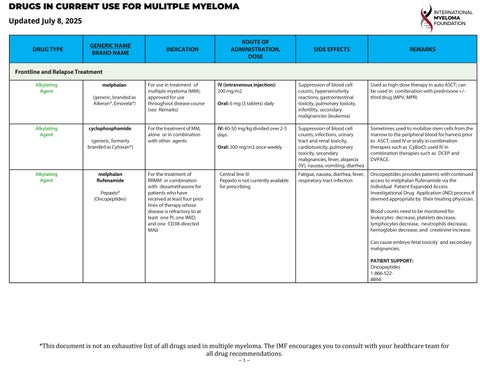
Used as high-dose therapy in auto ASCT; can be used in combination with prednisone +/third drug (MPV, MPR)
IV: 40-50 mg/kg divided over 2-5 days
Oral: 300 mg/m2 once weekly
For the treatment of RRMM in combination with dexamethasone for patients who have received at least four prior lines of therapy whose disease is refractory to at least one PI, one IMiD, and one CD38-directed MAb
Central line IV
Pepaxto is not currently available for prescribing.
Sometimes used to mobilize stem cells from the marrow to the peripheral blood for harvest prior to ASCT; used IV or orally in combination therapies such as CyBorD; used IV in combination therapies such as DCEP and DVPACE.
Oncopeptides provides patients with continued access to melphalan flufenamide via the Individual Patient Expanded Access Investigational Drug Application (IND) process if deemed appropriate by their treating physician.
Blood counts need to be monitored for leukocytes decrease, platelets decrease, lymphocytes decrease, neutrophils decrease, hemoglobin decrease, and creatinine increase.
Can cause embryo-fetal toxicity and secondary malignancies.
PATIENT SUPPORT: Oncopeptides
1-866-5228894
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
In combination with bortezomib in patients who have not previously received bortezomib and have received at least one prior therapy
ROUTE OF ADMINISTRATION, DOSE SIDE EFFECTS
IV regular doxorubicin: 9 mg/m2 days 1-4 of a 28-day cycle; 20 mg/ m2
IV doxorubicin liposome injection: 30 mg/m2 day 1 of a 28day cycle
Cardiotoxicity, secondary cancers, decreased blood cell counts, infusion site reactions, change in the color of urine, infection, lower sperm count, early menopause, hair loss, nausea, vomiting, mouth sores, eye problems, allergic reactions; Doxil also causes hand-foot syndrome
REMARKS
Lipsomal doxorubicin (Doxil) went off patent. Now there is an FDA-approved generic for Doxil as well as generic doxorubicin.
Bispecific T-cell Engager antibody
elrantamab-bcmm
Elrexfio® (Pfizer)
BCMA-directed therapy for the treatment of RRMM in patients who have received four prior lines of therapy, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 antibody.
SQ injection: The recommended dosage of ELREXFIO is step-up doses of 12 mg on Day 1, 32 mg on Day 2, and 76 mg on Day 3, followed by once-weekly dosing of 76 mg.
Can cause cytokine release syndrome (CRS), a potentially severe or fatal uncontrolled immune reaction in which cytokines become highly elevated and trigger an overwhelming immune system response that can damage body tissues and organs. CRS is managed by prevention using a step-up dose schedule. Premedication with tocilizumab before receiving bispecifics and CAR T-cell therapy is also being used in clinical trials. Should CRS occur, treatment depends on symptom severity, with mild cases (Grade 1-2) managed through supportive care like fluids, oxygen, and anti-inflammatory medications. Severe cases (Grade 3-4) may require tocilizumab, alone or with steroids, to control the immune response and cytokine storm.
Can cause hepatotoxicity. Monitor liver enzymes and bilirubin at baseline and during treatment as clinically indicated.
Can cause ICANS, a form of neurotoxicity that can occur days or weeks after taking ELREXFIO, with symptoms such as headache, encephalopathy, and motor dysfunction ICANS often occurs alongside
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
or after cytokine release syndrome (CRS) but can also develop independently.
Can cause severe, life-threatening, or fatal infections. Monitor patients for signs and symptoms of infection and treat appropriately. Withhold in patients with active infection during the step-up dosing schedule.
Can cause neutropenia. Monitor complete blood cell counts at baseline and periodically during treatment.
