

Treatment Teaches Behavior. Soberlink Reinforces it.



Your care transforms lives. Support your clients beyond in-person care with the only remote alcohol monitoring system with real-time results, facial recognition, tamper detection, and insightful Advanced Reporting to analyze patterns and celebrate progress.
Addiction Treatment Professionals,
The National Institute on Alcohol Abuse and Alcoholism highlights a troubling reality:
• Fewer than 10% of people with a substance use disorder receive treatment.
• Among those who do, dropout rates remain high, and long-term recovery success is difficult to measure.
This underscores the importance of expanding access to care, offering individualized options, and monitoring clinical outcomes to build lasting recovery.
Soberlink supports this effort with a remote alcohol monitoring system that promotes accountability. Our FDAcleared breathalyzer ensures trust and honesty with features like facial recognition and tamper detection to deliver real-time results, allowing providers to support clients beyond the walls of treatment.
Trusted by thousands of treatment professionals, Soberlink is also used in licensed professional and workplace monitoring programs, including those at major airlines, healthcare systems, and government agencies
Inside this resource booklet, you’ll find materials to support your work, including:
• 6-Month Longitudinal Study of 100 Soberlink Clients: A deep dive into how remote monitoring contributes to recovery and family reintegration.
• Consensus Statement on Best Practices for Clinical Monitoring: Developed by leading addiction specialists, this statement outlines when and how to implement Soberlink effectively in treatment.
• Helpful Whitepapers and Case Studies: Including provider stories, client testimonials, and frameworks for integrating monitoring into discharge plans, IOP, and continuing care.
These resources reflect our commitment to improving outcomes and supporting both clinicians and clients through technology and empathy.
Learn more and access our full library of resources at soberlink.com/treatment
We also offer Lunch and Learns with our Treatment Support Team to walk through best practices and help integrate Soberlink into your clinical model. To schedule a session, reach out to us at bizdev@soberlink.com
We look forward to supporting your work—and your clients’ success.
Sincerely,
Andy Rothman
Senior VP of Business Development

