HEALING PROCESS
The skin, when injured, immediately begins the healing process Skin restoration occurs through a dynamic, continuous, complex and interdependent process, comprising a series of overlapping phases, called healing To better understand this process, its various phases will be discussed below
a) Immediate reaction
It is the first stage of this process, constituted by the body's initial response to trauma. It occurs with a vascular and inflammatory reaction, which leads to hemostasis, the removal of cell debris and microorganisms Immediately after the trauma, vasoconstriction occurs, which stops the bleeding This process involves the presence of platelets, fibrin clots that activate the coagulation cascade, resulting in the release of substances to form the temporary extracellular matrix that supports the migration of inflammatory cells, followed by the activation of protection and preparation mechanisms tissue for the development of healing Inflammation leads to known clinical manifestations of heat, pain, edema and loss of function, signs that can be minimal, transient or lasting Infection intensifies and prolongs inflammation
b) Proliferation

It's the second step It occurs after the initial inflammatory reaction and comprises the following stages: granulation, epithelialization and contraction Granulation is the formation of new tissue, composed of new capillaries (angiogenesis), proliferation and migration of fibroblasts responsible for collagen synthesis With the production of collagen, there is an increase in the strength of the ulcer, called traction force, characterized as the ability of the ulcer to resist external forces and not break At the end of this phase, epithelialization occurs, which is the step that will lead to the closure of the ulcer surfaces, through the multiplication of epithelial cells at the edge, characterized by the reduction of capillarization and the increase in collagen. At this point, the contraction reduces the size of the ulcers, with the specialized action of fibroblasts
c) Maturation and remodeling
It is the third step in the healing process It is a slow process, which begins with the formation of granulation tissue and the reorganization of proliferated collagen fibers, extending for months after re-epithelialization It is responsible for increasing the traction force During remodeling, there is a decrease in cell activity and the number of blood vessels, loss of the fibroblast nucleus, leading to scar maturation In this phase, the lesion repair process is reorganized, with collagen deposition. Initially, the healing has a flat appearance; later, it stiffens and rises After a certain time, the scar b li h l i id d fl i i d i

17
INFLAMMATORY PROLIFERATIVE MATURATION
FACTORS THAT INTERFERE WITH HEALING
Among the various factors that make healing difficult, some stand out, such as: the longer the evolution of the ulcer, as well as its extension and depth, the longer the time required for healing

Continuous pressure on the injured area by bony prominences, calluses and/or continuous immobilization leads to interruption of the blood supply, preventing blood flow from reaching the tissues.
In infection, the presence of foreign bodies and devitalized or necrotic tissues prolong the inflammatory phase of the healing process, causing tissue destruction, inhibiting angiogenesis, delaying collagen synthesis and preventing epithelialization These must be removed by mechanical or autolytic process, for the repair phase to occur
Edema is characterized by the accumulation of fluid in the body (blood, lymph and others), due to trauma, infections, iatrogenic, infectious and inflammatory diseases It interferes with oxygenation and nutrition of tissues in formation, prevents collagen synthesis, reducing cell proliferation and reducing tissue resistance to infection.
The dressing technique can cause mechanical trauma, caused by aggressive cleaning (friction with gauze, liquid jets with excess pressure), dry coverings adhered to the ulcer bed and/or inadequate, which interfere in the healing process, delaying healing
Age is an important factor in healing In children, scarring occurs quickly, but they are prone to hypertrophic scarring Among young people, healing can be delayed by systemic processes added to the psychosocial process and activities of daily living
With advancing age, the inflammatory response decreases, reducing collagen metabolism, angiogenesis and epithelialization, especially if associated with conditions that often accompany senility such as malnutrition, vascular insufficiency and systemic diseases
An adequate nutritional intake of proteins and calories, in addition to vitamins such as vitamin C and zinc This contribution may be compromised in cases of malnutrition, gastrointestinal malabsorption and inadequate diets Obesity makes mobilization and walking difficult, leading to a sedentary lifestyle, which can cause disorders such as venous hypertension, which makes it difficult for ulcers to heal On the other hand, it is known that obesity acts as an immunosuppressive disease, which can inhibit the inflammatory reaction and, consequently, alter healing. Anemia has been referred to as an interfering factor in ulcer repair. Smoking reduces functional hemoglobin and causes pulmonary dysfunction, predisposing to tissue oxygen deprivation Nicotine produces vasoconstriction, which increases the risk of necrosis and peripheral ulcers Alcoholism can damage the brain, heart, liver and pancreas, and interfere with treatment adherence
18
ULCERS
Ulcer is any interruption in the solution of continuity of the cutaneous-mucosal tissue, causing alterations in the anatomical structure or physiological function of the affected tissues
CLASSIFICATION OF ULCERS
Ulcers can be classified, according to the cause, into: surgical, non-surgical; according to the repair time, in acute and chronic, and, according to the depth, in relation to the extension of the tissue wall involved (epidermis, dermis, subcutaneous tissue and deeper tissues such as muscles, tendons, bones and others), in degrees , I, II, III and IV.
Grade I: there is an involvement of the epidermis; the skin is intact but shows signs of redness, discoloration, or induration
Grade II: partial tissue loss involving the epidermis or dermis occurs; the ulceration is superficial and presents in the form of an excoriation or blister
Grade III: there is involvement of the epidermis, dermis and hypodermis (subcutaneous tissue)
Grade IV: involvement of the epidermis, dermis, hypodermis and deeper tissues
Grade 0: ulcers have intact skin.
Grade 1: ulcers are superficial with exposed subcutaneous tissue
Grade 2: ulcers have a deeper extension
Grade 3: ulceration implies the formation of an abscess or osteomyelitis
Grade 4: ulcers involve partial gangrene of the forefoot

