When ozone is dissolved into water, the powerful oxidising actions of the solution make it effective against pathogens including bacteria, viruses, protozoa, fungi, fungal spores and bacterial spores.
MATTER MORE THAN YOU THINK
In the ever-evolving field of perio therapy, one truth remains constant: sharp instruments are essential for effective care explains Tabitha Acret 22 OZONATED WATER APPLICATIONS IN INFECTION PREVENTION AND CONTROL – A 2025 UPDATE
Olivia Wann reviews the steps to take to avoid injuries from needlesticks
With improvements in the technology for generating ozonated water, the potential applications of this technology continue to expand details Prof. Laurie Walsh
Publisher & Editor: Joseph Allbeury
ENOUGH
In clinical practice, we often have discussions with patients about their occlusal function and the need to ensure sufficient opposing pairs of natural teeth, or their relevant prosthetic replacements. We assume that patients understand the importance of proper chewing for effective eating, but this may not be so according to Prof. Laurie Walsh
www.oralhygiene.com.au
Cammeray 2062
New Grin Remote Orthodontic Monitoring
Grin remote monitoring offers a safer and more convenient approach to orthodontic care. Grin includes an easy-to-use Scope that, when attached to your patient’s smart phone, enables them to take self-scans of their mouth. You can then remotely monitor treatment progress, answer questions and effectively address any emergency situations without a necessitating a faceto-face appointment. With Grin, you are able to keep an even closer eye on your patients oral hygiene and overall treatment progress without the need for additional appointments. Available from Liift Dental on Tel: (02) 8355-2200, email grin@liift.dental or visit www.get-grin.com.
3 ways to get the most out of www.dentist.com.au
When people want to find a dentist, they mostly use the internet and Google “Dentist in...”. That’s what the research shows. Word of mouth is no longer king! Google only shows 3 or 4 individual dental practices on the first page of its search results. The other results returned are for, among other things, the website www.dentist.com.au. This directory lists all practices and practitioners and is searched a million times a year
Get Listed! If you’re listed on dentist.com.au, your phone will ring! So just do it!
Upgrade your listing: Just like in Google, where your practice sits in the dentist.com.au search results list determines how often your phone rings. If you’re at the top of the list, then your phone will ring more often and if there is more detailed information listed about your practice, then this helps too. Unlike Google, you can increase your priority in searches for an annual fee. This increases your prominence in searches for your home suburb and often also in the surrounding suburbs. Plus you can add heaps of detailed information about your practice and practitioners.
Add your link for online bookings. If you accept online bookings, then once you’ve upgraded your listing, you can add the link to accept online bookings through your preferred booking engine and this will appear directly in the search results list. For details on how to upgrade, visit: dentist.com.au/information-for-dentists
High-level disinfection and sterilisation are complex processes, requiring initial and ongoing training of frontline staff. A key component of appropriate disinfection and sterilisation is point-ofuse precleaning performed by front-line staff. The removal of gross soil at the point of use and keeping items moist until cleaning are important to prevent the hardening of debris or the development of biofilm due to processing delays which can lead to less effective decontamination. Infection outbreaks have occurred when one or more steps of reusable device processing are missed or done incorrectly. For this study, training and competencies for staff precleaning reusable devices prior to processing were developed. Precleaning requirements were reviewed and updated if indicated. A train-the-trainer approach was employed. Staff were required to understand the device function and the specifics of the manufacturer’s instructions for use, be knowledgeable on processing best practices and be able to provide practical application of best practices to their respective devices. In total, 254 participants attended the training program from 2018 through 2021. Median test scores improved from pre-test to post-test for all participants. Overall test scores significantly improved after participants completed the training each year. The results also showed that basic knowledge does not degrade over a 1-year period. These results show that well-designed hands-on training is an effective way to train health care workers on precleaning of reusable devices that require processing.
Fox J et al. Impact of COVID-19 pandemic on reusable device precleaning training for front-line staff. American Journal of Infection Control 2025;53:269-271 1 2 3
A new dimension of Varnish Gel
A new dimension of Varnish Gel
A new dimension of Fluoride Varnish
A new dimension of Varnish Gel
Profisil® Fluoride Varnish contains 5 % sodium fluoride in a mucosa-friendly, pleasantly flavoured dimethicone gel. This formula is not made with ethyl alcohol* or c (rosin), thus reducing the potential of soft tissue irritation or rosin-based allerg
Profisil® Fluoride Varnish contains 5 % sodium fluoride in a mucosa-friendly, pleasantly flavoured dimethicone gel. This formula is not made with ethyl alcohol* or colophony (rosin), thus reducing the potential of soft tissue irritation or rosin-based allergies.
Profisil® Fluoride Varnish contains 5 % sodium fluoride in a mucosa-friendly, pleasantly flavored dimethicone gel. This formula is not made with ethyl alco which helps prevent the risk of allergic reactions and other ailments
Product Properties
Profisil® Fluoride Varnish contains 5 % sodium fluoride in a mucosa-friendly, pleasantly flavoured dimethicone gel. This formula is not made with ethyl alcohol* or colophony (rosin), thus reducing the potential of soft tissue irritation or rosin-based allergies.
Product Properties
Product Proper ties
Product Properties
This formula is designed to securely adhere to the tooth surface for several hours while releasing fluoride ions up to 24 hours
This formula is designed to securely adhere to the tooth surface for several hours while releasing fluoride ions up to 24 hours
Immediate and continuous fluoride release
Transparent and colourless after applying for optimal aesthetics
Transparent and colourless after applying for optimal aesthetics
This formula is designed to securely adhere to the tooth surface for several hours while releasing fluoride ions up to 24 hours
Constant viscosity and easy to spread
Transparent and colorless after applying for optimal aesthetics
Constant viscosity and easy to spread
Transparent and colourless after applying for optimal aesthetics
Constant viscosity and easy to spread
Constant viscosity and easy to spread
The single dose blister contains sufficient varnish to cover all affected teeth of both arches
The single dose blister contains sufficient varnish to cover all affected teeth of both arches
Patients appreciate the smooth mouth feel and refreshing lubricating properties
The single dose blister contains sufficient varnish to cover all affected teeth of both arches
Profisil® Fluoride Varnish can be applied in any direction to all affected tooth surfaces, migrating even to difficult to access areas
Profisil® Fluoride Varnish can be applied in any direction to all affected tooth surfaces, migrating even to difficult to access areas
Patients appreciate the smooth mouth feel and refreshing lubricating properties
Protective coating to tooth surfaces by occluding tubules with calcium fluoride crystals
Patients appreciate the smooth mouth feel and refreshing lubricating properties
Protective coating to tooth surfaces by occluding tubules with calcium fluoride crystals
No need to dr y the teeth prior to application
Profisil® Fluoride Varnish can be applied in any direction to all affected tooth surfaces, migrating even to difficult to access areas
A prophylactic cleaning is not required prior to use
A prophylactic cleaning is not required prior to use
Profisil® Fluoride Varnish can be easily applied
A prophylactic cleaning is not required prior to use
Unnecessary to dry teeth prior to application of the varnish gel
access areas
Unnecessary to dry teeth prior to application of the varnish gel
Unnecessary to dry teeth prior to application of the varnish gel
Increases fluoride acceptance
Lubricious, non-clumping formula No need to replace gummy brushes
Lubricious, non-clumping formula No need to replace gummy brushes
Lubricious, non-clumping formula No need to replace gummy brushes
Unnecessar y to dr y teeth prior to application of the varnish gel
Product range
The varnish is available in following versions:
Won‘t clog suction lines
Product range
Product range
BER RY UNF LAVORE D
Lubricious, non-clumping formula
The varnish is available in following versions:
The varnish is available in following versions:
Available as single dose unit incl. a brush for easy application.
No need to replace gummy brushes
Available as single dose unit incl. a brush for easy application.
k
Protective coating to tooth surfaces by occluding tubules with calcium fluoride crystals
No bitter taste or burning not made with ethyl alcohol*
No bitter taste or burning not made with ethyl alcohol*
Great taste and texture that provides a smooth mouth feel that patients will love
No bitter taste or burning not made with ethyl alcohol*
Non-allergenic dimethicone formula
Available as single dose unit incl. a brush for easy application. MINT BER RY UNF LAVORE D
Mint Normal Pack
Mint N ormal Pa ck
Berry Normal Pack
ALWAYS READ THE LABEL AND FOLLOW THE DIRECTIONS FOR USE.