What is Soberlink?
Studies show that monitoring can lead to significantly better outcomes by reinforcing accountability and transparency with your client’s recovery circle.
The Soberlink program is designed to empower people in their first year of recovery.
• Capability to send real-time results to unlimited recipients
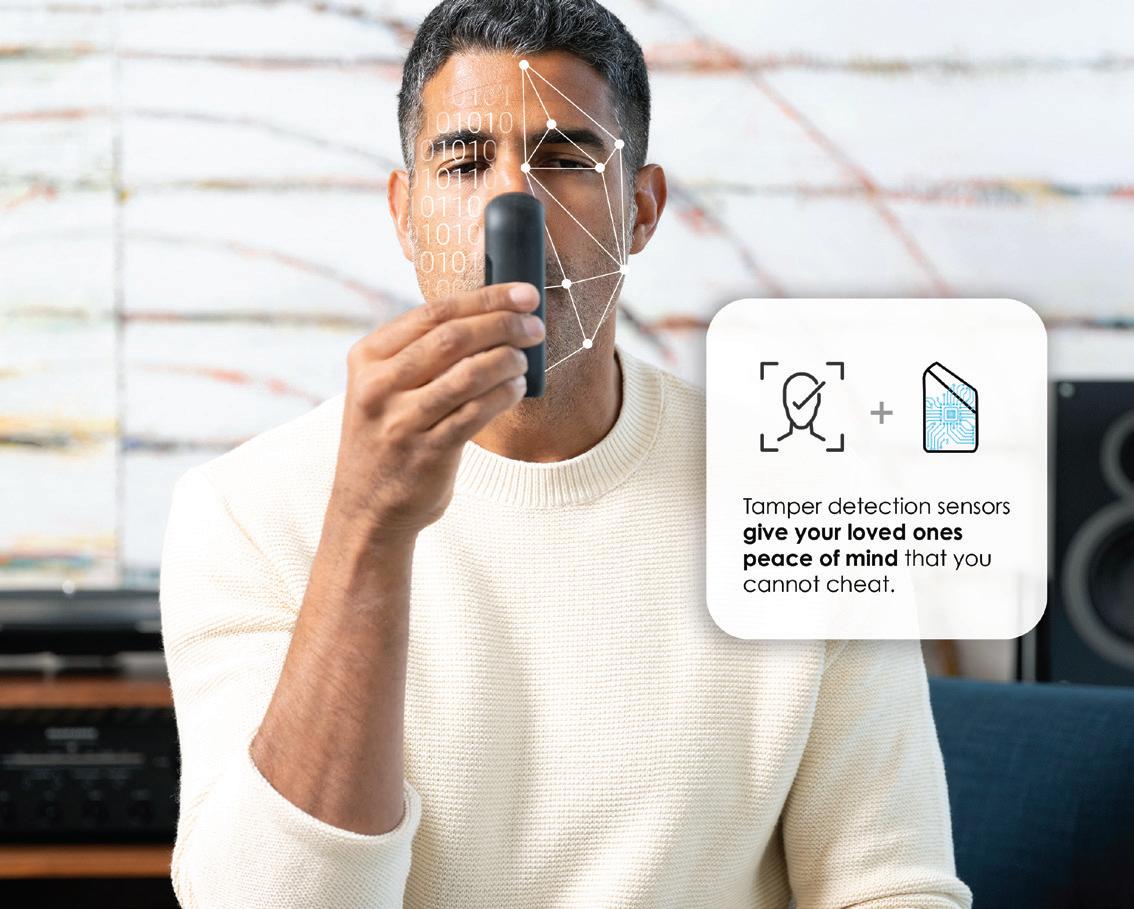
• Facial recognition that instantly verifies your client’s identity
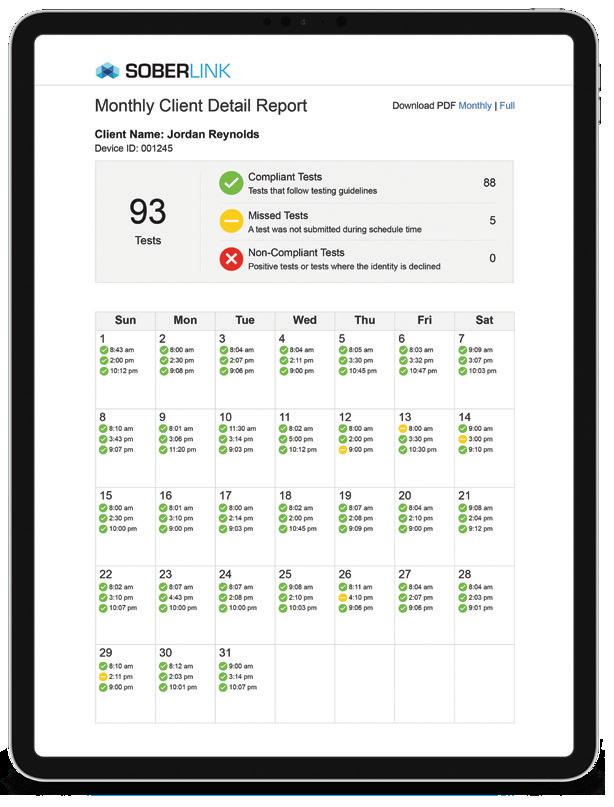
• Reports that are visually displayed in a calendar layout to analyze patterns
• Multiple sensors that prevent tampering
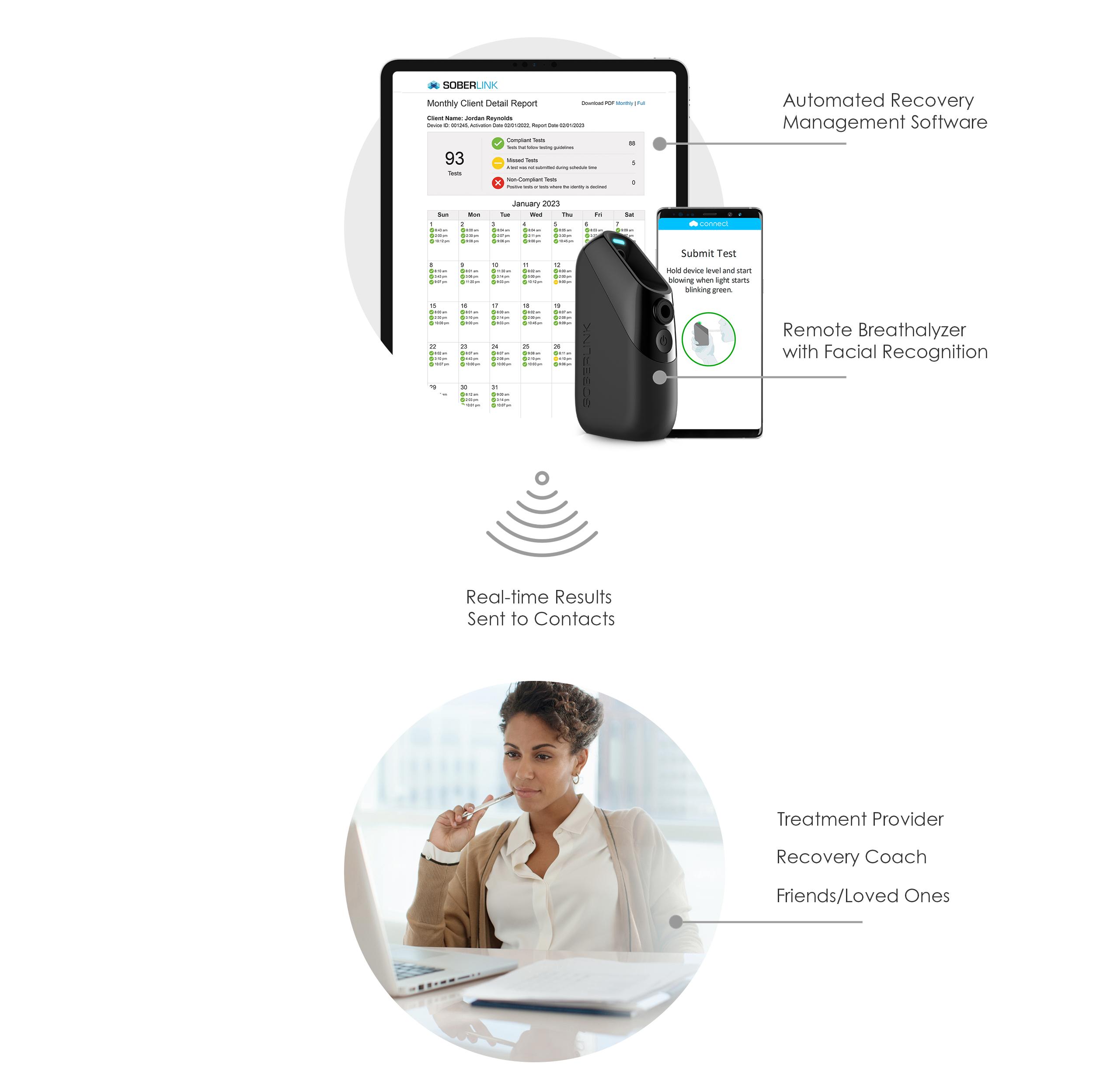
How Does Soberlink Work?
The Monitored Client blows into our mobile and discreet breathalyzer.
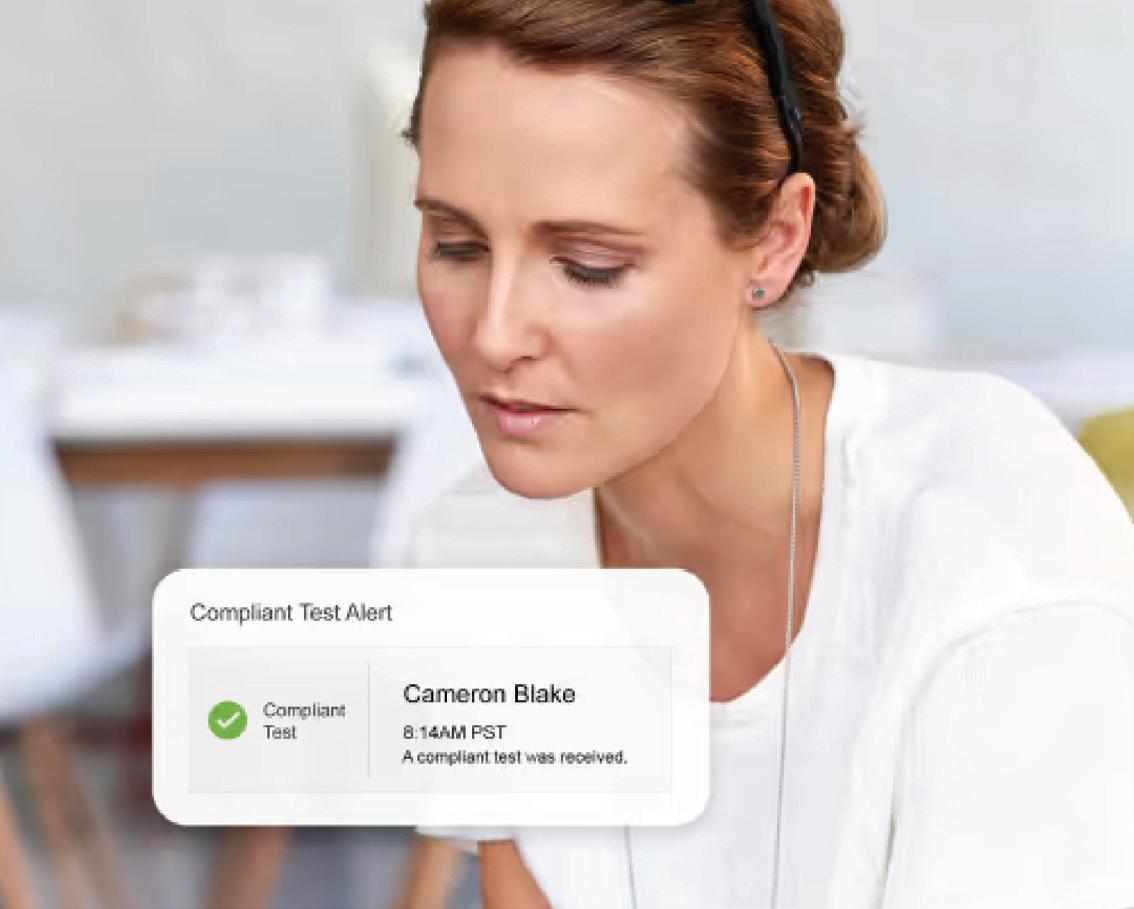
You and your client’s recovery circle receive instantly verified results via text or email.
Our reports help you analyze and celebrate your clients’ progress.

