19 minute read
Tamara Berg, DDS

ODA PAST PRESIDENT SPOTLIGHT
Tamara Berg, DDS (2010 to 2011)
By Makenzie Dean, ODA Programs and Operations Manager
If you are a member of the dental community, Dr. Tamara Berg is probably a name that you recognize. She served as President of the Oklahoma Dental Association from 2010 to 2011 but has been involved in countless councils and committees ever since she was a dental student at the OU College of Dentistry. Berg discovered early on that she wanted to pursue a career where she could help others and change their smiles. She started her own orthodontic treatment at the age of 13 and did not like her smile at the time. Correcting her smile helped her discover her desire to be in dentistry and blossomed her own self-confidence.
Though Berg is originally from Austin, TX, she crossed the Red River to attend Southern Nazarene University in 1987 and later chose to attend the University of Oklahoma’s College of Dentistry where she graduated in 1995. After she did an associateship for a few years, she purchased a practice in Yukon, OK in 1998 and remains there to this day. Dr. Berg and her husband, Lowell, celebrate their 30-year anniversary this June. They first met at Southern Nazarene University and were married just before she started dental school. Together they have two sons – Karsten and Clayton. Karsten plays Division II basketball at SNU, the school where his parents met, and Clayton is a sophomore in high school and a state qualifier in swimming. Berg notes that she has always had a passion for organized dentistry. She took steps in leadership that prepared her to be the ODA President from 2010 to 2011. She was active in as many councils and committees that she could be in since dental school. She served as the President of the Oklahoma Association of Women Dentists twice, in 1998 and in 2006, and as the President of the Oklahoma County Dental Society from 2003 to 2004. More recently, she served as the National President of the American Association of Women Dentists in 2018.
Berg most enjoyed the chance to represent our state and Oklahoma dentists at national events during her presidential term. It was there that she was able to meet people from around the nation and gained rewarding friendships. With the many opportunities that come with the title of ODA President, there also come some challenges. That same year, the ODA fought a denturist bill during the Legislative session and hosted an OkMOM during a snowstorm that kept a third of the
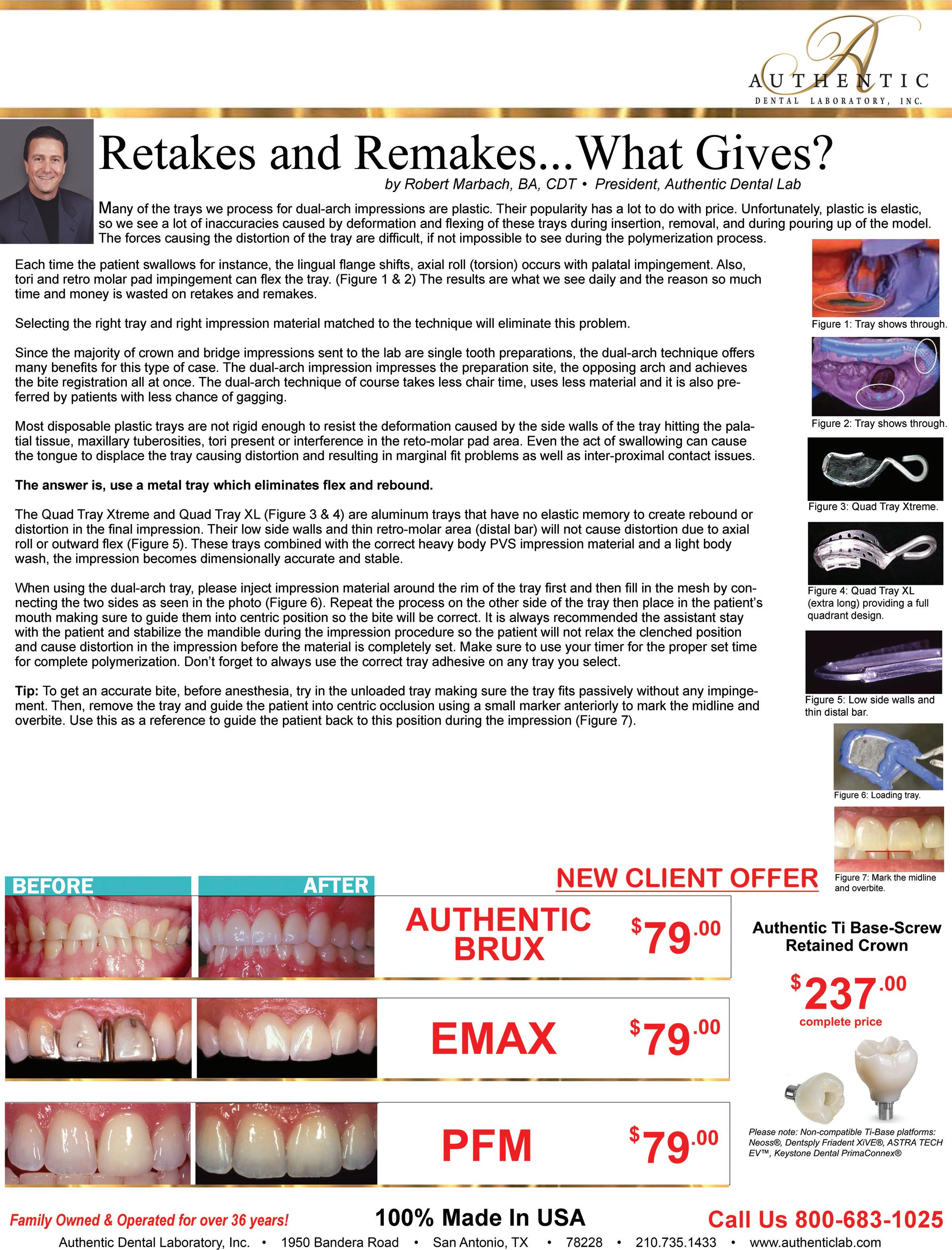
Dr. Tamara Berg with family.
FUN FACTS:
• What is one thing that most people do not know about you? Our family has gone plant based and we no longer eat meat or dairy.
• If you could have dinner with one famous person, who would it be and why? I would love to have a faceto-face conversation with Jesus. I would ask about things along my journey but would also want to know why we have mosquitos.