Embryo-Fetal Toxicity: May cause fetal harm. Advise females of reproductive potential of the potential risk to the fetus and to use effective contraception.
PATIENT SUPPORT: Pfizer 1-877-744-5675
Bispecific T-cell Engager antibody
linvoseltamab-gcpt Lynozyfic™
For the treatment of RRMM in patients who have received four prior lines of therapy, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 antibody.
As an infusion through a needle in your vein (called an intravenous or IV infusion).
Cytokine release syndrome (CRS); neurologic toxicities; infections; neutropenia (a reduced level of neutrophils, a type of white blood cell necessary to combat bacterial infection) and/or febrile neutropenia (the development of fever, often with signs of infection, in a patient with neutropenia); hepatotoxicity (liver injury or impairment); embryofetal toxicity
Can cause cytokine release syndrome (CRS), a potentially severe or fatal uncontrolled immune reaction in which cytokines become highly elevated and trigger an overwhelming immune system response that can damage body tissues and organs. CRS is managed by prevention using a stepup dose schedule. Premedication with tocilizumab before receiving bispecifics and CAR T-cell therapy is also being used in clinical trials. Should CRS occur, treatment depends on symptom severity, with mild cases (Grade 1-2) managed through supportive care like fluids, oxygen, and antiinflammatory medications. Severe cases (Grade 3-4) may require tocilizumab, alone or with steroids, to control the immune
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
response and cytokine storm.
Can cause hepatotoxicity. Monitor liver enzymes and bilirubin at baseline and during treatment as clinically indicated.
Can cause severe, life-threatening, or fatal infections. Monitor patients for signs and symptoms of infection and treat appropriately. Withhold in patients with active infection during the step-up dosing schedule.
Can cause neutropenia and/or febrile neutropena. Monitor complete blood cell counts at baseline and periodically during treatment.
Embryo-Fetal Toxicity: May cause fetal harm. Advise females of reproductive potential of the potential risk to the fetus and to use effective contraception. Advise patients who are breastfeeding or plan to breastfeed.
PATIENT SUPPORT:
Regeneron offers the Lynozyfic Surround™ program, which provides financial and educational resources to support patients throughout their treatment with Lynozyfic. For more information regarding Lynozyfic Surround™ or access and support, patients can call 1-844-RGN-HEME (1-844-7464363).
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
GPRC5D-directed therapy for the treatment of RRMM in patients who have received four prior lines of therapy, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 antibody.
ROUTE OF ADMINISTRATION, DOSE SIDE EFFECTS
SQ injection: The recommended dosage of TALVEY is step-up doses of 0.01 mg/kg on Day 1, 0.06 mg/kg on Day 2, and 0.4 mg/kg on Day 3, followed by once-weekly dosing of 0.4 mg/kg.
For patients whose healthcare team recommends bi-weekly dosing of TALVEY, the step-up doses are 0.01 mg/kg on Day 1, 0.06 mg/kg on Day 4, 0.4 mg/kg on Day 7, and 0.8 mg/kg on Day 10, followed by 0.8 mg/kg every two weeks.
Cytokine release syndrome (CRS); immune effector cellassociated neurotoxicity syndrome (ICANS); infections; cytopenias; hepatotoxicity (liver injury or impairment); embryofetal toxicity; oral toxicity such as dry mouth, distortion of sense of taste, or dysphagia (difficulty in swallowing); skin-related toxicities; and nail-related toxicities.
REMARKS
Can cause cytokine release syndrome (CRS), a potentially severe or fatal uncontrolled immune reaction in which cytokines become highly elevated and trigger an overwhelming immune system response that can damage body tissues and organs. CRS is managed by prevention using a step-up dose schedule. Premedication with tocilizumab before receiving bispecifics and CAR T-cell therapy is also being used in clinical trials. Should CRS occur, treatment depends on symptom severity, with mild cases (Grade 1-2) managed through supportive care like fluids, oxygen, and anti-inflammatory medications. Severe cases (Grade 3-4) may require tocilizumab, alone or with steroids, to control the immune response and cytokine storm.
Can cause hepatotoxicity. Monitor liver enzymes and bilirubin at baseline and during treatment as clinically indicated.