Grade 5: ulcers involve extensive gangrene
19
NEUROTROPHIC ULCER
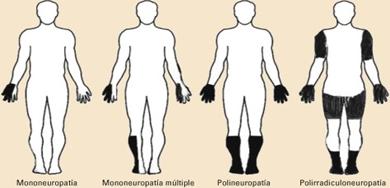
This ulcer is caused by peripheral neuropathy, due to some underlying pathologies, such as: leprosy, diabetes mellitus, alcoholism and others People with these pathologies, which affect the peripheral nerves, are at greater risk of developing injuries to the autonomic, sensory and motor fibers, which can result in primary injuries, such as claw hand, foot drop and ankylosis (hardened joints); and secondary, such as muscle paralysis, fissures, plantar ulcers and traumatic injuries
The autonomic fibers responsible for the maintenance of the sebaceous and sweat glands, when affected, lead to a reduction in the production of their secretions The skin becomes dry, inelastic and can easily cause cracks which, if left untreated, will compromise the structures of the hands and feet, increasing the risk of infection
Loss of protective sensation (thermal, painful and tactile) or anesthesia in the hands and feet influence the appearance of skin lesions This compromise leads to an increased risk of burns, the appearance of blisters and calluses, resulting from continuous pressure on support points, requiring the use of insoles and appropriate shoes Other factors that influence the appearance of these ulcers are changes in motor fibers, due to muscle weakness and paralysis This imbalance leads to deformities, compromising function and increasing the risk of triggering these ulcers In the country's primary healthcare services, a higher incidence of plantar ulcers caused by peripheral neuropathies has been observed The basic cause of neurotrophic ulcer is loss of protective sensation or anesthesia in the plantar region, due to damage to the posterior tibial nerve However, there are other factors that influence the appearance of an ulcer, such as: paralysis of the intrinsic foot muscles, loss of the normal pad under the metatarsal head and dry (anhydrous) skin Anhidrosis resulting from dysfunction of the sweat and sebaceous glands makes the palm and sole of the foot dry and its horny layer, hard and thick, tends to break. “Cracks” or fissures in the upper and lower limbs are very common and often act as an entry point for infectious agents

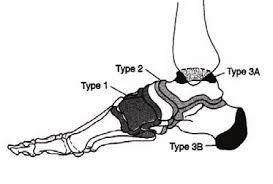
Changes in the anatomy of the foot caused by changes in the bone structure create abnormal pressures, facilitating the appearance of ulcers. The other functional factor is gait, that is, in addition to the lack of sensitivity, the foot is subjected to efforts, such as long walks, strides or jogging, the presence of foreign objects in the shoes (stones, nails), which contributes to the ulcer development. Neurotrophic ulcers are classified in degrees, according to tissue involvement, from a superficial lesion to deeper lesions, with involvement of the joint, tendons and bones, osteomyelitis being very common, with subsequent necrosis, gangrene and loss of bone segments
20
Callosity (thickening of the keratin caused by the pressure of the tissues to friction) and tension in areas that support the greatest weight are also a risk for ulcers
When the calluses are thin, they can be considered protective, but when they are thick and located in areas with reduced sensitivity, they damage the soft tissues and become predisposing factors for ulcers, in addition to being common on the edges of neurotrophic ulcers Considering the loss of sensitivity and increased pressure as risk factors for the development of ulcers, some measures can be taken to monitor the evolution of pressure in these risk areas, such as: guidance on the use of footwear, special insoles, on daily activities and adaptation of work instruments Neurotrophic ulcers can be described based on the following characteristics: they are anesthetic lesions, circular, usually hot and showing no signs of infection They develop over areas of bony prominences, more frequently in the lower limbs They are usually preceded by hyperkeratosis (callosities)




21
APPLICATION OF TOTAL CONTACT CAST IN NEUROPATHIC ULCERS
Total contact cast are recognized as the gold standard treatment for neuropathic plantar diabetic foot ulceration, endorsed by all national and international consensus documents Despite this, research has shown that there is a division between the existing evidence supporting the use of total contact models in the treatment of diabetic foot ulcers and their use in clinical practice
A cornerstone in the management of DFU (Diabetic Foot Ulcers) is the reduction of pressure through unloading. There are many products available for the physician to reduce the pressure of an DFU, including removable devices below the knee and non-removable full contact molds A total contact cast is a rigid or semi-rigid molded cast that extends from the patient's foot to just below the knee, maintaining contact with the entire plantar surface of the foot and leg and immobilizing the surrounding joints and soft tissue, allowing the patient to remain in outpatient treatment. A total contact mold uses minimal padding to protect the malleolus, tibial shaft and DFU
The use of padding provides full contact with the entire foot while isolating the DFU and significantly reduces peak pressure (p = 0.008) and pressure-time integral (p -0 0012)
The DFU is expensive to run, with an estimated annual expenditure of between $9-$13 billion in the US Hospitalization of patients with DFU represents between 73 7% and 80% of the overall overall cost, and leads to longer hospital stays Private health insurance payments nearly double in patients with DFU compared to patients without DFU ($28,031 vs $16,320 respectively) The estimated cost of a lower limb amputation is between $35,000-$45,000, although these numbers do not include past DFU management or indirect costs associated with lost productivity, family status, or quality of life
On the other hand, the use of total contact models showed substantial cost savings when compared to other treatments ($11,946 vs $22,494 per patient, respectively) In addition, a recent publication highlighted the cost-effectiveness of walkers with non-removable totalcontact cast compared to removable walkers due to the impossibility of removing the appliance, forcing its constant use
In addition, cure of DFU from all causes has been reported between 60% and 77% However, total contact models have shown improved cure rates when compared to other offloading devices in the treatment of plantar neuropathic DFU, with cure rates ranging from 89% to 92%, and in some cases over significantly shorter period
Despite these benefits, Sinacore reported that 45% of the clinics did not offer an efficient service with qualified and experienced professionals in the management of DFU and in the making of the full contact plaster
More recently, studies have shown that total contact molds are not regularly used in the management of plantar DFU and shoe modification is the preferred method of unloading despite its ineffectiveness in reducing plantar pressure and shear forces
This is despite the fact that total contact models are recognized as the gold standard treatment for plantar DFU by all consensus committees.
22
Traditionally, it was believed that a total contact cast worked by equalizing plantar pressure, as the entire plantar surface of the foot was in contact with the inner surface of the cast, creating a larger surface area, redistributing pressure across the entire foot However, other authors have reported a reduction in the plantar contact area as the load capacity of the fused rigid wall lifts the foot Total contact models also showed a greater reduction in plantar load when compared to ankle or below-theankle devices and below-the-knee removable walkers The cast shank has been shown to remove 30%-36% of foot pressure when compared to a cast shoe

