The latest national and international conference coverage
Top 10 unanswered questions in adults living with type 1 diabetes –a UK and Ireland JLA PSP
GO BEYOND LOWERING LDL-C ADD ON TO REDUCE CV RISK
When statins* and ezetimibe are not enough, add on once daily oral Bempedoic Acid earlier, to help your patients go even further.1,2Δ
* Concomitant use with simvastatin >40 mg daily is contraindicated; please refer to the relevant SmPC for more information.1,2
Δ
Δ NILEMDO® and NUSTENDI® are indicated in adults with established, or at high risk for, ASCVD to reduce CV risk by lowering LDL-C levels, as an adjunct to correction of other risk factors, who are on maximally-tolerated statins, or statin-intolerant, or statin-contraindicated with or without ezetimibe or not adequately controlled with ezetimibe treatment.1,2
NILEMDO® and NUSTENDI® are indicated in adults with established, or at high risk for, ASCVD to reduce CV risk by lowering LDL-C levels, as an adjunct to correction of other risk factors, who are on maximally-tolerated statins, or statin-intolerant, or statin-contraindicated with or without ezetimibe or not adequately controlled with ezetimibe treatment.1,2
▼These medicinal products are subject to additional monitoring. This will allow quick identification of new safety information. Refer to Summary of Product Characteristics (SmPC) prior to prescribing.
Abbreviated Prescribing Information
▼These medicinal products are subject to additional monitoring. This will allow quick identification of new safety information. Refer to Summary of Product Characteristics (SmPC) prior to prescribing.
Presentation: Each Nilemdo film-coated tablet contains 180 mg bempedoic acid. Each Nustendi film-coated tablet contains 180 mg of bempedoic acid and 10 mg of ezetimibe. Indications: Hypercholesterolaemia and mixed dyslipidaemia: Nilemdo/Nustendi are indicated in adults with primary hypercholesterolaemia (heterozygous familial and non-familial) or mixed dyslipidaemia as an adjunct to diet: In combination with a statin (Nilemdo: or statin with other lipid-lowering therapies) in patients unable to reach LDL-C goals with the maximum tolerated dose of a statin; alone or in combination with other lipid-lowering therapies in patients who are statin-intolerant, or for whom a statin is contraindicated (Nustendi: and are unable to reach LDL-C goals with ezetimibe alone). Cardiovascular disease: In adults with established or at high risk for atherosclerotic cardiovascular disease to reduce cardiovascular risk by lowering LDL-C levels, as an adjunct to correction of other risk factors: in patients on a maximum tolerated dose of a statin and not adequately controlled with additional ezetimibe or, in patients who are either statin-intolerant, or for whom a statin is contraindicated (Nustendi in patients already being treated with the combination of bempedoic acid and ezetimibe as separate tablets with or without statin.) Posology and method of administration: The recommended dose is one tablet of 180 mg Nilemdo or 180 mg/10 mg Nustendi taken once daily, with or without food. Tablet should be swallowed whole. Concomitant simvastatin therapy: When Nilemdo/Nustendi are co-administered with simvastatin, simvastatin dose should be limited to 20 mg daily (or 40 mg daily for patients with severe hypercholesterolaemia and high risk for cardiovascular complications, who have not achieved their treatment goals on lower doses and when the benefits are expected to outweigh the potential risks). Coadministration with bile acid sequestrants:
Dosing of Nustendi should occur either at least 2 hours before or at least 4 hours after administration of a bile acid sequestrant. Patients with renal impairment: No dose adjustment is necessary when Nilemdo/Nustendi is administered in patients with mild or moderate renal impairment. Additional monitoring for adverse reactions may be warranted in patients with severe renal impairment and patients with end-stage renal disease (ESRD) on dialysis when Nustendi is administered. Patients with hepatic impairment: No dose adjustment is necessary when Nilemdo/Nustendi is administered in patients with mild hepatic impairment (Child-Pugh A). Treatment with Nustendi is not recommended in patients with moderate (Child-Pugh B) or severe (Child-Pugh C) hepatic impairment due to the unknown effects of the increased exposure to ezetimibe. Contraindications: Hypersensitivity to the active substance or any of the excipients (see SmPC); pregnancy; breast-feeding; concomitant use with simvastatin > 40 mg daily. When Nustendi is co-administered with statin in patients with active liver disease or unexplained persistent elevations in serum transaminases; when Nustendi is coadministered with a statin, consult the SmPC for that particular statin therapy. Warnings and precautions: Potential risk of myopathy with concomitant statins: Bempedoic acid increases plasma concentrations of statins. Patients receiving Nilemdo and a statin should be monitored for adverse reactions that are associated with high doses of statins. Statins occasionally cause myopathy. In rare cases, myopathy may take the form of rhabdomyolysis with or without acute renal failure secondary to myoglobinuria and can lead to fatality. In post marketing experience with ezetimibe, very rare cases of myopathy and rhabdomyolysis were reported. Most patients who developed rhabdomyolysis were taking a statin with ezetimibe. Patients receiving Nilemdo/ Nustendi and a statin should be advised of the potential increased risk of myopathy and told to report promptly any unexplained muscle pain, tenderness, or weakness. If such symptoms occur, a lower maximum dose of the same statin or an alternative statin, or discontinuation of Nilemdo/Nustendi and initiation of an alternative lipidlowering therapy should be considered under close monitoring of lipid levels and adverse reactions. If myopathy is confirmed by creatine phosphokinase (CPK) > 10× upper limit of normal (ULN), immediately discontinue Nilemdo/ Nustendi and any statin. Doses of simvastatin > 40 mg should not be used with Nilemdo/Nustendi. Increased serum uric acid: Bempedoic acid may raise serum uric acid due to inhibition of renal tubular OAT2 and may cause or exacerbate hyperuricaemia and precipitate gout in patients with history of gout or predisposed
Presentation: Each Nilemdo film-coated tablet contains 180 mg bempedoic acid. Each Nustendi film-coated tablet contains 180 mg of bempedoic acid and 10 mg of ezetimibe. Indications: Hypercholesterolaemia and mixed dyslipidaemia: Nilemdo/Nustendi are indicated in adults with primary hypercholesterolaemia (heterozygous familial and non-familial) or mixed dyslipidaemia as an adjunct to diet: In combination with a statin (Nilemdo: or statin with other lipid-lowering therapies) in patients unable to reach LDL-C goals with the maximum tolerated dose of a statin; alone or in combination with other lipid-lowering therapies in patients who are statin-intolerant, or for whom a statin is contraindicated (Nustendi: and are unable to reach LDL-C goals with ezetimibe alone). Cardiovascular disease: In adults with established or at high risk for atherosclerotic cardiovascular disease to reduce cardiovascular risk by lowering LDL-C levels, as an adjunct to correction of other risk factors: in patients on a maximum tolerated dose of a statin and not adequately controlled with additional ezetimibe or, in patients who are either statin-intolerant, or for whom a statin is contraindicated (Nustendi in patients already being treated with the combination of bempedoic acid and ezetimibe as separate tablets with or without statin.) Posology and method of administration: The recommended dose is one tablet of 180 mg Nilemdo or 180 mg/10 mg Nustendi taken once daily, with or without food. Tablet should be swallowed whole. Concomitant simvastatin therapy: When Nilemdo/Nustendi are co-administered with simvastatin, simvastatin dose should be limited to 20 mg daily (or 40 mg daily for patients with severe hypercholesterolaemia and high risk for cardiovascular complications, who have not achieved their treatment goals on lower doses and when the benefits are expected to outweigh the potential risks). Coadministration with bile acid sequestrants: Dosing of Nustendi should occur either at least 2 hours before or at least 4 hours after administration of a bile acid sequestrant. Patients with renal impairment: No dose adjustment is necessary when Nilemdo/Nustendi is administered in patients with mild or moderate renal impairment. Additional monitoring for adverse reactions may be warranted in patients with severe renal impairment and patients with end-stage renal disease (ESRD) on dialysis when Nustendi is administered. Patients with hepatic impairment: No dose adjustment is necessary when Nilemdo/Nustendi is administered in patients with mild hepatic impairment (Child-Pugh A). Treatment with Nustendi is not recommended in patients with moderate (Child-Pugh B) or severe (Child-Pugh C) hepatic impairment due to the unknown effects of the increased exposure to ezetimibe. Contraindications: Hypersensitivity to the active substance or any of the excipients (see SmPC); pregnancy; breast-feeding; concomitant use with simvastatin > 40 mg daily. When Nustendi is co-administered with statin in patients with active liver disease or unexplained persistent elevations in serum transaminases; when Nustendi is coadministered with a statin, consult the SmPC for that particular statin therapy. Warnings and precautions: Potential risk of myopathy with concomitant statins: Bempedoic acid increases plasma concentrations of statins. Patients receiving Nilemdo and a statin should be monitored for adverse reactions that are associated with high doses of statins. Statins occasionally cause myopathy. In rare cases, myopathy may take the form of rhabdomyolysis with or without acute renal failure secondary to myoglobinuria and can lead to fatality. In post marketing experience with ezetimibe, very rare cases of myopathy and rhabdomyolysis were reported. Most patients who developed rhabdomyolysis were taking a statin with ezetimibe. Patients receiving Nilemdo/ Nustendi and a statin should be advised of the potential increased risk of myopathy and told to report promptly any unexplained muscle pain, tenderness, or weakness. If such symptoms occur, a lower maximum dose of the same statin or an alternative statin, or discontinuation of Nilemdo/Nustendi and initiation of an alternative lipidlowering therapy should be considered under close monitoring of lipid levels and adverse reactions. If myopathy is confirmed by creatine phosphokinase (CPK) > 10× upper limit of normal (ULN), immediately discontinue Nilemdo/ Nustendi and any statin. Doses of simvastatin > 40 mg should not be used with Nilemdo/Nustendi. Increased serum uric acid: Bempedoic acid may raise serum uric acid due to inhibition of renal tubular OAT2 and may cause or exacerbate hyperuricaemia and precipitate gout in patients with history of gout or predisposed
to gout. Discontinue Nilemdo/Nustendi if hyperuricaemia accompanied with symptoms of gout appear. Elevated liver enzymes: Liver function tests should be performed at initiation of therapy. Discontinue Nilemdo/Nustendi if increase in transaminases > 3× ULN persists. Renal impairment: Additional monitoring for adverse reactions may be warranted in patients with severe renal impairment (eGFR < 30 mL/min/1.73 m2) or patients with ESRD on dialysis. Hepatic impairment: Periodic liver function tests should be considered for patients with severe hepatic impairment (Child-Pugh C) taking Nilemdo. Nustendi is not recommended in moderate to severe hepatic impairment (Child-Pugh B and C) due to unknown effects of increased exposure to ezetimibe. Fibrates: If cholelithiasis is suspected in a patient receiving Nustendi and fenofibrate, gallbladder investigations are indicated, and therapy should be discontinued. Ciclosporin: Caution when initiating Nustendi in the setting of ciclosporin. Ciclosporin concentrations should be monitored. Anticoagulants: Appropriately monitor INR if Nustendi is added to warfarin, other coumarin anticoagulants, or fluindione. Contraception: Women of childbearing potential must use effective contraception during treatment. Patients should be advised to stop Nilemdo/Nustendi before stopping contraceptive measures if planning to become pregnant. Excipients: Patients with rare hereditary problems of galactose intolerance, total lactase deficiency, or glucose-galactose malabsorption should not take Nilemdo/Nustendi as it contains lactose. Patients at high risk of cardiovascular disease: Evidence for the use of the fixed combination medicinal product of bempedoic acid with ezetimibe in patients at high risk of cardiovascular disease is only available for the lipid-lowering effect in absence of any cardiovascular risk reduction estimation for ezetimibe in primary prevention patients. Driving and use of machines: Nustendi has minor influence on ability to drive and use machines. Dizziness has been reported. Interaction with other medicinal products: Refer to SmPC for full information on interactions. Adverse reactions: Nilemdo: Common (≥ 1/100 to < 1/10): Glomerular filtration rate decreased, anaemia, gout, hyperuricaemia (includes blood uric acid increased), AST increased, pain in extremity. Uncommon (≥ 1/1,000 to < 1/100): weight decreased, haemoglobin decreased, ALT increased, liver function test increased, blood creatinine increased, blood urea increased, Consult Nilemdo SmPC in relation to other adverse reactions. Nustendi: Common (≥ 1/100 to < 1/10): Glomerular filtration rate decreased, anaemia, decreased haemoglobin, hyperuricaemia (includes uric acid increased), decreased appetite, dizziness, headache, hypertension, cough, constipation diarrhoea, abdominal pain, nausea, dry mouth, flatulence, gastritis, liver function test increased (includes liver function test abnormal), back pain, muscle spasms, myalgia, pain in extremity, arthralgia, blood creatinine increased, fatigue, asthenia, gout, AST increased (for bempedoic acid), blood CPK increased. Uncommon (≥ 1/1,000 to < 1/100): weight decreased, ALT increased, blood urea increased, hot flush, dyspepsia, gastrooesophageal reflux disease, AST increased (for ezetimibe), GGT increased, pruritus (with statin), neck pain, muscular weakness (with statin), chest pain, pain, oedema peripheral (with statin). Frequency not known: Thrombocytopaenia, hypersensitivity (including rash, urticaria, anaphylaxis, angio-oedema), depression, paraesthesia (with statin), dyspnoea, pancreatitis, hepatitis, cholelithiasis, cholecystitis, erythema multiform, myopathy / rhabdomyolysis. Consult Nustendi SmPC in relation to other adverse reactions. Legal Classification: POM. Package quantity, marketing authorisation (MA) number: Nilemdo 28 tablets: EU/1/20/1425/002. Nustendi 28 tablets: EU/1/20/1424/002. MA Holder: Daiichi Sankyo Europe GmbH, Zielstattstrasse 48, 81379 Munich, Germany. Further information available on request from Daiichi Sankyo Ireland Ltd. D09 YF97. Telephone: (01) 489 3000. Fax: (01) 489 3033. Email: medinfo@daiichi-sankyo.ie Date of Preparation: May 2024
JOB ID: IE/BIL/05/24/0004
to gout. Discontinue Nilemdo/Nustendi if hyperuricaemia accompanied with symptoms of gout appear. Elevated liver enzymes: Liver function tests should be performed at initiation of therapy. Discontinue Nilemdo/Nustendi if increase in transaminases > 3× ULN persists. Renal impairment: Additional monitoring for adverse reactions may be warranted in patients with severe renal impairment (eGFR < 30 mL/min/1.73 m2) or patients with ESRD on dialysis. Hepatic impairment: Periodic liver function tests should be considered for patients with severe hepatic impairment (Child-Pugh C) taking Nilemdo. Nustendi is not recommended in moderate to severe hepatic impairment (Child-Pugh B and C) due to unknown effects of increased exposure to ezetimibe. Fibrates: If cholelithiasis is suspected in a patient receiving Nustendi and fenofibrate, gallbladder investigations are indicated, and therapy should be discontinued. Ciclosporin: Caution when initiating Nustendi in the setting of ciclosporin. Ciclosporin concentrations should be monitored. Anticoagulants: Appropriately monitor INR if Nustendi is added to warfarin, other coumarin anticoagulants, or fluindione. Contraception: Women of childbearing potential must use effective contraception during treatment. Patients should be advised to stop Nilemdo/Nustendi before stopping contraceptive measures if planning to become pregnant. Excipients: Patients with rare hereditary problems of galactose intolerance, total lactase deficiency, or glucose-galactose malabsorption should not take Nilemdo/Nustendi as it contains lactose. Patients at high risk of cardiovascular disease: Evidence for the use of the fixed combination medicinal product of bempedoic acid with ezetimibe in patients at high risk of cardiovascular disease is only available for the lipid-lowering effect in absence of any cardiovascular risk reduction estimation for ezetimibe in primary prevention patients. Driving and use of machines: Nustendi has minor influence on ability to drive and use machines. Dizziness has been reported. Interaction with other medicinal products: Refer to SmPC for full information on interactions. Adverse reactions: Nilemdo: Common (≥ 1/100 to < 1/10): Glomerular filtration rate decreased, anaemia, gout, hyperuricaemia (includes blood uric acid increased), AST increased, pain in extremity. Uncommon (≥ 1/1,000 to < 1/100): weight decreased, haemoglobin decreased, ALT increased, liver function test increased, blood creatinine increased, blood urea increased, Consult Nilemdo SmPC in relation to other adverse reactions. Nustendi: Common (≥ 1/100 to < 1/10): Glomerular filtration rate decreased, anaemia, decreased haemoglobin, hyperuricaemia (includes uric acid increased), decreased appetite, dizziness, headache, hypertension, cough, constipation diarrhoea, abdominal pain, nausea, dry mouth, flatulence, gastritis, liver function test increased (includes liver function test abnormal), back pain, muscle spasms, myalgia, pain in extremity, arthralgia, blood creatinine increased, fatigue, asthenia, gout, AST increased (for bempedoic acid), blood CPK increased. Uncommon (≥ 1/1,000 to < 1/100): weight decreased, ALT increased, blood urea increased, hot flush, dyspepsia, gastrooesophageal reflux disease, AST increased (for ezetimibe), GGT increased, pruritus (with statin), neck pain, muscular weakness (with statin), chest pain, pain, oedema peripheral (with statin). Frequency not known: Thrombocytopaenia, hypersensitivity (including rash, urticaria, anaphylaxis, angio-oedema), depression, paraesthesia (with statin), dyspnoea, pancreatitis, hepatitis, cholelithiasis, cholecystitis, erythema multiform, myopathy / rhabdomyolysis. Consult Nustendi SmPC in relation to other adverse reactions. Legal Classification: POM. Package quantity, marketing authorisation (MA) number: Nilemdo 28 tablets: EU/1/20/1425/002. Nustendi 28 tablets: EU/1/20/1424/002. MA Holder: Daiichi Sankyo Europe GmbH, Zielstattstrasse 48, 81379 Munich, Germany. Further information available on request from Daiichi Sankyo Ireland Ltd. D09 YF97. Telephone: (01) 489 3000. Fax: (01) 489 3033. Email: medinfo@daiichi-sankyo.ie Date of Preparation: May 2024 JOB ID: IE/BIL/05/24/0004
▼ These medicinal products are subject to additional monitoring. This will allow quick identification of new safety information. Reporting suspected adverse reactions after authorization of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the HPRA Pharmacovigilance Website: www.hpra.ie. Adverse events or a product complaint about a Daiichi Sankyo medicine can also be directly reported to Daiichi Sankyo Ireland Ltd. D09 YF97 by telephone: +353 (1) 4893000
▼ These medicinal products are subject to additional monitoring. This will allow quick identification of new safety information.
Reporting suspected adverse reactions after authorization of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the HPRA Pharmacovigilance Website: www.hpra.ie. Adverse events or a product complaint about a Daiichi Sankyo medicine can also be directly reported to Daiichi Sankyo Ireland Ltd. D09 YF97 by telephone: +353 (1) 4893000
WLatest improvements in endocrinology research and management in the digital age
elcome to the latest annual edition of Update Endocrinology and Diabetology. The revolution has indeed continued for another year in both fields. Rapid advancements in technologies, incretinbased therapies, and improved disease understanding are among the myriad developments that have significantly improved patient outcomes across the spectrum of endocrine disorders on a global scale, while the updated National Clinical Guidelines for Adults with Type 1 Diabetes and Integrated Model of Care for Adults with Type 2 Diabetes are among this year’s achievements at a national level.
Much of this progress was discussed at the recent inaugural Joint Irish-UK Endocrine Meeting 2024, which took place in Belfast in October, and conveyed a very real prospect of achieving disease control beyond mere management in many areas that were traditionally difficult to treat. In this edition of Update we detail highlights from that event which include developments in diabetes care, improved detection of patients with a high fracture risk using artificial intelligence, and updates from the rapidly advancing specialty of bariatric surgery.
The 2024 European Congress of Endocrinology also explored a wide-ranging array of emerging
developments, including improved control of menopause symptoms and outcomes, gestational diabetes and risk identification, and the potential links between body composition and fracture risk. Coverage of the event is also included in this edition.
In clinical articles, Dr Faisal I Almohaileb and Prof Carel le Roux from the Diabetes Complications Research Centre at UCD reflect on the evolution of obesity – once viewed as a disorder of diet and lifestyle and now recognised as a chronic disease – as well as the breakthroughs in treatment strategies that have significantly improved patient outcomes in recent years. Also in obesity care, Advanced Nurse Practitioner Sharon Egan presents positive data from a nurse-led obesity clinic in the general practice setting.
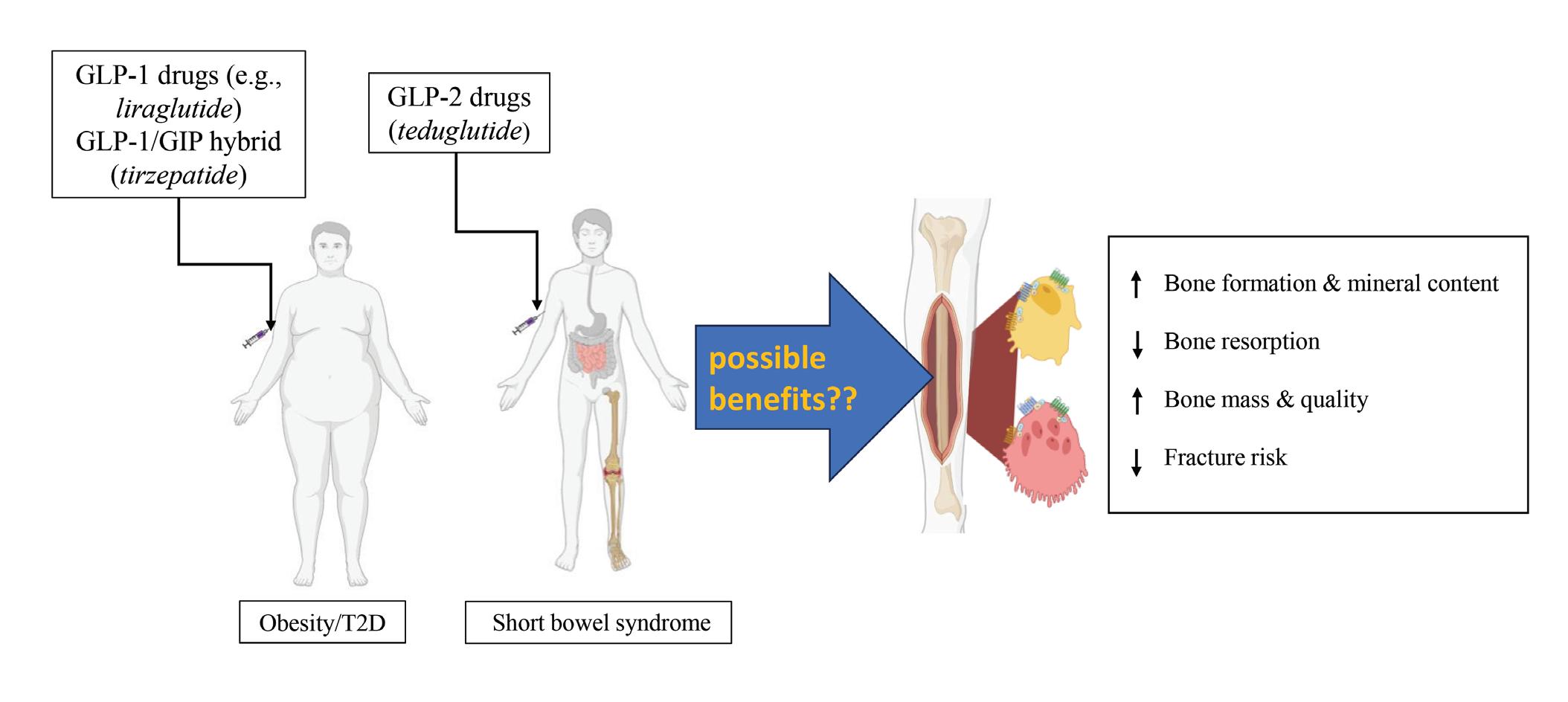
Improved understanding of gut hormones and their wide-reaching effects has now rippled into many areas of healthcare research. Mr Asif Ali, Prof Peter R Flatt, and Prof Nigel Irwin from the Diabetes Research Centre in Northern Ireland summarise the current literature on gut-derived hormones in relation to bone homeostasis, with a particular emphasis on subsequent therapeutic application for bone disease.
The need for a holistic approach that goes beyond medication management of hypothyroidism and Hashimoto’s thyroiditis is examined by Dr Shandeep Momi, who advocates for strategies that encopass nutritional, physical, and psychological wellbeing and presents the data supporting this viewpoint. Dr Momi details the differences between
hypothyroidism and Hashimoto’s thyroiditis, the limitations of conventional management, and explores additional factors such as immune dysregulation, inflammation, and the gut-thyroid axis.
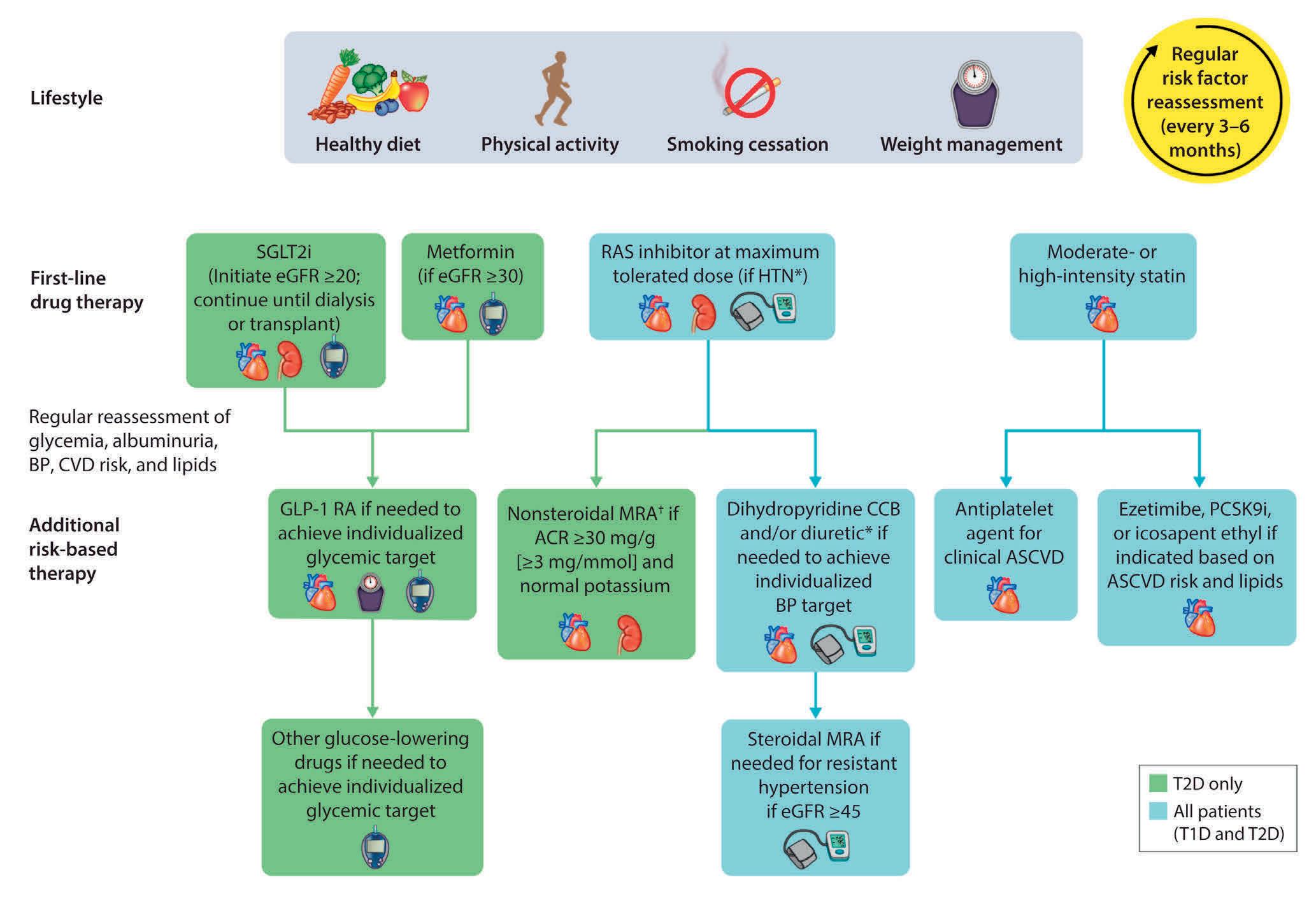
Concerning diabetology, this edition of Update includes a comprehensive overview of diabetic retinopathy and a separate article depicting the management of diabetic nephropathy in patients with type 2 diabetes, with a focus on the most recent KDIGO guidance. Dr Hannah Forde, Consultant Endocrinologist, Beaumont Hospital, Dublin, presents the evolution of technology in the management of type 1 diabetes; and Clinical Specialist Podiatrist Astrid Codemo describes local research investigating the value of accessible vascular assessment tools in diabetic foot disease.
Finally, the top 10 priorities for diabetes research, established through a James Lind Alliance PSP, are described.
Overall, we hope you enjoy another packed and diverse edition of Update Endocrinology and Diabetology We wish all of our readers a happy Christmas and a peaceful New Year.
A large thank you to all our contributors for sharing their knowledge and expertise to promote clinical excellence, evidence-based practice, and optimal patient outcomes throughout 2024. We look forward to bringing you the latest clinical and research updates in 2025. As always, we welcome feedback, suggestions, and new contributors. If you would like to comment or write an article for Update, please contact denise@greenx.ie
A message from Denise Doherty, Editor
3
Highlights from the Joint Irish-UK Endocrine Meeting 2024
8
Coverage of the 2024 European Congress of Endocrinology
11
In focus: Polycystic ovary syndrome
14
Top 10 unanswered questions in adults living with type 1 diabetes –a UK and Ireland JLA PSP
21
The evolution of technology in the management of type 1 diabetes
25
The value of accessible vascular assessment tools in diabetic foot disease: An audit of a tertiary level hospital
29 GIP, GLP-1, GLP-2, and bone
38
The impact of a nurse-led obesity management clinic in general practice
Editor Denise Doherty denise@greenx.ie
Sub-editors
Emer Keogh emer@greenx.ie
Elaine Walsh elaine@greenx.ie
Creative Director
Laura Kenny laura@greenx.ie
Managing Director Graham Cooke graham@greenx.ie
Administration
Daiva Maciunaite daiva@greenx.ie
42
Obesity medication is not only for Christmas but for life
44 A holistic approach to hypothyroidism and Hashimoto’s thyroiditis
48 Management of diabetic nephropathy in patients with type 2 diabetes
53 In focus: Diabetic retinopathy
Update is published by GreenCross Publishing Ltd, First Floor, Ebony House, Main Street, Wicklow Town A67R272
Tel +353 (0)1 441 0024 www.greencrosspublishing.ie
The contents of Update are protected by copyright. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form by any means – electronic, mechanical or photocopy recording or otherwise – whole or in part, in any form whatsoever for advertising or promotional purposes without the prior written permission of the editor or publisher.
Disclaimer
The views expressed in Update are not necessarily those of the publishers, editor or editorial advisory board. While the publishers, editor, and editorial advisory board have taken every care with regard to accuracy of editorial and advertisement contributions, they cannot be held responsible for any errors or omissions contained.
GreenCross Publishing is owned by Graham Cooke
Highlights from the Joint Irish-UK Endocrine Meeting 2024
All
reports: Denise Doherty
The inaugural Joint IrishUK Endocrine Meeting, which took place in the International Cultural Centre, Belfast, from 13-14 October, welcomed a host of leading national and international experts,
clinicians, and guest speakers to a rich and diverse scientific programme, the latest updates in endocrine-related research, and opportunities for multidisciplinary collaboration. Multiple plenaries, symposia, lectures, and posters covered a
The endocrinologist’s role along the cancer journey
The Hadden Lecture was among the many highlights during the Joint Irish-UK Endocrine 2024 Meeting; described by Irish Endocrine Society (IES) President Prof Fidelma Dunne, Professor in Medicine at the National University of Ireland, Galway, Consultant Endocrinologist at Galway University Hospital, as the “highest honour the IES can bestow on a colleague in our field”. The lecture is given in memory of Prof David Hadden, who was a Consultant Physician at the Royal Victoria Hospital and Honorary Professor of Endocrinology at Queen’s University, Belfast. Prof Hadden was instrumental in uncovering the role of diet in type two diabetes, among many other contributions to his field, before his death is 2014, and was as a founding member of the IES.
Prof Maralyn Druce, Consultant Endocrinologist at Barts Health NHS Trust, Professor of Endocrine Medicine at Barts and the London School of Medicine and Dentistry, and Senior
Editor of Clinical Endocrinology, delivered the Hadden Lecture with a talk entitled: ‘The endocrinologist’s role along the patient cancer journey – from pre-diagnosis to survival and vitality and beyond’. She began with a personal and professional tribute to Prof Hadden, adding that he “inadvertently got me started on my journey as an endocrinologist”, when he co-edited a book for which Prof Druce had written a chapter on diabetes in her early career. Quoting his obituary in The Lancet , she said Prof Hadden “was always a gentleman, very open to talk to, and a pleasure to work with”.
