13 minute read
Growing Your Knowledge – Sysmex Scientific Focus

Growing Your Knowledge
Sysmex Scientific Focus
Sysmex is one of the world’s leading healthcare companies. We work hard to retain these distinctions. One of the ways we excel at what we do is by focusing on knowledge.
Sysmex stands out from other companies in our areas of expertise in terms of substantiated, scientific knowledge and its application. As we increase the clinical significance and applicability of our analyses, however, we fully appreciate the importance of providing comprehensive backgrounds and explanations. After all, while our findings can increasingly help clinicians and other specialists determine the root causes and developments of illnesses or other scientific investigations, this also means you, as our user, have to trust these findings.
The following paper provides the scientific and, where applicable, clinical backgrounds so you can make the most of our analysers in your daily work.
Sysmex Scientific Focus Haemoglobinisation parameters on the Sysmex XN-Series Haematology analysers
Reticulocyte haemoglobin content is a marker that provides a snapshot of iron availability for erythropoiesis in the bone marrow, an indicator of iron therapy response, and an early marker of iron-deficient erythropoiesis.
As well as providing the standard parameters for red blood cell and reticulocyte counting, the Sysmex XN-Series systems can analyse the cell-by-cell haemoglobin content of both mature RBC’s and reticulocytes. These parameters have been shown in independent studies to provide clinically relevant insight into RBC metabolism including direct assessment of the incorporation of iron into haemoglobin, and a faster indication of response to changes from therapy. They provide a sensitive indicator of iron deficient erythropoiesis.
Measurement
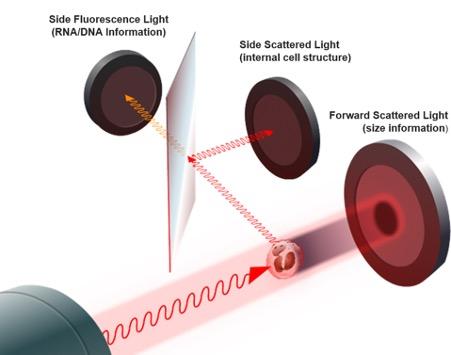
The haemoglobin content of a red blood cell can be calculated from its index of refraction in the forward scattered light generated as it passes in front of a laser beam. In the XN-Series, both mature RBC’s and reticulocytes are analysed by fluorescence flow cytometry in the reticulocyte channel using three detectors including one for forward scattered light (Figure 1).
Fig 1: XN-Series Fluorescent flow cytometry system
Values for mean RBC haemoglobin content (RBC-He) and mean reticulocyte haemoglobin content (RET-He) are generated. RBC-He can be thought of as an alternative MCH value, except that it is measured optically rather than by impedance. RET-He has a reference range of 28 - 36 pg. The difference between the RET-He and RBC-He value for a particular patient is displayed as the Delta-He in pg (Figure 2). The values can be either positive or negative and the reference range is in the region of +2 to +8pg. Negative values indicate an impaired haemoglobinisation of newly formed reticulocytes compared with mature erythrocytes.