Frictional shear forces are also controlled when the foot is held firmly in position. When compared to shear-reduced walkers, total contact casts are associated with improved cure rates This suggests that there are several mechanisms that reduce pressure and shear forces and improve DFU outcome and cure time.
It is widely accepted that total contact casts "force compliance and enhance treatment" as patients are unable to remove the cast, maintaining plantar load distribution and decreasing pressure points at ulcer sites. Armstrong and colleagues evaluated the difference between computerized accelerometers worn at the waist and those hidden in removable plaster walkers in the same patients The results showed that participants recorded higher levels of daily activity on the waist accelerometer compared to that found on the removable walker, which recorded only 28% of daily activity
This suggests that patients use removable below-the-knee walkers less than a third of the time thus reducing treatment efficiency; whereas a non-removable device enforces continued use compliance Patients treated with a total contact cast are also significantly less active compared to other discharging devices, thus reducing the number of repetitive stress cycles and improving DFU healing Shorter stride lengths and reduced walking speeds have also been recorded using total contact casts, reducing vertical forces through the foot.
Total contact models may be contraindicated under certain circumstances Some authors recommend its use only in uninfected neuropathic ulcers in the absence of PAD (Peripheral Arterial Disease)
However, Nabuurs-Franssen and colleagues conducted a study involving 98 patients with a combination of DPN (Diabetic Peripheral Neuropathy), moderate PAD (Peripheral Arterial Disease), and infection (PEDIS grade ≤2)
23
In this prospective, nonrandomized study, researchers aimed to determine the outcome and complications of total contact models in patients with DFU complicated by DPN, DPN and PAD, DPN and infection or DPN, DAP and infection. They treated the patients in one or a combination of traditional full contact cast, removable bi-valve contact cast and shoe model cast The authors found that patients with DPN or DPN and infection or DPN and PAD cured 90%, 87%, and 69% of the time, respectively Importantly, the authors reported rates of new ulcerations and pre-ulcer changes of 9% and 29%, respectively Although none of these were related to PAD or infection and resolved before the main ulcer healed, suggesting that patients with moderate PAD or infection are no more at risk of developing full plaster complications than patients without PAD or infection Patients with the triad of DPN, PAD, and infection had worse outcomes, with cure occurring in only 36% of DFUs The authors did not allude to the reason for this significant difference However, it is well established that DFU with PAD and infection have the worst treatment outcomes. Although this trial was non-blinded and non-randomized, the use of full contact casts was found to improve DFU outcome in the presence of moderate PAD and infection and has now been endorsed by the International Working Group on the Diabetic Foot However, patients must be monitored carefully, and the clinician must have a high degree of experience in managing these types of wounds

The decision to use a cast may depend on the level of exudate around the wound Highly exudative wounds may require daily dressing changes In these circumstances, a bivalve or removable plaster may be considered or the creation of a window at the DFU site.
The most common side effects resulting from the use of a full contact cast are skin abrasion or iatrogenic ulceration However, a study evaluating the development of iatrogenic ulceration found only 22 new ulcers in a sample of 398 devices, which equates to an iatrogenic ulceration rate of 5 52%, as important, the author reported no deterioration in pre DFU -existing It has also been found that the iatrogenic ulcer heals before the primary ulcer To reduce the risk of iatrogenic ulceration, padding should be used to protect the bony prominences, and patients should be advised to check for signs of bleeding or redness in the exposed toes and to protect the contralateral leg with a long sock or pillowcase when in bed to reduce contact with fiberglass mold Patients should also be taught to check the integrity of the cast and the treating physician should review any problems
24
Long-term use of total contact cast has been associated with muscle atrophy and reduced bone density To eliminate these problems, Carvaggi et al (2000) first applied two layers of fiberglass for flexibility and strength (Softcast 3M; 3M Health Care, St Paul, MN) A second high load-resistance fiberglass bandage was used to reinforce the design (Scotchcast 3M; 3M Health Care) This was placed first between and extended beyond the two malleolus A second layer was then applied to the plantar aspect of the plaster, which gave the plaster a rigid construction. They found that using a combination of rigid and semi-rigid casting materials minimized these complications Furthermore, the introduction of a gait rehabilitation program can reduce the adverse effects of muscle atrophy and loss of bone density, although this has not yet been examined
A leg-length discrepancy can also occur, resulting in further postural instability or worsening. This must be considered during patient selection. Low-profile plasters can be used with a lightweight material to minimize instability, or patients can purchase shoe balancers for the contralateral limb
25
INDICATION AND TECHNIQUE OF MAKING THE TCC
Peripheral neuropathy ultimately leads to numb feet and loss of proprioceptive ability, which reduces the reflex arc of defense against trauma
Repetitive trauma or even gait itself, when associated with loss of protective sensitivity, can trigger capsuloligamentous injuries, collapse of the medial arch, predisposing to fractures and dislocations not perceived by the patient
The resulting deformity can lead to the appearance of abnormal pressure zones predisposing to the development of ulcers The formation of ulcers creates a highrisk situation, as they can become contaminated, evolving with involvement of adjacent soft tissues, reaching the bone, progressing to amputations, sepsis or death
Several methods have been proposed for the treatment of this type of ulcers, including bed restriction, local wound care with debridement, changing shoes, topical agents and surgical interventions such as: ostectomy, arthrodesis and amputations
The concept of total contact cast, first described by Brand in 1950, created a new trend in the treatment of this pathology, based on the principle of load distribution across the surface in contact with the soil Remembering that Pressure=Force/Area, increasing the area of contact with the ground will decrease the vertical pressure in the plantar region, distributing it evenly

Regarding the technique for making the plaster cast, we observed that it is fundamentally important to model the sole of the entire plantar area of the foot, including the support of all the toes, providing load distribution over the largest possible contact area Thus, there is no load concentration in the ulcerated region, allowing local tissue regeneration and progressive healing
Originally, the TCC was described and is still widely used today in its "closed" form, that is, covering all fingers and leaving no opening for them Sometimes, for varied needs such as the patient's feeling of "claustrophobia", dorsal lesions on the skin of the fingers, skin irritations or erythema in the areas of bony prominences, we use the "open" form of the TCC, maintaining an opening for the fingers
26
In this way, we obtained the claustrophobic patient's collaboration and adherence in continuing the treatment and we were able to better monitor the evolution of the dorsal lesions of the toes, as well as the general condition of the forefoot, without having noticed any damage or delay in the healing of these ulcers
Another advantage observed in open plaster is the possibility of ventilation, which greatly reduces the unpleasant odor that invariably accompanies closed TCC
In addition, the association of the foul odor with the non-visualization of the toes generates in the patient and family members the constant doubt about "whether the foot is not rotting in the plaster", often contributing to giving up or avoiding the continuity of the plastered treatment