The endocrinologist’s role in cancer care
Moving on to her presentation, Prof Druce examined the complexity of the endocrinologist’s role throughout the cancer trajectory and said that overall, “listening, thinking, explaining options to patients, and linking with different
substantial array of specialist and general areas, ranging from the management of adrenal insufficiency, to pituitary health, diabetes and metabolism, thyroid disease, and polycystic ovary disease, among many other areas of endocrine-related health.
members of the multidisciplinary team are perhaps the greatest contribution we can make”. She discussed the different ways that endocrinologists might interface with a cancer journey, such as managing patients with an increased risk of cancer in endocrine organs, patients with proven cancer in endocrine organs, and patients at risk of endocrine injury because of either their cancer or cancer treatment.
Attendees heard several direct quotes from the lived experiences of patients before Prof Druce discussed the limitations of existing guidelines and the “explosion of data” in the literature. “It’s not always the cancer itself that impacts life,” she emphasised, adding that many cancer therapies result in “direct and intended acute toxicities to the endocrine system”, as well as long-term effects. “We need to be literate, not just in the management of long-term sequalae such as bone health, but also increasingly in the management of symptoms associated
with them,” she said.
Prof Druce then presented data on persistent and later toxicities in childhood cancer, highlighting the substantial increases in survivorship of “patients living beyond cancer”. “Mortality is not the only issue,” she noted, before focusing on the range of morbidities “that can stack up over time”. The conference heard that survivors of childhood cancers have significantly higher risks of developing morbidities when compared to their siblings and that notably high rates of late endocrine effects exist among this population. “There’s a high prevalence of endocrinopathy, but not necessarily
high mortality, from late endocrine effects in general,” Prof Druce said, and discussed the various postcancer pathologies that can affect the thyroid, the hypo-pituitary-axis, bone health, obesity, metabolism, and other endocrine processes, and what this means for endocrinologists.
“What is clear from some of these long-term cohort studies is that the impact of endocrine late effects is not just on the endocrine system…. We might think that if we replace the hormones everything will be fine. In fact, endocrine late effects, excluding weight-based effects, track with life morbidity, such as depression, PTSS
Hypo-METRICS in continuous glucose monitoring
The use of continuous glucose monitoring (CGM) by individuals with type 1 diabetes (T1D) has “revolutionised the management of hypoglycaemia”, Dr Patrick Divilly, Consultant of Endocrinology and Diabetes Mellitus, St Vincent’s University Hospital, Dublin, told the inaugural Joint Irish-UK Endocrine Meeting 2024, before highlighting issues surrounding hypoglycaemia in the age of the new technology. He compared the original definition of hypoglycaemia to CGMdetected hypoglycaemia, which relates to glucose levels below the hypoglycaemic threshold for at least 15 minutes, and emphasised that over 60 per cent of these episodes are asymptomatic.
He then detailed his work in the Hypo-METRICS study, a multinational, multicentre investigation conducted as part of the HypoRESOLVE consortium. “The primary aim was to provide an evidence-based definition of CGM-hypoglycaemia, and to further our understanding of clinical and psychological health
impacts of hypoglycaemia,” he said, and gave a detailed account of the study methodology and recruitment process. Participants wore a blinded CGM for 10 weeks and recorded their hypoglycaemia experiences “in real time using a smartphone app”. The study recruited 350 participants with insulin-treated type 2 diabetes, 200 with T1D and awareness of hypoglycaemia, and 50 with T1D and impaired awareness of hypoglycaemia.
“We asked them to report all episodes of hypoglycaemia that were either symptomatic episodes, which resolved after carbohydrate ingestion, or selfmeasured glucose of less than 4mmol/L. They also filled in three short surveys per day with key domains of quality of life that allowed us to compare the impact of days with and without hypoglycaemia.”
Findings from Hypo-METRICS revealed that while asymptomatic, sensor-detected hypoglycaemia went “unnoticed” and had no impact on daily functioning, episodes that were identified by participants did correlate with a negative impact on daily
(post-traumatic stress syndrome), emotional regulation, and social function; even when well managed.”
Concluding, Prof Druce said “we don’t yet have the data on late effects” and acknowledged the existence of many clinical, economic, and practical “unanswered questions”. Regarding the role of the endocrinologist, she said “we are there to guide our patients to the roadblocks with the information and knowledge that we have”, and advocated supporting the patient “through their chronic ill-health, keeping them optimal both in terms of their psychological and quality of life, and also in terms of their endocrine health”.
functioning. “The real driver of reduced quality of life is not what the CGM is saying, but what the person is reporting to you,” Dr Divily said. “The current consensus definition of hypoglycaemia doesn’t correlate well with the lived experience of hypoglycaemia,” he added, and described the steps taken in attempts to optimise definitions.
“What this might mean in the future is the development of personalised hypoglycaemia alarms. This would hopefully reduce the number of false alarms that people are experiencing, and reduce the psychological impact of hypoglycaemia without significantly increasing the biological risk; obviously within certain parameters. This might reduce alarm fatigue and diabetes stress, especially important with alarm fatigue being a key reason people discontinue a lot of the technology that we use…. The really important message is that the impact of hypoglycaemia on the person with diabetes depends not just on the threshold, but on their lived experience.”
ADOPTing AI to facilitate timely bone care
The Joint Irish and UK Endocrine Annual Scientific Meeting 2024 was presented with a practical and clinically-grounded overview of the UK ADOPT (AI-enabled Detection of OsteoPorosis for Treatment) study from lead author Prof Kassim Javaid, Professor of Osteoporosis and Adult Rare Bone Diseases, University of Oxford, UK.
ADOPT uses artificial intelligence (AI) to review hospital computed tomography (CT) scans and identify appropriate patients, who are not critically unwell or in the final stages of life, that will benefit from a prompt bone health assessment. In his talk, he provided insight into AI algorithms in clinical practice, how healthcare systems and clinicians “can use them intelligently”, and why he and his team now include the technology in their osteoporosis pathway.
Undetected fractures and high-risk patients
Prof Javaid began by presenting the empirical data and a patient case study to show that while patients undergo CT scans for many reasons, up to 50 per cent of moderate to severe vertebral fractures on images that include the spine are not detected. “This has led to a tsunami of AI models that look at different [radiological] modalities to automate the detection of bone fractures,” he said, and added that healthcare systems “don’t have the manpower” required to do so in the same manner.
Discussing the available technologies, Prof Javaid detailed “ensemble AI”– which
involves training several AI models to achieve optimal fracture prediction and detection. “Why use one model when you can use four?” he said, explaining that agreement between the separate models provides “a much higher performance rate”, and diminishes dependence on just one system.
“CT has a lot more information than just the shape of the bone,” Prof Javaid continued, and went on to describe the “valuable” data AI can produce and analyse regarding muscle, age, and other demographics. Attendees then heard that the technology can improve fracture prediction even without analysing radiological images or bone parameters, instead using “very old” and other data sets, such as ICD [International Classification of Diseases] 10 codes. He then presented evidence to show that AI is “quite impressive” when compared to the traditional mode of osteoporosis detection, the DXA (dual-energy x-ray absorptiometry) scan. “There is a massive amount of [AI] models in the literature,” he said, and told his colleagues that they did not need to “keep up” with the ongoing advances, and should instead just wait for those that are granted regulatory approval, as most will “drop off” during the process.
Practical insight from ADOPT
Prof Javaid proceeded to share some of the practical knowledge he gained while successfully implementing a “very simple AI pathway way using CT data” in five
hospitals during ADOPT. “We did this in four work packages,” he explained. “Does AI actually work in the hospital setting? What are the regulatory pathways for deployment? Do we actually improve the number of patients we manage? And finally, do we prevent fractures?”
Prof Javaid then gave a step-by-step description of the methodology, approval, and implementation phases of the study, as well as an overview of practical issues, tips for adoption, litigation considerations, and “lessons learned”. He emphasised the importance of identifying “humans in the loop”, as well as the “massive IT requirements”, and described carrying out a shadow test before going live “to see what happens” within a clinical context and identify areas to be fixed.
“AI is going to revolutionise healthcare in coming years,” Prof Javaid told the room. “The good news is that after 2,000 patients, we’ve only had positive feedback. Most patients are delighted that AI is now helping them achieve bone health.” Concluding, he emphasised the necessity of “human review”, multidisciplinary collaboration, particularly with general practice, and patient follow-up after the AI has identified those at risk.
“I would suggest you spend 90 per cent of your time thinking about the patient and 10 per cent thinking about AI, because the AI will work. You’ll get lots of patients and your AI implementation group has to focus on what happens once they get confirmed.”
Developments in bariatric surgery
Attendees at the Joint Irish and UK Endocrine Annual Scientific Meeting 2024 received a tour de force presentation from Prof Helen Heneghan, Consultant Bariatric Surgeon, St Vincent’s University Hospital,
Dublin, on the latest advances, findings, and outcomes in bariatric surgery in a talk entitled: ‘Metabolic surgery: Which to choose and new developments’.
The gastric band is “becoming a redundant procedure” and has the highest rates of long-term complications, Prof Heneghan began with the current trends, adding that the approach is also the least effective in terms of weight loss and
comorbidity resolution when compared to the commonest operations performed – sleeve gastrectomy and gastric bypass. Delegates received a detailed overview of each procedure, noting that bypassing the foregut (duodenum and proximal jejunum) leads to “a lot of the gut hormone benefits responsible for metabolic improvements”. Prof Heneghan also stated that sleeve gastrectomy “leads the way in terms of volume”, accounting for over 60 per cent of bariatric surgeries performed worldwide.
Describing her own practice and experiences, Prof Heneghan talked about the value of “enhanced recovery after surgery”, which she described as a “bundle of things done before, during, and after
do not have a preference regarding sleeve gastrectomy or bypass, “it’s not an easy decision.” She added that only around half of patients will have a preference, and that many come misinformed, particularly due to social media. “There are pros and cons to both procedures,” she said. Benefits of sleeve gastrectomy include the fact it is simple and quick to perform, is relatively safe, and is effective for weight loss and obesity complications. On the other hand, it is not reversible and weight regain occurs in up to 70 per cent of patients. Gastrooesophageal reflux disease (GORD) occurs in 20-30 per cent of patients, with one-infive developing non-dysplastic Barret’s oesophagus, the conference heard.
outperform the sleeve…. The bypass is now as safe as a sleeve and as cost-effective, but that data has yet to be published.”
Novel therapies
...‘every organ affected by obesity can be improved’, an array of positive outcomes which also extend to mental health benefits and a reduced risk of cancer (excluding lung cancer)
surgery” to enhance safety, get people out of hospital sooner, and reduce risks, including a simple laprascopic approach and early resumption of mobility postoperatively. Prof Heneghan told the conference that bariatric surgery carries a mortality rate equal to cholecystectomy, which is less than one-in-1,000. Major complications arise in 1-2 per cent of cases, while one-in-10 patients will experience mild to moderate problems, she said.
Moving to the benefits of bariatric surgery, Prof Heneghan noted that “every organ affected by obesity can be improved”, and described an array of positive outcomes which also extend to mental health benefits and a reduced risk of cancer (excluding lung cancer).
The superiority debate:
Choosing a procedure
Prof Heneghan explained that if patients
“Bypass is also quick,” Prof Heneghan compared, adding that the procedure is also reversible, slightly more effective than sleeve gastrectomy, and reduces obesity complications. “There is a risk of ulcers and strictures at the first anastomosis,” she said, and noted the surgery carried a slightly higher risk of iron deficiency.
“There is some new data to help decide which procedure to choose,” Prof Heneghan presented the latest published, and some unpublished, findings to summarise current understanding that “bypass outperforms a sleeve, which outperforms a band”, and that gastric bypass achieved a better quality of life.
“Bypass is more clinically effective than a sleeve and a band in short- to medium-term. We need data beyond three years, particularly beyond five years. I think based on experience and non-randomised data, the bypass will
A range of novel approaches are emerging in bariatric surgery, delegates heard, including the inter-gastric balloon; an endoscopic procedure that is “very safe for temporary weight loss or patients unsuitable for surgery”, but not for long-term results as “weight goes back on when [the balloon] is removed”. Prof Heneghan also mentioned the EndoBarrier device, which is placed endoscopically in the duodenum to “mimic aspects of bypass”, and leads to 11 per cent weight loss and a notable HbA1C reduction in one year. “The device lost approval four or five years ago” due to a particularly high incidence of liver abscesses and gastrointestinal bleeds, likely tied to the anchoring mechanism of the device, Prof Heneghan said, but added that the “second generation of that device will be interesting”.
“The most novel endoscopic device coming to market is the magnet anastamotic system,” she added, which “involves placing a magnet in the proximal jejunum using endoscopy and one in the terminal ileum using colonoscopy, let them meet each other, and compression will form an anastomosis in a really safe way”. Prof Heneghan also discussed selecting patients for the duodenal mucosal resurfacing procedure, which involves endoscopic ablation to resurface the mucosa, “takes less than one hour to perform, is really safe, and is associated with an improved A1C and weight loss of around 7 per cent at one year.”
Concluding her talk with a summary of current knowledge in the field, Prof Heneghan said: “Bariatric surgery is clinically- and cost-effective for the treatment of obesity. A gastric bypass is more effective and as safe as a sleeve gastrectomy. Patient choice is also important in determining which procedure people have. They have to be informed on the likely procedure outcomes. There are really exciting novel metabolic procedures on the way that I think combined with medications will transform the treatment of obesity in future.”
Real-time glucose readings sent right to your patients’ smartphones4,5
Outstanding 14-day accuracy, even in the low glucose range7 Significant clinical outcomes for T1D8 and T2D2,9,10 Optional glucose alarms6
2. Haak, T. Diabetes Therapy (2017): https://doi.org/10.1007/s13300-016-0223-6. 3. Data on file, Abbott Diabetes Care. Data based on the number of users worldwide for the FreeStyle Libre portfolio compared to the number of users for other leading personal use sensor-based glucose monitoring systems. 4. The FreeStyle LibreLink app is only compatible with certain mobile devices and operating systems. Please check the website for more information about device compatibility before using the app. Use of FreeStyle LibreLink may require registration with LibreView. 5. Glucose readings are automatically displayed in the app only when the smartphone and sensor are connected and in range. 6. Patients choose which device they want to receive alarms: FreeStyle Libre 2 reader or FreeStyle LibreLink app. They must start their FreeStyle Libre 2 sensor with that selected device. Once the patient scans their FreeStyle Libre 2 sensor with that device, they can receive alarms only on that device. Alarm notifications will only be received when alarms are turned on and the sensor is within 6 metres (20 ft) unobstructed of the reading device.
1. Campbell, F. Pediatr Diabetes (2018): https://doi.org/10.1111/pedi.12735. 2. Haak, T. Diabetes Therapy (2017): https://doi.org/10.1007/s13300-016-0223-6. 3. Data on file, Abbott Diabetes Care. Data based on the number of users worldwide for the FreeStyle Libre portfolio compared to the number of users for other leading personal use sensor-based glucose monitoring systems. 4. The FreeStyle LibreLink app is only compatible with certain mobile devices and operating systems. Please check the website for more information about device compatibility before using the app. Use of FreeStyle LibreLink may require registration with LibreView. 5. Glucose readings are automatically displayed in the app only when the smartphone and sensor are connected and in range. 6. Patients choose which device they want to receive alarms: FreeStyle Libre 2 reader or FreeStyle LibreLink app. They must start their FreeStyle Libre 2 sensor with that selected device. Once the patient scans their FreeStyle Libre 2 sensor with that device, they can receive alarms only on that device. Alarm notifications will only be received when alarms
All reports: Denise Doherty
Link between premature menopause and mortality risk Highlights from the European Congress of Endocrinology, 11-14 May 2024, Stockholm, Sweden
Women who experience premature ovarian insufficiency (POI) before the age of 40 are more likely to die early, but hormone therapy may lower this risk, according to research presented at the 2024 European Congress of Endocrinology (ECE). The long-term Finnish study is the largest to date on the links between premature menopause and mortality, and highlights the importance of evidencebased, appropriate hormone therapy for these patients. Around 1 per cent of women go through menopause before the age of 40 and are subsequently at a higher risk of long-term health problems such as cardiovascular disease. The cause is largely unknown, but can be brought on spontaneously or by some treatments such as chemotherapy or bilateral oophorectomy.
In this study, researchers from the University of Oulu and Oulu University Hospital, Finland, investigated 5,817 women who were diagnosed with spontaneous or surgical POI in Finland between 1988 and 2017. They compared these women with 22,859 women without POI and found that those who had experienced early menopause were more than twice as likely to die of any cause or of heart disease,
and more than four times as likely to die of cancer. However, the risk of all-cause and cancer mortality was approximately halved in women who used hormone replacement therapy (HRT) for more than six months.
Previous studies have also shown that women with premature
spontaneous POI in women’s all-cause, cardiovascular, and cancer-related mortality, and examine whether HRT for over six months may reduce mortality risk. Our findings suggest specific attention should be paid to the health of women with spontaneous POI to decrease excess mortality.”
Various health risks of women with POI have not been well recognised and the use of HRT is often neglected
menopause have a higher risk of early death. However, this association has never been studied in women on such a large scale before, or for such a lengthy follow-up period (up to 30 years). “To our knowledge, this is the largest study performed on the linkage between POI and mortality risk,” said Ms Hilla Haapakoski, a PhD student at the University of Oulu, who led the study.
She added: “Our study is one of the first to explore both surgical and
The team will now assess whether women with premature menopause are more likely to have other illnesses or conditions, such as cancer or heart disease, and whether long-term use of HRT affects these conditions. “Various health risks of women with POI have not been well recognised and the use of HRT is often neglected. We hope to improve the health of these women by increasing awareness of the risks among healthcare professionals and the women themselves,” added Ms Haapakoski.
Fezolinetant safely reduces hot flushes in menopause for almost six months
Attendees at the ECE Congress 2024 heard that fezolinetant reduces the frequency and severity of hot flushes during menopause for 24 weeks without serious side-effects. Vasomotor symptoms (VMS) affect up to 80 per cent of women going through menopause and can severely impact many aspects of wellbeing. Hormone replacement therapy (HRT) is not suitable for, or desired by, all women, and fezolinetant – which was recently approved in Ireland for VMS – acts directly on the thermo-regulatory pathway to alleviate these issues, and is a non-hormonal alternative for symptom management. Previous late-stage clinical trials (SKYLIGHT 1 and SKYLIGHT 2) have shown that fezolinetant reduces both the frequency and severity of hot flushes in women with moderate or severe symptoms compared to placebo over 12 weeks. This phase 3b study, known as DAYLIGHT, investigated the effect of fezolinetant use over 24 weeks. A total of 453 menopausal women aged 40-65 with moderate or severe hot flushes, who were unsuitable for HRT, were randomised to receive either fezolinetant or placebo. The primary endpoint was mean change in daily VMS frequency of moderate to severe episodes from baseline to week 24, while secondary endpoints included mean change in VMS severity and safety. Women who took fezolinetant
reported less frequent and severe hot flushes throughout the 24 weeks. They had consistently fewer hot flushes in the first week, with the strongest decrease during the first three days. The severity of their hot flushes was also reduced significantly by the drug in the first week from the second day. No safety issues were found for the 45mg fezolinetant dose over the 24 weeks.
“DAYLIGHT is the first study of fezolinetant to investigate placebo-
A safe and effective non-hormonal molecule may be available for the very high number of menopausal women who suffer from VMS and improve their overall health
controlled efficacy over 24 weeks,” said Prof Antonio Cano, INCLIVA Research Institute in Valencia, Spain, and senior author of the study. “Fezolinetant was effective and well tolerated for 24 weeks and the effect was observed as early as day one of treatment. While there are other NK (neurokinin-3) antagonists, none have shown a similar concurrence of efficacy and safety in clinical studies with a sufficiently high number of participants. A safe and effective nonhormonal molecule may be available for the very high number of menopausal women who suffer from VMS and improve their overall health, quality of life, and work performance. However, these symptoms vary in prevalence or intensity depending on ethnicity – for example, VMS are more frequent and severe in black women – so more clinical data are needed in different populations or geographical areas in the world.”
Arm fat may indicate risk of spinal fracture
Measuring the total fat mass of the arms could potentially predict those over 50 who are at increased risk of spinal fracture, according to research presented at the ECE Congress 2024. Osteoporosis is a common disease among older people, but is also one of the most underdiagnosed and untreated medical conditions in the world. The findings may help identify highrisk individuals with a very simple and inexpensive method.
To date, the relationship between body composition and bone health is still unclear. Therefore, to further understanding in the area, researchers from the National and Kapodistrian University of Athens, Greece, analysed 14 men and 101 women without osteoporosis. The sample had an average age of 62 and demonstrated that total fat mass is negatively associated with trabecular bone score (TBS). Moreover, total lean mass was positively associated with TBS. Visceral fat, in particular, was associated with lower
quality trabecular bone.
The researchers then looked at the distribution of subcutaneous body fat and discovered that individuals with higher fat mass in the arms were more likely to have lower bone quality and strength in the spine. “Surprisingly, we identified, for the first time, that the body composition of the arms – in particular, the fat mass of the arms – is negatively associated with the bone quality and strength of the vertebrae,” said senior author Prof Eva Kassi, Professor of Endocrinology/ Biochemistry, National and Kapodistrian University of Athens, Medical School, Athens, Greece. “This could mean that the arm’s subcutaneous fat, which can be easily estimated even by the simple and inexpensive skin-fold calliper method, may emerge as a useful index of bone quality of the spine, possibly predicting the vertebrae fracture risk. It should be noted that visceral fat, which we found to be strongly correlated with low bone quality,
is the hormonally more active component of the total body fat. It produces molecules called adipocytokines that provoke a low-grade inflammation, so the increased inflammatory status plausibly poses a negative impact on bone quality.”
Prof Kassi also acknowledged that larger studies are needed to confirm the link between arm fat and spinal fracture risk, and that research is still ongoing. “Although our results remain robust after controlling for age and weight, we will now increase the number of participants and expand the age range by including younger adults between the ages of 30 and 50 years old, as well as more men. Moreover, using the loss of arm fat mass as a marker, we will try to determine the most effective physical exercise routine that not only targets the visceral fat, but also focuses on the upper part of the body so that these higher-risk adults lose arm fat and achieve a favourable effect on vertebrae bone quality.”
Blood sugar levels at gestational diabetes diagnosis correlate with level of risk
The level of glucose above diagnostic threshold at the time of gestational diabetes (GD) diagnosis is associated with worse neonatal outcomes and abnormal maternal glucose homeostasis, but not with obstetric outcomes, according to data presented at the ECE 2024 Congress. GD affects around 20 million pregnancies worldwide and poses a range of health risks for both mothers and their babies. The higher the blood sugar level in pregnant women when first diagnosed, the higher the risk of complications, attendees heard.
Researchers from the Tâmega e Sousa Hospital Centre, Portugal, conducted a retrospective study based on the national register of GD. A total of 6,927 women
aged between 30-37 with live-born singleton pregnancies were included and analysed between 2012 and 2017. The researchers found that for every 5mg/L increase in their blood sugar levels, there was a 9 per cent higher risk of hypoglycaemia and a 6 per cent higher risk of large birth weight in newborns, as well as a 31 per cent higher risk of postpartum maternal hyperglycaemia. The findings suggest that high-risk women with GD should be classified further to limit these complications for both mothers and newborns.
“While it is not surprising that high glucose levels are associated with these adverse outcomes in mothers and newborns, our study shows for the first
time how much increase in risk there is with 5mg/dL of increase in the mother’s blood glucose levels when first diagnosed with GD,” said study co-lead Dr Catarina Cidade-Rodrigues. “The magnitude of elevated risk can be calculated with our measurements and, in practice, could be used to identify and stratify women at higher risk of developing these complications. We now want to evaluate if there is a benefit in further stratifying these high-risk women with GD, who will need to be more closely monitored and to whom pharmacological interventions can be carried out appropriately. This may help reduce complications during labour and in newborns and prevent future diabetes in these women.”
IN FOCUS: Polycystic ovary syndrome
Author: Theresa Lowry Lehnen: RGN, PG Dip Coronary Care, RNP, BSc, MSc, PG Dip Ed (QTS), M Ed, PhD, Advanced Nurse Practitioner Candidate South East Technological University
Polycystic ovary syndrome (PCOS) is a prevalent and complex endocrine disorder affecting women of reproductive age. It is characterised by a combination of reproductive, metabolic, and hormonal disturbances, with significant variations in symptoms and severity among individuals. The global prevalence of PCOS has risen substantially throughout the years. It affects approximately 8-20 per cent of women of reproductive age worldwide and is considered a leading cause of infertility. Although the precise cause of PCOS remains unclear, research suggests that a combination of genetic, environmental, and lifestyle factors play a significant role in its development. 1,2,3,4
Pathophysiology
The pathophysiology of PCOS involves several interconnected mechanisms, the most prominent being hyperandrogenism, insulin resistance, and ovarian dysfunction. These processes contribute to the characteristic symptoms seen in women with PCOS, including menstrual irregularities, hyperandrogenism, and metabolic disturbances. Several genetic studies have also revealed that many potential genes with single-nucleotide polymorphisms or mutations are connected to a variety of PCOS symptoms.2,5,6 Hyperandrogenism is a key feature of PCOS, with elevated levels of androgens such as testosterone being produced by the ovaries and, to a
lesser extent, the adrenal glands. The increase in androgen production is linked to the dysregulation of the hypothalamic-pituitary-ovarian axis. In women with PCOS, there is often an abnormal increase in luteinising hormone (LH) secretion, which stimulates the ovaries to produce more androgens. Insulin resistance also plays a major role in the development of PCOS. Up to 70 per cent of women with PCOS exhibit insulin resistance, independent of obesity. As a result, the body compensates by producing higher levels of insulin, a condition known as hyperinsulinemia. The excess insulin stimulates the ovaries to produce androgens, exacerbating the hyperandrogenic state. 5,6,7
Insulin resistance also reduces the levels of sex hormone-binding globulin (SHBG), a protein that binds to androgens in the blood. With lower SHBG levels, there is an increase in the free and bioavailable androgens, which intensifies symptoms such as hirsutism, acne, and male-pattern baldness. At the same time, the increased insulin levels impair normal follicular development in the ovaries. In PCOS, multiple small
follicles develop, but they do not mature properly, resulting in chronic anovulation and irregular menstrual cycles.5,6,8
Clinical manifestations
PCOS presents with a wide range of clinical manifestations, making diagnosis challenging. The most common symptoms are related to menstrual irregularities, hyperandrogenism, and metabolic disturbances. Many women with PCOS experience oligomenorrhea or amenorrhea, due to the failure of normal ovulation. The lack of ovulation can also lead to infertility, which is one of the most distressing symptoms for many women. 1,2,5
Hyperandrogenism manifests as physical signs such as hirsutism on the face, chest, and back, acne, and androgenic alopecia. These symptoms are often the most noticeable and can have a profound impact on a woman’s self-esteem and quality of life. 2,6
Metabolic complications are common in PCOS. Women with the condition are at a higher risk of developing metabolic syndrome, a cluster of risk factors that includes obesity, insulin resistance,
Hyperandrogenism manifests as physical signs such as hirsutism on the face, chest, and back, acne, and androgenic alopecia
dyslipidaemia, and hypertension. Obesity is a common feature of PCOS, although the condition can also occur in women of normal weight. Insulin resistance, irrespective of body mass index, increases the risk of T2D, and studies have shown that women with PCOS have a significantly higher lifetime risk of developing the disorder compared to the general population.1,2
There is growing evidence that PCOS is also associated with an increased risk of cardiovascular disease. Women with PCOS often have elevated levels of lowdensity lipoprotein cholesterol, reduced high-density lipoprotein cholesterol, and elevated triglycerides, contributing to the development of atherosclerosis. Other potential long-term complications include an increased risk of endometrial cancer, due to the unopposed oestrogen exposure from chronic anovulation.1,2,6
Diagnosis
Three sets of diagnostic criteria, Androgen Excess Society, Rotterdam, and National Institute of Health are commonly used for PCOS, and all require the exclusion of other known disorders. Among the different diagnostic criteria used to define PCOS, the Rotterdam criteria are the most widely used and recommended, and, like the more liberal AES criteria, they allow for different phenotypes of the disorder. Based on the Rotterdam criteria, a diagnosis of PCOS requires two out of three of the following: Hyperandrogenism, menstrual irregularities, and polycystic ovaries on ultrasonography. Other potential causes of hyperandrogenism, such as adrenal hyperplasia, androgensecreting tumours, and Cushing’s syndrome, must be excluded before making a diagnosis of PCOS. 4
Differential diagnoses for polycystic ovarian disease include: The use of androgenic steroids; hypothyroidism; late-onset congenital adrenal hyperplasia; idiopathic/familial hirsutism; and ovarian malignancies. 4
Laboratory testing is important in the evaluation of PCOS, primarily to assess hormone levels. Elevated testosterone and LH levels, with normal or low follicle-stimulating hormone, are commonly seen. Other tests include fasting glucose, insulin levels, lipid profiles, and screening for thyroid and adrenal function. It is also important to routinely screen for T2D and hypertension in view of the increased associated risks.1,2,5,6
In women showing signs of androgen excess, it is recommended to check serum total testosterone levels. If the testosterone level exceeds twice the upper limit of normal, referral to a specialist is advised for further evaluation. Based on clinical presentation, additional tests such as beta-HCG, thyroid function tests, prolactin levels, a 1mg overnight dexamethasone suppression test, and early morning serum 17-hydroxyprogesterone may be required. Mild increases in serum prolactin are often observed in PCOS, but if macroprolactin is ruled out and levels exceed twice the normal limit, further investigation is necessary. Elevated anti-Müllerian hormone levels, produced by ovarian follicle granulosa cells, are also frequently found in PCOS and can aid in diagnosis. 2,6,7
Screening for coronary artery disease and obstructive sleep apnoea should be considered for women at high risk. In women with PCOS, obesity increases the likelihood of developing endometrial cancer three-fold. Although routine screening for endometrial cancer with ultrasonography is not currently recommended, it is important to maintain a heightened awareness for patients experiencing prolonged oligomenorrhea, with more than three months between menstrual cycles. 2,5,9
Iron deficiency is frequently observed in PCOS and may contribute to symptoms like fatigue and androgenic alopecia. It is advisable to screen for iron deficiency and provide treatment if
Psychological wellbeing is a key concern in PCOS due to the effects such as weight gain, acne, and hirsutism
needed, aiming for serum ferritin levels in the upper quartile of the reference range. Vitamin D deficiency is common in PCOS patients and can exacerbate issues related to fertility, insulin resistance, and glucose intolerance. Screening for vitamin D levels and addressing deficiencies may prove beneficial. 2,5,9
Psychological wellbeing is a key concern in PCOS due to the physical effects such as weight gain, acne, and hirsutism, which impact on self-esteem. It is important to be aware and observe for signs of poor mental health like depression, anxiety, and self-harm.1,2,4
Treatment and management
The management of PCOS is individualised, depending on the symptoms and concerns of the patient, and it often requires a multidisciplinary approach involving endocrinologists, gynaecologists, dermatologists, and dietitians. 1 Lifestyle modification, particularly weight loss through diet and exercise, is considered the firstline treatment for women with PCOS, especially those who are overweight or obese. Even modest weight loss (5-10 per cent of body weight) can improve insulin sensitivity, regulate menstrual cycles, and reduce androgen levels. An ideal diet is rich in fibre and low in saturated fats and carbohydrates. Exercise and physical activity play a key role in weight reduction and may be beneficial to improve insulin sensitivity. 1,6,7
Pharmacological interventions are tailored to the patient’s symptoms and goals, whether they are focused on menstrual regularity, fertility, or hyperandrogenism. 7 For women seeking to regulate their menstrual cycles or reduce symptoms of hyperandrogenism, combined oral contraceptive pills (COCPs) are a commonly prescribed option. COCPs suppress ovarian androgen production and increase SHBG levels, reducing the symptoms of hirsutism, acne, and androgenic alopecia.
Anti-androgen medications, such as spironolactone, may be added to further reduce androgenic symptoms. Antibiotics and retinoic acid derivatives can also be used for acne treatment. Retinoids reduce the formation of comedones and cystic acne by reducing inflammation and desquamation of follicular epithelial cells. 1,2,6
It is important for patients to understand that improvements in hirsutism and other symptoms of androgen excess, such as acne, often take at least six months to become noticeable. For more immediate control of facial hirsutism, topical application of eflornithine can be used, although consistent application is essential for effectiveness. Laser hair removal offers a more permanent solution and can be a valuable option for patients experiencing significant distress from their symptoms. 1,2
In women with insulin resistance, metformin, an insulin-sensitising agent, may be used to improve insulin sensitivity and restore ovulatory function. Metformin is particularly beneficial in women with PCOS who are at risk of or have already developed T2D. 2,5
For women with PCOS who are seeking to conceive, ovulation induction is usually required. Clomiphene citrate has been a first-line agent for many years, but recent evidence suggests that letrozole, an aromatase inhibitor, is more effective for achieving ovulation and pregnancy in women
with PCOS. Gonadotropins or in vitro fertilisation are considered if oral agents fail. Metformin may also be used in conjunction with clomiphene or letrozole to improve ovulation rates, particularly in women with obesity or insulin resistance. 1,2
Emerging therapies
Several promising new therapies for PCOS are currently being developed, focusing on a variety of pharmacological approaches to address androgen excess, neuroendocrine dysfunction, and metabolic abnormalities. Although no androgen receptor antagonists are currently approved specifically for PCOS treatment, there is increasing interest in the therapeutic potential of modulating SHBG levels to help control hyperandrogenism. 10,11,12
2. Sadeghi, Hosna Mohammad et al. Polycystic ovary syndrome: A comprehensive review of pathogenesis, management, and drug repurposing. International Journal of Molecular Sciences; 23:2583.