Fig 2: Retic channel scatterplot showing haemoglobinisation parameters on the Forward scatter (FSC) axis
Use in anaemia differentiation
Iron deficiency (ID) is a major but highly underestimated health problem worldwide, which in the long run can lead to iron deficiency anaemia (IDA) and impaired erythropoiesis. Assessment of erythropoietic activity is therefore of prime importance in anaemia diagnostics. Conventional biochemical markers of iron status, such as ferritin or transferrin, are influenced by an acute phase response or by clinical conditions like chronic inflammation, cancer, or end stage renal failure. RET-He enables an early detection (Levy & Schapkaitz 2018) and indication (Joosten et al 2013) of Iron deficiency owing to not only its short life span (1-2 days) in the circulation as compared to mature erythrocytes (120 days) but also its better predictive value (Schoorl 2016) than hemocytometric parameters, for example, MCV, red cell distribution width (RDW), and Hb. These are insensitive markers in detecting early erythropoietic disturbances as their changes (MCV: 21 days, RDW: 30 days, and Hb: 60 days (Sunkara & Kotta 2016) are observed when Iron deficiency anaemia has already taken place. In contrast, RET-He is a peripheral blood count marker that is abnormal in the presence of iron deficiency (Powers & Buchanan 2014). It is also an early indicator of response to iron therapy, of which effect is detected about two days after initiation of the optimal treatment (Doig 2016) as opposed to ferritin, of which first response occurs in 1-2 weeks (Powers & Buchanan 2014). The measurement is not affected by physiologic interferences, except in cases of thalassemia (Skarmoutsou 2003) and macrocytosis/megaloblastosis (Mast et al 2002). Several studies are now available that consistently suggest a reticulocyte count with reticulocyte haemoglobin measurement may be a vital tool for determining both simple IDA as it evolves, and for defining more complicated situations. A reduction of the reticulocyte haemoglobin below the lower limit of normal (28 pg) indicates that only limited iron is available to the erythropoietic marrow. A recent example is the paper by Ucar et al (2019) that found RET-He was significantly lower in IDA, compared to other groups (IDA: 21.0 ± 4.1, ID: 26.0 ± 4.9, non-ID anaemia: 32.1 ± 6.8, control: 36.6 ± 7.0; < 0.001). The ID group had a lower RET-He compared to the non-ID anaemia group and the control group. On the 5th day of treatment, the ID and IDA group showed no significant differences in terms of Hb while the RET-He level demonstrated a significant increase. The increase in the RET-He level observed in the IDA group on the 5th day was significantly higher compared to the increase observed in the ID group. In the International consensus statement on the management of postoperative anaemia after major surgical procedures (Munoz et al 2018) it is stated that postoperatively, iron deficiency should be defined by ferritin concentration < 100 lg, ferritin < 100–300 lg and transferrin saturation < 20%, or reticulocyte haemoglobin content < 28 pg.
Studies in children have demonstrated that measurements of reticulocyte Hb content have greater success than other traditional parameters in determining both the present state of and the future likelihood of iron deficiency (Ullrich 2005).
It has been suggested that RET-He could be used to detect latent ID in blood donors (Tiwari et al 2018). It is also suggested that RET-He can be a useful tool in the developing area of patient blood management (PBM). This international campaign aims to reduce the requirement for blood transfusions, one of the most overused treatment in modern medicine with > 50% of transfusions possibly being inappropriate or avoidable (Anthes 2015). PBM is a multidisciplinary, evidence-based approach to optimising the care of patients who might need a blood transfusion following several international initiatives over the past 20 years (NHSBT 2020). It was launched in England in June 2012 and its recommendations had the support of NHS England. PBM is founded on three pillars;
Optimise RBC mass
Minimise blood loss
Manage anaemia It is the third of these pillars where haemoglobinisation parameters can be of benefit. Within a PBM program, low preoperative Hb and iron deficiency are two of the few modifiable risks factors for reducing RBC transfusion and improving a patient’s condition. Being able to identify IDA reliably and take appropriate steps prior to surgery will help prevent the need for transfusion in these cases if measurements are taken with sufficient time to instigate therapy (approx. 1 month).
Hema-plot
Researchers from Germany have published data looking at the difference between the reticulocyte and erythrocyte haemoglobin content (Delta-He) to differentiate between various diseasespecific types of anaemia. In their paper Weimann et al (2016) describe a matrix which they call the ‘Hema-plot’ and how they feel it is a helpful tool for differential diagnosis and disease-monitoring in various types of disease-specific anaemia, especially in anaemia of chronic disease (ACD) and mixed ACD/IDA. Weimann and his colleagues found that negative values for DeltaHe were seen in all of their patients with ACD who were not undergoing therapy, as well as those with combined ACD/IDA, sepsis, or inflammatory diseases. Patients with IDA alone had positive values. RET-He values did not distinguish between the ACD/IDA and IDA patients. The researchers then created a nine-bay Hema-Plot with RET-He on the y-axis and Delta-He on the x-axis and marked out various quadrants to specific anaemia causing diseases. In particular they identified the area where both RET-He and Delta-He were below the normal range as the place where ACD or combined ACD/IDA patients would fall if they were not undergoing therapy. Untreated sepsis or acute inflammatory patients also fell in this area but IDA and Haemoglobinopathy patients did not and could be separated out into a quadrant with normal Delta-He (2 – 8pg) and low RET-He (<28pg). Changes in the Delta-He value could occur within a few hours following therapy and this led the authors to suggest that treatment could be monitored by plotting successive measurements using the Hema-plot. It would in theory be possible to directly report the plot to a clinician using a web-based client.