* ‘Mint’ and ‘Unflavored’ are not made with ethyl alcohol, ‘Berry’ may contain traces of ethyl alcohol.
J.Wisbey & Associates Pty
Non-allergenic dimethicone formula
Protective coating to tooth surfaces by occluding tubules with calcium fluoride cr ystals
Suitable for all ages and for children with primary teeth
Non-allergenic dimethicone formula
Suitable for all ages and for children with primary teeth
No stinging, burning or bitter after taste not made with ethyl alcohol
Suitable for all ages and for children with primary teeth
Patients can immediately resume eating and drinking*
of 30 x 0.5ml (10 x Mint, 10 x Berry, 10 x Unflavoured)
of 50 x 0.5ml Single Dose Blister Pack
Mint Normal Pack Box of 50 x 0.5ml Single Dose Blister Pack Berry Normal Pack
Unflavoured Normal Pack
MINT BER RY UNF LAVORE D Unflavoured N ormal Pa ck
Unflavoured Normal Pack
ALWAYS READ THE LABEL AND FOLLOW THE DIRECTIONS FOR USE.
‘Mint’ and ‘Unflavored’ are not made with ethyl alcohol, ‘Berry’ may contain traces of ethyl alcohol.
Box of 50 x 0.5ml Single Dose Blister Pack
Box of 50 x 0.5ml Single Dose Blister Pack
Box of 50 x 0.5ml Single Dose Blister Pack Berry N ormal Pa ck Box of 50 x 0.5ml Single Dose Blister Pack
Box of 50 x 0.5ml Single Dose Blister Pack Box of 50 x 0.5ml Single Dose Blister Pack
*Avoid hot liquids , hard crunchy foods and alcohol.
ALWAYS READ THE LABEL AND FOLLOW THE DIRECTIONS FOR USE. * ‘Mint’ and ‘Unflavored’ are not
J.Wisbey & Associates Pty Ltd trading as WISBEY DENTAL / ABN 98 052 034 238 Suite 17, 265-271 Pennant Hills Rd, Thornleigh NSW 2120. PO Box 291, Thornleigh. NSW T: + 61 2 9875 5588 www.wisbeydental.com
AKT14804
AKT14806
Box of 50 x 0.5ml Single Dose Blister Pack AKT14802
Combi pack
Box of 30 x 0.5ml (10 x Mint, 10 x Berry, 10 x Unflavoured) AKT14801
Combi pac
Box
Grin debuts its AI-driven remote orthodontic monitoring ecosystem in Australia and New Zealand
Grin’s full virtual care ecosystem, offering personalised care, revenue boosting and AI-powered optimisation solutions, is now available to doctors and patients across both countries
GGRIN, the leading remote monitoring and care platform for digital oral healthcare solutions, announced that its comprehensive system is now available to oral care professionals across Australia and New Zealand.
This marks a major milestone in the company’s mission to create the next era of orthodontics globally. Grin now delivers AI-powered, human-first care across the US, Canada, Brazil, the EU, Israel and now Australia and New Zealand.
Grin’s full platform—including the FDA- and TGA-listed Grin Scope® and Scope Mini, now approved in Australia—features a powerful app, doctor portal and AI-enabled tools that strengthen patient relationships through virtual monitoring, human intelligence and real-time communication.
Typically, Grin Doctors provide patients undergoing orthodontic treatment, whether with brackets and wire or aligners, with a Grin Scope that attaches to their smartphone. The innovative Grin app then guides patients to video scan their teeth in treatment in front of a mirror.
These scans are then immediately available to the clinician for review via the doctor portal to monitor treatment progress and address any clinical issues.
Importantly, at the heart of it all is the Grin Care Specialist— an extension of your team who ensures virtual care is seamless, your workflows stay efficient and your patients remain connected, engaged and on track every step of the way. Human Grin Care Specialists are able to maintain a dialogue with patients and alert Grin Doctors when required, increasing efficiency.
With features like Grin CoPilot™, Grin 3D Tx Tracker™, Grin RapidReferral™ and other enhanced AI-enabled tools, as well as a new integration with Clarity™ by Solventum, Grin’s platform offers an unmatched, scalable, patient-first solution.
“At Grin, our mission is to simplify care and make quality oral health more accessible to patients everywhere,” said Dr Adam Schulhof, CEO and Co-Founder of Grin. “We’re excited to extend this mission to providers across Australia and New Zealand, who, until now, haven’t had access to a comprehensive platform that combines AI-powered technology with human clinical oversight to deliver precision, streamline operations and foster stronger patient connections.”
Grin’s Australasian launch also sets the stage for greater access in rural and remote regions, reducing barriers to care. Grin’s ecosystem allows doctors to continue to scale while maintaining care with remote patients.
“I’ve watched Grin evolve over the past several years,” said Dr Vas Srinivasan, specialist orthodontist and practice owner at Invisible Orthodontics in Hervey Bay, Queensland. “I value its sleek, intuitive design that enables me to monitor progress, step in when necessary and minimise unnecessary appointments.
Most importantly, I feel confident scaling my practice with Grin, knowing it was built by Dr Adam Schulhof—an orthodontist who truly understands what it takes to grow successfully.”
“Grin brings something truly fresh to the ANZ market—a smart, clinically driven platform that meets the evolving needs of both providers and patients,” said Andrew Holmes, CEO of Liift Dental, distributor of Grin in Australia and New Zealand.
“Having seen the challenges practices face in balancing growth with efficiency, I believe Grin’s combination of AI-powered tools and human clinical oversight offers a practical, scalable solution. Its flat-fee pricing model that includes the Grin Scope and what amounts to lifetime monitoring delivers real financial value to Australian practices—providing cost predictability, supporting increased patient volume and helping improve the bottom line without the burden of rising fees. It’s a smarter way to grow and exactly the kind of innovation this region has been waiting for.”
About Grin
Based in New York, Grin is a comprehensive digital platform that provides solutions for all oral health needs. The Grin App and Grin Scope® allow doctors to access a full patient management suite. Patients can access quality professional care from the convenience of their smart devices. Doctors can remotely monitor patients via virtual check-ins for complete visibility—reducing chair time, increasing patient volume, and ensuring safety.
For more information on Grin ®, visit www.get-grin.com or call ANZ Country Manager Andrew Holmes on 0420-985-661, email grin@liift.dental or call (02) 8355-2200.
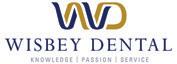
The Waterpik Water Flosser: Significantly more effective than interdental brushes for improving gingival health
Comparison of water flosser and interdental brush on reduction of gingival bleeding and plaque: A randomized controlled pilot study
Objective
To determine the efficacy of a Waterpik Water Flosser vs interdental brushes for plaque and gingivitis reduction.
Methodology
Twenty-eight subjects completed this two week study. Subjects were assigned to one of two groups: the Waterpik Water Flosser (WF) plus a manual toothbrush or interdental brushes (IDBs) plus a manual toothbrush. Gingival health was evaluated by measuring bleeding on probing (BOP) at six sites per tooth. Plaque removal was measured using the Rustogi Modification of the Navy Plaque Index (RMNPI).
Results
The Waterpik Water Flosser was significantly more effective than the interdental brushes for reducing gingival bleeding. Notably, the Water Flosser was 56% more effective for reducing whole mouth bleeding and 53% more effective for reducing whole mouth approximal bleeding
Conclusion
The Waterpik Water Flosser is significantly more effective than interdental brushes for improving gingival health.
To book your free Professional Education Waterpik Lunch & Learn Session or to try Waterpik yourself at Professional Trial rates, visit www.waterpikshop.com.au or email professionalAU@waterpik.com
Inner ergonomics - a practical recipe to career longevity
By Dr Anikó Ball, BDSc (Melb), Dip.Clin.Hypnosis, Adv.Dip. Alexander Studies
Wrldwide research shows an alarming incidence of musculoskeletal disorders in dentistry, resulting in early retirement or reduced work hours for many and a career change for some.
Ergonomic research and design have focused on dentists’ work environment - the so-called Outer Ergonomics, overlooking the importance of their efficiency in posture and movement - the Inner Ergonomics.
HOW a dentist sits on a stool and bends over the dental chair is as important as the stool and chair design. The WAY instruments are held is as important as the shape and the weight of the instrument.
Dental schools don’t provide a “User Guide” on how to bend over patients and what to do with shoulders and arms to ensure career longevity. An understanding of how your body was designed to work, especially during work postures held for prolonged periods, is essential.
