37 minute read
CPD: FOCUS ON WOMEN’S HEALTH


Continuing Professional Development CPD CPD
60 Second Summary
The menstrual cycle is controlled by multiple factors - endocrine, autocrine and paracrine, which regulate ovarian follicular development, ovulation, luteinisation, luteolysis, and endometrial remodelling. Endometriosis is a chronic, inflammatory condition that is oestrogen dependent, affecting women in their reproductive year. It is linked to pelvic pain and infertility, and is caused by the occurrence of endometrial-type mucosa (uterus lining) outside of the uterus, predominantly in the pelvic compartment. The most common endometriosis lesions can be subdivided into peritoneal implants, ovarian cysts, and deep nodules/plaques, which can involve and infiltrate other peritoneal structures. A symptom diary can aid with diagnosis. If initial treatments do not help, further investigations like a transvaginal or transabdominal ultrasound or laparoscopy can be useful. A laparoscopy is the only definitive way to diagnose the condition. Unfortunately there is still no prevention or cure for endometriosis. The therapeutic goal for endometriosis is to relieve pain, slow the growth of endometrial tissue, improve fertility, and prevent return of symptoms as much as possible. In Ireland, 1 in 6 couples are affected by infertility. Female factors generally account for ~40% of cases of infertility with male factors accounting for the other ~40%. In about 20% of cases, no specific cause of infertility is ever found. The average age of menopause diagnosis in the UK is 51, although this can vary depending on ethnicity. In the estimated 20% of women who have a hysterectomy, the menopause is often earlier than usual, even though the ovaries may be preserved.
AUTHOR: Donna Cosgrove PhD MPSI
Donna graduated with a BSc in Pharmacy from the Royal College of Surgeons in Ireland. She then returned to university to complete a MSc in Neuropharmacology. This led to a PhD investigating the genetics of schizophrenia, followed by a postdoctoral research position in the same area. Currently Donna works as a pharmacist in Galway, and as a clinical writer.
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice? 2. IDENTIFY - If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area. 3. PLAN - If I have identified a knowledge gap - will this article satisfy those needs - or will more reading be required? 4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs? 5. WHAT NEXT - At this time you may like to record your learning for future use or assessment. Follow the 4 previous steps, log and record your findings. Published by IPN. Copies can be downloaded from www.irishpharmacytraining.ie Disclaimer: All material published is copyright, no part of this can be used in any other publication without permission of the publishers and author.
Focus on Women’s Health
There are many unique ways in which women’s health differs from men’s. Women have specific experiences related to reproduction, such as periods, pregnancy and menopause. This article will focus on some of the health issues specifically relating to the menstrual cycle that women encounter.
The Menstrual Cycle
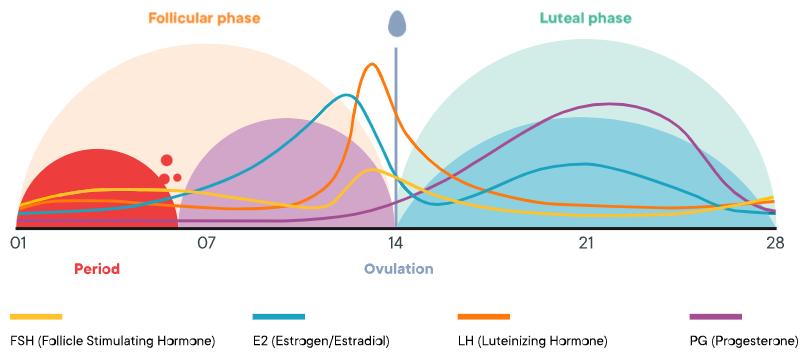
The menstrual cycle is controlled by multiple factors - endocrine, autocrine and paracrine, which regulate ovarian follicular development, ovulation, luteinisation, luteolysis, and endometrial remodelling. The average woman has a reproductive lifespan of about 36 years on average, starting when menstruation begins, between the ages of 8.5 to 13, until menopause (defined as one year of anovulation), at about 51 years. Puberty in females lasts about 2.3 years (usually between 2 and 5 years), beginning with breast development, then pubic and axillary hair growth, and concluding with the first menstrual period.1 The average menstrual cycle lasts for 28 days (Figure 1). Prediction of cycle stage and ovulation in individual women is difficult due to the highly variable length of the menstrual cycle, i.e. 24 to 34 days, even among similarly aged women. It also changes over time.. In the years following the beginning of menstruation and the years prior to menopause, there can be high variability, long cycle lengths and bleeding irregularities.
