Executive Summary
The health care system in the United States (US) is currently transitioning toward value based care (VBC), an approach that links payment to quality and value. Despite this trend, significant gaps and barriers remain that challenge widespread engagement in value based oral healthcare (VBOHC). Notably, dental provider and payer engagement is necessary for successful implementation of VBOHC. Insight into dentist and payer perceptions and experiences related to VBOHC is necessary to understand the current state of the transition and identify barriers and opportunities to increase VBOHC participation.
To that end, Discern Health collaborated with GlaxoSmithKline (GSK) Consumer Health (now Haleon) and The Gerontological Society of America (GSA) to develop a survey and qualitative interview guide to investigate VBOHC perceptions, experiences, and challenges. This report discusses the combined results of a survey and in depth interviews as well as the implications for the VBOHC landscape. Findings show that while there are barriers to overcome, VBOHC is becoming more prevalent and expected to be a standard of practice. Key insights uncovered during this project include:
Need for greater dissemination of educational information on VBOHC evidence based models and best practices from trusted sources of authority
Consistent incentives that reward dental providers are required for widespread VBOHC engagement
Limited use of diagnostic coding and exchange of electronic data with external providers hinders collaboration with medical care delivery and quality measure reporting capabilities
Integrated medical and dental care delivery helps to improve access to oral health care, reduce disparities, and improve patient outcomes
Moving forward, collaboration among all dental health stakeholders and VBOHC education and exposure should be prioritized to advance VBOHC in the US.
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 5
Introduction
The United States (US) health care system has been steadily shifting towards paying providers based on the quality of care they provide, instead of the volume of services, through the implementation of value based programs and payment models. The transition to value based care (VBC) supports the Centers for Medicare & Medicaid Services’ (CMS’) triple aim of providing better care for individuals, improved population health, and reduced costs.1
Despite the growing popularity of VBC in medical care, value based oral health care (VBOHC) trails the medical field because of factors such as lack of medical dental integration.2 Nevertheless, VBOHC is gaining more traction due to rising oral health care costs, enduring and profound oral health disparities, and variability in quality of oral health care.3 In particular, the high cost of dental care contributes to oral health disparities and represents a major access barrier for adults and seniors, as evidenced by the 59% increase of dental care expenditures per capita for the US geriatric population between 1996 and 2016.4
A major challenge for the transition to VBOHC is the hesitancy among the US dentist population, as dental provider buy in is key to successfully advance VBOHC.5 Dentists are ideally positioned to lead VBOHC initiatives because of their direct, on the ground experience, deep understanding of the field, and trust within the dental community. In addition to dentists, dental payers are central to this transition as they are responsible for developing and implementing VBC arrangements. Gathering and assessing the perceptions, experiences, and knowledge of VBOHC from these two groups is foundational to understand where we are in the journey towards VBOHC, and what is needed to achieve this goal. These learnings can inform targeted strategies by policy leaders and other oral health stakeholders to increase dental provider and payer engagement in VBOHC and drive momentum towards VBOHC.
Methods
This study employed a mixed methods approach that included a quantitative survey and qualitative interviews. Data collection for both methods was conducted concurrently.
Quantitative Survey
A quantitative survey was fielded between April 22 26, 2022 using an online survey platform. The survey was comprised of a variety of question formats, including ranking, select all that apply, sliding scales, and level of agreement questions. Screener questions were used to restrict respondents to general dentists with an active license, those between the ages of 18 to 75, and those who see a minimum of five patients at their practice in a typical day, and those without affiliation to an advertising
1 CMS. Value based Programs. https://www.cms.gov/Medicare/Quality Initiatives Patient Assessment Instruments/Value Based Programs/Value Based Programs. Updated March 2022.
2 Esselman, K., et al. Using Quality Tactics to Advance Value Based Oral Healthcare. https://www.discernhealth.com/wp content/uploads/2022/01/Oral Health Convening White Paper 2022 01 10.pdf Published January 2022.
3 Glassman P. Oral Health Quality Improvement in the Era of Accountability. Pacific Center for Special Care, University of the Pacific Arthur A. Dugoni School of Dentistry. https://dentaltherapyresourceguide.wkkf.org/resources/resource/oral health quality improvement in the age of accountability/. Published December 2011.
4 Hung M, Lipsky MS, Moffat R, et al. Health and dental care expenditures in the United States from 1996 to 2016. PLoS One. 2020;15(6):e0234459. https://doi.org/10.1371/journal.pone.0234459.
5 See n. 2, Supra.
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 6
agency. Outreach was conducted to 150 individuals. A total of 50 individuals were excluded due to questions posed in the screener, the final sample size was 100 respondents.
The survey included 9 demographic (e.g., gender, race and ethnicity) and background questions (e.g., practice type) and 11 content questions related to the following general content areas:
VBOHC experiences, perceptions, and engagement
Medical dental integration education and challenges
Use of diagnostic coding and interoperability
For a full list of survey questions, please see Appendix A
Qualitative Interviews
Discern conducted one hour semi structured, in depth interviews with dental payers and providers using the discussion guides in Appendix C. The study employed a double blinding method to prevent biased responses and allow for open dialogue. In total, Discern completed 15 interviews with 9 dental providers and 6 payers from various US geographic regions and practice settings (Table 1).
Table 1: Qualitative Interview Participant Demographics
Interviewee Type
Dental Providers
Payers
Regions (N) & Settings (N)
• Midwest (3), Northwest (1), Southwest (2), West Coast (2), East Coast (1)
• Community health center (4), Private practice (2), Academic (2), Center for Dental Health (1)
• East Coast (1), Midwest (2), West (2), National (1)
• Commercial medical/dental (2), Commercial dental (3), All payer (1)
Interviews Conducted
9
6
Totals 15
Results
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 7 Quantitative Survey Results
Table 2 provides an overview of demographics from the 100 dentists surveyed. Most respondents were male (71%), between the ages of 45 64 years (65%), and had been practicing dentistry for 21 years or more (71%). Most respondents (72%) identified as White/ Caucasian. There was even representation across US regions. This is largely representative of the U.S. dental workforce; however female dentists
are slightly under represented in survey respondents. The American Dental Association estimated that in 2020 34.5% of dentists were female while only 29% of survey respondents identified as female.6
About half (53%) of the surveyed dentists work in a solo practice operated by one dentist and serve adult patients (91%), and the majority work in suburban settings (64%).
Table 2. Survey Sample Demographics (N=100)
Demographic Category Participants (%)
Age Bracket
25 34 years
Gender
Race
Ethnicity
Region
Practice Type
2%
35 44 years 19%
45 54 years 29% 55 64 years 36% 65 75 years 14%
Male 71% Female 27%
Prefer not to respond 2%
White/ Caucasian 72%
Black/ African American 3% Asian/ Pacific Islander 13% American Indian/ Alaska Native 0% Other or Multiracial 6% Prefer not to answer 6%
Hispanic 4% Non Hispanic 89% Prefer not to respond 7%
South 31% West 24% Midwest 24% Northeast 21%
3%
9%
17%
32%
39%
Solo practice (operated by one dentist) 53%
6 Health Policy Institute, American Dental Association. The Dentist Workforce Key Facts. https://www.ada.org/ /media/project/ada organization/ada/ada org/files/resources/research/hpi/hpigraphic_0221_1.pdf?rev=1829a4f788c14974a1ac89ff1e288c0f&hash=A27C6AD199EB6FCA B15DB069BAF0CC85. Published February 2021.
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 8
Years Practicing Dentistry 0 5
6 10
11 20
21 30
31+
Demographic Category
Participants (%)
Small group practice (operated by multiple dentists at one location) 28%
Large group practice (operated by multiple dentists at multiple locations) 12%
Multispecialty group practice 6% Other (nonprofit dental center) 1%
Practice Setting
Suburban 64% Urban 28% Rural 8%
Primary Population Served
Children and/ or adolescents (ages <18) 5%
Adults (18 64) 91%
Older adults (ages 65+) 4%
Specific Work Environments
Integrated Delivery Network/ System 13%
Federally Qualified Health Center (FQHC) 2%
Patient Centered Medical Home (PCMH) 4%
Dental safety net provider 6%
Accountable care organization (ACO) 0%
None of the above 75%
Value based Oral Health Care
The majority (91%) of respondents were not currently participating in VBC arrangements; however, among this group, about half (43%) were interested in participating in VBC arrangements in the future. Most dentists reported that their respective dental practice understands how oral health care fits into VBC (61%) and agree that VBC has the potential to improve oral health care for their patients (60%).
Many dentists were ambivalent about VBOHC (selecting either slightly disagree or slightly agree). Most dentists (70%) did not feel that their practice was incentivized to participate in VBC, with 20% strongly disagreeing with this statement. Figures 1‐3 below show the level of agreement with these statements across respondents.
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 9
Figure 1. Responses to “Indicate your level of agreement with the following statement: My practice understands how oral health care fits into VBC”


