannot remove the intrinsic discoloration and the best treatment is bleaching using
various penetrating agents into enamel and dentin to oxidize the chromogens. 8
- Pulp necrosis:
Pulp necrosis can be caused by mechanical, bacterial or chemical irritations. Chromogenic degradation products such as protein degradation products of the pulp tissues can be generated by pulp necrosis leading to tooth discoloration. 1
The degree and the severity of the intrinsic discoloration is proportional to the period that pulp tissues has been necrotic. 2, 3
The treatment of choice for this discoloration is the intracoronal bleaching. 2, 3
- Intrapulpal hemorrhage:
After dental trauma, the intrapulpal bleeding is the most common etiology of tooth discoloration. 1 After rupture of blood vessels, the blood will penetrate the tubules of dentin and its consecutive break down will lead to different chromogenic degradation products like hematoidin, hemine, hemosiderin and hematin. 1, 5 Added to that, pulp extirpation can generate hemorrhage in the pulp chamber. 1, 2, 3, 26
At first, a pink coloration of the crown can be noticed. 2, 3
The iron (Fe) formed by the combination of heme and the putrefying tissue of the pulp will be turned into dark colored iron sulfates by hydrogen sulfates causing a grey staining of the tooth2 Referring to Umar et al. 2014, the modification of tooth color is related to the degree of disintegrated hemoglobin.
- Calcification of the pulp:
In case of calcification of the pulp, there is an obliteration of the dentinal tubules and accumulation of reactionary tertiary dentin.1 Referring to Fearon et al. 2007, we observe a yellow discoloration in case of accumulation of tertiary dentin in the canal and the pulp chamber. This yellow discoloration is not only due to the important volume of additional dentin in the pulp chamber but also due to the translucent enamel.
Generally, the treatment of calcified and discolored tooth is invasive and not conserving the vitality of the pulp (direct or indirect veneers, or ceramic crowns). However, according to Ramos et al. 2013, when respecting the concepts of minimally invasive dentistry and preserving tooth vitality, performing an in- office external bleaching combined with supervised home bleaching is the recommended treatment especially when there is no indication for endodontic treatment.
- Endodontic materials:
The incomplete removal of filling materials, sealer residues and medicaments with tetracycline in endodontically treated tooth can cause coronal discoloration. 2, 3 , 26
Personalized coaching for better coverage, reduced scrubbing and ideal pressure via the Philips Sonicare app Smart Sensor Technology




Smart Brush Head Recognition Technology
Automatically chooses the optimal mode and intensity level and monitors brush head lifetime
High Performance Brush Heads
Up to: 10x better plaque removal,1 7x healthier gingiva1 and 5x more stain removal2
Referring to Zimmerli et al. 2010, the combination of some irrigants like sodium hypochlorite and chlorhexidine will cause brownish-red precipitates. That is why a separate rinse between the two different solutions with distilled water or Ringer’s solution is recommended. Despite intracoronal bleaching is the best treatment; the prognosis is related to the type of materials and the contact period. 2, 3
- Incomplete removal of pulp tissue:
The incomplete removal of the pulp tissue especially in the pulp horn area during endodontic treatment can cause discoloration by the persistent residual tissue. 1, 5, 26
The residual tissues will disintegrate progressively, and blood components will infiltrate into the dentinal tubules, causing discoloration. 2, 3 The elimination of the remaining tissue and the intra-coronal bleaching is the recommended treatment. 3
- Coronal restorative materials:
Ancient composite restorations can lead to dark discoloration of margins and even discoloration of dental tissues due to the microleakage formed in resin composite. 2, 3
The amalgam can produce a dark grey coloration of dentin when it is used after endodontic treatment because of the black metallic compounds. 2, 3 The use of metal posts for realizing a core can cause discoloration of the crown because of the metallic ion release and transparent enamel. 2, 3
Bleaching agents of Root-filled Teeth
Referring to Carey et al. 2014, bleaching procedure is determined as the chemical degradation of the chromogens. The most used bleaching agents are hydrogen peroxide, carbamide peroxide and sodium perborate. Other ingredients may be present in the different bleaching products like thickening agents, surfactant, carrier and pigment dispersant, preservative, and flavoring. 8
- Hydrogen peroxide HP (H2O2): 2, 4, 9, 26
Nowadays, it is the active and most commonly used ingredient in whitening products. It is used directly or resulting from a reaction involving sodium perborate or cabamide peroxide. Referring to Bahuguna et al. 2013, the commonly used bleaching chemical agents are oxidizers since they degrade the organic structures of the tooth into shorter lighter in color molecules.
- Carbamide peroxide CP (CH4N2O • H2O2): 1, 2, 9, 19, 25
It is also called urea peroxide. An organic white crystalline compound formed by hydrogen peroxide and urea. Bleaching agents with 10% carbamide peroxide will release 3.5% hydrogen. The stable complex will decompose in contact with water to release hydrogen peroxide.
Most of the time, carbamide peroxide is used in a 37% concentration for internal bleaching.
Referring to Douglas et al. 2016, the use of carbamide peroxide for non-vital bleaching is a safe and secure alternative since the diffusion of the hydrogen peroxide to the external root surface is lower and the pH in the external root surface is higher. Added to that, the use of 37% carbamide peroxide generates less structural weakening of the bleached structure compared with sodium perborate.
- Sodium perborate: 1, 2, 25, 26
It is also called perboric acid. Different forms: mono-, tri(NaBO2 • H2O2 • 3H2O) or tetrahydrate. It is an oxidizing agent presented as a powder.
Sodium perborate will decompose to form sodium metaborate, hydrogen peroxide and nascent oxygen when it is in contact with water, acid or even warm air.
It is often used for internal bleaching since it has excellent results and it respects the periodontal tissues.
Different authors recommend the use of a mixture of sodium perborate and distilled water. However, Kwon et al. 2011 suggested that when we use 30% of hydrogen peroxide mixed with sodium perborate (ratio 2:1 g/mL), we obtain an alkaline pH and the bleaching agent will be more effective.
26, 27
The initial examination is very important in the treatment plan. It includes the evaluation of the color of teeth and the adjacent gingiva.
Added to that, the vitality of teeth must be tested and a radiographic examination is recommended. Dentists must question patients that are presenting a discolored tooth about any history of traumatic injury.
Referring to Van B. Haywood et al. 2010, pulpal problems can happen from 1 to 20 years after dental trauma. Dentists should evaluate the color of the gingival tissues, their thickness and their level. In addition, the color of the root must be taken into consideration.
The discolorations of the gingival tissues may lead to a tooth with a not harmonious color match. Referring to Kwon et al. 2011, the root dentin is different from the dentin in the crown and does not bleach well if at all, nevertheless internal or external bleaching is done. In case that the patient suffers from a gummy smile or hyperactive lip, these problems will be more evident.

To learn about the advanced design and the future of ceramic appliances, contact your local distributor or email us on marketing.emeai@ormco.com
— Carl SaganFrom the introduction of the original Straight-Wire™ launched in 1970 by A-Company, Ormco is uniquely positioned to marry the wisdom of legacy with the latest in ceramic materials and our advanced manufacturing technology

COMING SOON





The different bleaching techniques
- The walking bleach technique:
In this therapy, clinician applies a bleaching agent into the empty pulp chamber of an endodontically treated and discolored tooth.5
This technique was first described using a mixture of sodium perborate and distilled water. Later, some authors suggested replacing water by 30% hydrogen peroxide to ameliorate the bleaching efficiency. 1, 2
However, referring to Zimmerli et al. 2010, there is no difference in efficiency between the two methods and that using carbamide peroxide in concentrations of 10% or 35% mixed with sodium perborate will improve the bleaching effectiveness.
Treatment steps referring to Kwon et al, 2011:
• Make a radiographic exam to evaluate the presence or not of a root canal filling and to assess the quality of the endodontic filling.
• Isolate the tooth by means of a rubber dam.
• Clean the pulp chamber and the pulp horns of any debris or pulpal remnants to have the entire pulpal cavity visible and cleanable.
• Eliminate the gutta percha with a heated instrument or a low-speed small round bur to 2 mm below the cementoenamel junction CEJ. We can also use Gates-Glidden or Largo burs. This step can be controlled with a periodontal probe.
• Place a cervical barrier of 2mm thickness with a glass-ionomer cement or a flowable resin to seal the endodontic filling material from the pulp chamber. It is important that the shape of the cervical barrier should be like to the external anatomic landmarks replicating the CEJ level and the interproximal bone level.
• Mix sodium perborate with water or hydrogen peroxide in a ratio of 2:1 (g/mL) to a thick mix.
• Insert the mixture into the pulp chamber with an amalgam carrier or an applicator.
• Use a damp cotton pellet to eliminate the excess.
• Seal the access cavity with a provisional filling material like Cavit, glass-ionomer cement or IRM.
Referring to Fearon et al 2007, the bleaching agent should be covered with cotton pellet and sealed with an adhesive temporary restoration. 5
The provisional adhesive restoration is recommended because it ameliorates the seal against the penetration of bacteria. 1
In the next appointment (after 3 to 5 days), the bleaching result is evaluated and, if necessary, the walking bleach procedure is repeated (3 to 5 times) until the color becomes similar to the adjacent teeth. 26



