

SPOTLIGHT Pulse
Dr. Sanjey “Jay” Gupta brings a systems-level vision grounded in frontline care to his role as SAEM26 program chair.
2025 –2026 SAEM BOARD OF DIRECTORS
EXECUTIVE COMMITTEE

Michelle D. Lall, MD, MHS
SAEM President
Emory University School of Medicine
Board Liaison to:
• Bylaws Committee
• Governance Committee
• Ethics Committee

Jody A. Vogel, MD, MSc, MSW
SAEM President-Elect
Board

Ava E. Pierce, MD
SAEM Secretary-Treasurer
UT Southwestern Medical Center
Board Liaison to:
• Global Emergency Medicine Academy
• Finance Committee
• Program Committee
• Clinical Researchers United Exchange Interest Group
• Wilderness Medicine Interest Group

Pooja Agrawal, MD, MPH
Member at Large Yale Department of Emergency Medicine
Board Liaison to:
• Clerkship Directors in Emergency Medicine
• ED Administration and Clinical Operations Committee
• Grants Committee
• Behavioral and Psychological Interest Group
• Pediatric Emergency Medicine Interest Group

Bryn Mumma, MD, MAS
Member at Large University of California, Davis
Board Liaison to:
• Academy for Women in Academic Emergency Medicine
• Research Committee
• Disaster Medicine Interest Group
• Palliative Medicine Interest Group
• Research Directors Interest Group
• Trauma Interest Group

Cassandra Bradby, MD Member at Large East Carolina University
Board Liaison to:
• Academy of Emergency Ultrasound
• Awards Committee
• Critical Care Interest Group
• Oncologic Emergencies Interest Group
• Toxicology/Addiction Medicine Interest Group

Jane H. Brice, MD, MPH Chair Member University of North Carolina at Chapel Hill School of Medicine
Board Liaison to:
• Faculty Development Committee
• Vice Chairs Interest Group

Jeffrey P. Druck, MD
Member at Large
The University of Utah
Board Liaison to:
• Academy for Diversity & Inclusion in Emergency Medicine
• Fellowship Approval Committee
• Climate Change and Health Interest Group
• Evidence-Based Healthcare & Implementation Interest Group
• Tactical and Law Enforcement Interest Group

Patricia Hernandez, MD Resident Member
Massachusetts General Hospital
Board Liaison to:
• Wellness Committee
• Innovation Interest Group
• Neurologic Emergency Medicine Interest Group,
• Telehealth Interest Group
Ryan LaFollette, MD
Member at Large University of Cincinnati
Board Liaison to:
• Simulation Academy
• Education Committee
• Airway Interest Group
• Operations Interest Group
• Transmissible Infectious Diseases Interest Group

Ali S. Raja, MD, DBA, MPH
SAEM Immediate Past President
Massachusetts General Hospital/ Harvard Medical School
Board Liaison to:
• Academy of Administrators in Academic Emergency Medicine
• Workforce Committee
• Educational Research Interest Group
• Informatics, Data Science, and Artificial Intelligence Interest Group
• Quality and Patient Safety Interest Group

Nicholas M. Mohr, MD, MS
Member at Large University of Iowa Carver College of Medicine
Board Liaison to:
• Academy of Emergency Medicine Pharmacists
• Academy of Geriatric Emergency Medicine
• SAEM Federal Funding Committee
• Membership Committee
• Emergency Medical Services Interest Group

Erin Campo,
•
HIGHLIGHTS
Jet Fuel to Mushrooms: Recognizing GABA Antagonist Toxicity in the Emergency Department
Oxygen: Evolving Management of Carbon Monoxide and Cyanide Poisoning
Understanding Pediatric Risk in
Navigating the Emergency Medicine Match: What Applicants Need to Know
Desmopressin in Traumatic Intracranial Hemorrhage: Don’t PATCH the Leak—Dose Matters
The Nerve Block Paradox: High-Value Care That Feels Hard in the Emergency Department
Point-of-Care Ultrasound Training After Milestones 2.0: Are We Losing Accountability?
Scouting the Signs: A Nature-Inspired Expedition Through Point-of-Care Ultrasound
Point-of-Care Ultrasound in Left Ventricular Assist Device Patients: A Systematic Emergency Department Approach
Beyond Training: Later Career Transitions, Identity, and Finding Alignment
Medicine Anaphylaxis in the Backcountry: Recognition and Management
2026 Research & Education Grantees
Chairs Are Powering Possibilities in

Community, Connection, and What Comes Next PRESIDENT’S COMMENTS

Michelle D. Lall, MD, MHS
Emory University
2025-2026
President, SAEM
I can hardly believe this is my final message to you as president of SAEM. Serving this organization and all of you has been one of the greatest honors of my career. What an extraordinary year it has been.
Together, we have celebrated remarkable milestones. At SAEM25 in Philadelphia, we welcomed a record number of attendees, reflecting the strength and vitality of our community. We launched the Academy of Emergency Medicine Pharmacists (AEMP), expanding the breadth of our academic mission, and established a new Federal Funding Committee to further elevate our advocacy and impact. We also advanced critical leadership transitions, including selecting a new editorin-chief for Academic Emergency Medicine, while conducting a thoughtful and comprehensive search for SAEM’s next CEO.
Our organization continues to grow and evolve in meaningful ways. SAEM stands as a dynamic, forwardlooking community driven by innovation, collaboration and a shared commitment to advancing academic emergency medicine. I remain deeply inspired by the passion, creativity and dedication that define this organization.
“Our organization continues to grow and evolve in meaningful ways. SAEM stands as a dynamic, forward-looking community driven by innovation, collaboration and a shared commitment to advancing academic emergency medicine.”

Looking ahead, I am thrilled to invite you to my hometown of Atlanta this May for a reimagined Annual Meeting designed to energize, connect and inspire. This year, we have thoughtfully enhanced the meeting experience to deliver greater value and engagement for every attendee.
For the first time, workshops and consensus conferences (two this year) are included with registration— unlocking expanded access to highimpact content. The four-day meeting, running Monday morning through Thursday afternoon, features 27 complimentary workshops across two days, including the debut of the EM Hackathon. New this year, Innovation Theater on the Main Stage spotlights bold ideas from SAEM academies shaping the field. The meeting also offers dynamic mentorship opportunities for both learners and senior leaders.
Our plenary and keynote sessions have been redesigned to be truly interactive, pairing cuttingedge science with dynamic, live conversations. We are honored to feature inspiring keynote speakers Drs. Brendan G. Carr and Laura Hopson. You will also experience an expanded Lightning Oral format, replacing traditional e-posters with fast-paced, engaging presentations that keep ideas moving and conversations flowing.
Beyond the educational sessions, we are excited to bring back community favorites like MedWARs, introduce a new pickleball tournament and offer meaningful opportunities to give back through our Food Is Medicine initiative—all while enjoying the vibrant city of Atlanta.
I closed my presidential address last year with a reflection that feels even
more meaningful today: The work we do in academic emergency medicine is not only about knowledge and skill—it is about the connections we forge, the relationships we build, and the community we create. That belief has guided me throughout this year of service.
As I conclude my term, I encourage each of you to get involved. Join an academy, participate in an interest group and engage with this incredible community. SAEM has been central to my own professional journey, and I hope it will be for you as well.
Thank you for the privilege of serving as your president.
ABOUT DR. LALL: Michelle D. Lall, MD, MHS, is professor and vice chair of community and belonging in the Department of Emergency Medicine at Emory University School of Medicine.
Designing Systems Ready for the Moment That Matters
Sanjey “Jay” Gupta, MD, brings a systems-level vision grounded in frontline care to his role as SAEM26 program chair.
For more than a quarter century, Sanjey “Jay” Gupta, MD, has built a career defined by momentum—advancing emergency care not only at the bedside, but across entire health systems and disciplines that stretch far beyond hospital walls.
As senior vice president and executive director of the emergency medicine service line at Northwell Health, Dr. Gupta operates at the intersection of clinical practice and large-scale systems leadership. In this role, he oversees emergency medicine operations across one of the nation’s largest health systems, driving innovations designed to improve patient flow, reduce wait times, and elevate care delivery. Among these efforts are the widespread implementation of splitflow models, optimization of observation services, and development of interdisciplinary workflows to expedite clinical services for any patient who seeks emergency care.
In his system SVP role, Dr. Gupta remains closely connected to frontline care, guiding leadership teams through the daily realities of high-acuity medicine while influencing departmental strategy and culture. His academic role as a professor at the Zucker School of Medicine at Hofstra/Northwell reflects his commitment to developing the next generation of emergency physicians.
Dr. Gupta’s work extends beyond traditional emergency medicine. A Fellow of the Academy of Wilderness Medicine and a member of DMAT NY-4, he is recognized for his work in austere and resource-limited environments, where adaptability and clinical judgment are essential. He is also board-certified in addiction medicine by the American Board of Preventive Medicine, with a focus on treating substance use disorders from the emergency department, including ED-initiated medication-assisted treatment, naloxone saturation campaigns, and ED alcohol use disorder treatment. Through this dual expertise, he brings a broad perspective to patient care that bridges acute intervention with long-term recovery and prevention.
His leadership also extends into organized medicine, where he serves as a councillor and previously served two terms on the board of directors for the New York chapter of the American College of Emergency Physicians. He has contributed to policy and advocacy for emergency medicine since his time as a resident.
Now, as program chair for the 2026 SAEM Annual Meeting, Dr. Gupta is helping shape one of academic emergency medicine’s most important gatherings— bringing together clinicians, researchers, educators, and leaders to explore the future of the field. It is a role that reflects both his breadth of experience and his ability to connect innovation, operations, and clinical care into a cohesive vision.
Across every setting—from wilderness expeditions to highvolume urban emergency departments—Dr. Gupta’s work is guided by a consistent principle: emergency medicine is not just about responding to crises, but about designing systems that are ready for them.


What drew you to serve as program chair for the 2026 SAEM Annual Meeting, and what does this role mean to you at this point in your career?
I have been a member of the program committee for as long as I can remember, and I served as the advance workshop subcommittee chair for more than five years. The meeting has always been a great source of knowledge exchange, upskilling, network building, and exposure to expertise for me, and I could not ignore the opportunity to contribute at a high level to an entity that has meant so much to me in my professional career.
How have your experiences as a clinician, educator, and system leader shaped your approach to designing this year’s meeting?
The design of this year’s meeting is a reflection of my personal commitment to innovation, expanding opportunity, and wellness. The meeting will be heavy on current topics like AI use in research, education, and problem-solving. We have expanded the number of research presentations, workshops, and didactics to allow more researchers and educators to participate in the main body of the meeting. Further, we have introduced new wellness-related activities like pickleball, MedWars, and a wellness room to meet the stress-mitigation needs of our attendees.
What is your overarching vision for the 2026 SAEM Annual Meeting, and how does it reflect where academic emergency medicine is headed?
We are at the crossroads of emerging technology that has the potential to make emergency care safer and more
efficient, but also has the potential to reduce our ability to critically think and separate us from our humanity. We are doubling down with our 360 review of AI as it affects teaching, research, ethics, and clinical use cases. Simultaneously, we are trying to increase our interpersonal connections with each other at the meeting with increased opportunities for mentoring, networking, and research and pedagogical presentations.
What themes or priorities were most important to you in shaping the program—and why?
My priority in the meeting was inclusiveness. I wanted to make sure that everyone had an opportunity to feel comfortable and connected to some aspect of the meeting, whether in a technically advanced workshop, a peer-to-peer mentoring event, at SonoGames, at a wellness event, at our newly expanded lightning oral research sessions, or at something new.
How are you thinking about engaging both early-career academics and established leaders in meaningful ways throughout the meeting?
The programming will allow for significant interactions between all groups. We have world-class keynote speakers who will be able to speak to attendees of all levels of experience. We have replaced our poster sessions with “standing room” lightning orals to blend the experience of full research presentations with the group-based interaction that we always cherished from posters. We
continued on Page 8
Dr. Gupta and family witness Alex Ovechkin, the Great 8 of the Washington Capitals, break Wayne Gretzky’s NHL all time goal record.
Dr. Gupta and extended family on a trip to the Grand Canyon.
leaned heavily this year on AI and academic emergency medicine, a topic that engages academics and leaders at all levels.
What new formats, innovations, or experiences can attendees expect this year?
A wellness room that will provide a lower-stimulation environment and therapy dogs during the meeting. Expanded programming into all four days of the meeting to allow for more workshops, didactics, and research presentations. We will see the return of MedWars for those who enjoy the combination of critical thinking, gamesmanship, and resource-limited environments. There will also be a focus on physical health with the introduction of pickleball.
How do you balance the need to be forward-thinking and innovative while still addressing the immediate, realworld challenges facing emergency medicine today?
Our thoughtful approach to the submission process, independent peer review, high-level discussion, and final
selection of educational and research sessions allows for all aspects of meeting needs to be fulfilled—from the present to the future. Having the smartest and most committed committee members, who are always encouraged to share their viewpoints and opinions, allows for an open dialogue that drives the creation of a meeting that is relevant for all participants and that touches upon all thematic and professional challenges facing the practice of academic emergency medicine.
What sets the SAEM Annual Meeting apart from other conferences in academic emergency medicine?
Our focus on the growth of students, residents, and earlycareer academics. We are continuously investing in and maturing the pipeline for our future academic experts and leaders.
For someone attending for the first time, what advice would you offer to help them get the most out of the experience?
Definitely use the app and plan your sessions. Don’t be afraid to network and ask questions. Make those connections. And don’t forget to enjoy Atlanta.

Dr. Gupta’s Leadership Lens
A systems-driven approach grounded in people, purpose, and practice
• Design for readiness: “Emergency medicine is about designing systems that are ready for crises.”
• Balance innovation with humanity: Embrace new technologies while preserving critical thinking, connection, and compassion.
• Lead with inclusiveness: Create environments where everyone can find a place to engage, contribute, and belong.
• Foster connection across all stages: Build meaningful interactions between students, early-career academics, and established leaders.
• Stay anchored in the bedside: Ensure every advancement in research, education, and operations ultimately serves the patient.
Dr. Gupta with the emergency department team at South Shore University Hospital.


Getting to Know Dr. Gupta
Coffee or tea—and how do you take it?
Coffee, always. Black.
What’s your go-to way to decompress after a long shift?
If you could ensure every attendee walks away with one key insight or takeaway, what would you want that to be?
Success in academic emergency medicine comes in all shapes and forms. SAEM strives to advance and innovate in academic medicine in all areas of scholarship, research, and leadership.
What do you see as the most pressing challenges—and opportunities—facing academic emergency medicine right now?
This is multimodal. From shrinking research and academic funding, financial headwinds affecting all of health care, and the “death of expertise,” we are at a pivot point of sustainability. This is also an opportunity to remain optimistic, agile, and to innovate in our practice, in our scholarship, and in how we teach future generations.
After more than 25 years in emergency medicine, what continues to inspire and motivate you in your work? My motivation always goes back to the bedside. Every advancement in research, scholarship, and clinical practice is anchored in doing better for the patient who trusts us with their care.
Usually something physical, like a run, workout, or hitting the driving range.
Favorite travel destination—or dream place you still want to explore?
Just put me on a mountain, no matter where it is. I love nothing more than seeing a sea of wildflowers and a freshwater mountain lake. This probably started as a kid when my parents would take my sisters and me on excursions to Kashmir and Shimla during visits to India.
What’s one item you always have with you on shift (besides the essentials)?
A snack. You definitely don’t want to be around me when I’m hangry.
If you weren’t in medicine, what career might you have pursued?
Hands down, I am an unrealized civil engineer. What’s a small habit or routine that helps you stay grounded in a high-pressure field?
A daily, unplugged morning walk with my dog, no matter the weather. It gives me undisturbed time to plan the day and brainstorm solutions for nagging issues.
Dr. Gupta building a snow shelter during the Winter Wilderness Medicine education day at South Shore University Hospital.
Dr. Gupta helping with a moulage education event at the SAEM Annual Meeting.
26 YOUR ANNUAL MEETING GUIDE

New Experiences. Reimagined Favorites. Unmatched Value
At SAEM26, innovation meets tradition—bringing together new experiences and reimagined favorites that inspire, engage, and connect the academic emergency medicine community.
This year’s meeting is designed to deliver more at every turn—from expanded learning and hands-on workshops to new ways to connect and recharge. With fresh ideas, dynamic formats, and opportunities to engage across every career stage, SAEM26 is set to be the most energizing and comprehensive annual meeting yet.
Experience SAEM26 in New Ways
SAEM26 brings a fresh approach to the annual meeting— expanding access, rethinking formats, and creating more opportunities for connection, discovery, and impact. Here’s what’s new and not to miss:
More Ways to Learn, All Week Long
This year’s meeting delivers more education than ever, with four full days of programming running Monday morning through Thursday afternoon. Attendees can take advantage of two full days of workshops (27 in total)—along with the Medical Student Symposium, Chief Residents Forum, and Leadership Forum—all now included with registration, making it easier to engage across interests and career stages.
New Formats. Bold Ideas. Fresh Perspectives.
The meeting introduces dynamic new ways to share and explore ideas. Lightning Orals replace traditional ePosters, offering fast-paced, high-energy presentations that keep ideas moving and audiences engaged. Two major consensus conferences—Artificial Intelligence and the Future of Emergency Medicine and Rebuilding Trust in Emergency Medicine—tackle timely issues shaping the field.
The new Innovation Theater spotlights breakthrough thinking from SAEM academies in a live, interactive format, where attendees vote in real time on the ideas with the greatest potential to influence the future of academic emergency medicine.
Hands-On. High-Energy. Unforgettable.
SAEM26 leans into hands-on, high-energy experiences. The EM Hackathon returns as a collaborative innovation challenge focused on real-world, data-driven solutions. MedWAR, the ultimate wilderness medicine race, brings teams together for a fast-paced medical adventure through Atlanta’s Piedmont Park. And for something entirely new, the Pickleball Tournament adds a dose of fun, fitness, and friendly competition. Come watch the action unfold!
Make an Impact Beyond the Meeting
Attendees can also make a meaningful impact through the
Food Is Medicine volunteer event with Open Hand Atlanta. This hands-on experience invites participants to help prepare and package nutritious meals for individuals and families in need—an energizing way to give back during the meeting.
Connect, Recharge, and Refocus
Recognizing the importance of balance, SAEM26 introduces The Oasis, a calm, restorative space designed for quiet, screenfree recharging. Attendees can also take part in a simple, one-time Annual Meeting Mentorship Program, making it easy to build meaningful professional connections.
Explore, Connect, and Discover in the Exhibit Hall
The SAEM26 Exhibit Hall has been reimagined with new spaces that support learning, career development, and meaningful engagement. Attendees can explore innovations in academic emergency medicine while connecting with organizations across the field in a more interactive environment.
With so much to explore—from groundbreaking sessions to high-energy events—SAEM26 is designed to keep you engaged from start to finish. Plan your schedule, follow your curiosity, and get ready for an unforgettable annual meeting experience.
Spaces That Support Your Experience
Childcare
On-site childcare provided by Jovie offers a safe, engaging environment with vetted caregivers, age-appropriate activities, and supervised play. For preregistration participants only; no on-site registration.
Location: L401–L403, Level L
Hours:
Mon–Wed, 7:30 a.m.–5:30 p.m.; Thu, 7:30 a.m.–1 p.m.
Family Room
A quiet, comfortable space for attendees with caregiving needs, with amenities including a refrigerator, changing table, wipes and sanitizer, seating, water, and light snacks.
Location: L404, Level L
Hours:
Mon–Wed, 7:30 a.m.–5:30 p.m.; Thu, 7:30 a.m.–noon
Join Us On the SAEM Main Stage!
Prayer Room
A private, welcoming space for reflection, meditation, or religious observance, designed to support a range of faiths and personal practices.
Location: L405, Level L
Hours: Mon–Wed, 7:30 a.m.–5:30 p.m.; Thu, 7:30 a.m.–noon
The Oasis
A calm, screen-free space to pause and recharge, supporting focus and well-being throughout the meeting.
Location: L503, Level L
Hours: Mon–Wed, 8 a.m.–5 p.m.; Thu, 8 a.m.–2 p.m.
Special Oasis programming: RAMS wellness session (Tue, 8 a.m.); therapy dogs (Wed, 11:30 a.m.)
The SAEM Main Stage, Atrium Ballroom B-C (Level A) is where the community comes together to celebrate excellence, share bold ideas, and explore the issues shaping academic emergency medicine.
Tuesday, May 19 | 9–11 a.m.
Awards Ceremony
Honoring achievement in research, education, leadership, and service.
Presidential Address
Celebrating the past year and looking ahead as leadership transitions.
Dr. Peter Rosen Memorial Keynote
From the Trauma Bay to the Board Room: Insights and Perspectives
Brendan Carr, MD, MS (Mount Sinai), explores how lessons from high-acuity care inform leadership, teamwork, and decision-making
Plenary Abstract Presentations
Two top-scoring abstracts with moderated discussion.
Wednesday, May 20 | 9 a.m. – 11 a.m.
Awards Ceremony
Recognizing distinguished contributions to academic emergency medicine.
Education Keynote
Will Artificial Intelligence Be the Death of Clinical Reasoning?
Laura R. Hopson, MD, MEd (University of Michigan), examines AI’s impact on decision-making and training, including risks and strategies to preserve clinical reasoning
Plenary Abstract Presentations
Three additional top abstracts with live Q&A.
26 YOUR ANNUAL MEETING GUIDE






What to Know Before You Go
Get ready for SAEM26 with everything you need to make the most of your time at the annual meeting—before you arrive and once you’re on site. From travel and hotel details to registration, the meeting app, and helpful resources throughout the conference, this guide will help you plan ahead, stay informed, and navigate the meeting with ease.
Plan Your Stay
Host Hotel: Atlanta Marriott Marquis
The Atlanta Marriott Marquis is the official host hotel and central hub for SAEM26 meetings, education sessions, and select events.
An iconic landmark in downtown Atlanta, the hotel rises more than 50 stories and features a breathtaking atrium spanning the full height of the building—creating a dramatic and unforgettable arrival experience. Its striking design has been featured in major films and television productions.
Amenities include:
• Multiple dining options
• Indoor/outdoor pool
• Skyline-view rooms
Location & Access
• Full-service spa
• Fitness center
Located on Peachtree Center Avenue, the hotel connects directly to the MARTA transit system for easy airport
access. It is also within walking distance of Centennial Olympic Park, the Georgia Aquarium, Mercedes-Benz Stadium, and Atlanta’s convention district.
Getting to the Hotel
From the Airport (ATL)
Hartsfield-Jackson Atlanta International Airport is approximately 10–11 miles from the hotel (15–30 minutes travel time).
• MARTA Rail (Best Value): Red or Gold Line to Peachtree Center Station; 3–5 minute walk
• Rideshare (Most Convenient): Uber/Lyft typically $25–$40
• Taxi: Flat rate to downtown approximately $37.50
Note: The hotel does not provide an airport shuttle.
Getting Around Atlanta
• Rideshare: Reliable, efficient, and ideal for door-to-door travel—especially at night
• MARTA: Affordable, traffic-free access to Midtown, Buckhead, and the airport
• Walking: Many attractions are within a 10–15 minute walk
• Taxis/Pedicabs: Available in high-traffic areas for short trips

Get Oriented On Site
Registration & Badging
Location: Marquis Ballroom Foyer (Level M)
Hours (Eastern Time):
• Sunday, May 17: 3–6 p.m.
• Monday, May 18: 7 a.m.–5 p.m.
• Tuesday, May 19: 7 a.m.–5:30 p.m.
• Wednesday, May 20: 7 a.m.–7:30 p.m.
• Thursday, May 21: 7 a.m.–1 p.m.
Preregistered Attendees
Use self-service kiosks to print badges and tickets. Badge holders and lanyards are available onsite.
On-Site Registration
Visit the staffed registration desk for assistance during registration hours.
Important:
All attendees—including members, nonmembers, partners, children, and guests—must register and wear badges to access sessions, the exhibit hall, and most events.

Key Locations
App Help Desk and Member Services: International Hall Foyer (Level I)
Hours (Eastern Time):
• Monday–Wednesday: 7 a.m.–5:30 p.m.
• Thursday: 7 a.m.–1 p.m.
Speaker Ready Room: Room A703 (Level A)
Hours (Eastern Time):
• Monday–Wednesday: 7 a.m.–5 p.m.
• Thursday: 7 a.m.–noon
Note: Presentations with disclosures cannot be edited on-site.
Use Meeting Tools
Annual Meeting App & Program Planner
Plan your schedule and navigate the meeting with the SAEM Annual Meeting app or desktop Program Planner.
• Browse sessions • Explore the exhibit hall
• Access presentations • Build your personalized schedule
Install instructions and a video user guide are available
Wi-Fi Access
Free Wi-Fi is available throughout the meeting space.
• Network: SAEM26
• Password: AnnualMeeting
Make the Most of SAEM26

Need Assistance?
• Visit the App Help Desk or Member Services (International Hall Foyer, Level I)
• Look for Medical Student Ambassadors in blue SAEM jackets
• Stop by the registration desk or SAEM Booth #315 during exhibit hours
First-Time Attendees & New Members
Visit SAEM Booth #315 to:
• Introduce yourself • Get a professional headshot
• Pick up SAEM swag • Enter the prize drawing
Stay Connected
Follow SAEM and join the conversation using #SAEM26:
• X: @SAEMOnline and @SAEM_RAMS
• Bluesky

First
Time at
the SAEM Annual Meeting? Start Here!
Dress Smart and Pack Essentials
• Wear layers. While May in Atlanta is typically warm, meeting rooms can be chilly.
• Pack snacks, such as protein bars or fruit, and bring a refillable water bottle to stay energized.
• Bring a charger or portable battery pack—your devices will get a workout.
• Comfortable shoes are a must.
Have a Game Plan
• Download the SAEM Annual Meeting app before you arrive to plan your schedule.
• Search for sessions by topic, academy or interest group, or speaker.
• Note session locations to make it easier to move between overlapping sessions.
• Access slide decks and take notes directly in the app; consider a tablet for easier viewing.
• Keep your conference badge and tickets with you at all times.
Explore the Exhibit Hall
• Discover new tools and innovations
• Connect with industry partners
• Pick up resources, giveaways, and a Passport to Prizes card at the SAEM booth (#315) for a chance to win cash prizes
• Explore new hubs designed to support learning, career development, and connection
• Check the schedule for special events, including networking coffee breaks and the opening reception
• Stop by the SAEM booth (#315) to ask questions, share feedback, and learn how to get involved
Network, Network, Network
• Attend networking events hosted by academies and interest groups; many are announced on SAEM community pages.
• Introduce yourself to people around you and keep business cards handy.
• Don’t underestimate informal moments—new connections can lead to collaborations, mentorship, and career opportunities.
After the Annual Meeting
• Visit SAEM Online Academic Resources (SOAR) to access presentations and additional educational content.
• Follow up with new contacts to maintain connections.
• Claim your CME/CPE credits within 60 days of the meeting.
• Save and submit receipts if your employer offers reimbursement.
Submitted by Tara Flack, PharmD; Alli Cowett, PharmD; and Dustin Williams, MD, on behalf of the SAEM Membership Committee
Discover What’s Next—Visit Our SAEM26 Exhibitors!
Explore the Exhibit Hall and connect with a diverse group of organizations shaping the future of academic emergency medicine. Visit booths to discover new innovations, resources, and career opportunities—and use the exhibitor list and floor plan to plan your route and make the most of your time.
SAEM26 Premiere Exhibitors















SAEM26 Exhibitors

Explore New Educational and Networking Opportunities in the Exhibit Hall
Discover new spaces designed to support learning, career development, and meaningful connection. The SAEM26 Exhibit Hall features several dedicated areas where attendees can explore innovations in academic emergency medicine and engage with organizations across the field.
Job Pavilion
A centralized space to explore academic emergency medicine career opportunities. Connect with recruiters and have focused conversations about jobs, career paths, and professional growth.
Knowledge Hub
A career-focused destination offering brief, practical sessions alongside opportunities to connect with recruiters. Designed to help attendees prepare for impactful job and career conversations.
Roundtable Hub
An informal setting to continue the conversation after sessions. Engage directly with speakers, ask questions, and dive deeper into topics in a more interactive environment.
Academies Hub
Connect with SAEM’s Academies to learn about their work, explore specialty-specific career pathways, and engage with like-minded colleagues. Check the schedule to meet with the academies that align with your interests.
Passport to Prizes Competition
Pick up a Passport to Prizes card at the SAEM booth (#315) and collect stamps by visiting participating exhibitor booths. Enter for a chance to win cash prizes throughout the Annual Meeting.




ASK THE PHARMACIST

Beyond Hypertensive Urgency: A New Framework for Evaluation and Management
By Madison Savidge, PharmD, MBA and Hayley Gartner, PharmD, on behalf of the SAEM Academy of Emergency Medicine Pharmacists
At a Glance
• Why this matters now: Updated American Heart Association and American College of Cardiology guidance moves away from “hypertensive urgency,” reshaping how clinicians interpret elevated blood pressure and avoid unnecessary acute treatment
• What you’ll learn: How to distinguish asymptomatic markedly elevated blood pressure from hypertensive emergency, apply new terminology, and manage patients safely without overtreatment
• Who this is for: Emergency clinicians and trainees who frequently evaluate elevated blood
pressure and need clear, evidencebased guidance for real-time decision-making
Why Terminology Is Changing
The 2024 American Heart Association (AHA) Scientific Statement and the 2025 AHA/ American College of Cardiology (ACC) guidelines have replaced the term hypertensive urgency with more objective terminology that better reflects clinical risk and guides appropriate management.
Historical terms such as hypertensive crisis and hypertensive urgency may oversimplify the clinical spectrum and, through subjective or emotive language, encourage unnecessary acute antihypertensive
treatment. Updated terminology instead emphasizes the presence or absence of acute target organ injury as the key determinant of management.
The new recommended terminology is included in Table 1. Notably, the terms asymptomatic markedly elevated inpatient BP and severe hypertension are synonymous, though derived from different guideline documents with different scopes (i.e., inpatient vs. all settings).
Importantly, target organ damage may occur even at BP levels below the 180/110–120 mmHg threshold, particularly when BP rises rapidly from baseline. This numeric
threshold should not be interpreted as an absolute requirement for injury. Rather, markedly elevated BP in the absence of acute target organ injury does not represent a medical emergency requiring immediate intensive intervention. Instead, it presents an opportunity for careful evaluation and optimization of chronic antihypertensive therapy, often in the outpatient setting.
Epidemiology and Clinical Context
Acute severe hypertension accounts for approximately 4.6% of all emergency department (ED) visits in the United States. Hypertensive emergencies are relatively uncommon, occurring in approximately 2 per 1,000 adult ED visits overall and 6 per 1,000 visits among patients with a prior diagnosis of hypertension.
A systematic review reported the prevalence of hypertensive emergencies at 0.3% and asymptomatic markedly elevated BP at 0.9%, with asymptomatic elevations occurring approximately 2.5 times more frequently. In hospitalized patients, elevated BP is even more common, occurring in approximately 50% to 72% of hospitalizations, with about 10% meeting criteria for asymptomatic markedly elevated BP.
Over the past two decades, rates of hypertensive emergencies have increased; however, associated mortality has declined and currently ranges from 0.2% to 11% Certain populations are disproportionately affected, including older adults, Black patients, and individuals with comorbid conditions such as diabetes, chronic kidney disease, and cardiovascular disease. Socioeconomic factors also contribute to increased risk, particularly among individuals who are underinsured, live in lower-income communities, or are nonadherent to antihypertensive therapy.
Common triggers for hypertensive crises include stress or anxiety (44.9%), increased dietary sodium intake (33.9%), and medication nonadherence (16.2%). Notably, approximately 23% of patients presenting with hypertensive crises
Hypertensive emergency
SBP/DBP >180/110-120 mmHg WITH evidence of new or worsening targetorgan damage
Asymptomatic markedly elevated inpatient BP (2024 AHA Scientific Statement)
SBP/DBP >180/110-120 mmHg WITHOUT evidence of new or worsening target-organ damage
Inpatient setting only
Severe hypertension (2025 AHA/ACC Guideline)
Markedly elevated BP WITHOUT acute target organ damage
Allsettings(inpatientandoutpatient)
Component Target Organ Examples of Acute Target-Organ Damage
B Brain
A Arteries
R Retina
K Kidney
H Heart
Hypertensive encephalopathy, intracranial hemorrhage, acute ischemic stroke
Aortic dissection
Acute hypertensive retinopathy with papilledema
Acute kidney injury
Acute myocardial infarction, unstable angina, acute left ventricular failure with pulmonary edema
“Updated terminology instead emphasizes the presence or absence of acute target organ injury as the key determinant of management.”
have previously undiagnosed hypertension.
Asymptomatic Elevated BP vs. Hypertensive Emergency
The critical distinction between asymptomatic markedly elevated BP and hypertensive emergency is the presence or absence of acute target organ damage.
Asymptomatic markedly elevated BP is defined as systolic BP greater than 180 mmHg or diastolic BP greater than 110–120 mmHg without evidence of acute target organ injury. It is not associated with increased short-term morbidity or mortality
continued on Page 20
BARKH
Table 2: Target-Organ Damage in Hypertensive Emergencies: The BARKH Acronym
Table 1: Classification of Markedly Elevated Blood Pressure
from Page 19
and can generally be managed with gradual medication adjustment and outpatient follow-up.
Patients may report nonspecific symptoms such as headache, dizziness, or chest discomfort; however, these symptoms alone do not indicate acute target organ injury. Medication nonadherence is the most common underlying cause, though other contributing factors include acute illness, pain, anxiety, sleep deprivation, volume overload, and medications that increase BP.
Hypertensive emergencies, by contrast, require immediate BP reduction to prevent further endorgan damage. These conditions can be conceptualized using the BARKH framework— Brain, Aorta, Renal, Kidney, and Heart—which highlights the major organ systems affected (Table 2).
Management often requires admission to a higher level of care for continuous BP monitoring, evaluation and treatment of target organ injury, and administration of parenteral antihypertensives. These events are associated with substantial morbidity and in-hospital mortality.
A key clinical principle is that BP values alone do not reliably predict the presence of acute target organ injury. Both the absolute BP level and the rate of BP elevation influence risk. Rapid increases in BP—even to levels such as 160/100 mmHg in a previously normotensive patient—may result in severe injury, particularly involving the cerebral vasculature.
Inpatient Management: Avoiding Overtreatment
Although asymptomatic elevated BP is much more common than hypertensive emergencies, optimal management strategies in hospitalized patients remain unclear.
Despite limited evidence supporting acute pharmacologic intervention, treatment is

frequently initiated—often to meet administrative transfer requirements (e.g., SBP <180 mmHg for unit acceptance) rather than clinical indications.
In general, rapid BP reduction with as-needed parenteral antihypertensives should be avoided. Abrupt BP lowering may result in hypoperfusion due to loss of autoregulation and lead to adverse outcomes.
Unnecessary acute treatment of asymptomatic markedly elevated BP has been associated with increased risk of hypotension, acute kidney injury, myocardial injury, and prolonged hospital length of stay.
Management should instead focus on:
• Confirming accurate BP measurement
• Identifying reversible causes (e.g., pain, anxiety, sleep deprivation, volume overload, acute illness)
• Reviewing medication lists and assessing adherence
• Identifying medications that may contribute to elevated BP
Reviewing outpatient BP measurements, when available, can help determine whether chronic hypertension is present and guide appropriate follow-up.
If antihypertensive therapy initiation or adjustment is necessary during hospitalization, oral medications are preferred, and gradual BP reduction is recommended. BP may require several days to weeks to stabilize following medication changes.
Management of Hypertensive Emergencies
In adults with a hypertensive emergency, admission to an intensive care unit is recommended for continuous BP monitoring, evaluation of target organ injury, and administration of parenteral antihypertensive therapy.
Common forms of acute hypertension-related target organ damage include:
• Acute heart failure or pulmonary edema
• Acute ischemic stroke
• Intracerebral hemorrhage
• Hypertensive encephalopathy
• Acute kidney injury
Aortic dissection is the least common but among the most critical presentations.
Hypertensive emergencies require immediate BP reduction to prevent or limit further target organ damage. In nonpregnant adults without stroke, BP management depends on the specific clinical scenario (Table 2).
For most hypertensive emergencies:
• Reduce SBP by no more than 25% within the first hour
• If stable, reduce BP to approximately 160/100–110 mmHg over the next 2 to 6 hours
• Gradually normalize BP over the subsequent 24 to 48 hours toward the patient’s chronic BP goal (typically <130/80 mmHg)
Intravenous antihypertensives available for treatment are outlined in Table 3. Selection of an appropriate agent should be guided by patient-specific factors, comorbidities, and the type of target organ injury present.
What Changed (and Why It Matters)
The shift away from the term hypertensive urgency reflects a
Comorbidity
Acute aortic dissection
Acute pulmonary edema
Acute coronary syndromes
Acute kidney injury
Eclampsia or preeclampsia
Perioperative hypertension (BP > 160/90 mmHg or SBP elevation > 20% of the perioperative value that persists for > 15 min)
Acute sympathetic discharge or catecholamine excess (e.g., pheochromocytoma)
Acute intracerebral hemorrhage
Acute ischemic stroke
Preferred Drugs
Clevidipine, esmolol, labetalol, nicardipine
Clevidipine, nitroglycerin, nitroprusside
Esmolol, labetalol, nicardipine, nitroglycerin
Clevidipine, fenoldopam, nicardipine
Hydralazine, labetalol, nicardipine
Clevidipine, esmolol, nicardipine, nitroglycerin
Clevidipine, nicardipine, phentolamine
Clevidipine, nicardipine, esmolol, labetalol, hydralazine
Clevidipine, nicardipine, esmolol, labetalol, hydralazine
BP Goals
SBP ≤120 mmHg ideally within 20 min; HR ~60 bpm
SBP ~140 mmHg within 1 hr
SBP ~140 mmHg within 1 hr; maintain DBP >60 mmHg
25% reduction in first hr, then to ~160/100-110 mmHg over 2-6 hr
SBP ~160 mmHg; target DBP ~85 mmHg
Individualized based on baseline and surgical context
Avoid overly aggressive reduction; gradual lowering preferred
SBP 130-140 mmHg; avoid SBP <130 mmHg; if initial SBP >220 mmHg target 160-180 mmHg
If receiving thrombolytics: ≤185/110 mm Hg before, ≤180/105 mmHg after; Otherwise: no treatment unless SBP ≥220 mmHg or DBP ≥120 mmHg
Table 3: Intravenous antihypertensive drugs for treatment of hypertensive emergencies in patients with select comorbidities
broader evolution in clinical thinking: moving from rigid numeric thresholds toward a more nuanced, patientcentered assessment of risk.
By focusing on target organ injury rather than BP alone, clinicians can avoid unnecessary interventions, reduce harm, and better align treatment with the underlying pathophysiology
ABOUT THE AUTHORS

Dr. Savidge is an emergency medicine pharmacy resident at the University of Maryland Medical Center in Baltimore. She serves on the career development committee and communications committee for the SAEM Academy of Emergency Medicine Pharmacists.

Dr. Gartner is an emergency medicine pharmacist and clinical toxicologist at University of Florida Health in Jacksonville and Florida Poison Control. She serves on the communications committee for the SAEM Academy of Emergency Medicine Pharmacists.
Asymptomatic Elevated Blood Pressure vs Hypertensive Emergency: What Matters
Asymptomatic Markedly Elevated Inpatient Blood Pressure
• Definition: Systolic blood pressure >180 mmHg or diastolic blood pressure >110–120 mmHg without target organ damage
• Key point: Common and often transient; low short-term risk
• Do: Confirm accurate measurement and assess for subtle organ injury
• Address: Pain, anxiety, illness, volume status, medication issues
• Management: Adjust oral therapy; avoid intravenous or rapid lowering
• Risk: Overtreatment can cause hypotension, hypoperfusion, and organ injury
Hypertensive Emergency (Non-Stroke, Non-Pregnant)
• Definition: Systolic blood pressure >180 mmHg or diastolic blood pressure >110–120 mmHg with target organ damage
• Common: Heart failure, acute kidney injury, encephalopathy, hemorrhage, aortic dissection
• Management:
o Reduce systolic blood pressure ≤25% in first hour
o Then to ~160/100–120 mmHg in 2–6 hours
o Gradual normalization over 24–48 hours
• Exceptions: Aortic dissection, pheochromocytoma crisis, pregnancy-related conditions
• Setting: Intensive care unit with intravenous antihypertensives
• Key principle: Treat the organ injury, not just the number

From Scene to Emergency Department: Managing Behavioral Emergencies Across Systems
By Christian Holt and Katherine Dowdell, MD
At a Glance
• Why this matters now: Behavioral emergencies make up a growing share of emergency department visits, yet care approaches differ significantly before and after hospital arrival.
• What you’ll learn: Key differences between emergency department and prehospital management of agitation, including training gaps, legal constraints and escalation risks.
• Who this is for: Emergency physicians seeking better understanding of emergency
medical services workflows and opportunities to improve coordination and patient outcomes.
Behavioral emergencies in the emergency department are challenging and can run the gamut from a patient asking for help with depression to a severely agitated patient who risks harm to self and others. Behavioral emergency concerns may comprise up to 6% to 10% of ED visits in many communities. Providing safe and appropriate care often requires significant departmental resources
and staff readiness. Within the broad scope of behavioral emergencies, agitation presents unique and immediate challenges.
Emergency Department Approaches to Agitation
Many models for behavioral triage and care of agitated patients in the emergency department have been developed not only to help reduce the need for physical restraints, but also to prevent the escalation of agitation and improve safety for both patients and staff. Patients who can exercise agency and access behavioral health care on a voluntary
“Behavioral emergency concerns may comprise up to 6% to 10% of emergency department visits in many communities.”
basis may be more likely to engage with their behavioral health care team in the future.
One approach to agitated patients, Project BETA, promotes best practices in the treatment of agitation in the emergency department and identifies overlapping dimensions of care. In addition to the creation of an evidence-based intervention strategy for agitated patients, another goal of the Project BETA guidelines is to promote patient trust in emergency psychiatry resources so patients may be willing to seek care earlier in a future behavioral crisis, ideally well before reaching a highly agitated state.
A key goal of the Project BETA guidelines is to encourage patients to seek help earlier in a behavioral health crisis—ideally before reaching a highly agitated state.
Prehospital Realities and Constraints
However, care strategies like Project BETA and the regulatory guardrails around the use of restraints are only effective after the patient has entered the emergency department. In many cases, the patient—or a third party on their behalf—has requested assistance by calling 911. Often, the patient’s outpatient behavioral health team lacks the resources to evaluate the patient in a timely manner and refers the patient for immediate assessment by members of law enforcement or EMS.
In stark contrast to the ED setting, many patients evaluated outside of the hospital for behavioral emergencies are not always afforded the opportunity to grant consent for evaluation. While EMS often lacks the legal authority to treat or transport a psychiatric patient without consent,

other behavioral health providers and emergency responders may be able to trigger involuntary hospitalization. State law often relegates the legal authority to commit a patient for psychiatric evaluation against their will, by statute, to members of law enforcement, social workers, psychologists and physicians.
Training Gaps and Protocol Variability
EMS education is primarily focused on acute medical and trauma care. National EMS education standards offer limited training in behavioral emergencies and do not explicitly require de-escalation techniques as a core competency.
EMS protocols define the scope of treatment provided by EMS personnel and may outline specific treatment options. They often include behavioral emergency protocols, which can vary from system to system and meet specific local needs.
These protocols may provide some guidance for assessing and treating agitation in the prehospital setting. While every community has different needs, consensus guidelines are available to assist in the development of EMS protocols for the safe and effective evaluation and treatment of agitation.
Training, Protocols, and System Variation
EMS training and education are primarily focused on the assessment and treatment of acute illness and trauma. Nonmedical responders, by contrast, may have training that covers state laws about emergency psychiatric commitment National EMS education standards, which guide the development of state and local courses for EMTs and paramedics, are limited in the scope of training for behavioral emergencies and do
on Page 25

“For emergency medical services, time is often of the essence once patient contact is made so the responding unit can return to service quickly to handle the next emergency.”
continued from Page 23
not explicitly consider de-escalation techniques as a required knowledge domain for EMS certification.
EMS protocols define the scope of treatment provided by EMS personnel and may outline specific treatment options. They often include behavioral emergency protocols, which can vary from system to system and meet specific local needs.
These protocols may provide some guidance for assessing and treating agitation in the prehospital setting. While every community has different needs, consensus guidelines are available to assist in the development of EMS protocols for the safe and effective evaluation and treatment of agitation.
Challenges in the Field
Despite recommendations from consensus guidelines promoting deescalation strategies and agitation scales in EMS protocols, opportunities for de-escalation—including environmental controls that minimize stimulation—are more difficult to facilitate outside of the hospital. Comparatively, the ED is a controlled environment with the ability to request additional staff at a moment’s notice in an emergency. By contrast, an
Pulse Points
Key clinical and practice takeaways:
EMS unit responding to a behavioral patient’s emergency often consists of responders not previously known to the patient who have entered the patient’s home.
For EMS, time is often of the essence once patient contact is made so the responding unit can return to service quickly to handle the next emergency. This places pressure on both the EMS crew and the patient to reach a decision point quickly, which may escalate the situation. Additionally, the presence of law enforcement personnel on scene may inadvertently increase anxiety in agitated patients and further complicate the use of de-escalation techniques by EMS
Opportunities for Coordination and Improvement
Emergency physicians can engage local stakeholders and the EMS medical control system to facilitate safe and effective care for agitated patients who will arrive in the ED via EMS. A multidisciplinary approach that involves local EMS, behavioral health providers and law enforcement is likely to lead to better coordination among the sometimes disjointed elements of the care systems that behavioral health patients encounter.
An encouraging number of communities have allocated funding
for dedicated mental health teams to respond to individuals with behavioral health challenges before they are in crisis and have no option but to request help via the 911 system. These systems have different staffing models but frequently include a social worker and paramedic. One key element of many of these programs is that they are not bound by the limitations of the EMS system with respect to transport destination. Instead of transporting to the ED, these behavioral health teams might treat in place and follow up later, or transport the patient directly to appropriate behavioral care and bypass the ED altogether.
Conclusion
Despite having limited training in behavioral health, EMS personnel often have first contact with patients experiencing behavioral emergencies. The regulatory framework in hospitals that is designed to safeguard patients and staff is much more limited in the prehospital setting, where opportunities for rapid escalation are greater. Escalation in the field may worsen the patient’s presentation at the ED and undermine the patient’s willingness to access the behavioral health system in the future.
Emergency physicians should understand the prehospital resources in their community and engage with local stakeholders to safely treat patients with agitation before and after they arrive at the ED—and to improve outcomes for all behavioral health patients who seek help
• De-escalation starts before the emergency department—understand how emergency medical services constraints and scene dynamics shape patient presentation on arrival.
• Know your local system: engage with emergency medical services, behavioral health teams and law enforcement to improve coordination and reduce escalation risk.
• Training gaps matter—advocate for stronger emphasis on behavioral emergencies and de-escalation in emergency medical services education and protocols.
• Not every patient needs the emergency department—support community response models that allow treatment in place or direct transport to behavioral health care.
• Early interactions shape long-term trust—what happens in the field can influence whether patients seek care in future behavioral crises.
ABOUT THE AUTHORS


Christian Holt is a third-year medical student at the American University of the Caribbean School of Medicine.
Dr. Dowdell is an attending physician in the department of emergency medicine at Beth Israel Deaconess Medical Center and an instructor of emergency medicine at Harvard Medical School.
CAREER DEVELOPMENT
Behind the Scenes of Academic Publishing: Reflections From AEM E&T Fellow Editors-in-Training
For many early-career educators, academic publishing can feel opaque—a process that begins with submission and ends with a decision, with little visibility into what happens in between. Editorial fellowships offer a rare opportunity to step inside that process, providing hands-on experience in peer review, manuscript evaluation, and scholarly decisionmaking.
The Academic Emergency Medicine Education and Training (AEM E&T) Fellow Editor-in-Training program is designed to do just that. Over a
12-month term, fellows serve on the journal’s editorial board, participating in manuscript review, editorial discussions, and mentored decisionmaking while developing skills in writing, editing, and peer review.
The reflections that follow offer two complementary perspectives from fellows who participated in the program in 2025–2026. Together, they highlight both the structure of the editorial experience and the personal growth that comes from engaging deeply with the craft of peer review.
Understanding the Editorial Process
Natasha Aguirre, MD
Medical Education Science Fellow
The University of Colorado

As an earlycareer educator, the process of academic publishing can sometimes feel like a black box. Manuscripts move from submission to decision, and much of what happens
Dr. Natasha Aguirre
in between remains unseen. Serving as a Fellow Editor-in-Training with AEM E&T offered me the opportunity to step behind the scenes and experience the editorial process firsthand.
The AEM E&T editorial board is composed of leaders in medical education scholarship who guide the peer review and publication of research that advances emergency medicine education. As a fellow, I was able to participate in the full editorial experience, from reviewing submitted manuscripts to observing the discussions that shape editorial decisions.
Critically evaluating medical education research alongside experienced editors sharpened my approach to peer review and helped me better understand what makes a strong manuscript. I began to appreciate how editors weigh clarity, organization, methodological rigor, and potential impact. Seeing these considerations unfold in real time helped me become a more thoughtful reviewer and a more intentional writer.
One of the most rewarding aspects of the fellowship was staying closely connected to the evolving landscape of medical education research. Reviewing manuscripts and following the work published in AEM E&T offered a unique perspective on emerging ideas and the questions educators across institutions are exploring. It was exciting to see where the field is heading and to feel, even in a small way, that I was contributing to the scholarly conversation.
Mentorship was central to the experience. Under the guidance of Dr. Esther Chen, fellows were supported not only in learning the mechanics of peer review and editorial decisionmaking but also in developing our own scholarly interests. Manuscripts were thoughtfully paired with fellows’ areas of interest, and the environment encouraged curiosity, reflection, and growth.
The fellowship also fostered meaningful connections. Participating in editorial board meetings provided the opportunity to learn from
experienced leaders in medical education, while smaller meetings with co-fellows created space for discussion and shared learning. Having a peer navigating a similar stage of training made the experience particularly valuable.
Reflecting on the year, the AEM E&T Editorial Fellowship provided more than an introduction to journal editing. It offered a supportive entry point into academic emergency medicine and medical education research.
The mentorship, collaboration, and insight into the editorial process have been invaluable as I transition into junior faculty, strengthening my skills and reinforcing my commitment to contributing to the scholarship that shapes how we educate the next generation of emergency physicians.
Learning the Craft of Peer Review
Juhi Varshney, MD Medical Education Fellow Emory University Department of Emergency Medicine

A manuscript arrives—a paper shaped by countless revisions, discussions, and decisions before it ever reaches peer
review. It tells a story: a problem identified, a study designed, results presented, and meaning constructed. By the time it reaches a reviewer, it has already traveled a long path.
As reviewers, we inherit a responsibility: how do we engage with that work in a way that helps it leave the process stronger than when it began?
As a fellow-in-training on the AEM E&T editorial board, I spent the past year exploring this question. Through editorial board meetings, I observed how experienced leaders approach challenges facing the journal—what questions they ask, how they interpret feedback, and how they arrive at decisions. In parallel, monthly fellow meetings created space to reflect on our own reviews, discuss manuscripts, and learn from those who bring scholarly work to life.
Over time, I developed a more deliberate approach to peer review. I begin with an initial read to understand the overall narrative, followed by a period of reflection before returning for a more detailed, line-by-line review. This process allows me to move from general impressions to specific, actionable feedback.
continued on Page 29
Dr. Juhi Varshney
“Editorial fellowships offer a rare opportunity to step inside that process, providing hands-on experience in peer review, manuscript evaluation, and scholarly decision-making.”
CAREER DEVELOPMENT
continued from Page 27
I also learned where to focus my attention: identifying areas where clarity can be improved, where arguments can be strengthened, and where claims need to be better aligned with the data. Just as importantly, I learned how to communicate feedback in a way that is constructive and actionable—offering suggestions that authors can meaningfully incorporate.
In this role, reviewers serve as a kind of mirror, reflecting both a manuscript’s strengths and the areas that can be refined. The goal is not simply to critique, but to help a paper become clearer, stronger, and more impactful.
Peer reviewing my colleagues’ work has also deepened my understanding of academic writing. It has sharpened
my sense of structure, strengthened my attention to rigor, and encouraged me to think more critically about study design and interpretation. Reviewing early versions of manuscripts provides insight into common challenges and opportunities for improvement— lessons that carry forward into my own scholarly work.
Before this experience, peer review felt intimidating. Over time, it became an opportunity for growth—both as a reviewer and as a writer. As this year comes to a close, the experience feels less like a discrete training period and more like the beginning of a new chapter: contributing as an independent peer reviewer within the broader community of medical education scholarship.
From Observer to Contributor
Taken together, these reflections highlight the value of early exposure to the editorial process in shaping
emerging scholars. Beyond learning how manuscripts are evaluated, fellows develop the skills to critically appraise research, communicate constructive feedback, and refine their own academic writing.
Equally important, the experience fosters mentorship, collaboration, and a sense of belonging within the academic community. By engaging directly with the processes that shape scholarly publication, fellows move from observing the system to actively contributing to it.
For early-career educators, stepping behind the scenes of academic publishing is not only instructive—it is formative, marking a transition toward deeper engagement in the scholarship that advances emergency medicine education.
Applications for the 2027–2028 Fellow Editor in Training program opens in December.
How an Editorial Fellowship Can Shape Your Career
Editorial fellowships such as the AEM E&T Fellow Editor in Training Program, offer more than exposure to the publishing process—they provide a foundation for long-term academic growth.
Skill Development
• Strengthens critical appraisal of research
• Improves academic writing and manuscript structure
• Builds confidence in providing constructive feedback
Scholarly Insight
• Reveals how editorial decisions are made
• Clarifies what distinguishes strong manuscripts
• Deepens understanding of research design and rigor
Professional Identity
• Transitions early-career clinicians from consumers to contributors
• Builds confidence as an independent peer reviewer
• Encourages engagement in medical education scholarship
Mentorship and Network
• Provides direct access to experienced editors and leaders
• Creates opportunities for longitudinal mentorship
• Connects fellows with a community of emerging scholars
Career Advancement
• Strengthens academic portfolio
• Demonstrates commitment to scholarship and service
• Opens doors to future editorial and leadership roles
Bottom line: An editorial fellowship is not just training— it is an entry point into the community and craft of academic medicine.
CAREER DEVELOPMENT

Beyond Mentorship: Understanding Advising, Mentorship, and Sponsorship in Academic Emergency Medicine
By Katherine Stewart, MD; Sarah Rabinowitz, MD; Tiffany Moadel, MD; Suzanne Bentley, MD on behalf of the SAEM Simulation Academy
At a Glance
• Why this matters now: Mentorship is increasingly tied to academic productivity, promotion, and leadership advancement, yet many clinicians lack clarity on how advising, mentorship, and sponsorship differ—and why that distinction matters.
• What you’ll learn: A practical framework to distinguish advising, mentorship, and sponsorship, plus strategies to build an effective mentorship network and set expectations that drive meaningful career growth.
• Who this is for: Emergency physicians, residents, fellows, and faculty seeking to intentionally develop mentorship relationships that support advancement, visibility, and long-term success.
Mentorship in academic emergency medicine is essential to career longevity and productivity, yet it is rarely examined with the nuance it deserves. During a recent panel hosted by SAEM’s Simulation Academy, simulation-trained emergency physicians Drs. Suzanne Bentley, Keegan McNally and Janice Shin-Kim reflected on their
experiences as both mentees and mentors.
Finding and Developing Mentorship
Mentorship often begins in structured environments, with assigned faculty advisers during residency or fellowship. Dr. ShinKim recalled her residency program director’s affirmation: “You are going to do this, you’re going to thrive in this, and let me help you get there.” While assigned mentorship may feel prescriptive, it often provides essential early-career scaffolding.