3. Health Service Executive. Polycystic ovary syndrome (PCOS). Dublin: HSE; 2024. Available at: www2.hse.ie/ conditions/polycystic-ovary-syndrome/
4. Havelock J. Polycystic Ovarian Syndrome. BCMJ. 2018;60(4):210-216.
5. Singh S, Pal N, Shubham S, et al. Polycystic ovary syndrome: Aetiology, current management, and future therapeutics. J Clin Med 2023;12(4):1454.
6. Witchel SF, Oberfield SE, Peña AS. Polycystic ovary syndrome: Pathophysiology, presentation, and
There is growing interest in the use of inositol, particularly myo-inositol and D-chiro-inositol, as a treatment for PCOS. These compounds are insulin sensitisers that have been shown to improve ovulation and metabolic parameters. While promising, larger randomised controlled trials are needed to establish their role in the standard treatment of PCOS. 10,12
Another area of research is the gut microbiome’s role in PCOS. Alterations in the gut microbiota have been observed in women with PCOS, and there is evidence to suggest that restoring a healthy microbiome through diet, probiotics, or faecal microbiota transplantation may improve metabolic and reproductive outcomes. However, these treatments currently remain experimental. 5,10 l
treatment with emphasis on adolescent girls. J Endocr Soc 2019;3(8):1545-1573.
7. Dong J, Rees DA. Polycystic ovary syndrome: Pathophysiology and therapeutic opportunities. BMJ Med 2023;2(1):e000548.
8. Hajam Y, Rather H, Neelam, et al. A review on critical appraisal and pathogenesis of polycystic ovarian syndrome. Clin Epidemiol Glob Health 2024;14:100194.
9. Walter K. What is polycystic ovary syndrome? JAMA . 2022;327(3):294.
10. Tay CT, Garrad R, Mousa A, et al. Polycystic ovary syndrome (PCOS): International collaboration to translate evidence and guide future research. J Endocrinol. 2023;257(3):e220232.
11. Che Y, Yu J, Li YS, et al. Polycystic ovary syndrome: Challenges and possible solutions. J Clin Med 2023;12(4):1500.
12. Glendining KA, Campbell RE. Recent advances in emerging PCOS therapies. Curr Opin Pharmacol. 2023;68:102345.
Top ten unanswered questions in adults living with type 1 diabetes –a UK and Ireland James Lind Alliance Priority Setting Partnership
Authors: Dr Christine Newman and Prof Fidelma P Dunne, Institute for Clinical Trials, College of Medicine, Nursing and Health Sciences, University of Galway; Irish Collaborative Clinical Trial Network in Diabetes, Galway University Hospital
Across Ireland and the UK, nearly 300,000 adults and children live with type 1 diabetes (T1D), a chronic metabolic condition defined by hyperglycaemia and associated with multiple complications.1,2,3 While T1D, its complications, and treatment options are the subject of a huge number of studies, there is strong evidence to say that investigators and researchers do not always understand and share the priorities of those living with T1D every day. 4
To rectify this, the James Lind Alliance (JLA), a non-profit organisation, aims to bring together people living with health issues, their families, carers, and healthcare professions to take a multi-stakeholder approach to determining the most important questions in health research. 5 This process, called a priority setting partnership (PSP), brings people together as equal partners, firstly to identify questions through public surveys, and then to prioritise those questions. The final questions are then brought to research funders to ensure that research which is relevant and important to patients is prioritised. In 2011, a UK-only PSP was completed in T1D; however, since that time, the landscape of diabetes management has changed significantly.
Positively though, many of the 2011 top 10 questions have not only been answered, but have become part of standard clinical care for those living with the disease. 6,7,8 The aim of this PSP was to review and refresh the priorities for adults living with T1D across Ireland and the UK, as both offer free healthcare and medications for adults living with T1D, and have access to similar ranges of diabetes technology.
JLA process and results
To complete this PSP, we adhered to established JLA methodology.9 Step one involved forming a steering committee and outlining the scope of this PSP. Our steering group was made up of four people living with diabetes and one parent of a child living with diabetes, six clinicians (four endocrinologists, one consultant clinical psychologist, and one senior dietitian), and three members of diabetes charities from across Ireland and the UK. We invited two members of the 2011 PSP to join the steering group to ensure their experience was represented.
In order to ensure that the JLA process was followed, the steering group was overseen by an impartial JLA adviser who chaired all steering group meetings. Key members of the steering group also included an information specialist, who collated survey data and
performed evidence checking (discussed below), and the project co-ordinator, who organised steering group meetings, managed communication with the steering group and other stakeholders, and oversaw the survey software. The co-ordinator and information specialist also worked together to target different, under-represented groups during the course of the survey and promoted engagement through social media channels and emails.
The steering group was balanced in terms of gender and had 10 UK- and four Irish-based members. The scope of the PSP included adults living with T1D, their families, and carers, and welcomed all questions about living with the disorder, its complications, prevention, causes, co-morbidities, and treatment, as well as its physical, social, cultural, economic, and psychological impacts. We excluded questions about paediatric care, questions or priorities about other forms of diabetes including maturity-onset diabetes of the young (MODY), type 2 diabetes and gestational diabetes, T1D in pregnancy (due to recent completion of a PSP in the area of diabetes in pregnancy), and cystic fibrosis-related diabetes. We also excluded questions that did not have an Irish or UK focus.
The second step was to establish the uncertainties. The JLA process
has a set pathway for determining uncertainties 9 which includes designing and disseminating a primary survey that asks adults living with T1D, their families/carers, and healthcare professionals to list up to three questions they would like to see answered about the condition.
We also asked participants to provide some basic demographic details. The survey was available in English only and ran for three months. It was promoted predominately through social media networks, however, targeted interventions included emails to healthcare professionals in endocrinology, nephrology, cardiology, ophthalmology, and general practice throughout Ireland and the UK. Printed posters with QR code links to the survey were placed in diabetes clinics and general practice offices.
To ensure a diverse range of voices were included we also ran a phoneline for two hours each week for individuals with visual impairment or who preferred spoken to written English, emailed organisations working with under-represented patient groups, and contacted professional networks. We also utilised social media platforms (Facebook, X (formerly Twitter), and Instagram) to contact local community champions to promote this survey in different localities.
In the survey, all participants were provided with an explanation of how their data and information would be used and participants gave consent before completing the survey. Next, the information specialist manually reviewed each individual question and ruled them in or out of scope. From the ‘in scope’ questions, indicative summary questions were formed in a PICO (population, intervention, comparison, and outcome) structure. The steering group reviewed all questions deemed out of scope by the information specialist. Three steering committee sub-groups reviewed each of the indicative summary questions
(with the original questions) to minimise individual bias and ensure the summary questions were truly reflective of the questions asked. The steering sub-groups were free to edit the summary questions provided the group was in agreement and all changes were tracked and recorded. Once the steering group was satisfied with the summary questions, evidence checking commenced. This involved the information specialist checking all summary questions against evidence sources (Ireland and the UK guidelines, PubMed, and the Cochrane database for systematic reviews
psychological queries (4 per cent), weight management (4 per cent), assessment and initial diagnosis (2 per cent), the impact of Covid-19 on T1D (2 per cent), and communication and education (1 per cent). Of the 82 indicative summary questions, 17 were answered by recent evidence, leaving 65 questions unanswered.
Significant differences were noted between healthcare professionals and those with lived experience
published from 2020 onwards).
The initial survey received 13,387 views. In total, 1,050 individuals filled at least one question box and the average number of questions asked was 2.9. Respondent demographic details can be found in Table 1 . When all text boxes were analysed by the information specialist, there were 3,457 individual questions. After excluding spoiled or non-sensible boxes, 2,937 questions were individually reviewed and 82 indicative summary questions were formed with questions on cause and aetiology (28 per cent), cure (19 per cent), treatment and prevention (18 per cent), long-term outcomes and complications (11 per cent), questions regarding sexual health and fertility (5 per cent), service access (5 per cent),
The fourth step was interim priority setting and this involved ranking the 65 unanswered questions in order of importance. This interim survey was distributed via the same media as before; however, participants of the first survey who gave their consent and contact details were emailed directly to complete the second survey. In this survey, participants were asked to select up to 10 questions which they felt were important for research to answer. This survey ran for a total of eight weeks and received 497 replies. The demographic make-up of respondents closely matched those from survey 1 ( Table 1).
While analysing the replies from the interim survey, we reviewed the results from the general population and separately reviewed responses from subgroups, including healthcare professionals, people living with diabetes and their carers, ethnic minorities, and those who identified as being on a lower income. We also reviewed the answers from male participants as they accounted for only one third of replies. Significant differences were noted, for example, between healthcare professionals and those with lived experience, only five out of 10 priorities overlapped. Similarly, when the replies from ethnic minorities were compared to replies from the general population, only five out of 10 priorities overlapped.
To ensure that the priorities carried to the final workshop adequately reflected the priorities of the entire community, we followed the JLA process of granting priorities ranked highly by underrepresented groups higher scores to ensure they are fairly represented
and not diluted by over-representation of a certain cohort (eg, this survey had a large response rate from white female participants). We then combined the scores from the general population and each of the sub-groups mentioned (healthcare professionals, people living with diabetes and their carers, ethnic minorities, those who identified as being on a lower income, and male participants) to determine the most popular priorities. By giving equal weight to all sub-groups and combining these weights to achieve an average score, we were able to ensure there that was a fair representation from all under-represented groups.
Lastly, we held a final workshop to decide the final top 10 priorities. To ensure a diverse and representative panel, the steering group reviewed the final workshop invitees to ensure ethnicity and clinical and lived experience were balanced. Where deficits in diversity and expertise – either by profession or lived experience – were identified, targeted interventions were undertaken to ensure fair representation. The final workshop was held virtually with 27 participants (14 healthcare professionals – two dietitians, two advanced diabetes nurse practitioners, two podiatrists, one general practice nurse, five endocrinologists – four adult and one paediatric –, one psychologist, and one mental health nurse who is also trained as a behavioural scientist – and 13 individuals living with T1D and their family members).
A total of 15 members of the final workshop were female (55.5 per cent), 11 were male (40.7 per cent), and one member identified as non-binary. Two members (7.4 per cent) of the final group were from black or minority ethnic groups. Three members of the steering group also sat on the final workshop panel.
The final workshop was led by the JLA adviser and three other JLA moderators were present to facilitate
insulin glargine
glargine
From the start,1 there to help your
• Help your patients find balance between HbA1c reduction and hypoglycaemic risk1-7
•Offers
From the start,1 there to help your patients on their basal insulin journey1
• Help your patients find balance between HbA1c reduction and hypoglycaemic risk1-7
•Offers flexibility† (+/- 3 hours) in dosing time
1,8,9
•Offers flexibility† (+/- 3 hours) in dosing time1,8,9
Toujeo® DoubleStar™ prefilled pen is recommended for patients requiring at least 20 units per day.1
† Toujeo® is available in easy-to-use pens,1,8,9 to be administered once daily at any time of the day, preferably at the same time every day.1 When needed, patients can administer Toujeo® up to 3 hours before or after their usual time of administration. Flexible dosing time was evaluated in two randomised, open-label clinical studies, in patients with T2DM.1
oujeo® is available in easy-to-use pens, Toujeo® up to 3 hours
oujeo® is available in easy-to-use pens, Toujeo® up to 3 hours
Prescribing Information: Toujeo (insulin glargine 300 units/ml) Please refer to Summary of Product Characteristics (SmPC) before prescribing. Presentation: Toujeo SoloStar and DoubleStar pre-filled pens. Each ml contains 300 units of insulin glargine. SoloStar pen contains 1.5ml (450 units) of solution for injection. DoubleStar pen contains 3ml (900 units) of solution for injection. Indication: Treatment of diabetes mellitus in adults, adolescents and children from the age of 6 years. Dosage and Administration: Toujeo is administered subcutaneously, by injection into the abdominal wall, the deltoid or the thigh, once daily, at any time of the day, preferably at the same time every day. Injection sites must be rotated within a given injection area from one injection to the next in order to reduce the risk of lipodystrophy and cutaneous amyloidosis. The dose regimen (dose and timing) should be adjusted according to individual response. Do not administer intravenously. In type 1 diabetes mellitus, Toujeo must be combined with short-/rapidacting insulin to cover mealtime insulin requirements. In patients with type 2 diabetes mellitus, recommended daily starting dose is 0.2 units/kg followed by individual dose adjustments. Toujeo can also be given together with other anti-hyperglycaemic medicinal products. Switch between insulin glargine 100 units/ml and Toujeo: Insulin glargine 100 units/ml and Toujeo are not bioequivalent and are not directly interchangeable. When switching from insulin glargine 100 units/ml to Toujeo, this can be done on a unit-to-unit basis, but a higher Toujeo dose (approximately 10-18%) may be needed to achieve target ranges for plasma glucose levels. When switching from Toujeo to insulin glargine 100 units/ml, the dose should be reduced (approximately by 20%). Switching from other basal insulins to Toujeo: A change of dose and/or timing of the basal insulin and concomitant anti-hyperglycaemic treatment may be required. Dose adjustments may also be required if the patient’s weight or lifestyle changes, the timing of insulin dose is changed, or other circumstances arise that increase susceptibility to hypo- or hyperglycaemia. Toujeo must not be mixed or diluted with any other insulin or other medicinal products. Close metabolic monitoring is recommended during a switch and in the initial weeks thereafter. SoloStar 1-80 units per single injection in steps of 1 unit and DoubleStar 2-160 units in steps of 2 units. When changing from Toujeo SoloStar to Toujeo DoubleStar, if the patient’s previous dose was an odd number, then the dose must be increased or decreased by 1 unit. Toujeo DoubleStar prefilled pen is recommended for patients requiring at least 20 units per day. Special Populations: Insulin requirements may be diminished in the elderly or patients with renal or hepatic impairment. Paediatric: When switching basal insulin to Toujeo, dose reduction of basal and bolus insulin needs to be considered on an individual basis, in order to minimise the risk of hypoglycaemia. The safety and efficacy of Toujeo in children and adolescents below 6 years of age have not been established. Contraindications: Hypersensitivity to insulin glargine or any excipients. Precautions and Warnings: Traceability: In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded. Toujeo is not the insulin of choice for treatment of diabetic ketoacidosis. Patients must be instructed to perform continuous rotation of the injection site to reduce the risk of developing lipodystrophy and cutaneous amyloidosis. There is a potential risk of delayed insulin absorption and worsened glycaemic control following insulin injections at sites with these reactions. A sudden change in the injection site to an unaffected area has been reported to result in hypoglycaemia. Blood
Prescribing Information: Toujeo (insulin glargine 300 units/ml) Please refer to Summary of Product Characteristics (SmPC) before prescribing. Presentation: Toujeo SoloStar and DoubleStar pre-filled pens. Each ml contains 300 units of insulin glargine. SoloStar pen contains 1.5ml (450 units) of solution for injection. DoubleStar pen contains 3ml (900 units) of solution for injection. Indication: Treatment of diabetes mellitus in adults, adolescents and children from the age of 6 years. Dosage and Administration: Toujeo is administered subcutaneously, by injection into the abdominal wall, the deltoid or the thigh, once daily, at any time of the day, preferably at the same time every day. Injection sites must be rotated within a given injection area from one injection to the next in order to reduce the risk of lipodystrophy and cutaneous amyloidosis. The dose regimen (dose and timing) should be adjusted according to individual response. Do not administer intravenously. In type 1 diabetes mellitus, Toujeo must be combined with short-/rapidacting insulin to cover mealtime insulin requirements. In patients with type 2 diabetes mellitus, recommended daily starting dose is 0.2 units/kg followed by individual dose adjustments. Toujeo can also be given together with other anti-hyperglycaemic medicinal products. Switch between insulin glargine 100 units/ml and Toujeo: Insulin glargine 100 units/ml and Toujeo are not bioequivalent and are not directly interchangeable. When switching from insulin glargine 100 units/ml to Toujeo, this can be done on a unit-to-unit basis, but a higher Toujeo dose (approximately 10-18%) may be needed to achieve target ranges for plasma glucose levels. When switching from Toujeo to insulin glargine 100 units/ml, the dose should be reduced (approximately by 20%). Switching from other basal insulins to Toujeo: A change of dose and/or timing of the basal insulin and concomitant anti-hyperglycaemic treatment may be required. Dose adjustments may also be required if the patient’s weight or lifestyle changes, the timing of insulin dose is changed, or other circumstances arise that increase susceptibility to hypo- or hyperglycaemia. Toujeo must not be mixed or diluted with any other insulin or other medicinal products. Close metabolic monitoring is recommended during a switch and in the initial weeks thereafter. SoloStar 1-80 units per single injection in steps of 1 unit and DoubleStar 2-160 units in steps of 2 units. When changing from Toujeo SoloStar to Toujeo DoubleStar, if the patient’s previous dose was an odd number, then the dose must be increased or decreased by 1 unit. Toujeo DoubleStar prefilled pen is recommended for patients requiring at least 20 units per day. Special Populations: Insulin requirements may be diminished in the elderly or patients with renal or hepatic impairment. Paediatric: When switching basal insulin to Toujeo, dose reduction of basal and bolus insulin needs to be considered on an individual basis, in order to minimise the risk of hypoglycaemia. The safety and efficacy of Toujeo in children and adolescents below 6 years of age have not been established. Contraindications: Hypersensitivity to insulin glargine or any excipients. Precautions and Warnings: Traceability: In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded. Toujeo is not the insulin of choice for treatment of diabetic ketoacidosis. Patients must be instructed to perform continuous rotation of the injection site to reduce the risk of developing lipodystrophy and cutaneous amyloidosis. There is a potential risk of delayed insulin absorption and worsened glycaemic control following insulin injections at sites with these reactions. A sudden change in the injection site to an unaffected area has been reported to result in hypoglycaemia. Blood
Prescribing Information: Toujeo (insulin glargine 300 units/ml) Please refer to Summary of Product Characteristics (SmPC) before prescribing. Presentation: Toujeo SoloStar and DoubleStar pre-filled pens. Each ml contains 300 units of insulin glargine. SoloStar pen contains 1.5ml (450 units) of solution for injection. DoubleStar pen contains 3ml (900 units) of solution for injection. Indication: Treatment of diabetes mellitus in adults, adolescents and children from the age of 6 years. Dosage and Administration: Toujeo is administered subcutaneously, by injection into the abdominal wall, the deltoid or the thigh, once daily, at any time of the day, preferably at the same time every day. Injection sites must be rotated within a given injection area from one injection to the next in order to reduce the risk of lipodystrophy and cutaneous amyloidosis. The dose regimen (dose and timing) should be adjusted according to individual response. Do not administer intravenously. In type 1 diabetes mellitus, Toujeo must be combined with short-/rapidacting insulin to cover mealtime insulin requirements. In patients with type 2 diabetes mellitus, recommended daily starting dose is 0.2 units/kg followed by individual dose adjustments. Toujeo can also be given together with other anti-hyperglycaemic medicinal products. Switch between insulin glargine 100 units/ml and Toujeo: Insulin glargine 100 units/ml and Toujeo are not bioequivalent and are not directly interchangeable. When switching from insulin glargine 100 units/ml to Toujeo, this can be done on a unit-to-unit basis, but a higher Toujeo dose (approximately 10-18%) may be needed to achieve target ranges for plasma glucose levels. When switching from Toujeo to insulin glargine 100 units/ml, the dose should be reduced (approximately by 20%). Switching from other basal insulins to Toujeo: A change of dose and/or timing of the basal insulin and concomitant anti-hyperglycaemic treatment may be required. Dose adjustments may also be required if the patient’s weight or lifestyle changes, the timing of insulin dose is changed, or other circumstances arise that increase susceptibility to hypo- or hyperglycaemia. Toujeo must not be mixed or diluted with any other insulin or other medicinal products. Close metabolic monitoring is recommended during a switch and in the initial weeks thereafter. SoloStar 1-80 units per single injection in steps of 1 unit and DoubleStar 2-160 units in steps of 2 units. When changing from Toujeo SoloStar to Toujeo DoubleStar, if the patient’s previous dose was an odd number, then the dose must be increased or decreased by 1 unit. Toujeo DoubleStar prefilled pen is recommended for patients requiring at least 20 units per day. Special Populations: Insulin requirements may be diminished in the elderly or patients with renal or hepatic impairment. Paediatric: When switching basal insulin to Toujeo, dose reduction of basal and bolus insulin needs to be considered on an individual basis, in order to minimise the risk of hypoglycaemia. The safety and efficacy of Toujeo in children and adolescents below 6 years of age have not been established. Contraindications: Hypersensitivity to insulin glargine or any excipients. Precautions and Warnings: Traceability: In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded. Toujeo is not the insulin of choice for treatment of diabetic ketoacidosis. Patients must be instructed to perform continuous rotation of the injection site to reduce the risk of developing lipodystrophy and cutaneous amyloidosis. There is a potential risk of delayed insulin absorption and worsened glycaemic control following insulin injections at sites with these reactions. A sudden change in the injection site to an unaffected area has been reported to result in hypoglycaemia. Blood
glucose monitoring is recommended after the change in the injection site, and dose adjustment of antidiabetic medications may be considered. Hypoglycaemia: In case of insufficient glucose control or a tendency to hyper/hypoglycaemic episodes, the patient’s adherence to the prescribed treatment regimen, injection sites and proper injection technique and all other relevant factors must be reviewed before dose adjustment is considered. Particular caution should be exercised, and intensified blood glucose monitoring is advisable for patients in whom hypoglycaemic episodes might be of clinical relevance and in those where dose adjustments may be required. Warning signs of hypoglycaemia may be changed, less pronounced or absent in certain risk groups, potentially resulting in severe hypoglycaemia and loss of consciousness. Risk groups include patients in whom glycaemic control is markedly improved, hypoglycaemia develops gradually, an autonomic neuropathy is present, or who are elderly. The prolonged effect of subcutaneous insulin glargine may delay recovery from hypoglycaemia. Intercurrent illness: Requires intensified metabolic monitoring and often it is necessary to adjust the insulin dose. Insulin antibodies: administration may cause insulin antibodies to form. Use with pioglitazone: Cases of cardiac failure have been reported when pioglitazone was used in combination with insulin, especially in patients with risk factors for development of cardiac heart failure. If the combination is used, patients should be observed for signs and symptoms of heart failure, weight gain and oedema. Pioglitazone should be discontinued if any deterioration in cardiac symptoms occurs. Medication errors: Insulin labels must always be checked before each injection to avoid errors between Toujeo and other insulins. Patients must be instructed to never use a syringe to remove Toujeo from the SoloStar or DoubleStar prefilled pen, A new sterile needle must be attached before each injection. Needles must not be re-used. Pregnancy and lactation: There are no data from exposed pregnancies in controlled clinical trials. However, there is a large amount of data on use of insulin glargine 100 units/ml in pregnant women indicating no specific adverse effects on pregnancy and no specific malformative nor feto/neonatal toxicity. The use of Toujeo may be considered during pregnancy, if clinically needed. Careful monitoring of glucose control is essential. It is unknown if insulin glargine is excreted in breast milk. Interactions: Substances that affect glucose metabolism may require adjustment of insulin glargine. Adverse Reactions: Very common: Hypoglycaemia. Prolonged or severe hypoglycaemia may be life-threatening. Common: Lipohypertrophy, injection site reactions, including redness, pain, itching, hives, swelling, or inflammation. Prescribers should consult the SmPC in relation to other adverse reactions. Legal Category: POM. Marketing Authorisation Number: SoloStar 5 pen pack: EU/1/00/133/035; DoubleStar 5 pen pack: EU/1/00/133/038. Marketing Authorisation Holder: Sanofi Aventis Deutschland GmbH, D-65926 Frankfurt am Main, Germany. Further information is available from: Medical Information, Sanofi, 18 Riverwalk, Citywest Business Campus, Dublin 24 or contact IEmedinfo@sanofi.com. Date of preparation: July 2022. MAT-IE-2200355 (V1.0)
glucose monitoring is recommended after the change in the injection site, and dose adjustment of antidiabetic medications may be considered. Hypoglycaemia: In case of insufficient glucose control or a tendency to hyper/hypoglycaemic episodes, the patient’s adherence to the prescribed treatment regimen, injection sites and proper injection technique and all other relevant factors must be reviewed before dose adjustment is considered. Particular caution should be exercised, and intensified blood glucose monitoring is advisable for patients in whom hypoglycaemic episodes might be of clinical relevance and in those where dose adjustments may be required. Warning signs of hypoglycaemia may be changed, less pronounced or absent in certain risk groups, potentially resulting in severe hypoglycaemia and loss of consciousness. Risk groups include patients in whom glycaemic control is markedly improved, hypoglycaemia develops gradually, an autonomic neuropathy is present, or who are elderly. The prolonged effect of subcutaneous insulin glargine may delay recovery from hypoglycaemia. Intercurrent illness: Requires intensified metabolic monitoring and often it is necessary to adjust the insulin dose. Insulin antibodies: administration may cause insulin antibodies to form. Use with pioglitazone: Cases of cardiac failure have been reported when pioglitazone was used in combination with insulin, especially in patients with risk factors for development of cardiac heart failure. If the combination is used, patients should be observed for signs and symptoms of heart failure, weight gain and oedema. Pioglitazone should be discontinued if any deterioration in cardiac symptoms occurs. Medication errors: Insulin labels must always be checked before each injection to avoid errors between Toujeo and other insulins. Patients must be instructed to never use a syringe to remove Toujeo from the SoloStar or DoubleStar prefilled pen, A new sterile needle must be attached before each injection. Needles must not be re-used. Pregnancy and lactation: There are no data from exposed pregnancies in controlled clinical trials. However, there is a large amount of data on use of insulin glargine 100 units/ml in pregnant women indicating no specific adverse effects on pregnancy and no specific malformative nor feto/neonatal toxicity. The use of Toujeo may be considered during pregnancy, if clinically needed. Careful monitoring of glucose control is essential. It is unknown if insulin glargine is excreted in breast milk. Interactions: Substances that affect glucose metabolism may require adjustment of insulin glargine. Adverse Reactions: Very common: Hypoglycaemia. Prolonged or severe hypoglycaemia may be life-threatening. Common: Lipohypertrophy, injection site reactions, including redness, pain, itching, hives, swelling, or inflammation. Prescribers should consult the SmPC in relation to other adverse reactions. Legal Category: POM. Marketing Authorisation Number: SoloStar 5 pen pack: EU/1/00/133/035; DoubleStar 5 pen pack: EU/1/00/133/038. Marketing Authorisation Holder: Sanofi Aventis Deutschland GmbH, D-65926 Frankfurt am Main, Germany. Further information is available from: Medical Information, Sanofi, 18 Riverwalk, Citywest Business Campus, Dublin 24 or contact IEmedinfo@sanofi.com. Date of preparation: July 2022. MAT-IE-2200355 (V1.0)
glucose monitoring is recommended after the change in the injection site, and dose adjustment of antidiabetic medications may be considered. Hypoglycaemia: In case of insufficient glucose control or a tendency to hyper/hypoglycaemic episodes, the patient’s adherence to the prescribed treatment regimen, injection sites and proper injection technique and all other relevant factors must be reviewed before dose adjustment is considered. Particular caution should be exercised, and intensified blood glucose monitoring is advisable for patients in whom hypoglycaemic episodes might be of clinical relevance and in those where dose adjustments may be required. Warning signs of hypoglycaemia may be changed, less pronounced or absent in certain risk groups, potentially resulting in severe hypoglycaemia and loss of consciousness. Risk groups include patients in whom glycaemic control is markedly improved, hypoglycaemia develops gradually, an autonomic neuropathy is present, or who are elderly. The prolonged effect of subcutaneous insulin glargine may delay recovery from hypoglycaemia. Intercurrent illness: Requires intensified metabolic monitoring and often it is necessary to adjust the insulin dose. Insulin antibodies: administration may cause insulin antibodies to form. Use with pioglitazone: Cases of cardiac failure have been reported when pioglitazone was used in combination with insulin, especially in patients with risk factors for development of cardiac heart failure. If the combination is used, patients should be observed for signs and symptoms of heart failure, weight gain and oedema. Pioglitazone should be discontinued if any deterioration in cardiac symptoms occurs. Medication errors: Insulin labels must always be checked before each injection to avoid errors between Toujeo and other insulins. Patients must be instructed to never use a syringe to remove Toujeo from the SoloStar or DoubleStar prefilled pen, A new sterile needle must be attached before each injection. Needles must not be re-used. Pregnancy and lactation: There are no data from exposed pregnancies in controlled clinical trials. However, there is a large amount of data on use of insulin glargine 100 units/ml in pregnant women indicating no specific adverse effects on pregnancy and no specific malformative nor feto/neonatal toxicity. The use of Toujeo may be considered during pregnancy, if clinically needed. Careful monitoring of glucose control is essential. It is unknown if insulin glargine is excreted in breast milk. Interactions: Substances that affect glucose metabolism may require adjustment of insulin glargine. Adverse Reactions: Very common: Hypoglycaemia. Prolonged or severe hypoglycaemia may be life-threatening. Common: Lipohypertrophy, injection site reactions, including redness, pain, itching, hives, swelling, or inflammation. Prescribers should consult the SmPC in relation to other adverse reactions. Legal Category: POM. Marketing Authorisation Number: SoloStar 5 pen pack: EU/1/00/133/035; DoubleStar 5 pen pack: EU/1/00/133/038. Marketing Authorisation Holder: Sanofi Aventis Deutschland GmbH, D-65926 Frankfurt am Main, Germany. Further information is available from: Medical Information, Sanofi, 18 Riverwalk, Citywest Business Campus, Dublin 24 or contact IEmedinfo@sanofi.com. Date of preparation: July 2022. MAT-IE-2200355 (V1.0)
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie; email: medsafety@hpra.ie Adverse events should also be reported to Sanofi Ireland Ltd. Tel: 01 403 5600. Alternatively, send via email to IEPharmacovigilance@sanofi.com FOR
Intended for Healthcare Professionals in the Republic of Ireland only.
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie; email: medsafety@hpra.ie Adverse events should also be reported to Sanofi Ireland Ltd. Tel: 01 403 5600. Alternatively, send via email to IEPharmacovigilance@sanofi.com
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie; email: medsafety@hpra.ie Adverse events should also be reported to Sanofi Ireland Ltd. Tel: 01 403 5600. Alternatively, send via email to IEPharmacovigilance@sanofi.com
Abbreviations: HbA1c, Hemoglobin A1c; PD, Pharmacodynamics; PK, Pharmacokinetics; T1DM, Type 1 Diabetes Mellitus; T2DM, Type 2 Diabetes Mellitus.
Intended for Healthcare Professionals in the Republic of Ireland only.
Abbreviations: HbA1c, Hemoglobin A1c; PD, Pharmacodynamics; PK, Pharmacokinetics; T1DM, Type 1 Diabetes Mellitus; T2DM, Type 2 Diabetes Mellitus.
Abbreviations: HbA1c, Hemoglobin A1c; PD, Pharmacodynamics; PK, Pharmacokinetics; T1DM, Type 1 Diabetes Mellitus; T2DM, Type 2 Diabetes Mellitus.
References: 1 Toujeo® Summary of Product Characteristics July 2020. 2. Home PD, et al. Diabetes Care 2015;38(12):2217-2225. 3. Matsuhisa M, et al Diabetes Obes Metab 2016;18(4):375-383. 4. Danne T, et al. Diabetes Care 2020; 43(7):1512–1519. 5. Riddle MC, et al. Diabetes Care 2014;37:2755-2762. 6. Yki-Jarvinen H, et al. Diabetes Care 2014;37:3235-3243. 7. Bolli GB, et al. Diabetes Obes Metab 2015;17:386-394. 8 Singh R, et al Eur Endocrinol 2018;14:47-51. 9 Pohlmeier H, et al. J Diabetes Sci Technol 2017;11;263-269. MAT-IE-2200486 (v1.0) | December 2022 Intended for Healthcare Professionals in the Republic of Ireland only.