"My practice understands how oral health care fits into VBC" (N=100)
Percent of Dentists (%)
40
30
20
10
0
24%
16% 19%
4%
Strongly Disagree DisagreeSlightly DisagreeSlightly AgreeAgreeStrongly Agree
Level of Agreement
25% "VBC has the potential to improve oral health care for my patients" (N=100)
Figure 2. Responses to “Indicate your level of agreement with the following statement: VBC has the potential to improve oral health care for my patients.”
30
20
10
34% 19% 7% 0
Percent of Dentists (%)
40 Strongly Disagree DisagreeSlightly DisagreeSlightly AgreeAgreeStrongly Agree





40
30
20
10
9% 14% 17%
Level of Agreement
12% 20%
Figure 3. Responses to “Indicate your level of agreement with the following statement: My practice is incentivized to participate in VBC.”

31% 19% “My practice is incentivized to participate in VBC” (N=100)


21%
2% 0
Strongly DisagreeDisagreeSlightly DisagreeSlightly AgreeAgreeStrongly Agree
Level of Agreement
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 10 Percent of Dentists (%)





7%
Slightly less than half of respondents (45%) reported using quality measures. Among those who use quality measures (n=45), the primary use was tracking and monitoring quality improvement efforts (49%), followed by establishing and tracking progress toward performance benchmarks (36%). Only a small number of respondents reported utilizing quality measures for provider comparisons (9%) or identifying variations in care (7%). Most measures being used were developed by dental provider practices (78%), followed by measures required by the state(s) they practice in (31%), measures required by payers (20%), Dental Quality Alliance measures (9%), and other measures (7%) such as Accreditation Association for Ambulatory Health care (AAAHC) measures. Slightly more than half of respondents (55%) did not use quality measures. Within this group, 40% had some degree of interest in using quality measures in the future.
Around a third of all dentists (34%) reported no education regarding quality measures. Among the 66% with previous quality measurement education, the most common educational source was continuing dental education (67%). Some respondents noted other education during their DDS or DMD degree (41%), through a specialty/professional society or study club (24%), or another source (8%) such as dental corps training, work at a health management organization (HMO), or during residency.
Most dentists (88%) reported that their practice did not participate in alternative payment models (APMs). For the small number of dentists that reported using APMs (n= 12), the most common model type was pay for performance or pay for reporting (7% of total respondents), followed by shared savings (2%), bundled or capitated payment models (2%), and other APMs (1%). Most dentists (63%) did not have any education regarding APMs. Among dentists with education in this area (n=37), the most common sources of education mirrored the educational sources reported for quality measures: continuing dental education (46%), followed by a specialty/professional society or study club (43%), and during their DDS/ DMD degree education (24%).
Integrated Care
Over half of dentists (62%) had previous education regarding medical dental integration. Among those with medical dental integration education (n=62), the most common sources of education were similar to the sources reported for quality measures and APMs, with continuing dental education (65%) leading, followed by DDS/ DMD degree education (44%), and through a specialty/professional society or study club (34%).
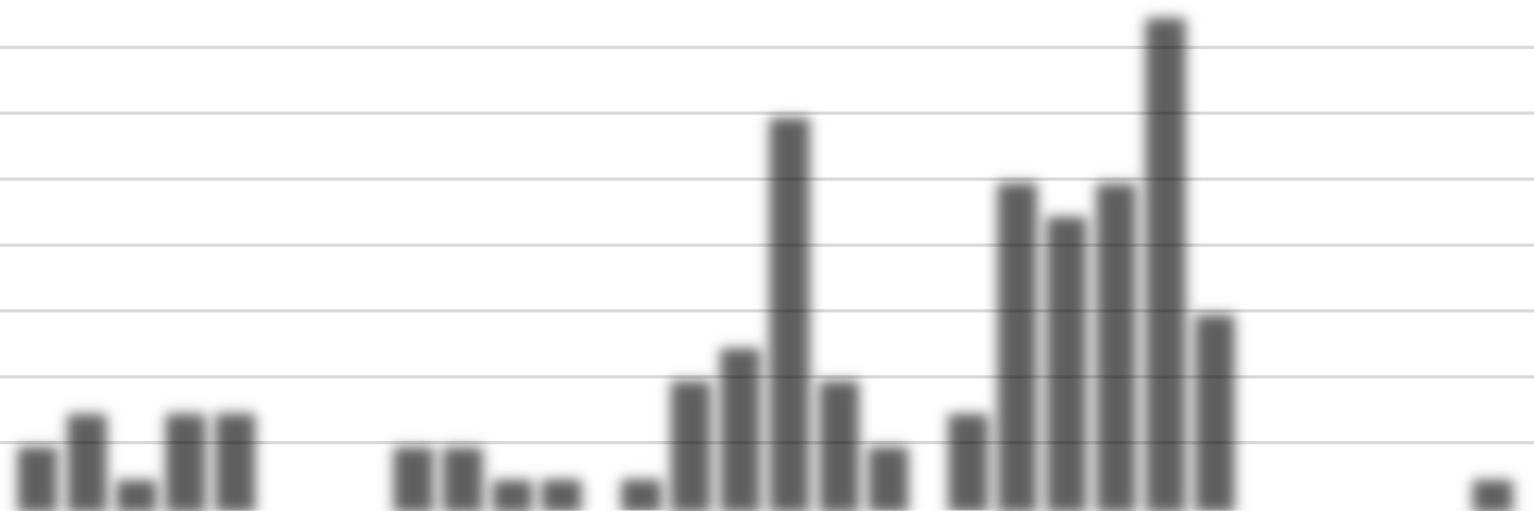
Participants were asked to select and rank the top 3 challenges for medical dental integration. Figure 4 below shows the distribution of ranked answers across the different challenges. Overall, the lack of established models or guidelines was the most selected challenge regardless of rank (47%) and 14% of respondents ranked it as the most challenging. Lack of collaboration between medical and dental practitioners was the most ranked top challenge among respondents (19%) and was the second most reported challenge across all respondents regardless of rank (45%).
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 11
Figure 4. Top 3 Challenges for Providing Integrated Medical and Dental Care
Top 3 Challenges for Providing Integrated Medical and Dental Care
Lack of performance metrics