Role in renal failure management
National Institute for Health and Care Excellence (NICE) guidelines for managing anaemia in chronic kidney disease (NICE Guidelines NG8, Published June 2015) recommend the RET-He value as a method for evaluating and monitoring iron status in renal patients. Physicians dosing chronic kidney disease (CKD) patients with erythropoietic stimulating agent (ESA) therapy can use a RET-He cut off value of 29pg to determine iron status, predict response to iron therapy and monitor iron status during treatment. Functional iron deficiency (FID) may occur in these patients when sufficient iron is in the body stores but cannot be made available for erythropoiesis. The guidelines recommend that clinicians should offer iron to people receiving ESA maintenance therapy to keep their: percentage of hypochromic red blood cells less than 6% (unless serum ferritin is greater than 800 micrograms/litre)
or
RET-He above 29 pg (unless serum ferritin is greater than 800 micrograms/litre) The marker of iron status should be monitored every 1–3 months in people receiving haemodialysis. In people who are pre-dialysis or receiving peritoneal dialysis, levels are typically monitored every 3 months. If these people have a normal full blood count there is little benefit in checking iron status. Once RET-He is above 29 pg, or transferrin saturation is greater than 20% and serum ferritin level is greater than 100 micrograms/ litre, it is suggested to offer maintenance iron to people with anaemia of CKD who are receiving ESA’s.
The dosing regimen will depend on modality, for example haemodialysis patients will need the equivalent of 50–60 mg intravenous iron per week (or an equivalent dose in children of 1mg/kg/week).
Use in thalassaemia diagnosis
Lian (2019) found significantly higher RET-He and lower RBC distribution width (RDW) were prominent in thalassemia trait compared to congenital sideroblastic anaemia (CSA) and IDA and the combination was powerful in the differentiation of these conditions.
Use in detection of bacterial infection
Reduction in Delta-He resulting in a value less than 2 or negative, has been identified in patients with a bacterial infection when compared to a control group (Henriot et al 2017). It is hypothesised that the reduced values of Delta-He result from the sequestration of iron in the body as a response to a bacterial challenge, withdrawing the iron that invading bacteria need for their growth. A rise in certain cytokines, such as interleukin-6 triggers an increase in hepcidin, an acute phase protein. Hepcidin ensures that transmembrane iron-export proteins are internalised from the cell surface. There is a resultant reduction in iron availability for erythropoiesis and as a result the haemoglobin content of Reticulocytes drops within a day or so but the RBC-He value does not alter until much later. It is projected that including Delta-He in algorithms to identify infection could be beneficial.

Other applications
A special algorithm combining RBC-He, RET-He and lactate dehydrogenase has potential as a marker of haemolysis strongly correlated with albuminuria in sickle cell anaemia patients (MaierRedelsperger et al 2010).
Conclusion
The cell-by-cell haemoglobin content measurements provided by the Sysmex XN-Series Reticulocyte channel are proven tools to assist in the assessment of the incorporation of iron into haemoglobin. They feature in NICE guidelines for the management of renal anaemia and consensus statements on the management of postoperative anaemia as well as being shown to be valuable in many other areas.
Focus on science
Do you have a specific topic you would like to see in the Sysmex Scientific Focus? Let us know at marketing@sysmex.co.uk.
References
• Anthes 2015. Evidence-based medicine: Save blood, save lives. Nature; 520, 24–26 • Doig 2016. Disorders of iron kinetics and heme metabolism. In: Keohane EM,
Jm W, Smith LJ, eds. Rodak’s Hematology: Clinical Principles and
Applications (5th edn). St.Louis, Missouri: Elsevier Saunders; 297-305 • Henriot et al 2017. New parameters on the hematology analyzer XN -10 (Sysmex™) allow to distinguish childhood bacterial and viral infections. Int J
Lab Hematol; 39: 14-20 • Joosten et al 2013. Is analysis of the reticulocyte haemoglobin equivalent a useful test for the diagnosis of iron deficiency anaemia in geriatric patients?
