HIMSS23 Chicago
Reimagining health

ROBOTIC SURGERY | CLIMATE CHANGE SOLUTIONS | VIRTUAL WARDS | THE METAVERSE
Nine | April 2023 LEADING THE DEBATE IN INTERNATIONAL HEALTHCARE & LIFE SCIENCES
Issue

 Vincent Buscemi Partner and Head of Independent Health
Vincent Buscemi Partner and Head of Independent Health

vincent.buscemi@bevanbrittan.com
Letitia Winterflood-Blood Senior Associateletitia.winterflood-blood@bevanbrittan.com
 Jodie Sinclair Senior Partner Employment, Immigration and Pensions
Jodie Sinclair Senior Partner Employment, Immigration and Pensions





jodie.sinclair@bevanbrittan.com


Bevan Brittan is the market-leader in the provision of legal, governance and regulatory advisory services to businesses delivering and providing healthcare services within the UK and internationally. Our award-winning healthcare teams provide organisations with outstanding corporate, commercial, clinical negligence, litigation, regulatory, property and employment legal advice.

With years of experience and global exposure, Bevan Brittan’s healthcare teams have the expertise to support client’s endeavours anywhere in the world. Our reputation as a leading healthcare firm has taken us across the globe, working with a wide range of clients (from NHS bodies to independent health and social care providers, operators and developers as well as funders and investors) on a multitude of commercial health projects. Our in-depth practical and commercial knowledge of the challenges and opportunities of expanding overseas are second-to-none and a true benefit to our clients in the increasingly global healthcare market.

Welcome to the HIMSS23 edition of Healthcare World. It’s always exciting to visit a new city and the Healthcare World team are on site in Chicago with a delegation of British and European companies looking to highlight their innovations and services to a wide audience. You’ll also catch our MD Steve Gardner and Operations Director Ritu Chopra there, so keep an eye out for them and free to ask them about the exciting work Healthcare World and our partners are doing at HIMMS and beyond, and how you could get involved.
We have a wide variety of o erings for you in the pages of this magazine. Our new Insight section features dynamic thought leaders such as Daniel Kra MD, a physician-scientist who presents the future of digital healthcare in the shape of the metaverse, or medaverse as it’s now being dubbed. There’s HIMSS President and CEO Hal Wolf on the changing face of healthcare as it becomes fully digital, and Dr Hinda Daggag from SEHA, the Abu Dhabi Health Services Company, on the role of genomics in the new healthcare age.
It’s becoming clear that patients and global citizens are now on board with the idea of digital healthcare. The more they can see the benefits, the more they will be willing to donate or share their data to advance medicine and healthcare. Mott MacDonald’s Digital Lead Abhi Shekar comments on this as he
 Sarah Cartledge Group Editor
Sarah Cartledge Group Editor


outlines how digital twins are helping hospitals and care centres deliver better and more joined-up care with patient wellbeing at the centre.



Former policeman Phil Anderton has broken new ground with ADHD 360, treating more than 2,000 patients each month online to help them with the debilitating and sometimes criminal side-e ects of ADHD. Similarly, HUMA is helping literally thousands of people manage their hypertension through their digital platform by monitoring them and raising the alarm if their symptoms suddenly become severe.


So we’re all becoming more used to self-care –whether it’s via wearables or apps. We are learning to monitor ourselves and discover our normal. Now it’s up to healthcare systems to respond in a comprehensive manner so this public willingness to participate in the new era of healthcare isn’t wasted. This is where HIMSS comes in. Each visitor or exhibitor understands how they can contribute to this new landscape and events such as this one enable new connections, ideas and innovations to be given air. We’ve all missed meeting our peers and colleagues across the world, and now that we can travel we can reap the benefits.
And enjoy the magazine! If you have any comments, do let me know – sarah@healthcareworld.com. I look forward to covering the latest stories in our next issue so do get in touch with me or the Healthcare World team either onsite or via email.


































Rhapsody offers interoperability and enterprise health data management solutions that power meaningful interactions, connecting more than 1 million data endpoints across more than 1,700 healthcare organizations and over 3,000 applications.












We put the right data into the right hands at the right time, in the way people need.


Computing and the use of information has become tied to the advancement of healthcare globally, says HIMSS President, Hal Wolf 32

Addressing GP and nursing shortages requires NHS organisations to focus on interoperability, says Drew Ivan, Chief Strategy O icer, Rhapsody
… and potentially billions of dollars, says Bjorn Almer, Chief Business O icer at Skåne Care AB
Phil Anderton, CEO of ADHD 360, speaks passionately about his mission to help every individual through diagnosis and support
Christina Sochacki, Senior Counsel at Al Tamimi & Company, examines the issues around adopting the metaverse in healthcare delivery
45 Regulating healthcare professionals
Helen Featherstone, General Manager of GMC Services International speaks to Healthcare World’s Editor-in-Chief Sarah Cartledge
48 Digital and data health solutions
Partners James Cassidy, Vincent Buscemi and Dan Morris of Bevan Brittan LLP analyse the current trends and challenges for implementation
52 The intelligent hospital Digital twins can improve smooth running of the hospitals, says Abhi Shekhar, Digital Healthcare Lead, Mott MacDonald
54 The benefits of experience
Health Education England’s International Director, Ged Byrne discusses new ways for global health systems to access the knowledge and experience of the NHS Consortium
56 The importance of sharing healthcare data
Dr Patrick Wynn discusses collaborative data systems in his regular column
58 Improving diversity across clinical trials
Trial participation should enable balanced representation, says Mike Failly Founder and Managing Director of Zanteris
62 Revolutionising healthcare
Robotic surgery in the Middle East is coming of age, says Mansoor Ahmed, Executive Director – Middle East & Africa (MEA) Region at Colliers
66 The UK’s international business bootcamp
The Yorkshire and Humber Academic Health Science Network is transforming healthcare by nurturing new technologies
68 Technology and patient safety
Paul Johnson, Founder and CEO of Radar Healthcare, discusses how organisations can improve patient safety through technology
70 Matching supply and demand
Automation can create a better healthcare ecosystem, Praful Mehta CEO of Vamstar tells Healthcare World
73
The automation of simple tasks, through to AI based programmes presents a total solution to support the delivery of the best quality care, says Jennifer Nobbs, Head of International Advisory, Beamtree

76 Opinionated
Healthcare World’s Managing Director Steve Gardner looks back at the lessons from COVID-19








Beamtree provides decision support and data solutions to support healthcare providers globally. We believe in creating a better future for health by turning data into insights and action through automation.

Our services help solve real-world problems in healthcare by developing smart tools that aim to improve patient outcomes. They also o er an unrivalled range of analytics covering core healthcare provider priorities, notably improving coding quality, bolstering revenue assurance, delivering better patient safety and supporting sta wellbeing.
We believe it starts with better data and ends in better care - and that better has no limit.
Find out more beamtree.com.au
A group of researchers have recently come across a way to repair damaged heart muscles following a heart attack
As global health education levels have increased, more than 90 per cent of people hospitalised with a myocardial infarction survive the heart attack. This is primarily due to recognising the symptoms, getting immediate treatment and awareness of preventions through lifestyle changes.
However, the weakening of the heart leads to related deaths in the years following the attack. Those who experience a heart attack over the age of 65 only have a 35 per cent chance of surviving the following eight years.

The most common cause of heart attacks is coronary artery disease, where the arteries become narrowed due to a build up of fatty deposits which in turn can cause blood clots to block the artery. The damage incurred by the heart muscle is unable to regenerate and never fully repairs, it is instead replaced by scar tissue.
Researchers in the Weizmann Institute of Science Molecular Cell Biology Department have identified a protein which, when expressed, leads to the regeneration of cells by reversing cell
growth through dedi erentiation. Tests carried out by Dr Avraham Shakked have shown that the damaged cells are able to retain a level of healing capacity when exposed to the specific protein sequence.
“Perhaps the most exciting is the cardioprotective e ect of this whole sequence of events that we weren’t really expecting to find or see at all, and actually that has the most potential impact,” says Dr Avraham.
The team are continuing their research to develop an accessible and e ective treatment.
In March a novel test for bladder cancer was launched at the Annual Meeting of the European Association of Urology
GALEAS Bladder is the result of a partnership between the University of Birmingham researchers and Nonacus, specialists in liquid biopsy cancer detection and screening.
“We are very excited to launch GALEAS Bladder. We are striving to develop a suite of meaningful non-invasive tools that can have real impact on the diagnosis and treatment of patients with suspected
cancer. GALEAS Bladder represents the first in this pipeline, helping to improve patients’ lives and reducing the burden of cystoscopy on over stretched clinics.” says Chris Sale, CEO of Nonacus.
The test is completely non-invasive, using highly specialised technology to detect the presence of bladder cancer in urine. The test analyses samples for DNA from tumour cells by employing innovative liquid biopsy technology and a panel of biomarkers.
“Since 2009, Dr Douglas Ward and I have been working on various strategies to accurately and reliably detect bladder cancer from a urine sample.” says Professor Rik Bryan from the University of Birmingham’s Bladder Cancer Research Centre.
“The DNA-based genomic approaches that we have been developing over the last eight years, with funding from Cancer Research UK and support and expertise from Nonacus, have allowed us to do just that with a test that appears to rival cystoscopy with regard to sensitivity and specificity for the diagnosis of bladder cancer in patients being investigated for hematuria.” he adds.
The biomarker panel has been successfully identified in over six hundred patient samples from three UK based clinical cohorts, with high diagnostic accuracy across all stages of bladder cancer.
This non-invasive test presents a viable, reliable and cost e ective alternative to cystoscopy across the entire bladder cancer patient pathway, and can act as an e icient triage system for hematuria.
At the end of March, Azerbaijan and Tajikistan joined the growing list of malaria free countries
Caused by parasites spread by female mosquitoes, and irrigation systems, malaria kills more than six hundred thousand people per year. Although treatable, the disease still plagues large areas of the Southern Hemisphere, including most of Africa, Central and Southern America, Asia and the Middle East.
Following on from their recent success, Moderna has announced its intention to deliver vaccines for life threatening conditions including cancer and heart disease
During the pandemic, unprecedented innovations condensed fi een years of progress into eighteen months, according to researchers. The speed of advancements in vaccine technology over the past two years has kickstarted a chain reaction of innovation. Pfizer is in the late stages of clinical trials for a flu vaccine and has entered a partnership with BioNTech to develop a shingles vaccine.
“There has been a massive acceleration, not just of traditional vaccine technologies, but also novel ones that hadn’t previously been taken through licensure. Certainly, mRNA falls into that category,” says Dr Filip Dubovsky, President of Research and Development
For decades a global e ort has been made to diagnose and treat malaria. In addition, public health programmes have been in place to educate people on prevention methods, including bed-nets, insecticides and safe water management.
Both Azerbaijan and Tajikistan have also introduced Mosquito Fish, which feed o the larvae of mosquitoes. These
fish have been widely used across most modern mosquito control programmes.
“The people and governments of Azerbaijan and Tajikistan have worked long and hard to eliminate malaria,” says Dr Tedros Adhanom Ghebreyesus, Director General of the World Health Organisation.
In order for a nation to be deemed free of malaria, there has to be a minimum of three consecutive years with no local transmissions and comprehensive systems must be in place to detect and address any future transmission.
According to the WHO Azerbaijan last reported a locally transmitted case in 2012, and Tajikistan reported the last locally transmitted case in 2014.
“Their accomplishment is further proof that, with the right resources and political commitment, eliminating malaria is possible,” Dr Tedros adds.
In the meantime,Ghana is the first country to licence the lR21/Matrix-M vaccine for use in children aged 36 months to five years. Marking the culmination of 30 years malaria vaccine research at Oxford University, the vaccine can be manufactured at mass scale and modest cost, enabling hundreds of millions of doses to be supplied to African countries.

create proteins, the injection of synthetic forms uses a spike protein to cover the surface of a virus, enabling the body’s cells to generate spike copies, training the immune system to defend against disease and infections.
for Novavax, who are developing a new generation of protein based vaccines.
In 2021 Moderna released the mRNA COVID-19 vaccine for emergency use, and has since been continuing its development of mRNA vaccines to save millions of lives worldwide.
“I think we will have mRNA-based therapies for rare diseases that were previously undruggable, and I think that ten years from now, we will be approaching a world where you truly can identify the genetic cause of a disease and, with relative simplicity, go and edit that out and repair it using mRNA-based technology,” says Dr Paul Burton, chief medical o icer of Moderna.
The mRNA molecule encourages cells to
Moderna is designing personalised mRNA cancer vaccines for each type of tumour, which will act as an alarm, alerting the body to existing cancer cells, which are already growing. The protein fragments, which are only present on the surface of cancerous cells, are identified, triggering an immune response. A biopsy is taken from the tumour in order for sequencing of the genetic material to take place, identifying cancerous mutations.

“[mRNA] can be applied to all sorts of disease areas; we are in cancer, infectious disease, cardiovascular disease, autoimmune diseases, rare diseases, we have studies in all of these areas and they have all shown tremendous promise.” Burton adds.
With a release date of 2030, Moderna is encouraged by the developments made over the past three years, however there are concerns that distractions could damage any further progress. For these revolutionary scientific innovations to be made, it is essential that high level investments are maintained and secure.
The NHS Consortium for Global Health provides a single point of access to expertise from the UK’s national health organisations, including the major National Health Service executive agencies and public bodies.
Technical capabilities:
•Pandemic Response, Health Security, & Climate Change
•Workforce Planning & Development
•Health Financing & Strategic Purchasing
•Digital Health & Transformation
•Public Health & Reduction of Health Inequalities
•Health Technology Assessment, Clinical Guidelines & Quality Improvement
•Genomics in Healthcare
•Government Relations
•Monitoring, Evaluation & Learning
To find out more about working with the NHS Consortium for Global Health, contact:
Kevin Miles, Senior Lead Global Health Partnerships, Health Education England Stewart House, 32 Bloomsbury Square, London WC1B 5DN
E: kevin.miles@hee.nhs.uk
M: +44 (0)7467 004 560
It’s time to build the future together, says Daniel Kraft, Physician-Scientist and founder of NextMed Health

When we think of the metaverse, we tend to think about traditional VR and AR. But how can we now connect the dots to combine our global healthcare knowledge in a new digital intelligence that is more data driven? Part of this new world of metaverse or medaverse will be generative health where we can create environments, instructions
and patient communications on the fly, and match the individual or the age cultural language. It’s the beginning of a very exciting age minuses that’s going to really evolve very quickly.
Healthcare is built upon not just one technology but by the interface and convergence of many accelerating technologies. As a result, it can get very siloed in technologies and clinical fields.
The opportunity now is to overlap them and put them together to enable us to solve things in new ways and, leverage the new technologies that didn’t exist 20 years ago when I was a Stanford medical student. It’s a really exciting time to rethink and reimagine health care, not just for now, but for the next decade.
The convergence of VR and web3 in new forms of connectivity will help us move beyond the sick care model of traditional medicine to precision wellness and optimizing health span as well as lifespan. We will move the needle from where we are now - an intermittent reactive, one size fits all sick care- to a future that’s much more health and selfcare focused.
Daniel Kra is a Stanford and Harvard-trained physician-scientist, inventor, entrepreneur, and innovator with degrees from Brown University and Stanford. He specialises in internal medicine and pediatrics (Harvard residency) and has fellowships in hematology, oncology, and bone marrow transplantation at Stanford. He was one of the keynote speakers at Informa’s Future of Healthcare event at Arab Health this year and o en called upon to speak to the future of health, medicine and technology.
COVID has been a catalyst - we went from incremental to exponential. Yet despite the explosion of telehealth during the pandemic, we are still back to waiting rooms and thinking about healthcare in old fashioned silos, rather than the metaverse.
If we look ahead 10 years, we must be careful not to have a failure of imagination. Even the next one or two years will make the last decade look slow. Of course, healthcare needs to move a little more slowly than some other fields and we need to have some guardrails.
I’ve been looking at the convergence of future for a while. At the recent Next Med Health conference I chaired in San Diego, 400 people from 30 plus countries

