
12 minute read
Combination treatment in myopia management


Combination treatment in myopia management
When do Miyosmart and low-dose atropine complement one another?
A few years ago, Hoya Vision Care introduced the Miyosmart spectacle lens, at this time the first noninvasive method to slow down myopia progression in children with defocus segment technology. Additionally, experts use either special contact lenses, multifocal spectacle lenses or atropine eye drops for myopia management in children. The obvious question is whether the different approaches can be successfully combined. With initial studies showing promising results, Hoya Vision Care is now investigating with global experts when is the ideal time to prescribe atropine for patients with severe myopia progression. By Torben Othersen
Almost immediately after the market launch of Miyosmart in Germany, ophthalmologists and orthoptists began to wonder what a combination of special specatcle lenses and atropine might achieve, particularly in patients with severe myopia progression. At that time, there were no data on this, but now clinical evidence is available.
Miyosmart with DIMS (Defocus Incorporated Multiple Segments) Technology first became available in Germany in March 2021, and since then Hoya Vision Care has been working with experts from around the world to build up an evidence-based foundation and consensus on how ophthalmologists might best combine the use of those spectacle lenses with atropine.
Great interest in spectacle lenses
“Spectacle lenses offer an opportunity for safe, non-invasive and effective myopia management in children and teens,” said Torben Othersen, Professional Affairs Manager for myopia at Hoya Len
Germany. “Since the Miyosmart spectacle lenses became available in Germany, there has been a very high level of interest in intelligent myopia management for children using Miyosmart; both on the part of ophthalmology and orthoptics as well as optometry. We are very pleased about it, because the interdisciplinary exchange between eye care professionals is enormously important for any serious and sustained discussion of myopia management,” adds Othersen.
Confidence in the special spectacle lenses by eye care professionals has been further reinforced following publication of the 6-year results from the long-term clinical study in April 2023, showing that these lenses remain effective over a long period of time.[1] This is the longest study on spectacle lenses for myopia management ever carried out.
The 6-year results are follow-up on the 2-year double-blind randomized controlled clinical trial (RCT) published in the British Journal of Ophthalmology in 2019.[2]
Results from this study indicate that the children aged 8 to 13 who received Miyosmart spectacle lenses from the beginning demonstrated a slowdown on average by 60% in axial eye length growth and on average by 59% in refractive error progression, compared to the control group who wore conventional single vision spectacle lenses during the first two year of the study.[2]
After the Miyosmart spectacle lens was able to establish itself globally, with over four million lenses already sold in Asia, Australia, Canada and Europe from launch in 2018 up to the end of 2022, [3] Othersen says: “It was appropriate for Hoya Vision Care to initiate a discussion about a combination treatment with low-dose atropine. Thus, Hoya convened a meeting with global experts in 2022, with the aim of finding a consensus on how the use of atropine could best be combined with these spectacle lenses.”
Experts from around the world
The participants included renowned experts from Europe and Asia, among them was the respected myopia researcher Professor Hakan Kaymak from Düsseldorf, Germany, who shared with the expert´s insights from his clinical experience and research.
All experts as well shared their experience with Miyosmart spectacle lenses, including their clinical use in combination with 0.01% atropine in myopic children and adolescents in Europe, when the desired results were not achieved with using Miyosmart spectacle lenses as a monotherapy.
Key findings
The experts noted a “better control effect” with the combination treatment and reported that there were no clinically significant differences in visual acuity, contrast vision or binocular vision depending on whether Miyosmart spectacle lenses were used alone or in combination with low-dose atropine. According to Othersen, the consensus helps ophthalmologists to distinguish whether a patient should continue having a monotherapy or whether a greater myopia control effect could be achieved through the combination of spectacle lenses with low-dose atropine.
“This largely depends on whether the treatment goal has been achieved in the patient or not. If myopia progresses at the rate of emmetropic eye growth, continuation of a monotherapy with Miyosmart spectacle lenses is recommended,” Othersen explained. “However, when the treatment goal has not been achieved, it is important to inform eye care professionals about the additional benefit of combination treatment with low-dose atropine. Both procedures offer different approaches to slow down fast myopia progression; as such they are complementary.”
When the treatment goal has not been achieved, it is important to inform ECPs about the additional benefit of combination treatment with low-dose atropine.
Treatment goals and geographical differences
Much of the discussion concerned the question of whether the treatment goal has been achieved or not. But what is the goal in myopia management? Led by Prof. Kaymak, the five experts pointed out that while the approach of using emmetropic respectively physiologic eye-length growth as a guide to myopia progression has been described in several papers, it has not been fully accepted yet.
However, eye growth in axial length of 0.10 mm per year between the ages of 10 and 13 has been shown to be associated with normal emmetropic eye growth,[4] whereas eye growth of more than 0.20 mm per year indicates that the treatment goal has not been achieved. Here it is important to mention that emmetropic eye growth is age-dependent. A Dutch study found that annual eye growth averaged 0.09 mm in 10- to 13-year-old emmetropes and 0.19 mm on average in 6- to 9-year-old emmetropes.[5]
However, treatment goals may also vary depending on which part of the world is concerned. “Treatment goals in diopters differ in Asian and Caucasian children. In Asian children, an annual increase in refractive error of less than -0.80 D is considered successful. In Caucasian children, European experts recommend a threshold of -0.50 D or less per year,” experts say.