The final step after the last walking bleach technique is the restoration of the access cavity with resin composite. This procedure is achieved 2 to 3 weeks later when the desired color change is obtained and the bond strength to the tooth has returned to normal. 26 The resin composite used for final restoration should have a light color. 5
The walking bleach technique is not recommended only for adults but also for children with colored non-vital tooth. A case report of a 12-year-old female patient treated with internal bleaching and with 6 years follow-up showed good prognosis and no reversal of tooth discoloration. 21
The walking bleach technique using sodium perborate mixed with distilled water is recommended as a secure alternative in whitening non-vital primary teeth with intrinsic discoloration. 28
- The inside/outside bleach technique:
The principle of this technique is to apply the bleaching agent in the same time on the facial enamel (outside) and the sealed cavity access (inside) of the discolored endodontically treated tooth. 1, 5
For this technique, we use a vacuum-processed plastic mouthguard that is cut to the facial and lingual margins after taking an alginate impression of the whole arch. 5 The preparation of the cavity access and the achievement of the cervical barrier were performed as previously described for the walking bleach technique.
The bleaching agent used is 10% to 20% carbamide peroxide gel (syringe) that the patient inserts in the access cavity and the marked tooth of the vacuum-drawn splint. 1, 5, 26, 27
Some instructions to give to the patient: To eliminate the excess of the bleaching agent after inserting the splint with a fingertip or a cotton swab and to place a cotton wool plug in the cavity access to prevent accumulation of food particles. 1, 5
In the control visits, when the non-vital tooth has been bleached, the steps followed are as previously described for the walking bleach technique. The major drawback of this technique is the lack of bacterial control affecting the result and the endodontic treatment longevity. 1
The risk of this technique is stopping the bleaching by the patient himself and not returning to the dental office in time to seal the cavity access. 27
- In-office bleaching technique:
For this technique, a high concentration of hydrogen peroxide 35% is used like in-office bleaching of vital teeth. 26
The hydrogen peroxide will be applied in the external and/ or the internal surface of the discolored tooth and it can be activated with light and/or heat to increase the chemical reaction. 27
The major risk of this technique is resorption and loss of the tooth because of the history of trauma, the high concentration of hydrogen peroxide used, the high heat used to activate the bleaching agent, the absence of seal over the gutta-percha and the absence of connection between enamel and cementum. 27 For this technique, it is recommended to isolate the tooth with a rubber-dam. [1, 26]
The application time of the bleaching agent is 15–20 minutes. Then, the gel is eliminated and rinsed off. The application is repeated until the desired shade is obtained. [1]
- Cervical root resorption:
Referring to Bahuguna et al. 2013, it is defined as an inflammatory mediated external resorption affecting the root, occurring after trauma and after internal bleaching. The bleaching agent will diffuse via dentinal tubules and reaches the cervical cementum and the periodontal ligament initiating an inflammatory reaction. 4, 6
The use of an important concentration of hydrogen peroxide activated with heating can lead to cervical root resorption. 4, 5, 6 This complication of bleaching can develop when a thermo-catalytic bleaching technique is employed in teeth presenting cervical defects of the cementum. 4
The use of 30% hydrogen peroxide alone or mixed to sodium perborate is more toxic and dangerous for the periodontal ligament cells than the mixture of sodium perborate and water. 5 Most of the times, the diagnosis of the cervical root resorption is done after several years. 4
This complication is observed through routine radiographs. However, in some cases we can note the presence of papillary swelling and tenderness to percussion. [5] Referring to Leith et al. 2009, there is no evidence that cervical resorption can occur after using a low concentration of hydrogen peroxide associated with heat like in inside/outside bleaching procedure.
A clinical case treated by Kim et al. 2012 showed an invasive cervical resorption. The explanation of the authors was the damage of the cervical cementum resulting from avulsion (after trauma) and from intra-coronal walking bleach technique (sodium perborate and distilled water).































- Effects on enamel:
Bleaching of non-vital teeth can lead to substantial alteration of the enamel surface topography. The amount of alteration depends on concentration of peroxide used and the period of exposure. 5 The considerable alterations affecting the enamel after bleaching described in literature are: 8
• Augmentation of porosity of the superficial enamel structure.
• Demineralization.
• Reduction of protein concentration.
• Degradation of organic matrix.
• Changing in the calcium: phosphate ratio, calcium loss. Other morphological alterations that can affect enamel surface are shallow depressions and slight erosion. 8
After bleaching, the surface roughness will be increased and the bleached teeth will be more vulnerable to extrinsic discoloration. 5 Added to that, the use of 35% hydrogen peroxide increase the diminution of hardness and the histomorphologic changes of the enamel surfaces exposing the tooth to risk of caries. 8 Reducing the contact time of 35% hydrogen peroxide or its concentration will produce a progressive color change of the tooth and will minimize the diffusion of hydrogen peroxide through both enamel and dentin. 12
The diminution of bond strength of enamel and dentin treated with HP is caused by residual oxygen existent in enamel and dentin pores after bleaching treatment. 10
- Effects on dentin:
Referring to Berger et al. 2014, the presence of calcium in the composition of bleaching products will influence the flexural strength of bovine dentin after bleaching procedure (office bleaching 35% HP and home bleaching 7.5% HP).
A study of Pessarello et al. 2012 that evaluated the bond strength of adhesive systems and composite resin to bleached dentin concluded that the association with fluoridated adhesive and flowable resin ameliorates the shear bond strength of dentin submitted to internal bleaching.
- Effects on restorative materials:
The oxygen released into the tooth structure after bleaching will inhibit the polymerization of resin. 5
The use of 10–16% carbamide peroxide will lead to an increase in surface roughness and numbers of porosities of microfilled and hybrid composite resins. 8
Referring to Bahannan et al. 2015, the influence of bleaching agents on surface roughness can be considered concentration dependent.
Carbamide peroxide with different concentrations did not produce a prejudicial effect on the fracture toughness and flexural strength of composite resin. Added to that, in-office bleaching agents (35% CP and HP) did not
affect the tensile strength of composite resin. 13 The microhardness of nano composite resin and resin modified glass ionomer is reduced significantly with 20% and 35% carbamide peroxide. 11
Clinicians have to inform their patients concerning possible modifications that may affect their existing restorations by bleaching agents and the possibility of replacing them after the treatment due to color difference and surface or subsurface alteration. 8, 13 Concerning the glass ionomer cement, the setting of cement is inhibited by the residual oxygen. 10
It is necessary to wait at least 2 weeks before placement any adhesive restorative material after completion of bleaching. 13
Referring to Vohra et al. 2013, bleaching procedure using 10% carbamide peroxide reduce importantly the microtensile bond strength of resin composite to enamel. Moreover, it is recommended to use 10% sodium ascorbate when resin composite restoration will be placed instantly after bleaching. The application of 10% sodium ascorbate for 10 min is enough to have a reversal effect. 14
Referring to Feiz et al. 2017, the use of antioxidant agents, regardless of their type, form, concentration and duration of application, can improve the shear bond strength after bleaching. To dissolve the remnants of peroxide, dentists can clean the cavities with catalase or 10% sodium- ascorbate. However, their applications can be time-consuming or expensive. 10
The placement of a protective varnish on the surface of restoration can be advantageous to reduce the adverse bleaching effects on restorations. 13
When the duration of application of sodium perborate –hydrogen peroxide mixture is increased, the rate of microleakage of the restored access cavities will be more important. For this reason, it is recommended to use intracoronal medication of calcium hydroxide (7 days) after walking bleach technique. 10
A study of Azevedo et al. 2011, evaluated the fracture resistance of teeth treated with internal bleaching and restored with various procedures. The conclusion was that bleached teeth can be restored with composite resin alone and the use of posts in these teeth did not ameliorate their resistance.
Another study of Leonardo et al. 2014, evaluated the fracture resistance of teeth exposed to several internal bleaching protocols using 35% hydrogen peroxide, 37% carbamide peroxide, 15% hydrogen peroxide with titanium dioxide nanoparticles photo activated by LED-laser or sodium perborate. The conclusion was that all these protocols reduce, in equal values, the fracture resistance of endodontically treated teeth.
Minimally invasive, maximally effective

The force in bone surgery:
Piezomed offers extremely high performance, yet is gentle on soft tissue. In addition, it includes automatic instrument recognition and LED handpiece illumination. The handpiece with the cable is thermo washer disinfectable and sterilizable!
Clinical cases:
Case report N°1:
A 17-year old patient was unsatisfied with the discoloration of the tooth 21. History: trauma. The treatment proposed was the endodontic retreatment of the 21 and walking bleach technique using Endoperox kit (100 % carbamide peroxide).
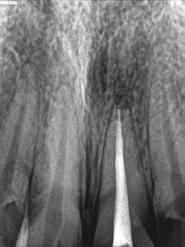
Non-vital


2:
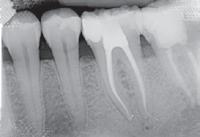
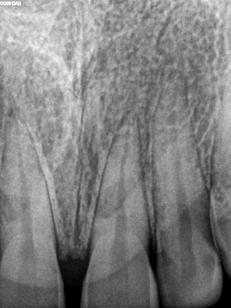
Periapical radiograph showing bad quality of root canal filling.
3: Endodontic retreatment of the tooth 21.
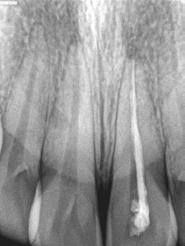


Removing the gutta
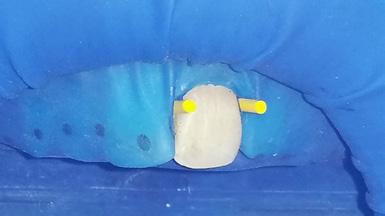
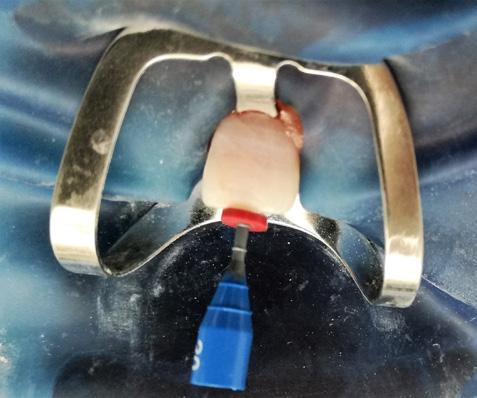
root canal filling material with a round ended, long shank bur below the CEJ and placing a cervical barrier of 2mm thickness with glass-ionomer cement to protect the periodontal ligaments from the diffusion of the bleaching agent.

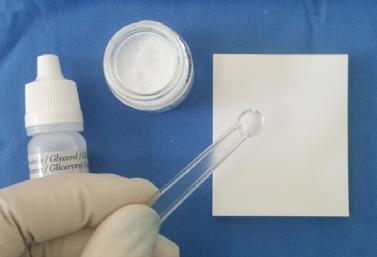
Figure 9:
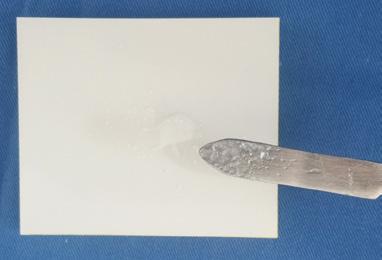
The bleaching agent used Endoperox kit (100 % carbamide peroxide). Kit containing: 1 x 5 g bottle of powder, 1 x 5 ml flask of glycerol and 1 measuring spoon.


