4 minute read
Congenital Heart Surgery: Emma's Story


Emma was born in 2010 with hypoplastic left heart syndrome (HLHS), a serious heart defect in which the left side of the heart fails to properly develop. The standard treatment includes three open-heart surgeries — typically around 2 weeks, 6 months and 2 years of age. After her second surgery, Emma developed heart failure, which occurs in about 10% of all cases. When she was 9 months old, Emma was placed on the heart transplant list.
Despite this, life began to stabilize for Emma and she was discharged from the hospital. But things took a serious turn almost two years later. While Emma was undergoing a cardiac catheterization to evaluate her for the third and final HLHS surgery, Michael Mitchell, MD, discovered that the arteries and veins in her groin had collapsed. 10-20% of heart transplants will fail due to rejection. In the first year following the transplant, patients are tested for rejection up to a dozen times. After that, they must undergo regular surveillance biopsies for the rest of their lives. Without vascular access to her heart, doctors would not be able to perform the necessary biopsies to test for organ rejection when Emma ultimately received a transplant. That also meant she was a high-risk candidate and her transplant was unlikely to be approved.
Dr. Mitchell refused to accept that, and thanks to a groundbreaking blood test developed by Dr. Mitchell and Aoy Tomita-Mitchell, PhD, he won’t have to. The idea for this test arose half a decade earlier, when Dr. Mitchell and Dr. Tomita-Mitchell developed a non-invasive, DNA-based blood test that could diagnose Down syndrome in utero. It proved successful and they believed the same principles could be applied to donor rejection.
“In the test for Down syndrome, we were able to quantify fragments of fetal DNA present in the mother’s blood,” said Dr. Tomita-Mitchell. “Mike hypothesized that, similarly, fragments of donor DNA might be present in a transplant recipient’s blood and, if so, that might help us determine if rejection was taking place or not. Mike and his colleagues applied for a grant from the National Institute of Health and we are now conducting a multi-site clinical study.”
The new test starts with a simple blood draw. The sample is shipped overnight to the TAI Diagnostics lab in Wauwatosa. A robot extracts the DNA from the sample and separates the donor DNA from the recipient’s DNA. The test looks for how much donor DNA is present in the patient’s blood — a high level of donor DNA indicates rejection. “We have fragments of DNA that circulate in our blood,” said Dr. Mitchell. “If you’ve had a transplant, a fraction of the DNA comes from the donor organ, and this fraction increases with injury to the donor organ.” In addition to being faster, cheaper and less invasive than a physical biopsy, testing for DNA levels is more accurate and can lead to earlier detection.
Fortunately, Emma has not yet needed the blood test. After making incredible progress these past few years, she was officially taken off the transplant list in November 2017. But her mother knows that it’s likely a matter of when, not if. And knowing that this test now exists gives her great peace of mind.

Emma holding a penguin cookie.
“Nothing has been easy, and Emma has overcome so much to get where she is today. This test definitely takes away one of the biggest risk factors against her having a transplant,” said her mother. “I think that Emma inspired the test is wonderful. I’ve always felt that she has a purpose.”
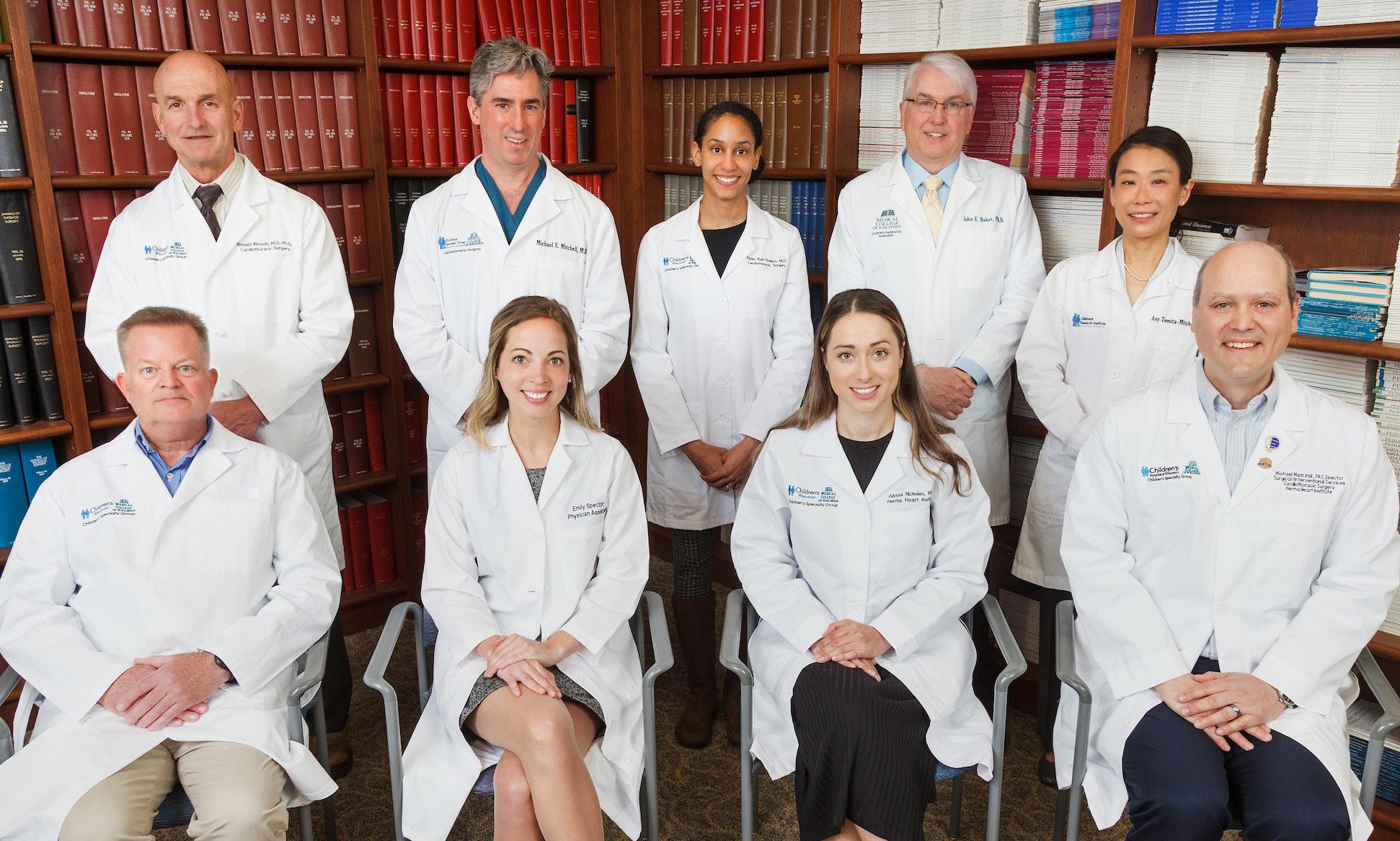
Division of Congenital Heart Surgery Faculty and APPs. Back row: Drs. Ronald Wood, Michael Mitchell, Elyan Ruiz Solano, John Baker, Aoy Tomita-Mitchell. Front row: APPs L. Eliot May, Emily Spector, Alyssa Nicholas, Michael Madrzak. (Not pictured: Drs. Tracy Geoffrion and Viktor Hraska).