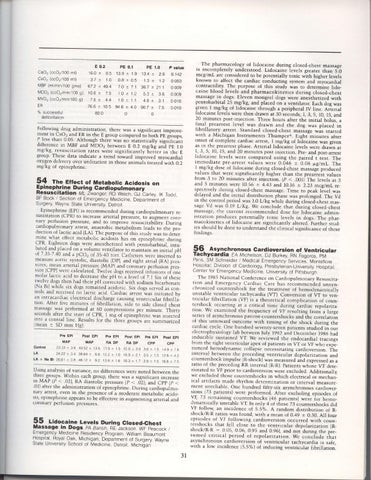
E O.2 PE 0.1 PE 1.0 P value 1 6 0 + 0 . 5 1 3 . 9+ 1 . 9 1 3 4 * 2 . 8 0 1 4 2 C s O , ( c c O r / 1 0 0m l ) 3.7+ 1.6 0 8 + 0 . 5 1.3+ 1.2 0.003 M B F ( m l / m i n / 1 0g0m s ) 6 7 2 * 4 9 4 7 . 0* 7 1 3 6 7 * 2 1 1 0009 N / D O 2( c c o ' / m i n / i O Og ) 1 0 6 * 7 5 10 :t 1.2 5 3 * 36 0009 M V O 2( c c o 2 / m i n / i 0 O g) 7 6 * 4 . 4 1 . 0* 1 . 1 4 8 * 3 1 0 0 1 0 ER 7 6 . 6+ 1 0 . 5 9 4 . 6 + 4 . 0 9 0 . 7 + 7 . 5 0 0 1 0 o/.successful 800 0 0 d e fi b r i l l a t i o n C a O , ( c c O r / 1 0 0m l )
Following d,rug administration, there was a significant improve_ ment in CsO2 and ER in the E group comparcd"to both pE gio,rpr, P less than 0.05. Although there was no statisti"aily silrilfi.a'.,t difference in MBF and MDO, between E 0.2 mg/kg nrri pE t.O mg/kg, resuscitation rates *ere significantly ictter in the E group. These data indicate a trend toward improved myocardial oxygen delivery over utilization in those animals treated with 0.2 mg/kg of epincphrine.
The-Effect of Metabotic Acidosis- on 9l During Gardiopulmon;;t-Cartey, lqinenlf1g Resuscitation
ML Zwanger, RD Welcn, GJ tK Todd, BF Bock / Section of Emergency Medicjne, Department of Surgery, Wayne State Unjversity, Detroit Epinephrinc (EPI)is recommended during cardiopulmonary rc_ suscitation (CPR) to increase arterial p.ess.-r.e,to augment coro_ nary perfusion pressure, and to imprbve resuscitabiiity. Dunng alle,:t, anaerobic mctabolism lcads to the pni :arolopulmonary d u c t r o n . o f l a c _ t i ca c i d ( L A ) . T h e p u r p o s e o f t h i s s t u d y w a s to deter_ minc what cffect metabolic acldoiis has on cpinephrinc during CPR Eightcen dogs werc ancsthctized with pentobarbital, intul D a r c dJ n d p l a c c d o n a v o l u m e v e n t i l a t o r t o m a i n t a i n a n initial pH o f 7 . 3 5 - 7 . 4 0a n d a p C O 2 o f 3 5 - 4 0 t o r r . C a t h e t c r s w c r c inscrted to m e a s u r c a o r t i c s y s t _ o l i c ,d i a s t o h c ( D p ) , a n d r i g h t a t r i a l ( R A ) p r e s surcs;^rrcdn arterial pressure (MApJ and coronary pcrfusion pres_ s u r c I C P P )w c r c c a l c u l a t c d . T w c l v c d o g s r e c c i v c d i n f u s i o n s oi one m o l a r l a c t i c a c i d t o d e c r e a s ct h e p H t o a l e v c l o f Z . t S i * of thcsc twclve dogs thcn had their pH corrected with sodium bicarbonatc (Na Br) while six iJogs_rcmiined acidotic. Six dogs scrvcd as con_ trols and rcccived no lactic acid. Cardiac arrcst was initiated by an intracardiac electrical dischargc causing ventricular fibrillal tion. Aftcr fivc minutes of fibrillition, sidc to side closcd chest massage was performed at comprcssions per minutc. Thirty *6O seconds after thc start of CpR, I mg o{ epineihrinc was rnjectcd rnto a central linc. Results for thc ihrce gro.rps a.e summarized lmean :t SD mm Hg): Pre Ept
post Ept
pre Ept
post Epl
PE EPI
MAP
MAP
RA DP
RA OP
CPP
Post Epl
CPP 2333i36 4052t136 ti9at5 l 5 8 t 3 . O 3 6 1 1 5 1 4 9 17 6 LA 2 4 2 2 t 3 4 3 8 . 6 4 i6 6 1 2 2 t 1 0 1 6 9 1 2 i 3 5 i 15 1 2 6 r 42 L A + N a B i 2 6 8 1 t 3 . 84 6 1 2 ! 9 2 1 3 6 1 1 6 i 8 3 a t 7 3 9 : :1 5 1 6 8 1 7 5 Control
Using analysis of variance, no differences were noted between the threr groups. Within each group, therc *rr, ,ignifi..nt Increase tl-y+l'lP.< .02), RA diastolic pressure (p < .02),antt Cpp {pl . 0 1 )a f t e r t h e a d m i n i s t r a t i o n o { e p i n e p h r i n e . D u r i n g cardiopujmo_ nary arrest, cven in the presence of a moderate metabolic acido_ srs, eprnephrlne appears to be effective in augmenting arterial and coronary perfusion pressures.