“Mentorship in academic emergency medicine is essential to career longevity and productivity, yet it is rarely examined with the nuance it deserves.”
However, many impactful mentorship relationships develop informally. Dr. McNally described a pivotal moment during residency when a mentor recognized potential he had not yet seen in himself: “I didn’t really consider simulation as a future path until she sat me down and said, ‘You seem pretty good at this… do you want to explore the opportunity?’” That simple act—naming a strength and opening a door—reshaped his career trajectory.
Advising, Mentorship and Sponsorship
A key framework discussed during the panel distinguishes among advisers, mentors and sponsors. As Dr. Bentley noted, advisers often support task completion, while mentors invest in understanding the individual and supporting long-term growth.
Mentorship is a developmental relationship that provides guidance, feedback and support over time. Sponsorship, by contrast, is an advocacy relationship in which a senior individual actively promotes and creates opportunities for a junior colleague.
This conceptual spectrum is increasingly recognized in academic medicine, with advising, mentoring, and sponsorship as understood as distinct roles that each contribute to career development. Notably, evidence suggests that sponsorship — more than mentorship alone — is often associated with career advancement and leadership opportunities.
Dr. Shin-Kim illustrated this through her own experience: “She looked at my CV and started nominating me… really
thinking about how to position me better than the year before.”
Setting Expectations for Effective Mentorship
Even when mentorship develops organically, effective relationships require structure. Panelists emphasized the importance of setting expectations around communication preferences, meeting frequency, and shared goals.
A common failure point is lack of follow-through, which can erode trust. As Dr. Bentley observed, “You meet… and then you meet again… and nothing has moved forward.” Closing meetings with clear next steps, and maintaining accountability, are simple but effective strategies.
Building a Mentorship Network
Rather than relying on a single mentor, panelists emphasized building a “mentorship team.” Different mentors can support different domains,

continued from Page 31
including clinical practice, simulation, career development, and personal growth. As Dr. Bentley summarized, “You may need a simulation mentor, a clinical mentor, and a life mentor.”
This network-based model allows for more targeted guidance and reflects evolving approaches to mentorship in academic medicine. Within simulation, this may be particularly relevant as simulation emphasizes communication, reflection, and systems thinking, all skills that naturally extend into mentorship and career development. Professional organizations such as SAEM often facilitate these connections, with mentorship relationships frequently beginning through brief interactions at meetings, and developing through intentional follow-up and collaboration.
The Dual Identity: Always a Mentee, Always a Mentor A consistent theme was the absence of a clear transition from mentee to mentor. Dr. Shin-Kim described this as “always a mix of both,” while Dr. McNally identified a “chain throughout your entire career.” This reflects the graduated responsibility of medical training, where individuals simultaneously teach and learn. As Dr. Bentley emphasized, “you’re doing it correctly when you’re
Pulse Points
Key clinical and practice takeaways:
mentoring others and you’re still being mentored.”
Mentorship is increasingly recognized as a component of academic productivity and promotion, though expectations and documentation vary by institution, creating challenges in defining and measuring meaningful mentorship. Nevertheless, its long-term impact— including mentee development, collaboration, and scholarly output— remains highly valued within academic emergency medicine.
Conclusion
Mentorship in academic emergency medicine is not a single relationship, but a dynamic, evolving process. It is best understood as an ecosystem that includes advising, mentorship, and sponsorship, with each playing a distinct role as career needs change.
Effective mentorship requires clarity and structure. Explicit expectations around communication, goal-setting, and follow-through are essential, as many challenges stem from unspoken assumptions. These relationships are also bidirectional—mentees who prepare, and follow through, build trust, creating opportunities for deeper investment and growth.
Rather than relying on a single mentor, individuals benefit from cultivating a network that provides complementary guidance across clinical, academic, and personal domains. Most clinicians function
• Mentorship alone is not enough—actively seek sponsorship, as it is more strongly linked to career advancement, visibility, and leadership opportunities.
• Build a mentorship network, not a single relationship—different mentors should support clinical work, academic growth, and personal development.
• Set expectations early—clarity around goals, communication, and followthrough is what turns mentorship from passive to productive.
• Follow-through builds trust—consistent preparation and accountability are what move relationships from mentorship to sponsorship.
• You are always both—developing as a mentee and a mentor simultaneously is essential to long-term growth and contribution in academic emergency medicine.
simultaneously as both mentors and mentees, and developing these skills early supports ongoing growth, and strengthens the broader academic community
ABOUT THE AUTHORS




Dr. Stewart is a simulation fellow with the SAEM Simulation Academy and an assistant professor of emergency medicine at Tufts University School of Medicine. She works clinically at Maine Medical Center.
Dr. Rabinowitz is a medical simulation fellow at Northwell Health and a simulation fellow with the SAEM Simulation Academy. She serves as an attending emergency physician at Long Island Jewish Medical Center.
Dr. Moadel is president of the SAEM Simulation Academy and director of the medical simulation fellowship within Northwell Health. She is an assistant professor of emergency medicine at the Zucker School of Medicine at Hofstra/Northwell.
Dr. Bentley is chief wellness officer at Elmhurst Hospital, immediate past president of the SAEM Simulation Academy, and a professor at the Icahn School of Medicine.
ABOUT THE PANELISTS


Dr. Bentley is chief wellness officer at Elmhurst Hospital, immediate past president of the SAEM Simulation Academy, and a professor at the Icahn School of Medicine.
Dr. McNally is director of the medical simulation fellowship and director of the resident simulation program at Brown University Health, where he also serves as an assistant professor of emergency medicine.
Dr. Shin-Kim is director of emergency medicine simulation and an assistant professor in the department of emergency medicine at Columbia University Medical Center.
CLIMATE CHANGE & HEALTH

Emergency Medicine in a Changing Climate: 10 Practical Tools for Clinical Practice
By Adrian Cois, MD
At a Glance
• Why this matters now: Climaterelated illness is increasingly shaping emergency department volume, acuity, and patient presentations.
• What you’ll learn: A practical, evidence-informed framework with 10 actionable tools to integrate climate into bedside care, education, and quality improvement.
• Who this is for: Emergency physicians, residents, and educators seeking clinically relevant ways to address climate in everyday practice.
Every shift, clinicians assess temperature, pulse, blood pressure, respirations, oxygen saturation, and pain. A seventh vital sign is often overlooked: climate. It is increasingly shaping how patients present to emergency departments and may warrant more deliberate attention.
Emergency medicine sits at the intersection of climate-related illness amplified by a warming world. A recent scoping review of curricula identified only 17 published climaterelated curricula across all graduate medical education specialties, despite emergency medicine’s disproportionate exposure to these conditions.
What follows is a practical framework built around a simple concept: Educate, Mitigate, and Advocate. This framework offers 10 scalable, evidence-informed tools that align with existing quality and safety priorities.
Educate: Close the Knowledge Gap
Tool 1 — Reframe the message
Climate communication often relies on fear. While effective in headlines, fear can be less useful in clinical encounters. An alternative approach is to highlight co-benefits and use asset-based framing. Understanding where patients fall on the spectrum of climate concern can help tailor

“Every shift, clinicians assess temperature, pulse, blood pressure, respirations, oxygen saturation, and pain. A seventh vital sign is often overlooked: climate.”
messaging. The Yale Program on Climate Change Communication’s “Six Americas” framework offers one practical model.
For a patient with COPD, this might sound like: “Let’s talk about what you can do during smoke season to protect your lungs.” For an administrator: “Reducing emissions may help decrease heat-related illness during peak months.”
Tool 2 — Educate patients at the bedside
For some patients, an ED visit is their only point of contact with the health care system in a given year. Even brief counseling can be impactful. Giudice and Rublee describe how this aligns with the American Board of Emergency Medicine’s Knowledge, Skills, and Abilities related to prevention and education.
In practice, clinicians might review AirNow.gov with a patient after a smoke-related exacerbation and
explain how to interpret the air quality index. During heat waves, medication review, hydration guidance, and information about cooling centers may be appropriate. Documenting these conversations similarly to tobacco counseling may help normalize the practice.
Tool 3 — Teach the teachers
Graduate medical education programs do not necessarily require standalone climate curricula. Content can be integrated into existing lectures in small increments. A model described by Kuczmarski et al., incorporates a single climate-health slide into standard didactics.
Faculty can insert pre-developed slides with minimal preparation, and learners often engage readily. Resources such as Climatehealthed. org provide evidence-based materials. Even small pilots, if evaluated and shared, may contribute meaningfully to a limited evidence base.
Mitigate: Turning Sustainability Into Quality Improvement
While clinicians manage climaterelated illness, the U.S. health care sector contributes approximately 8.5% of national greenhouse gas emissions. If considered a country, it would rank among the top global emitters. Approximately three-quarters of these emissions originate in the supply chain.
Sustainability and quality improvement often share similar frameworks, offering opportunities for alignment.
Tool 4 — Quantify and document
When Oregon Health & Science University residency programs transitioned to virtual interviews during COVID-19, analyses estimated median savings of 0.47 metric tons of CO₂ and $490 per applicant per cycle—

continued from Page 35
the equivalent of carbon sequestered by 22 mature trees annually.
Incorporating a sustainability component into QI projects—tracking emissions, waste reduction, and energy use—may provide additional value and insight.
Tool 5 — Green the fleet
Austin–Travis County EMS transitioned to hybrid and biodiesel ambulances, reducing emissions by 14.2 metric tons of CO₂ annually while lowering fuel costs. This is roughly equivalent to removing 30 cars from the road.
Potential interventions include antiidling systems, route optimization, and green procurement policies. Framing these changes in terms of cost savings and operational efficiency may support adoption.
Tool 6 — Green the supply chain
Virginia Mason Medical Center redesigned elements of its supply chain, prioritizing reprocessed devices and saving $3 million while diverting 19,000 pounds of waste over three years. Similarly, a surgical residency program described by Vacharathit et al. reduced CO₂ equivalents by 717 metric tons annually over five years.
Pilot efforts might include reprocessed pulse oximetry probes or improved waste segregation.
Pulse Points
Key clinical and practice takeaways:
These initiatives can be framed as cost reduction, risk mitigation, and alignment with emerging accreditation priorities.
Tool 7 — Make sustainability a standing QI metric
Departments may consider selecting one sustainability goal annually and applying a Plan-Do-Study-Act (PDSA) cycle. Examples include motionsensor lighting or optimized afterhours HVAC use.
Tracking both emissions and cost savings alongside traditional QI metrics may reinforce the role of environmental stewardship within clinical excellence.
Advocate: Leverage Physician Credibility to Support Change
Tool 8 — Plan for climate-related disasters
Climate-related events often manifest as acute system stressors. During Hurricane Harvey in 2017, flooding reduced hospital capacity by nearly 40%, disrupting transfers and care delivery. Facilities with redundant power and flexible staffing models reported improved outcomes.
Regular tabletop exercises incorporating wildfire smoke, extreme heat, and flooding scenarios may strengthen preparedness.
Tool 9 — Incorporate sustainability into purchasing decisions
During contract negotiations, institutions may request Environmental Product Declarations or
• Climate is already shaping emergency department case mix—recognizing patterns (heat, smoke, flooding) can sharpen clinical anticipation and patient counseling.
• Small actions scale: a 30-second bedside conversation or a single curriculum slide can begin integrating climate into routine practice.
• Treat sustainability like quality improvement—track emissions, waste, and cost savings alongside traditional performance metrics.
• Operational decisions are clinical decisions: supply chain, fleet, and energy choices directly affect patient outcomes and system resilience.
• Trainees have an entry point—climate-related projects align with accreditation requirements and offer meaningful opportunities for scholarship and leadership.
Scope 1–3 emissions data. Including sustainability as a procurement criterion can align financial and operational goals with environmental considerations.
Framing these decisions around resilience—for example, protecting infrastructure during grid instability— may support broader engagement.
Tool 10 — Mentor and support trainees
Climate health offers opportunities for resident scholarship aligned with ACGME competencies. Potential projects include:
• ED heat protocol audits
• Waste stream analyses
• Patient education initiatives during smoke events
• Incorporating environmental factors into morbidity and mortality reviews Presenting results locally or nationally may help build momentum. Faculty engagement can play an important role in encouraging trainee participation.
Three Things to Try This Month
• Teach one thing: Incorporate air quality or heat risk into a patient discussion and document it as preventive counseling.
• Change one thing: Identify a waste or energy opportunity and initiate a small QI cycle.
• Share one thing: Bring a relevant data point or success story to a meeting or conference.
The climate is our seventh vital sign. We already measure it in the asthma spikes after wildfire smoke, the renal colic during heat waves, and in the surge after every flood. The question is whether we will also manage it and improve it, as we do every other vital sign we care for.
ABOUT THE AUTHOR

Dr. Cois is an assistant professor of emergency medicine at Oregon Health & Science University in Portland, Oregon. He has authored publications in Annals of Emergency Medicine, Wilderness & Environmental Medicine, and the Journal of Graduate Medical Education.
CLIMATE CHANGE & HEALTH

From Climate Shift to Clinical Impact: Vector-Borne Diseases in a Warming World
By Ana Ritz, DO, and Kevin Watkins, MD, on behalf of the SAEM Climate Change and Health Interest Group and the SAEM Wilderness Medicine Interest Group
At a Glance
• Why this matters now: Climate change is rapidly expanding the range and transmission of vector-borne diseases, including those increasingly encountered in the United States emergency department setting
• What you’ll learn: How shifting vector ecology is driving disease patterns, which infections are emerging domestically, and what this means for clinical awareness and prevention
• Who this is for: Emergency medicine residents and medical students seeking practical context on evolving infectious risks and their implications for frontline care
Climate change is already reshaping the transmission and
geographic reach of vector-borne diseases, with impacts expected to intensify in the coming decades. Globally, diseases such as malaria, dengue, Zika and chikungunya remain leading causes of morbidity and mortality. In the United States, the burden is shifting rapidly; reported cases of tick-borne illnesses, including Lyme disease, Rocky Mountain spotted fever and anaplasmosis, have more than doubled in the past 15 years. These now represent the vast majority of domestically acquired vector-borne infections.
This shift is driven by a complex interplay of environmental changes, including climate variability, land-use shifts and ecosystem disruptions. Understanding interactions among pathogens, vectors, hosts and
human behavior is critical for predicting risk and guiding future public health strategies.
Climate Change and Vector Ecology
Anthropogenic greenhouse gas emissions have raised global temperatures by approximately 1 C above preindustrial levels, contributing to more frequent extreme heat events and altered precipitation patterns. If current trajectories continue, a 4-5 C increase by the end of the century could fundamentally alter the public health landscape.
Vectors such as mosquitoes and ticks are ectothermic, meaning their internal physiological processes are highly sensitive to external temperatures. Warmer conditions

“Climate change is already reshaping the transmission and geographic reach of vector-borne diseases, with impacts expected to intensify in the coming decades.”
generally enhance vectorial capacity — the efficiency with which a vector transmits a pathogen — through several mechanisms:
• Increased survival and reproduction: Warmer winters reduce winter kill, allowing more vectors to survive into the next season. Increased humidity and precipitation further boost survival rates of both eggs and active adults. Life cycles may also shift in ways that increase vector populations.
• Accelerated pathogen development: The extrinsic incubation period — the time it takes for a pathogen to
develop within a vector — shortens at higher temperatures, allowing vectors to become infectious more quickly. Increased pathogen replication may also accelerate evolution, including the development of treatment resistance.
• Behavioral shifts: Warmer weather extends seasons of activity and increases feeding frequency.
• Geographic expansion: As previously uninhabitable regions warm, vectors migrate into new territories, bringing pathogens to immunologically naive human populations.
Beyond the vectors themselves, climate change also alters host ecology. It shifts migration patterns of birds and affects the population density of mammals that serve as natural reservoirs for disease. Human behavior also changes, including increased time spent outdoors in warmer weather. However, climate is not the sole determinant. Urbanization, international travel and the strength of public health infrastructure all interact with environmental factors to shape modern disease patterns.
continued on Page 41
“Understanding hosts and human guiding

“Understanding interactions among pathogens, vectors, human behavior is critical for predicting risk and guiding future public health strategies.”
CLIMATE CHANGE & HEALTH
continued from Page 39
The Global and Domestic Burden
Globally, the burden remains dominated by mosquitoes. Malaria, transmitted by Anopheles mosquitoes, still claims hundreds of thousands of lives annually. Meanwhile, Aedes mosquitoes spread dengue, Zika and chikungunya, while Culex species primarily drive transmission of West Nile virus.
In the United States, however, ticks are the primary threat, accounting for approximately 95% of reported vectorborne cases.
• Lyme disease: Caused by Borrelia burgdorferi, it remains the most prevalent infection. The range of its primary vector, the blacklegged tick (Ixodes scapularis), is expanding across the Northeast and Midwest.
• Emerging threats: Other species, such as the Lone Star tick, are migrating
Pulse Points
Key clinical and practice takeaways:
more rapidly, bringing associated illnesses into new regions.
• Mosquito trends: While less common than tick-borne illness in the U.S., mosquito-borne diseases are also changing. Southern states have seen a reemergence of locally acquired malaria in areas where it was once eradicated, as well as local transmission of diseases such as dengue. West Nile virus also continues to spread.
Prevention and Control Strategies
Addressing these threats requires a multitiered approach focused on personal protection, environmental management and robust surveillance. Personal protection: The first line of defense remains individual behavior. This includes using EPA-approved repellents (such as DEET or picaridin), wearing permethrin-treated clothing, performing diligent tick checks and showering promptly after outdoor activity.
• Vector-borne diseases are no longer “geographically fixed”—expect to see traditionally regional infections presenting in new U.S. locations
• Tick-borne illnesses now account for the vast majority of U.S. vector-borne cases—maintain a high index of suspicion, especially in expanding endemic areas
• Warmer temperatures shorten pathogen incubation in vectors, meaning faster transmission cycles and potentially earlier seasonal presentations
• Surveillance still lags behind reality—clinical recognition remains a critical early warning system in the emergency department
• Climate-driven disease patterns are a clinical competency, not just a public health issue—understanding them will increasingly shape frontline emergency care
Environmental and systemic management: Broader strategies include insecticide use, habitat modification and wildlife management. However, while these approaches can reduce vector populations, evidence directly linking large-scale environmental interventions to decreased human infection rates remains limited.
Effective surveillance is perhaps the most critical tool. Many regions rely on passive reporting of human cases, which often lags behind actual outbreaks. Strengthening active environmental surveillance, such as testing vectors directly, may be essential for early detection. Additionally, it is important for health care professionals to become familiar with vector-borne diseases that are expanding into previously unaffected regions.
Conclusion
Vector-borne diseases underscore the One Health concept: Human, animal and environmental health are inextricably linked. With roughly 60% of emerging infectious diseases originating in animals, the environmental transformations of a warming world are creating a perfect storm for pathogen transmission.
Addressing this challenge requires more than medical intervention. It demands integrated vector management, coordinated public health strategies and a sustained global effort to mitigate the underlying drivers of climate change.
ABOUT THE AUTHORS


Dr. Ritz is an emergency medicine resident and education chief at Cleveland Clinic Akron General. Dr. Watkins is associate program director at Cleveland Clinic Akron General and assistant professor at Northeast Ohio Medical University.

Severe Aortic Stenosis in the Unstable Emergency Department Patient: Implications for Resuscitation and Bedside Cardiac Ultrasound
By Thomas R. Holman, MD and Gregory P. Wu, MD
At a Glance
• Why this matters: Severe aortic stenosis can drive rapid hemodynamic collapse, and standard resuscitation strategies may worsen instability if the condition is unrecognized.
• What you’ll learn: How to identify severe aortic stenosis at the bedside using cardiac ultrasound and apply physiology-driven resuscitation strategies.
• Who this is for: Emergency clinicians managing undifferentiated shock, airway decisions, and high-risk resuscitations in unstable patients.
Introduction
Severe aortic stenosis (AS) is an often underrecognized yet critical contributor to cardiovascular collapse. In severe AS, fixed left ventricular outflow tract (LVOT) obstruction profoundly alters resuscitation physiology. Failure to identify this lesion early may lead to inappropriate hemodynamic management and catastrophic deterioration—particularly during procedural sedation and airway management. Early recognition with bedside cardiac ultrasound allows emergency physicians to tailor resuscitative strategies and mitigate preventable harm.
This review outlines key pathophysiologic principles of severe AS in unstable emergency department (ED) patients and emphasizes the role of point-ofcare ultrasound (POCUS) in rapid diagnosis, risk stratification, and informed resuscitation.
Pathophysiology of Severe
Aortic Stenosis in Hemodynamic Instability
Severe AS is defined by an aortic valve area ≤1.0 cm², peak jet velocity ≥4.0 m/s, or mean gradient ≥40 mm Hg. It is characterized by progressive leaflet calcification and immobility, resulting in worsening systolic
outflow obstruction. In response, the left ventricle develops concentric hypertrophy to generate higher ejection pressures. Although systolic function may initially be preserved, diastolic compliance declines and filling pressures rise.
The result is a functionally fixed cardiac output with limited ability to augment flow in response to metabolic demand. The ventricle becomes highly preload-dependent, requiring adequate filling time and pressure to maintain stroke volume. Impaired diastolic relaxation of the hypertrophied ventricle renders tachycardia and loss of atrial contraction poorly tolerated. Atrial fibrillation—particularly with rapid ventricular response—often leads to hemodynamic compromise.
Bedside Cardiac Ultrasound
POCUS is central to the ED evaluation of undifferentiated shock. Although comprehensive Doppler quantification of AS may not be feasible during resuscitation, focused cardiac ultrasound can identify structural abnormalities within minutes.
Findings suggestive of severe AS include:
• Heavily calcified, thickened aortic valve leaflets
• Markedly restricted leaflet excursion
• Concentric left ventricular hypertrophy
• Turbulent transvalvular flow on color Doppler
• Continuous-wave Doppler velocity >4 m/s
Recent studies by Alzahrani et al., Furukawa et al., and Gulic et al. demonstrate that emergency physicians and novice providers can identify significant valvular pathology with focused training. Recognition of calcified, immobile aortic valve leaflets in an unstable patient may be sufficient to alter immediate management. These findings should prompt caution, urgent cardiology consultation, and anticipation of hemodynamic instability.
Implications for Emergency Resuscitation
Management principles in severe AS
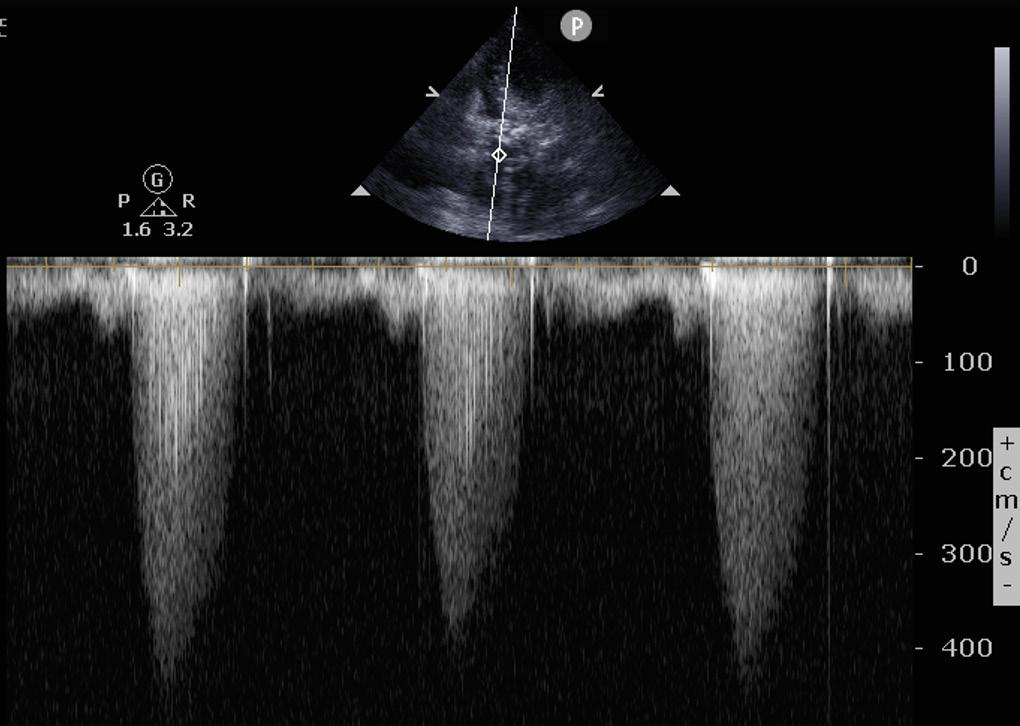
differ from those in other shock states and center on three key goals: Maintain adequate preload. In the setting of left ventricular hypertrophy, reduced ventricular compliance necessitates sufficient diastolic filling pressures to preserve stroke volume. Volume administration
must be carefully balanced: While these patients are preload-dependent, excessive fluid can precipitate pulmonary congestion due to impaired diastolic relaxation. Small, judiciously titrated fluid boluses with frequent
continued on Page 45
Figure 1: B-mode, parasternal long axis view during systole demonstrating heavy calcification of the aortic valve, thickening of the leaflets, and minimal leaflet mobility. The left ventricle is also significantly hypertrophied.
Figure 2: B-mode, apical five-chamber view during systole of the same patient with continuous wave Doppler through the aortic valve. The peak velocity through the AV is >4m/s, essentially diagnostic of severe AS.
“Failure
to identify this lesion early may lead hemodynamic management and catastrophic particularly during procedural sedation and

lead to inappropriate catastrophic deterioration— airway management.”
CRITICAL CARE
continued from Page 43
reassessment—ideally guided by bedside ultrasound—are preferred over large empiric infusions.
Maintain normal rate and sinus rhythm. With a fixed stroke volume, cardiac output is highly rate-dependent. Bradycardia can reduce perfusion, while tachycardia and loss of atrial contraction impair filling and worsen stroke volume. Careful rate and rhythm control is essential. Amiodarone is commonly used to manage tachydysrhythmias while minimizing the risk of bradycardia.
Maintain systemic vascular resistance. In the setting of left ventricular hypertrophy and fixed afterload, myocardial oxygen demand is elevated. Coronary perfusion— occurring predominantly during diastole—depends on adequate diastolic pressure and time. Both
Pulse Points
Key clinical and practice takeaways:
tachycardia and systemic hypotension should be avoided. Phenylephrine, which increases systemic vascular resistance without direct chronotropic effects, may be advantageous. Norepinephrine, with predominantly alpha-adrenergic vasoconstriction and modest beta-1 support, is also a reasonable choice for hypotension. In contrast, agents with significant inotropic or chronotropic effects (e.g., epinephrine, dobutamine) may be deleterious by increasing myocardial oxygen demand and shortening diastolic filling time. Medications that reduce systemic vascular resistance or provoke tachycardia should be used with caution.
Airway Management and Procedural Sedation
Airway management is particularly high risk in patients with severe AS. Induction agents reduce systemic vascular resistance and preload, while positive-pressure ventilation decreases venous return. Even brief hypotension may precipitate cardiovascular collapse in fixedoutput physiology. Alternatives to intubation, such as noninvasive ventilation, should be considered when appropriate.
Ketamine may preserve sympathetic tone but can increase heart rate and myocardial oxygen demand. Etomidate is often preferred for its relative hemodynamic stability, though data in severe AS are limited.
• Severe aortic stenosis creates fixed cardiac output—standard shock resuscitation (e.g., aggressive fluids, vasodilators) can worsen instability if applied reflexively.
• Use bedside cardiac ultrasound early: identifying a calcified, immobile aortic valve can immediately change management in undifferentiated shock.
• Protect preload and avoid tachycardia—small fluid boluses, rhythm control, and careful vasopressor selection are critical.
• Intubation is a high-risk moment: even brief hypotension or reduced venous return can precipitate cardiovascular collapse.
• When in doubt, slow down and individualize—physiology-driven resuscitation is more important than protocol-driven care in these patients.
A cautious, titrated approach to induction, with vasoactive agents immediately available, is recommended. Preintubation optimization is critical, and arterial and central venous access can facilitate continuous hemodynamic monitoring and ensure reliable vascular access. A deliberate sedation and vasopressor strategy may further reduce peri-intubation instability.
Conclusion
Without definitive valve intervention, symptomatic severe AS carries a poor prognosis, with survival typically limited to 2 to 4 years. In critically ill ED patients, failure to recognize severe AS may contribute to avoidable morbidity through misaligned resuscitative strategies. Although ED-specific randomized data are lacking, existing cardiology and perioperative literature support a tailored, physiology-driven approach to management.
Severe aortic stenosis fundamentally alters resuscitation physiology. Fixed LVOT obstruction, marked preload dependence, and sensitivity to hypotension necessitate deliberate hemodynamic control. Common emergency interventions— particularly sedation and intubation— carry substantial risk when AS is unrecognized. Integration of POCUS facilitates early identification, risk stratification, and more informed, patient-specific resuscitation.
ABOUT THE AUTHORS

Dr. Holman is an instructor of emergency medicine at Albany Medical Center in the divisions of emergency ultrasound and emergency critical care. He is board-certified in emergency medicine and has advanced echocardiography training, including ASCeXAM certification and registered diagnostic cardiac sonographer credentials.
Dr. Wu is an associate professor of emergency medicine and internal medicine at Albany Medical College. He is an emergency physician and medical intensivist and serves as clerkship director for critical care and associate fellowship director for resuscitation and emergency critical care.
EDUCATION & TRAINING
How Artificial Intelligence Is Transforming Emergency Medicine Education
By Scotty Jones; Christopher Gray, DO; Michael Zdradzinski, MD; and Nicole Prendergast, MD
At a Glance
• Why this matters now: Artificial intelligence is rapidly reshaping how emergency medicine trainees study, learn on shift, and process clinical information.
• What you’ll learn: Practical, high-yield ways to use artificial intelligence for targeted studying, clinical reasoning, and postshift reflection—along with key limitations to avoid overreliance.
• Who this is for: Medical students and residents seeking to improve efficiency, deepen understanding, and integrate new tools into real-world emergency medicine training.
Artificial intelligence (AI) has become a powerful tool in health
care. First introduced in emergency medicine (EM) around 2000 as a decision-support tool for triage optimization, AI has evolved into a routine resource for clinicians and learners, both in and out of the clinical environment. The widespread adoption of large language models marks an inflection point in medical education, introducing both significant opportunity and potential risk to learning and clinical practice.
This article examines the practical integration of AI into EM training from the perspective of medical students and residents. From navigating acting internships to optimizing on-shift teaching in residency, AI platforms are increasingly shaping how learners acquire knowledge, think, and
reflect. This article highlights both the advantages and the potential unintended consequences of incorporating AI into daily educational practice.
Medical Student Applications
Medical students must master large volumes of material within condensed time frames. When used appropriately, AI can enhance both learning and efficiency. The most effective approach is to engage AI in active learning rather than using it as a substitute. Several strategies allow medical students to integrate AI into their study processes.
Individualized Practice Questions
A triage-based approach to studying offers an efficient strategy for mastering large volumes of
“Artificial intelligence has evolved into a routine resource for clinicians and learners, both in and out of the clinical environment.”
information. Learners identify areas of weakness and focus accordingly, reducing time spent on topics already mastered. For example, during a lecture on the ear and hearing, a student may quickly grasp the anatomy but struggle to interpret Weber and Rinne tests. AI can generate targeted practice questions in multiple formats—interpretationbased, vignette-style, or rapid recall— allowing learners to focus precisely where needed.
This approach creates a strong feedback loop: generating targeted questions, assessing performance, identifying knowledge gaps, and repeating the cycle. Over time, it can also build a personalized, comprehensive question bank.
Personalized Image Mnemonics
Image-based mnemonics remain a popular learning tool in medical education. However, commercial resources can be costly and may not cover all topics. AI image generation allows students to create customized mnemonics tailored to their needs.
For example, a student seeking to recall key points about ventricular tachycardia (VT) might enter the following prompt:
I am a fourth-year medical student on an EM rotation. Create an image mnemonic for VT in which the scene is set in a cemetery with multiple tombstones (wide QRS), a lightning bolt (shockable rhythm) in the background, and a physician holding epinephrine in one hand and amiodarone in the other.
This method reinforces learning through dual encoding and mental mapping, linking visual imagery to clinical concepts.
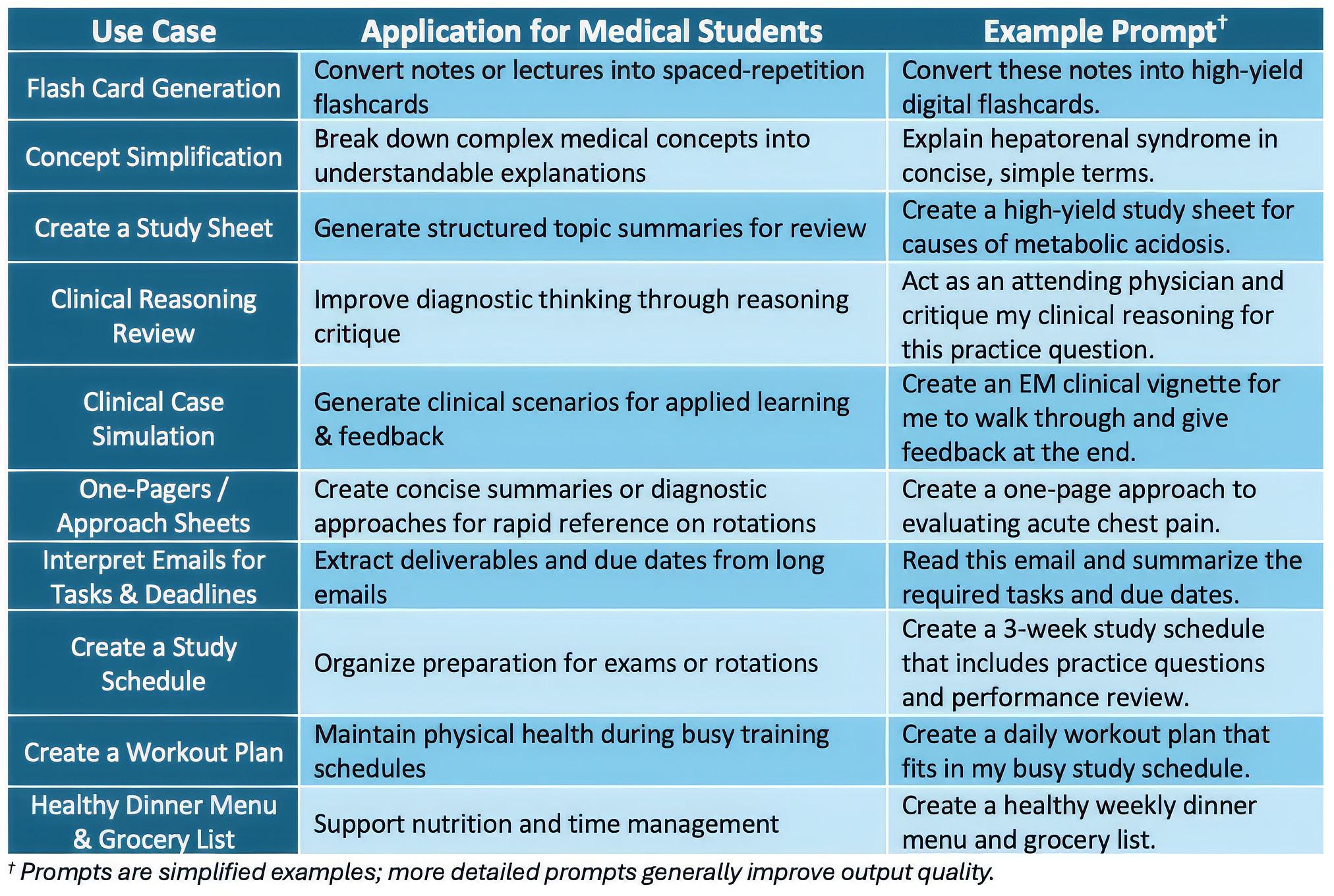
Improving Efficiency
AI offers a wide and rapidly expanding range of applications in medical education. While this section highlights several high-yield strategies, Table 1 outlines additional practical ways trainees can use AI to support learning and daily workflow.
Resident Applications
Residents must absorb large volumes of information while applying knowledge in dynamic clinical environments. Trainees are often inundated with resources, including question banks, podcasts, textbooks, and open-access medical education materials. During clinical shifts, attending physicians frequently reference studies or request rapid review of specific conditions or management nuances.
Many residents find that pairing new knowledge with a specific
patient case improves retention. For example, evaluating a patient with a COPD exacerbation provides immediate context for understanding pathophysiology, diagnosis, and management. AI can also help explain complex concepts and summarize the results, strengths, and limitations of multiple studies.
Early in training, the volume and depth of information can feel overwhelming. Prioritizing areas for growth becomes essential. AI can assist by organizing and summarizing post-shift reflections, helping residents make sense of numerous learning opportunities. A structured self-reflection guide (see Image 1) can be used to assess performance after each shift. Adding notes allows for
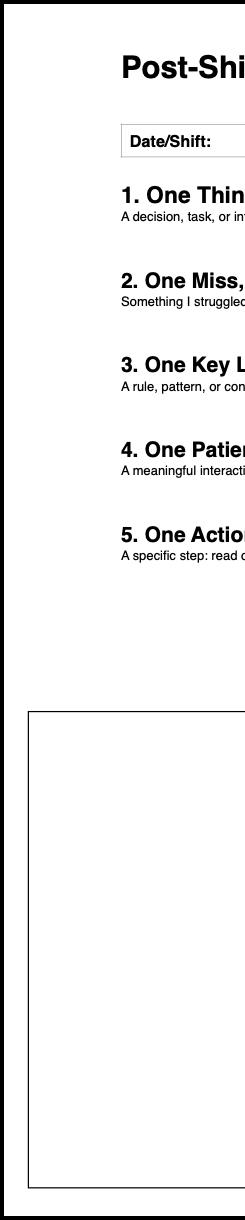
“Engaging rather students
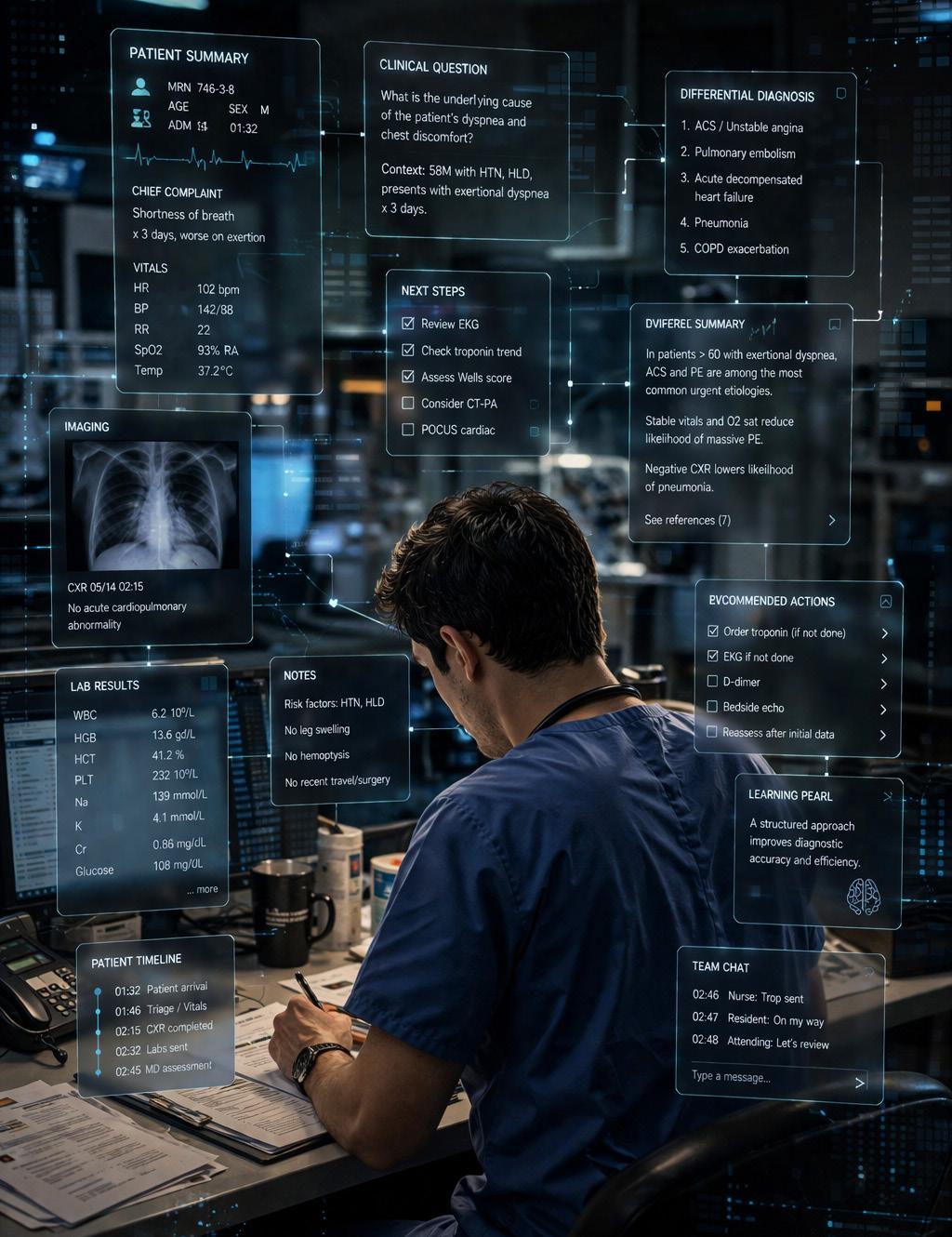
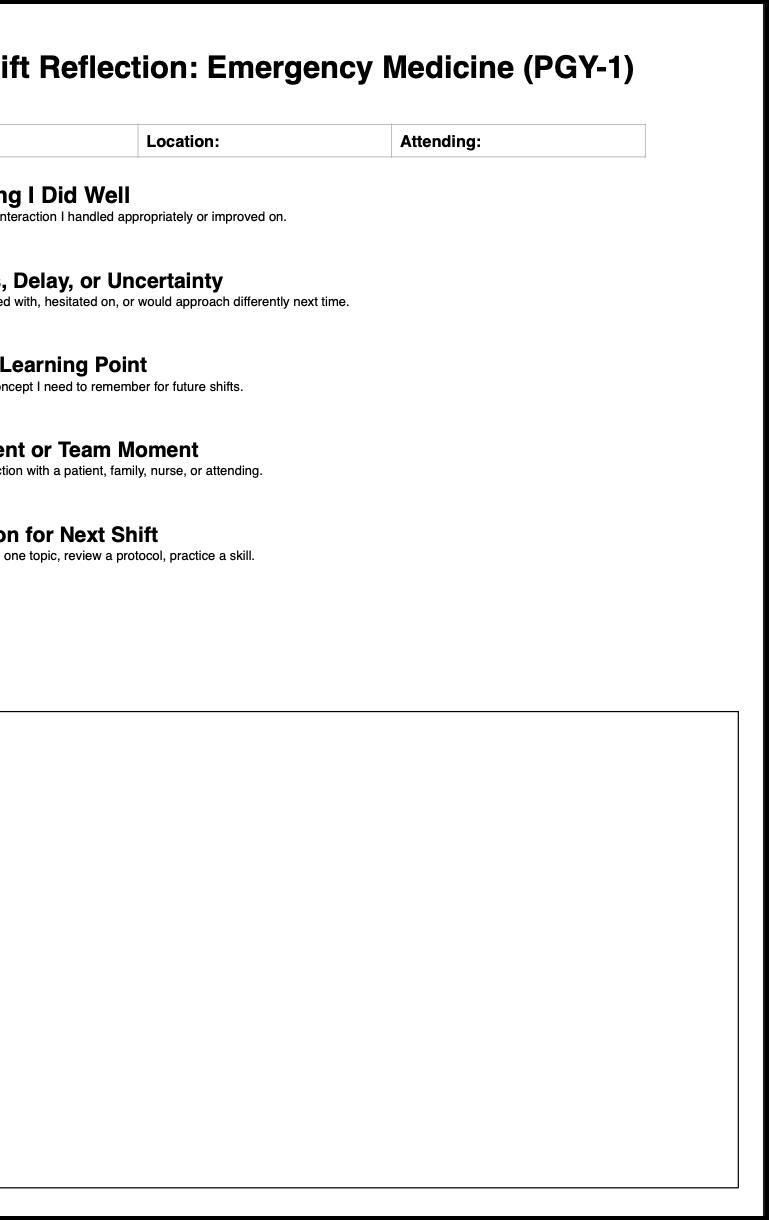
continued from Page 47
review of specific topics or reflection on particular experiences.
Using a self-reflection guide with targeted assessment questions helps residents identify recurring themes and track progress over time. This process enables learners to recognize strengths, address weaknesses, and focus on areas for continued growth.
Benefits and Limitations
AI can enhance clinical proficiency by expanding differential diagnoses, modeling evidence-based reasoning, enabling rapid literature searches, and providing point-of-care educational support. However, HIPAA compliance considerations may limit independent use, reinforcing AI’s role as a supplementary tool.
Generated content should always be verified against reliable sources for accuracy and completeness.
“Engaging artificial intelligence in active learning rather than using it as a substitute allows medical students to enhance both learning and efficiency.”
Pulse Points
Key clinical and practice takeaways:
• Use artificial intelligence to target knowledge gaps—generate focused practice questions instead of reviewing material you already know.
• Pair artificial intelligence with real patient cases to strengthen clinical reasoning and improve retention during shifts.
• Incorporate post-shift reflection with artificial intelligence to identify patterns, gaps, and areas for growth.
• Always verify artificial intelligence–generated content against trusted clinical resources before applying it in practice.
• Use artificial intelligence to support—not replace—core clinical thinking and decision-making.
Overreliance on AI—particularly before mastering clinical fundamentals—can hinder skill development. Similarly, using AI to automate rather than support diagnostic reasoning may negatively affect clinical judgment. When used thoughtfully, AI functions best as an adjunct. Strategic implementation helps ensure it supports, rather than replaces, core cognitive processes and human clinical decision-making.
Conclusion
AI is increasingly serving as a valuable learning partner in EM, offering personalized feedback, decision support, and enhanced educational experiences. Integrating AI into EM education can help address gaps in traditional training and foster interdisciplinary collaboration. SAEM provides comprehensive AI medical education resources to support educators and learners interested in further exploring this evolving landscape EDUCATION &
ABOUT THE AUTHORS