Figure 1. The menstrual cycle2
Anovulation affects up to 7% of women aged 25-39 with cycles of normal length, but is seen more frequently in women with shorter or longer cycles: 60% of 10-14 year old girls and 34% of women over 50 do not ovulate. Menstrual bleeding is usually the external symptom of the cycle, occurring at the end of the luteal and the beginning of the follicular phase. This lasts on average between 3 and 6 days. Certain psychological changes, as well as physiological, have been known to occur during the fertile phase.3 Features widely thought to be indicative of genetic benefit such as masculinity and symmetry show increased attractiveness ratings to women: women are more attracted to characteristics reflective of high genetic quality in ancestral males, i.e. the presence of genes with beneficial effects, absence of genes with harmful effects, or a low overall number of mutated genes, on high-fertility days of the ovulatory cycle. This is however only the case when these men were evaluated in the context of short term relationships. The same preference did not emerge when women evaluated men as prospective partners for a longterm relationship like marriage. Scent cues are also detected by men and women - young women and mothers-daughters can synchronise their menstrual cycles. This may be due to the olfactory detection of 5-alpha-androst-16en-3alpha-ol, an androgen believed to act as a pheromone which is secreted during the fertile phase.
Endometriosis
Endometriosis is a chronic, inflammatory condition that is oestrogen dependent, affecting women in their reproductive years.4 It is linked to pelvic pain and infertility, and is caused by the occurrence of endometrial-type mucosa (uterus lining) outside of the uterus, predominantly in the pelvic compartment.5 The prevalence of the disease is estimated to be about 5%, with peak occurrence between 25 and 35 years. One theory on why this happens is called the retrograde menstruation phenomenon: during menstruation, viable endometrial fragments are driven through the fallopian tubes, possibly by uterine contractions. Another theory is that endometrial cells can spread through the bloodstream or lymphatic system. Once in the peritoneal cavity the fragments can implant and grow. The risk of endometriosis is increased with regular, heavy
Figure 2. Epidemiological factors involved in endometriosis development5 periods, and a family history also increases risk (Figure 2). The presence of ectopic tissue leads to inflammation due to overproduction of prostaglandins, cytokines and chemokines. The most common endometriosis lesions can be subdivided into peritoneal implants, ovarian cysts, and deep nodules/plaques, which can involve and infiltrate other peritoneal structures.
Symptoms and Diagnosis
The main symptoms of endometriosis are:4, 5, 6
Chronic pain in the lower abdomen or back (pelvic pain) – usually worse during your period Period pain, i.e. dysmenorrhoea, that stops a woman from doing her normal activities
Dyspareunia (i.e. pain in the genital area or within the pelvis before, during or after sexual intercourse) Dyschezia (i.e. painful bowel movements, particularly periodrelated) Dysuria (painful urination, particularly period-related) Feeling sick, constipation, diarrhoea, or bloody urine during menstruation
Difficulty becoming pregnant The most frequent symptoms are dysmenorrhoea (i.e. throbbing or cramping pain, 80%) and dyspareunia (30%). Intermenstrual pelvic pain unrelated to periods can also occur, but less often. Hyperalgesia is also a feature in some cases. This is characteristic of neuropathic pain, and may be due to the chronic inflammatory environment promoting nociceptor sensitisation. Increased pain perception as a separate phenomenon can occur due to an increase in the intensity of nociceptive input ascending to the cortex.

A symptom diary can aid with diagnosis. If initial treatments do not help, further investigations like a transvaginal or transabdominal ultrasound or laparoscopy can be useful. A laparoscopy is the only definitive way to diagnose the condition.4, 6 Infertility arises often in endometriosis. The reasons for this are not fully understood but it is probably as a consequence of chronic pelvic inflammation, with inflammatory molecules creating an environment unfavourable to conception, in addition to damage to the fallopian tubes and ovaries.4, 5
Treatment
Unfortunately there is still no prevention or cure for endometriosis. The therapeutic goal for endometriosis is to relieve pain, slow the growth of endometrial tissue, improve fertility, and prevent return of symptoms as much as possible. The choice of treatment depends on several factors including age, main symptoms, family planning, attitude to surgical intervention, and previous treatment history.4, 6 Analgesics, either OTC paracetamol/ibuprofen or prescription medication can help to reduce pain. Hormone treatment aims to limit the production of oestrogen, which causes endometriosis tissue to grow and shed. These medications prevent ovulation and make periods lighter and less painful. However, hormone treatment has no impact on adhesions or improving fertility. Low dose oral contraceptives are often used for multiple reasons: they decrease retrograde menstruation, and have demonstrated good levels of overall safety, cost and tolerability. No real differences have been shown between various oral contraceptives, but a good
approach is to choose one with the lowest possible oestrogen content to prevent endometrial proliferation. Certain progestogens such as oral norethisterone may also help with symptoms. Another option is the insertion of a levonorgestrel IUD, which causes menstruation to stop in about a third of women, and decreases the amount of bleeding in another third. The contraceptive injection, implant or progestogenonly-pill can also be considered. Evidence suggests these hormone treatments are equally effective at treating endometriosis, but they have different side effects. Progestogen therapy however may reduce libido in up to a fifth of women. NICE have produced a patient decision aid7 for the different choices of hormonal treatment (“Hormone treatment for endometriosis symptoms – what are my options?”) describing what each option involves, likely relief of pain and effect on periods and fertility, and how best to stop each one. It also discusses the potential side effects such as possible blood clots and increased risk of breast cancer. If a trial period of e.g. three months with NSAIDs and/or hormonal treatment is ineffective or not tolerated, referral to a specialist should be considered. Surgery to remove patches of endometriosis (laparoscopy) is an option, but as it does not affect the pathogenic origins of the condition, recurrences of lesions and symptoms are common if no postoperative adjuvant treatment is used.5 After surgery, hormonal treatment should be considered in order to prolong the benefits of surgery. Prior to surgery, GnRH analogues, which bring on a temporary menopause by reducing the production of oestrogen, may be prescribed. This helps reduce the amount of endometrial tissue.
