SEPTEMBER 2023










OPINION
MY LAB
THE BIG QUESTION the event for you?”
THE BIG STORY
We ask: “What makes Congress the ‘go-to’ p.16










A look at traditional medicines through the ages: p.34

PARASITOLOGY

A lab tour at the Liverpool School of Tropical Medicine:

PARASITOLOGY tour at School of Medicine: p.54
the discovery of the double helix
HI S TORY
MYLAB
T HEBIOMEDICALSC
Race to reveal the secret of life 70 years since the discover y of
IENTIST.NE T
A proven, world-class LIMS for today’s modern labs

Around the world, InterSystems TrakCare Lab Enterprise is powering the data-driven lab.
With over a billion tests carried out annually by more than 138,000 users in 7,373 labs, using over 6,000 interfaced
© 2023 InterSystems Corporation. All rights reserved. InterSystems is a registered trademark of InterSystems Corporation. See us at IBMS Congress 2023 Stand #713
EDITORIAL
5 Looking forward to Congress, which takes place this month
NEWS
7 News in numbers
9 Research, funding, developments and clinical updates
13 Product advances and launches

OPINION
14 One-to-one: What happens when you accelerate the ageing of blood cells? Professor Meng Wang explains his research
16 The big question: What makes Congress the “go-to” event?
SCIENCE
18 Race to reveal the secret of life: The work of scientists that led to the discovery of the double helix 70 years ago, which has shaped biomedical science ever since
23 Point-of-care testing and the new ISO 15189:2022: David Ricketts, Alyson Bryant and Sarah Glover on accreditation and point-of-care testing
29 Recent advances and updates in biomedical science: Summaries of articles in the British Journal of Biomedical Science

EDITOR Rob Dabrowski
SENIOR DESIGNER Gary Hill
PICTURE EDITOR

Akin Falope




PUBLISHING DIRECTOR

Aaron Nicholls
PRODUCTION
Rachel Young
34 The evolution of traditional medicine: From shamans and witches to contemporary use of medicinal plants and health tourism

40 Sickle cell anaemia and thalassaemia: Shahid Muhammad reviews the issues in relation to transfusion medicine



MY IBMS
45 Institute news: The latest from the IBMS
47 Journal-based learning: CPD exercises based on journal articles
51 World Alzheimer’s Month: Francis Yongblah talks through his personal experiences
53 Here to help: An update on the new website and CPD system
MY LAB
54 Jayne Jones gives a guided tour of her parasitology lab
ISSN
COVER FEATURE 34 29 23 18 THE BIOMEDICAL SCIENTIST 3 CONTENTS September 2023 CONTENTS
2023 IBMS.ORG COVER IILLUSTRATION: MARTIN O'NEILL Best Magazine < 20K circulation Memcom Membership Excellence Awards 2020 Gold – Best Membership International Content Marketing Awards 2020
SEPTEMBER
RECRUITMENT ADVERTISING +44 0 20 7880 7621 biomedicaljobs@redactive.co.uk
1352
2023 Institute of Biomedical Science
plc
Lincolnshire PE10 9PH
Subscriptions are available by calling 01580 883844
7673 ©
PRINTED BY Warners Midlands
Bourne,
SUBSCRIPTIONS
publication.
particular circumstances.
advice
published is done so without the Institute,
servants or agents and any contributors having liability in respect of its content.
Neither the publisher nor the IBMS is able to take responsibility for any views or opinions expressed in this
Readers are advised that while the contents are believed to be accurate, correct and complete, no reliance should be placed upon its contents being applicable to any
Any
or information
its
paper envelope – please recycle with other paper and cardboard.
PUBLISHED BY Redactive Publishing Ltd 9 Dallington Street, London EC1V 0LN redactive.co.uk Recycle your magazine’s
DISPLAY ADVERTISING +44 0 20 7880 7556 biomedical@redactive.co.uk
With 40 years of laboratory expertise and over 1,450 lab professionals, Clinisys supports some 3,000 laboratory organisations worldwide to process billions of tests. Our world leading industry and discipline specific solutions are transforming laboratories through digital innovation and intelligent informatics. We







Visit us at: IBMS Congress 2023 Connect + Recharge Hall 4 foyer
can help you to deliver lab data that solves real world challenges. clinisys.com
Later this month we will see the return of IBMS Congress (25–28 September) and, if ticket sales are anything to go by, it will be the most successful one for many years.
Since the great success of IBMS Congress 2022, our specialist panels have gone above and beyond to bring together another impressive roster in a much-reduced timescale. We have an expansive education and lecture programme with over 20 key specialisms and areas of professional interest – with the most innovative and esteemed leaders in their fields talking and presenting.
This year also sees the Association for Clinical Biochemistry and Laboratory Medicine hosting the Laboratory Medicine Leadership Summit at IBMS Congress. It’s wonderful that this essential strategic meeting for senior laboratory staff and managers, across all pathology disciplines, is now on the agenda.
The sheer scale and depth of the programme demonstrates the IBMS’ primacy in biomedical science and diagnostics – as does having the UK’s largest biomedical science exhibition, featuring the leading diagnostic companies with all the major suppliers and innovators from industry. It is truly the UK’s most significant biomedical science event by far.
I’m also proud of the support that we offer to our eStudents at IBMS Congress –organising the UK’s largest dedicated

RETURN OF CONGRESS
IBMS Chief Executive
David

biomedical science student event with a programme that is free to attend and aimed at jump-starting and informing early careers.
With just over a year between Congresses this time, it will be interesting to see just how quickly the concerns of our profession have shifted and moved, and what has stayed the same.
This year’s theme is “Linking learning to the laboratory” and this, at core, is what the IBMS excels at. However, it is thanks to the efforts of our members who are trainers and managers, researchers and innovators, specialists and advanced clinicians, that we can put on such a fascinating event.
I never lose sight of the fact that IBMS Congress is essentially a display of our membership’s talent and achievements, and I am always overwhelmed by the determined application of our profession’s intelligence and its vision for better patient care.
I can’t wait to get there and learn from the brightest and best that the UK has to offer. BMS
David Wells Chief Executive



THE BIOMEDICAL SCIENTIST 5 EDITORIAL David Wells Institute of Biomedical Science is the professional body for the biomedical science profession. INSTITUTE OF BIOMEDICAL SCIENCE 12 Coldbath Square London, EC1R 5HL United Kingdom +44 (0)20 7713 0214 +44 (0)20 7837 9658 Email: mail@ibms.org Web: www.ibms.org FOLLOW THE INSTITUTE Join us on facebook.com/ biomedicalscience Follow us on Twitter @IBMScience Find us on LinkedIn PRESIDENT Debra Padgett
FIBMS CHIEF EXECUTIVE David Wells CSci FIBMS DEPUTY CHIEF EXECUTIVE Sarah May CSci FIBMS EXECUTIVE HEAD OF MARKETING AND MEMBERSHIP Lynda Rigby HEAD OF COMMUNICATIONS Dan Nimmo EDUCATION AND TRAINING education@ibms.org EXAMINATIONS examinations@ibms.org MEMBERSHIP mc@ibms.org CHARTERED SCIENTIST chartered@ibms.org
Wells looks forward to the UK’s most significant biomedical science event.
CSci
INNOVATIONS IN CELLULAR PATHOLOGY




Same day diagnosis
Faster TAT
Streamlined

Improved specimen safety and quality
Enhanced user safety
Optimised reagent use





No daily maintenance
No downtime, continuous loading of samples











SCIENCE NEWS IN NUMBERS
£7.79BN ON COVID
The total cost of the response to COVID-19 in Northern Ireland was £7.79bn, the Northern Ireland Audit O ce has estimated.
Spending by Stormont was estimated at £4.94bn, with £2.85bn relating to the costs of UK-wide schemes. The furlough scheme was estimated to have cost £1.72bn in Northern Ireland.
EXTRA BEDS
An extra 5000 hospital beds will be available this winter to help the NHS in England to cope, it has been revealed.
It will mean nearly 100,000 permanent beds accessible at the busiest time of the year – a 5% rise on current levels. Last winter, one in eight beds were taken by patients who were ready to be discharged, but could not be because of a lack of available support. 5000
98%
OF DNA UNDER-EXPLORED
Scientists from The University of Edinburgh have been awarded more than £46.3 million from the Medical Research Council for work that will include research into the lesser-known areas of DNA. The work will involve studying the 98% of DNA that they say is under-explored
250
More than 250 NHS buildings in Scotland could contain a potentially dangerous type of concrete that can collapse.
NHS Scotland issued a Safety Action Notice and completed a “desktop survey” of its estate in June. Reinforced autoclaved aerated concrete was used to build roofs, walls and floors from the 1960s to the 1990s NHS Scotland warned the material is potentially vulnerable to “catastrophic failure”. The Scottish government said there is “no evidence to suggest that these buildings are not safe”
748 , 395
Hospital waiting lists have risen again in Wales, with 748,395 “patient pathways” waiting for hospital treatment in May.
This is an extra 5000 on the list, with 136,549 of these waits of more than a year. There is a target that no-one should wait more than two years, but 30,769 are still waiting that long.
The Welsh government said although it is disappointing, the number of two-year waits fell for a th consecutive month.
THE BIOMEDICAL SCIENTIST 7 NEWS In numbers


New tool for medical biosensors
A team of US researchers have developed a new method using nanopores — nanometre-sized holes — to help scientists advance their discoveries in neuroscience and other medical applications.
For context – a single sheet of paper is about 100,000 nanometres thick.
Professor Li-Qun Gu said: “Potential applications include studying the structures of DNA- and RNA-based diseases and disorders, such as COVID-19, HIV and certain types of cancers, to see how drug therapies work.”
The technique involves aptamers, or single strands of DNA or RNA molecules that selectively bind to a specific target. This allows researchers to know exactly what they are detecting with the nanopores and study how individual molecules are interacting with each other.
bit.ly/45irS7F
For a small percentage of cancer patients, doctors are unable to determine where their cancer originated. This makes it much more di cult to choose a treatment, because many cancer drugs are typically developed for specific cancer types.
A new approach developed by researchers at Massachusetts Institute of Technology (MIT) and Dana-Farber Cancer Institute may make it easier to identify the
ANTIBIOTIC RESISTANCE LINKED TO AIR POLLUTION?
Reducing levels of harmful air pollution could help reduce antibiotic resistance, according to the first in-depth global analysis of possible links between the two.
Findings from the study highlight that controlling air pollution could greatly reduce deaths and economic costs stemming from antibioticresistant infections.
It indicates that the relationship between the two has strengthened, with increases in air pollution coinciding with larger increases in antibiotic resistance in recent years.
Misuse and overuse of antibiotics are the main drivers of antibiotic resistance, but evidence suggests air pollution also contributes.
However, until now,
there was limited data on how much influence PM air pollution – which is made up of particles times smaller than the width of a human hair – has on antibiotic resistance globally.

Sources of PM include industrial processes, road transport and burning coal and wood. Recent findings indicate billion people globally are directly exposed to unsafe average annual PM levels.
The findings indicate antibiotic resistance increases with PM , with every % rise in air pollution linked with increases in antibiotic resistance of between .% and %, depending on the pathogen. The association has strengthened over time, with changes in PM levels leading to larger increases in antibiotic resistance in more recent years.
bit.ly/443Bkeb
sites of origin for those cancers.
The researchers created a computational model that can analyse the sequence of about genes to predict where a given tumour originated.

The researchers were able to accurately classify at least % of tumours of unknown origin with high confidence in a dataset of about patients. This approach enabled a -fold increase in the number of patients who could
have been eligible for a genomically guided, targeted treatment, based on where their cancer originated.
“The most important finding in our paper was that this model could be potentially used to aid treatment decisions, guiding doctors toward personalised treatments for patients with cancers of
unknown primary origin,” says Intae Moon, the lead author of the new study.
The model was also tested on about tumours that it hadn’t seen before, but whose site of origin was known. It was able to predict their origins with about % accuracy.
bit.ly/4511rUe
IMAGES: ISTOCK/SHUTTERSTOCK/GETTY/SCIENCE PHOTO LIBRARY
GLOBAL ANALYSIS
COMPUTER MODELLING AI MODEL TO DETERMINE WHERE CANCER ORIGINATED BIOMEDICAL ENGINEERING
NEWS Science 9 THE BIOMEDICAL SCIENTIST SCIENCE
NEWS
HOT BACTERIA
Scientists have found a naturally occurring strain of bacteria that could help stop malaria transmission to humans. It was a chance discovery, after a colony of mosquitoes in one experiment did not develop the malaria parasite.


HOT PORTON DOWN
The Vaccine Development and Evaluation Centre, based at Porton Down, is working to develop vaccines against new killer pathogens within three months of identification.


AUTOMATED MEDICAL IMAGING FOR SCHISTOSOMIASIS DIAGNOSIS



HOT INTERPRETATION
Two hospitals are to trial a mobile translation service to remove language barriers between patients and staff Peterborough City and Hinchingbrooke hospitals will trial the “Interpreters on Wheels” for four weeks.
NOT NOSE PICKING

Healthcare workers who pick their noses could be more likely to get COVID, according to a small study. Of 219 participants, 17% who admitted nose-picking tested positive for COVID-19, compared to 6% of those who did not.



NOT FAST FOOD

A town that has seen a rise in childhood obesity is to ban ads for unhealthy food from council-owned property. Luton Council said no adverts that include items high in fat, salt and sugar will appear on its billboards, lampposts or screens.


NOT SUMMER HOLIDAYS

Researchers have shown that too much sun exposure negatively affects short-term diversity and composition of the skin’s bacterial make-up.






Schistosomiasis, a parasitic disease affecting millions worldwide, poses a significant public health and economic burden, particularly in impoverished regions.


Currently, microscopy is the standard for diagnosing schistosomiasis, but it is time-consuming, operator-dependent, and requires specialised expertise, making it challenging for resource-limited areas.
Researchers have now developed the Schistoscope – an innovative optical tool equipped with an autofocusing and automated slide-scanning system. This device captures microscopy images of urine samples, enabling efficient detection of Schistosoma haematobium (SH) eggs, a common cause of urogenital schistosomiasis.
The team created an SH dataset consisting of 12,051 images of urine samples collected in a rural area in central Nigeria and captured using the Schistoscope device.
They then manually annotated the images, marking the eggs and differentiating them from artefacts, such as crystals, glass debris, air bubbles, and fibres, which can hinder diagnosis.
In the first stage, the framework performs semantic segmentation to identify candidate SH eggs in the captured images. The second stage refines the segmentation by fitting overlapping ellipses, effectively separating boundaries of clustered eggs, leading to more accurate egg counts.
The researchers implemented it on an edge AI system and tested it on 65 clinical urine samples obtained in a field setting in Nigeria. The results showed high sensitivity, specificity and precision, with the automated egg count closely correlated to the manual count by an expert microscopist.
 bit.ly/3OOTfRi
bit.ly/3OOTfRi
, 051


THEY CREATED AN SH DATASET CONSISTING OF 12,051 IMAGES OF URINE SAMPLES COLLECTED IN A RURAL AREA IN CENTRAL NIGERIA AND CAPTURED USING THE SCHISTOSCOPE DEVICE.

12
MICROSCOPY
THE BIOMEDICAL SCIENTIST 10 NEWS Science
WHAT’S HOT AND WHAT’S NOT
Blood pressure for predicting outcomes

A new method derived from standard blood pressure assessments can improve monitoring of critically ill patients with circulatory shock, it is reported.

The team behind the breakthrough said it accurately predicts risk of death, length of hospital stay and blood lactate levels.
The work involved designing an approach to measure a property of the circulation called the critical closing pressure, which is the blood pressure at which small blood vessels collapse and blood flow stops.
Critical closing pressure can provide an indication of blood vessel tone in

response to disease and therapy, but it has not been possible to measure this parameter routinely in clinical care.


Development of the new approach utilised highresolution waveform data from blood pressure monitoring of 5532 patients in US cardiac intensive care. Researchers developed an analysis based on measured parameters to define the critical closing pressure. They then defined a value called tissue


Our full range of ELISA Automation








perfusion pressure– the difference between average arterial blood pressure and critical closing pressure – and found that it predicted a patient’s risk of death, length of hospital stay and peak blood lactate.