Scotty Jones is an osteopathic medical student and incoming postgraduate year 1 resident at Baylor Scott & White.
Dr. Gray is a postgraduate year 1 resident at Prisma Health Upstate.
Dr. Zdradzinski is an associate professor of emergency medicine at Emory University School of Medicine.
Dr. Prendergast is an assistant professor of emergency medicine at Wake Forest University School of Medicine.
EDUCATION & TRAINING
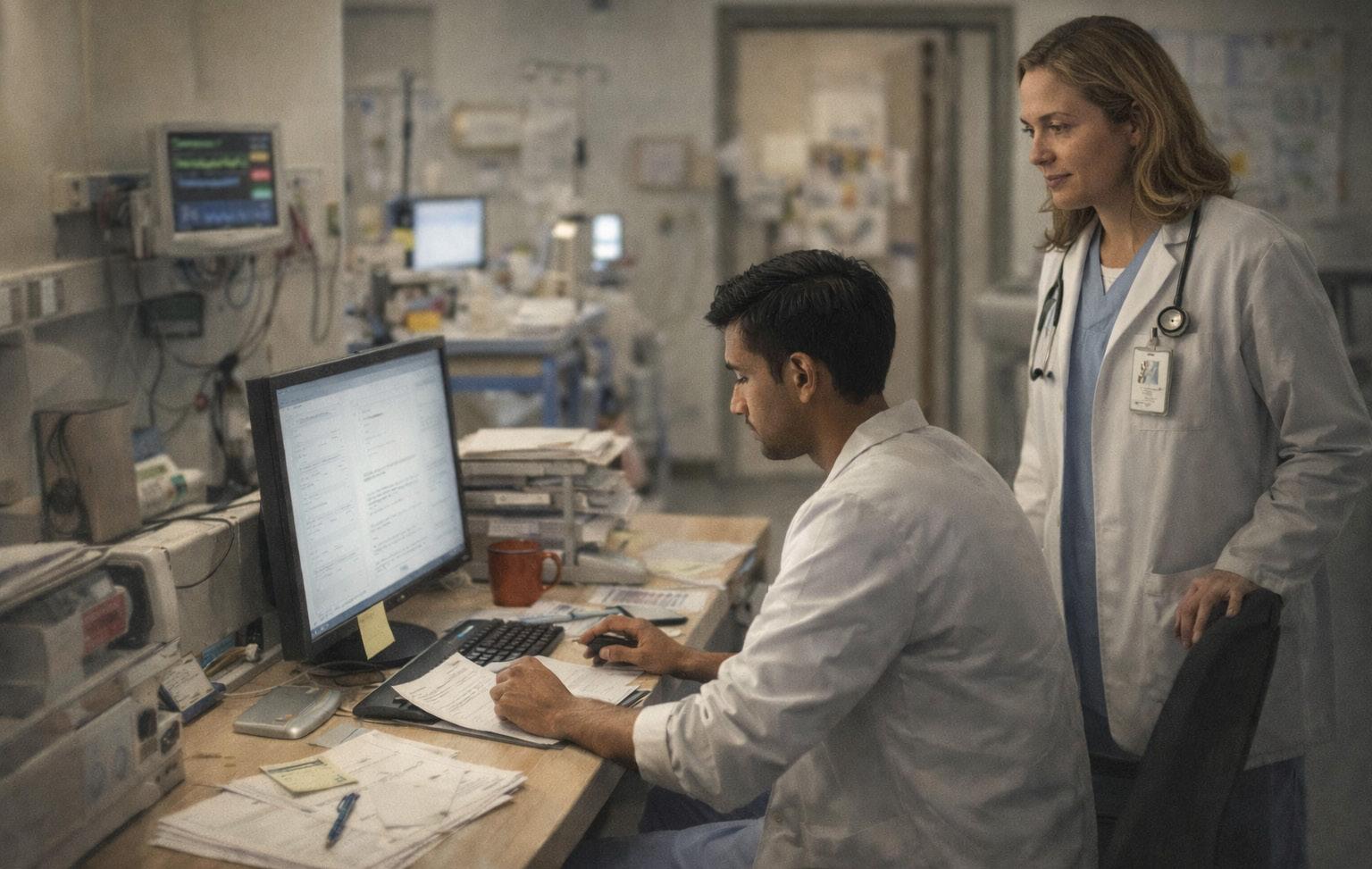
Making Efficiency a Teachable Skill in Emergency Medicine Training
By Aliza Abezis, MD; James VandenBerg, MD, MSc; Laura Sprunt, MD; Wayne Satz, MD; and Kraftin E. Schreyer, MD, MBA
At a Glance
• Why this matters now: Clinical efficiency is essential in emergency medicine, yet often under-taught in formal training despite increasing patient volume and operational demands.
• What you’ll learn: How one residency program uses direct observation, data-informed feedback, and coaching to help residents improve multitasking, prioritization, and workflow.
• Who this is for: Emergency medicine educators interested in practical approaches to developing efficiency as a core clinical skill.
Why Efficiency Training Deserves More Attention
Emergency medicine training is built on milestone-based competencies established by the Accreditation Council for Graduate Medical Education. While these milestones address many critical skills, clinical efficiency—particularly multitasking and task-switching—is addressed only indirectly.
In a specialty where timely decision-making and patient throughput are essential, developing efficiency is not just a productivity goal; it is a core clinical skill. Recognizing this gap, one residency program developed a structured
approach to help residents improve efficiency through targeted coaching and real-time feedback.
Identifying the Gap
At a large urban academic medical center with a three-year emergency medicine residency, program leadership observed variability in resident efficiency. While traditional evaluations provided valuable feedback, they did not always offer clear, actionable strategies for improvement.
At the same time, data from the electronic medical record provided insight into workflow patterns, including metrics related to patient throughput and timeliness.
These observations highlighted an opportunity to better support residents who were struggling with efficiency in a structured, individualized way.
Designing the Program Program leaders created a performance-learning initiative focused on helping residents strengthen efficiency skills through a combination of data-informed feedback and direct observation.
Key components of the program included:
• Individualized feedback: Residents received structured guidance based on observed workflow patterns and performance trends.
• Direct observation: Residents were paired with attending physicians for focused observation shifts during regular clinical duties.
• One-on-one debriefing: Each observation was followed by a dedicated discussion to identify strengths, challenges, and practical strategies for improvement.
• Ongoing coaching: Residents engaged in longitudinal feedback and advising to support continued growth. The program emphasized practical skill development, including prioritization, task-switching, and workflow organization in the emergency department setting.
Implementation in Practice
The initiative was integrated into existing residency structures, including regular meetings with
Pulse Points
Key clinical and practice takeaways:
program leadership. Participation expectations, program goals, and key efficiency concepts were clearly outlined to ensure alignment and transparency.
Importantly, the program was designed to be supportive rather than punitive, positioning efficiency as a skill that can be developed over time through deliberate practice and coaching.
Lessons Learned
Several insights emerged from the development and implementation of the program:
• Efficiency can be taught: With structured feedback and coaching, residents can develop stronger workflow habits and clinical organization.
• Direct observation is valuable: Realtime assessment provides insights that are difficult to capture through traditional evaluations alone.
• Data can guide conversations: Objective metrics help identify trends and focus feedback, but they are most effective when paired with individualized coaching.
• Culture matters: Framing the program as developmental encourages engagement and reduces stigma around performance improvement.
Discussion
As emergency departments continue to face increasing patient volumes and operational complexity, training
• Efficiency is a trainable clinical skill, not just an inherent trait—deliberate coaching and feedback can measurably improve performance.
• Direct observation reveals workflow gaps that traditional evaluations miss— build it into routine training, not just remediation.
• Use data to guide, not judge—pair performance metrics with individualized coaching to drive meaningful change.
• Normalize efficiency struggles early—framing improvement as developmental increases engagement and reduces stigma.
• Stronger resident efficiency supports both patient care and department flow—this is an educational priority, not just an operational one.
programs must prepare residents not only to deliver high-quality care, but to do so efficiently.
Programs like this one reflect a broader shift in medical education toward competency-based, practicefocused learning. By explicitly addressing efficiency, residency programs can better equip trainees for the realities of modern emergency medicine.
Conclusion
A structured performance-learning program offers a practical approach to improving resident efficiency through coaching, observation, and feedback. By treating efficiency as a teachable skill, training programs can support both resident development and patient care
ABOUT THE AUTHORS




Dr. Abezis is a second-year emergency medicine resident at Temple University Hospital in Philadelphia.
Dr. VandenBerg is an associate professor of clinical emergency medicine at Temple University Hospital.
Dr. Sprunt is an assistant professor of clinical emergency medicine at Temple University Hospital.
Dr. Satz is an associate professor of clinical emergency medicine at Temple University Hospital.
continued on Page 51
Dr. Schreyer is an associate professor of emergency medicine and director of the emergency medicine administrative fellowship at Temple University Hospital.
EDUCATION & TRAINING
Building a Social Emergency Medicine Curriculum: An Anti-Racist Approach to Residency Training
By Fahad Ali, MD; Ambuj Suri, MD; Denise Marte, MD; Gianna Petrone, DO; and Almaz Dessie, MD
At a Glance
• Why this matters now: Emergency medicine training often lacks structured approaches to teaching about structural drivers of health and care for marginalized populations
• What you’ll learn: A practical, replicable curriculum model using small-group learning, livedexperience voices, and integrated training strategies
• Who this is for: Educators and program leaders seeking to strengthen health equity in residency training and clinical practice
One of the greatest privileges of practicing emergency medicine (EM) is that the “door is always open.” However, this also means we provide care to a disproportionate number of patients whose lives are shaped by significant structural drivers of health. Historically, there has been limited formal education in EM on caring for marginalized groups. When such education is offered, trainees from underrepresented backgrounds may report unwelcoming learning environments Physicians from minoritized racial and ethnic backgrounds frequently describe feelings of isolation or being
overlooked, and cultural mismatch between learner and institutions has been shown to affect learning and retention.
At Brown Emergency Medicine, we recognized these gaps within our own department and developed a novel Social EM curriculum for our residency program. This approach has enabled us to foster a more inclusive, respectful, and engaging learning environment, particularly when addressing important but sensitive Social EM topics.
Our curriculum, Striving for Equity in Emergency Medicine (SEEM), is designed to help learners:
“One of the greatest privileges of practicing emergency medicine is that the ‘door is always open.’ However, this also means we provide care to a disproportionate number of patients whose lives are shaped by significant structural drivers of health.”
1. reflect on their identities as providers,
2. understand their role within the larger structures that drive inequity in the health care system, and 3. develop familiarity with the specific social needs and resources of the communities they serve.
Each session lasts 90 to 120 minutes and combines self-reflection with practical knowledge about available local resources. The curriculum addresses a broad range of topics that affect our patients, including homelessness, substance use, incarceration, immigration, and LGBTQ+ health.
What makes SEEM truly unique is its foundation in anti-racist pedagogy, intentionally designed to create an inclusive and supportive learning environment for all participants. Each session incorporates four core tenets that guide discussion and ensure a thoughtful, consistent approach to these important and often challenging topics.
Bring in Diverse Speakers
We intentionally prioritize the voices of individuals who are true experts on a topic through their lived experiences. For example, we have welcomed formerly incarcerated individuals, a refugee activist who founded a local resettlement organization, and a panel of patients experiencing homelessness to share their stories. While faculty with topic expertise may assist with a session, they rarely lead them, allowing the focus to remain on the voices of those most impacted.
The value of lived experience is profound and is consistently identified by residents as one of the most meaningful aspects of the curriculum. These sessions not only provide key teaching points and practicechanging insights but also cultivate empathy and a deeper understanding of the structural barriers patients face. Learners consistently leave with a renewed sense of connection to their community and a stronger commitment to delivering equitable, compassionate care.
Incorporate Small-Group Activities
This is one of our non-negotiables. Traditional classroom settings can be especially challenging for
marginalized learners, who may feel excluded or unsafe and, as a result, less likely to participate. To address this, our curriculum applies principles of anti-racist pedagogy by intentionally minimizing lecture time and prioritizing self-reflection and small-group discussion.
This format fosters inclusion, encourages participation, and values each person’s contributions regardless of expertise. We believe this approach not only supports marginalized learners but also enriches the learning experience for all participants.
“What makes truly unique intentionally supportive
makes
continued from Page 53
We structure sessions so that learners break into pairs or small groups of two to four participants, creating a more comfortable environment for engagement without putting individuals on the spot. This format has been especially well received by our residents. For example, during a session on human trafficking, learners first receive a brief overview of risk factors and warning signs, then divide into small groups to work through case scenarios. This approach allows them to immediately apply their knowledge in a collaborative and practical way while still having space to ask questions.
Involve Learners in Development
Anti-racist pedagogy builds on the principle of the flipped classroom, emphasizing that learners are more engaged when their perspectives and ideas are actively incorporated into the discussion. Our residency program is fortunate to have a chief resident of health equity serve on the SEEM curriculum committee, providing feedback and representing the resident perspective.
Additionally, we invite residents with expertise or dedicated interest to collaborate on sessions. For example, two residents with disabilities helped curate a deeply meaningful program on caring for patients with disabilities.
We collect feedback from learners at the conclusion of each session
Striving
for
Equity in Emergency Medicine
unique is its foundation in anti-racist pedagogy, intentionally designed to create an inclusive and supportive learning environment for all participants.”
Pulse Points
Key clinical and practice takeaways:
• Build intentionally: A structured Social Emergency Medicine curriculum can be integrated into existing residency programs using adaptable, scalable components
• Prioritize lived experience: Bringing in community voices adds depth, credibility, and impact that traditional faculty-led sessions often cannot replicate
• Rethink teaching formats: Small-group, discussion-based learning fosters engagement, especially for complex or sensitive topics
• Embed, don’t isolate: Health equity principles are most effective when integrated across simulation, conferences, and clinical teaching—not confined to a single curriculum
• Measure and evolve: Continuous learner feedback and iteration are essential to keeping content relevant and meaningful
through comprehensive, anonymous surveys, as well as through an annual program review. This iterative process allows the curriculum to evolve in response to learner needs.
Build Your Curriculum to Be Everywhere
Finally, we strive to integrate elements of this curriculum beyond dedicated Social EM didactic sessions. Rather than isolating these concepts, we have worked to build a culture that incorporates principles of health equity throughout all aspects of resident education, recognizing their relevance across the full scope of emergency care.
Examples include simulation sessions focused on caring for patients with limited English proficiency, a health equity-focused journal club, and structuring Morbidity and Mortality conferences to highlight how bias may have influenced care
ABOUT THE AUTHORS





Dr. Ali is an assistant professor at Brown Emergency Medicine.
Dr. Suri is a health equity chief resident at Brown Emergency Medicine. Dr. Marte is an assistant professor at Brown Emergency Medicine.
Dr. Petrone is an assistant professor at Brown Emergency Medicine. Dr. Dessie is an associate professor at Brown Emergency Medicine.
continued on Page 51
EDUCATION & TRAINING

Harmonizing the Chaos: How a Student Symphony Prevented a Procedural Failure
By David Benaron, MD, and Jose Luis Martinez
At a Glance
• Why this matters now: Procedural success in emergency medicine depends as much on team coordination and communication as on technical skill—especially in high-acuity, unpredictable scenarios.
• What you’ll learn: How to leverage team strengths, manage cognitive load, and use nonpharmacologic strategies to maintain safety during complex procedures.
• Who this is for: Emergency educators and clinicians navigating real-time teaching and leadership at the bedside.
In the simulation lab, teaching central venous catheter (CVC) insertion is a controlled exercise in anatomy and dexterity. In the emergency department (ED), however, the procedure is rarely the only moving part. The true challenge of academic emergency medicine requires more than technical instruction. It demands leadership, clinical decision-making, and realtime crisis resource management.
To teach through complexity is to model adaptive leadership. As Hunziker et al. emphasize in their research on resuscitation, the quality of teamwork and leadership often dictates clinical
outcomes as much as technical skill. A recent shift involving a patient in diabetic ketoacidosis (DKA) and three medical students offered a compelling example of how leadership—grounded in interdisciplinary collaboration—can transform a potential near-miss into a sophisticated lesson in safety and wellness.
The Case: Precision vs. Pandemonium
The patient presented with classic DKA: tachypneic, dehydrated, and profoundly acidotic. While initially calm, the metabolic derangement soon manifested as fluctuating encephalopathy. A central line was

“This case serves as a reminder that the most important instrument in the resuscitation symphony is not the ultrasound or the central line kit—it is the ability to communicate, collaborate, and teach within the dynamic, demanding environment that defines emergency medicine.”
necessary for reliable access and aggressive resuscitation.
The bedside team was an eclectic mix of future specialists: an EMbound student on their fourth CVC, an orthopedics-bound student, and a psychiatry-bound student. As the EM student began the ultrasound-guided approach, the patient’s confusion escalated. He reached for the sterile drape, his movements becoming jerky, unpredictable, and chaotic.
At that moment, the procedure was no longer just about line placement. It became a test of team coordination and situational awareness.
Leveraging the Team
In a high-acuity environment, maintaining team wellness means preventing the “panic spiral” that
occurs when a situation feels out of control. By recognizing the unique career interests of the students present, tasks were delegated to align with their natural strengths—creating a human safety net that preserved both the sterile field and the team’s collective calm.
The psychiatry-bound student became the patient’s cognitive anchor, employing active listening and maintaining a consistently calm, soothing voice. According to the American Association for Emergency Psychiatry Project BETA workgroup, these verbal techniques are essential in managing the agitated patient without escalating the crisis. By narrating the sensations the patient was experiencing—such as the cold prep or the pressure of the ultrasound
probe—the student reduced the startle response that often leads to sudden, dangerous movement.
Simultaneously, the orthopedicsbound student recognized that a sudden lurch could result in an arterial stick, a needlestick injury, or disruption of the sterile field. He applied a gentle but firm grip, providing steady proprioceptive feedback to the patient’s shoulders and arms.
Amid this support, the EM-bound student demonstrated the pinnacle of crisis listening. Under the attending’s continuous verbal guidance, the student maintained procedural focus and technical precision despite the noise and movement in the room.

“Teaching
through complexity is to model adaptive leadership.”
EDUCATION & TRAINING
continued from Page 57
Each role complemented the others. The sterile field was preserved, patient safety improved, and the procedure continued without interruption.
Teaching Through Complexity: Cognitive Load Management
The attending’s primary tool in this scenario is cognitive load management. In the chaos of the ED, the attending must shield the learner from environmental noise, patient agitation, and situational pressure. This allows the learner to focus on the intrinsic demands of the procedure itself.
By narrating the procedure aloud, the attending does more than teach anatomy—they set the emotional tone for the room. This “talk-through” method ensures the proceduralist does not have to guess what the attending is thinking, reducing sympathetic activation and preserving fine motor control.
This modeling of calm, adaptive leadership is a core component of fostering both competence and
Pulse Points
Key clinical and practice takeaways:
wellness in the ED.
The Sedation Dilemma in DKA
A common reflex when a patient becomes agitated during a procedure is to reach for a sedative. In the context of DKA, however, this is a highrisk decision that requires nuanced clinical judgment.
As Nyce et al. note in relation to airway management, patients in DKA rely on a compensatory respiratory alkalosis to offset metabolic acidosis. Medications such as opioids or benzodiazepines can suppress respiratory drive, reduce ventilation, and worsen acidemia. In severe cases, this can lead to rapid clinical deterioration.
If verbal de-escalation and physical positioning fail, ketamine may be considered as an adjunct for procedural dissociation. Ketamine is often preferred in this setting because it typically preserves airway reflexes and ventilatory drive. As highlighted by Green et al., its unique profile allows for analgesia and cooperation with significantly less risk of respiratory depression.
In this case, however, student-led de-escalation eliminated the need for
• Technical skill alone is not enough—team coordination and communication often determine procedural success in high-acuity settings.
• Assign roles based on individual strengths to create a real-time safety net that stabilizes both the patient and the team.
• Use cognitive load management: narrate, guide, and filter distractions so learners can focus on the critical task.
• De-escalation is a clinical skill—clear communication and physical positioning can prevent the need for sedation.
• In complex cases like diabetic ketoacidosis, reaching for sedation first may be riskier than slowing down and leading the room.
pharmacologic intervention entirely— demonstrating that communication is often the most effective sedative.
A Broader Lesson
Practicing medicine in the ED is the ultimate team sport. By empowering students to step into roles aligned with their strengths and developing skill sets, high-risk moments can be transformed into meaningful teaching opportunities.
The procedure succeeded not through technical execution alone, but through coordinated teamwork. Communication reduced agitation. Physical stabilization preserved the sterile field. Structured guidance maintained procedural focus. Each contribution was essential.
The focus shifts from completing a procedure to reinforcing patientcentered care, adaptive leadership, and shared responsibility.
This case serves as a reminder that the most important instrument in the resuscitation symphony is not the ultrasound or the central line kit—it is the ability to communicate, collaborate, and teach within the dynamic, demanding environment that defines emergency medicine.
ABOUT THE AUTHORS


Dr. Benaron is an assistant professor and vice chair of the department of emergency medicine at the University of Nevada, Reno School of Medicine.
the University of Nevada, Reno School of Medicine
into emergency medicine at Texas Tech University Health Sciences Center El Paso.
Jose Luis Martinez is a fourth-year medical student at
who matched
EDUCATION & TRAINING

Improving Emergency Department Triage Through a Case-Based Workshop Model
By Vanya Zvonar, MD; Patrena Campbell; Jordan Ferreira, MD; Ann Palladino, MD; Vaishnavi Warrier, MD; and Allison Lockwood, MD
At a Glance
• Why this matters now: High nursing turnover and increasing emergency department volume have made consistent, accurate triage more critical—and more challenging—than ever.
• What you’ll learn: How a casebased, interdisciplinary workshop improves triage decision-making, communication, and early recognition of high-risk patients.
• Who this is for: Emergency department leaders, educators, and clinicians seeking practical, scalable approaches to strengthen triage and patient flow.
Background
The Elmhurst Hospital Nursing Triage Workshop is an interdisciplinary curriculum serving 12 to 20 nurses per session on a bimonthly basis. It was developed in response to the COVID-19 pandemic, which hit Elmhurst Hospital in Queens, New York, with devastating force and led to significant nursing turnover.
As a result, many talented but less experienced nurses were tasked with making rapid triage decisions in a high-volume, highpressure environment with limited information. Small differences in how acuity is interpreted can
significantly affect patient flow and the early recognition of critical illness.
Strengthening triage education supports a more consistent and efficient process while preserving the clinical judgment that experienced emergency nurses rely on each shift. This workshop was designed to address the evolving staffing environment and challenges in triage decision-making.
Using de-identified cases of both mistriage and successful triage, the workshop applies a structured approach with facilitated discussion. It standardizes acuity assessment, enhances communication, and

“Strengthening triage education supports a more consistent and efficient process while preserving the clinical judgment that experienced emergency nurses rely on each shift.”
improves team-based decisionmaking in an overcrowded emergency department. By bridging nursing and physician workflows, the initiative strengthens shared accountability for safe, efficient care in a safety-net emergency department with more than 130,000 annual visits.
Design
The workshop consists of interactive, case-based sessions focused on highrisk clinical presentations. Topics are selected in collaboration with nursing leadership to ensure relevance to clinical practice and alignment with departmental protocols and national guidelines.
Each session includes three to four cases of escalating acuity based on real patient encounters. For example, a hyperkalemia session progresses from a normal electrocardiogram (ECG) to peaked T waves and then to
QRS widening, illustrating increasing clinical severity.
Before each session, cases are distributed electronically to attending physicians and senior residents via an online survey. Participants select a triage disposition for each scenario, such as assignment to a mid-acuity area, initiation of a “resus consult,” or direct transfer to the resuscitation bay. A “resus consult” is defined as a brief bedside evaluation in triage by a resuscitation resident or attending physician.
The same survey is later administered to nurses participating in the workshop. Responses are compared across groups to reinforce key principles, including appropriate Emergency Severity Index (ESI) level assignment, early recognition of highrisk features, and effective allocation of critical care resources.
Implementation
Each one-hour session is facilitated by two residents with oversight from an attending physician and follows a roundtable format. Cases are presented as short clinical scenarios with three triage destination options.
Participants first select their responses before physician survey results are revealed. Facilitators then review the rationale behind each option, highlighting red flags and reassuring findings in the triage assessment.
After discussion, pooled responses from physicians are displayed. While consensus is often reached, variability in decision-making is common. For example, in a case of suspected pulmonary embolism in a patient with
“Small differences affect patient flow

continued from Page 61
known deep vein thrombosis and stable but abnormal vital signs, about 75% of respondents selected a “resus consult.”
These discussions create a collaborative learning environment that encourages peer teaching and open dialogue. At the conclusion of each case set, residents lead a brief interactive lecture on the relevant clinical topic. Feedback is collected in real time and used to refine future sessions.
From a nursing perspective, the program has reinforced the goal of making triage more efficient and consistent in a busy emergency department. Reviewing real cases and discussing variability in decisionmaking has improved confidence in identifying high-risk patients and escalating concerns early.
Overall, the workshop fosters a supportive environment where both new and experienced nurses can refine triage decision-making. Similar programs may benefit other emergency departments, particularly high-volume settings where triage decisions are critical to patient safety. Key implementation strategies include offering sessions at varied times, using locally relevant cases, and focusing on clinical “gray areas” to encourage discussion. EDUCATION &
Outcomes
The workshop has increased nurses’ awareness of clinical “red flags” and improved communication between triage nurses and physicians. Comparative case questions have been especially effective in highlighting subtle differences that influence triage decisions but may not be obvious to less experienced staff.
This shared understanding supports smoother patient flow and helps ensure that critically ill patients are recognized promptly, even during periods of high volume and time pressure.
Future sessions will expand beyond level-of-care decisions to include patient placement within care areas. For example, while both a stable patient with gastroenteritis and one with a chronic obstructive pulmonary disease exacerbation may be assigned to a mid-acuity area, the latter may require closer monitoring and placement within direct line of sight of clinical staff.
differences in how acuity is interpreted can significantly flow and the early recognition of critical illness.”
Pulse Points
Key clinical and practice takeaways:
• Standardize triage through case-based learning: Use real, de-identified cases with escalating acuity to sharpen clinical judgment and reduce variability.
• Align nurses and physicians early: Structured comparison of triage decisions builds shared mental models and improves communication at the front door.
• Focus on “gray areas”: Teaching subtle distinctions—not just obvious emergencies—drives better patient placement and earlier escalation.
• Make it operationally relevant: Tie education directly to patient flow, throughput, and safety in high-volume settings.
• Scalable and adaptable: Short, repeatable sessions with local cases can strengthen triage performance in any emergency department.
ABOUT THE AUTHORS





Dr. Zvonar is a third-year emergency medicine resident at Mount Sinai Hospital/Elmhurst Hospital. Patrena Campbell is an emergency department nurse.
Dr. Ferreira is a third-year emergency medicine resident at Mount Sinai Hospital/Elmhurst Hospital.
Dr. Palladino is a third-year emergency medicine resident at Mount Sinai Hospital/Elmhurst Hospital.
continued on Page 51
Dr. Warrier is an emergency medicine physician and chief resident at Mount Sinai Hospital/ Elmhurst Hospital.

Dr. Lockwood is an assistant professor of emergency medicine at the Icahn School of Medicine at Mount Sinai and faculty at Elmhurst Hospital.
EDUCATION & TRAINING
Mastering the Embedded Participant Role in Medical Simulation
By Kavita Joshi, MD; Colin Jewell, MD; Deepa Patel, MD; Christine Ju, MD; and Tim Friedmann, MD, on behalf of the SAEM Education Committee
At a Glance
• Why this matters now: Simulationbased education is central to training, and embedded participants play a critical role in shaping realism, learner engagement, and outcomes.
• What you’ll learn: Practical strategies to prepare, participate effectively without over-directing, and contribute meaningfully to debriefing.
• Who this is for: Medical students, residents, faculty, and educators involved in simulation-based learning.
Simulation-based learning is an invaluable tool in medical education, allowing health care professionals to hone skills in a controlled environment. Whether you are a seasoned faculty member or a medical student, you may be asked
to help facilitate a simulation. This often means being in the room with learners, playing a role such as a parent or nurse, while the primary facilitator operates the mannequin from a control room. This role is known as an “embedded participant.”
This guide outlines key steps for preparation, participation, and debriefing to ensure a productive experience for both learners and facilitators.
“Although you may know the intended direction of the case, avoid leading learners and allow them time and space to think through problems independently.”
Preparation
Several steps should be completed before the event. First, read the case thoroughly. If the full case is unavailable, review at least a summary. Understand the learning objectives, which may be explicitly stated or may require clarification from the case author. Review key teaching points and refresh any unfamiliar content areas.
Next, consider the learners’ level of training. Awareness of their experience helps tailor interactions
appropriately and compassionately. For example, when working with more advanced learners, you may need to require greater specificity (e.g., medication name and dosage), whereas less experienced learners may need more flexibility.
It is also important to understand your role, including its purpose and any required actions or dialogue. For example, you may play a nurse who is unable to obtain IV access, prompting learners to consider alternatives such as intraosseous or central access. Or
you may play a parent who provides history and helps facilitate the exam.
Memorizing lines is usually unnecessary; keeping a copy of the case nearby is often sufficient. In some scenarios, you may use an earpiece to receive prompts from the control room. If props or simulation equipment are required—such as simulated blood products—be sure you know where they are and how to use them effectively.
“Maintain a professional, the more authentic learners
continued from Page 65
Finally, anticipate how you will respond to different learner decisions. If the case does not outline expected pathways or common errors, consider how your role can help guide learners without directing them.
In the Room
During the simulation, your behavior can significantly enhance—or detract from—the learning experience. Avoid speaking directly to simulation staff unless instructed, as this can disrupt realism. Communication is often handled through nonverbal cues (e.g., thumbs up or down) in response to prompts via earpiece.
Maintain a professional, bedsideappropriate demeanor. Avoid drawing attention to realism gaps or using humor that undermines the scenario. The more authentic the experience feels, the more effectively learners will retain it as a clinical reference.
Although you may know the intended direction of the case, avoid leading learners. Allow them time and space to think through problems independently. If they are struggling, you may be prompted by the control room to offer a subtle cue. In the absence of such guidance, consider pausing briefly before offering limited direction.
As the scenario unfolds, take note— mentally or in writing—of learner performance, including both strengths and opportunities for improvement. These observations will be valuable during the debrief and for refining future simulations.
The Debrief
The debrief is often where the most meaningful learning occurs. As an embedded participant, you provide a unique in-room perspective. Sharing your observations can support discussion of teamwork, communication, and clinical decisionmaking.
professional, bedside-appropriate
authentic the
experience feels,
the
demeanor, as
more effectively learners will retain it as a clinical reference.”
Pulse Points
Key clinical and practice takeaways:
• Preparation drives realism—know the case, learner level, and your role to support the scenario without disrupting flow.
• Don’t lead the learners—strategic silence and restraint are essential to preserve critical thinking and decision-making.
• Stay in character—maintaining realism directly impacts how well learners translate simulation to clinical practice.
• Your observations matter—embedded participants offer unique insights that strengthen debriefing and future case design.
• The debrief is where learning sticks—balanced feedback and real-world connections turn simulation into lasting clinical growth.
When appropriate, relate the simulation to real clinical experiences to reinforce learning objectives. Keep comments focused and aligned with the facilitator-led discussion. Be sure to highlight successes as well as areas for improvement. This balanced approach fosters psychological safety and encourages learners to reflect openly on their performance.
Participating in a simulation is a rewarding experience that requires minimal preparation. With a few best practices, you can help ensure the scenario is realistic, engaging, and educational for all involved.
ABOUT THE AUTHORS





Dr. Joshi is an assistant professor of emergency medicine at UT Southwestern Medical Center and the assistant fellowship director of the UT Southwestern medical simulation fellowship.
Dr. Friedmann is an assistant professor in the department of emergency medicine at the Icahn School of Medicine at Mount Sinai. He is an assistant program director for the residency program.
Dr. Ju is an assistant professor and director of undergraduate medical education in the department of emergency medicine at UTHealth Houston McGovern Medical School.
Dr. Jewell is an assistant professor of emergency medicine at the University of Wisconsin School of Medicine and Public Health. He is the director of medical student education in the BerbeeWalsh Department of Emergency Medicine and serves as a longitudinal teaching coach.
Dr. Patel is an assistant professor of emergency medicine and anesthesiology (critical care) at Emory University. She serves as director of the emergency medicine critical care section, associate program director for the anesthesiology critical care medicine fellowship, and co-director of multiprofessional education for the Emory Critical Care Center.

When No One Speaks: DecisionMaking for Unrepresented Patients
By Megan Polniak
At a Glance
• Why this matters now: Unrepresented patients—those without decision-making capacity or identifiable surrogates—present urgent ethical challenges that emergency clinicians must navigate in real time.
• What you’ll learn: A case-based exploration of how clinical teams apply ethical principles and shared decision-making when patient preferences are unknown.
• Who this is for: Emergency physicians, residents, and trainees involved in high-stakes care decisions and ethics-informed clinical practice.
A common presentation in the emergency department is the patient with altered mental status. Many arrive from long-term care facilities for evaluation of infection or injury. Others present with substance toxicity, metabolic derangements, or psychiatric crises—conditions that are often reversible with appropriate treatment.
Far less common, but far more complex, is the unrepresented patient: an individual who lacks decision-making capacity and has no identifiable surrogate to guide goals of care.
A Case Without a Voice
Consider the following case, referred to the hospital ethics committee, of which I am a member as a medical student.
The patient was an 80-year-old man visiting from out of state to see family, though he could not provide names or contact information. He had previously received care at a VA hospital in his home state, but no recent documentation of goals of care or code status was available. His medical history included colon cancer, status post colectomy and ileostomy.
On presentation, his exam raised concern for bowel obstruction, later confirmed on imaging to be caused by a malignant mass.
During his hospitalization, clinicians became concerned about an underlying psychiatric condition, such as schizophrenia or a delusional disorder. He appeared to
deny his cancer diagnosis and refused multiple recommended interventions, including antibiotics, nasogastric decompression, and surgical management. A formal evaluation determined that he lacked decisionmaking capacity.
Despite extensive efforts, no surrogate decision-maker could be identified. Meanwhile, his condition deteriorated. Laboratory values worsened, the bowel obstruction persisted with concern for ischemia, and imaging revealed diffuse metastases to the lungs and liver. He became increasingly somnolent. When asked whether he wanted to be made comfortable, he nodded.
The Decision Without Certainty
The central question became how to proceed: pursue surgery or transition to comfort-focused care.
Surgical intervention offered limited benefit given his advanced disease and carried significant risks, including the likelihood of requiring chemical and physical restraints postoperatively. Although hospice care aligned more closely with his apparent wishes, he did not meet criteria for inpatient hospice. Transfer to a skilled nursing facility with palliative services was considered but complicated by his rapid decline, and transfer to his home-state VA hospital was deemed unsafe.
Pulse Points
Key clinical and practice takeaways:
“In the absence of decisionmaking capacity and surrogate input, responsibility shifts to the clinical team.”
After deliberation, the committee recommended transitioning the patient to do-not-resuscitate comfort care status. The decision reflected his poor prognosis, the limited benefit of surgery, and his expressed preference for comfort.
The Weight of Responsibility
This case illustrates the ethical and practical challenges of caring for unrepresented patients. In the absence of decision-making capacity and surrogate input, responsibility shifts to the clinical team. That
• When a patient lacks decision-making capacity and no surrogate is available, responsibility for major decisions shifts to the clinical team—this is common enough to require deliberate preparation, not improvisation.
• Ethical frameworks guide but do not resolve uncertainty; applying substituted judgment and best interest standards still requires clinical judgment and team consensus.
• Early engagement of ethics resources can structure decision-making, reduce conflict, and support shared responsibility across the care team.
• Absence of patient preferences increases the risk of unintentional paternalism—clinicians must actively reflect on whether decisions align with the patient’s likely values or their own.
• The emotional residue of these cases is real; acknowledging uncertainty and sharing responsibility are essential to sustaining clinician well-being and ethical practice.
shift is inherently uncomfortable— it challenges patient autonomy, introduces elements of medical paternalism, and alters the physician–patient relationship.
Even when guided by frameworks such as substituted judgment and best interest standards, uncertainty remains. Without knowledge of a patient’s values, clinicians must approximate what the patient might have wanted.
That uncertainty is not abstract. It raises difficult questions:
• Are we honoring this patient’s dignity, or imposing our own values?
• Are we alleviating suffering, or prematurely limiting care?
Reasonable clinicians may disagree, and no option feels entirely right.
Acting Without Answers
Even after consensus is reached, the moral weight of these decisions lingers. The “what-ifs” do not fully resolve. Over time, clinicians may learn to compartmentalize this uncertainty, but it remains an enduring part of caring for vulnerable patients without voices.
Cases such as this call for shared moral responsibility—what might be understood as the collective care of the unrepresented patient.
When certainty is impossible, the obligation is to act with integrity, guided by beneficence, nonmaleficence, respect for autonomy, and justice, grounded in empathy.
In doing so, clinicians honor not only the patient before them, but also the broader commitment of medicine to care for those who cannot advocate for themselves.
ABOUT THE AUTHOR

Megan Polniak is a fourth-year medical student at Saint Louis University School of Medicine. She worked as an emergency medical technician and patient care technician in an emergency department during the COVID-19 pandemic before medical school. She has a scholarly interest in medical ethics and philosophy.

From Evidence to Action: Applying Implementation Science in Emergency Medicine
By Rohit Mukherjee, MD; Bryan Kane, MD; Dan Mayer, MD; and Sangil Lee, MD
At a Glance
• Why this matters: Evidence-based interventions often fail in the ED without attention to workflow, context, and system constraints.
• What you’ll learn: How implementation science frameworks (CFIR, RE-AIM) help translate evidence into real-world practice.
• Who this is for: Emergency physicians, trainees, and leaders involved in quality improvement and systems-based care.
Implementation science (IS) is the systematic study of methods that promote the integration of evidencebased interventions into routine clinical practice. Unlike traditional clinical research, which evaluates the efficacy or effectiveness of interventions under controlled conditions, IS examines how and under what conditions evidencebased practices are successfully adopted in real-world health care settings.
The context of an intervention— including who delivers it, how it is
executed, how it fits into routine workflow, and the environment in which it is implemented—introduces significant complexity.
Emergency departments (EDs) operate in high-acuity, resourceconstrained, and highly variable environments where even wellvalidated interventions fail without thoughtful integration into existing systems. IS provides a structured framework to understand how factors such as workflow design, staffing models, leadership engagement, and
“Even well-validated interventions fail without thoughtful integration into existing systems.”
resource availability influence the fidelity, adoption, sustainability, and equity of innovations in acute care delivery. By systematically studying these contextual factors, IS enables emergency physicians to translate evidence into practice more effectively.
Core Implementation Science Frameworks in Emergency Medicine
The ED is uniquely suited for IS as a critical interface between community health systems and the hospital. Emergency physicians routinely work in high–decision-density environments, creating opportunities to implement strategies that reduce error and improve care delivery. IS frameworks help investigators evaluate how these systemic factors influence the success of clinical and operational interventions.
Two of the most widely used frameworks in implementation research are the Consolidated Framework for Implementation Research (CFIR) and RE-AIM framework (Reach, Effectiveness, Adoption, Implementation, and Maintenance). CFIR provides a comprehensive structure for assessing implementation across five domains: intervention characteristics, inner setting, outer setting, individual characteristics, and implementation processes. RE-AIM evaluates population-level impact and sustainability by examining reach, effectiveness, adoption, implementation fidelity, and long-term maintenance.
Aligning IS With ACGME Competencies
Implementation
Science in Practice
• Define the problem
• Assess context (workflow, staffing, environment)
• Select framework (CFIR or RE-AIM)
• Map barriers and facilitators
• Test and measure
• Iterate and adapt
Together, these frameworks enable investigators to assess how interventions perform across diverse ED settings and improve external validity when scaling innovations across health systems.
As Accreditation Council for Graduate Medical Education (ACGME) program requirements evolve, IS aligns closely with several core competencies. IS equips trainees with tools to analyze errors in emergency care, identify quality gaps through applied data analysis, and implement structured strategies to improve care delivery.
Emergency medicine residency programs increasingly emphasize quality improvement over traditional
on Page
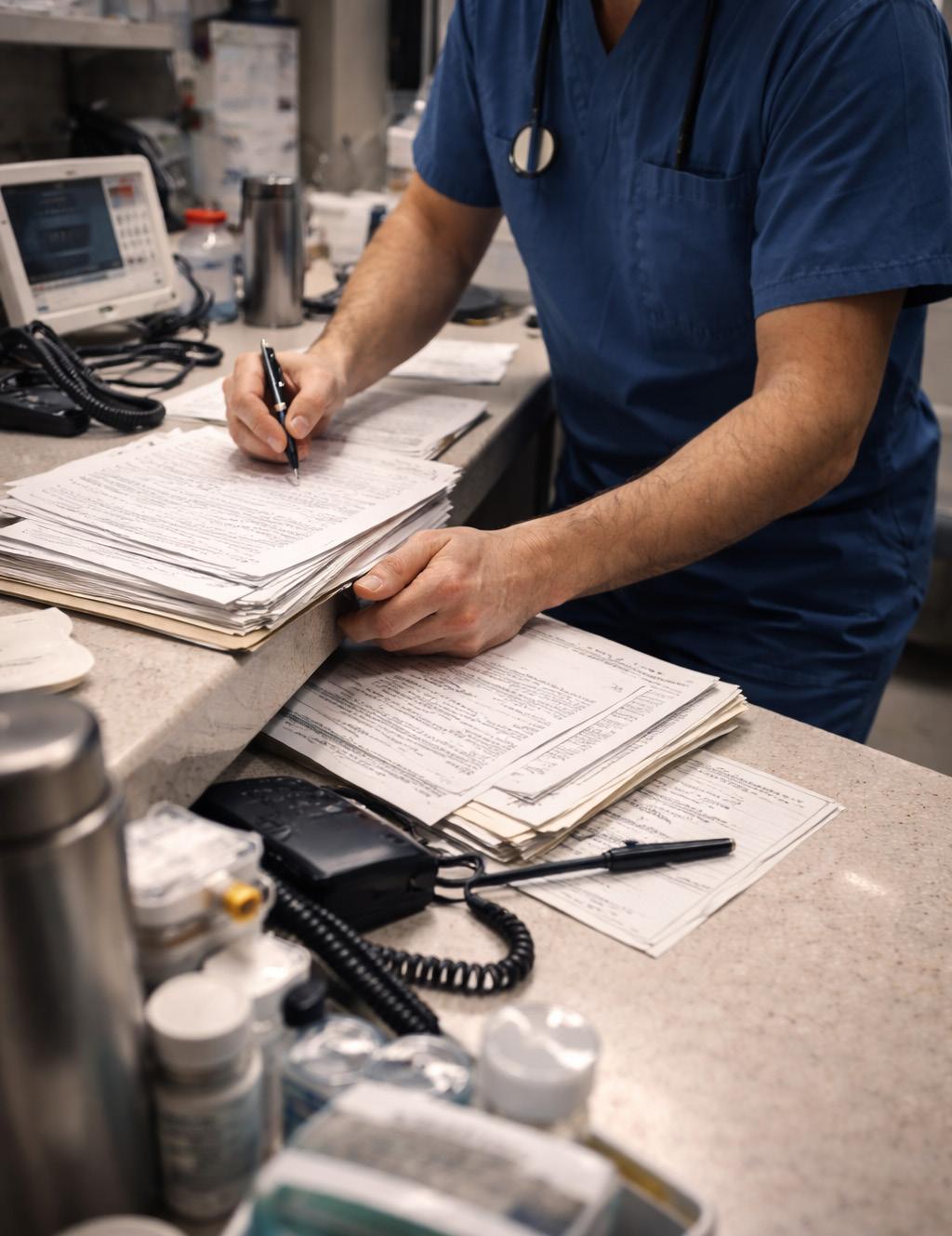
continued from Page 71
research, creating opportunities for system-level approaches that incorporate implementation methodologies. Through exposure to IS frameworks, trainees learn to engage stakeholders, evaluate health care processes, interpret operational data, and lead interdisciplinary improvement initiatives—skills essential for physicians working in complex systems.
Applying IS to ED Quality Improvement
For clinicians new to IS, existing quality improvement (QI) initiatives provide a natural entry point. IS frameworks integrate into ongoing QI efforts to map implementation strategies, identify barriers, and prospectively evaluate process outcomes.
Mixed-methods approaches— including qualitative interviews,
pragmatic outcome mapping, and cluster-randomized designs— strengthen local improvement initiatives and increase generalizability.
IS also emphasizes learning from both successes and failures. When interventions do not achieve expected outcomes, these frameworks help determine whether the issue lies in the intervention itself or in contextual barriers to implementation. This approach reduces stigma around reporting negative findings and supports more transparent dissemination of implementation experiences.
Dissemination and Impact in Emergency Medicine
Emergency physicians play a central role in advancing evidence-based care by disseminating implementation research through national meetings, peer-reviewed publications, and collaborative learning networks. The Society for Academic Emergency Medicine (SAEM) continues to
“Implementation science shifts the focus from whether something works to how it works in practice.”
Pulse Points
Key clinical and practice takeaways:
• Evidence doesn’t implement itself: Even strong interventions fail without alignment to workflow, staffing, and environment.
• Use a framework early: CFIR and RE-AIM help identify barriers and measure success before rollout—not after failure.
• Start where you are: Existing QI projects are a practical entry point for applying implementation science.
• Train for systems thinking: IS builds skills in stakeholder engagement, process evaluation, and leading change in complex environments.
• Failure is data: Negative results often reflect context—not concept—and should inform iteration, not abandonment.
recognize the importance of implementation-focused scholarship through dedicated abstract categories and awards, including the Engineer Award, which highlights innovative system redesign and implementation efforts.
Framing emergency medicine research using IS methodologies strengthens external validity, increases scholarly impact, and generates actionable insights that are more readily adopted. IS ensures that evidence does not remain confined to journals but translates into meaningful improvements in patient care where it matters most: the emergency department
ABOUT THE AUTHORS

Dr. Mukherjee is a recent match into the emergency medicine residency program at the University of Pennsylvania. He was a dean’s scholar at Rutgers Robert Wood Johnson Medical School and a United States Fulbright research fellow for the Columbia University sidHARTe – Strengthening Emergency Systems Program.


Dr. Lee is a clinician-scientist focused on emergency medicine research. His work includes delirium screening and intervention programs in the emergency department.
Dr. Mayer served as an attending physician at Albany Medical Center Hospital from 1987 until his retirement in 2014. He taught evidence-based medicine, medical decision-making, and emergency medicine to learners across training levels. He remains active in reviewing and publishing research, teaching evidence-based medicine, and serving as an associate editor for Western Journal of Emergency Medicine and JACEP Open.

Dr. Kane is a professor of medicine at the University of South Florida Morsani College of Medicine and an adjunct professor of emergency medicine at Sidney Kimmel Medical College at Thomas Jefferson University. He serves as associate program director for research for the emergency medicine residency at Jefferson Lehigh Valley and has held leadership roles within SAEM, CORD, and ACEP.

