A closer look at some of the companies – and plastic surgeons –furthering innovation in the specialty through Society support.
Page 19
Face transplant restores life, hope for Michigan man
Page 7
Remembering ASPS past President Norman Hugo, MD
Page 9
PlastyPAC’s wins in 2024 elections
Page 12
COMMERCIAL DEVICE FOR FAT PROCESSING
in the US for aesthetic and reconstructive procedures1,*
Surgeon survey data, March 2024 (n = 143)
•Time efficient
2
INTEGRATED, CLOSED
SYSTEM Featuring an
In a retrospective study, REVOLVE™ System processed more fat per minute than centrifugation. •Easy to use2-4 •Predictable3
In an animal model, REVOLVE™ System yielded significantly higher fat graft retention than decantation and similar results to centrifugation.†,‡
†Correlation between these results and results in humans has not been established.
‡In this preclinical study, human fat was processed using 3 different methods: REVOLVE™ System, decantation, and centrifugation (processed at 1200 g for 3 minutes). Fat samples from each group were implanted into mice, then explanted after 28 days and evaluated for a head-to-head comparison of volume retention.
INDICATIONS AND IMPORTANT SAFETY INFORMATION
INDICATIONS
The REVOLVE™ Advanced Adipose System (REVOLVE™ System) is used for aspiration, harvesting, filtering, and transferring of autologous adipose tissue for aesthetic body contouring. This system should be used with a legally marketed vacuum or aspirator apparatus as a source of suction. If harvested fat is to be re-implanted, the harvested fat is only to be used without any additional manipulation. REVOLVE™ System is intended for use in the following surgical specialties when the aspiration of soft tissue is desired: plastic and reconstructive surgery, gastrointestinal and affiliated organ surgery, urological surgery, general surgery, orthopedic surgery, gynecological surgery, thoracic surgery, and laparoscopic surgery.
IMPORTANT SAFETY INFORMATION
CONTRAINDICATIONS
Contraindications to autologous fat transfer include the presence of any disease processes that adversely affect wound healing, and poor overall health status of the individual.
WARNINGS
REVOLVE™ System must be used within the same surgical procedure. Reuse of this device in the same patient in a subsequent surgical procedure, or for more than one patient, may result in infection and/or transmission of communicable diseases. Do not use the product if sterile packaging is damaged.
This device will not, in and of itself, produce significant weight reduction. This device should be used with extreme caution in patients with chronic medical conditions such as diabetes, heart, lung, or circulatory system disease or obesity. The volume of blood loss and endogenous body
fluid loss may adversely affect intra and/or postoperative hemodynamic stability and patient safety. The capability of providing adequate, timely replacement is essential for patient safety.
PRECAUTIONS
REVOLVE™ System is designed to remove localized deposits of excess fat through small incision and subsequently transfer the tissue back to the patient. Use of this device is limited to those physicians who, by means of formal professional training or sanctioned continuing medical education (including supervised operative experience), have attained proficiency in suction lipoplasty and tissue transfer. Results of this procedure will vary depending upon patient age, surgical site, and experience of the physician. Results of this procedure may or may not be permanent. The amount of fat removed should be limited to that necessary to achieve a desired cosmetic effect. Filling the device with adipose tissue over the maximum fill volume line can lead to occlusion of the mesh resulting in mesh tear.
ADVERSE EFFECTS
Some common adverse effects associated with autologous fat transfer are asymmetry, overand/or under-correction of the treatment site, tissue lumps, bleeding, and scarring. Potential adverse effects associated with REVOLVE™ System include fat necrosis, cyst formation, infection, chronic foreign body response, allergic reaction, and inflammation.
REVOLVE™ System is available by prescription only.
For more information, please see the Instructions for Use (IFU) and User Manual for REVOLVE™ System available at www.allergan.com/RevolveIFU or call 1.800.678.1605.
To report an adverse reaction, please call Allergan at 1.800.367.5737.
References: 1. Data on file, Allergan Aesthetics, March 2024; Aesthetic Monthly Tracker. 2. Gabriel A, Maxwell GP, Griffin L, Champaneria MC, Parekh M, Macarios D. A comparison of two fat grafting methods on operating room efficiency and costs. Aesthet Surg J. 2017;37(2):161-168. 3. Ansorge H, Garza JR, McCormack MC, et al. Autologous fat processing via the Revolve system: quality and quantity of fat retention evaluated in an animal model. Aesthet Surg J. 2014;34(3):438-447. 4. Data on file, Allergan Aesthetics, June 2022; Fat Grafting Final Report.
ways to ease the awkward money talk
Financial conversations don’t have to be difficult. Here are practical ways to smooth them out.
We know talking about cost is one of the toughest parts of cosmetic care— these conversations can feel uncomfortable or even intimidating. Check out these strategies for discussing flexible financing, which can help smooth communication and ease stress for all parties.
Tip 1
Before the Consultation
Let patients know flexible financing is available when they call to schedule their consultation.
Tip 3
Addressing Concerns About Cost & Financing
Remind patients that the CareCredit credit card can be used for copays, deductibles and out-of-pocket costs for surgery, as well as prescriptions, skincare products, and minimally invasive treatments.
“Our cost ranges from $XXXX to $XXXX and varies based on your specific needs. We do accept the CareCredit health, wellness and beauty credit card to help you pay over time. You can ask questions and get an estimate for your procedure during one of our complimentary consultations. Would you like to schedule that today?”
Tip 2
During the Consultation
In addition to total cost, give patients an estimate of what their monthly payment could be with the CareCredit credit card. You can use the online payment calculator or patient financing brochure to show estimated monthly payments and disclosures to the patient.
Practice:
“I’m glad you’re happy with the surgeon’s recommendation. You’re going to love the way you look and feel! The total cost for your procedure is $XXXX. With the CareCredit health, wellness and beauty credit card, your estimated monthly payment could be $XXX. Would you like to learn more about this option?”
The online payment calculator and patient financing brochure are available at carecreditprovidercenter.com
“We want to help you look and feel your best, which is why we accept CareCredit. It’s a health, wellness and beauty credit card that can help you fit the procedures you want or need into your budget.”
“With the CareCredit credit card, promotional financing is available on purchases of $200 or more. If you’re approved, you can use it again and again to pay over time for additional cosmetic procedures at our office. Would you like to learn more about CareCredit or see if you prequalify?”
Tip 4
Handling Patients Not Yet Ready to Schedule
If the patient says they need to think about the procedure, be empathetic and have a strong follow-up plan.
need time to think it over.” “I really want this procedure, but I just don’t have room in my budget right now.”
“We understand this is a big investment. Here’s a printout of the surgeon’s full recommendation. If cost is a concern, we have a link to the CareCredit credit card application on our site so you can apply from home. Would you mind if we followed up in a few days to address any additional questions?”
Make sure patients know CareCredit offers a way to help pay for the care they want or need. Display a window cling at your front door, stock brochures at the front desk, and place counter displays in waiting areas to highlight the CareCredit health, wellness and beauty credit card. Display your custom QR code in your office reception area and add your custom link to your website so patients can see if they prequalify and apply easily from their mobile device.
IN THIS ISSUE
man’s
A 50-hour face transplant procedure led by ASPS member Samir Mardini, MD, gives man his life back.
MultiPlan, Inc., faces a landmark antitrust lawsuit for allegedly orchestrating a nationwide price-fixing scheme.
Remembering ASPS past President Norman Hugo, MD, 1933-2024
Colleagues, mentees remember Dr. Hugo’s leadership and commitment to the specialty.
Vedder, MD, discusses his path to the specialty and national leadership roles.
The November meeting in Orlando, Fla., placed focus on Medicare payment reform and surgical standards.
ASPS members share insights on a variety of topics – and pressures – that face young plastic surgeons.
A
January/February 2025 Vol. 36 No. 1
The mission of the American Society of Plastic Surgeons is to support its members in their efforts to provide the highest quality patient care and maintain professional and ethical standards through education, research and advocacy of socioeconomic and other professional activities.
ASPS PRESIDENT
Scott Hollenbeck, MD dr.scott.hollenbeck@gmail.com
Erin Finnegan; Frances Hackler; Stella Hiltzik; Matt Lavin, JD; Kaibrea Schoning; Alex Walton
COVER DESIGN
Paul Snyder
DISPLAY ADVERTISING SALES
Michelle Smith, (646) 674-6537
michelle.smith@wolterskluwer.com, Wolters Kluwer Health
CLASSIFIED ADVERTISING
Jeanne Embrey, jembrey@plasticsurgery.org
Plastic Surgery News (ISSN 1043-4119) is published eight times per year: March, June, September, December single issues – and combined January/February, April/May, July/August and October/November issues – by ASPS. Phone: (847) 228-9900; Fax: (847) 228-9131
POSTMASTER, send address changes to: ASPS Membership Department Plastic Surgery News 444 E. Algonquin Road Arlington Heights, IL 60005
Periodicals postage paid at Arlington Heights, IL, and at additional mailing offices. USPS# 508-890. The views expressed in articles, editorials, letters and other publications published by PSN are those of the authors and do not necessarily reflect the opinions of ASPS. Acceptance of advertisements for PSN is at the sole discretion of ASPS. ASPS does not guarantee, warrant or endorse any product, program or service advertised.
2024 Subscription Rates:
Basic subscription rate: $90; for foreign subscriptions add $90 for first class service. The subscription price for PSN is included in annual membership dues. Letters, questions or comments should be addressed to: Editor, Plastic Surgery News, 444 E. Algonquin Road, Arlington Heights, IL 60005. plasticsurgery.org
The PSF is the engine that drives the future of plastic surgery
By Alan Matarasso, MD The PSF President
When The PSF – then known as The Plastic Surgery Educational Foundation – was seeded by a $5,000 U.S. Savings Bond in 1948 by founder Jacques Maliniac, MD, the directors deemed the purpose of the new organization was to “support research pertaining to congenital and acquired deformities; promote high standards of training, practice and research in plastic surgery; confer prizes and establish scholarships; and promote lectures, seminars, and medical and public meetings to educate the lay public in matters pertaining to the field.” Then and now, these aspirations improve the quality of life of our patients through education, research and development.
For a technical start, ASPS is a 501(c)6 and The PSF is a 501(c)3 organization, which distinguishes The PSF’s operations as exclusively for charitable, educational and scientific purposes. Your annual membership dues directly fund ASPS – not The PSF. The PSF is sustained through gifts, which you can make by checking a separate box on your dues statement. Donations support The PSF Annual Fund, a variety of specific programs and grants and the National Endowment for Plastic Surgery, which was started by ASPS past President Norman Cole, MD, in the 1990s. These generous gifts continue to seed the research and innovation that drive our initiatives – and the entire specialty of plastic surgery – forward.
Scholars and various international programs that enable plastic surgeons to engage in bidirectional exchange such as Surgeons in Humanitarian Alliance for Reconstruction, Research, and Education (SHARE) and Global Advancement for Academic Plastic Surgeons (GAAPS). It continues to provide valuable opportunities for young plastic surgeons to come to the United States to train with and learn from our leaders.
The three ‘C’s
More than three-quarters of a century later, The PSF still adheres to many of those original designs, while also having evolved into an engine for our entire specialty and providing more than $1 million per year through a variety of grant opportunities. It serves as a hub for the Plastic Surgery Registries Network (PSRN), an umbrella under which rests the PROFILE registry, the National Breast Implant Registry (NBIR), Tracking Operations and Outcomes for Plastic Surgeons (TOPS) and the General Registry of Autologous Fat Transfer (GRAFT). These registries collect critical patient, device and procedural data to improve safety and fortify clinical evidence on an array of procedures and products.
ASPS and The PSF work in concert – and perhaps because of the vast array of activities that fall under The PSF’s purview (or any number of other factors), I still hear members ask a common question: How is what The PSF does different from ASPS?
EDITOR’S MESSAGE
The mission of The Foundation is to advance plastic surgery through innovative research, to develop scientific leaders and improve the quality of life of our patients. Our expansive registry network allows us to trace, analyze and promote data regarding the plastic surgery procedures, patient safety and quality outcomes. We’re always building on The PSF’s platform to partner with plastic surgeons, patients, industry and others to increase access to safe, effective and affordable plastic surgery care that meets the needs of individuals and populations. The grants that we provide advance research and the career development of plastic surgery residents and our plastic surgeon-scientists, as well as support emerging innovators and leadership collaboration. Groundbreaking research has both taken root and advanced thanks to the funds generated through our grant programs – a continually vital option for plastic surgery researchers who might not be able to otherwise secure funding through NIH offerings.
The PSF selects and funds individuals for the Visiting Professors program, International
I personally believe that The PSF – and, frankly, plastic surgery itself – is anchored by the three “C”s: collegiality, collaboration and contribution. One needs look no further than the hallways of any state, regional or international meeting to see firsthand the collegiality that plastic surgeons share with each other and how that spirit fosters any number of networking connections and opportunities for plastic surgeons at various stages of their careers.
As many of my predecessors in the presidential line have noted, a spirit of collaboration is also necessary to keep the life blood pumping through our specialty. We all recognize that several procedures innovated by plastic surgeons have been co-opted (if not outright hijacked) by other specialties. Trying to exist on our own specific island, however, will only put us in a demonstrably weaker position. We should continue to collaborate with each other and other specialties to advance patient care and research.
The common denominator to everything The PSF does is contribution. Each of us can and should contribute in some way to organized plastic surgery. Whether you contribute your time volunteering, teaching, assisting a colleague, performing research or through providing financial gifts, the specialty continues to stand as a bedrock of innovation from this ongoing spirit of giving back. When you look forward or reflect on your career, I think we can
all agree that an essential, fulfilling component of your professional life has been enhanced and enriched by the contributions to the profession to which you’ve devoted your education and life.
The PSF seeds the future of plastic surgery and advances all of our innovation. This issue of PSN highlights some of the plastic surgeon innovators within our ranks who are making gains from the partnership ASPS forged with MedTech Innovator to pull great ideas off paper and into the O.R. (see story on page 19). Many of the most important and routinely incorporated operations we perform were born decades ago from research grants seeded by The PSF. Furthermore, over the past 50 years plastic surgery has incorporated hand surgery into our repertoire, initiated microsurgery techniques and used them all over the body for an entire arsenal of reconstructive procedures. We’ve pushed microsurgery from what landed Joe Murray, MD, his 1990 Nobel Prize in Physiology or Medicine for transplantation, to now microsurgically performing full face transplantation (see a news story on the latest example of this on page 7).
Plastic surgeons essentially created liposuction surgery, revolutionized breast reconstruction, spurred the evolution of aesthetic medicine, helped establish techniques for gender surgery and more. We can only continue to make these prodigious advances through your voluntary, generous contributions to and participation in The PSF. We owe it to our patients, ourselves and the future of plastic surgery to continue to fuel this machine that drives the specialty. PSN
Plastic surgeon and mother: The impact of wearing two hats
By B. Aviva Preminger, MD, MPH PSN Chief Medical Editor
My first conversation about wanting to be a plastic surgeon took place when I was 14 years old. I was so excited to finally meet a female plastic surgeon. The conversation, however, was disappointing. She told me – in no uncertain terms – that I “just shouldn’t do it.” My kids would resent me for it, and I would miss out on all of the important moments.
I never forgot her words.
At my own peril, I somehow disregarded her recommendation. Ten years later, I found myself in the burn unit paired with a plastic surgery resident from another program. She introduced herself, and her last name immediately rang a bell.
training and went on to raise children who are now teenagers. In the years since my training, of course, there have been notable changes made by the ABPS and academic institutions to better facilitate a balance between becoming a plastic surgeon and starting (or growing) a family. The Women Plastic Surgeons Forum also provides a vital network of colleagues who
can share their own experiences with women who might have concerns about the impact of issues ranging from changing practice types to chasing a new opportunity somewhere across the country – or even simply wanting to be a plastic surgeon – might have on their kids. These remain valid concerns and conversations that still need to be had.
Close to two decades later, I have decided to go to the source (my daughter, Stella) to get a better understanding of the impact of the decision I made, in the hopes of providing young plastic surgeons – or maybe not-soyoung plastic surgeons – with some insight into the impact of being a plastic surgeon and a mom. PSN
Growing up with a plastic surgeon mom: A teen’s perspective
“Is your mother a plastic surgeon?” I asked.
“Yes,” she replied.
“Your mother warned me not to do this,” I said.
“Yeah – she told me the same,” she laughed. Yet, there we were – two female plastic surgery residents who eventually completed their
Editor’s note: The views expressed in the “President’s Message” and “Editor’s Message” columns are those of the author and do not necessarily reflect the opinions of ASPS.
By Stella Hiltzik
When I tell people that my mom is a plastic surgeon, I usually get a wide-eyed reaction.
“Wow,” they’ll say. “That is so cool!”
They’re not wrong. Growing up with a mom who’s a plastic surgeon definitely shaped my view of the world, body image – and even how I think about beauty and confidence.
But it’s not exactly what most people imagine.
First, I think it’s important to explain that my mom’s job is not like an episode of some flashy reality show. People often think plastic surgery is all about glamour, quick fixes and vanity, but what I see every day is far from that stereotype. My mom’s work is meticulous, complex and deeply meaningful to her and her patients.
For example, she doesn’t just help people “look better” – she helps people feel better. Some of her work is reconstructive surgery for patients who’ve been through tough situations, such as accidents or illness. She always talks about how her goal is to enhance what’s already there and to help people feel more like themselves, rather than someone they’re not. This has made me understand that plastic surgery, when done with care and purpose, can be about healing and empowerment – not just appearance.
I’ve seen how she spends hours in surgery – completely focused – knowing that her work will help someone reclaim their confidence or sense of normalcy. Even when it’s exhausting, she genuinely cares about each person who walks into her office.
When she comes home though, no matter how tired she is, she changes hats and is in full “mom” mode, asking about our day, prepping dinner and helping with homework.
One of the things that shaped me most is
how my mom talks about beauty. Growing up, she taught me that confidence doesn’t come from fitting into a certain mold or achieving a specific look. She always emphasized that beauty is individual and that true confidence comes from feeling comfortable in your own skin. Ironically, being a plastic surgeon gave her a unique perspective on natural beauty and self-acceptance. I don’t feel pressured to look perfect, but I do feel a sense of responsibility to take care of myself. My mom taught me that taking care of your body is a form of respect for yourself. So, while having a plastic surgeon mom might sound glamorous, it’s actually taught me a lot about empathy, resilience and self-acceptance. What matters is finding a path that helps you feel true to yourself.