The management of endometriosis related subfertility should have input from a fertility specialist.6 Surgery for adhesiolysis may re-establish better relationships between pelvic organs, reduce inflammation and improve the chance of spontaneous pregnancy. Laparoscopic ovarian cystectomy where appropriate can also improve the chance of spontaneous pregnancy. IVF can be performed, which overcomes potential issues with fallopian tube patency and adhesions, although women with moderate to severe endometriosis still tend to have a lower chance of pregnancy with IVF than usual.
Endometriosis is a risk factor for epithelial ovarian cancer and is associated with negative psychosocial consequences including anxiety, depression, isolation, familial and intimate implications including negative emotional impact in partners, decreased quality of life and ability to perform everyday activities, and greater healthcare costs. Affected women lose an estimated 10 hours of work weekly, due to reduced effectiveness at work because of endometriosis symptoms.4 It is important to treat patients with empathy, reassurance and encouragement, with realistic treatment expectations. Delayed diagnosis is often a significant issue for women with endometriosis. This is due to both healthcare professionals seemingly not recognising the significance of the symptoms, and a delay in women seeking help because of the perception that a certain level of pelvic pain is normal.
Fertility
In Ireland, 1 in 6 couples are affected by infertility. Female factors generally account for ~40% of cases of infertility with male factors accounting for the other ~40%. In about 20% of cases, no specific cause of infertility is ever found. The biggest contributors to reducing fertility are:8, 9 Increasing age in women Elevated scrotal temperature in men
Alcohol consumption Smoking Being underweight or obese for women
Recreational drug use Some prescription drugs, e.g. NSAIDs, spironolactone, neuroleptics in women; sulfasalazine and anabolic steroids in men
If conception has not occurred within a year of trying (i.e. unprotected sex every 2 to 3 days), the couple should be clinically assessed. If there is a known clinical cause of infertility, history of predisposing factors, or the woman is 36 or older, earlier clinical assessment is appropriate.8, 9 The key regulator of the reproductive axis is gonadotropin hormone-releasing hormone (GnRH), which is released by the hypothalamus, and then acts on the pituitary gland. This results in the production and secretion of the gonadotropins, luteinising hormone (LH) and follicle stimulating hormone (FSH), which are transported to the ovaries and testes.
In females, LH and FSH stimulate the ovarian follicle (which contains a maturing egg) to produce oestrogen. After ovulation, LH (which has caused the egg to be released from the follicle at around day 14, Figure 1) promotes production of progesterone by the corpus luteum (this develops from an ovarian follicle), which contributes to a negative feedback loop, suppressing GnRH release from the hypothalamus, and therefore LH release from the pituitary. If conception occurs, the production of progesterone from the developing foetus helps maintain the pregnancy, and inhibits this loop. The main causes of infertility in women include: Damaged or blocked fallopian tubes (where conception usually occurs) Conditions affecting the cervix or uterus - these include large fibroids or large polyps in the uterus Endometriosis Ovulation disorders Polycystic ovarian syndrome (PCOS) Early menopause (before age 40) Sexually transmitted infections (STIs) Hypothalamic-pituitary-adrenal (HPA) axis (reproductive axis) dysfunction
Treatment
There are multiple pharmacological options to help with fertility issues depending on the nature of the problem. In hyperprolactinaemia (which can block ovulation), a dopamine agonist which inhibits prolactin production may help to normalise levels, e.g. bromocriptine or cabergoline10, 11 Clomifene or tamoxifen12 promote oestrogen production via effects on the hypothalamus, and can be used to restore or stimulate ovulation. The
aromatase inhibitor letrozole,13 which inhibits conversions of androgens to oestrogens, is also used (unlicensed use) Metformin decreases circulating insulin and androgen levels.
It can be used to stimulate ovulation, although there is no official clinical trial evidence for this (unlicensed use). It can take ~6 months to have an effect.