References: 1 Toujeo® Summary of Product Characteristics July 2020. 2. Home PD, et al. Diabetes Care 2015;38(12):2217-2225. 3. Matsuhisa M, et al Diabetes Obes Metab 2016;18(4):375-383. 4. Danne T, et al. Diabetes Care 2020; 43(7):1512–1519. 5. Riddle MC, et al. Diabetes Care 2014;37:2755-2762. 6. Yki-Jarvinen H, et al. Diabetes Care 2014;37:3235-3243. 7. Bolli GB, et al. Diabetes Obes Metab 2015;17:386-394. 8 Singh R, et al Eur Endocrinol 2018;14:47-51. 9 Pohlmeier H, et al. J Diabetes Sci Technol 2017;11;263-269. MAT-IE-2200486 (v1.0) | December 2022
References: 1 Toujeo® Summary of Product Characteristics July 2020. 2. Home PD, et al. Diabetes Care 2015;38(12):2217-2225. 3. Matsuhisa M, et al Diabetes Obes Metab 2016;18(4):375-383. 4. Danne T, et al. Diabetes Care 2020; 43(7):1512–1519. 5. Riddle MC, et al. Diabetes Care 2014;37:2755-2762. 6. Yki-Jarvinen H, et al. Diabetes Care 2014;37:3235-3243. 7. Bolli GB, et al. Diabetes Obes Metab 2015;17:386-394. 8 Singh R, et al Eur Endocrinol 2018;14:47-51. 9 Pohlmeier H, et al. J Diabetes Sci Technol 2017;11;263-269. MAT-IE-2200486 (v1.0) | December 2022
four small group discussions. Prior to the workshop, each participant was asked to rank all 19 questions from 1-19. During the workshop, participants were split into four sub-groups. At the end of the workshop, all four groups’ rankings were combined to create a final 1-19 ranking, with the focus being on the top 10 most important priorities. The four JLA facilitators oversaw small sub-group discussions over the course of the two days. There were three sessions for small group discussion which were held in virtual ‘break-out rooms’. During these discussions, the facilitators oversaw conversation and debate between groups, and each group was balanced in numbers of healthcare professionals and those with lived experience. Equal input was sought
from each member of the group.
During the first sub-group session, each participant identified their highest and lowest priority and gave a brief explanation of why they ranked the question in that way. The JLA facilitator kept a record of how each question was ranked and placed each question in either a ‘high’, ‘middle’, or ‘low’ priority category. In the second session, the sub-groups remained the same and the group reviewed the questions using visual aids and ranked the questions in the ‘high’ and ‘middle’ categories to create a top 10. At the end of day one, the rankings from each sub-group were combined to create an overall ranking.
At the start of day two, these results were shared with the entire group and new sub-groups were formed,
again made up equally of healthcare professionals and those with lived experience to ensure participants heard different perspectives. These groups reviewed the priorities and debated the order of questions to create a top 10 list. Once again, the results of each of the sub-groups were combined to form the final top ranking and top 10.
During the break-out groups, there was discussion on what forms of technology are currently available versus how reliable certain forms of technology – including artificial intelligence – currently are, and how they will progress in future. Other topics of discussion included the importance of ensuring treatment accessibility for all people living with T1D, and if this was research or a policy
sugar over a three-month period)?
How can healthcare professionals better take into account the physical, psychological, and social aspects of type 1 diabetes in clinics?
Why do some people with type 1 diabetes become insulin resistant and does resistance increase with the number of years a person has diabetes and, if so, why?
question. In particular, the differences in priorities between healthcare professionals and those living with diabetes were discussed at length, and careful consideration was given to the final ranking of questions.
The results of the ultimate top 10 priorities from the final workshop and their ranking in the interim survey can be found in Table 2 . It is notable that the top 10 questions identified by the interim survey overlapped significantly with the final top 10 priorities (seven out of 10 carried forward). As the workshop was held in a virtual format there was no follow-up discussion on the top 10 in the plenary setting, as this would have given greater influence on more confident participants. Instead, participants were invited to give formal feedback on both the top 10 results and their experience of the process.
Discussion
This PSP, led by the Diabetes Collaborative Clinical Trials Network and the JLA, brought together over one thousand individuals with lived experience of, or working with, T1D to identify the most important unanswered questions in this area. Following evidence checking, 65 summary questions were carried forward to a second-round survey in which a top 19 were selected. A final workshop, held online over two days, facilitated detailed and thoughtful discussions between all stakeholders and resulted in the final top 10 priorities.
During this PSP, we adhered to the JLA’s five-step process (establishing steering group, gathering uncertainties, data process and evidence checking, interim priority setting, and final priority setting). The ultimate aim of this robust, multi-step pathway is to identify key areas for research that can improve outcomes and quality of life for those living with T1D and to work with funders to direct researchers and resources towards these topics.
This was a refresh PSP updating
the 10 priorities outlined in 20117 and is one of only four refresh JLA PSPs to date. A refresh PSP is conducted when there has been considerable research developments or changes in clinical practice in an area. 10 The change in diabetes management is evident from the differences in the topics covered by the 2011 and 2024 PSPs and limited overlap. In 2011 there was a focus on insulin pumps, continuous glucose monitors, and closed loop therapy. Most, if not all, of these treatments are now part of routine diabetes care in the UK and Ireland. Current priorities include the use of artificial intelligence; the use of newer technologies to identify foods and accurately count carbohydrates; and
10 space. These questions focused on diabetes distress, insulin resistance, and women’s health. This reflects the importance of group interactions and meaningful exchange in the JLA process. There were also some geographical differences in priorities. Questions regarding the use of hybrid closed loop (HCL) therapy were common to participants from both the UK and Ireland. However, while questions from respondents living in Ireland focused on its safety and efficacy in optimising glucose management, multiple questions from UK participants focused on geographical limitations in technology access – the so-called technology ‘postcode lottery’.11 Differences between diabetes care in
The ultimate aim is to identify key areas for research that can improve outcomes and quality of life for those living with T1D
access to therapies including stem cell transplants and immunotherapy. There was also a new focus on the impact of hormonal changes, menstruation, and menopause on glycaemic management, and the impact of T1D on cognition in older adults, while the impact and the prevention of hypoglycaemia; the psychological burden of living with T1D; and for healthcare professionals, the importance of a person-centred approach during clinical interactions, are of ongoing importance in T1D.
During the final workshop there was enthusiastic debate about the ranking of questions. Different viewpoints were exchanged, and this had a meaningful impact on the ranking of questions. While seven of the final top 10 questions also ranked in the top 10 on the interim survey, three questions moved up from positions 11, 18 and 21 to occupy a top
Ireland and the UK were also illustrated by an announcement from the National Institute of Clinical Excellence’s (NICE) technology appraisal between the initial survey closing and the launch of the interim survey. This approved HCL therapy for any adult with suboptimal diabetes management (ie, a haemoglobin A1c of 58mmol/mol or higher or with disabling hypoglycaemia) despite the use of continuous subcutaneous insulin infusion (CSII) or continuous glucose monitoring.12 This led to a challenge during the evidencechecking phase as questions about availability were comprehensively answered by UK but not Irish guidelines. Due to the number of queries received about HCL therapy and the likelihood that challenges will remain in the rollout of HCL therapy in the UK for some time due to capacity issues, the decision
was made to carry this question forward to the interim survey.
We received nearly 300 individual queries on questions like “when will there be a cure”, “what are the barriers to cure”, and “when a cure is available what will be done to make sure it is offered to everyone with T1D”. While accepting that a cure for T1D is the ultimate goal for all individuals impacted by the disease, the decision was made by the steering group to rule these queries ‘out of scope’ as there is currently no strict definition for cure. 13 For example, some people living with T1D might be satisfied with a once monthly infusion that eliminates the need for insulin delivery and blood glucose monitoring; however, for others this still represents a burden of disease and does not meet the
threshold for cure. 14
This process had a number of strengths, including its robust methodology and the efforts made to establish a diverse range of opinions. Despite this, we also identified some limitations. Although the steering group was balanced based on gender, it was exclusively made up of individuals from white Irish and UK backgrounds. Despite multiple targeted efforts to engage respondents from ethnic minority groups, this population was under-represented at both survey stages. Moreover, the surveys were available in English only, which may have also have limited the range of respondents. 15 Finally, although another media for survey completion was offered, the predominant use of social media and online platforms
to promote the survey may have disadvantaged individuals exposed to digital poverty. 16
Conclusion
Further research is needed to respond to and answer adequately the top 10 important questions identified by this JLA refresh PSP. This rigorous process has highlighted ongoing inadequacies in T1D care in the areas of hypoglycaemia prevention and treatment, holistic care and psychological health, and the need to harness advancements in technology, including artificial intelligence, to improve outcomes for people living with T1D. The publishing of this top 10 priority should serve to motivate researchers and direct funders towards the most pressing unanswered questions in type 1 diabetes. l
References
1. Gajewska KA, Biesma R, Sreenan S, et al. Prevalence and incidence of type 1 diabetes in Ireland: A retrospective cross-sectional study using a national pharmacy claims data from 2016. BMJ Open. 2020;10(4):e032916.
2. Group NS-SD. Scottish Diabetes Survey 2021. In: Service NH, editor. NHS2021.
3. Digital N. National Diabetes Audit 2021-22, Type 1 Diabetes. In: NHS, editor. NHS Digital2022.
4. Crowe S, Fenton M, Hall M, et al. Patients’, clinicians’ and the research communities’ priorities for treatment research: There is an important mismatch. Res Involv Engagem 2015;1:2.
5. Partridge N, Scadding J. The James Lind Alliance: Patients and clinicians should jointly identify their priorities for clinical trials. Lancet 2004;364(9449):1923-4.
6. Oliver N, Holt RIG. The James Lind Alliance research priorities
for diabetes. Diabet Med 2019;36(3):267-8.
7. Alliance JL. Diabetes (type 1) Top 10 2011. Available at: www.jla.nihr. ac.uk/priority-setting-partnerships/ diabetes-type-1
8. Gadsby R, Snow R, Daly AC, et al. Setting research priorities for type 1 diabetes. Diabet Med 2012;29(10):1321-6.
9. Alliance JL. JLA guidebook version 10 2021. Available at: www.jla. nihr.ac.uk/jla-guidebook/downloads/ JLA-Guidebook-Version-10March-2021.pdf
implementation strategy 2024. Available at: www.england.nhs. uk/long-read/hybrid-closed-looptechnologies-5-year-implementationstrategy/
13. Roep BO, Montero E, van Tienhoven R, Atkinson MA, Schatz DA, Mathieu C. Defining a cure for type 1 diabetes: A call to action. Lancet Diabetes Endocrinol. 2021;9(9):553-5.
14. Pettus J, Von Herrath M. The shifting paradigm of a “cure” for type 1 diabetes: Is technology replacing immune-based therapies? Acta Diabetol. 2018;55(2):117-20.
15. Wenz A, Al Baghal T, Gaia A. Language proficiency among respondents: Implications for data quality in a longitudinal face-to-face survey. Journal of Survey Statistics and Methodology. 2020;9(1):73-93.
16. Heponiemi T, Jormanainen V, Leemann L, et al. Digital divide in perceived benefits of online healthcare and social welfare services: National cross-sectional survey Study. J Med Internet Res . 2020;22(7):e17616.
The evolution of technology in the management of type 1 diabetes
Author: Dr Hannah Forde, Consultant Endocrinologist, Beaumont Hospital, Dublin
Type 1 diabetes (T1D) is a chronic autoimmune disease characterised by progressive destruction of the pancreatic beta cells causing insulin deficiency and resultant hyperglycaemia.1
T1D accounts for approximately 5-10 per cent of all diabetes and there are between 20,000 to 30,000 people currently living in Ireland with this disease.2,3 There is currently no cure for T1D and the mainstay of treatment is physiological insulin replacement via multiple daily injections (MDI) of insulin or continuous subcutaneous insulin infusion (CSII) therapy. The aim of care and management is to support the person with diabetes to live a long and healthy life by achieving glycaemic targets, effectively managing cardiovascular risk factors, minimising hypoglycaemia, and maintaining quality of life.
People with T1D must learn to self-adjust their insulin doses in order to achieve glycaemic targets and minimise the risk of microvascular and macrovascular complications. The landmark Diabetes Control and Complications Trial (DCCT) demonstrated that intensive insulin therapy reduced the risk of development and progression of diabetic retinopathy, neuropathy, and nephropathy compared with conventional treatment in people with T1D.4 Data from the Epidemiology of Diabetes Interventions and Complications (EDIC) follow-up observational study confirmed sustained benefits of early intensive glycaemic control for diabetes related microvascular complications and a lower incidence of cardiovascular disease.5 The intervention group in the DCCT maintained a mean haemoglobin (Hb)A1c
of approximately 7 per cent (53mmol/mol), and this study forms the basis for current glycaemic target recommendations for most people with T1D.4
One of the greatest challenges in the management of T1D is balancing tight glycaemic control with the risk of hypoglycaemia, and indeed there was a two- to three-fold increase in the rate of severe hypoglycaemia in the intervention group in DCCT.4 Reported rates of severe hypoglycaemia in unselected cohorts of people with T1D vary from 0.3-3 events per year, whilst non-severe hypoglycaemic events tend to occur twice per week.6
Structured education courses (eg, DAFNE) have been shown to reduce the incidence of severe hypoglycaemia and newer diabetes technologies can also help with many aspects of daily diabetes management including hypoglycaemia prevention.7
CGM: The evidence
Continuous glucose monitoring (CGM) devices have proven to be effective at improving glycaemic control whilst also reducing hypoglycaemia.8,9 These devices consist of three components. A sensor containing a glucose oxidase electrode is inserted under the skin and reacts with glucose in the interstitial fluid to generate hydrogen peroxide and an electron signal.10
A transmitting device sends the electric signal to a receiving device (eg, an insulin pump, a mobile phone, a handheld receiver) which displays the glucose reading, the direction the glucose is travelling, and retrospective glucose data over the preceding number of hours.
These devices have multiple benefits, most obviously, the instant availability of
24 hours of sensor glucose data without any additional fingerstick glucose measurements required of the person with diabetes. In addition, trend arrows are useful for the person with diabetes when deciding on how much quick acting insulin to deliver. Alerts on sensors can warn the person with diabetes about impending hypo-or hyperglycaemia, allowing the person time to take action and prevent the event. In randomised controlled trials, CGM has been associated with a HbA1c reduction of approximately 0.5 per cent compared with self-monitoring of blood glucose.8,11 In 2021, the American Diabetes Association and European Association for the Study of Diabetes published a joint consensus statement recommending CGM for all people with T1D.12 This was mirrored in the updated National Institute for Health and Care Excellence (NICE) guidelines published in 2022, and in the recently published guidelines for the management of T1D in Ireland.3,13
As CGM is now the standard of care in T1D, there are numerous agreed-upon CGM metrics which provide guidance for clinicians and individuals with diabetes in using, interpreting, and reporting CGM data in clinical practice. The most commonly used metric to guide diabetes management is time in target range (sensor glucose between 3.9-10mmol/l), and the international consensus recommendation is that most people with type 1 and type 2 diabetes should aim to spend >70 per cent of their time with their sensor glucose values in the target range.14
Pump therapy
The first use of CSII with an insulin pump was described in 1978.15 However, rapid
uptake of pump therapy did not occur until publication of the DCCT, as individuals on CSII had better glycaemic outcomes compared to those treated with MDI.4 Insulin pumps are small computerised devices that continuously deliver rapid acting insulin to the person with diabetes via a subcutaneous cannula. Historically in Ireland, uptake of pump therapy has been far lower than that of our European counterparts. However, recent data indicates that the number of pump users in Ireland is increasing, and approximately 15 per cent of people with T1D in Ireland are using insulin pump therapy.16 The main advantages of traditional pump therapy were the ability to vary basal insulin delivery and the ease of administering frequent boluses throughout the day. Although the evidence-base for pump therapy suggests their use is associated
typically, if sensor glucose is dropping or predicted to drop below the glucose target, the system will reduce basal insulin delivery. If sensor glucose is rising or predicted to rise above the glucose target, the system will increase insulin delivery. Most systems will deliver autocorrections to manage hyperglycaemia and will halt basal insulin delivery if sensor glucose is predicted to enter the hypoglycaemic range. HCL systems do not fully automate diabetes management and users must continue to deliver boluses for their meals. All of the systems have an override feature which will make the algorithm less aggressive and this is commonly enabled by the person with diabetes to manage insulin delivery around exercise/ activity. There is now ample randomised control trial data, as well as real world evidence, demonstrating the benefits of
Over the last 10 years or so, insulin pump technology has significantly progressed and most pump users are now using hybrid closed loop (HCL) therapy
with reduced hypoglycaemia and improved quality of life, pump use only modestly improves glycaemic control.17-19
Over the last 10 years or so, insulin pump technology has significantly progressed and most pump users are now using hybrid closed loop (HCL) therapy. HCL therapy (also called automated insulin delivery systems or the artificial pancreas) is the most advanced form of insulin delivery available. It involves the augmentation of pump therapy with integrated realtime CGM and a control algorithm which automatically adjusts basal insulin delivery every few minutes based on sensor glucose values. Although there are differences between the various algorithms contained within the systems,
HCL therapy for people with T1D.
The ADAPT study was a multi-centre randomised controlled trial, which compared advanced HCL therapy with the Medtronic 780G system with intermittently scanned CGM and MDI in 82 adults with T1D who had HbA1c levels above 8.0 per cent. 20 In this study, the mean HbA1c of the participants in the intervention group decreased from 9.0 per cent at baseline to 7.3 per cent after three months of HCL.20 This improvement in HbA1c was sustained at six months. Participants in the control group had minimal improvement in their mean HbA1c levels which reduced from 9.1 per cent at baseline to 8.9 per cent at six months.20
Studies comparing HCL therapy with
sensor augmented pump therapy in young children and older adults with T1D have also yielded positive results, with HCL use being associated with higher time in range compared to sensor augmented pump therapy.21,22 In 2021, the National Health Service in England announced funding for a real world pilot of HCL systems for people with T1D who had suboptimal HbA1c levels (>8.5 per cent) despite the use of CGM and traditional pump therapy. Hundreds of individuals from adult diabetes centres in England were invited to participate in this pilot and offered any of the commercially available closed loop systems at the time. Glycaemic and psychosocial outcomes from 520 people with diabetes who were included in the pilot were assessed after six months of HCL therapy.23 The use of HCL was associated with significant improvement in glycaemic metrics, with a mean reduction in HbA1c of 1.7 per cent and a mean increase in time in range of 27.6 per cent.23 Use of HCL was also associated with a reduction in diabetes distress and an improvement in awareness of hypoglycaemia.23
In the past, people with very high HbA1c levels, on MDI, would never have been considered suitable candidates for pump therapy due to concerns around adherence with glucose monitoring, performing set changes, engaging with the clinical team, etc. However, it is likely that this cohort will derive the most benefit from HCL systems. Indeed, a recent observational study investigating the impact of initiating closed loop therapy in high risk individuals with diabetes who had a mean HbA1c of 10.5 per cent at baseline, demonstrated substantial and sustained improvements in both glycaemic control and quality of life after 12 months of HCL therapy.24
In 2023, NICE criteria for HCL eligibility was updated and now all children with T1D under 18 years of age are eligible for HCL therapy. Adults with T1D are eligible for HCL therapy if, despite the use of either CGM or open-loop pump therapy, they have a HbA1c above 7.5 per cent, are experiencing disabling hypoglycaemia, or trying for pregnancy.25 In Ireland, there are no specific eligibility criteria for HCL in T1D. In
theory, anyone with T1D could access HCL, however, significant geographical variation exists in terms of the number of adult diabetes services providing pump therapy.
Available technology
There are currently three commercially available HCL systems in Ireland; the Medtronic 780G system with Smartguard algorithm, the Tandem T:slim X2 pump with Control-IQ algorithm, and the Ypsomed pump with mylife loop algorithm. Unfortunately, Omnipod 5, which is currently the only tubeless automated insulin delivery system, is not available in Ireland at present. There are several factors that need to be considered by the person with diabetes when choosing the right HCL for themselves.
There are differences in the licensing for the systems which may need to be taken into account for young people with diabetes or those planning pregnancy. Some people may have a preference for a particular pump or CGM device which may dictate their choice of HCL system. There are also subtle differences in the algorithms which may have an impact on which system the person with diabetes deems most suitable for their needs. Fortunately, glycaemic outcomes from each of the three systems are very similar. Data from thousands of users of these systems have demonstrated that the mean time in range associated with these systems is 71.5-72.6 per cent, with minimal hypoglycaemia.26,27,28 Glycaemic outcomes with HCL can be further improved by optimising algorithm settings, pre-meal bolusing, accurate carbohydrate counting, and appropriate management of
hypoglycaemia, set failures, and activity. With HCL therapy, as with MDI regimes, optimal bolusing behaviours is associated with higher time in range, ie, bolusing for all meals in advance of the meals. An ancillary study from a randomised control trial evaluating HCL in children with T1D demonstrated time in range of 80 per cent when timing of boluses were optimum. 29 However, time in range was still 59 per cent when the children had two or more suboptimal boluses per day. Furthermore, when children missed two or more boluses per day, they were still able to achieve a time in range of 62 per cent, indicating that the closed loop system in this study compensated remarkably well for missed meal boluses. 29
Historically, in many diabetes services, completion of a structured education course (eg, DAFNE) was a pre-requisite for commencement on insulin pump therapy. However, HCL therapy can somewhat alleviate hyperglycaemia resulting from an underestimation of carbohydrate intake by increasing basal insulin delivery and administering autocorrections. This was demonstrated in the FLEX study, which evaluated adolescents using the Medtronic 780G system, and compared accurate carbohydrate counting with simplified meal announcements, ie, inputting fixed carbohydrate amounts into the bolus advisor for each meal.30
After 12 months of follow-up, there was no significant difference in HbA1c levels between the two groups, although time in range was higher in those who were accurately carbohydrate counting.30
The importance of completing set
changes every two to three days cannot be reiterated strongly enough to people using HCL systems. Any reduction in insulin absorption because of a problem at the insertion site or an issue with the infusion set can affect the algorithm as the system operates based on the assumption that the person is receiving the insulin being delivered by the pump. The absence of long-acting basal insulin in pump users contributes to the rapid development of diabetic ketoacidosis in the event of an infusion set failure. With HCL therapy, it is very unusual to have glucose readings above 15mmol/l for over two hours. If this occurs, the person with diabetes should give the pump one opportunity to correct the hyperglycaemia, and if this does not result in an improvement in glucose levels, infusion site failure should be considered and a complete set change performed.
Conclusion
Over the last decade considerable progress has been made in diabetes care with advancements in automated insulin delivery systems. HCL technology may be useful in a wide array of patient populations including older adults, those with cystic fibrosis-related diabetes, or chronic kidney disease, and could also address unmet needs in inpatient diabetes care. The technology continues to evolve and more advanced systems with more aggressive algorithms and no requirement for food boluses are in development. The future looks bright for T1D care, but increasing access and ensuring equitable access to these technologies is likely to challenge diabetes services going forward. ●
References
1. Katsarou A, Gudbjörnsdottir S, Rawshani A, et al. Type 1 diabetes mellitus. Nat Rev Dis Primers. 2017;3:17016.
2. Daneman D. Type 1 diabetes. Lancet. 2006;367(9513):847-58.
3. Department of Health. Type 1 diabetes mellitus in adults version 2: National
4. Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of longterm complications in insulin-dependent
diabetes mellitus. New Eng J Med 1993;329(14):977-86.
5. The Diabetes Control and Complications Trial (DCCT)/Epidemiology of Diabetes Interventions and Complications (EDIC) Study Research Group. Intensive diabetes treatment and cardiovascular outcomes in type 1 diabetes: The DCCT/EDIC study 30-year follow-up. Diabetes Care
2016;39:686-693.
6. Pedersen-Bjergaard U, Thorsteinsson B. Reporting severe hypoglycaemia in type 1 diabetes: Facts and pitfalls. Curr Diab Rep 2017;17(12):131.
7. Hopkins D, Lawrence IA, Mansell P, Thompson G, Amiel S, Campbell M, Heller S. Improved biomedical and psychological outcomes one year after structured education in flexible insulin therapy for people with type 1 diabetes: The UK DAFNE experience. Diabetes care 2012;35(8):1638-42.
8. Beck RW, Riddlesworth T, Ruedy K, et al. Effect of continuous glucose monitoring on glycaemic control in adults with type 1 diabetes using insulin injections: The DIAMOND randomised clinical trial. JAMA. 2017;317(4):371-8.
9. Heinemann L, Freckmann G, Ehrmann D, Faber-Heinemann G, Guerra S, Waldenmaier D, Hermanns N. Realtime continuous glucose monitoring in adults with type 1 diabetes and impaired hypoglycaemia awareness or severe hypoglycaemia treated with multiple daily insulin injections (HypoDE): A multicentre, randomised controlled trial. Lancet 2018;391(10128):1367-77.
10. Soni A, Wright N, Agwu JC, et al. Fifteen-minute consultation: Practical use of continuous glucose monitoring. Archives of Disease in Childhood-Education and Practice 2022;107(3):188-93.
11. Leelarathna L, Evans ML, Neupane S, et al. Intermittently scanned continuous glucose monitoring for type 1 diabetes. New Eng J of Med. 2022;387(16):1477-87.
12. Holt RI, DeVries JH, Hess-Fischl A, et al. The management of type 1 diabetes in adults. A consensus report by the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes care. 2021;44(11):2589-625.
13. National Institute for Health and Care Excellence. Type 1 diabetes in adults: Diagnosis and management. NICE guideline [NG17]. NICE; 2022. Available at: https://www.nice.org.uk/guidance/NG17.
14. Battelino T, Danne T, Bergenstal
RM, et al. Clinical targets for continuous glucose monitoring data interpretation: Recommendations from the international consensus on time in range. Diabetes Care. 2019;42(8):1593-603.
15. Pickup JC, Keen H, Parsons JA, Alberti KG. Continuous subcutaneous insulin infusion: An approach to achieving normoglycaemia. Br Med J 1978;1(6107):204-7.
16. Blood Sugar Trampoline. Insulin pump use in Ireland. 2023. Available at: www.bloodsugartrampoline.com/ blog/2023/8/16/insulin-pump-usein-ireland
17. Misso ML, Egberts KJ, Page M, O’Connor D, Shaw J. Cochrane review: Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus. Evidence-Based Child Health: A Cochrane Review Journal 2010;5(4):1726-867.
18. REPOSE Study Group. Relative effectiveness of insulin pump treatment over multiple daily injections and structured education during flexible intensive insulin treatment for type 1 diabetes: Cluster randomised trial (REPOSE). BMJ. 2017;356:j1285.
19. Pickup JC, Sutton AJ. Severe hypoglycaemia and glycaemic control in type 1 diabetes: Meta-analysis of multiple daily insulin injections compared with continuous subcutaneous insulin infusion. Diabetic Medicine. 2008;25(7):765-74.
20. Choudhary P, Kolassa R, Keuthage W, et al. Advanced hybrid closed loop therapy versus conventional treatment in adults with type 1 diabetes (ADAPT): A randomised controlled study. Lancet Diabetes Endocrinol. 2022;10(10):720-31.
21. Ware J, Allen JM, Boughton CK, et al. Randomised trial of closed loop control in very young children with type 1 diabetes. New Eng J Med 2022;386(3):209-19.
22. McAuley SA, Trawley S, Vogrin S, et al. Closed loop insulin delivery versus sensor-augmented pump therapy in older adults with type 1 diabetes (ORACL): A randomised, crossover trial. Diabetes Care. 2022;45(2):381-90.
23 Crabtree TS, Griffin TP, Yap YW, et al. Hybrid closed loop therapy in adults with type 1 diabetes and above-target HbA1c: A real-world observational study. Diabetes Care. 2023;46(10):1831-8.
24. Michaels VR, Boucsein A, Watson AS, et al. Glucose and psychosocial outcomes 12 months following transition from multiple daily injections to advanced hybrid closed loop in youth with type 1 diabetes and suboptimal glycaemia. Diabetes Technol Ther. 2024;26(1):40-8.
25. National Institute for Health and Care Excellence. Hybrid closed loop systems for managing blood glucose levels in type 1 diabetes. Technology appraisal guidance. TA943. NICE; 2023. Available at:www. nice.org.uk/guidance/ta943/
26. Choudhary P, Arrieta A, van den Heuvel T, Castañeda J, Smaniotto V, Cohen O. Celebrating the data from 100,000 real-world users of the MiniMed 780G system in Europe, Middle East, and Africa collected over three years: From data to clinical evidence. Diabetes Technol Ther 2024;26(S3):32-7.
27. Messer LH, Breton MD. Therapy settings associated with optimal outcomes for t: Slim X2 with controlIQ technology in real-world clinical care. Diabetes Technol Ther 2023;25(12):877-82.
28. Alwan H, Wilinska ME, Ruan Y, Da Silva J, Hovorka R. Real-world evidence analysis of a hybrid closed loop system. J Diabetes Sci Technol. Published online July 8, 2023.
29. Coutant R, Bismuth E, Bonnemaison E, et al. Hybrid closed loop overcomes the impact of missed or suboptimal meal boluses on glucose control in children with type 1 diabetes compared to sensoraugmented pump therapy. Diabetes Technol Ther. 2023;25(6):395-403.
30. Petrovski G, Campbell J, Pasha M, et al. Twelve-month follow-up from a randomised controlled trial of simplified meal announcement versus precise carbohydrate counting in adolescents with type 1 diabetes using the MiniMed 780G advanced hybrid closed loop system. Diabetes Technol Ther 2024;26(S3):76-83.
The value of accessible vascular assessment tools in diabetic foot disease: An audit of a tertiary level hospital
Author: Astrid Codemo, Clinical Specialist Podiatrist, Beaumont Hospital, Dublin
Diabetes is a serious chronic disease which carries devastating complications such as renal disease, blindness, peripheral neuropathy, diabetic foot disease (DFD), and lower limb amputations. The Irish Longitudinal Study on Ageing estimates that 10 per cent of adults aged 50 years and older have type 2 diabetes (T2D) and 16 per cent of those aged 80 years and older. 1 This rising figure is of particular concern, as the report further suggests that one-in-10 people remain undiagnosed and untreated for their diabetes, resulting in increased risks for future complications such as DFD. DFD accounts for a growing percentage of hospital admissions due to the development of chronic foot ulcerations. This has been reflected in an acute tertiary level hospital in Ireland with persistently rising rates of major and minor lower limb amputation ( Figure 1). These figures have a significant influence over the healthcare budget in Ireland, directly affecting the provision of care for all patients. A registry-based study estimated the approximate costs of a minor diabetic foot amputation to be €23,940, and €42,814 for a major amputation. 2 These figures do not account for the full burden of disease and it is well reported in the literature that the five-year mortality rate post lower limb amputation is over 50 per cent. 3
Current guidelines within the HSE stress the importance of preventative care to identify, educate, and manage DFD. A significant portion of amputations are classified as preventable with timely accessibility to care. However, barriers exist in the provision of this timely care.
BlueDop audit
Inadequate resources, funding, and staffing levels are all contributing factors that reduce timely access to care. An Irish tertiary level hospital was able to identify in an audit that patients were waiting 10 weeks on average for non-invasive vascular assessments,
such as ankle brachial pressure indices (ABPIs) and toe brachial pressure indices (TBPIs). These tests are widely used to diagnose peripheral arterial disease, which is a major risk factor for DFD and helps steer clinical decision making. Delays in interventions and assessments are associated with increased amputation rates and poor outcomes. 4 The BlueDop is a noninvasive bedside measurement of peripheral arterial disease and can be used as an alternative to the gold standard ABPIs and and TBPIs.
The BlueDop device was invented by Vascular Scientist David H King in 2010, and measures the arterial blood pressure
1: Diabetic foot amputation rates at an Irish tertiary level hospital
FIGURE
in the posterior tibial or dorsalis pedis artery through an algorithm. The device then extrapolates information in respect to the velocity of the blood flow and waveform. Additional data such as the brachial arm pressure is inputted, providing the user with a cuff-free ABPI. The result is communicated wirelessly to a tablet monitor.
The BlueDop has several benefits. It can identify peripheral arterial disease, the test can be performed at the bedside by a podiatrist or a nurse, it requires minimal training, and is easy to execute. BlueDop does not need to be performed in a vascular lab by a vascular technician; and so, delays in diagnosing peripheral arterial disease are reduced.
Aims and objectives
The primary objective of the audit was to compare the BlueDop with the hospital vascular laboratory; assessing its accuracy and reliability. The overarching aim was to ascertain the level of value the BlueDop would offer in a clinical setting.
Methodology
The audit was retrospective in nature and resulted in a sample size of 23 patients who met the essential criteria –a history of diabetes and an active foot ulceration. Patient records and results were evaluated across a number of platforms including CELLMA, NIMIS, McKesson Radiology Manager, and HIPE data. The data was collected, anonymised, and entered into a working excel document in line with GDPR requirements.
Findings
General demographics
All of the subjects except for one were male, 20 of the 23 patients had T2D, and the remainder had T1D. Average age of the sample was 67 years. The majority of cases had a history of hypertension, high cholesterol, and many had received some level of vascular intervention (39
per cent). A total of 17 per cent were smokers and 4 per cent had end stage renal failure.
Accessibility to care
Accessibility to care was determined by the wait time for either a podiatry appointment or for ABPIs in the vascular laboratory. Wait time to see the podiatrist and have the BlueDop performed was 11 working days. The Bluedop assessment took an average of 13 minutes to perform.
The average wait time for the vascular laboratory assessment to have ABPIs
devices. The Bluedop only assessed the posterior tibial pulse location, whereas dorsalis pedis was often assessed in the vascular reports reviewed. This variation in locations makes it difficult to draw consistent trends and comparisons.