Figures 10, 11, 12:
Making a paste by mixing two spoonfuls of powder with 1 drop of glycerol to a firm consistency then placing the mixture into the pulp chamber.
week

Case report N°2:
A 29-year old patient was unsatisfied with the discoloration of the tooth 21. History: trauma. The treatment proposed was the endodontic treatment of the tooth 21 and walking bleach technique using Endoperox kit (100 % carbamide peroxide).
Pre-treatment

Safety
Quality of cleaning
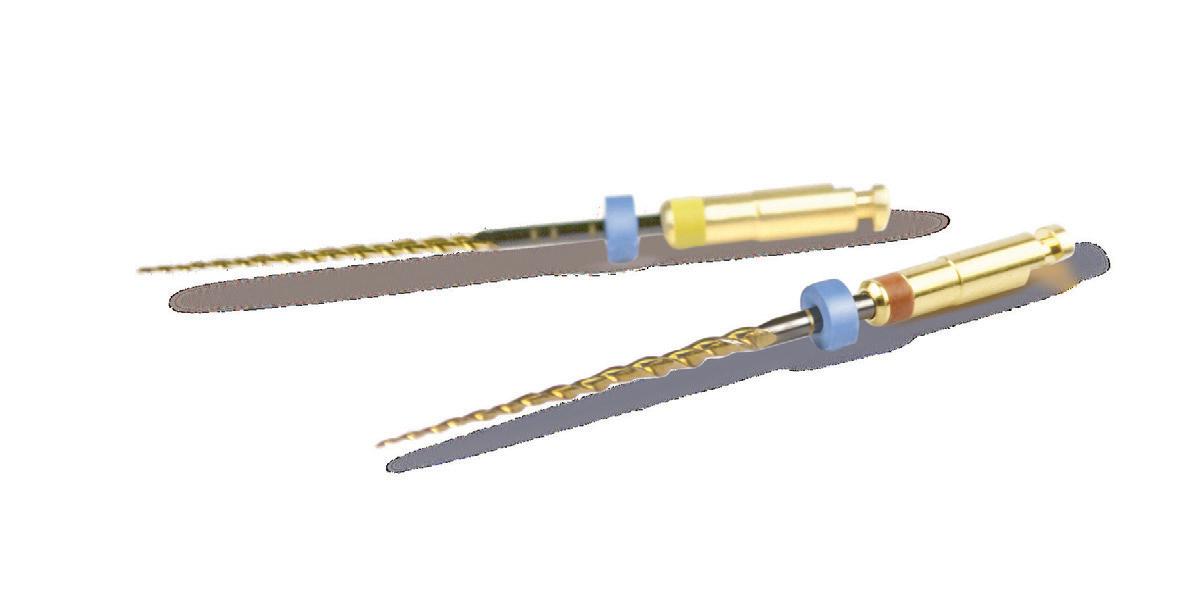
P ropri e tary H eat Tre a tm e n t p ro ces s
Inc reas e s flex i b i lit y Mini m iz e s th e ris k o f i nstrumen t fra c tu re



Usability







Asiga MAX TM : For the digital workflow in your laboratory.
the most compact UV HD 3D printer on the dental market 62 μm resolution
SPS (smart positioning system) for precise printing results fill-quantity monitoring individual support for the complete service life

www.scheu-dental.com


4 shades cover 8 VITA classical A1-D4® shades
Increased wear resistance and strength
Smooth high gloss finish every time
• Non-sticky consistency makes it simple to sculpt
• Low volumetric shrinkage to offset marginal stress
• 4 universal shades to minimise inventory
• No slumping and holds its shape
• Available in syringes and complets
SDI’S

One Bulk Fill placement up to 5mm depth of cure†
20 sec. LED light cure
Natural-looking finish with just one universal shade
High depth of cure without the need for a capping layer
Easy placement in a matter of seconds
The waxy consistency is packable and non-sticky to optimise handling
Low volumetric shrinkage
aura bulk fill delivers reduced stress to provide long-lasting restorations
Excellent flexural strength
aura bulk fill resists major deformations without fracturing
High compressive strength
aura bulk fill resists the high forces of compression in the mouth

Case report N°3:
A 64-year old patient was unsatisfied with the discoloration of the tooth 11 caused by trauma. The treatment proposed was the walking bleach technique using sodium perborate with distilled water.
19: Clinical appearance of the discolored traumatized tooth 11 before treatment.

20: The panoramic radiograph.
Figure 21:
Opening the cavity access and removing the gutta percha root canal filling material to 2 mm below the CEJ.
Figure 22: The bleaching agent used was a mixture of sodium perborate and distilled water. Then, Cavit was used as a temporary filling material.



23: After reaching the final result (1 month), the definitive resin composite restoration was placed.




Case report N°4:
A 32-year-old patient was unsatisfied with the discoloration of the tooth 11 caused by trauma. The treatment proposed was the walking bleach technique using sodium perborate with distilled water.




Bleaching of non-vital teeth can be achieved by either walking bleach technique, inside/outside bleach technique or in-office bleaching procedure. The bleaching agents used are sodium perborate, hydrogen peroxide and carbamide peroxide.
The above clinical cases highlight the effectiveness of the walking bleach technique in producing successful esthetic results and patients showed satisfaction with the outcome. Referring to literature, bleaching of non-vital teeth is an effective and safe technique to manage discoloration. However, clinicians must inform their patients about the potential risk of cervical resorption.
After termination of bleaching, it is recommended to delay resin composite restoration for at least 1–3 weeks. Each year follow-up visits are advisable to control the outcome and to repeat the bleaching treatment when clinician detects a regression of the initial result to preserve the desired esthetic color.
1. BleaChing oF nonvital teeth a CliniCally relevant literature revieW. Brigitte ziMMerli, Franziska Jeger, aDrian lussi sChWeiz MonatssChr zahnMeD 120: 306–313 (2010).
2. nonvital tooth BleaChing: a revieW oF the literature anD CliniCal ProCeDures gianluCa Plotino, laura Buono, niCola M. granDe, Cornelis h. PaMeiJer, FranCesCo soMMa. Joe voluMe 34, nuMBer 4, aPril 2008.
3. BleaChing DisColoreD Devital teeth With using oF neW agents iBrahiM uMar, hakan kaMalak iosr Journal oF Dental anD MeDiCal sCienCes (iosr-JDMs) voluMe 13, issue 3 ver i. (Mar. 2014), PP 79-82.
4. CerviCal root resorPtion anD non vital BleaChing nikhil Bahuguna enDoDontology voluMe: 25 issue 2 DeCeMBer 2013.
5. tooth Whitening: ConCePts anD Controversies. Johnny Fearon Journal oF the irish Dental assoCiation 2007; 53: 132 – 140.
6. an eFFeCtive BleaChing teChnique For non-vital, DisColoureD teeth in ChilDren anD aDolesCents rona leith, aBigail Moore, anne C. o’Connell Journal oF the irish Dental assoCiation 2009; 55 (4): 184 – 189.
7. PreFerenCes on vital anD nonvital tooth BleaChing: a survey aMong Dentists FroM a City oF southern Brazil. Flávio FernanDo DeMarCo, MarCus Cristian Muniz ConDe, Caroline ely, eliana nasCiMento torre, José riCarDo souza Costa, María raquel FernánDez, sanDra Beatriz Chaves tarquinio. Brazilian Dental Journal (2013) 24(5): 527-531.
8. tooth-BleaChing ProCeDures anD their Controversial eFFeCts: a literature revieW. MohaMMeD q alqahtani the sauDi Dental Journal (2014) 26, 33–46
9. tooth Whitening: What We noW knoW. Carey CM. the Journal oF eviDenCe-BaseD Dental PraCtiCe (2014), Doi: 10.1016/J JeBDP.2014.02.006.
10. eFFeCt oF BleaChing on restorative Materials anD restorations a systeMatiC revieW thoMas attin, Christian hannig, annette WieganD, rengin attin. Dental Materials (2004) 20, 852–861.
11. eFFeCts oF DiFFerent BleaChing agent ConCentrations on surFaCe roughness anD MiCroharDness oF esthetiC restorative Materials salMa a. Bahannan the sauDi Journal For Dental researCh (2015) 6, 124–128.
12. eFFeCtive tooth-BleaChing ProtoCols CaPaBle oF reDuCing h2o2 D FFusion through enaMel anD Dentine. Diana g soares, FernanDa g. Basso, elaine C.v. Pontes, luCas Da F.r garCia, JosiMeri heBling, Carlos a De souza Costa Journal oF Dentistry 42 (2014) 351-358.
13. eFFeCts oF BleaChing agents on Dental restorative Materials: a revieW oF the literature anD reCoMMenDation to Dental PraCtitioners anD researChers hao yu, Changyuan zhang, shao-long Cheng, hui Cheng. Journal oF Dental sCienCes (2015) 10, 345-351.
14. inFluenCe oF BleaChing anD antioxiDant agent on MiCrotensile BonD strength oF resin BaseD CoMPosite to enaMel. FahiM ahMeD vohra, kaMsiah kasah the sauDi Journal For Dental researCh (2014) 5, 29–33.
15. non-vital tooth BleaChing. MaCieJ zaroW httPs://WWW styleitaliano org/MaCieJ-zaroW-non-vital-tooth-BleaChing/
16. eFFeCt oF BleaChing agents on the Flexural strength oF Bovine Dentin. Berger sB, Pazenhagen r, Martinelli n, Moura sk, De Carvalho rv, guiralDo rD. J ConteMP Dent PraCt 2014;15(5):552-555.
17. BonD strength oF Dentin suBMitteD to BleaChing anD restoreD With DiFFerent Materials nelize MarCelino Pessarello, yara t. Correa silva-sousa, FuaD JaCoB aBi raCheD-Junior, aline evangelista souza-gaBriel rsBo. 2012 Jul-seP;9(3):286-91.
18. invasive CerviCal resorPtion: treatMent Challenges yookyung kiM, Chan-young lee, euiseong kiM, Byoung-DuCk roh httP://Dx Doi org/10.5395/rDe.2012.37.4.228
19. esthetiC rehaBilitation With tooth BleaChing, enaMel MiCroaBrasion, anD DireCt aDhesive restorations. Bezerra-Júnior DM, silva lM, Martins lDe M, Cohen-Carneiro F, Pontes Dg gen Dent. 2016 Mar-aPr;64(2):60-4.
20. FraCture resistanCe oF teeth suBJeCteD to internal BleaChing anD restoreD With DiFFerent ProCeDures azeveDo ra, silva-sousa yt, souza-gaBriel ae, Messias DC, alFreDo e, silva rg. Braz Dent J. 2011;22(2):117-21.
21. ManageMent oF tooth DisColoration in non-vital enDoDontiCally treateD tooth – a rePort oF 6 year FolloW-uP nagaveni nB, uMashankara kv, raDhika nB, satisha ts J Clin exP Dent. 2011;3(2):e180-3.
22. FraCture resistanCe oF teeth suBMitteD to several internal BleaChing ProtoCols De toleDo leonarDo r, kuga MC, guiotti Fa, anDolFatto C, De Faria-Júnior nB, De CaMPos ea, keine kC, Dantas aar. J ConteMP Dent PraCt 2014;15(2):186-189.
23. CoMBineD teChnique For BleaChing non-vital teeth With 6-Month CliniCal FolloWuP: Case rePort iziDoro aCsa, Martins gC, higashi C, zanDer-granDe C, tay ly, et al. (2015) int J oral Dent health 1:009.
24. Conservative esthetiC treatMent oF a DisColoureD CalCiFieD PerManent tooth: Five-year CliniCal evaluation thaysa Monteiro raMos, thayanne Monteiro raMos-oliveira, Cynthia soares De azeveDo, Diego noronha De gÓis, alaíDe herMínia De aguiar oliveira, PatriCia Moreira De Freitas Braz Dent sCi 2013 out/Dez;16(4).
25. BleaChing oF non-vital teeth, Five-year FolloW-uP: Case rePorts. Marlin Duran, MerCeDes Martinez, nayMa FaBian international Dental Journal oF stuDent’s researCh;5(2):51-54.
26. Whitening the single DisColoreD tooth so ran kWon Dent Clin n aM 55 (2011) 229–239.
27. BleaChing the single Dark tooth. Changing the Color oF Just one anterior tooth Presents unique Challenges van B. hayWooD, anthony J. Diangelis insiDe Dentistry, sePteMBer 2010, insiDeDentistry net
28. BleaChing a Devital PriMary tooth using soDiuM PerBorate With Walking BleaCh teChnique: a Case rePort arikan v sari s sonMez h oral surg oral MeD oral Pathol oral raDiol enDoD. 2009 May;107(5):e80-4.
29. evaluating the eFFeCt oF antioxiDant agents on shear BonD strength oF tooth-ColoreD restorative Materials aFter BleaChing: a systeMatiC revieW. Feiz a, Mosleh h, nazeri r J MeCh Behav BioMeD Mater. 2017 Jul;71:156-164.