Assisted conception options available through private healthcare in Ireland are:
IUI (intrauterine insemination) IVF (in vitro fertilisation) ICSI (intracytoplasmic sperm injection) In IVF egg production is stimulated, the eggs produced are removed, fertilised, and then transferred back into the uterus. This process involves the following steps: 1. Suppressing the natural menstrual cycle to take control of the ovulation cycle. One cycle of an oral contraceptive may be given, followed by a
GnRH analogue, e.g. buserelin or nafarelin, or a GnRH antagonist, e.g. cetrorelix.
Continued stimulation with these desensitises the pituitary, and stops FSH/LH production. 2. Encouraging egg (ovarian follicle) production with the administration of recombinant
FSH. Trans-vaginal ultrasound scans can be performed to monitor follicle size. 3. When the eggs are ready for collection, an injection of recombinant human chorionic gonadotropin (hCG) is administered. This mimics an LH surge, which triggers final follicular maturation and ovulation. 4. Oocyte collection is performed under sedation about 36 hours after the injection.
A progesterone gel or pessaries may be prescribed for the woman to use from around now for luteal phase support14 to increase likelihood of implantation and successful pregnancy. 5. Sperm are mixed with the retrieved eggs to allow fertilisation to occur. 6. After a few days of incubation, the embryo (or embryos) is transferred into the uterine cavity.
There are many other medicines and protocols for assisted conception methods. The main side effects of these medications used in assisted conception include headaches, injection site reactions, fatigue, mood swings, hot flushes, bloating, breast tenderness, abdominal pain, and sometimes ovarian hyperstimulation syndrome (OHSS).
Menopause
The average age of menopause diagnosis in the UK is 51, although this can vary depending on ethnicity. In the estimated 20% of women who have a hysterectomy, the menopause is often earlier than usual, even though the ovaries may be preserved. On average, the symptoms of menopause last from 5-7 years, but in some cases can go on for up to 10-15 years. During the peri-menopause, when the ovaries gradually stop functioning (which lasts for about 4 years on average), the levels of oestrogen and progestogen (and testosterone) fall. This is usually diagnosed based on the presence of vasomotor symptoms, e.g. hot flushes, headaches, palpitations; and irregular periods, as the cycle can shorten to two to three weeks, or conversely, lengthen substantially. Ovarian failure can be caused by radio- or chemotherapy or some types of surgery, and this can lead to severe menopausal symptoms. One in 10 women’s periods will stop abruptly. An estimated 10% of women go through an early menopause between 40-45 years of age. If menopause occurs before this, it is categorised as premature ovarian insufficiency, which happens in about 4% of women. A test for FSH to diagnose menopause may be considered in women under 45 when menopause is suspected.15, 16
Symptoms
The most common symptoms are hot flushes and night sweats, which are experienced by up to 80% of women. Urogenital symptoms occur in 40%. This is due to thinning and shrinking of the vulval, vaginal, urethral and bladder tissues caused by the reduction in oestrogen. Smoking is linked to earlier menopause, and with more severe symptoms of vaginal dryness. These symptoms increase in severity over time. The risk of osteoporosis and fractures also increases with declining oestrogen levels. Other symptoms include , but are not limited to: Vaginal dryness and irritation, also leading to discomfort during sexual activity Decrease in libido (due both to tissue irritation and diminishing testosterone and oestrogen levels) Urinary symptoms such as frequent need to urinate Increased rate of infections: this is caused by the change of pH that results from alterations in urethral and vaginal microbiomes Joint, bone, and muscle pain Disturbed sleep (aggravated by night sweats) Irritability Poor concentration
Depression and other mood disorders like loss of confidence, panic attacks and anxiety Hair and nail changes Some medicines can worsen menopausal symptoms, e.g. anti-oestrogens, some antihypertensives and antidepressants (e.g. high dose venlafaxine). Women with a higher BMI and/or a greater proportion of body fat may experience more pronounced vasomotor symptoms.
Management
Non- pharmacological measures to help with hot flushes and night sweats include:
Wearing light clothing Keeping the bedroom cool at night Taking a cool shower, using a fan or having a cold drink Trying to reduce stress levels Avoid/reduce potential triggers: spicy food, caffeine, hot drinks, smoking and alcohol Exercise regularly Losing weight if overweight CBT can also help manage hot flushes.