Can cause ICANS, a form of neurotoxicity that can occur days or weeks after taking TALVEY, with symptoms such as headache, encephalopathy, and motor dysfunction. ICANS often occurs alongside or after cytokine release syndrome (CRS) but can also develop independently.
Can cause severe, life-threatening, or fatal infections. Monitor patients for signs and symptoms of infection and treat appropriately. Withhold in patients with active infection during the step-up dosing schedule.
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
Updated July 8, 2025
Can cause cytopenias, including neutropenia and thrombocytopenia. Monitor complete blood cell counts at baseline and periodically during treatment.
Embryo-Fetal Toxicity: May cause fetal harm.Advise females of reproductive potential of the potential risk to the fetus and to use effective contraception.
PATIENT SUPPORT:
Janssen Biotech, Inc. 1-833-565-9631
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
DRUG TYPE GENERIC NAME BRAND NAME INDICATION
ROUTE OF ADMINISTRATION, DOSE SIDE EFFECTS
REMARKS
Bispecific T-cell Engager antibody
teclistamab (cqyv)
Tecvayli™ (Janssen)
BCMA-directed therapy for the treatment of RRMM in patients who have received four or more prior lines of therapy including a proteasome inhibitor, immunomodulatory drug, and anti-CD38 monoclonal antibody
SQ injection: The recommended dosage of TECVAYLI is step-up doses of 0.06 mg/kg and 0.3 mg/ kg followed by 1.5 mg/kg once weekly until disease progression or unacceptable toxicity.
Pyrexia, cytokine release syndrome, musculoskeletal pain, injection site reaction, fatigue, upper respiratory tract infection, nausea, headache, pneumonia, and diarrhea.
Can cause cytokine release syndrome (CRS), a potentially severe or fatal uncontrolled immune reaction in which cytokines become highly elevated and trigger an overwhelming immune system response that can damage body tissues and organs. CRS is managed by prevention using a stepup dose schedule. Premedication with tocilizumab before receiving bispecifics and CAR T-cell therapy is also being used in clinical trials. Should CRS occur, treatment depends on symptom severity, with mild cases (Grade 1-2) managed through supportive care like fluids, oxygen, and antiinflammatory medications. Severe cases (Grade 3-4) may require tocilizumab, alone or with steroids, to control.
Can cause hepatotoxicity, including fatalities. Monitor liver enzymes and bilirubin at baseline and during treatment as clinically indicated.
Can cause severe, life-threatening, or fatal infections. Monitor patients for signs and symptoms of infection and treat appropriately. Withhold in patients with active infection during the step-up dosing schedule.
Monitor complete blood cell counts at baseline and periodically during treatment. Hypersensitivity and local injection site reactions can occur. Withhold or consider permanent discontinuation based on severity.
Embryo-Fetal Toxicity: May cause fetal harm. Advise females of reproductive potential of
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
Updated July 8, 2025
the potential risk to the fetus and to use effective contraception.
PATIENT SUPPORT: Janssen Biotech, Inc. 1-800-526-7736
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
Updated July 8, 2025
DRUG TYPE GENERIC NAME BRAND NAME INDICATION
Corticosteroid dexamethasone
(generic, branded as Decadron®)
Immunomodulatory drug (IMiD) thalidomide
Thalomid® (plus dex) (Bristol Myers Squibb)
Immunomodulatory drug (IMiD) lenalidomide
Revlimid® (Bristol Myers Squibb)
No specific FDA approval for myeloma; approved for “palliative management of leukemias and lymphomas.”
Used in most regimens for front-line and relapsed MM; not often used in maintenance because of side effects from longterm use
Approved in combination with dexamethasone for the treatment of newly diagnosed myeloma, but is used throughout the disease course, including for maintenance therapy (without dex)
Approved throughout the disease course, including as maintenance therapy (without dex)
ROUTE OF ADMINISTRATION, DOSE SIDE EFFECTS
Oral therapy given in 4 mg tablets at a dose of 20-40 mg weekly. May be used as monotherapy, given orally at 40 mg, 4 days on, 4 days off, for urgent management. Can be given IV.
Caution about drug interactions see Understanding Dexamethasone for details. Several studies have demonstrated that reducing dex dose in combination therapy improves tolerance, extending treatment duration and OS.