Variations in medical and dental payer requirements

Lack of established models or guidelines
Challenges
Unclear benefits for my patients
Low utilization of diagnostic codes among dentists
Separation of medical and dental electronic record systems





Interoperability issues with medical and dental coding conventions
Lack of collaboration between medical and dental practitioners
Diagnostic Coding and Interoperability
Number of Responses
Most challenging Second most Third most
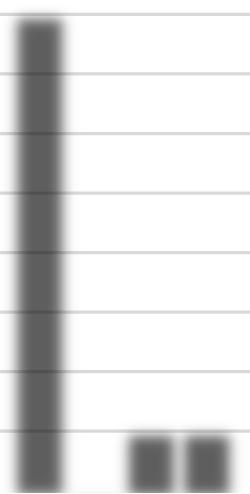
Respondents were asked to select all that apply with regards to their use of diagnostic codes. Most dentists (79%) reported using diagnostic codes in their clinical practice. Figure 5 below shows respondents’ use of diagnostic codes. By far the most common use of diagnostic codes was for dental insurance claims, reported by 61% of respondents. Other uses include to record data in the electronic health record (EHR) (27%), medical insurance claims (25%), communication with external providers (14%), and quality improvement initiatives (12%). The least reported uses among dentists were for quality measure reporting (6%) and recording data in non electronic record systems (7%).
Figure 5. Use of Diagnostic Codes Among Dentists (*question allowed for multiple responses)



Number of Responses

Record data in non electronic systems

Record data in EHR
Communicate with external providers
Dental insurance claims
Medical insurance claims
Uses of Diagnostic Codes
Quality measure reporting
Quality improvement initiatives
I do not use diagnostic codes
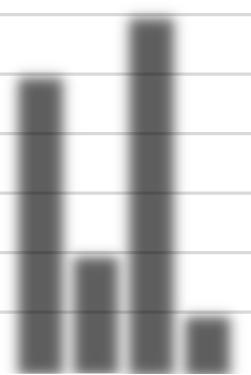
Lastly, the survey investigated potential ways to increase utilization of diagnostic codes among dentists. The survey asked dentists to rank the 3 most helpful options. Figure 6 below shows the different responses for each option. Education on the use and value of diagnostic codes was characterized as the
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 12 Respondents' Use of Diagnostic Codes*
19 12 18 1 13 14 7 6 10 10 12 7 8 15 17 12 16 5 9 9 12 18 10 12 01020304050
7 27 14 61 25 6 12 21 0 10 20 30 40 50 60 70
most helpful way to increase utilization of diagnostic codes among dentists (35%), closely followed by increased dental coverage (32%). Increased dental coverage and education were the most selected across all three ranking options, being selected by 70% and 66% of respondents, respectively.
Figure 6. Top 3 Potential Ways to Increase Utilization of Diagnostic Codes Among Dentists (*question allowed for multiple responses)
Top 3 Potential Ways to Increase Utilization of Diagnostic Codes*
Ways to Increase Utilization of Diagnostic Codes
Financial incentives for quality patient outcomes
Increased dental coverage
Improved information systems
Increased payer requirements
Education
Most helpful
Second most
Third most
Number of Responses
Qualitative Interview Results