• What hobbies do you enjoy? I enjoy gardening, scrapbooking and reading.
volunteers from attending. Under Berg’s leadership, that denturist bill did not pass, and they were still able to serve 2,201 patients at OkMOM even with a shortage of volunteers. During her term, Berg learned to rely on others to support her and now knows that you cannot get it all done so you must surround yourself with others who will join you in your goals. She believes that the greatest benefit of the ODA is the voice that we share. One individual dentist may not be able to make a change by themselves but collectively, we can do more legislatively, in community service projects and supporting one another to better our patients, our state and our future dentists. Her advice to anyone who is interested in becoming President of the ODA would be to get involved in your local dental society and at the state level, volunteer to serve on a council or committee, network with the other leaders and find out more about the organization. Dr. Berg has remained a key player in enhancing the profession of dentistry. She is currently serving as an ADA Delegate for Oklahoma, was recently appointed to the ODA Investment Committee and on the DENPAC Board and is also on her third year of serving on the ADA’s Council on Membership.



Dr. Berg with Dr. Rieger Wood at her installation The 2011-2012 ODA Officers Dr. Berg with her two sons
8 Million and Counting





17% of people who visit ADA Find-a-Dentist® take the next step to contact an ADA member. That’s more than 5x the industry average, so don’t miss out!
ADA.org/completemyprofile





DIFFERENTIAL DIAGNOSIS:
RED AND WHITE LESION INVOLVING THE BUCCAL MUCOSA
By: Glen D. Houston, DDS, MSD (gdhdds@heartlandpath.com)
CASE HISTORY
A 42-year-old female presents for an oral cancer screening examination during a health care fair. During the examination, a red-and-white lesion on the buccal mucosa was observed. Other similar lesions were also noted. The patient was unaware of their presence and no reliable estimate of their duration could be determined. Medical history revealed a 30-pack/year history of cigarette smoking and heavy alcohol consumption.
QUESTION #1
A working differential diagnosis for this condition should include (multiple answers): a. Lichen planus b. Candidiasis c. Allergic response d. Epithelial dysplasia/squamous cell carcinoma
e. Factitial injury
ANSWER #1
Your differential diagnosis should include all of the conditions noted in Question #1. Lichen planus (a) is of particular interest because involvement of the oral mucosa frequently accompanies or precedes the appearance of lesions on the skin. Early in the course of this disease lesions may appear red to reddish-white in color. The majority of the cases occur in women and the buccal mucosa is the most common intraoral location.