OUser Guide for the spine
nce you know that all the intervertebral joints below C2 (just under ear level) are gliding joints, which are not designed for prolonged bending, you will want to avoid work postures that involve bending forward and leaning to the side. Intervertebral discs are distorted when the spine is bent and twisted, resulting in cumulative trauma and a high risk of developing a pain syndrome.
Unless you are using refractive loupes or an operating microscope, you cannot sit upright and see into patients’ mouths without spinal trauma.
Working with nonrefractive loupes or without loupes, you need to pivot your torso slightly forward at the hip joints, without bending the spine and look down by rotating your head at the atlanto-occipital joint (at ear level). As there is only a 10-degree freedom for downward head rotation available at this joint, non-refractive loupe users need an adequate declination angle to avoid compensatory neck bending.
User Guide for shoulders and arms
Most dentists work with a raised non-dominant shoulder and elbow.
The muscles moving the shoulders and arms are designed for a short contraction. Prolonged use of movement muscles to hold up the shoulder, or the arm against gravity when hovering with the mouth mirror without a finger rest, results in cumulative trauma. Always have a finger rest and don’t raise your shoulder or elbow.
Take care of yourself, you are your most precious instrument.
Dr Anikó Ball is the Founder of Optimum Dental Posture. For info, see www.optimumdentalposture.com
� byron medical
Place your order before June 22nd to enjoy savings of up to $3,300* in tax in this financial year!
Ends June 22nd. T&C's apply. Scan the QR code to check out our deals
The cutting edge: Why sharp instruments matter more than you think
By Tabitha Acret, BOH, Grad.Cert (Public Health), Current Master’s Student
In the ever-evolving field of periodontal therapy, one truth remains constant: sharp instruments are essential for effective care. Yet surprisingly, many clinicians overlook this foundational aspect of treatment. Blunt curettes, over-worn sickles and poorly maintained universal scalers not only compromise outcomes— they put clinicians and patients at risk. It’s time to revisit the basics of instrument sharpening and redefine it not as a chore, but as a clinical priority.
Dull instruments are not just inefficient—They’re dangerous!
Let’s start with the obvious. A dull curette or scaler cannot remove calculus effectively. It requires increased lateral and apical pressure, more strokes and more physical exertion. But the downstream effects go far beyond inefficiency. Using blunt instruments has been linked to:
• Incomplete calculus removal;
• Burnishing of subgingival deposits;
• Soft tissue trauma;
• Root surface gouging;
• Patient pain and sensitivity;
• Slipping and operator loss of control; and
• Clinician fatigue and repetitive strain injuries.
One study cited in Dimensions of Dental Hygiene describes instrument sharpness as a key factor influencing therapeutic success, operator fatigue, musculoskeletal injury, time management and stress. In simple terms: if your instruments are dull, your body and your patients pay the price.
“Burnished calculus becomes difficult to remove because the instrument’s cutting edge tends to slip over the smooth surface.” Gehrig & Willmann, 2019
The physical toll on clinicians
Blunt instruments increase gripping force and prolong scaling time—two major contributors to musculoskeletal disorders (MSDs). According to data, 60–93% of dental hygienists experience work-related MSDs, particularly in the hands, wrists, neck and shoulders. These injuries are often preventable and instrument sharpness is one of the simplest interventions.
Repeated forceful strokes increase the risk of:
• Carpal tunnel syndrome;
• Tendonitis;
• Trigger finger; and
• Chronic neck and back pain.
Many of these conditions are careerending. Investing time into sharpening instruments correctly isn’t just about scaling efficiency—it’s about professional longevity.
“Blunt instruments increase gripping force, linked to carpal tunnel syndrome and tendinitis.” Dimensions of Dental Hygiene, 2022
A matter of patient experience
From the patient’s perspective, a dull curette can feel like a rake on soft tissue. This can lead to:
• A dragging sensation during instrumentation;
• Prolonged tenderness post-procedure;
• Heightened sensitivity to air, water, or touch; and
• Anxiety during future appointments.
Patients may not understand why a scaling appointment is painful—but they’ll often assume it’s the clinician’s technique. One painful visit is sometimes enough to erode trust or trigger non-compliance.
The science of effective debridement
Effective periodontal therapy depends on thorough debridement—not just of supragingival plaque but also tenacious, embedded subgingival calculus.
According to Carranza (2015), subgingival calculus can attach to cementum via mechanical interlocking, making its removal particularly challenging.
Research shows that even after careful root debridement, 17–64% of subgingival calculus may remain. Even surgical intervention doesn’t guarantee total removal, with 7–24% of deposits still found post-flap. These figures highlight just how precise and sharp our instruments must be.
Burnished
calculus: The invisible enemy
One of the most insidious consequences of blunt instrumentation is burnished calculus—smoothed-over deposits that remain attached but are nearly impossible to detect. These burnished surfaces resist removal and continue to harbour pathogenic biofilms, delaying healing and contributing to persistent inflammation.
Burnished calculus is most often found:
• In furcations;
• Around CEJs;
• In root concavities; and
• Deep subgingival pockets.
“Burnishing of calculus may lead to delayed healing of the periodontal tissue and possible periodontal abscesses.”
Wilkins & Wyche, 2020
The ethical and legal imperative
Blunt instruments don’t just hurt patients—they can get you into trouble. Failing to maintain functional instruments may be seen as clinical negligence, especially if it leads to:
• Soft tissue trauma;
• Missed calculus contributing to disease progression;
• Instrument fracture or breakage; and
• Unreported adverse events.
The Dental Board of Australia’s Code of Conduct reminds us that we have a professional and ethical obligation to provide care that minimises harm.
Using a curette with a worn or rounded edge—especially when you know it’s not functioning properly—breaches that standard.
How to sharpen smart:
Instrument-by-instrument
Sickle Scalers
Sickles have two cutting edges per working end. The terminal shank should be held at 12 o’clock, with the stone angled at 1 o’clock (100–110°). Sharpen both sides from heel to tip and finish with a downward stroke to remove any wire edge.
Gracey Curettes (11/12 & 13/14)
Gracey curettes are area-specific, with only one cutting edge per end—the lower cutting edge.
The terminal shank should be at 11 o’clock and the stone at 1 o’clock. Sharpen only the tip and middle third, avoiding the heel and non-working edge. Sharpening the wrong edge destroys the built-in 70° angulation, rendering the instrument ineffective.
“Sharpening the wrong side—typically the non-working edge—compromises the instrument’s design. Mistakenly sharpening the upper edge ruins the offset angle.” Gehrig & Willmann, 2019
Universal Curettes
Universals have two cutting edges that require symmetrical sharpening. Terminal shank at 12 o’clock, stone at 1 o’clock (right edge) and 11 o’clock (left edge). Avoid over-thinning the toe or flattening the blade—these changes reduce adaptability and cutting power.
Common sharpening mistakes to avoid
6 Sharpening the wrong edge on Graceys
6 Over-sharpening the heel
6 Flattening the rounded toe
6 Sharpening past the middle third
6 Using excessive force or the wrong stone
6 Continuing to sharpen an instrument that should be retired
When to retire an instrument
Even with perfect sharpening, curettes and scalers don’t last forever. If you’re finding that:
• Your instrument looks shortened;
• The shape is distorted or asymmetrical;
• You’re still struggling to remove deposits; or
• You’ve already reshaped the toe... ...it’s time to replace it.
“A curette that’s been shortened too far no longer performs its job and may put your patients and your reputation at risk.” Wilkins, 2020
In high-traffic hygiene departments where kits are used multiple times a day, instruments may need to be replaced every 6–12 months.
Build this into your preventative care department’s annual budget.
The financial argument: Sharpening saves money— Until it doesn’t
Instrument sharpening extends the life of your tools and can delay replacement. But repeated sharpening of an already-compromised instrument wastes time and compromises care.
Investing in quality instruments and maintaining them properly is more cost-effective in the long run than struggling through appointments with underperforming tools.
These options can reduce sharpening frequency while maintaining precision.
A
sharpening culture in every clinic
Creating a culture of sharpening and instrument maintenance starts with:
• Routine sharpening protocols (e.g., weekly or post-each-use);
• Sharpening logs to track instrument condition;
• Clinical audits on blade sharpness and shape;
• In-clinic training on sharpening techniques; and
• Team accountability—every clinician is responsible for their tools!