55 Lido_caine Levets During-lackson, Glosed.Ghest llassage in Dogs pA Barish, Re WipeacockI Emergency program, Medicine Residency William Beaumont RoyalOak Mrchigan; Department of Surgery, Wayne !9:?ilgl StateUnrversity Schootof Medicine, Detroit, Michi6an
The pharmacology of lidocaine during closed-chest massage is incompletely understood. Lidocaine levels greater than 510 mcg/ml are considered to be potentially toxic with higher levels known to affect the cardiac ionducting system and i-ryocardiai contractility- The purpose of this study was to determ;ne lidol caine blood levels and pharmacokinetics during closed_chest massage.in dogs. Eleven mongrel dogs were aneJthetized with pentobarbital 25.mg/kg, and-placed on a ventilator. Each dog was given I mg/kg of lidocaine through a peripheral IV line. Arierial lidocaine levels were then drawn at 30 seconds, l, 3, 5, 10, 15,and 20 minutes post-iniection. Three hours after the iniiial bolus, a final_prearrest level was drawn and the dog was placed rn fibrillatory arrest. Standard closed-chert -"rirg" wis started with a l\,lichigan Instruments Thumperri. Eight minutes after onset of complete cardiac arrest,.l_ mgTkg of li"docarne was grven as in the prearrest phase. Arterial lidocaine levels were drain at 1,3, 5, 10, 15, and 20 minutes post injection. pre- and post_arresi lidocaine levels were compaied using the paired t test. The immediatc pre-arrest values were 0.0+e ,t 0.06 pglmL. The I mg/kg dose of lidocaine during closed-chest massagi produced values that significantly higher than the prcarrest values ^wcrc rr()m J to LU mrnures after rniection lp < .001)The levelsat 3 and 5 minutes were 10.5(r + 4.43 and 10.16 :t 2.23 mcg/ml re_ s.pectivcly during closed-chest massage. Time to peak livel was dclaycd and thc initial distributron pliase was prolonged. The VJ in thc control period was 1.0 L/kg whilc duringclosed-chest mas_ sagc Vd was 0. l9 L/Kg. We conclude that d"uring closed-chest m a s s a g c ,t h c c u r r c n t r e c o m m e n d e d d o s e f o r l i d o c a i n e a d m r n _ lstratlon produces potcntially toxic levels in dogs. The phar_ m a c o k i n c t i c s o f l i d o c a i n e a r e s i g n i f i c a n t l y a l t c r e d . ' - F u r t h e rs t u d _ i c s s h o u l d b e d o n c t o u n d e r s t a n < L t h ec l i n i c a l s i g n i f i c a n c e o f t h e s e findings.
-56- l"y4ghronous Gardioversion of Ventricular
Tachycardia EA Michelson, DJ Burkey, RN Fogoros, pM Paris,SM Schneider / Medical Emergency Serviced, Montefiore H o s p i t a l ; D i v i s i o n o f C a r d i o l o g y , p r e s b y t e i i a n - U n i v e r s i t yH o s p i t a l , C e n t e r f o r E m e r g e n c y M e d i c i n e , U n i v e r s i t yo f p i t t s b u r g n T h c l 9 l l 5 N a t i o n a l C l o n f e . r c n c co n C a r d i o p u l m o n a r y R e s u s c i t a _ t i o n a n d . E n - r c r g c n c yC a r d i a c C a r e h a s r e c o m m e n i e d u n s y n chronized countershock for the treatment of hemody""-i.Jtty unstable ventricular tachycardia (VTJ. Conversion of VT tn u..rtricular fibrillation (VF) is a theoretical complication of coun_ t c r s h o c k o c c u r r i n g _a t a c r i t i c a l t i m e d u r i n g c a r d i a c r e p o l a r i z a tion. We cxamined the frequency of VF reJulting from a large scrics of asynchronous patient-countershocks and ihe .orr.lrirJn ot thrs untoward outcome.with timing of the shock during the cardiac cycle. Onc hundred r.u"nty-r.u"., patients studied in our elcctrophysiology lab between fuly l9g2 and December l9g6 had induciblc sustained VT We reviiwed the endocardial tracrnls from the- right ventricular.apex of patients in VT or VF who exp"e_ ricnccd. hemodynamic collapse necessitating cardioversion. The interval _between the preceding ventriculai depolanzation and countershock impulse {R-shocklwas measured and expressed as a r a t i o o f _t h e p r e c e d i n g R R i n t e r v a l iR-R).patients whose VT deteriorated to VF,prior to cardioversion were excluded. Additionally, we excluded those countcrshocks in which electrical or mechanl ical artifacts made rhythm determination or interval measure_ ment unreliable. One hundred fifty-six asynchronous cardioversrons (73 patientsl werc performed. After excluding episodes of VF, 73 remaining countershocks {46 patients) were for hemo_ dynamrcally unstable VT In only 4 of these Z3 countershocks did VF follow, an incidence of 5.5"/o. A random distribution of R_ shock/R-R ratios was found, with a mean oI O.49 * 0.30. All four episodes of VF following cardioversion occurred with coun_ tershocks that fell close to the ventricular depolarization lR_ shock/R-R - 0:05, 0.06, 0-95 and 0.96), and not during the pre_ sumed critical period of repolarizaiion. We .o.r.l-ud. thrt asynchronous cardioversion of ventricular tachycardia is safe, with a low incidence (5.5%f of inducing ventnc;lar fibrillation.