Eur J Intern Med; 24: 63-66 • Levy & Schapkaitz 2018. The clinical utility of new reticulocyte and erythrocyte parameters on the Sysmex XN 9000 for iron deficiency in pregnant patients. Int J Lab Hematol; 40: 683-690 • Mast et al. 2002. Clinical utility of the reticulocyte hemoglobin content in the diagnosis of iron deficiency. Blood; 99: 1489-1491 • Munoz et al 2018. An international consensus statement on the management of postoperative anaemia after major surgical procedures Anaesthesia. 2019, 73, 1418–1431 • NHSBT 2020. https://hospital.blood.co.uk/patient-services/patientblood- management/ (Last accessed July 2020). • Powers & Buchanan 2014. Diagnosis and management of iron deficiency anemia. Hematol Oncol Clin North Am; 28: 729-745 • Schoorl 2016. Innovative haematological parameters in clinical practice. Ned
Tijdschr Klin Chem Labgeneesk; 41: 6-16 • Skarmoutsou 2003: Erythroid bone marrow activity and red cell hemoglobinization in iron sufficient beta-thalassemia heterozygotes as reflected by soluble transferrin receptor and reticulocyte hemoglobin in content: correlation with genotypes and Hb A(2) levels. Haematologica; 88: 631-636 • Sunkara & Kotta 2016. Evaluation of red cell indices and reticulocyte maturity indices including reticulocyte haemoglobin concentration in iron deficiency anaemia adult female population. J Evid Based Med Healthc; 3: 5315-5318 • Tiwari et al 2018. Applying newer parameter RET-He (reticulocyte haemoglobin equivalent) to assess latent iron deficiency (LID) in blood donorsstudy at a tertiary care hospital in India. Vox Sang; 113: 639 • Ucar et al (2019). The importance of RET-He in the diagnosis of iron deficiency and iron deficiency anemia and the evaluation of response to oral iron therapy. J Med Biochem 38: 496 –502 • Ullrich 2005. Screening healthy infants for iron deficiency using reticulocyte hemoglobin content. JAMA; 294: 924–30 • Weimann et al 2016. Delta-He, RET-He and a New Diagnostic Plot for
Differential Diagnosis and Therapy Monitoring of Patients Suffering from
Various Disease-Specific Types of Anemia. Clin Lab; 62: 667-77

Date: Thursday 17th June 2021 – Time: 2-5pm
If you would like to attend, please email CN-Series@sysmex.co.uk
Live Webinars
ENGAGE
with presentations on a range of topics
OPPORTUNITY
to gain CPD recognition
PARTICIPATE
in live Q&A sessions with keynote speakers
Register
Login
Live

Call for Posters. To register your interest, please email the title of your poster to: usermeeting@sysmex.co.uk by Friday 23rd July 2021. Deadline for submitting posters: Friday 22nd October 2021
Essential contact information
Sysmex UK
Main reception:..................................................... 0333 320 3460 Customer support centre

Product hotline: ....................................................0333 320 3466 Service hotline:........................................................ 0333 320 3467 pocH-100i hotline:...........................................0333 320 3463 MSC hotline:..................................................................0333 320 3464 Reagents and consumables
Reagent ordering:..............................................0333 320 3470 Ireland customer support centre
Hotline:........................................................................................... 1800 936 590 Ireland reagents and consumables
Hotline:..............................................................................................1800 936 591 Online Sysmex Academy Online: https://uk.sysmex-academy.com Support portal: http://support.sysmex.co.uk/focalpoint Website: www.sysmex.co.uk
About Sysmex Sysmex UK Ltd. is the distributor and support network for Sysmex automated haematology, haemostasis and urinalysis diagnostic analysers, reagents and information systems for laboratories and healthcare facilities within the UK and Ireland. Sysmex Corporation is the global leader in systemisation, providing solutions to streamline and improve the workflow of the busiest laboratories. For further information please contact Sysmex UK by email info@sysmex.co.uk or phone 0333 320 3460. For product information please visit the Sysmex UK website www.sysmex.co.uk Sysmex UK Ltd, Sysmex House, Garamonde Drive, Wymbush, Milton Keynes, MK8 8DF Company Registration Number: 2598523