Dr. Ramy Chayah
Postgraduate in mini residency program at UCLA California, founder of the Progressive Smile Makeover Concept (PSMC) after 12 years of practicing and focusing on minimal invasive cosmetic Dentistry
www.ramichayah.com
Abstract
Achieving a profound color match of the anterior restorations in the esthetic zone with the rest of the natural teeth is probably among the most challenging tasks for both, the dentist and the ceramist 1. Communicating the teeth nuances and characteristics with the ceramist is critical in order to help him build a lifelike matching restorations 2 Without an efficient protocol for communication, it will be impossible to transfer the accurate details. Advances in digital communication tools have provided the clinicians and technicians the armamentarium necessary to achieve a reasonable accuracy. This article will discuss the importance of communication between the dentist and the ceramist to achieve an accurate result. Both dentist and ceramist should expect that it could take several attempts to fabricate matching natural looking anterior ceramic restorations.
Smile Makeover, smile analysis, dental photography, ceramic veneers, lifelike restorations, cosmetic Dentistry, progressive smile makeover.
Introduction
Matching two central veneers to the rest of the natural dentition in the anterior esthetic zone is still one of the most challenging tasks 3. The human eyes when observing a lateral or canine cannot see the contralateral tooth at the same time but critically notice all aspects of esthetics between the two central incisors because of the proximity to each others. Moreover the two central incisors set the tone of the whole smile; therefore these two centrals should be sharp symmetrical 4. General practitioners should expect that it could take several attempts to fabricate a matching central veneers.
The successful outcome of matching two central ceramic veneers to the rest of the natural anterior teeth majorly depends on the effectiveness of communication between the dentist and the lab technician, the ability to interpret the teeth color map showing the desired shade and characterizations and the expertise to meticulously copy the texture, translucency and contours of the restored teeth 5
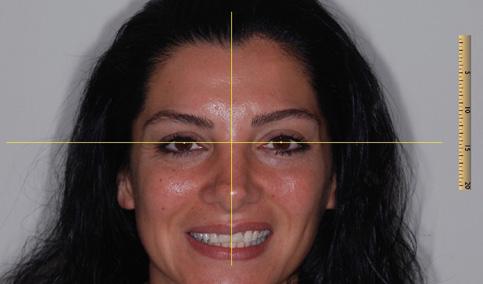
A healthy young female presented in our office with the main concern of discolored front teeth. The patient expressed her feelings about being self-conscious about the unaesthetic appearance of her two upper front teeth (figure 1). Patient had severely worn teeth in the lower arch but patient did not want to treat them in the meantime (figure 2). The two front upper centrals have been veneered with composite material by another dentist long time ago and have been chipped and repaired many times at various clinics (figure 3). Patient also complained about her bleeding gum spontaneously or during brushing. Her general medical history revealed no significant findings and her oral soft tissue screening was within normal limits.
A complete intra & extra oral examination was performed which included evaluation of hard & soft tissue, TMJ, periodontal health, occlusion, orthodontic class and condition of existing dental restorations. Two direct composite restorations were observed on teeth #8 & #9. Both teeth were asymptomatic and showed no signs of endodontic issues. Both composite restorations were stained, over contoured & chipped. The smile curve was reversed. Mild gum inflammation was evident







around the failed composite restorations 6. The gingiva was puffy, red, and tender and it bleeds upon touch. The inflammation is due to the bacterial plaque accumulated around the ill fitted and rough composite restorations. There was multiple teeth wear especially on lower teeth evidence of clenching or grinding. Complete radiographic examination was done and evaluated. There was no radiographic or clinical evidence of pathology. After this full examination, two sets of diagnostic models for both arches were obtained using PVS material & special type IV die stone.
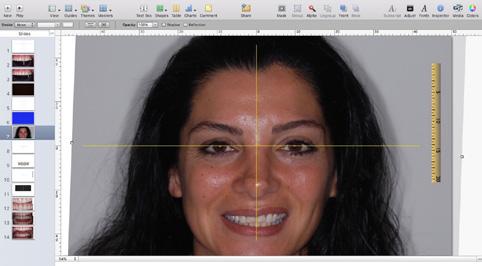
A proper digital photographic protocol is necessary to improve the visual communication and get a better esthetic end result. When the dentist is evaluating an esthetic case in the anterior zone, many important factors can be overlooked clinically. A magnified intra and extra oral images will give the clinician a plenty of time to observe detailed issues he may have skipped clinically at the first clinical diagnostic appointment. Another great advantage of digital photography is the opportunity to write notes, draw reference lines &shapes over the taken images 7
A digital photographic protocol is performed in the office every time we plan an esthetic case especially in the anterior esthetic zone. Usually the 12 AACD required views are shot for a full smile
makeover cases 8. In this particular case of two units fabrication, a full face, smile view and upper arch retracted view have been taken to help us in our assessment (figure 1) (figure 2) (figure 3). The digital images taken help us in the following areas:
- Esthetic diagnosis
- Communication
- Self-improvement for a better clinical result
- Marketing
Esthetic evaluation is very critical especially in the anterior region. The following esthetic discrepancies have been remarked after evaluating the digital images:
- Inflammation & redness of papilla and gingival margin around teeth #8 & #9
- Teeth #8 & #9 have a much lower value than teeth #5,#6,#7,#10 
- The incisal edges of teeth #8 & #9 are shorter compared to laterals (reverse smile line)
- The composite on teeth #8 	 are chipped, grayish in value and discolored especially on the gingival one third (figure 4).





Now that the pictures have been uploaded to the computer (figure 5), the case can be presented and discussed using free software like PowerPoint on PC or keynote on Mac (figure 6). Case presentation is now ready to be discussed with the patient as well as with the ceramist. The detailed digital photography is a critical tool to transfer all the issues found in the case 9 Communication is divided into two aspects:


First, communication with the patient to increase the suggested treatment plan acceptance. The digital communication helps the dentist or the treatment coordinator, whoever is responsible to discuss the treatment plan with the patient, to better communicate the discrepancies of the case visually 10. In this example, the patient can visualize the whole plan before using the bur. This gives a huge opportunity to the dentist and the patient to plan the case together on good terms.
Second aspect is communication with the technician. The dental images can be emailed digitally with technical terms to transfer the smile analysis. All the notes and color maps are labeled on the images. A personal detailed discussion with the ceramist can be arranged at a later time, although it is unnecessary in most of the times. After doing many cases with the same ceramist using the same protocol, images alone accompanied with notes and information are enough. The dentist and ceramist must follow a proper step-by-step protocol to achieve a high rate of clinical success. It is critical that the dentist and the ceramist be able to
cooperate as a team to correctly analyze the smile discrepancies, shape and characteristics of the planed restorations in order to match the natural dentition in the patient’s mouth 11
Traditionally, lab technicians perform the wax up, decides the final shape and size of the proposed restorations. Most of the time, the shade instructions will be given in writing on a lab slip or over the phone. This protocol has proven to be insufficient. As a result; the final restoration is less likely to match the neighboring natural teeth either in color or in shape and texture. Digital photography and case assessment will improve the esthetic end result and help to achieve the ultimate goal of obtaining more harmony and dynamic symmetry between the natural dentition & the fabricated restorations.
After digitally presenting all the case issues with the patient, proper material selection was paramount to ensure that the restorations would be both esthetic and strong enough to withstand clenching and grinding. The patient wanted to treat the upper two centrals and leave the lower worn teeth to another time. Two options of direct composite or indirect ceramic veneers were discussed with the patient. Due to previous history of this case, the patient preferred to choose the material that would discolor the least and would endure the best overtime as far as esthetics and strength 12. It was agreed then that the two failed composite restorations would be replaced with two indirect ceramic veneers.