Preparing Emergency Medicine Workforce to Navigate Health Misinformation
By John Robert Bautista, PhD, MPH and Alexander Y. Sheng, MD, MHPE, on behalf of the Planning
Consensus Conference on Rebuilding Trust and Mitigating Unreliable Information
At a Glance
• Why this matters now: Health misinformation is increasingly shaping patient behavior, driving preventable illness, and placing additional strain on emergency care systems and clinicians.
• What you’ll learn: Practical, evidence-based communication strategies and training approaches to help emergency medicine providers identify and address misinformation in real time.
• Who this is for: Emergency medicine clinicians, educators and trainees seeking to strengthen patient communication and navigate misinformation in highstakes clinical settings.
Health Misinformation Is a Public Health Threat
Health misinformation—publicly available information related to health or health care that is misleading or inconsistent with the best available
Committee for the SAEM 2026
scientific evidence—has emerged as a significant public health threat. Whether spread deliberately (disinformation) or unintentionally (misinformation), it undermines trust, distorts decision-making, and complicates patient care.
The COVID-19 pandemic made these risks visible in real time. Emergency medicine (EM) providers on the frontlines faced not only a surge of critically ill patients, but also the consequences of widespread
“Health misinformation—publicly available information related to health or health care that is misleading or inconsistent with the best available scientific evidence—has emerged as a significant public health threat.”
misinformation influencing patient behavior.
National organizations, including the American Board of Emergency Medicine (ABEM), the American College of Emergency Physicians, and American Academy of Emergency Medicine, have warned that COVID-19 misinformation is both widespread and dangerous. Johns Hopkins Center for Health Security estimated that voluntary COVID-19 nonvaccination— driven in part by persistent exposure to misinformation—resulted in between $50 million and $300 million in harm each day since May 2021, including avoidable hospitalizations, deaths and long-term complications.
Less visible, but equally important, is the operational strain on the emergency care workforce. Misinformation contributed to operational strain through preventable patient surges and staffing disruptions, including recurrent infections among clinicians. It may also play a role in burnout and workforce attrition, though this impact remains underexamined.
The problem extends beyond the pandemic. A 2025 survey found that nine in 10 physicians believe health misinformation is more widespread than five years ago, and 57% report that it has negatively affected their ability to deliver quality care. At the same time, patients are increasingly exposed to sophisticated forms of misinformation, including AIgenerated deepfakes
Together, these trends underscore an urgent need for the EM workforce to take a more active role in

addressing health misinformation particularly as future public health crises are inevitable.
Closing the Training Gap in Emergency Medicine
Despite the growing scope of the problem, formal training remains limited. A 2021 study found that 18% of physicians reported receiving formal training on addressing health misinformation, while 39% reported
informal exposure. More recent data from 2025 suggest progress: approximately half of physicians report high confidence in identifying and correcting misinformation in clinical encounters.
However, important gaps remain. One in 10 physicians report lacking
continued on Page 77
Read More, Learn More
• The Role of Graduate Medical Education in the Fight Against Health Misinformation
• The Role of Emergency Physicians in the Fight Against Health Misinformation: Implications for Resident Training
• Equipping Health Professions Educators to Better Address Medical Misinformation
• Mitigating Misinformation Toolkit: A Medical Student Role-Play Curriculum on Communication Techniques to Facilitate Vaccine Misinformation Conversations

continued from Page 75
the tools or institutional support needed to effectively engage patients who present misinformation.
Addressing these gaps requires structured educational approaches grounded in evidence-based communication strategies. Prior work by Sheng and colleagues outlines practical frameworks for training EM learners, including motivational interviewing, conversational receptiveness, the “Three C” approach, and the elicit-share-elicit model. These approaches emphasize empathy, trust-building and patient-centered dialogue.
Additional guidance comes from broader interdisciplinary efforts. A 2023 report by Southwell and colleagues highlights effective interventions such as online motivational interviewing training, team-based communication strategies, collaborative learning environments and responsible social media engagement.
Toolkits and structured workshops are also emerging as valuable resources for health professionals and medical students. Programs such as the Duke Program on Medical Misinformation provide clinicians with practical training to respond to
Pulse Points
Key clinical and practice takeaways:
Get Involved!
On May 18 at SAEM26 in Atlanta, SAEM will host a consensus conference to rebuild trust and mitigate the impact of health misinformation on emergency care. Co-sponsored by ABEM, Consensus Conference I: Rebuilding Trust and Mitigating Unreliable Information will bring together a diverse group of stakeholders, including physicians, researchers, public health experts, and patient representatives, to develop a 10-year research agenda aimed at strengthening and supporting emergency care professionals in navigating an evolving information environment.
All participants are welcome, and the cost to attend the consensus conference is included in the registration fee for SAEM26.
misinformation while maintaining patient dignity and trust.
The Role of Emergency Medicine Organizations
Recognizing the long-term implications of health misinformation, EM organizations are increasingly investing in education and leadership on this issue.
• Health misinformation is now a routine part of emergency care—not an exception—and directly affects patient outcomes and clinician workload.
• Communication is a clinical skill: approaches such as motivational interviewing and the elicit-share-elicit method can improve trust and patient understanding in real time.
• Training remains inconsistent—formal education on addressing misinformation should be integrated across undergraduate, graduate and continuing medical education.
• Emergency medicine leaders have an opportunity to define this as a core competency, shaping both workforce resilience and patient care quality.
• The next public health crisis will include an information crisis— preparedness must include both clinical and communication readiness.
At the 2026 Council of Residency Directors in Emergency Medicine (CORD) Academic Assembly, Monica L. Wang, ScD, delivered a keynote address focused on responding to health misinformation in real time. Drawing on clinical scenarios and emerging evidence, the session emphasized communication strategies that integrate storytelling, scientific evidence and trust-building.
These efforts signal a broader shift within the specialty toward acknowledging misinformation as a core competency challenge, not simply a communication nuance.
Making Formal Education a Priority Health misinformation is unlikely to diminish in the near future. Preparing the EM workforce to address it effectively will require sustained, coordinated effort across the educational continuum.
Formal curricula at the undergraduate, graduate and continuing medical education levels are essential to equip clinicians with the skills needed to navigate misinformation in high-stakes clinical environments. Without this investment, the gap between patient information exposure and clinician preparedness will continue to widen.
Building a resilient emergency medicine workforce—capable of responding to both clinical and informational crises—must be a priority for the specialty
ABOUT THE AUTHORS

Dr. Bautista is an assistant professor at the Sinclair School of Nursing at the University of Missouri-Columbia. He has published several articles examining how and why health care professionals address inaccurate health information on social media. He is co-chair of SAEM Consensus Conference I: Rebuilding Trust and Mitigating Unreliable Information.
Dr. Sheng is an associate professor and residency program director for emergency medicine at the Warren Alpert Medical School of Brown University. He is co-chair of SAEM Consensus Conference I: Rebuilding Trust and Mitigating Unreliable Information.
FACULTY DEVELOPMENT
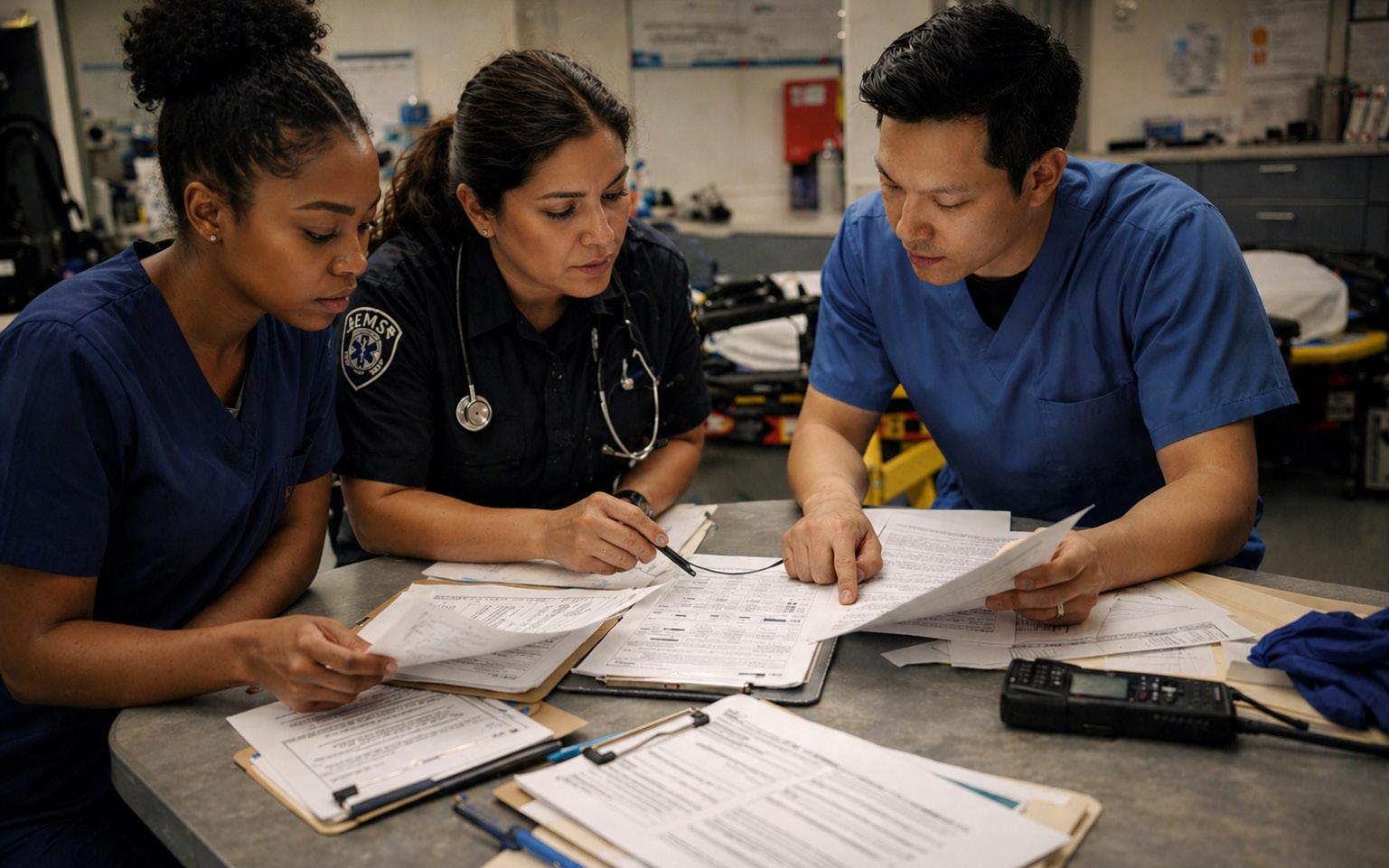
Building the Future of EMS Research: Mentorship, Collaboration, and Perseverance
By Salvador-Kelly, MD, and Nancy Kwon, MD, on behalf of the SAEM Faculty Development Committee and the SAEM Research Committee
At a Glance
• Why this matters now: EMS research is critical to improving early patient care, yet remains underdeveloped due to structural, funding, and operational barriers.
• What you’ll learn: Practical strategies for building a research career, including mentorship, collaboration, grant seeking, and navigating real-world challenges in EMS research.
• Who this is for: Emergency physicians and faculty interested in developing research skills, advancing academic careers, or expanding EMS-related scholarship.

In the demanding field of emergency medicine, prehospital emergency medical services (EMS) serve as a critical first link in the chain of patient care. At Northwell Health, a leading nonprofit integrated health system in the Northeast, two epidemiologists—Dr. Timmy Li and Dr. Molly McCann-Pineo—are shaping the future of EMS research through the development of a dedicated
Emergency Medicine Service Line research team.
Although Drs. Li and McCannPineo followed distinct paths, they share a commitment to EMS, research, and faculty development. Their work is grounded in a common goal: improving patient care while advancing clinician development. Drawing on their experiences, they offer practical guidance for building successful research careers in academic emergency medicine.
Navigating the Hurdles: Perseverance as a Guiding Principle
The path to impactful research is rarely straightforward. Drs. Li and
Dr. Timmy Li
Dr. Molly McCann-Pineo

McCann-Pineo describe persistent challenges in EMS research, including obtaining informed consent in chaotic prehospital environments, navigating political and administrative barriers, and addressing the lack of seamless data linkage between EMS and hospital electronic medical records.
Institutional hurdles—from data use agreements to IRB approvals—add further complexity. Funding instability is another constant. Dr. McCann-Pineo recalls the temporary loss of NIOSH funding, which disrupted multiple grant applications.
Yet these challenges have reinforced a central philosophy: perseverance.
“The P in PhD is for perseverance,” Dr. Li says.
Both emphasize the importance of learning from rejection, refining proposals based on feedback, and applying broadly. “There is a home for every paper,” Dr. McCann-Pineo says, reflecting on projects that ultimately succeeded after multiple submissions.
Words of Wisdom for Aspiring Researchers
For those pursuing academic
“They are in the homes, on the streets… shaping the trajectory of care.”
emergency medicine, Drs. Li and McCann-Pineo offer the following guidance:
• Formulate a clear research question. Begin with clinical observations and refine them into testable hypotheses with defined comparison groups and outcomes.
• Start small and build momentum. Quality improvement projects and descriptive studies can provide early publications and pilot data.
• Seek mentorship. Identify experienced, accessible mentors both within and outside emergency medicine.
• Embrace collaboration. Research is inherently team-based; interdisciplinary partnerships strengthen both design and impact.
• Persevere. Rejection is inevitable. Use feedback to improve and continue moving forward.
• Pursue funding strategically. Start with smaller foundation grants before advancing to larger federal opportunities.
• Foster inclusivity. Engage advanced practice providers, nurses, research staff, and EMS clinicians as active contributors.
Dr. Li: Building the Research Infrastructure
Dr. Li’s path into academic emergency medicine began nearly two decades ago as an emergency medical technician. During his undergraduate studies at the University of Rochester,
continued on Page
he discovered epidemiology as a way to combine clinical interests with scientific inquiry.
His early work focused on prehospital topics including spinal immobilization, trauma triage, and stroke care. After gaining experience in clinical trials at Mount Sinai, he returned to the University of Rochester to pursue a PhD in epidemiology, focusing on prehospital stroke care.
When he joined Northwell Health in 2017, research infrastructure within the Department of Emergency Medicine was limited. Under the mentorship of Dr. Lance Becker, Dr. Li began building that foundation— identifying interested clinicians, mentoring early-career investigators, and supporting publication and grant development.
A key initiative has been a cardiac arrest video review program, which led to a major publication in the Journal of the American Heart Association. This work contributed to an increase in survival to hospital discharge rates from 6.6% in 2017 to 16% in 2024.
Subsequent funding from the ZOLL Foundation allowed expansion into a multicenter data coordination effort, creating new opportunities for collaboration and faculty development across institutions.
Pulse Points
Key clinical and practice takeaways:
Dr. McCann-Pineo: Advancing EMS Clinician Wellness
Dr. McCann-Pineo’s career path began on a pre-med track before shifting to public health after discovering a passion for epidemiology. She earned her master’s degree from SUNY Albany and her PhD from the University of Rochester, where her research examined opioid overdose dynamics and prehospital care.
She credits Dr. Jeremy Cushman as a formative mentor, highlighting the importance of accessible, engaged guidance in shaping her career. Dr. Li similarly acknowledges Dr. Cushman’s influence.
After postdoctoral training at Northwell, Dr. McCann-Pineo joined the EMS research team in 2022. Her current work focuses on EMS clinician wellness, particularly among women.
Her “Female EMS Experience” study examines the challenges faced by women in EMS and highlights critical gaps in understanding workplace and health outcomes. She is now expanding this work to study pregnant and postpartum EMS clinicians.
To deepen her perspective, she obtained EMT certification in 2022— an experience that informs both her research and her mentorship of others entering the field.
A Synergistic Partnership
Together, Drs. Li and McCann-Pineo have built a collaborative research
• Start with what’s in front of you: Transform everyday clinical observations into research questions—small, practical inquiries are the foundation of larger programs.
• Build before you scale: Early wins (QI projects, descriptive studies) create the momentum and data needed for grants and broader collaboration.
• Mentorship is infrastructure: Strong, accessible mentors are as critical as funding—seek them out and invest in them.
• Rejection is part of the process: Treat every declined paper or grant as iteration, not failure—“there is a home for every paper.”
• EMS is a research frontier: Prehospital care offers unique, underutilized data that can directly shape patient outcomes and system performance.
environment that emphasizes inclusion, mentorship, and practical relevance.
They actively engage EMTs, paramedics, and EMS supervisors in research design, data collection, and interpretation. This approach not only strengthens study design but also fosters professional development across the workforce.
As Dr. McCann-Pineo notes, EMS clinicians are uniquely positioned to capture data that shapes patient outcomes: “They are in the homes, on the streets … able to collect information that directly impacts the trajectory of care.”
A Future Driven by Faculty Development
Their vision for the future centers on expanding clinician engagement in research through mentorship programs, skill-building initiatives, and cross-disciplinary collaboration. They aim to increase transparency and coordination across projects to reduce duplication and maximize impact. National collaborations, including multicenter registries, further extend opportunities for faculty and trainees.
Through this work, Drs. Li and McCann-Pineo are advancing both EMS research and the development of the next generation of emergency medicine investigators—ensuring that prehospital care continues to evolve through rigorous, inclusive scientific inquiry
ABOUT THE AUTHORS


Dr. Salvador-Kelly is deputy chief medical officer and senior vice president of medical affairs for Northwell Health, and an associate professor of emergency medicine at the Zucker School of Medicine at Hofstra/Northwell.
Dr. Kwon is vice president for the Central Market of Northwell Health, Central Market medical director for Advancing Health for All, and a professor of emergency medicine at the Zucker School of Medicine at Hofstra/Northwell.
FEDERAL FUNDING FOCUS

Bridging the Gap: Aligning Emergency Medicine Research With National Institute of Child Health and Human Development Funding
By Stephanie Carreiro, MD, PhD; Peter Chai, MD, MMS; and Edward R. Melnick, MD, MHS for the SAEM Federal Funding Committee
At a Glance
• Why this matters now: Significant federal funding exists for research on children and pregnant people, yet emergency medicine remains underrepresented despite strong alignment with national priorities.
• What you’ll learn: How the Eunice Kennedy Shriver National Institute of Child Health and Human Development prioritizes funding—and where emergency medicine research fits within those opportunities.
• Who this is for: Emergency medicine investigators, early-stage researchers, and faculty seeking to expand funding through better alignment with National Institutes of Health priorities.
More than one-third of emergency department (ED) visits involve children and pregnant people.
Data from the National Pediatric Readiness Project highlight significant variability in ED readiness to care for children, particularly in general EDs, where more than 80% of children receive emergency care. Variability in evidence-based practice further contributes to disparities in care.
Emergency medicine (EM) investigators play a critical role in generating evidence to close knowledge gaps and improve outcomes for millions of children and pregnant people who require emergency care each year. This article provides an overview of the mission and priorities of the
Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), with a focus on opportunities for EM researchers to align their work with NICHD funding priorities.
NICHD’s Mission and Priorities
Founded in 1962 with an initial focus on human development across the life span, NICHD’s mission is “to lead research and training to understand human development, improve reproductive health, enhance the lives of children and adolescents, and optimize abilities for all.” Its current portfolio includes $1.9 billion in funding supporting more than 3,600 projects.
The 2025 NICHD Strategic Plan outlines five broad goals:
“Emergency medicine investigators play a critical role in generating evidence to close knowledge gaps and improve outcomes for millions of children and pregnant people who require emergency care each year.”
• Understanding the molecular, cellular, and structural basis of development
• Advancing gynecologic, andrologic, and reproductive health
• Establishing the foundation for healthy pregnancies and lifelong wellness
• Improving child and adolescent health and the transition to adulthood
• Fostering safe and effective therapeutics and devices for pregnant people, lactating people, children, and people with disabilities
EM investigators whose research aligns with one or more of these
goals should contact NICHD program officials to assess alignment and explore funding opportunities across the National Institutes of Health.
Why EM Is Essential to NICHD’s Mission
Trauma is the leading cause of death in children, with firearm-related injuries and motor vehicle crashes representing the most common causes. Injured children often present to the ED immediately after injury, placing EM clinicians at the front line of care.
EM investigators bring essential clinical insight into the evaluation and management of acute injury and critical illness. This expertise aligns
closely with NICHD’s Pediatric Trauma and Critical Illness Branch (PTCIB), which supports research focused on preventing, treating, and reducing childhood traumatic injury and critical illness across the care continuum.
More broadly, EM clinicians routinely manage conditions that fall within NICHD’s funding priorities, including child abuse and intimate partner violence, pain management, respiratory failure, sepsis, and sexually transmitted infections. Additional relevant areas include diabetes, reproductive health, traumatic brain
continued on Page 85
continued from Page 83
injury, asthma, shock, cardiac arrest, seizures, and anaphylaxis.
NICHD also supports systems-level research affecting emergency care delivery, including emergency care planning, mobile health, pediatric readiness in EDs, teleconsultation for emergency medical services (EMS), and triage accuracy.
Despite this alignment, most NICHD funding currently supports investigators outside of EM and pediatric EM. This gap underscores the opportunity for EM investigators to pursue NICHD funding where strong alignment exists.
Key NICHD Programs Relevant to EM
The PTCIB supports research on the diagnosis, treatment safety, and effectiveness of care for critically ill and injured children. Key program areas include:
• Pediatric critical care medicine, including pathophysiology and management of critical illness
• Ethical, translational, and applied research in pediatric critical care
• Unintentional injury prevention and trauma care
Pulse Points
Key clinical and practice takeaways:
• Emergency medical services for children and disaster management
• Trauma, violence, and maltreatment
• Psychological trauma, resilience, and well-being (Program Official: Valerie Maholmes, PhD, CAS –maholmev@mail.nih.gov)
Investigators are encouraged to engage program officials early to assess alignment and refine research direction.
A Challenge Ahead
Recent changes in NIH funding policy, including the reduced emphasis on Notices of Special Interest (NOSI), have decreased transparency around priority alignment. This shift creates uncertainty for applicants seeking to understand how programmatic priorities influence funding decisions.
Even so, funding priorities remain accessible through NICHD programmatic guidance, website resources, and direct communication with program officials. These channels are critical for identifying alignment between proposed research aims and available funding mechanisms.
Strategies for EM to Expand Its NICHD Portfolio
• Engage program officials early across relevant NIH institutes to determine the best fit for proposed research
• Alignment matters: emergency medicine research already overlaps with Eunice Kennedy Shriver National Institute of Child Health and Human Development priorities—explicitly framing that fit strengthens funding potential.
• Don’t self-select out: most funding currently goes outside emergency medicine, signaling opportunity—not exclusion—for investigators who engage early.
• Program officers are critical: early, direct communication can clarify fit, redirect aims, and significantly improve funding success.
• Think beyond one institute: many emergency care topics span multiple National Institutes of Health institutes—dual alignment can expand funding pathways.
• Strategy is part of scholarship: articulating a long-term research vision and aligning with federal priorities can be as important as the science itself.
• Clearly articulate a long-term research vision, including how current aims contribute to sustained impact
• Align proposed research with federal priorities, including the Make America Healthy Again (MAHA) initiative, where appropriate
• Advocate for the importance of federal funding in advancing emergency care research
Conclusion
NICHD priorities intersect with many of the clinical conditions and systems challenges encountered in emergency care. EM investigators are uniquely positioned to address critical gaps affecting children and pregnant people across the emergency care continuum. Strengthening alignment between EM research and NICHD priorities offers a meaningful opportunity to expand funding and improve patient outcomes.
ABOUT THE AUTHORS

Dr. Shah is a pediatric emergency physician and director of academic affairs in the department of emergency medicine at Stanford University. He has National Institute of Neurological Disorders and Stroke funding focused on evaluating the safety and effectiveness of agebased midazolam dosing for paramedic-witnessed seizures in children.

Dr. Nishijima is an emergency physician and vice chair of research in the department of emergency medicine at University of California, Davis. He has National Center for Injury Prevention and Control funding focused on developing and validating a prediction tool for mental health sequelae in adolescents after mild traumatic brain injuries.

Dr. Samuels-Kalow is an emergency physician and vice chair for research in the department of emergency medicine at Mass General Brigham. She has National Institute of Dental and Craniofacial Research funding focused on reducing unmet oral health and social needs in the emergency department while collecting information to inform subsequent implementation strategies.
GERIATRIC EM

From Admission to Assessment: Transforming Care for Older Adults After Falls
By Alexander Quinones, MD; Michael Mitchell, MD; Elizabeth Goldberg, MD, ScM on behalf of the SAEM Academy of Geriatric Emergency Medicine
At a Glance
• Why this matters now: Falls are a leading cause of injury and admission in older adults, yet mobility assessment in the emergency department is often inconsistent or absent.
• What you’ll learn: A practical, emergency department–based pathway integrating physical and occupational therapy to improve disposition decisions and reduce return visits.
• Who this is for: Emergency physicians and clinical leaders interested in geriatric care, disposition strategy, and quality improvement in everyday practice.
Introduction
Falls account for approximately 65% of injuries in patients age 65 years and older presenting to the emergency department (ED). During 2025 at the UCHealth Highlands Ranch Hospital (HRH) ED, 17% of visits among patients age 65 years
and older were coded as fall-related, and nearly 39% of those patients were subsequently admitted to the hospital. Because the ED opened in 2019, this presented an opportunity to develop an ED-led system prioritizing the most appropriate disposition for older adults presenting after a fall.
Identifying the Problem
Physical therapy (PT) and occupational therapy (OT) evaluation can reduce ED recidivism and modify
1
Geriatric Fall Risk Assessment Tool (GEDFRAT)
1. Have you had 2 or more falls in the past year?
2. Is the patient confused or disoriented?
3. Is the patient intoxicated or sedated?
4. Do you feel unsteady when you are walking?
5. Have you been told you should use a cane, walker, or other assistive device to get around safely?
6. Do you take more than 6 medications?
7. Is the patient experiencing altered elimination?
8. Do you feel lightheaded or dizzy when walking?
Total Score: ______
Note. Each item is scored 1 (Yes) or 0 (No). A total score of 3 or greater indicates high fall risk.
fall risk in older adults presenting after a fall. HRH historically did not have a culture of utilizing rehabilitation services in the ED. The typical care process was to admit patients with mobility concerns following a fall for inpatient PT, OT, and case management evaluation. However, hospitalization in this population carries risks, including delirium, in-hospital falls, and functional decline. Additionally, many patients with substantial fall risk declined admission.
Staff anecdotally reported that a high proportion of patients returned to the ED with subsequent injuries after an initial fall. To evaluate this concern, a review of prioryear data was conducted. Patients who returned within nine days and required admission after a traumatic chief complaint (most commonly a fall) were tracked through the HRH Clinical Review Committee database. Although this dataset did not capture visits to non-UCHealth facilities, it represented the best available data on readmissions and suggested either missed injury or failure of outpatient disposition.
Among patients readmitted within nine days after a fall, 42% had no documented mobility status at the index ED visit. These patients were discharged in a wheelchair or transported home via ambulance stretcher without assessment of their ability to ambulate or other functional evaluation. Failure to assess mobility can result in missed injuries, such as occult pelvic or tibial plateau fractures, and represents a missed opportunity to identify functional impairment or balance issues that could prompt intervention.
This gap was identified as an opportunity to engage rehabilitation therapy services and nursing staff in a systematic approach to improve patient mobility and safety while minimizing unnecessary and potentially harmful hospital admissions.
Partnering with Rehabilitation Therapy Services
The HRH ED Geriatric Committee was formed shortly after the department achieved Geriatric Emergency Department Accreditation (GEDA) Bronze status. The committee
included representation from PT, OT, nursing, care management, and physician leadership. Its primary goal was to ensure the most appropriate disposition for older adults presenting after a fall, including discharge with outpatient support services, durable medical equipment, or facility placement.
One concern among stakeholders was that expanding therapy services into the ED would increase disposition times and contribute to department congestion. Available evidence did not support this concern. An evidence-based tiered approach was initially proposed, incorporating nursing assessment with the Activity Measure for Post-Acute Care (AMPAC), followed by the Timed Up and Go (TUG) test for patients with midrange scores, and PT evaluation when indicated
PT leadership at HRH determined that staffing capacity was sufficient to directly evaluate most fall patients in the ED. Nursing staff were already using a local screening instrument,
Figure 1: Geriatric ED Fall Risk Assessment Tool. Source: University of Colorado. Geriatric ED Fall Risk Assessment Tool. Accessed March 25, 2026. Internal institutional resource.
What is the patient's Geriatric ED Fall Risk Assessment Tool (GEDFRAT) score?
Score ≥ 3
Score 1-2
Evaluate, treat, dispo as indicated
Fall precautions per nursing PT/OT not necessary but can be ordered per physician discretion
Background
Key contributors and content approvals
Contact
References
Assess and treat accordingly
ED RN: Initiate Send ESC to EM Physician
Fall Precautions
EM Physician: Perform mobility evaluation workup:
Orthostatic Vital Signs
Assess polypharmacy
Evaluate level of substance use
Assess level of deconditioning & living situation
if significant concerns, consult SW
Does patient require admission for injuries or other diagnosis?
Spine and Neuro-Trauma should be admitted to Trauma per the Trauma Admission Service Line Agreement
Is the patient amenable to an ED evaluation by Social Work AND/OR PT/OT?
Discuss with patient and include family members as appropriate
Utilize shared decision making & document discussion
Yes No Yes No
Geriatric Consult order panel
Use to order Social Work, PT, & OT
Admit to Trauma vs. Medicine
Reference Trauma Admission Pathway
RN: Give
Physician:
RN Fall Packet
Ambulatory referral to outpatient OT Discharge Home
Use to order Social Work, PT, & OT Geriatric Consult order panel
ED Consult to Social Work
ED PT Eval and Treat
ED OT Eval and Treat
Ambulatory referral to outpatient PT
(Reason: Fall) (Reason: Fall)
Send In-basket message to PCP
Is it after-hours?
PT/OT available: 7:30 AM to 3:30 PM Social work available: 7 AM to 3:30 PM
Yes, after-hours No, day-time hours
SW & PT/OT Evaluation in Main ED
Disposition per SW & PT/OT recommendations with individualized resources to patient
If discharge, RN gives RN Fall Packet
Follow No Medical Indication for Admission Pathway
Ensure patient amenable to stay overnight awaiting PT/OT
Figure 2: Geriatric Fall Pathway. Source: University of Colorado. Geriatric Fall. Agile MD Clinical Pathway. Version 1, Modified August 2025. Accessed March 14, 2026. Internal institutional resource.
Copyright Regents of the
Copyright Regents of the University of Colorado. All Rights Reserved. Created by the University of Colorado Hospital Emergency Department. This quality improvement document is to be maintained solely within the institution and may not be released to any third party without written permission from the department, hospital, and university legal counsel.
Figure 2: Geriatric Fall Pathway
GERIATRIC EM
continued from Page 87
the Geriatric ED Fall Risk Assessment Tool (GEDFRAT) (Figure 1), integrated into the electronic medical record to assign patients a binary fall-risk designation (high or low). Because clinicians and nursing staff were familiar with this tool, GEDFRAT was selected as the institutional screening instrument, with PT and OT evaluation for high-risk patients. The resulting pathway is shown in Figure 2.
Enacting Culture Change
The initiative was framed around expanding focus on mobility and designing a system to keep patients safely out of the hospital—messaging that resonated with both clinical staff and patients.
Patients were often hesitant to remain in the ED for a therapy evaluation after completion of their medical workup. Clinical staff reinforced that the evaluation was intended to reduce the risk of future falls, injuries, and hospitalizations.
PT and OT clinicians were embedded within the ED and regularly engaged with clinicians and nursing
Pulse Points
Key clinical and practice takeaways:
staff in real-time disposition planning. Within six months, PT, OT, and ED staff had developed a shared workflow and common mission focused on safe disposition of older adults after falls.
Return visits were tracked using quality improvement data from the electronic medical record. Although this dataset did not capture visits to non-UCHealth facilities, it provided insight into return visits before and after pathway implementation.
Pre-implementation (Jan. 1–July 13, 2025), there were 961 fall-related ED visits among adults age 65 years and older. Of these, 87 patients (9%) returned within 30 days with a fallrelated visit. Post-implementation (July 14–Dec. 31, 2025), there were 863 fall-related ED visits, with 62 patients (7%) returning within 30 days for a repeat fall-related visit.
Work is ongoing to build a dashboard to track outcomes among patients evaluated by rehabilitation services in the ED. Planned analyses include identifying return ED visits and hospital admissions among high fallrisk patients who received PT and OT evaluation compared with those who did not.
• Mobility assessment is a clinical decision point—failure to assess ambulation can lead to missed injuries and unsafe discharge.
• Embedding physical and occupational therapy in the emergency department can shift care from default admission to function-based disposition.
• Concerns about increased length of stay with therapy evaluation are common but not supported by available evidence.
• Small system changes—standardized screening tools and shared workflows—can produce measurable reductions in return visits.
• Culture change requires alignment: success depends on consistent messaging, interdisciplinary collaboration, and frontline engagement.
Conclusion
At HRH, a fall pathway was implemented to improve mobility assessment and support appropriate disposition after falls. Common barriers included patient reluctance to remain in the ED for evaluation and a persistent, though unsupported, concern that therapy evaluation would increase ED length of stay.
Key elements of success included identification of a care gap through retrospective data analysis, alignment among stakeholders around a shared mission, and sustained engagement from frontline clinicians. Integration of rehabilitation services into ED care has been associated with reduced return visits and improved disposition decisions in older adults presenting after a fall
This experience demonstrates that, through multidisciplinary collaboration, evidence-based fall-prevention strategies can be implemented successfully in a community ED setting serving a high volume of older adults.
ABOUT THE AUTHORS



Dr. Quinones is a clinical instructor of emergency medicine at the University of Colorado School of Medicine and practices at Anschutz Medical Center and Highlands Ranch Hospital.
Dr. Mitchell is an emergency physician and medical director overseeing community emergency departments within UCHealth.
Dr. Goldberg is associate vice chair for research in the department of emergency medicine at the University of Colorado Anschutz Medical Campus.

Barriers to Emergency Care for Patients With Disabilities: Communication, Access, and Equity
By Brooke D. Jones; Shivram Kumar; London S. Smith; Sophia Ellis; Courtney Jones, MD, MPH; and Jason M. Rotoli, MD, MS on behalf of the SAEM Academy for Diversity, Equity & Inclusion
At a Glance
• Why this matters now: Patients with disabilities—particularly those who are deaf or hard of hearing— continue to face significant barriers to care in emergency departments, contributing to delays, miscommunication, and poorer health outcomes.
• What you’ll learn: How communication challenges, inaccessible environments, and systemic inequities affect emergency care delivery, and what
clinicians should understand about accommodations and patientcentered communication.
• Who this is for: Emergency medicine trainees and clinicians seeking to improve equitable care, communication practices, and accessibility in high-acuity emergency settings.
The Americans With Disabilities Act (ADA) defines a disability as a physical or mental impairment that substantially limits one or more major life activities. However,
disability is a nuanced concept, often encompassing conditions that require formal documentation and/or are socially perceived as impairments within environments that are not designed for accessibility.
According to the Centers for Disease Control and Prevention, approximately one in four adults in the United States lives with a disability. Individuals with disabilities are more likely to experience secondary health conditions, including fatigue, chronic pain,
“Approximately one in four adults in the United States lives with a disability and faces disproportionately reduced access to health care.”
obesity, and depression. They also face disproportionately reduced access to health care compared with those without disabilities.
Structural and Social Barriers to Care
Disabilities are associated with a range of structural and social barriers, including stigma, systemic inequities, and insufficient institutional resources. These barriers can significantly restrict an individual’s ability to participate fully in health care decision-making, employment, education, and community engagement.
Within health care settings, patients with disabilities frequently encounter clinicians who lack adequate training in disability-informed care. Individuals who are deaf or hard of hearing (DHH), as well as those with visual or cognitive impairments, may require assistive technologies or professional interpreters to communicate effectively.
Access to equitable health care is a fundamental right. However, patients with disabilities often face significant obstacles in obtaining appropriate accommodations. Family members and friends are frequently expected to assist with communication and other needs, placing an undue burden on both patients and their support networks. This reliance on informal support increases the risk of miscommunication and suboptimal care.
Environmental and Infrastructure Challenges
Environmental and infrastructural barriers further exacerbate these disparities. Inaccessible health care facilities—such as those lacking

ramps, featuring narrow doorways, or providing nonadjustable medical equipment—limit access for patients with physical disabilities. Transportation challenges can also hinder timely access to care.
Even within clinical environments, examination rooms are often not designed to accommodate diverse patient needs. For example, standard examination tables may be inaccessible to individuals with mobility impairments.
Collectively, these barriers contribute to delays in care, decreased utilization of health services, and poorer health outcomes among individuals with disabilities. Addressing these challenges requires systemic interventions, including comprehensive training for health
care professionals and institutional prioritization of accessibility.
Communication Barriers in Emergency Care
Compared with individuals without disabilities, deaf and hard-of-hearing patients experience disproportionately higher rates of health inequities and adverse outcomes. Communication barriers are a primary driver of these disparities, as they can affect diagnosis, treatment planning, and disease management.
These challenges are particularly pronounced in emergency department settings, where high patient acuity, time constraints, and limited resources create additional obstacles to effective communication.

One documented case describes a 95-year-old man with congenital deafness who presented to the emergency department after a fall resulting in a hip fracture. Communication relied on shouting and handwritten notes, which proved inefficient and burdensome. He was ultimately labeled a “poor historian,” and clinicians relied heavily on collateral information. This case highlights how inadequate communication strategies can compromise patient-centered care.
In many settings, individuals with hearing loss are expected to rely on lip reading. However, many DHH individuals in the United States identify American Sign Language as their primary language. Requiring communication through lip reading or written English may be ineffective and inappropriate if it does not align with a patient’s linguistic preference or fluency.
Health care providers must assess each patient’s preferred communication method and ensure access to appropriate accommodations, including qualified interpreting services.
Intersection of Race and Hearing Status
The existing literature on health
Pulse Points
Key clinical and practice takeaways:
outcomes within the Black DHH community remains limited. However, available evidence suggests that disparities are compounded at the intersection of race and disability.
The combined effects of audism— the belief that typical hearing is superior—and systemic racism contribute to poorer health outcomes in this population. Studies show that Black DHH adults have a higher prevalence of chronic conditions, including diabetes, hypertension, lung disease, and cancer, as well as greater overall comorbidity compared with their hearing Black counterparts.
These inequities are further exacerbated in emergency care settings, where patients may experience prolonged wait times, limited access to professional interpreting services, and reliance on ineffective communication methods. While virtual interpreting services can be helpful, they may also present logistical and technological challenges that impede effective communication.
Moving Toward More Equitable Care
Addressing disparities affecting DHH individuals and the broader disability community requires the integration of disability-inclusive frameworks within anti-racist health care policies. It also requires improved provider education and a sustained institutional commitment to accessibility.
• Do not assume communication method—ask patients who are deaf or hard of hearing how they prefer to communicate and document it clearly.
• Avoid relying on family members for interpretation; use qualified interpreters or appropriate assistive technologies whenever possible.
• Recognize that “inaccessible” is often systemic, not individual— environment, equipment, and workflow design directly impact patient care and safety.
• Build awareness of intersectionality: race and disability together can compound disparities and worsen outcomes in emergency settings.
• Small changes matter—improving communication access and physical accessibility can significantly enhance patient trust, accuracy of care, and overall outcomes.
Efforts must target environmental, institutional, and provider-level barriers to create a more accessible health care system and reduce disparities in outcomes. By prioritizing inclusive practices and appropriate accommodations, emergency departments can better serve all patients and advance equitable care
ABOUT THE AUTHORS





Brooke D. Jones is a fourth-year medical student at the University of Rochester School of Medicine and Dentistry and an incoming emergency medicine resident at the University of California, Los Angeles.
Shivram Kumar is a research assistant in the department of emergency medicine at the University of Rochester School of Medicine and Dentistry.
Sophia Ellis is a third-year medical student at the University of Rochester School of Medicine and Dentistry.
London S. Smith is a third-year medical student at the University of Rochester School of Medicine and Dentistry. Dr. Jones is an associate professor in the departments of emergency medicine, orthopaedics, and public health sciences at the University of Rochester Medical Center and director of the evidence-based medicine curriculum, journal club, and the research track within the University of Rochester Medical Center emergency medicine residency program.

Dr. Rotoli is an attending emergency physician and associate professor of emergency medicine at the University of Rochester Medical Center and serves as associate emergency medicine residency program director and director of the Deaf Health Pathways humanities elective at the University of Rochester School of Medicine and Dentistry.
INFORMATICS, DATA SCIENCE & AI
AI Literacy as Procedural Competence in Emergency Medicine
By Neha P. Raukar, MD, MS, and Ronny Otero, MD, MSHA, on behalf of the SAEM Vice Chairs Interest Group
At a Glance
• Why this matters now: Artificial intelligence is already shaping evaluation, education, and clinical reasoning in emergency medicine—often without clear standards or oversight.
• What you’ll learn: A practical framework that reframes artificial intelligence literacy as procedural competence, with guidance on prompting, supervision, and responsible integration into academic and clinical work.
• Who this is for: Vice chairs, department leaders, educators, and emergency physicians seeking to define expectations and reduce variability in artificial intelligence use.
“Every increase in knowledge requires an increase in wisdom,” Bertrand Russell.
At the end of a shift, an attending physician opens a resident evaluation and uses an AI tool to generate structured feedback from brief notes. The result is fluent and
efficient—but dependent on how the prompt was written.
The variability in that output is not incidental. A poorly constructed prompt can introduce bias, including tone shifts and gendered descriptors—patterns well documented in recommendation letters and resident evaluations. AI systems, trained on historical data, do not escape these patterns unless guided carefully.
This shifts the locus of responsibility. The quality of AI
“Artificial intelligence literacy is not a technical skill but a form of applied judgment, including the ability to construct precise prompts, recognize unreliable outputs, and determine when artificial intelligence is appropriate to use.”
output reflects the quality of human input. Prompt construction, bias awareness, and critical review are not technical curiosities; they are emerging elements of professional judgment.
AI Output Reflects Human Input
Emergency medicine has long defined competence through observable skills. Procedural proficiency is not assumed—it is taught, assessed, and maintained. To become boardcertified in emergency medicine, trainees must demonstrate competency in what the American Board of Emergency Medicine defines as Knowledge, Skills, and Abilities (KSAs).
Learners progress from basic understanding—indications, complications, and equipment preparation—to expert performance under variable and high-risk conditions. Mastery includes not only execution, but also complication avoidance, adaptability, and quality assurance.
AI literacy follows a similar trajectory. Early use is often superficial and task-oriented— generating summaries or text without deeper awareness of limitations or bias. With experience, clinicians refine prompts, anticipate failure modes, and adapt outputs to context. At higher levels of competence, AI use becomes flexible and situationally aware, including the ability to recognize subtle inaccuracies and calibrate reliance based on clinical stakes.
AI use, by contrast, has entered practice without a comparable
framework. Faculty use these tools for evaluation writing, teaching materials, and information synthesis, yet expectations remain largely implicit.
The result is uneven practice. Some faculty use AI deliberately and effectively. Others avoid it or engage with it uncritically. The issue is not adoption—it is variation without a shared standard. In other domains of clinical care, such variability would prompt a structured response. In procedural training, inconsistent technique or outcomes would trigger standardized instruction, direct observation, feedback, and reassessment. AI use lacks these guardrails, despite influencing evaluation, education, and clinical reasoning.
From Individual Use to Shared Standards
AI literacy in this context does not require technical expertise. It is a form of applied judgment: the ability to construct precise prompts, recognize unreliable outputs, and determine when AI is appropriate to use.
It also includes awareness of authorship norms, data handling, and the ethical implications of generated content—issues increasingly emphasized in AI research and clinical applications. This mirrors procedural competence, where mastery is defined not only by execution but also by judgment—knowing when to perform a procedure, when to defer, and how to manage complications.
Similarly, AI competence includes knowing when not to use AI, when
to override it, and when its use introduces unacceptable risk.
A parallel shift is occurring among learners. Residents increasingly use tools such as OpenEvidence and other AI platforms to answer clinical questions and supplement learning. For experienced physicians, AI often functions as a cognitive aid within an established knowledge framework. For learners, it may function as a primary source of that framework.
This distinction matters. Without sufficient foundational knowledge, learners may not recognize incomplete or incorrect outputs—a concern reflected in studies evaluating AI performance on medical licensing examinations. This parallels procedural training, where competency cannot be achieved by memorizing steps alone without understanding risk, complications, and performance under non-ideal conditions.
The risk is not simply error. It is misplaced confidence.
Faculty, therefore, are not only users of AI but also models of its use. How AI is incorporated into teaching, documentation, and scholarship becomes part of the learning environment.
In procedural education, supervision decreases as competence increases— but only after demonstrated reliability. AI use is often inverted; high-stakes outputs are generated with minimal oversight or validation. Re-aligning
continued on Page 97

Domain Focus Approach
Expectations Define baseline AI competence Incorporate into faculty standards and review processes
Skills Emphasize prompting and critical appraisal
Boundaries Clarify ethical and professional use
Consistency
Reduce variability in practice
Integration Align with existing systems
INFORMATICS
continued from Page 95
this model requires treating AI engagement as a skill that progresses from supervised to independent use, with explicit benchmarks for entrustment.
Departments have begun to respond pragmatically. Rather than developing entirely new curricula, some are integrating AI into existing faculty development through case-based sessions and peer demonstration. These approaches emphasize application over theory and reduce the perception that AI is a separate domain.
For vice chairs and department or residency leadership, the question is less about adoption and more about definition: What constitutes appropriate use? What level of
Pulse Points
Key clinical and practice takeaways:
Use real academic tasks as training contexts
Provide guidance on authorship, privacy, and bias
Share examples and establish norms
Connect AI use to promotion and evaluation structures
competence is expected? How should AI intersect with evaluation, promotion, and scholarship?
Operationalizing AI Competence
A practical approach can be framed in terms of alignment rather than innovation:
Emergency medicine has repeatedly adapted to new forms of knowledge and technology. Ultrasound and electronic documentation required not only adoption, but also standardization. AI presents a similar challenge—on a compressed timeline.
The central issue is not whether AI will be used. It already is. The question is whether its use will remain individual and variable or become structured and shared.
In this sense, AI literacy resembles earlier transitions in clinical competence. It is not an additional
skill layered onto existing practice—it is a change in how work is done. The task ahead is not simply to adopt artificial intelligence, but to define the standards by which it is used
ABOUT THE AUTHORS


Dr. Raukar is an associate professor at Mayo Clinic and vice chair for faculty development and academic affairs.
Dr. Otero is vice chair for clinical operations in the department of emergency medicine at Froedtert & the Medical College of Wisconsin, professor of emergency medicine, and director of the Health Executive and Administrative Leadership fellowship.
• Artificial intelligence output is only as reliable as the prompt—poor input can introduce bias, tone distortion, and misleading conclusions.
• Treat artificial intelligence use like a procedural skill: it requires training, supervision, feedback, and clear standards— not informal adoption.
• Variability in artificial intelligence use is already affecting evaluation, education, and clinical reasoning—lack of structure is itself a risk.
• Faculty are not just users but role models—how artificial intelligence is used in documentation and teaching shapes learner behavior and expectations.
• The greatest risk is not error but overconfidence—especially for learners who may rely on artificial intelligence without sufficient foundational knowledge.
INFORMATICS, DATA SCIENCE & AI

The Hidden Second Shift: How Artificial Intelligence Is Reshaping Your Academic Career
By Christopher Awad, MD, MBA; Donald Wright, MD, MHS; Arwen Declan, MD, DPhil; Neha P. Raukar, MD, MS; Wendy W. Sun, MD, MBA
At a Glance
• Why this matters now: Physicians spend up to two hours on administrative work for every hour of direct patient care, revealing a hidden “second shift” that strains academic careers.
• What you’ll learn: How artificial intelligence can organize academic data, streamline faculty workflows, and create more transparent, structured pathways for career advancement.
• Who this is for: Emergency physicians, faculty, and academic leaders navigating promotion, mentorship, and professional development alongside demanding clinical roles.
The Hidden Second Shift of Academic Medicine
You’re wrapping up a shift in the emergency department. You’ve managed critically ill patients, supervised residents, and coordinated with consultants — a job
well done. As the clinical work winds down, another set of responsibilities comes into focus: updating a CV for promotion review, responding to mentorship emails, reviewing trainee evaluations, and documenting teaching activities for an annual faculty report. The list goes on.
For many emergency medicine faculty, this administrative work has become an expected — but exhausting — part of academic life. While artificial intelligence (AI) is
“Physicians spend up to two hours on administrative tasks for every hour of direct patient care, underscoring the scale of this burden and the opportunity for workflow redesign.”
widely discussed in medicine for its potential to improve diagnostics, imaging interpretation, and clinical decision support, its potential impact on faculty careers and academic infrastructure has received far less attention.
Recent national analyses suggest physicians spend up to two hours on administrative tasks for every hour of direct patient care, underscoring the scale of this burden and the opportunity for workflow redesign.
AI Moves Beyond the Bedside
This is beginning to change. AI tools are already entering the workflows of emergency physicians — not only at the bedside, but also in education, research, and professional development. As these technologies mature, they may fundamentally reshape how academic careers are supported and evaluated.
Understanding this shift is important for emergency medicine faculty because the same technologies transforming clinical practice may also transform how faculty build their careers, track their achievements, and engage in professional development.
The Complexity of Academic Career Infrastructure
For academic physicians, career success depends on more than clinical expertise. Promotion dossiers, mentorship networks, scholarly output, teaching evaluations, and leadership development all influence advancement. Yet many of these processes remain fragmented across
systems, manually curated, and administratively burdensome.
Artificial intelligence offers an opportunity to rethink how these systems function. Rather than replacing the work of faculty, AI has the potential to augment professional development, streamline administrative processes, and create more transparent pathways for career advancement. This concept — often referred to as “augmented intelligence” — emphasizes human-AI collaboration rather than automation alone.
From Data Overload to Insight
Academic medicine generates enormous volumes of information. Faculty maintain CVs and promotion portfolios while simultaneously producing research publications, teaching evaluations, clinical productivity metrics, committee service documentation, and mentorship records. These data are often distributed across multiple institutional systems, increasing administrative burden and requiring manual synthesis.
AI systems — particularly those based on natural language processing and large language models — are well suited to assist with these tasks. Such technologies can extract structured information from large bodies of text, summarize academic outputs, and generate reports from disparate data sets. In other sectors, similar tools already create continuously updated professional profiles and performance
dashboards, reducing reliance on selfreported documentation.
Applications in Faculty Development and Workforce Design
Outside health care, AI-driven workforce tools help organizations map career pathways and identify opportunities for professional growth. Similar approaches are emerging in health professions education and academic workforce development
For emergency medicine faculty, who balance demanding clinical schedules with teaching, research, and service responsibilities, reducing administrative workload could be transformative.
Emerging literature reflects both enthusiasm and caution. AI tools can support personalized learning pathways, tailoring educational content and feedback to individual learners. These approaches could extend to faculty development, enabling individualized career planning and competency-based growth. Large language models have also been used to augment coaching, acting as a sounding board for physicians preparing to give feedback or negotiate.
Implications for Scholarship and Academic Life
Scholars are also examining how AI may influence academic life more broadly. One commentary describes how an AI-generated manuscript passed blinded peer review, illustrating both the capabilities and disruptive potential of these technologies. Articles in Nature and JAMA have highlighted both productivity gains and integrity risks associated with generative AI in scientific writing, underscoring how rapidly AI is reshaping scholarly communication.
Emerging Use Cases in Faculty Affairs
Although still developing, several use cases are becoming apparent. AI tools are beginning to automatically gather publications, teaching activities, and service contributions from institutional
continued on Page 101
“Artificial intelligence has the potential to development, streamline administrative processes, more transparent pathways for career

continued from Page 99
databases and external sources, generating continuously updated academic profiles. Integration with persistent identifiers such as ORCID enhances the feasibility of automated portfolio construction.
Promotion committees often review extensive documentation to evaluate faculty achievements. AI systems could help summarize scholarly output, identify patterns in productivity, and highlight key accomplishments. Institutions could also analyze historical promotion data to clarify expectations and provide more transparent benchmarks.
Mentorship remains one of the strongest predictors of academic success, yet many institutions struggle to match mentors and mentees effectively. AI tools could analyze research interests, collaboration patterns, and career trajectories to recommend mentorship pairings and identify gaps in mentorship networks.
Ethical Considerations and Risks
Despite these opportunities, integrating AI into faculty affairs raises important ethical questions. AI models trained on historical promotion or evaluation data may replicate existing inequities within academic medicine. Research has show that algorithmic tools can reproduce gendered language patterns present in historical evaluations
Concerns about bias, transparency, and data governance are well documented across health care AI applications, reinforcing the need for deliberate oversight.
Why Emergency Medicine Is Well Positioned
Emergency medicine departments may be particularly well positioned to benefit from AI-supported faculty development. The specialty already operates within data-rich environments that track clinical productivity, operational metrics, and educational outcomes.
Applying similar approaches to faculty affairs could help departments monitor workload distribution, identify early signs of burnout, and recognize faculty approaching promotion milestones.
medicine faculty, the question is no longer whether AI will influence academic medicine — it already is.
The more important question is whether faculty will help shape how these tools are used to build, evaluate, and sustain their careers. Faculty engagement will be critical to ensure AI augments — rather than constrains — academic identity, creativity, and career development.
Departments that engage thoughtfully with AI — balancing innovation with ethical oversight — may be better positioned to support faculty success, reduce administrative burden, and foster the next generation of academic leaders
ABOUT THE AUTHORS

Dr. Awad is a second-year resident in emergency medicine at The Ohio State University.
processes, and create career advancement.”
Pulse Points
Key clinical and practice takeaways:
• Faculty engagement is critical—without it, artificial intelligence risks reinforcing existing inequities rather than improving academic systems. augment professional
The Bottom Line: Augmentation, Not Replacement
Artificial intelligence is often framed as a technology that will transform patient care. That transformation is already underway For emergency


Dr. Wright is a clinical informatics fellow at Yale School of Medicine.
• Administrative work is the hidden second shift—recognizing its scope is the first step toward redesigning how academic careers are supported.
• Artificial intelligence is not just a clinical tool—it can streamline curriculum vitae management, teaching documentation, and promotion preparation.
• Data already exist—what is missing is integration; structured systems can turn fragmented academic work into usable insight.
• Transparency changes behavior—clearer benchmarks and visible career pathways can reshape how faculty plan and progress.