The following topics emerged as the key themes from the both the dental payer and provider stakeholder interviews.
There is hesitancy from providers about the transition to VBOHC
One of the most reported barriers to VBOHC identified during the interviews was provider hesitancy. Both payer and provider participants indicated that many dentists, particularly those in private practices, are accustomed to and satisfied with their current payment system and do not feel the desire to implement value based payment models. Additionally, some providers expressed concerns over accountability for their patients’ behaviors, such as non adherence to preventative care and treatment recommendations.
Other concerns mentioned during the interviews included who would be determining quality of care and what “value” means and having payers dictate treatment for patients. There were a few participants that expressed concerns over “benign neglect” as an unintended consequence with a shift to VBOHC. Benign neglect is a concept in which the perception of limited incentives by providers may lead to certain elevated risk or vulnerable populations being deprioritized in favor of meeting quality measure benchmarks and higher reimbursement.
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 13
35 11 11 32 3 16 13 25 23 15 15 9 19 15 32 020406080
There is a need for stakeholder awareness and education to drive VBOHC
Participants indicated that there was a lack of awareness about VBOHC among payers and providers. Payers from both dental specific and integrated medical/dental plans7 described their efforts to implement VBOHC programs, which received varying levels of success in garnering the needed buy in and engagement, whether from providers or internal leadership. One participant from a dental specific payer organization described an initiative that incentivized dentists to utilize a performance scorecard; however, despite offering a bonus pool for being an active user, only about 20% of providers participated in the program. Barriers to program uptake included lack of knowledge on quality measurement and the relation to value based payment, and providers being too busy.
Participants highlighted the need for medical leaders to appreciate the importance of dental health to overall health to increase collaboration with dental stakeholders. A payer participant with prior experience at an integrated medical/dental plan mentioned the challenge they faced in garnering support from medical payer leadership to integrate dental and medical programs and consider the impact of oral health care on disease management. This participant noted that standalone dental payers do not have the same resources as large integrated medical/dental plans and may be more limited in their integration efforts, indicating a need for greater advocacy for dental collaboration with medical plans.
In contrast, a payer from an integrated medical/dental plan described a successful value based arrangement focused on patients with chronic conditions who could benefit from additional dental care. As an integrated medical/dental plan, the organization was in a unique position to invest money on dental coverage and initiatives because they were able to generate a return on investment on the medical services side. Overall, this initiative helped to control dental inflammation among patients and produce better health outcomes. This participant also indicated that their VBOHC programs were well received and generated engagement from the provider community.
Providers revealed that their VBOHC awareness and education primarily came from working in clinics and being involved with professional societies. FQHC and community health dentists attributed their knowledge of VBC due to their exposure working in a collaborative setting with medical providers.
The lack of educational focus on VBOHC and separation of medical and dental curriculums were acknowledged as potential barriers to driving awareness. Two providers interviewed were from academic settings and described the division in medical and dental education. One of the providers expressed that medical health care providers may not appreciate the full benefits of including dentists in overall health care. They explained that some educational initiatives exist to unite the fields but feel that these interdisciplinary programs did not fully integrate dental students. The other academic provider explained that there is a need to teach students to advocate for greater dental coverage and that VBOHC needs to be better integrated into the dental school educational curriculum.
Some participants also expressed the importance of VBOHC education for patients. Participants mentioned that dentistry is often viewed as a procedural health care service and patients could be better educated on the value and importance of oral health to their overall health. Particularly in private
7For the purposes of this report, dental specific plans refer to payers that provide dental benefits only while integrated medical/dental plans that provide both medical and dental benefits.
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 14
practices, patients are a driving force as consumers and patient literacy may help to create a demand for VBOHC that providers will need to meet.
VBOHC initiatives and progress are locally driven
Some of the provider participants described their own efforts to develop quality activities such as practice based quality improvement systems and internal reporting metrics to collect data and analyze trends. These individual efforts were cited as a method to fill a gap in nationally required measurement and quality activities.
Priority populations of interest also varied among participants depending on the needs of their communities. Efforts on care coordination (e.g., referrals) and integrated services (e.g., co location) were primarily reported in FQHC or community health settings. One FQHC provider depicted how their clinic offers an obstetrics package that includes a dental visit for pregnant patients. Another provider mentioned conducting HbA1c testing for patients during dental appointments. Some integrated dental/medical payers have incentivized preventive services based on their population’s needs. For instance, one payer participant described how their integrated organization offers enhanced dental benefits for patients with diabetes, heart disease, cancer, autoimmune diseases, and during pregnancy.
Multiple participants discussed state based initiatives that allowed them to pursue VBOHC activities. States in both the West and Midwestern regions were pointed to as examples where local legislative efforts are used to encourage VBOHC through practice pilot programs. One provider cited that their practice was able to implement a tele dentistry program from the legislative and resource support their state provided. Another provider was involved with their state’s dental collaborative program and elaborated on their success in getting their state to conduct a dental home demonstration project.
Overall, a clear theme emerged from the interviews: local level initiatives and leaders are driving VBOHC. The VBOHC initiatives described and noted in during interview discussions were isolated efforts and not scaled to a national level.
The dental data infrastructure has limitations
The analytic and reporting limitations of dental EHRs were frequently mentioned as barriers to advancing VBOHC. Dental practices tend to use different health record systems than medical practices, which are not typically designed to exchange health information. The interoperability gap presents a challenge for medical/dental integration and hinders care coordination. One provider described the necessity to use a third party software program to pull reports and build dashboards to connect the internal dental and medical records. Another FQHC provider that utilizes the same EHR vendor as their medical colleagues described some of the benefits of having systems that are connected such as using the EHR to align scheduling for same day dental and medical appointments in priority population patients (i.e., infants, pregnant patients, diabetic patients) and eliminate the referral process, which can impact access. Overall, interview participants characterized the use of diagnostic codes by dental providers as extremely limited, making it difficult for payers to evaluate the efficacy of treatments and capture the impact of changes. As one participant stated “value based payment without performance measures doesn’t work.”
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 15
Discussion
Our research illuminates the need for greater dissemination of educational information from trusted sources of authority. This will help to counter provider hesitancy and foster greater stakeholder buy in, which are essential to advancing VBOHC. Across survey responses and interviews, continuing dental education and conferences were the most reported sources for information on VBOHC, revealing an opportunity to increase momentum for VBOHC education through these venues. It is paramount for professional societies to prioritize and disseminate knowledge and resources on VBOHC across the dental and medical communities.
Beyond education about VBOHC, identifying and disseminating evidence based models and best practices is needed to demonstrate the impact of VBOHC. There is a general lack of uniformity in how to execute VBOHC initiatives and what success looks like.8 Sharing lessons learned and innovative strategies from states that are making progress (e.g., Oregon, Minnesota), outcomes based pilot studies, and care delivery organizations driving value in oral care helps create champions for VBOHC adoption9 and generate buy in from providers to modify their current care delivery practices.10 As such, dental providers and others may learn from their peer’s successes and custom fit best practices into their own workflow. Oral health stakeholder collaboration is needed to identify current successful models and develop a framework for implementation of VBOHC models.
As revealed in our quantitative survey, many dentists are not being incentivized to participate in quality measurement or other VBOHC activities. Engagement from dentists will be amplified with consistent incentives that reward providers for keeping patients healthy, preventing dental disease, and coordinating care for their patients will help to achieve value in oral health care.11 The low participation rate in VBC arrangements and APMs is not surprising considering most dentists don’t currently feel they are incentivized to engage in VBOHC. Prior research supports this sentiment, as over two thirds (67%) of key oral health stakeholders (including providers, payers, policy makers, and patient advocates) strongly agree that VBC reimbursement in oral health is necessary to have a successful health care system.12 Payers providing coverage for dental services should consider greater engagement in VBC models and establishing additional methods for incentivizing provider participation.
A key challenge to successfully implementing VBOHC models is the limited use and exchange of electronic data, which hinder the ability to monitor and report on quality measures and outcomes. Within the data infrastructure, limited use of diagnostic codes is a major challenge. Dentistry currently lacks a standardized vocabulary to classify and identify dental diseases13 and interviewees noted that diagnostic codes are not being used by dental providers or required by dental payers. Furthermore,
8 Jivraj A, Barrow J, Listl S. Value Based Oral Health Care: Implementation Lessons from Four Case Studies. J Evid Based Dent Pract. 2022 Jan;22(1S):101662. Doi: 10.1016/j.jebdp.2021.101662. Epub 2021 Nov 6. PMID: 35063180.
9 Northridge ME, Kumar A, Kaur R. Disparities in Access to Oral Health Care. Annu Rev Public Health. 2020 Apr 2;41:513 535. Doi: 10.1146/annurev publhealth 040119 094318. Epub 2020 Jan 3. PMID: 31900100; PMCID: PMC7125002.
10 Center for Health Care Strategies. Moving Toward Value Based Payment in Oral Health Care. Published February 2021.
https://www.chcs.org/media/Moving Toward VBP in Oral Health Care_021021.pdf
11 DentaQuest. What is value based care? What does it mean for oral health care? Published March 27, 2019.
https://whatsnew.dentaquest.com/what is value based care what does it mean for oral health care/
12 Boynes S, Nelson J, Diep V, Kanan C, Pedersen DN, Brown C, et al. Understanding value in oral health: the oral health value based care symposium. J Public Health Dent. (2020) 80:S27–34. Doi: 10.1111/jphd.12402.
13 White JM, Kalenderian E, Stark PC, Ramoni RL, Vaderhobli R, Walji MF. Evaluating a dental diagnostic terminology in an electronic health record. J Dent Educ. 2011 May;75(5):605 15. PMID: 21546594; PMCID: PMC3119719.