Literature is vague when referring to the mean time to closure of ulcers treated with the TCC Usually, an average period of six to eight weeks for the ulcer to heal is mentioned Walker et al reported closure around 30 6 days for forefoot ulcers and 42.1 days for hindfoot ulcers. Myerson et al reported a mean healing time of 5.5 weeks for ulcers with a mean diameter of 3 5 cm Bridges and Deitch reported a mean period of six to eight weeks, without reporting the mean ulcer size
In our survey, the mean healing time of ulcers was 46.3 days, and the mean size was 2 1 cm for grade I lesions and 5 2 cm for grade II
Thus, we believe that the adjusted model for calculating the healing time based on the size of the ulcer or the use of the adjusted table for this purpose is extremely valuable, as it allows the individualization of each case and informing the patient and their families of the most accurate period when healing should occur and, consequently, when everyone will be involved in the ulcer closure process. Such information provides greater involvement and collaboration on the part of the patient and their families, allowing for family, social and economic planning that are important in the routine of patients undergoing long-term treatments
27
The analysis of the variable grade (ulcer depth) was significant, showing that patients with grade II ulcers took longer to heal The average size of grade II ulcers was greater (5 2cm) than that of grade I ulcers (2 1cm), explaining the longer healing time due to their larger size and not due to their greater depth

Regarding the use of closed and open casts, the statistical tests showed that the means and medians of the ulcer size versus plasters needed for healing did not show any significant difference (Student's test with p value = 0 42 and the test of Mood with p value = 0.666). Thus, the use of closed or open cast does not change the healing time

28
INDICATIONS
The TCC is indicated in patients with peripheral neuropathy presenting superficial plantar ulcers, grades I and II of Wagner (and in cases of neuroarthropathy of Charcot in phases I and II of Eichenh0ftz)
CONTRAINDICATIONS
The absolute contraindications are: deep infection, dermatoses, arterial insufficiency and grades III, IV and V of Wagner. Relative contraindications include diseases that lead to edema in the lower limbs such as heart failure and kidney disease, blindness and morbid obesity
CONSTRUCTION TECHNIQUE
The first cast is applied for approximately 1 week or less if excessive drainage is anticipated. Subsequent molds are changed every 2 weeks. Average healing time is 6 weeks
Charcot fractures are cast for up to 3 months or when surface temperatures are within 2 degrees centigrade.
Indications:
Plantar ulcers of the insensitive foot Neuropathic Fractures (Charcot Fractures)
Contraindications:
Acute infection
Wound tracking, ulcer depth greater than width
Overdraining wound
Claustrophobia
Fragile skin
Excessive edema
Benefits:
Immobilization
Protects tissue from further trauma
Reduces / controls edema
Keep walking
Disadvantages:
Possible joint stiffness if immobilization is prolonged
Possible secondary abrasions if cast is incorrectly applied or not carefully monitored
29
It is important that the person responsible for placing the TCC is a qualified professional and that the monitoring of the patient is strict in order to reduce risks and avoid complications.
The TCC is applied differently from other casts, as the filling is only used on the anterior part of the tibia, instep and malleolus, thus achieving close contact with the leg, foot and ulcers on the bony prominences are also avoided.
It is applied with the patient placed in a prone position, with the leg flexed at 90º in relation to the thigh, and the ankle in a neutral position In this position, the gastrocnemius muscles are relaxed and better contact with the leg can be obtained and the excess soft tissue is directed towards the knee, which facilitates maximum use of the "cone effect"; also, in this position, the professional has more access to the plant, which is the most important area, and the formation of edema decreases during application
The wound is first covered with a sponge dressing, then the cotton layer is placed over the feet and extends to the base of the knee, pulling on its distal part to cover the toes
Subsequently, a pad or several layers of cotton is placed on the anterior aspect of the tibia, the instep, the sole, heel and malleolus to prevent pressure ulcers. Lie the patient in the prone position and two bandages are placed, in plaster or fiberglass, in a spiral from distal to proximal, covering the fingers and rising to 3 cm below the knee. The base of the cast is molded carefully and intimately with the sole of the foot
All folds made must be over padding Later, two splints are formed with plaster or fiberglass covering of the fingers in the proximal part of the plaster; when placing them one on top of the other, the excess is folded to fill the plantar arch and, therefore, the sole is completely flat
The splints are fixed with a plaster or fiberglass bandage placed in a spiral shape
Plaster has to be left to dry for 15 min, or until it cools and becomes hard
The first change in the TCC is made after 7 days, which is when there is a greater reduction in the edema, and the plaster loses its fit, favoring friction Subsequent changes will ideally be made fortnightly if TCC is used in Charcot foot
It may be that patients with ulcers with profuse exudate require more frequent exchanges to prevent ulcer maceration; Likewise, very active patients may need more frequent changes due to deterioration of the cast
TCC discharge should be continued, as with any discharge method, for a week or two after healing so that the foot is ready to change to shoes with special insoles or orthosis
30
Preparation for cast placement includes debridement of all necrotic wound tissue and callus removal If the tissue is devitalized, scraping until there is bleeding from the wound may be evaluated

ULCER ASSESSMENT, DEBRIDEMENT AND DRESSING
The assessment of the wound must be done in detail, checking the depth, diameter, tissue types and the presence and type of exudate
Characteristics of the ulcer and the skin around it: may indicate skin changes, such as: hyperemia, heat, edema, pain, maceration, dryness, desquamation, eczema, hyperpigmentation, or other changes, which are also valuable to guide the treatment
Exudate characteristics: can be valuable indicators to determine treatment The color and consistency of this may vary Serous and bloody fluids are considered normal Purulent exudate indicates an infectious process
Appearance of the ulcer: the type of tissue present indicates the stage of the healing process in which the ulcer is:

Necrotic tissue: varies in color, from black, gray, whitish, brown, to greenish and black It corresponds to dead, dehydrated tissue, and pus and fibrous material may also be present
Fibrinous tissue: yellow in color, with a creamy consistency, due to the amount of cell degradation Fibrin may cover the entire length of the ulcer or appear as fibrin points partially covering the lesion
Grain fabric: It looks red, shiny and moist The diseased tissue has a pale-dark appearance, may bleed spontaneously and has a friable appearance (which breaks easily), indicating an ongoing infectious process
Epithelialization tissue: it has a pinkish-white appearance, which migrates from the margin to the center of the ulcer.
Measurement of the ulcer: allows you to follow the evolution of the healing process
The frequency of this procedure will depend on the type of ulcer
31
Excess tissue from the bora should be removed to prevent the callus from macerating the wound and delaying healing
The cleaning of the wound bed should be done until vitalized tissue is noted, to favor spontaneous granulation The ulcer must be measured at its largest and smallest diameter


The ulcer is covered with an appropriate dressing and also gases are placed between the fingers to minimize lateral-medial pressure, preventing maceration of the interdigital space.

BAND AID
Dressing is the set of care given to an injury or ulcer, aiming to provide safety and comfort to the patient and promote healing
PURPOSES OF DRESSINGS
A dressing, to be effective, must serve the following purposes:
Be impermeable to water and other fluids, allowing gas exchange.
Be easy to apply and remove, without causing trauma
Assist in hemostasis
Protect the ulcer against mechanical trauma and infections.
Limit tissue movement around the ulcer

Promote a moist environment
Absorb secretions.
Treat the existing ulcer cavities
Promote debridement
Relieve pain.
Provide favorable conditions for the patient's activities of daily living
32
CHARACTERISTICS OF AN IDEAL DRESSING
Remove exudate
Keep high humidity between wound and dressing
Allow gas exchanges
Be impervious to bacteria
Provide thermal insulation
Be free of contaminated particles and toxic substances from ulcers
Allow removal without causing local trauma
Ulcer cleaning
The ulcer cleaning technique consists of removing cell debris, foreign materials, necrotic or devitalized tissue and reducing the amount of microorganisms present on the surface This cleaning must be performed with proper technique, using sterile material
The handling of the ulcer must be carried out carefully and rigorously, in all its extension and depth, and may be carried out with mechanical cleaning and irrigation
Mechanical cleaning, with gauze or cotton balls, is currently not indicated, as it can traumatize newly formed cells, triggering inflammatory reactions and increasing healing time Cleaning with gentle irrigation with saline or saline solution of 0 9% sodium chloride is recommended, because this solution does not harm the tissues and cleans the ulcer, removing all exudate and/or foreign body present, without traumatizing the cells of the bed of it, accelerating the healing process
The ulcer bed must be kept moist, and the entire surrounding skin must be cleaned with gauze moistened with saline solution After cleaning the area around the ulcer, dry it with gauze to avoid maceration of the intact skin and facilitate the fixation of the cover
Covers
As we consider the term curative as the process of topical care for the ulcer, we will adopt the term coverage to designate the product used to cover the ulcer bed Covers can be classified as primary, secondary and mixed The primary coverage is the product that remains in direct contact with the ulcer bed on the adjacent skin, in order to absorb its exudate, facilitating the free flow of drainage, preserving the moist environment and non-adherence This type of dressing requires permeability to fluids, non-adherence and impermeability to bacteria The secondary covering is the product that covers the primary covering, in order to absorb excess drainage, providing protection and compression This type of dressing needs to have satisfactory absorption and protection capacity Mixed coverage is the product that has two layers, one in contact with the ulcer bed and the other in contact with the external environment
33
MAIN TYPES OF COVERAGE
DRESSING WITH MOISTED GAUZE IN PHYSIOLOGICAL SOLUTION
Composition: sterile gauze and 0 9% saline solution
Mechanism of action: maintains moisture in the ulcer, favors the formation of granulation tissue, softens devitalized tissues, stimulates autolytic debridement, absorbs exudate
Indication: maintenance of moist ulcer, indicated for all types of ulcer
Contraindications: none
HYDROCOLOIDS
Hydrocolloids are dressings that can be presented in the form of a plaque, paste, gel and granules
Composition: hydrocolloid in plaque is a synthetic dressing derived from natural cellulose, which contains hydrophilic particles that form a self-adhesive elastic plaque
Mechanism of action: Cellulose particles expand when absorbing liquids and create a moist environment, which allows cells in the ulcer microenvironment to provide self-lytic debridement This condition stimulates the growth of new vessels, granulation tissue and protects nerve endings
Indication: plaques are indicated for ulcers with a small or moderate amount of secretion
Contraindication: they are contraindicated in cases of infection, mainly by anaerobes.
TRANSPARENT FILM
Composition: the transparent film is a sterile dressing made up of a polyurethane membrane, covered with a hypoallergenic adhesive and has a certain degree of permeability to water vapor.
Mechanism of action: maintains a moist environment between the ulcer and the dressing, favors autolytic debridement, protects against trauma, favoring healing
Indication: it should be used in superficial ulcers with minimal drainage, in grade I, and in the prevention of pressure ulcers
Contraindications: not recommended for exudative, deep and infected ulcers
CALCIUM ALGINATE
Composition: alginate is a polysaccharide composed of calcium, derived from some algae
Mechanism of action: this type of dressing has debriding properties Before use, it is dried and, when the alginate fibers come into contact with the liquid medium, they carry out an ion exchange between the calcium ions of the dressing and the sodium ions of the ulcer
Indication: can be used on infected and exudative ulcers
34
ACTIVATED CHARCOAL
Composition: this type of dressing has a covering made up of a pillow containing a fabric of activated carbon whose surface is impregnated with silver, which exerts a bactericidal activity, reducing the number of bacteria present in the ulcer, especially gram negative ones
Mechanism of action: this dressing has a high degree of absorption and elimination of ulcer odor Activated carbon fabric removes and retains exudate molecules and bacteria, exerting a cleansing effect
Indication: it is indicated in exudative ulcers, infected with accentuated odors, in fistulas and gangrene
Note - In little exudative ulcers and in cases of osteotendinous exposure, it should be used with restrictions, due to the possibility of dryness of the lesion site
SILVER SULFADIAZINE
Composition: 1% silver sulfadiazine, hydrophilic
Mechanisms of action: the silver ion causes protein precipitation and acts directly on the cytoplasmic membrane of the bacterial cell, and has residual bacteriostatic action, by releasing this ion
Indication: colonization prevention and burn treatment
Contraindication: hypersensitivity
Note - There is silver sulfadiazine with cerium nitrate, which can be used on burns, infected and chronic ulcers, reducing infection and acting against a wide variety of microorganisms
ESSENTIAL FATTY ACIDS OR MEDIUM CHAIN TRIGLICERIL
Composition: it is a product originating from polyunsaturated vegetable oils, mainly composed of essential fatty acids that are not produced by the body, such as: linoleic acid, caprylic acid, capric acid, vitamin A, E, and soy lecithin
Mechanism of action: promote chemotaxis (attraction of leukocytes) and angiogenesis (formation of new blood vessels), keep the environment moist and accelerate the tissue granulation process
Indication: prevention and treatment of dermatitis, pressure ulcers, venous and neurotrophic; treatment of open ulcers with or without infection.
Note - Essential Fatty Acids may be associated with calcium alginate, activated carbon and other types of coatings
35
A cotton stockinette is worn down to the infra patellar region, taking care to avoid creases Distally the mesh is folded over the fingers and secured with tape Carefully so that there are no wrinkles that could cause secondary lions.