Dr. Declan is assistant research director at Prisma Health Upstate and a clinical assistant professor at the University of South Carolina School of Medicine–Greenville and Clemson University.
Dr. Raukar is an associate professor at Mayo Clinic and vice chair for faculty development.
Dr. Sun is an assistant professor at Columbia University Medical Center and assistant medical director at NewYork-Presbyterian Allen Hospital.

From Clinical Question to Model: Building Machine Learning Pipelines in Emergency Medicine
By Wayne Martini, MD
At a Glance
• Why this matters now: Machine learning is rapidly moving into clinical workflows, but most emergency physicians lack a practical roadmap to build usable models from electronic health record data.
• What you’ll learn: A step-by-step, clinically grounded approach to building machine learning pipelines, from cohort extraction
in structured query language to model validation and deployment.
• Who this is for: Emergency physicians, residents, and clinicianresearchers who want to turn clinical questions into data-driven tools without formal training in data science.
You have a clinical question, access to your institution’s electronic health record (EHR) data warehouse, and a growing sense that machine learning (ML) could help you answer
it. But where do you start? Unlike bench research or even traditional clinical studies, building an ML pipeline requires stitching together skills most clinicians never learned in residency — SQL, Python, and the statistical thinking that bridges them.
Over the past two years, our group has built end-to-end ML pipelines to predict clinical outcomes at emergency department triage, from CT utilization to acute surgical abdomen to lab ordering patterns, using data extracted from an Epic

“Deliberately excluding laboratory results, imaging findings and consultant notes forces your model to mirror what a triage nurse or physician actually knows at the moment of decision-making.”
Clarity database and analyzed in Python. Here is the practical, step-bystep workflow we wish someone had handed us when we started.
Start With the Decision Point: Ask a Triage-Answerable Question
The strongest ML applications in emergency medicine constrain themselves to information available at a single clinical decision point.
For triage-based models, this includes demographics, chief complaint, arrival vital signs, mode of arrival, Emergency Severity Index level, and past medical history. Deliberately excluding labs, imaging results and consultant notes forces your model to
mirror what a triage nurse or physician actually knows at the moment of decision-making.
This constraint is not a limitation — it is what makes a model clinically deployable.
Build the Foundation: Extract a Clean Cohort in SQL
If your institution runs Epic, the Clarity data model is a common starting point. The ED encounters table anchors each visit with arrival time, departure time, ESI level, disposition and provider. From there, join outward to capture additional elements such as triage vitals, chief complaint, comorbidities, orders and medications.
A
few practical lessons:
• Use temporary tables with explicit indexing. Queries spanning millions of encounters across multiple years will time out without them. Build your cohort first, index it on encounter ID, then join all additional data to that table.
• Engineer features in SQL, not Python. Binary flags for orders (for example, CT or complete blood count), comorbidity counts, bounceback windows and complaint categories are cleaner and faster when computed at the database layer. Your
continued on Page 105

continued from Page 103
Python workflow should receive a ready-to-model dataset, not raw EHR data.
• Filter vital signs to physiologic ranges. Extreme values are often data entry artifacts. Identify reasonable bounds and replace outliers rather than dropping entire rows.
• Exclude test patients. Even small numbers can introduce bias into your training data.
Translate Data Into Features: Preprocess and Engineer in Python
With a clean dataset exported from SQL, the Python workflow becomes manageable. Core tools include pandas for data manipulation and scikit-learn for preprocessing and modeling.
A typical preprocessing pipeline includes:
• Numeric features (vital signs, age): median imputation followed by scaling
• Categorical features (chief complaint category, sex, race): most-frequent imputation followed by one-hot encoding
• Binary features (order flags, comorbidities): passed through unchanged
You can also add clinically meaningful derived variables, such as
Pulse Points
Key clinical and practice takeaways:
shock index, mean arterial pressure or simplified early warning scores. Interaction terms — for example, age combined with ESI level — can help models capture relationships clinicians already use intuitively.
Test What Matters: Train, Validate and Explain the Model
Begin with a stratified 80/20 train-test split. Stratification is essential when outcomes are imbalanced, which is common in clinical data.
For class imbalance, apply resampling techniques such as SMOTE only to the training set. Applying them before the split introduces data leakage.
Train multiple model types in parallel, including:
• Logistic regression (interpretable baseline)
• Random forest
• Gradient boosting models such as XGBoost or CatBoost
Compare performance using crossvalidation, then evaluate the best model on a held-out test set.
Go beyond area under the curve. Report:
• Calibration: how predicted probabilities match observed outcomes
• Precision-recall: especially important for rare events
• Threshold analysis: sensitivity, specificity, positive predictive value and negative predictive value
Model explainability tools, such as SHAP values, help translate model behavior into clinically meaningful insights.
If multi-site data are available, leave-one-site-out validation can approximate external validation without requiring formal data-sharing agreements.
From Model to Impact: Close the Loop
A model that lives only in a notebook does not change patient outcomes.
Export the trained model and preprocessing pipeline, then build a simple interface or deploy to a cloud-based endpoint. Even a basic dashboard allows colleagues to interact with predictions in real time.
This step often distinguishes a publishable model from one that meaningfully affects clinical practice.
Getting Started: What You Actually Need
You do not need a computer science degree. You need:
• A clear clinical question
• Access to your EHR data warehouse
• A Python environment (for example, Anaconda)
• Willingness to iterate
The first query may take a week. The tenth may take an afternoon. Once built, the pipeline becomes reproducible and transferable across clinical problems.
The emergency department generates enormous volumes of structured data at every patient encounter. ML provides the tools to learn from that data systematically.
• Start with the decision point: models built on information available at triage are far more likely to translate into real clinical use.
• Do the heavy lifting in structured query language, not Python: clean, wellengineered data upstream makes modeling faster, simpler and more reliable.
• Guard against data leakage: how you split, balance and preprocess data can matter as much as the model you choose.
• Performance is not just area under the curve: calibration, threshold analysis and clinical usefulness determine whether a model actually informs care.
• A model is only as valuable as its implementation: moving from notebook to usable tool is what turns a project into impact.
The bottleneck is not the technology. It is clinicians willing to build the bridge
ABOUT THE AUTHOR

Dr. Martini is an assistant professor at Mayo Clinic College of Medicine and Science and a consultant in the department of emergency medicine at Mayo Clinic in Phoenix, Arizona.

Measuring What Matters: A New Approach to Emergency Department Boarding
By John Riggins, Jr. MD, MHA
At a Glance
• Why this matters now: Emergency department boarding remains a national crisis, but inconsistent definitions and flawed metrics continue to obscure its true impact and hinder effective solutions.
• What you’ll learn: A clearer, systems-based approach to defining and measuring boarding, with practical domains that better reflect patient outcomes, workforce strain, and hospital-wide performance.
Introduction
Emergency department (ED) boarding is a widely recognized crisis among health care leaders, researchers, policymakers, and regulators. Despite broad agreement that boarding harms patients, clinicians, and health systems, there is no standardized definition or set of meaningful measurements to describe its true impact. Professional organizations have attempted to standardize definitions for key stakeholders, but challenges
• Who this is for: Emergency department leaders, administrators, and policymakers seeking more accurate, actionable ways to understand and address boarding.
in applying these definitions across domains persist. Although the literature consistently demonstrates adverse outcomes associated with ED boarding, definitions vary widely and measurements remain inconsistent. Without consensus on what constitutes boarding and how to measure it accurately, policy, operational, and research efforts remain fragmented and ineffective.
Current State of ED Boarding Definitions and Measurements
ED boarding has been defined inconsistently across research, operational, and regulatory domains since its recognition. It has been described using different triggers
“Without consensus on what constitutes emergency department boarding and how to measure it accurately, policy, operational, and research efforts remain fragmented and ineffective.”
and endpoints, including the decision to admit, placement of admission orders, a fixed time threshold after admission, or physical departure from the ED. Some studies apply arbitrary time cutoffs, while others focus on specific populations, including medical, surgical, intensive care unit, or behavioral health patients.
This variability makes it difficult to synthesize findings or draw definitive conclusions about the magnitude and mechanisms of harm associated with ED boarding. Although regulatory bodies such as the Centers for Medicare & Medicaid Services (CMS) and The Joint Commission provide definitions of boarding, these frameworks are designed for reporting and compliance rather than for accurately measuring clinical care delivery or system performance.
The consequences of inconsistent definitions extend across research, operations, and policy. From a research perspective, variability limits the ability to aggregate evidence on outcomes such as mortality, adverse events, and patient experience. It also hampers efforts to quantify the true impact of boarding on the ED workforce, departmental performance, and hospital operations.
Operationally, disparate definitions allow hospitals to improve reportable ED-centric metrics without addressing upstream contributors such as inpatient capacity constraints, inefficient throughput, or discharge bottlenecks. At the policy level, regulatory measurements tied
continued on Page 109

Read More, Learn More
• Emergency department operations dictionary: results of the second performance measures and benchmarking summit
• The association between length of emergency department boarding and mortality
• Inpatient boarding definitions and mitigation strategies: A cross-sectional survey of academic emergency departments in the United States
• The Joint Commission. Chart-abstracted measures for accreditation: emergency department measures
“Metrics
time

“Metrics that remain emergency department-centric or rely on arbitrary time thresholds will continue to obscure root causes and stall progress.”
OPERATIONS
continued from Page 107
to incentives and penalties risk misattributing system-level failures to emergency departments. This may penalize EDs for problems beyond their control and discourage meaningful structural reform.
Key Boarding Measurement Domains to Consider
Boarding measurements become meaningful only when they are patient-centered, clinically relevant, actionable, and capable of holding the broader health care system accountable. Metrics that remain ED-centric or rely on arbitrary time thresholds will continue to obscure root causes and stall progress. Several domains may better reflect the true impact of ED boarding. These include standardized, clinically relevant time-based metrics, such as time from admission decision to inpatient bed placement, stratified by acuity, or boarding hours per admitted patient-day.
Additional measures should capture peak boarding periods,
Pulse Points
Key clinical and practice takeaways:
when ED crowding most severely affects care delivery. Risk-adjusted metrics for high-risk populations— including ICU-level, elderly, and behavioral health patients—are also essential. Workforce and experience measures, such as clinician-topatient workload ratios and patientreported experiences during boarding, offer critical insight into safety and workplace sustainability.
Finally, system-level capacity and flow metrics—including hospital occupancy during peak boarding periods and discharge-before-noon rates—are necessary to place ED boarding in proper operational context.
Conclusion
By more clearly defining and measuring ED boarding and its consequences, emergency department leaders can shift the narrative from viewing boarding as an ED throughput failure to recognizing it as a system-level failure.
Achieving this shift will require interdisciplinary collaboration among key stakeholders to establish national consensus on definitions and measurements. Researchers
can promote multicenter adoption of standardized definitions, while policymakers and regulators can better align quality measures, payment incentives, and regulatory frameworks with system-level accountability.
Emergency medicine leaders are uniquely positioned to lead these efforts and shape the national conversation through partnerships with hospital administrators, researchers, policymakers, private accrediting organizations, and regulators. Until ED boarding is measured honestly, consistently, and comprehensively, it will continue to be mischaracterized as an ED problem, and effective solutions will remain out of reach
ABOUT THE AUTHOR

Dr. Riggins is an assistant professor of emergency medicine at NewYorkPresbyterian/Columbia University Department of Emergency Medicine and Columbia University Vagelos College of Physicians and Surgeons. He serves as medical director of the NewYork-Presbyterian/Allen emergency department and chair of the emergency department’s Bridge Builders Board.
• Start with the decision point: models built on information available at triage are far more likely to translate into real clinical use.
• Do the heavy lifting in structured query language, not Python: clean, well-engineered data upstream makes modeling faster, simpler and more reliable.
• Guard against data leakage: how you split, balance and preprocess data can matter as much as the model you choose.
• Performance is not just area under the curve: calibration, threshold analysis and clinical usefulness determine whether a model actually informs care.
• A model is only as valuable as its implementation: moving from notebook to usable tool is what turns a project into impact.
OPERATIONS

From Interruptions To Flow: Redesigning Result Management To Support Clinician Well-Being
By Jennifer Goebel, DO; Jessica Sidle; Megan Wider; Diana Fuzailov; Joe Aquilino; Nicole Serviss; Dana Cortapasso; and Karen Kline
At a Glance
• Why this matters now: Postdischarge test result management can disrupt emergency department workflow, contributing to inefficiency and clinician fatigue in already high-demand environments.
• What you’ll learn: How a centralized callback model improved workflow efficiency, reduced interruptions, and standardized patient follow-up across a large health system.
• Who this is for: Emergency physicians, advanced care providers, and leaders seeking practical, system-level strategies to reduce administrative burden and support clinician well-being.
When Every Minute Matters, What Gets in the Way?
In emergency medicine, every minute of a clinician’s shift is designed around patient care. Yet many emergency physicians and advanced care providers find themselves pulled
away from the bedside to manage post-discharge test results—a task that, while essential, can interrupt workflow, divide attention and contribute to fatigue.
Efficiency of practice is a foundational component of health care delivery, directly influencing both patient outcomes and clinician well-being. The Stanford Model of Occupational Well-Being identifies workplace efficiency, along with a culture of wellness and individual factors, as essential drivers of
“When systems support clinicians, they can focus on what matters most: delivering high-quality, patient-centered care.”
professional satisfaction. When systems support clinicians, they can focus on what matters most: delivering high-quality, patientcentered care.
At Northwell Health, variation in how post-discharge results were managed revealed an opportunity to better align operations with that goal.
Identifying the Opportunity
The Emergency Medicine Service Line at Northwell Health spans 18 sites, including community hospitals and tertiary and quaternary care centers and now includes Legacy Nuvance Health. Historically, approaches to managing post-discharge laboratory and radiology results varied across the system.
Some sites used dedicated staff to handle patient callbacks. Others relied on clinicians to complete
callbacks during active clinical shifts. This inconsistency created uneven workload distribution and, in many cases, required clinicians to balance bedside care with administrative follow-up tasks.
For clinicians working in already demanding environments, these interruptions affected workflow efficiency and, at times, their sense of professional well-being.
The Patient Results Now Program
To address these challenges, the Emergency Medicine Service Line implemented the Patient Results Now (PRN) program—a centralized model for managing post-discharge laboratory and radiology results.
The program established a dedicated team of advanced care providers responsible for:
• Monitoring post-discharge results in near real time
• Communicating results to patients
• Coordinating follow-up care when needed
Using platforms such as Microsoft Dynamics (ListApp) and the PeerVue radiology system, the PRN program created a standardized, systemwide approach to result management.
Impact on Clinical Practice
The transition to a centralized callback model produced several meaningful changes across participating sites.
Clinicians experienced fewer interruptions during active shifts, allowing them to maintain focus on direct patient care. Workflows became
continued on Page 113

continued from Page 111
more predictable, with less need to shift between clinical responsibilities and administrative tasks.
Patients benefited from more timely and consistent communication regarding test results. A dedicated team ensured that follow-up outreach was coordinated and reliable.
Just as importantly, the program aligned with broader organizational efforts to support clinician well-being by reducing nonclinical workload—a known contributor to burnout.
Lessons Learned
Several key insights emerged from the implementation of the PRN program:
• Standardization reduces variability. A centralized approach promotes consistency in both clinician workflow and patient experience.
• Dedicated roles improve focus. Assigning responsibility for callbacks to a specific team allows clinicians to concentrate on core clinical duties.
• Operational changes support wellbeing. Reducing administrative burden is a practical and effective way to address clinician fatigue.
• Technology supports—but does not replace—process design. Digital tools are essential, but clearly defined roles and workflows are what drive success.
Pulse Points
Key clinical and practice takeaways:
Discussion
The PRN program reflects a broader shift in health care toward systemlevel solutions that improve both efficiency and workforce well-being. Research has consistently shown that clinician well-being is closely tied to patient outcomes. When clinicians are supported, they are better positioned to deliver safe, compassionate and patient-centered care.
By redesigning how post-discharge results are managed, Northwell Health aligned operational processes with the principles outlined in the Stanford Model of Occupational WellBeing and national efforts to reduce administrative burden in health care.
Conclusion
The Patient Results Now program demonstrates that thoughtful process redesign can improve efficiency, enhance patient communication and support clinician well-being at the same time.
Centralizing post-discharge callback responsibilities reduced interruptions to clinical care and created a more sustainable workflow for emergency providers. Efforts to improve clinician well-being are not separate from patient care—they are integral to it.
Programs like PRN show that when health systems remove barriers to efficiency, they create space for clinicians to do what they are trained to do best: care for patients
ABOUT THE AUTHORS






Dr. Goebel is director of wellness for the emergency medicine service line and an attending physician in emergency medicine at Northwell South Shore University Hospital.
Jessica Sidle is a physician assistant in emergency medicine at Northwell Health Huntington Hospital.
Megan Wider is assistant vice president for the emergency medicine service line at Northwell Health.
Diana Fuzailov is senior manager of advanced clinical providers in emergency medicine at Northwell Health Long Island Jewish Medical Center.
Joe Aquilino is senior manager of operations in emergency medicine at Northwell Health Long Island Jewish Valley Stream Hospital.
Nicole Serviss is senior program manager for the emergency medicine service line at Northwell Health.
• Centralizing post-discharge result management reduces interruptions, allowing clinicians to stay focused on bedside care during active shifts.
• Dedicated roles matter: assigning callbacks to a specific team improves workflow efficiency and consistency across sites.
• Reducing administrative burden is a practical, system-level way to support clinician well-being and mitigate burnout.
• Standardization drives reliability—aligning processes across sites improves both clinician experience and patient communication.
• Technology enables efficiency, but clear workflows and role design are what ultimately make systems work.


Dana Cortapasso is chief of staff and assistant vice president of operations in facilities services at Northwell Health.
Karen Kline is vice president of integrated operations and executive shared services for the emergency medicine service line at Northwell Health.
SIMULATION
Beyond Points and Leaderboards: Designing Meaningful Gamification in Simulation
By Sarah Rabinowitz, MD; Katherine Stewart, MD, MEHP; Tiffany Moadel MD; and Suzanne (Suzi) Bentley, MD, MPH, on behalf of
the SAEM Simulation Academy
At a Glance
• Why this matters now:
Gamification is gaining traction in medical education, but its value depends on intentional design—not novelty or competition alone.
• What you’ll learn: Practical strategies to implement gamification in simulation, from low-resource approaches to larger systems, while preserving learning objectives and psychological safety.
• Who this is for: Emergency medicine educators and simulation leaders looking to make learning
more engaging without sacrificing rigor or outcomes.
Gamification in medical education is often discussed as a set of tools—points, leaderboards, escape rooms—but in practice, it is far more nuanced. At the SAEM Simulation Academy Early Career Subcommittee panel on gamification in simulation, Stephanie Cohen, DO, Michael Nguyen, MD, and Dr. Gianna Petrone, DO, offered a more grounded perspective: gamification is not about turning learning into a game, but about thoughtfully leveraging what makes games engaging to
deepen how learners interact with simulation.
What emerged from their discussion was not a single approach, but a spectrum— ranging from small, low-resource interventions to large-scale, longitudinal systems embedded within residency training.
From Everyday Incentives to Intentional Design
For Dr. Cohen, gamification starts with a simple observation: “We use gamification so much in everyday life and don’t notice it—airline points, Starbucks points, credit card points.”
“Gamification is not about turning learning into a game, but about thoughtfully leveraging what makes games engaging to deepen how learners interact with simulation.”
These systems work because they tap into motivation in ways that feel intuitive and rewarding. In medical education, she explained, similar structures can drive engagement when aligned with clear goals.
That alignment is critical. As Dr. Cohen emphasized, “learning objectives should be identified ahead of time,” ensuring the educational purpose remains central. In her experience, gamification works best when it reinforces—not replaces—the clinical reasoning and decisionmaking at the heart of simulation. Learners still need to complete critical actions; game elements simply shape how they move through the experience.
Dr. Nguyen, who has incorporated gamification into simulation for more than a decade, described how even small design choices can influence behavior. In wilderness medicine simulations, his team uses “accumulating micro-awards like points” to encourage learners to stay on schedule and move efficiently between stations. These subtle incentives help maintain flow without disrupting the educational experience.
At the same time, he noted an important distinction: “Escape rooms are almost a different topic than gamification.” While both are engaging, escape rooms require a level of immersion and complexity that demands additional planning and infrastructure.
Designing for Engagement and Inclusion
As the panelists described their approaches, a recurring theme emerged: effective gamification is not one-size-fits-all.
Dr. Petrone highlighted this in the context of wilderness medicine.
“Not every learner appreciates the physicality,” she said, which prompted her team to incorporate puzzles, riddles and other cognitive challenges. The goal was not just engagement, but inclusivity—ensuring every learner could find a meaningful way to participate.
Dr. Nguyen echoed this philosophy, pairing objective scoring systems— such as critical action checklists and time-based metrics—with lighter, more creative elements. In some sessions, teams might also earn points for “best outfit” or “best selfie,” adding levity while maintaining transparency about how subjective elements are judged.
Across these examples, the principle is consistent: the “game” should enhance the experience, not dominate it.
The Hidden Work Behind the Scenes
While gamified simulation can feel seamless to learners, the panelists were candid about what happens behind the scenes.
“It’s a lot of extra planning,” Dr. Petrone said, recalling the challenge of running an escape room for an entire residency within a limited space. Dr. Cohen similarly emphasized the resource demands of larger events such as SimWars or SonoWars, which require significant faculty time, coordination and logistical support.
Dr. Nguyen pointed to another critical step: piloting. “You want to have the opportunity to pilot your escape room to make sure people can’t skip puzzles and that they can succeed in a reasonable amount of time,” he said. Even tabletop
walkthroughs can reveal gaps in design before full implementation.
These insights highlight an often overlooked reality: successful gamification depends as much on preparation as it does on creativity.
Balancing Engagement With Psychological Safety
As engaging as gamification can be, it also introduces potential tension— particularly around competition.
Dr. Petrone shared that some residents are uncomfortable being compared with peers or having scores made public. In response, the panelists described a shift toward team-based models that diffuse individual pressure.
“We keep individual scores private ... and only the team winners are identified,” Dr. Cohen said. This approach preserves the motivational benefits of competition while minimizing its downsides.
Dr. Nguyen described going a step further by asking residents about their preferences—whether they wanted to participate in competitive or noncompetitive teams. “That way,” he said, “residents didn’t feel overwhelmed or frustrated.”
Within teams, learners can gravitate toward roles that match their strengths—whether leading a procedure, solving a puzzle or contributing in other ways.
Even the stakes are carefully calibrated. “Using prizes that are not inconsequential,” Dr. Nguyen said— such as a mug rather than a highvalue reward—helps keep the focus on learning rather than winning.
continued on Page 117
“Successful gamification thoughtful preparation as
continued from Page 115
Where the Learning Happens
Despite the emphasis on gameplay, all three panelists returned to the same point: the most important part of simulation remains the debrief.
“It’s easy to get caught up in the event,” Dr. Cohen said, “but not making time for debriefing ... that’s where the learning happens.” In her programs, gamified sessions include the same structured debriefing as traditional simulations, ensuring space for reflection and discussion.
Assessment also remains grounded in familiar methods. Pre- and postsession knowledge testing, along with blinded feedback surveys, provide insight into learner experience and knowledge gains. But as Dr. Nguyen cautioned, “gamified scores may not translate to how you do clinically.” These activities are best understood as tools for reinforcement, not formal measures of competence.
gamification depends as much on as it does on creativity.”
Starting Small and Scaling Thoughtfully
For educators interested in incorporating gamification, the panelists offered a consistent message: start small.
“Start with low-scale gamified events,” Dr. Cohen advised, pointing to simple interventions such as procedural relay races, timed challenges or point-based trivia within didactics. These approaches can be highly effective without requiring extensive resources.
Dr. Nguyen highlighted the natural compatibility between gamification and protocol-driven care. “Procedures and algorithmic cases ... are already ordered and protocolized,” he said, making them well-suited to gamebased formats. At the same time, he emphasized that not everything needs to be scored. Some of the most effective activities are unscored, such as hands-on airway setup exercises using case cards to reinforce practical skills.
Across the discussion, there was clear agreement that gamification is not a replacement for traditional teaching. Lectures, standard simulations and other foundational methods remain essential. What gamification offers is a way to make reinforcement more engaging, interactive and memorable.
Pulse Points
Key clinical and practice takeaways:
• Start small and be intentional: simple, low-resource gamification strategies can meaningfully improve engagement when tightly aligned with learning objectives.
• Design for inclusion, not just competition: offering multiple ways to participate ensures broader engagement and protects psychological safety.
• The real work happens behind the scenes: effective gamification requires planning, piloting and iteration—not just creative ideas.
• Keep the focus on learning, not winning: game elements should reinforce clinical reasoning, not distract from it.
• Debrief is nonnegotiable: regardless of format, structured reflection remains the most critical component of simulation-based learning.
A Tool, Not a Trend
As gamification continues to gain traction in medical education, its value lies not in novelty, but in intentionality. When thoughtfully designed, it can transform familiar content into experiences that resonate more deeply with learners.
As Drs. Cohen, Nguyen and Petrone illustrated, the goal is not to turn education into a game—but to borrow just enough from games to make learning stick.
As Drs. Cohen, Nguyen, and Petrone illustrated, the goal is not to turn education into a game—but to borrow just enough from games to make learning stick
ABOUT THE AUTHORS

Dr. Rabinowitz is a medical simulation fellow at Northwell Health and a simulation fellow with the SAEM Simulation Academy. She is an assistant professor in the department of emergency medicine at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell.


Dr. Stewart is a simulation fellow with the SAEM Simulation Academy and an assistant professor of emergency medicine at Tufts University School of Medicine, based at Maine Medical Center, Maine Health.
Dr. Moadel is president of the SAEM Simulation Academy and director of simulation in the department of emergency medicine at North Shore University Hospital, Northwell Health. She is also an assistant professor in the department of emergency medicine at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell.


Dr. Shin-Kim is director of emergency medicine simulation and an assistant professor in the department of emergency medicine at Columbia University Medical Center.
Dr. Bentley is immediate past president of the SAEM Simulation Academy and chief wellness officer at NYC Health + Hospitals/Elmhurst Hospital. She is also a professor in the departments of emergency medicine and medical education at the Icahn School of Medicine at Mount Sinai.

SIMposium Spotlight: The Real Work After Simulation—Lessons on Debriefing and Learning
By Avery Keesee, Katherine Stewart, MD; Sarah Rabinowitz, MD; Marcus Sinewe, MD; Janice Shin-Kim, MD; Tiffany Moadel, MD; Suzanne Bentley, MD, on behalf of the SAEM Simulation Academy
SIMposium is a national presentation series hosted every other month by the SAEM Simulation Academy. The series highlights simulation careers and achievements while offering practical insights and reflections from experienced simulation educators.
Over the past decade, simulation in emergency medicine has grown increasingly sophisticated. Advances
in technology now allow educators to recreate clinical environments with remarkable detail. Yet as simulations have become more complex, a key question remains: what truly drives learning?
The Simulation Academy’s January 2026 SIMposium explored this question not through technical instruction, but as an invitation
to pause and reflect on the fundamental purpose of simulation.
“Simulation Is Really an Excuse to Debrief”
Marcus Sinewe, MD, a Stanford emergency medicine simulation fellow and former U.S. Air Force physician who served with ground surgical teams, brought a perspective shaped by both
“If we believe simulation matters, then we have to treat it like serious educational work.”
academic simulation and frontline trauma care. Early in the session, he offered a line that anchored the discussion:
“Simulation is really an excuse to debrief.”
In a field increasingly focused on technological sophistication, Dr. Sinewe reminded attendees that realism alone does not guarantee meaningful learning.
“The scenario creates the shared experience,” he explained, “but the learning happens afterward.”
Rather than emphasizing highfidelity mannequins or elaborate cases, Dr. Sinewe highlighted the importance of clear purpose, psychological safety, and deliberate debriefing. The scenario creates a shared experience; the deeper work begins afterward through structured reflection on what occurred and why.
Lessons From the Field
Dr. Sinewe drew on his experience training military trauma teams in austere environments, where realism was often limited by circumstance rather than design.
“In those environments,” he noted, “we did not have the luxury of distraction.”
Ground surgical teams trained with minimal equipment and limited time, requiring simulations to be focused and intentional, paired with meaningful reflection. The goal was preparation for deployment— not theatrical replication of clinical chaos—and to help teams communicate clearly, maintain shared
on Page 121

“Simulation is really an excuse to debrief.”
SIMULATION
continued from Page 119
mental models, and learn from both successes and mistakes.
For many educators, this perspective resonated. One participant noted the session was reassuring, particularly for programs with limited resources, demonstrating that simpler approaches can still produce high-quality learning outcomes.
Sustainability and the Hidden Cost of Faculty Time
Dr. Sinewe also addressed a familiar challenge: sustainability. While military programs often invest heavily in equipment and infrastructure, the most critical resource is less visible— faculty time.
“Faculty time is the hidden cost,” he said.
Meaningful simulation requires dedicated preparation, skilled facilitation, and thoughtful debriefing—more than expensive equipment. These are not intuitive skills; they require training, practice, and reflection.
Pulse Points
Key clinical and practice takeaways:
“If we believe simulation matters,” Dr. Sinewe said, “we have to treat it like serious educational work,” including investing in faculty development and protected time.
Clarity Over Complexity
Throughout the session, Dr. Sinewe returned to the principle of clear objectives. High-intensity scenarios have a role, but only when paired with transparent goals and psychological safety. Complexity alone does not produce insight; without structured reflection, even the most sophisticated simulation risks becoming performance rather than learning.
By the end of the session, his central message returned:
“Simulation is an excuse to debrief.”
In an era when simulation is often measured by the fidelity of mannequins or the complexity of scenarios, Dr. Sinewe’s perspective offers a clear reminder: the most impactful simulations are rarely the most elaborate. More often, they are designed with purpose, executed thoughtfully, and followed by intentional reflection
ABOUT THE AUTHORS


Avery Keesee is a medical student at the University of Illinois College of Medicine Rockford.
• Simulation is not the learning—the debrief is. Design sessions with reflection as the primary objective, not the scenario itself.
• Clarity beats complexity: simple, well-structured simulations with clear objectives often outperform high-fidelity, resource-heavy designs.
• Psychological safety is not optional—it is foundational. Without it, debriefing becomes superficial and learning stalls.
• Faculty time is the real investment. Effective simulation depends more on skilled facilitation and preparation than on equipment.
• Treat debriefing as a learned skill: intentional training in facilitation and reflection is essential for meaningful educational impact.
Dr. Stewart is a simulation fellow with the SAEM Simulation Academy and an assistant professor of emergency medicine at Tufts University School of Medicine. She works clinically at Maine Medical Center.
Dr. Rabinowitz is a medical simulation fellow at Northwell Health and a simulation fellow with the SAEM Simulation Academy. She serves as an attending physician in the department of emergency medicine at Long Island Jewish Medical Center.
Dr. Sinewe is a Stanford emergency medicine simulation fellow and a former U.S. Air Force physician who served with ground surgical teams in austere trauma care. He served as an emergency medicine instructor for the ground surgical team austere course at the School of Aerospace Medicine.

Dr. Shin Kim is director of emergency medicine simulation and an assistant professor in the department of emergency medicine at Columbia University Medical Center.
Dr. Moadel is president of the SAEM Simulation Academy and director of the medical simulation fellowship at Northwell Health. She is an assistant professor of emergency medicine at the Zucker School of Medicine at Hofstra/Northwell.
Dr. Bentley is chief wellness officer at Elmhurst Hospital, immediate past president of the SAEM Simulation Academy, and a professor at the Icahn School of Medicine.
SOCIAL EM & POPULATION HEALTH

From Crisis To Connection: Substance Use, Psychosis, and the Emergency Department
By Kyra Benowitz and Heather Henderson, PhD, on behalf of the SAEM Social Emergency Medicine and Population Health Interest Group
At a Glance
• Why this matters now: Cooccurring substance use disorder and psychosis is common, highrisk, and increasingly encountered in the emergency department, with significant implications for mortality and disposition.
• What you’ll learn: A practical framework to differentiate substance-induced versus primary psychosis and apply evidencebased management, harm reduction, and care coordination strategies.
• Who this is for: Emergency physicians and trainees managing acute psychiatric presentations and seeking to improve outcomes for patients with complex comorbidities.
“What I have found difficult is not seeking an escape hatch out of pain, whether that be pills, alcohol, or the dogged pursuit of a cure.”
― Esmé Weijun Wang, The Collected Schizophrenias: Essays Substance use disorder (SUD) is a common and challenging
comorbidity for patients with schizophrenia, with a lifetime prevalence exceeding 40%. This significantly affects morbidity and mortality. Comorbid SUD is associated with a 50% to 100% increased risk of mortality compared with schizophrenia alone, with particularly elevated risks for suicide and other non-natural causes of death.
Individuals with schizophrenia frequently seek out substances in an attempt to self-medicate or, in the words of Esmé Weijun Wang,
“Comorbid substance use disorder is associated with a 50 percent to 100 percent increased risk of mortality compared with schizophrenia alone, with particularly elevated risks for suicide and other non-natural causes of death.”
to find “an escape hatch out of pain.” As emergency physicians, we are often the first—and sometimes most consistent—point of contact offering a different kind of “escape hatch,” one that connects patients to long-term care.
This article reviews key considerations in determining the cause of psychosis in the emergency department, best practices in management, and the role of systemsbased interventions and harm reduction approaches in improving patient outcomes. While stimulants and cannabis are the most common substances associated with druginduced psychosis, specific attention is given to opioid use disorder (OUD) in patients with primary psychotic disorders. Co-occurring OUD worsens clinical outcomes and makes patients significantly less likely to receive standard-of-care addiction treatment
Differentiating Primary Psychosis
From Substance-Induced Psychosis
Distinguishing drug-induced psychosis from primary psychotic disorders in the emergency department is difficult but essential. It can alter acute treatment decisions, influence the likelihood of hospitalization, and shape long-term management.
Currently, no single tool reliably distinguishes substance-induced psychosis from primary psychotic disorders in the emergency department. Collateral history from family members or caregivers is often critical to understanding the onset and progression of symptoms. Evaluation in the emergency department should
focus on determining the most likely cause of psychosis based on available information and is not a substitute for comprehensive psychiatric assessment in a nonemergent setting.
Factors that may suggest substanceinduced psychosis include:
• Temporal relationship to substance use
• Resolution with abstinence (typically within days to weeks)
• Atypical age of onset (older than 35 years)
• Absence of prior independent psychotic episodes
Compared with patients with primary psychotic disorders, those with substance-induced psychosis often demonstrate greater insight, a less florid psychotic features, more depressive symptoms, and increased anxiety. Features more characteristic of primary psychosis include auditory hallucinations, prominent cognitive symptoms, and complex delusions
While overlap is common, recognizing these patterns can support disposition decisions.
Best Practices in the Management of Acute Presentations of Psychosis
The American College of Emergency Physicians recommends against routine laboratory testing in alert patients presenting with acute psychiatric symptoms because of low diagnostic yield.
The American Association of Emergency Psychiatry’s Project BETA (Best Practices in the Evaluation and Treatment of Agitation) provides evidence-based guidance for stabilizing acutely agitated patients. Verbal de-escalation is recommended as the first-line intervention, followed by targeted evaluation to guide pharmacologic management.
continued on Page 125
from Page 123
When psychosis is present, combining parenteral benzodiazepine and haloperidol may achieve more rapid sedation than monotherapy Ketamine may be considered for refractory agitation; however, clinicians should use caution in patients with psychosis or schizophrenia, as ketamine may exacerbate symptoms
Across all approaches, guidelines emphasize a noncoercive, collaborative, and trauma-informed approach to care.
Systems-Based and Harm Reduction Interventions
Systems-based interventions, including screening programs and care coordination models, may be particularly effective for patients with co-occurring SUD and psychosis. Harm reduction strategies, including syringe services programs, can promote treatment engagement and patient autonomy while reducing complications associated with substance use.
Screening, Brief Intervention, and Referral to Treatment (SBIRT) is a widely implemented and scalable approach for identifying SUD in the
Pulse Points
Key clinical and practice takeaways:
emergency department. In a statewide Maryland implementation, problematic substance use was identified in 17.2% of visits, and 38.3% of referred patients successfully engaged in outpatient treatment.
Substance use navigators help address barriers to care by assisting with insurance, transportation, housing, and appointment coordination after discharge. In one implementation across three emergency departments in Alameda County, California, 50.4% of patients who received navigator support engaged in outpatient treatment compared withs 15.9% without navigation
Successful programs require dedicated personnel, strong community partnerships, and systems to track patient engagement.
The BRIDGE Model: Reimagining the ED as an Anchor to Recovery
The University of South Florida and Tampa General Hospital’s BRIDGE program (Building Integrated Recovery for DruG Users Into Emergency Medicine) offers a model for integrating emergency care with longterm recovery.
By pairing immediate buprenorphine initiation with peer recovery specialists, the program positions the emergency department as a critical
• Differentiating substance-induced from primary psychosis is critical in the emergency department, as it directly influences treatment, disposition, and long-term care pathways.
• Avoid reflexive testing—focused history, collateral information, and clinical patterns often provide more diagnostic value than routine laboratory work.
• Start with de-escalation: verbal techniques and a trauma-informed approach remain first-line, with pharmacologic strategies tailored to underlying etiology.
• Leverage the emergency department as a bridge—not a stopgap—by initiating treatment for substance use disorder and connecting patients to follow-up care before discharge.
• Systems matter: navigation programs, harm reduction strategies, and lowbarrier access to treatment significantly improve engagement and outcomes for high-risk patients.
entry point into sustained treatment.
Preliminary observational data show that patients with OUD and co-occurring psychiatric disorders, including schizophrenia, had a 68% follow-up rate for addiction treatment, compared with 51% among those without psychiatric comorbidities When medications for OUD and direct referrals are provided at the point of crisis, patients with co-occurring mental illness appear highly receptive to integrated care pathways.
The BRIDGE analysis highlights the potential of ED-centered, harmreduction-aligned programs to reach populations often viewed as difficult to engage.
Research Imperatives and Key Takeaways
Evidence supporting harm reduction strategies tailored to patients with psychosis remains limited. The exclusion of patients with mental illness from many clinical trials, along with variation in state and local policies governing harm reduction programs, has hindered large-scale research.
Emergency physicians play a critical role in advocating for integrated care models that combine acute stabilization with harm reduction, care coordination, and inclusive research practices. By prioritizing low-barrier access to treatment over rigid abstinence models, the emergency department can shift from a revolving door to a bridge toward recovery and community-based care
ABOUT THE AUTHORS


Kyra Benowitz is a third-year medical student at Touro University California.
Dr. Henderson is an assistant professor in the department of emergency medicine at the University of South Florida and founding director of the social medicine division.
TOXICOLOGY & ADDICTION

From Jet Fuel to Mushrooms: Recognizing GABA Antagonist Toxicity in the Emergency Department
By Kelsey Billups, PharmD and Tiana Patriarca, PharmD, on behalf of the SAEM Academy of Emergency Medicine Pharmacists Toxicology Writing Group
At a Glance
• Why this matters now: Uncommon toxins such as hydrazines, isoniazid and Gyromitra mushrooms can cause rapid, life-threatening seizures through disruption of gamma-aminobutyric acid pathways, requiring immediate recognition and treatment.
• What you’ll learn: A clinically focused overview of mechanisms, exposure sources and high-yield management strategies, including
antidote use with pyridoxine and seizure control in gammaaminobutyric acid antagonist toxicity.
• Who this is for: Emergency physicians, pharmacists, residents and toxicology clinicians managing acute seizures and undifferentiated neurotoxicity in the emergency department.
Gamma-aminobutyric acid (GABA) is the primary inhibitory
neurotransmitter of the central nervous system, acting at GABA receptors to balance excitatory glutamate neurotransmission and maintain normal cognition and behavior.
GABA antagonists inhibit chloride-driven hyperpolarization at GABA-A receptors, leading to neuroexcitation and decreased inhibitory tone. Profound agitation, refractory seizures, and death may result. Because toxicity from these
GABA Synthesis Inhibitors
Mechanism Compound
GAD inhibition
Cyanide, domoic acid (found in amnestic shellfish), hydrazines, isoniazid, 4-methoxypyridoxine from Gingko biloba (Ginkgo toxin)
PK Inhibition Hydrazines, isoniazid
Treatment of Seizures
Pyridoxine 70 mg/kg (max 5 g)
note: 5 grams = 50 x 100 mg/mL vials
Escalation of GABA agonism with benzodiazepines, propofol, and phenobarbital (10-20 mg/kg)
Table 1: Adapted from Curry, Steven C., et al. "Neurotransmitters and Neuromodulators." Goldfrank's Toxicologic Emergencies, 11e Eds. Lewis S. Nelson, et al. McGraw-Hill Education, 2019
agents requires prompt identification, familiarity with their mechanisms, sources and management is critical.
GABA Antagonists
While many compounds directly or indirectly inhibit GABA-A receptors, several compounds alternatively inhibit GABA chloride conductance by impairing GABA synthesis. GABA is synthesized when glutamate is enzymatically converted by glutamic acid decarboxylase, which requires pyridoxal 5’-phosphate (PLP) as a cofactor. PLP is formed from pyridoxine (vitamin B6) by pyridoxine kinase, making this pathway essential for GABA production. Toxins that inhibit either enzyme reduce GABA synthesis and lead to accumulation of excitatory glutamate, further potentiating toxicity.
Hydrazines
Hydrazines reduce PLP and GABA synthesis through inhibition Compounds in this class include hydrazine, monomethylhydrazine, 1,1-dimethylhydrazine and 1,2-dimethylhydrazine. In addition to inhibiting GABA synthesis, hydrazines are highly reactive alkalis with significant flammability and corrosive risks. Because they are readily combustible, these agents are commonly found in jet fuels and aerospace settings.
Jet Fuels
Acute toxic exposures to hydrazinecontaining fuels and industrial chemicals are rare. Most reported exposures are inhalation or dermal and result in mild to moderate respiratory symptoms and skin findings related to their caustic properties Despite predominantly localized effects, systemic neurotoxicity has been reported.
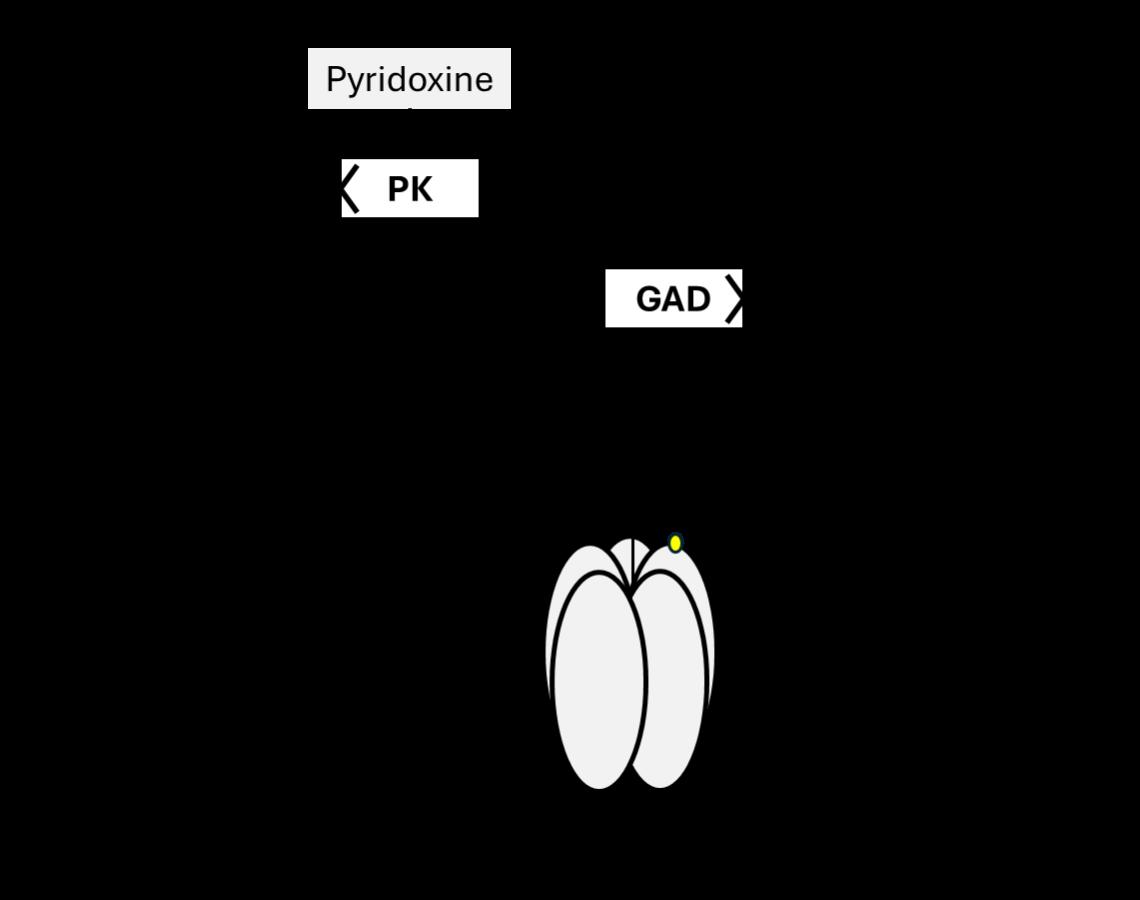
Figure 1: GABA Synthesis Inhibitors.
*Inhibition of pyridoxine kinase is the primary inhibitory mechanism of hydrazine and isoniazid. INH: isoniazid, PK: pyridoxine kinase, GAD: glutamic acid decarboxylase, GABA: gamma-aminobutyric acid, Cl-: chloride ion. Adapted from Curry, Steven C., et al. "Neurotransmitters and Neuromodulators." Goldfrank's Toxicologic Emergencies, 11e Eds. Lewis S. Nelson, et al. McGraw Hill Education, 2019
In two cases, exposure to a hydrazine-methylhydrazine mixture resulted in twitching, hyperreflexia and clonic movements, with rapid improvement after pyridoxine, steroid and bronchodilator therapy. In another case, ingestion of a cup of liquid hydrazine led to loss of consciousness, agitation, ataxia, nystagmus and seizures.
Hydrazines are also associated with pulmonary edema, methemoglobinemia and hepatotoxicity. Transient liver function test elevations have been reported even in isolated inhalation exposures.
Gyromitra Mushrooms
Beyond industrial sources, hydrazines are found in nature, most notably in Gyromitra mushrooms. Often mistaken for Morchella (true morels), Gyromitra species are commonly referred to as “false morels” and have epileptogenic potential due to hepatic conversion of gyromitrin to monomethylhydrazine.
Poisoning from misidentification may initially cause gastrointestinal symptoms, including abdominal pain,
continued on Page 129

vomiting and diarrhea. These are followed by neurologic effects such as dizziness, ataxia, tremor and central nervous system depression.
In a review of 201 Gyromitra ingestions, seizures occurred in 14.1% of cases, and patients with seizures had an 82.1% mortality rate. Hepatotoxicity developed in 53.3% of exposures.
Isoniazid
Isoniazid, a potent antitubercular agent, is structurally similar to hydrazines and chemically classified as isonicotinic acid hydrazide. Toxicity resembles that of other hydrazine compounds, and exposures are well documented.
Seizures from acute isoniazid toxicity can occur with doses as low as 20 mg/kg. Isoniazid also inhibits conversion of lactate to pyruvate, resulting in refractory metabolic acidosis.
Treatment Considerations for Hydrazine Toxicity
In inhalation or dermal exposures, management begins in the prehospital setting. Decontamination should be performed once emergency medical services personnel are able to don appropriate personal protective
Pulse Points
Key clinical and practice takeaways:
equipment. Clothing should be removed, visible liquid blotted away and skin irrigated with water.
Due to fire risk, oxygen should be administered only after decontamination. Ventilation using a bag-valve mask may be performed prior to decontamination if needed. If bronchospasm occurs, a beta agonist such as albuterol may be nebulized.
In cases of isoniazid or Gyromitra ingestion, activated charcoal use is controversial because of the risk of seizure and aspiration.
Neurologic symptoms, including agitation and seizures, result from impaired GABA synthesis. Highdose GABA agonists such as benzodiazepines (midazolam 10 mg, lorazepam 4 to 8 mg, diazepam 5 to 10 mg) and/or phenobarbital 10 to 20 mg/kg may be used initially to terminate seizures.
Pyridoxine ( vitamin B6) is the antidote for hydrazine and related toxicities. It is converted to PLP, a cofactor in multiple amino acid metabolic pathways, including GABA synthesis. Pyridoxine is not proteinbound in plasma and readily crosses cell membranes.
This antidote is used to terminate seizures, correct metabolic acidosis, and improve central nervous system depression. The role of prophylactic pyridoxine after hydrazine exposure
• Consider gamma-aminobutyric acid antagonist toxicity in any patient with refractory seizures—especially when the cause is unclear or response to standard therapy is limited.
• Exposure history matters: ask about industrial settings, fuel contact and foraged mushroom ingestion to uncover uncommon but high-risk toxicities.
• Pyridoxine is a time-sensitive antidote—early administration can rapidly reverse seizures and metabolic derangements in hydrazine and isoniazid toxicity.
• Seizure control requires escalation: high-dose benzodiazepines and phenobarbital may be necessary due to impaired gamma-aminobutyric acid synthesis.
• Not all “benign” exposures are low risk—dermal or inhalational contact with hydrazines can still lead to systemic toxicity and delayed neurologic effects.
remains unclear but is often considered after large isoniazid ingestions, particularly when presentation occurs within six hours.
Dosing varies by exposure. After hydrazine-containing aircraft propellant exposure, prehospital guidelines recommend pyridoxine 70 mg/kg (maximum 5 g). For Gyromitra toxicity, 25 mg/kg (maximum 5 g) may be used if supportive care is insufficient. In isoniazid overdose, if the ingested amount is known, pyridoxine should be administered in a 1:1 mg ratio. If unknown, a dose of 5 g in adults or 70 mg/kg (maximum 5 g) in children is recommended.
Pyridoxine should be administered intravenously at a rate of up to 1 g per minute and may be repeated every 15 to 20 minutes until seizure activity resolves. When used for seizure activity, benzodiazepines should be given concurrently to enhance GABA neurotransmission.
Pyridoxine is generally well tolerated. However, adverse effects such as ataxia, peripheral neuropathy, and seizures have been reported with chronic use or extremely high doses exceeding 2 g/kg.
Following isoniazid-induced seizures, pyridoxine should be administered as soon as possible. An emergency supply of 5 to 10 g, and possibly up to 20 g, should be readily available to avoid treatment delays. Hemodialysis may be considered in cases of isoniazid toxicity refractory to pyridoxine and anticonvulsants
ABOUT THE AUTHORS


Dr. Billups is an emergency medicine pharmacy specialist at the Medical University of South Carolina in Charleston, South Carolina.
Dr. Patriarca is a clinical toxicology fellow at the Alabama Poison Information Center in Birmingham, Alabama.