Final thought:
Don’t graduate and retire with the same instruments
Too many clinicians continue to use the same instruments they had in dental school—10 years later. In reality, sharpness begins to degrade within weeks of regular use. Our patients deserve better. So do our hands, our backs and our standards of care. As dental professionals, we don’t just scale—we diagnose, assess, and intervene in diseases that affect systemic health. If our tools are dull, our message is too. It’s time to stay sharp— in every sense of the word!
References
1. Gehrig, J.S., & Willmann, D.E. (2019). Foundations of Periodontics for the Dental Hygienist (5th ed).
2. Wilkins, E.M., & Wyche, C.J. (2020). Clinical Practice of the Dental Hygienist (13th ed).
3. Neuman, T. (2022). Instrument Maintenance and Sharpening. Dimensions of Dental Hygiene, 20(9), 34–37.
4. American Academy of Periodontology. (2015). Comprehensive Periodontal Therapy Statement, J Periodontol, 86(7), 835–838.
5. Chapple, I.L.C., et al. (2015). Primary prevention of periodontitis: managing gingivitis. J Clin Periodontol, 42(Suppl 16): S71–S76.
6. Dental Board of Australia. (2020). Code of Conduct for Registered Health Practitioners.
7. Carranza’s Clinical Periodontology (12th ed).
About the author
Tabitha Acret is a dedicated and passionate award-winning Dental Hygienist. She studied a Bachelor or Oral Health at Newcastle University , Graduate Certificate in Public Health and is a current Masters student. Tabitha has become one of the most sought-after Hygienists and Educators in Australia and internationally with a fast-growing and loyal customer base of patients, dental professionals and media. Tabitha was previously the National Vice-President for the Dental Hygienists Association of Australia and has volunteered in many roles since graduation for the Association. She also has a passion for educating with students, working as a Clinical Educator at Sydney University and Newcastle University as well as working in private clinical practice and as a Clinical Educator within the dental industry.
Feel the difference Soft ergonomic handles and advanced instrument coatings reduce finger force and forearm fatigue for the same effect at the instrument tip.*
GRACEY 11/12 SD
• For molars and premolars.
• For mesial surfaces.
LM211-212SDES
GRACEY 7/8 SD
• For premolars and molars.
• For buccal and lingual surfaces. LM207-208MSDES
*SCAN CODE to see how the LM Test & Feel Machine works.
Why choose sharp?
‘Sharpen-free’ micro coating
Enjoy full control and improved tactile sense while easily and e ectively removing the calculus.
Saves time & money in the long run. Long-lasting superior sharpness. Improved productivity & clinical results.
‘Sharpen free’
Superior sharpness
Highest rated ergonomics
Minimum maintenance Diamond-like features
oral|hygiene CPD CENTRE
Question 1. What is the primary risk of using dull dental instruments during periodontal therapy?
a. Reduced appointment time.
b. Increased plaque formation.
c. Ineffective calculus removal and patient harm.
d. Over-polishing of tooth enamel.
Question 2. Which of the following is not a consequence of using blunt instruments, as mentioned in the article?
a. Root surface gouging.
b. Decreased need for anaesthesia.
c. Soft tissue trauma.
d. Clinician fatigue and repetitive strain.
Question 3. Why is burnished calculus particularly problematic?
a. It is harmless and can be ignored.
b. It is more visible and easier to detect.
c. It resists removal and can harbour biofilm.
d. It is only found in the upper arch.
Question 4. Which instrument has only one cutting edge per working end and requires sharpening only on the lower edge?
a. Universal curette
b. Sickle scaler
c. Gracey curette
d. Explorer
Question 5. According to the article, when should a dental instrument be retired?
a. Every two years, regardless of condition.
b. When the tip appears shiny.
c. When the shape is distorted or performance declines.
d. When the sharpening stone cannot touch the blade.
Question 6. What is one of the main reasons ozonated water is preferred over gaseous ozone in dental settings?
a. It is less costly and more convenient to use.
b. It has a longer half-life than gaseous ozone.
c. It is more corrosive, providing better sterilization.
d. It penetrates deeper into bacterial cell walls.
Question 7. Why does ozonated water act more quickly on Gram-negative bacteria than Gram-positive bacteria?
a. Gram-negative bacteria are smaller.
b. Gram-positive bacteria lack a cell wall.
c. Gram-negative bacteria have thinner cell walls.
d. Ozonated water selectively targets Gram-negative species.
Question 8. What is a major limitation of ozonated water as a disinfectant?
a. It causes irreversible damage to human tissues.
b. It degrades rapidly into oxygen, reducing its effectiveness over time.
c. It corrodes dental appliances.
d. It is toxic if ingested in small quantities.
Question 9. Compared to sodium hypochlorite (NaOCl), ozonated water is advantageous for disinfecting impressions because...
a. It increases surface wettability.
b. It creates a protective plastic coating.
c. It preserves impression surface detail better.
d. It forms stable chlorine compounds on the surface.
Question 10. Which of the following is NOT a documented application of ozonated water in dentistry, as mentioned in the article?
a. Treating periodontal pockets.
b. Disinfecting toothbrushes.
c. Decontaminating dental impressions.
d. Polishing dental prostheses.
INSTRUCTIONS:
Question 11. To help minimise the risk of sharps injuries:
a. Provide annual infection control training for all staff.
b. Implement a sharps injury prevention program.
c. Have protocols in place in case an injury occurs.
d Ensure all clinical staff are vaccinated against hepatitis B.
e. All of the above.
Question 12. A key benefit of using instrument cassettes is:
a. A reduction in time spent sorting instruments.
b. Fewer instrument breakages including scratched mirror heads.
c. Reduced sharps injuries as instruments are handled less.
d. That instruments are better organised.
e. All of the above.
Question 13. The risk of sharps injuries are minimised by using instrument cassettes through reduced instrument handling because:
a. After use, contaminated instruments are returned to the cassette and locked into place for transport to the instrument processing area.
b. The entire cassette is automatically cleaned in an ultrasonic cleaner or washer/disinfector.
c. The entire cassette is wrapped and steam sterilised, all without removing instruments from the cassette.
d. All of the above
Question 14. Practices can minimise the risk of sharps injuries by:
a. Avoiding transporting loose instruments and sharps on trays.
b. Only handling loose contaminated instruments with heavy duty, utility gloves in the sterilisation area rather than patient exam gloves.
c. Never retrieving instruments and patient care items with contaminated gloved hands in cabinets and drawers.
d. All of the above.
Question 15. According to the US CDC, collision with a worker or a sharp is the cause of 10% of needlestick injuries:
a. True
b. False
Question 16. Which of the following is not a direct benefit of prolonged chewing cycles?
a. Enhanced release of nutrients during digestion.
b. Increased appetite and food intake.
c. Suppression of ghrelin levels.
d. Improved insulin responsiveness.
Question 17. Why is prolonged chewing thought to have a positive impact on cognitive function?
a. It increases salivary amylase levels only in older adults.
b. It reduces appetite and leads to more sleep.
c. It stimulates cerebral blood flow, activating brain areas.
d. It prevents tooth loss, which directly improves memory.
Question 18. According to the article, what is one hormonal mechanism by which chewing helps regulate hunger?
a. Chewing increases cortisol and decreases leptin.
b. Chewing stimulates ghrelin, which reduces hunger.
c. Chewing decreases ghrelin and increases GLP-1 and insulin.
d. Chewing inhibits insulin secretion to maintain glucose levels.
Question 19. What factor contributes to individual differences in salivary amylase concentration?
a. The type of food consumed.
b. The number of teeth present.
c. The frequency of chewing gum.
d. The number of amylase gene copies.
Question 20. What is one major limitation of research studies on the effects of chewing, as highlighted in the article?
a. All studies are based only on children and teenagers.
b. The studies used artificial foods instead of real meals.
c. Blinding is difficult because participants are aware of their chewing activity.
d. The results are inconclusive due to extremely small sample sizes.
dentevents presents...
