13 minute read
Wellbeing


Talking Dentistry
This month we’re talking restorative dentistry with Dr Andrew See who combines passion, artistic flare and extensive knowledge of dentistry to answer any questions you may have. He has advanced training in aesthetic and implant dentistry.
Advertisement
Reader’s question: “I’m in my 30s and still have a baby tooth! It’s smaller than my other teeth and is becoming painful, what can be done?”
Dr See says: Great question. A baby tooth retained in adulthood is largely due to congenitally missing adult teeth. The prevalence of congenitally missing adult teeth or hypodontia is around 2.2% of the population. The cause of it is largely unknown. The mandibular (lower) second premolars are the most frequently missing teeth. The baby tooth that is retained often becomes a problem due to it becoming ankylosed and fused to the bone. Often these teeth are hard to clean because they sit so much lower than the adult adjacent teeth. These cases can have festering decay underneath, eating away the tooth and jaw bone like termites. Baby teeth can remain, if they don’t affect the bite position or have active decay. If the tooth is unviable, patients have the option for it to be removed and replaced with a denture, bridge or dental implant.


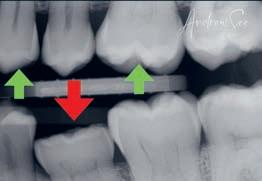
Let’s look at a recent case that we completed with the removal of the baby tooth and replacement with a dental implant. Kristy came to see us because she was experiencing pain in her lower tooth which was a baby tooth and had remained into adulthood. It was ankylosed and lower than the adjacent teeth. It also had a previous filling placed on top of it to build it up into the bite. After further investigation, we discovered it had deep decay and irrational to treat prognosis. She didn’t want a gap in her teeth after extraction and decided to have it replaced with a fixed dental implant. The porcelain crown was made to a normal adult sized tooth to match her bite position and smile line.

THE PROBLEMS:
• Baby tooth present • Painful • Deep decay and infection
THE SOLUTION:
• Removal of infected baby tooth that had hopeless prognosis • Extraction, bone grafting and implant placement • Adult sized porcelain implant crown to match bite position and smile line
Advanced qualifications and experience ensured that we achieved the results that Kristy wanted. Visit www.advanceddentistrysydney.com.au/implants for more information.
** Any surgical or invasive procedure caries risk. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner **
If you have any questions you have always wanted to know about aesthetic or implant dentistry, write to us at info@advanceddentistrysydney.com.au

9816 4885 dr.andrewsee advanceddentistrysydney.com.au DR ANDREW SEE

BDS Hons (Syd), FRACDS, MSc(Lond), PGDipDentImplantology, MFGDP(UK), FICOI, MFDS RCSEng
HOW ARE WE DIFFERENT?
Dr Andrew See has dedicated the last 19 years to Aesthetic Dentistry and has unique qualifications in cosmetic dentistry and rehabilitation.
This includes a three year Masters in Aesthetic Dentistry from the prestigious King’s College London and a Postgraduate Diploma in Dental Implantology.
Dr See completed his Fellowship by primary and secondary examinations for The Royal Australasian College of Dental Surgeons (FRACDS). FRACDS is the mark of professional achievement in dentistry and demonstrates attainment of an advanced level and skill in Dentistry.

If you have any questions you have always wanted to know about aesthetic or implant dentistry write to us at: info@ advanceddentistrysydney. com.au
When bad news arrives
BY DR CARL WONG
DR CARL WONG IS A LANE COVE-BASED GP AND SITS ON THE BOARD OF SYDNEY COMMUNITY SERVICES

There is no easy way to receive bad news about your health. As a doctor, I know this all too well. Sadly as much as I love it not to be true, there is also no easy way for doctors to break bad news to their patients either. The challenging thing about bad news is that it is subjective. In other words, bad news has different meanings and significance for each and every person. What is significantly bad news to one person may not be as significant for another person. This is affected by a number of factors including how expected (or unexpected) the news was, the person’s prior understanding of the new information, social and family circumstances, and by one’s cultural and religious beliefs. It may come by way of a terminal diagnosis or a diagnosis that will have a significant impact on one’s livelihood (such as a career-ending injury). It could be for a woman with infertility issues or a genetic abnormality in a child. What makes it even more challenging is the variety of emotional reactions associated with the receiving of bad news.
The ‘five stages of grief’ model was first developed by psychiatrist Elisabeth Kübler-Ross in 1969, to describe those facing death due to terminal illness. This has since been adapted to thinking about bad news and grief in general. They are all natural responses, usually occur in order but not always so, and the stages may overlap with one another: • Denial – often the first response, where one is in a state of shock and denial. It is a defense and coping mechanism to help us handle and to allow time to process the news. • Anger - can be towards oneself, someone else, something else, or even lost opportunities and the life changes that are to come.