drug contact lenses. We saw the evolution of diagnostics 10 years ago in the shape of a basic ECG or EKG on a phone. Now a phone camera can diagnose vitals in about 10 or 20 seconds. And they can be diagnostic devices too. There is an Israeli company, Healthy.io, that can undertake urine analyses via phones straight away. There are many examples where wearables and other models can measure almost every element of our physiology from patches to ultrasound devices to sensor socks and underwearables. Now we can predict pregnancy five days before a pregnancy test, and also understand a COVID booster response. Acoustic epidemiology can diagnose whether you have a cold or COVID from the sound of your voice. Mike Snyder and others at
a whole body scan at a very low price - we’ve already started seeing very low cost scanners come to market in the last two years. There are even wearable versions that can diagnose strokes or haemorrhages that don’t just measure the brain but also provide therapeutic energy to treat certain neurologic diseases.
The big picture in this new metaverse is that the diagnostic toolset is moving from our hospital to home to our pocket via a whole new set of tools that can enable anybody to listen to a heart and diagnose a murmur. And of course, this can be blended with air or via intelligence augmentation to give us the ability to see replace the radiologists. And when there’s no radiologist, they can do a pretty good job of doing initial readings, whether it’s radiology, pathology, dermatology and even gastroenterology.
Bio intelligence can stream an intensive carrying level of data, but we still have a challenge of understanding who owns that data, and how do we even take small data and send a patient home from a hospital visit?
looked at the future from all di erent angles, from psychedelics to chatbots to drones and more. Part of the theme was the digital twin, the ability to layer all this information together and make it useful for the optimisation of health prediction, diagnostics, therapy, public and global health. As an oncologist, I think it’s going to be particularly applicable to personalised oncology, both in prevention diagnostics and therapy.
As we look at this metaverse, we need to keep in mind that it’s still a little clunky, but things are moving in an exponential manner. For example, our phones are going to start dissolving theoretically this year into air guided glasses or dissolving
Stanford have just published evidence about the use of wearables to predict who has COVID, sometimes two or three days before a positive COVID test.
Another area that’s moving quickly is imaging diagnostic imaging or predictive imaging and we’re now leveraging these into new ways of predicting everything from Alzheimer’s to cancers. For example, I had a scan a few weeks ago for a full body MRI enhanced with AI radiology in just 60 minutes. It gave me pretty good deep insights into my health and I can communicate that to my primary care doctor as well.
In the next decade we’ll see the ability to go to the local pharmacy and have
The even bigger challenge is how to integrate all this data to make it really useful for the individual, the clinician and the health care system. Everything is becoming digital – right the way through to prescribing digital apps and therapeutics as opposed to drugs and devices. There are now more than 250,000 digital health related solutions. Some of them are very clear, like digital therapeutics that treat ADHD with a video game as opposed to medication and these are now blending with empowering the patient. Each of us now can take our quantified data and make it more useful.
But increasingly, our quantified, connected data from our wearables and other tools are going to shi to our metaverse-based conditions to optimise wellness, to diagnose disease early, and then to treat disease in a much more personalised and intelligent way. With all of this connecting to our smartphones, we can start to crowdsource that knowledge project baseline to make sense of it, either to create a warning system score for every individual or patient, like an engine check light for the body. Thus, we are entering an era of predicting diseases before we even know we have them.
“It’s a really exciting time to rethink and reimagine health care, not just for now, but for the next decade”
Founder NextMed Health, Digital.Health and Exponential Medicine
Another challenge is to make sense of this new universe of technologies. I’ve recently launched a platform called Digital. Health to search for any new technology. I don’t work for these companies or have any real a iliation, but it is a good resource for discovering what is already out there and then to enable their use.
Finally, the challenge of all these new forms of tools and technologies is to integrate them into the workflow of the already overwhelmed physician, nurse, pharmacist. No clinician wants more data. We want the actionable information, and there’s an opportunity not just to prescribe digital solutions, but to connect the dots in the virtual and the physical space and to make it part of the clinician workflow. One recent example is a new Microso solution that will listen to the patient doctor interaction and write it up, so the clinician won’t have to spend so much time navigating horrible EMR systems.
Part of this future will be increasingly crowdsourced. Just like we crowdsource our driving, we can imagine a real time Google Maps or Waze for healthcare. Being a data donor empowers each of us to be part of the solution. The future of care is going to shi from our usual intermittent episodic once a year check-up to a future with much more
proactive information that can take place anywhere at much lower cost, democratising healthcare across the world.
Chat bots are getting better and better at knowing you. They will have your entire medical history and they’ll be leveraging wearable data and beyond. And of course, that brings us to this era of the metaverse. How will we interact with our care teams in a virtual hospital or caregiving location where your doctor will show up as an avatar, as demonstrated by AI Medis at Arab Health?
So how do we learn as clinicians to interact and have a good website manner as well as a good bedside manner? The whole future of medical education needs to be looked at. Part of the metaverse is medical education - we can now simulate and learn in virtual environments and practise on patients, just like pilot practice in a flight simulator.

Fortunately, global ecosystems are opening up. Starlink, for example, is providing internet access to almost 50 per
cent of remote and rural locations across the globe, creating massive amounts of new data. And our opportunity in the new metaverse is not just that data, but actual information that’s useful to the clinician and the patient.
I’m excited about this new metaverse or new health age. It’s not about any one technology but how we connect the dots, escaping from our old ideas and mindsets to solve some of the highest and hardest problems in healthcare. It’s an incredible time to be thinking about where we might go next. If we take the new exponential and collaborative mindset, we can go for more. It’s time to not predict the future, but build it boldly together.
www.danielkraftmd.net
“The even bigger challenge is how to integrate all this data to make it really useful for the individual, the clinician and the health care system”










Weofferyouagovernment partnershipwherewebring thelearningpointsfromthe Swedishmodel. Weprideourselvesin understandingyourneedsand adaptingadvicetoyour situation.

















Dr Hinda Daggag, Head of Genetics at SEHA, explains the importance of the field
Genomics has the potential to reshape clinical practice and to fundamentally change the way we prevent, diagnose, treat, and monitor illness, providing the opportunity to have more precise and tailored treatments, according to Dr Hinda Daggag, Head of Genetics at SEHA, the Abu Dhabi Health Services Company.
“With the increasing population lifespan, genomics has the potential to transform health care and the national economy and make genetic diagnosis of disease a more e icient and cost-e ective process.”
The Emirati Genome Project is a national project which aims to use genomic data to improve the health of the Emirati population. Similar to the
UK’s 100,000 Genomes Project, the UAE is beginning to profile and determine the genetic architecture among UAE nationals to aid in the development of preventive and personalised healthcare, the mapping of the Emirati genome, the study of susceptibility to diseases and the development of more targeted treatment plans. The delivery of such an ambitious programme testifies to the UAE’s commitment to embedding the promise of Genomics into the National Health system.
“The understanding of genetic variation in the Arab population is a challenge due to the lack of a high-quality Arab reference genome,” says Dr Hinda. “By producing a


Dr Hinda Daggag is a geneticist who joined the SEHA team in April 2020 as the Corporate Head of Genetic Projects. Her core values reflect her passion and drive to build a sustainable genomics framework within SEHA which will eventually enable better patient care and facilitate genomic research and development. Furthermore, she advocates for and is involved in initiatives driving national actions for personalised medicine advancement. She also specialises in supporting public-health related genomic initiatives and establishing international networking opportunities. She received her PhD in Genetics in 2009 from Melbourne University, Australia and later obtained a postgraduate certificate in genetic counselling from the UK.
reference genome specific to UAE citizens, it will enable us to deliver better and more targeted healthcare to the local population, which is largely under-represented in international reference databases.”
As head of genetic projects at SEHA, Dr Hinda sits at the corporate o ice under the Medical and Clinical A airs Unit. Her current role is to lead, manage and develop SEHA Genomics and help build a sustainable clinical genomics framework within SEHA which will eventually enable
lack of data standardisation in genomic reference databases as well as a shortage of clinical geneticists and genetic counsellors,” she says.
“Nevertheless these challenges can be overcome and, by incorporating genomic data into healthcare management, we can provide individuals with more tailored healthcare solutions when it comes to disease diagnosis, prevention, and treatment and informing reproductive decisions”, she adds. “Right now, it’s about being able to have reproductive choices by being properly informed. For example, Preimplantation Genetic Testing (PGT) can
pharmacogenomics or more traditional clinical genetics tools utilised for diagnosis, management and treatment, genetics is bound to be embedded in routine clinical practice. Also, more recently there is an emphasis on moving from reactive to proactive healthcare model.
Much of the work undertaken by geneticists is in the field of research, o en isolating the scientists from the frontline experiences of clinicians. Dr Hinda’s career has taken her from research to becoming a clinical lab manager, back to research and then to her current role in strategy within a corporate environment rather than a hospital.
“When I was working with patients within the genetics field in Jordan, I realised the importance of sitting with the parents and explaining to them in simple terms what they are facing. This covers the challenges, the condition and how we are going to try to address it, as well as what the diagnosis means for them and for their children,” she says. “It’s that human element - empathy and someone caring about what you go through as a family a ected by a genetic condition - that matters at the end of the day.”
Many countries don’t have the resources for genetic counsellors, and this vacuum is o en filled by clinical geneticists or specialised physicians. “Ideally a genetic counsellor should be sitting with the families but when this is not possible, upskilling programmes can be utilised to equip other clinicians to deliver the message, such as genetic nurses for example.”
better patient care and facilitate genomic research and development. She is also involved in genomics initiatives driving national actions for personalised medicine advancement.
“In light of decreasing costs of genomic technologies and their increasing relevance to healthcare, many countries have been restructuring their genomic medicine services to prepare for increased demand. However, integrating genetics into the clinical workflow is a persistent challenge and will require addressing issues identified universally such as inconsistency in laboratory testing procedures, incompatible data systems,
be o ered on early embryos created by in vitro fertilisation (IVF) for specific genetic conditions that run in the family. This way parents can make a fully informed decision regarding their reproductive choices. Such important work has profound implications for families who have to deal with the consequences of hereditary diseases.”
Once genomic data is incorporated into healthcare management, healthcare practitioners will be able to deliver personalised medicine tailored to an individual’s unique genetic makeup. Whether it is through preventative and proactive testing platforms such as carrier testing, pre-marital screening,
“Out of everything I have achieved so far, my work with the families has stuck with me most. It was giving them the knowledge to deal with their situation. I felt so many times it was just the fact that they didn’t have the right information in their hands - they wanted it so badly but they didn’t know where to go or how to get it. Giving them that information to empower them le the most impact on me.”
“Overall, genetics is such an interesting area to be in because you can contribute and make a di erence from so many di erent perspectives - whether it’s in research, life sciences, biotechnology, AI and data, or at the government level and writing the policies. Genetics is now at the forefront of medical innovation.”
“The understanding of genetic variation in the Arab population is a challenge due to the lack of a high-quality Arab reference genome”
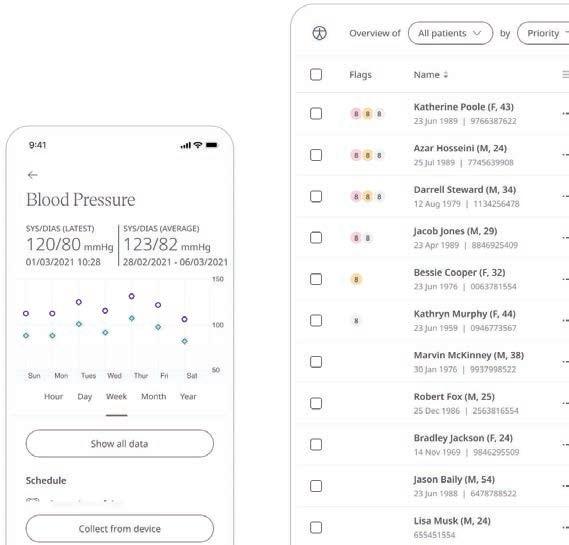
Digital health technologies are transforming the way hypertension is managed says Kaushik Gune, Head
While surfing the web recently, I paused when I came across a consumer review of the best blood pressure monitors for home use. Not because I’m looking for a new one, but because this article is at least the sixth such comparison I’ve seen in the press in the past couple of months. As Head of US Healthcare at Huma, a leading global digital health company, I’m relieved to know that people want to ‘know their numbers’
ofUS Healthcare at Huma
because undiagnosed and uncontrolled hypertension, or high blood pressure, puts us at greater risk of cardiovascular events such as stroke, heart attack, atrial fibrillation, renal dysfunction, and other disorders.
120 over 80 is a big numbers game. Hypertension a ects a staggering 1.28 billion people globally. In 2020 more than 670,000 deaths in the United States had hypertension as the primary or contributing cause. According to the
US Centers for Disease Control and Prevention, nearly 1 out of 2 adults— around 108m —have high blood pressure, and only 1 in 4 have their condition under control. It’s costing the nation up to $198 billion annually in healthcare services, medications, and loss of productivity from premature death. Fortunately, high blood pressure is treatable, and thanks to the rapid growth of digital technologies, we have a real chance at getting a handle on our systolic and diastolic numbers.
Previously, it would have been usual for clinicians to make 2 or 3 attempts at measuring blood pressure during an appointment. Reading anomalies might occur due to classic white coat syndrome, or because things weren’t
going well at home, or simply because of the time of day. Now, we understand that having more data points in the home and ambulatory setting can unmask a person’s true blood pressure, allowing for better control through medication and behavior changes. Worldwide guidelines recommend treating hypertension based on 24-hour ambulatory blood pressure monitoring and home blood pressure measurements, rather than one-o recordings in a doctor’s o ice.
Measuring pressure at a distance
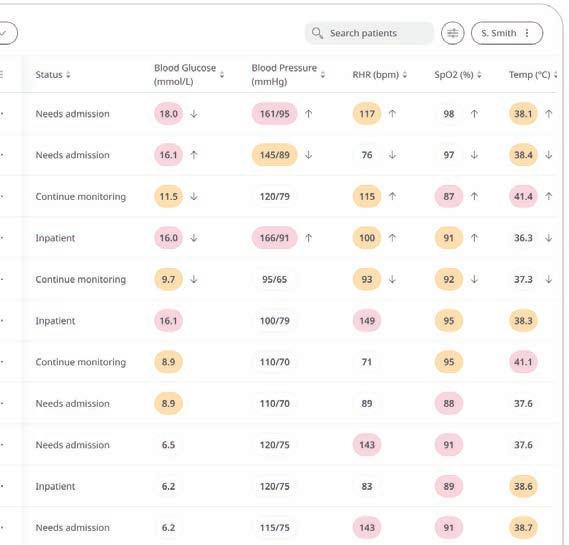
Huma’s digital platform is readily configurable to support the remote monitoring of hypertension. It is device
agnostic, so a range of blood pressure cu s and sensors are able to be used, and it has around 150 modular components to choose from to build a bespoke programme. This flexibility allows clinicians to create the hypertension virtual clinic that meets their needs versus being forced to use a one-size-fits-all solution. For example, they can choose from a variety of questionnaires to capture an holistic picture of the patient through selfreported readings and symptoms which can be read on a customisable dashboard. Healthcare providers can buy the monitoring module alone and manage the portal themselves, or as many prefer, Huma can provide a clinicallyqualified team to monitor data from patients on their behalf. The monitoring team operates under the general supervision of the healthcare provider according to a red, amber, green referral system: depending on the pre-agreed parameters, red usually triggers a clinical notification right away; amber may mean the doctor’s o ice can decide; two consecutive ambers can equal a red and so on. And rather than setting the same thresholds for everyone, Huma’s so ware accommodates individual patients, meaning that the monitoring team will only escalate to clinicians depending on each person’s profile.
While the monitoring team gathers additional readings and data and presents this to the provider, they don’t currently triage patients in terms of making medical decisions. This may change in the future. Last month, Huma became the first company in the world to gain EU-MDR Class IIb regulatory status for our disease-agnostic So ware as Medical Device. This level of certification means that, in Europe and the United Kingdom, our platform is now able to host machine learning algorithms that support risk
prediction and diagnosis, and is permitted to aid clinicians in managing serious and critical health conditions. In other words, ClassIIb approval turns data reporting into data insight, reducing the burden on HCPs by delivering proactive care through advanced triage alerts, filters and flags.

Remote patient monitoring allows the e ects of therapeutic interventions to be assessed in real time rather than waiting weeks until another in-person visit. Antihypertensive medicines act quickly, o en within hours, to bring about blood pressure lowering, and automated recording with associated data on how the patient is feeling and their general health is very valuable. Plus, a patient doesn’t make recording errors, or forget to bring their logbook. Automated readings o er better, real world control.
Sometimes patients do not fully understand their condition. Huma’s platform therefore also contains educational materials to help coach patients with hypertension to make lifestyle changes, such as improving their diet and exercise habits, quitting smoking, and reducing stress levels to empower patients.
Our monitoring team also supports clinics in the billing codes for remote patient monitoring programmes by providing a comprehensive report with details of clinical support, connected device data, and patient utilisation.
As healthcare turns increasingly towards value-based care to answer many of the issues caused by a focus on feefor-service, Huma is well-positioned to partner with forward-thinking healthcare leaders in providing e ective, low-cost, outcome-based care. Value-based payment models are moving mindsets towards upstream disease management and the holistic insights that come from remote patient monitoring to support quality initiatives and revenue drivers within this new system. We estimate that annual medical costs for patients with high blood pressure are up to $2,500 higher than those for patients without hypertension. We have to help turn the tide: in the US, approximately 90 per cent of all health expenses go to disease and injury treatment rather than to addressing the predisposing factors of these illnesses and injuries.
“Huma’s EU MDR Class IIb platform is now able to host machine learning algorithms that support risk prediction and diagnosis”
Kaushik Gune Head of US Healthcare Huma
Huma’s platform is disease agnostic and hypertension is only one of the cardiovascular disease (CVD) conditions for which it can help people live longer, fuller lives. Together with Bayer, we currently have a campaign running across the US encouraging people to take a brief web or app based assessment which is underpinned by our peer-reviewed algorithm that accurately estimates an individual’s CVD risk over the next decade. As with blood pressure measurements,

these types of risk assessment tools were historically designed to be applied in the doctor’s o ice.
The Bayer campaign aims to reach more than 100m people who may be at risk of CVD across the US with actionable insights to help improve their heart and overall health; all that is needed is access to a digital device. Through digital excellence, our goal is to empower everyone, regardless of where they live, their background or socioeconomic status, to be able to assess their individual risk of CVD and initiate a conversation with a healthcare professional where necessary. Working with researchers from Stanford University School of Medicine, our Decentralized Trial in Atrial fibrillation Patients study was one of the first peerreviewed assessments to examine whether a clinical trial operated remotely, away from a clinical centre, would be feasible and e ective for patients with a heart condition. The study, known as DeTAP and published last year saw rapid recruitment (94 per cent of patients signed up for the study in just 12 days), high engagement, and patients who otherwise failed to comply with their treatment regime showed an increased adherence to medication when linked remotely through our digital interface to their clinicians.
When it comes to heart failure, there are plenty of novel therapies available but identification of the patients who benefit from these treatments remains a challenge. Working with two health boards in the UK to conduct pilot studies in heart failure patients discharged from hospital, we successfully demonstrated that remote monitoring of patients can facilitate significant reductions in treatment optimisation times by helping upgrade patients to newer, highly-e ective medical therapies much earlier in a guidelinedirected manner.
I’m immensely proud of the positive contribution to healthcare across all disease areas that our digital platform is making. And given that most chronic disease management occurs outside of the traditional health care setting, I’m optimistic that as digital technology becomes part of mainstream healthcare, we will achieve better health outcomes for all and reduce health care spending. The future of health is digital.
“Remote patient monitoring allows the effects of therapeutic interventions to be assessed in real time rather than waiting weeks until another in-person visit”
Kaushik Gune Head of US Healthcare Huma