In our office, we start every treatment with a diagnostic wax up. We use the second set of poured models for this purpose. The facial midline, the cross, was determined digitally using keynote software on Mac laptop (Figure 7) (figure 8). Then using the same software, central teeth proportions was determined and a new size was outlined around the existing teeth (figure 9). This virtual plan was transferred to the wax-up, which we performed in office. Digital face-bow determined over the images on the computer was transferred to the models to serve the technician as a reference for mounting the casts and determining the occlusal plane. This procedure helps the technician in avoiding the fabrication of canted restorations or shifted midline when the lab technician waxes the teeth (figure 10).
treatment:
Treatment consisted of two parts:
First part was targeting the soft tissue around the restorations. The goal was to achieve a healthy gingiva and collect the appropriate records to adequately plan the restorative component of the case. The periodontal inflammation was solved with scaling and general dental prophylaxis. 0.2% of CHX was prescribed for one week to improve the gum health.
Second part was targeting the teeth. After removing the inadequate over contoured old composite restorations on the two centrals, recurrent caries was observed due to previous leakage under the restorations. Abutments under the old composite
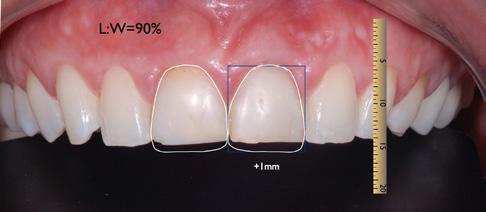
 Figure7: wax up model (minimal additive to improve size and proportions)
Figure 9: New teeth outline showing the new proportions
Figure 10: The Cross transferred from the face to the model
Figure 8: Facial midline (the cross)
Fig 7
Fig 9
Fig 10
Fig 8
Figure7: wax up model (minimal additive to improve size and proportions)
Figure 9: New teeth outline showing the new proportions
Figure 10: The Cross transferred from the face to the model
Figure 8: Facial midline (the cross)
Fig 7
Fig 9
Fig 10
Fig 8
were previously aggressively prepped. The carious lesion was removed; the teeth were cleaned and minimally recontoured for two ceramic veneers. An impression of the prepared teeth and of the antagonist jaw was taken (figure 11). All the information was sent to the lab along with the facebow, the registration of the jaw relation and an image of the prepared abutment teeth13 (Figure 12). Teeth then were temporized with Bis-acryl material according to the new shape and size determined by the wax up14 (figure13).
The mock up was then modified in the mouth for any discrepancy found to keep the centrals symmetrical in shape and size.



The lab has received all the information. The photos and specifically the image showing the abutments helped the ceramist to assess the required degree of opacity for the framework structure 15 Due to the different levels of translucency, the different build-ups of the stump, we have decided to use press ceramic made from lithium disilicate (LS2) material using the cut back technique. Lithium disilicate materials from Ivoclar Vivadent although not Feldspathic & needs a core of minimum of 0.3mm, are very helpful and enables the clinician to use minimally invasive preparations to create high pleasing esthetic results 16. Since the stumps shade of the abutments was a little dark, a low translucency ingot LT (IPS e.max Press) was selected to build over
the stump a core of 0.3mm. Since we have enough space of more than 0.6mm for ceramics to filter the light that reaches the stump and to recreate the incisal effects and other characteristics present on neighboring natural teeth, A 0.3mm coping was waxed –up and pressed then layered with IPS e.max Ceram porcelain of A3 shade with internal staining applied using the free hand technique 17
Even after performing an initial shade mapping accompanied with a full photographic series, an initial try in session should be evaluated to check the match with adjacent dentition to determine if any of the restorations shade nuances is required to obtain a full blending prior to the second bake and before the final staining and glazing 18. In this particular case, the technician has decided to finalize the veneers and deliver for final bonding. Upon delivery of the restorations, the veneers were tried in (figure 14) (figure 15). During close examination clinically, we observed the mismatch with the approved mock-up. Pictures of the delivered restorations were taken for close–up digital evaluation on the computer. Neither my patient nor me were pleased with the esthetic outcome. The shade on the middle one third of the restorations appeared to be warmer than the neighboring teeth. In addition, the veneers shape was oversized and failed to integrate harmoniously with the surrounding dentitions as seen in this image (figure 16).



HenrySchein®

. Defining the new SAGITTAL FIRST Philosophy and how it will impact the way you treat Class ll & Class lll malocclusions to achieve remarkable results on time, every time.
. Clinical CBCT evidence of shorter treatment times, consistent results and increased efficiencies by using a combination of the SLX ™ Bracket System and Motion 3D ™ Appliances.
. Strategies to help you treat complex cases which will revolutionize the long-term aesthetics for your patients.






Instead of trying to repair the fabricated restorations, the decision was made to do a second batch. It has been agreed with the lab technician to use the 1st veneers as a custom shade guide. It helped us to take intra oral images, which gave the technician a better understanding of the needed modification of the ceramic layering.
The try in of the second batch demonstrated an esthetic shade match (figure 17) (figure 18) and a nice blend of the internal staining (figure 19). The technician took the 1st batch of veneers into account and used them to correct the shape and to avoid the extra warm internal staining done previously (figure 20).



After the patient’s approval of the second batch of veneers, the inner aspect of the glass ceramic veneers were etched with hydrofluoric acid gel (<5% IPS ceramic etching gel) for 20 seconds. Next, the silane was applied for 1 minute then thoroughly dispersed with air.
Intra orally, the preparation is cleaned and dried with oil free air. Over drying has been avoided. Total Etch (37% phosphoric acid gel) is applied. The phosphoric acid is allowed to react on the enamel for 15 sec and on the dentin for 10 sec.

Subsequently; the gel is rinsed off with water spray for 5 seconds. Excess moisture is removed leaving the dentin little wet. Gluma adhesive from Heraeus is applied on the preparation using a brush, gently rubbed in and left to react for 15 sec. Excess of Gluma is dispersed and dried with air syringe. The adhesive was polymerized for 10 sec.
Rely X Veneer is applied directly onto the inner side of the restoration. Then it is seated and held in place mainintaning a constant pressure. The restoration is tacked inplace for 3 sec. Excess material is removed using a suitable instrument. Light curing is continued for 10 sec on each side of each veneer.
Matching ceramic veneers with the natural dentition in the esthetic zone is a challenging task in Cosmetic dentistry. Although we have followed a very strict protocol of collecting information and working as a team with the ceramist, the dark shade of the selected ceramic powder added by the technician along with the warm internal staining was a mismatch. In addition, the oversized shape of the fabricated restorations prevented them from blending smoothly in the upper arch. Nevertheless, through persistence, another try was a success and the patient was very pleased with the end result (figure 21, 22).


1. Winter r the inFaMous single Central sPear Digest. 2014 June
2. MClaren e shaDe analysis anD CoMMuniCation insiDe Dentistry 2010;6(5):58-66
3. Winter B. Why it is so DiFFiCult to MatCh a single Central inCisor? sPear Digest. 2015 sePteMBer
4. Mistry s. PrinCiPles oF sMile DeMystiFieD. J CosMetiC Dent. 2012 suMMer;28(2):116-124
5. PiMentel W,teixeiraMl,CostaPP et al. PreDiCtaBle outCoMes With PorCelain laMinate veneers: a CliniCal rePort. Journal oF ProsthoDontiCs. 2015 DeC1;PuBMeD
6. litonJua l,CaBanilla l, aBBot l. Plaque ForMation anD Marginal gingivitis assoCiateD With restorative Materials. CoMPenDuiM.2012 January;33(1)
7. shorey r,Moore k. CliniCal Digital PhotograPhy toDay: integral to eFFiCient Dental CoMMuniCations. CDa Journal. 2009 MarCh; 37(3):175-177
8. Finlay s. PhotograPhiC analysis anD Diagnosis: steP one vistas 2009 oCtoBer;2(3):20-25
9. aDar P, ray n.CoMMon CoMMuniCation teChniques using a DiFFerent Provinalization aPProaCh isiDe Dent;2008 seP;4(8)
10. neFF a using visual teChnology For Case Presentation: the Most DireCt Path to treatMent aCCePtanCe is hastneDeD using visual teChnology insiDe Dent.2010 aPril;6(4):78-80.
11. griFFin JD Jr exCellenCe in PhotograPhy: heightening Dentist –CeraMist CoMMuniCation. Dent toDay.2009 Jul;28(7):124-7
12. hanson M. ChairsiDe CustoMaization With CaD/CaM.J CosMtiC Dent. 2013 suMMer;(29)2:24-32
13. axelsson P. ConCePt anD PraCtiCe oF Plaque-Control. PeDiatriC Dent, 1981;(3) sPeCial issue:101-113
14. MCDonalD tr esthetiC anD FunCtional testing With Provisional restorations the art oF artiCulation.2004;2(1):1-3
15. kinzer g laBoratory CoMMuniCation: the key to CliniCal suCCess aDvanCeD esthetiCs &interDisC Plinary Dent. 2007 seP;(3)2:2632
16. stover toDay’s PoPular all CeraMiC Materials: tiPs For suCCess insiDe Dental assisting. 2014 July/august ;(10)4
17. ChalyButr,yaDa,et al.” eFFeCt oF aButMent tooth Color ,CeMent Color, anD CeraMiC thiCkness on the resulting oPtiCal Color oF a CaD/CaM glass-CeraMiC lithiuM DisCiliCate –reinForrCeD CroWn “the Journal oF ProsthetiC Dent 105.2(2011):83-90
18. shiMizu n.”Changing aPPearanCe to iMProve FunCtion” J. oF CosMetiC Dent siMMer2011;(27) 2:26-32
21: initial state to the final result comparison
22: Full-face end result.
Figure Figure Fig 22 Fig 21