A 1 3 cm layer of foam is pre-molded and cut to avoid creases and overlaps This is used to close the forefoot, if you want to opt for a closed cast A long rectangular piece is applied to the pretibial crest, two circular segments are applied to the malleolus and a platform with an orifice for the ulcerated region is fixed to the plantar region






36
The technician should stand in front of the patient, with the patient sitting with the leg dangling and the knee bent at 90 degrees The cotton is rotated from the tibial tubercle to the forefoot


Cotton stockinette should be applied evenly with thin layers and without wrinkles or accumulation of material From the distal region to the proximal region, from the fingers to 3 cm below the knee.

Cotton should be applied with extra layers on the bony protrusions to avoid friction.

37
Placing plaster bandages from the distal part to the proximal part is started with enough tension for a good fit in the segment and a good impression, paying attention to the 90-degree angle of the ankle joint and the functional position of the fingers The plaster must be molded in every segment so that the contact with the plaster is total
A plaster base is placed in the plantar region to reinforce the support area with the soil. After fixing it, the patient must stand and step with the plaster still wet on the floor so that there is an increase in the contact area of the plaster with the ground, distributing the force evenly and relief in the region of the ulcer where a circular segment was made in the foam




38
The plaster must be molded again along the entire length of the segment, increasing the contact with the entire surface


The TCC allows charging as soon as it is dry, after 48h. Plaster application leads to a significant reduction in edema The patient will have to return in one week to change the first plaster, subsequently it will have to be changed every one to two weeks, depending on factors such as wound size, drainage and edema