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 16
diagnostic codes are contained within the International Classification of Diseases (ICD) 10 structure and is based on medical vocabulary which may not be comprehensive for oral health.14 Discussions of ICD 10 coding utility in dental care across interviewees resulted in mixed views, though there was a general agreement that these were widely underutilized by dental providers. Formal and continuing education needs to be provided to dentists to standardize use of diagnostic codes and their importance to quality measurement and participation in VBOHC.
While greater emphasis is being placed on oral health care, many in the oral health community do not recognize the role and importance of VBC in achieving better oral health care. Medical and dental providers are trained separately and often practice separately.15 However, a greater focus on preventive oral health care and integration in primary care has the potential to improve patient outcomes, such as reducing emergency department visits for dental care and hospitalization for primary systemic diseases (e.g., diabetes), and reduce health care costs.16 Efforts to incorporate interventions at multiple levels can improve access to and quality of services, through implementation of multidisciplinary health care teams that provide patient centered care.17 This can help to narrow gaps in access to oral health and reduce health care disparities. One such example in multidisciplinary care delivery are FQHCs, which are uniquely positioned to provide integrated, patient centered care.18 FQHCs are required to report on dental quality measures to HRSA, encouraging some providers to develop and track their own internal metrics.19 However, integration of oral health into overall health care needs to go beyond FQHCs to see system level improvements in and benefits of medical dental integration.20
The figure below summarizes the key insights garnered from jointly assessing the results of the quantitative survey and the qualitative interviews.
Need for greater dissemination of educational information on VBOHC evidence-based models and best practices from trusted sources of authority
Consistent incentives that reward dental providers are required for widespread VBOHC engagement
Limited use of diagnostic coding and exchange of electronic data with external providers hinders collaboration with medical care delivery and quality measure reporting capabilities
Integrated medical and dental care delivery helps to improve access to oral health care, reduce disparities, and improve patient outcomes
14 Ibid.
15 See n. 12, Supra.
16 Goldstein L, Alshukri M, Trombly R, Dillenber J. Value based payment for oral health in an accountable care organization. Aegis Dental Network, Compendium of Continuing Education in Dentistry. Volume 40, issue 10. (2019). https://www.aegisdentalnetwork.com/cced/2019/11/value based payment for oral health in an accountable care organization
17 See n. 9, Supra.
18 Lee, H., Chalmers, N.I., Brow, A. et al. Person centered care model in dentistry. BMC Oral Health 18, 198 (2018).
https://doi.org/10.1186/s12903 018 0661 9
19 HRSA. Uniform Data System 2022 Manual Health Center Reporting Requirements. https://bphc.hrsa.gov/sites/default/files/bphc/data reporting/2022 uds manual.pdf.
20 See n. 9 , Supra.
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 17
Our research has several limitations. Qualitative interviewees were selected based on their current work and association with VBOHC, which could have resulted in respondent bias. Few perspectives were included from dental providers that are not well versed in VBC arrangements, quality measurement, and/or medical dental integration. Interviewees also included more participants from FQHCs than is representative of the dental provider population. This may have created a bias in the themes that emerged from these discussions. Results from the survey were not assessed for statistical significance, limiting our ability to make definitive statements on associations. Lastly, 70% of survey respondents self identified as White/Caucasian and 71% self identified as Male. While this is representative of the broader dental provider population, 21 it does not fully capture the experiences and perceptions of providers from racial and ethnic minority populations.
We have identified several areas for consideration for future research. Placing an emphasis on reaching a greater diversity of dental providers from minority groups (e.g., Black, Asian, women) and those who are younger and have fewer years of experience practicing dentistry for a quantitative survey is needed to better understand their experiences with VBOHC and uncover potentially unique challenges and key differences with the findings depicted within this report. This would also allow to trend knowledge and attitudes as the dental provider population evolves, with a higher proportion of female dental school graduates, among other changes.22 Variations in dental and medical coverage requirements and the impact on integration of dental and medical care is important to explore further.
Conclusion
While dental providers and payers face challenges, opportunities described in this report offer entry points to advance VBOHC initiatives. A collaborative effort among all stakeholders involved is needed to overcome underlying challenges, including the novelty of VBOHC arrangements and the chasm between dental and medical care. Local initiatives exist that depict successful, integrated models of care—these initiatives should be disseminated to increase education and understanding about VBOHC. The foundation for whole person centered care that incorporates both dental and medical care needs to be further established through interprofessional education curriculums and greater awareness and acceptance among both the dental and medical communities. While there are challenges to overcome to successfully implement VBOHC, it is a worthy cause due to its potential impact on patient care and outcomes.
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 18
21 See n. 6, Supra. 22 See n. 6, Supra.
Appendix A: Survey Questions
Background Questions
1. In which state is your primary practice located?
[INSERT DROP DOWN MENU FOR ALL 50 STATES + DC]
2. Which of the following categories describe your race? Select all that apply:
White / Caucasian
Black / African American
American Indian/ Alaska Native
Asian / Pacific Islander
Other; please specify:
Prefer not to answer
3. Ethnicity
Hispanic
Non Hispanic
Prefer not to respond
4. Which of the below most closely align with your gender identification?
Female
Male
Other; please specify:
Prefer not to respond
5. How many years of experience do you have practicing dentistry?
6. In what setting is your primary practice located?
Rural
Urban
Suburban
7. Which of the following best describes your current work environment as a dentist?
Solo practice (operated by one dentist)
Small group practice (operated by multiple dentists at one location)
Large group practice (operated by multiple dentists at multiple locations)
Multispecialty group practice
Other; please specify:
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 19
0 5 6 10 11 20 21 30 31+
8. Does your dental practice fall under any of the following categories? Select all that apply:
Integrated Delivery Network/ System
Federally Qualified Health Center (FQHC)
Accountable Care Organization (ACO)
Patient Centered Medical Home (PCMH)
Dental safety net provider
Other; please specify:
9. Which of the following age groups accounts for the largest proportion of patients you serve as a dentist?
Older adults (ages 65+)
Adults (ages 18 64)
Children and/or adolescents (ages <18)
VBOHC Awareness and Acceptance
The dental profession is moving toward value based care (VBC), an approach to care that ties reimbursement to the quality and value of care provided (in contrast to traditional approaches to reimbursement based on the quantity of services provided). A key component of VBC is use of quality measures, which capture the quality of care provided and patient outcomes achieved. For example, the Dental Quality Alliance (DQA) has developed quality measures, including measures that evaluate preventive care processes (e.g., “Oral Evaluation”), access to care (e.g., “Usual Source of Services), and care outcomes (e.g., “Ambulatory Care Sensitive Emergency Department Visits for Dental Caries in Children”).
1. Does your dental practice utilize quality measures? Select all that apply:
Yes, to track and monitor quality improvement efforts
Yes, for public reporting purposes
Yes, for alternative payment model arrangements that tie quality of care to provider reimbursement (e.g., pay for performance)
Yes, to identify variations in care
Yes, for provider comparison purposes
Yes, to establish and track progress toward performance benchmarks
Yes, for other reasons; please specify:
No, my practice doesn’t utilize quality measures
2. If yes, which quality measure(s) does your practice utilize? Select all that apply:
Dental Quality Alliance (DQA) measures
Measures developed by my practice
Measures required by payers
Measures required by my state
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 20
I use other quality measures; please specify:
My practice does not utilize quality measures
3. If you do not utilize quality measures, on a scale from 0 10, how interested are you in using quality measures in your dental practice?
0 1 2 3 4 5 6 7 8 9 10
Not at all interested in using quality measures
Neither interested nor disinterested
Very interested and planning to use quality measures in the future
Another component of VBC is use of alternative payment models (APMs). APMs tie provider reimbursement to quality of care provided, as opposed to fee for service reimbursement based on volume of services. The following are examples of APMs that can be used by oral health providers or provider organizations:
a) Shared savings: Providers receive a percentage of the total cost savings for a defined patient population
b) Pay for performance (P4P): Financial rewards or penalties based on quality measure performance benchmarks
c) Pay for reporting: Financial bonuses for reporting data or penalties for not reporting data
d) Bundled payments: Prospective or retrospective payments based on an entire episode of care (e.g., a specific procedure, a time limited condition, or condition specific care management); Payment adjustments are based on quality measure performance
e) Capitated payment models: Prospective payments to providers (per member and per month) covering health services that are based on quality measure performance measured against quality benchmarks
4. Does your practice participate in any alternative payment models (APMs)? Select all that apply:
Shared savings
Pay for performance or Pay for reporting
Bundled or Capitated payment models
My practice does not participate in an APM
Other; please specify:
Another important component for value based oral health care is the integration of medical and dental care. Medical dental integration refers to an approach to care that integrates and coordinates dental medicine into primary care and behavioral health.
5. Indicate how you learned about the following; select all that apply:
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 21
a. I learned about quality measures…
During my education for my DDS/DMD degree
Through continuing dental education
Through a specialty/professional society/ study club
I do not have any education in this area
Other, please specify:
b. I learned about alternative payment models (APMs)…
During my education for my DDS/DMD degree
Through continuing dental education
Through a specialty/professional society/ study club
I do not have any education in this area
Other, please specify:
c. I learned about medical dental integration…
During my education for my DDS/DMD degree
Through continuing dental education
Through a specialty/professional society/ study club
I do not have any education in this area
Other, please specify:
As a reminder, value based care (VBC) rewards dental providers based on the quality and value of care provided. This is in contrast to the traditional model of payment in which dentists are paid based on volume of services performed.
6. Do you currently participate in a value based care arrangement?
Yes
No
7. If no, indicate your level of agreement with the following statement: I am interested in participating in value based care arrangements.
1 2 3 4 5 6
Strongly disagree Disagree Slightly Disagree Slightly Agree Agree Strongly Agree
8. Specify your level of agreement with the following statements:
a. Value based care has the potential to improve oral health care for my patients.