Feedback Medical enables clinical data to travel with the patient, says CEO Dr Tom Oakley
Many healthcare systems are in a state of transformation, so patients and the clinical workforce need easy-to-use, flexible digital solutions available from anywhere. Feedback Medical enables clinicians to make better decisions faster from any location as our solutions are designed to be applicable to any care setting internationally.
We provide a digital infrastructure that ensures clinical data travels with the patient
– making it available to all care settings and enabling clinicians to contribute to their care from anywhere. It also removes the geographic constraints of care, giving patients choice, clinicians flexibility and care providers workforce resilience.
Our solutions are currently in use in the UK National Health Service trusts (providers of state-funded acute, community and mental health services), regional NHS crossprovider care pathways and community diagnostic centres and private healthcare
facilities. In India they are found in remote care facilities and regional acute hospitals in Odisha State and clinical imaging centres in Indore.
Bleepa allows clinicians to review medical imaging and other clinical results and discuss cases collaboratively on the go. The Bleepa app on each clinician’s mobile device enables them to:
• Communicate with members of their clinical team who are based at other locations
• Work collaboratively with colleagues at times and at locations that work for them both
• Refer patients across their network with all relevant documentation
• Quickly take photographs for patient care (e.g. wounds, dermatological conditions and scar tissue)
• Easily capture the patient’s consent for their medical use. Securely upload photos and documents to the patient’s e-health record, to be viewed by a specialist at the most appropriate time

“The referral form in Bleepa allowed us to capture really important clinical information about the patient which importantly not only allowed us to plan treatment but also gave the clinicians more information, in one place, at one time, in order to aid them to triage patients’ requirements,” Janine Beattie, EPR Clinical Configuration Lead, told us.
Having centralised data around a patient in Bleepa, CareLocker provides a patientcentric way of storing that data in the cloud, ensuring its availability to any care setting that the patient attends. Patients can view their medical data on their own device, share it with others, and upload other documents allowing for a comprehensive care record.
In December 2019, when the respiratory team at the Royal Oldham Hospital in the UK wanted to improve the referral
process and response time for inpatient referrals, Feedback Medical deployed Bleepa to manage inpatient referrals to the respiratory team. By moving away from a process that was manual and paper based, the respiratory referral workflow was streamlined by ensuring a single point of access for inpatient specialist referrals. In addition, the use of Bleepa has standardised the referral process to include greater clinical detail, informing clinical decision making and collaboration.
The introduction of Bleepa and removal of manual administrative steps reduced the length of time for respiratory inpatient referrals to be actioned to just 0.4 days, an average saving of 1.7 days per referral. In addition, response time to referrals was reduced to less than one minute from an average 7.5 minutes, saving around 6.5 minutes per referral, or around 5.6 weeks of a full-time clinician’s time per year.
Similarly, over the past year Feedback Medical has been working with a UK regional cross-provider care system, connecting primary and secondary care via its community diagnostic centre (CDC), to deliver end-to-end symptom-based pathways. Our digital infrastructure enables patients to move seamlessly between primary and secondary care for definitive investigation and management based on their symptoms.
At Queen Victoria Hospital we have demonstrated that CDCs can be used
to successfully deliver cross-provider symptom-based diagnostic pathways that transform the patient journey within the NHS and we expect to be able to show a meaningful impact on patient waiting lists as a result. ICSs need to adopt a symptombased pathway approach to CDCs if they are going to deliver the expected impact on cancer and elective care waiting times. This pilot is the first example in the country of how this can be delivered, and our digital infrastructure is an essential component of delivering it.
Many healthcare systems globally face the challenge of a high proportion of people managing lifestyle-based non communicable diseases (NCDs). Bleepa can enable more proactive preventive care to reduce complications around chronic conditions like diabetes, chronic obstructive pulmonary disorder (COPD) and coronary heart disease by providing enhanced communication among primary care doctors to help keep patients out of a secondary care setting, as well as swi and flexible sharing of results and imaging for clinical review.
Feedback Medical provides both the digital and physical infrastructure for remote TB screening in Odisha state to enable frontline clinicians in remote areas to carry out X-ray studies and transmit them securely to specialists. Once the x-rays are transmitted by Bleepa to our CareLocker cloud store, the scans are then processed by our AI partner Qure.ai, which generates a patient report that is made available to the scanning clinician via Bleepa. The clinician is then able to quickly identify tuberculosis patients or those most at risk and act accordingly. Our initial pilot, which went live in March 2022, identified signs of TB in around 21 per cent of patients scanned in its first five months.
For patients, having their clinical data readily available is the best option, enabling better patient outcomes through streamlined care.







Delivering safe and technical facilities to give healthcare a cooler future will save lives say Padraig McMorrow, Associate Manager, Architecture, and Andrew Street, Studio Principal, Architecture, Arcadis IBI Group
The 2022 global heatwave, where temperatures hit a record 40 degrees in the UK, highlighted the serious risks to the UK’s most vulnerable and particularly to those recovering in healthcare facilities. As the country hit boiling point and a nationwide drought was declared, healthcare sta worked around the clock to keep people as comfortable as possible, and ultimately, alive.
Simply put, patients need to be kept in an environment with a cool and stable temperature for their safety and comfort. Ideally, this would be in a sealed, airconditioned space; however, this is an energy-intensive strategy that doesn’t necessarily aid recovery.
In addition, multiple highly specialised technological considerations, both for patients and healthcare professionals, add to the challenge of designing healthcare facilities. These technical requirements vary as buildings are designed for di erent clinical and operational services, specialist equipment, workplace and therapeutic requirements, patient comfort, and high-risk and secure unit considerations.
The question is: how can we deliver safe and highly technical healthcare facilities for

the good of patients and the planet? And can architects design buildings that actively contribute to patient recovery?
How a building promotes health benefits can range from individual to individual. But what’s best for the patient experience isn’t necessarily optimal for building e iciency. Examples include operable windows and highly e icient air ventilation needed by healthcare buildings, which leads to higher energy use relative to residential environments. These are key factors a ecting the operational energy cost of healthcare estates.
Most healthcare buildings require air conditioning to deal with our increasingly extreme climate.
Where indoor ambient temperatures exceed 26˚C, a risk assessment is carried out and action is taken to keep vulnerable patients safe. The UK’s Chartered Institute of Building Services Engineers (CIBSE) Technical Memorandum 52 requirements dictate that building design must maintain a stable temperature and avoid overheating.
According to National World, the latest figures for 2020/21 published by NHS Digital “show more than 4,100 overheating incidents were recorded across 104 NHS Trusts – the second highest since current records began.”
To reach operational carbon targets developed by a range of built environment organisations including Royal Institute of British Architects (RIBA)photovoltaic, London Energy Transformation Initiative (LETI), and World Green Building Council, we must design buildings optimally to limit how o en energy-intensive air conditioning systems operate. At the risk of worsening already volatile conditions, a combination of poor environmental management with energy-intensive mechanical systems fitted to ine icient buildings is simply not an option.
While variances in thermal comfort can negatively a ect anxiety, mental health and stress, so too would recovering in environments with insu icient daylight

“Patients need to be kept in an environment with a cool and stable temperature for their safety and comfort”
Andrew Street Studio Principle, Architecture Arcadis IBI Group
or operable windows. Studies show that a connection to nature and a sense of control over our environment benefits health and recovery—even if it’s only perceived.
It makes sense then that hospital rooms enabling patients to view green space and open windows could help them recover more e ectively. The window becomes ‘therapeutic’.
Arcadis IBI Group (Arcadis IBI) leads healthcare building design across 60 global studios, including healthcare buildings operating year-round in some of the hottest and most extreme climates in the world.
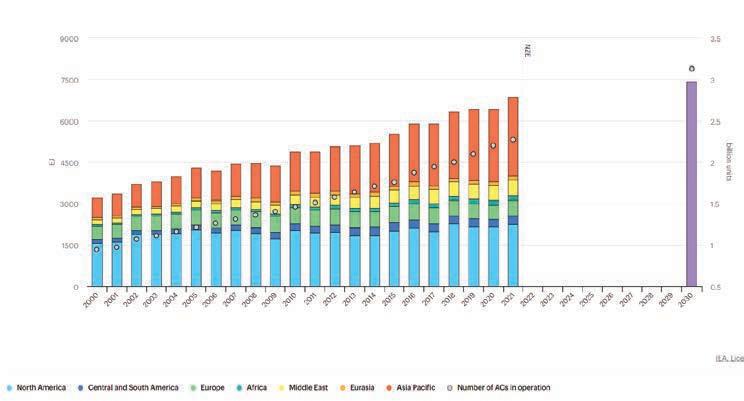
Cooling energy consumption for these spaces is rising, and 2021 saw the largest annual increase in demand of the past decade. Energy demand for space cooling has increased at an average pace of 4 per cent per year since 2000, twice as quickly as for lighting or water heating. Higher energy consumption for cooling a ects peak electricity demand, especially during hot days when equipment is operating at full capacity.
Building orientation and window shading are the two primary techniques we use to reduce the load on a building’s mechanical systems. Reducing the building’s space cooling energy demand is our first step in decarbonising any building in a hot climate. Additionally, we apply Passive House solar design principles to reduce the risk of overheating and limit unwanted solar gains reaching glazed building surfaces.
Engrained in the architectural design of healthcare buildings from inception are optimum window size and location, room programming and building operations.
By identifying key design parameters, which can reduce unwanted heat gains in early design stages, we can avoid added costs at later design stages. We also can incorporate more decarbonisation parameters, including photovoltaic panel space allocation to generate maximum renewable energy for cooling. Energy recovery through mechanical ventilation allows us to transfer cooling energy from exhaust air to incoming warmer air. The same principle is used in cold climates to retain heating energy. By building to Passive House standard, we can drastically reduce the cooling energy requirements in hot climates with high insulation and airtightness levels. Conversely, Arcadis IBI have significant experience building to international
Passive House standard in heatingdominated, colder climates of Canada.
By applying these high-performance building techniques to hotter climates, we can apply fabric-first principles to reduce the energy demand to cool spaces and deliver buildings that are comfortable, functional, future-proofed and decarbonised.
On a wider scale, our approach to landscape and urban design integrates ‘green’ and ‘blue’ areas into cities, reducing the ‘urban heat island’ e ect and the cooling energy required in buildings alongside areas of vegetation or water.
According to the Greener NHS programme’s Third Health and Care Adaptation Report 2021, “the portfolio of government-owned NHS property comprises more than 3,000 properties with 7,000 tenants across England, representing around 10 per cent of the NHS estate. NHSPS is developing new reporting metrics to ascertain the extent that overheating impacts their portfolio.
Meanwhile, several NHS Trusts across the UK are looking at partnerships with local authorities to install solar farms to run their healthcare estates more e iciently. In the West Midlands, a Trust and Council have made a joint planning application for a solar farm. The farm is projected to be the size of 21 football pitches and aims to power one of the Trust’s hospitals with renewable energy.

Reviewing the challenges and providing solutions requires constant creative solutions and cross-system leadership at a national level. To build climate-resilient health systems and institutions, leaders play a key role in raising the profile of climate change and holistic recovery methods for patients while reducing emissions.
Ultimately, our goal is to reach a point where passive internal air quality is improved so that patients can recover faster in optimal temperature-controlled environments.
“Studies show that a connection to nature and a sense of control over our environment benefits health and recovery”
Padraig McMorrow Associate Manager, Architecture Arcadis IBI Group


Oncology
Immuno-oncology
Immunology
Berkeley Research Group, LLC (BRG) is a global consulting rm that helps leading organizations advance in three key areas: disputes and investigations, corporate nance, and performance improvement and advisory. Headquartered in California with o ces around the world, we are an integrated group of experts, industry leaders, academics, data scientists, and professionals working across borders and disciplines. We harness our collective expertise to deliver the inspired insights and practical strategies our clients need to stay ahead of what’s next.

Computing and the use of information has become tied to the advancement of healthcare globally, says HIMSS President Hal Wolf

The evolution of healthcare has always been fuelled by data and information. HIMSS has been on the same journey from day one and continues to help accelerate information and technology as a part of healthcare. This vision dates back to 1961 at Georgia Tech, a technical university in Atlanta, and was the brainchild of the head of the computer science department who saw that hospitals could use data and information to help run themselves better.
It’s important to recognise that HIMSS is a society - a group of people with like-minded goals around a particular discipline, but not just a single discipline or a single component. As a result, today HIMMS encompasses physicians to nurses to technologists, and everyone in between.
Our mission is to reform the global health ecosystem through the power of information and technology based upon a fundamental vision, which is to realise the full health potential of every human,
everywhere. And so those pieces come together around health equity and the goals of the organisation, which is that every human, no matter where they are, should be able to reach their full health potential. And the critical component of the methodology is the utilisation of information and technology.
So, how do we utilise information and technology for the betterment of the delivery of care for every person everywhere? In the last five years, HIMSS has grown from under 80,000 members to more than 120,000 as computing and the use of information has now become incredibly tied to the advancement of healthcare. It’s not just about access but about information to improve quality, and we have comparative data and information as never before with the dependencies such as interoperability that sit underneath it, where we have to be able to have the information exchanged on a fundamental basis. But when you look at the bigger picture of healthcare and the challenges of healthcare overall, they have remained largely the same.
We are dealing with an ageing population, the silver tsunami and the baby boomer generation, who are developing more chronic disease burdens which we are much better at diagnosing. There is also the lack of knowledge about the burden of Long COVID. Within this framework, we have the issue of geographic displacement - you can live in the shadow of some of the greatest hospitals in the world but it doesn’t mean you have access. Geographic displacement is both a world issue as well as an urban issue and there are fundamentals behind it. First of all, it takes a heck of a lot of funds to build
Hal President & CEO HIMSSHarold (Hal) Wolf is the president and CEO of HIMSS, a global advisor and thought leader supporting the transformation of the health ecosystem through information and technology. Wolf is respected internationally as a healthcare and informatics leader, with areas of expertise in mHealth, product development, integrated care models, marketing, distribution, information and technology, and large-scale innovation implementation.
a system, and secondly, you’ve got to have the people to man them. And there is another chronic problem, a shortage of people to manage healthcare systems around the globe.
So we use digital health to be able to extend care or diagnosis of care to individuals as they move forward. We now have an educated consumer group - one of the silver linings of the COVID era was that people realised they could do a number of things to support their health online without sitting in front of a nurse or a doctor. Equally, systems learned that they had no choice but to do that so the whole world of digital health has changed dramatically.
We see an app ecosystem which continues to develop. We see the beginnings and the utilisation of AI as well as machine learning tool capabilities in order to support it, both of which have a huge impact in supporting systems as they exist today. They also impact health equity and are really starting to break down the barriers on that geographic displacement.
The recognition is emerging that there is almost too much physical infrastructure, and healthcare has to be delivered di erently in societies that have been built on the encounter-based paradigm. I call it the anomaly, meaning that we’re trying to define normal at the individual level or predict an anomaly against the norm at the population health level. Traditionally we would run tests and then put the patient into a defined care pathway. We have always carried out preventative tasks where we ask people to come in and have blood taken for example, or try to define risk through behaviour.
Digital health has seen the development of predictive modelling in anticipation of the anomaly before it occurs. This could be via an app or machine in the home that can detect and decipher that an anomaly has occurred, which may not even be recognised by the individual themselves. This is where the substitution of digital health starts to transition itself into the delivery of care, both within and outside the institution.
I would say digital health is a critical complement to the encounter-based paradigm, and they have to work hand in glove with each other. It will help both with the identification and the prioritisation
of where those highly valuable resources in the encounter-based paradigm should be utilised and focused. It will then extend beyond the walls of that physical infrastructure through digital capabilities to the person in the remote village or wherever the case may be, so that geographic displacement can be overcome.
The need for human to human contact will always be there. But if we can maximise utilisation of digital health, if we see the development of the health ecosystem and we allow the utilisation of data and information to be de-identified, highly secure information will be able to work with us on predictive modelling.