Pelvic floor muscle training can help with urinary symptoms, especially for stress and mixed incontinence related to the menopause. Physiotherapists can advise, and there are also numerous apps available for this. Specific vaginal moisturisers and lubricants can be useful alone or when used in addition to vaginal oestrogen preparations. NICE recommends low dose vaginal oestrogen (vaginal tablets, creams, rings or gels) as first line treatment for vaginal or urinary symptoms caused by the atrophy linked to oestrogen reduction. Due to the low systemic absorption of vaginal oestrogen preparations, no progestogen is needed with these for endometrial protection. These treatments are best started early, before any irreversible changes have occurred. Symptoms often return when treatment is stopped, however. There is some evidence that black cohosh, isoflavones and St John’s Wort may relieve vasomotor symptoms, but it is important to only use reputable brands with good quality constituents in their products. Due to many menopausal products being referred to as ‘natural’, there is the false impression that these ingredients are safer than prescribed medicines. It is important to inform people that there are potential drug interactions with other medications. Phytooestrogens have also been investigated for their effect on menopausal symptoms but evidence is mixed. The following additional therapies may be useful for improving mental health during the menopause: Cognitive Behavioural Therapy Breathing exercises/structured relaxation
Mindfulness
Good sleep hygiene practices Exercise
Systemic oestrogen therapy is the most effective treatment for symptoms of hot flushes or night sweats. Women with a uterus need a progestogen also (e.g. as part of a combination patch, tablets or an intrauterine system) to reduce the risk of endometrial cancer that can be caused by using oestrogen alone. Systemic HRT can be used alongside a low dose vaginal oestrogen product if required. Vaginal bleeding is a common side effect of HRT in the first three months of treatment - the prescriber should be informed at the recommended 3 month review after starting the treatment, and promptly if bleeding occurs after the first 3 months. Taking HRT increases the risk of venous thromboembolism, although for women using standard doses of transdermal preparations (as opposed to oral) the risk is no greater. Similarly, there is a slight increase in the risk of stroke, but only from oral preparations. Any potential increased risk in breast cancer is related to treatment duration, and reduces after stopping HRT again. Risk of fractures while on HRT is reduced, and there is also limited evidence that HRT may improve strength and muscle mass.
SSRIs, SNRIs and clonidine should not be recommended as first line treatments: there is no evidence to suggest that SSRIs/ SNRIs improve mood symptoms attributable to the menopause. Clonidine may however help some women with vasomotor symptom relief in certain cases. Testosterone (produced by the ovaries) supplementation can be considered in cases of low libido that is not helped by HRT. Although fertility declines during the perimenopause, contraception should still be continued for two years after the last menstrual period in women younger than 50, and one year if over 50 and under 55. Using protection for STI prevention is still recommended at all stages. To reduce the risk of osteoporosis and fractures, women should be advised to exercise (weight bearing), take vitamin D supplements (especially during the winter months), eat a balanced diet, quit smoking, and only consume alcohol in low to moderate amounts (as this is a dose-dependent risk factor for fractures).
Summary
Pharmacists have an important role in providing advice on the safe and appropriate use of medicines during all stages of women’s health. This includes providing support and information on menstrual health, menstrual cycle dysfunction, and menopause. Pharmacy teams can do this by initiating conversations and brief interventions, raising awareness, removing stigma, managing symptoms, supplying medication, and referrals.
References Available Upon Request
Men’s Health

Advocating for Men’s Health
The COVID-19 pandemic led to a sharp drop in consumer spending in 2020. However, sales have been steadily increasing in 2021, putting the economy in a position to continue doing well in 2022.

An interesting aspect of this growth is that men have begun to spend more on consumer goods than women.
It is anticipated that the global business of the men’s personal care market will grow at a compound annual growth rate of 9.1% from 2022 to 2030 from USD 30.8 billion in 2021. It is expected that the market will benefit from men’s demand for gender-specific products such as shampoos, conditioners, shaving creams, masks, and peels. Furthermore, the thriving e-commerce sector is expected to boost the market growth. This is where the most dramatic shift has been seen, men are spending more online and more frequently. As a result of this increase, investing in digital ads, especially those targeted at men and men’s goods, is expected to pay off. These sales may slow down as retailers face a major challenge in trying to keep prices down for consumers to remain competitive while offsetting the impact of rising costs across their product lines and supply chains. As social media use grows, men tend to search for products more on social media than women. Those brands that haven’t branched into sales elements similar to what social sites such as Instagram and Facebook have made available have a huge opportunity to grow. Through social media, brands can express themselves through brand purchases, especially in the lifestyle sector. The use of social media by men is increasing, and causing them to discover products they wouldn’t have noticed otherwise, leading them to make purchases they wouldn’t have made otherwise, and becoming more open to social media as a source of inspiration and motivation.
Another surprise was the significant increase in men connecting with brands through email marketing channels, as the Voyado Index 2022 revealed. The overall email open rate increased in 2021, young men between the ages of 18 and 25 accounted for the biggest increase (23%) but there were noticeable increases in other age groups too. Men are likely to remain engaged with brands through email marketing based on the data from the Index.
According to the Index, retailers personalised their emails 15% more in 2021 thanks to improved personalisation. Personalised emails sent to men between the ages of 18 and 35 saw the greatest increase in open rates (27%). A small tweak, such as adding personalised fields to the subject line, can have a significant impact on the open rate of your email. With this shift, many malefocused health and wellbeing
Written by Stephen Cuffe, Pharmacist, Inish Pharmacy
companies have popped up offering personalised health and subscription services for men. With men using online services more this may lead to an improvement in their looking after their wellbeing. Regarding men’s health, a specific focus remains urgent. In general, men are particularly bad at looking after their health.