Having a mom as a plastic surgeon has also shown me that I can accomplish anything I put my mind to. For that, I’m grateful to have such an incredible role model in my life. PSN
‘Extensive’ Mayo Clinic face transplant gives man his life back
By Jim Leonardo
The technique and scale of facial transplantation have advanced so rapidly and greatly since the first successful partial face transplant – performed on a French woman in 2005 – that one of the most extensive full-face transplants, completed in February 2024 at Mayo Clinic, Rochester, Minn., could almost be considered routine. Almost.
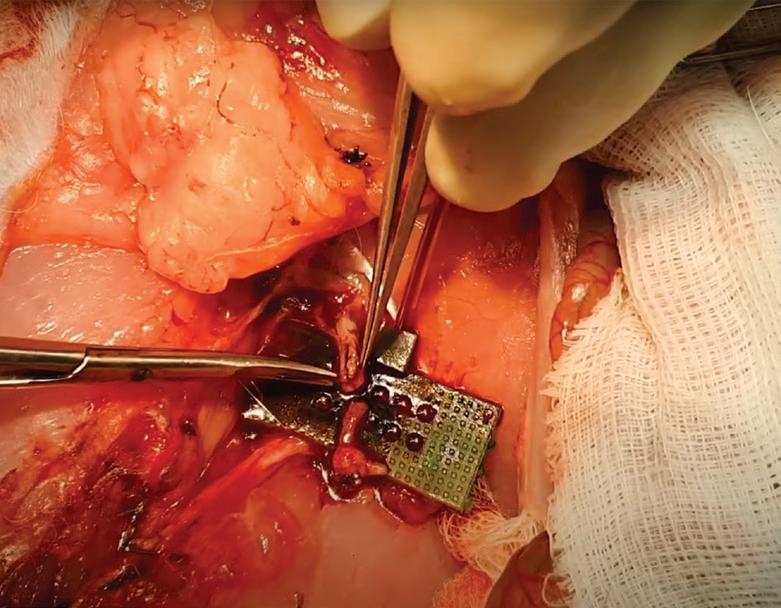
Approximately 85 percent of Derek Pfaff’s face was replaced by donor tissue – everything below his eyebrows and part of his forehead –including his upper and lower eyelids and intraorbital fat on one side; upper and lower jaws; teeth; nose; cheek structure; hard palate; parts of his soft palate and the entire skin of the face and neck. Thanks to hundreds of hours toiling in a cadaver lab and countless additional hours of virtual planning and 3D modeling by ASPS member Samir Mardini, MD, Derek’s 50-hour procedure concluded without a hitch.
“It was long and it was a lot of delicate work, but it went very smoothly,” says Dr. Mardini, who is the surgical director of the Mayo Clinic Reconstructive Transplant Program.
Dr. Mardini, professor and chair of the Division of Plastic Surgery, says face transplants are always the last and most drastic option for patients, and Derek, who hails from Harbor Beach, Mich., had undergone 58 reconstructive procedures since a shotgun blast destroyed much of his face in 2014.
“From an anatomic standpoint, Derek had exhausted all reconstructive options, and continuing to pursue reconstruction only would be deleterious to other, healthy parts of Derek’s body,” Dr. Mardini tells PSN. “Doing that would damage other parts of the body that are important to Derek – and make it much more challenging to perform a face transplant.
“He had several morbidities from donor sites for his ongoing reconstruction around his body that were affecting his function, including a bad contracture of his forearm from a radial form flap,” Dr. Mardini adds. “Doing more of
the related function. It was an effort that was greatly aided by technology – and concerted effort.
“To a great extent, what led to the success of Derek’s procedure was all the prep work and virtual surgical planning,” Dr. Mardini says. “One part of the virtual surgical planning was ‘guide creation.’ You print the model of the donor and the recipient and have them to look at. We had a CAT scan of the donor and the recipient, which allowed us to work with biomedical engineers to do a simulation of the surgery.”
Dr. Mardini estimates that between the two procedures at Mayo, he and his teams spent more than 300 hours with virtual planning and in the cadaver lab.
For Derek, now age 30, the surgery achieved even more than he had hoped.
“It exceeded my expectations,” he tells PSN “I have a face. I have a nose. I have lips. I can wear my glasses, which I couldn’t do for the last 10 years. Dr. Mardini and the entire team did a great job. As far as undergoing the surgery itself, it was pretty easy. The toughest part was knowing that my parents had to wait while I was having the surgery.”
A clinical program
Dr. Mardini, who trained and spent more than five years in Taiwan under renowned reconstructive microsurgeons Fu Chen Wei, MD, and Hung-Chi Chen, MD, PhD, as well as craniofacial surgeon Yu-Ray Chen, MD, at Chang Gung Memorial Hospital, says that unlike other transplantation efforts nationwide, the Mayo Clinic program was not built as a research program.
the same wasn’t going to give him the functional and aesthetic outcomes that he was looking for. So it was obvious very quickly that he was a good face transplant candidate.”
Once that had been determined, the wait for an appropriate donor began. The answer came nearly two years after Derek entered the face transplant program, with events moving rapidly from there.
ASPS members meet in Shanghai
Several ASPS members attended the Ninth World Congress for Plastic Surgeons of Chinese Descent in Shanghai, China, which was held Dec. 13-15. The event took place in at Tongji University in Shanghai and was combined with the 2024 Oriental Aesthetic and Plastic Art Conference. From left to right, Ernest Chiu, MD; Lee L.Q. Pu, MD; June Wu, MD; David T.W. Chiu, MD; ASPS past President Gregory R.D. Evans, MD; Angela Cheng, MD; and Haiyan Cui, MD, who is chairman of the Ninth World Congress. PSN
“We learned of a potential donor for Derek on a Thursday,” Dr. Mardini says. “Following careful evaluation, we accepted the offer for the donor and our organ-procurement organization began discussions with the donor family. We then began our process of virtual surgical planning and team preparation.”
Once all agreed to move forward, the organ procurement organization took over allocating the other organs – which meant the earliest the donor tissue would be available was the middle of the night Saturday. In light of that, he and the team instead decided to start the following Sunday morning. Dr. Mardini assembled the team for an early briefing and then made the initial incision around noon. Nearly 60 hours and no serious complications later, Derek left the O.R. with a new face – and hope for the future.
Preparation and effort
Dr. Mardini’s team counted more than 80 medical professionals, including surgeons, anesthesiologists, nurses, various medical technicians, assistants and others that preceded that Sunday trip to the O.R. This also wasn’t the Mayo Clinic’s first face transplant procedure; in 2016, Dr. Mardini led a team at Mayo that performed the procedure for another gunshot victim, with that experience paying dividends for Derek.
“Between the two face transplants, we spent more than 85 evenings and weekends in the cadaver lab, trying to make sure we understood every step of the operation,” Dr. Mardini says. “We were determined to avoid unexpected outcomes and intraoperative surprises – and there were few, if any, surprises after we took Derek into the O.R.”
Planning for Derek’s February procedure entailed detailed facial nerve mapping of the donor and recipient, in order to match nerves between the two and allow the donor to gain
“We started our program as a clinical program, making Mayo the first in the country to offer facial transplantation as a clinical program,” Dr. Mardini says. “We did this because we felt, including our research IRB team, that the surgery itself had been done several times before; therefore, it didn’t need to be a program under the research umbrella. We also realized there would be some research protocols coming through, such as dealing with psychosocial matters and long-term outcomes – so research would still be served.”
Dr. Mardini says Derek’s story is the latest success in the program that he helped launch as the first of its kind in the nation.
“There was a lot of excitement over the years as we tried to get the Mayo program approved,” Dr. Mardini recalls. “Once the institution said, ‘Go ahead,’ I felt a massive weight on my shoulders. I had to think about how to execute this and make sure that the patient survives the face transplant while also ensuring that the patient achieves their goals. It’s quite a daunting feeling. That’s why we started going to the cadaver lab, and we went there probably more than we needed to. You’re in good shape if you over-prepare, but you could be harmed if you’re underprepared. And you never know when you’re fully prepared for something you’ve never done.”
After having been through so much over the past decade, Derek’s recovery is remarkable.
“He’s doing amazingly well,” Dr. Mardini says. “He’s back to life, he’s connecting with old friends and he’s doing well from the surgery. He’s got some facial function. He’s strong. One thing that was very, very meaningful to me occurred about a month ago when he sent a family photo to my phone. In the photo is Derek – just one of the guys standing there. And the text message that followed it read: ‘The first family photo in 15 years. We’re so grateful to you and the Mayo team for giving us this gift.’ That was more touching than I’ll ever be able to describe.” PSN
(Top) ASPS member Samir Mardini, MD, leads a surgical team work through a 50-hour face transplant procedure for Derek Pfaff; (bottom left) Pfaff with his mother prior to the transplant operation; and (bottom right) Pfaff poses with his new face after the successful procedure. Photos courtesy of Mayo Clinic.
Understanding the MultiPlan lawsuit for plastic surgeons
By Matt Lavin, JD
MultiPlan, Inc., faces a landmark antitrust lawsuit for allegedly orchestrating a nationwide price-fixing scheme, with major insurers – including Aetna, Cigna, UnitedHealthcare and Blue Cross Blue Shield affiliates – named as co-conspirators. The litigation challenges MultiPlan’s systematic reduction of out-of-network healthcare payments, a practice that could fundamentally reshape reimbursement standards. For ASPS members who rely heavily on out-of-network billing, this case represents a critical opportunity to address systematic underpayment issues that threaten the sustainability of plastic surgery practices.
In short, the suit alleges that MultiPlan systematically decreased reimbursements to providers for important healthcare services, while the company – along with its insurer co-conspirators – kept the difference as profit.
Understanding the case
Moving forward as multi-district litigation in federal court in the Northern District of Illinois, the lawsuit accuses MultiPlan and insurance companies of coordinating since 2015 to systematically suppress payments for out-of-network services. The lawsuit alleges that MultiPlan and major insurers violated the Sherman Antitrust Act by operating as a “huband-spoke” business model. In this case, MultiPlan allegedly acted as a central hub to facilitate coordination among multiple competing companies (the “spokes”) without the competitors ever speaking to each other.
More specifically, the scheme’s mechanics allegedly center on MultiPlan’s repricing practices
that allow insurers to standardize artificially low payments while eliminating competition among themselves. MultiPlan’s fee structure incentivizes this underpayment, with the company receiving compensation based on the difference between initial claim amounts and final payments, according to the lawsuit. In other words, the company’s profits increase as provider reimbursements decrease, the suit reads.
It’s alleged that MultiPlan’s explosive growth – from $23 million in revenue in 2012 to $709 million in 2021 – has come at the expense of healthcare providers, who frequently receive payments below their operating costs.
A pattern of behavior
This current situation echoes previous industry
practices. In the late 1990s, UnitedHealthcare created a subsidiary called Ingenix and acquired independent databases to control “usual, customary, and reasonable” (UCR) rates. Major insurers – including Aetna and Cigna –contributed claims data to Ingenix and used it to determine out-of-network payments.
Investigations by the New York Attorney General and the U.S. Senate revealed that these databases were manipulated to artificially depress reimbursement rates by 10 to 28 percent. This led to substantial settlements, with United paying $350 million and insurers agreeing to shut down the Ingenix database and fund the creation of FAIR Health, an independent database designed to ensure accurate UCR rates.
However, after insurers’ obligations to use FAIR Health ended in 2015, MultiPlan
stepped in to fill the void. MultiPlan’s pricing tools are now alleged to serve the same function that Ingenix once did, suppressing out-ofnetwork rates and harming providers.
Evidence of impact
Evidence of systematic underpayment emerged in an April 2020 study by the Office of the New York State Comptroller (“An Analysis of Reasonable and Customary Out-of-Network Reimbursement Rates for Medical/Surgical Services in the New York State Health Insurance Program”), which found that payments using MultiPlan’s repricing methodology were anywhere from 1.5 to 49 times lower than traditional out-of-network calculations. The lawsuit argues these actions violate the Sherman Act by eliminating competition among insurers and depriving the healthcare market of fair pricing practices.
The impact on healthcare providers has been severe – particularly affecting smaller medical practices. Many have been forced to reduce services, cut staff or close entirely. This consolidation has restricted patient access to specialized care and created a healthcare landscape with fewer options for both patients and providers.
Why plastic surgeons should care
ASPS members face unique challenges in the current reimbursement landscape. The specialty’s high volume of out-of-network claims – combined with the complexity of procedures such as reconstructive surgeries after trauma or cancer – makes practices particularly vulnera-
Continued on page 26
IN MEMORIAM
A professor and leader: Remembering Norman Hugo, MD
By Paul Snyder
Plastic surgeons are paying tribute to ASPS
past President Norman Hugo, MD, who passed away on Dec. 9 at age 91.
“He was always ‘The Professor’ to us,” recalls ASPS past President Richard D’Amico, MD, who trained under Dr. Hugo at Columbia-Presbyterian Hospital in New York. “He was a leader. He took on tough tasks and never backed down from his principles. He made us better people and better surgeons. He taught us about leadership – not just in the O.R., but in society and in our Society.”
His passion for medicine was the specialty’s gain, as Dr. Hugo’s stature and athletic prowess could have set him on a different path. Richard Peinert, MD, past president of the Massachusetts Society of Plastic Surgeons and a friend of Dr. Hugo’s for more than 40 years, says Dr. Hugo turned down a scholarship to the University of Kentucky to play basketball for Adolph Rupp so that he could attend Williams College. Basketball wasn’t his only athletic forte, either.
“He was a larger-than-life character – both physically and in how he acted,” Dr. Peinert says, noting that Dr. Hugo was also an all-scholastic baseball player in Massachusetts and would tell the story of how he once hit a towering fly ball off of Bill Monbouquette, who would find fame in the major league as a member of the Boston Red Sox, Detroit Tigers, New York Yankees and San Francisco Giants.
“This was in a field that didn’t have a fence,” Dr. Peinert says. “So Norman would talk about how he just stood there admiring his hit. He forgot to run, so he only ended up with a double. He was mad that he couldn’t say he homered off Bill Monbouquette.”
Dr. Hugo completed his general and plastic surgery training at Cornell Medical School, training at New York Hospital with The PSF past President Herbert Conway, MD, who Dr. Hugo counted as his most important mentor. He held true to Dr. Conway’s mantra that “If you do not write, it did not happen” – and Dr. Hugo was a frequent contributor to several medical journals throughout the course of his career.
Following his residency, Dr. Hugo served as professor at Indiana University in 1966-67, when he was drafted into the U.S. Army (he ultimately served as a major). He suspended his private practice and was stationed at Walter Reed Hospital from 1967-69 as assistant chief of plastic surgery. The experience during the Vietnam War had a lasting effect on him, and he would speak at various events to honor American veterans and pay tribute to those who suffered lasting effects from the wounds sustained in battle.
Following Dr. Hugo’s discharge from the Army, he relocated to Chicago, where he served as associate chief of plastic surgery at Michael Reese Hospital in 1969-71, and then as associate chief of plastic surgery at Northwestern Hospital in 1971-82. In 1982, Dr. Hugo was named chief of plastic surgery at Columbia Presbyterian Hospital in New York – a role he maintained until his retirement on Dec. 31, 1997.
“He might be tough on us in a closed room – but in a positive way, because he always wanted the optimal outcome and wanted us to become the best surgeons we could be,” notes ASPS Trustee Jeffrey Ascherman, MD, who trained under Dr. Hugo and is now site chief of the Division of Plastic Surgery and professor at Columbia University Irving Medical Center. “Outside of that room, he would protect and
Tribute to a pioneer and a friend
By Richard Hamilton, MD
One of the great pioneers of microsurgery in Scandinavia died Oct. 19 in Gothenburg, Sweden, after a short battle with pancreatic cancer. He was 83.
Ingemar Fogdestam, MD, was born in Blekinge, Sweden, on Sept. 29, 1941, and maintained his connection with the region for his entire life. His father was an engineer in the Swedish Air Force, and Ingemar attended school in Ronneby and proceeded to gymnasium in nearby Karlskrona.
Ingemar gained admission to medical school in Gothenburg in 1961. His early surgical experience was in Eskilstuna, Sweden, and he soon discovered an affinity for plastic surgery. He gained a residency position at the Sahlgrenska Hospital in Gothenburg in 1970, where he worked under clinic chief Prof. Bengt Johanson, a larger-thanlife character in the Swedish plastic surgery scene and a contemporary of Tord Skoog, MD. Bengt encouraged Ingemar to undertake a research project on wound healing and sent him to Aarhus, Denmark, from 1974-76, where he studied delayed primary closure under the supervision of Prof. Andrus Viildik, ultimately obtaining his doctorate degree in 1980.
Bengt Johanson recognized the importance that microsurgery would play in the future of plastic surgery, which prompted him to recommend Ingemar join the fellowship program of Bernard O’ Brien, MD, and Wayne Morrison, MD, in the microsurgical unit at St. Vincent’s Hospital, Melbourne, Australia. During the year he spent there, we first crossed paths, when I was chief resident in plastic surgery. Together in Melbourne, we carried out anatomical studies on the blood supply of the lower abdominal wall.
At the end of this time, Ingemar invited me to work with him at Sahlgrenska, where we built Scandinavia’s first microsurgical unit. During this period, in 1978-79 we carried out the first clin-
support you any way he could in the hospital. He considered us family. I have fond memories of him taking us to Army/Navy football games and to the best steakhouses around, so that we could rate the top ones in New York. Being the department chief wasn’t just a job to him – he invested all his time in that role to help us become the best possible doctors.”
Dr. D’Amico remembers starting rounds at Columbia Presbyterian Hospital with his fellow resident John LaManna, MD, at 6 a.m.
“One evening, Dr. LaManna and I were leaving at 6 p.m.,” Dr. D’Amico recalls. “The elevator door opened and he was standing there. He looks at us and goes, ‘Half a day, boys?’ You definitely had to toe the line with him.
ical cases for free abdominoplasty flap (now known as the DIEP flap) for breast reconstruction. The operation is now mainstream and has improved the lives of tens of thousands of women suffering from breast cancer around the world.