And surprisingly, the countries with the least healthcare infrastructure will be able to take advantage of these new systems first. They are not burdened by the albatross of legacy health care systems. The days of building computers in the basement of a hospital are long gone. I believe emerging economies will build
cloud-based infrastructures that sit in one place within their country – for example a lightweight electronic medical record that uses 3G up, not 5G down. Once it is in the field with a minimal level of bio capability IDs, they can track an individual’s basic state immunisation record and deliver simple pharmacy alone which is a massive upli . It’s critical for maternal health and it’s critical for health equity.
I’ve spent time in villages in Africa and other places, and I’ve talked to many a physician with Doctors Without Borders. I think the absolute forefront of digital health is to build these cloud-based infrastructures that are secure and flexible, using algorithms to li these fundamental economies up by having better health. Any society that has a healthy society produces more, lives longer, does a better job and has a chance to grow. The second we improve healthcare and make it more universally accessible, we give life. And that’s the truth.
“The substitution of digital health starts to transition itself into the delivery of care, both within and outside the institution”
Supporting international health care providers to deliver best in class primary and step down care
Providing partnership opportunities for investors looking at building international and UK based portfolios


Addressing GP and nursing shortages requires NHS organisations to focus on interoperability infrastructure for data integration, identity, and clinical terminology, says Drew Ivan, Chief Strategy Officer, Rhapsody
Facing a deepening crisis of GP and nursing shortages, the call to ease clinician burden and burnout throughout the NHS has never been greater. Reducing sta ing shortages requires more than an attempt to add
human resources. Instead, it’s necessary to use existing resources more e iciently and leverage them through interoperable systems.
Results from a recent HTN poll support this notion. When asked “If you could
solve one challenge in the health tech industry, what would it be?” 42 per cent of respondents answered Integration/ Interoperability.
Alleviating the challenge depends on clinician access to and confidence in data quality to make timely, informed decisions about patient care. Prioritising health data management can help increase not only clinician e iciency but also patient engagement.
When transparent and reliable data is more easily accessible to patients through online portals and applications, they are empowered to stay involved in their care journey and enabled to use this information to make healthier decisions. A strong foundation of quality data impacts initiatives across the care continuum — and most importantly keeps patients healthy and out of traditional care settings.
What does a truly interoperable health and social care system look like?
It will happen with clean, timely, actionable data is accessible at the right time, in the right way, to the right people and systems. These systems include:
• Electronic health records (EHRs)
• Financial systems
• Remote patient monitoring systems
The problem is that these technologies don’t inherently integrate with one another, leaving healthcare providers and sta to do the manual work. Overcoming these interoperability roadblocks depends on the depth, breadth, speed, and flexibility of the underlying interoperability infrastructure.
As healthcare leaders consider what investments to make in interoperability infrastructure, they should consider how they plan to:
• Access and exchange data stored in di erent systems within and outside the care environment
• Positively identify patients at every point of encounter

• Map di erent clinical terminology and data sets, including unstructured data
• Choose an interoperability partner who understands all aspects of healthcare data interoperability
Essential infrastructure: An integration solution Integration involves accessing and exchanging data. Integration solutions,
such as Rhapsody Integration Engine, help healthcare organisations move data among di erent systems, including routing, data transformation, and business rules.
In the absence of a best-of-breed integration engine built for healthcare, organisations across the NHS rely on manual processes to extract, compile, standardise, and pass data between disparate systems. This is a tedious, expensive, and error-prone administrative exercise that leaves data disconnected.
With the Rhapsody Integration Engine — also known as a Trust Integration Engine or TIE, NHS organisations aggregate and send data automatically, ensuring fast, accurate, and e icient exchange, unburdening health organisations by putting the right data in the right hands at the right time. More than 85 NHS trusts already use Rhapsody as their integration solution to support all healthcare message formats and standards, including HL7 (v2 and v3), HL7 FHIR®, CCDA, NCPDP, X12, IHE, DICOM, XML, and more.
Essential infrastructure: an enterprise master person Index (EMPI)
Identity involves understanding who you’re talking about — which patients and providers are related to the data you’re exchanging.
Inaccurate identification and disconnected records are a major challenge for health systems because they introduce ine iciencies, billing errors, data issues, poor experiences, and clinical or legal risk. Rhapsody EMPI addresses the datamatching process and reduces duplicate record creation by using advanced data science, iterated on in working with healthcare organisations around the globe.
Rhapsody EMPI enables positive identification of each person — including the patient’s past medical history — at the point of service for a better experience and ultimately improved outcomes. It achieves this by creating a common view of each person across the health and social care landscape and can easily incorporate national identifiers.
It connects to disparate systems via Rhapsody and open standard REST APIs, allowing downstream and upstream communication to synchronise the demographic record across multiple integrated HIEs, EHRs, regional and national systems. These APIs
can be exposed to enable integration with biometric systems — for instance fingerprint, facial recognition, and palm print technologies — to further enhance positive ID. Third-party referential matching can also be invoked to further improve connectedness, where regulations allow.
Essential infrastructure: clinical terminology solution
Semantic interoperability involves knowing what you’re talking about. Rhapsody Semantic — a combined terminology solution, authoring tool, and FHIR terminology service — allows healthcare organizations to synthesise health records from more than one system and to analyse data.
To achieve a high level of interoperability, high-quality clinical information, and accurate analytics, all data sent by or received into a healthcare ecosystem should be mapped to a recognised standard. This enables you to achieve clinical expression by cross-mapping all

major healthcare vocabularies, including diagnostic, lab, and procedure codes — and even unstructured data.
Rhapsody Semantic is one application and one source of truth that handles everything from metadata to content management, as well as all phases from development to publication, in consistent and proven workflows. It features code lookups, algorithmic mapping, electronic clinical quality measure (eCQM) value sets, condition subsets, and custom subsets.
As NHS leaders consider partners who can help ease sta ing shortages by smartly deploying interoperability solutions, look for one who:
• Supports any data standard
• Deploys where you want to — in the cloud, on-prem, or a hybrid of the two
• Right-sizes the services and support you receive
• Prioritises service and services experience
• Is fully committed to solving healthcare problems
• Meets your requirements, whether you want to develop operational skills to maintain integrations in-house or outsource them
• Helps connect caregivers to the data that they need when they need it, improving outcomes and optimising operations
• Increases confidence in insights by ensuring analytics are fed by the most complete and accurate data
• Navigates you away from pitfalls, and never leaves you exposed
... and potentially billions of dollars, says Bjorn Almer,
 Chief Business Officer at Skåne Care AB
Chief Business Officer at Skåne Care AB

The world’s first e-prescription was dispensed in Sweden in 1983. Since the late 90’s there has been a strong ambition to phase out paper prescriptions and a er a final push, by 2022 Sweden reached 100% digital. Few IT-projects have proven as profitable as this and the entire investment in the latest AI-based platform was recovered in the first year only by measuring the savings in reduced adverse e ects.
By using AI to ensure the e icacy of medicine and alert doctors to conflicting medication, Sweden has seen a reduction in adverse e ects. In addition, digitisation has brought benefits such as better inventory control, legibility, and fraud protection, further improving patient safety and streamlining processes. This results in lower costs and a better patient experience.

Accelerating any nation’s progress on e-prescription is wise as it is likely to more than pay for itself almost instantly. And save lives.
Skåne Care is part of the Swedish public healthcare system and as a governmental entity we can access a wealth of know how. Regardless of if you need a second opinion
on your plans, a study visit to get inspired by another country, leadership training for your management team or some clinical upskilling for your sta … or you need comprehensive on-site support on a larger project. Sweden can help!

“Accelerating any nation’s progress on e-prescription is wise as it is likely to more than pay for itself almost instantly”
Bjorn Almer Chief Business Officer Skåne Care AB
Phil Anderton, CEO of ADHD 360, speak passionately about his mission to help every individual through diagnosis and support
There are very few poacher turned gamekeeper stories that ring true, but Phil Anderton can justifiably claim to have one. A former senior police o icer, he made it his mission to help youngsters turning to crime to identify the cause of their behaviour. His findings led to a national UK policy, the Youth Crime Action Plan, and since leaving the force he has devoted his career to consolidating this work, both nationally and internationally.
“About 20 years ago my chief constable Sir Paul Stephenson came into my o ice
to say there were too many young people coming into the criminal justice system and he needed me to sort it out,” he tells Healthcare World. “I asked my team to look into what we could be doing better to keep young people out of crime. One of my sergeants Steve Brown brought up a genetic condition called ADHD or Attention Deficit Hyperactivity Disorder which is passed on genetically the same as height, it’s 80% inheritable. It presented an explanation for the reasons that some people come into crime and criminality,
not least of which is di iculty regulating emotions, a propensity to try substances, to abuse alcohol, and an inability to control impulse in terms of conflict situations leading to assaults, and so on.”
At this time it was so unusual to discuss mental health in conversations about crime that Phil had to co-opt serious academic and clinical research to validate his hypothesis. “I didn’t want to go public without this validation for fear that the message would be mistaken and the police would be accused of demonising individuals for being unwell.”
For six months he and his team worked with support from some of the most eminent psychiatric researchers and clinicians in the world. Once they discovered the statistic that 5 per cent of the general population has ADHD, and that 25 per cent of the prison population has ADHD, it confirmed his hypothesis.

The chief constable gave the green light for Phil to instigate this new way to combat crime.
“For example, if a young person received a warning by the police, we began to log those warnings,” he recalls. “On the second warning the perpetrator would be referred for ADHD assessment and it
proved to be quite successful. We did some work with magistrates on how to convene a court to be more sensitive to ADHD to give people a fairer trial, and we did a serious amount of parochial work as well.”
Soon Phil and his team were asked to North America to speak about their work, and their methods also gained more traction back in the UK. “We met a couple of times with central government and we went to 10 Downing Street to look at policy,” he says. “These meetings led to the publication of a national Youth Crime Action Plan which included ADHD as a causation factor.”

A er leaving the police force at 43, Phil became a management consultant ultimately with PWC, but he still

maintained his links with ADHD. “I approached one of the big pharmaceutical companies and suggested they think about bringing new drugs to market slightly di erently. I knew that NHS clinics are very ine icient and I asked to be supported for two years to change this,” he says. “My premise was that if the clinics see more patients, more people would be treated and their market share would increase.”
Most of the medications for ADHD are in the controlled drug bracket and according to Phil they are valuable, well researched, hard cra ed drugs. “They stimulate activity in the right parts of the brainbasically where the brain doesn’t have enough dopamine in simple terms. These medications stimulate the production or the availability of more dopamine, and it’s our job at ADHD 360 to put you clinically on the right level.”
“Medicine cannot cure the situation, but it helps people avail themselves of the opportunity to live their best lives”
Phil Anderton CEO ADHD 360
He goes on to say that the deficit of dopamine in the brain isn’t something that can be overcome on a permanent basis. As the medication wears o , the patient returns to their normal deficit position. “The medicine cannot cure the situation, but it helps people avail themselves of the opportunity to live their best lives.”
A er two years and having published a paper on what excellence would look like in an ADHD clinic, Phil decided to set one up with two colleagues. “We thought we’d see 20 patients a month, but this month we’ll see 1200 and we’re still we’re still not keeping up with demand!”
ADHD 360 is a telehealth clinic that assesses individuals via video conference questionnaires and then moves a ected people into a treatment plan. “People are far more aware of ADHD than before,” he says. “We see many young people and children because waiting lists are at least two or three years on the NHS, which is too long at a young age. In addition, we see many adults coming through because previously there were no adult services, so our youngest patient is five and our oldest patient is 76.”


Phil o en wears ADHD 360 branded clothing as he goes about his daily life, and this has led him into chance encounters with former patients. Recently he walked into an Apple Store to fix his phone, when one of the floor walkers noticed his t shirt and asked Phil about his role in the company. “When I told him, he called over his colleagues and told them that I had changed his life by allowing him to be the man he is.
“Just 48 hours later, I was chatting to a schoolteacher on a train about neurodiversity in the classroom. Another passenger leaned over and said: ‘I’m a patient of yours and
you’ve changed my life. Would you mind meeting my wife because you’ve changed her life as well. Just looking at her face was the perfect thank you and it’s quite humbling to understand you can bring about such a change.” On an international level, the organisation has assessed English people in Australia and the Middle East. But language is not a barrier, and they are looking to work with the Asian community in the northwest of England with clinicians who are multilingual. For Phil, it’s a continuation of the job he first started as a police o icer. As he says, “I was a cop asking the NHS to do more to keep people out of crime. Now we are on contract to the NHS, doing what we can to keep young people out of crime. You don’t get many poachers and gamekeeper stories with better ending than this.”
“We thought we’d see 20 patients a month, but this month we’ll see 1200”
Phil Anderton CEO ADHD 360












Christina Sochacki, Senior Counsel at Al Tamimi & Company, examines the issues around adopting the metaverse in healthcare delivery
Did you know that the concept of the metaverse is not new?

Apparently, the term ‘metaverse’ was coined in 1992 by author Neal Stephenson in his sci-fi novel Snow Crash. As far back as 1938, the concept of a 3D immersive internet was contemplated; the French poet and playwright Antonin Artaud is documented as using the term virtual reality in his collection of essays, “The Theater and its Double”. But when and how we will adopt the metaverse in healthcare delivery, and how
the data can be monetised, are some of the big questions.
Organisations are increasingly dataheavy. As Middle East businesses go through a rapid process of digital transformation, they are increasingly looking for insight and advantage from the large datasets they hold and have access to. The laws concerning health data in the Middle East generally do not make specific reference to monetisation. This is because the laws are generally focused on the public health. Where monetisation
is expressly referred to, such as in terms of national health information exchanges, it is expressed to be not permissible.
Further, in the Middle East region we see a number of countries having data localisation requirements where, even with a patient’s consent, the law prohibits use of health information, and deidentifying it isn’t necessarily su icient to get around the use and transfer restrictions set out in the laws.
With the growing trend for Middle East countries adopting European data protection legal principles, which focus on regulating a previously underregulated data economy and providing rights to individual data subjects to better control the use of their data, Middle East organisations need to ensure that their data monetisation strategies are in place, tested, and future-proofed to ensure that they can continue to secure value from the data they hold.
The metaverse, or Internet 3.0 / Web3, is not simply augmented reality (AR), virtual reality (VR), or mixed reality (MR), but rather a digital ecosystem, a hybrid of these technologies that adds artificial intelligence, as well as other immersive technologies, and blockchain. The metaverse is a parallel digital world, or visual electronic depiction of reality. The movie Ready Player One instantly comes to mind (although I hope our reality doesn’t become as dystopian as in that movie).
Historically, healthcare delivery required physical patient and provider interactions; however, we already see that with telehealth services healthcare providers can make a diagnosis, administer medical treatment, or perform surgical procedures, among other things, remotely. Now, add in AR, VR, AI and a bunch of other techy acronyms, and digital health solutions
appear to be at a pivotal transition point to unprecedented adopting in the healthcare industry (and life sciences too!).
Of course, this shi comes with its own legal and regulatory hurdles. The metaverse in healthcare (“Medaverse”) market is typically segmented by:
1.Component, such as:
a. So ware,
b. Hardware (VR Headsets, AR Devices),
c.Technology, such as:
d.Telemedicine,
e.Augmented Reality
f. Virtual Reality
g.Mixed Reality,
h.Artificial Intelligence,
i.Digital Twins, and
j.Blockchain.
Christina Sochacki Senior Counsel, Head of Healthcare & Life Sciences, KSA Al Tamimi & Co
“When and how we will adopt the metaverse in healthcare delivery, and how the data can be monetised, are some of the big questions”

2.Applications, such as:
a.Patient Engagement,
b. Pre-Operation & Post-Operation Planning,
c.Immersive 3D Training,
d.3D Lectures,
e.VR Therapy,
f. Diagnosis and Treatment, and
g.Remote Monitoring.
3.By End-User, such as:
a.Hospitals,
b. Pharmaceutical, and
c.Insurance Companies.
Across all these segments are data transfer elements - requiring access to the data from outside the country, or transfer of the data to another country. By way of example, Article 13 of the UAE Federal Law No. 2 of 2019 Concerning the Use of Information and Communication Technology in Healthcare (“ICT Heath Data Law”), sets out the requirements for storing and transforming the health data and information outside State: “It is not permissible to store, process, generate or transform the health data and information outside State -which are related to the health services provided inside Stateexcept in the case where a resolution is issued from the competent Health Authority in coordination with the Ministry of Health and Prevention.” The supporting Ministerial Resolution No. 51 of 2021 Concerning Cases Where Health Data and Information May Be Stored or Transferred Outside the State, allows data transfer outside the UAE in limited circumstances:
Across the Middle East region, we are seeing national health information exchanges launched. In the Emirate
of Abu Dhabi, UAE there is Mala i. In the Emirate of Dubai, UAE there is the Dubai Health Authority’s (“DHA”) Nabidh. And at the federal level in the UAE there is the Ministry of Health’s Riayati. In the Kingdom of Saudi Arabia, there is the Saudi health Information Exchange (“SHIE” or Saudi eHealth Exchange “SeHE”). In general, health data held in the local governmentcontrolled health information exchanges cannot be shared with third parties (beyond those identified by statute) nor monetised.
To dive a bit further, Nabidh is a secure healthcare platform that allows public and private healthcare facilities in Dubai to exchange trusted healthcare information. Healthcare providers can use Nabidh to securely share patient health information electronically, while adhering to the Nabidh policies and guidelines for data collection, storage, and sharing. Mala i is a health exchange platform governed by the Health Information Exchange policy (“ADHIE Policy”) of the Abu Dhabi Department of Health (“DOH”). This policy enables healthcare providers to share patient health information electronically, with guidelines in place for the collection, storage, and sharing of health data. For any patient health data held in the health information exchanges of DOH and DHA, there are prohibitions on data sharing with third parties and monetisation. The use of (including monetisation of) identified patient data requires both consent and approval from regulators upon being satisfied that confidentiality is protected.
Thus, where the Medaverse expects to draw upon Middle East locally generated or hosted data, it will be necessary to further analyse the source of such data, restrictions on its transfer or access (whether from in or outside the country), and whether monetisation of such is permitted.
We are also seeing the launch of genomics programmes in the Middle East. Abu Dhabi, Dubai, and Saudi Arabia have the most notable programmes.
Under the Abu Dhabi Emirati Genome Program, all genomic data is owned by the government and there are strict provisions regarding its storage, access, and use. All research including data sharing arrangements requires regulatory approval. While local policy on genomics research speaks to the concept of value creation (benefiting the population,
innovators, and stakeholders, as well as introducing public private partnerships and incentives schemes to motivate the sharing of genomic data), regulatory approval is required for such activities.
In Dubai, in general, the sharing of health data with private third parties for ‘secondary use’ (e.g., research, public health, quality improvement, safety initiatives, insurance, payment, and marketing), requires regulatory approval. The DHA’s Policy for Health Information Assets Classification sets out their requirements for classifying health information in the Emirate of Dubai. This policy applies to both identifiable and de-identifiable patient health data and is in accordance with the DHA Policy

on Confidentiality and Data Protection. Specifically, it requires that the “sharing of Sensitive Data with Private third parties
“Middle East organisations need to ensure that their data monetisation strategies are in place, tested, and future-proofed”
Christina Sochacki Senior Counsel, Head of Healthcare & Life Sciences, KSA
Al Tamimi & Co
should be evaluated and approved by the DHA [Health Informatics & Smart Health Department]”. Under the policy, “Sensitive Data” is defined as personal data which includes information data about a person’s family, ethnicity, health, a iliations, political views, religious beliefs, or personal life.
In KSA, the Saudi Human Genome Program is specifically created to, amongst other things, enable scientists and researchers to benefit from the genetic information in the programme, utilising the information to develop diagnostic and prevention tools to reduce the incidences of genetic disease in KSA. Saudi Arabia’s Ministry of Health has published a suite of policies
relating to the SHIE, which are broadly aimed at the use of health information, including patient data, in the context of the increased adoption of technology and digitalisation in the health system. Under the SHIE framework, the implementation of ongoing technological improvements to the healthcare system is contemplated on two main fronts. The first is the adoption of secure technology solutions to enable streamlined patient care via online health records. The second is making available de-identified patient data that can inform research. This can be used by both the public sector, for example, by guiding public health policy responses (e.g. containment and prevention of epidemics, or targeting health awareness programs),

and by the private sector, for example, by developing new treatments and pharmaceuticals.
I leave you with the 64-million-dollar (adjusted for inflation) question: Which segments will be accepted into and used in the Medaverse first?