Infection Control BOOT CAMP
29 VIDEOS - 8+ HOURS OF EDUCATION
Presented by Emeritus Professor Laurence Walsh AO BDSc, PhD, DDSc, GCEd, FRACDS, FFOP (RCPA), FFDT (RCS Edin)
8
Learn from Australia’s leading authority on infection prevention and control in dentistry about recent changes in infection control including from the Dental Board of Australia (July 2022), the ADA (4th edition guidelines August 2021 and the ADA Risk management principles for dentistry during the COVID-19 pandemic (October 2021)), the new guidelines from NHMRC (May 2019), Hand Hygiene Australia (Sept 2019) and the CDNA (Dec 2018) as well as recent changes in Australian Standards and TGA regulations that are relevant to infection control. The course provides a summary of how those changes interlink with one another and also covers practical implementation of the new requirements and what it means for everyday dental practice. Hear about the why and the how and keep up-to-date with the changes that are happening.
COURSE TOPICS
This one day course will cover changes in regulations and guidelines from 2018 to 2022 including:
n Risk-based precautions.
n Hand hygiene and hand care practices.
n Addressing common errors in personal protective equipment.
n Biofilm reduction strategies.
n Efficiency-based measures to improve workflow in instrument reprocessing and patient changeover.
n Correct operation of mechanical cleaners and steam sterilisers.
n Wrapping and batch control identification.
n Requirements for record keeping for instrument reprocessing.
n Correct use of chemical and biological indicators.
Laurie Walsh is a specialist in special needs dentistry who is based at the University of Queensland in Brisbane, where he is an emeritus professor. Laurie has been teaching and researching in the areas of infection control and clinical microbiology for over 25 years and was chief examiner in microbiology for the RACDS for 21 years. His recent research work includes multiple elements of infection control, such as mapping splatter and aerosols, COVID vaccines and novel antiviral and antibacterial agents. Laurie has been a member of the ADA Infection Control Committee since 1998 and has served as its chair for a total of 8 years, across 2 terms. He has contributed to various protocols, guidelines and checklists for infection control used in Australia and represented dentistry on 4 committees of Standards Australia and on panels of the Communicable Diseases Network of Australia and of the Australian Commission on Safety and Quality in Health Care.
REGISTRATION
n On-Demand access to 29 Online Learning Videos (Over 8 hours of education).
n Watch and re-watch at your leisure 24/7
n Digital Online Learning Companion.
n Digital Suggested Reading Material.
n Online Questionnaire to earn 8 Hours of CPD.
Oral Hygiene Abstracts 2025
By Emer. Prof. Laurence Walsh AO
Masks and PFRs for the public have limited performance
Source control refers to the use of a face-worn product that covers a person’s mouth and nose to reduce the spread of large respiratory droplets to others when the person talks, sneezes or coughs. Members of the general public wear masks of various types to provide source control and reduce the spread of viral particles through airborne transmission. Masks sold to the public often do not meet any standards, raising concerns about their effectiveness in reducing the spread of respiratory viruses. Most cloth masks, whether homemade or those existing in the market, have not been evaluated to determine how well they perform. To assess the effectiveness of face-worn products used for source control, this study assessed the total outward leakage (TOL) for products from 9 categories to determine how much products reduced the leakage of exhaled aerosol. This was calculated by dividing the concentration outside the face-worn product by the concentration inside the face-worn product. The TOL accounts for leakage around the edges and through the filter material (i.e., penetration). Testing used a benchtop system with 2 different-sized headforms with silicone elastomer skin. Each unit was donned 5 times per headform. TOL varied from 10% to 58% and was significantly affected by both product category and head form size. TOL was greater for the medium headform than the large headform. Overall, single-layer cloth masks were the least effective measure for source control, with the highest TOL. Medical level 2-compliant 3-layer masks had a lower mean TOL of 16.4%, while level 1 masks 27.4% to 35.4%, due to poorer fit on the headform, thus indicating the importance of fit. Overall, these data suggest that 3-layer disposable level 2 face masks would be preferred for source control for the public. Single-layer cloth masks should be selected with caution as a source control measure for reducing airborne transmission of virus-laden aerosols, given the high total TOL observed in this study.
Yang W et al. Total outward leakage of face-worn products used by the general public for source control. American Journal of Infection Control 2025;53:239-244.
Check your own respirator fit using near infrared light
The need for effective respiratory protection in health care settings is paramount, particularly in light of the ongoing challenges posed by airborne pathogens. N95/P2 particulate filtering respirators (PFRs) are widely used to protect health care workers from infectious aerosols. The fit of PFRs and half-face respirators is critical. Fit-testing is done so that individual health care workers can achieve the required protection factor (PF). PF 10 is desired, which means a 10-fold reduction in the dose of pathogen respired (inside the respirator) compared with the environment. At present, no objective ways exist to evaluate the implementation of respirators at the point of use. Previously, it was shown that 26% of health care workers achieve appropriate fit at point of use. This study developed a prototype infrared (IR) kiosk that can be deployed in the health care setting to increase the efficacy of fitchecking. The kiosk is intended to be used as a visual aid with real-time feedback on areas of air leak and if leaks are present, guide the user where they may need to adjust their respirator. A total of 657 quantitative fits were conducted on 166 subjects using 4 different respirator styles (cup style, tri-fold, flat-fold and duckbill style). Randomisation was performed, with controls employing a standard “fit-check” and the intervention group using the infrared video kiosk. In the latter group, participants had 1 minute to use the IR kiosk to detect and adjust for thermal gradient leaks. The kiosk provided real-time visual feedback, highlighting areas where the respirator might be leaking. Participants could adjust their respirators based on this feedback before undergoing the fit test. The primary outcome was passing rates of quantitative fit, with secondary outcomes of respirator type, gender, ethnicity and previous experience. In the kiosk group, there was a significantly higher pass rate (50.6%) compared with controls (30.8%), with an odds ratio for passing of 2.3 (95% confidence intervals [CI] 1.8-2.9, P < .001). The duckbill style improved the greatest (OR 4.1, 95% CI 2.1-7.9, P < .001), and Tri-fold also showing substantial benefit (OR 2.66, 95% CI 1.4-5.2, P < .001). Gender and ethnicity did not influence outcomes when using the kiosk, nor did previous experience. Thus, the point-of-use kiosk improved the odds of achieving a satisfactory fit of common respirator styles, independent of participant demographics. This approach could address a gap in PFR use by providing individual assessment and interventions that improve worker safety.
Chapman D et al. Evaluation of a point-of-use kiosk for improving the fit of N95/P2 respirators in health care settings: A randomized controlled trial. American Journal of Infection Control 2025;53:36-43.
Ozonated water applications in infection prevention and control – a 2025 update
By Emeritus Professor Laurence J. Walsh AO
With improvements in the technology for generating ozonated water, the potential applications of this technology continue to expand. This article is an update to a 2021 comprehensive review of the applications of ozonated water,1 with particular emphasis on applications related to infection prevention and control in the area of prosthodontics.
OBack to basics
zone dissolved into water has been used for many years in various fields of dentistry due to its well-known antimicrobial effects and high biocompatibility. Ozonated water is highly effective in killing both Gram positive and Gram negative bacteria, working more quickly on the latter than the former.1,2 The reason for this difference relates to variations in cell wall, which then affect the sensitivity of different species of bacteria to oxidising agents. A Gram-positive cell wall is thicker and provides greater resistance.
The antibacterial action of ozone occurs through oxidation of glycoproteins, glycolipids, amino acids and other components of the cell membrane, resulting in increased membrane permeability, leakage of cell contents, damage to intracellular components and eventually microbial lysis.3,4
The rapid timeframe within which cell membrane damage occurs to bacteria means that ozonated water works more quickly than biocides and disinfectants that need to penetrate into the bacterial cell cytoplasm. A further advantage of the pattern of membrane attack to bacteria is that this type of action cannot lead to the development of resistance by bacteria. This is because ozone attacks multiple types of molecules and inhibits numerous enzymatic pathways and control systems of bacteria.