Other groundbreaking microsurgical procedures done by Dr. Fogdestam at Sahlgrenska included lower-limb reconstructions with the osteocutaneous groin flap; free-fibular transfer for congenital pseudarthrosis of the tibia; vaso-epididymal anastomosis for male infertility; and unique cases such as scalp replantation in a young girl and hand replantation in a young boy. He published numerous articles on these and other microsurgical works.
Ingemar was admired for his clear thinking, his absolute care and dedication to his patients and his willingness to undertake challenging cases. Dr. Morrison wrote to me recently and shared his fondness for Ingemar, saying he “thought he was one of the most genuine and honest fellows that we had at St. Vincent’s.”
In the final years of his professional life, Ingemar applied his skills to aesthetic surgery at Art Clinic in Gothenburg. Outside of surgery, he was an officer in the Swedish Air Force Reserves, and he had an encyclopedic knowledge of military history and an extraordinary memory. We remember him as a faithful, fine friend and he will be greatly missed by his family, friends and colleagues in Sweden, Denmark, Australia and the United States.
Despite all his professional commitments, Ingemar found time for and was dedicated to his family. He’s survived by his three daughters, Ilona, Ellen and Hanna, and six grandchildren. PSN
“But when I was his chief resident, we’d also have long talks at the end of the day,” Dr. D’Amico adds. “To the point where his fabulous wife, Gerry, called me and implored me to let him go earlier because it was such a long drive back from New York to his home in New Canaan, Conn. But those are the times I cherish, because that’s when the real learning took place.”
During his time as ASPS president in 1988, Dr. Hugo encouraged the Society to become more involved in political and economic activities. He also began the work of providing standards of clinical care for the specialty – a years-long effort that ultimately included input from several ASPS members. The result of their combined work, the Society’s first “Clinical Practice Guidelines,” was published in 1994. Dr. Hugo also served as ABPS vice chairman.
“I was honored to follow him by exactly 20 years as ASPS president,” Dr. D’Amico notes. “He sent me on my first committee assignment in 1988. He lived leadership, understood leadership and taught leadership. He was always there for you, and whenever I had my own questions or struggles with leadership, I always had his example to look to.”
After retirement, Dr. Hugo continued to maintain an active schedule – both as a nationally ranked squash player and in auto shows around the country where his Morgan (a handmade British automobile crafted from wood and steel) took home no fewer than 15 first-place awards. He enjoyed traveling around the world with his wife, Geraldine, family and other friends.
“My advice to young surgeons is to stay true to your ideals and work hard,” he told PSN in 2007. PSN
When venous return is a problem, the Hirudo Medicinalis can help provide the solution. Call Leeches U.S.A. and get an immediate, Door to Door, delivery of leeches. Efficacy, too
• Provide the strongest anticoagulant known to man.
• Provide temporary outflow of blood until the body restores venous ingrowth to the affected tissue.
ASPS past President Norman Hugo, MD
Ingemar Fogdestam, MD
The PSF Distinguished Service Award Becoming the ‘consummate role model’ for plastic surgery
By Paul Snyder
Plastic surgery was not even a blip on the radar of The PSF past President Nicholas Vedder, MD, when he graduated from medical school at Case Western Reserve University and began his surgical residency at the University of Washington (UW). Fortunately for the specialty, Dr. Vedder was left uninspired by his original path of cardiac surgery.
“As a resident, I realized cardiac surgery was pretty boring,” he says. “They did the same operation again and again. I got interested in vascular surgery for a while, but it wasn’t until I was a fourth-year resident in surgery when a new plastic surgery faculty member came in and performed microvascular surgery. It just blew my mind.”
At the time, Dr. Vedder had no idea how far his new fascination would take him. Born in Chicago and raised in Evanston, Ill., Dr. Vedder completed his undergraduate work at Stanford University – where he met his wife, Susan Heckbert, MD, on the first day, and they would ultimately go to Case together. It might be strange to consider now, considering the long and distinguished careers Dr. Vedder and Dr. Heckbert cemented in the Seattle area, but when they couple-matched to the University of Washington for residency, Dr. Vedder laughs that he thought it was the end of the world.
“It was my third choice, after University of California-San Francisco and Massachusetts General Hospital for surgery residency,” he notes. “But coming to UW turned out to be the beginning of my world. After my surgery residency, I did a two-year, NIH-sponsored trauma research fellowship here, too.”
Nevertheless, armed with an immediate interest in microsurgery and hand surgery – and citing The PSF past President (and then-UCSF Plastic Surgery Chair) Stephen Mathes, MD, as a personal hero, Dr. Vedder hoped to undergo his plastic surgery training at UCSF, landing an interview there one week and another at Mass General the following week.
“I called Dr. Mathes to tell him how much I loved UCSF and would really love to be there,” Dr. Vedder recalls. “He said, ‘Yeah, we really liked you, too. We’re going to meet next week, and we’ll let you know.’ So I got on the plane to Boston.”
At the time, the MGH plastic surgery department was run by James May Jr., MD, and Dr. Vedder was given a tour of the department from Rod Rohrich, MD, who was the hand surgery Fellow at the time.
“I remember it like yesterday,” says Dr. Rohrich, who would go on to become ASPS president in 2004. “Nick was young, brilliant and enthusiastic. He wanted to change the world and make a difference in plastic surgery and hand surgery. I told him the best place to do that was at MGH under the tutelage of Dr. May.”
In addition to recruiting Dr. Vedder during the tour, Dr. Rohrich showed him how to K-wire a zygoma fracture (“Not something you typically do,” Dr. Vedder laughs). At the end of the day, Dr. May offered Dr. Vedder the job on the spot, which he immediately took.
At MGH, a veritable who’s-who of future specialty leaders – including Jeff Fearon, MD; Dan Del Vecchio, MD; and W.P. Andrew Lee, MD – were among his peers.
“Even back in surgery residency at UW, two of my senior residents were James Grotting, MD, and James Stuzin, MD, and all three of us went on to become chair of the ABPS,” Dr. Vedder notes.
Setting an example
Upon completion of his training, he returned to the Pacific Northwest to become UW’s first hand surgery Fellow. A decade later, he would
become the university’s chief of the Division of Plastic Surgery and begin the work of building a program that’s now one of the specialty’s national leaders in training. He’s also a professor, and the Jamie Hunter Endowed Chair.
“We now have more than 130 graduates from our combined orthopedic plastic surgery hand program,” Dr. Vedder tells PSN. “When I joined the plastic surgery faculty in 1990, there was only one other faculty member – Loren Engrav, MD. We hired two more, Richard Rand, MD, and Joe Gruss, MBBCh, from Toronto. Joe, in six years, took our craniofacial program from nothing to the top-volume program in the country. Tom Trumble, MD, and I took the hand program to one of the largest programs in the country. We now have 19 full-time plastic surgery faculty, 30 integrated residents and tremendous fellowships in hand surgery, combined with orthopedics, microsurgery and craniofacial surgery. I’m very proud to have been part of that growth.”
And then there’s the work that Dr. Vedder has performed in the O.R. over the course of his career. The excitement that made him seekout plastic surgery training all those years ago has never waned, and he’s helped shape (and reshape) the lives of countless patients.
“As reconstructive plastic surgeons, we are given a gift,” Dr. Vedder says. “That gift is the ability to use what we do to rebuild patients’ lives. Every day I get up is a day that I may have an opportunity to make a difference that will last a patient’s entire life. There’s nothing more rewarding on Earth.”
Now in the late stages of his career – Dr. Vedder will retire from practice in July – he acknowledges that the days of “career-defining” cases are behind him. However, he still has many to reflect upon. From performing microvascular replantation for a young woman who suffered a total-scalp avulsion in a fish processing plant and later tissue expanding the replanted scalp, to surgically replanting all five amputated digits on the dominant hand of an engineer at a Boeing plant, Dr. Vedder says that cases he’s handled have never ceased to cement his love for the specialty.
“There was a 7-year-old girl who had her feet nearly pulled off in a boating accident on Lake Washington, and we were able to replant those and reconstruct the defect,” he recalls. “Just to be able to watch her have her life rebuilt
gine for innovation in our specialty. To watch The PSF grow from what was a pretty small organization back when I first got involved to now giving out more than $1 million a year in research grants and truly being that engine for the specialty has been really rewarding. My wife and I are part of the Maliniac Circle, and we’ll always continue help The PSF grow – and watch proudly as it does.”
Dr. Vedder also helped play a critical role in advancing the ASPS/PSF governance restructure spearheaded by ASPS past President Joe Losee, MD, during his 2021 term.
“The idea of this bottom-up structure that raises the voices of so many members was just a wonderful idea by Dr. Losee, and I’m very fortunate that I got to be involved in the early planning stages of that,” he notes. “I think the restructure is already showing positive change and I believe the representation is going to benefit this organization in ways we can’t even see yet.” Dr. Vedder’s commitment to not only furthering plastic surgery, but ensuring that more voices within the specialty are heard, earned him the distinction of receiving The PSF Distinguished Service Award, which was given to him by his 2013 counterpart, ASPS past President (and The PSF immediate-past President) Scot Glasberg, MD.
has been wonderful – she’s now a grad student at Cornell. There was another woman who had a severe crush injury to her hand, and I did a very low profile, free fascia flap and skin-grafted that. She got back to doing what she loves to do, which is playing piano. She sent me a video of her playing the piano, and although I haven’t seen her in 15 years, she just emailed me out of the blue, saying she’d like to come across the mountains and say hi to me and thank me for giving her life and avocation back.
“These are the kinds of things we get to do as plastic surgeons that no one else gets to do,” he adds. “It’s a special treat.”
Organizational leader
Concurrent with building UW’s plastic surgery program, Dr. Vedder also found himself helping to shape the specialty’s profile on a national level through his involvement with various organizations. However, he’s the first to note that he didn’t necessarily seek those roles.
“I kind of got dragged into many national leadership positions,” Dr. Vedder laughs. “But I’m very proud of the work – especially having been chair of the PSRC and the ABPS, because those are the two positions when you’re really selected by your peers.”
Nevertheless, Dr. Vedder’s leadership has fortified several organizations – he also served as president of the American Association for Hand Surgery and as a governor of the American College of Surgeons. His research techniques have been recognized by the NIH through the James A. Shannon Director’s Award, an R29 grant, and he’s the recipient of six Golden Scalpel Awards for best reconstructive case from the Washington Society of Plastic Surgeons.
Dr. Vedder’s involvement with ASPS and The PSF started shortly after he completed his residency, and while he recalls chairing various committees and moderating panels at annual meetings, he says he’s still surprised to see the amount of involvement he provided when he looks through his CV. All that work culminated in becoming The PSF president in 2013, which Dr. Vedder calls a highlight of his career.
“Plastic surgery doesn’t own any part of the human body,” he says. “The one thing that we own is innovation – and The PSF is the en-
“I was surprised that someone so dedicated to The PSF over all these years had not yet been given an award like that,” Dr. Glasberg says. “I’d always wanted to acknowledge him for his hard work and especially his partnership while we were presidents together – it was an honor for me to be able to bestow that award upon Nick.” Dr. Rohrich says the enthusiasm he recognized in Dr. Vedder during his first tour of MGH manifested itself in myriad ways for plastic surgery.
“He has made such a difference for this specialty,” Dr. Rohrich says. “We became lifelong friends, served together on the ABPS – and especially on the RRC, where we changed the entire program structure and training for plastic surgery that remains in place to this day. Nick played a pivotal role in transforming plastic surgical training and education during his amazing academic career at UW. His focus, hard work and dedication to our specialty is unmatched in his leadership of The PSF and beyond. Nick is the consummate role model for all of us with his unique spirit and sense of humor.”
New horizons
With his career as a practicing plastic surgeon set to close this summer, Dr. Vedder says there are a few changes he’s already excited about.
“I’m looking forward to not getting up at 4:30 in the morning for conferences and meetings – and I’m looking forward to very few Zoom calls lasting late into the night,” he says. “I’m also excited to do a lot more sailing, which is my passion, and traveling with my wife.”
Dr. Vedder is part of a group known as Sailing Plastic Surgeons, founded by Dr. Grotting, that consists of members from around the world – and who travel the high seas together.
“We travel around the world, either sailing on each other’s boats or chartering other boats. Two years ago, we chartered a boat in French Polynesia and sailed from Tahiti to Bora Bora and other islands. Last October, we did a trip in Croatia with half a dozen couples, sailing from Split to Dubrovnik, stopping at islands along the way. So I’m always looking forward to the next Sailing Plastic Surgeons trip.”
Still, even with his eyes on corners of the world yet to explore, he’s proud to note that home is his third choice from all those years ago.
“As I said, what I thought was the end of the world was really the beginning,” he says. “At this point in my life, I couldn’t live anywhere other than Seattle.” PSN
The PSF past President Nicholas Vedder, MD
Highlights from the 2024 AMA House of Delegates Interim Meeting
By Kaibrea Schoning
The American Medical Association House of Delegates (HOD) 2024 Interim Meeting was held in November in Orlando, Fla., with 20 plastic surgeons in attendance to represent their specialty through ASPS and its Plastic Surgery Caucus, along with the Section Council on Plastic, Reconstructive and Maxillofacial Surgery. In doing so, they ensured that the voice and values of plastic surgery were a part of the House’s consideration as it examined hundreds of resolutions and reports on many critical aspects of healthcare.
The meeting marked the first instance of ASPS past President Lynn Jeffers, MD, MBA, Oxnard, Calif., serving on the AMA’s Board of Trustees following her June election to the position during the Annual Meeting of the House of Delegates.
Dr. Jeffers’ service as a trustee left a gap in the Section Council on Plastic, Reconstructive and Maxillofacial Surgery, where she had previously served as the chair. To fill this gap, Michele Manahan, MD, Baltimore, was elected as the new chair of the Section Council, which consists of AMA delegates from ASPS and The Aesthetic Society, American Academy of Cosmetic Surgery, American Academy of Facial Plastic & Reconstructive Surgery, American Association for Hand Surgery, American Hernia Society, American Society of Maxillofacial Surgeons, American Society of Ophthalmic Plastic and Reconstructive Surgery, American Society for Reconstructive Microsurgery and International Society for Hair Restoration.
With this enhanced presence, ASPS played a key role in discussions on policies that resonate deeply within plastic surgery – and the most impactful policymaking came in the areas of pressing issues such as the highly anticipated Medicare payment reform, setting clear standards for surgical care and scope of practice.
Medicare payment reform
Medicare payment reform was a central topic at the meeting. Delegates emphasized the specter of continuing cuts to physician reimbursement, which has not kept pace with inflation by a wide margin over the past two decades – and has actually decreased in recent years. The discourse focused on how these rates are unsustainable and particularly detrimental to small practices, which affects access to care in rural or underserved areas.
For plastic surgeons, the Medicare Merit-Based Incentive Payment System (MIPS) can be a double-edged sword. Although the system aims to improve the quality and cost-effectiveness of care, its administrative demands often detract from the time physicians can spend with patients. At the Interim Meeting, the HOD stressed the following shortcomings of the program:
• MIPS is an administratively costly program that has failed to improve the quality of care.
• Mere compliance with MIPS requires a considerable investment in time and financial capital.
• MIPS operates in favor of physicians affiliated with better-resourced health systems, thus negatively impacting those practicing independently and patients in underserved areas.
The HOD passed a resolution, introduced by the New York delegation, that called for major reform of MIPS and urged the AMA to advocate for the repeal of this system, and for the establishment of a new, physician-designed program with a focus on outcome-based measures and reduced administrative burdens.
This resolution is a step toward a more streamlined system, where quality measures are
developed by practicing physicians who understand the day-to-day realities of patient care. A reformed program would allow physicians to focus more on clinical excellence and innovation rather than on burdensome compliance tasks. The AMA’s support for this resolution aligns with ongoing efforts by ASPS to reduce administrative burdens, ensuring that time and resources are directed toward what truly matters – providing high-quality, patient-centered care.
Clear standards for surgical care
At the meeting, the years-long focus on scopeof-practice issues continued. ASPS supported a resolution introduced by the American Society of Ophthalmology that amended existing AMA policy on laser surgery standards. The
newly revised policy specifies that laser surgery should be performed only by those licensed to practice medicine and surgery, or by practitioners with proper training and licensure from the state to perform surgical services. Additionally, it emphasizes AMA’s support for legislation prohibiting optometrists from performing surgical procedures that fall under the AMA’s definition of surgery.
The resolution, which was adopted after amendment, marks a significant victory for patient safety. For plastic surgery professionals, it means that those performing delicate and complex procedures involving laser technology must meet stringent licensing and training requirements. It ensures a high level of expertise and aims to prevent unqualified individuals from performing surgeries that should be reserved for trained medical professionals.
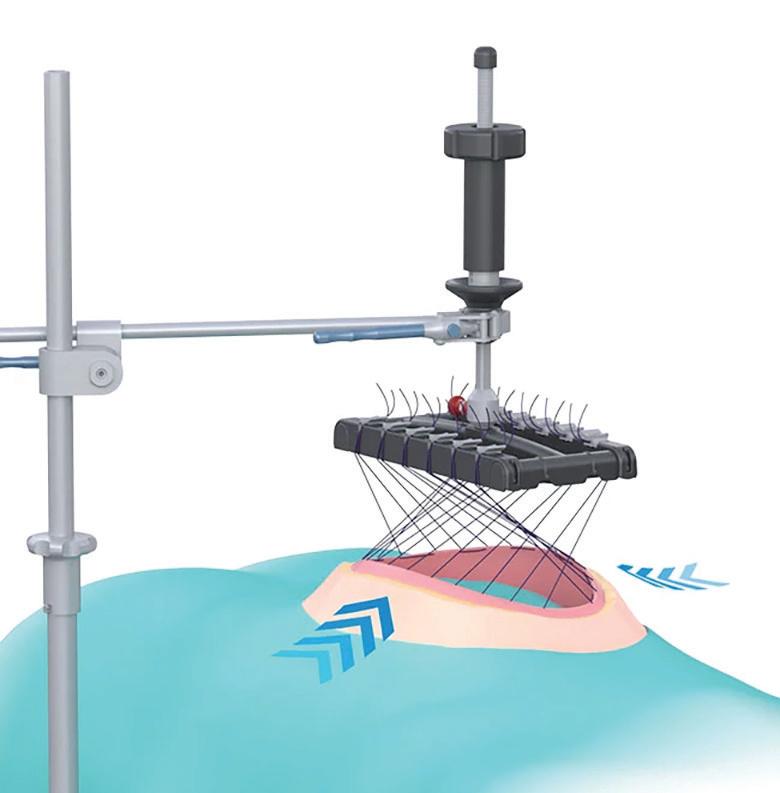
Breast Reduction Compression Device
Navigating crossroads
The AMA Medical Student Section introduced a resolution to address recent upheaval in the regulatory space following the Supreme Court’s reversal of the Chevron doctrine, a legal principle that historically required courts to defer to federal agencies when interpreting ambiguous laws. The court in June overturned this 40-year-old doctrine, leaving healthcare regulations in a state of uncertainty. The resolution proposed codifying Chevron deference, giving federal agencies the authority to interpret complex healthcare laws – including those impacting patient care and physician practice.