Quality, Accuracy, and Security You Can Trust
Most Tested, Most Trusted

Our commitment to accuracy drives thousands of testing hours and extensive quality control programs.
Facial Recognition Technology

We have integrated a high-resolution camera and facial recognition technology to confirm identity.
Soberlink has given me accountability when nothing else could do that consistently. I am forever grateful!
— Soberlink
Client

Top Quality
Reliability and security you can trust since 2011

FDA Cleared For Medical Use and held to the highest medical standards

ISO Certified Assembled in the USA under ISO certifications
Only the Highest Quality Tamper Resistance

Our U.S.-engineered Devices use professional grade fuel cell sensors to deliver consistent, reliable BAC readings.

Our internal sensors can detect when the client is attempting to defeat the system by tampering, ensuring test integrity.
Soberlink is a game-changer for AUD treatment. The real-time results provides the opportunity for immediate intervention and follow up by clinicians
— Dr. Kieran Executive Director of
Ayre Counseling

Tamper Resistant
Detects a wide variety of tampering attempts

Admissibility
Passes Frye and Daubert Standards

Law Enforcement
Accepted by law enforcement/ courts since 2011
Program Options and Pricing

Treatment providers have two options for referring Soberlink:
1. Share Program
Refer clients to user Soberlink, we’ll handle the rest.
• Devices start from $19/mo
• Plans start from $169/mo
Share Program Plans
Designed specifically for individuals who want to share their sobriety and rebuild trust.
Emailed results of previous day’s tests
Real-time email alerts of test results
Real-time text alerts & email of test results
2. Certified Provider Program
A Certified Soberlink Provider (CSP) is a Treatment Professional or Treatment Program trained on the best use and practices of the Soberlink System. CSPs will have access to their own Soberlink portal to set up and manage multiple clients.
Contact our business development team at bizdev@soberlinlk.com for custom pricing.
More info: soberlink.com/pricing

Summary of the Soberlink Research Study: A six-month longitudinal study of 100 Soberlink clients
Submitted to:
Soberlink Healthcare July 2022
Authors: Jenna Lee Mathews, Julia Ricotta & Charlotte Gray
OMNI Contributors: Sara Bayless, Holen Hirsh, Natalie Wheeler
For More Information:
Jenna Lee Mathews jmathews@omni.org 800-279-2070 ext. 156
Suggested Citation:
The OMNI Institute (2022). Summary of the Soberlink Research Study: A six-month longitudinal study of 100 Soberlink clients. Submitted to Soberlink Healthcare
Introduction
Soberlink is a comprehensive alcohol monitoring system designed to remotely monitor a person’s blood alcohol concentration (BAC) and provide accountability for users to support recovery from Alcohol Use Disorder (AUD)1. Soberlink has been helping people in their recovery from addiction since 2011. In recent years, Soberlink has been working to advance its scientific evidence base by demonstrating the impact of using Soberlink on whole-health outcomes through rigorous outcomes data collection. Beginning in 2019, Soberlink partnered with OMNI Institute (OMNI) to study outcomes data from Soberlink clients. OMNI is an independent nonprofit, social science consultancy that provides integrated research and evaluation, capacity building, and data utilization services to accelerate positive social change.
OMNI worked with Soberlink to design a research study to understand the impact of using Soberlink on individuals’ recovery and health outcomes Study participants were recruited from individuals enrolling in the Share Program, a program within Soberlink that allows participants to share Soberlink test results (reliable and accurate data on BAC) with a “recovery circle” of trusted individuals in their support network such as loved ones, sponsors, and/or therapists. This study was designed to gain deeper insights into participants’ experiences using the Soberlink technology; identify short - and long-term sobriety and other health outcomes for clients; and to better understand the impact of Soberlink, specifically for individuals who include a licensed therapist in their recovery circle.2
This report summarizes findings based on data shared by the current study’s 100 participants.3 Slightly more than half of participants identified as male and their ages ranged from 25 to 74. Generally, study participants had similar demographic characteristics and were white, not Hispanic or Latinx, highly educated, employed, and earning high salaries. A small percentage of participants reported previous criminal justice system involvement.4
The following sections highlight the study results most relevant to Soberlink Share Program experience and program outcomes. For a more complete summary of the study that includes findings related to program adherence, mental health outcomes and treatment engagement, and general helpful and challenging aspects of recovery, please visit omni.org/soberlink-research-study-full-report
Results: Soberlink Client Experiences
The following section outlines results associated with the study’s first research goal of gaining insight into participants' experiences and satisfaction with Soberlink though the Share Program It is important to note in this section and throughout the re port that participants were given the option to skip questions and display logic was used for some questions. As such, not all participants responded to all questions on the survey. Sample sizes are indicated (i.e., n=) for questions where at least one participant did not provide an answer.
1 For additional information about the Soberlink Syste m functionality and data security, see Appendix A.
2 For additional information about study objectives , design, and methods , see Appendix B.
3 Throughout this report, “participants” refers to Soberlink Share Study participants unless otherwise stated.
4 For additional information about study participant demographics, see Appendix C.
Experiences Using Soberlink Technology
Participants were asked about their experiences using the Soberlink technology for their recovery process at each follow-up (1-month, 3-month, 6-month). Participants were asked to rate a series of related statements using a scale from strongly disagree (1) to strongly agree (5).
Overall, participants were satisfied with Soberlink and the Share Program, and satisfaction remained consistent across follow-ups.
91% of Soberlink clients agreed or strongly agreed that they would recommend the Soberlink device to others who are struggling with AUD across all follow-ups
91% of Soberlink clients agreed or strongly agreed that the Soberlink Share Program kept them accountable across all follow-ups
86% of Soberlink clients agreed or strongly agreed that using the Soberlink device was a good decision across all follow-ups
Soberlink was convenient to use Using Soberlink was a good decision
Soberlink kept me accountable I would recommend Soberlink to others Sharing results positively impacted my recovery
Soberlink helped my feel in control of my recovery
Note: Results above are displayed on a scale of 1 to 5.
Helpful Aspects of the Soberlink Share Program
Participants described the most helpful parts of the Soberlink Share Program in open-ended responses. Responses largely fell into six main categories: a accountability, family, routine and structure, relapse prevention, accomplishment, and freedom
Accountability
Accountability was by far the most prominent theme related to helpful aspects of the Soberlink Share Program. Over 60% of participants mentioned accountability in their response to this question at all three follow-up timepoints. Regular testing and sharing results with one’s social support network held participants accountable in refraining from using alcohol.
[Soberlink has helped me to be] accountable no matter what, even while living alone - which was always the hardest part of being sober for me. I would always drink if I were to be alone, as I felt I didn't have to be accountable, the Soberlink Share Program has given me that accountability all the time.
The Soberlink Share Program has helped hold me accountable to myself and my circle.
Family

A large portion of respondents mentioned family involvement as a helpful component of the Soberlink Share Program. Specifically, participants named that Soberlink provides firm evidence of their sobriety to their family, which in turn builds trust.
The ease of providing evidence of sobriety to family members allows for participants’ lives and relationships to center around factors beyond recovery and sobriety
Additionally, knowing that family members are going to see results can provide motivation to remain sober.

[Soberlink] gives me freedom to my own recovery and it also allows my family to feel secure when they receive the resultsbuilds tons of trust back.
It’s been nice that my wife can see on her emails that I am staying sober without having to talk about it every day.

Knowing that my daughter will be devastated if she sees that I’m not sober [has helped]
Share Study (cont.)