When ozone is dissolved into water, the powerful oxidising actions of the solution also make it effective against other forms of pathogens beyond bacteria, including viruses and protozoa. It is also effective against fungi, fungal spores and bacterial spores. Of the various species of fungi that can be found within the normal oral mycobiome, isolated water is highly effective against Candida species, including C. albicans, C. krusei and C. tropicalis 5
The wide antimicrobial spectrum of ozonated water explains the breadth of its documented applications in dentistry, which range from the treatment of caries, through to its use as an irrigant in root canal treatment and for periodontal pockets,6-11 and its use for treating dental unit waterlines.1,12,13
An important trend over the past two decades has been a greater emphasis in research on the applications of ozonated water as opposed to gaseous ozone. There are several reasons behind the shift including lower cost and greater convenience, including the development of compact handheld battery-powered devices for generating ozonated water on demand. Adding to these obvious practical benefits, dissolving ozone into water lowers the potential for oxidative injury to human tissues, while still maintaining the antimicrobial actions. Ozonated water has been used as a mouthwash, in both children and adults.14 It is not toxic for use and no negative gastrointestinal effects have been found from its accidental or deliberate ingestion.15 Cell culture studies have revealed that minor and reversible dose-related changes can occur on keratinocytes and fibroblasts of the gingival tissue, but that prolonged exposure times are needed for significant changes to occur. Moreover, all changes seen were reversible after 48 hours.16 This underscores its high biocompatibility. Indeed, of the available biocides and disinfectants, ozonated water is considered one of the safest for direct contact with the tissues of humans.17
One of the most important limitations of ozonated water is its short half-life. Under normal room temperature conditions, the half-life of ozonated water is only about 20 minutes, after which time the dissolved ozone will degrades back into normal diatomic oxygen. This is why ozonated water must be used within the first 5-10 minutes after being produced.18
There is a considerable body of research being undertaken internationally to extend the applications of ozonated water. A comprehensive review undertaken in 2021 of major patent databases identified a total of 620 individual patents and 134 patent families.17 South Korea and United States were the countries of origin for the largest number of patent applications, with a total of 103 and 91 applications, respectively.
infection | CONTROL
Figure 1. The Hydrozone Health Ozone Rinse Tumbler generates ozonated water in 90 seconds and is ideal for mouth rinsing, impression disinfection and other applications including surface cleaning using the built-in spray feature.
Some of the more notable applications that are documented for ozonated water include as a sanitising material to be used as a component of hand hygiene. The strong actions of ozone on enteric bacteria and enteric viruses,19-21 as well as respiratory viruses22 underpin such clinical applications. Several clinical studies conducted in Japan and Sweden have shown strong performance for ozonated water when used for hand hygiene, especially for individuals with severe forms of dermatitis who are unable to tolerate alcohol-based products.23,24 At the present time, the National Hand Hygiene Initiative in Australia does not include the use of ozonated water as a substitute for the existing TGAlisted alcohol-based hand gel products with proven antimicrobial activity. This gap does not prevent in any way the use of ozonated water for physical handwashing and a number of dental practices have installed taps for physical handwashing with ozonated water.
infection | CONTROL
Using gaseous ozone to decontaminate impressions
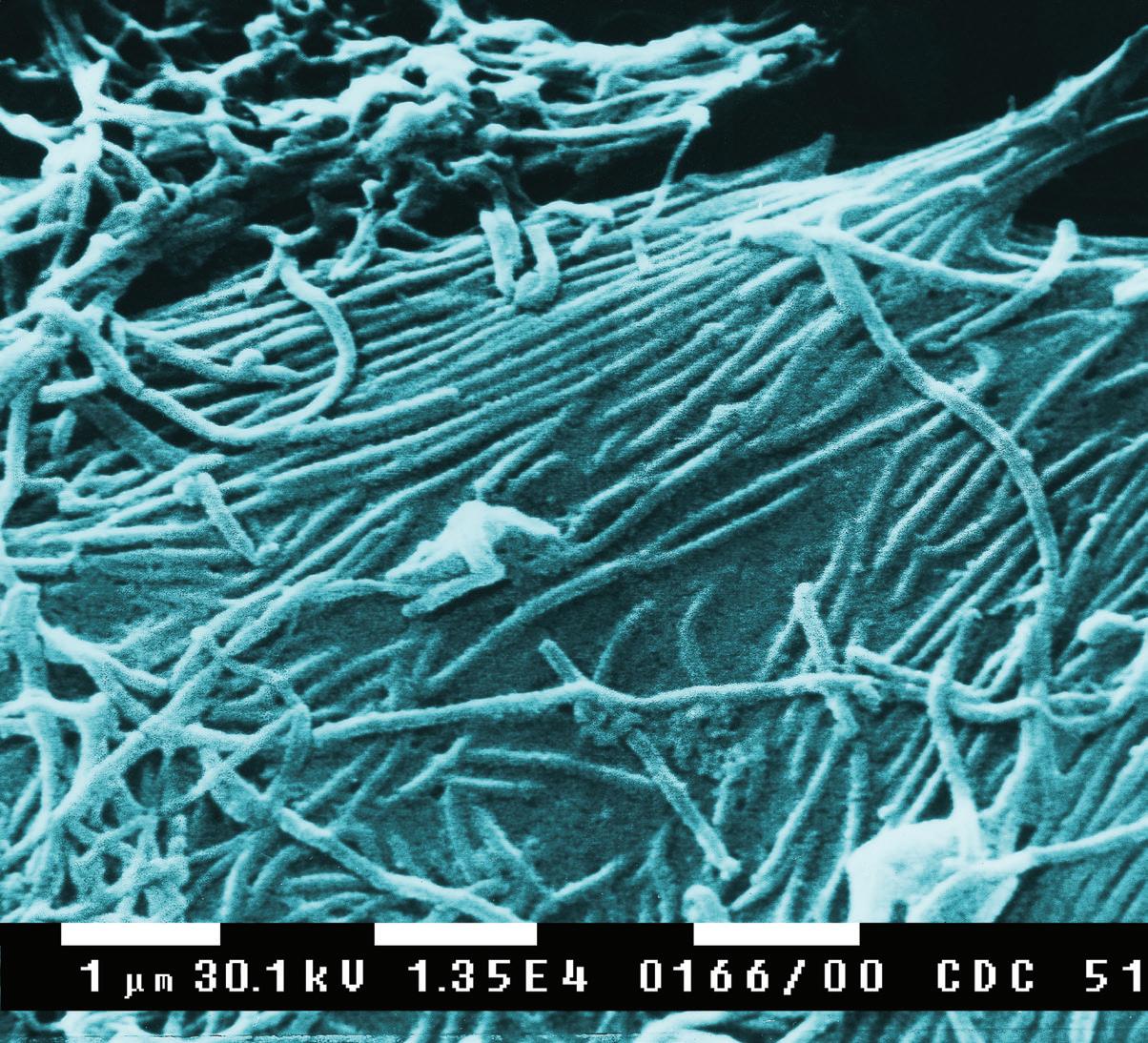
An important responsibility of clinicians is to prevent contamination spreading from the patient treatment area to other parts of the practice and to external locations. Regardless of whether the clinic has its own laboratory or whether items are being sent to an external laboratory, the responsibility of limiting the spread of contamination remains nonetheless. A typical patient will have in their oral microflora about 280 bacterial species and numerous species of fungi. A 1 mL volume of the resting saliva from a healthy patient with good oral hygiene contains approximately 750 million microorganisms.25 A dental impression will pick up around 1 mL of saliva. This reinforces the need for appropriate decontamination of impressions before they are poured up or scanned.
Microbiological studies of impressions have shown that the most common species of microbes present are Streptococcus, Staphylococcus, Actinomyces and Candida, 26 all of can be readily transferred through to the dental laboratory when decontamination procedures are inadequate.27-29 Organisms transferred on impressions can then contaminate study models and working models.30
Typical procedures for impression decontamination include vigorous rinsing under running water followed by the application of a detergent and further rinsing. Based on assessment of risk, many clinicians choose to use a disinfection solution as a further step in the protocol. This can lead to issues since the antimicrobial agents that are present may alter the impression and reduce the surface quality of the resulting cast or scan. Hence, it is critical to consider the extent to which ozone may influence impression materials, when compared to other commonly used agents such as sodium hypochlorite (NaOCl).
Several studies have examined the use of gaseous ozone for the disinfection of elastomeric impression materials, including
condensation silicones and addition silicones of various consistency (e.g. Panasil putty, medium and light). The typical approach used is to measure the reductions of Pseudomonas aeruginosa, Staphylococcus aureus and Candida albicans by counting colony-forming units (CFU) on the surface of treated samples.