Healthcare World’s Editor-in-Chief Sarah Cartledge speaks to Helen Featherstone, General Manager of GMC Services International about the importance of a comprehensive regulatory framework
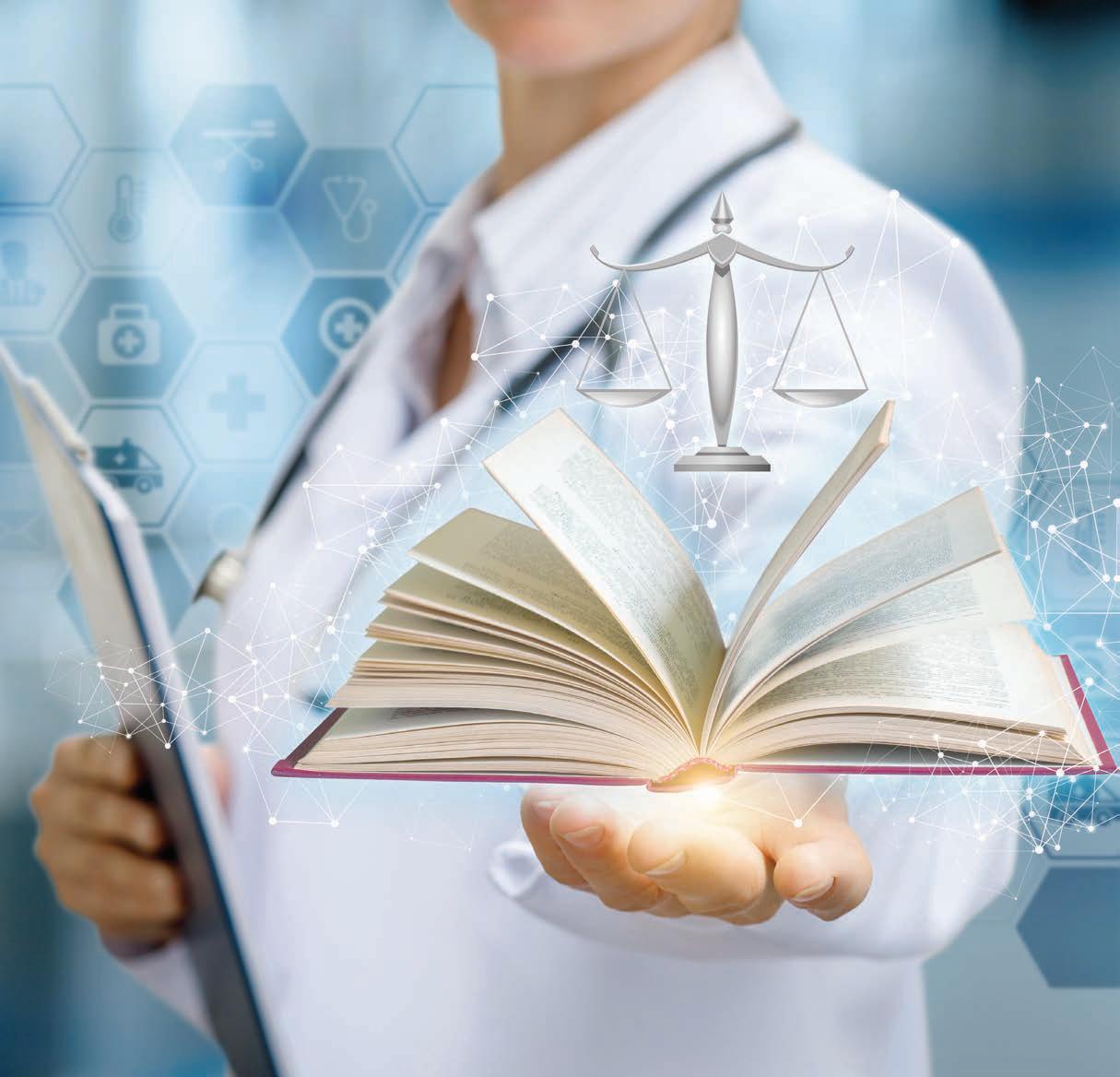
Over the past 160 years, the UK’s General Medical Council (GMC) has become one of the leading professional healthcare regulators in the world.
From setting the standards by which all medical doctors need to abide by to registration, revalidation, the setting of medical education and standards, medical school accreditation and having a robust
complaints handling process, the GMC works through every phase of a doctor’s professional life. The GMC Services International (GMCSI) has been established to support the core services provided by the GMC globally, delivering advisory services through a non-UK-centric model.
At the centre of every healthcare system is a secure regulatory framework, surrounded by implementation processes and structures. The GMCSI o ers a peoplecentred approach, with patient safety, workforce supply, governance and quality as standard. The knowledge base behind the GMCSI allows for flexibility through
experience, o ering tailored services to improve the landscape for all healthcare professionals and thereby improving patient safety.
Helen Featherstone, General Manager of GMCSI, works closely with International Ministries of Health and Regulators to identify opportunities for more e ective regulatory systems. “Ethical guidance is the core of regulation,” she says. “We focus on prevention rather than punishment, and on culture, values, teamwork and leadership as well as process and standards.”
This approach allows the cultivation of a patient-focused culture within a healthcare system to improve safety, access, quality and consistency across highly diverse workforces in order to ‘professionalise the professionals.’ In delivering programmes
GMCSI is able to access the GMC’s pool of 1,300 sta and a further 1,000 associates.

By creating supportive environments and nurturing healthcare workers through their professional journey, and by using the subject matter expertise of the GMC, GMCSI is able to provide structures to maintain and improve standards. These structures form an important component of the overall healthcare system and places healthcare practitioner regulation at the core.
“Medical doctor registrations ensure all practicing professionals in the region are suitably qualified, and regulators can maintain contact with registered doctors through the revalidation process which take place every 5 years,” she says. Medical doctor registration and revalidation are two important elements of successful regulation. Other elements include the regulation of medical education and the handling of complaints made against medical doctors, called Fitness to Practice (FTP). E icient data tracking of the medical doctors’ journeys during their careers feeds into the overall healthcare system, enabling input into workforce planning as well as the calculation of medical school placements, to mention a few examples.
GMCSI has o ered advice and guidance on setting up robust registration and licensing processes to a number of countries which
promoted revalidation as standard to encourage continuous career development for their workforce.

One example looked specifically at reforming an overly bureaucratic process that was unable to deliver the number of licensed doctors needed. The process delayed newly qualified medics from registering and applicants were moving on to other regions before their registration had gone through. The system review led to the implementation of a fast-track system for applicants with certification from other reputable healthcare systems regulators, under the guidance of the GMC. The system took advice on considering appropriate thresholds from other countries and enabled the establishment of an e ective process with a balance between competitiveness and risk. In order to ensure e iciency, a programme to reduce the wait time for primary source documentation verification for the regulation of new healthcare professionals was produced.
Consulting work has also been done in the setting of medical education standards and medical school assessments to ensure these standards are being adhered to. “It is important for regulators to work with medical schools to make sure they are delivering against all the required standards,” states Helen, highlighting the importance of consistent medical education standards across the country to ensure standardised medical education.
In order to deliver a completely comprehensive system, the regulatory framework must go even further.
“Fitness to practice is key, but actually we find the complaints process is of huge importance. It is important for the public to raise concerns over medical treatment received and to have a robust system in place to address these concerns. Serious complaints can then be investigated and action taken if deemed necessary. This is very important for overall patient safety.
GMCSI recently supported a new regulator of healthcare professionals, specifically focused on the processes behind complaints handling. The regulator focused on setting up fitness to practice rules and was given guidance on legislative requirements, as well as dra ing decision outcomes, information handling, detailed triage decision making policy, sanctions and a fitness to practice publications policy.
GMCSI is able to draw on a wealth of experience from the GMC and provides knowledge and guidance for every aspect of the regulatory framework with access to consultants in standards, registration, revalidation, fitness to practice, medical education and director-level executive functions. Regulatory system reviews are crucial, and up to date practices provide the foundations for a stable healthcare landscape. Taking care of this environment provides the best service possible to patients, with patient safety as the core focus at all times. .
These regulatory frameworks set the standards which all medical doctors need to adhere to, thereby promoting trustworthiness and giving patients confidence in the care they receive.
“Ethical guidance is the core of regulation”
Helen Featherstone General Manager GMC Services International

















James Cassidy, Partner Information Law & Governance, Vincent Buscemi, Partner Commercial Healthcare and Head of Independent Health and Care and Dan Morris, Partner – Clinical Risk at Bevan Brittan LLP analyse the current trends and challenges for implementation
Digital and data driven technology continues to revolutionise healthcare at a rapid pace. It


o ers enormous opportunity to transform and future-proof healthcare systems so that they are more a ordable, sustainable and equitable. Utilising digital solutions e ectively can result in lives saved
and improved standards, and provides the ability for healthcare operators to manage and engage with patients in new ways.
Research shows that the COVID-19 pandemic dramatically accelerated the uptake of digital solutions. Now, barely a day seems to pass without news of yet another market-defining deal or
technological first in the world of digital health. But while opportunity abounds, challenges remain so innovators and investors need to remember that the attrition rate in this field can be brutal. With this in mind, we consider some of the trending areas for growth as well as some of the ongoing challenges to uptake and wider adoption in the digital health space.
Ongoing challenges of capacity - whether that be due to seasonal spikes in demand, backlogs in elective surgical lists or congestion surrounding discharge into longer term care packages - mean that

digital solutions that assist healthcare providers to monitor and manage patients safely at home are high on any agenda at the moment. The nomenclature might not be universally agreed but whether we are talking about “virtual wards”, “hospitals without walls” or “remote care”, the core concept is to extend the reach of clinical sta , liberating time and space, while allowing patients to benefit from the comforts and familiarity of care in their own homes.
We o en hear about the potential risks associated with the adoption of technology in these new delivery models, but they need to be balanced against e iciencies in the way in which the care can be provided. There are numerous pitfalls associated with inpatient care which are minimised through the use of remote care including reductions in the risks associated with infection control, muscle wastage, pressure sores and general deconditioning. Remote monitoring, wearables and data transfer platforms that securely allow clinically reliable data to be passed from patient to the treating healthcare practitioner without the need for face to face care are all attractive areas for providers, investors and funders at the moment.
The ability to harness benefits of using Artificial Intelligence (AI) in the provision of healthcare is undoubtedly vast. While AI continues to dominate the news headlines at the moment for potentially the wrong reasons, the use of AI in healthcare provides some very exciting opportunities, particularly in the field of diagnostics. Trials utilising machine learning algorithms to review scans, imaging and analyse test results are already being rolled out in certain areas of medicine with promising results.
AI can enable those in imaging and pathology to optimise working patterns and utilise their time more e ectively. AI can be used to triage and risk rate patients, allowing those who need to be seen promptly to jump to the front of the queue. Equally, AI can be used to filter out unnecessary referrals, again freeing up workforce time to focus on growing the capacity of imaging services.
Another area with high potential is that of systems e iciency. Technologies that can help to analyse and solve problems around patient flow, triaging, sta and clinic rostering, discharge bottlenecking, DNAs and consumable supplies are, understandably, high priority for purchasers of health tech. Digital and data solutions that are able intelligently and safely stratify risk, as well as redirect patients to the most appropriate care settings and resources to the most needed areas, are likely to be big winners in the race for digital adoption.
Digital therapeutics are evidence-based interventions driven by so ware that assist patients to self-manage symptoms and thereby improve quality of life and clinical outcomes. Conditions such as asthma, COPD, diabetes and other chronic health conditions have been targeted as areas where patient empowerment and data ownership can shape behavioural change to improve morbidity. Wearables, alarms and interactive symptom checkers all help to reduce health crises and keep people from having to attend urgent and emergency care settings. The next challenge will be to move this technology beyond purely physical health conditions to support mental health and psychological well-being.
Genomics – broadly the study of genes, their functions and their influence on the growth, development and workings (or not) of the human body – is yet another area where data driven technology has the potential to be a complete game changer. Big data analytics in DNA sequencing, digital genomics support tools and
chatbots that assist with the genetic counselling process are revolutionising an area of medicine that already seemed at the vanguard of scientific possibility.
While the opportunities to dramatically improve the e iciency and equitable access to treatment through digital healthcare are undeniable, there remain a number of significant challenges to be overcome.
When compared to the pharmaceutical industry, the systems, processes and infrastructure relating to the development of digital health solutions is not comparable in its maturity. Strong partnerships between industry, providers and governments will be important to ensure that all relevant stakeholders are able engage in an open and collaborative manner and to identify a shared vision and direction for all to follow.


There is a need for the regulatory standards required of digital health products to be harmonised and agreed across health systems and jurisdictions. Driving innovative and dynamic markets attractive to innovators must be balanced with the need to ensure patient safety. Regulation o en lags behind innovation, the use of AI being a key example, and a sophisticated digital health system must set minimum requirements that can adapt as quickly as the technology.
With thousands of products on the market already, and thousands more waiting
“Innovators and investors need to remember that the attrition rate in this field can be brutal”
James Cassidy Partner, Information Law & Governance Bevan Brittan
“Digital solutions that assist healthcare providers to monitor and manage patients safely at home are high on any agenda at the moment”
Vincent Buscemi Partner + Head Independent Health & Social Care Bevan Brittan
in the wings, identifying those solutions which are truly ground-breaking can be hard. Multiple products will make identical (or near identical) claims about how innovative they are and the benefits they can bring, but this duplication can just cause confusion. Providing clarity on what products really do, how they work in practice and the benefits they bring will drive the ability for providers to adopt new technologies.
Finding ways to ensure that access to digital healthcare is available to all is a complex problem and the desire to grow the uptake of digital healthcare should not come at a cost of widening inequality of access. Furthermore, demonstrating to patients, clinicians and operators that they can put their trust in digital solutions to provide evidence based healthcare will be vital. Many still have reservations about the motivations and ethics behind digital
solutions, so providing transparency around how they work and how data is used will be an important factor in developing trust.
With the wide range of digital health solutions on the market, they must be able to talk to one another. Solutions


which are designed to be used with proprietary so ware result in an inflexible system and one which increases vulnerability to supply chains. With a single hospital potentially reliant on thousands of di erent digital products, developing a universal specification and standards (including minimum safety standards) will be key to ensuring a joined-up healthcare system.
These challenges are not easy to resolve and will require strategies to be put in place to drive innovation in a way that ensures change continues at pace, while providing certainty for all. A starting point will be for all those within the sector to develop and use common language to ensure the discussion can continue and the opportunities are not missed. www.bevanbrittan.com
“Developing a universal specification and standards (including minimum safety standards) will be key to ensuring a joined-up healthcare system”
Dan Morris Partner, Clinical Risk Bevan Brittan