A considerable body of evidence supports the need for genderspecific approaches to engage with men more effectively, as well as the imperative to build upon the progress been made to-date to address gender-based issues of life expectancy and mortality and health disparities between various subpopulations of men. These were the main reasons which led to the development of Ireland’s National Men’s Health Policy, which was the first of its kind in the world. To the development of Ireland’s National Men’s Health Policy, which was the first of its kind in the world. Although there are areas of success in the policy, it is not a quick fix. The challenges in persuading services to change and the benefits to men’s health take time to occur. Women are typically invited to more frequent check-ups throughout their lifetimes, such as prenatal care and cervical cancer screenings. Contrastingly, men may not receive gender-specific screenings and may never need health care until being requested to submit a stool sample for a bowel cancer screening program in their fifties. In Europe, men are more likely to engage in unhealthy behaviour than women and are more at risk for all major causes of death. Despite this, males report greater subjective health than women and are less likely to believe they are at risk for health issues. A lot of men don’t talk about their physical or mental health this may be due to a tendency to minimise or not accurately report symptoms, not wanting to appear weak, or just difficulty in communicating their emotions. Moreover, healthcare is not designed to complement the lifestyles of many men. Success in their careers is often regarded as a great deal of self-worth for men. Men may typically have to take time out of work to seek healthcare. Multiple appointments spread out over a long period may be necessary for full engagement in therapy or treatment. Taking that time off from work is not an option for many men. Men can become more involved in their health to some extent by using the conventional strategy of public health education campaigns through printed media, social media, and television. However, perhaps the key to encouraging men to engage with their health and GP is in digital health technologies. Since the development of digital communication technology, telemedicine has become more and more popular. Additionally, the COVID-19 pandemic’s arrival has brought about many changes and has increased the use of this method of healthcare delivery. In addition to lowering the chance of exposure to an illness, digital health has several other advantages. Men’s healthcare has a strong connection to three specific benefits. Starting with the obvious, which is attendance. Men have always had difficulty making medical appointments. When a situation is time-sensitive, this hesitation can have terrible consequences. Many of the obstacles associated with in-person visits, such as taking

time off work, getting to the office, or passing the time in a waiting room, are eliminated with telehealth. This implies that there is no longer a justification for delaying care. It now only takes twenty minutes to complete an appointment that used to take up a half-day. Not only that, but disclosure is another unexpected benefit of telehealth. In contrast to an in-person consultation, many men feel more at ease speaking candidly during a telemedicine appointment. The privacy that telehealth provides over in-person care is a contributing factor in this transformation. In the doctor’s office, you might not feel comfortable talking about the symptoms of erectile dysfunction, but a phone call or even a Zoom call may make the discussion less intimidating. The third benefit is having access to specialty care that might not be offered locally. Simply put, there aren’t that many medical professionals with expertise in treating hormone imbalances and improving performance in men’s health. It is a significant improvement in healthcare to be able to see a specialist wherever you (or they) may be. The field of health care and methods of delivering healthcare must change and evolve as technology does. Although telehealth has shown its importance as an extra tool for contacting and treating patients, it may not be able to completely replace in-person medical consultations. But it has eliminated barriers that have previously prevented men from obtaining healthcare when they are in need and made it possible for men to receive healthcare more quickly and easily than ever before. Both medical professionals and patients had to adapt to and change their behaviour to use the new digital healthcare system. However, we may use this new way of life as a positive catalyst for change to address the problem in male health. There is no question about the importance of men’s health. The goal is to educate men on their risk factors and treatment options so that they become aware of their risks. By advocating for men’s wellbeing and health, pharmacists can help them aid themselves making them aware of the importance of visiting their doctor for screening and treatment.
Many online pharmacies are now becoming a one-stop source for men by assisting them with their health, wellness, and grooming requirements. The benefit of this is that you can get professional advice and expertise about the health issues that matter to you without the embarrassment or privacy concerns that might prevent you from visiting your local pharmacy.

Men’s Health News Mission isPossible for Male Heart Health
For Men’s Health Week 2022 the Irish Heart Foundation urged all men to take the first steps to protect their heart health.
Men’s Health Week is an initiative of Men’s Health Forum in Ireland, a charity that works across the island of Ireland to improve the health of men and boys. Men’s Health Week aims to raise awareness of preventable health problems, support men and boys to live healthier lives, and encourage them to seek help or treatment at an early stage. The theme for Men’s Health Week 2022 was ‘MISSION: isPOSSIBLE’ where men and boys on the island of Ireland were asked to step up and accept their own personal health challenge. Research clearly shows that men are dying too young as a result of ill health with more men than women dying from almost all of the leading causes of death at all ages. Research has also shown that men’s poorer lifestyles are responsible for a high proportion of chronic diseases including heart disease.