• Bargaining – by trying to make deals and do something different to change the present circumstances. Asking oneself ‘what if I changed my life now this way…’ or ‘only if I had done this….’. This is often accompanied by guilt, trying to find fault in oneself and how we think we could have done things differently. • Depression – for many, life can lose meaning and all joy is lost; sleep, appetite, and previous enjoyable pursuits all can be affected. Self-harm and suicidal thoughts can also occur. It can also lead to destructive behaviour such as excessive alcohol intake to cope.
• Acceptance – finally acknowledging and accepting the news, learning to live with and adjusting one’s life accordingly. There is no standard ideal best way to receive bad news, which can be very different for each person. Some receive the news with stunned silence, some with outward emotion and distraught whilst others may have lots of questions.
Here is my general advice to you when it’s comes to receiving and accepting bad news: 1. Bring a family member or trusted friend with you to the
consultation, if you have forewarning or a ‘sixth sense’ that the news you will be receiving from your doctor may not be good. They will be able to provide you with emotional support and also help you remember things later that you may forget. 2.Keep it as clear as possible. Studies have shown that patients are best looked after when the language from their doctor is clear and honest but also sensitive to their individual needs. There is no one-size-that-fits-all approach. Guide your doctor as to the amount and level of information provided is right for you at this time.
3.Ask questions. Do not be afraid to ask your doctor to repeat or explain something that you don’t fully understand. Doctors use lots of medical jargon words (it’s been estimated that they pick up approximately 35,000 new medical words during their professional career!).
4.Take your time. You may want to find out about relevant information such as treatment options, quality of life effects, prognosis and life expectancy. This does not have to all occur in the one consultation, and it can scheduled for another visit so you don’t get ‘information overload’.
5.Seeing a psychologist can help you with the swirling emotions that come with it all.
6.Be wary of doing your own internet searches as it may lead to incorrect information which may worsen your worries. Ask for written material or reputable websites for facts that you can read later. Go to reputable relevant internet sources such as the Cancer Council or the Heart Foundation of Australia.
7. Explore your personal wishes and goals. Moving forward, what is most important to you?
These conversations are never easy, but the aim is for you to feel as informed, supported and hopeful for the future as much as possible by the end.
Are you living with, or worried about, someone suffering with BACK PAIN?’
If that is you or a loved one, it’s time to request our FREE report. We have detailed what could be the real solution to your pain that you have been looking for - a solution that could help you or a loved one keep active, maintain independence and avoid having to take painkillers. In this report we detail:

• Discover the secret to being able to walk further for longer with much less backache! • The single biggest back pain mistake everyone makes each and every day and how to avoid it • The changes you can make in the bedroom to get a better night’s sleep • A simple remedy for easing back pain which will cost you nothing - perfect to stay active and mobile • Discover how to move more freely and improve posture with some tips you can do in the comfort of your home • If you are currently held back and restricted from things like: • Getting a good night’s sleep, being able to work, walking with friends, playing golf or enjoying time with the grandkids then this easy reading report “How to end Back pain and Stiffness” will help you.
Request your FREE copy of “How to end Back Pain and Stiffness” by calling 9427 8333 or emailing lanecove@weareswitch.com.au

Burns Bay Physiotherapy 9427 8333
161 Burns Bay Rd, Lane Cove E: info@burnsbayphysiotherapy.com.au www.burnsbayphysiotherapy.com.au
James Becerra Harrison Brown
Wearing shoes in the house is just plain gross:
the verdict from scientists who study indoor contaminants