1 2 3 4 5 6
Strongly disagree Disagree Slightly Disagree Slightly Agree Agree Strongly Agree
b. My practice understands how oral health care fits into value based care.
1 2 3 4 5 6
Strongly disagree Disagree Slightly Disagree Slightly Agree Agree Strongly Agree
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 22
c. My practice is incentivized to participate in value based care.
Strongly disagree Disagree Slightly Disagree Slightly Agree Agree Strongly Agree
Integrated Care, Coding, and Interoperability
9. What are the top 3 challenges that your dental practice faces in providing integrated dental and medical care?
Lack of collaboration between medical and dental practitioners
Separation of medical and dental electronic record systems
Interoperability issues stemming from different medical and dental coding conventions
Low utilization of diagnostic codes among dentists
Unclear benefits for my patients
Lack of established models or guidelines
Variations in medical and dental payer requirements
Lack of performance metrics to monitor, evaluate, and improve integration efforts
Other; please specify:
This question is not applicable to my dental practice
10. Indicate functions for which you use diagnostic codes (e.g., ICD 10 codes). Select all that apply:
Record clinical data in non electronic record systems
Record clinical data in the electronic health record
Facilitate communication/ collaboration with external providers
Dental insurance claims
Medical insurance claims
Quality measure reporting
Quality improvement initiatives
I do not use diagnostic codes
Other; please specify:
11. Which of the following would be most helpful to increase utilization of diagnostic codes in your dental practice? Select the top 3 options:
Education on the use and value of diagnostic codes
Increased payer requirements to include diagnostic codes on claim submissions
Improved information systems that capture diagnostic codes within the dentist’s workflow
Increased dental coverage
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 23
1 2 3 4 5 6
Financial incentives for quality patient outcomes that are tracked using diagnostic codes
N/A
Other; please specify:
Additional Opportunities
12. Are there any additional considerations related to the transition to VBC and/ or your ability to participate in VBC arrangements that are important to mention?
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 24
Appendix B: Key Definitions
Alternative Payment Model (APM): “Payment approach that gives added incentive payments to provide high quality and cost efficient care. APMs can apply to a specific clinical condition, a care episode, or a population.” 23
Interoperability: “The ability of different information systems, devices, and applications (systems) to access, exchange, integrate and cooperatively use data in a coordinated manner, within and across organizational, regional, and national boundaries, to provide timely and seamless portability of information and optimize the health of individual and populations globally.”24
Medical Dental Integration: “An approach to care that integrates and coordinates dental medicine into primary care and behavioral health to support individual and population health.”25
Quality: “The degree to which healthcare services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.”26
Quality Measure: “Tools that help us measure or quantify healthcare processes, outcomes, patient perceptions, and organizational structure and/or systems that are associated with the ability to provide high quality healthcare and/or that relate to one or more quality goals for healthcare. These goals include effective, safe, efficient, patient centered, equitable, and timely care.”27
Value‐based Care: “Care delivery model in which providers are rewarded for quality health outcomes rather than the quantity of care delivered. In this approach, providers focus on improving the health of a population of patients by offering care that is focused on prevention, best evidence, and personalization.”28
23 Centers for Medicare & Medicaid Services (CMS). “APMs Overview”. https://qpp.cms.gov/apms/overview
24 Healthcare Information and Management Systems Society (HIMSS). “Interoperability in Healthcare”. https://www.himss.org/resources/interoperability healthcare.
25 DentaQuest. “Medical Dental Integration”. https://dentaquest.com/oral health resources/medical dental integration/.
26 Agency for Healthcare Research and Quality. “Understanding Quality Measurement”. https://www.ahrq.gov/professionals/quality patient safety/quality resources/tools/chtoolbx/understand/index.html
27 CMS. “Quality Measure”. https://www.cms.gov/medicare/quality initiatives patient assessment instruments/qualitymeasures/index.html.
28 DentaQuest. “Value Based Care”. https://dentaquest.com/oral health resources/value based care/
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 25
Appendix C: Interview Discussion Guide Questions
Value based Oral Health Care: Payer Interview Guide Discussion Questions
The questions below are meant to serve as general guideposts for the discussion. We may ask additional follow up questions throughout the interview to clarify a response or obtain more information.
Introduction
Please describe your current roles/responsibilities as they pertain to oral health.
o What is your typical beneficiary demographic (age, race/ethnicity, coverage)?
VBOHC Knowledge and Engagement
How would you describe the trend towards value based care in oral health in your network?
o How would you describe the current payer interest in VBOHC?
How has your organization engaged in value based oral health?
o How does your organization utilize quality measures to improve patient care, determine value for procedures/treatments?
How do you prioritize which quality measures are implemented?
What types of data points would be of most interest to your organization (e.g., structure, process, outcome, patient reported)?
How do current guidelines and evidence affect your prioritization or use of quality measures?
What quality related partnerships or collaborations has your organization engaged in?
o What payment models related to oral health has your organization engaged in?
What methods do you use to incentivize dental providers to engage in value based care?
o What are some challenges or barriers that are preventing payers from implementing value based payment models related to oral health?
What support would be needed (e.g., federal, provider, patient) to overcome those barriers?
Do you have any recommendations on how to address those barriers or challenges?
How would you describe the level of interest in VBOHC among dental providers?
o What percent of participating providers are engaged in VBC? How do you anticipate this trend to change over the next 5 10 years?
o Are there barriers limiting provider participation?
o Do you provide any resources or education around VBOHC for dental providers?
Which population(s) are the top priority for quality improvement in oral health care at your organization?
o How do you identify these priority populations?
o How do you anticipate VBOHC will impact these populations?
o What are potential barriers to developing or implementing VBOHC initiatives to address disparities?
o What would you suggest to reduce those barriers?
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 26
Diagnostic Coding and Interoperability
We have heard that dental systems lag compared to medical systems in consistently collecting diagnostic codes. Can you talk about your experiences with dental diagnostic coding?
o What improvements are needed to enhance the dental information technology infrastructure?
o What is needed to improve coding standardization?
Does your organization require diagnostic codes on claims submissions?
o What codes are required?
o For what purposes are codes required (e.g., service authorization)?
o What are the benefits of dental providers submitting ICD 10 codes?
o Are there any gaps in diagnostic codes?
o What opportunities would increase use of diagnostic codes by dental providers?
o For organizations that don’t require diagnostic codes on claims submissions:
Closing
Has your organization considered implementing diagnostic code requirements in the near future? Why or why not?
As we discussed in our introduction, the US health care system is increasingly beginning to adopt value based oral health care through tactics such as medical dental integration, alternative payment models with oral health incentives, etc. How do you view this change with regards to how it will impact your organization?
How will value based oral health care affect population health overall/in your beneficiary population?
o How will this shift towards value based care impact health equity?
What might be potential unintended consequences on vulnerable populations (e.g., realignment of resources)?
What are your concerns about transitioning to value based oral health care?
What is needed for value based oral health care to be widely and successfully implemented?
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 27
Value based Oral Health care: Provider Interview Guide
Discussion Questions
The questions below are meant to serve as general guideposts for the discussion. We may ask additional follow up questions throughout the interview to clarify a response or obtain more information.
Introduction
Please describe your current roles/responsibilities.
o What type of setting do you work in?
General dentist and chief dental officer
o What is your typical patient demographic (age, race/ethnicity, coverage)?
VBOHC Knowledge and Engagement
How would you describe your level of knowledge regarding value based oral health care?
o What would you say was the most significant source of your knowledge and experience in value based oral health care (e.g., DDS/DMD education, continuing dental education, specialty/professional society resource, study club, etc.)?
How much would you say your education prepared you for value based care in the clinical setting?
What recommendations do you have for how your education or other dental schools could improve their efforts to prepare students?
What resources, materials, or specific issues and topics did you find the most helpful?
How does your practice engage in value based care?
o How do you track oral health quality measures?
What quality measures or data points are most important for you in providing care for your patients?
If not, what might incentivize you to use measures?
What support or resources would you need to start collecting data on quality measures (i.e., technology support)?
How might using measures be useful to you and your practice?
o Do you participate in any value based care arrangements?
How are you incentivized by payers to engage in value based care?
o What are some challenges or barriers that have prevented or limited your engagement?
o Conversely, are there any resources or external factors that have helped your practice’s participation in value based oral health care?
Integrated and Team based Care
How would you describe the relationship between medical and dental health delivery?
o Do you work directly with primary care or other health care providers as part of an integrated team?
What kind of health care providers do you collaborate with? Can you briefly describe the workflow?
What partnerships or collaborations would you suggest to increase team based care? (e.g., data sharing, payment models)
o What are the challenges to medical dental integration?
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 28
Closing
o What recommendations do you have for how medical and dental professionals can work collaboratively to improve patient oral health?
As we discussed in our introduction, the US health care system is increasingly beginning to adopt value based oral health care through tactics such as medical dental integration, alternative payment models with oral health incentives, etc. How do you view this change with regards to how it will impact your practice and how you deliver care to your patients?
How will it affect population health overall/in your patient population?
o How will this shift towards value based care impact health equity?
What might be potential unintended consequences on vulnerable populations (e.g., uneven allocation of resources, lack of focus on outcomes important to patients, increasing health disparities)?
What are your concerns about transitioning to value based oral health care?
What is needed for value based oral health care to be widely and successfully implemented?
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 29
Appendix D: Additional Quantitative Analysis Graphs
Figure D1. Responses to “Indicate your level of agreement with the following statement: I am interested in participating in VBC arrangements.”