Regarding the start of treatment, the expert panel recommended that older children with a lower risk of developing severe myopia, may initially be treated with optical interventions alone. In young children with a high-risk profile and myopia progression of -0.50 D or greater over the previous six months, starting immediately with combination treatment should be considered.
But what concentration of low-dose atropine is appropriate?
The experts explained that the dosage is usually set individually, depending on the myopia control and the side effects. They referred to the LAMP study which was conducted on Chinese children. The study evaluated the efficacy of different dosages of 0.01%, 0.025% and 0.05% over a three-year period. Dose-dependent efficacy for myopia control was observed, i.e. the higher the dosage, the better the myopia control. While side effects appeared acceptable at a dosage of 0.05% in Asian children, this was not the case in Caucasian children with lighter eyes.[6]
“The experts did not find clinically significant changes in visual acuity or binocular vision when comparing Miyosmart spectacle lenses as a monotherapy and in combination with low-dose atropine”, the consensus document states.
“Contrast vision with Miyosmart spectacle lenses alone and in combination with 0.01% atropine was investigated. No differences in contrast vision were found.[7] Where the expected treatment goal was not achieved with Miyosmart spectacle lenses alone as a monotherapy, the experts observed an improved myopia management effect using a combination treatment with low-dose atropine.” Another important consideration is variations in how atropine is prescribed in different parts of the world. Currently, atropine is prescribed in doses ranging from 0.01% to 0.5% for children in Asia.
In young children with a high-risk profile and myopia progression of -0.50 D or greater, over six months, starting immediately with combination treatment should be considered.
However, this also depends on the individual country and the particular preferences of the eye care professionals concerned.
In some countries, reimbursement by health insurance companies also plays a role. In Taiwan, for example, only concentrations of 0.125% and higher are reimbursed, and thus these are more commonly prescribed than lower dosages.
In many European countries, where atropine is not reimbursed by the health insurance, the most common dosage is still 0.01%. However, the consensus of most professional ophthalmic associations now tends to be towards a higher dosage of 0.02% to 0.05%.
What studies show
In parallel with the consensus document, the investigations on combination treatment with spectacle lenses and atropine are growing.
In October 2022, Prof. Kaymak published his study examining the safety of combination treatment with Miyosmart spectacle lenses and 0.01% atropine.[7] In a pilot study of 12 young adults, he analyzed combination treatment in terms of safety. In each subject, bestcorrected visual acuity, contrast vision, and glare sensitivity were examined under the influence of the spectacle lenses alone and in combination with 0.01% atropine.
Miyosmart spectacle lenses with DIMS. technology do not pose any safety risk.[7] No significant changes were observed in visual acuity and binocular vision between Miyosmart spectacle lens alone and in combination with low-dose atropine.[8]
In an even more recent study, led by Zhu Huang et al. at Zhejiang University in Hangzhou, China, published in December 2022, the research team evaluated the efficacy of DIMS spectacle lenses in combination with 0.01% atropine. To the best of their knowledge, this study was the first to examine the treatment effect as a combination therapy with 0.01% atropine in terms of slowing axial eye length growth in myopic children.[9]
The retrospective study of 107 children was designed to determine whether combination treatment could slow the myopia progression, compared with a monotherapy or single vision spectacle lenses on their own.
“After the one-year follow-up period, the monotherapy with Miyosmart spectacle lens showed that myopia progression and axial eye length growth were lower compared to single vision spectacle lens use and even better in subjects treated with combination treatment with 0.01% atropine. This indicates a synergetic effect due to the combination treatment,” the authors report.
First European study on combination treatment [10]
The study, designed by Prof. Paolo Nucci and his team, was conducted with the aim to evaluate the efficacy of spectacle lenses with DIMS technology in slowing the myopia progression in young children and teenagers aged 6-18 years.
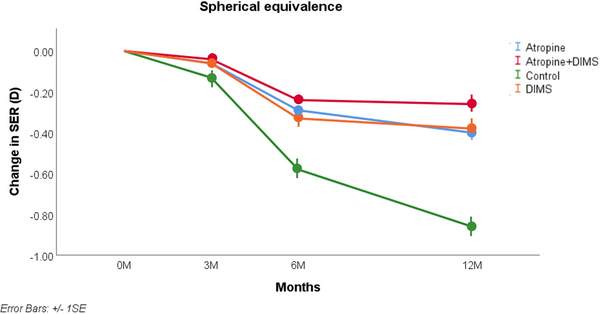
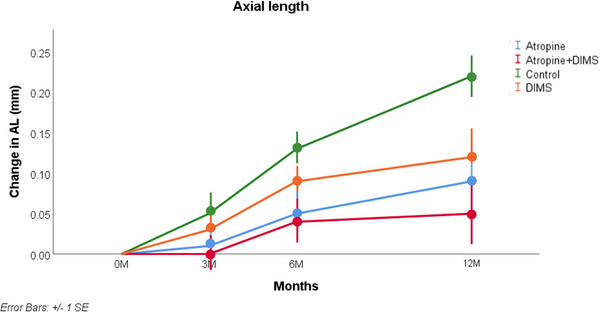
Subjects were treated with either 0.01% atropine, Miyosmart spectacle lenses, or a combination treatment using both, depending on patients and parents’ choice. The refractive and axial elongation changes of the three groups were then compared with a group of children wearing conventional single-vision spectacle lenses (control group).