Beyond Oxygen: Evolving Management of Carbon Monoxide and Cyanide Poisoning
By Jordan A. Woolum, PharmD and Peter Tran, PharmD
At a Glance
• Why this matters now: Inhalational injuries from fires continue to drive preventable morbidity and mortality, with carbon monoxide and cyanide acting as key, often underrecognized contributors.
• What you’ll learn: A clinically focused update on evolving management strategies, including hyperbaric oxygen controversies, adjunctive therapies, and emerging antidotes for cyanide toxicity.
• Who this is for: Emergency physicians, trainees, and pharmacists managing toxicologic and inhalational exposures in acute care settings.
Introduction
Inhalational injuries from fire-related events resulted in an estimated 3,800 deaths in 2021, equating to one death every two hours and 17 minutes. These injuries and fatalities result from a complex mixture of heated air, particles, and chemicals, the composition of which depends on the source of the fire and fumes.
General care strategies for patients with inhalational injury include standard supportive measures such as removal from the source, external decontamination, and administration of oxygen. Despite advancements in supportive care, significant morbidity and mortality persist,
likely attributable to the chemical asphyxiants carbon monoxide and cyanide. Although existing treatments improve outcomes, gaps remain. Here, we describe recent advancements in the management of these exposures, with a focus on novel therapeutic strategies.
Carbon Monoxide
Carbon monoxide (CO) is an odorless, colorless gas formed during the partial combustion of carbon-containing compounds. Acute fatalities from CO exposure are primarily due to a leftward shift in the oxygen-hemoglobin dissociation curve, which increases oxygen’s affinity for hemoglobin
and decreases its release to tissues. Additional mechanisms include impairment of oxidative phosphorylation and subsequent cardiodepressant and arrhythmogenic sequelae.
Less appreciated are the longterm cognitive, vestibular, and motor impairments that survivors may experience. The pathophysiology is thought to involve lipid peroxidation in specific regions of the brain.
Acute Management
Acute management of CO exposure consists of administering 100 percent oxygen via nonrebreather mask or endotracheal tube. This reduces the half-life of carboxyhemoglobin from approximately five hours on room air to about one hour at one atmosphere.
For select patients (Table 1), hyperbaric oxygen (HBO) therapy has been recommended. HBO further reduces the halflife of carboxyhemoglobin to approximately 20 minutes and may mitigate brain lipid peroxidation, ischemia-reperfusion injury, and the development of delayed neurocognitive sequelae (DNS), including amnesia, dementia, apraxia, agnosia, and peripheral neuropathies.
Syncope
Coma
Seizure
Altered mental status or confusion
Carboxyhemoglobin ≥ 25%
Vestibular abnormalities
Pregnancy +
Carboxyhemoglobin ≥ 15%
Fetal distress
Table 1: Indications for Hyperbaric Oxygen
Hyperbaric Oxygen: Ongoing Debate
Evidence supporting HBO therapy remains mixed. Animal studies and some randomized trials suggest benefit, but human data are inconsistent. Critics argue that observational studies demonstrating benefit are subject to selection bias
and that randomized controlled trials showing improved outcomes have notable methodological flaws. Despite these concerns, efforts continue to optimize HBO delivery given its cost and logistical burden. A recent randomized, double-blind, sham-controlled trial evaluated whether a single HBO session provides outcomes comparable to the traditional three-session protocol.
Seventy-two patients were randomized to either a single-session group (n = 35) or a three-session group (n = 37). No differences in cognitive impairment were observed at six weeks (50 percent vs 55 percent, p = 0.8) or six months (42 percent vs 46 percent, p = 0.76). Safety events were similar between groups and primarily included mild ear barotrauma (34 percent vs 41 percent).
The trial was stopped early due to slow enrollment. Limitations included insufficient statistical power, exclusion of severely poisoned patients, and exclusion of intentional exposures and smoke inhalation cases. Despite these limitations, the findings suggest that three-session HBO therapy may not be superior to a single session for patients with mild CO poisoning.
Adjunctive and Emerging Therapies
HBO is not the only modality under investigation for reducing DNS. Animal studies and case reports suggest that corticosteroids may attenuate neuroinflammation and reduce the incidence of DNS.
A retrospective registry study evaluated dexamethasone in addition to standard supportive care. Patients receiving dexamethasone (n = 99) at 10 mg IV every 24 hours for three doses were compared with a standard care group (n = 29). Dexamethasone use was associated with a lower rate of DNS (OR = 0.122, 95 percent CI 0.031–0.489).
Limitations include the retrospective design, unequal group sizes, and a higher proportion of intentional CO exposures in the treatment group
(78.1 percent). No significant safety concerns were identified. Given its availability and the underlying pathophysiology of CO injury, dexamethasone may be considered as a potential adjunct, particularly in resource-limited settings.
Cyanide
Hydrogen cyanide is a lethal toxin produced during residential and industrial fires through the combustion of materials such as silk, plastics, and wool. Cyanide binds to ferric iron in cytochrome c oxidase, leading to rapid cellular asphyxiation.
Hydroxocobalamin is a commonly used antidote for cyanide toxicity. However, recent wildfires and sterility concerns have contributed to supply shortages which may persist given the single-source manufacturing of this medication. These shortages, along with the requirement for intravenous access, have prompted interest in alternative therapies and renewed evaluation of historical treatments.
Traditional Antidotes
Traditional cyanide kits include amyl nitrite, sodium nitrite, and sodium thiosulfate, two of which require intravenous access. Amyl nitrite and sodium nitrite induce methemoglobinemia, increasing cyanide binding and drawing it away from tissues. However, they also reduce oxygen-carrying capacity and may cause hypotension, which can be detrimental in patients with smoke inhalation.
Sodium thiosulfate acts synergistically by providing sulfur groups to the enzyme rhodanese, facilitating conversion of cyanide to thiocyanate. Its use is limited by a relatively delayed onset of action.
Emerging Antidotes
Given the limitations and availability concerns of existing therapies, several alternative agents are under investigation.
Cobinamide, a precursor to cobalamin, contains two ligandbinding sites compared with one in cobalamin, allowing for greater
on Page 133
Table 2: Past, Present, and Future Cyanide IT: Intratracheal, INH: Inhalation. ¥: Potential utility

Cobinamide¥
Dicobalt Edetate Hydroxocobalamin¥
Amyl Nitrite
Sodium Nitrite¥
Dimethyl Trisulfide
Sodium Tetrathionate
Sodium Thiosulfate
Direct binding
Direct binding
Methemoglobin formation
Methemoglobin formation
Sulfur
Cyanide Antidotes utility in hydrogen sulfide poisoning
Hypertension
Hypotension
Arrythmia
Dextrose coadministration
Requires reconstitution
Hypertension
Lab disturbances
Oxalate nephropathy
Requires reconstitution
Hypotension
Abuse potential
Pulse Points
Key clinical and practice takeaways:
• High-flow oxygen remains the cornerstone of carbon monoxide management—early, aggressive administration reduces carboxyhemoglobin half-life and tissue hypoxia.
• Hyperbaric oxygen therapy remains controversial—current evidence suggests no clear advantage of multiple sessions over a single session in mild poisoning.
• Consider dexamethasone as a potential adjunct in select patients—emerging data suggest a role in reducing delayed neurocognitive sequelae, though evidence is limited.
TOXICOLOGY
continued from Page 131
cyanide-binding capacity. It is also more water soluble, enabling higherconcentration formulations suitable for intramuscular administration.
Sulfur donor agents such as sodium tetrathionate and dimethyl trisulfide (DMTS) function similarly to sodium thiosulfate but provide additional sulfur moieties. Preclinical studies have not fully evaluated their use alongside methemoglobin inducers, and concerns remain regarding potential reductions in oxygencarrying capacity.
Sodium tetrathionate carries risks of renal toxicity and formulation instability. Reformulated DMTS has demonstrated improved bioavailability and stability, allowing for lowervolume intramuscular administration. While these agents offer potential advantages, including alternative routes of administration, further research is needed to establish their safety, efficacy, and clinical role.
Conclusion
Inhalational injuries continue to impose a significant global burden. Emerging strategies for carbon monoxide poisoning and novel antidotes for cyanide toxicity have the potential to improve outcomes. Continued research and thoughtful integration of these therapies into clinical practice will be essential to advancing care in this high-risk population
ABOUT THE AUTHORS

Dr. Tran is an emergency medicine pharmacist at Ochsner LSU Health Shreveport.
Dr. Woolum is an emergency medicine pharmacist and clinical toxicologist at UK HealthCare in Lexington, Kentucky. Mechanism of
• Cyanide toxicity may be underrecognized in fire victims—maintain a high index of suspicion, especially in patients with severe lactic acidosis or altered mental status.
• Emerging antidotes such as cobinamide and dimethyl trisulfide may expand future treatment options, particularly in settings with limited intravenous access or antidote shortages.

TOXICOLOGY & ADDICTION MEDICINE

Dose Over Definition: Understanding Pediatric Risk in a Changing Cannabis Market
By Irene Morcuende Gonzalez, MD, and Richard J Hamilton, MD, MBA on behalf of the SAEM Pediatric Emergency Medicine Interest Group
At a Glance
• Why this matters now: Pediatric cannabis ingestions are rising rapidly with legalization and the spread of hemp-derived products that can contain high doses despite appearing “legal.”
• What you’ll learn: A practical, weight-based (milligrams per kilogram) framework to assess risk, anticipate toxicity and navigate increasingly complex product exposures.
• Who this is for: Emergency physicians, trainees and clinicians managing pediatric ingestions in
an evolving and often misleading cannabinoid landscape.
Unintentional cannabis ingestion in children has increased dramatically over the past decade, paralleling legalization and commercialization of cannabis products. Pediatric exposures reported to U.S. poison centers have risen substantially following recreational legalization in multiple states, with the majority occurring in children younger than 6 years. Edible products account for most severe cases.
More recently, hemp-derived intoxicating cannabinoids — enabled
by provisions within the Agriculture Improvement Act of 2018 (the “2018 Farm Bill”) — have expanded access to psychoactive products outside regulated dispensary systems and across state lines. This evolving marketplace complicates dose estimation, product identification, and toxicity prediction in the emergency department (ED), particularly in children
Cannabis 101: Clarifying Terminology
• Cannabis refers to the plant genus Cannabis sativa L., which includes both hemp and marijuana varieties.
“Because legality hinges on delta-9-tetrahydrocannabinol percentage—not total milligrams—single edible products can legally contain toxic doses for children.”
• Hemp is federally defined as cannabis containing less than 0.3% Δ9-tetrahydrocannabinol (Δ9-THC) by dry weight prior to harvest. It may contain cannabidiol (CBD), a nonintoxicating cannabinoid.
• Marijuana refers to cannabis containing more than 0.3% Δ9-THC by dry weight and remains federally classified as a Schedule I substance under the Controlled Substances Act, though state laws vary.
Before 2018, federal law did not distinguish hemp from marijuana; all Cannabis sativa plants were treated as Schedule I substances. The 2018 Farm Bill legalized hemp at the federal level, provided Δ9-THC concentration remains below 0.3% by dry weight at harvest.
Critically, this definition is based on percentage by dry weight—not total milligrams in a finished product. That distinction created a regulatory gap, allowing highly concentrated, psychoactive consumer products to remain federally lawful if they technically meet the dry-weight threshold.
Δ9-THC Dosing in Children
For emergency clinicians, one principle remains central: dose per kilogram predicts severity.
Children are uniquely vulnerable to large, unintentional ingestions. A single adult edible gummy may contain 5–10 mg of Δ9-THC. Products containing well over 100 mg total THC are not uncommon in unregulated markets.
Pediatric cohort studies demonstrate that higher mg/kg ingestion correlates with more severe toxicity, including prolonged central

nervous system (CNS) depression and respiratory compromise. When history is reliable, a threshold of 1.7 mg/kg or greater of Δ9-THC is associated with increased risk of severe and prolonged toxicity. Furthermore, ingestions greater than 3 mg/kg are known to cause seizures, bradycardia, and hypotension.
The 2018 Farm Bill Loophole: Why “Legal” Does Not Mean “Low Dose”
Under the 2018 Farm Bill, hemp must contain less than 0.3% Δ9-THC by dry weight. After harvest, however, oversight shifts away from USDA regulation, and finished products are governed inconsistently across states.
Because legality hinges on Δ9-THC percentage—not total milligrams— single edible products can legally contain toxic doses for children. A standard 60-gram chocolate bar labeled as containing 30 mg THC would legally be considered hemp by dry weight but represent a severe exposure in a toddler. In many cases, these products resemble common
candies or baked goods, increasing pediatric appeal and risk of large ingestion.
The Cannabinoid Expansion
A second regulatory gap involves cannabinoids derived from CBD. While Δ9-THC concentration is limited by federal definition, manufacturers have modified CBD into psychoactive compounds such as Δ8-tetrahydrocannabinol (Δ8THC), hexahydrocannabinol (HHC), tetrahydrocannabinol-O-acetate (THC-O), tetrahydrocannabiphorol (THCP), tetrahydrocannabivarin (THCV), among others. Some preliminary laboratory data suggest certain compounds may have higher CB1 receptor binding affinity than Δ9-THC, raising theoretical concerns about enhanced potency. There are currently no human pediatric data defining mg/kg toxicity thresholds for these compounds.
Additional clinical challenges include:
continued on Page 137

• Variable cannabinoid composition
• Inconsistent product labeling
• Unpredictable drug screen results
• Uncertain pharmacokinetics
• Potential co-formulated contaminants
For the emergency clinician, this translates to increased uncertainty in risk stratification.
Emerging Federal Legal Changes
Federal lawmakers have recently moved to address regulatory gaps created by the 2018 Farm Bill. In November 2025, Congress passed legislation redefining hemp, with implementation expected in November 2026.
Major changes:
• Total THC limit: Hemp must contain 0.3% or less total THC (including THCA) by dry weight.
• Product potency cap: Finished products are limited to 0.4 mg total THC per container, which industry analysts say could eliminate more than 95% of current hemp-derived products.
• Synthesized cannabinoid ban: Cannabinoids created outside the plant (e.g., Δ8-THC) are no longer considered legal hemp.
Pulse Points
Key clinical and practice takeaways:
• Implementation timeline: The rules take effect Nov. 12, 2026, after a one-year transition period.
The 2025 funding law drastically restricts intoxicating hemp products by redefining hemp and imposing strict THC limits. However, multiple bills in 2026 are attempting to delay, repeal or replace those rules before they take effect.
Back to the ED: A Practical Bedside Approach
1. Calculate mg/kg whenever possible. Document total labeled milligrams and estimated amount consumed. Dose per kilogram remains the most reliable predictor of severe toxicity in children, particularly those younger than 6 years. Children younger than 3 years are especially prone to respiratory depression.
2. Use 1.7 mg/kg or greater Δ9-THC as a high-risk threshold. Children exceeding this exposure merit prolonged observation and management in a setting with pediatric capability. Higher exposures (3 to 5 mg/kg or greater) may require ICU monitoring.
3. Expect prolonged sedation. While inhalational use of cannabis results in immediate CNS effects and self-regulation of dose, edible exposures may result in delayed
• Dose—not legality—drives risk: calculate milligrams per kilogram whenever possible, as even “legal” products may contain toxic exposures for children.
• Edibles are high risk: delayed onset and high total tetrahydrocannabinol content increase the likelihood of prolonged central nervous system depression and respiratory compromise.
• “Hemp-derived” does not mean safe: products meeting federal definitions can still contain clinically significant psychoactive doses.
• Expect uncertainty: variable labeling, novel cannabinoids and inconsistent drug screens make risk stratification more challenging than traditional cannabis exposures.
• Use thresholds to guide care: exposures of 1.7 milligrams per kilogram or greater warrant close observation, while higher doses may require escalation to intensive monitoring.
peak effects and prolonged CNS depression.
4. Consider activating your child protection team and provide caregiver education. This is particularly important in children younger than 5 years. Clear discharge counseling should include:
o “Hemp-derived” does not mean nonintoxicating.
o Δ9-THC less than 0.3% by dry weight does not mean low total dose.
o CBD-labeled products may contain psychoactive or synthesized cannabinoids.
o All cannabis products should be stored locked and out of reach.
Conclusion
The pediatric cannabis exposure landscape is evolving rapidly. Legal definitions based on percentage rather than total milligrams have enabled high-dose edible products to proliferate, while synthetic cannabinoid derivatives further complicate toxicity prediction.
For academic emergency clinicians, the bedside framework remains grounded in fundamentals: calculate mg/kg, anticipate prolonged CNS depression and determine disposition based on weight-based dose and clinical trajectory.
In a marketplace defined by regulatory nuance and product variability, dose—not legality—predicts pediatric risk
ABOUT THE AUTHORS


Dr. Morcuende Gonzalez is a pediatric emergency medicine fellow at St. Christopher’s Hospital for Children in Philadelphia.
Dr. Hamilton is chair of emergency medicine and a medical toxicologist at Drexel University College of Medicine. He is executive medical director of pediatric emergency medicine at St. Christopher’s Hospital for Children.
TRAINING TOOLKIT

Navigating the Emergency Medicine Match: What Applicants Need to Know
By Eileen Williams, MD; Mel Ebeling, MD; and Anita Goel, MD
Amid the ever-changing landscape of emergency medicine, another Match Day has come and gone. Students submitted their rank lists without knowing if or when residency programs will be required to expand to a four-year format, how to best use new features such as geographic preference signaling, or what new board certification exams will mean for them. Across the board, uncertainty remains a major source of stress.
Traditionally, strong grades and a high Step 1 score provided clear metrics for programs to evaluate applicants. With Step 1 now pass/fail
and many schools moving toward competency-based or narrative evaluations instead of class rank or honors grades, students often feel unsure how to demonstrate competitiveness. Add ongoing questions about away rotations— with some programs limiting them or shifting expectations post-pandemic—and many are left wondering: How do I stand out?
Away Rotations
Q: Should I even bother doing away rotations anymore? Are they worth it?
A: In the past, students were often expected to complete as many as two away rotations. Now, as third-
year students approach application season, decisions about away rotations feel more complex. Some view them as an opportunity to gain visibility, especially without a home EM program. Others question whether one or two rotations justify the stress, cost, and logistics of relocating.
Programs vary widely. Some treat away rotations as essential “auditions,” while others emphasize holistic review.
• If you have a home EM program: One away rotation is usually sufficient to gain exposure and secure a strong SLOE.

“Across the board, uncertainty remains a major source of stress.”
• If you do not have a home EM program: Two away rotations are often recommended to demonstrate interest and obtain letters, but prioritize quality over quantity.
• General guidance: Choose rotations strategically. Select programs that align with your goals or offer strong mentorship opportunities. Avoid completing multiple away rotations solely to “check boxes.”
Q: Does it matter where I do my away rotation?
A: In most cases, yes—for several reasons. First, it is important to rotate at an institution that regularly hosts visiting students, as the number of learners evaluated annually is included in your SLOE. Programs that assess many students can typically provide more reliable comparisons than those that rarely evaluate learners.
Second, geographic choice can help “unlock” other regions of the country. Rotating in a different area signals openness to relocating and can demonstrate genuine interest in programs outside your home region. For students hoping to move across the country without existing ties, this can be a meaningful way to show commitment.
Competitiveness in a Changing Landscape
Q: If Step 1 is pass/fail and grades are less emphasized, how do I stand out?
A: Students are increasingly focusing on several key areas:
1. Step 2 CK: Now the primary numerical benchmark, making timing and preparation critical decisions.
2. Research and Scholarship: A visible way to demonstrate interest, especially without a home EM program. This may include clinical research, simulation, or medical education work.
3. Leadership and Extracurricular Involvement: EM interest groups, quality improvement projects, teaching, and community service can demonstrate initiative and teamwork.
4. Strong SLOEs: Standardized letters of evaluation from EM faculty remain essential, particularly when written by individuals who know you well.
Despite these strategies, many applicants still struggle with
“Competitiveness is increasingly defined by presenting a well-rounded application rather than meeting a single numeric benchmark.”
TRAINING TOOLKIT
continued from Page 139
comparability, given the variability in narrative evaluations and competency-based assessments across institutions. Competitiveness is increasingly defined by presenting a well-rounded application rather than meeting a single numeric benchmark.
Letters of Recommendation and Networking Pressures
Q: How can I get SLOEs if I do not have a home EM program?
A: Securing meaningful, personalized SLOEs requires initiative and often depends on identifying mentors willing to write detailed, specialtyspecific letters. Students without a home program may face challenges due to fewer built-in connections and limited opportunities for longitudinal mentorship.
For these applicants, away rotations often become the primary avenue for building relationships with EM
Pulse Points
Key clinical and practice takeaways:
faculty. It can also be helpful to proactively connect through national organizations such as SAEM, which offer mentorship opportunities and networking resources.
Student Mental Health and WellBeing
Q: Beyond academics and metrics, how can I stay grounded during the application process?
A: The application cycle carries a significant emotional burden. Stressors may include:
• The risk of burnout during a prolonged cycle of applications, away rotations, board preparation, and interviews.
• Comparison with peers, often amplified by curated social media portrayals.
• Imposter syndrome, especially when evaluation criteria feel unclear or constantly shifting.
To address these concerns, students frequently seek greater
• Away rotations still matter—but strategy matters more than volume. Choose programs that align with your goals and offer meaningful evaluation.
• Standardized letters of evaluation remain essential. Prioritize building relationships with faculty who can write detailed, specialty-specific letters.
• Competitiveness has shifted. With Step 1 pass/fail, Step 2 Clinical Knowledge, leadership, and a well-rounded application carry more weight.
• Lack of a home emergency medicine program is a challenge—but not a barrier. Use away rotations and national organizations to build mentorship and visibility.
• The process is inherently stressful. Proactively managing comparison, uncertainty, and burnout is as important as strengthening your application.
transparency from programs regarding evaluation processes and expectations. Clear guidance on away rotations, Step 2 CK weighting, and interpretation of narrative evaluations can help reduce uncertainty. Equally important is reassurance that holistic review is applied consistently and meaningfully.
Conclusion
The EM Match continues to evolve, and applicants are navigating that change in real time. Clear communication, standardized expectations, and greater transparency in application review would go a long way toward reducing stress. In the meantime, students are working to balance performance with well-being, hoping their individual strengths and authentic motivations stand out in a system still adapting to modern assessment practices.
ABOUT THE AUTHORS

Eileen Williams is a third-year emergency medicine resident and incoming medical education fellow at the University of Texas Southwestern. She earned her undergraduate degree from Stanford University and her medical degree from Baylor College of Medicine in Houston, Texas.


Dr. Ebeling is a resident physician at the University of Cincinnati and a board member-at-large for SAEM Residents and Medical Students.
Dr. Goel is an associate professor of emergency medicine at the University of Cincinnati. She directs longitudinal programs for medical students in emergency medicine and leads a section of the transitions to residency course.

Desmopressin in Traumatic Intracranial Hemorrhage: Don’t PATCH the Leak— Dose Matters
By Aubrey Evers, PharmD; Zachary Senger, PharmD; and Justin Reinert, PharmD, MBA
At a Glance
• Why this matters now:
Antiplatelet-associated intracranial hemorrhage remains a high-risk, time-sensitive emergency where optimal reversal strategies are still evolving.
• What you’ll learn: How desmopressin works, what the evidence shows, and why weight-based dosing may be more effective than fixed-dose approaches.
• Who this is for: Emergency physicians, pharmacists, and trainees making real-time decisions about bleeding management in intracranial hemorrhage.
Background
Traumatic intracranial hemorrhage (ICH) remains one of the most timesensitive and high-stakes conditions in emergency care. For patients taking antiplatelet therapy, even brief delays in achieving hemostasis
can lead to hematoma expansion, neurologic deterioration, and longterm disability. Limiting bleeding is associated with improved survival and functional outcomes
Platelet transfusion was historically considered a firstline intervention for antiplateletassociated bleeding. However, the PATCH trial challenged this approach, demonstrating increased mortality and worse functional outcomes among patients receiving
“Traumatic intracranial hemorrhage remains one of the most time-sensitive and high-stakes conditions in emergency care.”
platelet transfusion for spontaneous intracerebral hemorrhage (odds ratio, 2.05; 95% CI, 1.18–3.56), without reducing hematoma expansion. These findings shifted practice away from transfusion and toward pharmacologic strategies such as desmopressin.
Desmopressin (DDAVP) increases circulating von Willebrand factor and factor VIII and enhances platelet adhesion, providing a mechanistic rationale for reversing antiplateletassociated bleeding. Current Neurocritical Care Society guidelines recommend considering a single dose in patients with ICH receiving antiplatelet therapy, although this recommendation is based on limited observational data.
Review of Evidence
What Does the Evidence Show?
Key findings are summarized in Table 1.
Early observational studies demonstrated biologic plausibility. In a prospective study, Naidech et al. found that 14 patients with aspirin-associated ICH who received desmopressin 0.4 mcg/ kg had significant improvement in platelet function within one hour, along with increased von Willebrand factor activity. Similarly, Kapapa et al. observed normalization of platelet function within 30 minutes after a fixed 24 mcg dose, with effects diminishing by three hours— highlighting the drug’s transient action.
Subsequent studies explored clinical outcomes with mixed results. Feldman et al., in a retrospective cohort of 124 patients, found that desmopressin (mean dose, 0.34 mcg/ kg) was associated with a lower rate of hematoma expansion (10.9% vs

36.2%; P = 0.002; OR, 0.22; 95% CI, 0.08–0.57), without increased adverse events.
In contrast, McManus et al. reported no difference in hematoma expansion or clinical outcomes in a propensitymatched cohort of patients with nontraumatic ICH. Rech et al. similarly found no difference in hemostatic efficacy despite greater baseline severity in treated patients.
Randomized data remain limited. The phase 2 DASH trial evaluated a fixed 20 mcg dose versus placebo in 54 patients with antiplateletassociated ICH. Hematoma expansion rates were similar between groups,
and although fewer patients receiving desmopressin had poor functional outcomes at 90 days, the study was not powered for efficacy. The use of fixed dosing may have contributed to the lack of observed benefit.
Dosing Strategy and Pharmacologic Considerations
Available evidence supports weightbased dosing in the range of 0.3–0.4 mcg/kg as the most consistent approach. Fixed-dose regimens may lead to underdosing in larger patients and variable pharmacologic effects.
continued on Page 145
Author/ year Study Design
Naidech et al. 2014 Prospective Observational 14 patients; all received DDAVP ASA or reduced platelet
Kapapa et al. 2014 Prospective Observational 13 patients; all
Feldman et al., 2019
Retrospective Cohort 124 patients; 55 DDAVP
McManus et al., 2022
Retrospective Cohort
156 patients; 49 DDAVP
18.5% DAPT
1 patient = ASA + dipyridamole
12.25 hours (5.7-23.1)
Outcomes
Platelet Function Analyzerepinephrine decreased from 192±18 to 124±15 seconds (P=0.01) vWF antigen increased from 242±96% to 289±103% activity (P=0.004)
Platelet function returned to normal 30 minutes after administration of desmopressin acetate. Platelet function worsened again after three hours
Desborough et al. 2023
Phase 2 RCT
Rech et al. 2025
Retrospective Cohort
Table 1: Summary of Studies
54 patients; 27 DDVAP
1 patient = DAPT 0.34 ± 0.1 mcg/kg 3.2 hours after injury (median), 7 hours after hospital triage
93.6% ASA 18.6%
Clopidogrel
1 patient = ticagrelor
1 patient = dipyrimadole
14.7% DAPT
46% ASA 43% Clopidogrel 9% ASA + Clopidogrel
0.3-0.4mcg/kg +/- 10%
1 patient = ASA + dipyridamole 20 mcg
Median of 3.9 hours [3.7-4.5]
10.9% vs 36.2% hematoma expansion >3 mL (p = 0.002, OR = 0.22 (0.08-0.57). No difference in mRS
Hospice/inpatient mortality (16.2% vs 29%, p=0.13) No difference in reduced hematoma expansion (11.8% vs 11.1%, p = 0.99) and appeared to be safe
Within 24 hours of symptom onset
21% vs 23% hematoma expansion
22.2% vs 37% mRS >4 at 90 days OR 0·74 (0·29–1·93)
324 patients; 45 DDAVP
100% of DDAVP patients on ASA; 5 patients on DAPT with clopidogrel
0.3 mcg/kg (0.30.4) 163 minutes
74.3% vs 85% good or excellent hemostatic efficacy -10.7% (-28.1% to 6.7%)
No difference in change of hematoma volume
“Weight-based dosing in the range of 0.3 to 0.4 micrograms per kilogram is the most supported strategy, while fixed-dose regimens may lead to inconsistent pharmacologic effects.”
continued from Page 143
A key limitation of desmopressin is its short duration of action, typically 75 minutes to three hours. Platelet function may normalize quickly after administration but decline within hours, raising concern that a single dose may be insufficient in ongoing bleeding.
Despite this, guidelines recommend a single dose due to the absence of evidence supporting repeat dosing. While repeat administration may be reasonable in select high-risk patients, such as those with expanding hematomas or exposure to potent antiplatelet agents, this strategy remains unstudied in prospective trials.
Safety and Limitations of the Evidence
Safety data are generally reassuring. Multiple studies report low rates of thrombotic events and no significant
Pulse Points
Key clinical and practice takeaways:
differences in adverse outcomes compared with control groups. Hyponatremia and fluid retention remain theoretical concerns, particularly with repeated dosing, due to the drug’s antidiuretic effects.
Important limitations persist across the literature. Most studies include predominantly aspirin-exposed patients, with limited representation of P2Y12 inhibitors or dual antiplatelet therapy. In addition, many cohorts combine spontaneous and traumatic intracranial hemorrhages, which differ in pathophysiology and clinical course. These factors limit generalizability and complicate interpretation of treatment effects.
Clinical Takeaways for Emergency Practice
For emergency clinicians, several practical points emerge:
• Desmopressin is a reasonable, guideline-supported option for antiplatelet-associated bleeding in traumatic ICH.
• Weight-based dosing (0.3–0.4 mcg/ kg) is the most supported strategy.
• Early administration is likely important given the time-dependent nature of hematoma expansion.
• The effect is transient; clinicians should anticipate potential waning activity.
• Repeat dosing remains investigational and should be considered cautiously.
Conclusions
Desmopressin is a biologically plausible and low-risk intervention for antiplatelet-associated bleeding in traumatic ICH. While definitive evidence is lacking, current data support early, weight-based dosing as the most rational approach. Ongoing trials, including DASH-2, are expected to clarify optimal dosing strategies and clinical impact
ABOUT THE AUTHORS

Dr. Evers is a pharmacy resident at Corewell Health William Beaumont University Hospital.
• Desmopressin is a reasonable first-line adjunct for antiplatelet-associated intracranial hemorrhage—but the evidence remains mixed and largely observational.
• Dose matters: weight-based dosing (0.3–0.4 micrograms per kilogram) is more consistent than fixed dosing and may reduce hematoma expansion.
• Time is critical—early administration is likely more important than perfect patient selection.
• The effect is short-lived; a single dose may not sustain platelet function in ongoing bleeding.
• Repeat dosing is a plausible but unproven strategy—use cautiously and recognize the evidence gap.


Dr. Senger is a pharmacy resident at Parkview Health Systems.
Dr. Reinert is a trauma pharmacist at the University of Toledo Medical Center and faculty at the University of Toledo College of Pharmacy and Pharmaceutical Sciences.

The Nerve Block Paradox: High-Value Care That Feels Hard in the Emergency Department
By David Dorfman, MD, MS; Carrie D. Walsh, MD; Leland Perice, MD; and Lachlan Driver, MD
At a Glance
• Why this matters now: Ultrasoundguided nerve blocks offer highvalue, opioid-sparing analgesia, yet remain underused in emergency departments due to persistent perceptions of difficulty.
• What you’ll learn: A systemsbased framework explaining why nerve blocks feel hard in practice, with practical strategies to improve workflow integration, equipment access, and adoption.
• Who this is for: Emergency physicians, residents, and department leaders seeking to expand procedural analgesia through systemlevel improvements rather than individual skill alone.
Background
Ultrasound-guided nerve blocks are increasingly recognized as highvalue tools in emergency medicine. They provide targeted analgesia, reduce opioid requirements, and
improve patient comfort across a multitude of ED presentations, ranging from traumatic injury to abscess management and analgesia for conditions such as appendicitis, cholecystitis, and pancreatitis. Educational efforts, national registries, and evolving training standards have all contributed to their growing adoption within emergency medicine
Despite these advances, many clinicians still describe nerve blocks
“Despite these advances, many clinicians still describe nerve blocks as ‘hard,’ and this perception persists even among physicians who are otherwise highly proficient with ultrasound and procedural care.”
as “hard.” This perception persists even among physicians who are otherwise highly proficient with ultrasound and procedural care. The question, then, is not simply whether nerve blocks are technically challenging, but why they are felt to be difficult in routine emergency department (ED) practice. A closer look suggests this difficulty may be less about the procedure itself and more about the environment in which it is performed.
The Procedural Paradox
From a technical standpoint, many commonly performed ED nerve blocks are not inherently complex. Several target superficial structures, rely on recognizable sonographic landmarks, and can be performed using skills already familiar to emergency physicians. In fact, some may be less technically demanding than procedures such as central venous access or lumbar puncture, both of which are routinely integrated into ED workflows.
Unlike these procedures, nerve blocks are often perceived as optional for patient disposition rather than essential. As a result, they are more vulnerable to being deferred in busy clinical settings. This creates a paradox: a high-value, relatively accessible procedure that is consistently felt to be difficult to implement.
Time and Workflow Constraints
One of the most commonly cited barriers to performing nerve blocks in the ED is time. Emergency physicians operate in an environment defined by constant patient turnover, competing
priorities, and frequent interruptions. Even safe and short procedures can feel difficult to initiate when clinicians are managing multiple patients simultaneously.
Time pressure in the ED is not simply a matter of individual efficiency, but a reflection of broader system design. Procedures embedded into standard workflows, such as peripheral IV placement or dislocation reduction, are easier to execute because they are expected, supported, and resourced. In contrast, nerve blocks often exist outside of these established pathways. Without integration into routine care processes, even brief procedures can become difficult to prioritize.
Equipment and Environmental Friction
Practical barriers also play a meaningful role. Access to appropriate equipment—ultrasound machines, nerve block needles, local anesthetics, and sterile supplies— can vary significantly between departments and even between shifts. When equipment is not readily available or standardized, clinicians must invest additional time and effort to gather necessary materials. Dissimilar storage methods at different clinical sites further slow this process. These small inefficiencies accumulate, increasing the likelihood that the procedure will be deferred altogether.
In high-functioning systems, the default setup supports efficient care delivery. When that infrastructure is lacking, even simple procedures can feel unnecessarily complex.
Cognitive Load and Interruptions
Performing an ultrasoundguided nerve block requires focused attention. Clinicians must simultaneously interpret imaging, maintain needle visualization, and monitor patient response. These tasks demand cognitive bandwidth. In the ED, however, attention is frequently divided. Interruptions are common, and clinicians are often managing multiple patients with varying levels of acuity. This environment increases cognitive load, making it more challenging to perform procedures that require sustained concentration. The perceived difficulty of nerve blocks may therefore reflect not only technical demands, but also the context in which they are performed.
Variability in Training and Experience
Training pathways for ultrasoundguided nerve blocks remain variable across institutions. While some clinicians complete residency with extensive experience, others may have limited exposure. This variability can influence both confidence and perceived difficulty. In addition, ongoing opportunities for skill reinforcement differ widely between practice environments. Less commonly performed procedural skills such as pediatric intubation atrophy over time, and there is no reason why this would not apply to nerve blocks.
Emerging data from multicenter efforts such as the National Ultrasound-Guided Nerve Block Registry (NURVE) suggest that
continued on Page 149

“A
closer look suggests this difficulty may be less about the procedure itself and more about the environment in which it is performed.”
ULTRASOUND
continued from Page 147
reported technical difficulty is influenced not only by patient and procedural factors, but also by site-level variation. This finding reinforces the idea that local systems and training environments play a meaningful role.
Moving Toward Systems-Based Solutions
If the challenges associated with nerve blocks are largely system-driven, then solutions must also be systemfocused.
Several approaches may help reduce barriers to implementation:
• Workflow integration: Incorporating nerve blocks into standard care pathways for common conditions (e.g., hip fractures) can normalize their use and improve efficiency.
• Equipment standardization: Readily accessible, pre-assembled kits or carts can reduce setup and preparation time.
• Training consistency: Structured
Pulse Points
Key clinical and practice takeaways:
curricula and ongoing opportunities for practice can improve confidence and support skill retention.
• Cultural reinforcement and institutional support: Framing nerve blocks as standard, high-value care rather than optional interventions may increase adoption.
These strategies shift the focus from individual performance to system design, a key factor in the success of previous departmental practice change efforts. Education on how to perform blocks is only one part of the system-focused solution needed to implement them regularly in the ED.
Reframing the Narrative
The perception that nerve blocks are “hard” is widespread but may be misleading. Recognizing this distinction shifts the focus away from individual clinicians and toward system-level factors that shape care delivery. Addressing these structural barriers is essential to achieving meaningful and sustained implementation of nerve blocks in the emergency department

ABOUT THE AUTHORS


• Nerve blocks are not inherently difficult—the barrier is often the emergency department environment, not the procedure itself.
• If a procedure is not built into workflow, it will be skipped—integrate nerve blocks into standard pathways to increase use.
• Equipment access drives behavior—standardized kits and consistent storage reduce friction and improve uptake.
• Cognitive load matters—procedures that require focus are more likely to be deferred in high-interruption settings.
• This is a systems problem, not a skills problem—improving adoption requires operational and cultural change, not just more training.


Dr. Dorfman is an emergency medicine resident in the department of emergency medicine at Brown University Health in Providence, Rhode Island.
Dr. Walsh is an emergency medicine attending and core emergency ultrasound faculty member in the department of emergency medicine at Jackson Memorial Hospital in Miami, Florida.
Dr. Perice is an assistant professor in the department of emergency medicine at Brown University Health in Providence, Rhode Island.
Dr. Driver is an ultrasound fellow in the department of emergency medicine at Brown University Health in Providence, Rhode Island.
ULTRASOUND