Audit design: The audit design was a major limitation in this study, as the auditing team was not comparing data from the same point in time, therefore, making it impossible to draw an accurate comparison. Around 65 per cent of ABPIs reports reviewed from the vascular lab
BlueDop does not need to be performed in a vascular lab by a vascular technician; and so, delays in diagnosing peripheral arterial disease are reduced
and TBPIs was 10 weeks in nine cases, the other 14 cases were still awaiting a vascular laboratory appointment by the time the audit had finished. There were a further two cases of booked vascular studies that were cancelled with no rescheduled date.
Comparability to the traditional ABPI
Non-compressible vessels: Peripheral arterial disease and vessel calcification is a common occurrence in diabetic patients. A significant portion of the cases (five) indicated non compressible vessels in excess of 250mmHg. However, the Bluedop was able to produce an ABPI reading and mmHg values for all of these cases, as the technology is not impacted by vessel calcification.
Variation in assessment locations: The location of the peripheral pulse was not consistent between the two
were more than 12 months old. This further demonstrates a significant level of strain on the service. Further refinement of the audit design would allow for a direct comparison.
Discussion
The National Institute for Health and Care Excellence guidelines outline that under the suspicion for peripheral arterial disease, a cardiovascular, ABPI, and doppler assessment must be performed. 5 These assessment tools are operator dependent and can produce skewed readings due to arterial calcification, often seen in diabetes and ageing demographics. ABPIs and TBPIs can be difficult to do in patients with active foot ulceration as the site of the ulcer can interfere with the application of the test.
Accessibility to care is outlined in the
Flexitol is a medically proven regime for dry, cracked heels and feet. All of our products contain Urea; a major constituent of the skin’s natural moisturising factor, which improves hydration by increasing the water uptake from dermis, removing dead skin cells, enhancing skins ability to retain water and improving amount of water the skin can hold.
contain Urea; a major constituent of the skin’s natural moisturising factor, which improves hydration by increasing the water uptake from dermis, removing dead skin cells, enhancing the skins ability to retain water and improving the amount of water the skin can hold.
STEP 1
TREAT
Contains 25% Urea
Intense moisturisation
Visible results in 1 day
Suitable for diabetics
Medically proven STEP 1
PROFESSIONAL
Contains 25% Urea
Intense moisturisation
Visible results in 1 day
Suitable for diabetics
Medically proven
PROFESSIONAL
STEP 2 MAINTAIN
STEP 2
MAINTAIN
Use to maintain healthy skin after treatment with Flexitol Heel Balm
Contains 10% Urea
Use to maintain healthy skin after treatment with Flexitol Heel Balm
Enriched with Vitamin E
Contains 10% Urea
Intensive hydration and skin nourishing, rapidly absorbed
FOOTCARE EVERY STEP OF THE WAY
Enriched with Vitamin E
Intensive hydration and skin nourishing, rapidly absorbed
FOOTCARE EVERY STEP OF THE WAY
AVAILABLE IN ALL GOOD PHARMACIES. ALWAYS READ THE LABEL.
AVAILABLE IN ALL GOOD PHARMACIES. ALWAYS READ THE LABEL.
HSE Diabetic Foot Model of Care 6 as a key requirement for a multidisciplinary foot unit. To facilitate this, the correct provision of resources and adequate staffing levels are required. The results identify that there are significant wait times for bedside vascular studies in laboratory setting in the tertiary
waiting to have their up-to-date ABPIs performed in the vascular laboratory. Due to these limitations, previous ABPI results done at different time points were used as a comparison for the audit, however the location of the peripheral pulse differed between the BluDop device and the ABPI reports
The BlueDop is a portable device that can be used in an outpatient setting or in the community, allowing for an immediate bedside vascular assessment, with an average assessment time of 13 minutes
hospital. This patient demographic has active DFD and delayed access to care will impact outcomes. This audit was undertaken during the time of the HSE recruitment embargo, likely further impacting staffing levels and the provision of care to some degree. The audit did not assess if there were any amputations as a result of the delayed access to care. However, all ulcerations remain active to date.
The BlueDop is a portable device that can be used in an outpatient setting or in the community, allowing for an immediate bedside vascular assessment, with an average assessment time of 13 minutes. It is a user-friendly device which can be operated by a multitude of healthcare professionals. Increasing vascular screening services at community level may reduce the strain on tertiary level services as inappropriate referrals can be effectively triaged.
The premise of the audit was not to determine whether the BlueDop is as accurate as the ABPI machine or could replace the ABPI machine as a diagnostic test. The rationale was that a small cohort of patients were and are still
reviewed. Therefore, more patients and a standardisation of the BluDop and ABPI examination is required before we could say that the BluDop machine could take the place of the ABPI in the
References
1. Leahy S, O’ Halloran AM, O’Leary N, et al. Prevalence and correlates of diagnosed and undiagnosed type 2 diabetes mellitus and pre-diabetes in older adults: Findings from the Irish Longitudinal Study on Ageing (TILDA). Diabetes Res Clin Pract 2015;110(3):241-249.
2. Mealy A, Tierney S, Sorensen J. Lower extremity amputations in Ireland: A registry-based study. Ir J Med Sci. 2022;191(2):839-844.
3. McPherson M, Carroll M, Stewart S. Patient-perceived and practitioner-perceived barriers to accessing foot care services for people with diabetes mellitus: A systematic literature review. J Foot Ankle Res . 2022;15(1):92.
measurement of peripheral arterial disease in people with diabetes.
Limitations
Audit design is a major limitation as it was reliant on previously performed vascular studies. Conducting a study in lab conditions at the same point in time would provide a clearer picture. The sample size was relatively small, limiting its applicability.
Conclusion
Due to study design limitations, an accurate conclusion cannot be drawn in respect to comparing ABPIs at a tertiary level hospital vascular laboratory to the BlueDop. The study demonstrates significant strains on the healthcare system, with wait times impacting patient outcomes. The BlueDop device is an innovative tool that could be used in a multitude of settings to help triage and direct care patient care. However, further research needs to be performed to conclude if this tool can replace traditional ABPI methods. ●
4. Nickinson ATO, Bridgwood B, Houghton JSM, et al. A systematic review investigating the identification, causes, and outcomes of delays in the management of chronic limb-threatening ischaemia and diabetic foot ulceration. J Vasc Surg. 2020;71(2):669-681.e2.
5. Kordzadeh A, Hoff M, Tokidis E, King DH, Browne T, Prionidis I. Novel assessment (BlueDop) device for detection of lower limb arterial disease: A prospective Comparative Study. J Ultrasound Med. 2018;37(3):763-768.
6. Health Service Executive. Diabetic foot model of care. Dublin: HSE; 2022. Available at: www.hse. ie/eng/about/who/cspd/ncps/ diabetes/moc/diabetic-foot-modelof-care-2021.pdf.
GIP, GLP-1, GLP-2, and bone
Authors: Asif Ali; Prof Peter R Flatt; and Prof Nigel Irwin, Diabetes Research Centre, Biomedical Sciences Research Institute, Ulster University, Coleraine, Northern Ireland
Bone formation and resorption are dynamic processes that exhibit diurnal variations. This circadian rhythm is regulated by food intake, and specifically, secretion and biological action of gut derived peptide hormones, including glucose-dependent insulinotropic polypeptide (GIP), glucagon-like peptide-1 (GLP-1), and glucagon-like peptide-2 (GLP-2). GIP and GLP-1 have wellestablished roles in regulating glucose and energy metabolism, whereas GLP-2 is better known for intestinotrophic actions. However, in addition to this, these hormones can also influence bone turnover by directly, or indirectly, modulating the activity of osteoblast and osteoclast cells. As such, postprandial secretion of GIP, GLP-1, and GLP-2 inhibits bone resorption and/or promotes bone formation, representing a ‘gut-bone’ axis. Notably, GLP-1 and GIP/GLP-1 hybrid drugs are now clinically employed for diabetes and obesity, whereas GLP-2 drugs are used in the clinic to treat short bowel syndrome. However, clinical data relating to the potential of these drugs to improve bone health is only now beginning to emerge. In addition, preclinical studies with dual-acting GIP/GLP-2 hybrid peptides demonstrate particular therapeutic promise for bone disorders, which merits further clinical exploration. This review summarises current literature on gut-derived hormones in relation to bone homeostasis, with particular emphasis on subsequent therapeutic application for bone disease.
Introduction
Bone is a dynamic tissue that serves as a structural framework for the body,
1: Origin of bone cells. Mesenchymal stem cells and haematopoietic stem cells represent precursors in the development of osteoblasts and osteoclasts, respectively
facilitating movement, protecting vital organs, and acting as a reservoir for minerals such as calcium and phosphate in the form of hydroxyapatite. 1 Along with the intestine and kidneys, bone plays a key role in regulating circulating calcium levels. 1 The origin of bone tissue is rooted in early embryonic development, which follows two distinct pathways that include intramembranous ossification and endochondral ossification. 1,2 Intramembranous ossification primarily occurs in the skull as well as a portion of the clavicle, where mesenchymal stem cells (MSCs) directly differentiate into osteoblasts ( Figure 1). This process involves three main stages, namely proliferation, matrix maturation, and mineralisation, leading
to the formation of bone without a prior cartilaginous phase. 1,2,3
In contrast, endochondral ossification is the predominant mechanism controlling bone formation throughout the remainder of the skeletal system. It occurs in two main phases, firstly a cartilage template is formed in a nonvascularised environment, and then subsequently this template is gradually replaced by bone tissue through the formation of the periosteum, which harbours immature osteoprogenitor cells that differentiate into osteoblasts. Osteoclasts are derived from haematopoietic stem cells (HSCs), specifically from the monocyte/ macrophage lineage (Figure 1). 1,2,3 These processes continue to play essential roles
FIGURE
in bone growth, repair, and regeneration throughout life.
Disruption of the bone remodelling equilibrium leads to skeletal diseases including osteoporosis, Paget’s disease of bone, rheumatoid arthritis, as well as osteogenesis imperfecta. 4 Further to this, metabolic disorders, for example diabetes and obesity, have been shown to negatively alter the bone microenvironment and compromise bone quality. 5 A major component of this detrimental effect is thought to originate from obesity-diabetes induced changes in the secretion and biological action of gut-derived peptide hormones. Thus, an emerging area of research into the relationship between gut health and bone metabolism, often referred to as the ‘gutbone axis’, has gained much attention of late. 5 For example, recent preclinical and clinical observations highlight the role of gut-derived peptides such as GIP, GLP-2, and to a lesser extent, GLP-1 in the maintenance of overall skeletal health ( Figure 2), 6,7,8 opening new avenues for the understanding and potential treatment of bone disorders.
In this review, the roles of GIP, GLP-1, and GLP-2 receptor signalling in the regulation of bone homeostasis are appraised (Figure 2). Mechanisms of action and implications for clinical practice are then considered, alongside the promise of continuing research to unlock new therapeutic opportunities for managing bone-related disorders and improving patient outcomes.
Gut-bone axis
Overview
Bone remodelling exhibits well recognised diurnal variations, regulated by the circadian rhythm and influenced through the secretion of gut-derived peptide hormones.9 During the day, bone resorption is suppressed, presumably related to food intake and secretion of intestinal-derived hormones, whereas resorption increases at night and during periods of extended fasting ( Figure 2).9,10 As well as gut hormones,
FIGURE 2: Schematic demonstrating the link between food intake, gut-derived hormones, and bone health. Emphasis is placed on secretion and action of GIP, GLP-1, and GLP-2 as part of the gut-bone axis. GIP and GLP-1 may exert direct and/or indirect positive effects on bone health through increased bone formation, reduced resorption, and improved bone material properties. For GLP-2, inhibition of bone resorption is mediated indirectly, as detailed within the text
bone remodelling is also known to be regulated by parathyroid hormone (PTH) and influenced by various other biochemical factors, such as calcitonin, oestrogen, thyroid hormones, glucocorticoids, insulin-like growth factors (IGFs), bone morphogenetic proteins (BMPs), prostaglandins, vitamin D, and transforming growth factor β (TGF-β), 4,11 but the focus of this report will primarily be gut hormones.
Clinically, bone density can be assessed by dual-energy x-ray absorptiometry (DEXA), with interpretation used to diagnose or assess risk of osteoporosis. 12 However, in addition to this, bone formation and resorption can be appraised through measurement of specific circulating biomarkers. For bone formation, procollagen type 1 N propeptide (P1NP) and osteocalcin (OCN) serve as key indicators, 13 both being secreted from osteoblasts. Bone resorption on the other hand, can be monitored through assessment of serum
carboxy-terminal telopeptide of type I collagen (CTX-I) levels. In this regard, CTX-I, derived from mature type I collagen, directly reflects the degradation of collagen fibres during the process of bone resorption.7,8,13
Gut-derived peptides and bone
There is now unmistakable evidence to demonstrate that gut hormones play a key role in regulating bone metabolism, particularly through inhibition of bone resorption. 10 Importantly, this suppression is not observed during daytime fasting when gut hormone secretion is reduced, 14 highlighting direct effects of peptide hormones on bone turnover in response to nutritional status. Moreover, reductions of circulating CTX-I are more pronounced following oral glucose administration than intravenous glucose infusion, further indicating that gut derived hormones, rather than glucose levels per se, modulate bone turnover. 15 As such, GIP, secreted by
enteroendocrine K-cells, and GLP-1, released from corresponding intestinal L-cells, collectively referred to as the incretin hormones, are well-studied for their roles in glucose homeostasis and energy balance. 6,7,8,9,10,16 Indeed, GLP-1 receptor (GLP-1R) agonists, such as liraglutide and semaglutide, are approved for the treatment of both type 2 diabetes (T2D) and obesity.7,8,17 Moreover, the dual GIP and GLP-1 receptor agonist tirzepatide has also recently been clinically approved for the same applications. 18 GLP-2, also secreted by enteroendocrine L-cells, differs from GLP-1 and GIP in that it appears to have less influence on metabolic control and primarily functions as an intestinotrophic factor, helping maintain intestinal health. 3,19 On this basis, the long-acting GLP-2 mimetic, teduglutide, has gained clinical approval for short bowel syndrome. 20 Thus, drugs utilising GIP, GLP-1, or GLP-2 receptor signalling pathways are already in clinical use, which should make potential application within the bone disease arena less complicated (Figure 3).
Diabetes, obesity, and bone health
In conditions such as obesity and T2D, the balance between bone formation and resorption is disturbed, leading to bone health issues. 5 There is no doubt that chronic hyperglycaemia, a hallmark of all types of diabetes, as well as insulin resistance, adversely affects bone integrity. 5,6 In addition, receptor activator of nuclear factor kappa beta ligand (RANKL), that plays a crucial role in osteoclast activity and bone resorption, 21 also directly influences pancreatic betacell function and overall metabolism, with its activity being compromised in obesity and T2D. 5,21 Furthermore, 24 months treatment with the anti-osteoporotic drugs denosumab (Dmab) and alendronate in T2D lead to improvements of bone mineral density (BMD), but Dmab also induced a modest improvement in glycaemic control when compared to alendronate. 22 This further highlights the link between glucose regulation, T2D, and bone disease, suggesting Dmab may offer dual benefits in managing both bone health and hyperglycaemia.
Hyperglycaemia can also elevate levels of tumoir necrosis factor (TNF)-α and interleukin (IL)-6, cytokines linked to increased osteoclast activity.5,6 Additionally, high glucose levels negatively impact osteoblast function, contributing to bone defects partly through the production of advanced glycation end-products (AGEs), which upregulates sclerostin, an inhibitor of osteoblast activity.23 Studies in insulin-resistant and insulin-deficient animal models, as well as humans, continue to highlight the adverse effects of obesity and T2D on bone integrity.5-8,10 Ultimately, obesity and T2D are associated with detrimental structural changes in bone, such as decreased trabecular bone connectivity and cortical bone thickness, increasing the risk of fractures and impairing healing.5-8 In this regard, it is well recognised that the secretion and action of GIP and GLP-1 is disturbed in obesity and T2D,5-10,16-18 which could also directly impact skeletal health. It follows that drugs used for the treatment of T2D, and especially those that increase bioactivity of gut-derived hormones, could exert added benefits on bone health.11,15-18
FIGURE 3: Potential impact of clinically approved GLP-1, GLP-2 as well as GIP/GLP-1 hybrid peptides on bone. GLP-1 drugs (exenatide, liraglutide etc), as well as GIP/GLP-1 hybrid peptides (tirzepatide), are clinically approved for diabetes and/or obesity, with GLP-2 based drugs (teduglutide) approved for the treatment of short bowel syndrome. Potential additional beneficial effects of these drugs on bone are depicted
GLP-1
GLP-1 plays a key role in maintaining glucose homeostasis by enhancing glucose-dependent insulin secretion from pancreatic beta-cells,7 as well as inhibiting glucagon secretion and suppressing appetite.7,10 The mechanisms by which GLP-1 influences bone remodelling are thought to involve several pathways. GLP-1R activation in osteoclasts can modulate bone turnover through the mitogen-activated protein kinase (MAPK) and nuclear factor kappa B (NF- κ B)/MAPK- nuclear factor of activated T-cells 1 (NFATc1) pathways, respectively. 24 However, the GLP-1R is not evidenced in mature osteoblasts, but it is expressed in bone marrow stromal cells (BMSCs). Furthermore, GLP-1 has been shown to stimulate calcitonin secretion
MC3T3-E1 cells by activating ERK5 signalling pathway. 28 In rodent models, genetic knockout of the GLP-1R reduces bone quality and maturity of the collagen matrix. 29 In keeping with this, the GLP-1 mimetics exendin-4 and liraglutide improve trabecular bone microarchitecture and reduce osteoclast activity in ovariectomised (OVX) mice. 30 Additionally, GLP-1 and exendin-4 restored femur and vertebrae bone mass in hyperlipidaemic and hypercaloric Wistar rats. 31 In OVX insulin-deficient streptozotocin (STZ) diabetic rats, liraglutide significantly lowered serum CTX-I levels and inhibited osteoclast differentiation. 32 Fortunately, successful introduction of GLP-1 drugs into clinical practice has facilitated more detailed study of GLP-1 effects on bone health in
Fortunately, successful introduction of GLP-1 drugs into clinical practice has facilitated more detailed study of GLP-1 effects on bone health in the human setting
from the thyroid gland, which may further contribute to protective effects on bone, 25 but whether this action is relevant in humans still needs to be clarified. 26
GLP-1 and effects on bone metabolism
Several studies show that the GLP-1R is expressed in some bone cells, including osteoclasts and BMSCs, but appears to be absent in mature osteoblasts, indicating a complex role in bone homeostasis that is incompletely understood. 27 In vitro activation of the GLP-1R by exendin-4 enhanced osteogenic differentiation while inhibiting adipogenic differentiation of BMSCs. 28 In addition, liraglutide enhanced osteoblastic differentiation and proliferation in
the human setting (Figure 3). Accordingly, liraglutide was initially found to increase bone formation and preserve bone mineral content in obese women, providing early clinical evidence of GLP-1 drug benefits on bone health. 33 Moreover, liraglutide treatment for 26 weeks reduced body weight without adversely affecting bone mineral density (BMD) in patients with T2D. 34 Equally, the GLP-1 mimetics exenatide, dulaglutide, liraglutide, albiglutide, and semaglutide helped preserve bone density and reduce fracture risk in older adults with T2D. 35 Notably, this protective effect appears to be dependent on the duration of treatment, with only a GLP-1RA treatment period exceeding 52 weeks being associated with decreased fracture
risk. 36 In good accordance, increased postprandial GLP-1 levels are associated with a reduced risk of osteoporosis in non-diabetic postmenopausal women. 37 In addition, Zhang et al (2020) found that a single nucleotide polymorphism (SNP) in GLP-1R, rs2295006, was negatively associated with lumbar and total hip BMD in postmenopausal women, and similar observations have been made more recently by others. 38,39 That said, there are also reports of no significant impact of exenatide on BMD or fracture risk in T2D, 40 with subsequent metaanalyses also yielding conflicting outcomes. 41,42 Overall, whilst slightly inconsistent, there does appear to be a neutral or potential positive impact of GLP-1R signalling on bone health. Furthermore, the impact of GLP-1 mimetics to inhibit appetite and reduce body weight should also be considered when interpreting effects of these drug on bone turnover in humans.
GIP
Similar to GLP-1, GIP is best known as an incretin hormone with fundamental effects on the maintenance of glucose homeostasis. 16,18 However, in addition to this, the presence of functional GIP receptor (GIPR) on bone osteoblast cells has been confirmed many years ago. 43 Similarly, Zhong et al (2007) identified GIPRs on murine osteoclasts, suggesting an important and direct impact of GIP in both the formation and breakdown of bone tissue. 44
GIP and effects on bone metabolism
In agreement with direct receptor effects on osteoblasts and osteoclasts, GIP exerts both an anabolic and anti-catabolic action in bone. 10,16,18 Initial observations in rodents demonstrated that native GIP positively affected bone density in OVX rats. 43 Subsequent preclinical research utilising enzyme-resistant longacting GIP peptides, as well as genetic manipulation of the GIPR, reinforced these early findings. For instance, in STZ-
& colecalciferol (vitamin D )
DESUNIN ®
• Available in 800 IU tablets and 4000 IU tablets
• Daily flexible dosing of 800 IU - 4000 IU Vitamin D3
ABBREVIATED PRESCRIBING INFORMATION:
Desunin (colecalciferol), 800 IU & 4000 IU Tablets.
Please refer to Summary of Product Characteristics (SmPC) before prescribing.
Indications, Dosage and Administration:
Desunin 800 IU:
Desunin 800 IU is indicated for the prevention and treatment of vitamin D deficiency in adults and adolescents.
In addition to specific osteoporosis treatment of patients who are at risk of vitamin D deficiency, preferably in combination with calcium
Desunin 4000 IU:
Desunin 4000 IU is indicated for the treatment of vitamin D deficiency in adults and adolescents.
Vitamin D deficiency is defined as serum levels of 25-hydroxycolecalciferol (25(OH)D) < 25 nmol/l.
Recommended dose: One tablet per day.
The dose should be adjusted dependent upon desirable serum levels of 25-hydroxycolecalciferol (25(OH)D), the severity of the disease and the patient´s response to treatment.
The daily dose should not exceed 4000 IU.
Pediatric population
The safety and efficacy of Desunin in children under 12 years have not been established.
Dosage in hepatic impairment
No dose adjustment is required.
Dosage in renal impairment
Desunin should be used with caution in patients with renal impairment (see section 4.4 of the SmPC).
Administration: The tablets can be swallowed whole or crushed. The tablets can be taken with food.
Presentation: Tablets
Contraindications:
• Diseases and/or conditions resulting in hypercalcaemia or hypercalciuria.
• Nephrolithiasis
• Nephrocalcinosis
• Hypervitaminosis
D
• Hypersensitivity to the active substance or to any of the excipients listed in section 6.1 of the SmPC
Warnings and precautions:
Desunin should be prescribed with caution to patients suffering from sarcoidosis due to risk of increased metabolism of
During long-term treatment, serum calcium levels should be followed, and renal function should be monitored through
metabolised normally and other forms of vitamin D may therefore be needed.
The content of vitamin D (800 IU or 4000IU) in Desunin should be considered when prescribing
excretion frequently.
Excipients: Desunin contain sucrose, isomalt and sodium. Patients with rare hereditary problems of fructose intolerance, glucose-galactose malabsorption or sucrase-isomaltase insufficiency should not take this medicine.
This medicine contains less than 1 mmol sodium (23 mg) per tablet, that is to say essentially ‘sodium-free’.
Interactions with other medicinal products and other forms of interactions:
Thiazide diuretics reduce the urinary excretion of calcium. Due to the increased risk of hypercalcaemia, serum calcium should be regularly monitored during concomitant use of thiazide diuretics.
Concomitant use of phenytoin or barbiturates may reduce the effect of vitamin D since the metabolism increases.
Excessive dosing of vitamin D can induce hypercalcaemia, which may increase the risk of digitalis toxicity and serious arrhythmias due to the additive inotropic effects. The electrocardiogram (ECG) and serum calcium levels of patients should be closely monitored.
Glucocorticoid steroids may increase vitamin D metabolism and elimination. During concomitant use, it may be necessary to increase the dose of Desunin tablets.
Simultaneous treatment with orlistat or ion exchange resins such as cholestyramine or laxatives such as paraffin oil may reduce the gastrointestinal absorption of vitamin D.
Fertility, pregnancy and lactation:
Fertility - There are no data on the effect of Desunin on fertility. However, normal endogenous levels of vitamin D are not expected to have any adverse effects on fertility.
Pregnancy - Desunin should be used during pregnancy, only in the case of a vitamin D deficiency. Desunin is not recommended during pregnancy in patients without a
Studies in animals have shown reproductive toxicity of high doses of vitamin D (see section 5.3 of the SmPC).
There are no indications that vitamin D at therapeutic doses is teratogenic in humans.
Breast-feeding - Vitamin-D can be used during breast-feeding. Vitamin D3 passes into breast milk. This should be considered when giving additional vitamin D to the child.
Undesirable effects:
Very common (≥1/10): None
Common (>1/100, <1/10): None
For details of uncommon, rare and very rarely reported adverse events and those of unknown frequency, see SmPC.
Reporting of adverse reactions:
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance, Website: www.hpra.ie.
Adverse reactions/events should also be reported to the marketing authorisation holder at the email address: pv.ireland@viatris.com or phone 0044(0)8001218267.
Legal Category: Product subject to prescription which may be renewed (B)
Full Prescribing Information available on request from: Viatris, Dublin 17. Email: enquiry.ire@viatris.com.
Date of revision of Abbreviated Prescribing Information: 30 June 2023
Reference Number: IE-AbPI-Desunin-v005
Viatris,
diabetic mice the GIPR agonist, (D-Ala2) GIP, improved bone quality and halted matrix degradation, ultimately enhancing fracture resistance. 45 Additional studies confirmed that N-AcGIP, another longacting GIP agonist, 46 decreased osteoclastmediated bone resorption and enhanced cortical bone quality in rodents. 46 In keeping with this, transgenic mice overexpressing GIP exhibit increased bone mass and enhanced osteoblast activity at 24 months of age, whilst GIPR KO leads to decreased BMD, cortical thickness, and overall bone strength. 47,48 Human studies yield somewhat mixed results regarding the impact of GIP on bone metabolism. Early studies found no significant effect of intravenous GIP on bone resorption, 10 whereas more recently, GIP infusion was shown to suppress the bone resorption marker CTX-I and transiently increase the bone formation marker P1NP in people with T1D as well as healthy controls. 16,49 Similarly, Skov-Jeppesen et al (2019) reported that subcutaneous GIP injection increased P1NP by 15 per cent in healthy men, that is thought to be associated with transiently lowered PTH levels. 50,51 Moreover, GIP infusion significantly reduced CTX-I levels in healthy humans, 52 as well as in T1D or T2D, 53 indicating a robust suppression of bone resorption in various settings that is independent of the established effects of GIP on insulin secretion. Further investigations of inherent variations of the GIPR within the normal population reveal that the missense GIPR variant, rs1800437 (Glu354Gln) that results in diminished GIPR signalling, leads to lower BMD and increased risk of non-vertebral fractures in perimenopausal Danish women. 54 Interestingly, in a similar study of 426,824 individuals, another GIPR variant, Glu288Gly, was associated with lower BMD, but no increase in fracture risk. 55 Indeed, a more recent large metaanalysis confirmed that while GIPR variants may influence BMD, this does not necessarily translate to increased bone fracture risk. 56 Taken together, it is
clear that GIPR signalling affects bone turnover, but the overall significance of these effects need to be fully determined. Interestingly, tirzepatide, a dual-acting GIP/GLP-1 receptor agonist that is now clinically approved for both obesity and T2D, was designed with an amino acid sequence closely resembling that of native GIP, resulting in strong preference for GIPR binding over the GLP-1R. This unique receptor activity makes tirzepatide a promising candidate for improving bone health in obesity and diabetes, through the positive effects of GIP, and potentially GLP-1, on bone metabolism. Although tirzepatide has not demonstrated anabolic bone actions
Human studies yield somewhat mixed results regarding the impact of GIP on bone metabolism
in animals, 57 an assessment report from the European Medicine Agency observed trends of decreased P1NP and increased CTX-I levels in people with T2D after 29 days of treatment. The exact mechanism behind this action on bone remains unclear, but likely relates to benefits of GIP, and perhaps GLP-1, on bone as described in ( Figure 3). 58
GLP-2
The primary physiological effect of GLP-2 appears to be within the intestine, where GLP-2 promotes small and large intestinal growth through stimulating cell proliferation and inhibiting apoptosis in the crypt compartment. 19 GLP-2 also enhances intestinal barrier function, increases glucose transport, and boosts mesenteric blood flow. 50 Together this has led to the approval of long-acting GLP-2 drugs for the treatment of short bowel syndrome. 20 In relation to bone, GLP-2 receptors have been detected in osteoblast-like cell lines such as MG63 and TE-85, 59 but presence in mature osteoblasts and other bone-related cells is yet to be confirmed. This has led to speculation that GLP-2 may act indirectly on bone cells in humans, with the presence of GLP-2R on the parathyroid gland suggesting a potential link between GLP-2, PTH secretion, and bone turnover. Consistent with this, the anti-resorptive effect of GLP-2 is absent in patients with hypoparathyroidism, 50 further supporting a role of PTH in GLP-2 mediated effects on bone in humans.
GLP-2 and effects on bone metabolism
In osteoporotic (SAMP6) mice, sixweek treatment with GLP-2 was shown to reduce bone loss and improve bone microstructure. 60 In contrast, the longacting enzyme resistant form of GLP-2, namely (Gly2)GLP-2, did not provide benefit on bone strength in a mouse model of bone fragility, 61 despite promoting the expression of bone matrix genes and reducing osteoclast number in the in vitro setting. 60 However, in humans, early studies demonstrated that GLP-2 administration for five weeks increased spinal BMD in people with short bowel syndrome, 62 but had limited overall bone benefits. Interestingly, GLP-2 administration leads to a reduction in PTH levels in people with an intact intestine, but not in those with short bowel syndrome, 63 indicating that an intact small intestine is required for GLP-2 mediated suppression of PTH secretion. Further to this, a dose escalation study with GLP-2 (100, 200, 400, and 800μg, single subcutaneous injections) in postmenopausal women revealed dosedependent reductions of CTX-I levels and related bone resorption, 10 that are believed to be sustainable in nature. 64 Overall, GLP2 appears to be an important regulator of bone metabolism, primarily through
inhibiting bone resorption, but with minimal effects on bone formation.
Clinical relevance and future studies
The relationship between diabetes, obesity, and bone health is of significant clinical importance. Obesity and T2D disrupt the balance between bone formation and resorption, leading to increased bone fragility and fracture risk. 65 In this regard, the incretin hormones, namely GIP and GLP-1, represent key targets for the treatment of T2D and obesity, but are also known to play significant roles in bone metabolism, especially in terms of GIP. In addition, GLP-2, an intestinotrophic hormone with clinical application for short bowel syndrome, reduces bone resorption. Thus, drugs that target GIP, GLP-1, or GLP-2 receptor signalling pathways could be employed for treating bone diseases. The potential success of this approach is enhanced given that GIP, GLP-1, and GLP-2 based drugs are already in clinical use, although postulated benefits on bone health still need to be fully confirmed (Figure 3). Thus, whilst data linked to specific bone effects of these clinically
approved drugs in humans is still evolving, the initial outlook is positive. In addition, multi-acting unimolecular peptides have emerged as highly promising therapeutics in obesity and T2D, typified by the GIP/GLP-1 hybrid peptide tirzepatide. Observations relating to the impact of tirzepatide on bone are still very much in their infancy, but there are suggestions that this drug could improve bone strength and reduce fracture risk. Further to this, early preclinical work with dual GIP/GLP-2 hybrid analogues demonstrates considerable therapeutic promise. Specifically, GL-0001 represents a first-inclass dual-acting GIP/GLP-2 peptide that improves bone biomechanical properties, preserves trabecular bone structure as well as increasing collagen cross-linking. 66 Targeting multiple peptide hormone receptors with the same drug entity appears to be the most promising strategy, where additive, or even synergistic, benefits of simultaneously activating two receptor signalling pathways in bone can be fully realised.
Conclusion
Gut hormones play a fundamental role in controlling bone homeostasis and
maintaining optimal bone strength and quality. Preclinical studies in rodents with long-acting GIP, GLP-1, and GLP-2 analogues, alongside related clinical trials, suggest these molecules are safe, and furthermore, may improve overall bone health. Additionally, agents capable of positively modulating more than one peptide hormone receptor simultaneously, such as tirzepatide or the recently characterised GL-0001 peptide, could offer an even more exciting avenue to help realise the potential of gut-derived hormones to treat bone disease. ●
ACKNOWLEDGEMENTS AND FUNDING
The authors’ work on gut-derived hormones and obesity-diabetes has been generously supported over many years by Diabetes UK, Invest Northern Ireland, the Irish Endocrine Society, Northern Ireland Department for the Economy, and Ulster University Strategic Funding.
References
1. Su N, Yang J, Xie Y, et al. Bone function, dysfunction and its role in diseases including critical illness. Int J Biol Sci 2019;15(4):776-787.