“We have developed a new metric that can identify individuals with inadequate tissue perfusion who are at risk for adverse outcomes. We believe this method can be used to optimise treatment decisions for patients in the intensive care unit,” said Aaron Aguirre, an Assistant Professor of Medicine at Harvard Medical School.
bit.ly/47CNDkH
RISK ASSESSMENT
| 01829 824 825
THE BIOMEDICAL SCIENTIST 11 NEWS Science


































Liverpool School of Tropical Medicine (LSTM) and charitable medical research organisation LifeArc are launching a new Translational Development Fund to help tackle infectious diseases. LifeArc will invest £. m to support the progression of new technologies and treatments for emerging viral threats and neglected tropical diseases. LifeArc will also join the LSTM-led Infection Innovation Consortium, making its platform to progress antibody-based treatments available to partners. lifearc.org

A new study demonstrates how the combination of DNA-encoded libraries (DELs) and NanoBRET Target Engagement technology can accelerate early-stage drug discovery. Researchers from Promega Corporation and WuXi AppTec generated new chemical probes from molecules identified through a DEL screen. This offers opportunities to develop novel NanoBRET Target Engagement Assays aimed at many understudied proteins, accelerating efforts in identifying new potential therapeutics. promega.co.uk

Innovative technology that creates ultra-thin layers of human cells in tube-like structures could lead to the development of lifelike blood vessels and intestines in the lab. The technique, known as RIFLE, enables the construction of separate layers as delicate as one cell thick. Developed by experts at the University of Edinburgh, RIFLE involves injecting a small volume of liquid containing cells into a tube rotating at high speed – up to rpm. The speed of the rotation causes the cells to distribute evenly across the internal surface, with higher speeds resulting in thinner layers. ed.ac.uk
 IMAGES: SHUTTERSTOCK
IMAGES:
IMAGES: SHUTTERSTOCK
IMAGES:
©IAN HOLLAND
EMERGING
LIFEARC
VIRAL THREATS
PROMEGA
DNA-ENCODED LIBRARIES
TUBULAR TISSUE ADVANCE THE BIOMEDICAL SCIENTIST 13 NEWS Technology TECH NEWS •C. difficile •Sepsis •STD •MRSA •Salmonella •Candida auris •Pneumocystis •Meningitis •Antibiotic resistance Introducing Amplex eazyplex® LAMP assay. Molecular diagnostics made eazy! 30 minutes The Eazyplex System is a cutting-edge molecular diagnostics platform that uses loop-mediated amplification (LAMP) to rapidly diagnose a range of infections directly from sample. HELPING SOLVE MICROBIOLOGICAL PROBLEMS Telephone: 01782 516010 welcome@bioconnections.co.uk www.bioconnections.co.uk Visit us at IBMS Congress Hall 3, Stand 124
THE UNIVERSITY OF EDINBURGH
What happens when you accelerate the ageing of blood cells? Professor Meng Wang explains his research.
The process of ageing affects every part of the human body, from individual cells to the major organ systems, such as the circulatory system, which includes the blood. Though this vital body fluid is constantly refreshed, even it cannot evade the depredations of the years.
Attempting to pin down the processes behind this deterioration, a joint research team from the Medical Research Council (MRC) Molecular Haematology Unit, the MRC Laboratory of Molecular Biology and the Wellcome-MRC Cambridge Stem Cell Institute has just published the results of its work in the article “Genotoxic aldehyde stress prematurely ages hematopoietic stem cells in a p53-driven manner” in Molecular Cell.
Ageing blood
The co-lead author is Meng Wang, formerly of the Wellcome-MRC Cambridge Stem Cell Institute and now Assistant Professor in Nutritional Sciences at Cornell University. The impetus for the research, he says, was to close the gap between the knowledge of the problems associated with ageing blood and the mechanism that drives it. “Blood, like any other cells, tissues and organs in our body, suffers from this process, which essentially is a natural decline in the ability to function. What it means is that once we reach the age of 70 or so, our ability to replenish blood cells and form blood is just not as good as when we were 20 or 30.”
This can create a number of problems, not least that the blood struggles to meet the physical demands of the body.
NOT THE SECRET TO EVERLASTING LIFE… NOT YET


“The blood just can’t carry oxygen to get around to your body as efficiently. Another serious problem is that our blood cells fight infections, but if we don’t make as many immune cells and they don’t function properly, we are much more susceptible to infections. As the blood gets older there also is an increased risk of blood cancers.”
What do we already know about the causes of these detrimental effects?
“Surprisingly little, other than the fact that it’s an inevitable part of living. In the lead-up to our study, we did know that certain factors such as inflammation can accelerate the ageing process, as can some genetic conditions. This gave rise to the hypothesis that perhaps damage to the
DNA is a factor. When I say ‘inflammation and DNA damage’ these are really end processes as we live our lives.”
The researchers settled on analysing chemicals produced by the body, and in particular by the metabolism, that could damage the DNA and in turn trigger the ageing process and diseases such as cancer. The suspect put under the spotlight was the reactive chemical group, the aldehydes. One of the most common aldehydes is formaldehyde, known for its strong preservative qualities.
“What was quite surprising from research in the last few years initiated by Professor Ketan Patel and his team, which I was part of, is that our body makes a lot of these aldehydes itself. This raised the
THE BIOMEDICAL SCIENTIST 14 OPINION One-to-one
IT’S
idea that maybe our main exposure to aldehydes is not from the environment but perhaps occurs every day in our bodies, which led to us wonder, do we make enough for it to be toxic and, if it is, what is the actual detrimental effect?”
Raising aldehyde levels
To test this, the team raised the level of aldehydes in mice. “We genetically deleted enzymes whose natural job is to detoxify formaldehyde. Taking off this brake allowed us to see how much the natural metabolism makes formaldehyde and what accelerated pathologies take place.”
The first effect was an increased incidence of cancer, discussed in a study published a couple of years ago. The

second, and the subject of this latest article, is that when the team looked at the blood stem cells, they saw multiple attributes normally found in much older stem cells. “Mice that were around eight weeks’ old had stem cells with features that you only really see in a two-year old mouse. In human terms, it is like a 10-year-old with the blood stem cells of an 80-year-old. We had accelerated blood ageing by raising formaldehyde levels.”
Now the team was in a position to investigate the steps leading up to that process. “We focused on one major cell-response pathway that’s driven by the transcription factor called p53, which plays a critical role in how a cell detects and responds to DNA damage. Looking at these aged cells, did they age because they accumulated various damage or did some response switch on to turn them old?”
To answer this question, the DNA damage response within the cells was switched off by genetically deleting p53. “Once we’d done that, all the DNA damage and the formaldehyde remained, but the stem cells no longer aged. They reverted to looking like the blood stem cells that you would normally expect to find in an eight-week-old mouse.”
Predetermined pathway
One potential interpretation of this is that ageing might not be the simple function of the passage of time. “This gradual decline in the blood stem cells is a response. It is as if there is a predetermined pathway, triggered by certain events and pushing certain
MENG WANG
2005: BA, Medical and Veterinary Science
Tripos, University of Cambridge
2010: PhD, Biological Sciences, MRC Laboratory of Molecular Biology, University of Cambridge
2011: MD, University of Cambridge Medical School
2015: MPhil, Clinical Sciences, University of Cambridge
2022: Cancer Research UK Clinician Scientist Fellowship, Dept of Haematology, University of Cambridge
2023: Assistant Professor, Division of Nutritional Science, Cornell University.

buttons within the cell, but you can shut down this response with the surgically precise genetic deletion of p53.”
Thoughts are now turning to how the findings might translate to further research, technology or therapeutics. “We have pinpointed that too much of this chemical made by our own bodies is not good. But the first important question is exactly which pathways in our body are making this chemical? We have some ideas.”
As part of this, the team needs to determine if formaldehyde is produced at a constant level every day or comes in bursts during periods of stress, if it is linked to infection or inflammation, or related to diet? “Understanding where it comes from is critical. If we have a concrete answer to that, the next question is can we modulate it and would it have a beneficial effect on health?”
It’s not the secret to everlasting life, not yet. “But perhaps with chronic degenerative conditions that have a basis in pathologically high levels of formaldehyde, we could switch that down. While we can’t stop people ageing, we may be able to help to them to age more healthily.” BMS
IMAGES: WELLCOME COLLECTION
THE BIOMEDICAL SCIENTIST 15 OPINION One-to-one
“In human terms, it is like a 10-yearold with the blood stem cells of an 80-year-old”
THE BIG QUESTION
THIS MONTH WE ASK







“What makes Congress the ‘go-to’ event for you?”





THE BIOMEDICAL SCIENTIST 16 OPINION The big question
Janet Gilbertson

Principal Scientist
National Amyloidosis Centre, Royal Free London NHS Foundation Trust

As a naïve Trainee Biomedical Scientist in the early eighties, I was amused to witness the hype surrounding the upcoming IBMS Triennial, as Congress was known then. My first thought was: “What is all the excitement and buzz about?” My second was: “How do I get involved?”
I now look back on my years attending Congress, reflecting on the vast opportunities. The event was a vital tool in expanding my pathology knowledge early in my career, exposing myself to novel technologies and techniques, specialist training and understanding the importance of quality management. Not forgetting the invaluable hands-on experience received whilst trialling equipment at the vast trade show.
Now, at the height of my career, managing the clinical service for histopathology and proteomics at the National Amyloidosis Centre, I have transitioned from a naïve trainee to a leading scientist in my specialist field. I have enjoyed attending the IBMS Congress over the last 25 years, using it as a platform to share my clinical knowledge and research in histopathology and the rare disease amyloidosis. I have been very privileged to present posters, facilitate workshops and deliver lectures.
Congress will always be the event I look forward to, from socialising with friends and networking with colleagues, to learning from the next generation of scientists.
Amy Read




 Trainee Consultant Clinical Scientist Gloucestershire Hospitals Foundation Trust
Trainee Consultant Clinical Scientist Gloucestershire Hospitals Foundation Trust


The major draw of Congress for me is that it gives context to the day-to-day work done in microbiology laboratories. Whilst we are conscious there is a patient at the end of everysample, it can be difficult to see how the daily work fits into the national and global picture. Regional networks act and plan based on local epidemiology, but it is important to appreciate the changing microbiology landscape resulting from the emergence of novel pathogens, climate change and migration. Talks given at Congress provide perspective and act as a reminder that our work feeds directly into data on national and global epidemiology and outbreaks.

The second selling point of Congress is that it encourages attendees to think about the future, offering attendees the chance to discover research and technologies with the potential to change how testing is delivered in the future. “Future thinking” is rounded out with talks focusing on accreditation, service and workforce planning and leadership and it is wonderful that these conversations are accessible to individuals of all grades and experience.
Finally, Congress provides a fantastic opportunity for networking and catching up with old friends. The amazing work undertaken by the biomedical workforce has been recognised in recent years and IBMS Congress gives us the opportunity to celebrate our successes and our bright future. I always leave with new knowledge and re-ignited enthusiasm for the daily work we all do. I hope the same for you.
Jeyrroy Anjalo Gabriel


The IBMS congress is always a highlight of the biomedical science calendar and I have been fortunate to have attended a number of times over the years. The event offers a diverse range of educational sessions, including presentations by experts, workshops and seminars, which are helpful to stay updated on the latest developments in a broad spectrum of disciplines. It can be a wellspring of inspiration, with keynote speakers and industry leaders motivating creative thinking. I have found Congress also provides a platform to network with peers, exchange ideas and establish collaborations within the biomedical science community. Congress often includes opportunities for researchers to present their work through poster sessions or oral presentations, allowing you to share your findings and, for someone junior in their research career, it is a great opportunity to grow as a scientist and improve your public-speaking skills.
The event also features an exhibition where companies and organisations showcase their products, services and technologies, providing an opportunity to identify innovative solutions to issues. By attending Congress, you can broaden your global perspective, boost your knowledge base and get an insight into emerging technologies, all while forming lasting connections and recharging your enthusiasm for your career path.
Senior Biomedical Scientist Dermatopathology Laboratory, St Thomas' Hospital, Synnovis Analytics
THE BIOMEDICAL SCIENTIST 17 OPINION The big question IMAGES: ISTOCK

THE BIOMEDICAL SCIENTIST 18 SCIENCE Cover feature
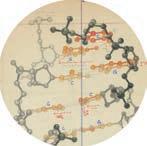
here were several people looking for the structure of DNA at the same time and the people who really showed everybody what it was were Rosalind Franklin and her student Ray Gosling,” says Denise Syndercombe Court, Professor of Forensic Genetics at King’s College London.
“They took this beautiful photograph of a strand of DNA, and it was immediately obvious to anybody who knew that this was a helical structure,” she adds. “Photo 51” was an X-ray diffraction image of a paracrystalline gel of DNA fibre taken in 1952 by Raymond Gosling when he was a research student at King’s College London. The university describes it as “one of the world’s most important photographs”.
The measurements and gaps in the photo showed that the helical structure was “slightly displaced” and this “defined the structure of the double helix”, Professor Syndercombe Court says.
Franklin – who had previously used X-ray diffraction to study the structure of coal – then used mathematical calculations to establish that it was DNA.
The story of the discovery of the double helix spans a century and a range of scientific disciplines. The research made possible since Watson and Crick’s 1953 model was published appears limitless. From medical screening of genetic diseases, to editing genetic mutations that lead to diseases and growing stem cells to replace damaged cells, dozens and dozens of applications of our understanding of the structure of DNA have been demonstrated.
The role of crystallography

Just over 70 years ago, work on DNA had begun in the Biophysics Research Unit at King’s College, when Gosling and biophysicist Maurice Wilkins – who had previously worked on the atom bomb –
modified an X-ray diffraction camera by filling it with hydrogen, in order to reduce background scattering.
They photographed moistened samples of DNA fibres, and were able to show that atoms in DNA had a regular structure. Another physicist in the unit, Alec Stokes, used mathematical calculations to predict from these photographs that the DNA molecule was probably helical in shape.
Franklin had already produced images of a DNA sample in two forms – long and thin when humidity was higher than 75% (she called this “wet” or B-DNA), and short and fat when drier (called crystalline or A-DNA). The absence of reflection on the meridian in the crystalline form led Franklin to suggest it had a spiral structure. Earlier theories had suggested that phosphates and sugars were attached to the four ring-shaped nucleobases that were arranged like a stack of pancakes.
ILLUSTRATIONS: MARTIN O'NEILL
The work of scientists from many disciplines led to the discovery of the double helix, 70 years ago. It has shaped biomedical science ever since.
THE BIOMEDICAL SCIENTIST 19 SCIENCE Cover feature
70 YEARS SINCE THE DISCOVERY OF THE DOUBLE HELIX
She also reasoned that because many water molecules could cling to DNA, presented these findings at a 1951 lecture Watson, showing the patterns produced