Dose reductions may be recommended following initial cycles of therapy and demonstrated response.
Oral: approved at 200 mg daily, but is rarely given above 100 mg daily because it is effective at lower doses and higher doses are not generally well tolerated
Embryo-fetal toxicity, venous and arterial thromboembolism, peripheral neuropathy, constipation, drowsiness, dizziness, low white blood cell counts, rash
Patients must participate in a REMS (risk assessment and management program); both partners must use contraception. Causes irreversible peripheral neuropathy.
Oral: 25 mg days 1-21 of a 28day cycle, maintenance 10 mg continuous
Embryo-fetal toxicity, low white blood cell counts, low platelet counts, venous and arterial thromboembolism, diarrhea, fatigue, anemia, constipation, rash
Patients must participate in a REMS (risk assessment and management program); both partners must use contraception. Given in combination with dex, patients should receive anti-thrombotic prophylaxis (type determined by risk factors). FIRST trial demonstrated the benefit of continuous Rd in newly diagnosed mm patients who are not candidates for transplant.
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
Updated July 8, 2025
bmscustomerconnect.com/
*As of 3/22 – TEVA Generics offers a generic version of Revlimid. 1-888-838-2872. Prescribing information, boxed warnings, and medication guide can be found here.
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
DRUG TYPE GENERIC NAME BRAND NAME
Immunomodulatory drug (IMiD) pomalidomide
Pomalyst® (Bristol Myers Squibb)
Proteasome inhibitor bortezomib
Velcade® (Takeda)
In combination with dexamethasone for the treatment of patients with mm who have relapsed after at least 2 prior therapies including Revlimid and a proteasome inhibitor
ROUTE OF ADMINISTRATION, DOSE SIDE EFFECTS REMARKS
Oral: 4 mg days 1-21 of a 28-day cycle
Embryo-fetal toxicity, low white blood cell counts, low red blood cell counts, low platelet counts, venous and arterial thromboembolism, fatigue, weakness, dizziness and confusion, constipation, nausea, diarrhea, neuropathy
Patients must participate in a REMS (risk assessment and management program); both partners must use contraception. Patients should receive anti-thrombotic prophylaxis (type determined by risk factors).
Approved as treatment for myeloma and as retreatment for patients who had previously responded to treatment and who have relapsed at least 6 months after completing prior Velcade treatment.
IV or SQ (subcutaneous injection) at 1.3mg/m2 days 1,4,8,11 every 21 days
May be given weekly for patients with PN or other ongoing side effect(s) and for frailer patients; dose may also be reduced to 1.0 mg/m2. Patients should be given antiviral prophylaxis for herpes zoster (shingles) infection.
PATIENT SUPPORT:
Takeda Oncology 1866-835-2233
https://www.velcade.com/support-andresources
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
Proteasome inhibitor carfilzomib
Kyprolis® (Amgen)
As a single agent for adult pts w/ RRMM who have received at least 1 or more prior lines of therapy including bortezomib and an IMiD® and have demonstrated disease progression on or within 60 days after last therapy. For the treatment of adult pts with RRMM who have received one to three lines of therapy in combination with dexamethasone; or lenalidomide and dexamethasone; or daratumumab and dexamethasone.
ROUTE OF ADMINISTRATION, DOSE SIDE EFFECTS
IV: 10-minute infusion twiceweekly on 2 consecutive days for 3 weeks out of every 4-week cycle 20mg/m2 cycle 1, days 1+2; 27mg/m2 cycle 1 days 8,9,15,16 and all future cycles
Fatigue, anemia, thrombocytopenia, shortness of breath, diarrhea, fever, low blood pressure, cardiac failure and other cardiac events, infusion reactions, embryofetal toxicity
Patients with pre-existing heart conditions may be at greater risk for cardiac complications. Outperformed Vel/dex in RRMM for PFS, OS regardless of age, cytogenetics, prior Rx. Patients should receive antiviral prophylaxis for herpes zoster (shingles) infection.