2. Olsen BR, Reginato AM, Wang W. Bone development. Annu Rev Cell Dev Biol 2000;16:191-220.
3. Percival CJ, Richtsmeier JT. Angiogenesis and intramembranous osteogenesis. Dev Dyn. 2013;242(8):909-22.
4. Feng X, McDonald JM. Disorders of bone remodeling. Annu Rev Pathol 2011;6:121-45.
5. Wang J, You W, Jing Z, et al. Increased risk of vertebral fracture in patients with diabetes: A meta-analysis of cohort
studies. Int Orthop. 2016;40(6):1299-307.
6. Ali A, Flatt PR, Irwin N. Gut-derived peptide hormone analogues and potential treatment of bone disorders in obesity and diabetes mellitus. Clin Med Insights Endocrinol Diabetes 2024;17:11795514241238059.
7. Mabilleau G, Pereira M, Chenu C. Novel skeletal effects of glucagon-like peptide-1 (GLP-1) receptor agonists. J Endocrinol 2018;236(1):R29-R42.
8. Mabilleau G, Bouvard B. Gut hormone analogues and skeletal health in diabetes and obesity: Evidence from preclinical models. Peptides. 2024; 177:171228.
9. Bjarnason NH, Henriksen EE, Alexandersen P, et al. Mechanism of circadian variation in bone resorption.
Bone. 2002;30(1):307-13.
10. Henriksen DB, Alexandersen P, Bjarnason NH, et al. Role of gastrointestinal hormones in postprandial reduction of bone resorption. J Bone Miner Res. 2003;18(12):2180-9.
11. Chen YJ, Jia LH, Han TH, et al. Osteoporosis treatment: Current drugs and future developments. Front Pharmacol. 2024;15:1456796.
12. Blake GM, Fogelman I. The role of DXA bone density scans in the diagnosis and treatment of osteoporosis. Postgrad Med J. 2007;83(982):509-17.
13 Kuo TR, Chen CH. Bone biomarker for the clinical assessment of osteoporosis: Recent developments and future perspectives. Biomark Res. 2017;5:18.
14. Kueper J, Beyth S, Liebergall M, Kaplan L, Schroeder JE. Evidence for the adverse effect of starvation on bone quality: A review of the literature. Int J Endocrinol. 2015;2015:628740.
15. Lei WS, Kilberg MJ, Zemel BS, et al. Bone metabolism and incretin hormones following glucose ingestion in young adults with pancreatic insufficient cystic fibrosis. J Clin Transl Endocrinol 2022;30:100304.
16. Bergmann NC, Lund A, Gasbjerg LS, et al. Separate and combined effects of GIP and GLP-1 infusions on bone metabolism in overweight men without diabetes. J Clin Endocrinol Metab. 2019 Jul 1;104(7):2953-2960.
17. Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in the treatment of type 2 diabetes – state-ofthe-art. Mol Metab. 2021;46:101102.
18. Nauck MA, D’Alessio DA. Tirzepatide, a dual GIP/GLP-1 receptor co-agonist for the treatment of type 2 diabetes with unmatched effectiveness regrading glycaemic control and body weight reduction. Cardiovasc Diabetol 2022;21(1):169.
19. Drucker DJ, Erlich P, Asa SL, Brubaker PL. Induction of intestinal epithelial proliferation by glucagonlike peptide 2. Proc Natl Acad Sci US 1996;93(15):7911-6.
20. Jeppesen PB, Lund P, Gottschalck IB, et al. Short bowel patients treated for two years with glucagon-like peptide 2: Effects on intestinal morphology and absorption, renal function, bone and body composition, and muscle function. Gastroenterol Res Pract 2009;2009:616054.
21. Vega D, Maalouf NM, Sakhaee K. CLINICAL Review: The role of receptor activator of nuclear factor-kappaB (RANK)/RANK ligand/osteoprotegerin: Clinical implications. J Clin Endocrinol Metab. 2007;92(12):4514-21.
22. Wang K, Gao L, Liu C, Bao X, Tian Y, Li Y. Denosumab improves glycaemic parameters in postmenopausal osteoporosis patients with combined type 2 diabetes mellitus. Cell Mol Biol
2023;69(8):185-191.
23. Piccoli A, Cannata F, Strollo R, et al. Sclerostin regulation, microarchitecture, and advanced glycation end-products in the bone of elderly women with type 2 diabetes. J Bone Miner Res 2020;35(12):2415-2422.
24. Li Z, Li S, Wang N, Xue P, Li Y. Liraglutide, a glucagon-like peptide-1 receptor agonist, suppresses osteoclastogenesis through the inhibition of NF- κ B and MAPK pathways via GLP-1R. Biomed Pharmacother 2020;130:110523.
25. Yamada C, Yamada Y, Tsukiyama K, et al. The murine glucagon-like peptide-1 receptor is essential for control of bone resorption. Endocrinology. 2008;149(2):574-9.
27. Meng J, Ma X, Wang N. Activation of GLP-1 receptor promotes bone marrow stromal cell osteogenic differentiation through β -Catenin. Stem Cell Reports 2016;6(4):579-591.
28. Sun Y, Liang Y, Li Z, Xia N. Liraglutide promotes osteoblastic differentiation in MC3T3-E1 cells by ERK5 pathway. Int J Endocrinol. 2020;2020:8821077.
29. Mabilleau G, Mieczkowska A, Irwin N, Flatt PR, Chappard D. Optimal bone mechanical and material properties require a functional glucagon-like peptide-1 receptor. J Endocrinol. 2013;219(1):59-68.
30. Pereira M, Jeyabalan J, Jørgensen CS, et al. Chronic administration of Glucagon-like peptide-1 receptor agonists improves trabecular bone mass and architecture in ovariectomised mice. Bone. 2015;81:459-467.
31. Nuche-Berenguer B, Lozano D, Gutiérrez-Rojas I, et al. GLP-1 and exendin-4 can reverse hyperlipidicrelated osteopaenia. J Endocrinol 2011;209(2):203-10.
32. Wen B, Zhao L, Zhao H, Wang X. Liraglutide exerts a bone-protective effect in ovariectomised rats with streptozotocin-induced diabetes by inhibiting osteoclastogenesis. Exp Ther Med. 2018;15(6):5077-5083.
33. Iepsen EW, Lundgren JR, Hartmann B, et al. GLP-1 receptor agonist treatment increases bone formation and prevents bone loss in weight-reduced obese women. J Clin Endocrinol Metab 2015;100(8):2909-17.
34. Hygum K, Harsløf T, Jørgensen NR, Rungby J, Pedersen SB, Langdahl BL. Bone resorption is unchanged by liraglutide in type 2 diabetes patients: A randomised controlled trial. Bone 2020;132:115197.
35. Zhang YS, Weng WY, Xie BC, et al. Glucagon-like peptide-1 receptor agonists and fracture risk: A network meta-analysis of randomised clinical trials. Osteoporos Int. 2018;29(12):26392644.
36. Cheng L, Hu Y, Li YY, et al. Glucagonlike peptide-1 receptor agonists and risk of bone fracture in patients with type 2 diabetes: A meta-analysis of randomised controlled trials. Diabetes Metab Res Rev. 2019;35(7):e3168.
37. Montes Castillo MC, Martínez Ramírez MJ, Soriano Arroyo R, et al. Glucagon-like peptide 1 and Glucagonlike peptide 2 in relation to osteoporosis in non-diabetic postmenopausal women. Sci Rep. 2019;9(1):13651.
38. Zhang L, He J, Sun X, et al. Relationship between glucagon-like peptide-1 receptor gene polymorphism and bone mineral density in postmenopausal women in Shanghai. Ann Palliat Med. 2020;9(4):1732-1741.
39. Liu C, Bao X, Tian Y, Xue P, Wang Y, Li Y. Polymorphisms in the glucagonlike peptide-1 receptor gene and their interactions on the risk of osteoporosis in postmenopausal Chinese women. PLoS One. 2023;18(12):e0295451.
40. Bunck MC, Eliasson B, Cornér A, et al. Exenatide treatment did not affect bone mineral density despite body weight reduction in patients with
type 2 diabetes. Diabetes Obes Metab 2011;13(4):374-7.
41. Mabilleau G, Mieczkowska A, Chappard D. Use of glucagon-like peptide-1 receptor agonists and bone fractures: A meta-analysis of randomised clinical trials. J Diabetes 2014;6(3):260-6.
42. Hansen MS, Wölfel EM, Jeromdesella S. Once-weekly semaglutide versus placebo in adults with increased fracture risk: A randomised, double-blinded, twocentre, phase 2 trial. EClinicalMedicine 2024;72:102624.
43. Bollag RJ, Zhong Q, Ding KH, et al. Glucose-dependent insulinotropic peptide is an integrative hormone with osteotropic effects. Mol Cell Endocrinol 2001;177(1-2):35-41.
44. Zhong Q, Itokawa T, Sridhar S, et al. Effects of glucose-dependent insulinotropic peptide on osteoclast function. Am J Physiol Endocrinol Metab 2007;292(2):E543-8.
45. Mansur SA, Mieczkowska A, Flatt PR, Bouvard B, Chappard D, Irwin N, Mabilleau G. A new stable GIPOxyntomodulin hybrid peptide improved bone strength both at the organ and tissue levels in genetically-inherited type 2 diabetes mellitus. Bone. 2016;87:102-13.
46. Mabilleau G, Mieczkowska A, Irwin N, et al. Beneficial effects of a N-terminally modified GIP agonist on tissue-level bone material properties. Bone. 2014;63:61-8.
47. Ding KH, Shi XM, Zhong Q, et al. Impact of glucose-dependent insulinotropic peptide on ageinduced bone loss. J Bone Miner Res 2008;23(4):536-43.
48. Mieczkowska A, Irwin N, Flatt PR, Chappard D, Mabilleau G. Glucosedependent insulinotropic polypeptide (GIP) receptor deletion leads to reduced bone strength and quality. Bone 2013;56(2):337-42.
49. Westberg-Rasmussen S, StarupLinde J, Hermansen K, et al. Differential impact of glucose administered intravenously or orally on bone
turnover markers in healthy male subjects. Bone (2017) 97:261-66.
50. Skov-Jeppesen K, Svane MS, Martinussen C, et al. GLP-2 and GIP exert separate effects on bone turnover: A randomised, placebo-controlled, crossover study in healthy young men. Bone. 2019;125:178-185.
51. Gabe MBN, Skov-Jeppesen K, Gasbjerg LS, et al. GIP and GLP-2 together improve bone turnover in humans supporting GIPR-GLP-2R co-agonists as future osteoporosis treatment. Pharmacol Res 2022;176:106058.
52. Gasbjerg LS, Hartmann B, Christensen MB, et al. GIP’s effect on bone metabolism is reduced by the selective GIP receptor antagonist GIP(330)NH2. Bone. 2020;130:115079.
53. Christensen MB, Lund A, Calanna S, et al. Glucose-dependent insulinotropic polypeptide (GIP) inhibits bone resorption independently of insulin and glycaemia. J Clin Endocrinol Metab 2018;103(1):288-294.
54. Torekov SS, Harsløf T, Rejnmark L, et al. A functional amino acid substitution in the glucose-dependent insulinotropic polypeptide receptor (GIPR) gene is associated with lower bone mineral density and increased fracture risk. J Clin Endocrinol Metab 2014;99(4):E729-33.
55. Kizilkaya HS, Sørensen KV, Kibsgaard CJ, et al. Loss of function glucose-dependent insulinotropic polypeptide receptor variants are associated with alterations in BMI, bone strength, and cardiovascular outcomes. Front Cell Dev Biol. 2021;9:749607.
56. Styrkarsdottir U, Tragante V, Stefansdottir L, et al. Obesity variants in the GIPR gene are not associated with risk of fracture or bone mineral density. J Clin Endocrinol Metab. 2024;109(8):e1608-e1615.
57. Mishra R, Raj R, Elshimy G, et al. Adverse events related to tirzepatide. J Endocr Soc. 2023;7(4):bvad016.
59. Pacheco-Pantoja EL, Ranganath LR, Gallagher JA, Wilson PJ, Fraser WD. Receptors and effects of gut hormones in three osteoblastic cell lines. BMC Physiol. 2011;11:12.
60. Huang YM, Xu B, Kuai Z, et al. Glucagon-like peptide-2 ameliorates age-associated bone loss and gut barrier dysfunction in senescence-accelerated mouse prone 6 mice. Gerontology 2023;69(4):428-449.
61. Gobron B, Bouvard B, Legrand E, Chappard D, Mabilleau G. GLP-2 administration in ovariectomised mice enhances collagen maturity, but did not improve bone strength. Bone Rep 2020;12:100251.
62. Haderslev KV, Jeppesen PB, Hartmann B, et al. Short-term administration of glucagon-like peptide-2: Effects on bone mineral density and markers of bone turnover in short bowel patients with no colon. Scand J Gastroenterol. 2002;37(4):392-8.
63. Gottschalck IB, Jeppesen PB, Hartmann B, Holst JJ, Henriksen DB. Effects of treatment with glucagonlike peptide-2 on bone resorption in colectomised patients with distal ileostomy or jejunostomy and short bowel syndrome. Scand J Gastroenterol. 2008;43(11):1304-10.
64. Henriksen K, Neutzsky-Wulff AV, Bonewald LF, Karsdal MA. Local communication on and within bone controls bone remodelling. Bone 2009;44(6):1026-33.
65. Xing B, Yu J, Zhang H, Li Y. RANKL inhibition: A new target of treating diabetes mellitus? Ther Adv Endocrinol Metab. 2023;14:20420188231170754.
58. Gasbjerg LS, Rosenkilde MM, Meier JJ, Holst JJ, Knop FK. The importance of glucose-dependent insulinotropic polypeptide receptor activation for the effects of tirzepatide. Diabetes Obes Metab. 2023;25(11):3079-3092.
66. Gobron B, Couchot M, Irwin N, Legrand E, Bouvard B, Mabilleau G. Development of a first-in-class unimolecular dual GIP/GLP-2 analogue, GL-0001, for the treatment of bone fragility. J Bone Miner Res 2023;38(5):733-748.
The impact of a nurse-led obesity management clinic in general practice
Obesity is described by the HSE as a chronic, complex, and progressive neuroendocrine disease, and is defined as abnormal or excessive adiposity that impairs health. It is reportedly the fastest growing disease globally, placing a massive burden on healthcare systems worldwide. General practice is the ideal setting for identifying and treating obesity, as it encompasses patientcentred care across the lifespan of the patient, and is often described as care ‘from the cradle to the grave’.
Background
I joined general practice as an advanced nurse practitioner (ANP) in 2019 after specialising in acute and interventional cardiology. I have a Masters in Preventive Cardiology and a professional interest in the preventative side of health, as it is so important in all aspects of life.
In general practice I saw that there is fantastic software to keep records and data; however, after completing an audit, I noted that weight, height, and body mass index (BMI) were generally not recorded for patients. This triggered a subsequent inhouse audit and a change in local policy that all patients would have demographics recorded as part of their vital signs.
Identifying patients for review
All nursing staff aligned to make every contact count, including an ANP, a
general practice nurse (GPN), and a phlebotomy/medical assistant. Every patient that attended for review or annual bloods had their height, weight, and waist circumference recorded. Once a patient was identified as obese or having a BMI that was not within a healthy range, they were coded for early intervention and booked in for a visit with the ANP. We recognise that
the disease of obesity is not defined by anthropological measurements alone, therefore, we also utilised a Canadian staging tool – the Edmonton staging system for a holistic assessment which considers physical, psychological, and metabolic parameters – to determine optimal obesity treatment.
Once patients were booked in for review, it became evident that most of
them were happy to be identified and to discuss their obesity. These patients had never had their obesity acknowledged before, with many not realising that it was a disease, and instead they believed it was self-inflicted. A lot of these patients had no weight recorded on their electronic health record and had never been told by their healthcare professional that they were obese. Some patients also perceived a stigma associated with their weight, with many being told to ‘eat less, move more’, which was the primary framework and approach to weight loss and obesity until recent years.
In 2021, when medications became available for people living with obesity without diabetes, it was a game changer. We now had a tool in our arsenal that could significantly improve outcomes and wellbeing for this patient group. In response to Ireland’s National Obesity Policy and Action Plan, which was launched in 2016 and aligns with the National Framework for the Integrated Prevention and Management of Chronic Disease in Ireland, I attained SCOPE certification – an internationally recognised standard of obesity management expertise – and we launched our obesity management clinic.
Results from a nurse-led obesity management clinic
Once a patient is identified, he or she is invited in for a consultation, where full anthropological measurements and vital signs are obtained. We discuss the disease of obesity and its impact on their life, as well as dietary and lifestyle modifications, previous weight loss journeys, and medications. I ensure the patients are aware that obesity is a disease and not their fault, confirming they understand it is the condition of obesity that makes them overeat and not the overeating that causes obesity. I also introduce the concept of medication during consultations and educate on the mechanisms of action. It is important to ensure the patient
TABLE 1: BMI values at six and 12 months
TABLE 2: Weight loss (kg) at six and 12 months
understands that all chronic diseases are treated with medications to keep them under control and that obesity is no different. The medications are available, and they regulate the hunger and satiety hormones, quietening the hunger voices. Medications, in conjunction with healthy lifestyle choices, used to treat obesity and comorbidities such as pre-diabetes, metabolic syndrome, infertility, and cardiovascular disease (CVD), are showing favourable results.
An inhouse audit of patients in our clinic without diabetes on glucagon-like peptide 1 (GLP-1) medications for obesity management from 2021 to present was undertaken. The demographics were audited from patients that continued on the medication and included:
Effects on hypertension;
Effects on wellbeing;
Reduced BMI;
Cardiovascular benefits.
The results are positive and reflect a reduction in BMI, an improvement in wellbeing, and a reduction in CVD risk, including hypertension and lipid profile. The results are outlined in Tables 1-4 . A numerical value of 0 has been allocated where data was unavailable.
Conclusion
While these are positive and promising outcomes, obesity, like all chronic diseases, requires life-long therapy and these medications are currently very expensive. There is a reimbursement pathway for liraglutide, but it has a very rigid criteria that not all patients fit into. The patient must have a BMI above 35 with CVD risk factors such as hypertension or hypercholesteraemia, be on medications, plus present with both impaired fasting glucose and elevated glycated haemoglobin (A1C).
There are a range of new therapies on the market; however, not all are available, reimbursable, or licensed for this patient cohort in Ireland at this time, which is frustrating. For now, we work with what we have and there is a lot more hope for the future. For patients
TABLE 3: Blood pressure values at baseline and 12 months
not responding to existing treatment or requiring bariatric services, we work closely with our colleagues in speciality care. We are also lucky to have a collaborative ANP contact in Loughlinstown and Galway to discuss cases with and refer patients to when it is outside our capacity to treat appropriately. But usually, for most patients, nurse-led clinics in general practice are the ideal setting for managing their chronic disease. ●
TABLE 4: Perceived mental health status at six and 12 months
Obesity medication is not only for Christmas but for life
Authors: Dr Faisal I Almohaileb and Prof Carel le Roux, Diabetes Complications Research Centre, University College Dublin
In the late 19th Century, obesity was largely dismissed as a mere spectacle rather than a genuine medical concern. Figures like Miss Conley, infamously labelled the ‘fattest woman in the world’, and Daniel Lambert, who weighed an astonishing 335kg at his death in 1809, were objects of public curiosity rather than being considered as patients with a severe form of a common disease. Their extreme cases captivated the public’s imagination, yet they were exploited for entertainment rather than managed medically. During this period, the prevailing view was that obesity was a visible manifestation of gluttony and sloth due to a lack of self-control. Obesity was thus considered a personal failure rather than a disease.
The history of obesity as a chronic disease
In 1904, Dr Leonard Williams suggested that obesity might not solely result from overeating and sedentary behaviour, but could also be linked to metabolic imbalances. This revolutionary idea challenged the simplistic view that weight gain was entirely within an individual’s control. Williams recognised that the habit of overeating often formed in youth, during periods of high physical activity, and these habits could persist into adulthood, even as physical activity levels decreased. He also noted that drinking fluids with meals could increase appetite and accelerate the passage of food through the stomach, leading to greater food consumption. Williams emphasised the importance of
chewing food until it becomes fluid and tasteless as a natural method to reduce food intake. His approach to treating obesity focused on dietary modifications and increased physical activity, laying the groundwork for more structured interventions in the future.
In 1902, WM Bayliss and EH Starling published their discovery of secretin, a hormone released into the bloodstream by the small intestine when acidic stomach contents enter it. This hormone stimulates the secretion of digestive juices from the pancreas needed for food breakdown. This showed that pancreatic regulation involves the nervous system and chemical signals, allowing Bayliss and Starling to speculate that organs can communicate and coordinate their activities through bloodborne chemical messengers; a concept now fundamental to our understanding of endocrinology and human biology.
In 1958, Dr Daniel Cappon argued that obesity should not be defined solely by body weight, but by the pathological accumulation of adipose tissue. He emphasised that obesity was not just about how much someone weighed, but about the distribution and function of fat within the body. This perspective highlighted the inadequacy of using simple bodyweight measurements to define obesity. In 1994, leptin was discovered, and, in 1999, ghrelin was also shown to regulate hunger and fat storage. Leptin, produced by adipose tissue, signals the brain to reduce appetite when fat stores are sufficient, while ghrelin, made in the gastrointestinal tract, stimulates hunger. These discoveries
were pivotal in shifting the understanding of obesity from a matter of willpower to a complex endocrine disorder, and a turning point that began to focus on the intricate systems that regulate metabolism and body weight. It became clear that obesity was not simply a result of overeating, but involved a complex interplay of genetic, hormonal, and environmental factors. This realisation laid the groundwork for a more sophisticated approach to treating obesity – one that considered the underlying biological processes driving weight gain.
The birth of statins
Another disease that caused high rates of cardiovascular death, dyslipidaemia, was managed primarily through diet and exercise. However, in 1985, the work of Michael Brown and Joseph Goldstein was awarded the Nobel Prize for discovering the low-density lipoprotein (LDL) receptor and the HMG-CoA reductase pathway, which explained how cholesterol is synthesised and regulated in the liver. Their research led to the development of statins, a class of drugs that inhibit the HMG-CoA reductase enzyme in the liver, lowering LDL cholesterol levels and reducing the risk of cardiovascular death. Statins quickly became the gold standard for managing dyslipidaemia and preventing death, transforming the treatment landscape. The introduction of statins was a watershed moment, as it provided a highly effective pharmacological tool for managing a condition previously unsuccessfully treated with diet and exercise. Despite their effectiveness, statins also highlighted the challenges of long-term
therapy for chronic diseases. By the late 1990s, it became clear that while statins were highly effective in reducing cholesterol levels and preventing cardiovascular events, patient adherence was a significant issue. Recognising dyslipidaemia as a disease catalysed effective management. This shift paved the way for innovative strategies addressing the root causes of poor adherence. By integrating patient-centred approaches and leveraging technology, we have developed personalised treatment plans and support systems that enhance patient engagement and adherence – resulting in patients living longer and with a better quality of life. This lesson is now relevant when treating obesity, where long-term adherence to therapy is equally critical for achieving sustained health benefits.
Pharmacological management of obesity
The story of how the treatment of dyslipidaemia was transformed is repeated for obesity treatment with glucagonlike peptide (GLP) receptor agonists. In the 1980s, the role of GLP-1 in glucose metabolism was discovered, particularly its ability to stimulate insulin secretion, inhibit glucagon release, and slow gastric emptying – fundamental mechanisms for managing type 2 diabetes and obesity. However, the native GLP-1 peptide was rapidly degraded in the body, necessitating the development of long-acting analogues.
In 2004, liraglutide was discovered as a longer-acting GLP-1 receptor agonist, allowing for once-daily dosing. Approved by the US Food and Drug Administration in 2009 for type 2 diabetes, and later in 2014 for obesity, liraglutide significantly improved glycaemic control and promoted weight loss, marking a significant advance in obesity treatment.
Building on liraglutide’s success, semaglutide was developed as a onceweekly GLP-1 receptor agonist, offering greater convenience and efficacy. Approved in 2017 for diabetes and in 2019 for obesity, semaglutide enabled 15 per cent weight loss, which was unprecedented for obesity
pharmacotherapies. The next leap came with tirzepatide, a dual GIP (gastric inhibitory polypeptide, also known as a glucosedependent insulinotropic polypeptide), and GLP-1 receptor agonist, pushing weight loss to over 20 per cent. These drugs also significantly improved obesity-related complications such as type 2 diabetes, hypertension, and dyslipidaemia. The turning point was in 2023, when, for the first time ever, a randomised control trial confirmed that treating the disease of obesity with semaglutide resulted in fewer cardiac deaths.
However, as with the introduction of statins, the widespread adoption of GLP-1 therapies faced significant hurdles. By 2024, adherence to these medications remained a challenge. The high cost of GLP-1 analogues also posed a substantial barrier to longterm use. Additionally, gastrointestinal side-effects such as nausea and vomiting, while generally mild, especially during the initial phase of treatment, contributed to the discontinuation of therapy for some patients. Most importantly, neither patients nor doctors thought of obesity as a biological disease, and, hence, taking lifelong medication made little sense to them. This was problematic because the full benefits of GLP-1 therapy only manifest with long-term usage. Early discontinuation prevents many patients from realising these long-term health improvements. This mirrored the challenges seen with statins, where the benefits of continuous use were clear, but patient adherence was the Achilles’ heel.
A complex and chronic disease
The evolution of obesity treatment reflects a broader shift in understanding the disease as complex and chronic, requiring longterm management. Treating obesity as a biological disease, much like dyslipidaemia, offers significant opportunities for improving patient outcomes. Just as statins became a lifelong therapy for those at risk of cardiovascular disease, GLP-1 analogues and other emerging obesity treatments will have to become integral components of long-term management strategies, focusing on sustained health improvements rather
than short-term weight loss. This approach requires a shift in how clinicians and patients view obesity. The goal must move beyond short-term weight loss to achieving health gain, sustained improvements in overall health metrics such as blood pressure, glucose levels, lipid profiles, and, most importantly, obesity complications prevention. Treating obesity as a chronic disease necessitates lifelong management strategies akin to the treatment of hypertension or diabetes. It also means that healthcare systems must adapt, ensuring that these treatments are accessible and that patients receive the ongoing support they need to adhere to long-term therapy.
The understanding of obesity has changed from lifestyle choices to recognising it as a biological disease. This marks a significant milestone in medical science, opening doors to more effective and compassionate patient care. The evolution from essential dietary advice to advanced hormonal therapies highlights the tremendous strides in treating obesity. This progress underscores the critical need for ongoing research, robust patient education, and the development of comprehensive, accessible treatment strategies to maximise the benefits of these advancements.
Conclusion
The journey of GLP-1 receptor agonists –from their initial research stages to their prominent role in managing obesity –mirrors the broader evolution in chronic disease treatment. By acknowledging obesity as a biological disease that demands continuous management rather than a one-time cure, the focus has shifted toward long-term health outcomes instead of merely achieving short-term weight loss. This approach aligns obesity management with the treatment models of other chronic diseases, such as asthma, hypertension, and diabetes. Obesity is thus no more or less unique than any other chronic disease, and all we need to do is put it in the same box and manage it the same way we do with other chronic diseases. ●
References available on request
A holistic approach to hypothyroidism and Hashimoto’s thyroiditis
Author: Dr Shandeep Momi, MRCGP, Functional Thyroid Care, Dublin
Thyroid disorders, particularly Hashimoto’s thyroiditis, are among the most common endocrine conditions encountered in clinical practice. Conventional treatment protocols, typically centred around levothyroxine (T4) replacement and monitoring thyroid-stimulating hormone (TSH) levels, are effective for many patients, but leave a significant subset with persistent symptoms despite normalised biochemical markers. 1 These patients often report continued fatigue, cognitive impairment, weight gain, and mood disturbances, among other symptoms, even with TSH levels within the reference range.
A more comprehensive approach to thyroid care, focusing not just on TSH but also on triiodothyronine (T3) levels, thyroid antibodies, adrenal health, gut function, sleep, and stress management, is critical for improving clinical outcomes. This well-rounded methodology recognises that thyroid disease, particularly Hashimoto’s, is not merely a thyroid disorder, but often a manifestation of broader systemic dysfunction, particularly involving the immune system and other hormonal axes. This article will explore the limitations of conventional thyroid management, the role of T3 in clinical outcomes, the importance of addressing autoimmunity in Hashimoto’s thyroiditis, and the value of an all-inclusive approach in managing these complex cases.
Hypothyroidism vs Hashimoto’s: Understanding the difference In a clinical setting, there is very little distinction made between the diagnosis of Hashimoto’s and hypothyroidism. It is understood the two are effectively the same, which is why they are managed clinically in the same way. However, to appropriately manage them, it is incumbent that two diagnoses be properly understood.
Hypothyroidism refers to the general condition in which the thyroid gland does not produce enough thyroid hormone (T3 and T4), resulting in a reduction of the metabolism of the body. This slowdown is caused by a number of factors including iodine deficiency, radiation/ chemotherapy treatment, medications, infective disorders, and a host of unknown drivers. More rarely, dysfunction of the pituitary gland or hypothalamus can also directly impact hormone production in the thyroid gland. There are over 400 symptoms associated with an underactive thyroid, but the most common tend to be fatigue, brain fog, depression/anxiety, cold intolerance, constipation, weight gain, and hair loss (eyebrows in particular). Hashimoto’s, known also as Hashimoto’s thyroiditis or Hashimoto’s disease, is a specific autoimmune condition wherein the thyroid gland is directly impacted. The usual case is when the immune system mistakenly attacks the thyroid gland, leading to inflammation and gradual destruction of the thyroid tissue. Over time, if the process is not curtailed, the damage reduces the gland’s ability to produce thyroid hormones, resulting in hypothyroidism. Hashimoto’s is the most
common form of hypothyroidism in the developed world and is characterised by the combination of underactive thyroid symptoms, the presence of thyroid antibodies (anti-thyroid peroxidase antibodies and anti-thyroglobulin antibodies), and/or the presence of a positive ultrasound for chronic inflammatory changes.
Thyroid physiology and the limitations of conventional management
The thyroid gland secretes T4 and T3 as the main thyroid hormones. T4 is converted to the active hormone T3, primarily in the liver, kidneys, muscles, and other peripheral tissue. T3 exerts the main metabolic effects at the cellular level, affecting the cell at all levels and stimulating cellular DNA to increase metabolism and thermogenesis. TSH is secreted by the anterior pituitary and acts as a regulatory signal for thyroid hormone production. Conventional management of hypothyroidism relies heavily on monitoring serum TSH and adjusting T4 replacement accordingly. This approach is rooted in the assumption that normalising TSH will restore euthyroid status across all tissues, a hypothesis that holds for many, but not all, patients. TSH and free thyroxine (FT4) measurements, while useful, do not always reflect the intracellular availability of T3, the biologically active thyroid hormone. A significant number of patients on T4 monotherapy fail to convert adequate amounts of T4 to T3, leaving them with persistent hypothyroid symptoms
despite normal TSH levels. This phenomenon, often referred to as ‘tissue hypothyroidism’, highlights the need for a more nuanced approach to thyroid hormone replacement therapy.
The role of T3:
Beyond
TSH and T4
T3, the metabolically active form of thyroid hormone, is responsible for binding to nuclear receptors and regulating gene expression involved in metabolic processes, thermogenesis, and cognitive function. Research has shown that a subset of patients, especially those with low peripheral conversion capacity (T4 to T3), continue to exhibit hypothyroid symptoms on levothyroxine monotherapy due to suboptimal T3 levels. The failure to adequately convert T4 to T3 can be attributed to several factors, including chronic inflammation, insulin resistance, nutrient deficiencies (selenium and zinc), and genetic polymorphisms such as those affecting the deiodinase enzymes (particularly DIO1 and DIO2). 2,3,4
Clinical trials suggest that combination therapy using both T4 and T3 may offer symptom relief for patients who fail to thrive on T4 monotherapy. A meta-analysis of randomised controlled trials has demonstrated that a subset of patients report improved quality of life and symptom relief with combination therapy compared to T4 alone, despite equivalent serum TSH levels. Another randomised clinical trial showed use of T3 medication reduced body weight and resulted in greater thyroid hormone action on lipid metabolism, without detected differences in cardiovascular function or insulin sensitivity. 5 Furthermore, reverse T3 (rT3), an inactive isomer of T3, can competitively inhibit the binding of T3 to its receptor, further exacerbating symptoms in patients with elevated rT3. Conditions such as chronic stress, critical illness, and systemic inflammation can increase rT3 production, leading to functional hypothyroidism at the tissue level, despite normal serum T4 and TSH.
Hashimoto’s thyroiditis: Autoimmunity at the core Hashimoto’s thyroiditis, the most common cause of hypothyroidism in developed nations, is an autoimmune condition characterised by lymphocytic infiltration and destruction of the thyroid gland. The conventional approach to Hashimoto’s often overlooks the autoimmune nature of the disorder, focusing instead on managing hypothyroidism solely through thyroid hormone replacement via levothyroxine. However, thyroid hormone replacement does not address the underlying immune dysregulation that drives the progression of Hashimoto’s, leaving patients at risk for continued thyroid destruction and the potential development of additional autoimmune conditions like asthma, lupus, and type 2 diabetes, to name a few.