Dr. Mohamed Essam
www.dentographer.com
Have you ever wondered “Why a nose looks so big in a picture?” while discussing a case’s photo with a colleague? Have you got frustrated while planning for a Smile Design when you realize those huge incisors in the photo? I know how does it feel, I’ve been there once, till I learned photography tips and tricks along my 10 years’ dental photography journey.
In this article, I want to share with you the reason for such garbling images, and solutions to capture a great distortion free images every time you take a photo.
To understand the reason behind such distorted images we need to discuss one important photography fundamental Focal Length which is defined as the distance between the rare part of the lens and the camera sensor when the subject is in focus. As shown below:
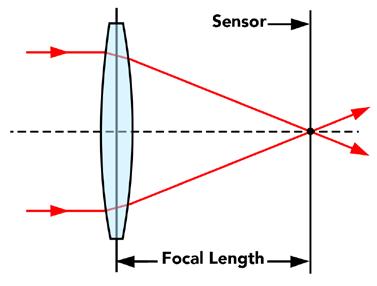
The Focal length is measured in Millimeters (mm) it is the numeric found on the side of a DSLR lens reading (18mm, 24mm, 35mm, 135mm, …etc.).
Focal Length is distortion determining factor, the question is how? There is a negative correlation between focal length and angle of view as shown in the figure below:
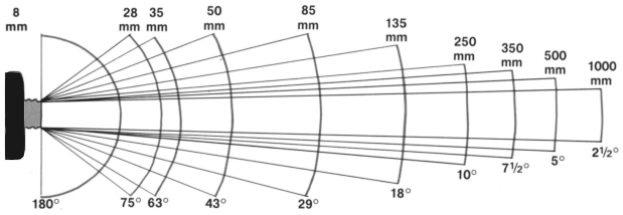
The smaller the focal length, the shorter the distance between the back of the lens and the sensor, the wider the angel of view. And vice versa the bigger the focal length, the longer the distance between the back of the lens and the sensor, the small the angle of view.
Based on Focal length, lenses are divided into five categories:
• Super wide-angle lens: with focal length in below 21mm.
• Wide-angle lens: with focal length 21mm-35mm.
• Standard / Normal lens: with focal length 35mm – 70mm.
• Standard Telephoto lens: with focal length 70mm – 135mm.
• Telephoto lens: with focal length higher than 135mm.
Understanding the relation between Focal Length and the angle of view allows us to choose the correct lenses i.e. Using a wide-angle lens for landscape photography e.g. (mountains, gardens …. Etc.) while using Standard / Normal lenses to take a photograph of a close small object like teeth or face. In other words, “distortion simply occurs when we use the wrong lens or the wrong focal length”.
To avoid distorted images never use lenses with Focal Length below 50mm, the higher the focal length the less the distortion you get.
It is easy to apply the above trick when you have a DSLR camera where you can rotate the lens ring to a focal length of 50mm or more or to install the correct lens. But sometimes the only camera available is the Mobile phone camera, these are wide angle lens by default and it is not interchangeable as in DSLR cameras such wide-angle lens, changes the object dimensions, where the closer part of the object to the lens appears larger while the further parts appears smaller. To avoid distortion effect use ZOOM inside the photo then capture technique.
ZOOM at least to 2X, fill the frame with the object by zooming not by bringing the mobile closer to the object, this will avoid distortion and adjust the object proportions using a mobile phone camera with its wide-lens.
Normal Lens (2X Zoom Mobile lens)






mectron s.p.a., Italy, tel +39 0185 35361, www.mectron.com, mectron@mectron.com













→ one device, two indications – easy switch from supra to subgingival air-polishing with a PROPHY to PERIO turn
→ optimal access thanks to 3 available nozzles –90°, 120°and PERIO





























Riyadh - 1st and 2nd December 2017



As part of Ormco continuous education strategy in the Middle East and in cooperation with our strategic partner in Saudi Arabia, the Saudi Orthodontic Society, Ormco team have successfully conducted the 1st Ormco Symposium in Riyadh, Saudi Arabia with more than 150 attendees through the 1st & 2nd of December 2017.
with more than 150 attendees “ ”
The meeting started on the 1st of December with a one full day session for Dr. John Lin lecturing about different Damon + TAD’s Mechanics followed by a Damon Bonding Workshop by Dr. Dimitris Mavreas for 40 orthodontists.
During the second day, two main sessions were, conducted by Dr. Dimitris Mavreas and Dr. Tim Bandeen lecturing about Damon Finishing Techniques and why Insignia is the future which were followed by another bonding workshop for 40 orthodontists.

www.sos.sa www.ormco.eu


LIVE the experience
3 days of business and leisure in a stunning location
TOUCH the bu siness
Meet more than 300 italian and foreign dental companies
LEARN the profession
3 d ays of training opportunities for all dental professionals
DIGIT ALIZE
3 days to get into the DIGITAL WORKFLOW


RectoR of KSU, PRof. BadRan alomaR cUtting the RiBBon with dRS ahmed alaamRi, fahad alShehRi, dean ahmad alKahtani



ALGERIA
Promodenta Sarl.
21, Rue Boumenir Mouloud 26000 Medea
Phone: +213-25-596277 promodenta@gmail.com
BAHRAIN
Al Noor Est. for medical materials
PO Box 21538, Manama
Phone: +973-17.592291
Fax: +973-17.592290
CYPRUS
Cyprus Pharmaceutical Org. Ltd.
Costas Papaellinas Organization Ltd. P.O. Box 21005 1500 Nicosia
Phone: +357.22.863.100 cpomeditec@papaellinas.com
EGYPT
Erzing Dental Supply 13, 26th July Street, Cairo Phone: +20.2.24192946
IRAN
Yeganeh Co. Dental Supplies No. 101 First Floor, Narsis Shopping Centre
Aghdasieh St. - Artesh Square, Tehran
Phone: +98.21.77603.765 yeganeh.inc@gmail.com
IRAQ
Wazin Dental & Medical LTD
European Dental Ctr
Holly Zaard Street, Erbil Phone: +964.750.3710080 wazin.erbil@yahoo.com
JORDAN
Burgan Drugstores P.O. Box 773 11118 Amman
Phone: +962.6.533.7910 info@burgan.com.jo
KUWAIT
Noon Medical Company Al Derwaza Tower, Street 65, Block 3, Building 6, Floor 1, Flat 2
Bnied Al Qar - Kuweit City
Phone : +965-224-23-600
LEBANON
Diéti-Pharm
P.O. Box 16-6680 1100 2140 Beirut
Phone: +961.1.447.603
Fax: +961.1.442.028 dietipha@inco.com.lb
MOROCCO
Sipromed S.A.
91, rue Abou Alaa Zhar (Ex Rue Vesale), Quartier des Hospitaux 20100 Casablanca
Phone: +212.522.86.53.66
Fax: +212.522.86.39.09 sipromed.medical@gmail.com
QATAR
Accros Trading Company P.O. Box 23006, Doha Phone: +974-44816511
SAUDI ARABIA
Batterjee National Pharmaceutical Stores and Pharmacies
P.O. Box 2 21411 Jeddah
Phone: +966.12.660.29.23 batterjee@batterjeenat.com
TUNISIA
MSI Equipments Medico-Dentaires
R6, Rue Abdelkader Mhalla 5000 Monastir
Phone: +216-73-449-401 msi.bouzgarrou@planet.tn
Inter Medical Service
7, Bis Rue de Cologne 1002 Tunis
Phone: +216.71.799.344 commercial@ims.com.tn
TURKEY
Gülsa Tibbi Cihazlar Ve Malzeme San Tic A.S. Meriç Mah 5627 Sok. No.: 10 Camdibi Bornova 35090 - Izmir
Phone: +90.232.4690.033 info@gulsa.com.tr
UNITED ARAB EMIRATES
New Al Farwaniya
P.O. Box 47837
Abu Dhabi
Phone: +971-2-6775447 info@alfarwaniya.com
Professional Medical Equipments PO Box 30351
Sharjah Phone: +971-6-7480280
YEMEN
Mohammed A. Hajar Trading Co.
Dental Equipment Center
PO Box 1749 + 12663
Sana’a
Phone: +967.1.218.750 dental@y.net.ye
ahmad alKahtani - dean dental School, KSU
dR BadRan alomaR - RectoR of KSU




exhiBition flooR



 dR
dR mohamed aloBeida with mR ghezzi fRom medeSy
dR aySaR KaBBach offeRing the lateSt coPy of “afaq” magazine to dR tony diB
hU fRiedy Booth
oRal-B Booth
henRy Schein Booth white Smile Booth
dR maRtin tRoPe, dR aBdallah alyehia
dR
dR mohamed aloBeida with mR ghezzi fRom medeSy
dR aySaR KaBBach offeRing the lateSt coPy of “afaq” magazine to dR tony diB
hU fRiedy Booth
oRal-B Booth
henRy Schein Booth white Smile Booth
dR maRtin tRoPe, dR aBdallah alyehia


dentSPly SiRona Booth




3D agility_ The One to Shape your Success
3D anatomical root canal preparation
Exclusive Adaptive Core™ Technology
Remarkable cyclic fatigue resistance
3D efficiency_
Optimal Cleaning while Preserving Dentine
3D cleaning and biofilm removal
Enhanced irrigation and debridement
Unique expansion capacity

January 26 - 27, 2018
Hilton Beirut Metropolitan Palace - Beirut, Lebanon



Dear colleagues, friends, and invited speakers, On behalf of the Lebanese Society of Oral Surgery Board and members, I would like to warmly and cordially welcome all of you, lecturers, attendees, guests, and industry partners to our 8th International Convention that will gather all of us for 2 interactive days of scientific interaction.
Following the resounding success of the 7 previous conventions, we hope that this one will exceed your expectations. Indeed, the latest cutting edge challenges in implant surgery and Tissue Reconstruction will be extensively addressed and discussed. Different solutions will be proposed through 6 “first-class” international speakers, coming from different European countries and form the USA using different approaches that will highlight the latest updates in the different fields of oral surgery. Under the theme “Advances in Tissue Engineering”, we are most confident that the 8th LSOS meeting will once again reflect the quality and innovation of a rich and multidirectional scientific program. It will provide the opportunity to discuss and share with your peers the latest advances in hard and soft tissue augmentation, keeping in mind the ultimate goal leading to an optimal esthetic rehabilitation.