PATIENT SUPPORT: AMGEN
1-888-427-7478
https://www.amgenassist360.com/patient/
Proteasome inhibitor
ixazomib
Ninlaro® (Takeda)
In combination with Rev/dex for treatment of patients with MM who have received at least 1 prior therapy
Oral: 4mg on days 1,8,15 of a 28-day cycle
Thrombocytopenia, neutropenia, diarrhea, constipation, nausea, vomiting, peripheral neuropathy, peripheral edema (swelling of the feet) rash, liver toxicity, back pain, upper respiratory tract infection
Dose at 3 mg for pts with moderate to severe liver or kidney impairment. Causes embryo-fetal toxicity.
Patients should receive antiviral prophylaxis for herpes zoster (shingles) infection.
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
DRUG TYPE GENERIC NAME BRAND NAME
Monoclonal antibody (mAb) daratumumab
Darzalex® and Darzalex Faspro® (Janssen)
CD38-directed therapy for multiple myeloma
IV: in combination with lenalidomide and dexamethasone in newly diagnosed patients who are ineligible for autologous stem cell transplant (ASCT) and in patients with relapsed or refractory multiple myeloma who have received at least 1 prior therapy; in combination with bortezomib, melphalan and prednisone in newly diagnosed patients who are ineligible for ASCT; in combination with bortezomib, thalidomide, and dexamethasone in newly diagnosed patients who are eligible for ASCT; in combination with bortezomib and dexamethasone in patients who have received at least 1 prior therapy; in combination with carfilzomib and dexamethasone in patients with relapsed or refractory multiple myeloma who have received 1 to 3 prior lines of therapy; in combination with pomalidomide and dexamethasone in patients who have received at least 2 prior therapies including
ROUTE OF ADMINISTRATION, DOSE SIDE EFFECTS REMARKS
IV: 16mg/kg weekly for cycles 1-8, every 2 wks cycles 9-24, every 4 wks cycle 25 onward
Injection: 1,800 mg and 30,000 units hyaluronidase given by a healthcare provider under the skin in the stomach area (abdomen) over 3-5 minutes *Different dosing schedules are used for different combinations; please refer to the prescribing information for more detail
Injection: Serious allergic reactions and other severe systemic administrationrelated reactions, injection site reactions, decreases in blood cell counts, changes in blood tests, upper respiratory infection, fatigue, nausea, diarrhea, shortness of breath, trouble sleeping, fever, cough, muscle spasms, back pain, vomiting, cold-like symptoms, peripheral neuropathy, constipation, pneumonia
IV: Patients must be premedicated prior to infusion to reduce/prevent infusion reactions. Patients should receive antiviral prophylaxis for herpes zoster (shingles) infection. Can affect the results of blood tests to match blood type. Interference with SPEP and IFE tests.
Injection: Patients must be premedicated and post medicated. Patients should receive antiviral prophylaxis for herpes zoster (shingles) infection. Tell your HCP if you have a history of breathing problems, have had shingles, have had or might have a hepatitis B infection, are pregnant or plan to become pregnant, are breastfeeding or plan to breastfeed. Darzalex Faspro™ may harm your unborn baby and it is not known if it passes into your breast milk. Can affect the results of blood tests to match blood type. Interference with SPEP and IFE tests. Is contraindicated in patients with a history of severe hypersensitivity to daratumumab hyaluronidase or any of the components of the formulation.
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
lenalidomide and a PI; as monotherapy, in patients who have received at least three prior lines of therapy including a PI and an immunomodulatory agent or who are doublerefractory to a PI and an IMid
Injection: In combination with Rd or VMP for newly diagnosed ASCTineligible pts; in combination with VTd in newly dx’d patients eligible for ASCT; in combination with bortezomib and dexamethasone in patients who have received at least one prior therapy; in combination with pomalidomide and dexamethasone in patients who have received at least one prior line of therapy including lenalidomide and a proteasome inhibitor; in combination with carfilzomib and dexamethasone in patients with relapsed or refractory multiple myeloma who have received one to three prior lines of therapy; as monotherapy for pts who have had 3 or more prior lines of therapy if prior therapies included a PI or an IMiD or who are double-refractory to a PI and an IMiD.
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
Monoclonal antibody (mAb)
elotuzumab
Empliciti® (BMS)
Monoclonal antibody (mAb)
isatuximab
Sarclisa® (Sanofi Genzyme)
SLAMF7-directed therapy for multiple myeloma
In combination with lenalidomide and dex after 1-3 prior therapies.