Candidiasis (b) is a disease caused by infection with the yeast-like fungus Candida albicans. Its occurrence has increased because of the prevalent use of antibiotics, which alter the normal inhibitory oral bacterial flora. The oral lesions of candidiasis may exhibit many different forms, one of which is red or erythematous areas in association with white plaques. An allergic response (c) following exposure to any one of a great many drugs or chemicals (systemically or at localized sites after repeated contact with the causative agent) can be observed in the sensitive individual. Oral lesions usually appear as erythematous lesions that can occur throughout the oral cavity or at the area of contact with the causative agent. Epithelial dysplasia and/or squamous cell carcinoma (d) may present as areas of erythroplakia and/or leukoplakia. These areas may be quite variable in size and are more common in men than women. These areas typically are observed in adults and are asymptomatic. The factitial injury (e) is a self-induced injury on the basis of a habit with a frequent psychogenic background. The injury originates as a result of such habits as cheek chewing, lip biting, and unconscious mucosal trauma. The clinical appearance of the mucosa at the site of the injury will usually present as a mixed red-white area.
QUESTION #2
Your treatment plan should include (multiple answers): a. Oral cytologic smear b. Biopsy of the lesion c. Consultation with a dermatologist for clinical examination of all skin surfaces d. Follow the patient for 10-14 days after cessation of cigarette and alcohol habits in order to evaluate for any changes in the lesions e. Advise the patient of the "hyperkeratotic areas" and that no treatment is necessary
ANSWER #2
Your treatment plan should include: a. Oral cytologic smear b. Biopsy of the lesion c. Consultation with a dermatologist for clinical examination of all skin surfaces d. Follow the patient for 10-14 days after cessation of cigarette and alcohol habits in order to evaluate for any changes in the lesions
The oral cytologic smear (a) can be very helpful in detecting fungal elements as well as epithelial dysplasia. Following the patient for 10-14 days after cessation of the cigarette and alcohol habits (d) will be helpful. If the lesions are reactive/inflammatory, resolution will be observed. If there is no resolution, then biopsy of the lesion (b) is indicated. Consultation with a dermatologist for evaluation of the cutaneous surfaces (c) for the presence of lesions is also of benefit in patients that have lichen planus or other systemic diseases. Ultimately, a biopsy of the lesion (b) may be indicated in order to render a definitive diagnosis. To advise the patient that the lesion is a "hyperkeratotic area" and that no treatment is necessary (e) is of no benefit in the management of this patient.

QUESTION #3
An oral cytologic smear is performed and is negative for the presence of fungal hyphae and epithelial dysplasia. A biopsy reveals hyperkeratosis, "sawtooth" rete ridges, liquefaction degeneration of the basal cell layer of the surface epithelium, and a bandlike infiltrate of lymphocytes subjacent to the surface epithelium within the superficial lamina propria. These findings are diagnostic of: a. Allergic reaction b. Factitial injury c. Lichen planus d. Leukoplakia e. White sponge nevus
ANSWER #3
The correct diagnosis is (c) lichen planus. See "Discussion" section.
The other possibilities are not considered here because:
The allergic reaction (a) may manifest some of the histologic features of lichen planus. However, because signs and symptoms for allergic reactions usually regress with discontinuance of the causative agent (local and/or systemic), when this is accomplished there is usually prompt remission of all lesions.
The factitial injury (b) usually demonstrates reactive changes microscopically (i.e., hyperkeratosis, ulcer, chronic inflammation) and can be easily distinguished from lichen planus. Leukoplakia (d) is a clinical term that describes a "white patch or plaque that White sponge nevus (e) demonstrates specific histologic criteria that can easily distinguish it from lichen planus. The features of white sponge nevus are not observed in the present case.
DISCUSSION
A British physician, Erasmus Wilson, first reported lichen planus in 1869. It is a dermatologic condition frequently demonstrating manifestations in the oral cavity. Current evidence indicates that it is an immunologically mediated mucocutaneous disorder.
This condition is most frequently observed in females between 40 and 70 years of age. The following distribution of oral lesions has been observed: buccal mucosa, 80%; tongue, 65%; lips, 20%; palate, floor of the mouth, and gingiva, less than 10%. Lichen planus can present in many different forms from a clinical standpoint. The most common presentation is characterized by a papular eruption in a linear, annular, or retiform arrangement forming typical lacy patches, rings, and streaks known as Wickham's striae (as observed in this current case). Other forms include atrophic erosive, vesiculo-bullous, and hypertrophic types. Over 40% of the patients with oral manifestations of lichen planus will have skin lesions as well. Conversely, over 80% of the patients with dermal lichen planus have associated oral lesions of the disease. Lichen planus is frequently symmetrical and bilateral in its presentation in the oral cavity as well as on skin surfaces. When it presents with cutaneous lesions, the areas of involvement exhibit a red or violet hue and a pruritic nature. The flexor surfaces of the extremities are favored sites for development of the cutaneous lesions. The microscopic appearance of lichen planus is characteristic and pathognomonic. Typical findings, as noted earlier, include hyperkeratosis, "sawtooth" rete pegs, degeneration of the basal cell layer of the surface epithelium, and a "band-like" infiltrate of lymphocytes in the subjacent connective tissue.