She e he allso so s rea e son s ed e tha ha hat b beca e ause use maany n ny y watater er mol m ecu e les l le coould ld cl c ing g to DN DNA, A, A the h wa w ter ter-attracti c ng phosphates m sm s ust t u be on o the he ouutsiside of o the he h he h lix. F Franankli k in n pre presen se ted d these e findi nd ngs at t a 195951 l lect t e ure ur att a tend end n ed e by Ame me m ric ic i an a biolog o ist James m Watatson onn, s show o owing n p pattern e s p spprodduce ucced d by A-D A NA and a BB DNA D an a d how w the h he two o for o fo ms seeemed d to o be pr p odu du d ced ed by b sur su rououndiding n the DNNA m A ole l cul c cules es e witith h diffffererent ammoun unnts ts of fo wat w wa er. er r
The role of modelling
FA C T F I L E :
Selected research made possible by the discovery of the double helix
Biological sciences: nematode genomes to understand comparative genome structure and evolution
Computational genomics: using computational and statistical analysis to decipher biology from genome sequences
Watson, who started his career studying attended a 1951 lecture by Maurice Wilkins
Wat W tsonon, w w ,who ho sta ta tarte r d his car ca eer r e sttudy ud ing bir b ds, s, s ds vi v rus us u an and b db d act accterierial a gen g eti e cs, c cs attend ndded ed a 1 a 951 95 9 lectu ct re Mau Ma ric ri r e W e ilklkins ins on o his h hi i findindings ng on the s estru tr ctu c ure re e of fo the h DNA A mo m lec e ule ul . H .HHe j e oined ed d the e Un U ive ve versi r ty y of Cammbri b dge e d ’s s Cavvend enddish is La Laborratotory ry spepeciaalising ng in n XX ray ay diiffractionon. A Also so s wor w king i g n C nC n ave avendidish sh wa was Enngli l sh h phy h ph sic i ist s Fr Franc n is i Cri Cr ck, k ck wh w o h oh o ad des d ign ig ed d undnderwateer m rm r mineines d duri u ng Wor Wo ld War W 2 and nd d haad k dknow nowwled eddge g of X-rray a ay cryrystallogra a g phyhy.
physicist Francis Crick, who had designed and had knowledge of X-ray crystallography. In their first encounter in 1951, Watson and Crick had already discussed that the three-dimensional configuration of the gene was needed to understand heredity and reproduction. They “pursued it with the next eighteen months” and immersed
In n theeir ir firrst st encncounounter teer in i 19951, 51 5 Wa W tsoon n and d Crick k i had a dalre lr ad ady di discuussesssedt d that ha th the thrree-e-dimimens nssion on o al configfigura u tio ti n o of t fthe he gen gene w ewas as nee e ded d to un underrsta sta t nd d her h edi e ty y and nd n re repro p duc u tio ti i n. n The Th y “purrsue ueed i it w with h siningle gl -mi -minde nd d f dffocucus over e thhe c ec e our ourse e of o the h ne n xt eigghte h en mon mo m ths t ths” a and imm mm m erssed ed e the e themselve l s i sin g n ene en e tic ic i ti s, bioche ch mis i try, , che hech mis mi tryy, p , hys hy ica i l c chemisttry, r an and d X-ray ay a cry c ystatalloogragraphy ph h
Dentistry: a tooth generated from a person’s own blood cells.
Diagnostics: mapping the human genome to identify genes involved in rare common

Gene targeting: growing stem cells that can replace damaged cells and treat disease
Epigenetics: understanding how the actions of genes can be temporarily modified to meet therapeutic targets and develop drug treatments
Physical sciences:



to structure even cells
using cryo-electron microscopy and X-ray crystallography to understand the structure of molecules and even macromolecules inside cells.
Technology: developing CRISPR to edit the including genetically modified animal models, biofuels and food and drink.
edit the genome for research purposes,

– Photo 51. They set it aside because they were working on A-DNA images.
– P –Phot ho h o 5 o 1. The Th y set t it aside de e bec b causause e the t y were r wo worki k ng on n A-DNA NA A ima m ges ges. .
But u thhere e waas t s enssion o be b twe tw en n Fraankl kl k in n and n Wi W lkins and an , s shor ho tly after ter the h phhoto t waas taken, n n, Fraanklin in lefft K tK t ingng’s for fo Birkbbeck ec Un U iveersi r ty, t leavi av a ng the th phohoto to wit wi w h G Gosl os s ing inng. W .WWilklkins ns n becam amme e Gos Goslin in ing’s ’ Ph PhD supe u rvi v rvisor soor annd d Gos G ling s g howwed him h th the p photto. o Wil W kins t stthen showeowed d t dtthe pho h to to o his frien e d W dWWats t on, on who reecoggnis n ed the he h lic i al struct c ctture ur u . “ .““Crick c ck had h an und un u ders er tan a dining o g ft f the h hel h lical l asppect ct of f ha h emooglobin n an a d o doonce he had d se s en e the he phhoto t he e und un ers rs rstoo to o d w w dwhat haat it wa w s,” s Prrofe e o sso s ss r Syn Synder de commbe be e Court r rt sayys. s.

Franklin and Wilkins and, shortly after the photo was taken, Franklin left King’s photo with Gosling. Wilkins became
Already that year, American biochemist
Alr l ead addy t y hat h ye y ar, ar Am Amerierican c bi bioch h chemi emi em m st Lin i us s Pau a lin in i g h ghad ad d use u d b dball l annd s dstic c t k mod dmo els e and X d dX-raray d y iff iffracractioion d nd n ata a to t hyp h pothesiise se that t t he h siningle-st st s rananded d alppha ha a hel he ix xi sees s prote t in str t uct t u urees. s. Watson an a d C Crick h kh k adnn’t ’t t con c ducted e any y DNA D exxper peer p ime iments t nt n thems em m elv v lves e so o dre e d w on oth thherss’ r r ’rese e arc a h t htto m ommode de odel f lf l from o X-r X- ay y dat d a. a
But Bu B t th there e e was a san i ninit n ial a set t s bac a k i in t n heir p r ropopose se s d moddel. el fi efi e rsst m t modeodel l
alpha helix comprises protein structures. Watson and Crick hadn’t conducted any model. The first model
Wat W son s so annd C d ric i k b kbuil uilt a tand nd n pre p senented e to o Wi W lki lk ns, n Fra r Fr nkl n in n and d Go G sli sl s ng, ng ha had d thr t th ee long t gt g wists t of f the e sugar ar a -
magnesium ions. Franklin realised that their model did not allow for the amount of water that DNA crystals contained, and if DNA contained magnesium ions, the water would cling to them and tear
pho h ph sphhate at ch c ain i in n heeld ld l togethher er r by y mag m nes ne ium io i ns. n Fr F ankklin l n re reali l sed thhat at the h ir i mod o el l d no not a ta a t llo llow f wf w or e am amount t of wat wa a er that D tD t NA cry ryystaals ls l conontai aiinedd, , and an if i DN DNA c contontainined d ed e mag a nes n ium m ions, ns the h he wa water er rte would u ng to o them em e and teeaar ar the moolec le ule apart.
Establishing t he structure
nkl nk in n and Go G sling ng n had continnued d to o phhotootogra g grraph ph h DNA DN mo m lececule ul s, s foc f i using ng on
A-D A- NA. A NA In n onne i imag m e t ethey hey had exxpos po ed d ove ov rni n ght gh th the e DNA ha h d h dhydrydrated a d nd n the th h
B-DDNA N shot w twas unu u un n sua uaally lly sha sh h rp p wit wi w h a han o no n obvi bv ous us u X pat p ter te na n and sta taacke ck d DNA bas a es s
DNA molecules, focusing on A-DNA. In one image they had exposed overnight the DNA had hydrated and the B-DNA shot was unusually sharp with an obvious X pattern and stacked DNA bases
The photo provided crystallographic evidence of the structure of DNA and led Watson and Crick to create a model with two sugar-phosphate base chains linked, conjecturing that genes come in pairs
Donohue, who shared their office for the year, had told Watson and Crick that the
The Th h he phhoto o provi o ov ded d cr cryst yst y all allogr og aphhic evidennce ce e t struc c ructur ur ture D D fDNA NA a led Wat a son so an a dC d Crick t k to c o rea ea reate a m amode deel w lw two sugar g -phphospsphat h te b base a chain ai a s l sl s ink nkked, con on o jec je e tur turing ing th t at gen n g es e com co e i ein pairirs bec c b aus auuse m most organism smms h have ave twwo o parrent n s. s Ame Am m rican an che ch mis i t, t Jer Je J ry Don o ohu hu h e, e who w shhare r d t dtheir o office ce for or thhe e yea a ear, , had h told ld d Wat Watson on o and C C dCrick that h thhe con co figgura a u tio o t n f nf n or o rin i gs g of car carbon o , nit niitrogrogen, e hydro dr gen annd o doxyg x en in thyhymin mi m e ( e(T) T) and an gu guani ni n ne (G) ) gi g ven in n mos m mo t c chem hem hemististry ry y textbo b oks ok waas w swwron r ng. g. g
thymine (T) and guanine (G) given in most chemistry textbooks was wrong. This led them to create cardboard models of the T and G bases in atoms, and understand how the bases fit together. In shifting the models around, Watson realised that when adenine (A) and T were joined, they very nearly resembled a paired cytosine (C) and G, and each pair could hold together by forming
Thihisl s l s ed d the h m t mt m to c oc o rea reate te t car ar a dbo bo board rd ard mod mo m els l ls of f the T eT annd G G ba b ses e in i at a oms s o , a and nd d und n ers e tan a d how ow the h th t ba b ses e fit t ttoge g the th r. r In I shihiftifting ng the he mo m delels a saarou r nd, nd Watsoson n reaealisised ed tha th t w when h he addeni n ne n (A) (AA) and T d wer w e j e joinined, ed th t ey y ver v y n near ea a ly res reesemb em led ed e a p a air aired ed cyt c tosisine ne e (C) and G dGG, a and d nd eacch h pai ai air c rccoul u ou d h dhhold ol tooget g her y fo formi rmiing ng g hydydrog ro rogen en bon o d.
“The structure of DNA is incredibly elegant: two long strands wrap around each other in a double helix, zipped up by highly specific base pairs,” says Professor Chromosome Replication Laboratory and Associate Research Director at The Francis Crick Institute. “It explains how DNA can be copied – after pulling the two strands apart, each strand can act as a
“Th h The s estru tr ctu u c re e of DNA D is i inncre e c dibly ly elegan a gant: t two w lo l ng strtrand dan s w swrap ap ar a oun o d eac e h o othe h r i riin a na n do doubl l u e h ehheli el x, x zip z pped up p y hig ighi hly sppeci ec fic c ba b se pai pa rs, s ” s ”says y Pr P ofe f ssoor r Johohn D nDDifflffleyy, G Grouup L Leader er of the he e Chr hr hromo o som some R Replplica i tion L nLabo ab b rat at a ory or an Assocsociatate R eRRese ese sees arc ar a h D hDDirecto cttor a ra r t T tThe he Fra Fr nci n s C sCricick I kInst s itu tu t te. te t “It e te t expl p ains h how ow w DNA NA A D ca c n b nbe c ecopi opi p ed – a –afte f r p rppull u ing ng the t e etwo str t trand ndds a sapar pa p t, t eac a ach s hsstrand nd n can ca acct a tas a s
nematode
a bioengineered
and common diseases.
mapping
developing
rare
SOURCE IMAGES: WELLCOME COLLECTION/ALAMY/SCIENCE PHOTO LIBRARY/FRANCIS CRICK INSTITUTE
SOUR SOU CE I MAGE S: W S:W S ELLC C LC L OME COLL L ECTI EC ECT C ON/A /A ON LAMY Y /SCI /SC C ENCE E ENC C PHO H TO L TOL O IBRA BRA IBR RY/F RY/ / RANC ANC N A IS C ISC S RICK I R INS NS TITU I T TE T TH E BI OM ED IC AL SC IENTI ST SCI SC ENC NC E Cov ov o er fea f atur t e
template, using the specific base pairing

templa a plate, e,te us g thhe s e specpecifific b c ase a e paairi i ng to t mak akke a ea e not no her h do d ublle h e heli e x.”


How the discovery has shaped

How the discover y biomedical science

Professor Diffley’s team at the Crick studies the processes involved in copying DNA. “To copy our genomes quickly and efficiently, DNA replication begins from thousands of ‘origins’, or locations, distributed across our genomes,” he says. “Over the past three decades we have used a variety of DNA approaches to build a detailed picture of how replication begins at these origins and how the process is controlled to make sure each origin is used just once in every cell cycle.
Pro P fes f ssor o Di Diffley’y’s team am m at thhe C e eCrick k studie di s t s stthe he prooces c sses ses innvol v vo ved d v in n co c pyi y ying g DNA N . “To o cop co y our u gen ge g ome m s q s uic u kly k annd d effifficiient en ly, ly DNNA r Arepleplicaicatio io o t n b nbegiins n fro o from m tho h th usa a sands nds of ‘o ‘ rig iggins inns n ’, , or r locations ns n , dis i tri riibut bu b ed e acr across s ou our g geenoennomes me mes,” ,” , he e say ayys. s “Ov “OOver er the e pa past s thr h ee dec d de ade ad s w we h eh e ave e use se s d a da varie r ri ty y of o DNA N ap approach chhes es e to bui b bu ld a d ad a detaailed p d dppict t i ure u of f ho how r wrrepl p ica ic tio t n n ns s at t these se s es origi gi g ns n and d nd n ho how t w the he e prorocesess i si s s cont o rolled leed to ma make ke sur ur u e each c ch ori or gin g is i us u ed jus ju j t o toonce ce in n every ry ceell ll l cyccle. le e
“We’re only just beginning to grapple with how all the many processes that occur on the same DNA template, like DNA replication, DNA repair, and gene

“WeWe’re re e onnly jus b tb t egiginni nn n ng to t gra grappl p e witth h h ow w all thhe m emany y pr proce o oc ssees t that ha h occccur u ur r on n the th sa same me e DNA N templlate e te, l , ike ik DNA A D re r pli plicat ca ion ion, D D DNA NA repepair i , a and nd d gen enne e tra transc s rip ri tioion, are a e co coord or o ina in ted ted.
“What happens when the machines

“WhWhat at hap h pen pe p s w s swhen en th them e m machchine i s inv nvvolvlved ed in n the h se diff d ffer e ent e pr p oce o sse s s collid idde? ? e? How o do d es s DNA DN D A reepliplicat at ation on deeal al wit i h D DNA NA A damage, w whic hi h is o soccucurriring g all al l thhe t e imeme? A ?And nd how w is thhe n normormalllly


exquisite regulation of DNA replication
exq x ex uis u ite it reegul ul gulatiion on of DNA N NA re replilicat ca ion n dis d rup r ted ed in ca cancer?” ?
The understanding of the double helix’s structure has also been crucial in other contexts. “If I want to know how old a person is from the blood, I could investigate small molecules, usually methyl groups, that attach to the DNA. They don’t alter the sequence in any way but variably bind or fall off the DNA molecule at cytosine residues, normally in particular areas where there is cytosine and guanine next to each other, and they will influence whether a gene is switched on or off
The T un u der de sta st ndi nd d ng g of o the he do doubl ubl ub e h heli l x’s s ’ str t uct t u ure ur u ha h s a sal en cru c cia ia ial i li i l n o nothether r conntex exxts. ts s “I “ f I waant nt to t know h w old o a per er e son on is s from om m the heth bl b ood odd, I I could uld innvesvestigate e sma m mall ll mol mo m ecu e less, u ,uusuaally l me methy h thhyyl g l rououps, p tha haat a t atta tt t ch to the heth DN D A. A The h y d d yd y on’ o on n t a taalteter r the he se s que q nce nc in n an any w yw y way ay but ut t va varia i iably ly bi bind nd or r fal f ll o looff the th h DN DNA m Amole l cul ul ule a e t c cyto toosin i inne res e idu i id d es, s no norma rmmally ll in n pa partiticul cuullar are e a as s whe where re the th re e is cyt cytosiine n and d guuanianine ne nex ex ext t to eac a ea h othe th r, and d thhey ey wil wi l i liinflnfluen u nce ce e whe wh theher a ge g ne e is swi sw tch h t ed d on n or off off.
“There are different ‘epigenetic’ methylation patterns that influence repair mechanisms, which are not as good when

“Th T There r arre d e difffferent nt ‘ep ‘e e ige ge genetnetic’ ic met tme hylati atiion on o pat p ter t rns ns n tha ha hat i ti t nflfluen e ce c repa r mec e ecchanismsms, s, s whi wh w ch h are noot a t as g sg s od doo wh when
we get older,” Professor Syndercombe Court adds. “But as a forensic scientist, I have to be really careful not to step into the medical world and I have to be selective about what I use because in the complete DNA molecule there is all sorts of private information about their
we get et e older deer,” ,” Proofes fesssor r Sy S nde d nd rcombe m Cou C Court rt r add dd dds. s. s “Buut a taas a sa s foren e sic ic sccien en e tisst, t I h Ihave to be reeall a al y c careful l f no not t tt t to s os o tep p int in into t ot o he med me m ica ical w lwworl or o d a da and h Ihave e to b sel l s ect t e ive iv ab a out t wh w at I u use e bec becausse i ei e in t n he h com ommple l te t DNA DN mol mo ecu c le the he h re is s l a so sorts r o priivat vatte i e nfo nf rma rmmatioion a na n bou bo b ut thei i h r med meedica ca cal h l ist sttory oryy.” .” ”
The future
Ethics will be an ongoing issue, with greater study not just of genetic sequences of a gene but the areas around the sequence. “There are many other epigenetic changes where we can look at the environmental influence on our DNA, for example,” Professor Syndercombe Court says. “Editing genes is going to be really problematic,” as we need to consider the impact of correcting the single nucleotide or sequence that, for example, perhaps leads to sickle cell disease. “While it might stop the disease, how will that impact the population generally?”
Eth Et E ics wiill ll l be an ong n oin oiing i g ssu s e, e wit t w h g h rea re ter st s udy d no n t j of f genet n neettic c sequennces c ce of f a gen ge e b ebbut ut the ar a eas as a aroound unnd u thhe s esseququenc e ennce. . e. “ThThere ere ar are m em e any n oth other er r epi ep e gen enneti et e c chan ha h nges ge g whhere re we e caan n loo oo ook a k kaat t t he e env e enviro ro o i nme nm nmenta ta t l i liinflnfluen uence ce e on o our ou DNANA, for o or exa a e mpl m mp e,” e Pr P ofe of f fessosor S rS r ynd yn ynderc e combmbe Court rt t says. s. s “Ed E iti it ng g gen enge es is goi g ng to be b reaeally y l pr probl ob o ema emmatictic,” ,” as s we w neeed t d to c occons onsnside e der r the he h im i pac a t o of c c fcorr or ect ecting g thhe s e inggle le e nuc nucleo leootid ti e or s sequ eq encce t e ethat hatt, f f ,for or exaxampl mp e, e per r er e pe hapaps l sl s ead ea s t s o s osick i le cel c l dise seease ase ase. “ . Whi Wh le it mig mi m ht sto to top t the he dis i easase, e how h wi w ll ll tha th t imp m mppact ac p epopu op o latation on o geener errall l lly?” y?