Afterwards, it is possible to adapt a specific shoe for insensitive feet that must be extra deep, wide anterior chamber, without internal seams and with an insole molded to the patient's foot
39
IATROGENIC COMPLICATIONS OF FULL CONTACT PLASTER
A frequently changed total contact cast is a safe modality for unloading and immobilizing the neuropathic foot, albeit with an expected steady rate of minor reversible complications. Patients should be informed of these complications and risks prior to plaster application.
Contraindications and complications include infection, poor foot hygiene including elongated toenails, ischemia, non-compliance and claustrophobia
With respect to infection, the dark, humid and warm atmosphere inside this device is an excellent environment for bacterial growth
There are other ways in which offloading should be used until the infection is resolved before applying the TCC Xerotic skin should be treated with emollient lotions to avoid cracking and hyperkeratosis, if present, debrided Circumferences should be avoided in bandages Cut the bandage where reduced blood flow to the foot can occur As Kominsky puts it "It is much more important to be concerned about what is being removed from the ulcer, ie pressure, than what is being put in "
Before applying the plaster, the ulcer must be evaluated for width and depth
Ulcers that are deeper than their width can create a problem as epithelialization can occur before the depth of the wound is properly healed, possibly allowing an abscess to form These ulcers must be uncapped, treated with an open package, and then TCC applied
40
REFERENCES
Steindler A : The tabetic arthropathies JAMA 96: 250-256, 1931
Brodsky J W : "The diabetic foot" In: Mann R A , Coughlin M J : Surgery of the foot and ankle, 7th ed St Louis, Mosby-Year Book, 895-969, 1999
Vilar L , Castellar E , Moura E , et al: "Diabetes mellitus - New classification and diagnostic criteria" In: : Clinical endocrinology Rio de Janeiro, Medsi, 353-362, 1999
Chang B B , Shah D M , Darling III C , Leather R P : Treatment of the diabetic foot from a vascular surgeon's viewpoint Clin Orthop 296: 27-30, 1993
Pinzur M S : Benchmark analysis of diabetic patients with neuropathic (Charcot) foot deformity Foot Ankle Int 20: 564-567, 1999
Horibe S , Tada K , Nagano J : Neuroarthropathy of the foot in leprosy J Bone Joint Surg [Br] 70: 481-485, 1988
Bechelli L M : "Leprosy" In: Veronesi R Infectious and parasitic diseases, 8th ed Rio de Janeiro, Editora Guanabara Koogan, 349-366, 1991
DeFronzo R A , Reasner C : The diabetes control and complications trial study: implications for the diabetic foot J Foot Ankle Surg 33: 551-556, 1994
M S , Edwards W H B : Management of neuropathic fractures in the foot and ankle. J Am Acad Orthop Surg 7: 8-18, 1999.
Eichenholtz S.N.: Charcot Joints. Springfield, IL, Charles C., 1966. Johnson J.T.H.: Neuropathic fractures and joint injuries. J Bone Joint Surg [Am] 49: 1-30, 1967.
Myerson M.S., Papa J., Eaton K., Wilson K.: The total-contact cast for management of neuropathic plantar ulceration of the foot. J Bone Joint Surg [Am] 74:261-269, 1992
Doctor N , Pandya S , Supe A : Hyperbaric oxygen therapy in diabetic foot J Postgrad Med 38: 112-114, 1992
Morgan J M , Biehl III W C , Wagner W : Management of neuropathic arthropathy with the Charcot restraint orthotic walker Clin Orthop 296: 58-63, 1993
Fletcher F , Ain M , Jacobs R : Healing of foot ulcers in immunosuppressed renal transplant patients Clin Orthop 296: 37-42, 1993
Myerson M S , Henderson M R , Saxby T , Short K W : Management of midfoot diabetic neuroarthropathy Foot Ankle Int 15: 233-241, 1994
Slavens E R , Slavens M L : Therapeutic footwear for neuropathic ulcers Foot Ankle Int 16:663-666, 1995
Boninger J M L , Leonard J A : Use of bivalved ankle-foot orthesis in neuropathic foot and ankle lesions J Rehabil 33: 16-22, 1996
41
Schon L.C., Easley M.E., Weinfeld S.B.: Charcot neuroarthropathy of the foot and ankle. Clin Orthop 349: 116-131, 1998.
Hissink R.J., Manning H.A., Van Baal J.G.: The MABAL shoe, an alternative method in contact casting for the treatment of neuropathic diabetic foot ulcers. Foot Ankle Int 21: 320-323, 2000.
Brodsky J.W., Rouse A.M.: Exostectomy for symptomatic bony prominences in diabetic feet Clin Orthop 296: 21-26, 1993
Johnson J : Operative treatment of neuropathic arthropathy of the foot and ankle J Bone Joint Surg [Am] 80: 1700-1709, 1998
Sammarco G J , Conti S F : Surgical treatment of neuroarthropathic foot deformity Foot Ankle Int 19: 102-109, 1998
Kumagai S G , Mahoney C R , Fitzgibbons T C , McMullen S T , Connoly T L , Henkel L : Treatment of diabetic (neuropathic) foot ulcers with two-stage debridement and closure Foot Ankle Int 19: 160-165, 1998
Sticha R S , Franscone S T , Wertheimer S J : Major arthrodesis in patients with neuropathic arthropathy J Foot Ankle Surg 35: 560-566, 1996
Bono J V , Roger D J , Jacobs R L : Surgical arthrodesis of the neuropathic foot Clin Orthop 296: 14-20, 1993
Shibata T , Tada K , Hashizume C : The results of arthrodesis of the ankle for leprotic neuroarthropathy J Bone Joint Surg [Am] 72: 749-756, 1990
Kile T A , Donnelly R E , Gehrke J C , Werner M E , Johnson K A : Tibiocalcaneal arthrodesis with an intramedullary device Foot Ankle Int 15: 669-673, 1994
Moore T J , Prince R , Pochatko D , Smith J W , Fleming S : Retrograde intramedullary nailing for ankle arthrodesis Foot Ankle Int 16: 433-436, 1995
Pinzur M S , Kelikian A : Charcot ankle fusion with a retrograde locked intramedullary nail. Foot Ankle Int 18: 699-704, 1997.
Papa J., Myerson M., Girard P.: Salvage, with arthrodesis, in intractable diabetic neuropathic arthropathy of the foot and ankle. J Bone Joint Surg [Am] 75: 10561066, 1993.
Gruen G.S., Mears D.C.: Arthrodesis of the ankle and subtalar joints. Clin Orthop 268: 15-21, 1991
Alvarez R A , Barbour T M , Perkins T D : Tibiocalcaneal arthrodesis for nonbraceable neuropathic ankle deformity Foot Ankle Int 15: 354-359, 1994
Myerson M S , Alvarez R G , Lam P W C : Tibiotalocalcaneal arthrodesis for the management of severe ankle and hindfoot deformities Foot Ankle Int 21: 643650, 2000
Prokuski J L , Saltzman C L : External fixation for the treatment of Charcot arthropathy of the ankle: a case report Foot Ankle Int 19: 336-341, 1998
Pinzur M S : Amputation level selection in diabetic foot Clin Orthop 296: 68-70, 1993
Pinzur M S , Sage R , Stuck R , Osterman H : Amputations in the diabetic foot and ankle Clin Orthop 296:64-67, 1993
42
Scher K.S., Steele F.J.: The septic foot in patients with diabetes. Surgery 104: 661666, 1988. 2. Helm P.A., Walker S.C., Pullium G.: Total contact casting in diabetic patients with neuropathic foot ulcerations. Arch Phys Med Rehabil 65: 691-693, 1984.
Pinzur M.S., Slovenkai M.P., Trepman E.: Guidelines for diabetic foot care. Foot Ankle Int 20: 695-702, 1999.
Wagner W F : The dysvascular foot: a system for diagnosis and treatment Foot
