CONTINUING EDUCATION
The use of Kilroy Springs in the disimpaction of upper canines Dr. Maurizio Cannata explores the use of the Kilroy Spring to facilitate management of a challenging dentition Abstract Upper canine disimpaction is always a difficult task for general dentists or orthodontists. Here, by analyzing a clinical case, we aim to describe an approach that could facilitate its management by using a particular device: the Kilroy Spring.
Introduction Upper canine disimpaction represents a difficult task and a challenge in everyday practice. The principal task with affected young patients is to formulate an early diagnosis. This is done in two ways: First, by the evaluation of the angulation of maxillary canines since tilted canines can predict a difficult or impossible eruption, particularly if associated with a lack of space. Second, a family history of canine inclusion can also be an indication. If parents or family members have had canine impactions, a prediction of canine impaction is likely. So, when we’re confronted with a young patient with such features, we should try our best to allow a possible spontaneous eruption of maxillary canines. The first thing to do then is to confirm a palatal or buccal position of the canines. (A CBCT scan is now the gold standard.) The second is to make space for eruption. This can be done by expanding the palate in cases of transversal contraction. Soon after this phase, or if there is an eruptive problem, the clinician should apply an orthodontic fixed appliance and create space for the maxillary canine, and remove the primary maxillary canines. Sometimes, fortunately, the permanent canines will spontaneously
Maurizio Cannata, DDS, received his degree in 1990 at the Sapienza University of Rome. He is a private practitioner in his own dental office in Rende, Italy. He is a member of the National Italian Association of Dentists (ANDI) and of the Italian Society of Osseointegration (SIO). He is one among the main animators of Italian Implant Dentistry forum Osteocom. He studied periodontology and implant dentistry with Drs. Stefano Parma Benfenati and Carlo Tinti, Fixed Prosthesis with Drs. Fabio Bertagnolli and Domenico Massironi, and orthodontics with Dr. Davide Mirabella. Dr. Cannata is a lecturer in periodontology, implant dentistry, and orthodontics. Dr. Cannata can be emailed at mauricannata@gmail.com.
46 Orthodontic practice
Educational aims and objectives
This article aims to describe an approach to upper canine disimpaction using the Kilroy Spring.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions on page 50 to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can: • Identify how to make an early diagnosis of impacted maxillary canines. • Realize how to facilitate a spontaneous eruption of borderline canines. • Recognize how to create space for impacted canines. • Identify how to correctly use Kilroy Springs. • Realize how to finish treatment after Kilroy Springs achieve their purpose.
Figure 1
Figure 2
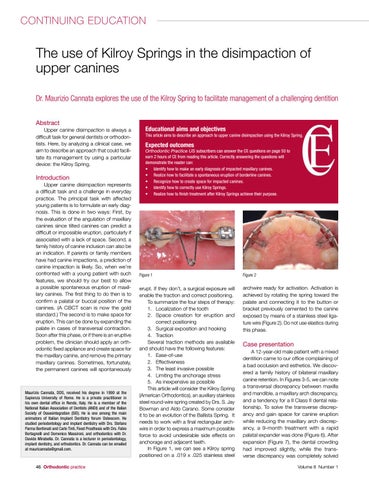
erupt. If they don’t, a surgical exposure will enable the traction and correct positioning. To summarize the four steps of therapy: 1. Localization of the tooth 2. Space creation for eruption and correct positioning 3. Surgical exposition and hooking 4. Traction Several traction methods are available and should have the following features: 1. Ease-of-use 2. Effectiveness 3. The least invasive possible 4. Limiting the anchorage stress 5. As inexpensive as possible This article will consider the Kilroy Spring (American Orthodontics), an auxiliary stainless steel round-wire spring created by Drs. S. Jay Bowman and Aldo Carano. Some consider it to be an evolution of the Ballista Spring. It needs to work with a final rectangular archwire in order to express a maximum possible force to avoid undesirable side effects on anchorage and adjacent teeth. In Figure 1, we can see a Kilroy spring positioned on a .019 x .025 stainless steel
archwire ready for activation. Activation is achieved by rotating the spring toward the palate and connecting it to the button or bracket previously cemented to the canine exposed by means of a stainless steel ligature wire (Figure 2). Do not use elastics during this phase.
Case presentation A 12-year-old male patient with a mixed dentition came to our office complaining of a bad occlusion and esthetics. We discovered a family history of bilateral maxillary canine retention. In Figures 3-5, we can note a transversal discrepancy between maxilla and mandible, a maxillary arch discrepancy, and a tendency for a II Class II dental relationship. To solve the transverse discrepancy and gain space for canine eruption while reducing the maxillary arch discrepancy, a 9-month treatment with a rapid palatal expander was done (Figure 6). After expansion (Figure 7), the dental crowding had improved slightly, while the transverse discrepancy was completely solved Volume 8 Number 1