Routine & Structure
Many participants appreciate the routine, schedule, and structure that Soberlink has provided them.
The regular tests provide some participants with a reminder of regular sobriety.
Relapse Prevention
Some participants described the relapse prevention and quick intervention after a return to use that Soberlink supports as particularly helpful.
Accomplishment
Some participants discussed the selfesteem boost that they receive when they successfully remain sober and have the evidence to support this from Soberlink.
Freedom

Some participants discussed the freedom that Soberlink gives them in their life.
As an organized, planned individual, I like the consistent goal posts each day that brings accountability to my recovery.
[Soberlink] reminds me every couple of hours that Sobriety is front and center
Knowing that a slip/relapse will be discovered quickly has helped minimize any thoughts about going out.
[Soberlink has helped] me be proud of myself when I show my family, through the program, that I'm remaining sober.
It has allowed me to drive and be reliable with the kids. It has given me back a sense of freedom.

Most participants felt the Soberlink device was easy to use and found the testing schedule easy to follow. Participants described many helpful components to the Soberlink Share Program, including providing accountability, building trust with family, creating routine, preventing relapses, giving a sense of accomplishment, and instilling greater freedom.
Impacts of a Positive Test
Individuals using a Soberlink device receive a positive test when a BAC above zero is detected For participants in the Share Program, if a positive test is confirmed, a client’s recovery circle receives a notification or an automated report, depending on user settings. See Appendix A for more information about Soberlink protocol for positive tests.
I cannot fall too far down when I slip up and drink because it will not be long before someone gets a Soberlink test report and holds me accountable.
Participants who indicated at least one positive test were asked about the impact of the positive tes t by rating statements on a scale from strongly disagree (1) to strongly agree (5).
Participants agreed that positive tests helped with aspects of their recovery . 6
I reached out to a loved one or treatment professional after a positive test.
The Soberlink device helped keep me accountable after a positive test.
I was able to gain control of my drinking after a positive test.
Having a positive test helped strengthen my commitment to sobriety.
After a positive test, I felt motivated to change my drinking behavior.
Note: Results above are displayed on a scale of 1 to 5.
Participants agreed that the Soberlink device kept them accountable after a positive test and helped them reach out to loved ones or a treatment professional for support.
6 There was not a significant change over time in positive test experience (p = 0.28).
Share Study (cont.)
Results: Soberlink Client Outcomes
The following section outlines results associated with the study’s second research goal of understanding short- and long-term outcomes for Soberlink clients. Questions about participants’ recovery-related outcomes, including substance use, treatment engagement, mental health, quality of life, and recovery capital were asked at one-month, three-month, and six-month follow-ups.
Also included in this section of the report are results related to the third study goal of exploring possible differences in outcomes for Soberlink Share Program participants who have a licensed treatment professional in their recovery circle versus those who do not. 50 study participants h ad a treatment provider in their recovery circle and 50 participants d did not have a treatment provider in their recovery circle. The two study groups were created by asking participants whether there was a treatment provider in their recovery circle at the time of enrollment and participants were enrolled until there were 50 individuals in each group (i.e., groups were not randomly assigned). Because the two groups were naturally occurring, we tested for demographic differences between the two groups to understand any key demographic characteristics that may have differentiated the groups. There were no significant differences in demographic characteristics between the groups.7 Areas where the groups differed in outcomes are highlighted throughout this section. Because the groups did not differ on key demographic characteristics at intake, it is more likely that differences in outcomes may be attributed to having or not having a treatment professional in participants’ recovery circles.
Substance Use
Participants were asked about substance use at intake, one-month, three-month, and six-month followup.
93% of participants reported no alcohol use in the p past week at intake.8
54% of participants reported no alcohol use in the p past month at intake.9
1% of participants reported no alcohol use in the p past year at intake.10

72% of participants had not used a substance other than alcohol in the past week at intake.
Among those who had used other substances, most reported using Benzodiazepines, Amphetamines, or Marijuana.

