T H I S D AY THURSDAY, APRIL 20, 2017
38
HEALTH
HEALTH MATTERS
goketakinrogunde@gmail.com
By Goke T. Akinrogunde 07036777348; 07029126776
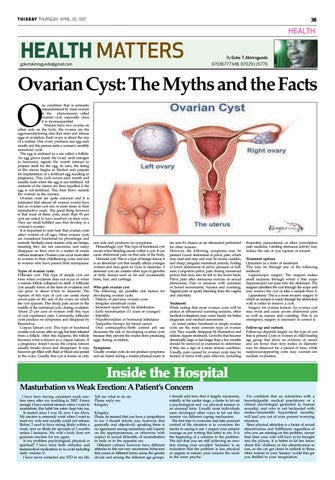
Ovarian Cyst: The Myths and the Facts
O
ne condition that is seriously misunderstood by most women is the phenomenon called ovarian cyst, especially since it is inconsequential. Women have two ovaries on either side on the body, the ovaries are the egg-manufacturing sites that store and release eggs at ovulation. Each ovary is about the size of a walnut. One ovary produces one egg each month, and this process starts a woman’s monthly menstrual cycle. The egg is enclosed in a sac called a follicle. An egg grows inside the ovary until estrogen (a hormone), signals the womb (uterus) to prepare itself for the egg. In turn, the lining of the uterus begins to thicken and prepare for implantation of a fertilized egg resulting in pregnancy. This cycle occurs each month and usually ends when the egg is not fertilized. All contents of the uterus are then expelled if the egg is not fertilized. This then flows outside the woman as the menses. Ovarian cysts are quite common and it is estimated that almost all women would have had an ovarian cyst one or more times in their reproductive years. The good thing however is that most of these cysts, more than 95 per cent are noted to have resolved on their own. They are small fulfilled sacs that develop in a woman’s ovaries. It is important to note here that ovarian cysts affect women of all ages. Most ovarian cysts are considered functional (or physiologic and normal). Similarly, most ovarian cysts are benign, meaning they are not cancerous, and many disappear on their own in a matter of weeks without treatment. Ovarian cysts occur most often in women in their childbearing years and less in women who have passed their menopause. Types of ovarian cysts: Follicular cyst: This type of simple cyst can form when ovulation does not occur or when a mature follicle collapsed on itself. A follicular cyst usually forms at the time of ovulation and can grow to about 4.5cm in diameter. The rupture of this type of cyst can create sharp severe pain on the side of the ovary on which the cyst appears. This sharp pain occurs in the middle of the menstrual cycle, during ovulation. About 25 per cent of women with this type of cyst experience pain. Commonly, follicular cysts produce no symptoms and disappear by themselves. Corpus luteum cyst: This type of functional ovarian cyst occurs after an egg has been released from a follicle. After this happens, the follicle becomes what is known as a corpus luteum. If a pregnancy doesn’t occur, the corpus luteum usually breaks down and disappears. It may however get filled with fluid or blood and persist in the ovary. Usually, this cyst is found on only
one side and produces no symptoms. Hemorrhagic cyst: This type of functional cyst occurs when bleeding occurs within a cyst. It can cause abdominal pain on that side of the body. Dermoid cyst: This is a type of benign tumor, it is an abnormal cyst that usually affects younger women and may grow to 12cm in diameter. A dermoid cyst can contain other type of growths of body tissues such as fat and occasionally bone, hair, and cartilage. Who gets ovarian cyst The following are possible risk factors for developing ovarian cysts: · History of previous ovarian cysts · Irregular menstrual cycles · Increased upper body fat distribution · Early menstruation (11 years or younger) · Infertility · Hypothyroidism or hormonal imbalance · Tamoxifen therapy for breast cancer Oral contraceptive/birth control pill use decreases the risk of developing ovarian cysts because they prevent the ovaries from producing eggs during ovulation. Symptoms Usually ovarian cysts do not produce symptoms and are found during a routine physical exam or