There is no specific treatment for lichen planus as it is typically asymptomatic. In severe cases where there is ulceration and episodic pain, topical or systemic steroid therapy, which was the situation in this particular case, is helpful in producing remission. The simultaneous occurrence of squamous cell carcinoma and lichen planus remains an open question. Periodic followup examinations, particularly with the erosive form, should be accomplished. About the Author: Dr. Houston works at Heartland Pathology Consultants, PC in Edmond, OK. He can be contacted with questions at gdhdds@ heartlandpath.com
REFERENCES Au J, Patel D and Campbell JH. Oral lichen planus. Oral Maxillofacial Surg Clin N Am, 25:93-100, 2013.
Usatine RP and Tinitigan M. Diagnosis and treatment of lichen planus. Am Fam Physician. 84:53-60, 2011.
Eisenberg E. Oral lichen planus: a benign lesion. J Oral Maxillofac Surg, 58:1278-1285, 2000.
Collect What You Produce: 10 WAYS TO INCREASE YOUR PRODUCTION THROUGH “IMPROVEMENT”
By: Cathy Jameson, PhD | Part 10 of a ten-part series
No matter how well you are currently doing or how much you are producing, there is always room for improvement. Continuously refining multiple areas or systems in your practice can add up to make a substantial difference. In an article for Forbes Magazine, Anna Powers (Marketing Associate & Manager, CRM) talks about the mathematical principle of exponents: If you do something continuously the effect is multiplied exponentially. The key point is that in order to have a big effect the task must be done continuously. The same can be said about improvement. If you want to see big results, you need to do things continuously. Management expert W. Edwards Deming always encouraged people and businesses to be on a continuous path of improvement. Recognize and solidify what is working well. But also be committed to identifying areas that can be improved—and go to work to do just that.
10 SYSTEMS TO REFINE FOR CONTINUOUS IMPROVEMENT
1. Get a clear picture of where you are. Do a complete analysis of the major systems and critical factors of your practice. (Contact Jameson
Management [info@jmsn.com] to receive the list of the 25 major systems in a dental practice.) As a team determine what is going well and what can be done to make the system better.
In his book The Tipping Point Canadian journalist and author Malcolm
Gladwell says that it’s the little things that make the big difference.” When you make even small adjustments to each system, the summation of those improvements can add up to make a substantial and positive difference in your overall practice. 2. Write goals and follow a specific process of goal accomplishment.
Organizations that write goals and take steps to accomplish them will see a minimum of a 10% increase in productivity. Revisit Part #2 of this Collect What You Produce series wherein a specific system for goal accomplishment is outlined. Self-help author Napoleon Hill, in his book
Think and Grow Rich, encourages creating a definite plan for carrying out your desires and beginning at once, whether you are ready or not, to put this plan into action. 3. Evaluate your hygiene retention percentage and strive to increase it by 5-10%. Add additional measures of contact/education for your patients to stimulate their interest in booking for hygiene. Make sure that all members of the family are coming in; use patient financing to help offset the fear of cost.
Educate your patients to the fact that there has never been a more important time for people to be taking care of their oral health than during this
COVID-19 pandemic.
In the October 2020 issue of RDH
Magazine, Karen Davis, founder of Cutting Edge Concepts, an international continuing education company, wrote, “Individuals with preexisting conditions, including periodontal disease, may be at increased risk of developing superinfections should they acquire the SARS-CoV-2 virus. Emerging evidence suggests that particular periodontal pathogens may contribute to an overabundance of pathogens circulating systemically in those with severe COVID-19 infections, contributing to a superinfection and subsequent serious outcome. While more scientific evidence is needed, it does remind us that optimal oral hygiene and maintaining routine preventive dental care have never been more important.” 4. Use photography even more than you are now. For an enhancement of your
Patient Education, develop a library of before and after photography and use it constantly. The following eight instances of using photography during patient appointments can result in an average increase in case acceptance of 25%.
• New patients A full series of photographs should be a part of the gathering of data on each new patient. • Case presentations Show the patient both their own mouth and before/after photographs of similar situations so they can see the excellent results you have been able to provide. • Hygiene Show areas of need (such as periodontal concerns), sites where new issues are evident, or dentistry diagnosed but incomplete that you as the dental hygienist want to bring to the doctor’s attention.