Late presentations by men to health services can also lead to a large number of problems becoming untreatable. According to MHFI, “all too often we set ourselves unrealistic targets. Therefore, this year, everyone is asked to focus upon small, simple, and practical things to improve their health.” Commenting Janis Morrissey, the Irish Heart Foundation said, “During Men’s Health Week 2022, take the first steps towards protecting your heart. The good news is that 80 per cent of premature heart disease and stroke is preventable and there are things men can do to reduce their risk. These include stopping smoking, reducing alcohol intake, getting their blood pressure and cholesterol checked, eating a healthy diet, being a healthy weight and being physically active. The Irish Heart Foundation is delighted to mark Men’s Health Week by holding heart health checks in a number of Men’s Sheds.”
Dr Noel Richardson, Director of the National Centre for Men’s Health in South East Technological University, said, “For me, the key message for Men’s Health Week is that small things can really make a difference – whether it’s going for a walk, taking time out, reconnecting with a friend. It’s about doing something positive for yourself and building momentum towards positive change, one step at a time.”
Hair, Nail, Skincare Scalp Recognising Upward Trends
At McCabes Pharmacy our customers expect expert knowledge, across all product categories.


Rebecca McMahon McCabes Pharmacy Supervisor Sarah Fitzpatrick McCabes Pharmacy Category Analyst
Every effort is made to ensure we offer them a comprehensive range of products, accompanied by expert advice from our store teams; extensive training is supplied to guarantee superior customer experience. Sarah Fitzpatrick, McCabes Pharmacy Category Analyst and Rebecca McMahon, McCabes Pharmacy Supervisor Swords Pavilions, share their insights into the fast developing Hair, Nail, Skin and Scalp categories. Beauty vitamins are at a growth in pharmacy with supplements to make hair grow thicker and faster, give skin a healthy glow and improve overall nail thickness the most in demand.
Sarah: “Consumer lifestyle and product design is essentially the key driver here. Working with suppliers that are continually innovating and developing new technologies is essential for growth. The hair product industry is continually evolving and so are we. Our customers trust us to provide innovative new products that will deliver that all important great hair day! This category is driven by a strong mix of central lines with a large topping of trends. We’re always monitoring market trends whilst keeping eyes peeled for new innovations and the next TikTok sensation!
This is a vast category, and there is certainly price sensitivity on the ‘non-essential’ end which is something to consider when building out a range, we like to offer something to suit all tastes and budgets. Due to the re-opening of salons, we are naturally seeing a shift in consumer behavior – going out is the new staying in – we are seeing an increased demand for hair styling product, hair tools, and of course travel minis”.
Rebecca: “We have seen a rise in consumer demand for vitamins and supplements with key ingredients such as Biotin, which is one of the most active ingredients found in hair, skin, and nails. As Biotin isn’t stored in the body you can become low in this if there isn’t enough in your diet. Some foods that contain this vitamin are, egg yolks, some nuts and seeds, avocado, mushrooms, sweet potato, bananas, and broccoli. We recommend adding these into your diet in moderation. In recent years we find a lot of customers are coming into store having gathered their own information online so quite often they are coming in already knowing what they want”.
Nails
Sarah: “Beauty trends increasingly led by social media drive growth in this category. The nail polish market is expected to be growing at a rate of +10% in the forecast period of 2022 to 2029 (data bridge). Nail care has become a ritualistic trend among many of the millennials and gen z’s. Although a large portion of growth in this category is salon based, the growth can also be seen at a retail level, across nail varnishes and polishes as well as accessories and vitamins and supplements that contribute to nail strength and growth. The right product mix is so important, at McCabes Pharmacy we offer a strong core line, and again top up with trending products. This category relies heavily on technology and brand presence. Brands that come to market offering new USPs drive the growth in this area. Similar to haircare we have seen an upward curve in demand for vitamins and supplements. This is echoed across the market with global beauty supplements anticipated to grow at a CAGR of 4.8% until 2027 (Coherent Market Insights). Vitamins and minerals such as Biotin, B Vitamins, Iron, Magnesium, Omega 3 fatty Acids, Vitamins C and Zinc are key factors that contribute to healthy nails. At McCabes Pharmacy, we are seeing a shift in behavior, specifically customers investing in prevention rather than cure, with customers investing in beauty supplements at a younger age. The nail category is certainly a growth area and with restrictions lifted we are seeing significant growth on the cosmetic side, along with consistent growth across beauty supplements.