“I am interested in participating in VBC arrangements” (n=91)








Dentists
Strongly
Level of Agreement
Figure D2. Utilization of Quality Measures Among Dentists
Does your dental practice utilize quality measures? (N=100)
Yes, to identify variations in care
of Measures
Yes, for provider comparison purposes
Yes, to establish and track progress toward performance benchmarks
Yes, to track and monitor quality improvement efforts
No, my practice doesn't utilize quality measures
Dentists
Figure D3. Utilization of Quality Measures by Measure Type (*question allowed for multiple responses)
Which quality measures do you use? (n=45)*
Type
Number of Responses

Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 30
15% 15% 22% 36% 11% 1% 0 10 20 30 40
DisagreeDisagreeSlightly DisagreeSlightly AgreeAgreeStrongly PercentAgree of
(%)
55% 22% 16% 4% 3%
0204060 Uses
Percent of
(%)
3 14 9 35 4 0102030405060 Other measures Measures required by my state Measures required by payers Measures developed by my practice DQA measures
Measure
Interest in Using Quality Measures












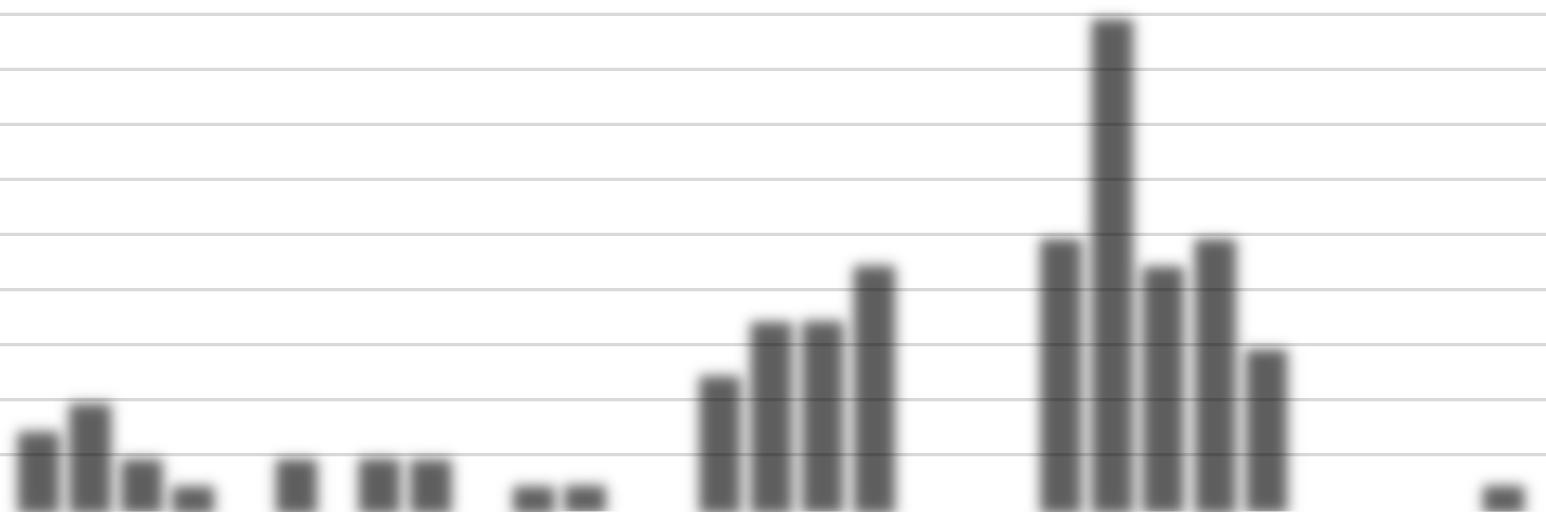
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 31 Figure D4. Interest in Using Quality Measures among Dentists not Currently Using Measures Key: 0 = Not at all interested, 5 = Neither interested nor disinterested, 10 = Very interested and planning to participate in the future Figure D5. Sources of Education Regarding Quality Measures, Medical Dental Integration, and APMs (*question allowed for multiple responses) 9% 2% 4% 2% 4% 40% 15% 9%9% 4% 2% 0 10 20 30 40 50 60 Percentage012345678910 of Dentists Level of Interest
(n=55) 34 5 16 44 27 38 3 21 40 27 63 2 16 17 9 020406080100120140160 No education Other Specialty/ professional society/ study club Continuing dental education DDS/ DMD degree Number of Responses Education Source I learned about quality measures, medical dental integration, and APMs through…* Quality Measures Medical Dental Integration APMs
of Dentists (%)
D6. Participation in Alternative Payment Models (APMs)
APM Participation (N=100)