Many other areas of research are of growing interest. Professor Syndercombe Court is also part of a group taking microbiome samples from urban environments around the world. “We have an understanding of what microbes are in New York, Singapore, London, for example, in the air and on surfaces,” she says. “And we can recognise things like antibiotic resistance that may develop differently across the world.”
Man a y o othe h her a area e re r s o soof r f frese e e arcch a h are r of gro g wining intenteres es e t. t Pro P fes f sor so Synde n ndercombe mb Cou ouurt rt is p o art of o a gro g up tak n mic microbrobiomioome s essamp m amples les fr from om urban an n env enviroironmements t nt arroun ou d t dthe h wor wo w ld. “WWe e hav have a an u unde deerst rst s and anding inng of o wh what at a mic mi rob ob o es are e a in n New Y w ork or o , S Sing innggapo apo p re, re e Londo nd n, for o fo exaxample, e in the aiir a raand nd n on n sururfac fa es, e ” s ” she he sayys. s “An A And w d dwwe c ec e an rec r ogn n o ise i e thhing innggs l sl s ike ke e ant a ibi bi bioti ot t c r crresi essi e sta st nce ce thhat at may ma a de d vel veelop op p diff d ffererent n ly y acr ac oss o the w e orld.” d
The possibilities afforded by the work to reveal the structure of DNA continue to appear endless 70 years later. Crick, Watson and Wilkins were jointly awarded the Nobel Prize for Physiology or Medicine in 1962. Franklin died of cancer in 1958 aged 37, and in the intervening years, the focus on the crucial role her work played has heightened. “She didn’t get recognised, as many women scientists don’t,” Professor Syndercombe Court says.
“Without that photo and measurements from that photo, the discovery would have

The he h po possi s bil b bi iti it es e aff afford or ed b the wo work rk k to t rev re reveal al a th the s es e tru u t cture re of o DNA DN D contitinue nu to t appppear ea e endle le l ss 70 0 yea years rs lat a la er. Cr Crick k ck, , Wat Wa son s an a d W dWWilklkins i we w re joiointl t y a awar ar warded ded de the heth No Nobel l b Pr Prize ze fo for P rPhys hy iol l i ogy o or r Me M dicine in n n 196 9 2. 2 Frarankl n in dieed o d of c fccanc an er r 195958 8 age a d 3 d3 37, 7 and a an n in n th the i e nte n rve rv n ning y gy g ear rea s, the foc c f us u on n the t cr c uci iuc al a rolle h eh e er wor p kp k play l yed ed d has ha h heeighghtenened. ed “She he h did id d d n’t t ge g t recocogniiseded, , as man m y wome om n s nscie i nti t sts do d n’t’t,” ,” Proofes fe f sor Syynde nd rco rcombe e Co C urt u saays. y “Wi W tho th ut ut t tha ha hat p p t hot h to a and nd n mea me measurureme me m nts t fro fr m t mt m hat h ha phhoto to t , t ,tthe h dis d scovvery ery r wo would ul ha have ve beeeen l nl n eft ef f to o otther he e s.” .” ” B M S

“Without that photo and measurements, the discovery would have been left to others”
TH E BI OM ED IC AL SC IENTI ST 2 1 SCI S ENC E E Cov C er r fea feeature
and measurements, the been to others” y








































ANTI MÜLLERIAN HORMONE (AMH) ACTIVE B12 BRAIN NATRIURETIC PEPTIDE (BNP) BONE MARKERS (SERUM) SERUM INDICES PRE-ECLAMPSIA ULTRA-LOW PSA XANTHOCHROMIA marketing@randox.com randox.com Visit store.randox.com to buy directly from Randox today Product availability may vary from country to country. Some products may be for Research use Only. For more information on product application and availability, please contact your local Randox Representative. INTRODUCING THE NEW ACUSERA TRUE THIRD PARTY CONTROLS Complete QC Solutions For Results You Can Trust VISIT US AT IBMS STAND 301 & 302
POINT-OF-CARE TESTING AND THE NEW ISO 15189:2022
In December 2022, version 4 of ISO 15189 was released. One major change was the inclusion of requirements relating to point-ofcare testing (POCT). This is set out in the introduction, as one of the three main changes. The other two are the realignment of the document to the format of ISO 17025 (Requirements for Calibration and Test Laboratories) and an increased emphasis on risk management. The standard highlights the importance of risk identification and management, encourages continuous improvement and puts the patient at its centre.
POCT was previously covered by two other ISO standards, ISO 22870, for POCT supported by medical laboratories, and ISO/TS 22583, a guidance document for services provided without access to




medical laboratory support. The advent of ISO 15189:2022 replaces ISO 22870 as an international standard, as of December 2025.
ISO 22870 was first written in 2003 and reviewed in 2016, to align with the 2012 version of ISO 15189. ISO 22870 provided specific requirements applicable to POCT and was required to be used in conjunction with ISO 15189. ISO 15189:2022 combines the two, creating one document for medical labs. The integration of POCT into ISO 15189:2022 helps to bring the accreditation of POCT to the fore, alongside accreditation of lab-based tests. Lab-supported POCT should be included in the scope of the management system and follow the requirements of the standard.
Specific references
Whilst there are references to POCT
throughout the document, the whole standard applies to POCT, as for any lab-based test. Where specific references to POCT are made in the standard (for example, with regard to reporting of results and management review), these don’t represent significant changes from the requirements of ISO 22870.
Specific references to POCT include clause 5.3.1, which requires medical laboratory services to describe and document their laboratory activities, including any POCT locations. This links to clause 6.3.1, which requires the facilities for POCT to be suitable premises to safely conduct POCT activities.
Clause 6.6 sets out the requirements for reagents and consumables, including POCT supplies. The acceptance testing requirements in this section give scope for various ways of acceptance testing, as long as no patient result is released before the test is verified. Whilst it is commonplace that non-lab staff perform POCT testing, it is important that the lab owns and controls the acceptance testing process.
Service agreements
A significant change for POCT is in the use of service agreements, between the laboratory and all locations using laboratory-supported POCT (clause 6.7). A service agreement is the tool medical laboratories will use to agree the level of service with clinical teams, including defining the clinical requirements, the governance arrangements and any
IMAGES: SHUTTERSTOCK
THE BIOMEDICAL SCIENTIST 23 SCIENCE POCT
David Ricketts, Alyson Bryant and Sarah Glover look at accreditation and point-of-care testing.
commercial considerations. It is an opportunity to define and communicate the responsibilities for all stakeholders who are involved in the clinical and financial approval or delivery of a POCT service.
Many organisations will recognise the challenges of establishing and running a multi-disciplinary POCT committee and will welcome the removal of this mandatory requirement from the standard. However, this certainly does not prohibit such committees. Services with a wellfunctioning committee may well continue to use this forum to agree and monitor POCT services and service agreements.
The revised ISO 15189 standard sets out requirements regarding patients, including the need to: establish and implement opportunities for patient and laboratory users to provide helpful information, to aid the laboratory in selection of methods and interpretations of results. provide patients and users with publicly available information about examination processes and when to expect results.
establish processes for identifying risks of harm to patients in pre-examination, examination and post-examination processes and mitigate these risks. identify opportunities for improved patient care and fulfilment of user needs, e.g. expanding the scope of activities, to develop actions to address these and to assess the effectiveness of those implemented.
These requirements are equally applicable to POCT services as lab-based testing, if not more so due to the direct patient contact involved in POCT testing.
Risk management
Risk management and the impact on the patient are paramount in
this version of the standard. Actions taken to address risks should be appropriate to the potential impact on results, personnel and patient safety. Validation and verification requirements include the service being clinically relevant to the question being asked for each test. The rules of quality control (QC) should be set and applied with regard to risk of a wrong result and assay stability. Other QC requirements point to the need of the IQC being as close to the human matrix as possible and that IQC tests clinically relevant decision points. It is important that the personnel delivering POCT testing have a good understanding of these requirements and ensure that any identified risks, deviations to process, or opportunities for improvement are recorded and discussed with the supporting laboratory.
One common pitfall when attempting to deliver POCT services is that there is often variation in location and staff/skill mix performing the tests. Care needs to be taken when training staff, to ensure that everyone understands the process, importance of POCT, and its impact on patient care.
Annex A of ISO 15189:2022 summarises specific requirements relating to POCT services, including governance, quality assurance and training (note that all of these are covered in detail throughout the main body of the standard). This Annex provides a good overall guide for the governance of POCT, including roles and responsibilities within a POCT service. The Annex also outlines the requirement for individual(s), with appropriate training and experience, to be appointed to be responsible for POCT quality, training and competency assessment. Each organisation will need to decide where these responsibilities will lie and be able to demonstrate how these are defined.
Extend accreditation
Uptake of accreditation of POCT services
in the UK is relatively low, with approximately 10 services holding accreditation to ISO 22870:2016. It is hoped that the inclusion of POCT in ISO 15189:2022 will encourage laboratories to extend their accreditation to include POCT services. POCT testing can be viewed as “just another pathology discipline” with its own clinical requirements and challenges, but able to be managed under the same management system as laboratory-based testing.
Even if POCT services don’t feel ready to apply for accreditation, working towards the requirements of ISO 15189:2022 will support service development and improvement.
ISO 15189:2022 aims to promote the welfare of patients, reducing potential harm to patients, personnel, the public and the environment. The standard facilitates cooperation between medical laboratories and other healthcare services and sets out the requirements to identify risks and opportunities for improvement throughout the patient pathway, from patient preparation to result reporting and advice to users.
The National Strategic Guidance for Point of Care Testing, published in May 2023, outlines how to deliver safe and highquality POCT within an accreditable framework. High-quality, safe and effective POCT has a vital role in supporting rapid growth in the delivery of healthcare and diagnostics closer to patients, at the point of need. BMS
David Ricketts is Head of Laboratory Process Improvement at Health Services Laboratories, Alyson Bryant is the Healthcare Accreditation Specialist at UKAS and Sarah Glover is a Consultant Clinical Biochemist and POCT Clinical Lead at Harrogate and District NHS Foundation Trust. UKAS will be delivering talks on accreditation of POCT services at IBMS Congress on , and September.
THE BIOMEDICAL SCIENTIST 24 SCIENCE POCT
•CE-IVD compliant

•Compatible
instruments
•Ideal for POCT due to its inactivated format






We look forward to meeting you on stand 126, where our dedicated experts will be available to discuss, share insights, and demonstrate the practical applications of our high-quality tools for accurate and efficient diagnosis.


These include a wide range of assays, from ACE to Zinc, and everything in between, plus verified Third Party Quality Controls for ISO 15189 compliance.




As the leading UK supplier of calprotectin assays, with solutions for every testing regime, we help simplify stool testing workflows with the CALEX extraction device, that now enables safe sample collection at home.



Discover our complete Faecal Immunochemical Testing (FIT) service, and the logistics benefits of our new online portal for FIT-KIT management.
Together with a wide range of laboratory consumables, many with sustainability benefits for your lab, there are many reasons to visit us at Congress. We look forward to seeing you.


HELPING SOLVE MICROBIOLOGICAL PROBLEMS Telephone: 01782 516010 welcome@bioconnections.co.uk www.bioconnections.co.uk Visit us at IBMS Congress Hall 3, Stand 124
offers reliable molecular controls that imitate patient samples, ensuring accurate and consistent assay performance for various infections, including HAI, STIs, GI Infections and Respiratory Infections
Microbiologics
and
with several diagnostic kits
Come visit us at stand 126 or for more information visit our NEW website at: www.alphalabs.co.uk 02380 483000 • sales@alphalabs.co.uk
Discover Laboratory Excellence: At IBMS Congress with Alpha Laboratories
A STAND 126
Interview with the University Hospitals of Morecambe Bay
Dr Andrew Brown and Janet Eglin discuss the benefits the DxI Access Immunoassay Analyser has had for their blood sciences laboratory.
What have you used the DxI Access Immunoassay Analyser for in your laboratory?
Dr Andrew Brown: We were pleased to get hold of a DxI to perform an independent evaluation of it in our busy blood sciences laboratory. We tested the performance of sixteen immunoassays to verify the company’s claims, especially focussing on precision.
What
are the strengths
of the DxI Access Immunoassay Analyser?
Dr Andrew Brown: With no daily maintenance, the analyser can be up and running very quickly. It’s also very easy to use – my colleagues even let me use

it, and I haven’t managed to break it yet! Its low maintenance and ease of use take the stress off staff, letting them have time to concentrate on the things they really want to focus on.
The assays are stable, and we have been really pleased with the precision.
How does it compare to other available equipment?
Dr Andrew Brown: We compared it to the DxI analysers. Although there is good agreement between results across the two systems, we’ve seen much better precision for a lot of assays on the DxI . Assay times are faster for all tests, which is important when analysing samples from A&E. In some cases, sample volume was reduced
when compared to the previous analyser, which benefits patient groups such as neonates.
How important is precision in lab tests?
Dr Andrew Brown: It’s very di cult to achieve anything without adequate precision.
Just how good the precision needs to be depends on what you are trying to achieve or what the assay is being used for. If you are monitoring a patient, precision is one of the most important assay characteristics. However, if you just want to screen for something, then having clear blue water between positive and negative is more important.
Can the DxI Access Immunoassay Analyser positively impact turnaround
times?
Dr Andrew Brown: Yes, with its high
THE BIOMEDICAL SCIENTIST 26 ADVERTISEMENT FEATURE: BECKMAN COULTER
throughput and faster assay times, the DxI will improve our turnaround times. For example, troponin has gone from a -minute assay to an -minute assay, which will greatly impact sample flow through our laboratory and reporting to our Emergency Department clinicians. For tests like troponin, you’d want the result really quickly because the clinicians need the result quickly.
Samples taken in our primary care setting may have taken several hours to reach us anyway, so assay time for the individual patient isn’t as important, but we still need to achieve the throughput.
What are the benefits of disposable tips?
Dr Andrew Brown: I have a lot of faith in the disposable tip on the DxI because rather than just relying on the tip doing the job that we think it’s doing, the instrument carries out lots of imaging and measurements to make sure that it has actually drawn up the right volume of sample. Other important stages of the analysis, such as substrate addition, are also monitored via images.
The previous generation of DxI has a fixed tip, and although the washing of it has been very good, we now have disposable tips, so any risk of sampleto-sample carryover is eliminated.
Will patients see any benefits when a laboratory uses this new instrument?
Dr Andrew Brown: Patients, especially those in the emergency department, will benefit from getting results faster, which will, in turn, mean that they can be triaged faster – either to a ward, another department or home.
I’m really pleased to see the new substrate’s impact on assay performance too - we’ve seen good precision for all the assays, but for some of them, it is noticeably better than it was. This is really important in terms of patient care when the test is
being used for monitoring purposes. Based on what we have seen with the new analyser and new substrate, I am looking forward to further assay developments and the benefits to both patients and staff
How much maintenance is required?
Janet Eglin: Remarkably, it requires no daily maintenance, only a quick weekly clean which runs in less than minutes, and a short monthly procedure which takes a similar amount of time.
Minimal maintenance is important so that we can ensure uptime within the laboratory, which helps us meet turnaround times and frees up staff
What benefits does it bring to the workforce?
Janet Eglin: The lack of daily maintenance and built-in instrumentguided troubleshooting procedures mean that our staff will have time to focus on the samples that need looking

at. This will ultimately benefit our patients, who are our primary responsibility.
Why should labs invest in the DxI Access Immunoassay Analyser?
Janet Eglin: It will improve turnaround times and give precise results. With no daily maintenance, early error detection, and reduced investigation time for problems, the DxI will give staff more time in their day. By saving staff time, it enables laboratories to look at the quality improvements that can be made to the entire sample journey. When you’ve got continuous quality improvement, then you are reducing time wasted. This means that every minute you are working actually benefits patients, and you’re wasting less time.
THE BIOMEDICAL SCIENTIST 27 BECKMAN COULTER: ADVERTISEMENT FEATURE
By saving staff time, it enables laboratories to look at the quality improvements that can be made to the entire sample journey
AutomatedImmunosuppressantAnalysis
Simultaneousquantificationofkeyimmunosuppressantdrugsinwholebloodwith:
Calibrators(6levelsandblank),Internal StandardsandQualityControls(4levels)
Ready-to-useconsumables: Calibrator, InternalStandard,QualityControl, MobilePhaseA,MobilePhaseB,System CleaningPhase,Extraction& ReconstitutionBuffer,Analytical&Trap Columns.