Digital twins can improve the smooth running of the hospitals, says Abhi Shekhar Digital
 Healthcare Lead, Mott MacDonald
Healthcare Lead, Mott MacDonald
In the current economic climate, it’s becoming more and more expensive to build anything, especially a hospital. It’s also more di icult to operate a hospital e ectively, so organisations are looking to optimise their assets and redefine them to meet increasing demand. Combined with a reduced healthcare workforce across the globe, resources are at all time low right across the healthcare spectrum.
“The question is, how do we make better use of what we have?” says Abhi. “It’s about using the data generated across the healthcare system to create adaptable health and wellbeing estates as well as integrating the human experience, which is at the core of it, delivering better outcomes for patients and better experiences for sta .”
The changing face of healthcare as a result of the sudden uptake of technology solutions is actually a benefit. For a start, the patient cohort is now used to the concept of telehealth and is no longer resistant to digital implementation if they can see the upside. Given this mindset change, hospitals can now pivot to redefine their spaces and o erings in a way that maximises the current estates and facilities in an entirely di erent way.
Yet the ageing worldwide population is creating increased demand, and so far the majority of patients don’t have the confident to manage their own health. In the meantime, hospitals need to look at how to design workspaces to support
remote patients and switch between remote and in-patient care.
It’s a journey that is a learning curve for all concerned. Added to this are the challenges of minimising carbon footprint to meet Net Zero targets and reduce operating costs while delivering capital improvements. It’s a squeeze all round, but Mott Macdonald has created a solution that can resolve many of the pinch points.
Once the patient understands the concept of a hospital as a digitally connected community rather than a physical space, the task becomes easier. “It’s about rethinking the mindset and making the journey digital,” Abhi says. “So how do we integrate the building with a digital element? It’s about using the data to make decisions better, faster and cheaper, whether that’s to optimise clinical operations, deliver better patient care, or to improve operational performance and reduce costs from a system perspective.
“The reason we call it intelligent is that, from our perspective, it’s an evolution. The intelligence comes from the data that’s generated at the hospital. Any building can be a smart building if you put enough technology in it, but if you’re not e ectively using technology and harnessing it in terms of how the building adapts to it, then it isn’t intelligent.”
Digital Healthcare Lead Mott
So how do we make it smart? “We have to harness the data about how people move and engage with the building to adapt it for the future,” he continues. “We also have to advance carbon-negative solutions to minimise carbon footprint? Alongside this we have to personalise the experience for patients and users to make it inclusive and compassionate.”
“The key thing is making sure that patient data flows seamlessly across multiple di erent settings. At the same time, it’s important that the sta can see the data so they can deliver a better experience.
It’s as simple as showing that the patient has turned up at the hospital. Once they require a bed, it’s about understanding where the beds are at capacity to ensure the flow is seamless and minimise the wait times across all the di erent aspects, as well as providing accurate information to the waiting patient.”
This information also includes the fabric technologies that are required to make a building work. They range from digital wayfinding, check in kiosks and getting updates on status updates to the patients and waiting lists for the sta - the flow technologies are at the heart of the hospital. Once the correct information is available to the right stakeholders -operational, political, estates or executives - there is an overview of the
“The data transmitted is fed back to the physical twin in real time or near real time to make an effective intervention”
Abhi Shekhar
MacDonald
whole picture which is integrated. That’s what drives an intelligent hospital.
As all this information is gathered, how does the hospital make sense of it? “The Digital Twin is the mechanism to bring together the data, analyse it and orchestrate the di erent technologies across the fabric and flow to support and deliver. It essentially acts as the single source of truth,” says Abhi. “It’s not just a digital copy of a physical asset or a process or system. The key thing is that the data transmitted is fed back to the physical twin in real time or near real time to make an e ective intervention. At a simplistic level, you can have a digital twin of a hospital boiler or asset and you can
then scale that out to the wider energy management to get a complete picture. From there it can be scaled across the entire facility.
“Similarly, this method can be used across an entire clinical pathway. It can be used to see where the blockages are, for example in receiving ambulance patients, understanding bed availability and seeing which patients can be moved from the Emergency Department to free up space. It can be as simple as a dashboard that maps out the patient flow and reveals how to optimise the resources available.”
Understanding the patient flow will enable hospitals to maximise their capabilities. There will be up to 38 per cent fewer emergency admissions

as hospitals expand their ability to treat patients at home. Once patients understand how to manage their own conditions and see where the hospital can be used e ectively, the benefits will be huge.
Alongside this, the digital twin will be in play to optimise hospital resources, inform both sta and patients of processes and flows, creating a better working environment and a more compassionate setting for those in need.
As the UK’s National Health Service approaches its 75th birthday, International Director Ged Byrne discusses new ways for global health systems to access its experience and knowledge via the NHS Consortium
The NHS has seen a huge amount of innovation in the past 75 years - from public private partnerships (PPPs) to pandemics, the rise of the internet and the birth of digital health to the beginnings of genomics and personalised medicine.
It saw the first IVF baby born and the earliest hand transplant take place.
It conducted the world’s first mass vaccination programme, for diphtheria and polio, in 1958 and it was the first health system to initiate the latest, for COVID-19 in 2020.
In nearly 75 years it has seen its share of mistakes, mis-steps, learning and lessons. It has amassed a huge amount of data, IP and experience, both right and wrong, in the delivery of universal healthcare.
But there is always a long way to go on the journey to outstanding.
With a huge amount to learn and share, the NHS o ers an opportunity for health systems around the world to benefit from its experience. Through the NHS Consortium we have created an easier way for our international partners and friends to access the knowledge, expertise and

experience of our 75 years, while also giving us the facility to access their examples and opportunities for our own health system.
For the last 10-15 years the NHS has started to forge partnerships around the world. My own team at Health Education England (HEE) has worked extensively creating earn, learn and return programmes in Africa, the Middle East and South Asia. Individual NHS providers such as Imperial College Healthcare NHS Trust and Great Ormond Street Hospital have provided consultancy work and knowledge to their colleagues across the globe. Our ambition is to build on these strong foundations to create a single, broad and welcoming front door to the NHS for the international healthcare community.
The new NHS Consortium initiative, launching at Arab Health, will help
international healthcare leaders to reach into the NHS and be provided with expertise, partnership, collaboration and friendship. The aim is to help build and develop existing health systems, enhance the NHS and create long lasting alliances to help face down the global health challenges of the future.
In 2023 the re-organisation of the NHS will mean that some of our nationwide functions will merge.
My own department at Health Education England along with NHS Digital, our national public health function formerly known as Public Health England, our regulators at the Medicines and Healthcare Products Regulatory Agency and the National Institute of Clinical Excellence, along with our regional bodies for Scotland, Wales and Northern Ireland, will become a new ‘NHS England’.
As part of this merger, this body will sit within the centralised NHS and provide

international engagement and partnership for international opportunity, both commercial and philanthropic.
With ‘bottom up’ engagement from individual NHS trusts and organisations paving the way, and continuing to create opportunities for partnership, the NHS Consortium will create a ‘top down’ approach to engaging with the NHS for global partners.
Our hope is that we will have global conversations at every level, from Governments and health systems to operators and payors, to discover where our common problems and challenges lie. We will also explore how we can assist each other to deliver high quality universal health coverage worldwide.
By identifying the right individuals, experience, IP and, most importantly, the right peer to peer conversations we will shed light on mutual ways to help each other. Enabling other healthcare systems to learn from our successes and failures in the UK will ensure that our own knowledge and understanding of di erent global approaches are up to date.
It is only through direct consultation and collaboration from peer to peer, clinician to clinician, educator to educator and administrator to administrator that we will learn where we can have an impact through vital transfer of learnings.
The key to this engagement and activity is to understand what the NHS is and what it o ers.
• The NHS is the national healthcare system of the United Kingdom
• It is free at the point of delivery and provides universal health coverage to the entire population of the United Kingdom
• It is not an international clinical operator

While the NHS is made up of a multitude of provider organisations (or Trusts) that span everything from primary care to mental health and acute & specialist hospitals, it is not (by and large) an international clinical operator. In rare cases individual NHS trusts may get involved in operational partnerships outside the UK with overseas providers, but this is very much not the norm.
•It is a global knowledge partner
The NHS is an organisation with a wealth of knowledge, IP and experience that can be shared for the benefit of patients everywhere. By discovering the ways in which other global systems have dealt with their issues, the NHS will acquire valuable tools to move forward. Such is the nature of true partnership.
•It is philanthropic
Our partnerships extend to working with aid agencies, the WHO and across the world to support e orts to ensure universal health coverage for all, even the poorest in our global society.
•It is also commercial
The NHS also o ers paid-for consultancy. It has the ability to use knowledge, experience and IP to provide commercial and paid-for solutions to providers, Governments and payors across the world. Our knowledge and advice is not theoretical; it is real and practical, based on 75 years of valuable lived experience.
•Most important of all, we are listening and we are open for business
It’s about conversation, discussion and opportunity. Contact me, my team or our partners at Healthcare World and let’s have a conversation about where the NHS fits into your health systems, your plans, your aspirations and ideas.
kevin.miles@hee.nhs.uk
“The aim is to help build and develop existing health systems”
Ged Byrne International Director HEE
The UK has healthcare data on 65m people. That’s a phenomenal amount of information and, as a nation, we are only just beginning to work out what we can achieve with it. But big data is one thing; ordinary data is another. We all have data; we are learning how valuable it is, and now we have to begin to share it.
In the UK, we’re historically inclined to resist information sharing. We must be one of the few European countries not to have identity cards. This doesn’t make sense when we share so much on social media. In fact, having identity cards would make more sense because then we could limit what information we share. And we’re also pathologically resistant to sharing our health data, despite the fact that it could deliver countless benefits if we did.
This isn’t just an individual bias; it’s also an institutional issue. Although most people think the NHS is one big national health service, it’s actually a group of di erent health trusts, ALBs, quangos and more that make up our medical provision. Each one has autonomy over its spending and decision on technology, with little national oversight.
So, as a GP in the north of England, we store our health records on two systems. There are a multitude of
 Dr Patrick Wynn
Dr Patrick Wynn
so ware add-ons and they come and go. Some are designed to optimise prescribing; some are designed to identify patients at risk; some add-ons are designed for accounting. Our principle system is SystmOne. There are a few others, but the problem is that they don’t communicate with each other.

This means that if a patient from one practice arrives at another practice, the doctors cannot see the patient history. That’s just madness. And the really big failure of communication is between di erent health care providers in terms of primary care, secondary care and the independent sector, none of whom have a common system.
In a hospital, there might be a laboratory that does cardiac scans with a scan machine that comes with its own so ware. The so ware will produce a report, but it has no mandatory requirement to directly communicate with the GP system or the hospital systems. As the patient’s GP, I cannot see it. But the patient assumes that I can, so I have to request it and this all takes time. And as we know, time is of the essence when it comes to medical symptoms.
Again, as a gynaecologist, when I sit as a specialist in a hospital, if I decide that a patient needs a tablet,
I specify a tablet and dose, dra a letter which is sent, albeit electronically these days, to the GP. Someone reads the letter and manually enters the data onto the patient’s notes in the computer system. This is pure duplication - I could have entered that data on a single system and not needed to waste anybody else’s time. And I could have typed up my own records and there would be no letters to be sent, no opportunity for losing information or sending it to the wrong place. It would be so much more productive.

From birth, every person in the UK is allocated a GP. This dates from the founding of the NHS back in 1948. It’s a di erent world today and everyone should be able to hold their own patient record on their phone, allowing them to opt in and out of sharing, access appointments, results and see their own health data.
If someone comes into the surgery or hospital unconscious, as a doctor I should be able to access their medical records to see if they have any allergies or other issues. But I can’t. So other countries should take a look at the issues the UK has, as they have huge potential to be overcome. There’s an inordinate amount of productivity gains that they would have over the current NHS operating systems.
I don’t advocate one system holding all records, just a common language that means all data can be accessed whatever system it is stored on. Rather like
the internet allows us to book a hotel on the other side of the world, no matter what operating system we use. The patient gives permission for their data to be used and they can be treated quickly and e ectively with less risk. The clinicians or provider can treat the patient immediately, confident they have all the requisite knowledge to do so. It’s as simple as that – and there are companies out there that have the solutions to do this.
In some countries patients can self-source specialists. But if they see a consultant for one issue, and a di erent one for another issue, is there a mechanism for the records to be combined? How much easier it would be if there was one central place to find such vital information.
I speak from the heart as an overworked and underresourced UK GP. Yet I do have experience and I hope my thoughts and insight are valuable. I hear that the Middle East health authorities are looking at primary care seriously as a gatekeeper for secondary care. Our role as GPs is to deliver preventative care, ensuring that appropriate cases are referred. With carefully curated systems, the Middle East could deliver the ideal primary care system that would be the envy of more established systems in other parts of the world.
Trial participation should enable balanced representation of the ethnic and racial diversity of the geographic locations where clinical trials are taking place, says Mike Failly Founder and Managing Director of Zanteris
Wellbeing is a combination of mental and physical health that a ects our environment, biology, social policies, behaviour, and significantly our lived experiences. The personal experiences of citizens in the United States di er based on their ethnicity and race, geographic location, socioeconomic status, gender identity, sexual orientation, and other socio-demographic features. The team at Zanteris has been
exploring the importance of diversity and representation across clinical trials to see how far personal experiences and sociodemographic features impact the results.

Clinical trials provide the foundations for assessing the safety, e icacy, and value of clinical treatments and devices, from diets, surgeries, drugs, behavioural approaches,
and lifestyle interventions. As the only way to ensure evidence for the safety and e icacy of new interventions or treatments are gathered, clinical trials play a vital role in the medical field. Some groups of patients might react di erently to specific treatment; for instance, women might respond another way than men - sex, age, race, and ethnicity can all impact how communities respond to a product or device.
To account for the various experiences and exposures of di erent communities, it is important to ensure that trial participants are representative of all communities and groups, enabling a more complete view of the e ectiveness, e iciency, and safety of each product.
Many people experience similar illnesses di erently. It is crucial that clinical trials
consider the combination of living conditions and personal experiences of a community, as well as other factors so that all individuals benefit from medical advances. Clinical trials do not always recruit participants that represent a community heavily a ected by a specific medical condition, behaviour, or disease, and on a general basis, evidence shows that these trials rely heavily on white male or female participants.

However, this lack of diversity and inclusion has created gaps in understanding conditions and diseases, preventive factors, and the e ectiveness of treatment across society. It also causes obstructions in the quality of decision-making, as well as in the methods for lessening risk, optimal treatment reactions, and the creation of e icient medications.
Ensuring diversity in clinical studies is a matter of fairness and impartiality. It is essential that trial participation is inclusive,
enabling balanced representation of the ethnic and racial diversity of the geographic locations where clinical trials are taking place. This leads to a global view of the epidemiology of the illnesses which are being treated.
“There are groups of being who aren’t included in clinical trials at the moment, but they can contribute a lot,” says Mike Failly. “It’s about expediting the trials as, with a greater population pool, the trial can be completed much more quickly. Time is money in the pharma industry as each new successful drug will be sold in the millions. It will also enable the trial population to have equitable access to the drugs they have trialled.”
Zanteris is dedicated to addressing practical and informational obstructions in clinical study participation to much wider representation. “We are committed to designing clinical studies where enrolment can mirror the ethnic and racial diversity of the geographic locations where these studies are performed and the epidemiology of the illnesses under investigation,” says Mike Failly.
The Middle East presents a large and varied population and, due to its presence on the global stage, it encourages large expat communities and immigrants. The UAE alone is home to over 200 nationalities, yet the region is seen to have low contribution rates to clinical trials. Reports show that the region only hosts six per cent of all worldwide registered trials, and more than 76 per cent of interventional trials taking place in the UAE are sponsored by the pharmaceutical industry.
Yet the UAE is especially well positioned to become the leader in clinical trials in the Middle East, with Abu Dhabi presenting an
attractive environment for international life sciences corporations. According to news reports, the UAE was one of the first countries to engage in clinical trials of coronavirus vaccines and Abu Dhabi made over 300,000 COVID-19 RNA extraction solution samples. With its small ethnically diverse population, it’s the ideal jurisdiction to conduct diverse clinical trials, in turn enabling the fair promotion of health equity, producing more innovative science, and reducing biases in clinical trials.
To promote clinical trials in the Middle East, Zanteris is supporting diversity-focused public policies, encouraging investment among the community. Zanteris is also promoting pharma and biotech clinical trial populations, encouraging a range of participants by building trust and collaborating on accessible information drives.

When participants choose to engage in a clinical trial, they are serving as representatives of their own community. The decision to take part in clinical research is personal and must be made in discussion with a professional health provider and an internal support network.
Advancing inclusive clinical trials or research is multifaceted and involves genomic particulars, as well as the interconnected social drivers of wellbeing. For Mike, achieving a wider range diversity, equity, and inclusion in clinical trials needs nothing less than a worldwide commitment to varied, equitable, and inclusive research, which can result in enhanced medical intervention or treatments for various communities.
By involving every community in trials, not only will research become more equitable and e ective, it will also become more widely available, enabling global access to life changing innovation and technology.
Click here for more information and to read the full White Paper: https://www.zanteris. com/wp-content/uploads/2023/04/ Diversity_Whitepaper_Zanteris_031323.pdf
https://www.zanteris.com/wp-content/uploads/2023/04/Diversity_Whitepaper_Zanteris_031323.pdf https://www.zanteris.com/wp-content/uploads/2023/04/Diversity_Whitepaper_Zanteris_031323.pdf https://www.zanteris.com/wp-content/uploads/2023/04/Diversity_Whitepaper_Zanteris_031323.pdf https://www.zanteris.com/wp-content/uploads/2023/04/Diversity_Whitepaper_Zanteris_031323.pdf https://www.zanteris.com/wp-content/uploads/2023/04/Diversity_Whitepaper_Zanteris_031323.pdf https://www.zanteris.com/wp-content/uploads/2023/04/Diversity_Whitepaper_Zanteris_031323.pdf https://www.zanteris.com/wp-content/uploads/2023/04/Diversity_Whitepaper_Zanteris_031323.pdf https://www.zanteris.com/wp-content/uploads/2023/04/Diversity_Whitepaper_Zanteris_031323.pdf
“There are groups of people who aren’t included in clinical trials at the moment, but they can contribute a lot”
Mike Failly Founder & Managing Director Zanteris
Our clients receive accelerated support to quickly identify the biggest, most solvable problems from a team of experts willing to pull a chair up to the table, roll their sleeves up, and identify the issues being faced. This collaborative environment results in rapidly providing recommendations and partnering to execute on the solution.
It’s not about us; it’s about you –and what is impactful to you.
We support our clients with data analytics and deep expertise. We help to identify problems, solutions and appropriate action. We enable our client’s success. We partner with your clinical and operational experts in the organization.