Point-of-Care Ultrasound Training After Milestones 2.0: Are We Losing Accountability?
By Levi Filler, DO, Caro Auger, MD on behalf of the SAEM Education Committee
At a Glance
• Why this matters now: Pointof-care ultrasound training expectations are expanding while formal competency structures in residency have become less explicit.
• What you’ll learn: A balanced analysis of Milestones 2.0, including the benefits of flexibility and the risks of reduced accountability in ultrasound education.
• Who this is for: Emergency physicians, residents and educators involved in training, assessment and curriculum design.
Over the past two decades, pointof-care ultrasound (POCUS) has become a defining tool in emergency medicine. What began as a focused
adjunct for trauma evaluation has evolved into a versatile diagnostic and procedural modality used across nearly every domain of care. Today, emergency physicians rely on bedside ultrasound to guide resuscitation, evaluate undifferentiated shock, diagnose time-sensitive conditions, and improve procedural safety.
Ultrasound training has long held a prominent place in residency education. In the original ACGME milestones introduced in 2012, POCUS was designated as its own subcompetency (PC12) (Figure 1), with defined expectations for training and assessment.
However, changes to graduate medical education frameworks have altered this structure. In the transition to ACGME Milestones 2.0 in 2021 (Figure 2), POCUS was
no longer maintained as a distinct procedural milestone. Instead, ultrasound competency was incorporated into broader procedural and clinical categories while remaining a “key index procedure.”
At the same time, ultrasound education continues to expand. Contemporary guidelines emphasize additional applications, including testicular ultrasound and ultrasoundguided regional anesthesia, as core knowledge for emergency medicine trainees. The original milestones also outlined explicit competency assessments—elements that are less clearly defined in the current framework.
Taken together, these developments raise an important question: Are we expanding the scope of ultrasound training while weakening the structures that ensure competency?
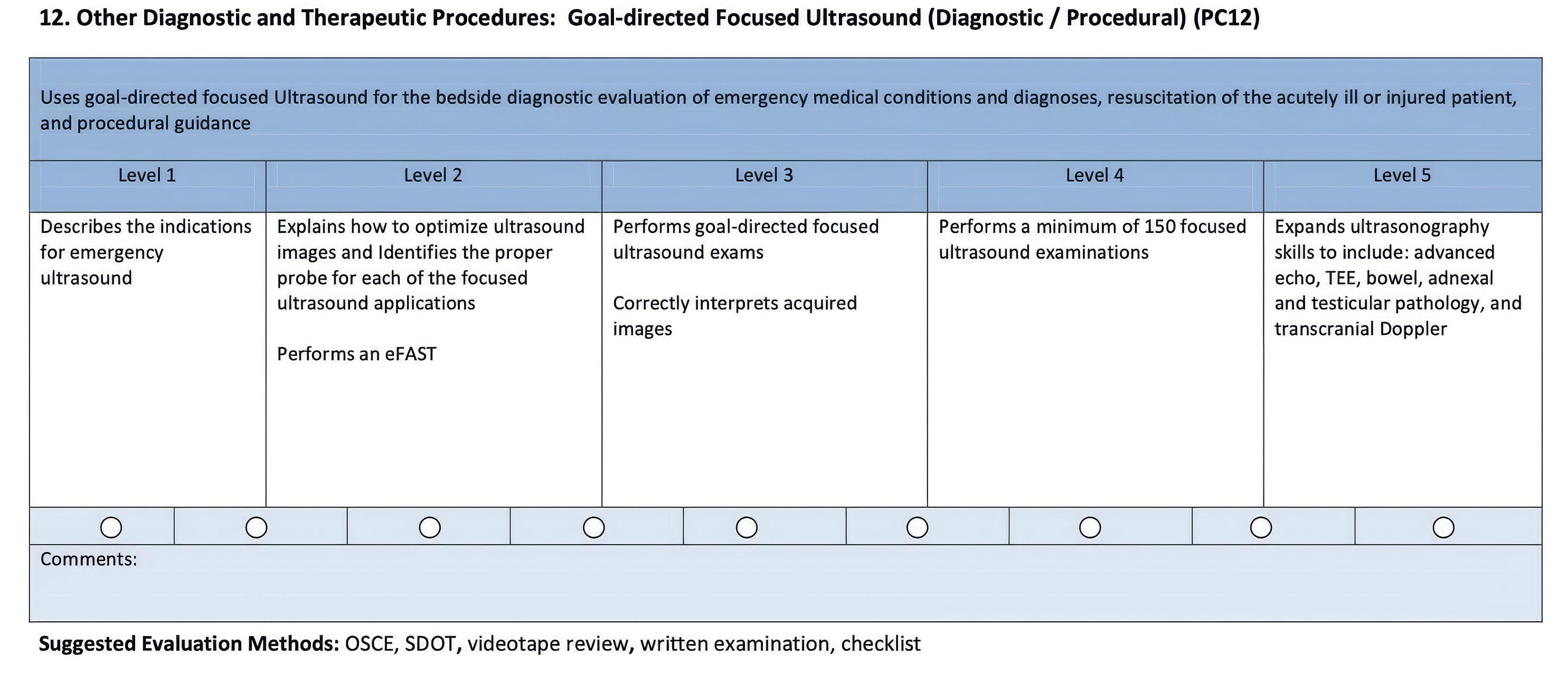
The Case for Greater Flexibility
The shift away from highly specific procedural milestones was not unique to ultrasound. Across specialties, Milestones 2.0 aimed to streamline competency frameworks and reduce the administrative burden of narrowly defined evaluation metrics. Rather than relying on procedure-specific checklists, programs were encouraged to assess residents through broader clinical competencies and local priorities.
This approach offers advantages. Residency programs vary widely in clinical volume, patient populations and faculty expertise. Greater flexibility allows educators to tailor training to their local environment.
From this perspective, integrating ultrasound into broader competencies may reflect the field’s maturation. As POCUS becomes embedded in routine clinical decision-making, it may no longer require the structural separation seen in earlier stages of adoption.
The Risk of Reduced Accountability
The removal of a dedicated ultrasound milestone also carries potential consequences.
Existing guidelines, such as the ACEP POCUS policy, outline training
expectations and quantitative benchmarks—typically 150 to 300 total exams for competency, including 25 to 50 per application and five per procedural application. However, no universally adopted, standardized curriculum exists, and training remains highly dependent on individual institutions.
Skills tied to explicit graduation requirements tend to receive sustained attention, dedicated curriculum time and consistent assessment. When expectations become less explicit, emphasis may vary significantly across programs.
Ultrasound training is particularly sensitive to these dynamics. Competency depends not only on image acquisition but also on interpretation, clinical integration and ongoing quality assurance. Developing these skills requires structured oversight, engaged faculty and consistent feedback.
Without clear expectations, the strength of these systems may become increasingly program dependent
Expanding Expectations
The scope of ultrasound applications in emergency medicine continues to grow. The inclusion of testicular ultrasound and ultrasound-guided
regional anesthesia reflects the expanding role of POCUS in both diagnosis and procedural care.
These additions introduce new challenges.
Testicular ultrasound may be relatively uncommon in some emergency departments, particularly those with large residency classes competing for limited clinical exposure. Ensuring meaningful experience may be difficult without deliberate educational planning.
Ultrasound-guided nerve blocks present a different challenge: faculty expertise. While interest in regional anesthesia has grown, the number of clinicians comfortable teaching and supervising these procedures varies across institutions. Effective training requires not only technical skill but also a strong understanding of anatomy, safety considerations and complication management. This can be particularly challenging for faculty who did not receive formal training in these techniques.
In other words, expanding the scope of POCUS may require more educational oversight—not less.
continued on Page 153
Figure 1. Original POCUS milestone
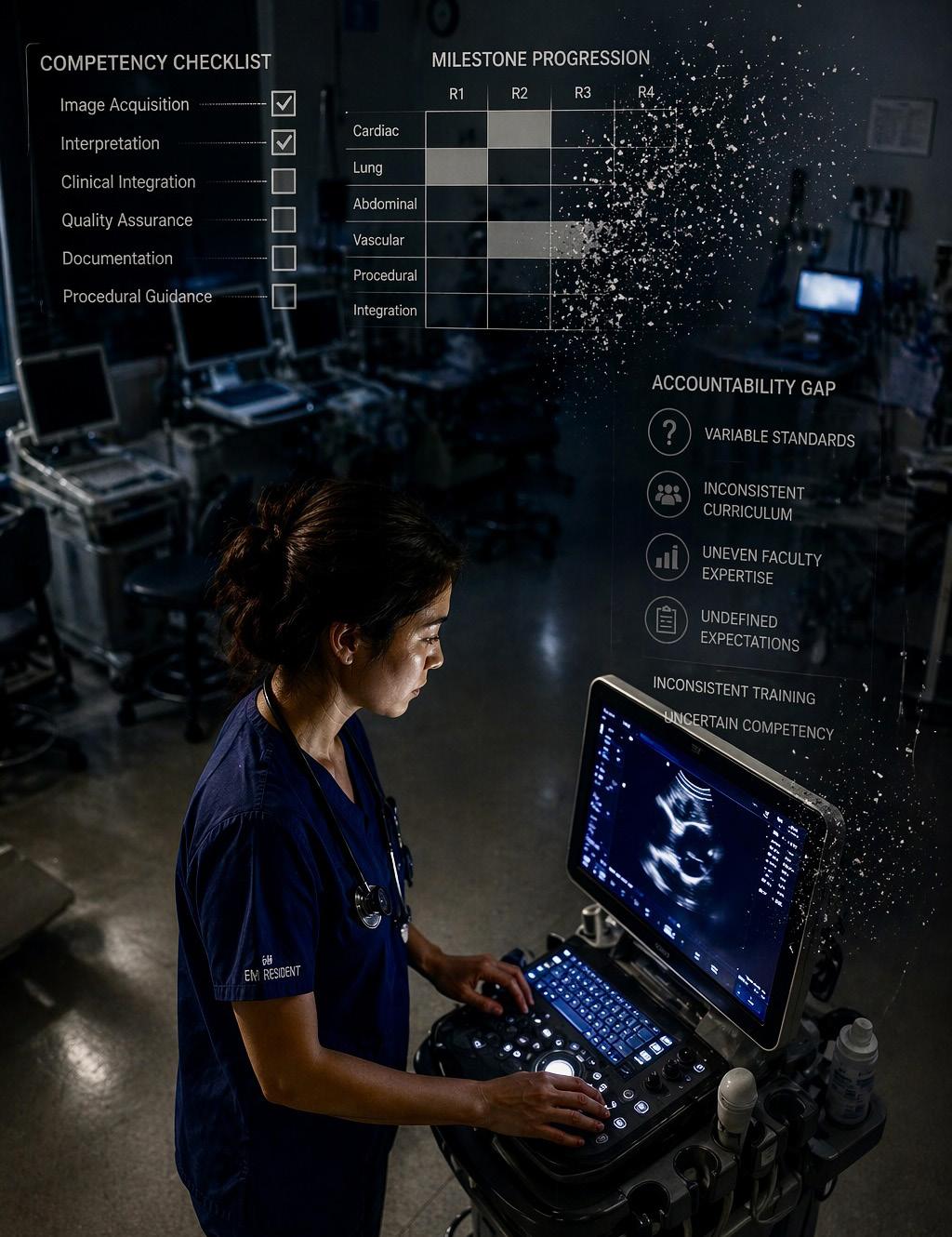
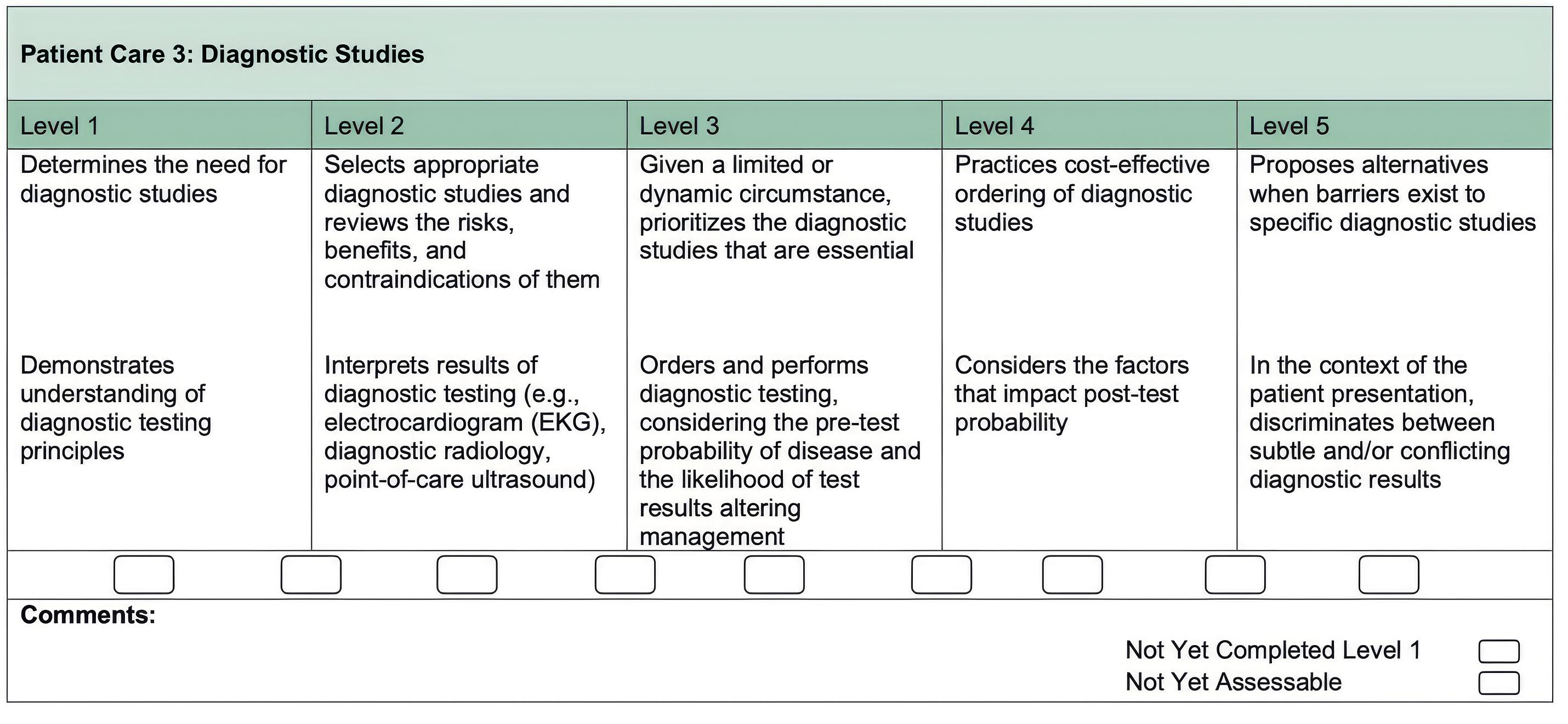
ULTRASOUND
continued from Page 151
Should POCUS Stand Alone?
These developments raise a broader question for emergency medicine educators: Does POCUS represent a sufficiently central clinical competency to warrant its own milestone?
Unlike many procedures performed intermittently, ultrasound functions as a real-time extension of the physical
Pulse Points
Key clinical and practice takeaways:
exam. It informs resuscitation, diagnostic evaluation, procedural safety and patient disposition. In many emergency departments, it is used dozens of times during a single shift.
Given this breadth, some educators argue that ultrasound competency should be recognized as a distinct domain with explicit training standards and assessment. Others contend that integration within broader competencies better reflects its role in everyday practice.
• Expanding ultrasound expectations without explicit milestones risks widening variability in resident competency across programs.
• If it is not measured, it may not be prioritized—formal assessment structures drive curriculum time, faculty attention and skill development.
• Ultrasound competency extends beyond image acquisition; programs must deliberately teach interpretation, integration and quality assurance.
• New applications like regional anesthesia and testicular ultrasound require not just learner exposure, but sufficient faculty expertise and supervision.
• Treat point-of-care ultrasound as a core clinical skill, not just a procedure— training models should reflect its role in real-time decision-making.
Both perspectives offer valid considerations.
Moving Forward
Emergency medicine has long been a leader in the adoption of point-ofcare ultrasound. The specialty now faces a new challenge: ensuring that training structures evolve to support consistent competency across residency programs.
Whether that solution involves restoring a dedicated milestone or developing new frameworks, the conversation is essential. If ultrasound is truly a core pillar of emergency medicine, the systems that train future physicians must reflect that reality
ABOUT THE AUTHORS


Dr. Filler is ultrasound fellowship director at Valleywise Health in Phoenix, Arizona.
Dr. Auger is a physician and medical education fellow at Hennepin County Emergency Medicine in Minneapolis, Minnesota.
Figure 2. Updated POCUS milestone

Scouting the Signs: A Nature-Inspired Expedition Through Point-of-Care Ultrasound
By Theresa Yeo, MD; William Mak, DO; and Ee Tay, MD
At a Glance
• Why this matters now: Rapid interpretation of point-of-care ultrasound findings is critical in emergency care, yet inconsistent terminology and variable recognition of classic “signs” can create confusion at the bedside.
• What you’ll learn: A clinically grounded, image-linked review of common ultrasound signs— using nature-based analogies—to improve recognition, interpretation, and diagnostic confidence.
• Who this is for: Emergency medicine trainees, early-career clinicians, and educators seeking practical frameworks to enhance
point-of-care ultrasound pattern recognition.
Ultrasound, like many other imaging modalities, uses pictorial references, or “signs,” to aid in recognizing anatomic structures and diagnostic findings. This is particularly useful in point-of-care ultrasound (POCUS), where rapid image interpretation is essential to determining clinical course.
While these signs support education, communication, and rapid recognition, their use is not without limitations. A lack of standardization, overlapping terminology, and inconsistent naming conventions can lead to confusion. In addition,
variability in operator skill may affect reliable identification.
This review highlights ultrasound signs that draw on memorable analogies from nature as a framework for categorization. The first section presents pointof-care ultrasound images from a pediatric emergency department to demonstrate common signs. The second section highlights additional nature-based signs without accompanying imaging.
Point of Care Ultrasound Images Bat Sign
The bat sign is a normal finding on lung ultrasound. The hypoechoic ribs on either side form the “wings,” while
the pleural line forms the ”body” of the bat.
This sign is absent in pathologic states where ultrasound waves are obstructed, such as subcutaneous emphysema, in which air prevents transmission of the ultrasound beam.
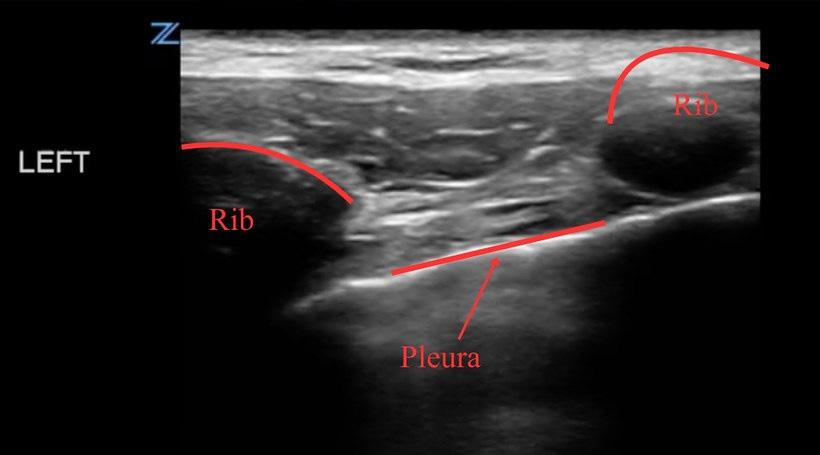

Jellyfish Sign
The jellyfish sign is seen on lung ultrasound in the setting of a pleural effusion. The collapsed lung represents the “jellyfish,” while the surrounding pleural fluid represents the “sea.” On dynamic imaging, the lung moves in a manner resembling a jellyfish swimming.
The presence of this sign may suggest a transudative effusion and the absence of pleural adhesions, as indicated by the free movement of the lung.
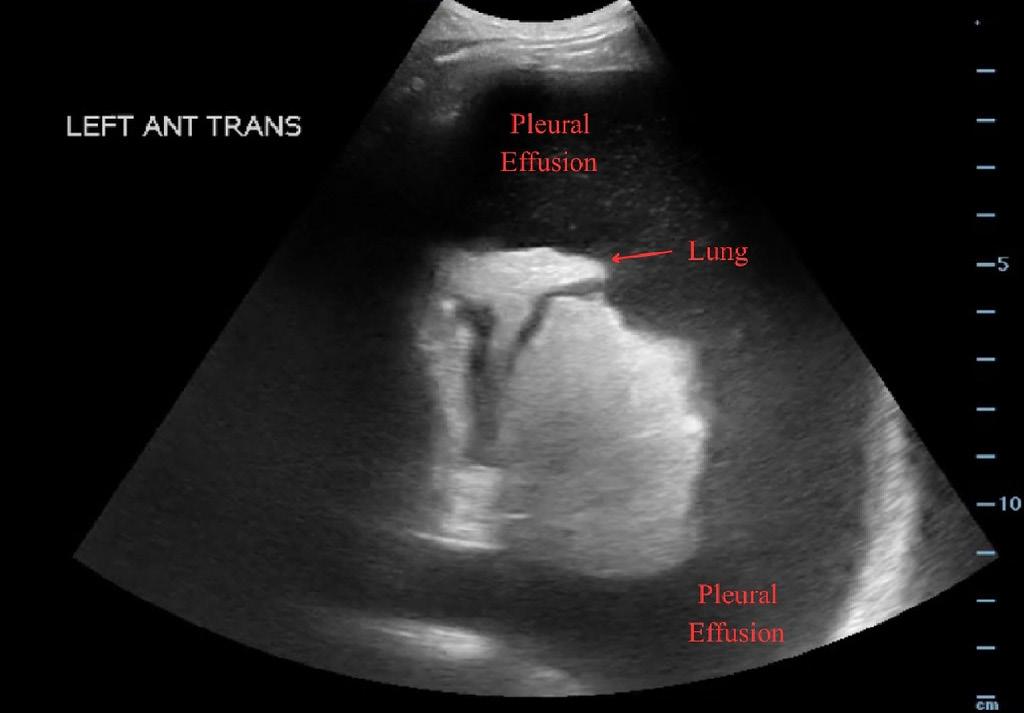

Plankton Sign
The plankton sign is observed in pleural effusions when floating debris is visualized within the fluid, resembling plankton drifting in the sea.
Compared with the jellyfish sign, the plankton sign is more commonly associated with exudative effusions, although both findings may be present simultaneously.
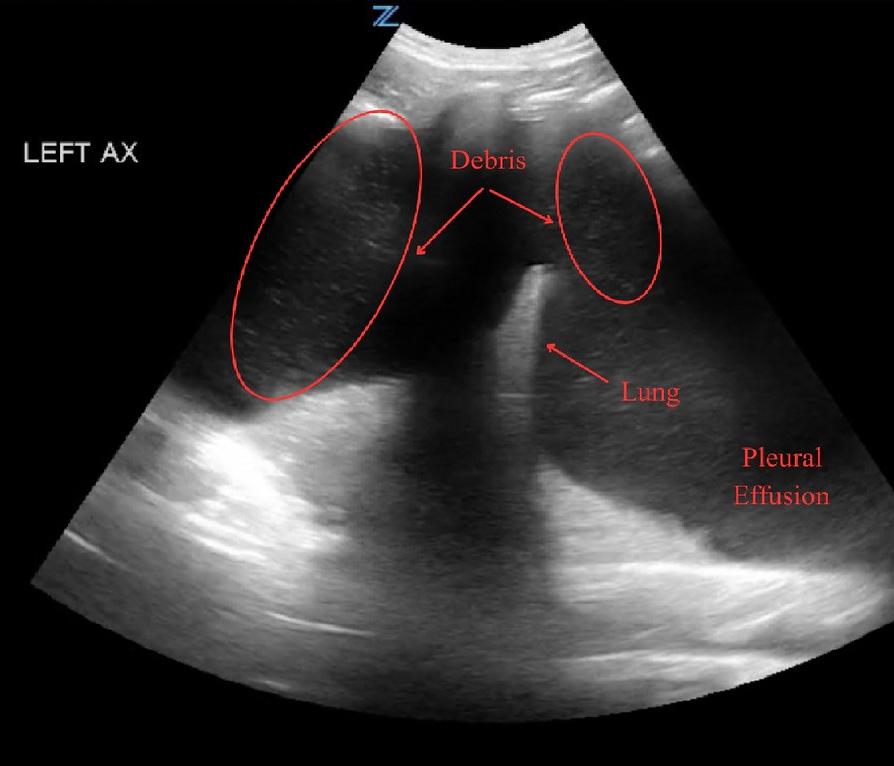
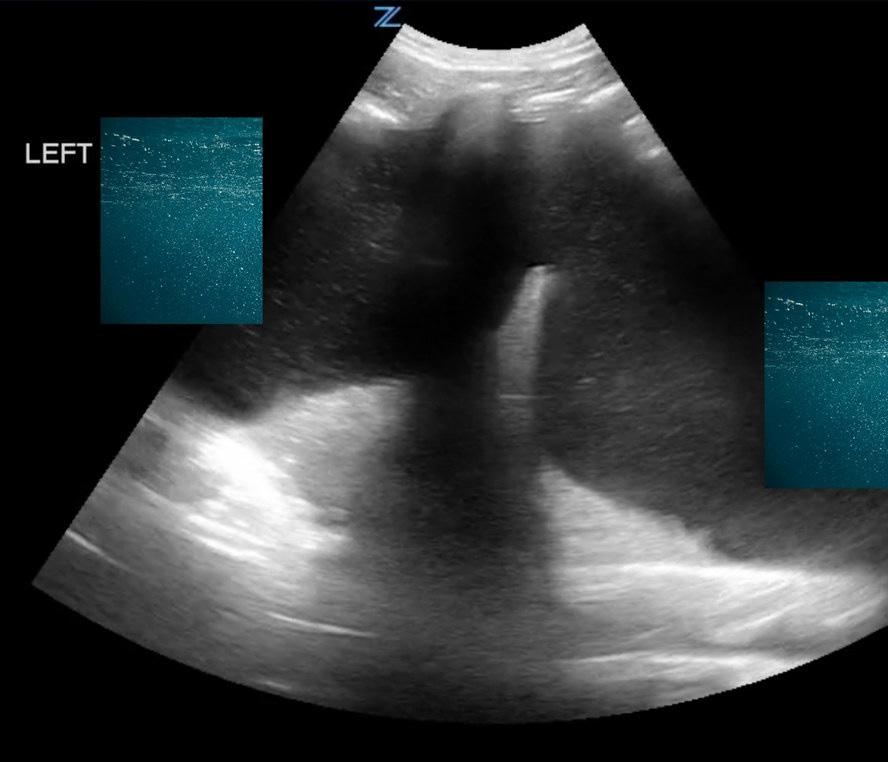
Seashore Sign
The seashore sign is a classic finding on lung ultrasound in M-mode. The superficial chest wall appears as horizontal lines (the “sea”), while the deeper lung tissue demonstrates a granular pattern (the “shore”) due to lung sliding.
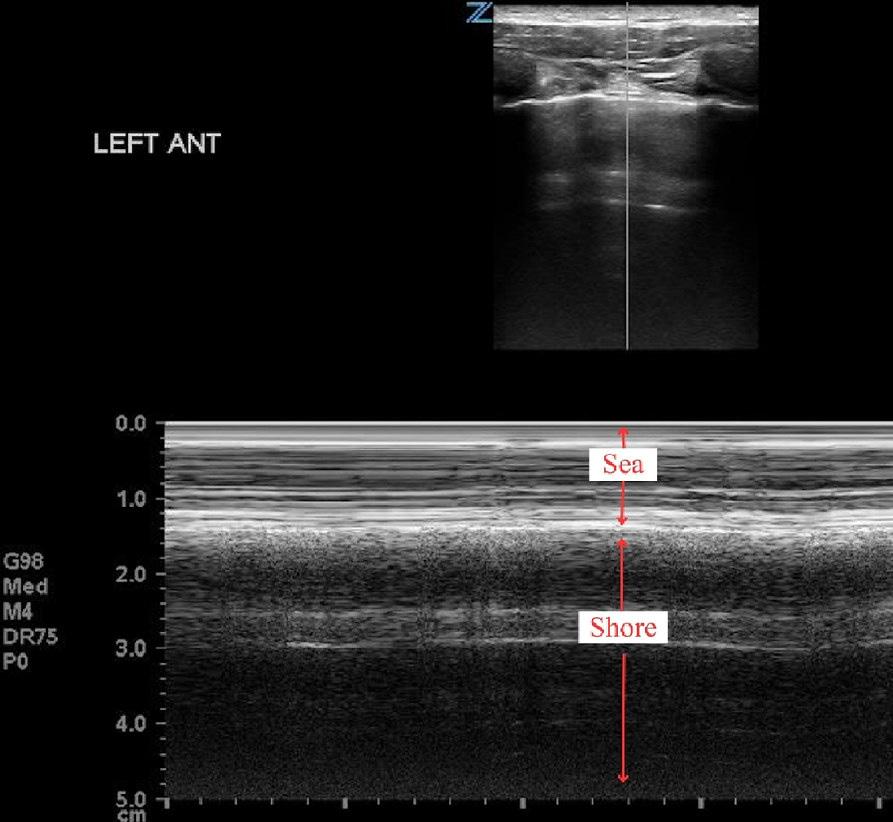
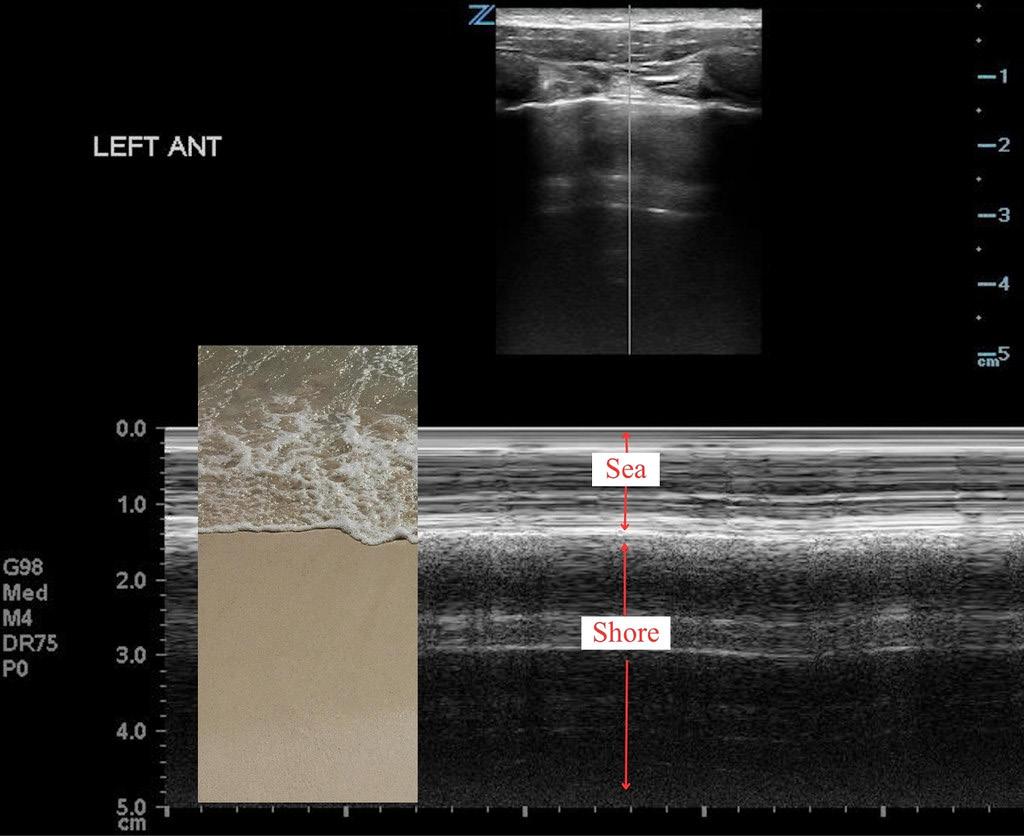
Twinkle Sign
The twinkle sign is seen with color Doppler and may occur anywhere in the body. It appears as a rapid alternation of color signals posterior to a reflective structure, such as a calculus or air.
This artifact is thought to result from intrinsic machine noise and is more pronounced with rough-surfaced objects. It is highly dependent on machine settings and operator technique. A related finding is the comet-tail artifact extending deep to the object.
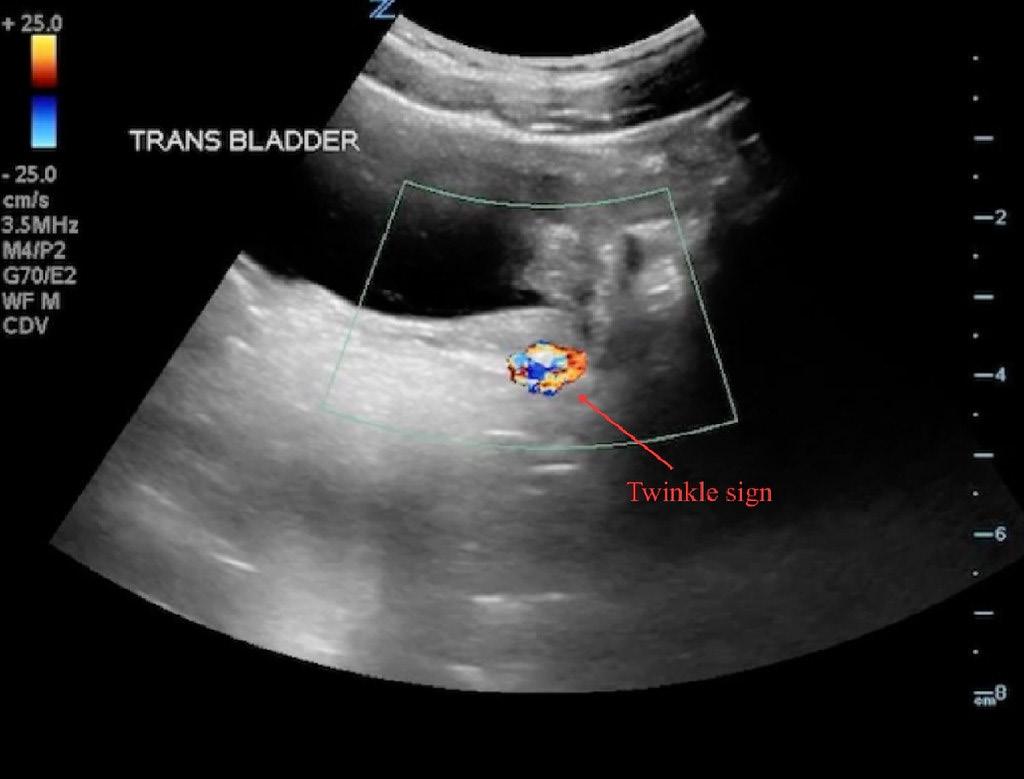
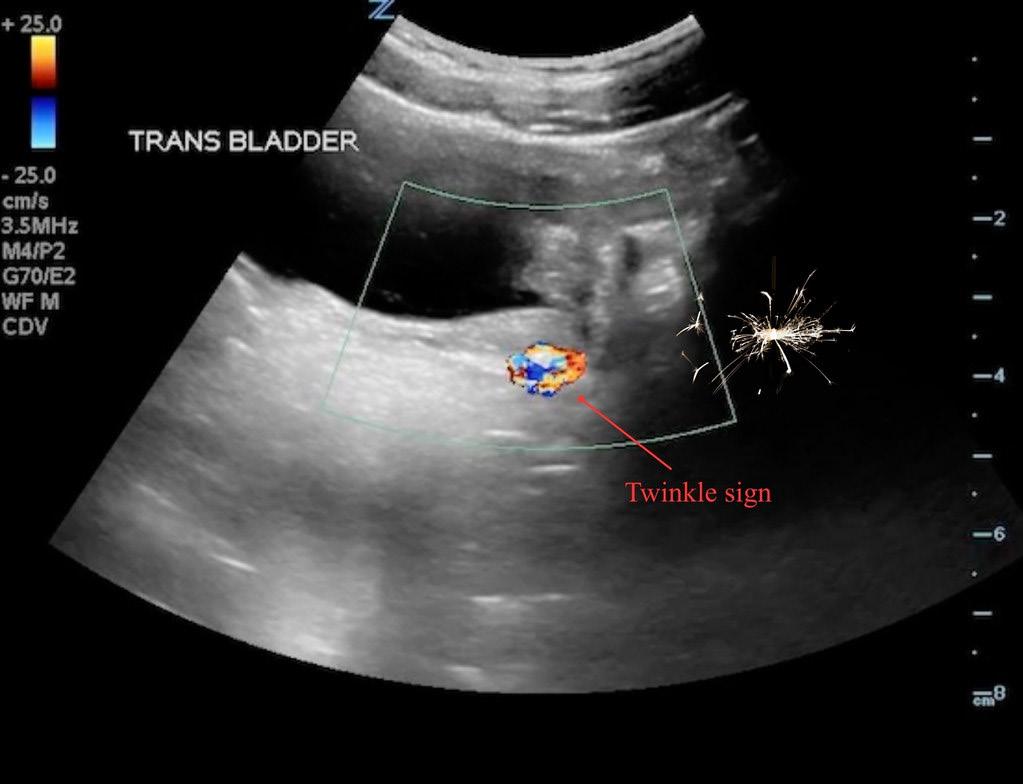
Bull’s Eye Sign
The bull’s-eye sign describes the characteristic appearance of intussusception on ultrasound.

Concentric alternating echogenic and hypoechoic bands represent layers of bowel, including the mucosa, submucosa, and muscularis propria.
This appearance is also described using other analogies, including a “target” or “donut” sign in transverse view and a “pseudo-kidney” or “sandwich” sign in longitudinal view.
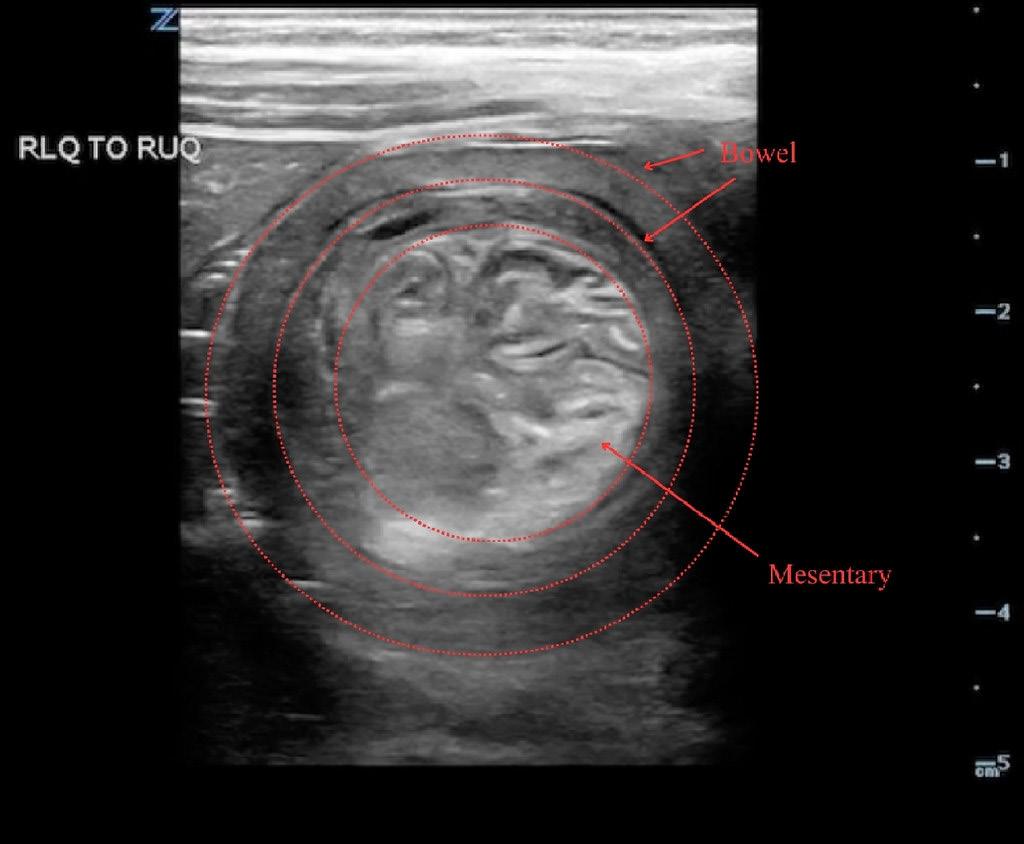
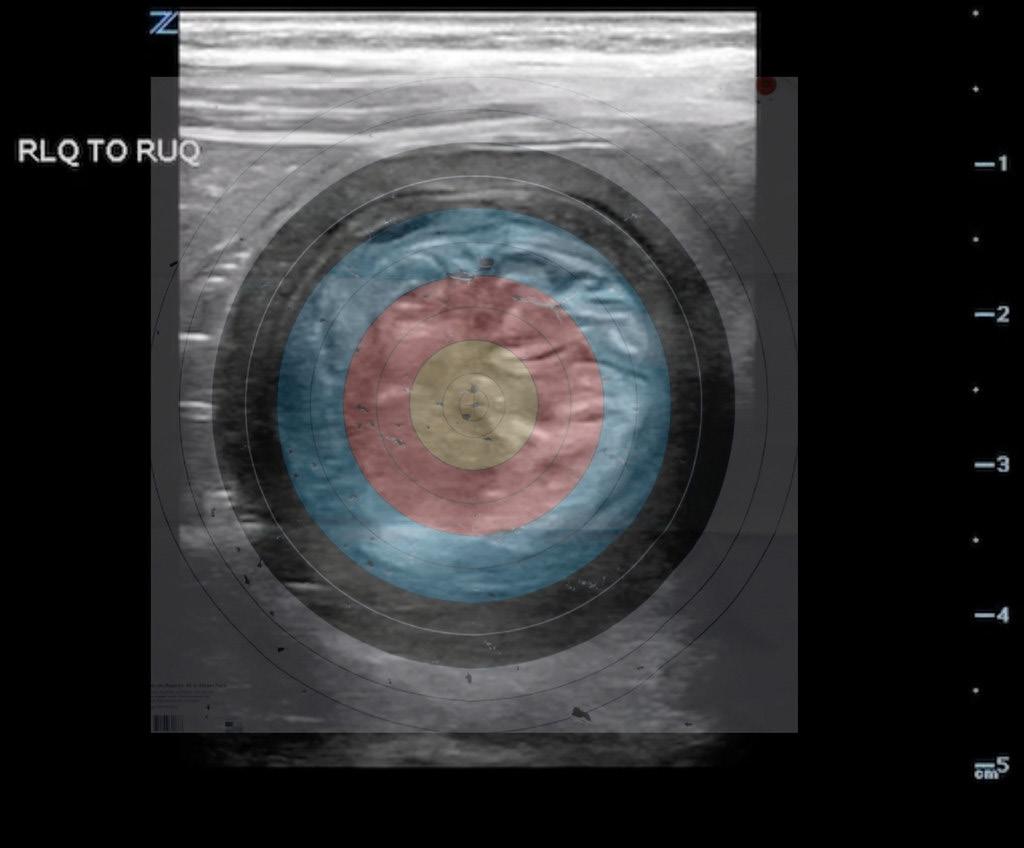
Pulse Points
Key clinical and practice takeaways:
Additional Signs Without Imaging
Stratosphere Sign
The stratosphere sign is seen on lung ultrasound in M-mode in the absence of lung sliding. Instead of the seashore pattern, the image shows uniform horizontal lines throughout, resembling a barcode.
Seagull Signs
The seagull sign refers to branching or converging structures that resemble a seagull in flight. It is most commonly used to describe abdominal vasculature.
The venous seagull is formed by the confluence of the splenic vein, superior mesenteric vein, and portal vein. The arterial seagull is formed by the celiac trunk dividing into the splenic and common hepatic arteries. This appearance is also referred to as the “whale’s tail” sign.
Deer Horn Sign
The deer horn sign is seen on liver ultrasound and may suggest passive congestive hepatopathy. The dilated hepatic vasculature, including the inferior vena cava and hepatic veins, resembles branching antlers.
This finding is also referred to as the bunny sign.
Starry Sky Sign
The starry sky sign is an abnormal liver ultrasound finding characterized by bright echogenic foci scattered
• Pattern recognition is a clinical skill: knowing classic ultrasound “signs” can accelerate bedside decision-making in time-sensitive scenarios.
• Not all signs are created equal—many lack standardization, so always interpret them in clinical context rather than in isolation.
• Dynamic imaging matters: several signs (e.g., jellyfish, seashore) rely on motion, not just static appearance.
• Use analogies as cognitive shortcuts: nature-based patterns can improve retention and teaching, especially for trainees.
• One surprising reality: the same ultrasound finding (e.g., pleural effusion) can produce multiple signs—recognizing overlap is as important as recognizing the sign itself.
throughout a relatively hypoechoic parenchyma.
This appearance is associated with a centrilobular pattern due to hepatocyte edema and is most commonly described in acute hepatitis, though it has limited sensitivity and specificity.
Snowstorm Sign
The snowstorm sign is seen on musculoskeletal ultrasound in the setting of crystalline anthropathy. Hyperechoic particulate matter within a hypoechoic joint effusion creates the appearance of a snowstorm.
This finding may suggest gout in the appropriate clinical context.
Conclusion
Ultrasound signs are valuable tools for recognizing and communicating key imaging findings. Their memorable nature supports learning and rapid identification. However, improved standardization of terminology and clearer definitions may enhance communication and diagnostic reliability while preserving their educational value in clinical practice.
ABOUT THE AUTHORS



Dr. Yeo is a pediatrics resident at NYU Langone Bellevue Hospital in New York.
Dr. Mak is an associate clinical professor in the departments of pediatrics and emergency medicine at NYU Grossman School of Medicine.
Dr. Tay is clinical site director of pediatric emergency services at Bellevue Hospital and an associate clinical professor in the departments of pediatrics and emergency medicine at NYU Grossman School of Medicine.
ULTRASOUND
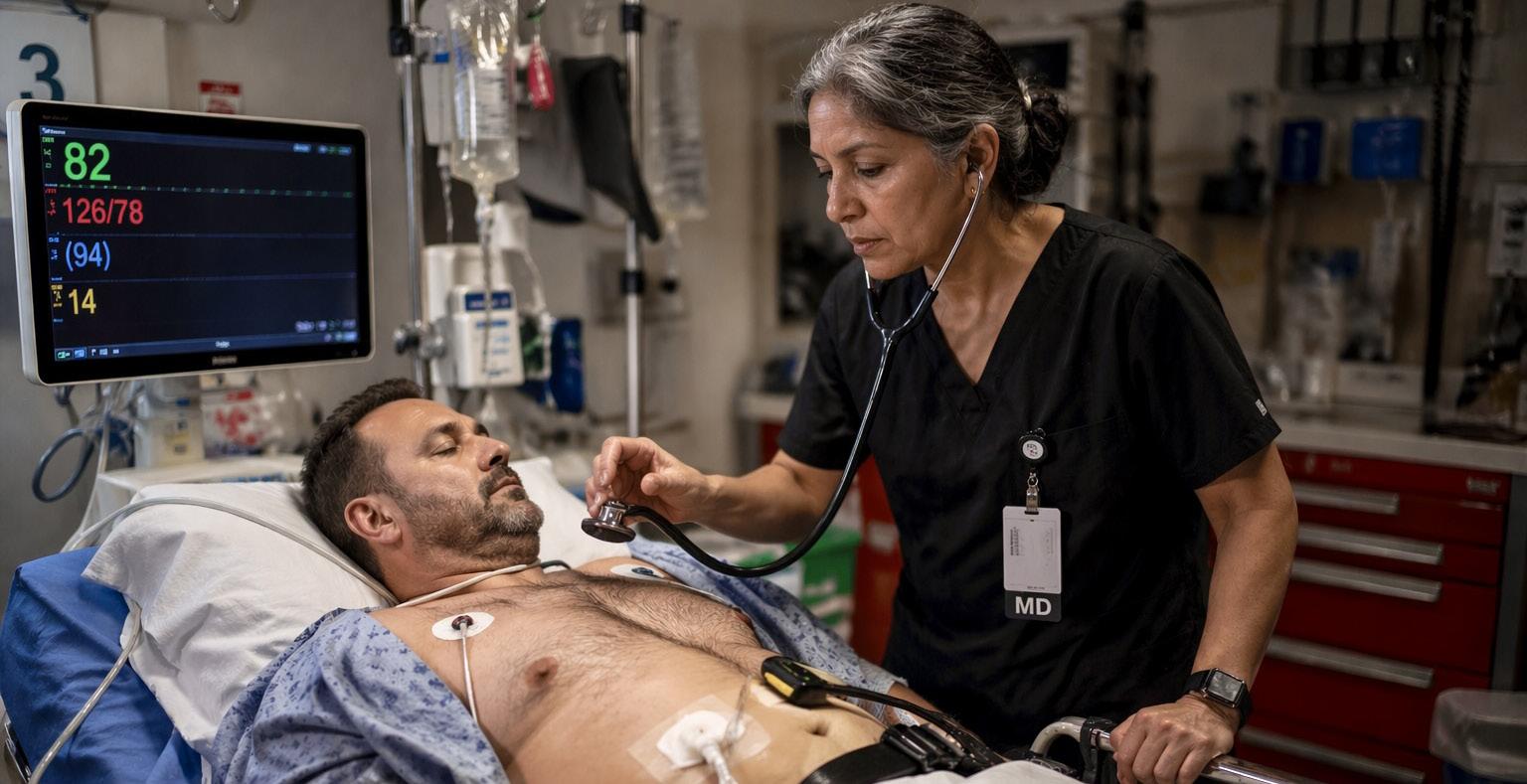
Point-of-Care Ultrasound in Left Ventricular Assist Device Patients: A Systematic Emergency Department Approach
By Andrew G. Theophanous; Denise Elizondo, MD; Nina Angeles, MD; and Rebecca G Theophanous, MD, on behalf of the SAEM Academy of Emergency Ultrasound
At a Glance
• Why this matters now: Patients with left ventricular assist devices are increasingly presenting to the emergency department, where traditional exam findings are unreliable and rapid, accurate assessment is critical.
• What you’ll learn: A practical, point-of-care ultrasound–driven framework to differentiate causes of hypotension and identify key device-related complications at the bedside.
• Who this is for: Emergency physicians, residents, and clinicians managing acutely ill patients with advanced heart failure and left ventricular assist devices.
Introduction
Cardiovascular disease (CVD) is the leading cause of mortality worldwide, with over 128 million Americans (48.6%) with CVD. Over six million Americans have acute congestive heart failure (CHF), and emergency departments (EDs) nationwide manage and initiate treatment for over 80% of these patients. Over 9,000 left ventricular assist devices (LVAD) were implanted in patients with advanced CHF as destination therapy or as a bridge to cardiac transplant between 2006-2013.
Cardiovascular disease (CVD) remains the leading cause of mortality worldwide, affecting more than 128 million Americans (48.6%) More than 6 million Americans
have congestive heart failure (CHF), and emergency departments (EDs) manage and initiate treatment for more than 80% of these patients. Between 2006 and 2013, more than 9,000 left ventricular assist devices (LVADs) were implanted in patients with advanced CHF as destination therapy or as a bridge to cardiac transplant.
Clinical evaluation of LVAD patients can be challenging. These patients often lack palpable pulses and may appear chronically ill. When they present to the ED, clinicians should assess for a mean arterial pressure (MAP) of 60–90 mmHg, auscultate for a characteristic machine “hum,” and evaluate for cardiac arrhythmias or ischemia on electrocardiogram.
Echocardiogram
Abnormally small LV (Right to left septum shift) Suction event
Large RV and LV Pump thrombosis/obstruction
Large RV and small LV
Small RV and LV
RV failure Pulmonary hypertension
Hypovolemia
GI bleed Sepsis
Low power
Normal or high PI
High speed (rpm)
Low pump flow
High power
Low PI
High speed (rpm)
Low or no hum
High power
High PI
Low flow
Intravenous fluid bolus to increase LV filling
Heparin or thrombolytic
Intravenous fluid bolus
Electrocardiogram
Consider inotropes
Intravenous fluid bolus
Consider blood transfusion and reversing coagulopathy
Antibiotics
Table 1: Summary of focused cardiac point-of-care ultrasound findings in LVAD patients with acute decompensation (credit is from Stainback et al)
Key: RV: right ventricle, LV: left ventricle, GI: gastrointestinal, PI: pulsatility index, rpm: revolutions per minute
Signs of volume overload include leg swelling, jugular venous distension, abdominal distension, and rales on lung exam. Device parameters should also be reviewed, including pump speed (typically 3,000–9,000 revolutions per minute for HeartMate 3), flow (4–6 L/min), power (4–6 watts), pulsatility index (1–10), and battery life. LVAD complications include infection, thrombosis, hypotension, bleeding, dysrhythmias, and device failure. If a low-battery alarm occurs, batteries should be replaced one at a time.
Role of Echocardiography and POCUS
Echocardiography plays a central role both before LVAD implantation and in reassessing cardiac function and volume status afterward. However, traditional physical exam findings— such as jugular venous distension, skin turgor, mucous membranes, and distal pulses—are often unreliable in LVAD patients
Focused cardiac point-of-care ultrasound (POCUS) is therefore an essential tool for ED clinicians evaluating LVAD patients with suspected decompensation, particularly in cases of hypotension or shock. POCUS can help guide
fluid and vasopressor management through assessment of the inferior vena cava (IVC) and jugular vein, although data on volume assessment accuracy are mixed.
LVAD physiology introduces unique risks. POCUS can help identify complications involving the pump, inflow or outflow cannulas, native cardiac dysfunction, driveline issues, and pulmonary edema. This article outlines a systematic approach to evaluating these patients at the bedside.
Key POCUS Findings in LVAD Patients
Focused cardiac POCUS can assess:
• Chamber size and function
• IVC diameter and respiratory variation
• Ventricular septal position (normally neutral/flat)
It can also identify pericardial effusion and signs of tamponade, including right atrial systolic or right ventricular diastolic collapse.
The inflow cannula should align with the mitral valve within the left ventricle, while the outflow cannula should be visualized in the proximal aorta. The aortic valve should open
intermittently, typically every 2–3 cardiac cycles.
Evaluation of Hypotension and Shock
In patients with hypotension (MAP <60 mmHg), POCUS findings may include a small IVC with greater than 50% respiratory variation and small right and left ventricles.
If hypotension is due to hypovolemia (e.g., diarrhea, vomiting, or poor oral intake), fluid resuscitation is indicated. In cases of hemorrhage (e.g., gastrointestinal bleeding), consultants should guide decisions about holding anticoagulation.
ED management may include tranexamic acid, prothrombin complex concentrate, fresh frozen plasma, and packed red blood cells for anemia (hemoglobin <8.0 mg/dL).
Suction Events vs. Pump Thrombosis
A suction event occurs when the left ventricle (LV) becomes underfilled. On POCUS, the LV appears small, and the interventricular septum deviates toward the LV. The inflow cannula may draw the septum inward.
ventricular these appear

continued from Page 159
In contrast, pump thrombosis presents with a dilated LV and right ventricle (RV), reflecting impaired unloading. Patients may report fatigue and dark urine. Device parameters often show increased power (>10–13 watts) and decreased flow.
Advanced echocardiographic findings may include reduced change in LV end-diastolic diameter (LVEDD slope > -0.16), decreased aortic valve opening time (<80 msec), and shortened mitral inflow deceleration time (<70 msec).
Treatment typically involves anticoagulation or thrombolytics in severe cases, including cardiac arrest
Right Ventricular Failure and Pulmonary Hypertension
In right ventricular (RV) failure or pulmonary hypertension, POCUS typically shows a dilated RV with hypertrophy and a small LV. Pulmonary arteries may also appear enlarged
A meta-analysis of 1,561 patients found that RV fractional area change (FAC) and RV global longitudinal strain (RVGLS) are strong predictors of right heart failure after LVAD implantation Additionally, tricuspid annular plane systolic excursion (TAPSE) <17 mm is associated with RV failure.
Management focuses on careful modulation of preload and afterload, often using vasodilators in coordination with advanced heart failure or transplant teams
Infection and Driveline Complications
POCUS can help identify fluid collections or abscesses around the driveline in patients with suspected infection. A sterile probe cover should be used, and driveline dressings should remain intact to minimize contamination during imaging
Conclusion
Emergency clinicians should take a systematic approach when using POCUS to evaluate LVAD patients. Key complications include issues with inflow or outflow cannulas, pump dysfunction, abnormal cardiac physiology, pulmonary edema, and valvular or shunt-related abnormalities.
“Clinical evaluation of patients with left ventricular assist devices can be challenging, as these patients often lack palpable pulses and may appear chronically ill, requiring clinicians to rely on alternative assessment strategies.”
Pulse Points
Key clinical and practice takeaways:
• Traditional vital signs can mislead—patients with left ventricular assist devices may lack a palpable pulse, making mean arterial pressure and device parameters essential for assessment.
• Point-of-care ultrasound is not optional—it is a frontline diagnostic tool for rapidly identifying volume status, ventricular function, and device-related complications.
• Hypotension is not one diagnosis—differentiate hypovolemia, suction events, pump thrombosis, and right ventricular failure early to guide targeted management.
• Device data matters—changes in power, flow, or pulsatility index can provide critical clues before clinical deterioration becomes obvious.
• Early coordination changes outcomes—engaging advanced heart failure or transplant teams early can accelerate definitive management and improve patient survival.
Early recognition of these findings can facilitate rapid coordination with advanced heart failure and transplant teams, leading to more timely treatment and improved patient outcomes.
ABOUT THE AUTHORS




Andrew G. Theophanous is a second-year medical student at the University of Toledo College of Medicine.
Dr. Elizondo is an emergency ultrasound fellow and faculty member at Duke University School of Medicine in the department of emergency medicine.
Dr. Angeles is an emergency ultrasound fellow and faculty member at Duke University School of Medicine in the department of emergency medicine.
Dr. Theophanous is an emergency medicine physician at Duke University and emergency ultrasound director at the Durham VA.