For those who had used any substance in the past year, a set of questions were asked that assessed if they qualified for a SUD.
99% of participants qualified for an alcohol use disorder. (n=98)
30 participants qualified for another SUD.
7 There were no significant differences between groups at intake in marital status (p = 0.47); education (p = 0.59); employment (p = 0.67); or income (p = 0.71).
8 There was not a significant difference between groups in alcohol use in the past week (p = 0.43) at intake
9 There was not a significant difference between groups in alcohol use in the past month (p = 0.32) at intake.
10 Because so few participants reported abstinence in the past year, differences between groups were not examined.
At each follow-up, participants were also asked about their substance use since the last follow-up survey. Rates of abstaining from alcohol were high among participants, ranging from 73% to 77% across followups. Rates of abstaining from other substances was slightly lower, ranging from 61% to 68%.
Overall, rates of sobriety from alcohol and substance use stayed high throughout the follow -up period for Share Program participants.11
At the six-month follow-up, 73% of participants had not use d alcohol since the three-month follow-up survey, and 62% had not used another substance.
Of those who reported using a substance in the past month, about half (51%) had used more than one substance in the past week at the six-month follow-up.
At follow-up, participants were asked to rate how troubled they felt by common issues of recovery. Participants could rate how troubled they were on a scale of not troubled at all (1) to very troubled (3).
Participants did not feel very troubled by alcohol or drug cravings across follow-ups.12
1 2 3 4 5 6 Months after intake
Almost all participants qualified for an alcohol use disorder (AUD). The number of participants reporting sobriety from alcohol was high, ranging from 73% to 77% between one- and six-month follow-up. Note: Results above are displayed on a scale of 0 to 2
11 There were no significant differences between groups in alcohol use at one- (p = 1.00), three- (p = 0.82), or six- (p = 1.00) months follow -up. There were also no significant differences between groups in substance use at one- (p = 0.31), three - (p = 0.48), or six- (p = 1.00) months follow -up.
12 There was not a significant change over time in how troubled participants felt by craving alcohol (p = 0.44). There was also not a significant change over time in how troubled participants felt by craving drugs (p = 0.95).
Substance Use Treatment Engagement
Participants were asked about substance use treatment at each follow-up. Understanding use of and re-engagement with treatment services helps demonstrate the level of care Soberlink clients need and if Soberlink contributes to individuals needing lower le vels of care.
The percentage of participants receiving any AUD treatment decreased across follow-ups.13
The number of participants receiving each type of treatment, from most intensive to least intensive, is below. Participants could select more than one treatment option.14
D Detoxification:
• 1-month – 1 participant
• 3-month – 6
• 6-month – 2
Residential/inpatient services:
• 1-month – 2 participants
• 3-month – 4
• 6-month – 3
Partial hospitalization program:
• 1-month – 3 participants
• 3-month – 4
• 6-month – 1
Intensive outpatient services:
• 1-month – 20 participants
• 3-month – 14
• 6-month – 12
Outpatient services program:
• 1-month – 15 participants
• 3-month – 20
• 6-month – 8
Telehealth:
Participants most frequently reported receiving some form of telehealth. The high use of this treatment option is likely in part due to the fact that the study took place during the COVID-19 pandemic when in-person options were limited. Highest
• 1-month – 32 participants
• 3-month – 29
• 6-month – 22
13 These changes are descriptive; inferential analyses were not conducted to assess whether the observed decrease over time was significant.
14 For all six levels of care there were no significant differences between groups in treatment participation at any of the follow-ups (p-values ranged from 0.09 to 1.00)
Participants primarily utilized lower levels of care, such as telehealth and outpatient services. Higher levels of care, such as detoxification and inpatient treatment were used less frequently. This suggests that Soberlink technology may be helpful in preventing more intensive and expensive treatment re-admissions. It may also demonstrate that clients receiving less intensive treatment, such as telehealth, are more likely to use the Soberlink device.
All participants had received treatment for AUD in the last six months at the time of enrollment into the study At the one-month follow-up, participants with a t treatment provider in their recovery circle reported higher rates of engagement with AUD treatment between intake and the one -month follow-up than participants w without a treatment provider in their recovery circle 15
At the one-month follow-up, 72% of participants with a treatment provider in their recovery circle had received treatment for AUD in the past month.
At the one-month follow-up, 49% of participants without a treatment provider in their recovery circle had received treatment for AUD in the past month.
This result could indicate that Soberlink clients with a treatment provider in their recovery circle have closer relationships to providers and are in more frequent contact with these professionals. However, this difference was only marginally significant and was not seen in other indicators of AUD, such as alcohol use and AUD medication use. In short, despite differences in treatment engagement, the groups otherwise had equal levels of SUD severity at intake.
Not having to worry about accountability [is the most helpful part of the Soberlink Share Program]. My therapist is going to know the truth and that’s basically a relief
Participants who reported receiving treatment services between follow-ups were also asked about arrangements for continuing services Across follow-up timepoints, of participants who had received treatment:
80% planned to use the Soberlink device for ongoing monitoring
77% arranged to have regularly scheduled appointments for continuing care
61% were currently participating in peer support groups
As a whole, participants were very engaged in either formal aftercare or other support groups, such as Alcoholics Anonymous (AA) Participants could indicate engagement for more than one group so total percentages below add up to more than 100%.
15 The difference at one -month follow-up was marginally significant (p = 0.03) There were no significant differences between groups in AUD treatment at three ( p = 0.22) or six (p = 0.45) months follow -up.
88% of all participants received support from AA at least once during follow-up.16
I find that attending meetings, working the steps, and doing Soberlink are helping to drive my sobriety.
Participants’ engagement in treatment services decreased over time . Generally, use of more intense and expensive treatment services ( e.g., detoxification, inpatient, and PHP) decreased over time.
Quality of Life & Recovery
Participants’ quality of life was assessed using the EUROHIS -Quality of Life 8-item index. This is a shortened version of the World Health Organization Quality of Life Instrument -Abbreviated Version (WHOQOL-BREF) that has been validated and shown acceptable cross -cultural performance. Scores on this measure can range from 8 to 40, with a higher score indicating higher quality of life.
For participants who had a treatment provider in their recovery circle, quality of life increased over time.17
With treatment provider (Significant growth)
Without treatment provider (Non-significant growth)
Note: Results above are displayed on a scale of 26 to 31.5.
16 For all four aftercare options, there were no significant differences in attendance between groups at any of the follow-ups (p-values ranged from 0.36 to 1.00)
17 For participants with a treatment provider in their recovery circle, quality of life significantly increased over time (p < 0.001); for participants without a treatment provider, quality of life did not significantly change over time ( p = 0.96)
Participants’ recovery capital was measured using the Brief Assessment of Recovery Capital (BARC -10) tool. Recovery capital is the characteristics and assets that a person develops in their recovery from a SUD. The BARC-10 is a validated questionnaire that assesses recovery capital using 10 questions corresponding to 10 domains that measure recovery capital. These domains include:
• Substance use and sobriety
• Global psychological health
• Global physical health
• Civic and community engagement
• Coping and life functioning
• Meaningful activities
• Housing status
• Risk-taking behavior
• Recovery experience
• Social support
Scores on the BARC-10 can range from 10 to 60. Research has demonstrated that scores over 47 predict sustained remission for one year or more . 18 The average recovery capital score for participants at intake was 48, indicating high recovery capital.19
Recovery capital increased significantly over time.20