Measuring thyroid antibodies – thyroid peroxidase antibodies (TPOAb) and thyroglobulin antibodies (TgAb) – is essential for diagnosing Hashimoto’s, yet these tests are not always included in routine thyroid screening. The most common method of testing is to screen for only TPOAb to confirm the diagnosis of Hashimoto’s, while ignoring the TgAb. To properly diagnose Hashimoto’s, either the TPOAb or the TgAb must be present in the blood results, in addition to hypothyroid symptoms. Elevation of either thyroid antibodies indicates an ongoing autoimmune process, even when TSH remains within the reference range. In patients with elevated antibodies, addressing the immune dysfunction is critical to halting or slowing the progression of thyroid damage.
A
comprehensive approach: Addressing immune dysregulation, inflammation, and the gut-thyroid axis
To effectively manage Hashimoto’s thyroiditis, it is necessary to address the autoimmune component of the disease. The immune system’s attack on the thyroid gland must be mitigated through a combination of dietary,
lifestyle, and therapeutic interventions aimed at reducing inflammation, supporting immune tolerance, and restoring gut integrity.
1. Gut health and the gut-thyroid axis
The gut plays a pivotal role in both thyroid hormone metabolism and immune system function. Approximately 20 per cent of T4 is converted to T3 in the gut, and intestinal dysbiosis or increased intestinal permeability (‘leaky gut’) can impair this conversion. Moreover, the gut-associated lymphoid tissue is a major regulator of immune function, and disruptions in gut health are linked to the development and exacerbation of autoimmune diseases, including Hashimoto’s thyroiditis. 6
Several studies have established the connection between gut permeability and autoimmune thyroid disease. Zonulin, a marker of intestinal permeability, is often elevated in patients with Hashimoto’s, suggesting that addressing gut integrity may play a crucial role in modulating the immune response. Dietary interventions, such as the removal of gluten or dairy (which shares molecular mimicry with thyroid tissue), can reduce intestinal inflammation and lower antibody levels in some patients.7
2. Adrenal function and the hypothalamic-pituitary-adrenal (HPA) axis
Chronic stress and adrenal dysfunction can significantly impact thyroid function. Elevated cortisol levels, commonly seen in states of chronic stress, inhibit the conversion of T4 to T3, reduce the efficiency of T3 receptor interaction, and increase rT3 production. This creates a state of functional hypothyroidism at the cellular level, even if serum T4 and TSH are within the reference range. Supporting adrenal health through stress reduction techniques, adequate sleep, and nutritional supplementation (eg, adaptogens, B vitamins, vitamin C) is essential for
optimising thyroid function in patients with hypothyroidism or Hashimoto’s. The interplay between the HPA axis and thyroid function underscores the importance of evaluating adrenal health in any patient with thyroid dysfunction. Symptoms such as fatigue (not associated with mineral deficiency), disrupted circadian rhythm, and difficulty coping with stress may suggest underlying adrenal dysregulation, which, if unaddressed, can perpetuate thyroid dysfunction.
3. Dietary and lifestyle interventions
Dietary modifications are a cornerstone of managing autoimmune thyroid disease. A nutrient-dense, antiinflammatory diet rich in antioxidants, omega-3 fatty acids, and micronutrients (such as selenium, zinc, iodine, and vitamin D) can help modulate the immune response and support thyroid function. Selenium, in particular, has been shown to reduce TPOAb levels and improve thyroid function in patients with Hashimoto’s. Similarly, optimising vitamin D levels is crucial for immune regulation, as vitamin D deficiency is common in patients with autoimmune conditions and is associated with increased disease severity. 8,9
In addition to dietary interventions, lifestyle modifications that reduce systemic inflammation and support immune function are equally important. Regular physical activity, sufficient sleep, and stress management techniques (eg, mindfulness, meditation, conflict resolution techniques) have all been shown to positively impact autoimmune disease progression and overall thyroid function.
T3-based therapy and combination treatment:
Clinical considerations
Given the role of T3 in cellular metabolism and its critical importance for symptom resolution, clinicians should consider combination therapy (T4 + T3) in patients who remain symptomatic on levothyroxine
monotherapy. The addition of T3, either in the form of synthetic liothyronine or natural desiccated thyroid (NDT) preparations, can provide patients with the active hormone they need for symptom relief. NDT is a good alternative for patients as it is substantially preferred over levothyroxine alone. 10 Careful monitoring of both serum T3 and reverse T3 levels is essential when adjusting therapy to avoid overmedication of symptoms (similar to hyperthyroid symptoms) and potential adverse cardiovascular effects.
Combination therapy has been shown to improve psychological wellbeing, cognitive function, and overall quality of life in certain patient populations. Clinicians should individualise thyroid treatment based on the patient’s clinical presentation, biochemical markers, and
References
1. Gullo D, Latina A, Frasca F, et al. Levothyroxine monotherapy cannot guarantee euthyroidism in all athyreotic patients. PLoS One. 2011;6(8):e22552.
2. Escobar-Morreale HF, BotellaCarretero JI, Gómez-Bueno M, et al. Thyroid hormone replacement therapy in primary hypothyroidism: A randomised trial comparing L-thyroxine plus liothyronine with L-thyroxine alone. Ann Intern Med. 2005;142(6):412-424.
3. Biondi B, Wartofsky L. Combination treatment with T4 and T3: Toward personalised replacement therapy in hypothyroidism? J Clin Endocrinol Metab 2012;97(7):2256-2271.
4. Wiersinga WM. Paradigm shifts in thyroid hormone replacement therapies for hypothyroidism. Nat Rev Endocrinol. 2014;10(3):164-174.
5. Celi FS, Zemskova M, Linderman JD, et al. Metabolic effects of liothyronine therapy in hypothyroidism: A randomised, double-blind, crossover trial of liothyronine versus levothyroxine. J Clin Endocrinol Metab. 2011;96(11):3466-3474.
6. Virili C, Centanni M. ‘With a little help
response to therapy, with an emphasis on optimising T3 availability at cellular level.
Conclusion
The management of hypothyroidism and Hashimoto’s thyroiditis require a paradigm shift from a purely biochemical approach to one that addresses the full spectrum of thyroid health, including the role of T3, immune system dysfunction, gut health, adrenal function, and lifestyle factors. A comprehensive, functional approach not only targets thyroid hormone optimisation, but also addresses the underlying causes of thyroid dysfunction, particularly autoimmunity and systemic inflammation. By expanding the clinical focus to include these critical elements, clinicians can achieve better outcomes and provide patients with lasting symptom relief. l
from my friends’ – The role of microbiota in thyroid hormone metabolism and enterohepatic recycling. Mol Cell Endocrinol. 2017;458:39-43.
7. Fasano A. Zonulin, regulation of tight junctions and autoimmune diseases. Ann N Y Acad Sci. 2012;1258(1):25-33.
8. Mazokopakis EE, Papadakis JA. The role of selenium and selenoproteins in Hashimoto’s thyroiditis. Hormones (Athens). 2017;16(1), 1-9.
9. Chahardoli R, Saboor-Yaraghi AA, Amouzegar A, et al. Can supplementation with vitamin D modify thyroid autoantibodies (anti-TPO Ab, anti-Tg Ab) and thyroid profile (T3, T4, TSH) in Hashimoto’s thyroiditis? A double-blind, randomised clinical trial. Horm Metab Res 2019;51(5):296-301.
10. Hoang TD, Olsen CH, Mai VQ, et al. Desiccated thyroid extract compared with levothyroxine in the treatment of hypothyroidism: A randomised, doubleblind, crossover study. J Clin Endocrinol Metab. 2013;98(5):1982-1990.
Management of diabetic nephropathy in patients with type 2 diabetes
Authors: Dr Mark Emanuel Debono, MD, (Melit), PGDip Endo (USW), NCHD, Letterkenny University Hospital; and Dr Francesca Briffa, MD, (Melit), BSc (Hons) Pod, NCHD, Letterkenny University Hospital
Diabetes mellitus is the leading cause of chronic kidney disease (CKD) and end stage renal disease (ESRD) globally. Around 20-40 per cent of diabetics develop diabetic kidney disease (DKD). This is a clinical syndrome characterised by progressive decline in estimated glomerular filtration rate (eGFR); elevated arterial blood pressure (BP); and persistent albuminuria (>300mg/d) on at least two visits, three to six months apart. Structural changes include thickening of the glomerular basement membrane (GBM), mesangial expansion, podocyte injury, and glomerulosclerosis. Extraglomerular lesions are also involved in the progression of the disease, including tubular atrophy, interstitial inflammation, and tubulointerstitial fibrosis. Functional changes encompass a paradoxically high eGFR in the early stages of the disease, termed glomerular hyperfiltration, caused by afferent arteriolar vasodilation and/or by efferent arteriolar vasoconstriction owing to activation of the renin-angiotensin-aldosterone system (RAS), leading to glomerular hypertension. Later, proteinuria, systemic hypertension, and loss of renal function develop.
Risk factors for DN
Non-modifiable risk factors for DN include increasing age, family history, and genetic factors, with genes such as
ACE, APOC1, GREM1, UNC13B, ALR2, APOE associated with the disease. DN is also more common in black people, Mexican Americans, Pima Indians, and Hispanics compared to Caucasians, and female gender is associated with a reduced risk of progression from moderate albuminuria to severe albuminuria or ESRD.
Modifiable risk factors include smoking; longer durations of diabetes; obesity; hypertension; poor glycaemic control; and dyslipidaemia (abnormal lipoprotein metabolism is accelerated in DN that causes further renal injury, leading to ESRD).
Clinical features
The most common clinical abnormalities of DKD are persistently elevated urine albumin excretion and/or persistently declining eGFR. These manifestations tend to be asymptomatic, being detected through routine periodic testing. For this reason, type 2 diabetics should undergo testing at the time of diagnosis, and yearly thereafter. On
some occasions, patients can complain of fatigue, foamy urine, and pedal oedema due to hypoalbuminaemia and nephrotic syndrome. They may also have associated peripheral vascular disease, hypertension, cardiovascular disease (CVD), and diabetic retinopathy.
Investigations
1. Routine blood tests: Renal profile, full blood count, electrolytes.
2. Urine albumin excretion: Albuminuria can be established if two to three urine collections obtained over three to six months show elevated levels of albumin.
3. Urine culture to exclude infection and microscopy to examine for red cell casts in glomerulonephritis.
4. Anti-DNA antibodies, antinuclear antibody, extractable nuclear antigen, complement levels, anti-neutrophil cytoplasmic antibodies, antistreptolysin O titre, rheumatoid factor, and antiglomerular membrane antibody to check for autoimmune disease.
5. Serum protein electrophoresis, immunoglobulins, urine protein
Extraglomerular lesions are also involved in the progression of the disease, including tubular atrophy, interstitial inflammation, and tubulointerstitial fibrosis
CLASS DESCRIPTION AND CRITERIA
I GBM thickening on electron microscopy: GBM >395nm (female), GBM >430nm (male)
IIa Mild mesangial expansion
IIb Severe mesangial expansion. A lesion is considered severe if areas of expansion larger than the mean area of a capillary lumen are present in >25 per cent of total mesangium
III At least one Kimmelstiel-Wilson lesion (nodular intercapillary glomerulosclerosis) and there is <50 per cent global glomerulosclerosis
IV Advanced diabetic glomerulosclerosis. There is >50 per cent global glomerulosclerosis, attributable to diabetic nephropathy
TABLE 1: Tervaert classification
electrophoresis for multiple myeloma.
6. Renal ultrasound.
7. Renal biopsy: The gold standard, but rarely used.
Classification
Tervaert classification provides a systematic approach with regards to the classification of the pathology of DN and gives a guide with regards to the prognosis of the disease.
An important limitation of this classification scheme is that not all pathologic lesions are included, such as presence of mesangiolysis, capillary aneurysms, exudative lesions, and focal/segmental sclerosis.
Treatment
There is no definitive cure for DKD, with management focused on lifestyle interventions and optimal glucose and BP control.
Lifestyle interventions
Input from a dietitian is often indicated for this patient cohort. Patients with diabetes and CKD should generally consume a diet rich in vegetables, fruits, fibre, legumes, plant-based proteins, unsaturated fats, and nuts whilst avoiding processed meats, sweetened
beverages, and refined carbohydrates. In advanced CKD, however, potassium in particular, needs to be restricted. Nutrition therapy can reduce levels of Hba1c to similar or even better ones to those achieved with glucose-lowering medications. However, too much protein can lead to reduced carbohydrate intake with consequent weight loss, and such diets can cause harm to kidney function due to increased urinary excretion of amino acids, which can elevate acid load and precipitate metabolic acidosis, especially in patients with poor kidney function.
On the other hand, in very limited studies, protein restriction has been associated with a slower decline in eGFR in non-diabetics with CKD. Most type 2 diabetic CKD patients would have already been counselled on the appropriate carbohydrate and fat intake, and with protein restriction, malnutrition, reduced quality of life, and hypoglycaemia can develop. In view of the lack of clinical trials, guidance for such patients is based on the World Health Organisation recommendations for protein intake of 0.8g/kg/day being associated with good outcomes. Patients on dialysis are recommended to consume 1.0-to-1.2g/kg/day as dialysis causes a
catabolic response, with loss of amino acids. In addition, the presence of uraemia promotes decreased appetite, increased catabolism, and reduced muscle mass.
Low sodium intake is associated with lower BP and improved cardiovascular (CV) outcomes in the general population. Patients with CKD tend to be saltsensitive and unable to regulate BP and extracellular fluid volume status when consuming high salt diets. Low salt intake is associated with improvement in volume status and reduced proteinuria, while high sodium intake is associated with increased mortality and morbidity. The guidelines advise that sodium intake should be restricted to <2g/day or <90mmol of sodium/day (<5g of sodium chloride/day).
Engaging in physical activity offers cardiometabolic, kidney, and cognitive benefits. Weight loss may reduce urinary albumin excretion and improve BP. Physical activity lowers inflammatory markers, improves insulin sensitivity and endothelial function, and is associated with slower decline in eGFR. Therefore, it is recommended that CKD patients with diabetes perform at least 150 minutes of moderately intense physical activity per week. Nonetheless, such patients tend to be elderly with increased risk of falls, obese, and anaemic, with further limitations in their functional capacity, so care needs to be taken.
Use of tobacco is a leading cause of death and also promotes the development of CKD, with a higher incidence of CV events noted among current and former smokers in diabetics with CKD versus never smokers. Second hand exposure is also associated with CKD and kidney disease. Therefore, diabetics with CKD, along with the general population, are advised to stop using tobacco products, with the help of pharmacotherapy and behavioural support. E-cigarettes are not recommended due to emerging links with lung cancer and CVD, and their impact on kidney disease is not fully known.
Pharmacological therapy
Angiotensin-converting enzyme inhibitor (ACEi) or an angiotensin II receptor blocker (ARB): It is recommended that patients with diabetes, hypertension, and albuminuria are started on ACEi or ARB, with dose titration as needed. Albuminuria is associated with increased risk of progression of CKD, and ultimately kidney failure, and with increased risk of CVD. Several trials have shown that through RAS (renin-angiotensinsystem) blockade, ACEi, and ARBs were effective in reducing albuminuria and even reversal of moderately increased albuminuria, slowing the rate of kidney function loss.
Use of ACEi/ARBs in type 2 diabetes (T2D), albuminuria, and without hypertension are beneficial. However, their use is not beneficial for patients with neither albuminuria nor elevated BP. For CKD patients with T2D and hypertension, but normal urine albumin excretion, BP control with any anti-hypertensive class is important to prevent CVD. Serum creatinine, eGFR, and potassium should be measured within two to four weeks of starting treatment or making a change in the dose of ACEi/ARBs. These drugs block the action of angiotensin II, leading to selective vasodilatation of the efferent arterioles, resulting in a decrease in the intraglomerular pressure with consequent rise in creatinine and decrease in eGFR, and block the action of aldosterone, potentially leading to hyperkalaemia.
ACEi should not be combined with ARBs as this can lead to hyperkalaemia and acute kidney injury (AKI).
It is also important to advise contraception for women of childbearing age or to discontinue treatment in women who are pregnant or planning to conceive, as ACEi/ARBs are associated with neonatal complications, especially when continued in the second/third trimester including:
Impaired foetal or neonatal kidney function resulting in oligohydramnios during pregnancy and kidney failure
after delivery;
Pulmonary hypoplasia;
Limb defects;
Cerebral complications;
Miscarriages or perinatal death.
ACEi can also cause dry cough and angioedema due to inhibition of bradykinin. Switching to ARBs is an option in such cases. Treatment should begin with the lowest possible dose and titrate to the maximum tolerated one, as with increasing dose, side-effect risks increase.
Sodium-glucose cotransporter-2 inhibitors (SGLTi): SGLTi are recommended for the treatment of patients with T2D, CKD, and eGFR ≥20ml/min per 1.73m2. These drugs inhibit kidney tubular reabsorption of glucose leading to lower blood glucose. In view of this glycosuria, a diuretic effect is caused, leading to increased urine output. SGLTi also alter metabolism by shifting away from carbohydrate utilisation to ketogenesis, leading to lower HbA1c, BP, and weight. In addition, they lead to a reduction in intraglomerular pressure and subsequent preservation of kidney function.
SGLTi are associated with CV and heart failure (HF) benefits, with reduction in CV death, all-cause mortality, and HF hospitalisation compared to placebo. Kidney benefits include a slower decline in eGFR, reduction in albuminuria, and reduced risk of dialysis, kidney transplant, and death from renal causes.
With regards to initial therapy for patients not yet started on glucoselowering drugs, different guidelines recommend different regimens, with some suggesting starting with metformin and others starting with SGLTi. Based on the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines, it is recommended that most T2D CKD patients with an eGFR ≥30ml/min per 1.73m2:
Start with a combination of metformin and SGLT2i.
Once eGFR declines to 30-45ml/ min/1.73m 2 , maximum dose of metformin should be halved.
Once eGFR <30ml/min/1.73m 2 or the patient is started on dialysis, metformin
is stopped.
Metformin can be administered to kidney transplant patients as long as eGFR is ≥30ml/min per 1.73m 2 .
Once eGFR <20ml/min/1.73m 2 one can continue treatment with SGLTi.
Very little data is available once patients are started on dialysis or have received a kidney transplant, so discontinuation of SGLTi is recommended at this stage.
SGLTi should not be started if eGFR is ≤20ml/min per 1.73m 2
When used as monotherapy, the risk of hypoglycaemia with SGLTi is low as the drug-induced glycosuria decreases as blood glucose normalises. However, when used with other therapies that can cause hypoglycaemia, the dose of these pre-existing medications needs to be adjusted. Withhold SGLTi during times of prolonged fasting or surgery, when patients may be at a greater risk of ketosis. In patients at risk of hypovolaemia, reduce thiazide or loop diuretic before starting treatment with SGLTi, as SGLTi are associated with an initial natriuresis. SGLTi can cause a reversible decrease in eGFR. An eGFR drop of ≤30 per cent should be tolerated and should not lead to discontinuation of treatment. If eGFR drops further, ensure the patient is not hypovolaemic, adjust diuretic dose, and seek other possible causes of the AKI. CKD or HF patients without T2D can be started on SGLTi, as they offer CV and kidney protection without conferring an increased risk of hypoglycaemia or diabetic ketoacidosis. Diabetic ketoacidosis is a rare sideeffect of SGLTi, as is an increased risk of genital mycotic infections.
Nonsteroidal mineralocorticoid receptor antagonist: Nonsteroidal mineralocorticoid receptor antagonist (MRA) are recommended for T2D patients with ≥eGFR 25ml/min/1.73m 2 , normal serum potassium concentration, and albuminuria ≥30mg/g despite on maximum tolerated dose of ACEi/ARBs. Through the use of ACEi/ARBs, there is kidney and CV benefit via RAS blockade.
Nonetheless, data has shown that there is incomplete suppression of serum aldosterone levels, thereby suggesting the need for further treatment to reduce residual albuminuria. Steroidal MRA are used to treat primary hyperaldosteronism levels, HF, and to reduce albuminuria, but data is lacking with regards to their effect on kidney disease progression. Moreover, they can cause hyperkalaemia and AKI, and spironolactone is associated with gynaecomastia.
Novel nonsteroidal MRA such as finerenone are more selective for mineralocorticoid receptors, and confer CV and renal benefits with reduced albuminuria and slower decline in eGFR. They are also associated with a lower risk of hyperkalaemia compared to steroidal MRA.
Patients with T2D, CKD, and albuminuria on SGLTi and ACEi/ ARBs can also start taking finerenone, provided that they have a normal serum potassium and albumin to creatinine ratio is ≥30mg/g. Use of SGLTi also reduces the risk of hyperkalaemia in patients already on ACEi/ARBs and finerenone. Moreover, finerenone can be added to patients on ACEi/ARBs only, despite not being on SGLTi.
A steroidal MRA is used in the treatment of HF, hyperaldosteronism, and refractory hypertension. Clinical evidence is lacking whether switching from a steroidal to nonsteroidal is associated with an improvement in clinical outcome. When the patient is treated with neither and has T2D, HF, and albuminuria and is already on ACEi/ ARBs and SGLTi, treatment should be based on the most concerning clinical indication. At present, a nonsteroidal MRA cannot replace a steroidal MRA for HF and hyperaldosteronism.
Finerenone can cause hyperkalaemia, and monitoring of this electrolyte is important. Treatment with finerenone should not be started if serum potassium is >5mmol/l. Finerenone has a short half-life, therefore stopping the drug for
72 hours will lead to resolution of the elevated potassium.
Steroidal and nonsteroidal MRA should not be combined due to risk of hyperkalaemia. Steroidal MRA are currently contraindicated in pregnancy, and in view of the lack of clinical data of the use of nonsteroidal MRA in pregnancy, this drug should be stopped.
Other anti-hypertensive treatment: KDIGO guidelines recommend that patients with albuminuria, T2D, CKD, and hypertension are started on ACEi/ ARBs until maximum tolerated dose. If patients have normal serum potassium and albumin to creatinine ratio is ≥30mg/g, finerenone can be added. If this is not the case and BP is still high, dihydropyridine calcium channel blocker and/or diuretic can be added. Should BP still remain high and eGFR ≥45, steroidal MRA can be added.
Glucagon-like peptide-1 receptor agonists: In T2D CKD patients who have not achieved the desirable glycaemic targets despite lifestyle interventions, treatment with metformin and SGLT2i, or in whom the latter two medications are not tolerated, guidelines recommend prioritising glucagon-like peptide-1 receptor agonists (GLP-1 RA) over other glucose lowering therapies.
GLP-1 RA have been shown to improve glycaemic control, confer weight loss and CV benefit, reduce albuminuria, and slow the rate of eGFR decline. In view of their proven CV benefit, GLP-RA are preferred over other glucose-lowering therapies (Dipeptidyl peptidase-4 inhibitor (DPP-4) inhibitors, thiazolidinediones, sulfonylureas, insulin). The risk of hypoglycaemia is generally low when GLP-1 RA are used alone. When used with other medications, the risk is increased, so the dose of sulfonylurea and/or insulin may need to be reduced. GLP-1 RA may be preferentially used in patients with obesity, T2D, and CKD to promote intentional weight loss. Further studies are required regarding the use of GLP-1RA in patients with very advanced CKD, patients on dialysis, and
in kidney transplant recipients. Sideeffects of GLP-1 RA include nausea/ vomiting, diarrhoea, and increased heart rate. Also, since most of them are given as a subcutaneous injection, they are associated with pain over the injection site. These medications are contraindicated in patients with a history of medullary thyroid carcinoma, multiple endocrine neoplasia 2, and patients with a history of acute pancreatitis.
Other glycaemic treatment: If the glycaemic target is still not achieved despite lifestyle interventions, metformin, SGLTi, and GLP-1 RA, then other glucoselowering agents can started, such as DPP-4 inhibitors, thiazolidinediones, sulfonylureas, and insulin.
Monitoring of blood glucose in T2D CKD patients
HbA1c is recommended to monitor glycaemic control in these patients, measured twice a year, or up to four times/year should glycaemic targets not be met. However, inflammation, oxidative stress, and metabolic acidosis associated with CKD, as well as anaemia, transfusions, and use of iron replacement therapies and erythropoiesis-stimulating agents, affect HbA1c level. These effects become more pronounced as the CKD advances or patients are treated with dialysis. Once HbA1c levels are not concordant with blood glucose levels, continuous glucose monitoring and self-monitoring of blood glucose can be used, as these are not influenced by CKD, dialysis, or other treatments. One should aim for target HbA1c of <6.5-to-8.0 per cent, with levels ≤6.0 per cent associated with greater risk of hypoglycaemia and increased mortality.
Dyslipidemia treatment
Managing dyslipidaemia, according to KDIGO recommendations, includes: CKD patients are at increased risk of adverse events when statins and fibrates are combined. Since statins confer a greater clinical benefit compared to fibrates, statins are preferred.
Statin or statin/ezetimibe combination in adults aged ≥50 with eGFR ≤60ml/ min/1.72m2, not on dialysis and without kidney transplant. Ezetimibe monotherapy is not recommended.
Statin in adults aged ≥50 with eGFR ≥60ml/min/1.72m2.
Statin in adults aged 18 to 49 with CKD, but not on dialysis and without kidney transplant if they have coronary disease (myocardial infarction or coronary revascularisation); diabetes mellitus; prior ischaemic stroke; estimated 10-year incidence of coronary death or non-fatal myocardial infarction >10 per cent.
If at the time of dialysis initiation, patients are already on statin or statin/ezetimibe combination, this can be continued.
Do not start statin or statin/ezetimibe combination in dialysis patients.
In adult kidney transplant recipients, treatment with a statin is recommended.
Statins are contraindicated in pregnant or breastfeeding females, patients with active liver disease or in patients in whom transaminase levels are three times or more the upper limit of normal.
For additional risk-based therapy, aspirin can be used lifelong for secondary prevention among those with established CVD. Ezetimibe or proprotein convertase subtilisin-kexin type 9 inhibitors (PCSK9i) can be added to a statin. PCSK9i can be used in statin-intolerant patients, with these medications showing an improvement in lipid profile and CV risk. Nonetheless, further studies are needed to ascertain their safety in patients with eGFR ≤20ml/min/1.73m2, those on dialysis, and/or renal transplant patients.
Conclusion
DKD is a constantly evolving subject with new guidelines issued very frequently. Nonetheless, a patient-centred approach with involvement of relatives and multidisciplinary team is required to achieve the best care possible, including involvement of nutritionist, physiotherapist, personal trainer, smoking cessation support, endocrinologist, cardiologist, GP, and various other medical disciplines.
KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease provides evidence-based recommendations and can be accessed at: www.kdigo.org/wp-content/uploads/2022/10/ KDIGO-2022-Clinical-Practice-Guidelinefor-Diabetes-Management-in-CKD.pdf. ●
References available on request
FIGURE 1: KDIGO management of patients with DKD
Diabetic retinopathy
Authors: Dr Mark Emanuel Debono, MD, (Melit), PGDip Endo (USW); and Dr Francesca Briffa, MD, (Melit), BSc (Hons) Pod, Letterkenny University Hospital
Diabetic retinopathy (DR) is the commonest microvascular complication of diabetes mellitus (DM). The retina is vulnerable to microvascular damage in DM as a result of its high oxygen and metabolic demands, as well as its dependence on an intact bloodretinal barrier (BRB). All people with DM will be at risk of developing DR. DM causes multiple physiological and metabolic changes in the retina, and it has been suggested that retinopathy starts to develop approximately seven years before the clinical diagnosis of type 2 DM is made. DR is considered to be a leading cause of vision loss in working-age populations globally, notably in middle- and high-income countries, and it imposes a substantial economic burden on healthcare systems. Vision impairment resulting from this condition also creates a significant burden on patients’ quality of life.
Epidemiology
The global prevalence of DM is predicted to increase substantially in the coming decades, with an estimated 592 million individuals affected by 2035 compared to 382 million in 2013. As the global prevalence of DM increases, so will the number of individuals with DR. The World Health Organisation has estimated that DR is responsible for approximately 15-17 per cent of total blindness in Europe and the US alone. From a worldwide perspective, DR is an even larger issue, with an estimated prevalence of 35 per cent. The global estimate for sight-threatening stages, typically proliferative DR (PDR) and
diabetic macular oedema (DMO), is around 7 per cent.
Risk factors
Poor glycaemic control, duration, and severity of DM and hypertension: These are the most relevant causative risk factors related to DR, however, control of blood glucose has been noted to have a greater impact than blood pressure control when it comes to the risk of development of DR.
Age: In younger onset DM, DR is unusual before 13 years of age, while in those with older onset DM, there is an increased frequency of DR in patients less than 50 years of age.
Gender: Women not only have twice the overall risk of blindness, but are also
more likely than men to have DM. Ethnicity: Moderate and more severe retinopathy is commoner in Polynesians than Europeans. Studies have also demonstrated other ethnic differences, with higher levels of DR in Hispanics (36 per cent), followed by African Americans (29 per cent), and non-Hispanic white individuals (22 per cent).
Smoking: Is a potential risk factor for the development of DR in type 1 DM. However, when it comes to type 2 DM, evidence is controversial and smoking in these individuals has been suggested to serve as protection against the progression of retinopathy in a certain number of patients, despite the fact that smoking is in itself an independent risk factor for cardiovascular disease and
death in patients with diabetes.
Genetics and family history: Various twin studies have also classified DR as a genetically inherited polygenic disorder with a recognisable familial clustering, also leading to a family history of DR being a risk factor.
Others: Include anaemia, dyslipidaemia, a high body mass index, puberty, pregnancy, nephropathy, cataract surgery, DR in the other eye, and vitamin D deficiency.
Classification/staging
The clinically visible lesions seen in DR are predominantly vascular in nature and, in view of this, DR has been regarded as a vascular disorder for a number of years. According to the International Clinical Disease Severity Scale, a modified classification originating from the Airlie House classification, DR is classified according to the presence of microvascular lesions in the retina. There is the non-proliferative stage, which is characterised by retinal haemorrhages, microaneurysms, vascular tortuosity, and lipid exudates, that can be further classified into mild, moderate, and severe; and the proliferative stage, during which there is the formation of new pre-retinal abnormal vessels.
An additional category of DR is DMO, which is characterised by fluid accumulation in the neural retina leading to aberrant retinal thickening and subsequent cystoid macular oedema. DMO can be subdivided into mild, moderate, and severe, and can occur across all severities of DR, both in non-proliferative diabetic retinopathy (NPDR) and PDR. It has been named as the commonest culprit of vision loss in patients with DR.
Presentation
DR is considered to be unusual among retinal diseases due to the fact that symptomatology may vary drastically and may be out of proportion to the severity of pathology within the
retina. Patients with NPDR are usually asymptomatic. However, if PDR develops, the patient could present with a sudden vision loss owing to vitreous haemorrhage. In cases of development of DMO, the patient might notice a more gradual loss of vision.
Pathophysiology
In DR, hyperglycaemia plays a crucial role in its pathogenesis. The elevated blood glucose levels lead to activation of a variety of pathways including:
Polyol mechanism: In high glucose levels, through the enzymatic activity of aldose reductase, sorbitol is produced from glucose with the cofactor
enzyme complex NADPH oxidase and nuclear factor-B (NF- κ B) are activated, leading to inflammation and cellular damage. Tumor necrosis factor- α (TNF- α), interleukin (IL)1 β , lipoprotein-PLA2, and other biomolecules are all involved in the inflammation caused in the vessels.
PKC activation: Elevated blood glucose levels lead to activation and stimulation of protein kinase C (PKC)- δ signalling, resulting in expression of PKC and p38 mitogen-activated protein kinase, as well as dephosphorylation of PDGF receptors. This in turn leads to a decrease in the signalling of PDGF receptors, and subsequent death of the cells of the pericytes.
In diabetic retinopathy hyperglycaemia plays a crucial role in its pathogenesis
nicotinamide adenine dinucleotide phosphate (NADPH). In turn, sorbitol is converted to fructose by sorbitol dehydrogenase. Sorbitol, in view of its hydrophilic properties, causes damage to the retinal cells via intracellular osmotic imbalance. In addition, fructose is metabolised to 3-deoxyglucosone and fructose-3-phosphate which lead to oxidative stress in the retinal cells, including pericytes via the promotion of advanced glycation end products (AGE).
Accumulation of AGE: AGE leads to an increase in reactive oxygen species (ROS), leading to damage of the retinal cells and also to reduced mRNA levels of pigment epithelium-derived factor (PEDF). PEDF has a protective role, therefore, reduced levels of PEDF lead to increased inflammation and damage to the microvascular endothelial cells of the retina. Simultaneously, the
Oxidative stress: Elevated glucose levels lead to increased intracellular NADL levels and elevated lactate levels in the tissue. This leads to an influx of excessive electrons into the mitochondria, inducing the formation of ROS causing retinal oxidative stress. This process alters DNA metabolism that in turn augments the nuclear enzyme PARP (poly-adenosine diphosphateribose polymerase) and enhances the activation of NF- κ B. This process leads to further formation of TNF- α and NFκ B-dependent genes that lead to further oxidative stress.