The debate surrounding this resolution is complex. On one hand, supporters argue that healthcare regulations, which require technical expertise, are best managed by agencies such
Continued on page 26
Celebrating PlastyPAC’s success in the 2024 elections
By Alex Walton
The weeks leading up to the 2024 general election were filled with uncertainty.
Polling for the White House, Senate and House of Representatives indicated that control of the federal government would come down to a small handful of states and districts. By election night, polling aggregates suggested both the presidency and the House were virtual toss-ups. Amid this uncertainty, the Society’s affiliated political action committee (PAC), PlastyPAC, remained focused on supporting candidates committed to advancing plastic surgery’s priorities.
The PlastyPAC Board of Governors, which comprises 12 ASPS member surgeons from private and academic practices across the country, invested significant time and resources into identifying and vetting candidates. Their focus: A proven record of leadership on key issues, including fair physician reimbursement, congenital anomaly coverage, prior authorization reform and access to breast reconstruction.
Over the past 22 months, PlastyPAC contributed $228,000 to 78 congressional candi-
dates seeking election or re-election. Of these candidates, 72 emerged victorious, resulting in an impressive 92 percent success rate.
How we succeed PlastyPAC’s success is no accident. The PAC
Advocacy in the states
A quick look at some of the work ASPS did in November and December to advocate on behalf of the specialty at the state level.
employs a nonpartisan, evidence-driven approach to candidate selection, guided by a sophisticated scorecard system. This system evaluates candidates based on their track records, committee assignments, leadership roles and alignment with ASPS priorities. By focusing on objective metrics, PlastyPAC ensures that every contribution will support candidates who champion issues critical to plastic surgeons and their patients.
The scorecard also emphasizes the importance of relationships between candidates and ASPS members. These personal connections, paired with insights from ASPS advocacy staff and contract lobbyists, are key to advancing the Society’s legislative agenda and amplifying its voice on Capitol Hill.
As part of the initiative to support microsurgical breast reconstruction, ASPS spoke with a member of the Arkansas Senate to discuss building support for his comprehensive bill to be introduced in 2025. Staff then met with the Arkansas Hospital Association to review recent modifications to the draft. ASPS also distributed state-specific legislation to 139 members of the North Dakota Legislative Assembly, requesting a champion to lead the same effort, while simultaneously communicating with representatives from the Arkansas Medical Society, the Medical Society of Delaware and the North Dakota Medical Association about the ongoing plans to improve breast reconstruction coverage in their states.
ASPS met with staff from the American Academy of Dermatology and the American Society for Dermatologic Surgery Association to discuss issues regarding medical spa operations around the nation and opportunities to utilize the Medical Spa Safety Coalition to advance patient safety through regulatory frameworks.
ASPS participated in a New Jersey Society of Plastic Surgeons Focus Group call to review the concerning medical spas landscape within the state and opportunities to enact legislation designed to tighten up their ownership and operation, thereby drastically improving patient safety.
Supplemental information was provided by ASPS to the Alaska Medical Spa Services Work Group in preparation for its December meeting. The work group has been tasked with providing direction to the state’s licensing boards in determining the scope of medical spa services.
The Society opposed legislation in Michigan that would increase the value of medical malpractice claims, raising the general noneconomic damages limit from $569,000 to $1 million and the exceptional noneconomic damages limit from $1,016,000 to $3 million, while also making earnings capacity damages available.
ASPS communicated with staff from the Connecticut Society of Plastic Surgeons regarding scope-of-practice determinations being conducted for dentists by the state’s Department of Public Health (DPH). The DPH also received requests to review the scope of practice for other health professionals, including estheticians, dental therapists, naturopaths and physical therapists.
Supporting physician legislators
A critical component of PlastyPAC’s strategy is supporting physician-legislators, whose firsthand experience in healthcare uniquely positions them to advocate for policies that improve patient care and reduce administrative burdens.
In the 119th Congress, PlastyPAC helped increase the number of physicians compared to the 118th Congress. The PAC supported 12 incumbent physician candidates, 11 of whom won re-election. These physician-legislators include:
• Sen. John Barrasso, MD (R-WY)
• Rep. Neal Dunn, MD (R-FL-12)
• Rep. Mark Green, MD (R-TN-07)
• Rep. Andy Harris, MD (R-MD-01)
• Rep. Ronny Jackson, MD (R-TX-13)
• Rep. John Joyce, MD (R-PA-13)
• Rep. Rich McCormick, MD (R-GA-07)
• Rep. Mariannette Miller-Meeks, MD (RIA-01)
• Rep. Greg Murphy, MD (R-NC-03)
• Rep. Ami Bera, MD (D-CA-06)
• Rep. Raul Ruiz, MD (D-CA-25)
• Rep. Kim Schrier, MD (D-WA-08)
PAdditionally, PlastyPAC supported five newly elected physician-legislators:
• Rep.-elect Maxine Dexter, MD (D-OR03)
• Rep.-elect Bob Onder, MD, JD (R-MO03)
• Rep.-elect Herb Conaway, MD (D-NJ-03)
• Rep.-elect Mike Kennedy, MD, JD (R-UT03)
• Rep.-elect Kelly Morrison, MD (D-MD03)
As a result, the 119th Congress will feature more physicians than any Congress this decade. Among PlastyPAC’s supported candidates, several physician-legislators stood out for their contributions to healthcare policy. Notably, Dr. Murphy and Dr. Bera were key leaders in sponsoring H.R. 10073, the Medicare Patient Access and Practice Stabilization Act of 2024. This legislation prevents cuts to the Medicare Physician Fee Schedule in 2025 and includes an inflationary adjustment. By retaining their seats, these leaders will continue to bring vital medical expertise to health policy debates that affect plastic surgeons and their patients.
Building on success
PlastyPAC’s achievements go beyond election victories. Over the years, the PAC has been instrumental in helping ASPS secure legislative wins that directly benefit plastic surgeons and their patients. From expanding breast reconstruction coverage through the Women’s Health and Cancer Rights Act and patient education through the Breast Cancer Patient Education Act, to advocating for COVID-19 relief measures for medical practices, PlastyPAC delivered results.
Looking ahead, PlastyPAC remains focused on advancing policies that matter most to our specialty. In the next legislative session, priorities will include introducing new legislation to expand access to breast reconstruction, ensuring fair physician reimbursement and addressing administrative burdens that interfere with patient care.
Investing in our future
As we celebrate the successes of the 2024 election, we recognize the challenges ahead. Opposing groups are ramping up their advocacy efforts, and the fight for sound healthcare policy continues. With the ongoing support of ASPS members, PlastyPAC is well-positioned to meet these challenges head-on.
Supporting PlastyPAC is an investment in the future of our specialty. Your contributions ensure that the voices of plastic surgeons and their patients are heard in the halls of power. Visit plastypac.net to learn how you can get involved and make a difference. PSN
Thank you, PlastyPAC contributors
lastyPAC, the bipartisan political action committee of ASPS, works to educate and influence Congress on issues that directly affect plastic surgery. As the largest voice for reconstructive and cosmetic surgery, PlastyPAC is grateful for the support of the following people whose contributions during November help play a key part in the specialty’s success on Capitol Hill.
Alabama
Christopher Park, MDu California
Debra Johnson, MDI
Florida
Massachusetts
Theodore Calianos, MDI
Carolyn Rogers-Vizena, MD
New York
North Carolina
Lynn Damitz, MDH
Ohio
R. Michael Johnson, MDI
B. Aviva Preminger, MD, MPHu Scot Glasberg, MDI
Christopher Brooks, MDI
Andrew Rosenthal, MDI
Ueno, MDI
Evaluation & Management
• 17 NEW codes to report Telemedicine Services
• Deletion of Telephone E&M codes
8 NEW codes for Skin Cell Suspension Autograft (SCSA)
Expanded section for Hand, Digits, Wrist & Forearm Repair
• Including NEW code for carpometacarpal (CMC) suspension arthroplasty
• Updated guidelines and revised code descriptor to reflect this addition and new reporting guidelines
YOUNG PLASTIC SURGEONS PERSPECTIVE
WRIT TEN BY AND FOR YOUNG PL ASTIC SURGEONS
Managing the stresses that can affect any plastic surgeon
By Andrew McGregor, MD
Stress and anxiety are unfortunate parts of everyone’s life – especially as surgeons. As the transition from resident to attending occurs, many young surgeons feel that the stress of residency will diminish or go away completely. Although the transition can have its positive aspects, the stress of becoming an attending can prove to be much more pronounced than most young surgeons realize. Being fully responsible for your own patients can be daunting within the first years of practice. Stress and anxiety management during the first years of an attending’s career can help facilitate better overall well-being and better long-term performance.
Stress as a young surgeon can manifest itself in many forms. For most plastic surgeons in the first years of practice, stress emerges in a much different way than it might have during residency. For example, as a resident, stress might have resulted from managing a large patient load between multiple attendings, anxiety about in-service, fellowship matching and/or an intense workload. As a young surgeon, stressors often shift to the more detailed, technical aspects of surgery, preparation for boards, the pressures of ensuring patient satisfaction and making yourself productive in early years of practice.
Stress and anxiety in these years can have downstream effects. Weight gain, poor sleep patterns and depression are some of the effects
of poorly managed stress levels. These can then affect your work patterns, performance and productivity – as well as interfere with personal relationships.
Fortunately, there are ways to combat and manage both stress and anxiety as a young plastic surgeon. Exercise is great a way to help mentally reset your mind, especially from a stressful day or long case. It can be done through many activities – walking, jogging, biking, swimming, weight training or any combination of these. Engaging in activities that help you reset, review your thoughts and provide a break from the demands of surgery can help you not only perform better in the O.R., but also make you more efficient in day-to-day tasks. Exercise does not have to be an intense activity all the time, either. Moderate-level activity has been shown to be better for fat loss and maintaining weight, rather than constant high-impact activities that can also put you at risk for injury.
Another area that many people forget to focus on is carving-out time for hobbies outside of surgery. Residency can make you feel that your entire life is consumed with – and must be dedicated to – medicine. As you become a young surgeon, it’s important to realize the inherent need to have interests outside of practice. Whether playing an instrument, cooking or any of the other array of hobbies (Editor’s Note: Every issue of PSN highlights ASPS members’ non-clinical pursuits on “The Last Stitch” page at the end of
the magazine), it’s vital to have an outlet of stress relief that does not involve medicine. Indulging in these activities can sometimes make surgeons feel guilty that they’re not devoting enough time to the profession. Nevertheless, having an outlet to do something outside of surgery can prevent the burnout and fatigue associated with surgical specialties.
Fuel, focus
It’s also easy to forget that an important way to manage stress and anxiety is by taking the time to focus on what kind of fuel you are putting into your body. As a resident, many of us survived on a diet of graham crackers and peanut butter to get through a long day. The sustainability of limited nutrition during the day, however, leads to binge behavior. This then sends your body into a state of innate stress. One lesson I personally learned is that being a surgeon can, at times, be akin to being a professional athlete. To perform well, you must have fuel in the tank to execute a great surgery. Plastic surgeons often neglect to eat in order to push through tasks. In the long run, however, this can have a negative effect of weight gain and metabolism regulation as well. Interpersonal relationships outside of your practice can also be a source of stress for young surgeons. Whether trying to navigate the waters of the dating world, working through issues with your spouse or trying to find the time
to focus on building a family, there are plenty of matters outside of the O.R. to exacerbate stressors in other facets of any surgeon’s life. Many young surgeons had children in residency, which often cut into the limited free time that surgeons enjoy or anchor school and extracurricular commitments on your spouse. Stress and anxiety can be managed by communicating well with your partner. Whether you are trying to have a baby or commuting two kids to soccer practices, you and your spouse are a team – and a lack of communication will ultimately foster a sense of anger and resentment. It’s also important to remember that your children are only young once. If your schedule permits, be there for them. They remember more than you think.
The first years of developing your career in practice are a great time to not only build your technical wheelhouse, but also fortify the cornerstones of who you are as a person. Stress and anxiety will never go away – they are, unfortunately, an inbuilt part of our lives. Being able to manage them to make you more productive is a key part of any plastic surgeon’s growth and development. This will not only lead to becoming a better professional – and to becoming a better individual overall. YPS
Dr. McGregor specializes in plastic surgery of the breast and body, and is in private practice in Melbourne, Fla
‘Temet nosce’ – or how The Matrix can help guide your job search
By Noah Saad, MD
Atall, handsome man walks into a cramped kitchen, freshly baked chocolate chip cookies filling his nostrils. An elderly woman sits by the oven waiting for the cookies to finish, as she greets him. He’s hesitant and cautious, unsure of what to expect of his meeting with “The Oracle.” Neo has risked his life and the lives of the other rebels to find out if he’s “The One.” During this meeting, the Oracle points to a piece of art that says “temet nosce” and tells Neo it means “know thyself.” After some time, the Oracle gives Neo the onceover and proclaims that while he has the gift, he’s not The One. (Spoiler alert: He is; he was just waiting for another life.)
Now some of you might be asking, “What the heck does The Matrix have to do with plastic surgery?” Even more to the point, “What does this have to do with whether I’m going to go into academics or private practice?”
Those are great questions, and the answer
lies in that Latin phrase: Temet nosce. Besides the fact it’s my favorite scene in one of my favorite movies, it has so much to offer in wisdom. In short: Nobody can tell you whether you should go into an academic practice or private practice.
Only you truly know where you will be happy, but to find your answer, you need to be honest with yourself. What drives you? What makes you happy? What is important to you? These are the questions you need to ask yourself before you make a decision. We’ve all spent years and decades of our lives training to weigh the risks, benefits, pros and cons of performing any procedure. In truth, there are no pros and cons when comparing an academic practice and a private practice. They each offer different things. One is no better or worse than the other.
When I was going through my own job search, I interviewed with both academic and private practices. After my interviews, I needed to sit down alone and weigh what each opportunity offered me. In the end, my path to becoming an attending informed my decision
that staying in academic medicine would provide me with the greatest sense of fulfillment.
I suppose I should lay out what each type of practice offers, seeing as how the idea for this column is to provide advice on forging your future path. When I’m asked by my residents why I chose academics, I tell them what it has offered me. I love watching residents progress through training. Seeing a once hesitant, uncertain intern become a confident, competent chief resident is fulfilling to me. It’s so much fun watching that lightbulb switch on for each resident. I love being a small part of their growth. I love the mentorship that I can provide. I was excited about the research opportunities and additional resources available to me – and the great mentors that could help me as I tried to focus on the type of research I wanted to pursue. Additionally, being in a larger academic institution provides opportunities to handle more complex cases with patients, which can be very exciting.
Nevertheless, when I considered private-practice opportunities, I was intrigued by
the potential to be my own boss (or one of them, when I became a partner). Private practice can also widen the geographic opportunities to consider. The partners with whom I interviewed all spoke of their lifestyle, built-in flexibility and the ability to have more free time. They also noted the financial benefits of being in private practice – as your salary can be significantly higher than in academics. Perhaps most importantly (at least to my own job search), going into private practice does not mean that teaching and educational opportunities will not be available or expected through academic affiliations.
At the end of the day, nobody can tell you where you will be happiest. The path to finding your own fulfillment is an individual process that requires no shortage of reflection and soul searching. So, temet nosce – and good luck! YPS
Dr. Saad is a clinical assistant professor of surgery in the Division of Plastic and Reconstructive Surgery in the Department of Surgery at the University of Michigan, Ann Arbor.
Failing… with style: Taking lessons and encouragement from defeat
The best predictor of failure in plastic surgery is inexperience. This is true no matter the subspecialty – microsurgery, craniofacial surgery, hand surgery or aesthetic surgery.
Moreso than the technique used, the severity of the injury or the complexity of the defect or deformity, the factor consistently associated with higher complication rates is the surgeon’s number of years in practice. Failure is a given and, in many ways, an enemy that only time can tame – though never fully defeat. The challenge then is to fail with style, to appreciate the process and learn how to fail better until the outcome consistently resembles something like success.
Failure in surgery feels personal and uncomfortable. In the late 1970s, Charles Bosk, then a graduate student in sociology at the University of Chicago, published a book called Forgive and Remember. He was interested in how surgeons behave in matters of uncertainty and how they deal with mistakes and failure. After spending 18 months shadowing the house staff and faculty of several surgical services, he surmised that surgeons differ from other specialties foremost in how they frame complications.
“When the patient of an internist dies, the natural question colleagues ask is, ‘What happened?’ ” Bosk wrote. “When the patient of a surgeon dies, colleagues ask, ‘What did you do?’ ”
A morbidity and mortality conference highlights what you could have done differently. Although this weighty personal responsibility for failure is what creates tension in early-career surgeons, there are also opportunities for growth that arise from mistakes. Importantly, there’s an inherent immediacy in the feedback and agency in making improvements. We have control over how we respond to failure. Failing with style
means taking ownership of mistakes and staying committed to the notion that the future surgeon we evolve into will benefit from them.