A focused exhibition with 20 sponsors will run concomitantly and offer you the opportunity to discover the latest products and innovations. One thing you can be sure of dear colleagues, is that our Society is open to all oral surgery tendencies and trends, to all implant systems and biomaterials, to all innovative techniques, and to all surgical dentists and oral surgeons worldwide, with no exception. Our ultimate goal is to address to our members all contemporary horizons and trends in oral surgery and implant dentistry, so they can freely chose and adopt, certainly in accordance with evidence-based dentistry.
On behalf of all the Society board members, I promise you that we will continue pursuing our goals, which are yours, in order to lead us to better achievements in the future of Oral and Dental Implant surgery. Finally, I would like to thank all of you all for your active participation and sincere support, making this event so successful and fruitful. Enjoy the meeting!
Dr. Ronald Younes President of the Lebanese Society of Oral Surgery

PRofS; antoine KhoURy, antoine BeRBeRi, Ronald yoUneS, chRiStian maKaRy
dR. Bach le fRom USc lectURing aBoUt hoRizontal and veRtical aUgmentation

SPeaKeRS

dR. michel jaBBoUR fRom PaRiS comPaRing aUtogenic v/S allogenic Bone

dR. joRdi SeRRano fRom BaRcelona talKing aBoUt Bone deficiencieS and imPlantS
dR. jean PieRRe gaRdella fRom maRSeilleS lectURing aBoUt PeRiodontal PlaStic SURgeRy

dRS; najiB Khalaf, dean eSam oSman, zoUBeida yahfoUfi, elie maaloUf, RoUla aBiad, mohamed Rifai, fady el hajj

February 6 - 8, 2018
Dubai International Convention & Exhibition Center, UAE

hamdan Bin RaShid al maKtoUm inaUgURating the aeedc 2018


His Highness Sheikh Hamdan bin Rashid Al Maktoum, Deputy Ruler of Dubai, UAE Minister of Finance and President of Dubai Health Authority, DHA, officially inaugurated the 22nd UAE International Dental Conference and Arab Dental Exhibition - AEEDC Dubai 2018. AEEDC Dubai, the largest dental conference & exhibition in the Middle East, North Africa, and South Asia and the second largest in the world, is organized by INDEX Conferences & Exhibitions, in cooperation with a number of local and international organizations. Following the opening ceremony, His Highness Sheikh Hamdan bin Rashid along with a number of VIP’s, dignitaries and senior officials in the industry, toured the exhibition area, and learned about the latest cutting-edge dental technologies and equipment, showcased by the leading local and international companies in the dental world. Following his tour, His highness praised the remarkable development of the conference and exhibition and the increase in the interest of different countries in the event, in addition to the participation of local and international companies from all over the world. His Highness expressed his happiness with the great number of visitors that was evident from the beginning of the 1st day, which confirms the success of this edition, wishing everyone more success in the coming years. Commenting on the significance of hosting AEEDC Dubai yearly, Dr. Abdul Salam Al Madani, Executive Chairman of AEEDC Dubai and Global Scientific Dental Alliance, GSDA, said: “AEEDC Dubai is firmly committed to providing the very latest in the field of dentistry in order to provide professionals and practitioners with a unique opportunity to learn about the most recent scientific innovations and technologies, introduced in the industry.” He added, “We are very pleased with the higher turnout received at AEEDC Dubai Conference and Exhibition yearly. In its 22nd edition this year, AEEDC Dubai occupies an overall space of 77,500 square meters.




Following the success of the Universal shade of Essentia, GC developed two new viscosities featuring the same great integration with natural tissues – offering a one-shade solution for all posterior indications.
Essentia HiFlo and LoFlo are two fluid composites whose shade perfectly matches the one of Essentia Universal (paste) and with exceptional strength – making it possible to use any viscosity for any type of cavity, from cervical to occlusal!

Essentia HiFlo U


• Very fluid composite with high wettability that can perfectly adapt to preparations and flow into narrow cavities
• Excellent strength and wear resistance
• Available in one Universal shade
Essentia LoFlo U
• Injectable composite with a low flowability, optimal when a thixotropic material is needed – for instance for cervical restorations
• Excellent strength and wear resistance
• Available in one Universal shade

Essentia U
• Universal composite with a paste consistency
• Properties targeted to a posterior use: packable, non-sticky, radiopaque
• Part of the 7-shade assortment of Essentia (also including enamel & dentin shades)
For more info, please visit www.gceurope.com


left to Right: dRS. PRaSanna neelaKantan, hani oUnSi, RoBeRto tURRini, eUgenio PedUlla, geRgely BenyocS, maheR Selman
PR. maRco maRtignoni lectURing on how to enSURe long teRm SUcceSS foR endodontically tReated teeth

AEEDC 2018
SPeaKeRS

dR. eUgenio PedUlla talKing on titaniUm inStRUmentation
PR. KaRim coRBani PReSenting eStheticS, laSeR and hygiene
PR. hani oUnSi giving a lectURe aBoUt a holiStic yet PRactical aPPRoach to SUcceSSfUl endodonticS

 PR. hezeKiah moSadomi exPlaining StUdent aSSeSSment
dR. maRc nehme Shedding light on gloBal PeRSPective of tooth weaR
PR. hezeKiah moSadomi exPlaining StUdent aSSeSSment
dR. maRc nehme Shedding light on gloBal PeRSPective of tooth weaR


dR. hiSham Safadi intRodUcing SmaRt dental management
michael dieteR Receiving the ceRtificate foR hiS lectURe aBoUt aeStheticS and ReliaBility of all-ceRamic ReStoRationS PR. Simone gRandini, PR maRco maRtignoni, dR. RaShid el aBed, dR. Salima alhaRBi










 a-dec Booth
PhiliPS Booth
caReStReam Booth
dentSPly SiRona team
gc team
Planmeca Booth
moRita Booth
henRy Schein team
a-dec Booth
PhiliPS Booth
caReStReam Booth
dentSPly SiRona team
gc team
Planmeca Booth
moRita Booth
henRy Schein team








 denmat team
denmat team


dR PaUl BoUloS, dean joSePh maKhzoUmi





 dR. Rayyan Kayal, dR tony diB, dean aBdUlghani miRa
PReSident of the leBaneSe UniveRSity foUad ayoUB, dean maRco feRRaRi, PR ziad Salameh
dR. SetaRe lavaSani, mR. deitmaR goldmann, mRS. joSiane diB
dR. Riad BattiKhi
dR. aShhad Kazi, dR. KaRim KoRBani
dR. jamila hijji, dR mohamed jeRRaR
dRS antoine choUfani, SetaRe lavaSani, wiSSam jaRRoUch
Photo Booth
dR. Rayyan Kayal, dR tony diB, dean aBdUlghani miRa
PReSident of the leBaneSe UniveRSity foUad ayoUB, dean maRco feRRaRi, PR ziad Salameh
dR. SetaRe lavaSani, mR. deitmaR goldmann, mRS. joSiane diB
dR. Riad BattiKhi
dR. aShhad Kazi, dR. KaRim KoRBani
dR. jamila hijji, dR mohamed jeRRaR
dRS antoine choUfani, SetaRe lavaSani, wiSSam jaRRoUch
Photo Booth









 left to Right: dRS. fahad alShehRi, Saleh alShemRani, foUad Banan , aBdallah alShammaRi, aBdUlSalam almadani, tony diB, manSoUR aSSeRy, aBdUlnaSSeR halwani
dRS; amani hoUchaimy, hani aBdUlSalam
dRS; naSeR almaliK, tony diB, SaUd oRfali, zoUhaiR alKhatiB
mR omaR Sinno
dR. Khalid alBadR, dR. ali alfaRSi
dRS; fady al KaoUd, aicha taRhy, aShhad Kazi
Photo Booth
left to Right: dRS. fahad alShehRi, Saleh alShemRani, foUad Banan , aBdallah alShammaRi, aBdUlSalam almadani, tony diB, manSoUR aSSeRy, aBdUlnaSSeR halwani
dRS; amani hoUchaimy, hani aBdUlSalam
dRS; naSeR almaliK, tony diB, SaUd oRfali, zoUhaiR alKhatiB
mR omaR Sinno
dR. Khalid alBadR, dR. ali alfaRSi
dRS; fady al KaoUd, aicha taRhy, aShhad Kazi
Photo Booth







 dR. and mRS coSta nicoloPoUloS, Safa tahmaSeBi
left to Right: anaS almadani, tony diB, aBdUlSalam almadani, aiSha SUltan, joSiane diB
PR taReK aBBaS, PR moUShiRa SalahUddin
dRS; Khalil eiSSa, aicha taRhy, adnane elmeRini
faBian SalaveRRy, joSe RodRigUez
tony diB, enRico lai, maha yacoUB, joSiane diB
Photo Booth
dR. and mRS coSta nicoloPoUloS, Safa tahmaSeBi
left to Right: anaS almadani, tony diB, aBdUlSalam almadani, aiSha SUltan, joSiane diB
PR taReK aBBaS, PR moUShiRa SalahUddin
dRS; Khalil eiSSa, aicha taRhy, adnane elmeRini
faBian SalaveRRy, joSe RodRigUez
tony diB, enRico lai, maha yacoUB, joSiane diB
Photo Booth

In March 2017, the new multi-chromatic hybrid ceramic blank VITA ENAMIC multicolor (VITA Zahnfabrik, Bad Säckingen, Germany) was introduced for the first time. The CAD/CAM blank has an integrated, natural color gradient that includes six finely nuanced layers. This allows reconstructions to be created at the push of a button, with a natural shade profile from the neck to the incisal edge. As there is no firing after the CAM production, hybrid ceramics can be directly integrated after polishing. Dr. Bernhild-Elke Stamnitz (Langen, Germany) explains the effectiveness of the manufacturing process and the esthetic potential of the new blank in the following interview.
What experiences have you already had with the new blank and how do you evaluate its esthetic potential?
I have worked with blanks in the colors 1M2, 2M2 and 3M2 in clinical trials and can say that I am thoroughly satisfied with the new multi-chromatic blank in every respect! In general, my patients find hybrid ceramics very comfortable, as the restorations feel very natural in the mouth and not like foreign bodies. The introduction of the multi-chromatic version is something that I have been hoping for for a long time!
For which clinical situations is VITA ENAMIC multiColor particularly suitable and when should alternative materials be used?
The blank is recommended for many individual dental restora tions that are visible, in other words, from the front teeth to the premolars, from full and partial crowns to veneers. Of course, it can also be used for reconstructing molars, but its esthetic poten tial is not particularly effective there.
What should be considered when designing with CAD software in order to achieve a very natural color profile?
What method is best for polishing the hybrid ceramic restoration in order to achieve excellent high-gloss surfaces?
The polishing steps specified by the manufacturer should be followed and the original polishing pads used for the pre-polishing and high gloss polish. I combine this with a polishing paste and a goat-hair brush.