20
2% 7% 2% 1%
Shared savingsPay for performance or pay for reporting
Stratifications by Practice Type
Bundled or capitated payment models
APM Type
Other APMMy practice does NOT participate in APMs
Figure D7. Responses to “Indicate your level of agreement with the following statement: My practice understands how oral health care fits into VBC,” Stratified by Practice Type
“My practice understands how oral health care fits into VBC," By Practice Type (N=100)
of Responses
Large group practice (n=12)
Multispecialty group practice (n=6) Small group practice (n=28)
Practice Type
Solo practice (n=53)Other (n=1)
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 32 Figure Strongly Disagree Disagree Slightly Disagree Slightly Agree Agree Strongly Agree
88% 0
40 60 80 100
Percent
1 3 2 4 10 3 2 5 9 1 2 12 10 3 1 4 15 1 3 1 2 6 0 2 4 6 8 10 12 14 16
Number
Figure D8. Utilization of Quality Measures, Stratified by Practice Type
Utilization of Quality Measures, By Practice Type (N=100)
Number of Responses
Large group practice (n=12)
Multispecialty group practice (n=6)
Small group practice (n=28)
Practice Type
Solo practice (n=53)
Other (n=1)
Yes, for any reason
No, my practice doesn't utilize quality measures
Figure D9. Different Uses of Quality Measures Among Dentists, Stratified by Practice Type (*question allowed for multiple responses)
Utilization of Quality Measures, By Practice Type (n=45)*
Number of Responses
Large group practice (n=12)
Multispecialty group practice (n=6)
Small group practice (n=28) Solo practice (n=53)
Practice Type
Other (n=1)







Track and monitor quality improvement efforts
Identify variations in care
Establish and track progress toward performance benchmarks
Provider comparison purposes
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 33
10 4 14 17 0 22 14 36 1 0 5 10 15 20 25 30 35 40
8 3 5 6 2 11 6 9 1111 0 1 2 3 4 5 6 7 8 9 10
Figure D10. Interest in Using Quality Measures Among Dentists Not Currently Using Measures, Stratified by Practice Type

Note: 0 = Not at all interested, 5 = Neither interested nor disinterested, 10 = Very interested and planning to participate in the future
Interest in Using Quality Measures, By Practice Type (n=55)
Number of Responses
Level of Interest
Large group practice (n=2)
Multispecialty group practice (n=2)
Small group practice (n=14)
Solo practice (n=36) Other (n=1)
Figure D11. Responses to “Indicate your level of agreement with the following statement: My practice is incentivized to participate in VBC,” Stratified by Practice Type
“My practice is incentivized to participate in VBC,” By Practice Type (N=100)
Number of Responses
Large group practice (n=12)
Multispecialty group practice (n=6)
Small group practice (n=28)
Practice Type
Solo practice (n=53)Other (n=1)
Strongly Disagree Disagree Slightly Disagree Slightly Agree Agree Strongly Agree
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 34
111111 2 5 1 3 1 5 1 2 1 17 2 4 2 111 0 2 4 6 8 10 12 14 16 18 012345678910
3 2 5 10 4 7 18 2 7 9 111 9 10 1 6 2 0 2 4 6 8 10 12 14 16 18 20
Figure D12. Utilization of Diagnostic Codes, Stratified by Practice Type (*question allowed for multiple responses)
Utilization of Diagnostic Codes, By Practice Type (n=79)*
Record clinical data in non electronic record systems
Record clinical data in EHR
Number of Responses
Large group practice (n=8) Multispecialty group practice (n=5)
Small group practice (n=25) Solo practice (n=40) Other (n=1)
Practice Type
Stratifications by Years Practicing Dentistry
Facilitate communication/ collaboration with external providers
Dental insurance claims
Medical insurance claims
Quality measure reporting
Quality improvement initiatives
Figure D13. Responses to “Indicate your level of agreement with the following statement: My practice understands how oral health care fits into VBC,” Stratified by Years Practicing Dentistry
“My practice understands how oral health care fits into VBC,” By Years Practicing Dentistry (N=100)
Number of Responses
years (n=17)21
Years Practicing
(n=32)31+ years (n=39)
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 35
2 1 2 5 4 6 11 1 22 3 7 8 4 20 28 111 10 13 1 22 11 3 2 1 6 0 5 10 15 20 25 30
11 2 1 2 7 6 1 44 55 2 5 8 10 2 4 7 11 111 4 5 0 2 4 6 8 10 12 0 5 years (n=3)6 10 years (n=9)11 20
30 years
Strongly Disagree Disagree Slightly Disagree Slightly Agree Agree Strongly Agree
Figure D14. Responses to “Indicate your level of agreement with the following statement: VBC has the potential to improve oral health care for my patients,” Stratified by Years Practicing Dentistry
“VBC has the potential to improve oral health care for my patients,” By Years Practicing Dentistry (N=100)
Number of Responses
years (n=3)6
years (n=9)11


years (n=17)21
Years Practicing
years (n=32)31+ years (n=39)
Strongly Disagree Disagree Slightly Disagree Slightly Agree Agree Strongly Agree
Stratifications by Geographic Region
Figure D15. Utilization of Quality Measures, Stratified by Geographic Region
Utilization of Quality Measures, By Geographic Region (N=100)
Number of Responses
Geographic Region
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 36
11 3 4 111 3 8 22 8 5 1 3 7 11 12 11 5 4 8 11 3 2 0 2 4 6 8 10 12 14 0 5
10
20
30
7 9 15 14 17 12 16 10 0 5 10 15 20 Midwest (n=24)Northeast (n=21)South (n=31)West (n=24)
Yes, for any reason No, my practice doesn't utilize quality measures
Figure D16. Responses to “Indicate your level of agreement with the following statement: My practice understands how oral health fits into value based care,” Stratified by Geographic Region
"My practice understands how oral health fits into value‐based care," By Geographic Region (N=100)
Number of Responses
Midwest (n=24)Northeast (n=21)South (n=31)West (n=24)
Geographic Region
Strongly Disagree Disagree Slightly Disagree Slightly Agree Agree Strongly Agree
Figure D17. Responses to “Indicate your level of agreement with the following statement: My practice is incentivized to participate in value based care,” Stratified by Geographic Region
"My practice is incentivized to participate in value‐based care," By Geographic Region (N=100)
Number of Responses
Midwest (n=24)Northeast (n=21)South (n=31)West (n=24)
Geographic Region
Strongly Disagree Disagree Slightly Disagree Slightly Agree Agree Strongly Agree
Discern Health | Dental Provider and Payer Perceptions of Value Based Oral Healthcare | August 2022 37
11 2 5 1 7 3 5 6 5 3 7 5 9 4 6 4 5 9 5 4 3 0 2 4 6 8 10
11 2 5 1 7 3 5 6 5 3 7 5 9 4 6 4 5 9 5 4 3 0 2 4 6 8 10