Skincare
Rebecca: “This category is particularly driven by our store advisors; we have our expert skincare advisors on duty everyday to help customers choose the right products. Our skincare advice service is also now available on our website mccabespharmacy. com. Customers answer a series of questions and are guided to the products that best suit their needs. We’ve recently added this service to our newly launched Citywest store, via a touchscreen. Customers love it! Our skincare range is fantastic, with a huge range of products from both premium and cult brands that target everything from wrinkles to dehydration, acne, pigmentation, and rosacea…just to name a few! We’ve noticed our customers are increasingly requesting vitamins and supplements that will work alongside their skin treatment, the most frequently requested skin supplement is collagen”.
Scalp
Sarah: “This category is particularly driven by our store advisors, the specialist training they receive is something we pride ourselves on. Due to the nature of this category being condition led, growth here is driven by suppliers and brands developing new technologies and innovations. Without strong assistance and product knowledge from our in-store advisors, this area could be overwhelming to customers, so staff training is crucial, so they are aware of the key differentials of each product, enabling them to match the needs of each individual customer”.
Digital Skin Advisor McCabes Pharmacy Citywest SC At McCabes Pharmacy, by keeping the customer at the core of our decisions, we’re confident we will always offer them the right product choice.

Digestive Market
Digestive Health – Core to OTC Market
Stretching from your head to your bottom, the digestive system (made up of the gut, bowel, and stomach) breaks down all that delicious food and drink we consume, absorbing the useful nutrients and energy, whilst getting rid of the waste. It’s a complex system that comes with various health concerns, from simple problems like indigestion to disorders which may be lifelong, such as IBS.
Many of the products in the Digestive Health category offer patients solutions and symptom relief. Generally the most common concerns presenting in pharmacy are constipation, diarrhoea, bloating, heartburn, and irritable bowel syndrome (IBS). Lifestyle advice can prevent and alleviate many of the symptoms related to this category. Such as avoiding trans and fatty foods, reducing sugar intake, eating more fibre, drinking water, not smoking, reducing caffeine and alcohol intake, eating regular healthy meals, and staying active. However, this advice is often easier said than done. So throughout our lives, at some stage many of us will need to visit a pharmacy to get something to alleviate digestive discomfort and symptoms. The Digestive Health category is core to the OTC offering in pharmacy. There has been little change in the category in recent years with established brands accounting for the majority of revenue and no recent new product launches. The category is well supported with advertising with major campaigns for Gaviscon, Nexium and others running throughout the year. The key products in the category are well established like Nexium, Dulcolax, Senokot, Imodium, Gaviscon, Arret. The last new product launch was about 4 years ago when Buscopan went from Rx to pharmacy only product. Like all categories currently there has been some supply issues with category leaders. Products like Fybogel, Dioraltye and Nexium have been going in and out of stock over the last 12 months. Alternatives for all these products were available and although patients didn’t always like changing they accepted alternatives and the advice of the pharmacy teams. Despite the lack of new products, the category is continually in growth. During covid growth came from difficulty accessing GP services and patients need for advice and support with simple digestion problems. Since society has opened up and we are back socialising in restaurants and pubs, the category is growing due to our changes in lifestyle. There have also been the usual tummy bugs and general illness during this time too.
Patient behaviour is changing in this category. Pharmacists are seeing well informed, welleducated patients who are pro-active about their health and wellness as well as the traditional symptom reactive patient. There is huge growth in the rehydration category. Post covid, there has been an increase in runners and gym active customers who are proactively rehydrating post workout with ORS, Dioralyte, Phizz, Oxylent and other rehydration products. Pro biotics are also growing and expanding and appealing to proactive and reactive consumers alike. Pro-biotic ranges are expanding with new products. Alforex and Zenflore have expanded their range to include new and broader products additions. Patients and customers alike are well informed on the benefits of gut health and good bacteria. There is also increasing awareness of the impact of gut health and diet on our mood and an understanding of the research of Professor Ted Dinon in UCC in this area.
IBS patients are very well educated and understand the balance of lifestyle and self-management of their condition.
Nexium is still the category leader in heartburn, despite generics entering the marketplace. However Gaviscon still is a relevant and strong category leader and is a unique liquid offering in the category. The role of the pharmacist is key in selling restricted sale products like Motilium appropriately and sales in this product are also growing and the importance of pharmacist advice and counselling is essential. Pharmacists play a vital role in supporting customers with their digestive health wellness and educating them on the different solutions available in pharmacy, lifestyle options and health advice. Pharmacists have a role empowering patient to self-care and self-manage digestive health symptoms. As Holiday season is kicking off and after nearly 3 years of lockdown, many are heading abroad for a holiday this year. Patients are pro-actively purchasing products like Nexium, Motiulium, Imodium and Dioralyte. We tend to overindulge or try new foods when abroad and no one wants to be caught feeling uncomfortable or suffering when on holidays.

Written by Emily Kelly, Community Pharmacist, McCauley Health & Beauty Pharmacy