It’s important to recognize that compared to the future version of ourselves, every day is a failure in some sense – be it in efficiency, management or delegation of team members, setup
or technique. These factors might not always lead to the dreaded complication but staying alert and cognizant to how they affect and directly impact our practice will accelerate what we ultimately hope for, which is to arrive at a future version of ourselves that’s less prone to mistakes.
The famous cellist Pablo Casals, on being asked why at the age of 93 he still devoted three hours a day to practicing, replied: “I’m beginning to notice some improvement.” Improvement happens in small, incremental – and often invisible – steps. However, it only happens through failure.
The framing of failure matters. Atul Gawande, MD, an endocrine surgeon at Brigham and Women’s Hospital in Boston, and the author of several best-selling books, has written extensively about surgical complications and the process of betterment. He emphasizes the importance of systematically analyzing performance and being deliberate in practice. Elite performers, he writes, set themselves apart by having a talent not only for their craft, but more importantly, a talent to practice at it. He sees failure as an opportunity and identifies the character of the practitioner as the most important predictor of future success. Most important, he argues, is to have people who are “conscientious, industrious and boneheaded enough to stick at practicing this one difficult thing day and night for years on end.” In other words, much of the style in failure lies in the response and the willingness to engage with it and convert it into something productive. That often requires seeking the advice of mentors and admitting one’s failings and mistakes.
It’s said that the best fellowship is the first year in practice. The intimacy of the failings during the preliminary years – when the expectation is that failure should be a thing of the past – make the lessons more profound. Failing with style means that these mistakes ultimately lead to improvement. The challenge is to try to live comfortably in the discomfort of constant failure – to put yourself in the same situation over and over again. To fail again, but to fail better. YPS
Dr. Prescher serves as a clinical assistant professor in the Division of Plastic and Reconstructive Surgery in the Department of Surgery at the University of Michigan, Ann Arbor.
The PSF thanks all those who donated in 2024
The PSF’s excellence and leadership within the specialty depend greatly on the generosity of ASPS members. From annual gifts that make an immediate impact to endowed gifts that support future generations of plastic surgeons, contributions to The PSF serve as the catalyst of innovation for our specialty.
Last year, your generous contributions, professional achievements and selfless enthusiasm enabled The PSF to perpetuate its reputation as the most distinguished research foundation in the specialty. Thanks to your generosity, The PSF provided grant funding for investigator-initiated research projects, international scholars at U.S. plastic surgery institutions, distributed Breast Reconstruction Awareness Fund grants to U.S.-based charities and awarded Charitable Care Breast Reconstruction Awareness Fund grants to cover breast cancer surgical care costs for women who otherwise could not afford reconstruction. A total of 1,385 donations were made from Jan. 1 through Dec. 31, 2024.
Sapphire
R. Barrett Noone, MD
Robert Ruberg, MD
Randy Sherman, MD*
Platinum
Eugene Podsiadlo
Sherwood Smith, MD
Diamond
Daniel Freet, MD
C. Scott Hultman, MD, MBA
Lindsay Nixon
Gold
Daniel Careaga, MD
Brooke Clark
Mimis Cohen, MD
Amber Leis, MD
Babak Mehrara, MD
Andrea Pusic, MD, MHS
Christine Rohde, MD, MPH
Justin Sacks, MD, MBA
Sterling
Frank Agullo, MD
Ashley Amalfi, MD
Jeffrey Ascherman, MD
Nebil Aydin, MD
Bruce Baker, MD
Mark Clemens, MD
Michael Costelloe
Lynn Damitz, MD
Dina Eliopoulos, MD
Heather Erhard, MD
Peter Fayek
Randall Feingold, MD
Brooke M. French, MD
Katerina Gallus, MD
John E. Gatti, MD
Lloyd Gayle, MD
Gayle Gordillo, MD
Amanda Gosman, MD
Karol Gutowski, MD
Josef Hadeed, MD
William Y. Hoffman, MD
Julie Holding, MD
Karen M. Horton, MD, MSc
Robert Howard, MD
Kenneth C. W. Hui, MD
Debra Johnson, MD
Timothy King, MD, PhD
Janice F. Lalikos, MD
Danielle LeBlanc, MD
Michele Manahan, MD, MBA
Bernard Markowitz, MD
Erik Marques, MD
Timothy Marten, MD
Alan Matarasso, MD
Evan Matros, MD
Leigh Spera, MD
David R. Stephens, MD
Srinivas Susarla, MD, DMD, MPH
Gregory Swank, MD
Raj Vyas, MD
Haven Barlow Jr., MD
C. Bob Basu, MD, MBA, MPH
Richard Baynosa, MD
Michael Bentz, MD
Gunnar Bergqvist, MD
Steven Bonawitz, MD
Earl Campbell, MD
Angela Cheng, MD
Jerry Chidester, MD
Michael Christy, MD
Maliniac Circle
The Maliniac Circle was named for ASPS co-founder Jacques Maliniac, MD. Fellows of the Maliniac Circle have made an outright gift of $50,000 or more, or a minimum deferred gift of $100,000, advancing plastic surgery to a higher level through research, innovation and public service. The following is a complete list of Maliniac Circle members. We thank them for their commitment to the specialty.
Dr. Bruce Achauer*
Dr. John and Candese
Alexander
Dr. Bernard and Susan Alpert
Drs. Darrick and Elizabeth Antell
Gwendolyn Maxwell, MD
Mark Migliori, MD
Paul B. Mills, MD
Andrea Moreira, MD
Brian Novack, MD
Linda Phillips, MD
Melissa Poh, MD
Samuel Poore, MD, PhD
Peter D. Ray, MD
Michael Reed, Esq.
Loren Schechter, MD
Dr. Stephan and Viviane Leao-Baker
Dr. Mark T. Boschert
Dr. Keith and Tina Brandt
Dr. Garry Brody*
Dr. Richard E. and Colleen A. Brown
Dr. Brentley and Diane Buchele
Dr. Rafael C. Cabrera
Dr. Theodore and Sheryl Calianos
Dr. John and Laurie Canady
Drs. Andrew and Amy Chen
Dr. Eugene and Ruth Ann Cherny
Dr. Norman and Pat Cole*
Dr. Sydney Coleman
Dr. Mark and Charlotte Constantian
Dr. Mary Ann Contongiannis and Ralph E. Huey
Dr. Robert N. Cooper
Dr. James R. and Gayle Cullington
Dr. J. Douglas and Barbara Cusick
Drs. Richard and Brenda D’Amico
Dr. Tancredi D’Amore
Dr. Lynn Damitz
Dr. Glenn and Maryann Davis
Dr. Sara R. Dickie
Dr. Sharadkumar Dicksheet*
Dr. T. Michael Dixon
Dr. Christine Dowbak*
Dr. Sepehr Egrari
Dr. Walter and Carolyn Erhardt
Dr. Daniel J. Freet
Silver
Todd Adam, MD
Ahmed Afifi, MD
Richard Agag, MD
Carl Askren, MD
Rafael Avila, MD
Glenn Becker, MD
Paris Butler, MD, MPH
James Butterworth, MD
M. Bradley Calobrace, MD
Holly Casey Wall, MD
Alexander Chase Castillo, MD
Manuel Chacon, MD
Edward I. Chang, MD
James Clarkson, MD
Brannon Claytor, MD
Michael Curtis, MD
Jorge de la Torre, MD, MSHQS
Anne DeLaney, MD
Sara Dickie, MD
Vidas Dumasius, MD
Themistocles Economou, MD
Sean Figy, MD
Ronald Ford, MD
Paige Fox, MD, PhD
Robert D. Galiano, MD
Noopur Gangopadhyay, MD
Patrick Garvey, MD
Jannine Griese
Meegan Gruber, MD, PhD
O. Allen Guinn, III, MD
Jeffrey Gusenoff, MD
Steven Haase, MD
Barry Handler, MD
Melinda Haws, MD
Drs. Heather Furnas and Francisco Canales
Dr. Roberta Gartside
Dr. John E. Gatti and Margaret M. Gatti, Esq.
Drs. David* and Lisa Genecov
Dr. Diane Gibby
Dr. Scot and Alisa Glasberg
Dr. R. Cole Goodman
Dr. Gayle M. Gordillo
Dr. Arun and Smita Gosain
Dr. Gregory A. Greco and Daniel Ranger
Dr. Richard and Robin Greco
Dr. Matthew Greives
Dr. B. Rai Gupta
Dr. Subhas and Seema Gupta
Dr. Geoffrey and Kathryn Gurtner
Dr. Karol and Ellen Gutowski
Dr. Bahman and Lora Guyuron
Dr. Dan and Mrs. Lynsi Hatef
Dr. James* and Barbara Hoehn
Dr. Scott & Julie Hollenbeck
Dr. C. Scott and Rev. Suzanne C. Hultman
Dr. Ron and Nancy Israeli
Dr. Ronald and Virginia Iverson
Dr. Jeffrey and Emily Janis
Dr. John and Marcia Jarrett
Dr. Debra J. Johnson
Dr. Michael Kalisman
Dr. Susan Kaweski
Dr. Brian Kinney*
Dr. Gurmander and Maninder Kohli
Drs. Joshua and Siobhan Korman
Scott Hollenbeck, MD
Henry Hsia, MD
Gary R. Jacobs, MD
Ellen Janetzke, MD
Jay Arthur Jensen, MD
Sang Yoon Kang, MD
Christopher Killingsworth, MD
Sugene Kim, MD
Jeffrey Kozlow, MD, MS
Aleksandra Krajewski, MD
Gordon Lee, MD
Sao Ieng Leong, MD
Scott Lifchez, MD
Samuel Lin, MD, MBA
David D. Lo, MD
Carl Manstein, MD, MBA, CPE
Aaron Mason, MD
Bruce Mast, MD
Gina McClure
Joyce McIntyre, MD
Alexander Mericli, MD
Charles A. Messa III, MD
Louis Miller, MD
Kerry-Ann Mitchell, MD, PhD
Lisa C. Murcko, MD
Jason Mussman, MD
Minh-Doan Nguyen, MD, PhD
Phuong Nguyen, MD
Son Nguyen, MD
Janet Parler, MD
Elizabeth Peterson, MD
Brett Phillips, MD, MBA
Ashley L. Pistorio, MD, MS
Julian Pribaz, MD
Edward Ray, MD
Edward Reece, MD
Renee Robbins
Carolyn Rogers-Vizena, MD
Paul Rollins, MD
Lorne Rosenfield, MD
Malcolm Roth, MD
Paul Ruff IV, MD
Marc J. Salzman, MD
Rajendra Sawh-Martinez, MD, MHS
Wesley Schooler, MD
Nicholas Webster, MD
Larry Weinstein, MD
Libby Wilson, MD
Michael Wong, MD, MBA
Arthur Yu, MD
Bronze
Peter Aldea, MD
Robert Allen Jr., MD
Adam Angeles, MD
Stephen Baker, MD
Jo Barta, MD
Michael Bernstein, MD
Alicia Billington, MD, PhD
Cristiano Boneti, MD
Keith Brandt, MD
Kristen Broderick, MD
Alberto Calvo Quiroz, MD
Chris Campbell, MD
Ubaldo Carpinteyro Espín, MD
Michael H. Carstens, MD
Ernest S. Chiu, MD
Carrie Kai-Cheng Chu, MD
Derek Cody, MD
Al Cohn, MD
J. Douglas Cusick, MD
Alexander Dagum, MD
Anthony N. Dardano, DO
Gloria de Olarte, MD
Patricia Eby, MD
Gregory Evans, MD
Robin Evans, MD
Erin Finnigan
Alberto Gallerani, MD
Lisa Gfrerer, MD, PhD
Amir Ghaznavi, MD
Cory Goldberg, MD, MSc, MBA
Luis Gonzalez Fernandez, MD
Gregory Greco, DO
Geoffrey C. Gurtner, MD
Anoush Hadaegh, MD
Adam Hamawy, MD
D’Arcy Honeycutt, MD
Tara L. Huston, MD
David Mathes, MD
G. Patrick Maxwell, MD
Tiffany McCormack, MD
Patricia McGuire, MD
Daniel A. Medalie, MD
Charlotte Michaelcheck, MPH
Taro Mikami, MD, PhD
Raymond Mockler, MD
Anita Mohan, MBBS, MRCS, PhD, MBA
Adeyiza Momoh, MD
Robert X. Murphy, Jr., MD
Paige Myers, MD
G. Neurohr, MD
Marilyn Ng, MD
Rajiv Parikh, MD
Anne Peled, MD
Alain Polynice, MD
Ariel N. Rad, MD
Sashank Reddy, MD, PhD
Brian Reedy, MD
Andrew H. Rosenthal, MD
Stephanie Rowen, MD
Moises Salama, MD
George Sanders, MD
Adam Schaffner, MD
Christopher Shale, MD
Makoto Shiraishi, MD, PhD
Sachin Shridharani, MD
Catherine Sommers
Jeff Swail, MD
Jordan Swanson, MD, MSc
Shruti Tannan, MD
Peter Taub, MD
Jesse Taylor, MD
Rudolf Thompson, MD
Winnie Tong, MD
Dawn J Wang, MD
Jane Weston, MD
Mark Wigod, MD
Steven Williams, MD
Warren Schubert, MD
Peter Schwartz, MD
Reginald Sherrill, MD
Lane Smith, MD
Isaac Starker, MD
Thomas Trevisani, MD
Victoria Vastine, MD
Christian Vercler, MD
Natalia Vidal, MD
Robert D. Wallace, MD
Dr. William and Linda Kuzon
Dr. David and Sherry Larson
Dr. David C. Leber
Drs. Bernard and Britt Lee
Dr. Charles K. Lee
Dr. Edward Lee
Dr. Samuel Lin
Dr. J. William Little
Drs. Joseph Losee and Franklyn Cladis
Dr. Dennis and Mary Lynch
Dr. Sergio Pasquale Maggi
Dr. Raman C. Mahabir
Fred* and Mary McCoy Foundation
Dr. Michael McGuire*
Dr. Dan and Jan Mills
Dr. Peter Neligan
Dr. Michael W. Neumeister
Laurene Isip
Ronald Iverson, MD
Sonu Jain, MD
Surinder Kaur, PhD
Shahrooz Sean Kelishadi, MD
Kenneth Kim, MD
Jason Ko, MD, MBA
Mark Labowe, MD
W. Thomas Lawrence, MD
Mary E. Lester, MD
Patricia Mars, MD
Dr. R. Barrett and Barbara Noone
Drs. John & Katie Osborn
Dr. Douglas Ousterhout
Dr. and Mrs. Vasu Pandrangi
Dr. Christopher Pannucci
Dr. Janet Parler
Dr. Ash Patel
Dr. James and Diane Payne
Dr. John and Susan Persing
Drs. Linda and William Phillips
Dr. B. Aviva Preminger
Dr. Patrick Proffer
Drs. Andrea and Martin Pusic
Dr. Norman and Deborah Rappaport
Dr. Debra Ann Reilly-Culver
Dr. William Riley
Dr. Luis M. Rios, Sr.*
Dr. Luis M. Rios, Jr.
Dr. Rod Rohrich and Diane Gibby
Dr. Stephen Ronan
Dr. Michelle Roughton
Dr. Robert and Cynthia Ruberg
Dr. Robert and Anne Russell
Dr. Justin Sacks
Dr. Kenneth* and Luci Salyer
Dr. Bernard* G. and Rhoda G. Sarnat
Dr. Loren S. Schechter
Dr. James D. and Kathleen Schlenker
Dr. Petra Schneider-Redden and Mr. Curt Redden
Dr. Paul and Barbara Schnur
Dr. Ali Seif*
Dr. Jack* and Anita Sheen
Kerri Woodberry, MD, MBA
June Wu, MD
Wayne Yamahata, MD
Diana Yoon-Schwartz, MD, PhD
Giving levels
Sapphire: $25,000+
Platinum: $10,000 - $24,999
Diamond: $5,000 - $9,999
Gold: $2,500 - $4,999
Sterling: $1,000 - $2,499
Silver: $500 - $999
Bronze: $375 - $499
Dr. Michele Shermak and Mr. Howard Sobkov
Dr. Randy Sherman*
Dr. Reginald L. Sherrill
Dr. Geoffroy and Lauren Sisk
Dr. Margaret and Stephen Skiles
Dr. Sherwood and Judith Smith
Dr. David H. and Janie Song
Dr. Scott* and Cynthia Spear
Dr. John (JT) Stranix
Dr. Anne Taylor and David Heutel
Dr. Kevin Tehrani
Dr. Jacob Unger
Dr. Karen Vaniver*
Drs. Nicholas B. Vedder and Susan R. Heckbert
Dr. Charles and Gale Verheyden
Dr. Amy Wandel
Dr. Philip D. and Elizabeth L. Wey
Dr. Linton and Renata Whitaker
Dr. Thomas C. Wiener
Drs Steven Williams and Anita Reddy
Dr. Robert* and JoAnne Winslow
Dr. Elvin* G. and Sharon Zook
Anonymous (2) *Deceased
PSF/DePuy Synthes Craniomaxillofacial Research Grant
Investigating a cell-free therapy for wound healing
By Jim Leonardo
Editor’s note: The following is part of an ongoing series highlighting The PSF Research Grant Award winners, and research they’re conducting to improve patient safety and develop new technologies for plastic surgeons. These features examine research funding awarded prior to the current year, as projects to which grants were awarded this year may not yet have results ready to discuss.
THE RESEARCHER
Justine Lee, MD, PhD
Title: Professor and Associate Chief, Bernard G. Sarnat Endowed Chair, UCLA Division of Plastic Surgery
Award: PSF/DePuy Synthes Craniomaxillofacial Research Grant
Project: Phosphate-eluting Composite Biomaterials for Skull Regeneration
PSN: What’s your objective in studying phosphate-eluting composite biomaterials?
Dr. Lee: The project seeks to assess the impact of a phosphate-eluting hydrogel (MCGPh) integrated with nanoparticulate mineralized collagen glycosaminoglycan (MC-GAG) on osteogenesis and skull regeneration. Specifically, it aims to evaluate how MCGPh enhances osteoprogenitor differentiation and mineralization compared to MC-GAG in vitro, and to determine its efficacy in promoting in vivo bone regeneration, biomechanical properties and safety in a rabbit calvarial defect model.