Ankle 2: 64-122, 1981
Boulton A J , Bowker J H , Gadia M , et al : Use of plaster casts in the management of diabetic neuropathic foot ulcers Diabetes Care 9:149-152, 1986
Walker S C , Helm P A , Pullium G : Total contact casting and chronic diabetic neuropathic foot ulcerations: healing rates by wound location Arch Phys Med Rehabil 68: 217-221, 1987
Myerson M , Papa J , Eaton K , Wilson K : The total-contact cast management of neuropathic plantar ulceration of the foot J Bone Joint Surg [Am] 74:261-269, 1992
Rossi W R : Diabetic foot: approach, classification and treatment Rev Bras Ortop 27: 459-467, 1992
Pinzur M S , Sage R , Stuck R , Osterman H : Amputations in the diabetic foot and ankle Clin Orthop 296:64-67, 1993
Papa J , Myerson M , Girard P : Salvage, with arthrodesis, in intractable diabetic neuropathic arthropathy of the foot and ankle J Bone Joint Surg [Am] 75: 10561066, 1993
Birke J A , Sims D S : Plantar sensory threshold in the ulcerative foot Lepr Rev 57:261-267, 1986
Levin S., Pearsall G., Ruderman R.J.: Von Frey's method of measuring pressure sensitivity in the hand: an engineering analysis of the Weinstein-Semmes pressure aesthesiometer. J Hand Surg [Am] 3:211-216, 1978.
Boyko E.J., Ahroni J.K., Davignon D., et al: Diagnostic utility of the history and physical examination for peripheral vascular disease among patients with diabetes mellitus J Clin Epidemiol 50: 659-668, 1997
Bridges Jr R M , Deitch E A : Diabetic foot infections Surg Clin North Am 74: 537555, 1994
https://repositorio chporto pt/bitstream/10400 16/1742/1/P%C3%A9%20de%20C harcot pdf
https://bvsms saude gov br/bvs/publicacoes/manual feridas final pdf
https://www icorfin com/pt-br/classificacao-wagner-de-ulceras-pe-diabetico/ https://www rbo org br/tais/569/pt-BR/pe-diabetico--tratamento-das-ulcerasplantares-com-gesso-de-contato-total-e-analise-dos-fatores -interfering-withhealing-time
43
PAULISTA ASSOCIATION OF HOSPITAL INFECTION STUDIES AND CONTROL (APECIH). Precautions and Isolations. São Paulo, 52p. 1999.
AZEVEDO, A. et al. Rules for performing dressings. Federal University of Minas Gerais. 2000.
http://www.angelfire.com/ma/pliniomaia/bandages.html BAJAY, H.M. et al. Wound care manual. Campinas State University. Clinical Hospital. Wound Study
Group 1999 79p BAJAY, H M
Recording the evolution of wounds: elaboration and applicability of an instrument Campinas, 2001 110p (Dissertation – Master – FCM Nursing
Department – UNICAMP)
BRAND, PW External stress on joint motion In: Converse testbook of plastic surgery, The hand and upper extremity Vols 7 and 8, chap 10, May J , Litter, K W J , W B Sanders, Phila, PA, 1985 BRAND, P W Clinical mechanics of the hand: C C Mosbry Co , St Louis, Chap 6, 1985 BATES-JANSEN, B M
Management of exudate and infection In: SUSMAN, C; BATESJANSEN, BM Wound care: A collaborative practice manual for physical therapy and nurses
An Aspen Publication Gaithrsburg, Maryland, 1998 p 159-77 BRAZIL
Ministry of Health National Health Foundation Leprosy Control Guide Brasilia
1994 156p BRAZIL
Ministry of Health National Health Foundation Participatory action: working with leprosy Health Education, Brasília, 1994 32p BRAZIL
Ministry of Health Department of Health Assistance Department of Assistance and Health Promotion Hospital Infection Control Coordination
Processing of articles and surfaces in healthcare facilities Brasilia 2nd ed ,
1994 49p BRAZIL
Ministry of Health. National Health Foundation. Manual for the prevention of disabilities, Brasília, 1997. 125p. 53 Management of Neurotrophic and Traumatic Ulcers
Leprosy Rehabilitation Manual BRAZIL. Ministry of Health. Health Policy Secretariat. Department of Primary Care. Technical Area of Sanitary Dermatology
Disability Prevention Handbook Brasília, 2001 107p CARNEIRO, M ; PROCHNOU, A G ; MAZZORANI, B M
Dressings what to use? Rio Grande do Sul, Convatec, 1998 37p COSTA, A A ;
ALMEIDA NETO, T S
Diabetes Manual: food, medication, exercise São Paulo, 3rd ed , 1998 DAVIS, M H et al
The herida program Center for Medical Education of the University of Dundee, Scottland, 1995 187p DEALEY, C translated by LACERDA, R A
Caring for Wounds: A Guide for Nurses São Paulo, Atheneu, 1996 256p
EAGLSTEIN, W H et al Wound care: an emerging discipline In Wound care manual: new directions in wound healing New Jersey; E R Squiss & Sons 1990 99p FERREIRA, A B H
44
New Aurélio Dictionary of the Portuguese Language 2nd ed Rio de Janeiro New Frontier 1986 FLANAGAN, M
A practical framework for wound determination 2: method Nursing Portuguese No. 117. Dec. 1997, year 10. LAX, I.P.; ALVAREZ, S.G; GRUN, D.
Wounds and their care 1st ed São Paulo Department of Educational Services
1992 MENEGHIN, P ; SOARES, L
Advances in dressings In: FERNANDES, AT
Nosocomial infection and its interfaces in the health area St Paul, Atheneu, ch 53, p. 998-1007. 2000. POLETTI, N.A.A.
Nursing care for patients with chronic wounds
The search for evidence for practice Ribeirão Preto, 2000 269 p Dissertation (Masters) at Ribeirão Preto College of Nursing University of Sao Paulo SAMPAIO, S A P ; RAYMUNDO M ; RIVITTI, E.A. Skin anatomy and physiology. Basic Dermatology. Porto Alegre. Medical Arts, 3rd ed , 1989 p 1-21 SANTOS, V L C G
Technological advances in wound care and some home applications In: DUARTE, Y A O ; DIOGO, M J D
Home care: a gerontological approach São Paulo, Atheneu, 2000, cap 21, p 265–
305. SÃO PAULO STATE SECRETARY OF HEALTH. Coordination of Research Institutes – CIP “Professor Alexandre Vranjac” Epidemiological Surveillance Center
Chronic non-communicable diseases and control of their risk factors São Paulo, 1997 SECRETARIAT OF STATE OF HEALTH OF MINAS GERAIS Operational Health Superintendence. Department of Primary Care. Technical Area of Sanitary Dermatology
A new vision in wound care Belo Horizonte, Minas Gerais, 2000 SINACORE, D R ; MUELLER,M J
Total-Contact Casting in the treatment of neuropathic Ulcers in: LEVIN; NEALS, O’ The Diabetic Foot 6th Edition Mosby A Harcout Health Sciences Co 2001 54
Booklet in 2 Leprosy Rehabilitation Manual TURNER, T D The development of wound management products In: KRASNER, D & KANE, D
Chronic wound care: a clinical source book for healthcare professionals 2nd ed Wayne, Health Management Publications, 1997. p.124-38. VAN RISWIJK L. Wound
assessment and documentation In: KRASNER, D ; KANE, D
Chromic wound care: a clinical source book for healthcare professionals Health Management Publications, Inc 2nd ed Wayne, 1997 VIEIRA, C S C A ; AGUIAR, C A ;
SAMPAIO, P
Update on Dressings. In: Semiology and Semiotechnics handout University of Taubate Department of Nursing 2001 /mimiographed/
YAMADA, H Strength of biological materials EVANS, F F , ed Baltimore, Williams and Wilkins, Co., p.225, 1970. WINTER, G.D.
Formation of scab and rate of epithelization of superficial wounds in the skin of domestic pig Nature, 193: 293-4, 1962
45