Data and actionable insights underpin everything we do. We are adept in recognizing and extracting the value of the data that exists in the healthcare industry, and in utilizing it to create, realize and protect value. We ensure your data is in sight.
Our work ethic and consistent delivery are built on an equally consistent data-lead discovery and prioritization process that leverages analytics in every initiative. While we often custom-build or tailor analytics for clients, we also use key digital solutions that focus our delivery to drive material impacts in cost, quality, and care.
We weave together our services with data, and technology, and our client’s resident expertise in these key areas.
Our clinical and quality experts partner with our client’s team to illuminate trends, opportunities, and outcome potential. Using internal and external benchmarking, we help highlight and guide improvement efforts that transform patient outcomes, public quality report card performance, and pay-for-performance programs. Our dynamic platform also allows for risk and disparity stratification of quality measures.
We partner with our clients to design value-based care programs, including measure construct, risk adjustment, and payment methodologies, as well as implementation of systems, service-line agreements, and narrow networks to drive coordination of care. We use dynamic analytics to highlight blind spots and areas of opportunity in their population and prioritize value opportunities.
is more than a consulting rm.
Our experts provide rigorous analysis, seasoned advice, and practical action, working hand-in-hand with our clients to deliver practical data analytics.Kristen Geissler Managing Director kgeissler@thinkbrg.com Julie Coope Senior Managing Consultant jcoope@thinkbrg.com
Our most powerful outcomes occur because we use our proprietary digital platform to combine data, people, and process. Symphony, a BRG product, allows us to provide quick insights, recommendations, and action plans directly tied to your data inside of our solutions. A targeted team of experts dive deeper into the data to provide insightful understanding, context, and prioritized action plans directly integrated with your data and our analytics tools. This provides real value more quickly than large teams of junior consulting staff who create ad hoc analysis and static PowerPoints.
Symphony unlocks your best thinking with our features, designed to make data-driven decision-making faster and easier:








Symphony provides a single, curated place for all analytics. And, you can connect all of your Tableau, Qlik and Power BI tools to create a richer analytics and storytelling experience beyond BRG’s solutions.

Our experts-- or your clinicians and/ or analysts-- add their narrative to instantly saved “slices” of data directly in Symphony. No time is wasted on static screenshots or slides. Bookmarks can be shared to individuals or groups to provide a unique reporting “view.”
Combined data and insights create the power and influence required to change. Data collaboration has immense value, with a range of use cases including analytics feedback, Q&A on quality control issues, and data-driven decision-making processes.
Using Symphony for digital delivery and collaboration led a client to 2,047 bed-day savings and 9.2M AED cost reduction in a single pathway.
Outcomes:
- Improved efficiency, productivity, and quality of care
- Increased clinician engagement
- Enhanced patient experience


Data needs a good narrative and vice versa. Symphony combines both to tell your story to the world without extra presentations, emails, and meetings. Data and decisions move quickly, so the way that you share perspective and buyin should be equally fit for purpose.









collaboration
storytelling: inform, in uence and inspire at scale.
Robotic Surgery in the Middle East is coming of age says Mansoor Ahmed, Executive Director – Middle East & Africa (MEA) Region at Colliers
The Middle East healthcare sector is going through a rapid expansion and transformation. Increases in population, income levels, life expectancy, along with lifestyle-related and non communicable diseases (NCDs) have caused Middle East countries to be ranked among the top 20 countries in world for the highest level of obesity, hypertension and diabetics. Facing these challenges, regulators, providers, payers and patients,
both in the public and private sector, are focusing on to improve the overall provision of the healthcare o ering the region.
Many regional governments have initiated and implemented positive reforms which are pivotal to improve the overall quality of healthcare services in the region and have resulted in increased private sector participation. These reforms include PPP initiatives, mandatory health insurance
and other initiatives to bridge the demandsupply gap.
Of late, especially a er the pandemic, a lot of emphasis is being placed on bringing in and implementing new technologies. There is also increased focus on specialised care models, such as genome sequencing, stem cell therapies and clinical trials with focus on virtual health, artificial intelligence (AI), wearables, blockchain and precision medicine.
Beside these and many other initiatives, robotic surgery in the region is coming of age with many healthcare providers both public and private beginning to o er robotic surgery as an option to patients. The benefits of robotic surgeries include better visuals compared to traditional

techniques by providing highly magnified and resolution vision of the operating field, resulting in physicians enhanced precision, higher flexibility and range of motion and dexterity, and more control during the procedures.
For centuries, surgeons have operated using large incisions to gain a full view of the organ they need to operate on the patient. Recovery time for such taxing procedures is extensive and post-operative complications are a common occurrence.
The introduction of Minimally Invasive Surgery (MIS), also known as keyhole surgery or laparoscopy, has drastically

improved patient outcomes. Using smaller incisions, the risk of infection can be reduced and recovery can be accelerated. Many studies have shown that MIS results in decreased post-operative hospital stays, quicker return to work, decreased pain and better immune function.
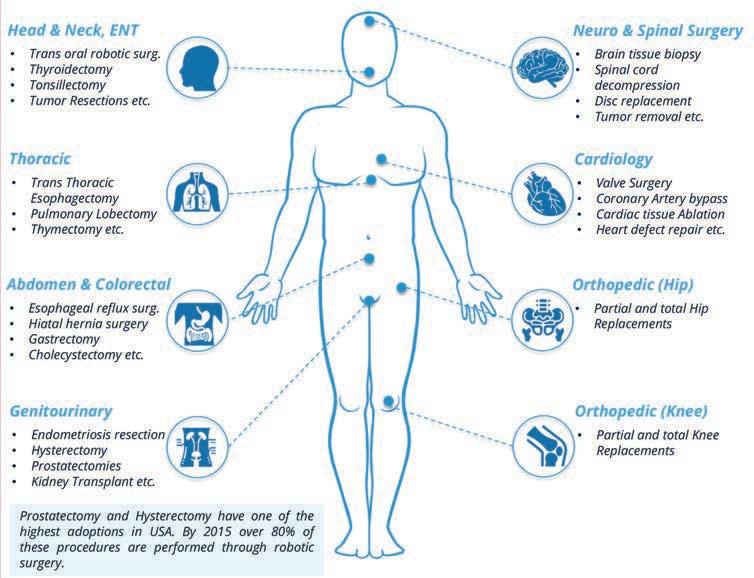
However, there are several drawbacks to MIS due to the technical and mechanical nature of the equipment. These limitations make MIS procedures more challenging, reduce their e iciency and increase operating time.

Computer-assisted surgery was developed to overcome the limitations of MIS and to expand its benefits. Classified as a type of MIS, it involves the use of robotic systems to execute surgical procedures. Although robotic surgery has technically been around for more than 30 years – the first documented robotic surgery was performed in 1985 - it has not been widely implemented in medical settings. However, in last 10 years or so, the robotic surgery market has expanded rapidly due to advancement in technology and increased acceptability across the globe. Based on various estimates, the global surgical robotic market was valued at between $7 billion to $8 billion in 2022 and is expected to reach $18 billion to US$ 20 billion by 2030.
Presently, around one million robotic surgeries have been performed worldwide with 75 per cent of the procedures performed in the USA. Robotic surgery was first introduced in the Middle East in Kingdom of Saudi Arabia in 2003, followed by Qatar in 2010, and Kuwait and UAE in 2014.
There are close to 50 Da Vinci surgical systems installed in the region. Saudi Arabia has the highest number of
“With robotic surgery becoming the new standard of care globally, the private sector in the Middle East, especially in the UAE & KSA, is catching up with the trend to provide this cutting-edge technology to the regional population”
Mansoor Ahmed, Executive Director (MEA) and Head of Healthcare, Wellness & Life Sciences MENA Region at Colliers
installations with 19 Da Vinci surgical systems and 930 documented robotassisted procedures performed between 2004-2010. The Middle East witnessed an increase in robot-assisted surgeries by 60 per cent between 2011-2017.
In the UAE, the Ministry of Health and Prevention (MoHAP) is a pioneer in adopting and encouraging robotic surgery. In 2014, MOHAP announced the launch of the first robot for catheterisation and cardiac surgery through computerised systems in Al Qasimi hospital, Sharjah. Rashid Hospital in Dubai under the governance of Dubai Health Authority (DHA) also adopted robots in cardiac surgeries.
With the successful use of robots in heart surgery, MOHAP initiated the Gynaecology and Obstetrics Robotic Surgeries Programme in 2019. During that year, MOHAP performed 126 robotic surgeries in six clinical specialties. The robotic systems are installed across di erent facilities of MOHAP such as Al Qasimi hospital - Sharjah, Kuwait Hospital and Dubai.
Abu Dhabi Health Services Company (SEHA) also adopted robotic surgery in its Sheikh Shakhbout Medical City (SSMC) and performed its first robotic surgery in 2020. Dubai Hospital has launched the Da Vinci Xi Surgical Robot for performing robotic assisted minimally invasive surgeries in 2022.

With robotic surgery becoming the new standard of care globally, the private sector in UAE is catching up with the trend to provide this cutting-edge technology to the UAE population. The focus is on the treatment of gastrointestinal surgeries, thoracic surgeries, gynaecologic surgeries and heart surgeries, with a focus on prostate cancer, digestive diseases, urological procedures, hysterectomy and mitral valve in the UAE.
In Dubai, robotic surgery was introduced in the private sector by American Hospital in 2020. Currently Mediclinic Hospital, Saudi German, Al Zahra and Clemenceau hospitals have robotic surgery platforms to cater to patients across di erent specialties. Cleveland Clinic performed its first robotic surgery in Abu Dhabi in 2015 through its Da Vinci system, while Burjeel Hospital has launched E-GPS Robot for spine surgeries.
Robotic surgery in the region is expected to grow exponentially in the coming years, with the UAE and the KSA to take the lead. Robotic surgery has great advantages over traditional and laparoscopic surgical methods by o ering greater precision, reduced bleeding, smaller incisions leading to smaller scars, reduced hospital stay and less chances of hospital acquired infection. With healthcare moving towards value-based care and implementation of mechanisms such as Diagnosis Related Groups (DRGs), the cost of complications and longer hospital stays must be absorbed by the hospital and not the insurer. With the advantages o ered by robotic surgery, in terms of better clinical outcome and reduced hospital stay, the hospitals will benefit from reduced patient care costs. Moreover, the growth of robotic surgeries increases ROI as a result of better medical outcomes and increased bed turnover, superior e iciency and lower costs, providing a competitive edge compared to competitors that can attract medical tourists and capture medical tourism outflows from the region.

We organise virtual events that bring the world of healthcare to your office or take you from your office to healthcare events all around the world.
We organise our own major events like Vision Health 2023 with the Saudi Government and we create networking events in the fringes of major global healthcare gatherings like Arab Health, HIMSS and Africa Health.
Above all we help our customers and friends enter new territories, supporting them with everything from content and marketing through to market scoping, product development and cultural fit.
Healthcare World is the world’s leading magazine for the business of healthcare, but we’re also far more than that.
The Yorkshire and Humber Academic Health Science Network is transforming healthcare by nurturing new technologies as part of the innovative networks established by NHS England to transform healthcare

The Yorkshire and Humber Academic Health Sciences Network (AHSN) is one of 15 AHSNs in England created to operate as the key innovation arm of the NHS. Across the country, AHSNs are building a pipeline of solutions for the NHS by acting as a bridge between healthcare providers, commissioners, academia and industry. The relationships and in depth understanding of the UK healthcare
ecosystem from AHSN’s give healthtech companies unique insights and pathways into the NHS. As the world’s largest single payer for healthcare, the NHS presents a substantial market for international healthcare companies.
Propel@YH first opened its doors to UK innovators in 2019. Since then, it has supported more than 45 companies. UK based innovators receive a six-month course of structured support and advice to help
them navigate the complexities of entering the NHS, increase market presence and accelerate their growth.
The Propel@YH Boot Camp was subsequently created in 2022 and has been designed with international healthtech SMEs in mind, o ering a week long accelerator programme to companies outside the UK. The five-day programme gives innovators a crash course on the UK market. The Boot Camp provides a series of intensive support and timetabled masterclasses from expert partners to promote direct engagement with local NHS stakeholders, as well as the wider regional ecosystem.
Each Boot Camp is customised to accommodate the specific needs of the cohort, providing a tailored series of masterclasses and advice. Through their partners, the Propel@YH Boot Camp is able
to o er a comprehensive support system to all SMEs involved. The Yorkshire and Humber AHSN and Leeds City Region Local Enterprise Partnership gives an overview of the region and expert local insights as an introduction to the Boot Camp. Partners including the Barclays Eagle Labs, Hill Dickinson, Nexus at the University of Leeds and West Yorkshire Health and Care Partnership provide investment advice, legal support, research and business services and guidance on sustainability and environmental impacts.
In addition to their partners, Propel@ YH have a range of supporter organisations including:
•Orcha, who deliver a masterclass on digital standards and compliance, digital technology assurance criteria and technical documentation
•HMA provides guidance on marketing and communications, including branding, identity and positioning alongside website development and social media management in the UK
•Thrive by Design outlines the complexity of the NHS, clinical safety by design, building an evidence base for innovations and inclusive digital design
•6B Digital focuses on the interfaces of interoperability across the NHS, looking at healthtech interfaces and systems integration

•The York Health Economics Consortium provides insights on the importance of real world evaluation and the economics of healthcare
In addition to these sessions, participating innovators have the opportunity to pitch and engage by networking with clinicians and stakeholders from local and regional health care organisations.
As one of the five US based SMEs selected to participate in the 2022 Propel@YH Boot Camp, Behavidence has established itself in the UK market.
Behavidence is a mental health app using AI to monitor mental health conditions by analysing mobile interactions which generate a mental health score which is then compared with that of other people diagnosed with ADHD, depression and anxiety. The app helps to identify the risk of conditions relapsing and provides screening as well as remote monitoring for clinical interventions if necessary.
Through Propel@YH, Behavidence was able to access advice and support from UK healthcare experts, understanding the NHS governance, procurement and financing frameworks. Through key stakeholder interactions, Behavidence was connected to the right support to evaluate their technology and its suitability to the UK market.
“The programme helped us to seek out other opportunities and helped us realise there’s a lot to do and even more opportunities in the North of England, rather than taking the classic route of settling in London,” says Roy Cohen, co-founder and CEO of Behavidence.
The company is now successfully established with an o ice in the Nexus community, part of the University of Leeds, and plans to expand their UK
team to support their growth plans. The support provided by Propel@YH has led to Behavidence generating investment and building a support network across the region.
Award-winning US based digital health platform and music app SingFit has been designed to support improved wellbeing through music. The therapeutic benefits of music provide a basis for the app’s work with Alzheimer’s, dementia, aphasia and Parkinson’s disease. SingFit technology provides a cost e ective and successful treatment used in cognitive behavioural therapy, speech therapy, occupational therapy and other cognitive decline therapies. SingFit also provides support and solutions to users su ering from the e ects of depression and social isolation.
The Propel@YH Boot Camp champions the adoption of digital solutions to improve health outcomes, as Rachel Francine, CEO and co-founder of Musical Health Technologies found.
“The speed of our UK launch was really fuelled by the information we gathered at Yorkshire and Humber AHSN’s international Boot Camp.”
Through the Boot Camp, SingFit was introduced to pilot partners, as well as supporting their regulatory approval journey by helping them to define and articulate their o ering to an audience of key UK stakeholders. “The AHSN brought together the players with knowledge that allowed our team to very quickly assess how long it would take to launch SingFit solutions in the UK and the resources it would take to do so.
“This knowledge, along with the introductions they made significantly compressed the amount of time and energy it took to assess that the SingFit platform and UK health systems are highly aligned in terms of product market fit.” Rachel adds. “A er the Boot Camp, the AHSN has continued to help us, strategically and tactically to bring SingFit’s therapeutic music solutions to the UK.”
Paul Johnson, Founder and CEO of Radar Healthcare, discusses how organisations can improve patient safety through technology
The World Health Organization (WHO) defines patient safety as the ‘reduction of risk of unnecessary harm associated with healthcare to an acceptable minimum’. Striving to embed patient safety within the culture of organisations has now become a significant concept for healthcare services across the globe in order to make a positive impact on the service and the care that they provide.
Patient safety failures are known to be extremely costly, dwarfing the costs of prevention. In the UK, of the entire healthcare budget for the NHS (National Health Service), clinical negligence claims have historically consumed about 2 per cent (BMJ). Therefore, if these were to be reduced, significant cost savings could be achieved.
Radar Healthcare works with several UK hospital trusts, aligning systems to create a single working interface that delivers both cost and time savings. User-friendly, compliant and transparent, it is a solution chosen most recently by Guy’s and St Thomas’ NHS Foundation Trust, starting in April this year, to integrate their risk management so ware systems across the whole Trust.
Health and care organisations across the world are facing the pressure of delivering high-quality, safe and e ective care to growing populations, with resources becoming increasingly stretched in an everchanging regulatory environment.
Radar Healthcare’s award-winning so ware takes a risk-based approach to managing quality and compliance. It supports the patient safety agenda and enhances health and care through comprehensive, innovative and personalised services that promote inclusivity and tolerance.
The Patient Safety Friendly Hospital Initiative (PSFHI) was created by the WHO to help and support healthcare organisations to launch a cohesive patient safety programme. It looks at five main domains:
• leadership and management
• patient and public involvement
• safe evidence-based clinical practices
• safe environment
• and lifelong learning
Health organisations such as the WHO, National Patient Safety Foundation (NPSF), the Joint Commission International (JCI), and the Institute for Health Care Improvement (IHI) are actively asking healthcare organisations to develop a culture of safety as an e ective strategy for improving patient safety.
The UAE’s Ministry of Health and Prevention (MOHAP) has commissioned Radar Healthcare to deliver its quality and compliance so ware to 17 hospitals and 72 primary care centres across the region. The system, delivered by local partner Memits Solutions, supports them in delivering clinical incident reporting and patient safety outcomes.
Such advanced regulatory compliance so ware helps health and social care organisations to have full visibility of all compliance processes to stay on top of patient safety, learn from previous incidents and events, handle complaints and compliments, monitor workforce compliance, improve services to reduce the risk of reoccurrence, and more.
A report by the OECD in 2017 entitled‘The Economics of Patient Safety’ strengthens a value-based approach to reducing patient harm at a national level. It highlighted that the 14th leading cause of the global disease burden (the impact of a health problem as measured by financial cost, mortality, morbidity, or other indicators) is estimated to be patient harm, comparable to diseases like tuberculosis. In some countries, patient harm is an even larger burden, comparable to diseases such as multiple sclerosis and some types of cancer.