In combination with pomalidomide and dex after at least 2 prior therapies including lenalidomide and a proteasome inhibitor
CD38-directed therapy for multiple myeloma
In combination with pomalidomide and dexamethasone to treat adults who have received at least 2 prior therapies, including lenalidomide and a proteasome inhibitor, to treat multiple myeloma
in combination with carfilzomib and dexamethasone, for the treatment of adult patients with relapsed or refractory multiple myeloma who have received 1 to 3 prior lines of therapy.
IV: 10mg/kg once weekly in a 28-day cycle for cycles 1+2; thereafter every other week, days 1 and 15, every 28 days
Patients should receive anti-thrombotic prophylaxis (type determined by risk factors) for the combination with Rd due to high incidence of deep vein thrombosis and pulmonary embolism. Patients must be premedicated before each dose to prevent infusion reactions.
Patients must be premedicated before each dose to prevent infusion reactions. Can affect the results of blood tests to match blood type. Interference with SPEP and IFE tests. Monitor patients for development of second primary malignancies. Potential for embryo-fetal toxicity.
PATIENT SUPPORT: Sanofi Genzyme 1-833-930-2273
https://www.sanoficareassist.com/sarclisa
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
DRUG TYPE GENERIC NAME BRAND NAME INDICATION
Nuclear export inhibitor selinexor
Xpovio® (Karyopharm)
In combination with bortezomib and dexamethasone for the treatment of adult patients with multiple myeloma who have received at least one prior therapy.
In combination with dexamethasone for the treatment of adult patients with relapsed or refractory multiple myeloma who have received at least four prior therapies and whose disease is refractory to at least two proteasome inhibitors, at least two immunomodulatory agents, and an anti-CD38 monoclonal antibody
ROUTE OF ADMINISTRATION, DOSE SIDE EFFECTS
XVd Oral: 100 mg (five 20mg tablets) taken orally once weekly on Day 1 in combination with bortezomib and dexamethasone
Xd Oral: 80mg (four 20mg tablets) taken in combination with dexamethasone on Days 1 and 3 of each week until disease progression or unacceptable toxicity
Doctor must carefully monitor blood counts and body weight at baseline and during treatment, especially during the first two months of treatment. Patients should receive a prophylactic anti-nausea agent prior to and during treatment.
PATIENT SUPPORT: Karyopharm
1-877-527-9493
https://www.karyforward.com
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
ROUTE OF ADMINISTRATION, DOSE SIDE EFFECTS REMARKS
BCMA-directed therapy for RRMM. Indicated for the treatment of adult patients with relapsed or refractory multiple myeloma who have received at least 4 prior therapies including an anti- CD38 monoclonal antibody, a proteasome inhibitor, and an immunomodulatory agent
IV:
Blenrep is not currently available for prescribing.
The most common side effects of BLENREP include vision or eye changes such as findings on eye exam (keratopathy), decreased vision or blurred vision, nausea, low blood cell counts, fever, infusionrelated reactions, tiredness, and changes in kidney or liver function blood tests. Conduct ophthalmic examinations (visual acuity and slit lamp) at baseline, prior to each dose, and promptly for worsening symptoms. Advise patients to use preservative-free lubricant eye drops at least 4 times a day starting with the first infusion and continuing until end of treatment.
GSK initiated voluntary withdrawal of Blenrep as requested by the FDA based on results from the DREAMM-3 phase III clinical trial which did not meet the requirements of US FDA Accelerated Approval regulations. Patients already enrolled in the Blenrep Risk Evaluation and Mitigation Strategy (REMS) program will have the option to enroll in a compassionate use program to continue access to treatment. Patients on Blenrep should consult their healthcare provider.
Initiation of the Process of Voluntary Withdrawal of the Biologic License Application for BLENREP®
GlaxoSmithKline - 1-877-768-0092
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
CAR T-cell therapy Idecabtagene vicleucel
Abecma® (BMS and bluebird bio)
Abecma is a B-cell maturation antigen (BCMA)-directed genetically modified autologous T cell immunotherapy indicated for the treatment of adult patients with relapsed or refractory multiple myeloma after two or more prior lines of therapy, including an immunomodulatory agent, a proteasome inhibitor, and an antiCD38 monoclonal antibody.