Pericytes enwrap the microvasculature and support endothelial cells. All of the above-mentioned mechanisms lead to oxidative stress, which in turn bring about loss of pericytes in the early stages of DR. Loss of pericytes and, subsequently, endothelial cells, leads to capillary occlusion which in turn results in retinal ischaemic conditions along with cotton wool patches, microaneurysms, and dot-and-blot haemorrhages. This is accompanied by basement membrane (BM) thickening in the early stages of DR. In view of the oxidative stress caused by these processes, the BRB breaks down. Dysfunction of the BRB leads to thickening of the retina and increased leukocytosis, which is an intravascular immune response.
Retinal ischaemia leads to an increase in VEGF levels, with the latter playing a critical role in restoring blood supply to the ischaemic retina. This process is referred to as neovascularisation, and it damages the retina more severely, possibly even causing retinal detachment. This process of neovascularisation leads to the formation of delicate and permeable blood vessels that result in vitreous haemorrhages. Such haemorrhages lead to the formation of fibrovascular scars and gliosis. Studies have shown that upregulation of VEGF is mediated by hypoxia-inducible factors (HIFs).
Genes regulated by HIFs, including stromal-derived growth factor-1 (SDF-1) and platelet-derived growth factor-B (PDGF-B), play important roles in this retinal neovascularisation. It is, therefore, no surprise that regulation of VEGF and HIFs is being targeted for the treatment of DR.
Apart from neovascularisation, neurodegeneration also plays an important role towards the end stage of DR. Neurodegeneration occurs in view of the reduced signalling and activation of neurotrophic factors, including NGF (nerve growth factor), PEDF, IRBP (interphotoreceptor retinoid-binding protein), and somatostatin.
The previously mentioned mechanisms also lead to retinal inflammation and retinal degeneration, which are features that can be detected from the early stages to the more chronic stages of DR. Glutamate excitotoxicity and loss of neuroprotective molecules further contribute to retinal neuronal cell death. Lipid dysregulation also plays a role in the development of DR, with studies showing a strong association between changes in the plasma levels of high-density and lowdensity lipoproteins (HDL and LDL) and development and severity of DR as well as diabetes. New research has in fact demonstrated that lipid-modifying drugs could have protective effects in DR.
More recent studies have been carried
out examining the vitreous humor of PDR patients. Barba et al (2010) showed that lactate levels increased whilst ascorbic acid levels decreased in PDR patients compared to control patients. Paris et al (2015) showed that there is upregulation of arginine and proline levels in PDR patients, while Haines et al (2018) demonstrated that pyruvate levels increased and purinerelated pathways were activated in PDR patients.
Diagnosis
The primary method for evaluation of DR involves direct and indirect ophthalmoscopy. However, a vast range of imaging modalities are available to aid the clinician when it comes to examining the retina. These imaging methods include the following, amongst others:
thickness, photoreceptor outer segment, hard exudates, intraretinal cystoid spaces, bridging retinal processes, and hyperreflective retinal and choroidal foci, amongst others.
Ultra-wide field retinal imaging: Clinical findings include microaneurysms, intraretinal haemorrhages, cotton-wool spot, venous beading, preretinal and vitreous haemorrhages, neovascularisation of optic disc or elsewhere, and intraretinal microvascular abnormalities.
Biomarkers of disease
Biomarkers related to glycation and oxidative stress:
Serum N-epsiloncarboxymethyllysine (CML) and pentosidine (AGEs) are increased in DR, as are asymmetric dimethylarginine (ADMA), symmetric dimethylarginine
The primary method for evaluation of diabetic retinopathy involves direct and indirect ophthalmoscopy
Fundus photography: Enables detection of microaneurysms, intraretinal haemorrhage, cotton-wool spot, venous beading, intraretinal microvascular abnormalities, and neovascularisation of optic disc or elsewhere. Throughout the years, it has been the gold standard for evaluating DR.
Fluorescein angiography: Able to detect microaneurysms, retinal capillary non-perfusion, vascular telangiectasia, capillary drop-outs, enlargement or irregularity of the foveal avascular zone, and the presence of neovascularisation.
Optical coherence tomography: Clinical findings include retinal thickness, subfoveal choroidal
(SDMA), and I-arginine.
Elevated Apo-A1 levels (a component of HDL protein) and low Apo-B levels (component of LDL) are protective factors of DR.
A serum level of Apo-A1 ≥7.4umol/L is associated with reduced risk of DR.
Biomarkers related to inflammation and endothelial dysfunction.
Higher levels of CRP, IL-1 β , IL-8, and TNF- α are associated with DR.
Levels of intercellular adhesion molecule-1 (ICAM 1) and vascular adhesion molecule-1 (VCAM 1) rise as DR progresses.
Hyperhomocysteinaemia is associated with greater risk of developing DR.
High levels of adiponectin (antiinflammatory role) is associated with
improved retinal microcirculation.
Biomarkers of BM thickening
Elevated urinary and serum levels of collagen type IV is associated with DR, as are metalloproteinases (MMP)
– MMP-9 in type 1 DM, and MMP-2 and MMP-9 in type 2 DM.
Biomarkers of angiogenesis and thrombosis
VEGF levels with over 90 per cent specificity and sensitivity in predicting the presence of DR.
Serum erythropoietin is associated with DR, with highest levels found in PDR and lowest levels in patients without DR.
Fibroblast growth factor-21 (FGF21) concentration is increased in DR, as is serum HIF-1 α
Elevated levels of TGF-β is strongly associated with the incidence of DR.
Reduced PEDF levels have been found in diabetics with retinopathy.
Research has shown that diabetics with levels of vitamin D below 30nmol/L had a 60 per cent greater chance of developing PDR compared to those with vitamin D levels above 75nmol/L.
Novel biomarkers
mRNA encoding retina-specific pigment-protein rhodopsin (RHO) rises with progression of DR.
Reduced circulating mRNA for retinal amine oxidase (RAO) and an elevation in RHO/RAO mRNA ratio as DR progresses.
Increased levels of circulating retinal pigment epithelium-65 (RPE65) mRNA and reduced retinoschisin mRNA as DR worsens.
Management
The principles of management of DR can be generally divided into prevention, early detection, and ophthalmological treatments. Luckily, much of the visual loss from DR can be prevented, and the rates of loss of vision from diabetes and DR have substantially decreased over the past
few years. The risk of developing DR can be diminished by early detection of disease by means of screening, as well as tight control of blood glucose, blood pressure, and lipids.
Due to the impact of DR on individuals with DM, screening for DR is of utmost importance to detect preventable blindness as early as possible. Studies have shown that the clinical outcome of patients with DR is better if these individuals are screened and treated as early as possible. Many different methods are available for screening DR, such as direct ophthalmoscopy, dilated stereoscopic fundoscopy, fundus analogue photography, the use of digital photography with wide-angle imaging, amongst others. It has been recommended that adults with type 1 DM should undergo an initial dilated and comprehensive examination of the eye by an ophthalmologist within the first five years of the onset of DM, while adults with type 2 DM should undergo this examination at the time of diagnosis of DM. If DR is not evident for one or more annual eye examinations, then examination every two years may be considered. However, if there is evidence of DR, consecutive dilated retinal examinations should be repeated at least annually for both type 1 and 2 DM patients.
Patients with any level of macular oedema, severe NPDR, or any PDR should be urgently referred to an ophthalmologist. Laser photocoagulation therapy is one of the treatments used in DR and it has been proven to diminish the risk of loss of vision in patients with highrisk PDR and in some instances, severe NPDR. Intravitreous injections of anti-VEGF (eg, ranibizumab) are indicated in cases in which there is central diabetic macular oedema as this occurs below the foveal centre and may threaten reading vision. Intravitreal corticosteroids are also
successful in patients with persistent DMO and loss of vision after the failure of conventional treatment, that is, laser photocoagulation therapy and risk factor modification. Vitrectomy has a prominent role in the management of retinal traction detachment associated with severe fibrovascular proliferations in cases of PDR.
DR as a predictor of other diabetic complications
The presence of DR indicates that there has already been damage to the microcirculation by the diabetic background and, hence, it can be considered to be a reliable biomarker of the destructive effects of DM in a certain individual. DR has been associated with two kinds of neuropathies – cardiac autonomic neuropathy and diabetic peripheral neuropathy. With DR, there is also an increase in the possibility of developing nephropathy and it is considered to be an independent and significant predictor of progression to macroand micro-albuminuria, along with a decline in the glomerular filtration rate in these individuals. There has also been a link between DR and the development of cognitive impairment and dementia. Apart from the aforementioned microvascular complications, individuals with DR are also prone to developing macrovascular complications including cardiovascular, cerebrovascular, and peripheral complications.
Conclusion
DR is a burdensome and challenging disorder that requires prompt diagnosis and management. Early screening and detection are paramount in reducing vision loss for this patient group, while prevention offers the best outcomes. In Ireland, the Diabetic RetinaScreen Programme offers annual screening to patients over 12 years with DM free of charge. ●
References on request
Clinical Podcast
EPISODE TWO TOPIC:
Vaccination in children
Presented by Dawn O’Shea with Dr. Cilian ÓMaoldomhnaigh
SCAN HERE TO LISTEN
SPONSORED BY
The journey to triple protection
The journey to triple protection in type 2 diabetes mellitus1†
INVOKANA® is indicated for the treatment of adults with insufficiently controlled type 2 diabetes mellitus as an adjunct to diet and exercise:
INVOKANA® is indicated for the treatment of adults with insufficiently controlled type 2 diabetes mellitus as an adjunct to diet and exercise:
> as monotherapy when metformin is considered inappropriate due to intolerance or contraindications
INVOKANA® is indicated for the treatment of adults with insufficiently controlled type 2 diabetes mellitus as an adjunct to diet and exercise: > as monotherapy when metformin is considered inappropriate due to intolerance or contraindications > in addition to other medicinal products for the treatment of diabetes
Dose adjustment recommendations according to eGFR¹
> as monotherapy when metformin is considered inappropriate due to intolerance or contraindications > in addition to other medicinal products for the treatment of diabetes
For study results with respect to combination of therapies, effects on glycaemic control, cardiovascular and renal events, and the populations studied, see sections 4.4, 4.5 and 5.1 of the Summary of Product Characteristics (SmPC).1
For study results with respect to combination of therapies, effects on glycaemic control, cardiovascular and renal events, and the populations studied, see sections 4.4, 4.5 and 5.1 of the Summary of Product Characteristics (SmPC).1
> in addition to other medicinal products for the treatment of diabetes
For study results with respect to combination of therapies, effects on glycaemic control, cardiovascular and renal events, and the populations studied, see sections 4.4, 4.5 and 5.1 of the Summary of Product Characteristics (SmPC).1
† Improvement in glycaemic control and reduction of cardiovascular and renal morbidity and mortality are integral parts of the treatment of type 2 diabetes.1 1. INVOKANA® Summary of Product Characteristics June 2023.
† Improvement in glycaemic control and reduction of cardiovascular and renal morbidity and mortality are integral parts of the treatment of type 2 diabetes.1
1. INVOKANA® Summary of Product Characteristics June 2023.
* If further glycaemic control is needed, the addition of other anti-hyperglycaemic agents should be considered. § Continue dosing until dialysis or renal transplantation.
* If further glycaemic control is needed, the addition of other anti-hyperglycaemic agents should be considered. § Continue dosing until dialysis or renal transplantation.
Abbreviated Prescribing Information: Please consult the Summary of Product Characteristics (SmPC) for full prescribing information. Presentation: Canagliflozin 100mg and canagliflozin 300mg, film-coated tablets.
† Improvement in glycaemic control and reduction of cardiovascular and renal morbidity and mortality are integral parts of the treatment of type 2 diabetes.1 1. INVOKANA® Summary of Product Characteristics June 2023.
Use: Adults with insufficiently controlled type 2 diabetes mellitus as an adjunct to diet and exercise: (1) as monotherapy when metformin is considered inappropriate due to intolerance or contraindications, or (2) in addition to other medicinal products for the treatment of diabetes. Dosage and administration: Oral administration. Recommended starting dose is 100mg once daily, preferably taken before the first meal of the day. Tablets should be swallowed whole. In patients needing tighter glycaemic control and tolerating canagliflozin 100mg once daily, dose can be increased to 300mg once daily if eGFR ≥ 60 mL/min/1.73 m2 [Refer to SmPC for dose adjustment according to eGFR]. Care when increasing dose in patients ≥ 75 years of age, patients with known cardiovascular disease (CVD), other patients for whom the initial canagliflozin-induced diuresis poses risk. Correcting volume depletion prior to initiation of canagliflozin is recommended. Consideration of a lower dose(s) of insulin/insulin secretagogue if using canagliflozin as an add-on therapy is recommended. Elderly (≥ 65 years old): Renal function and risk of volume depletion should be taken into account. Paediatric population: The safety and efficacy of canagliflozin in children under 18 years of age have not yet been established. Contraindications: Hypersensitivity to the active substance or any of the excipients. Warnings and Precautions: [Refer to SmPC for more detail] Renal impairment: Limit dose to 100mg once daily in patients with eGFR < 60 mL/min/1.73 m2 Regardless of pre-treatment eGFR, patients on canagliflozin may experience an initial fall in eGFR that attenuates over time. Monitor renal function prior to and after initiating canagliflozin. Also monitor after initiating concomitant products that may reduce renal function. Patients at risk of volume depletion: Canagliflozin induces osmotic diuresis which may reduce intravascular volume and decrease blood pressure (BP). Caution should be exercised in patients for whom a canagliflozininduced drop in BP could pose a risk. Advise patients to report symptoms of volume depletion. Canagliflozin is not recommended for use in patients receiving loop diuretics or who are volume depleted. Diabetic ketoacidosis (DKA): Rare cases of DKA, including life-threatening and fatal cases, have been reported in patients treated with SGLT2 inhibitors. Presentation of DKA may be atypical. Risk of DKA appears to be higher in patients with moderately to severely decreased renal function who require insulin. Assess patients immediately if symptoms occur, regardless of blood glucose level. Where DKA is suspected/diagnosed, discontinue canagliflozin immediately. Treatment should be interrupted in patients hospitalised for major surgical procedures or acute serious medical illnesses. Monitor ketones (preferably blood ketones) in these patients. Before initiating canagliflozin, consider factors in patient history that may predispose to DKA. DKA may be prolonged after discontinuation. Canagliflozin should not be used for treatment of patients with type 1 diabetes. Lower limb amputations: Before initiating canagliflozin, consider factors in patient history that may increase risk for amputation. Consider careful monitoring of patients with a higher risk for amputation, and counsel patients. Consider stopping canagliflozin in patients who develop events which may precede amputation. Necrotising fasciitis of the perineum: (Fournier’s gangrene): This rare but serious and potentially life-threatening event requires urgent surgical intervention and antibiotic treatment. Advise patients to seek medical attention if they experience a combination of pain, tenderness, erythema, or swelling in the genital or perineal area, with fever or malaise. Urogenital infection or perineal abscess may precede necrotising fasciitis. If Fournier’s gangrene is suspected, discontinue canagliflozin and institute prompt treatment. Elevated haematocrit: Monitor haematocrit levels in patients with an already elevated haematocrit. Elderly (≥ 65 years old): Elderly patients may be at a greater risk for volume depletion, are more likely to be
Date of preparation: July 2023 IR-INV-41-2023
Abbreviated Prescribing Information: Please consult the Summary of Product Characteristics (SmPC) for full prescribing information. Presentation: Canagliflozin 100mg and canagliflozin 300mg, film-coated tablets. Use: Adults with insufficiently controlled type 2 diabetes mellitus as an adjunct to diet and exercise: (1) as monotherapy when metformin is considered inappropriate due to intolerance or contraindications, or (2) in addition to other medicinal products for the treatment of diabetes. Dosage and administration: Oral administration. Recommended starting dose is 100mg once daily, preferably taken before the first meal of the day. Tablets should be swallowed whole. In patients needing tighter glycaemic control and tolerating canagliflozin 100mg once daily, dose can be increased to 300mg once daily if eGFR ≥ 60 mL/min/1.73 m2 [Refer to SmPC for dose adjustment according to eGFR]. Care when increasing dose in patients ≥ 75 years of age, patients with known cardiovascular disease (CVD), other patients for whom the initial canagliflozin-induced diuresis poses risk. Correcting volume depletion prior to initiation of canagliflozin is recommended. Consideration of a lower dose(s) of insulin/insulin secretagogue if using canagliflozin as an add-on therapy is recommended. Elderly (≥ 65 years old): Renal function and risk of volume depletion should be taken into account. Paediatric population: The safety and efficacy of canagliflozin in children under 18 years of age have not yet been established. Contraindications: Hypersensitivity to the active substance or any of the excipients. Warnings and Precautions: [Refer to SmPC for more detail] Renal impairment: Limit dose to 100mg once daily in patients with eGFR < 60 mL/min/1.73 m2. Regardless of pre-treatment eGFR, patients on canagliflozin may experience an initial fall in eGFR that attenuates over time. Monitor renal function prior to and after initiating canagliflozin. Also monitor after initiating concomitant products that may reduce renal function. Patients at risk of volume depletion: Canagliflozin induces osmotic diuresis which may reduce intravascular volume and decrease blood pressure (BP). Caution should be exercised in patients for whom a canagliflozininduced drop in BP could pose a risk. Advise patients to report symptoms of volume depletion. Canagliflozin is not recommended for use in patients receiving loop diuretics or who are volume depleted. Diabetic ketoacidosis (DKA): Rare cases of DKA, including life-threatening and fatal cases, have been reported in patients treated with SGLT2 inhibitors. Presentation of DKA may be atypical. Risk of DKA appears to be higher in patients with moderately to severely decreased renal function who require insulin. Assess patients immediately if symptoms occur, regardless of blood glucose level. Where DKA is suspected/diagnosed, discontinue canagliflozin immediately. Treatment should be interrupted in patients hospitalised for major surgical procedures or acute serious medical illnesses. Monitor ketones (preferably blood ketones) in these patients. Before initiating canagliflozin, consider factors in patient history that may predispose to DKA. DKA may be prolonged after discontinuation. Canagliflozin should not be used for treatment of patients with type 1 diabetes. Lower limb amputations: Before initiating canagliflozin, consider factors in patient history that may increase risk for amputation. Consider careful monitoring of patients with a higher risk for amputation, and counsel patients. Consider stopping canagliflozin in patients who develop events which may precede amputation. Necrotising fasciitis of the perineum: (Fournier’s gangrene): This rare but serious and potentially life-threatening event requires urgent surgical intervention and antibiotic treatment. Advise patients to seek medical attention if they experience a combination of pain, tenderness, erythema, or swelling in the genital or perineal area, with fever or malaise. Urogenital infection or perineal abscess may precede necrotising fasciitis. If Fournier’s gangrene is suspected, discontinue canagliflozin and institute prompt treatment. Elevated haematocrit: Monitor haematocrit levels in patients with an already elevated haematocrit. Elderly (≥ 65 years old): Elderly patients may be at a greater risk for volume depletion, are more likely to be
Abbreviated Prescribing Information: Please consult the Summary of Product Characteristics (SmPC) for full prescribing information. Presentation: Canagliflozin 100mg and canagliflozin 300mg, film-coated tablets. Use: Adults with insufficiently controlled type 2 diabetes mellitus as an adjunct to diet and exercise: (1) as monotherapy when metformin is considered inappropriate due to intolerance or contraindications, or (2) in addition to other medicinal products for the treatment of diabetes. Dosage and administration: Oral administration. Recommended starting dose is 100mg once daily, preferably taken before the first meal of the day. Tablets should be swallowed whole. In patients needing tighter glycaemic control and tolerating canagliflozin 100mg once daily, dose can be increased to 300mg once daily if eGFR ≥ 60 mL/min/1.73 m2. [Refer to SmPC for dose adjustment according to eGFR]. Care when increasing dose in patients ≥ 75 years of age, patients with known cardiovascular disease (CVD), other patients for whom the initial canagliflozin-induced diuresis poses risk. Correcting volume depletion prior to initiation of canagliflozin is recommended. Consideration of a lower dose(s) of insulin/insulin secretagogue if using canagliflozin as an add-on therapy is recommended. Elderly (≥ 65 years old): Renal function and risk of volume depletion should be taken into account. Paediatric population: The safety and efficacy of canagliflozin in children under 18 years of age have not yet been established. Contraindications: Hypersensitivity to the active substance or any of the excipients. Warnings and Precautions: [Refer to SmPC for more detail] Renal impairment: Limit dose to 100mg once daily in patients with eGFR < 60 mL/min/1.73 m2. Regardless of pre-treatment eGFR, patients on canagliflozin may experience an initial fall in eGFR that attenuates over time. Monitor renal function prior to and after initiating canagliflozin. Also monitor after initiating concomitant products that may reduce renal function. Patients at risk of volume depletion: Canagliflozin induces osmotic diuresis which may reduce intravascular volume and decrease blood pressure (BP). Caution should be exercised in patients for whom a canagliflozininduced drop in BP could pose a risk. Advise patients to report symptoms of volume depletion. Canagliflozin is not recommended for use in patients receiving loop diuretics or who are volume depleted. Diabetic ketoacidosis (DKA): Rare cases of DKA, including life-threatening and fatal cases, have been reported in patients treated with SGLT2 inhibitors. Presentation of DKA may be atypical. Risk of DKA appears to be higher in patients with moderately to severely decreased renal function who require insulin. Assess patients immediately if symptoms occur, regardless of blood glucose level. Where DKA is suspected/diagnosed, discontinue canagliflozin immediately. Treatment should be interrupted in patients hospitalised for major surgical procedures or acute serious medical illnesses. Monitor ketones (preferably blood ketones) in these patients. Before initiating canagliflozin, consider factors in patient history that may predispose to DKA. DKA may be prolonged after discontinuation. Canagliflozin should not be used for treatment of patients with type 1 diabetes. Lower limb amputations: Before initiating canagliflozin, consider factors in patient history that may increase risk for amputation. Consider careful monitoring of patients with a higher risk for amputation, and counsel patients. Consider stopping canagliflozin in patients who develop events which may precede amputation. Necrotising fasciitis of the perineum: (Fournier’s gangrene): This rare but serious and potentially
treated with diuretics, and to have impaired renal function. Genital mycotic infections: Vulvovaginal candidiasis, and balanitis/balanoposthitis were reported in clinical studies. Urinary tract infections (UTIs): Complicated UTIs including pyelonephritis and urosepsis have been reported. Temporary interruption of canagliflozin should be considered. Cardiac failure: Experience in New York Heart Association (NYHA) class III is limited, with no experience in clinical studies with canagliflozin in NYHA class IV. Urine laboratory assessments: Patients taking canagliflozin will test positive for glucose in their urine. Lactose intolerance: Patients with galactose intolerance, total lactase deficiency, or glucose-galactose malabsorption should not take this product. Interactions: Diuretics: may increase risk of dehydration and hypotension. Insulin and insulin secretagogues: risk of hypoglycaemia; consider lower dose of insulin or insulin secretagogue. Effects of other medicines on Invokana: Enzyme inducers (e.g. St. John’s wort, rifampicin, barbiturates, phenytoin, carbamazepine, ritonavir, efavirenz) may decrease exposure of canagliflozin; monitor glycaemic control. Consider dose increase to 300 mg if administered with UGT enzyme inducer. Cholestyramine may reduce canagliflozin exposure; take canagliflozin at least 1 hour before or 4-6 hours after a bile acid sequestrant. Effects of Invokana on other medicines: Monitor patients on digoxin, lithium, other cardiac glycosides, dabigatran. Inhibition of Breast Cancer Resistance Protein cannot be excluded; possible increased exposure of drugs transported by BCRP (e.g. rosuvastatin and some anti-cancer agents). Pregnancy and lactation: Do not use canagliflozin during pregnancy or when breast-feeding. Discontinue canagliflozin when pregnancy is detected. Effect on fertility unknown. Effects on ability to drive and use machines: Canagliflozin has no or negligible influence on ability to drive and use machines. However, patients should be alerted to the risk of hypoglycaemia when canagliflozin is used as add-on therapy with insulin/insulin secretagogue, and to the elevated risk of adverse reactions related to volume depletion. Side Effects (SEs): Adverse reactions are based on the pooled analysis of placebo-controlled, clinical studies. Very Common (≥ 1/10): vulvovaginal candidiasis, hypoglycaemia in combination with insulin or sulphonylurea. Common (≥ 1/100, <1/10): balanitis or balanoposthitis, urinary tract infection (pyelonephritis and urosepsis have been reported post-marketing), constipation, thirst, nausea, polyuria or pollakiuria, dyslipidaemia, haematocrit increased. Uncommon (≥ 1/1,000 to < 1/100): dehydration, dizziness postural, syncope, hypotension, orthostatic hypotension, photosensitivity, rash, urticaria, bone fracture, renal failure (mainly in the context of volume depletion), blood creatinine increased, blood urea increased, blood potassium increased, blood phosphate increased, lower limb amputations (mainly of the toe and midfoot) especially in patients at high risk for heart disease. For less frequent side effects see SmPC. Pack sizes: 30 x 1 film-coated tablets. Legal category: POM. Marketing
Authorisation number: EU/1/13/884/001-004 (100mg) and EU/1/13/884/005-008 (300mg). Marketing
treated with diuretics, and to have impaired renal function. Genital mycotic infections: Vulvovaginal candidiasis, and balanitis/balanoposthitis were reported in clinical studies. Urinary tract infections (UTIs): Complicated UTIs including pyelonephritis and urosepsis have been reported. Temporary interruption of canagliflozin should be considered. Cardiac failure: Experience in New York Heart Association (NYHA) class III is limited, with no experience in clinical studies with canagliflozin in NYHA class IV. Urine laboratory assessments: Patients taking canagliflozin will test positive for glucose in their urine. Lactose intolerance: Patients with galactose intolerance, total lactase deficiency, or glucose-galactose malabsorption should not take this product. Interactions: Diuretics: may increase risk of dehydration and hypotension. Insulin and insulin secretagogues: risk of hypoglycaemia; consider lower dose of insulin or insulin secretagogue. Effects of other medicines on Invokana: Enzyme inducers (e.g. St. John’s wort, rifampicin, barbiturates, phenytoin, carbamazepine, ritonavir, efavirenz) may decrease exposure of canagliflozin; monitor glycaemic control. Consider dose increase to 300 mg if administered with UGT enzyme inducer. Cholestyramine may reduce canagliflozin exposure; take canagliflozin at least 1 hour before or 4-6 hours after a bile acid sequestrant. Effects of Invokana on other medicines: Monitor patients on digoxin, lithium, other cardiac glycosides, dabigatran. Inhibition of Breast Cancer Resistance Protein cannot be excluded; possible increased exposure of drugs transported by BCRP (e.g. rosuvastatin and some anti-cancer agents). Pregnancy and lactation: Do not use canagliflozin during pregnancy or when breast-feeding. Discontinue canagliflozin when pregnancy is detected. Effect on fertility unknown. Effects on ability to drive and use machines: Canagliflozin has no or negligible influence on ability to drive and use machines. However, patients should be alerted to the risk of hypoglycaemia when canagliflozin is used as add-on therapy with insulin/insulin secretagogue, and to the elevated risk of adverse reactions related to volume depletion. Side Effects (SEs): Adverse reactions are based on the pooled analysis of placebo-controlled, clinical studies. Very Common (≥ 1/10): vulvovaginal candidiasis, hypoglycaemia in combination with insulin or sulphonylurea. Common (≥ 1/100, <1/10): balanitis or balanoposthitis, urinary tract infection (pyelonephritis and urosepsis have been reported post-marketing), constipation, thirst, nausea, polyuria or pollakiuria, dyslipidaemia, haematocrit increased. Uncommon (≥ 1/1,000 to < 1/100): dehydration, dizziness postural, syncope, hypotension, orthostatic hypotension, photosensitivity, rash, urticaria, bone fracture, renal failure (mainly in the context of volume depletion), blood creatinine increased, blood urea increased, blood potassium increased, blood phosphate increased, lower limb amputations (mainly of the toe and midfoot) especially in patients at high risk for heart disease. For less frequent side effects see SmPC. Pack sizes: 30 x 1 film-coated tablets. Legal category: POM. Marketing
* If further glycaemic control is needed, the addition of other anti-hyperglycaemic agents should be considered. § Continue dosing until dialysis or renal transplantation.
Authorisation number: EU/1/13/884/001-004 (100mg) and EU/1/13/884/005-008 (300mg). Marketing
Authorisation holder: Janssen-Cilag International NV, Turnhoutseweg 30, B-2340, Beerse, Belgium Marketed by: A. Menarini Pharmaceuticals Ireland Ltd. Further information is available on request from A. Menarini Pharmaceuticals Ireland Ltd., Castlecourt, Monkstown Farm, Monkstown, Glenageary, Co. Dublin A96 T924 or may be found in the SPC.
Date of preparation: July 2023.
Authorisation holder: Janssen-Cilag International NV, Turnhoutseweg 30, B-2340, Beerse, Belgium Marketed by: A. Menarini Pharmaceuticals Ireland Ltd. Further information is available on request from A. Menarini Pharmaceuticals Ireland Ltd., Castlecourt, Monkstown Farm, Monkstown, Glenageary, Co. Dublin A96 T924 or may be found in the SPC.
Date of preparation: July 2023.
Adverse events should be reported. Healthcare professionals are asked to report any suspected adverse events via: HPRA Pharmacovigilance Website: www.hpra.ie. Adverse events should also be reported to A. Menarini Pharmaceuticals Ireland Ltd. Phone no: 01 284 6744
treated with diuretics, and to have impaired renal function. Genital mycotic infections: Vulvovaginal candidiasis, and balanitis/balanoposthitis were reported in clinical studies. Urinary tract infections (UTIs): Complicated UTIs including pyelonephritis and urosepsis have been reported. Temporary interruption of canagliflozin should be considered. Cardiac failure: Experience in New York Heart Association (NYHA) class III is limited, with no experience in clinical studies with canagliflozin in NYHA class IV. Urine laboratory assessments: Patients taking canagliflozin will test positive for glucose in their urine. Lactose intolerance: Patients with galactose intolerance, total lactase deficiency, or glucose-galactose malabsorption should not take this product. Interactions: Diuretics: may increase risk of dehydration and hypotension. Insulin and insulin secretagogues: risk of hypoglycaemia; consider lower dose of insulin or insulin secretagogue. Effects of other medicines on Invokana: Enzyme inducers (e.g. St. John’s wort, rifampicin, barbiturates, phenytoin, carbamazepine, ritonavir, efavirenz) may decrease exposure of canagliflozin; monitor glycaemic control. Consider dose increase to 300 mg if administered with UGT enzyme inducer. Cholestyramine may reduce canagliflozin exposure; take canagliflozin at least 1 hour before or 4-6 hours after a bile acid sequestrant. Effects of Invokana on other medicines: Monitor patients on digoxin, lithium, other cardiac glycosides, dabigatran. Inhibition of Breast Cancer Resistance Protein cannot be excluded; possible increased exposure of drugs transported by BCRP (e.g. rosuvastatin and some anti-cancer agents). Pregnancy and lactation: Do not use canagliflozin during pregnancy or when breast-feeding. Discontinue canagliflozin when pregnancy is detected. Effect on fertility unknown. Effects on ability to drive and use machines: Canagliflozin has no or negligible influence on ability to drive and use machines. However, patients should be alerted to the risk of hypoglycaemia when canagliflozin is used as add-on therapy with insulin/insulin secretagogue, and to the elevated risk of adverse reactions related to volume depletion. Side Effects (SEs): Adverse reactions are based on the pooled analysis of placebo-controlled, clinical studies. Very Common (≥ 1/10): vulvovaginal candidiasis, hypoglycaemia in combination with insulin or sulphonylurea. Common (≥ 1/100, <1/10): balanitis or balanoposthitis, urinary tract infection (pyelonephritis and urosepsis have been reported post-marketing), constipation, thirst, nausea, polyuria or pollakiuria, dyslipidaemia, haematocrit increased. Uncommon (≥ 1/1,000 to < 1/100): dehydration, dizziness postural, syncope, hypotension, orthostatic hypotension, photosensitivity, rash, urticaria, bone fracture, renal failure (mainly in the context of volume depletion), blood creatinine increased, blood urea increased, blood potassium increased, blood phosphate increased, lower limb amputations (mainly of the toe and midfoot) especially in patients at high risk for heart disease. For less frequent side effects see SmPC. Pack sizes: 30 x 1 film-coated tablets. Legal category: POM. Marketing
Authorisation number: EU/1/13/884/001-004 (100mg) and EU/1/13/884/005-008 (300mg). Marketing
Adverse events should be reported. Healthcare professionals are asked to report any suspected adverse events via: HPRA Pharmacovigilance Website: www.hpra.ie. Adverse events should also be reported to A. Menarini Pharmaceuticals Ireland Ltd. Phone no: 01
Authorisation holder: Janssen-Cilag International NV, Turnhoutseweg 30, B-2340, Beerse, Belgium Marketed by: A. Menarini Pharmaceuticals Ireland Ltd. Further information is available on request from A. Menarini Pharmaceuticals Ireland Ltd., Castlecourt, Monkstown Farm, Monkstown, Glenageary, Co. Dublin A96 T924 or may be found in the SPC. Date of preparation: July 2023.
Continue 100 mg for patients already taking Invokana§ Invokana should not be initiated.
Dose adjustment recommendations according to eGFR¹