Beyond Training: Later Career Transitions, Identity, and Finding Alignment
By Jared Escobar, MD; Heidi Levine, DO; Pamela Dyne, MD; Al’ai Alvarez, MD; and Maia Winkel, MD, on behalf of the SAEM Resident
and Medical Student (RAMS) Board
At a Glance
• Why this matters now: Career transitions don’t end after training— later-stage shifts around identity, purpose, and alignment are common and often unsupported.
• What you’ll learn: How physicians navigate nonlinear career paths, redefine success over time, and find wellness through alignment, mentorship, and human connection.
• Who this is for: Emergency physicians, and early- to mid-career clinicians reflecting on career direction, identity, and long-term sustainability.
The assumption that career uncertainty ends once one becomes an attending is one of medicine’s
most persistent myths. In reality, some of the most significant transitions happen well after training, sometimes decades into practice.
It is worth remembering that the “heavy lifting” of training—the long hours of studying, the dizzying number of exams, and the constant rotation through different medical departments—is only the beginning. Medical school and residency occupy a relatively small portion of a physician’s career.
Most of our time in medicine unfolds after formal training ends. The transitions that occur during these years are often less about clinical competence and more about identity, values, and long-term sustainability.
As physicians gain experience and exposure to different aspects of medicine, opportunities often arise that were never part of the original plan. Some move into quality improvement, administration, education, or leadership. Others pursue advanced degrees, take on institutional roles, or develop entirely new areas of focus.
One emergency physician described a career that moved through several phases. It began with full-time clinical work, then expanded to quality and patient safety leadership, hospital administration, and multiple medical director roles. Over time, she chose to step away from administrative medicine when it no longer aligned with her evolving interests.
That departure, while difficult, created space for something unexpected. She began working with family medicine residents on clinician well-being, an experience that grew organically into leadership roles across multiple departments and training programs.
Some opportunities come through professional connections; others come from reaching out and asking. The common thread is openness to change, discomfort, and redefining success.
Later career transitions often prompt deeper reflection. Physicians begin to ask not only “What’s next?” but also “What matters now?” and “What do I actually want to spend my time doing?”
Earlier in their careers, many recall trying to prove themselves. They worked harder, stayed later, and often sacrificed personal relationships in pursuit of competence and credibility. Over time, confidence grows, and priorities begin to shift.
The desire to be seen as capable gives way to the desire to feel aligned.
At this stage, wellness is often shaped more by moments of human connection than by professional achievement. Physicians recall colleagues who noticed distress and responded with compassion—taking over care of patients during a difficult shift, offering quiet support, or simply acknowledging the shared challenges of the work without judgment.
Pulse Points
Key clinical and practice takeaways:
These experiences often become guiding principles for how physicians lead and care for others, sometimes extending beyond what the role or shift formally requires.
One physician recalled the lasting impact of a colleague who stepped in after his first unexpected patient death as an attending. Without hesitation, that colleague took over the shift and told him not to worry about the work, encouraging him to finish what he could and then go home and rest.
The message was simple: you are human, and you are not alone.
Years later, that moment still shapes how he supports colleagues in crisis.
What is often missing during later transitions is the same thing that is lacking early on: mentorship. Professional networks may grow over time, but structured guidance during periods of identity change remains rare.
Physicians are often expected to adapt on their own, even as the emotional stakes increase.
Later career transitions challenge the idea that success is linear or cumulative. Sometimes growth means stepping back. Sometimes it means leaving a role that looks impressive on paper but feels misaligned in practice.
Wellness does not come from constant advancement. It comes from the ability to choose differently and pivot when needed.
Ultimately, these transitions remind us that careers are not static; they evolve alongside our lives.
Physicians who have navigated career transitions often offer the same advice. It is simple but hard-won: do what makes you happy, not what you think you should do.
Allowing careers to move and change creates space not only for longevity, but also for meaning. The goal is not simply to stay in medicine. Too many years are dedicated to developing this career for it to be misaligned with your interests and goals. The aim is to build a career that you can live with, grow within, and carry forward—and you do not have to do it alone.
ABOUT THE AUTHORS



• Career paths are rarely linear—remaining open to change allows for growth, realignment, and long-term sustainability.
• Alignment matters more than achievement—wellness often comes from doing work that reflects your values, not just your credentials.
• Mentorship gaps persist beyond training—actively seeking guidance during later transitions is critical but often overlooked.
• Small moments of support shape culture—stepping in for a colleague or offering quiet empathy has lasting impact.
• Stepping back is not failure—leaving a role that no longer fits can be a necessary and strategic move forward.


Dr. Escobar is a third-year resident at New Jersey Medical School and a board member for the Resident and Medical Student Section of the Society for Academic Emergency Medicine.
Dr. Alvarez is a clinical professor and director of well-being at Stanford emergency medicine. He serves as subcommittee chair of the Stop the Stigma in Emergency Medicine initiative for the Society for Academic Emergency Medicine wellness committee. Dr. Levine is an assistant professor of emergency medicine at the Zucker School of Medicine and director of wellness at Northwell Health/ South Shore University Hospital.
Dr. Dyne is a professor of clinical emergency medicine at the David Geffen School of Medicine at the University of California, Los Angeles, and chief physician well-being officer at Olive ViewUniversity of California, Los Angeles Medical Center.
Dr. Winkel is a clinical instructor and physician wellness fellow at Stanford emergency medicine. She is a Stanford Health Professions Education and Scholarship Program honors scholar and a member of the Stanford Biodesign faculty fellowship.
WILDERNESS MEDICINE

Anaphylaxis in the Backcountry: Recognition and Management
By Kevin Watkins, MD
At a Glance
• Why this matters now: Anaphylaxis is time-critical and increasingly encountered in wilderness settings, where delayed recognition and limited resources can be fatal.
• What you’ll learn: How to recognize atypical presentations, apply updated diagnostic criteria, and deliver effective, fieldadapted management—including epinephrine use and disposition decisions.
• Who this is for: Emergency physicians residents, and outdoor medicine providers
managing allergic emergencies in resource-limited or prehospital environments.
Anaphylaxis is a frequent concern in wilderness medicine, supported by longstanding management traditions. Up to 5% of the U.S. population has experienced anaphylaxis, but its incidence in the backcountry remains poorly defined due to underreporting and evolving definitions. Data from major outdoor organizations, such as NOLS and Outward Bound, suggest it occurs in less than 1% of participants. While reported cases from the field are increasing, it is unclear whether this reflects a true rise in incidence or improved reporting. Annual U.S.
mortality is estimated between 200 and 1,500 deaths, though the case fatality rate remains low at less than 1%.
Diagnosis
Anaphylaxis is a systemic, multiorgan, life-threatening allergic reaction. In 2020, the World Allergy Organization simplified the diagnostic criteria to include either of the following after allergen exposure:
1. Mucocutaneous signs (e.g., hives, swelling) combined with hypotension, respiratory compromise, or persistent gastrointestinal symptoms
2. Hypotension or respiratory compromise alone
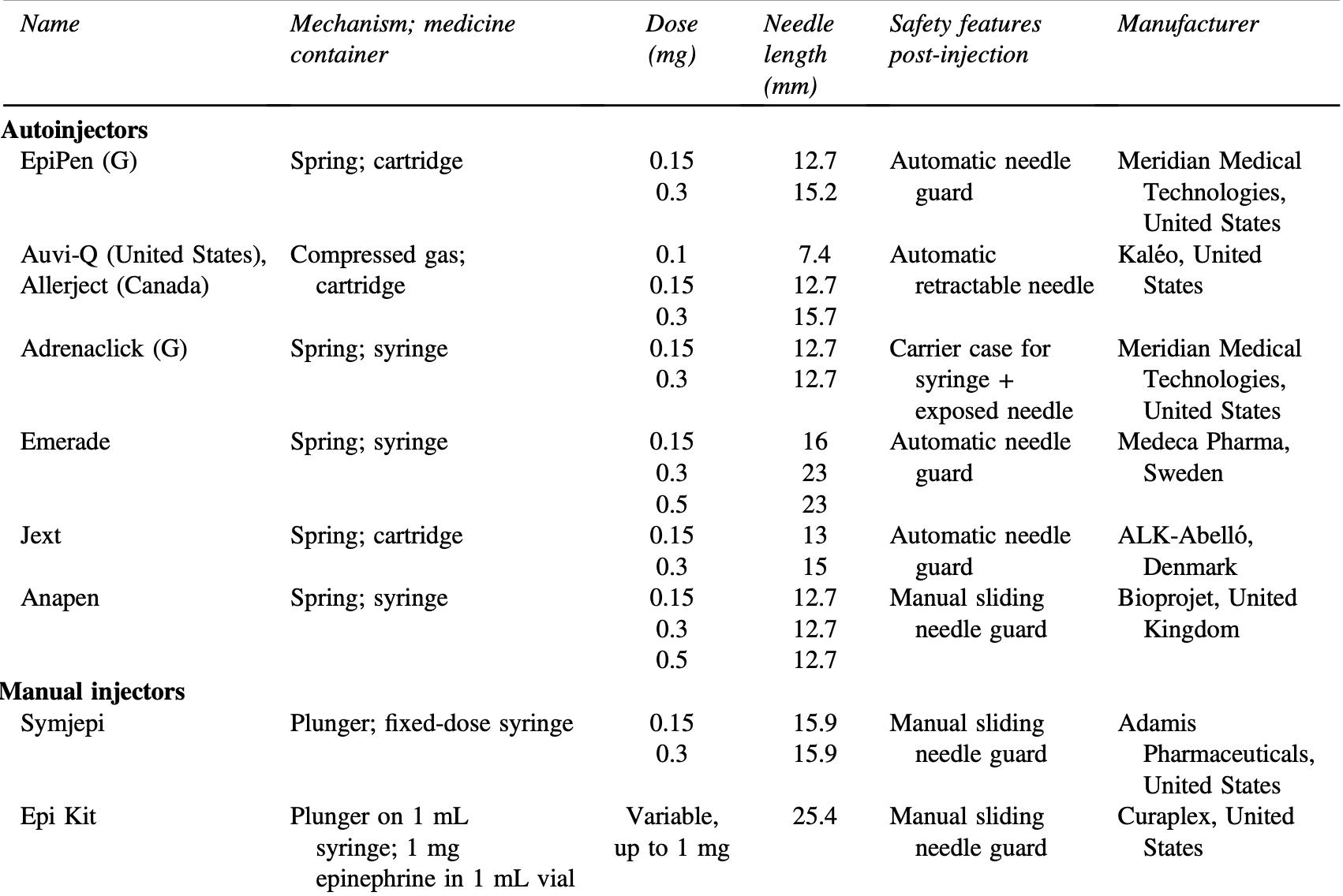
“Epinephrine is the primary treatment because it reverses clinical symptoms and promotes resolution by stabilizing mast cells.”
Notably, 10–20% of cases present without skin or mucosal involvement. While most reactions occur within minutes, some may be delayed by several hours.
Special Considerations
Several less common forms of anaphylaxis are important to recognize. Exercise-induced anaphylaxis is thought to result from increased plasma osmolarity leading to mast cell degranulation. Symptoms often begin with activity and improve with rest.
Alpha-gal syndrome is a red meat allergy transmitted by the Lone Star tick. Patients react to the sugar molecule galactose-α-1,3-galactose, which is found in red meat. Reactions may also occur with mammalianderived products, including porcine valves, heparin, and gelatincontaining medications. Symptoms typically develop hours after ingestion, often delaying diagnosis. Although historically confined to the southeastern United States, the Lone Star tick has demonstrated a clear northward expansion.
Management
Most cases resolve with appropriate treatment. However, ongoing or repeated exposure may prevent full recovery. Early management includes removal of the offending agent. Previous guidance recommended removing stingers without pinching to avoid additional venom release; however, current evidence supports rapid removal by any method.

Casual contact with food allergens rarely triggers reactions, though aerosolized exposure (e.g., cooking vapors) can cause anaphylaxis. Supportive care remains essential but may be limited in backcountry settings.
Epinephrine is the primary treatment. It reverses clinical symptoms and promotes resolution by stabilizing mast cells. Delays in administration are associated with fatal outcomes. Epinephrine is typically dosed at 0.3 mg IM every 5 minutes as needed, with the anterolateral thigh as the preferred site. The deltoid is a reasonable alternative. Some evidence suggests that a 0.5 mg dose may lead to more rapid symptom resolution.
Adjunctive therapies, including steroids and antihistamines, are secondary treatments. Secondgeneration antihistamines are preferred over diphenhydramine.
Autoinjectors, such as EpiPens, are commonly used in wilderness settings but may be more expensive than generic alternatives or prefilled syringes. While vials are less costly, they carry a higher risk of dosing errors when prepared in emergencies. Prefilling and clearly labeling syringes in advance is a safer alternative. Autoinjectors typically require 3 seconds of firm pressure to deliver the
Pulse Points
Key clinical and practice takeaways:

full dose. They can be administered through thin clothing but may not penetrate thicker layers.
Epinephrine should ideally be stored at 20–25°C but remains stable at higher temperatures for several days. If only expired epinephrine is available, it should still be used; studies suggest 80–90% potency is retained for up to 24 months after expiration. In emergencies, autoinjector casings can be opened to access remaining medication, which may contain additional doses. However, caution is required due to the spring-loaded mechanism.
Inhaled epinephrine is ineffective for anaphylaxis, and intranasal epinephrine lacks sufficient evidence for recommendation. Patients taking beta-blockers may have a reduced
• Epinephrine first, fast, and repeat as needed—delays are consistently associated with worse outcomes and preventable deaths.
• Do not rely on skin findings—up to 20% of anaphylaxis cases present without hives or mucosal involvement.
• In the wilderness, preparation is management—carry, prefill, and clearly label epinephrine to reduce dosing errors under pressure.
• Expired epinephrine is better than none—clinically meaningful potency is often retained well beyond the expiration date.
• Evacuate when in doubt—limited monitoring and risk of biphasic reactions make conservative disposition decisions the safer choice.
response to epinephrine and may require glucagon.
Disposition and Observation
Biphasic reactions—recurrence without reexposure—occur in approximately 5% of cases. These reactions can develop up to 78 hours after the initial event but most occur within 12 hours. They are more likely in severe presentations or when there is an incomplete response to treatment.
Although extended observation has traditionally been recommended, current evidence suggests that low-risk patients—those with mild reactions, complete symptom resolution, and no high-risk features— may only require approximately 1 hour of observation.
In the backcountry, evacuation is generally recommended due to limited access to advanced care. However, decisions should be individualized, and observation may be reasonable in select, low-risk scenarios.
ABOUT THE AUTHOR

Dr. Watkins is an emergency medicine physician at Cleveland Clinic Akron General, where he serves as associate program director for the residency and director of wilderness medicine. He also serves as associate director of academics for the Cuyahoga Valley Wilderness Medicine Group and chair of the SAEM Wilderness Medicine Interest Group, and is a member of the student and resident education committee for the Wilderness Medical Society.



























The Power of Possibility in Action: SAEMF Awards
$1 million+
to Advance Emergency Care
The SAEM Foundation (SAEMF), the philanthropic arm of SAEM, exists to power what’s possible— bridging critical research funding gaps in emergency medicine, advancing the science and innovation at the heart of the specialty, and cultivating the next generation of research and education leaders.

Learn more about SAEMF’s grantees on our website.
We invite you to join the SAEMF Board of Trustees and our generous community of donors in celebrating our newest cohort of grantees—awarded more than $1 million in research and education funding. These investigators embody the true Power of Possibility: transforming bold questions into discoveries that will shape the future of emergency care.
Their work spans the breadth and urgency of our field:
• Artificial Intelligence and Advanced Analytics: Improving pulmonary embolism diagnosis, optimizing care delivery across settings, and modeling emerging pathogen exposure
• Trauma and Critical Care: Targeting biologic pathways to improve perfusion and advancing real-time resuscitation strategies
• Simulation, Education, and Training: Advancing simulation-based mastery, ultrasound curriculum design, and resident learning optimization
• Public Health and Systems Science: Innovating in wastewater surveillance, ED workload saturation modeling, and patient throughput
• Vulnerable Populations: Addressing geriatric falls, pediatric CNS infections, behavioral health, elder abuse, and inclusive research participation
• Global and Emergency Preparedness: Strengthening disaster recovery, humanitarian response, and community-based participatory research
Beyond discovery, these grants are catalysts. They foster mentorship and collaboration, and connect emerging investigators with established leaders—accelerating careers while advancing the field. For many recipients, this support represents a pivotal step forward, turning potential into progress.
To our donors—thank you for bringing the Power of Possibility to life. To our grantees—congratulations. We look forward to the impact ahead.
Annual Alliance Benefits
Annual Alliance donors help unlock opportunities that shape the future of our specialty while receiving visible recognition for their giving*:
Recognition on the SAEMF website
Visibility in SAEM Pulse and across SAEM social channels
Challenge donor recognition for all Challenges that donor qualifies to participate in Special Annual Meeting recognition — early notice for registration and housing, VIP Lounge access, invite to networking events, airport transportation, and more — based on Annual Alliance level
Power More Possibilities: Become An SAEMF Annual Alliance Donor
By renewing your Annual Alliance gift-or becoming a member for the first time-you help turn more possibility into progress, fueling innovative ideas, developing future research leaders, and strengthening the future of academic emergency medicine. Your commitment connects you to a community united by shared purpose, and is recognized in thoughtful ways throughout the year.
Donate Today!
Or, email Julie Wolfe, CFRE at jwolfe@saem.org, to pledge your support and donate later in the year.

AACEM Chairs Are Powering Possibilities in Emergency Care
Thank you, AACEM Chairs! Since 2019, when the Chairs’ Challenge started, AACEM members have contributed mightily to support and train emergency medicine researchers and educators through SAEM Foundation — demonstrating the power of possibility in action. This year was no different – AACEM members exceeded the goal!
2026 Chairs’ Challenge Results: $188,506 committed! 97 Chairs and Chairs Emeriti Donors! 21 states green! 10 new AACEM Chairs donated!
The 2026 Chairs' Challenge Map
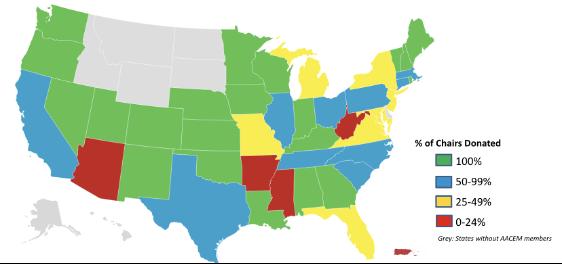
Your leadership is advancing academic emergency medicine—funding research, developing future leaders, and driving innovation through SAEM Foundation initiatives. Because of Chairs’ Challenge donors, SAEMF has funded over $1 million in research and education grants in each of the last two years. With your continued support, we look forward to doing it again! The map may be complete. The SAEMF’s mission is not. If you haven’t yet given, your leadership still matters—now more than ever. Your gift today helps power the next breakthrough in emergency care. saem.org/donate
The Power of Possibility
IT’S TIME FOR THE VICE CHAIRS’ CHALLENGE
SAEMF’s Vice Chairs’ Challenge showcases the generous giving that comes from our vice chairs each year and serves as a rallying call to unite vice chairs in support of more funding for future EM researchers and educators.
Become
a Vice Chairs’ Challenge donor www.saem.org/donate or email Julie at jwolfe@saem.org to pledge support

Donate or pledge a gift of $250 by August 31, 2026 and be recognized: Help your Vice Chairs Interest Group win a special celebration at SAEM27, if the Interest Group wins a category of the 2026 SAEMF Challenge and raises its goal of $35,000 in new pledges and donations before August 31, 2026
With the opportunity to network with grantees and leaders at the SAEMF’s Coffee & Networking session at SAEM26 when you become a Mentor Donor of the Annual Alliance through a donation/pledge of $1,000 in 2026, if committed by May 13, 2026
With your name in lights on the SAEMF’s digital donor display at SAEM26 Visit saem.org/vicechairschallenge for details Thanks for considering a donation today !
“I wanted to take this opportunity to thank everyone at the SAEM Foundation and all the donors for supporting my project…This [work] will better prepare our trainees to identify specific pathologies such as myocardial infarction or heart attack in diverse populations and ultimately to improve health equities in our community.”
- Marta Rowh, MD, PhD, MPH
2025 SAEMF Education Project Grantee
BRIEFS & BULLET POINTS
FEATURED NEWS
Record-Breaking Match: 3,058
New Interns Fuel the Future of Emergency Medicine
The emergency medicine community is celebrating a milestone year! A record 3,058 newly matched interns are joining our specialty — the largest cohort ever — alongside a remarkable 96% fill rate across programs. Interest remains strong, with growing numbers of MD and DO seniors choosing emergency medicine and aligning with our mission and values. As we welcome these future leaders, we also remain focused on workforce challenges and the need to strengthen training pathways and advocacy. Thank you to the educators and mentors shaping what’s next — because emergency medicine’s best days are ahead.
Sign Up Is Open for the July 20-23 Virtual Residency & Fellowship Fair!
Residents and medical students — meet online with top residency and fellowship programs from across the country, all of them ready to share insights and guide you through the application process. The fair is free and open to all residents and medical students. View the updated list of participating programs and sign up today to meet with as many as you'd like!
Residency and Fellowship Programs: Recruit Top Candidates — All in One Place! Maximize your recruitment impact by participating in the SAEM RAMS Virtual Residency & Fellowship Fair, July 20-23, 2026. Connect with hundreds of qualified candidates in this streamlined, cost-effective virtual fair. Showcase your program and evaluate fit efficiently. Space is limited — register your program today!
SAEM JOURNALS
Two-Part Geriatric Emergency Medicine Collection Launches in Academic Emergency Medicine
Academic Emergency Medicine spotlights care for older adults with a new two-part special collection, “Geriatric Emergency Medicine.” The first set of articles is available now, with a second to follow. This curated compendium features original
research, commentaries, reflections, and more — highlighting best practices in emergency care for an aging population. It brings together innovative research, impactful education, and forward-thinking clinical approaches in one accessible resource. The collection also features the updated Geriatric Emergency Department Guidelines and supporting systematic reviews, advancing evidence-based care and shaping the next generation of clinicians, educators, and researchers.
SAEM Journals Appoint 20262027 Resident and Fellow Editors



Roland Zemla, MD, PhD, has been selected for the Academic Emergency Medicine (AEM) Resident Editor-in-Training Program and will serve on the AEM Editorial Board for the 2026–2027 term. Eileen Williams, MD, and Niresh Perera, MD, have been selected for the Academic Emergency Medicine Education and Training (AEM
E&T) Fellow Editor-in-Training Program and will serve on the AEM E&T Editorial Board. Chosen from a competitive applicant pool, these editors will gain hands-on experience in peer review, manuscript editing, and academic publishing while receiving dedicated mentorship. Congratulations to Drs. Zemla, Williams, and Perera on this well-deserved honor.
SAEM REGIONAL MEETINGS
Secure Your Spot for the SAEM Southeastern Regional Meeting
Join us Saturday, July 11, 2026, at Lakeland Regional Medical Center in Lakeland, Florida, for the free SAEM Southeastern Regional Meeting. Emergency medicine residents and faculty will present research, compete in the “EM Madness” knowledge competition, and share scholarly activity in a collaborative, career-boosting forum. Enjoy e-poster sessions, keynote address by Dr. Neha Raukar, top abstract presentations, and networking opportunities. Don’t miss this chance to connect, learn, and compete! Register now!
Essential SAEM Resources for Building Your Academic Emergency Medicine Career
Advance your academic emergency medicine career with SAEM’s expertdeveloped resources. Whether you’re a student, resident, fellow, or faculty member, these guides provide practical tools and insights to help you succeed in education, research, and leadership.
The Reason for Research
A practical guide for medical students, residents, and junior faculty pursuing emergency medicine research. It outlines career pathways, training requirements, and strategic advice from experts to help build a meaningful and impactful research career.
Speakers Bureaus
SAEM’s four speakers’ bureaus connect organizations with expert presenters on a wide range of emergency medicine topics. From clinical care and
research to DE&I, gender equity, and palliative medicine, each bureau offers specialized, high-quality programming.
Boarding and Crowding Toolkit
A digital resource offering strategies to address emergency department boarding and crowding. It covers solutions such as telehealth optimization, observation units, and system-wide patient flow to improve efficiency and patient care.
Roadmap to Emergency Medicine Research Funding
A streamlined guide to help new researchers navigate funding opportunities in emergency medicine. It highlights sources ranging from institutional support to federal grants, including NIH funding.
Dr. Roland Zemla Dr. Eileen Williams Dr. Niresh Perera
SAEM FOUNDATION
SAEMF Grant Applications Now Open
The SAEM Foundation (SAEMF), in partnership with SAEM, annually invests in the future of emergency medicine through competitive research and education grants. To date, we have supported more than 600 emergency medicine academicians with over $15.5 million in funding—advancing innovation, developing careers, and building pathways for future emergency medicine research and education leaders. For the upcoming cycle, SAEMF expects to award over $1 million to SAEM members to support career development and tackle critical challenges in emergency care. Eligible projects must align with one of the grant categories below and reflect the shared mission of SAEM and SAEMF. Explore the opportunities below and apply by 5 p.m. CT on August 1, 2026.
• Research Training Grant (RTG)$300,000
• Research Large Project Grant (LPG)$150,000
• Updated! Education Research Training Grant (ERG) - $100,000
• SAEMF Emerging Infectious Disease and Preparedness Grant - Up to $100,000
• Updated! SAEMF/ED Benchmarking Alliance Clinical Operations Research Grant - $50,000
• NEW! The NAEMSP / SAEMF Innovations in Prehospital Care Pilot Grant, In Memory of E. Brooke Lerner, PhD - $50,000
• SAEMF ARMED Pilot Grant - $25,000
• SAEMF ARMED MedEd Pilot Grant$25,000
• Education Project Grant (EPG) - $20,000
• Geriatric Emergency Medicine Research Catalyst Grant, Supported by Michelle Blanda, MD and Donors - $10,000
• SAEMF/Clerkship Directors in Emergency Medicine (CDEM) Innovations in Undergraduate Emergency Medicine Education Grant$8,000
• MTF/SAEMF Toxicology Research Grant - $20,000
• SAEMF/Academy of Emergency Ultrasound (AEUS) Research Grant$10,000
• SAEMF/Global Emergency Medicine Academy (GEMA) Research Pilot Grant - $10,000
Neuro-EM Scholars Program: 2026 Applications Open
The Neuro-EM Scholars Program will fund four new K12 scholars beginning July 2026, providing up to three years of support with 75% protected research time.
Apply for
2026
Early-career emergency medicine physicians focused on neurological disorders commonly treated in the prehospital and emergency department settings may apply to the K12 Scholar Program or the Pipeline Program.
K12 applicants and selected Pipeline participants will be invited to attend the Neuro-EM Retreat in Ann Arbor, MI from December 1-4, 2026, joining current K12 scholars, Neuro-EM leaders, and NIH representatives.
K12 Program
Clinically practicing emergency medicine physicians within their first two years of a faculty position (after residency
or fellowship training) at the time of application.
• Up to $115,000 salary support annually (75% effort) + fringe (up to 3 years)
• $40,000/year for research and career development (up to 3 years)
• Key dates:
o Aug. 14, 2026: LOI form and draft aims page due
o Oct. 15, 2026: Full K12 application due
Pipeline Program
For senior EM residents, fellows, and first-year faculty interested in neurological sciences research.
• Includes funded attendance at the Neuro-EM Retreat.
• Key date:
o Oct. 1: Nomination form and candidate CV due from chair, division chief, or program director
• SAEMF/Academy for Women in Academic Emergency Medicine (AWAEM) Research Grant - $10,000
• SAEMF/Academy for Diversity and Inclusion in Emergency Medicine (ADIEM) Research Grant - $6,000
• SAEMF/Simulation Academy Novice Research Grant - $5,000
• SAEMF/Resident and Medical Students (RAMS) Research Grant - $2,500 - $5,000
• NEW! Dr. Gregory L. Henry, MD / RAMS Resident Research Grant - $5,000
• The Ali and Danielle Raja RAMS Medical Student Research Grant - Grant of $2,500 plus scholarship to defray costs of participation as a Medical Student Ambassador at the SAEM’s Annual Meeting
• The David E. Wilcox, MD, FACEP Endowed Scholarships - Scholarship: $1,250 bestowed upon the highest scoring RAMS Resident and RAMS Medical Student Research Grant recipients annually
Not all categories are offered every year.
Neuro-EM Retreat (Dec. 1–4, 2026 | Ann Arbor, MI)
Selected applicants participate in research feedback, grant writing sessions, and networking with national leaders.
Learn More
Visit neuroemscholars.org for details, webinars, and application information, or connect with program leaders at the SAEM Annual Meeting. For details, email Meagan Ramsey.
The Neuro-EM K12 Program is funded by the National Institute of Neurological Disorders and Stroke (NINDS), with select scholar support from the National Institute on Drug Abuse (NIDA) and the National Institute on Aging (NIA). The Neuro-EM Pipeline Program is supported by the National Foundation of Emergency Medicine.
SAEM REPORTS
COMMITTEES
Awards Committee
The Awards Committee oversees and selects recipients for SAEM and RAMS awards at the Annual Meeting, recognizing excellence in academic emergency medicine across leadership, service, research, education, patient care, and advocacy.
Updates/Status
Over the past three years, the committee has demonstrated thoughtful and impactful work in recognizing excellence in academic emergency medicine. It standardized letters of recommendation and improved clarity in scored domains, helping nominees better understand award criteria while enabling letter writers to address relevant elements more effectively. These efforts contributed to greater institutional diversity among applicants and an increase in submissions across award categories.
The committee also helped establish new awards recognizing emerging areas of excellence, including the SAEM Outstanding Departmental Wellness Award, under the leadership of Vicki Zhou, MD. In addition, members worked to standardize scoring rubrics for high-volume awards using achievement anchors, laying the groundwork for future enhancements, including potential use of artificial intelligence.
The committee expresses appreciation to its members for their dedication, insight and care in this work and welcomes Michelle Lin, MD, as incoming chair.
Ethics Committee
The Ethics Committee reviews conflicts of interest and advises the SAEM board on dispute resolution. It ensures the Society’s integrity by annually reviewing SAEM’s Conflict of Interest Policy and monitoring relevant policies from other societies and expert recommendations.
Updates/Status
The Ethics Committee has had a productive year marked by thoughtful dialogue and meaningful work across multiple initiatives. In collaboration with the Academy for Diversity and Inclusion in Emergency Medicine (ADIEM) and the Pediatric Emergency Medicine (PEM) Interest
Group, committee members Samantha Chao, MD; Josh Davis, MD; Monisha Dilip, MD; Dina Wallin, MD; and Amy Ziedan, MD, will present the didactic session, “Between a Rock and a Hard Place: Applying Ethical Frameworks to Immigration-Related Stressors in the Emergency Department,” at the national meeting in May. The session demonstrates the application of ethical frameworks to complex, real-world challenges, including those related to Immigration and Customs Enforcement presence in the emergency department.
An additional sponsored didactic by Kevin McGurk, MD; Edward Durant, MD; and Jolion McGreevy, MD, will address the ethics of hospital closures, a growing issue affecting access to quality emergency care.
The committee will also sponsor a half-day workshop, “The Ethics of Intelligence: Navigating Artificial Intelligence in Emergency Medicine Education.” This scenario-based session will focus on responsible integration of artificial intelligence into emergency medicine practice.
The committee continues to demonstrate a strong commitment to excellence in education and patient care through the depth and diversity of its work.
ACADEMIES
Academy of Administrators in Academic Emergency Medicine (AAAEM)
The Academy of Administrators in Academic Emergency Medicine (AAAEM) supports professionals managing the administrative and business functions of academic emergency medicine departments, including patient care, education, research, and residency program administration.
Updates/Status
The AAAEM Benchmark Committee presented data from the FY25 academic year annual benchmark surveys at the Chair/Administrator Retreat in March. These surveys are used to benchmark academic emergency medicine departments’ and divisions’ clinical, education and research missions, as well as to collect data on
faculty and fellow compensation and clinical and academic productivity.
AAAEM will share select results from the FY25 data collection at the SAEM booth during SAEM26. Attendees are encouraged to stop by to learn more about the surveys and AAAEM.
For questions or assistance regarding the AAAEM benchmark surveys, contact Alyssa Tyransky at alyssa.tyransky@osumc.edu
Academy of Emergency Medicine Pharmacists
The Academy of Emergency Medicine Pharmacists (AEMP) champions excellence, innovation, and advancement of emergency medicine pharmacy practice through advocacy, education, research, and collaboration. Its purpose is to advance emergency medicine pharmacy practice by fostering a community of dedicated professionals, driving research, enhancing training programs and disseminating best practices to improve emergency medicine pharmacy practice and patient care.
Join
Updates/Status
• AEMP looks forward to AEMP26 at SAEM26, with programming spanning three days of the conference and open to all attendees.
• Congratulations to newly matched postgraduate year 2 (PGY-2) pharmacy residents entering careers in emergency medicine and critical care, as well as new toxicology fellows.
Global Emergency Medicine Academy
The Global Emergency Medicine Academy (GEMA) aims to enhance emergency medical care worldwide. As global emergency medicine rapidly grows, GEMA supports this expansion through several committees/task forces, reflecting the increasing global interest in the specialty.
Updates/Status
• GEMA will host several upcoming webinars. View the schedule
SAEM Reports continued on Page 176
Academy
Interest Group!

continued from Page 175
• Individuals interested in a global emergency medicine fellowship are encouraged to reach out early for the upcoming application cycle. For more information, email GEMA@saem.org or visit our fellowship webpage.
• GEMA looks forward to the SAEM Annual Meeting. Join the GEMA business meeting on Wednesday, May 20, from 11 a.m. to 12:50 p.m., which will include a GEMA Science Fair featuring mentorship and discussion of current topics in global emergency medicine.
INTEREST GROUPS
Climate Change and Health Interest Group
The Climate Change and Health Interest Group at SAEM tackles the intersection of climate change and public health, focusing on research, education, and advocacy. It promotes sustainable practices
and policies to mitigate climate-related health impacts through a multidisciplinary approach.
Updates/Status
• Adrian Cois, MD, was elected chair of the Climate Change and Health Interest Group for the 2026–2028 term.
• Join our annual in-person meeting at SAEM26 on Tuesday, May 19, at 3:30 p.m.
• Attend the our sponsored didactic session at SAEM26 titled “Black-Legged, Lone Star, American Dog Ticks, Oh My!”
Oncologic Emergencies Interest Group
The Oncologic Emergencies Interest Group aims to raise awareness of supportive care guidelines while enhancing education and research on oncologic topics. Its focus is on improving the management and understanding of emergencies related to cancer care.

SAEM CONSULTATION SERVICES
Updates/Status
• Join our in-person meeting at SAEM26 on Tuesday, May 19, from 4 to 4:50 p.m.
• Our interest group is partnering with AEMP for an SAEM26 didactic session titled “Double the Fight, Double the BiTE: A Toxic Tale of Bispecific T-Cell Engaging Antibodies,” scheduled for Tuesday, May 19, from 8 to 8:20 a.m.
• Congratulations to Lindsay, MD, and Wattana, MD, co-editors of Oncologic Emergency Medicine Clinical Cases Illustrating Key Concepts, published by Cambridge University Press in April 2026. The book features clinical cases highlighting key oncologic emergencies authored by SAEM Oncologic Emergencies Interest Group members.
Operations Interest Group
The Operations Interest Group unites SAEM members to enhance the functioning of emergency departments for patients and staff. It fosters community and encourages sharing ideas to discover innovative approaches for managing departments in today’s challenging healthcare environment.
Updates/Status
• An interest group’s member institution implemented a systemwide telemedicine urgent care–emergency department integration model using a teletriage emergency physician based in a centralized command center within the department of emergency medicine. The pilot demonstrated nearly a 16% reduction in urgent care–to–emergency department transfers, improved resource utilization, enhanced patient and provider satisfaction, and avoided “double transfers,” with no 72-hour return visits among the first 240 eligible patients.
• Current or prospective emergency department administrative or leadership fellows interested in participating in a related scoping review are encouraged to contact Nick Tsipis, MD, MPH, at netsipis@carilionclinic.org
• SAEM26 programming includes our sponsored didactic session “Mathematical Modeling for Emergency Department Operations: Bridging Theory and Practice,” scheduled for May 19 from 3 to 3:50 p.m. in International Hall 2 (Level I).
• Join our annual in-person meeting at SAEM26 on Wednesday, May 20, from 11 to 11:50 a.m.
Pediatric Emergency Medicine Interest Group
The Pediatric Emergency Medicine Interest Group aims to enhance pediatric emergency care by advancing science and education. Its mission focuses on improving care through training, education, and fostering collaboration between general and pediatric emergency medicine specialists.
Updates/Status
• Join our in-person meeting at SAEM26 on Tuesday, May 19, at 8 a.m., featuring guest speaker Jim Holmes, MD, and announcement of award winners.
• Our interest group is sponsoring two SAEM26 didactic sessions: “Leaning Into the Gray: Navigating Uncertainty in Pediatric Emergency Care” on Tuesday, May 19, at 1 p.m., and “These Studies Will Change Your Practice (and Teaching): PEM Edition” on Thursday, May 21, at 9 a.m.
• Congratulations to Eva Delgado, MD, and colleagues for launching the Pediatric Emergency Medicine Resident Rotation Directors (PEM RaD) Community of Practice. This initiative supports faculty leading pediatric emergency medicine experiences for emergency medicine residents and promotes collaboration across disciplines. Those interested in participating may contact Dr. Delgado through the SAEM Community.
Wilderness Medicine Interest Group
The Wilderness Medicine Interest Group at SAEM brings together emergency physicians to address the challenges of medicine in wilderness and austere environments. It fosters research, education, and collaboration on topics like outdoor injuries and environmental emergencies, enhancing skills for resource-limited settings.
Updates/Status
• Multiple workshops and didactic sessions sponsored by our interest group will be offered at SAEM26. A trail map will be available with the final schedule to help attendees locate sessions.
• MedWAR returns this year, with teams forming and participation encouraged.
• A group dinner is planned immediately following MedWAR. Additional details will be shared soon.
ACADEMIC ANNOUNCEMENTS
Dr. Nathaniel R. Hunt Appointed Medical Director of Survival Flight

Nathaniel R. Hunt, MD, clinical assistant professor of emergency medicine, The University of Michigan Department of Emergency Medicine, has been appointed medical director of Survival Flight. Dr. Hunt brings extensive experience in prehospital and emergency care, with a career spanning paramedicine, nursing and academic emergency medicine. Dr. Hunt serves as director of the EMS fellowship program and remains active in technical rescue, hazardous materials response, disaster medicine and search-and-rescue operations, including service with Michigan Task Force One. In his new role, he will oversee clinical operations, education and quality initiatives supporting Michigan Medicine’s air medical transport program.
Dr. Kevin Ward Recognized with National Appointments and Innovation Achievements

Kevin Ward, MD, director of the Weil Institute for Critical Care Research and Innovation and professor of emergency medicine and biomedical engineering at the University of Michigan, has received several recent national appointments and honors. He was appointed to the American College of Surgeons Performance Improvement and Patient Safety Committee and the NIH National Institute of Neurological Disorders and Stroke Common Data Elements Committee for Traumatic Brain Injury. He was also named adjunct professor at the Uniformed Services University. In addition, Dr. Ward was awarded four new U.S. patents for innovations in trauma and critical care.
Dr. Daria Falkowitz Appointed Inaugural Medical Toxicology Fellowship Director

Daria Falkowitz, DO, has been appointed the inaugural fellowship director of a newly ACGME accredited Medical Toxicology Fellowship at Hackensack University Medical Center. Dr. Falkowitz is recognized for her clinical expertise in medical toxicology and her commitment to education and interdisciplinary collaboration. The fellowship, with its inaugural class expected in July 2027, will support institution-wide consultation across pediatrics, internal medicine, critical care and psychiatry in the management of complex poisonings, envenomations and substance-related conditions.
Dr. Laura R. Hopson Installed as Josiah Macy Jr. Distinguished Educator Professor

Laura R. Hopson, MD, MEd, clinical professor and associate chair of education in the Department of Emergency Medicine, at the University of Michigan, has been installed as the Josiah Macy Jr. Distinguished Educator Professor. The honor recognizes her leadership and lasting impact in medical education. A nationally respected educator, Dr. Hopson is known for her contributions to faculty development, learner assessment and advancing excellence in academic emergency medicine.
Dr. Nikki Binz Receives Parker J. Palmer Courage to Teach Award

Nikki Binz, MD, has received the Parker J. Palmer Courage to Teach Award at the 2026 Accreditation Council for Graduate Medical Education (ACGME) Annual Educational Conference in San Diego. The award recognizes program directors who foster innovation and serve as exemplary role models in graduate medical education. Dr. Binz is a clinical associate professor in the University of North Carolina at Chapel Hill Department of Emergency Medicine, vice chair of education, and director of the Education Fellowship. Dr. Binz previously served as emergency medicine residency program director at UNC at Chapel Hill for 10 years, where she graduated more than 100 emergency physicians.
Dr. Stephanie Stapleton Promoted to Clinical Associate Professor at Boston University

Stephanie Stapleton, MD, has been promoted to clinical associate professor at Boston University Chobanian & Avedisian School of Medicine. A dedicated clinician educator, she is recognized for her leadership in simulation in emergency care, her commitment to medical education and her focus on patient-centered practice.
Dr. Benjamin Weston Promoted to Professor with Tenure at Medical College of Wisconsin

Benjamin Weston, MD, has been promoted to professor with tenure of emergency medicine at the Medical College of Wisconsin Medical School, effective July 1, 2026. His work reflects sustained excellence in academic emergency medicine, research and education.
Dr. Nathaniel R. Hunt
Dr. Laura R. Hopson
Dr. Nikki Binz
Dr. Stephanie Stapleton
Dr. Benjamin Weston
Dr. Kevin Ward
Dr. Daria Falkowitz
Dr. Lana Shaker Promoted to Associate Program Director at Hackensack University Medical Center

Lana Shaker, MD, has been promoted to associate program director of the emergency medicine residency program at Hackensack University Medical Center. Since joining the faculty in 2022, she has demonstrated strong leadership in resident mentorship and medical education. Dr. Shaker is pursuing a Master of Education in the Health Professions at Johns Hopkins University. She is recognized for her commitment to advancing graduate medical education and supporting program growth.
Dr. Guy Carmelli Appointed Assistant Program Director at University of Miami/ Jackson Health System

Guy Carmelli, MD, MSEd, has been appointed assistant program director for the University of Miami/Jackson Health System Emergency Medicine Residency Program. Dr. Carmelli is recognized for his commitment to medical education, mentorship and resident development, and will play a key role in advancing the program’s educational mission.
Dr. Michael Quinn Appointed Interim Assistant Program Director at Hackensack University Medical Center

Michael Quinn, DO, has been appointed interim assistant program director of the emergency medicine residency program at Hackensack University Medical Center. Since joining the faculty in 2022, he has contributed significantly as clerkship director and as a core faculty member of the Clinical Competency Committee. Fellowship-trained in medical simulation, Dr. Quinn is known for his engaging, hands-on approach to resident education.
Dr. Christopher O. Hoyte
Named Chair of Emergency Medicine at University of Florida

Christopher O. Hoyte, MD, MBA, has joined the University of Florida College of Medicine as chair of the Department of Emergency Medicine. An expert in medical toxicology, Dr. Hoyte brings more than two decades of experience and most recently served in multiple leadership roles over 16 years at the University of Colorado. He is recognized for his expertise in toxicology, education and departmental leadership.
Dr. Aleksandr M. Tichter Appointed Interim Program Director at Hackensack University Medical Center

Aleksandr M. Tichter, MD, has been appointed interim program director of the emergency medicine residency program at Hackensack University Medical Center. He joined the department in 2024 as vice chair of education. Dr. Tichter previously served for more than a decade as associate program director at NewYorkPresbyterian and for over five years as program director at Baylor College of Medicine. He is recognized for his leadership in graduate medical education, curriculum innovation and resident mentorship.
Dr. Meera Muruganandan Promoted to Clinical Associate Professor of Emergency Medicine

Meera Muruganandan, MD, has been promoted to clinical associate professor of emergency medicine at Boston University Chobanian & Avedisian School of Medicine. She is recognized for her leadership in emergency ultrasound education and serves as director of the ultrasound section at Boston Medical Center. A former fellowship director, Dr. Muruganandan is also known for her global health contributions in point-ofcare ultrasound.
Dr. Taylor Sonnenberg Promoted to Associate Professor at Medical College of Wisconsin

Taylor Sonnenberg, MD, has been promoted to associate professor of emergency medicine at the Medical College of Wisconsin Medical School, effective July 1, 2026. Dr. Sonnenberg also serves as chief in the Division of Global and Population Health. She is recognized for contributions to clinical care, education and academic emergency medicine.
Dr. Jamie Jasti Selected for MACC-SIREN Faculty Fellowship in Acute Care Research

Jamie Jasti, MD, assistant professor in the Department of Emergency Medicine at the Medical College of Wisconsin Medical School, has been selected for the MidAmerica CTSA Consortium SIREN (MACCSIREN) Faculty Fellowship in Acute Care Research. This competitive, NIH-funded program provides 20% salary support to early-career physician investigators pursuing clinical trials in emergency and acute care settings.
Dr. Lana Shaker
Dr. Aleksandr M. Tichter
Dr. Meera Muruganandan
Dr. Taylor Sonnenberg
Dr. Jamie Jasti
Dr. Guy Carmelli
Dr. Michael Quinn
Dr. Christopher O. Hoyte
NOW HIRING
Accepting ads for our “Now Hiring” section!
Deadline for the next issue of SAEM Pulse is June 1. For specs and pricing, visit the SAEM Pulse advertising webpage.




Presented by Dr. Andrew M. Fine and Dr. Richard Rothman
Tuesday, May 19 | 12:00–12:50 PM


Presented by Dr. Jacob Manteuffel and Dr. Patrick Grace
Wednesday, May 20 | 11:30 AM–12:30 PM







Penn State Health Emergency Medicine
About Us: Penn State Health is a multi-hospital health system serving patients and communities across central Pennsylvania. We are the only medical facility in Pennsylvania to be accredited as a Level I pediatric trauma center and Level I adult trauma center. The system includes Penn State Health Milton S. Hershey Medical Center, Penn State Health Children’s Hospital and Penn State Cancer Institute based in Hershey, Pa.; Penn State Health Hampden Medical Center in Enola, Pa.; Penn State Health Holy Spirit Medical Center in Camp Hill, Pa.; Penn State Health Lancaster Medical Center in Lancaster, Pa.; Penn State Health St. Joseph Medical Center in Reading, Pa.; Pennsylvania Psychiatric Institute, a specialty provider of inpatient and outpatient behavioral health services, in Harrisburg, Pa.; and 2,450+ physicians and direct care providers at 225 outpatient practices. Additionally, the system jointly operates various healthcare providers, including Penn State Health Rehabilitation Hospital, Hershey Outpatient Surgery Center and Hershey Endoscopy Center.
We foster a collaborative environment rich with diversity, share a passion for patient care and have a space for those who share our spark of innovative research interests. Our health system is expanding and we have opportunities in both academic hospital as well community hospital settings.

Benefit highlights include:
• Competitive salary with sign-on bonus
• Comprehensive benefits and retirement package
• Relocation assistance & CME allowance
• Attractive neighborhoods in scenic central Pa.





Emergency Medicine Fellowships Creating leaders in health care
ADVANCE YOUR CAREER WITH FELLOWSHIP
AT THE OHIO STATE UNIVERSITY
WE OFFER FELLOWSHIPS IN:
• ADMINISTRATION
• EMS
• GERIATRICS
• GLOBAL HEALTH
• MEDICAL EDUCATION
• POPULATION HEALTH/SOCIAL EM
• RESEARCH
• ULTRASOUND
ABOUT OHIO STATE EMERGENCY MEDICINE
Learn more about our fellowships

Our department Is built on four key mission areas: providing excellent clinical care, educating residents, fellows, and medical students, conducting clinical and laboratory research, and developing top-tier faculty to advance emergency medicine. The department comprises over 80 physicians with experience across the spectrum of EM involved in clinical practice, education, research, and scholarly activities. More than half of the faculty are clinical educators dedicated to teaching at various levels, including medical students, residents, fellows, and faculty development in the College of Medicine.
ABOUT COLUMBUS

Columbus is one of the fastest-growing cities in the Midwest, offering the perfect blend of big-city opportunities and small-town friendliness. Home to The Ohio State University, a thriving arts and food scene, diverse neighborhoods, and an affordable cost of living, Columbus consistently ranks among the best U.S. cities for young professionals and families alike. With easy access to parks, trails, and cultural attractions, as well as a strong healthcare and Innovation ecosystem, Columbus Is a city where you can build both a career and a community. Columbus offers a vibrant, affordable urban experience with a cost of living 10% below the national average. Fellows enjoy a thriving downtown, diverse neighborhoods, world-class research opportunities, and a robust cultural scene including sports, dining, nightlife, and the arts.



Presenters

Who will win the 2026 Academy, Committee, Interest Group Challenge?
The annual SAEM Foundation (SAEMF) Challenge is underway! YOUR gift or pledge to SAEMF by August 31 will help your Academy, Committee, or Interest Group rise to the top.
Donate!

saem.org/donate
Winning groups will receive:
Bragging rights for a year!
A special treat at your group meeting during SAEM27
Recognition as the 2026 Challenge champions in SAEM communications
Challenge donors will also be recognized as Annual Alliance Donors
Thanks to generous SAEM members, many of whom are Challenge donors, SAEMF invested over $1 million in the research and career development of its 2026-27 research and education grantees. Let’s do our part to power more possibility for emergency care — become an SAEMF Challenge donor today at saem.org/donate.
“My project is a qualitative study investigating barriers experienced by key stakeholders to including nonEnglish language preferred patients in clinical research with the goal of creating systems to facilitate more equitable and generalizable research. I am deeply grateful to SAEMF for investing in this work and my development as a physician-scientist.”
- Alexa (Lexi) Curt, MD 2026 SAEMF/RAMS Resident Research Grantee



May 18-21, 2026 | Atlanta Marriott Marquis