Sustained Remission Benchmark
Note: Results above are displayed on a scale of 45 to 5 1
Participants were also asked to rate the supportiveness of people in their life. All participants reported having someone who was somewhat or very supportive of their recovery. At all follow-ups, participants rated an average of 5 5 people as somewhat or very supportive of their recovery
[Soberlink] has helped rebuild the trust I destroyed with the people I care about.
Participants who had a treatment provider in their recovery circle had higher quality of life scores at three-month and six-month follow-up, even though this group had slightly lower quality of life at intake. Recovery Capital increased over the course of the study period across all participants.
18 Vilsaint, C. L., Kelly, J. F., Bergman, B. G., Groshkova, T., Best, D., & White, W. (2017). Development and validation of a Brief Assessment of Recovery Capital (BARC -10) for alcohol and drug use disorder. Drug and Alcohol Dependence, 177, 71-76.
19 There was not a significant difference between groups in BARC-10 scores at intake (p = 0.54).
20 There was a significant main effect of time on BARC-10 scores (p = 0.002).
Share Study (cont.)
Limitations
All studies have limitations. In this section of the report, we note key limitations of the current study. First, findings may not be representative of all Soberlink clients. T here were a number of eligibility requirements, including participation in the Share Program; engagement in AUD treatment in the previous six months; and that Soberlink results could not be used for child custody or legal circumstances, among others Because the study took place during the COVID-19 pandemic, it is possible that a number of clients were excluded who had not received treatment due to the pandemic.
Next, findings may also not be representative of the impact that Soberlink use may have on the general population. The demographic characteristics of the participants enrolled in this study represent a group who is largely white, non-Hispanic/Latino, high earning, and employed. These demographic characteristics also tend to be related to quality of life and potentially recovery capital. Findings may vary in a similar study with a more diverse sample
Finally, participants in the study group who had a treatment professional in their recovery circle and those who did not have a treatment professional in their recovery circle were not randomly assigned. While the groups did not differ on key demographic characteristics at intake to the study, it is still possible that differences in outcomes that did emerge between the two groups may be predicted by f actors other than having a treatment professional in the recovery circle.
Conclusion
This study aimed to better understand Soberlink clients’ experiences using and short- and long-term outcomes of study participants. The study also looked at adherence to the Soberlink Share Program, including following the testing schedule and having the recovery circle receive all testing results. Eligible clients were asked to complete an intake survey and were contact ed one-month, three-months, and sixmonths after to complete a follow-up survey.
Almost all study participants had an AUD. More than three-quarters of participants had abstained from alcohol at each follow-up time point. Engagement with AUD treatment services decreased over time; however, participation in AA and other support groups remained high across follow -up surveys.
Study participants had high recovery capital that significantly increased over the study period, as measured by the BARC-10. Participants also had high quality of life scores. Participants who had a treatment provider in their recovery circle showed significant increases in quality-of-life scores over the follow-up period, while the group without a treatment provider showed no significant change .
The majority of participants were highly satisfied with Soberlink and the Share Program and would recommend the device to other individuals struggling with AUD. Many indicated that Soberlink and the Share Program held them accountable, which helped their recovery journey.
Appendix A: Soberlink System
Features of a Professional Remote Alcohol Monitoring System
• Professional grade handheld breathalyzer with embedded camera
• Real-Time facial recognition that ensures all identities are approved or declined minutes after the test is submitted
• Tamper detection sensors that detect if a person is trying to beat the system with artificial air
• Balancing sensors to ensure that a photo is being taken at the proper angle
• Two device options to ensure all types of clients are covered
• Device options should include a device with an embedded cellular module and another using Bluetooth and the power of a Smartphone
• Automated scheduled retesting upon a positive test being received or if the identity cannot be determined
• Device locks out for 15 minutes if a positive test is received to ensure that any contamination ca n evaporate before the re -test
• Ability to schedule tests at all times of the day
• Automated retesting up to 6 retests to determine contamination or if alcohol is consumed
• Reporting based on Artificial Intelligence that uses logic to report proper results
• Case load reporting to evaluate multiple clients on one page at-a-glance
• Robust web portal that supports unlimited number of users to manage clients
How the Soberlink System Works
The Soberlink System consists of a wireless breathalyzer that uses a professional grade fuel cell sensor to detect alcohol levels at an accuracy of +/-.005 BAC. The device also has an embedded camera and uses facial recognition software to automatically identify the client at the end of the test. The participant will have a set testing schedule that consists of a minimum of 2 tests per day. The participant will have a test window of 2 hours with a late window of 1 hour. When the participant blows into the S oberlink device, it will capture the BAC level while the embedded camera takes a photo of the participant during the test. The data is sent to the Soberlink web portal and analyzed in real -time. If the BAC is positive or if the identity could not be confirmed, a retest is automatically scheduled by the system. This retest is considered a confirmation test to verify the results. The system analyzes the test data and sends it to providers/caretakers in real-time or, if chosen, documented in an automated report they can receive daily, weekly, or monthly. Soberlink’s advanced reporting summarizes events with 3 color codes for simplicity: green is a compliant test where there is a BAC of .000, their identity is confirmed. A yellow icon in the report means that the participant missed their test window. A red icon means that the participant had a non-compliant event, which means they had a confirmed positive test, or their identity was declined. If the participant has a confirmed positive test, participants will be asked to retest until they are compliant or retest 6 times. This automated retest cycle helps evaluate a series of events into one noncompliant report. Treatment providers who monitor multiple clients have the option to choose a caseload report that groups all participants into one report showing either daily, weekly, or monthly test results in an at-a-glance view. As with all tests, Soberlink has built in sensors to evaluate the breath sample to confirm human breath and not artificial air or another air source that is sometimes used to tamper or “game” the system. The Soberlink System also provides professionals with a password protected, HIPAA compliant healthcare portal where they can set up a variety of advanced reporting tools. Soberlink i s designed and assembled in the United States and is one of the few FDA 510(k) cleared medical devices in remote alcohol monitoring.
Share Study (cont.)
Appendix B: Study Design & Methods
OMNI designed the current study to assess program experience and recovery outcomes of clients enrolled in the Soberlink Share Program. The research study was designed and executed by OMNI’s research team, and all research activities were reviewed, approved , and monitored by the Advarra Institutional Review Board (IRB). Specific research objectives of the study were as follows:
1. Gain insight into clients' experiences with Soberlink and the Share Program, including general satisfaction, the impact of positive tests, and ways that using Soberlink technology supported their recovery
2. Identify short- and long-term outcomes for clients, such as sobriety, engagement with various levels of treatment, and recovery capital.
3. Determine if differences in outcomes of Soberlink clients existed if they had a licensed treatment professional in their recovery circle versus if they d id not have a licensed treatment professional in their recovery circle.
Soberlink clients were identified to participate in the study at enrollment to the Soberlink Share Program by completing a short survey to determine eligibility. If eligible, clients could complete an IRB -approved consent form to formally enroll in the study. Per the study design, 50 participants had a treatment provider in their recovery circle and 50 participants did not have a treatment provider in their recovery circle. The study enrollment period lasted from June 2020 to May 2021.
Eligibility criteria to participate in the study were as follows:
• Client had an AUD (self-reported)
• Client’s goal was to abstain from alcohol use
• Client was 21 years of age or older
• Soberlink results were not being used for child custody or legal circumstance
• Client lives in the United States
• Client had received professional treatment for an AUD in the past 6 months (i.e., detoxification, outpatient services, intensive outpatient/partial hospitalization, residential/inpatient services, or medically managed intensive inpatient services)
• Client had at least one contact in their recovery circle
Once enrolled, participants completed surveys at four timepoints. Intake surveys were completed within three days of enrollment in the study. Follow-up surveys were completed one-month, three-months, and six-months after enrollment. After completing the intake, participants were required to use the Soberlink device for 30 days or longer to be eligible to complete the follow-up surveys.21
21 Only one enrolled participant used the device for fewer than 30 days and, as a result, was not co ntacted to complete follow-up surveys. The participant’s intake data was removed, and another participant was recruited in their place.
Intake Survey
Eligibility Survey
Eligibility Survey
Follow-Up Surveys
Participants had the option to earn up to $400 in incentives for completing the study surveys. A $50 Amazon gift card was provided for completing the intake survey. A $75 Amazon gift card was provided for completing the one-month and three-month surveys, and a $100 Amazon gift card was provided for completing the six-month survey. Additionally, there was a bonus $100 Amazon gift card for any participant who completed all surveys.
OMNI’s research team contacted clients to complete follow -up surveys and offered the option for participants to complete the survey electronically and independently or to complete the survey with a researcher over the phone. Participant retention in the study was high across follow -ups. The figures below show the percentage of participants who completed each follow-up survey.
Follow-Up Rate
The intake and follow-up surveys were designed to measure the outcomes of clients in the study. Items on the survey were derived from the National Association of Addiction Treatment Providers (NAATP) Outcomes Measurement Toolkit,22 the Brief Assessment of Recovery Capital (BARC-10),23 and the EUROHIS-QOL 8-Item Index 24 Follow- up surveys also included open-ended questions to qualitatively understand participants’ satisfaction with the Soberlink device and Share Program . Study surveys are available upon request.
22 Hirsh, H.K., Wheeler, N., Gelman, K., Swan, J. (2019). NAATP Addiction Treatment Outcomes Measurement Toolkit. Submitted to the National Association of Addiction Treatment Providers, Denver, Colorado. Access: https://www.naatp.org/sites/naatp.org/files/NAATP_Newsletter_Outcomes_FINAL.pdf
23 Vilsaint, C. L., Kelly, J. F., Bergman, B. G., Groshkova, T., Best, D., & White, W. (2017). Development and validation of a Brief Assessment of Recovery Capital (BARC -10) for alcohol and drug use disorder. Drug and Alcohol Dependence, 177, 71-76.
24 Sice de Rocha, N., Power, M.J., Bushnell, D.M., & Fleck, M.P. The EUROHIS -QOL 8-item index: Comparative psychometric properties to its parent WHOQOL_BREF. (2012). Retrieved from https://www.sciencedirect.com/science/article/pii/S1098301511036655
Share Study (cont.)
Participants completed surveys through the online survey platform Qualtrics or on the phone. Each survey took 10-15 minutes to complete. The survey was designed so that participants could skip any questions they did not feel comfortable answering . No survey responses were excluded from analyses.
Responses were analyzed in aggregate using the open-source software R and IBM’s Statistical Packages for Social Sciences (SPSS). Results are presented in two sections: (1) Soberlink Client Experiences an d (2) Soberlink Client Outcomes. Throughout the report we conducted inferential analyses to examine differences between the group of participants who had a treatment provider in their recovery circle and the group of participants who did not (referred to t hroughout the report as the ‘groups’) and changes over time in outcomes of interest for all participants.
Specifically, to assess differences between groups at intake, we conducted chi -square tests (for nominal data such as yes vs. no questions), and inde pendent samples t-tests (for continuous data such as BARC-10 scores). To assess changes from intake through the six -month follow-up for all participants, we conducted one-way ANOVAs (all outcomes assessed over time were continuous). Finally, in cases where there was significant change over time for all participants, we examined whether there were differences in that change between groups (those with a treatment provider and those without a treatment provider in their recovery circle); for these models, we c onducted two-way mixed ANOVAs.
Interpretation of the inferential analyses relied on s tatistical significance testing which uses a probabilityvalue (p-value). The p-value is the estimated probability that the observed differences between groups or changes over time occurred by random chance (rather than reflecting a true difference or change). In this study, multiple comparisons (between groups and over time) were conducted to address the research questions; to account for the fact that multiple compariso ns increase the chance of detecting false positives (i.e., concluding there is a significant difference when in fact there is not), we adjusted the pvalue criterion used to determine a statistically significant finding. Using the Bonferroni correction, a pvalue that was equal to or less than 0.0167 was considered statistically significant for this report. Additionally, a p-value that was less than 0.05 was considered marginally significant Of note, lower pvalues increase confidence that an observed effect is not random, but do not provide information on the strength of the effect
Participants also responded to four open-ended survey questions All quotes included in this report were provided by participants in these open-ended survey questions. Content analysis coding was completed for all responses to these four questions to identify high -level themes. Qualitative and quantitative study findings are integrated in the results sections.
Appendix C: Study Participant Demographics
One hundred participants were included in the study and their demographic characteristics are reported below. Not all participants responded to all questions on the survey. Sample sizes are indicated (i.e., n=) for questions where at least one participant did not provide an answer.
Participants were asked questions about their race, ethnicity, and marital status at intake. Participants were also asked about education, employment, and experiences with the justice system. Information about sex and age was provided by Soberlink via client records.
Participants identified as male more often than as female.
97% of participants identified as white. Almost all participants identified as neither Hispanic nor Latinx.
Participants’ ages ranged from 25 to 74.
More than half of participants were married or living as married.
Participants reported high levels of education , with 76% reporting having earned a Bachelor’s degree or higher .
More than half of participants were working full-time or part-time for pay.
Working full-time for pay
Working part-time for pay
Umemployed
Not working for pay by choice
Retired
The majority of participants were working as:
• Professionals
• Salespeople or in marketing
• Business owners/ upper management
The average time employed was 15 years.
Almost half of participants were earning more than $90,000 annually. (n=99)
Over $90,000