It is thought that in OECD countries, 15 per cent of hospital expenditure and activity are caused by treating safety failures. It
is important to remember that there are knock-on e ects from adverse events, like the loss of trust in health systems. These issues are healthcare-associated infections (HAI), venous thromboembolism (VTE), pressure ulcers, medication error, and wrong or delayed diagnosis.
The reports identified that better policies and practices need to be in place to prevent harm and drive the quality improvement of care. Prevention programmes for issues such as HAI and VTE are much cheaper to run than paying for the financial burden they cause.
Fundamental system-level items should be invested in as a start, such as education, training, and safety standards, forming the foundation of a national value-based approach where harm is reduced using limited resources.
An integrated patient safety strategy involves adopting a positive safety culture for all involved. Clinical governanceframeworks are critical, as well as listening to the patients. A patient

safety technology partner should provide the potential for continual improvements and sharing best practice.
Technology-powered healthcare can support the quest for excellence through incident management, risk management and audit management so ware, as well as quality improvement plans and workforce compliance. In this way healthcare providers can improve patient safety, reduce risks, know they are compliant, increase productivity and delivery of care through quality assurance and operational e iciency.
There is a real need for joined-up, automated, integrated data to be the driving force for this continuous improvement, influencing whether or not an organisation becomes a well-oiled machine. Intelligent analytics plays a huge role by enabling actions to be triggered directly from data,

in real time, by monitoring data patterns and using this data to create events, automate notifications around concerns that need addressing, and improve operational intelligence across one or multiple organisations. It aligns with existing processes; it is interoperable and easy to use. Radar Healthcare is uniquely flexible to support quality, compliance and risk management in all areas of health and social care.

“Clinical governance frameworks are critical, as well as listening to the patients”
Paul Johnson Co-Founder Radar Healthcare
Automation can create a better healthcare ecosystem,
Praful Mehta CEO of Vamstar tells Healthcare WorldThere is a general recognition that the healthcare sector provides huge amounts of data. It’s also agreed that there is a huge amount of waste and duplication of processes, given the complexity of healthcare organisations and the clinical requirements. And again, that many clinicians and data scientists have devoted time and energy to resolving the issues that a ect them most closely.
For Praful Mehta, this has been supply and demand. A geneticist by training, he moved into the industry 20 odd years ago and has played roles in commercialising various products in Asia. He then moved to GlaxoSmithKline globally within the
senior leadership, and for the last decade has focused on pricing access and value in various countries, advising governments and suppliers and buyers in the market on how to create a better healthcare ecosystem.
HW: How is Vamstar di erent from other platforms?
VamStar is the first fully AI based supply chain platform that looks at the demand and supply patterns in the market, and matches to the needs of the local ecosystem. We work in 100 countries and we collect data on the buyers side, looking at the demand from public systems along
with its scope and structure. We then have suppliers in the system matched to that demand. We have a number of tools and technologies built to support that supply and demand and to improve the e iciency of the transaction and trading processes that exist within markets. Much of our platform is super localised from that point of view.
We started the company in 2019 from three co-founders to 150 people today in five countries. We work locally in the UAE and Saudi and we are also expanding significantly in other GCC markets. Similarly in Europe, we work locally in the UK, in many of the countries in in Europe and in the Far East as well.
HW: What was it that you were able to o er during the pandemic that enabled you to grow so exponentially?
Within healthcare, there was a big realisation that digital is the way forward and engaging with the buyers must move digitally, so we leveraged that on the backdrop of COVID. Our clear value is that
costly and manually run processes can be automated with the help of our tools and platform. In addition, both the buyers and suppliers have much better visibility of the market, including pharmaceutical drugs, vaccines, all hospital and care setting medical supplies, and also surgical products and equipment.
Our platform is a two-sided approach on both the supply and buyer side. We set specific companies and organisations on the platform so they can keep their processes completely aligned and scan the wider market. We o er the entire platform as so ware as a service, or SAAS, which means that the buyer or the supplier can access the data at a fraction of the cost.
We work with all major companies, so we are well-versed in large enterprise systems or ERP systems. This inclues procurement systems on the buyer side and with CRM systems on the supply side. It’s very expensive for most buyers and suppliers to gain access to harmonised data, so we do this at scale for them.
We work with local laws and regulations
when it comes to data hosting, data privacy and regulation standards. We follow all local protocols so it’s hyper-fast and superconnected in one single platform.

Large organisations in these regions approached us during COVID for technologies to make them more e icient in their supplier engagement. We expanded quite significantly in the UAE, especially in the private sector - we began with one or two hospital groups and now have up to 70 per cent of all private hospitals on the platform. We are slowly making our way into other GCC markets by working again with large buying groups, bringing the use of analytics and AI in terms of understanding what buyers buy and where they buy.
Many customers focus on common and generic products such as medical supplies and everyday items. They utilise us for specialised products with only one or two select suppliers, and we provide them with the ability to manage their supply chain on the platform.

The real value add is being able to scan the market for comparable products. And in terms of hyper-specialised product, we can provide visibility of products that can improve the level of care, for example in diabetes or in oncology. It’s about an in depth understanding of the products, along with the data, that helps buyers make the right product decisions for the care environment.
We are making investments going forward in Saudi and will be expanding our teams both in Saudi Arabia and in the UAE. From our supply chain platform point of view, we are selectively focussed on key markets within GCC, Europe and Latin America, targeting the countries where we see maximum ine iciencies which we can resolve.
HW: What is your vision for Vamstar?
There’s a sizeable amount of waste in healthcare because the same processes are repeated by suppliers and buyers many times over. Our goal would be to aggregate and standardise those processes in a common system to improve e iciencies. This could also mean a common exchange for medical supplies and pharmaceuticals, developing into a clearinghouse for the industry and standardising repeated processes where there is a lack of data. Automation allows this to become leaner and cleaner, meaning better profits for both suppliers and buyers.
As we mature our data and connect systems, this will enable both buyers and suppliers to plan for the future. Not only in regard to products and services, but also when it comes to new innovations and new solutions. It would be around collaborating and even merging some of these products together into one common unified system.
The lack of standardisation is one of the major pain points in healthcare, especially around data, and we are trying to solve this problem. But when it comes to actual utilisation of that data, whether it’s in clinical processes or in supply chain, it’s very limited. We are looking at developing systems and scaling technologies which can utilise that data and improve the quality of care.
HW: Do you see healthcare from global viewpoint?
Yes, there is a lot of willingness to look at health care systems holistically. One big realisation has been that healthcare supply chains are completely intertwined and very complex, and the costs are out of control in pretty much most major markets. We actually see a lot of harmonisation coming up as buyers or healthcare actors are learning from each other.
The UAE and Saudi Arabia in particular are already taking some fast moving forward steps for the future around the digitalisation of healthcare. And we have much to share and learn from the stakeholders as well.
“One big realisation has been that healthcare supply chains are completely intertwined and very complex, and the costs are out of control in pretty much most major markets”
Praful Mehta CEO Vamstar
A specialist consulting company, specialising in all aspects of the regulation of healthcare practitioners
•Registration of healthcare practitioners
•The revalidation process

•Setting of standards and outcomes of medical education

•Medical school assessment
•Practitioner complaints handling process
A wholly-owned subsidiary of the General Medical Council, based in the UK
helen.featherstone@gmcsi.co.uk

From the automation of simple tasks through to AI based programmes, automation must be an essential part of our strategy, says Jennifer Nobbs, Head of International Advisory, Beamtree
As the healthcare service strives for better and more e icient systems and delivery, automation should be at the heart of transformation. There’s a view that automated services seek

to replace human activity and to an extent that’s true - automated services and systems refer to the creation and application of technologies to minimise human input. However, by controlling and monitoring the production and delivery of
products and services, human error can be significantly reduced and care can be delivered in the most e icient and e ective way.
Beamtree’s Global Impact Committee recently released a report, More Time to Care, which highlights the enormous potential of automation and digitisation in healthcare. Automated technologies can be adapted to every hospital and healthcare environment. They range from hybrid systems that combine automated and human activity, such as surgical robots, and fully automated systems,
for example rules-based programmes or AI-driven systems for accurate diagnosis.
Basic automation describes the automation of simple tasks, covering robotic process automation or so ware robotics to carry out back-o ice and administrative tasks. Specific processes can be designed to extract data, fill in forms and collate and send files. These processes can execute specific tasks with speed and precision, with little to no human intervention.
Process automation ensures uniformity through process applications and management, covering appointment scheduling and supply chain management, as well as robotic systems used in pathology laboratories.
AI automation enables programming with logic and rules which mimic human decision-making processes, relying on machine learning which allows the programme to teach itself and make decisions based on solutions it has seen and analysed.

Clinicians spend up to 70 per cent of their time on administration. From the automation of simple tasks through to AI based programmes, automation must be an essential part of our strategy to transform the health system and better support a tired workforce in delivering the best quality care.
In Australia, two doctors at the Sydney Adventist Hospital have built an algorithm to improve patient care delivery.
The Ainso Deterioration Index™ was developed from patient demographics, ward-based observations, lab values and trend analysis to create a model index. Using machine learning, the Index is able to detect signs of deterioration in a patient on a ward, ahead of traditional observation methods.
With the aid of a machine led monitoring system, alerts are sent to ward sta before an adverse event takes place by picking up signs a patient is worsening in advance of even the patient knowing.
Having successfully integrated the technology into a live hospital EHR, the Ainso Deterioration Index™ is saving precious time compared with ward sta identified monitoring and alerting systems.
At the moment, patients are having to wait longer than ever for care. This situation is made worse by the fact that users of the system – both patients and healthcare workers – o en have to navigate ine icient systems. Automation enables not only a more e ective triage system for care, but can provide diagnosis support through AI driven chatbots. Patients no longer need to wait for a doctor to be available; their concerns can be addressed immediately, lowering stress and anxiety levels. The impact of liberating the workforce allows for more concentrated and successful care to those in need.
Unsurprisingly, the healthcare sector has some of the lowest productivity rates while consuming great proportions of national spending, driving the cost of delivering low-productivity care on a huge scale. So it’s clear that the long-term sustainability of healthcare spending is reliant on the productivity gained through automating at least the most basic systems.
The benefits of investing in the automation of administrative processes are unambiguous: e iciency, cost e ectiveness, and liberation of the workforce. Automation will not replace the humans in healthcare, but will provide supplementation for simple and repetitive tasks to enable the highly skilled practitioners room to operate at the top of their skill set to enable more people to be serviced within the current workforce limitations. The success of all healthcare services relies heavily upon transformation, and automation is an essential tool.
For automation to transform the health sector, however, it is essential that it is seen at the heart of systems redesign. This is critical for success.
Clinicians’ time is already stretched and being presented with a new, complex programme can lead to wasted time if it is not welcomed, accepted and valued. So it is essential that automated systems are adopted and integrated with workforce planning, recruitment and training.
Introducing automated services on a piecemeal basis allows each team to adopt the new system and learn the benefits of automation before being presented with a more complex technology. Simple rules-based systems that focus on saving time spent on routine tasks can provide the feeling of liberation, eliminating the threat of the unknown within a team. Encouraging sta to test systems and suggest improvements enables a truly unique relationship with the so ware, and gives confidence to the idea of automation as a useful and welcome tool.
In support of the slow introduction of transformation systems, a culture of openness and transparency is essential. A strong ethical framework must be in place to secure and maintain the trust of sta and patients. Openness about how data is cleaned and structured for use must be clear and accessible. Clinicians should also be provided with a comprehensive understanding of how they should interact with the systems as tools, and how they remain the sole responsibility for clinical decisions.
Clarity and regulation play a major part in the success of automated systems. Firstly, it is essential that the regulation built around the systems is up to date with the technological developments. Developers, clinicians and healthcare organisations need reliable, e ective systems with clear process and evidence requirements, providing transparency and accountability, to give them the confidence to use them.

However, the regulatory framework around these systems is not moving fast enough to accommodate the adoption of automation. It’s essential
that frameworks are in place in order for automation to provide support to the health industry while it struggles under increased pressure in the wake of COVID-19. The regulators need to champion evidenced innovations and encourage the healthcare sector to adopt them at scale.
Healthcare organisations are learning health systems, and automation provides an opportunity to facilitate the better use of data and knowledge latent in these systems, and turn them into action. We must harness the power of automation to pursue our shared goals of error-free healthcare, higher productivity and a better patient experience, and we must support our healthcare professionals to seize the opportunities that automation provides.

“The impact of liberating the workforce allows for more concentrated and successful care to those in need”
Jennifer Nobbs
Head of International AdvisoryBeamtree
What did we learn? Or have we just gone back to ‘normal’ without a thought?
There are clearly some huge positive developments that came out of the COVID crisis. We now know that we can develop an e ective vaccine in an amazingly short space of time. But how much has really changed in our sector? How many lessons did we learn from two years of coronavirus and will we be better equipped for the next global healthcare crisis?
The rise of data and digitally-led healthcare provision also received a huge shot in the arm as a result of COVID-19. We are now in an age where every element of healthcare delivery is digitally driven and the benefits of population health and data modelling for healthcare are known, desired and acted upon in every health system, driving more e icient delivery of care.
But this revolution in healthcare was going to happen anyway. The arrival of a global pandemic has not been the cause of a digital healthcare revolution, but it has hastened its arrival. In many ways that’s just as well, because one of the huge negatives

of COVID has been its e ect on the global healthcare workforce.
An already impending crisis has been worsened massively by the pandemic causing a stressed, demotivated, underpaid and under-appreciated health care workforce. People have le the healthcare profession in droves and we cannot educate people quickly enough to replace them.
The wealthy economies of the globe must learn the lesson quickly that the time is rapidly approaching where health systems cannot rely on cheaper labour from less wealthy economies with a surfeit of supply in nursing or allied health professions. Growing your own workforce will have to become a key plank of the development of any health economy. And that workforce will inevitably become far more expensive. Just look to the current strikes in the UK where an exhausted workforce is refusing to accept that its hard work and e ort through unprecedented times has not been rewarded with the increases in pay and improvements in conditions that they demand.
Another area in which the world has flatly refused to learn the lessons of a pandemic is that of public health messaging. The fact
Steve Gardner Managing Director
that vaccination against a disease that threatened the very existence of humanity has become such a hot topic and divided some many people into pro and anti camps is a sad indictment of our times.
If our health systems need to learn one lesson for the next pandemic, it’s that we need clear, simple and decisive guidelines on what is and isn’t acceptable in the face of a threat from a deadly disease. And this doesn’t mean not giving people a choice about whether or not to be vaccinated. It means making sure that choice is properly informed and that the way in which a society behaves during the darkest days of a pandemic is better policed, clearer and easily understood.
The worst days of COVID-19 are behind us now but, in our rush to return to normality, the concern is that even those of us involved in policy making, decision making, funding and delivering healthcare have all too quickly forgotten the lessons of the pandemic.
There will be another pandemic down the track so will we deal with this one any better? And will we learn our lessons next time?

We are a unique, forward thinking and specialist global healthcare consultancy focused on healthy populations. Together with our clients we are influencing the factors which a ect health outcomes – both in terms of preventative measures and healthcare interventions.

Our experts connect thinking between health and infrastructure – o ering a broad range of skills and expertise to support clients design, plan, implement and evaluate their healthcare services. In all our work, we take a digital first approach.
We have permanent o ces across the GCC, including Saudi Arabia, United Arab Emirates, Qatar, Bahrain and Oman.

Our services and expertise include:
• Strategic and capacity planning
• Healthcare planning
• Service design and reconfiguration
• Digital healthcare and digital hospitals

• Business case development
• Project management
• Built environment and estate strategies
• Facilities management advice
Opening opportunities with connected thinking.





Using real-world data, predictive algorithms, digital biomarkers to advance proactive, predictive medicine. Huma’s technology powers digital ‘hospitals at home’ and decentralized clinical trials.