Highthroughputanalysiswithautomatedsamplepreparationand CE-IVD/IVDRclassAdevices

Exampleofhigh-throughputconfiguration
info@shimadzu.co.ukwww.shimadzu.co.uk
RECENT ADVANCES AND UPDATES IN BIOMEDICAL SCIENCE
Deputy Editor Ian Paterson, from the Department of Oral and Craniofacial Sciences at the University of Malaya, summarises the articles recently published in the British Journal of Biomedical Science.
Two articles published in April were submitted as part of the Journal’s special issue “Education and Training in Biomedical Science”. The first was a review by Pearse and Scott, which discussed the historical challenges in clinical laboratory education, training and progression and how these were impacted by COVID-19. Prior to the pandemic, the clinical laboratory workforce was already undergoing a transformation following the Carter reports and the Modernising Scientific Careers initiative. The creation of pathology networks, with an emphasis on standardisation, digitisation and IT connectivity, required laboratory professionals to be flexible and willing to undertake relevant lifelong learning
to react to changing demands. With the background of such challenges, the pandemic hit and had a huge impact on teaching and learning, including online assessments and the acquisition of practical skills for trainees in a virtual environment. A discussion of the impact on clinical services and the mental health of the workforce is beyond the scope of this summary, but is reviewed in detail by the authors. The review identifies the need for more research into the impact of pre- and post-COVID challenges on the workforce. Despite these challenges, long-standing issues, such as staffing, resources and the mental health of staff, are now receiving attention. It is hoped that the IBMS Corporate Strategy 2022 and the 2023 revised Quality
Assurance Agency (QAA) benchmark statement for biomedical sciences will be reflected in higher education courses, ensuring a sustainable, competent, flexible and diverse workforce that is rightly appreciated, respected and rewarded.
The ability to effectively communicate research findings to the scientific community and the public is a vital transferable skill that needs to be developed in both undergraduate and postgraduate settings. Both the IBMS and QAA require the development of such transferable skills in accredited programmes. The COVID-19 pandemic clearly highlighted the need to communicate complex biology effectively and clearly to the general public. Continuing with the general
IMAGES: SCIENCE PHOTO LIBRARY/SHUTTERSTOCK SCIENCE Journal synopsis 29 THE BIOMEDICAL SCIENTIST
theme of training and curriculum development, Millar et al. report on an action research project designed to create an online resource, or “toolkit” to develop communication and digital literacy for undergraduate biomedical science students at Ulster University. A mixed methods approach was used involving final-year students undertaking a research project and staff and included questionnaires, focus groups and surveys to develop the resource. An online scientific communication and digital capabilities toolkit was prepared to support students in preparing three outputs – a visual abstract, lay summary and written reflection focusing on educational experiences within the module and employability. Feedback from students and staff was positive and students recognised the importance of such transferable skills for employment.
Reference intervals for parathyroid hormone using Abbott methods
Parathyroid hormone (PTH) is secreted by the parathyroid glands and hyperparathyroidism is the term used for a group of disorders that result from excess PTH secretion. It can be primary as a consequence of autonomous secretion in one of the four glands, or secondary due to low calcium and/or low vitamin D. An accurate measurement of PTH is essential for the identification of patients with hyperparathyroidism and also upon an accepted range of PTH concentrations in healthy individuals – the reference interval (RI). Mirzazadeh and colleagues examined “local” RIs from four different sites across the UK – Oxford, Birmingham, Buckinghamshire and Epsom St Helier NHS trusts. All sites used the i2000 Abbott Architect intact PTH assay as recommended by the manufacturer. The study collected data from 1727 adults to calculate plasma PTH reference intervals. The manufacturer’s recommended normal range for plasma PTH was 1.6–7.2 pmol/L.
Although the manufacturer states that data from different labs may vary and local ranges should be determined, the reference range of 1.6–7.2 pmol/L is widely used in clinical practice. The results showed that all four sites had different upper limits and the site-specific upper limits were all higher than those quoted by the manufacturer. The combined RIs from the four sites was approximately 3–14 pmol/L. Interestingly, these limits were similar to those found in a recent report by Minieri et al. (2021) in Italian patients. The four sites involved have now adopted their own locally derived RIs and the data provide strong evidence that locally derived plasma PTH RIs are required for the adult UK population to prevent misdiagnosis and inappropriate patient follow-up.
Hospital reservoirs of multidrugresistant Acinetobacter species Hospital-acquired infections (HAIs) represent a major clinical problem.

It is estimated that environmental contamination contributes up to 20% of all such infections and there is strong evidence to show this contributes significantly to the spread of pathogens, including multidrug-resistant organisms (MDROs). In this review, Fahy et al. focus
on one opportunistic pathogen, Acinetobacter baumannii, to highlight some of the problems associated with environmental contamination and to suggest ways to reduce the impact of such HAIs in the future. A. baumannii are Gram-negative coccobacilli that are most often associated with aquatic environments that are thought to be responsible for approximately 2%–10% of all Gram-negative HAIs. A. baumannii is a particular problem because it is an opportunistic pathogen, a biofilm former and an environmental reservoir of mobile genetic elements that can potentially be transferred to other pathogens. One gene, ompA, encodes OmpA, a key stress and virulence factor that leads to apoptotic cell death. OmpA is also responsible for the formation of biofilms on surfaces, which increase bacterial survival in hospital environments. A. baumannii has also been shown to be extremely antibiotic resistant, with resistance to third-generation cephalosporins and carbapenems being reported several decades ago. The authors conclude that current screening for environmental contamination with MDROs in clinical settings is inadequate and needs to improve to extend the usefulness of current antibiotics. It is suggested that A. baumannii could be a useful marker organism in microbiological screening protocols for the presence of other pathogens.
Faecalibacterium prausnitzii as a potential therapy for type 2 diabetes
The microorganisms that grow in the intestinal tract, the gut microbiome, are now recognised as playing a major role in health and disease. One such organism, Faecalibacterium prausnitzii, has been shown to secrete anti-inflammatory compounds and a decreased abundance of F. prausnitzii has been found to be associated with a number of human diseases, including diabetes, suggesting that F. prausnitzii has some anti-diabetic properties. The study
THE BIOMEDICAL SCIENTIST 31 SCIENCE Journal synopsis
“Hospital-acquired infections represent a major clinical problem”
by Xuan et al. initially used qPCR to show that the abundance of F. prausnitzii was significantly lower in the faeces of patients with type 2 diabetes compared with healthy control subjects. They went on to use a mouse model of type 2 diabetes to examine the specific role F. prausnitzii in the disease. They used leptin receptor-deficient mice that developed a phenotype that is similar to type 2 diabetes with symptoms including insulin resistance, obesity, hyperphagia, hyperinsulinaemia and non-alcoholic fatty liver disease. The results showed that dietary supplementation with F. prausnitzii resulted in decreased fasting blood glucose and insulin resistance. F. prausnitzii also improved inflammation in both adipose tissue and liver, and ameliorate hepatic steatosis through inhibiting the activity of hepatic lipogenic enzymes. Taken together, these results suggest that F. prausnitzii might be a therapeutic option for patients with type 2 diabetes.
Elevated expression of miR-296 as a potential marker for pre-eclampsia

Pre-eclampsia (PE) is a condition that affects some pregnant women and affected women present with hypertension and proteinuria. There is a risk of serious complications for both mother and baby. However, the exact causes of PE are not well understood but it is thought to be due to problems with blood supply to the placenta. It would be beneficial to be able to identify those individuals who are at greater risk of developing PE. MicroRNAs are small, highly conserved non-coding RNA molecules involved in the regulation of gene expression. It was reported by Choi et al. in 2013 that a microRNA, miR-296, was elevated in patients with PE but the possible clinical utility of this observation has not been examined. The report by Zhu et al. shows that miR-296
expression was significantly increased in serum samples from both early and late onset PE compared with women with healthy pregnancies. The levels of miR-296 decreased after delivery. ROC curves were constructed and miR-296 levels could differentiate early and late PE patients from healthy control mothers. Interestingly, miR-296 is thought to play a role in angiogenesis. The authors suggest that miR-296 is a potential biomarker for the diagnosis and predicting the developing of PE.
CCAT1 – a potential biomarker in colorectal cancer
Colorectal cancer (CRC) is the third most common cancer and second deadliest cancer in both men and women in the world. The five-year survival of patients with CRC remains relatively low, particularly for those patients diagnosed with stage III and IV disease. Long non-coding (lnc) RNAs are non-coding RNAs longer than
200 nucleotides. lncRNAs primarily interact with mRNA, DNA, protein, and miRNA and consequently regulate gene expression at multiple levels to regulate many biological processes. Deregulated expression of many lncRNAs has been reported in carcinogenesis, including colon cancers. lncRNA colon cancerassociated transcript 1 (CCAT 1) is an oncogenic lncRNA that is overexpressed in CRC and is associated with tumorigenesis and resistance to chemotherapy. Liau et al. have reviewed the role of CCAT 1 in colon cancer and summarised its function in CRC carcinogenesis. CCAT 1 is produced as two isoforms – a short transcript, CCAT1-S, which resides in the cytoplasm, and a longer form, CCAT1-L, which remains in the nucleus. Both isoforms have been detected in CRC tissues. CCAT 1 is associated with advanced features of CRC, such as lymph node and distant metastasis, and functions to promote tumour cell proliferation, migration and invasion. It is associated with the inhibition of apoptosis and chemoresistance. Mechanistically, CCAT 1 positively regulates the transcription of the c-MYC oncogene and acts as a molecular sponge to bind and inhibit a number of miRNAs. Collectively, this information suggests that CCAT 1 is a potential biomarker for screening and prognostication, as well as being a possible future therapeutic target. BMS
THE BIOMEDICAL SCIENTIST 32 SCIENCE Journal synopsis
“miR-296 is a potential biomarker for predicting the developing of pre-eclampsia”







Short courses for CPD, and for PG Cert, PG Dip and MSc Awards in •Biomedical Science (Online) IBMS accredited •Haematology •Healthcare Management •Healthcare Quality Management Book now for April and October starts www.biomedonline.co.uk IBMS member discounts available
THE EVOLUTION OF TRADITIONAL MEDICINE






From shamans and witches to contemporary use of





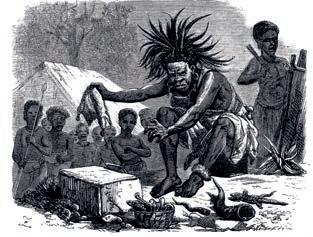

Seeking relief from pain is a common instinct to both man and animals, for example chimpanzees in Gombe national park in Tanzania eat the leaves of a plant called Aspilia rudis, which is not part of their usual diet, yet they seek them out and carefully eat the spiky leaves. Interestingly, local herbalists use extracts of the same plant for stomach upsets as it demonstrates both antibacterial and anti-parasitic activities.
Capuchin monkeys in Costa Rica rub their fur with leaves from the Piper plant (Piper fimbriulatum), a member of the chilli family that contains compounds like germacrene A and D (C15H24) that deaden pain and kill off insects. They also rub their fur with millipedes, which make toxic chemicals known as benzoquinones (C6H4O2) that keep other insects away, as well as killing bacteria.
The shaman

Conscious intelligence, which is peculiar to mankind, teaches people to seek pain relief intelligently. So, in the past a sick person might go and seek advice from the tribe’s healer, witch doctor, medicine-man, or shaman before they decided to embark on self-treatment. The idea of a shaman conjures up an image of a man or woman dressed in animal skins or bird feathers with elaborate tattoos, dancing or singing near a fire, and chanting admonitions to deities. Historically, however, the term shaman has been used by hunter and gatherer groups from the Pleistocene period onward and can be seen as the first religion of humankind, having been in

IMAGES: ©WELLCOME COLLECTION
From shamans and witches to contemporary use of medicinal plants and health tourism, Stephen Mortlock looks at traditional medicines through the ages.
TH E BI OM ED IC AL SC IENTI ST SC IEN C E The Big Stor y

THE BIOMEDICAL SCIENTIST 35 SCIENCE The Big Story
existence for more than 99% of our existence as a species.
Because they were from the community, traditional healers usually knew their patients personally, and were well acquainted with their backgrounds, lifestyles and cultural beliefs. They would take into consideration the emotional state of the person they were treating, as well as their harmony with the environment. The shaman/ witchdoctor acted as a conduit to harness the healing power of nature, using both herbs and foods as medicine. In these societies, those who wanted to become shamans or witchdoctors would often undergo prolonged rites of passage. At an early age, the future shaman was frequently set apart from others, submitting to painful initiations to establish their credentials and to instruct them in the ceremonial practices of the tribe and show them the collection and use of herbal remedies. On reaching maturity, and perhaps after enduring further ritual ordeals to test their vocation, they would be apprenticed to the elders before being allowed to practice.
For thousands of years, these healers have used plants to cure illness. Aspirin (acetylsalicylic acid – C9H8O4), the world’s most widely used drug, is based on compounds originally extracted from the bark of a willow tree (genus Salix), and more than a quarter of medicines found on pharmacy shelves contain plant compounds. The Amazon, the world’s largest tropical forest is home to a quarter of all botanical species on this planet – as well as many Indian tribes whose medicinal plants have never been studied by Western scientists. In Tales of a Shaman’s Apprentice (1994), ethnobotanist Dr Mark Plotkin recounted his travels and studies with some of the most powerful Amazonian shamans, who taught him the plant lore their tribes have spent thousands of years gleaning from the


rain forest and which we are now investigating as powerful new medicines to combat health crises such as Alzheimer’s disease and cancer. Early humans gained knowledge about edible materials and natural medicines that would alleviate and treat diseases either by accident or from knowledge passed down from one generation to another. Fossil records suggest that the human use of plants as medicines may be traced back at least 60,000 years in Iraq and 8000 years in China. Even written records about medicinal plants date back at least 5000 years to the Sumerians, who described well-established medicinal uses for such plants as laurel (Laurus nobilis), caraway (Carum carvi), and thyme (Thymus vulgaris). The Greek holistic medical system “Unani” can be traced back 2500 years and recognises the mental, emotional, spiritual and physical causes of illness or health, believing that everyone should take responsibility for their own wellbeing. Their doctors prescribed the fruit of the bullwort plant (Ammi majus), a member of the carrot family Apiaceae, to assist the harmony between physical and spiritual being, believing it acted as a blood purifier and diuretic. (It also helped to decrease flatulence.)
History