PSN: How far along are you in this work?
Dr. Lee: The project has successfully completed in vitro studies demonstrating that MCGPh significantly enhances osteogenic differentiation, late osteogenic gene expression and mineralization in human mesenchymal stem cells. In vivo studies have shown that MCGPh leads
Dr. Lee: The upregulation of OPG may be attributed to the extended phosphate release and mechanical properties of the hydrogel, which likely create a microenvironment conducive to anti-osteoclastogenic signaling. This highlights the interplay between material composition and cellular responses, suggesting a novel mechanism of action for the composite material.
PSN: Who are the individuals who helped with this work?
to improved skull regeneration, radiographic bone formation and biomechanical properties compared to MC-GAG. The most promising variant, aMCGPh40, showed sustained phosphate release, upregulated osteogenic signaling, and superior integration and stability.
PSN: What do you see as the practical possibilities of your research?
Dr. Lee: This project has potential clinical applications in developing off-the-shelf materials for skull regeneration and other bone defects. The findings could pave the way for more effective cell-free biocompatible scaffolds, addressing limitations in current bone grafting materials. Future possibilities include expand-
ing in vivo testing to other defect models and translating the material for human use.
PSN: Has anything unexpected surfaced, and how could it change your research?
Dr. Lee: An unexpected finding was the extent of osteoprotegerin (OPG) upregulation by aMCGPh40, which enhanced anti-osteoclastogenic activity. This suggests that MCGPh might not only promote osteogenesis but also modulate bone remodeling more effectively than anticipated. This could broaden the focus to explore its role in conditions with excessive bone resorption.
What are your thoughts as to what’s behind that development?
Dr. Lee: I would like to thank my co-investigators, Youngnam (Emma) Kang, PhD, and Wei Chen, PhD. Dr. Kang is a young material scientist who has been instrumental in all of the synthesis, material characterization and design of in vitro studies of the MCGPh material. Additionally, she and Dr. Chen, one of our project scientists in the lab, performed the in vivo experiments in conjunction with Meiwand Bedar, MD, MSc, a former postdoctoral Fellow in the laboratory who is currently a general surgery resident at Harbor-UCLA.
PSN: What did you want to be when you grew up?
Dr. Lee: Growing up, I aspired to be a pediatrician. Later, after completing my PhD, I thought I would become a pediatric hematologist-oncologist. When I finally encountered plastic surgery, I realized that I wanted to be a plastic surgeon. Ultimately, I merged the science side of my life with the medical side and became a surgeon-scientist.
PSN: What’s been your favorite research project besides this?
Dr. Lee: My favorite scientific project outside of my basic science work is understanding mental health quality-of-life outcomes for transgender and gender-nonbinary patients who undergo facial gender-affirming surgery. One of the most important aspects of this research is determining whether and how facial reconstruction improves symptoms of dysphoria, mental health and overall quality of life. Beyond improving patient outcomes, this research helps drive changes at the health policy and insurance coverage levels by providing rigorous data that was previously absent in the literature – an obstacle that has significantly hindered patient access to these surgeries.
PSN: How do you spend your time away from the lab?
Dr. Lee: I enjoy yoga, Pilates, hanging with my peoples and walking my skunk dog.
PSN: What sounds are most often heard in your lab?
Dr. Lee: I love ’90s hip-hop, especially West Coast. I detest angst.
For more information about the many research studies funded by The PSF or to support our current and future research initiatives, please go to ThePSF.org PSN
A costumed Dr. Lee (right of center, white-and-pink paw gloves) in her annual lab photo; a group selfie taken by Kelly Huang, BS, for Dr. Lee’s (powder blue shirt) lab graduation event; and 8-year-old Tiberius, named after Star Trek’s James Tiberius Kirk, lurks in the grass.
Furthering innovation
By Paul Snyder
Since its inception, plastic surgery has been a specialty built on a foundation of innovation – one which continually pushes the field of medicine toward new horizons. Whether these are groundbreaking medical advancements – such as Joseph Murray, MD, winning the 1990 Nobel Prize for Physiology and Medicine for the world’s first successful kidney transplant – or seemingly minor upgrades to O.R. equipment that made work incalculably easier for the generations that followed, the innovative spirit still burns brightly within the specialty. Now further fostered by ASPS offerings such as the Innovation Challenge at Plastic Surgery
The Meeting or through the ASPS/MedTech Innovator Accelerator program, which helps plastic surgeon innovators to get their ideas in the marketplace, the Society continues to actively support innovation in techniques and products that can change how plastic surgeons practice. The following are introductions to six companies that are toiling to advance medicine through an array of products and technologies.
Company: Akeyna
Location: Boston
Product: Sensor-enhanced injection needle
Presented: 2024 ASPS/MedTech Innovator Plastic Surgery Accelerator
Akeyna isn’t providing a detailed map of the location of a patient’s every blood vessel – but it might be providing the next best thing. The company has developed blood vessel-detection technology in the form of a miniature sensor embedded in the tip of a needle that warns physicians if they are about to inject dermal filler into a blood vessel.
“Safety is really the objective,” says Karen Cronholm, CEO and co-founder of Akeyna. “This is about providing the safest and best experience for their patients, but also peace of mind. One thing I kept hearing from physicians is the potential for catastrophic complications from these injections keeps them up at night.”
The sensor-enhanced needle is designed to be versatile and can be fastened to any standard syringe. Should the needle tip come in contact with a blood vessel, the physician will see a flashing red light. If they’re in a safe injection area, a green light is displayed.
was an ideal way to get plastic surgeons’ feedback and make inroads and develop working relationships with the ASPS community,” she says. “We gained valuable perspective on the kinds of complications that happen with dermal fillers, and larger issues that doctors face with fat-transfer procedures. It was wonderful to receive the insight and collaboration of the plastic surgeons who met with us in San Diego during Plastic Surgery The Meeting 2024 and who expressed an affinity for our technology. They see a clear benefit to their patients and their practices.”
Cronholm is not a plastic surgeon, but a scientist with 30 years’ experience in the life sciences industry who has worked on the development of multiple medical devices and products to support both dermatology and plastic surgery. The Akeyna technology was developed at Massachusetts General Hospital and Cronholm says the company’s participation in the ASPS/ MedTech Innovator Plastic Surgery Accelerator highlighted the specialty’s interest in the device.
“Being part of the ASPS/MTI cohort
The Akeyna technology has been licensed from MGH and is now in preclinical trials. Cronholm says the product has undergone animal testing and Akeyna is now planning clinical studies. FDA clearance will be needed to use the product on humans, and Cronholm anticipates the device will gain clearance and be in the market in the next couple of years.
“If patients see additional safety measures in place, they will feel a greater sense of comfort in undergoing these procedures,” she says. “The key thing about this product is that it is not a technology looking for a solution – it’s an answer to a problem that doctors are facing today.”
Company: Avance Innovations
Location: London, United Kingdom
Product: ORASIS
Presented: 2024 ASPS/MedTech Innovator Plastic Surgery Accelerator
When London-based plastic surgery resident Ankur Kha- juria, MD, went to India to do lab-based microsurgical training with rats, it didn’t take long for him to recognize an issue that’s faced microsurgeons for years.
“It was a pretty challenging task – con- necting vessels in a live rat model – and there was active bleeding and fluid pool- ing,” he says. “Without any assistance, I was having to clear the field and then try to stitch, and I thought: ‘There needs to be a better way of doing this.’ ”
Reaching out to contacts who had a 3D-printing facility and partnering with World Society for Reconstructive Microsurgery President-Elect Joon Pio Hong, MD, PhD, MBA, the wheels were quickly put in motion on ORASIS, a 3D-printed device for vascular anastomosis with autonomous irrigation and suction that cuts operative time, enhances vessel clarity and reduces costs for plastic surgery practices.
“I really think this will be a major disrup- tor in the space and transform the way we do microsurgical anastomosis,” Dr. Khajuria says. “It’s typically done with an assistant, and there are many interruptions that cause psychological stress and other burdens. It also can prolong operative time and cause patient safety concerns through possible damage to the vessel. With ORASIS, you’re
increasing autonomy, reducing stress and making the whole process much more effi- cient.”
The device was the runner-up in the ASPS Innovation Challenge in 2023 and got a further boost in being part of the 2024 ASPS/MedTech Innovator Plastic Surgery Accelerator.
“To meet and interact with other plas- tic surgeons and other innovators really seemed to fast-track my process and allow me to better anticipate potential problems with bringing the product to market,” Dr. Khajuria says. “Within the ASPS/MTI co- hort, we created a community where we reach out and talk to each oth er, make introductions – it’s all been great.”
Dr. Khajuria says he plans to begin clinical trials for ORA SIS, which is already on the FDA register, this year. After that he hopes for a limited mar ket release in some key hospitals throughout the United States.
“We’re starting with plas tic surgery, but I can see appli cability in lymphatic surgery, head-and-neck surgery, sarcoma surgery and more macrovascular applications, as well,” he says. “Once the device gets more widespread use, I think that will broaden the adoption into oth- er hospitals and enable some strategic partnerships with large distributors to scale the product.”
Company: Fasciotens GmbH
Location: Essen, Germany
Product: Fascial traction device for complex hernia surgery
Presented: 2024 ASPS/MedTech Innovator Plastic Surgery Accelerator
In the three years since fasciotens brought its fascial traction device to treat abdominal wall defects to market, it has become available in more than 30 coun- tries throughout Europe, Asia, Australia and Africa – and been part of more than 2,500 successful procedures
“The ultimate goal is to bring this to the United States,” says Clemens Winkler, MD, the company’s head of medical and scien- tific affairs.
That’s why Dr. Winkler says the interfacing with U.S.-based surgeons in the 2024 ASPS/MedTech Innovator Plastic Surgery Accelerator proved invaluable. It provided the opportunity to connect with experts and mentors who shared insights on what’s needed to gain FDA approval. The company would like to have its hernia device available in the U.S. market by 2026.
The product in question provides on-demand lengthening of the abdominal wall for complex hernia surgery. The typical approach to closing complex ventral herni- as without bridging involves extensive reconstructive procedures. These procedures often lead to higher complication rates and a weakened lateral abdominal wall. The hernia device applies standardized vertical-diagonal traction to the abdomi- nal wall. By using diagonal traction on the lateral abdominal wall, it enables myofas- cial lengthening and the possibility of direct fascial closure.
The prototype of the device, Dr. Winkler notes, emerged from a private project.
“We just wanted to see what was achievable,” he says. “Then it grew bigger
ImageAssist was born from a “pain point” that ASPS member Michael Golinko, MD, noticed in his Vanderbilt University medical practice. Although patient photography is critical to his – and most plastic surgeons’ – work, he says that trying to maintain consistency in those photographs was a constant challenge.
“It’s great that ASPS created photographic standards,” Dr. Golinko notes.
“The problem is that, as a plastic surgeon, if you’re training nurses to do it, it immediately can interrupt your workflow. If you’re a busy practice and you have 30 patients in clinic a day, it can be hard to get consistent photos. The photos we get back are so critical but of such variable quality – and we’re making medical decisions based on those photos. If I see a patient in the clinic, I depend on that photo when it comes time to operate.”
With the Society’s patient photography standards as a cue, Dr. Golinko teamed with coders at Vanderbilt, as well as Jonathan Sadlowe– who has more than 15 years’ experience as an entrepreneur and tech executive – to begin development of an iOS mobile application that automatically provides the standard ratios, frames and distances for any area that doctors need to photograph for reference.
“The core idea stems from a mobile bank deposit,” Dr. Golinko says.
By using your phone to photograph the patient, the app’s patent-pending ‘smart frames’ use a color-coded system to let you know when the subject is appropriately aligned. The app also deletes the background of the photo to provide an industry standard blue background for all pictures and it can be seamlessly integrated into Epic
and bigger. We didn’t set out with the idea of using this device for complex hernias or in- traoperatively – it all just came to light after we used it on the first few cases.”
The company also has two other devices in the European market for open abdomen pro- cedures and to repair congen- ital defects in pediatric patients. The company says the data it received from use in the European market is very convinc- ing, and that plastic surgeons who took part in ASPS/MTI cohort were enthused by the device’s possibilities.
“Many experienced plas- tic and general surgeons know that large abdominal wall defects require multi- ple techniques for closure,” Dr. Winkler says. “Beyond a certain defect size, closing them becomes extremely challenging, even with all the available surgical techniques. Our device is another tool in the box. It’s a completely new approach that can help you overcome these hurdles. The big and unique advantage is it stretches the ab- dominal wall in a controlled and repro- ducible manner. The data we’ve already gained from European studies show that, in most cases, we can lower the complica- tion and recurrence rates. This is an import- ant step to make abdominal wall recon- struction easier and better.”
medical software and the 4D-EMR system developed by ASPS member Robert Pollack, MD. Easy tag, search and export features provide seamless organization of photos and securing sharing options. Dr. Golinko also says the app can take video of particular areas to document range of motion and animation with different deformities. ImageAssist has body templates no matter where you operate – face, torso or extremities.
The developers add that even though the photos are taken with your phone, the app keeps that content secure behind a HIPAA-compliant cloud, meaning that patient photos will not show up when you pull out your phone to show a friend recent family or vacation photos. Security is also enhanced through biometric login.
The product was first launched in Vanderbilt’s Epic platform in 2021, and Dr. Golinko says that since then, it’s been used on more than 2,000 patients and put more than 5,000 photos into the system’s Epic platform. ImageAssist is now available for anyone to use through Apple’s App store.
“It’s been extremely enjoyable seeing how apps are developed – but it’s also a very real business for me,” Dr. Golinko says. “It’s a cool project that solved a pain point and turned into something much bigger. We get a lot of satisfaction from hearing about other people using it and say how it helped their practice, improved relationships with patients – but also saving them overhead and headaches down the line.”
Do you have an innovation that you want to share with your ASPS colleagues? Email PSN Managing Editor Paul Snyder at psnyder@plasticsurgery.org
Company: Lattice Medical
Location: Loos, France
Product: MATTISSE bioprothesis
Presented: 2024 ASPS/MedTech Innovator Plastic Surgery Accelerator (Winner)
It’s been nearly a decade since Julien Payen, the CEO and co-founder of Lattice Medical, first met with a biologist, a biochemist and a plastic surgeon to discuss the potential of a less-invasive autologous option for women undergoing breast reconstruction surgery.
“We wanted to provide something that would catch the best facets of breast implants and the best facets of autologous surgery,” Payen says.
After years of research – and the advancement of 3D-printing devices – the company developed the MATTISSE bioprothesis, a 3D-printed bioresorbable tissue-engineering chamber. The implant is made from a medical-grade resorbable biomaterial that has a porous base to fix the autologous tissue that needs to be regenerated, as well as a dome to provide the patient’s desired volume and shape. The benefits of 3D printing allow the device to be developed into various sizes and shapes to help individualize the patient’s reconstruction procedure.
Named for famed French painter Henri Matisse and doubling as an acronym for MAtrix Textile for TISSue Engineering, the MATTISSE bioprothesis emerged as the winner of the mid-stage grand final in the 2024 ASPS/MedTech Innovator Plastic Surgery Accelerator. Payen says the enthusiasm the product generated from plastic surgeons during the competition will become even more important as the company begins a years-long process to bring MAT-
In terms of regulatory requirements, the processes surrounding documentation and clinical trials are similar. The biggest difference for a startup company is the costs to bring it to market in Europe are lower, so we’re moving toward a European launch first.
“We will do the clinical trials in Europe and use this data to help our U.S. process – and what we heard during the ASPS/ MTI track was that a lot of plastic surgeons are interested in this technology and want to participate in further clinical trials,” he adds. “We are open to spontaneous candidatures for the future U.S. investigators.”
Although market clearances might still be up to seven years away, Payen says he’s excited by the prospects that advances in 3D printing can fortify in that time.
“I expect that after the clinical trial, we’ll have another version of the product based on input we receive from plastic surgeons,” he says. “Any kind of input from surgeons is crucial for us, so we are very glad to receive it. We will upgrade and adapt the product for the U.S. market. But as far as I know, we are also the only company in this segment to have developed our own printing factory – we are not subcontracting anything, we are doing all the implant printing ourselves. We want to demonstrate that you can make a reliable, cost-effective product – with new iterations that can be developed and generated quickly. The thing about the 3D-printing industry is that every year, you have a new machine. The evolution
Company: ReConstruct Bio
Location: Boston
Product: Breast BioImplant
Presented: 2024 ASPS/MedTech Innovator Plastic Surgery Accelerator
When Luba Perry, PhD, co-found- er and CEO of ReConstruct Bio, and part of Harvard’s Wyss Institute’s 3D Organ Engineering Initiative, began working toward a medical break- through in regenerative medicine, she ad- mits she didn’t yet realize the perfect target patient group for her team’s innovation.
“I did not know much about breast reconstruction or the limitations with the pro- cedure,” she says. “When I started talking with patients, I was stunned to learn how frustrated and deeply overlooked they feel. I couldn’t believe that breast implants are still kind of held to the same standards that they were in the late 1960s or 1970s.”
Most women who face a breast cancer diagnosis undergo mastectomy to treat the disease, and roughly 40 percent of those women choose to undergo breast recon- struction surgery. Artificial implants require monitoring and should be replaced within 10-15 years, and some implants’ associa- tion with other kinds of cancer have come under FDA scrutiny. Beyond reconstruction, artificial implants are also widely used for breast augmentation.
Although autologous tissue flaps are con- sidered a more “natural” approach, not all women have enough tissue for the proce- dure. The Breast BioImplant is a living, bioen- gineered free flap created from the patient’s own cells, obtained through liposuction and designed to provide a safer, more natural alternative to current standards. Dr. Perry’s team at the Wyss Institute worked on a pro- cess in which a patient’s cells are extracted to create dense, vascularized adipose tissue made of personalized pre-assembled organ
building blocks. These blocks are patterned into a network of interconnected channels that template blood vessels within the tissue and incorporate suturable cuffs to ensure that the implanted tissue has immediate and sufficient access to the patient’s own vascu- lar network.
The team developed a small-scale hu- man tissue prototype and successfully val- idated it in rats.
“We have demonstrated the tissue stays perfused and viable for nine days post im- plantation,” Dr. Perry says. “It was import- ant for us to get beyond seven days, which is the critical time point for flap survival in clinic.”