ROUTE OF ADMINISTRATION, DOSE SIDE EFFECTS REMARKS
The patient’s own T cells are genetically modified to recognize and attack BCMA on the surface of the patient’s myeloma cells.
Before giving you Abecma, your doctor will prepare your body by giving you chemotherapy for 3 days. Your Abecma dose is administered by an intravenous infusion given in one or more infusion bags. The infusion usually takes up to 30 minutes for each infusion bag. For at least 7 days after the infusion you will be monitored daily at the certified healthcare facility where you received your treatment. Premedicate with acetaminophen and an H1-antihistamine. Avoid prophylactic use of dexamethasone or other systemic corticosteroids.
The safety profile of Abecma is well-established and predictable, including cytokine release syndrome (CRS) and neurologic toxicities that are mostly low-grade with early onset and resolution.
The most common side effects of Abecma are fatigue, fever of 100.4°F/38°C or higher, chills or shivering, severe nausea or diarrhea, decreased appetite, headache, dizziness or lightheadedness, confusion, difficulty speaking or slurred speech, cough, difficulty breathing, and fast or irregular heartbeat.
Cytokine Release Syndrome (CRS), neurologic toxicities, Hemophagocytic Lymphohistiocytosis/Macrophage Activation Syndrome (HLH/MAS), hypersensitivity reactions, infections, prolonged cytopenias, hypogammaglobulinemia, secondary malignancies, effects on ability to drive and use machines
Patients must follow a Risk Evaluation and Mitigation Strategy (REMS) called ABECMA REMS
PATIENT SUPPORT: BMS
1-888-805-4555 https://www.celltherapy360.com
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
CAR T-cell therapy ciltacabtagene autoleucel
Carvykti™ (Janssen Oncology and Legend Biotech)
CARVYKTI is a B-cell maturation antigen (BCMA)-directed, genetically modified autologous T cell immunotherapy indicated for the treatment of adult patients with relapsed or refractory multiple myeloma after one or more prior lines of therapy, including a proteasome inhibitor, an anti-CD38 monoclonal antibody and are refractory to lenalidomide
ROUTE OF ADMINISTRATION, DOSE SIDE EFFECTS
CARVYKTI is made from a patient’s own white blood cells, collected and reprogrammed to find and attack multiple myeloma cells. It is given to the patient over 30-60 minutes in a one-time, single-dose infusion of chimeric antigen receptor (CAR)-positive viable T cells in one infusion bag. Before you get CARVYKTI, your healthcare provider will give you chemotherapy for 3 days to prepare your body. After getting CARVYKTI, you will be monitored at the certified healthcare facility where you received your treatment for at least 10 days after the infusion.
The most common nonlaboratory adverse reactions are pyrexia, cytokine release syndrome, hypogammaglobulinemia, hypotension, musculoskeletal pain, fatigue, infections-pathogen unspecified, cough, chills, diarrhea, nausea, encephalopathy, decreased appetite, upper respiratory tract infection, headache, tachycardia, dizziness, dyspnea, edema, viral infections, coagulopathy, constipation, and vomiting. The most common laboratory adverse reactions include thrombocytopenia, neutropenia, anemia, aminotransferase elevation, and hypoalbuminemia.
Cytokine Release Syndrome (CRS), including fatal or life-threatening reactions, occurred in patients following treatment with CARVYKTI. Do not administer CARVYKTI to patients with active infection or inflammatory disorders. Treat severe or life-threatening CRS with tocilizumab or tocilizumab and corticosteroids.
Immune Effector Cell-Associated Neurotoxicity Syndrome (ICANS), which may be fatal or lifethreatening, occurred following treatment with CARVYKTI, including before CRS onset, concurrently with CRS, after CRS resolution, or in the absence of CRS.
Monitor for neurologic events after treatment with CARVYKTI. Provide supportive care and/or corticosteroids as needed. Parkinsonism and Guillain-Barré syndrome and their associated complications resulting in fatal or life-threatening reactions have occurred following treatment with CARVYKTI. (Hemophagocytic Lymphohistiocytosis/ Macrophage Activation Syndrome (HLH/MAS), including fatal and life-threatening reactions, occurred in patients following treatment with CARVYKTI. HLH/MAS can occur with CRS or neurologic toxicities. Prolonged and/or recurrent cytopenias with bleeding and infection and requirement for stem cell transplantation for hematopoietic recovery occurred following treatment with CARVYKTI.