One study of this type undertook ozonation for 10 minutes (15 ppm, at an ozone flow rate of 800 mg/hour in a box with a volume of 8 L). This approach gave a 6-log reduction in S. aureus, P. aeruginosa and C. albicans 32 A second study using gaseous ozone reported reductions in Escherichia coli, S. aureus, P. aeruginosa and Enterococcus faecalis on the surface of addition silicone impression materials and noted a positive effect on the wettability of the material.33 Similar positive results were seen in a third study which used an exposure time of 5 minutes.34
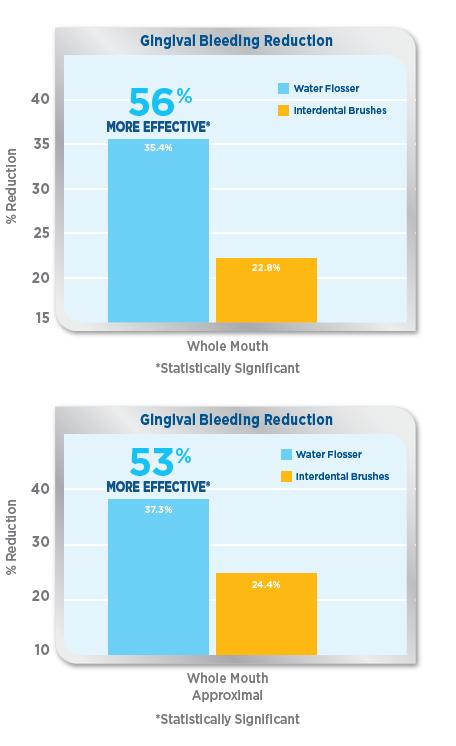
A potential concern with all types of disinfecting agents is that there may be subtle changes on the impression surface. With the elastomeric materials, the polymers can degrade through a polymer chain scission process, during which oligomers and finally monomers are formed, which then leave the polymer.35 This issue has been well described for NaOCl, when used at a tenfold dilution (i.e. 0.525% final concentration) on vinyl polysiloxane impressions. This causes surface degradation with emergence of silica crystals on the surface. Unlike NaOCl, a 5-minute exposure to gaseous ozone (10 mins at 4L/min with ozone production of 2.61 g/h) does not cause significant or visible surface degradation. This means that, when compared with common disinfectants, ozone treatment of impressions is more likely to lead to highly accurate prosthetic restorations. Careful inspection of the ozoneexposed impression surface using scanning electron microscopy has revealed subtle wavy-wrinkling surface structures. These result from surface oxidation and the subsequent formation of a stiff silicon dioxide film.36-38 Despite these minor changes to the surface, the utility of the impression is not impaired significantly.39
Figure 2. The Hydrozone Health Ozone Rinse Tumbler generates ozonated water in 90 seconds.
Figure 3. The Kona Infection Control (KIC) Tap ozonates tap water on on-demand basis.
infection | CONTROL
Figures 4-5. Ozonated water is an ideal pre-procedural mouth rinse particularly before implant or periodontal treatments.
Using ozonated water to decontaminate impressions
Several studies have demonstrated the usefulness of ozonated water for impression decontamination, for both irreversible hydrocolloid materials,40 as well as for elastomeric materials, including PVS, vinyl polyethers, addition silicones and condensation silicones in light body, medium body or putty variants.40-43 Ozonated water caused comparatively less changes to the surface than the reference materials of 0.5% NaOCl and 2% glutaraldehyde, making it a desired alternative as it was better able to preserve surface detail, whilst still being highly effective at reducing the load of microorganisms present. Of note, one study showed that treatment with ozonated water had no effect on the wettability and hydrophilicity of the surface. This was in contrast to NaOCl, which caused a reduction in surface wettability.43
Disinfection of contaminated stone casts
Inadequate impression decontamination can lead to the persistence of microorganisms from the patient which then survive on the surface of the study model or working model.44 Inactivating these microorganisms without damaging the surface of the cast is a significant challenge. Most agents that have been used to disinfect dental casts, including NaOCl, increase the surface roughness of the cast.45 On the other hand, ozonated water does not adversely affect the surface roughness or its topography at the microscopic scale. In addition, there is no chemical reaction between the calcium sulphate of the cast and the ozone in the water, meaning that the presence of gypsum does not accelerate the decomposition of the ozone that has dissolved. Hence, ozonated water can be used to disinfect dental stone casts.45
Disinfection of toothbrushes and dental prostheses
The rapid antimicrobial action of ozone dissolved in water makes it suitable for use for situations where a rapid sanitising action is required. This includes treating toothbrushes to prevent overgrowth of normal oral microflora46 and disinfecting removable appliances and dentures.47-50 An important advantage of this approach is that it does not cause corrosion, unlike NaOCl. Microorganisms that may be found on dentures, including Streptococcus spp., C. albicans and S. aureus, are readily inactivated by ozonated water.
Conclusions
This article has updated and extended the information summarised in the earlier 2021 review.1 It is clear from the information presented that there are a number of useful applications for water in everyday clinical practice, particularly for procedures involving impressions, appliances and prostheses, where there is a need for rapid and effective decontamination without the risks of corrosion to any metallic components which may be present. The availability of modern handheld ozonated water devices can assist in improving infection prevention and control, by limiting the spread of contamination from the patient’s mouth and the chair side to the dental laboratory. Ozonated water also provides a convenient solution to the challenge of a working castle study model that has become contaminated, and can augment physical handwashing when used as a final step after ordinary tap water.
References
1. Walsh LJ. Ozone in water: let the recent evidence speak. Australas Dent Pract. 2021;31(4):86-90.
2. Bialoszewski D, Bocian E, Bukowska B, et al. Antimicrobial activity of ozonated water. Med Sci Monit. 2010;16:MT71-MT75.
3. Nagayoshi M, Fukuizumi T, Kitamura C, et al. Efficacy of ozone on survival and permeability of oral microorganisms. Oral Microbiol Immunol 2004;19:240 246.
4. Almaz ME, Sönmez IS. Ozone therapy in the management and prevention of caries. J Formos Med Assoc. 2015;114:3-11.
5. Naito S, Shiga I. Microbiocidal properties of ozone on various microorganisms suspended in water. J Jpn Soc Food Sci Technol. 1982;29(1):1-10.
6. Azarpazhooh A, Limeback H. The application of ozone in dentistry: A systematic review of literature. J Dent. 2008;36:104 116.
7. Gopalakrishnan S, Parthiban S. Ozone – A new revolution in dentistry. J Bio Innov. 2012;1:58-69.
8. Case PD, George R, Bird PS, Walsh LJ. Treatment of root canal biofilms of Enterococcus faecalis with ozone gas and passive ultrasound activation. J Endod. 2012;38(4):523-526.
9. Hubbezoglu I, Zan R, Tunc T, et al. Antifungal efficacy of aqueous and gaseous ozone in root canals infected by Candida albicans. Jundishapur J Microbiol. 2013;6:1–3.
10. Goztas Z, Onat H, Tosun G, et al. Antimicrobial effect of ozonated water, sodium hypochlorite and chlorhexidine gluconate in primary molar root canals. Eur J Dent. 2014;8:469-474.
11. Giuroiu CL, Andrian S, Stoleriu S, et al. The combination of diode laser and ozonated water in the treatment of complicated pulp gangrene. Appl Sci. 2020;10:4203.
12. Walsh LJ. Disinfection of dental unit water with ozone. Australas Dent Pract. 2006;17(3):68-70.
13. Walsh LJ. Electrolytic ozonation of water: a new solution to the problem of dental unit waterline biofilms. Australas Dent Pract. 2011;22(1): 114-116.
14. D’Amario M, Di Carlo M, Natale SM, et al. Application of ozone therapy in paediatric dentistry. Appl. Sci. 2022;12:11100.
15. Durgapal S, Shetty M. Effectiveness of ozone against common dental problems: a literature review. J. Clin. Diagnostic Res. 2022;16:14-19.
16. Floare AD, Scurtu AD, Balean OI, et al. The biological effects of ozone gas on soft and hard dental tissues and the impact on human gingival fibroblasts and gingival keratinocytes. Processes 2021;9:1978.
17. Mascarenhas LAB, Oliveira FO, da Silva ES, et al. Technological advances in ozone and ozonized water spray disinfection devices. Appl Sci. 2021;11:3081.
18. Gupta S, Deepa D. Applications of ozone therapy in dentistry. J Oral Res Rev. 2016;8:86.
19. Shin GA, Sobsey MD. Reduction of Norwalk virus, poliovirus 1, and bacteriophage MS2 by ozone disinfection of water. Appl Environ Microbiol. 2003;69:3975-3978.
20. Suchomel M, Lenhardt A, Kampf G, Grisold A. Enterococcus hirae, Enterococcus faecium and Enterococcus faecalis show different sensitivities to typical biocidal agents used for disinfection. J Hosp Infect. 2019;103:435-440.