For many years, traditional medicines were often seen as fringe medicine, but they have been practised in many countries throughout the world over many centuries, are still used in some societies today and represent an important part of their healthcare.
Practices of traditional medicine, however, vary greatly
































from country to country and from region to region, as they are influenced by factors such as culture, history, personal attitudes, and philosophy. In the past, traditional medicine was often forced underground due to pressure from missionaries and governments who perceived such practices as witchcraft. In 1545, Spanish physician Andrés Laguna (1499–1559) provided an account of an ointment found at the residence of an elderly couple suspected of witchcraft: “…a jar half-filled with a certain green unguent… with which they were anointing themselves… was composed of herbs… which are hemlock, nightshade, henbane, and mandrake.” The herbs henbane (Hyoscyamus niger), nightshade (Atropa belladonna) and mandrake (Mandragora officinarum) contain tropane alkaloids, such as atropine (C17H23NO3), a muscle relaxant that has been used to calm patients during surgery before the administration of anaesthesia (atropine also remains the go-to antidote for nerve gas poisoning) and also hyoscine or scopolamine (C21H30BrNO4), a common treatment for motion sickness, nausea and stomach cramps.
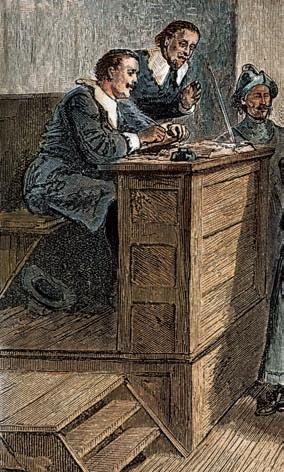
THE BIOMEDICAL SCIENTIST 36 SCIENCE The Big Story
Witches
The Salem witch trials between 1692 and 1693 saw more than 200 people accused of witchcraft and thirty were found guilty. Nineteen were executed by hanging, one man was pressed to death and at least five other people died in jail. Unfortunately, there was a gender bias, with most of the accused being women, but perhaps many of these women considered witches may have been practising traditional medicine and were, in fact, simply connoisseurs of plant species with biological properties. The seventeenth and eighteenth centuries saw the “Age of Enlightenment” across Europe with advances in science and medicine, and the dissemination of “rational” knowledge through the medium of newspapers, effectively dispelling witchcraft as “ignorant” beliefs. It was strongly believed that the passing of the 1736 Witchcraft Act would effectively consign the subject of witchcraft into the annals of the past. The differentiation between orthodox and unorthodox medicine was further defined with the Apothecaries Act of 1815, followed by the Medical Act of 1858. These pieces of legislation clarified that doctors who were officially trained and licensed practitioners on the medical register were the legitimate representatives of medicine, and all others were irregulars and open to prosecution if they misrepresented themselves.
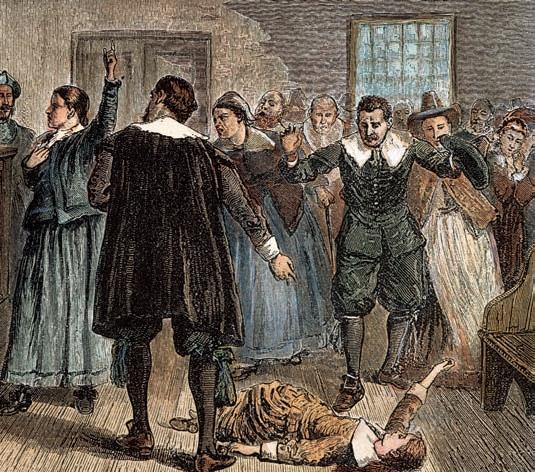
Modern times
In 1997, the WHO developed guidelines for “methodology on research and evaluation of traditional medicine”, the purpose of which was to promote the proper development, registration and use of traditional medicines and to harmonise the use of certain terms. In 2006, it established a global network of the worldwide regulatory authorities responsible for the regulation of herbal medicines to develop and issue technical guidelines for the assessment, safety and efficacy of herbal medicines.
In 2014, Dr Si-Yuan Pan and colleagues published Historical perspective of traditional indigenous medical practices: the current renaissance and conservation of herbal resources and took a thorough look at Chinese, Indian, and Arabic herbal medicine over the centuries. They found various kinds of herbal remedies have evolved based on the cultures and geographical region and have blossomed into an orderly often well-regulated system of medicine.
Traditional medicine evolved as a system of medical practice based on empirical knowledge as well as theories and concepts, many of which are unmapped by the scientific communities. Studies have shown that practitioners of traditional medicine tend to utilise a holistic approach to investigate problems on three levels: physical, emotional and spiritual, which can be quite effective in treating both chronic diseases and psychological problems, especially those associated with stress from social alienation, anxiety or loss of self-esteem. Holistic treatment emphasises disease prevention and positive changes in lifestyle to ensure a balance among these three aspects of life. Conversely, the Western medicine community tends to use evidence-based medicine, which integrates individual clinical expertise with the best available clinical evidence from systematic research. This has in recent years been established as the standard of modern medical practice for greater treatment efficacy and safety. But the use of traditional medicines has expanded globally and has gained popularity in the last few decades. Specifically, these practices have not only continued to be used for primary healthcare of the poor in developing countries but have also been used in other countries where conventional medicines are predominant in the national healthcare system.
Use of medicinal plants
Globalisation has brought about the availability and diversity of herbal medicines to the consumer and these have become increasingly popular throughout the world. Herbs and plants can be processed and taken in different ways and forms and they include the whole herb, teas, syrup, essential oils, ointments, salves, rubs, capsules, and tablets that contain a ground or powdered form of a raw herb or its dried extract. Medicinal

IMAGES: ALAMY/ISTOCK/SHUTTERSTOCK
THE BIOMEDICAL SCIENTIST 37 SCIENCE The Big Story
“The Salem witch trials saw more than 200 people accused”
plants can be broken down into several broad categories: Phenols: These are broadly distributed in the plant kingdom and are the most abundant secondary metabolite. Often antiseptic and anti-inflammatory, these are produced by plants to prevent infection. Plant phenolics include phenolic acids, flavonoids, tannins and the less common stilbenes and lignans. Some of the most common flavonoids include quercetin, a flavonol abundant in onion, broccoli, and apple; catechin, a flavanol found in tea and several fruits; naringenin, the main flavanone in grapefruit; cyanidin glycoside, an anthocyanin abundant in berry fruits (blackcurrant, raspberry, blackberry); and daidzein, genistein and glycitein, the main isoflavones in soybean. Carnosol, found in rosemary and sage, has anti-inflammatory, anticancer and nerve protective activity. While thymol, present in thyme, is antiseptic and antiviral. Volatile oils: Once extracted from the plant, these constituents are known as essential oils. They can contain 100s of different compounds and have many uses. Some oils are relaxants and relieve pain e.g. lavender, others are stimulants and anti-inflammatory, e.g. ginger.
Proanthocyanins: Known for the red, purple and blue colour they impart to flowers and fruit, e.g. hawthorn berry, these constituents support cardiovascular health and counter inflammation within blood vessels.
Coumarins: Present in many plants, e.g. the genus Angelica (family: Apiaceae), these constituents have variable activity; some are anti-inflammatory, some antimicrobial and anticancer
while some reduce anxiety. And of course, coumarins (e.g. warfarin) are used for the treatment and prophylaxis of venous and arterial thromboembolism.
Saponins: These form a soapy lather in water. Many have key medicinal activity, in part due to their similarity to the body’s own hormones, such as oestrogen and cortisol. For centuries, indigenous people around the world used the root of the sarsaparilla plant for treating joint problems such as arthritis and for healing skin problems, such as psoriasis, eczema and dermatitis. Sarsaparilla contains at least five different steroidal saponins.
Cyanogenic glycosides: In small doses, these constituents, which are based on cyanide, relax respiratory muscles, making them useful in soothing dry, irritable coughs. Elderberry contains low levels of these compounds.



Polysaccharides: Present in all plants, these compounds are found in mucilage and gums, and help the plant to maintain water levels. They are soothing to the skin and mucous membranes. Some also support immune function.
Alkaloids: These are some of the most powerful plant constituents, morphine from the opium poppy being a prime example. Capsaicin is another alkaloid –the constituent most responsible for the heat in chilli pepper.
Conclusions
Traditional medicine, as defined by the WHO, utilises the knowledge, skills, and practices based on the theories, beliefs, and experiences indigenous to different cultures for the maintenance of health as well as in the prevention, diagnosis, improvement, or treatment of physical and mental illness. Some traditional medicine systems are supported by huge volumes of literature and records of the theoretical concepts and practical skills;
others pass down from generation to generation through verbal teaching. As part of health and wellness tourism, Western travellers to many Asian countries now often visit herbal centres looking for a cure for their health problems, if unable to find suitable treatment in their own countries. But, Dr Plotkin advises that like physicians in the West, traditional medicine practitioners are not infallible and vary in abilities. Both depend on their tools and knowledge to carry out the healing work and to reintegrate the patient’s health, only the traditional medicine doesn’t deal only with the physical ailments of the body. The body itself is treated as a material and spiritual complex, in the same way that medicines – from plant sources, minerals or animals – are treated with the same spiritual dignity.
It should be noted, however, that the use of unlicensed herbal remedies is not without risk. Professor Roger Byard (a University of Adelaide forensic pathologist) found potentially harmful substances in some herbal medicines, which may be a contributory factor in deaths of “health tourists”. Studies have found some herbal remedies have been adulterated with approved or banned drugs and even toxic heavy metals. Adulterants have been linked to a range of side effects of varying severity including hypertension, heart problems, psychiatric disorders and in some instances death. But it should be remembered that plenty of traditional remedies have produced the staple drugs of today. Traditional Chinese medicine gave the world ephedrine for asthma and the Quechua people of Peru gave Western medicine quinine for malaria. BMS

Dr Stephen Mortlock is semi-retired and currently working as a Locum Biomedical Scientist in the microbiology department at Frimley Park Hospital in Surrey. To read this article with full references, visit thebiomedicalscientist.net

THE BIOMEDICAL SCIENTIST 38 SCIENCE The Big Story
Rapid, Whole Blood Analysers for Point of Care Testing
Simple, Fast Capillary Blood Analyser

•Glycaemic Control
•Kidney Function
•Lipids









•Coagulation
•Inflammation
NovaNet





With Wireless and Wired Connectivity to the LIS and EMR
Comprehensive Critical Care Blood Gas Analyser



•Combines blood gases, electrolytes, metabolites and CO-Oximetry
• Delivers a 24-test critical care profile in approximately 90 seconds, including urea, creatinine/eGFR

• Unique tests for iMg, and estimated plasma volume (ePV)
Glucose/Ketone POC Testing
•No known clinical interferences
•Only glucose meter cleared by US FDA and Health Canada for critically ill patients








Lactate/Hb/Hct POC Testing
•Rapid sepsis and anaemia screening and monitoring

•Measures both haemoglobin and haematocrit













novabiomedical.com





For more information contact us at uk-info@novabio.com
Creatinine, eGFR POC Testing


•Rapid identification of AKI
•STAT for renal function in imaging departments
Have you considered


determination of the biologically active or “free” fraction of target hormones.






Come and see us at IBMS Congress (Hall 3, stand 100) and discuss applications for saliva hormone testing, including sport medicine, womens health, fertility, sleep disorders and stress management.


Visit Us at Stand 307
Tel: +44 (0)1235 431390 Non-invasive sample collection Broad diagnostic applications • • • steroid hormones in saliva? Oxford Biosystems provide the IBL International highly sensitive ELISA and luminescence assays which have been specially developed and validated for saliva. www.oxfordbiosystems.com sales@oxfordbiosystems.com To advertise in The Biomedical Scientist please call: +44 (0) 20 7880 7556 Practical guidance for securing clinical A new tool developed of gene therapy: UNIVERSAL FLU VACCINE? Twenty strains, one jab Practica lab placemen too d lop p14 Twenty THEBIOMEDICALSCIENTIST.NET THE BIG QUESTION Biomedical scientists and direct-toconsumer testing: Working for continual improvement in the sample journey: Exciting new additions to the programme and speakers revealed: IT’S IN THE BLOOD Will liquid biopsies ever replace tissue biopsies? We investigate... An update from UKAS on transitioning to the new standard: p.22 How worried should we still be about COVID-19? p.16 A Ukrainian biomedical scientist discusses life in war zone: p14 THE BIOMEDICAL SCI ENTIST
SICKLE CELL ANAEMIA AND THALASSAEMIA A REVIEW
Shahid Muhammad, a Chartered Scientist and academic at Coventry University, looks at the issues in relation to transfusion medicine.
Haemoglobinopathies, especially sickle cell anaemia (SCA) and thalassaemia, are genetic conditions that, in severe forms, are affiliated with chronic life-threatening diseases with inherent haematological pathophysiology that can affect wellbeing and lead to death. SCA is estimated to affect one in every 2000 live births in England and there are currently up to 15,000 people with SCA in England, making it one of the most common genetic conditions. In the US, SCA is most prevalent among African Americans, and occurs in about one in every 365 AfricanAmerican births, compared with one in every 16,300 Hispanic births, and one in every 100,000 non-Hispanic White births.
Under certain conditions, individuals with SCA may require a blood transfusion or a series of transfusions. These may be episodic or for treatment of acute, potentially life-threatening disease complications. For some individuals, regularly scheduled, often life-long, chronic transfusions have been the primary treatment for disease.
Blood transfusion carries its own risk of significant, potentially life-threatening complications. The most concerning of these is red cell alloimmunisation, where the immune system of the host can elicit a response post-transfusion, which can cause delayed haemolytic transfusion reaction upon subsequent transfusion and iron overload. Patients with SCA/ thalassaemia and specific “clinical” symptomologies may not be considered
suitable to receive transfusion because of such alloimmunisation. Investigators inform us that examples of best practices for SCA/thalassaemia can be identified through the National Institutes of Health’s National Heart, Lung and Blood Institute (NHLBI).
Thalassaemia is an inherited red cell condition caused by quantitative defects in α- or β-globin chain synthesis leading to a shortened red cell lifespan. Thalassaemia major is the more serious form of the disease that results in severe anaemia and patients can become transfusion dependent. Every year, about 10,000 children are born with thalassaemia major. The condition also results in enlargement of organs such as the liver, spleen, and bone expansion, which occur as the body tries to