ReConstruct Bio is actively raising a seed round to fund large animal feasibility studies as a critical step toward clinical trials. ASPS member and clinical co-founder Samuel Lin, MD, MBA, who has been provided consul- tation to Dr. Perry’s team, says the product’s potential for plastic surgery could go beyond breast reconstruction.
“I see this as a key to being able to utilize and fabricate soft-tissue blocks to place anywhere in the body,” Dr. Lin says. “It could be head and neck for soft tissue defects after trauma, congenital issues – people born with soft-tissue asymmetries – or in the trunk area. Just to be able to minimize the donor site for these patients who otherwise might require a large incision somewhere on their body. This allows a more personalized approach to using their own tissue. In our lifetime, someone is going to be able to accomplish this. Why not us?” PSN
A Continuing Review and a valuable educational tool
Plastic Surgery: A Continuing Medical Education Review
Editor: Gustavo Chavarria-Leon, MD
ChavarriaPress, 2021
Plastic Surgery: A Continuing Medical Education Review is a comprehensive yet concise resource for all levels of plastic surgery learners, from trainees to veterans. Leveraging his wealth of experience, Gustavo Chavarria-Leon, MD, has artfully organized this book to inform readers of the ever-evolving techniques, technologies and ethical considerations within our specialty. It’s an excellent resource for students preparing for rotations, residents and Fellows preparing for board exams, as well as practicing plastic surgeons looking for a succinct update on a particular topic.
Each of the 58 chapters of this book is written by a different plastic surgeon, allowing for wide breadth of expertise and insight. The source materials for these chapters are from continuing medical education articles, Maintenance of Certification modules, peer-reviewed journal articles and the traditional texts of plastic surgery. The sources and suggested readings are also listed at the end of each chapter to allow for further reading on the topic if desired.
The material is arranged by each anatomic subspecialty of plastic surgery, including more broad chapters on fundamentals and aesthetics. The information is presented in a detailed, bulleted format for quick and clear understanding. Dr. Chavarria-Leon also included several high-quality and well-designed photographs, illustrations and figures to enhance both practical and deep understanding. The numerous graphics are a notable strength, depicting complex concepts in an easier-to-understand fashion.
One of the strengths of this volume is not only its depth, but the effort made to manage such an array of content while staying current in an ever-changing field. Dr. Chavarria-Leon covers many topics, from fundamental principles, basic anatomy and pathology to advanced procedures and innovations within the head and neck, breast, trunk, upper extremity and aesthetic surgery. The
inclusivity makes the book accessible to a broad audience, catering to medical students, residents in training and practicing surgeons aiming for continuous professional development. Complex concepts are presented clearly and concisely, ensuring that readers at varying levels of expertise can benefit from the material.
As a residency program director myself, the information contained within Plastic Surgery: A Continuing Medical Education Review is the kind of resource I encourage my trainees to study as they prepare for exams and clinical challenges. It’s an essential educational resource and an indispensable guide for anyone interested in advancing their knowledge of plastic surgery and fostering a deeper understanding of anatomy, pathology and surgical techniques. Dr. Chavarria-Leon’s expertise and dedication to education are evident, making this book a valuable asset for patient care and exam preparation. This book is a tremendous resource for those pursuing excellence in plastic surgery.
Don’t just survive the business of plastic surgery. Thrive
Society shares support, encourages donations for wildfire victims
ASPS supports our members, their families and staffs, patients and communities in Southern California as they cope with the devastating effects of the wildfires in their area. The thoughts of membership, leadership and staff are with all who have been displaced, experienced loss or are facing significant challenges during this difficult time.
ASPS has been in contact with the California Society of Plastic Surgeons, which encourages those interested in offering direct assistance to contribute to the American Red Cross (you can text the word CAWILDFIRES to 90999 to make a donation), which is on the ground supporting
Southern California residents, and the Los Angeles Fire Department Foundation.
“CSPS is here to support members in this crisis and its aftermath and work with our local and regional societies,” says CSPS Secretary Katerina Gallus, MD.
Links to additional resources helping plastic surgeons affected by the devastation can be found at plasticsurgery.org
“We admire the courage and dedication of all medical and emergency personnel as they continue to provide care in the face of extreme personal and professional adversity, and hope for a swift end to the destruction so that Californians can begin the process to rebuild their lives,” says ASPS President Scott Hollenbeck, MD. PSN
LATE-CAREER PERSPECTIVES
The transition from your practice: Essentials for success
By Enrique Fernandez, MD
As you begin to plan the transition away from your practice, it’s important to deliberate, develop a strategy and conceptualize the tactics necessary to support it. It’s also essential to consider your evolving role in the context of the transition process.
You are the leader
Throughout your career, you’ve functioned as the leader of your practice. You’ve developed a supportive staff and delegated a variety of responsibilities. Over time, this has fostered a mutual trust between you and your staff, based mostly on shared values as well as excellent performance focused on the welfare and safety of your patients.
However, transitioning away from practice is an unfamiliar process for you and your staff – and it’s important to keep this unfamiliarity at the front of your mind. You need to ensure you communicate your vision to staff with clarity and conviction to encourage their support. Early on, the path may not be clear – but the objective must be.
Situational awareness
As the process evolves, it coexists superimposed over ongoing patient care. It will require that you ensure there’s adequate staffing to support
the transition process. This might necessitate reassignments, modification of job descriptions and, perhaps, additional personnel. These changes have the objective of supporting and facilitating more senior staff to assist you directly through the transition. As you think ahead, you should also recognize that this evolution also represents the first steps of developing staff that will be needed to support another surgeon.
As leader of the transition, it’s essential that you also undertake a management role whereby you ensure efficient and effective execution. A central element of success is excellent communication characterized by clarity, timeliness and productiveness.
Matter of perspective
At this stage in your career, if you had to provide a quick assessment of your practice, you’d probably suggest it’s functioning just fine. Yes, it may need some fine tuning, but in general, you are satisfied with its performance.
Nevertheless, an essential element of preparation is ensuring that its current performance and profitability are optimized so that it’s ready for a future associate or buyer. In this context, the process also serves as the initial step to promote practice growth.
Take time to re-evaluate the big picture. Review your interests and think about the short- and long-term future as much as possible, but no further than you can see. Seek to
broaden your outlook and strive to consider the other party’s perspective. When you begin discussions with a prospect, ask questions that will inform you as to their expectations and overall outlook.
A buyer will likely have a different point of view, and you need to be able to put yourself in their place. The buyer might be coming into a new community, perhaps with a family. Buying a practice entails a significant financial investment and other commitments. For these and other reasons, you can expect that the buyer and their advisors will undertake a diligent evaluation of you, your practice and community.
What to do?
It’s important to be able to demonstrate that you have undertaken preparations to accommodate your new associate or buyer. You can address what you think is needed – as well as what you can reasonably anticipate from a buyer’s perspective. The due diligence put in upfront is often appreciated and will reflect upon you favorably.
It’s a good thing to “begin with the end in mind,” but it remains critical to know what needs to be done presently, and in a certain manner and order to achieve your goals.
The “what” can be summarized in one word: Preparation. This involves three specific goals:
1. To enhance the current function of your practice;
2. To increase the value of your practice by optimizing its profitability, and;
3. To prepare your practice to accommodate, support and promote a new plastic surgeon whether in a succession and/or sale.
To accomplish these goals, develop corresponding plans that are executed in sequence:
1. Optimize practice performance
2. Maximize practice profitability (and, therefore, value)
3. Prepare for a new plastic surgeon (via succession and/or purchase)
The creation of these plans is extremely valuable. Timely, ordered execution provides you with a methodology to achieve your goals and the success of your associate. Without them, the chances of achieving your goals will be considerably diminished. As it’s been said: “Hope is not a plan, it simply does not work.”
The design and execution of your customized plans will help you create a clear path marked by tranquility, triumph and the success of your design. PSN
ASPS Life Member Enrique Fernandez, MD, provides more retirement preparation insight online at enriquefernandezmd.com.
“Snow-Clad Evergreens, Grand Teton National Park, WY - 2010,” Photo by Enrique Fernandez, MD
For additional ASPS/PSF meeting information, visit the Meetings & Education page at www.plasticsurgery.org/meetings; e-mail registration@plasticsurgery.org; or call (800) 766-4955 / (847) 228-9900. Dates, locations and program information are subject to change without notice.
JANUARY
31-Feb. 2
Southeastern Society of Plastic and Reconstructive Surgery 40th Annual Atlanta Breast Surgery Symposium
Atlanta
Contact: (435) 901-2544
Web: sesprs.org
FEBRUARY
5-6
LIMITLESS Leaders Summit
Subscriptions:
• Plastic and Reconstructive Surgery Journal® (PRS)
• Plastic Surgery News® (PSN)
• ASPS Education Network (ASPS EdNet)
Members-only Access:
• Products and services to help grow your practice
• Inclusion on Find-A-Surgeon feature on PlasticSurgery.org
• Member discounts on educational meetings and symposia
• Advocacy that focuses on public and private sector issues, so you can focus on your practice
Boston
Contact: (847) 228-9900
Web: plasticsurgery.org/limitless
Jointly provided by ASPS, The Aesthetic Society and the American Hernia Society
6-8
Women Plastic Surgeons Symposium
Boston
Contact: (847) 228-9900
Web: plasticsurgery.org/wps
Directly provided by ASPS
20-23
12th Annual ACEPS Winter Meeting
Las Vegas
Contact: (978) 927-8330
Web: aceplasticsurgeons.org/Meeting/
24-28
Pan-African Plastic and Reconstructive Surgery Conference
Kigali, Rwanda
Contact: +250 791 693 973
Web: panafricansurgicalconference.com
28-March 2
ASPS Spring Meeting
Online
Contact: (847) 228-9900
Web: plasticsurgery.org/springmeeting
Directly provided by ASPS
14-15
ASPS Coding Workshop
Online
Contact: (847) 228-9900
Web: plasticsurgery.org/coding-workshop
Directly provided by ASPS
15
Northeastern Society of Plastic Surgeons Spring Workshop
New York
Contact: (978) 927-8330
Web: nesps.org/workshop/
20-23
The Aesthetic Meeting
Austin, Texas
Contact: (562) 799-2356
Web: theaestheticsociety.org
APRIL
3-5
ASPS Presents: The Global Plastic Surgery Congress (GPSC2025)
Buenos Aires, Argentina
Contact: (847) 228-3330
Web: plasticsurgery.org
Directly provided by ASPS
9-June 4
2025 In-Service Exam For Surgeons
Online
Contact: (847) 228-9900
Web: plasticsurgery.org/ise
Directly provided by ASPS
10-12
Diabetic Limb Salvage 2025
Washington, D.C.
Contact: (202) 451-6705
Web: dlsconference.com
Endorsed by ASPS
11
Wisconsin Society of Plastic Surgeons Annual Conference
Brookfield, Wis.
Contact: (920) 750-7721
Web: wisocietyplasticsurgery.com
MARCH
6-9
Mountain West Society of Plastic Surgeons 10th Annual Meeting
Olympic Valley, Calif.
Contact: (847) 228-3330
Web: mwsps.org
Jointly provided by ASPS
6
2025 In-Service Exam For Residents
Online
Contact: (847) 228-9900
Web: plasticsurgery.org
Directly provided by ASPS
MAY
1-4
70th Annual Plastic Surgery Research Council Meeting
St. Louis
Contact: 978-299-4510
Web: ps-rc.org/meeting
as the FDA or CDC. On the other hand, opponents worry that codifying Chevron deference could limit the AMA’s ability to challenge agency decisions that negatively affect healthcare providers, such as payment policies under Medicare – and that it would put too much power in vested political interests within agencies.
In other words, granting agencies more power could streamline healthcare regulations, but it also raises concerns about unchecked executive authority that might not align with physicians’ interests. The resolution was referred for further study, and ASPS will continue to track this issue closely, as its outcome could significantly impact the way healthcare policies are shaped moving forward.
Committed to physicians
From safeguarding surgical standards to reforming Medicare and examining the crossroads of medicine and the law, ASPS is committed to ensuring that the voices of plastic surgeons remain at the forefront of healthcare advocacy. The Society’s participation in the AMA is critical to ensuring that plastic surgery’s priorities are advanced in the House of Medicine. It’s imperative that ASPS members also join and take on active roles in the AMA to ensure the specialty is represented and plastic surgery’s voice is heard. To join the AMA or renew membership, visit member.ama-assn.org/ join-renew PSN
MultiPlan lawsuit
Continued from page 8
ble to unfair pricing practices. These specialized services require advanced skills, significant resources and lengthy recovery periods – all of which necessitate appropriate compensation.
Evaluating your claims
To determine if you should consider joining the litigation, review your practice’s out-of-network claims from 2015 onward, focusing on:
1. Claims processed by:
• MultiPlan (primary claims processor)
• Viant (a MultiPlan subsidiary specializing in medical bill review)
• Data iSight (MultiPlan’s data-analytics platform)
2. Claims involving defendant insurers:
• Aetna
• Cigna
• UnitedHealthcare
• Blue Cross Blue Shield affiliates
• Centene
• Humana
3. Documentation to gather:
• Explanation of Benefits (EOBs)
• Billing records
• Communications with insurers or MultiPlan about reimbursements.
4. Consult a healthcare attorney:
• A lawyer experienced in healthcare litigation can help you evaluate your claims and guide you through the process of joining the lawsuit.
A fight for the future
A master complaint has been filed in the litigation, and new plaintiffs now have a streamlined filing process that offers an efficient path to
the Mountain
join the lawsuit. Beyond the potential recovery of significant underpayments and damages, your participation carries broader implications. By challenging these practices now, ASPS members are fighting for the future of specialized medical care. The outcome of this case could establish crucial precedents for how insurers handle out-of-network claims, ultimately affecting the sustainability of independent plastic surgery practices across the United States. This is about maintaining the integrity of the profession and ensuring continued access to high-quality plastic surgery services for patients who need them. PSN
Matt Lavin is a Healthcare and Commercial Litigation partner in Arnall Golden Gregory LLP’s Washington, D.C., office, serving as court-appointed counsel for Direct Action Plaintiffs in the MultiPlan Health Insurance Providers Litigation.
CLASSIFIEDS
OPPORTUNITIES
You Just Found It! Are you looking for the best opportunity to launch your career, and have a great quality of life for you and your family?
Thriving 100% Cosmetic Surgery practice with 30-year regional reputation is looking for aesthetic fellowship trained surgeon, or experienced aesthetic surgeon to join our team. Freedom to grow the niche practice that you desire with overflow of surgical consultations and patient flow from 5 very busy aestheticians. No hospital call or climbing your way up the ladder doing injectables for years while you grow your surgical practice. You deserve to be supported by our experienced clinical and administrative family so you can focus on being your best and have the time to enjoy your family. Salary guarantee with productivity bonus, full benefits and partnership opportunity in only two years. Our not so senior, not so greedy senior surgeon will treat you like an equal, actually share consults with you, and help you grow your practice. We want future partners, not employees! Complete office renovation and expansion underway to support our rapid growth with the addition of in-house surgical suite. Located in an award-winning suburb with excellent schools, low cost of living, pro sports and busy entertainment and restaurant scene.
So what are you waiting for? Call our director Lisa Greaves, RN at 317-848-5518, or email at lgreaves@myplasticsurgerygroup.com.
West Coast Florida Plastic Surgeon
Well established 100% aesthetic surgery practice in Tampa Bay with accredited Office Surgery Facility seeks Board Certified / eligible Plastic Surgeon.
Submit CV and inquires to BPS500@aol.com.
Prime Location in Miami!
Are you a plastic surgeon seeking a modern, state-of-the-art practice space to share? We have the perfect opportunity for you!
Our brand-new office suite offers:
• Two fully equipped operating rooms
• Spacious, contemporary office space
Contact us today to schedule a tour. Info@EpicPlasticSurgery.com
For Sale: Maui Hawaii Plastic Surgery
Practice with AAAASF Surgery Center
Exclusive, turnkey plastic surgery practice with state-of-the-art, AAAASF certified surgical center. Stand-alone facility includes 4,340 sq. ft.: pre-op, recovery, exam, skin care rooms, waiting areas and exclusive parking lot. Attached bonus spaces ideal for Med-Spa. Well-established practice with a 25 year top “Best on Maui” reputation. Located in Kahului, close to airport, in prime business district. Ideal for new or expanding surgeon or consortium seeking a lifestyle change and/or second location. Maui offers world-class beaches, great schools, caring community, low taxes, and a relaxed yet vibrant lifestyle. Contact: mpsMaui2025@gmail.com
Office Sharing Opportunity
Newport Beach, California
A beautifully appointed office adjacent to Fashion Island area of Newport Beach, with onsite AAAASF operating room. Ideal for a second location, or someone building their practice. The senior surgeon specializes in Facelifts and would refer most of the “below the neck procedures”. The prospective candidate must have impeccable skills and affable personality, BC/ BE. Please submit a brief Cover Letter and CV to ackerman92660@gmail.com
100% Aesthetic Practice in Dallas/Fort Worth Metroplex
Signing bonus, large guaranteed salary and the ability to make huge bonuses with proven track record of success for young surgeons.
• 100% aesthetic practice
• Five locations in DFW Metroplex
• No insurance accepted
• No ER call, no nights, no weekends
• Dedicated 6 OR AAAASF accredited surgical facility
• 4 full-time anesthesia providers
• 5 medical spas
• Technology focused practice with 3-dimensional imaging, HIPPA compliant texting apps, state-of-the-art lasers and body contouring equipment
• Large dedicated social media team
• Personal patient care consultant for each surgeon
• 4 weeks paid vacation
• Additional paid time off for meetings
If you dream of being a successful aesthetic plastic surgeon, we can make it happen! Please email CV to sandy@northtexasps.com. To learn more about our practice, please check out our website www.northtexasplasticsurgery.com.
