SOLID TUMORS
CLINICAL ONCOLOGY NEWS • APRIL 2014 • CLINICALONCOLOGY.COM
SABCS 2013
NeoALLTo Data Supports pCR as End Point in Trials Surrogate end point may speed clinical trials, improve patient access to drugs San Antonio—Updated results from the NeoALLTo trial demonstrate that in breast cancer patients, a complete pathologic response (pCR) from treatment with neoadjuvant trastuzumab and lapatinib correlates with improved event-free survival and overall survival (OS). The results, presented at the San Antonio Breast Cancer Symposium (SABCS; abstract S1-01), support the use of pCR as an end point for breast cancer clinical trials. The NeoALTTo study enrolled 450 patients with invasive, operable, HER2positive breast cancer, and randomized them to six weeks of treatment with lapatinib (Tykerb, GlaxoSmithKline), trastuzumab (Herceptin, Genentech) or lapatinib plus trastuzumab. Paclitaxel was added to all three arms at week 6 for an additional 12 weeks of neoadjuvant therapy. Following surgery and the administration of three cycles of anthracyclinebased chemotherapy, patients in the lapatinib arm received that drug for 34 weeks; women in the trastuzumab arm received their drug for 34 weeks; and patients in the triple combination arm
received both lapatinib and trastuzumab for 34 weeks. Previously, researchers reported that patients were more likely to achieve a pCR if they received lapatinib plus trastuzumab (51%) than if they received monotherapy with either lapatinib (25%) or trastuzumab (30%). A pCR was defined at that point as no invasive disease in the breast.
invasive disease in the breast and the axilla, had a 62% lower risk for disease progression, cancer recurrence or death ( =0.0003), and a 65% lower risk for (P death from any cause ((P=0.005). “The divergence of the curves is much more pronounced in the hormone receptor–negative, HER2-positive subgroup,” said Martine Piccart-Gebhart, MD, PhD, the director of the Medicine Department
‘[This] is encouraging because you know that adjuvant trials in breast cancer take forever, are very time- and money-consuming, and require thousands of patients.’ —Martine Piccart-Gebhart, MD, PhD In an updated analysis from the trial, there were trends for 22% better eventfree survival and 38% better OS rates with the combination therapy compared with trastuzumab, although they were not significant. Women who achieved a pCR before surgery, this time using the FDA’s recommended definition of no
at Jules Bordet Institute in Brussels, Belgium, who presented the results. She said the data was encouraging for the dual combination, but “do not indicate that we should change the standard of care yet.” The study, she added, provides strong support for the concept of using pCR as an intermediate end point in neoadjuvant
trials in breast cancer. “[This] is encouraging because you know that adjuvant trials in breast cancer take forever, are very time- and money-consuming, and require thousands of patients,” Dr. Piccart-Gebhart said. Jennifer Litton, MD, an associate professor in the Department of Breast Medical Oncology at the University of Texas MD Anderson Cancer Center in Houston, said the study was important because it provided further evidence that pCR was “a strong surrogate end point,” one that can be used “to develop new drugs and get them to patients quicker, with a smaller number of patients involved and less cost.” In September, pertuzumab (Perjeta, Genentech) became the first breast cancer drug to be granted accelerated approval by the FDA for neoadjuvant treatment based on pCR. —Kate O’Rourke Dr. Piccart-Gebhart disclosed consulting fees from Roche. Dr. Litton has received grants and research support from Novartis.
by the
numbers
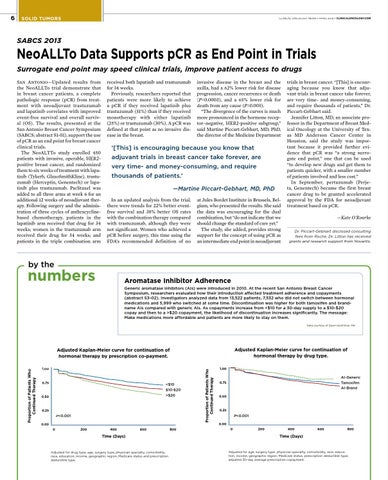
Aromatase Inhibitor Adherence Generic aromatase inhibitors (AIs) were introduced in 2010. At the recent San Antonio Breast Cancer Symposium, researchers evaluated how their introduction affected treatment adherence and copayments (abstract S3-02). Investigators analyzed data from 13,522 patients, 7,532 who did not switch between hormonal medications and 5,999 who switched at some time. Discontinuation was higher for both tamoxifen and brandname AIs compared with generic AIs. As copayments increase from <$10 for a 30-day supply to a $10-$20 copay and then to a >$20 copayment, the likelihood of discontinuation increases significantly. The message: Make medications more affordable and patients are more likely to stay on them. Data courtesy of Dawn Hershman, MD
Adjusted Kaplan-Meier curve for continuation of hormonal therapy by drug type.
1.00
0.75
<$10 $10-$20 >$20
0.50
0.25
P<0.001
Proportion of Patients Who Continued Therapy
Adjusted Kaplan-Meier curve for continuation of hormonal therapy by prescription co-payment. Proportion of Patients Who Continued Therapy
6
1.00
AI-Generic Tamoxifen AI-Brand
0.75
0.50
0.25
P<0.001 0.00
0.00 0
200
400
600
Time (Days)
Adjusted for drug type, age, surgery type, physician specialty, comorbidity, race, education, income, geographic region, Medicare status and prescription deductible type.
800
0
200
400
600
800
Time (Days)
Adjusted for age, surgery type, physician specialty, comorbidity, race, education, income, geographic region, Medicare status, prescription deductible type, adjusted 30-day average prescription copayment.