SCIENCE Haematology 40 THE BIOMEDICAL SCIENTIST
compensate by expanding haemopoietic tissue into these areas of the body. The clinical severity of SCA varies, in part based on different genotypes.
Those with SCA genotypes (homozygous Hb SS and Hb Sβ0 thalassaemia) generally have more severe anaemia and higher risk for severe complications than those with other SCA genotypes (e.g. Hb SC, Hb Sβ+ thalassaemia).
Red cell blood transfusion care
Transfusion practices are incorporating many novel pharmacological agents in view of the potential longer-term risks and side effects of transfusion. There is ever more need to consider the synthesis of the hormone erythropoietin (EPO) and in SCA/thalassaemia carriers, a synthesis defect can be the difference between morbidity and mortality.
Although risks are reported in the use of EPO; as pharmacological interventions are linked to varying pathophysiological
conditions, there has been a re-evaluation of the criteria for the use of blood. However, transfusion practices have not been modified due to fear of the mortality and morbidity related to anaemia, especially in “untransfusable” patients or those at risk of developing complications.
The ability of transfusion to facilitate the transport of oxygen from the environment to mitochondria has been repeatedly demonstrated in physiology research. The physical characteristics and properties of red blood cells (RBCs) are estimated to increase the solubility of oxygen 30-fold in blood relative to plasma. The affinity of RBCs for oxygen is modulated by regional acid–base conditions to favour oxygen loading at the pulmonary alveolar capillary interfaces as well as unloading at the tissue level. At present, there are no clinically available fluids that have the loading, unloading, and carrying properties of blood.
The paediatric population
In 2016/17 the NHS screening for SCA and thalassaemia programme identified 274 neonates in England with SCA and a further 8530 neonates as carriers. One investigation evaluated SCA care from 2004 to 2019, a period during which treatment approaches for paediatrics with SCA have changed significantly. These changes included the expanded use of hydroxyurea, which can reduce the severity of anaemia and lower the risk for SCA complications. There were 5316 unique paediatrics, ages 2–18 years old with SCA
enrolled in Georgia Medicaid from 2004 to 2019. Paediatrics receiving any transfusion increased from 2004 to 2010, then stabilised. In SCA patients, chronic transfusions initially increased from 2004 to 2010, then stabilised from 2010 to 2019. For chronically transfused paediatrics, monitoring of iron burden and filled chelator prescriptions both increased significantly. Hydroxyurea use in SCA patients increased from 12% to 37%, with increases noted within each age group, most notably from 21% to 60% in the 13–18-year-old cohort. While trends in clinical management do follow updates in treatment guidelines, there is still delayed and suboptimal uptake of guideline recommendations in paediatric SCA.
The decision to transfuse
The causes of preventable transfusionassociated complications are numerous and often occur because adherence to disease management and transfusion best practices are inconsistent. There is presently no unified system that provides ongoing, statewide education to healthcare service users and service providers. Clinical decisions are still challenged or questioned relating to patients’ understanding, professionals having knowledge about management guidelines, personal experiences with transfusion, and attitudes and beliefs. Biomedical/laboratory techniques and research have advanced over time, especially regarding human leucocyte antigen (HLA) tissue typing and crossmatching. Several authors also indicate failing tissue oxygenation would be ideal to guide the need for transfusion, but this has not proved effective, reproducible, or sensitive to tissue hypoxia. The clinical importance of the RBC storage lesion is still lacking. RBCs can be filtered, washed, frozen, or irradiated for specific indications. Donor screening and testing have dramatically reduced infectious
THE BIOMEDICAL SCIENTIST 41 SCIENCE Haematology
“In SCA patients, chronic transfusions initially increased from 2004 to 2010, then stabilised”
IMAGES: SCIENCE PHOTO LIBRARY/ISTOCK
risks in the developed world, making transfusion more widely accessible but infection remains a major hazard in developing countries, where 13 million units of blood are not tested for human immunodeficiency virus (HIV) or hepatitis viruses. Despite serious immunological and non-immunological complications, RBC transfusions (RBTs) still hold a therapeutic index that exceeds that of pharmacological interventions.
Guidelines and frameworks
Although RBT in the UK is safe, ensuring an effective blood supply has been vital. This requires a combination of highquality donor recruitment and selection, infection screening, serological testing and blood component production. The four UK Blood Services all maintain common standards for blood donation, testing and blood products. The Joint UK Blood Transfusion Services (UKBTS) and Joint Professional Advisory Committee (JPAC) are responsible for producing the guidelines for UK blood transfusion services, often known as the Red Book. Retrospectively, data from 2011 inform us that UK Blood Services issued 2.1 million units of red cells, 300,000 platelet doses, 288,000 units of fresh frozen plasma and 126,000 units of cryoprecipitate.
Managing anaemia

In “untransfusable” recipients large-scale trials are yet to take place to see whether, for example, EPO has wider advantages over RBTs, especially in patients who might be more at risk of transfusionlike reactions. One investigation retrospectively examined the association of EPO use with haemoglobin (Hb) recovery in anaemic untransfusable hospitalised patients. EPO-treated anaemic untransfusable patients were identified through the combination of a retrospective case review and a systematic review. Literature reports of untransfusable patients not treated with any EPO were used as a comparator
group. Investigators established that Hb recovery was higher in patients with lower baseline levels, irrespective of EPO utilisation. No association was identified between the rate of Hb recovery and EPO use, dose or duration. In anaemic, “untransfusable” hospitalised patients, EPO use was not associated with an increased Hb recovery. At the same time, the investigation did not include SCA/ thalassaemia cohorts as “untransfusable” patients at baseline, which may have provided some important insights of how to offer transfusion care in patients with such haematological conditions. There is still a requirement for a debate regarding transfusion and how care is managed and practised for SCA/thalassaemia recipients.
Transfusion alternatives
Different transfusion alternatives are known for the pre-, intra-, and postoperative period. Autologous blood donation and EPO-based pharmacological stimulating agents are efficacious in the pre-operative period. Intraoperatively, acute normo-volaemic haemodilution, cell salvage, anti-fibrinolytics, specific anaesthetic and surgical techniques, coagulation monitoring, acceptance of minimal Hb values
and artificial oxygen carriers can reduce allogeneic transfusion. In the postoperative period, cell salvage, antifibrinolytics, and accepting minimal Hb values are alternatives to transfusion.
The use of EPO to increase erythropoiesis offers an alternative to RBT, assuming normal, responsive progenitor cells and adequate iron, folate, and cobalamin stores. Prospective investigations should examine whether clinical outcomes from EPO use in SCA/ thalassaemia patients is effective. Because platelets play an instrumental role in primary haemostasis, platelet transfusions are often important in managing patients who are at risk of bleeding with thrombocytopenia or impaired platelet function. Platelet transfusions carry risks, and decisions to transfuse platelets must consider clinical circumstances, because platelet transfusion in such settings may fuel thrombosis and worsen clinical signs and symptoms and more issues for transfusion have been highlighted, even when considering alternatives.
Summary
An estimated 7% of the world population carry an abnormal Hb gene, while about 300,000–500,000 are born annually with significant haemoglobinopathies. Sickle cell syndromes are more frequent and constitute 70% of affected births worldwide; the rest are due to thalassaemias. Evidence in the literature stress the educational importance and necessity for patients and the public to be empowered and have capacity to link healthcare relating to history and haematological practices, including serology, immunogenetics, SCA/ thalassaemia phenotypes and immunohaematology. Alternatives to transfusion, including bone marrow transplants, should also be given consideration and focused evaluations of patient populations should help provide best use of treatment options deliberating haematology. BMS
THE BIOMEDICAL SCIENTIST 42 SCIENCE Haematology
“Although RBT in the UK is safe, ensuring an effective blood supply has been vital”
The Biomedical Scientist provides the best route for manufacturers and suppliers of clinical diagnostic products and systems, as well as general scientific laboratory products and services, wishing to influence this extremely important target audience.
For all the latest News, Events, Jobs, Resources and much more, visit thebiomedicalscientist.net










As the of cial magazine of the IBMS, The Biomedical Scientist is the main means of regular communication between the Institute and its membership of 20,000.

For all print and digital display advertising enquiries for The Biomedical Scientist please contact ibms@redactive.co.uk


Revolutionising Point-of-Care Testing: Exploring the Comprehensive Capabilities of QuikRead go®

Una Health unveils the new-generation point-of-care system QuikRead go®, overcoming the barriers to traditional testing pathways

Point-of-care testing (POCT) has the potential to reshape the delivery of healthcare.
The QuikRead go® analyser cuts through the noise of current POCT devices. This new-generation point-ofcare system is a versatile and reliable solution, designed to support diagnosis and treatment management when and where it is needed.
One device, multiple tests. What does QuikRead go do?
QuikRead go consolidates multiple lab-quality tests (CRP, Hb, HbAc, iFOBT, Strep A), into one portable, compact, automated platform, providing results in minutes; optimising workflow e ciency, reducing turnaround times and enhancing near-patient testing.
The QuikRead go platform complies with ISO: standards, has full connectivity and traceability of test results and participates in numerous EQA schemes. The minimal hands-on time, intuitive user interface and dedicated in-person or e-learning training (CPD accredited), make the QuikRead go system a platform of
choice for reliable, seamless and successful POCT implementation.
C-reactive protein testing. From paediatrics to hospital-at-home QuikRead go CRP combines e ciency, accuracy and speed with special features that make it highly versatile.
Broad measuring range: . to mg/l
Small finger prick sample: μl
Time to result: minutes
Wide haematocrit correction range
The precision and total CV value of % guarantee consistent and trustworthy measurements, enabling clinicians to make informed decisions based on the obtained result.
Widely embraced by the NHS and private healthcare sectors, QuikRead go CRP has gained popularity among hospital-at-home teams, providing a strong evidence base for optimal patient management at home.
HbAc measurement – where & when the patient needs it QuikRead go HbAc has the potential to reshape how diabetes management is being delivered, offering rapid, precise and sustainable testing within one patient contact.

Measuring range: -mmol/mol
Small finger prick sample: μl
Time to result: < minutes
The QuikRead go HbAc test is IFCC and NGSP certified and with a CV value of .%, it demonstrates high precision and consistency.
QuikRead go HbAc was used in a recent clinical trial, where it proved instrumental in optimising the management of diabetic patients, streamlining the check-up process, while improving the patient pathway and QOF compliance.
Faecal immunochemical test (FIT) - from community screening to GPs and hospitals
QuikRead go iFOBT is a game-changer in faecal immunochemical testing, taking the test to the patient. It can be easily deployed in hard-to-reach communities and low-compliance areas, improving accessibility to essential screening tools.
Wide measuring range: - μg Hb/g (aligns with national recommendations)
Time to result: minutes
Sensitivity: %; Specificity: %
Sample stability: up to days
QuikRead iFOBT was featured in an observational study showcasing its clinical utility for risk stratification, filtering referrals, preserving endoscopy and radiology capacity, cutting costs, and enhancing e ciency within the two-week wait pathway.
Want to find out more? Scan the QR code for more information and get in contact with us.


ADVERTISEMENT
UNA
FEATURE:
HEALTH THE BIOMEDICAL SCIENTIST 44
MY IBMS
#IBMSCHAT
NEW PODCAST SERIES LAUNCHED
Episodes of the new IBMS podcast series, "#IBMSChat Podcast", are now being added to SoundCloud, Spotify and iTunes to stream online. On the first Wednesday evening of every month, on Twitter, the IBMS continues to bring you the #IBMSChat to discuss various topics relevant to the profession.
Since the beginning of this year, Twitter Spaces has been used to deliver more engaging, live audio conversations that members can truly benefit from.
While these monthly Twitter Space-based #IBMSChats will continue to run as normal, the IBMS is also bringing members a new way of staying up to date with everything going on at the IBMS and the biomedical science profession with Series of the podcast.
ibms.org/resources/podcasts/ the-ibmschat-podcast
REGISTRATION TRAINING PORTFOLIO
Version 5.0 of the IBMS Registration Training Portfolio using a digital platform is now live.
The updated IBMS Registration Training Portfolio is aligned to the updated HCPC Standards of Proficiency (SoPs) for biomedical scientists.
For those who apply for the IBMS Registration Training Portfolio, Version 5.0 will be issued and completed using the established ePortfolio platform, Onefile.

Each module will retain three pieces of evidence. It is expected that across these all HCPC SoPs assigned to the module will be demonstrated and each piece of evidence will be clearly mapped to specific SoPs. Evidence two and three will be a free choice for candidates and their training officer, which should ensure flexibility, creativity and new ideas for evidence to be incorporated.
The IBMS has previously released a
simple mapping document to show where the updated HCPC SoPs will be in the sections and modules of the updated portfolio.
The stipulation of one piece of mandatory evidence for each module of the portfolio follows consultation with the Registration Training Portfolio working group, trainers and training managers, plus placement tutors and programme leads for IBMS Accredited programmes across the UK.
The rationale for introducing the mandatory pieces of evidence is to provide a scaffold for training plans and improve consistency.
Examples of evidence types, resources and further support will be provided by the IBMS at Congress 2023.
ibms.org/education/registrationportfolio
LEADERSHIP
CELEBRATING THE PROFESSION
The Pathologist’s “Power List” for has been announced.
Out of hundreds of submissions, scientists and laboratory professionals were selected –including two IBMS members:
IBMS President Elect Joanna Andrew, who is passionate about supporting the training and development of the next generation of biomedical scientists. Her work has enabled many laboratory support workers to train and study on apprenticeship degrees.
IBMS member Alan Deacon, who is passionate about using systemic leadership to effect positive change in pathology services and the wider health system. He has been the National Pathology Programme Lead in Wales since
IMAGES: ISTOCK
NEWS
EDUCATION
THE BIOMEDICAL SCIENTIST 45 XXXXXXXX Xxxxxxx xxxxxxxxxx MY IBMS News
Non-Gynaecological Cytology
Non-Gynaecological Cytology Updates for Experienced Staff
Urinary Tract, Respiratory & Serous Fluids
Three one-day courses covering serous uids, urine and respiratory. These are ideal for anyone wishing to further their experience in non-gynae and are suitable for both non-medical and medical staff.
8th, 9th and 10th November 2023
Non-Gynaecological Cytology Update
Salivary Gland and Thyroid Cytology
This course aims to provide an update and refresher of salivary gland and thyroid cytology. This day ia aimed at specialist registrars and quali ed pathologists as a refresher and workshop in these areas.
15th November 2023
Exam Practice for the ASD in Non-Gynae Cytology
Preparation sessions: Written Paper and Microscopy exam practice
This session will outline brie y what examiners are looking for in prospective candidates and allow them to answer questions and discuss answers.
Dates for 2024 coming soon – register your interest
Are you attending the IBMS Congress this year?
Why not pop along to our stand and have a chat about your training needs – you can nd us on stand R8 in the registration area – see you soon!
Training Opportunities 2023-24
Cervical Screening
Exam Practice for the ASD in Cervical Cytology
A two-day course ideal for anyone intending to sit the ASD in Cervical Cytology. The course will cover both written and practical elements and includes a marked mock exam.
Dates for 2024 coming soon – register your interest
Two-Day Course for Cervical Screening
Provider Leads (CSPL)
These one-day events have been put together in association with the NHSCSP Cervical Cancer Audit Management Group to help guide both new and experienced CSPLs through the various aspects of their role.

26th & 27th February 2024
One-Day Course - Breaking Bad News

This day is designed to give delegates the opportunity to explore some of the communication challenges they may face in their role as a CSPL.
28th February 2024
One-Day Update Courses in Cervical Cytology
These courses are designed to ful l the requirements of an update workshop.
Dates scheduled throughout 2023-2024
Enhanced liver fibrosismarkers
•
Histopathology/Molecular Sciences

Tumour Tissue Assessment for Molecular Testing


Theory & Practice within Histopathology & Cytology
This course has been developed for histopathologists, clinical scientists and biomedical scientists involved in the selection and assessment of tumour samples for genomic testing.
1st December 2023
Health Care Scientist Reporting in Histopthology
Stage A: GI, Gynae & Skin Exam Preparation
Day A one-day course speci cally for those working towards the scientist reporting quali cation and approaching or contemplating undertaking their stage A examination.
26th January 2024
Tissue Recognition, Section Quality and Clinical Consequences
This is aimed at BMSs preparing for their specialist portfolios and involved in the preparation of routine histology samples.
Dates for 2024 coming soon – register your interest
Haematological Morphology Study Days
Morphology and its Relationship to Disease
This course is designed for those studying for their specialist portfolio, also suitable as a refresher or an update for those already quali ed.
16th & 17th November 2023
rajvindergarcha@nhs.net
www.bcpathology.org.uk
0121 507 5348
Clinical Biochemistry, City Hospital
Dudley Road, Birmingham B18 7QH
@BCPathology
BCPathology
Black Country Pathology TV News
For further information contact our Admin Team: sht-tr.nepsec@nhs.net Tel: 0113 2466330 www.nepsec.org.uk
ELF & PIIINP
NPEX result reporting
•
Rapid automated immunoassay service
Clinical interpretation service
•
JOURNAL-BASED LEARNING EXERCISES
Please select your choice of correct answers and complete the exercises online at: www.ibms.org/cpd/jbl