WORDS:
MARK PATRICK TAYLOR (Chief Environmental Scientist, EPA Victoria; Honorary Professor, Macquarie University)
GABRIEL FILIPPELLI
(Chancellor's Professor of Earth Sciences and Executive Director, Indiana University Environmental Resilience Institute, IUPUI)
You probably clean your shoes if you step in something muddy or disgusting (please pick up after your dog!). But when you get home, do you always de-shoe at the door?
Plenty of Australians don’t. For many, what you drag in on the bottom of your shoes is the last thing on the mind as one gets home. We are environmental chemists who have spent a decade examining the indoor environment and the contaminants people are exposed to in their own homes. Although our examination of the indoor environment, via our DustSafe program, is far from complete, on the question of whether to shoe or de-shoe in the home, the science leans toward the latter.
It is best to leave your filth outside the door.
What contaminants are in your home, and how did they get there?
People spend up to 90% of their time indoors, so the question of whether or not to wear shoes in the house is not a trivial one. The policy focus is typically on the outdoor environment for soil, air quality and environmental public health risks. However, there is growing regulatory interest in the question of indoor air quality.
The matter building up inside your home includes not just dust and dirt from people and pets shedding hair and skin.
About a third of it is from outside, either blown in or tramped in on those offensive shoe bottoms.
Some of the microorganisms present on shoes and floors are drug-resistant pathogens, including hospitalassociated infectious agents (germs) that are very difficult to treat.
Add in cancer-causing toxins from asphalt road residue and endocrinedisrupting lawn chemicals, and you might view the filth on your shoes in a new light.
A roll-call of indoor nasties
Our work has involved the measurement and assessment of exposure to a range of harmful substances found inside homes including: • antibiotic-resistant genes (genes that make bacteria resistant to antibiotics)
• disinfectant chemicals in the home environment
• microplastics
• the perfluorinated chemicals (also known as PFAS or “forever chemicals” because of their tendency to remain in the body and not break down) used ubiquitously in a multitude of industrial, domestic and food packaging products
• radioactive elements
A strong focus of our work has involved assessing levels of potentially

It is best to leave your filth outside the door. Shutterstock Why walk muck around inside your house if you have a very simple alternative – to take your shoes off at the door? Shutterstock

Please don’t do this. Shutterstock

toxic metals (such as arsenic, cadmium and lead) inside homes across 35 nations (including Australia). These contaminants – and most importantly the dangerous neurotoxin lead – are odourless and colourless. So there is no way of knowing whether the dangers of lead exposure are only in your soils or your water pipes, or if they are also on your living room floor. The science suggests a very strong connection between the lead inside your home and that in your yard soil. The most likely reason for this connection is dirt blown in from your yard or trodden in on your shoes, and on the furry paws of your adorable pets.
This connection speaks to the priority of making sure matter from your outdoor environment stays exactly there (we have tips here). A recent Wall Street Journal article argued shoes in the home aren’t so bad. The author made the point that E. coli – dangerous bacteria that develop in the intestines of many mammals, including humans – is so widely distributed that it’s pretty much everywhere. So it should be no surprise it can be swabbed on shoe bottoms (96% of shoe bottoms, as the article pointed out). But let’s be clear. Although it’s nice to be scientific and stick with the term E. coli, this stuff is, put more simply, the bacteria associated with poo. Whether it is ours or Fido’s, it has the potential to make us very sick if we are exposed at high levels. And let’s face it – it is just plain gross. Why walk it around inside your house if you have a very simple alternative – to take your shoes off at the door? On balance, shoeless wins
So are there disadvantages to having a shoe-free household?
Beyond the occasional stubbed toe, from an environmental health standpoint there aren’t many downsides to having a shoe-free house. Leaving your shoes at the entry mat also leaves potentially harmful pathogens there as well. We all know prevention is far better than treatment and taking shoes off at the door is a basic and easy prevention activity for many of us. Need shoes for foot support? Easy – just have some “indoor shoes” that never get worn outside. There remains the issue of the “sterile house syndrome,” which refers to increased rates of allergies among children. Some argue it’s related to overly sterile households. Indeed, some dirt is probably beneficial as studies have indicated it helps develop your immune system and reduce allergy risk. But there are better and less gross ways to do that than walking around inside with your filthy shoes on. Get outside, go for a bushwalk, enjoy the great outdoors. Just don’t bring the muckier parts of it inside to build up and contaminate our homes.