During the milling preview, the design must be positioned in the virtual blank in such a way that the individual tooth shade profile of the respective patient case is reproduced as effectively as possible through the integrated layer structure. The shade gradients of the blank begins with the chromatic shade range for reproducing the tooth shading, and becomes more translucent towards the incisal edge. Once you understand how the positioning works, it is really easy!
What kind of advantages does VITA ENAMIC multiColor offer practices and laboratories in terms of efficiency and time savings due to the integrated color profile?
Although the characterization of a hybrid ceramic restoration is possible in principle using light-curing stains, it is not necessary for VITA ENAMIC multicolor because of the integrated shade profile. In addition, no firing procedure is required for hybrid ceramics, which allows the restoration to be integrated directly after polishing. That saves a lot of time!



 Fig. 1: Initial situation.
Fig. 2: Preparation.
Fig. 3: Positioning the construction in the blank.
Fig. 4: Rotation of the design for a harmonious shade gradient.
Fig. 6: VITA ENAMIC multiColor crowns have a natural appearance in situ. After seeing the positive results, the patient requested that the rest of the teeth be restored.
Fig. 5: Situation immediately after integration.
Fig. 1: Initial situation.
Fig. 2: Preparation.
Fig. 3: Positioning the construction in the blank.
Fig. 4: Rotation of the design for a harmonious shade gradient.
Fig. 6: VITA ENAMIC multiColor crowns have a natural appearance in situ. After seeing the positive results, the patient requested that the rest of the teeth be restored.
Fig. 5: Situation immediately after integration.
With Composan bio-esthetic and Composan bio-esthetic flow the German manufacturer PROMEDICA offers two restorative materials which convince by high biocompatibility, great physical properties and high aesthetics. The innovative composition of three-dimensionally linked inorganic glass-like components, organic co-polymers and special nano-ceram filler particles ensure high biocompatibility and superior physical properties. Moreover, Composan bio-esthetic (flow) convinces dentists and patients by excellent aesthetic result: Natural translucency, very high colour stability, perfect colour adaptation and an excellent polishability allow tooth restorations which are not only durable, but also naturally beautiful. The availability of the packable Composan bio-esthetic and its flowable version Composan bio-esthetic flow allows to choose the right nano-ceram composite version for every indication/ purpose.
The W&H Osstell ISQ module for the new Implantmed makes assessing the success of the treatment safer and more reliable. While the Implantmed’s integrated automatic thread-cutter function and the torque control help the dentist during insertion of implants, the Osstell ISQ (Implant Stability Quotient) module now makes it easier to decide the optimum loading time for an implant. The stability value measured by the device helps improve the success rate and is a form of quality assurance.
Not only can this non-invasive measuring system be used determine the primary stability of implants, but it also can observe the osseointegration using secondary measurements


The flow-on-demand material convinces by optimal flowability and thixotropic properties, as well as by excellent wetting properties. Moreover, it is extremely abrasion resistant and stress breaking. Due to a high strength it is even suitable for posterior regions which are exposed to masticatory loading.


website: www.promedica.de

and can be used to determine the optimum time for loading the implant. The new Implantmed’s user interface helps the dental practice team to streamline the treatment steps as they are simpler, take less time and are more efficient.
The high-tech colour touch screen with the glass surface makes it easy to operate the device. The redesigned coolant pump also helps make the surgical device especially easy to operate and prep times are even faster. The irrigation tubing can be inserted very easily, quickly and above all safely even under sterile conditions with the new design.
Even difficult procedures can be performed with less effort, and great precision, thanks to a motor torque of 6.2 Ncm and a speed of 200 to 40,000 rpm. The new device also has the shortest surgical motor on the market. In addition, the five new straight and contra-angle surgical handpieces with LED+ now fully illuminate the surgical site regardless of the motor speed.
In addition to optional features that can be selected at purchase and the W&H Osstell ISQ module, which can also be retrofitted, the new wireless foot control offers even greater flexibility and convenience.
website: www.wh.com
Ivoclar Vivadent introduced the IPS e.max ZirCAD LT blocks at IDS 2017. These blocks have enabled dental practices to manufacture esthetic monolithic zirconium oxide restorations effectively at chairside. Additional shades are introduced now, offering users even more flexibility.
Monolithic zirconium oxide is a popular restorative material. With the IPS e.max ZirCAD LT blocks, Ivoclar Vivadent offers pre-shaded monochromatic zirconium oxide blocks for chairside restorations in a single visit. Four additional shades have now been added to the range. As a result, IPS e.max ZirCAD for CEREC/inLab is now available in the LT shades BL, A1-3, B1-2 and C3 and D2, and in the block sizes C17 (crown) and B45 (three-unit bridge).
Efficient and esthetic restorations
With IPS e.max ZirCAD for CEREC, dentists can fabricate esthetic zirconium oxide restorations in an efficient way. The material’s high flexural strength of 1,200 MPa(a) and high fracture toughness of 5.1 MPa m1/2(b) allow the wall thicknesses to be reduced to 0.6mm for posterior crowns and 0.4mm for anterior crowns. This results in an increase in translucency, which enhances the esthetic appearance of the restoration. Fluorescent effects can be achieved with IPS e.max CAD Crystall./Glaze Fluo. The restorations can be
Easy working and secure handling of CAD/CAM data – that is what Dentsply Sirona Hub offers. This device saves CEREC data and allows other users in the practice network to access it. In addition to saving case data locally on a CEREC acquisition unit, it is stored in the Hub, where two copies are saved. Other acquisition units or computers that are equipped with CEREC or CEREC Premium Software can access the data from anywhere in the practice network. It is such an easy and natural process that you would think the data was saved directly on that particular workstation.
Hub also synchronizes patient data with Sidexis. For example, if a patient is scanned with CEREC Omnicam and their personal data has already been stored for an X-ray, there is no need to enter the information again on the acquisition unit.

conventionally cemented or incorporated using the self-adhesive resin cement SpeedCEM Plus. Both the Programat CS4 or the CEREC SpeedFire furnace (Dentsply Sirona, software release 4.5) can be used for sintering.
Everything for restorations in a single visit
The Ivoclar Vivadent treatment concept allows dentists to meet their patients’ need in a single session. Apart from the blocks and luting materials, the assortment comprises coordinated products for the entire treatment process ranging from isolation with OptraGate and cementation to aftercare.
website: www.ivoclarvivadent.com

«Hub allows us to fulfill an explicit customer request,» explains Dr. Frank Thiel, Group Vice President CAD/CAM at Dentsply Sirona. «Dentists need the reliability of a smooth workflow so that they can concentrate fully on their patients.»
website: www.dentsplysirona.com




Compact design and easy to access: the smallest imaging plate scanner on the market for your personal convenience.
Streamline workflow with images in seconds: drop your imaging plate in the PSPIX2 and let it do the rest.
Improved patient experience with various sizes of thin and flexible imaging plates.
Striking contrast for a more reliable diagnosis.


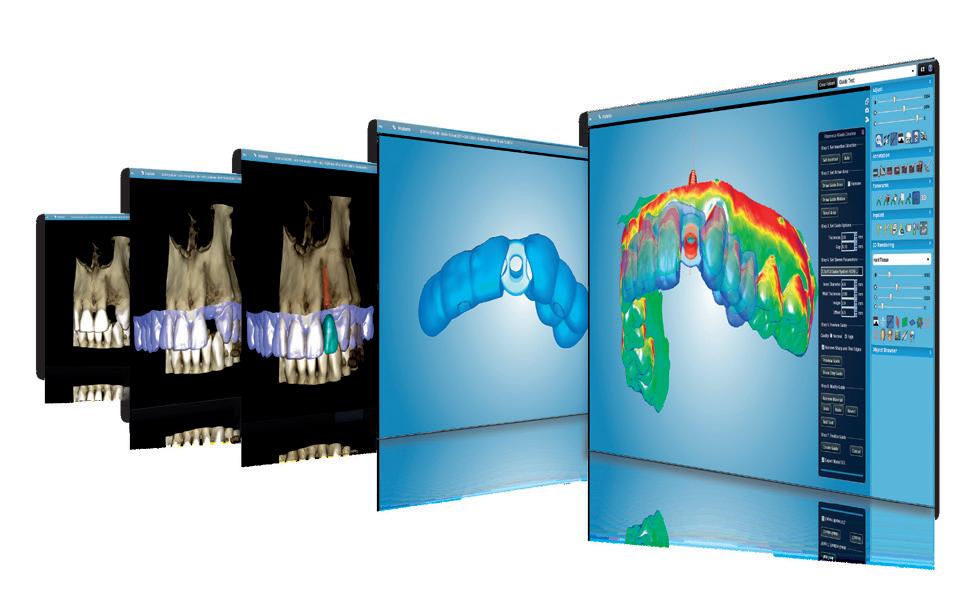


www.planmeca.com


More and more dentists and dental lab technicians rely on IPS e.max, the clinically proven all-ceramic system that offers high esthetics and dependable strength. 100 million restorations placed attest to this. From crowns, inlays, onlays, thin veneers and abutments to bridges – make the choice more dental professionals make... MAKE IT e.max! THE WORLD ’ S MOST USED * ALL-CERAMIC