$60,001 to 90,000
$35,001 to 60,000
$20,001 to 35,000
$10,001 to 20,000
$10,000 or less
The majority of participants had not been arrested frequently and did not have repeated issues with law enforcement. Of those who had been arrested, one time was the average number of arrests. This is notable as individuals who have experienced substance use o r mental health disorders are overrepresented within the criminal justice system 25 The study eligibility requirement that participants could not be using the Soberlink device for legal circumstances may have contributed to this characteristic of the study sample
90% of participants had never been arrested.
25 James, D. J. and Glaze, L. E. (2006). Mental health Problems of Prison and Jail Inmates. Bureau of Justice Statistics Special Report, U.S. Department of Justice.
Consensus Paper
CONSENSUS STATEMENT
HowShouldRemoteClinicalMonitoringBeUsedtoTreat AlcoholUseDisorders?:InitialFindingsFromanExpert RoundTableDiscussion
AlanGordon,MD,AdiJaffe,PhD,A.ThomasMcLellan,PhD,GaryRichardson,MBBCh, GregorySkipper,MD,MichelSucher,MD,CarlosF.Tirado,MD,MPH,andHaroldC.UrschelIII,MD
Scientificevidencecombinedwithnewhealthinsurancecoverage nowenableachronicillnessmanagementapproachtothetreatment ofalcoholusedisorders(AUDs),includingregularmonitoringof bloodalcoholcontent(BAC),asausefulindicatorofdiseasecontrol. Recenttechnicaladvancesnowpermitmanydifferenttypesof remote,real-timemonitoringofBAC.However,thereisnobody ofresearchtoempiricallyguidecliniciansinhowtomaximizethe clinicalpotentialofremoteBACmonitoring.
Asaninitialstepinguidingandsupportingsuchresearch,the manufacturerofoneremoteBACmonitoringsystemsponsoreda groupofexperiencedcliniciansandclinicalresearcherstodiscuss8 issuesthatgenerallyaffectremote,clinicalBACmonitoringof ‘‘adultsinoutpatientAUDtreatment.’’
TheexpertpanelunanimouslyagreedthatremoteBAC monitoringforatleast12monthsduringandaftertheoutpatient treatmentofAUDwasaclinicallyviabledeterrenttorelapse.There wasalsoconsensusthatpositivetestresults(ie,recentalcoholuse) shouldleadtointensifiedcareandmonitoring.However,therewas noagreementonspecifictypesofclinicalintensificationaftera positivetest.Thepanelagreedthatsharingpositiveandnegativetest resultswithmembersofthepatientsupportgroupwashelpfulin reinforcingabstinence,yettheynotedmanypracticalissuesregardinginformationsharingthatremainconcerning.Significantdifferenceswithinthepanelonseveralimportantclinicalissuesunderline theneedformoreclinicalandimplementationresearchtoproduce empirically-supportedguidelinesfortheuseofremoteBACmonitoringinAUDtreatment.
FromtheTreatmentResearchInstitute(ATM),Philadelphia,PA;Butler Hospital(AG),Providence,RI;AlternativesBehavioralHealth(AJ), LLC,LosAngeles,CA;EdgewoodHealthNetwork(GR),British Columbia,Canada;PromisesProfessionalsTreatmentProgram(GS),Santa Monica,CA;Greenberg&SucherPC(MS),Scottsdale,AZ;ABRI IntegratedHealth,LLC(CT),Austin;EnterhealthLLC(HCU),Dallas,TX. ReceivedforpublicationJuly12,2016;acceptedNovember12,2016. Conflictsofinterest:DrsGordonandSkipperservedasconsultantstothe meetingsponsor(Soberlink)in2015.Theremainingauthorsreportno financialconflictsofinterest. SendcorrespondenceandreprintrequeststoA.ThomasMcLellan,PhD,150 S.IndependenceMallWest,600PublicLedgerBuilding,Philadelphia,PA 19106.E-mail:tmclellan@tresearch.org.
Copyright 2017AmericanSocietyofAddictionMedicine ISSN:1932-0620/17/1102-0145
DOI:10.1097/ADM.0000000000000288 JAddictMed Volume11,Number2,March/April2017
KeyWords: addiction,alcoholusedisorder,breathalyzer,remote monitoring,treatment
(JAddictMed 2017;11:145–153)
Despitethefactthatthemedicalcostsassociatedwith alcoholusedisorders(AUDs)areover$120billionper year,untilveryrecently,therehasbeenrelativelylittle involvementofphysiciansorothergeneralhealthcareprovidersinthetreatmentofAUDs(Sacksetal.,2015).By convention,mostcontemporaryAUDtreatmenthasbeen deliveredoutsidemainstreamhealthcarebyspecialty‘‘treatmentprograms’’thataretime-limitedbyinsurancerestrictionsandhighlystructuredtodeliverastandardized ‘‘program’’ofcare(McLellanetal.,2005;Folletal., 2009).Withintheseprograms,carehaspredominantlyconsistedofvarioustypesofcounselingandbehavioraltherapies toachievepatientacceptanceoftheiralcoholuseproblem, promoteunderstandingofrelapsetriggers,andpromotea commitmenttonewattitudes,friends,andbehaviorsto promoteasoberlifestyle.Outcomeresearchhastypically concentrateduponprogram‘‘graduation’’ratesand‘‘posttreatment’’abstinenceasstandardmeasuresoftreatment ‘‘success’’or‘‘failure’’(McLellanetal.,2005).
Despitetheselongstandingconventions,thereis increasingmovementtowardsadifferentapproachtomanagingAUDs.First,thereisnowclearscientificevidenceof geneticvulnerabilitytoalcohol,opioid,andothersubstance usedisorders(VolkowandLi,2005;Folletal.,2009).In addition,thereisevidencethatpersistentbrainchangesoccur withheavyuseofalcoholandmanyotheraddictivesubstances(Mayfieldetal.,2002;Colemanetal.,2011).This neurobiologicalevidencesuggeststhatalcoholandother substanceusedisordersarebestconsideredacquiredchronic illnesses,similarinonset,progression,management,and outcomestootherchronicillnessessuchasasthma,hypertension,ordiabetes(McLellanetal.,2000).Finally,recent legislativechangesinhealthcarerequireessentiallyallhealth planstooffergenerallythesametype,duration,rangeofcare optionsfortreatmentofmentalandsubstanceusedisorders asiscurrentlyavailableforcomparablephysicalillnesses (MentalHealthParityandAddictionEquityAct,2008; AffordableCareAct,2010).However,mostphysicianshave

