
3 minute read
Vascular & Endovascular Surgery: Richard’s Story

When Richard Sobralski was told that he had an enlarging abdominal aortic aneurysm which was going to be very difficult to repair, had a high risk of rupture which could end his life, and fraught with complications, he was referred to Peter Rossi, MD, with the MCW Division of Vascular & Endovascular Surgery to receive a second opinion and second chance at life.
An abdominal aortic aneurysm, or AAA, is a bulge in the wall of the artery below your heart, called the aorta, which is the body’s largest artery. The bulge is caused by a weak section in the artery wall and is at risk of tearing which can result in death. On top of having a AAA, Rich also unfortunately had a large right groin aneurysm. Rich was pleased to hear when Dr. Rossi told him, “I can fix these for you.”
Rich is no stranger to vascular surgery. He had previous operations years ago at an outside institution including bilateral leg femoral-popliteal bypasses which were nearly blocked. This caused him pain when walking, along with numbness and pain in his feet at night. The first procedure that Dr. Rossi performed on Rich was a lower extremity angiogram, to save his leg from needing an amputation. “I was amazed when I walked out the hospital the next day to the parking lot without any pain at all. I can’t remember the last time I felt no pain in my legs, I was amazed and so pleased with the outcome,” Rich recalls.
Months later, Dr. Rossi performed the second, larger surgery on Rich’s AAA and femoral aneurysm. Rich remembers the day well, “ He did it the day before my birthday, February 11th, I’ll never forget.” An endovascular aneurysm repair (EVAR), is a minimally invasive method to treat an aortic aneurysm. The alternative is an open repair where the patient’s chest and abdomen are surgically opened. The endovascular repair reduces recovery time to a few days, and leaves only two small groin incisions. The surgeon inserts guidewires and catheters into these incisions, and using radiographic imaging, will locate the aneurysm and insert a stent graft to repair the aorta. Compared with open AAA repair, EVAR is associated with a significant reduction in perioperative mortality, shorter procedure time, less discomfort during recovery, and quicker return to daily activities. Rich was at Froedtert Hospital for his recovery for only five days before he returned home with his family.
Rich, who at 82 is now living an active lifestyle, is fully recovered, pain free, and is looking forward to returning to golfing several times a week, fishing with his sons, and keeping up with the yard work. Rich states that after surgery, “They did a great job managing my pain, I barely had any. Whoever is doing the training in manners is doing a pretty great job also. Everyone was just so wonderful to me. I’m very lucky to have met Dr. Rossi and his team and I would strongly recommend everyone to go there.”

Richard Sobralski.

Drs. Gary Seabrook and Kellie Brown in the OR.
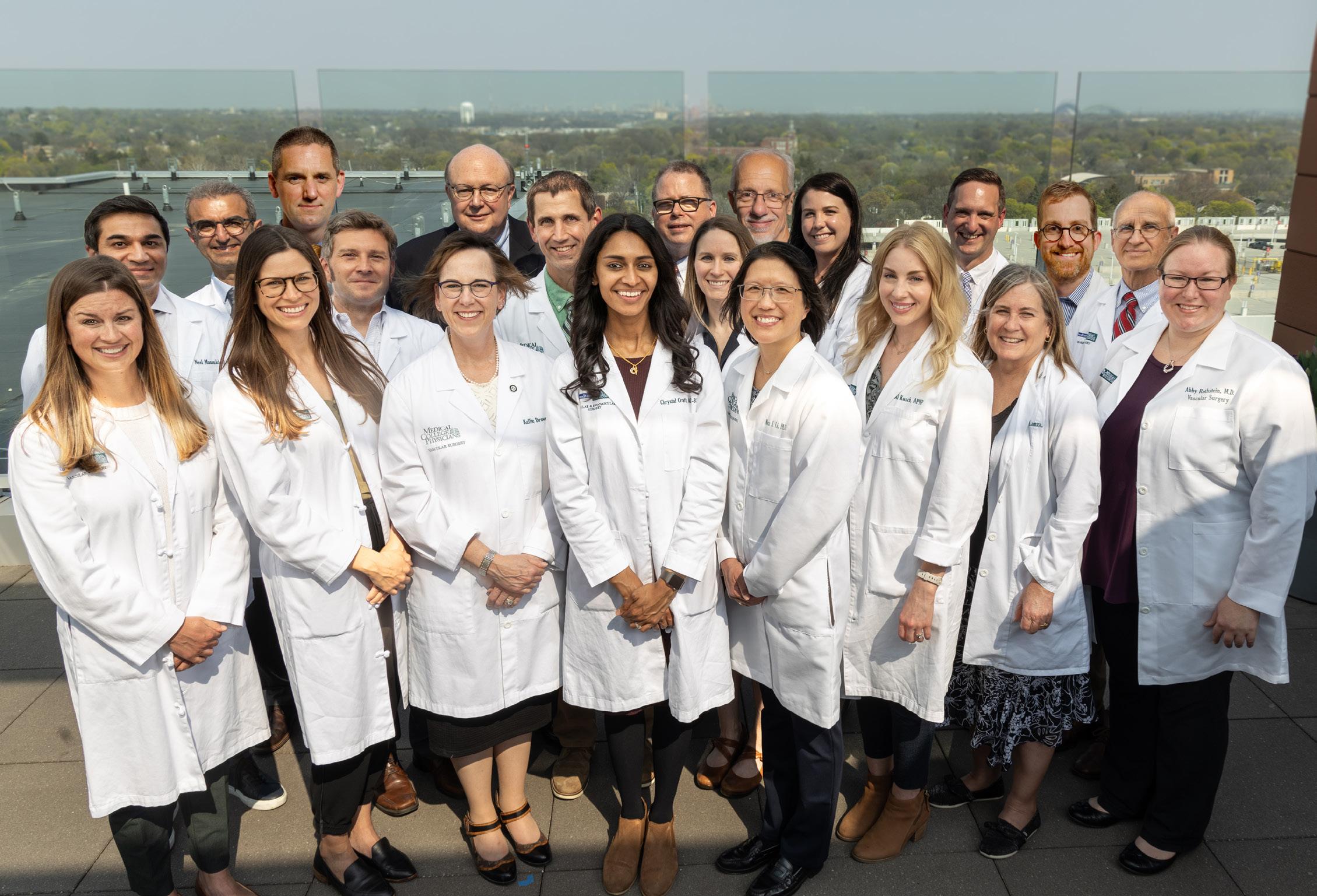
Division of Vascular & Endovascular Surgery Faculty & APPs. (Not pictured: Dr. Dyer.)