Unique Private Practice Opportunity in NYC
The ideal candidate is interested in performing breast reductions and top surgery for a small group practice in NYC specializing in these procedures. The practice is based in the Upper East Side of Manhattan, serves many patients who identify as people of color and/or LGBTQ, and takes pride as a health advocate for this demographic. A competitive pay structure with a generous productivity incentive, reasonable hours, and a routine schedule allow for a desirable work/life balance. The practice allows significant flexibility for surgeons to frequently work from home by relying heavily on telemedicine and physician assistants. Surgery and patient appointments are scheduled Monday to Friday, but not weekends. There is a call schedule for covering the practice, but no hospital call. Surgery is performed in an office OR, private ASC, or Lenox Hill Hospital, all within walking distance of each other. This position is only available for a full-time W2 employee, not a part-time independent contractor. Malpractice insurance is covered. Health insurance and 401k benefits are included. Applicants must be board certified/board eligible with the ABPS.
Please email a cover letter and CV to: info@breastsurgerygroup.com.
For more information about the practice please visit breastsurgerygroup.com.
Big City Practice Stress?
Tired of the rat race of a big city practice and ready for a change? After 31 years, I want to hand over my healthy solo private practice in a charming Southeastern town. My hospital is working with me.
Seeking a BC/BE plastic surgeon with microvascular/reconstructive surgery training looking for flexible and reduced hours and a great work/life balance. The candidate MUST have advanced training and proficiency in microsurgery with expertise in DIEP flap breast reconstruction. Only experienced candidates apply.
Email: LBoden@Greatrecruitingworks.com
Office Space Rental, San Francisco
Shared office space to rent 4 days a week in historic 450 Sutter building near Union Square. Great opportunity for plastic surgeon looking to expand or start their practice in the Bay Area.
If interested, please contact Chelsie at (415) 898-4161.
Desire to be your own boss in your own practice?
Seeking BC /BE surgeon desiring to assume ownership of established practice in America’s heartland, slower pace of life, no RVU pressure, physician-friendly state, metropolitan city with major university, active fine arts/music/ community.
Opportunity to purchase existing condo office, option of establishing offices in 2 states with different patient populations. Option to work with adjacent hospital, one office location has only one plastic surgeon in that area.
Opportunity to own and manage a private practice and make decisions independent of others.
For more information: http://pumc.com/aesthetic-practices-for-sale/
is an exciting turnkey opportunity providing all that the beautiful Palm Beaches has to offer. In addition to:
•Very competitive salary
•Excellent bonus incentive
•Full benefits program
•Retirement plan
•Excellent patient referral platform
•Luxurious and state of the art office environment
•Established practice for over 30 years
•Highly skilled support staff offering personalized care
•Supported by corporate business expertise and insight
Plastic and Reconstructive Surgery Opportunity with Partnership Track in New York City and Long Island.
Fast growing, well-established, and innovative practice seeking BE/BC Plastic Surgeon.
• Top Salary Match
• Immediate Bonus
• Benefit Package
• Personal Coordinator
• Dedicated PA/NP
• Devoted Staff
• Modern Office
• Private O.R.s
• State-of-the-Art Facility
Please email your CV to: drjnikfarjam@gmail.com executivedirector @thenewyouplasticsurgery.com
DM us @drjnikplasticsurgery
Plastic/Reconstructive Opportunity with Partnership Track Long Island & NYC
Excellent opportunity with partnership track. Well-established cosmetic plastic surgery practice with locations in Long Island and Manhattan seeks a plastic/reconstructive board certified/board-eligible surgeon to join our thriving practice. Modern offices, professional team environment, state-of-the-art and accredited facilities, knowledgeable and professional staff, competitive compensation and benefits.
Greenbergcosmeticsurgery.com
To apply, forward CV to docstg@aol.com or call 516-364-4200
Plastic & Reconstructive Surgeon
Southern Maine
Plastic & Hand Surgical Associates, the largest independent plastic surgery practice in Northern New England, seeks a BE/BC Plastic and Reconstructive Surgeon to join our group of 8 surgeons in South Portland, Maine in mid-2025. This opportunity involves a broad-based practice encompassing all areas of plastic surgery including general plastic, reconstructive, cosmetic, hand and microsurgery, for a diverse patient population. The practice operates an in-house AAAHC ASC. Our surgeons also provide plastic and hand services and coverage for the two hospital systems in Portland, one being a level 1 teaching hospital. We provide training to rotating residents from the Lahey Clinic plastic surgery residency program, general surgery residents from Maine Medical Center, and plastic surgery residents from Tufts University and Dartmouth-Hitchcock.
The ideal candidate has experience in all aspects of plastic, reconstructive and hand surgery. A candidate with specific interest in microsurgery and breast free flap surgery is preferred. Fellowship trained proficiency is encouraged but not necessary. Excellent people skills and a strong work ethic are required.
Plastic & Hand offers a collaborative environment where work-life balance is valued. The support of professionals including physician assistants, clinical, administrative and billing staff is provided. On call coverage, including hand, is required. We offer a competitive, guaranteed salary with potential to earn a productivity based bonus to start; eventual partnership buy-in is anticipated. Full benefits including but not limited to health insurance, malpractice insurance and 401k profit-sharing are included.
Please email CV to jswain@plasticandhand.com
Visit plasticandhand.com to learn more about our practice.
West Palm Beach, Florida
Plastic Surgery of Palm Beach, an established, Board Certified, Plastic Surgery Group located in beautiful West Palm Beach, Florida is seeking a Plastic Surgeon to join our team.
Make your home in South Florida where Palm Beach offers you beautiful beaches, water sports as well as the arts, culture and many outdoor events. You are Board Eligible/Board Certified, confident in your surgical skills, patient oriented and have an outgoing personality. Must possess a great work ethic and be willing to do reconstruction as well as cosmetic surgery. Call shared/flexible. We are looking for a long-term commitment that will lead to partnership for the right candidate. We offer a skilled support staff and a marketing team. Salary with bonus incentives, full benefits package including malpractice, health, dental, vision and retirement plan.
If you wish to join a great South Florida team, please send CV and cover letter to mds@plasticsurgerypb.com.
North Texas
Looking for a motivated surgeon to thrive in our state-of-the-art facility! Join a premier plastic surgery facility in North Texas, fully equipped practice with two operating rooms, offering patient comfort and privacy. Enjoy flexible terms, and comprehensive administrative support. Email us at karina@drplano.com for more details.
NW Plastic Surgery Practice For Sale
Sun Valley, Idaho, resort quality of life practice for sale; buy out or buy into 24-year practice and office building. Practice mostly outpatient cosmetic surgery and expanse of in office procedures. Letters of inquiry and CV to Tom Crais motsiarc@aol.com. 208 788 7700.
Opportunity for BC/BE Plastic Surgeon to Join a Busy Private Practice in Houston, TX Memorial Plastic Surgery (MPS) is a leading aesthetic and reconstructive plastic surgery practice. This is an excellent opportunity for a BoardCertified / Board-Eligible Plastic Surgeon, with a strong interest in microsurgery to perform DIEP flap breast reconstruction and/or cosmetic breast and body procedures, to join a well-established practice known to deliver unparalleled patient care and results.
MPS OFFERS:
• Heavy volume of patient overflow for associate to build practice
• Mentorship and hands-on training with premier group of board-certified plastic surgeons
• Team-oriented staff for administrative and clinical support, including marketing and social media needs
• Physician offices, spacious exam rooms, MedSpa area for non-surgical services
• Private AAAHC accredited ORs located on-site
• Multi-specialty ASC located directly one floor below with direct access to 4 additional ORs
COMPENSATION:
• Competitive compensation models
• Benefits package - Medical/Vision/Dental Insurance & 401k plan
• Partnership track opportunity
QUALIFICATIONS:
• Board Eligible or Board Certified in Plastic
Texas
• Aesthetic fellowship/training a plus, but not required
• Must have a passion for delivering high-quality patient care and results
Qualified applicants are encouraged to apply by submitting an updated CV & headshot photo to: APPLY@MEMORIALPLASTICSURGERY.COM
Office Sharing Opportunity in Beautiful Portland, Oregon
Amazing opportunity available now for a BC/BE Plastic Surgeon to share a medical office space with one established plastic surgeon. Suite is in a professional medical office plaza with outpatient surgery center in building, and connected to a busy hospital. Suite includes two doctors’ offices with mountain views, multiple exam rooms, and two separate reception desks to support separate practices. Outstanding opportunity for a surgeon starting a new practice or desiring a new or second location.
Please submit Cover Letter and CV to mia.skourtis@providence.org.
Long
Island Plastic Surgery Practice For Sale
Board certified plastic surgeon with over 25 years’ experience in same location looking to retire. Practice is 100% cosmetic and well established located in beautiful Eastern Long Island. Practice is located in 3,500 sq. ft. turnkey suite with stateof-the-art medical equipment including 3 lasers. Excellent location to raise a family and less than 2 hours from Manhattan. Owner willing to stay on during transition with option to finance sale. Please email eeprhs@gmail.com.
Beverly Hills Office Space To Share
This is a great opportunity for a BC/BE plastic surgeon to share a large, sunny office with an established plastic surgeon. The office suite is in one of the best-known medical buildings in Beverly Hills. There are multiple ambulatory surgery centers in the building, and is minutes away from the world-renowned Cedars Sinai Medical Center. The office space would include two dedicated offices for the surgeon and consultant, a reception desk, as well as the use of up to three exam rooms. This is an outstanding opportunity for a new surgeon starting out or an established surgeon who wants to relocate. Please submit cover letter and CV to drminniti@drminniti.com
TRAINING
Stanford Microsurgery Fellowship
A one-year position in Microsurgery is available beginning August 1, 2026, through July 31, 2027, at Stanford University Medical Center. Individuals acquire expertise in comprehensive microsurgery and complex reconstruction, including reconstruction of the breast (TRAM, DIEP, Omental, SGAP, TUG, SIEA, PAP), lower extremity, peripheral nerve, facial reanimation, hand, brachial plexus, nerve transfers, and lymphedema (LVA, lymph node transfer, liposuction). Stanford is a Level I Trauma Center as well as a Comprehensive Cancer Center.
You will be appointed as a Clinical Instructor. Opportunities are available for participation in global health, basic science, and clinical research projects, as well as medical device development. Individuals typically perform over 150 microvascular cases each, and work with ten full-time microsurgeons.
inquiries to: Dung Nguyen, MD, Director of Microsurgery, Division of Plastic Surgery; Stanford University Medical Center; 770 Welch Road, Suite 400, Palo Alto, California 943045715. Jhernan9@stanford.edu.
MISCELLANEOUS
Plastic Surgery Biller
Specializing exclusively in Plastic Surgery billing with over 25 years’ experience. We check for correct coding for maximum reimbursement and review each claim before submission. Once the claims are submitted, we follow closely and appeal when necessary. We work remotely, off-site with excellent references. Call Ana at 239-541-9993.
Please apply through SF Match. Please direct
SURGEON SPOTLIGHT
Editor’s note: The bulk of PSN’s pages are devoted to specific elements of our mission statement – to keep members informed of the social, political and economic trends and educational opportunities that affect the specialty of plastic surgery.
KEEPING TIME INSIDE AND OUTSIDE THE O.R.
At age 77, and having played drums essentially all his adult life, Robert Gilman, MD, DMD, Ann Arbor, Mich., has seen plenty – as well as inhabited the same spaces of some of the greatest figures in rock ‘n’ roll.
Dr. Gilman comes from a musically inclined family – his mother and sister played piano, while his father was a professional saxophonist and a distant cousin was head of the Hart School of Music in Hartford, Conn. He found himself drawn to the sound of percussion over that of musical notes, and developed an affinity for the sounds of jazz – in particular, that of Joe Morello, who sat behind the kit during the recording of the Dave Brubeck Quartet’s Grammy Award-winning instrumental, “Take Five.”
“I saw him play in college at an outdoor venue in Connecticut, where the opening act was (piano great) Thelonious Monk,” Dr. Gilman tells PSN. “I sat in the first row, and in the middle a song, Joe broke a stick that came out to me – and I kept it. About 20 years ago, I attended a drum camp where Joe was a featured guest, and I told him the story about the stick. He turned to me and said: ‘Oh, that’s where it went. I’ve been looking for it. I want it back!’ It was fantastic.”
Dr. Gilman eventually became part a 12-piece band called the Regressions. The breadth and scope of their repertoire attracted musicians from all fields and levels, including Eddie Willis – one of the Funk Brothers of Motown fame. A one-off meeting between band members and Willis turned into a long-lasting relationship between the physician and musician – strong enough that he invited Dr. Gilman to be a guest at his Hollywood Walk of Fame induction.
He also had the opportunity to play with other drummers of note, including Jim Chapin, the father of the late singer-songwriter Harry Chapin. “I was at a drum camp with Jim, who was one of Buddy Rich’s teachers in the 1930s and 1940s – and he regaled us with numerous stories. What a phenomenal opportunity.”
But not all of his encounters have had a positive ending. Dr. Gilman and his wife, Chris, have made dozens of trips to Antigua for relaxation, dwelling in an area known for its celebrities – including Keith Richards of the Rolling Stones and Eric Clapton, whose house is just two doors away from the Gilmans’ usual rental. One night, an obnoxious man accompanied by a younger woman joined them in conversation at a bar pre-dinner. “He told us stories that he had just come from South America and had gotten sick, the food was terrible, everything was terrible. Then he started hitting on my wife, but it was actually pretty funny,” Dr. Gilman says. “I asked the owner later who the guy was, and we were told it was the guitarist from another legendary band. My wife said: ‘I don’t care. He was an a------.’ ”
Dr. Gilman says playing the drums and his work in the O.R. are related through repetition. “Being a good surgeon is having all the rudiments down, and when you’ve practiced for a long time, as I have, when you see something new, you know how to deal with it, just like playing drums.”
While the ASPS Active Member is planning his retirement from plastic surgery, Dr. Gilman has no such plans for his drumming, his lifelong love. “I’m gonna go until the day I die,” he says. PSN
10 YEARS AGO IN PSN
With several major companies announcing security breaches and the theft of millions of consumers’ credit card information, the discussion on hackers and data breaches turned local after multiple plastic surgery practices had to inform thousands of patients that their personal information might have been compromised by cyberattacks. ASPS members, security experts and legal counsel provided insight and tips to plastic surgeons in the January/February 2015 issue of PSN:
“We often encounter the belief that data security is an issue for the managed-care world and large healthcare providers that traffic in ‘big data,’ but not for boutique private practices or elective procedures. We regularly encounter plastic surgeons who don’t think this really matters. Successful plastic surgeons who plan to stick around are going to need to take the issue seriously and have a strategy for data security. ”
– Harry Nelson, JD Managing Partner, Nelson Haridman LLP PSN
PSN is pleased to take liberties with the “social” aspect of its mission statement by presenting a good-natured look at the lives of notable members who we believe are making significant contributions to the specialty.
In this issue, we present ASPS member Patricia Mars, MD, Tucson, Ariz., a solo practitioner, and creator and owner of Venus by Mars Cosmetic Surgery. Dr. Mars serves on the Emerging Trends Subcommittee, Women Plastic Surgeons Steering Committee and the Assembly of Member Sections. She’s belonged to several additional ASPS committees, groups and panels over the past several years – and she was a quizzer for the PSN Presidents Forum held during PSTM24 in San Diego. Between hitting stores to gather the ingredients for her famous Christmas tamales, Dr. Mars found time to answer the following questions for PSN:
If I had to start my career over, I would... Do the same thing. I love my job and have never regretted my choice of career.
The best thing about being a plastic surgeon is... That I actually get to spend a good amount of time and build well-established relationships with my patients – I think more so than other specialties. There are patients in my practice who’ve been with me from the beginning. I enjoy the loyalty and longitudinal relationships where you really get to know people.
The worst thing about being a plastic surgeon is... Dealing with patients with unrealistic expectations. This is one of the hardest parts of my job.
The best part of next weekend will be... Making Christmas tamales, which is a serious family tradition. My family has been making red chili tamales for generations and my children now love this tradition. The whole family is involved, and we drink margaritas and listen to mariachi music the entire day. The tamales still turn out delicious!
The best thing I ever purchased for my office was... Our fancy Nespresso machine, which makes delicious, frothy coffee, which I love. It’s a treat and an indulgence. If I had to pick a surgical device, it would be my power-assisted liposuction cannula. The work of liposuction is no joke, and this makes a huge difference in effort.
My all-time favorite movie is... Pride and Prejudice, the 2005 Keira Knightly version. I love historical and period dramas, and this one has amazing cinematography and a beautiful soundtrack.
An operation I no longer perform is... Rhinoplasty. I decided about six years ago to concentrate on the operations I really love doing. With rhinoplasty, I just don’t enjoy the difficult personalities and the stress of how particular these patients tend to be.
During the shutdown, something I worked on outside of medicine was... After a long break, I started doing yoga again with all that time available – and to reduce stress. Since then, I’ve become very dedicated to practicing at least three times per week. I also got more into gardening and built an in-ground raised garden box. I love how they significantly improve my quality of life.
The best vacation I ever took was... A week in Paris for a significant birthday (none of your business). We spent the whole week just indulging in all things French: food, fashion, art and wine – and it was all incredible.
I couldn’t operate without my... Music. My anesthesiologist (and best friend, who I went to medical school with) is usually the one picking the tunes. We listen to a few different playlists: all-female pop, 1980s, 1990s and alternative.
My biggest surprise in the O.R. was... Becoming pre-eclamptic while doing a mommy makeover and going into early labor three weeks before my due date. All ended well, but that was one serious surprise, as it was my first pregnancy.
The best thing a grateful patient ever gave me was... I’ve gotten some incredible pieces of jewelry. My two favorites are a beautiful silver flower pin that my patient, a jewelry designer, made by hand for me. The other is a star-shaped pendant with little multi-colored pave sapphires embedded, given to me by another jewelry designer. I love them both so much.
The words I try to live by are... “Run toward your complications, not away.” I learned this from one of my mentors during general surgery training. We all have complications, but how you handle them is what sets you apart. Learning to handle these with grace, skill and perseverance makes for a very grateful patient. PSN
Dr. Gilman holds the tempo during a recent performance by his band the Regressions.
Patricia Mars, MD
Dr. Mars multitasks on the front patio of her Tucson home by nursing a margarita while assembling one of her traditional Christmas tamales.
U.S. Patent #8,328,598 B2 U.S. Patent #8,784,347 B1