Why Long-Term Monitoring Means Success for Licensed Professionals and General Recovery
How do we make recovery not just a possibility, but the expected outcome of addiction treatment?
This was a question thought leaders sought to answer at a 2013 symposium held at the Institute for Behavior and Health, Inc. What stemmed from this conversation was a new perspective on addiction recovery, one that focused on long-term monitoring as a means of achieving lifelong recovery.
For the last 40 years, this strategy, known as “New Paradigm for Recovery,” has been used to monitor individuals working in at-risk occupations – including physicians, airline pilots and, more recently, lawyers – and outcomes have been stellar. After witnessing these excellent results among licensed professionals, addiction treatment specialists have started to integrate this methodology into their programs as a means of promoting long-term sobriety after discharge.
What makes the New Paradigm for Recovery unique is that it treats and manages substance abuse disorders like chronic illnesses. Beginning with an initial assessment, the approach combines formal treatment with a monitoring agreement, which provides the leverage needed to stay sober. Monitoring agreements will include regular drug and alcohol tests and, if substances are detected, appropriate actions are taken based on the agreement. To make routine long-term monitoring as effective and convenient as possible, many treatment professionals choose remote monitoring systems, like Soberlink, for their clients. Unlike traditional methods of testing, such as urine screenings, these discreet and affordable devices can be used anytime, anywhere, keeping alcohol recovery top-of-mind following treatment.
In addition to addiction treatment, physician programs, specifically, have seen tremendous outcomes through long-term monitoring. A 2008 study published in The BMJ called Five year outcomes in a cohort study of physicians treated for substance use disorders in the United States outlines the history of these licensed professional programs, which were initially created by volunteer physicians who wanted to provide their cohort with support for substance abuse and mental health conditions. These volunteer groups soon developed into professional health programs tasked with promoting sobriety through “early detection, treatment and monitoring of substance use.”
One of the study’s head researchers, Dr. Gregory Skipper, medical director at the Center for Professional Recovery, was curious to learn how physician health programs differed from state to state. “Everybody thought these programs probably had good outcomes, but nobody knew for sure,” said Dr. Skipper. “We wanted to study them to prove how they were set up, what they do and if they work.” What resulted was a comprehensive study – known by industry insiders as “The Blueprint Study” – that outlined the innerworkings and outcomes of professional health programs across country. Dr. Skipper and his team divided the project into two phases: Phase 1 determined which states had professional health programs and described operational components, such as staffing, funding and treatment specifics. Phase 2 uncovered the outcomes of these
programs by analyzing data from doctors who had been in the program for at least five years.
The study’s final results showed that 79 percent of doctors in licensed professional programs remained completely abstinent of drugs and alcohol. Of the surveyed group, only 21 percent had at least one relapse. These statistics were groundbreaking, not only because they proved the success of licensed professional programs, but also because the success rate was much higher than traditional treatment programs. The average treatment program typically lasts 6 months or less and the rate of abstinence is only about 50 percent. Looking at the licensed professional programs’ nearly 80 percent success rate, there was clearly a discrepancy between treatment for licensed professionals and treatment for the general population.
So, what makes licensed professional programs so much more successful than general treatment programs? According to Dr. Skipper, it’s because licensed professional programs play the long game when it comes to addiction treatment: “With professional programs, the focus is more on the individual; assessing them thoroughly, seeing what they need and how they’re doing and making sure that they’re safe to graduate from treatment and go back to work. It’s more open-ended and oriented toward the individual’s needs.” While many treatment programs end at the 30-day mark, licensed professional programs require ongoing care and monitoring that lasts years after treatment. While these programs don’t necessarily treat physicians, they do provide evaluation, diagnosis and a contract detailing formal treatment, monitoring and ongoing professional support.
Dr. Skipper accredits alcohol monitoring tools, like Soberlink, with supporting accountability for sobriety and workplace compliance. According to Dr. Skipper, Soberlink is becoming a widely accepted means of monitoring licensed professions with a history of alcohol use disorder. Noting the system’s convenient, real-time monitoring and the documented proof of sobriety, Dr. Skipper believes that Soberlink is a helpful resource for preventing professional impairment: “Soberlink offers a convenient means of accountability, documentation of sobriety and early detection of relapse, should it occur. Being real-time offers the advantage that, before going to work, the individual, whether a pilot, surgeon or anyone in a safety sensitive role, can test prior to work (and, if needed, during work) to document their abstinence from alcohol use, thus offering protection to the public who are depending on that professional.”
In addition, Dr. Skipper also highlights the power of leverage in maintaining sobriety. Oftentimes, the motivation professionals need to get sober is the threat of losing their job. In developing a contingency monitoring program, professionals are presented with a contractual ultimatum designed to keep them accountable: continue to monitor your sobriety or lose your license.
Asking Dr. Skipper where he foresees the future of addiction treatment and recovery heading, he mentions his hopes for widespread contingency monitoring: “I believe, and hope, that increased used of contingency monitoring with active, good, long-term monitoring will improve outcomes.” – And, with alcohol monitoring systems, like Soberlink, that future is possible.
To learn how Soberlink can benefit your licensed professional treatment program, visit soberlink.com.


714.975.7200 bizdev@soberlink.com
support@soberlink.com
Real People. Real Impact.

“
The disease of addiction is really powerful, more powerful than me. I decided to use Soberlink because I knew what the outcome would be, which would be the truth. It’s best alcohol monitoring method there is for someone like me who needs daily accountability.
– Krista, Soberlink Client

“
The family feels a bit of extra security knowing that this piece of technology, Soberlink, is part of their treatment plan, whether it’s day one or day 101.
– Greg Champion, Founder of Start Up Recovery


“
I trusted Soberlink because it came highly recommended from all of my clinicians in treatment. It gives you the opportunity to really lengthen that runway of your sobriety.
– Jack, Soberlink Client