Patients must follow a CARVYKTI REMS program: 1-844-672-0067
PATIENT SUPPORT: Janssen 1-800-559-7875 for MyCARVYKTI Patient Support Program
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
Supportive Care
bisphosphonate pamidronate
Aredia® (generic)
bisphosphonate zoledronate, zoledronic acid
Zometa® (Novartis)
For the treatment of osteolytic bone metastases in conjunction with standard antineoplastic therapy
IV: 4 mg over no less than 15 minutes every 3-4 weeks; usually 3045 minutes once monthly
IV: 90mg infused over 2-4 hours once monthly
IV: 4 mg over no less than 15 minutes every 3-4 weeks; usually 30-45 minutes once monthly
Renal toxicity, fever, vein irritation, general aches and pains, ONJ (osteonecrosis of the jaw)
Long-term use (5+ years) can lead to atypical fractures of the femur; patients without documented myeloma-related bone disease should not take bisphosphonates
Bone-modifying agent denosumab
Xgeva® (Amgen)
Prevention of skeletalrelated events in patients with multiple myeloma
SQ: 120mg every 4 weeks as a subcutaneous injection in the upper arm, upper thigh, or abdomen
Renal toxicity, fever, vein irritation, general aches and pains, ONJ
Long-term use (5+ years) can lead to atypical fractures of the femur; patients without documented myeloma-related bone disease should not take bisphosphonates; dose should be reduced for patients with renal impairment; 500 mg calcium and 400 IU vitamin D should be taken daily.
All patients should receive calcium and vitamin D.
Oral exam should be done prior to starting treatment.
If a patient stops denosumab, that patient must be given bridging therapy with a bisphosphonate to prevent rapid bone breakdown
PATIENT SUPPORT AMGEN
1-866-822-4832 www.xgeva.com/support-tools
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.
DRUGS IN CURRENT USE FOR MULITPLE MYELOMA
DRUG TYPE GENERIC NAME BRAND NAME INDICATION
Supportive Care
Stem cell mobilizer plerixafor
Mozobil® (Genzyme)
Stem cell mobilizer motixafortide
Aphexda® (BioLineRX)
Reversible CXCR4 antagonist for use in combination with GCSF to mobilize hematopoietic stem cells prior to ASCT in patients with NHL or MM
Reversible CXCR4 antagonist for use in combination with GCSF to mobilize hematopoietic stem cells prior to ASCT in patients with MM.
ROUTE OF ADMINISTRATION, DOSE SIDE EFFECTS REMARKS
SQ: Weight-based daily dosing, given approximately 11 hours prior to each apheresis
<83 kg: 20mg fixed-dose or a dose based on 0.24mg/kg body weight
83-160kg: 0.24mg/kg body weight
>160kg: fixed-dose at 40mg
SQ: 1.25mg/kg body weight given as a slow injection, 10-14 hours prior to first apheresis.
A second dose can be administered 10 to 14 hours before a third apheresis, if necessary
Nausea, vomiting, diarrhea, tiredness, headache, dizziness, joint or muscle pain, injection site reaction, low platelets
May cause embryo-fetal harm
May be scheduled or used “on demand”
Injection site reactions (73%) including pain, redness, and itching at the injection site; itching (38%); flushing (33%); back pain (21%), hypersensitivity reaction.
May cause embryo-fetal harm. Motixafortide should not be used in people with leukemia.
Premedicate all patients before each dose of this drug to reduce the risk of hypersensitivity and injection site reactions. Administer approximately 30 to 60 minutes before injection of this drug:
• Diphenhydramine (12.5 mg IV or 25 mg to 50 mg orally, or another H1-antihistamine)
• H2 blocker (e.g., famotidine)
• Leukotriene inhibitor (e.g., montelukast)
• The addition of an analgesic medication (e.g., acetaminophen) to the premedication regimen is recommended.
PATIENT SUPPORT
BioLineRx Connect 866-524-5646
*This document is not an exhaustive list of all drugs used in multiple myeloma. The IMF encourages you to consult with your healthcare team for all drug recommendations.