Subjective visual acuity, cycloplegic refraction (SER), and axial length (AL) were assessed at 3, 6 and 12 months after the start of treatment. The analysis, performed on a total of 146 subjects, showed a reduction in the myopia progression in the three treatment groups, both in terms of change in refractive error and axial eye length growth. Among these, the group which received combination treatment showed an even more significant reduction in myopia progression. The results confirm the efficacy of low-dose atropine and of Miyosmart spectacle lens, as monotherapy in each case, in slowing myopia progression. The efficacy of both interventions is further increased when prescribed in combination.
The group which received combination treatment showed an even more significant reduction in myopia progression.
Raising standards
According to Othersen, in light of the emergence of new research and consensus on combination treatment, Hoya Vision Care aims to continue to play its leading role in myopia management and ensure that eye care professionals can make clear, informed decisions about evidence-based treatment for myopic children. This is part of a sustained effort to try and raise the standard of myopia management worldwide. It includes Hoya Vision Care's partnership
with Haag-Streit to market the Biometer (Lenstar Myopia) for measuring axial eye length.
“More and more eye care professionals are realizing that they can use optical biometry to provide and ensure the gold standard for myopia management,” Othersen says: “The ability to take objective measurements, such as measuring eye length, is related to the consensus document and provides information on whether treatment goals are best met with Miyosmart spectacle lenses as a monotherapy or whether it should rather be combined with additional low-dose atropine,” concluded Othersen. ◆
This article was written in collaboration with Torben Othersen, Professional Affairs Manager Myopia at Hoya Lens Germany. The Master Optician has many years of experience with chain stores and traditional opticians. Most recently he worked as Key Account Manager Myopia Program in the Professional Service DACH division in the optical industry.
References:
[1] Lam, C.S.Y., Tang, W.C., Zhang, H.Y. et al. Long-term myopia control effect and safety in children wearing DIMS spectacle lenses for 6 years. Sci Rep 13, 5475 (2023). https:// doi.org/10.1038/s41598-023-32700-7
[2] Lam CSY, Tang WC, Tse DY, Lee RPK, Chun RKM, Hasegawa K, Qi H, Hatanaka T, To CH. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomized clinical trial. British Journal of Ophthalmology. Published Online First: 29 May 2019. doi: 10.1136/bjophthalmol-2018-313739
[3] Based on the number of lenses sold according to Hoya sales data (as of January 2023) (in German). Individual wearer’s results may vary.
[4] Gifford KL, et al. IMI – Clinical Management Guidelines Report. Invest Ophthalmol Vis Sci. 2019;60(3):M184-M203.
[5] Rationale for Intervention. MYOPIE.NL. Available from: https://www.myopie.nl/en/ professionals/rationale-for-intervention/ (Accessed 30. June 2023).
[6] Joachimsen L, Farassat N, Bleul T, Böhringer D, Lagrèze WA, Reich M. Side effects of topical atropine 0.05% compared to 0.01% for myopia control in German school children: a pilot study. Int Ophthalmol. 2021;41(6):2001-2008. doi:10.1007/ s10792-021-01755-8
[7] Kaymak H., Reliability of DIMS spectacle lenses and atropine in combination therapy to inhibit myopia progression (in German). Klin. Monatsbl. Augenheilkd. 2022; 239: 1197–1205.
[8] Kaymak H, et al. Safety of DIMS Spectacle Lenses and Atropine as Combination Therapy for Myopia Progression. Klin Monbl Augenheilkd. 2022,239(10):1197-1205.
[9] Huang, Z., Chen, XF., He, T. et al. Synergistic effects of defocus-incorporated multiple segments and atropine in slowing the progression of myopia. Sci Rep 12, 22311 (2022). https://doi.org/10.1038/s41598-022-25599-z
[10] Nucci P, Lembo A, Schiavetti I, Shah R, Edgar DF, Evans BJW. A comparison of myopia control in European children and adolescents with defocus incorporated multiple segments (DIMS) spectacles, atropine, and combined DIMS/atropine. PLoS One. 2023 Feb 16;18(2):e0281816. doi: 10.1371/journal.pone.0281816. PMID: 36795775; PMCID: PMC9934319.
Picture: standret/stock.adobe.com