DEADLINE WEDNESDAY 6 DECEMBER 2023
Geographically, a % increase in monthly COVID- cases was associated with %, %, and % higher macrolides sales in Europe, North America, and Africa, respectively.
Previous research has shown that one of the main causes of AMR is the inappropriate and excessive use of antibiotics in humans, but not in animals.
12
13
The clinical microbiology laboratory, as well as biomedical scientists, do not have a role to play in combatting AMR.
The consequences of failure to adequately address AMR are profound, with estimations of a return to the pre-antibiotic era, where everyday infections relating to childbirth, surgery and open fractured limbs could be potentially life-threatening.
In a survey, % of participants admitted that antibiotics could be used to treat bacteria and % of participants believed that antibiotics could be used to treat viral infections.
Some million deaths worldwide in were linked to bacterial AMR, and million of those deaths were directly caused by bacterial AMR.
A significant strong association was reported in a longitudinal study between the use of antibiotics and AMR, particularly carbapenems and carbapenem resistance.
14
Recent advances in biomedical science have allowed the development of total laboratory automation for the rapid detection and identification of pathogens, as well as for the determination of their antimicrobial susceptibility.
15 Investment by biotechnology companies into developing commercially available kits has allowed the widespread adoption of novel AMR diagnostics.
16
AMR has been discovered in bacteria, parasites and fungi, but not in viruses.
The agriculture sector is taking a proactive role in ensuring the responsible use of veterinary medicines, through the development of various antimicrobial stewardship programmes.
17
Gentami-cin-resistant Enterococcus was first identified in 08
The United Nations has identified sustainable development goals to combat AMR.
According to the World Health Organization (WHO), six countries and territories have established multi-stakeholder national action plans on AMR while countries are in the final stages of creating national action plans.
A recent study investigating global antibiotic use during the SARS-CoV- pandemic showed that sales of cephalosporins, penicillins, macrolides, and tetracyclines increased dramatically during April–May
18
Research indicates that % of all antibiotics used worldwide are used in farm animals, largely for food production. 09
19
The emergence of AMR now threatens the ability to detect pathogens using traditional selective microbiological media, without a radical rethink and reformulation of many of these selective agars.
20
Antimicrobial stewardship: how does your laboratory contribute to this effort? 02




AMR is receiving substantial political input from the G countries and continues to be on the agenda of numerous political conferences.
Antimicrobial resistance and SARS-CoV-: what impact did the pandemic have on your laboratory’s ability to contribute to the fight against AMR?
resistance (AMR). Tang KWK, Millar BC, Moore JE. Br J Biomed Sci. 2023 Jun 23;
: 11387. doi: 10.3389/ bjbs.2023.11387. eCollection 2023.
No 090123 01
Antimicrobial
80
Assessment
It is forecast that antimicrobial resistance will result in million deaths per year globally by 11
02
03
Human life expectancy has increased on average by years, since the first antibiotic was introduced in
04
05
06
07
10
LEARNING 01
REFLECTIVE
THE BIOMEDICAL SCIENTIST 47 MY IBMS Continuing professional development
DEADLINE WEDNESDAY 6 DECEMBER 2023
Acute myeloid leukemia: 2023 update on diagnosis, risk-stratification, and management
Shimony S,Stahl M,Stone RM. Am J Hematol.2023; 98 (3):502–26. doi:10.1002/ajh.26822.
Assessment No 090423
01
02
03
04
Estimated five-year overall survival rates for acute myeloid leukaemia (AML) range from % in younger patients to less than % in patients over years of age.
Because the NPM mutation is so common, it cannot be considered an AML-defining mutation.
The WHO considers secondary myeloid neoplasms as conditions caused by either cytotoxic therapy or germline predisposition.
Patients with a DDX mutation have a poorer prognosis than those with wild-type DDX.
From the following list of Enasidenib, Midostaurin, Ivosidenib, Venetoclax, Glasdegib, Gilteritinib, CC and Olutasidenib, only Ivosidenib is an IDH inhibitor AND is approved by the FDA for use as a combination therapy.

According to the European Leukaemia Network guidelines, the FLT-ITD allelic ratio is no longer included within the risk classification, in part, due to poorly standardised FLT assays.
07
The ICC requires a % blast threshold for acute myeloid leukaemias with recurrent genetic abnormalities, except for those with BCR::ABL.
11
12
13
14
In the context of AML, t(;)(q ; q ) is associated with the adverse risk category.
Rearrangement of KMTA is associated with a worse prognosis than its translocation involving MLLT::KMTA
In the context of the assessment of minimal residual disease, routine use of intensive screening with any technique is valuable for determining treatment outcomes.
According to ELN , complete remission with partial haematological recovery includes bone marrow blasts <%, absence of peripheral blasts, an absolute neutrophil count of ≥/
platelets
15
16
The general approach to cure AML is to achieve complete remission to reduce the leukaemia burden by several orders of magnitude and then to administer post-remission therapy.
Gemtuzumab ozogamicin and midostaurin are both monoclonal antibody-based therapies directed at CD
17
Referring to a study of patients with newly diagnosed AML, the one-year overall survival rate for patients treated with venetoclax combined with cladribine, idarubicin and cytarabine was %.
18 Ivosedinib and enasidenib both prevent the epigenetic alterations caused by the formation of R--hydroxyglutarate.
fi
karyotype includes cases with numerical chromosomal abnormalities (hyperdiploid karyotypes with multiple trisomies) in the absence of structural changes.
10 RT-qPCR can be used to establish minimal residual disease without the need for knowledge of specific cytogenetic abnormalities or mutations.
19 Gilteritinib plus venetoclax and gilteritinib plus venetoclax and azacitidine in relapsed AML could serve as a bridge to transplant.
20
In a trial of newly diagnosed AML enriched with TP mutations, % of patients achieved a complete response when treated with a combination of azacytidine and magrolimab.
REFLECTIVE LEARNING
Critically discuss the contribution basic research has made to our current understanding of the involvement of CEBPA disruption in leukaemogenesis and its role in the subsequent classification of acute myeloid leukaemia.
IBMS RESOURCES CONTINUING

My CPD


02
PROFESSIONAL DEVELOPMENT
Members can enhance their professional practice and development with the IBMS CPD scheme. The scheme offers members a flexible system of recording CPD that
is easy to use and meets the requirements for achieving and maintaining professional registration. The scheme is now electronic, so recording, amending and validating are all carried out online.
Provide an evidence-based justification for the differences in the WHO and ICC definitions of AML with recurrent genetic abnormalities.
Journal-Based Learning (JBL)
IBMS JBL involves reading and answering questions based on articles in scientific journals. It is an excellent way to learn about scientific
advances and techniques as part of CPD.
Reading resources
IBMS reading lists, textbooks and journals support learning and development.

,
L.
μL and
≥
/μ
05
06
08 WHO
uses a hierarchical approach to classification in comparison to the ICC’s use of two group classification.
09 The
de
nition of complex
01
THE BIOMEDICAL SCIENTIST 48 my ibms Continuing professional development











































































































































22
& 23 November
THE BIOMEDICAL SCIENTIST LIVE IS BACK FOR 2023! #IBMSLive23 For partner sponsorship/showcase enquiries, contact advertising@thebiomedicalscientist.net live.thebiomedicalscientist.net SIGN UP AT:
The virtual event, brought to you by the Institute of Biomedical Science (IBMS) , will be delivered over two days in November 2023. The Biomedical Scientist Live 2023 will feature a packed line-up of knowledge-sharing sessions, including seminars, presentations, discussions and demonstrations.













IVD solutions through partnership Quantitative FIT and Calprotectin from the same sample OC-FCa Faecal Calprotectin Contact us today for more information: +44 (0) 151 933 7277 email: FIT@mastgrp.com www.fit-screening.co.uk FIT and Calprotectin from the same sample Simplified lab processing with no sample extraction High throughput fully automated analysis Ready to use liquid controls and reagents
WORLD ALZHEIMER’S MONTH
Laboratory Manager Francis Yongblah talks through his personal experiences supporting service users with Alzheimer’s and dementia.
Thursday 21 September is the start of World Alzheimer’s Month. This month is essential for raising awareness, educating, encouraging support of and demystifying dementia. Alzheimer’s disease is a progressive condition, which means symptoms can develop gradually over many years and eventually become more severe. Alzheimer’s disease is the commonest cause of dementia.
There is lots of support out there for those with Alzheimer’s disease or dementia and support for family members and loved ones. More can be found on the NHS.uk website about diagnosing dementia and further information about World Alzheimer’s Month can be found on the Alzheimer’s Society website.
A day in the life of a carer
While studying my degree in biomedical science, I had a part-time job working as a carer. This was a job that I wanted to take on to get a bit of frontline
experience with the public and those that require the use of healthcare services. The role of being a carer was to visit the service user in their home to see how they were doing and to give much needed support to families and loved ones. I got to work with and support several service users with Alzheimer’s and dementia.
I always remember my first day and being quite anxious about what the job would entail. We drove up to see our first service user. On arrival we rang on the front doorbell before their wife came to open the door.
I initially found it quite upsetting on my first day to see individuals with so much life experience having loss of memory, or showing many different emotions due to confusion or frustration. On my first day I got to speak to the wife of our first service user. It was amazing to hear the lived experience of this individual.
I had learnt about all the travelling that they had done for work and that they had been all over Europe
and the UK. I heard stories about when they were raising their children and seeing them grow. Although they had lost some of their memories, there would be moments that they would remember, or mention particular words, which I learnt were related to an event or a memory they still had. It was nice to see they could still be themselves – finding joy and being able to smile. There were sad times, where there was frustration or confusion, even when they were in their own home. While it was sad, it was good to be able to be present to support their family at those difficult moments.
I will always cherish the time that I worked as a carer and having the opportunity to work with those with Alzheimer’s/dementia. Most important was being able to support those families and loved ones who may have been going through a difficult time. My time as a carer has always linked to my career as a healthcare scientist… always having a line of sight to the patient. BMS
THE BIOMEDICAL SCIENTIST 51 MY IBMS EDI IMAGES: SHUTTERSTOCK
IBMS Congress 2023 Back Bigger & Better!

IBMS Congress 2023 is just around the corner and Sonic Healthcare UK are pleased to be returning to the largest biomedical science conference in the UK. It is the perfect opportunity to engage with colleagues and share information across the professional network. This is the third edition of the event that Sonic Healthcare UK have attended – representing both The Doctors Laboratory and Health Services Laboratories under the one name.
Proud to Sponsor: Sonic will again be sponsoring the Education and Training programme.
way to build and retain a dedicated workforce that puts patient care at the forefront of their day-to-day decisions.
“We recognise the importance of supporting and developing our staff and are pleased to sponsor part of IBMS Congress. We are looking forward to listening to the range of speakers and taking the opportunity to share with delegates the training achievements of our own staff.”
What to See on the Stand: stand space to date.
A range of delegates attend Congress at different points in their career and
To arrange a chat with a Sonic
events@hslpathology.com


about potentially partnering with learn how their hub and spoke model coffee whilst learning more about the launch of the Sonic Training Academy competition to win anything from a

www.sonichealthcare.co.uk/ ibms-congress

Advertisement Feature
Sonic Healthcare UK sponsoring in 2022
Potential Academy Apprentices Visiting the Halo Building
Although it has been a year since our last website update, a lot of work has been going on in the background as software developers have been trying to find ways to integrate our website with our membership database to ensure that members’ data are securely and seamlessly transferable between the systems. In that time we have exhausted many different avenues to try to find solutions that enabled us to launch the new website and move users on to a different CPD system.
I’m sure that many of our members who work in IT, integrating different databases and software, will share some of the issues and frustrations we have faced. However, as the integration issues have still not been fixed, the website will not be ready to “go live” anytime soon.

Whilst the reasons we cannot launch are
A BETTER DIGITAL OFFERING
frustrating, the delay of the project has given us the opportunity to look at the whole of our IT infrastructure and to consider how we can develop a major IT plan to put the IBMS in a stronger position as we look to create a better digital offering for our members. This means that what started as a project to create a new website and bespoke CPD system has developed into a project that is far greater than we originally envisaged.
Under the direction of a new IT strategy, we are currently undertaking a review of our membership database that will act as the central piece of software for our other systems. This includes the new website and CPD system that will link to our e-learning portal and our new digital platforms for Certificates of Achievement, Registration Training Portfolios and the Specialist Diplomas.
This work will see the IBMS undertake major investment in technology that will better support our members and





























will ensure that we are future-proofed for many years to come. Due to the scale of the work required, it does mean that we will be delaying the website launch until further notice. All work already completed means that when other systems are ready and fully tested we will be in a better position to go live more quickly.
We understand that this is not the update that we had hoped to share with members, and we apologise for any inconvenience the move to a new CPD system may have caused. But we wish to reassure you that we will only go live with a system that is robust, fully tested and that protects our members’ data to the level that you would expect of us.
These further delays will give us time to update our current website and we will be making some improvements to the layout and navigation, making content easier to find and more engaging. Our CPD system also remains in place for all members to use and you can continue using it to record your activities and store your evidence in time for HCPC renewals this year. BMS






HERE TO HELP
53 THE BIOMEDICAL SCIENTIST MY IBMS Here to help IMAGES: ISTOCK/SHUTTERSTOCK
Dan Nimmo, IBMS Head of Communications, provides an update on the new website and CPD system.
CLINICAL DIAGNOSTIC PARASITOLOGY
The Clinical Diagnostic Parasitology Laboratory (CDPL) sits within the clinical sciences department of Liverpool School of Tropical Medicine (LSTM).

It provides a specialist diagnostic parasitology service to aid clinical diagnosis. Samples are received from many streams, including hospitals, clinics and health professionals locally and throughout the UK. The unit has a close relationship with the local infectious disease team within the Liverpool University Hospitals NHS Foundation Trust and hosts an NHS tropical outpatient clinic for the trust.
LSTM was the first institution in the world to be dedicated to clinical parasitology research and teaching, and is celebrating its 125th anniversary this year. Liverpool was an ideal port location for trade with West Africa in the late 19th century; this resulted in many patients suffering from diseases such as malaria arriving at the local hospitals. Medical officers started to examine entire ships’ crews, which resulted in the call for the establishment of a school specialising in tropical medicine, hence the formation of CDPL.
CDPL offers a wide variety of tests utilising a wide variety of sample types, including: microscopy and concentration techniques for blood parasites, including malaria, filariasis and trypanosomiasis; microscopy and molecular techniques for faecal parasites, including intestinal protozoa, nematodes, cestodes and
trematodes; microscopy, molecular and concentration techniques for the diagnosis of schistosomiasis; parasite antibody tests, including strongyloides, hydatid, schistosomiasis, malaria, filaria, fasciola and Entamoeba histolytica; examination of a variety of samples and tests for Leishmania diagnosis, including molecular test for diagnosis and speciation; cyst fluid examination for parasites and examination of whole worms and insects. The wide variety of tests offered and samples received ensures a dynamic workplace for the team with multiple hands-on tests being performed at the same time – there is no automation or analysers used within the unit.
Microscopy is an interesting area of the unit, utilising years of experience and expertise by the team to ensure a rapid accurate diagnosis for the patient. The most common parasites diagnosed via microscopy are Plasmodium falciparum, found
in blood samples, and Giardia intestinalis, found in faecal samples. Some of the methods and stains used for malaria diagnosis are techniques over one hundred years old and are still the gold standard test for malaria diagnosis today. Some parasitic investigations are rare and the team need to ensure continued knowledge and competency for these tests that may only be requested once every 10 years. Microscopy leads to interesting team discussions, as the biomedical scientists are making diagnostic decisions very rapidly in the instance of malaria diagnosis, with no two microscopy samples being the same.
We are a small team of seven staff: one manager, one senior biomedical scientist, two biomedical scientists, one medical laboratory assistant and two part-time administrative staff. The team has more than 40 years’ collective service working at the CDPL, due to the interesting aspects of the work and the family feel of the team.
The team are starting to see slow change in geographical distribution of parasites due to a number of factors, including changes to how people travel and climate change. The number of samples being processed in the CDPL continues to increase year on year. LSTM clinical teams and researchers globally link together to enhance diagnostic methods for parasitology and will continue to be at the forefront of knowledge in parasitic and infectious diseases and diagnostics. BMS
LAB
Unit Manager Jayne Jones gives a guided tour of her laboratory at the Liverpool School of Tropical Medicine.
MY
THE BIOMEDICAL SCIENTIST 54 MY LAB Jayne Jones


































The past, present and future of diagnostics

Roche Diagnostics is proud to be a Principal Sponsor of the IBMS Congress 2023.
We look forward to seeing you in person on our stand, or in our Roche Discovery Hub.

Let‘s talk about how we can partner with you to optimise your laboratory to deliver for patients today, and for generations to come.
diagnostics.roche.com

©2023 Roche Diagnostics Limited. All rights reserved.