• Diagnosed but incomplete dental/ hygiene needs. • Before/after photographs to illustrate what you are recommending (cosmetics, implants, tooth whitening, comprehensive restorative,
Invisalign, etc.).
• Emergencies. • Backup for insurance. • Marketing/Social Media. 5. Use patient financing as often as necessary. (Refer to Part 4 of this
Collect What You Produce series.) As an illustration: If one more patient per week uses patient financing than last year production can increase $24,000 ($500 x 48 wks).
to Carlson Marketing and Forbes,
Inc., a 5% increase in case acceptance will lead to a 65% increase in profit margin. While increasing the number of new patients is critical to your practice, retaining your existing patient family and having more of those patients proceed with diagnosed treatment is equally important. In addition, satisfied existing patients are your major source of new patients; marketing experts indicate that approximately 70% of new patients will come from a personal referral. 7. Study non-surgical periodontal therapy.
Attend an available course or invite an expert into your office for in-service training. Set a goal of having 4050% of your hygiene productivity be periodontal services, and consider how you can upgrade the services you are providing in your hygienic therapy. 8. Add three new customer service entities to your mix. There are many great dental practices out there, many of them in your own community.
While providing excellent dental care is essential, this is not usually what patients refer to when someone asks them about their dentist. More than likely, they speak about their total experience and how they were treated not only by the dentist but by the entire team. Never before has customer service been more important to your patients and to your practice. Business experts in the field of customer service have identified the three most vital aspects of customer service in today’s competitive world:
A. Good, Positive Attitude and Mindset
A sincere desire to help patients to fulfill their needs is critical -- even if the patient is not easy. This takes a positive attitude. Practices that make customer service training a priority and invest both the time and money to support their team’s continuous improvement in this area are rewarded with reciprocal success. When you recognize and reward team members for outstanding customer service, that kind of quality care continues.
Key team member attitudes that can prove to be valuable include: a. Sincerely caring about patients; b. Understanding that patients are critical to the success of the practice; c. Feeling accountable and motivated to provide excellent care to each patient; d. Being role models of excellent customer service; and
e. Being empowered to do what they see as beneficial to provide outstanding customer service to any individual
B. Excellent Communication Outstanding customer service starts by honoring excellent and healthy communication with team members, vendors, and patients. Communication does not only refer to face-to-face interactions you have when a patient or parent is in the office with you. It also refers to every encounter on the telephone, or through your social media, website, newsletter, email, etc.
Sixty percent of a message being sent or received is body language. Approximately 30% is tone of voice. That leaves about 10% to the words themselves. Words are critical; depending on how you say something, the response can be positive or negative. The important point here is that with communication devices today (text, email, etc.) there is no body language or tone of voice. Your words are critical and must be chosen carefully. Perhaps the most important communication skill of all is the art of listening. You may not agree with a patient, but your willingness to listen to them will go a long way in building or maintaining a positive relationship with them. Patients have their own points of view that may differ from yours. Nevertheless, they have value. When you listen carefully and with empathy to your patients, oftentimes intense emotions are reduced.
No one is born knowing how to communicate excellently. These are skills that must be learned. Such skills take lots of training and practice. C. Teamwork Great customer service starts -- and ends -- with communication among your own team members. If they are not communicating well with one another, treating one another with respect or speaking to one another with grace and congeniality, then no matter what you try to portray to patients, it will be false and your patients will know it. If your team cannot honestly show respect to one another, it will be difficult to show respect to patients. The negative energy in the office will be very evident.
Outstanding customer service begins and ends with strong, open, honest, caring relationships between and among the members of your team.
The team depends upon one another to do what each is supposed to do, when they are supposed to do it, and how they are supposed to do it. That is accountability. Without accountability, nothing happens. 9. Add three new marketing protocols to your mix. No matter how much marketing you feel you are doing at this time, it may not be enough. Marketing experts say that you should never stop marketing. Just when you think everyone knows who you are and what you do, you can fall off the map and someone else comes to the forefront -- new doctors, new practices, new materials, new procedures.
Refer back to the article in this series on Vision. Determine the vision for your ideal practice and then design a plan of action for how you intend to bring that vision to reality. It can be devastating to get to the end of a day, week, month, year, a career, or a lifetime -- and look back with regret wishing you had done something you didn’t. Let the world know who you are, what you do, and why coming to you is a good idea. 10. Increase your treatment mix. The ADA defines Dentistry as “the evaluation, diagnosis, prevention and/or treatment (nonsurgical, surgical or related procedures) of diseases, disorders and/or conditions of the oral cavity, maxillofacial area and/or the adjacent