are seen by chance on an ultrasound performed for other reasons. However, the following symptoms may be present: Lower abdominal or pelvic pain, which may start and stop and may be severe, sudden, and sharp; Irregular menstrual periods; Feeling of lower abdominal or pelvic pressure or fullness; Long-term pelvic pain during menstrual period that may also be felt in the lower back; Pelvic pain after strenuous exercise or sexual intercourse; Pain or pressure with urination or bowel movements, Nausea and vomiting; Vaginal pain or spotty bleeding from the vagina and infertility. Treatment While noting that most ovarian cysts will be picked at ultrasound scanning sessions, other medical evaluations may come handy for better diagnosis and medical assessment. As noted earlier, functional or simple ovarian cysts are the most common type of ovarian cyst. They usually disappear by themselves and seldom require treatment. Growths that become abnormally large or last longer than a few months should be removed or examined to determine if they are a sign of a more serious condition. Usually, pain caused by ovarian cysts may be treated at home with pain relievers, including
ibuprofen, paracetamol, or other prescription pain medicine. Limiting strenuous activity may reduce the risk of cyst rupture or torsion. Treatment options Operation as a form of treatment This may be through any of the following methods: Laparoscopic surgery: The surgeon makes small incisions through which a thin scope (laparoscope) can pass into the abdomen. The surgeon identifies the cyst through the scope and may remove the cyst or take a sample from it. Laparotomy: This is a more invasive surgery in which an incision is made through the abdominal wall in order to remove a cyst. Surgery for ovarian torsion: An ovarian cyst may twist and cause severe abdominal pain as well as nausea and vomiting. This is an emergency, surgery is necessary to correct it. Follow-up and outlook Follow-up depends largely on the type of cyst that is present. Cysts in women in child bearing age group that show no evidence of cancer and are fewer than 6cm inches in diameter may be observed for a period of time, while suspicious-appearing cysts may warrant immediate evaluation.
Inside the Hospital Masturbation vs Weak Erection: A Patient’s Concern I have been having consistent weak erection since after my wedding in 2007. Funny enough I have normal erection when I want to masturbate, this habit has eaten deep into me. It started since I was 18, now I am 43yrs. My erection is extremely weak when I want to meet my wife and usually could not release. Before, I used to have strong libido within a week, now no libido for upwards of 2 months unless I fantasize. My wife’s body does not generate erection for me again. Is my problem psychological, physical or spiritual? I have tried both orthodox and tradomedical medications to no avail including daily vitamin E. I have never contacted any STD in my life.
Tell me what to do sir. Please reply me. Kingsley Kingsley, Please, be assured that you have a sympathizer in me. I should inform you, however, that generally and objectively speaking there is no agreement among researchers and experts on the appropriateness, or otherwise with respect to sexual ill-health, of masturbation in male or in the opposite sex. Different cultures however have different attitudes to this not very uncommon behaviour that comes in different forms across the gender divide and among the different age groups.
I should add here that it largely represents, initially at the earlier stage, a desire to let out a psychological and /or physical tension in an unusual form. Usually most individuals soon developed other ways to let out this tension via different coping mechanism. The first step to overcome and take personal control of the situation is to overcome the inertia to saying it out. I respect your present courage as per writing this letter to me. It is the beginning of a solution to the problem. The fact that you are still achieving an erection during your so-called ‘fantasies’ is an indication that the problem is less physical or organic in nature; your concern lies more in the inner psyche.
I’m confident that an interaction with a knowledgeable medical practitioner or a clinical psychologist grounded in human sexuality, and who is not beclouded with undue/unscientific hypocritical morality, will lead you out of your present worrying situation. Since physical attraction is a factor of sexual attractiveness and fulfillment, regardless of who you are meeting on this problem, sooner than later your wife will have to be brought into the picture, it is better to let her know about this ‘dullness in her attractiveness to you, so she can get closer in outlook to those other women in your ‘fantasy’ world that get you thrilled in your imagination.