21. Walsh LJ. Handling the challenges of Norovirus and C. difficile infection. Australas Dent Pract. 2020;31(1):106-108.
22. Jia-min Z, Chong-yi Z, Geng-fu X, et al. Examination of the efficacy of ozone solution disinfectant in inactivating SARS virus. Chin J Disinfect. 2004;21:27-28.
23. Nakamura K, Saito K, Kashiwazaki J, et al. Evaluation of ozonated water using ASTM E1174 for standardized testing of handwash formulations for healthcare personnel. J Hosp Infect. 2018;100: 211-213.
24. Breidablik HJ, Lysebo DE, Johannessen L, et al. Ozonized water as an alternative to alcohol-based hand disinfection. J Hosp Infect. 2019;102:419-424.
25. Mantena SR, Mohd I, Sajjan S, Ramaraju A. Disinfection of impression materials: a comprehensive review of disinfection. Int J Dent Mater. 2019;1:7-16.
26. Egusa H, Abe K. Clinical evaluation of the efficacy of removing microorganisms to disinfect patient-derived dental impressions. J Prosthet Dent. 2009;102:56.
27. Powell GL, Runnells RD, Saxon BA, Whisenant BK. The presence and identification of organisms transmitted to dental laboratories. J Prosthet Dent. 1990;64:235-237.
28. Samaranayake LP, Hunjan M, Jennings KJ. Carriage of oral flora on irreversible hydrocolloid and elastomeric impression materials. J Prosthet Dent. 1991;65:244 249.
29. Rice CD, Dykstra MA, Gier RE, Cobb CM. Microbial contamination in four brands of irreversible hydrocolloid impression materials. J Prosthet Dent. 1991;65:419 423.
30. Mitchell DL, Hariri NM, Duncanson MG, et al. Quantitative study of bacterial colonization of dental casts. J Prosthet Dent. 1997;78:518 521.
31. Amin WM, Al Ali MH, Al Tarawneh SK, et al. The effects of disinfectants on dimensional accuracy and surface quality of impression materials and gypsum casts. J Clin Med Res. 2009;1:81 89.
32. Wezgowiec J, Wieczynska A, Wieckiewicz M, et al. Evaluation of antimicrobial efficacy of UVC radiation, gaseous ozone, and liquid chemicals used for disinfection of silicone dental impression materials. Materials 2022;15:2553.
33. Celebi H, Büyükerkmen EB, Torlak E. Disinfection of polyvinyl siloxane impression material by gaseous ozone. J Prosthet Dent. 2018;120:138-143.
34. Poulis N, Kyriacou A, Kotsou M, Bezirtzoglou E, Prombonas A, Drakoulis N. Effectiveness of low-flow high-ozone concentration disinfection of dental impressions: A comparative study to immersion disinfection. Br J Appl Sci Technol. 2014;4:2528-2537.
35. Evensen HT, Jiang H, Gotrik KW, et al. Transformations in wrinkle patterns: Cooperation between nanoscale cross-linked surface layers and the submicrometer bulk in wafer-spun, plasma-treated polydimethylsiloxane. Nano Lett. 2009;9:2884-2890.
36. Hillborg H, Karlsson S, Gedde UW. Characterisation of low molar mass siloxanes extracted from crosslinked polydimethylsiloxanes exposed to corona discharges. Polymers 2001;42:8883-8889.
37. Efimenco K, Wallace WE, Genzer J. Surface modification of Sylgard-184 Poly (dimethyl siloxane) networks by ultraviolet and ultraviolet/ozone treatment. J Colloid Interface Sci. 2002;254:306-315.
38. Zhu Y, Otsubo M, Honda C. Degradation of polymeric materials exposed to corona discharges. Polym Test. 2006;25:313-317.
39. Poulis N, Prombonas A, Yannikakis S, et al. Preliminary SEM observations on the surface of elastomeric impression materials after immersion or ozone disinfection. J Clin Diagnost Res. 2016;10 (12):ZC01-ZC05.
40. Savabi O, Nejatidanesh F, Bagheri KP, et al. Prevention of cross-contamination risk by disinfection of irreversible hydrocolloid impression material with ozonated water. Int J Prev Med. 2018;9:37.
41. Abinaya K, Muthu Kumar B, Ahila S. Evaluation of surface quality of silicone impression materials after disinfection with ozone water: an in vitro study. Contemp Clin Dent. 2018;9(1):60-64.
42. Shankar K, Dandekeri S, Shetty R, et al. Comparative evaluation of ozone water and glutaraldehyde on surface detail reproduction of vinyl polyether silicone impression materials at different time intervals. J Pharm Bioallied Sci. 2024;16(Suppl 4):S3837-S3839.
43. Fulsundar PD, More V, Bhadekar R, Bhola J. Comparative evaluation of ozonated water and 0.5% sodium hypochlorite for their effect of disinfection and surface wettability on polyvinyl siloxane impression material. World J Dent. 2022;10:5005.
44. Ivanovski S, Savage NW, Brockhurst PJ, Bird PS. Disinfection of dental stone casts: antimicrobial effects and physical property alterations. Dent Mater. 1995;11:19-23.
45. Nishikori R, Sawajiri M, Okuda T, et al. Effect of ozonated water on the surface roughness of dental stone casts. Dent Mat J. 2018;37(5):740-745.
46. Bezirtzoglou E, Cretoiu SM, Moldoveanu M, et al. A quantitative approach to the effectiveness of ozone against microbiota organisms colonizing toothbrushes. J Dent. 2008;36:600-605.
47. Murakami H, Sakuma S, Nakamura K, Ito Y, Hattori M, Asai A, et al. Disinfection of removable dentures using ozone. Dent Mater J. 1996;15:220 225.
48. Arita M, Nagayoshi M, Fukuizumi T, et al. Microbicidal efficacy of ozonated water against Candida albicans adhering to acrylic denture plates. Oral Microbiol Immunol 2005;20: 206-210.
49. Murakami H, Sakuma S, Nakamura K, et al. Disinfection of removable dentures using ozone. Dent Mater J. 1996;15:220 225.
50. Murakami H, Mizuguchi M, Hattori M, et al. Effect of denture cleaner using ozone against methicillin resistant Staphylococcus aureus and E. coli T1 phage. Dent Mater J. 2002;21:53 60.
About the author
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology.
Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 400 journal papers, with a citation count of over 20,000 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
Simply fill with tap water and turn it on
Ozonated water on-demand in 90 seconds
Ideal for...
Mouth rinsing prior to invasive treatments
Hand washing
Waterline disinfection
Surface disinfection
Impression disinfection
Rinsing of dentures, splints & appliances
Ozone Tumbler with Sprayer
When ozone is dissolved into water, the powerful oxidising actions of the solution make it effective against pathogens including bacteria, viruses, protozoa, fungi, fungal spores and bacterial spores.
The Aqueous Ozone Tumbler with built-in sprayer...
Generates up to 300ml of ozonated water - Dimensions 220mm x ø 60mm
Rechargeable (USB-C)
3 settings - 1ppm for oral rinsing (90 seconds)
2ppm for oral appliances (180 seconds)
3ppm for surface spraying (270 seconds)
Risk of sharps...
Steps to take to avoid injuries from needlesticks
By Olivia Wann, RDA, JD
According to the World Health Organisation, there are two million injuries from needlesticks and other sharp objects to the world’s 35 million healthcare workers every year. In Australia, it has been estimated there are 18,000 reports of needle and sharps injuries to healthcare workers annually. But because approximately half of all injuries are not reported, this means the actual number of injuries could double that figure.
The most common infections occupationally transmitted via sharps injuries during patient care include hepatitis B, hepatitis C and HIV. The US Centers for Disease Control and Prevention (CDC) also notes that the risk includes herpes, malaria and tuberculosis.
I founded Modern Practice Solutions in 2000, a compliance firm specialising in dental practices. Therefore, having been a dental employee, a consultant and now a lawyer, I understand the perspectives both of the dental worker and their employer and the challenges they each face in their day-to-day operations, including the issue of safety. Our company analyses workflow, audits documentation and conducts hazard assessments.
We work with dental practices throughout the USA and we’ve met hygienists and assistants who tell us that they’ve experienced needlesticks and sharps injuries and unfortunately, they did not have a protocol in place to ensure proper follow-up as required by law. Some workers fear that an injury imputes poor work performance. Others fear the practice might incur an unnecessary expense.
Recently, the US Department of Labor filed suit against a dentist in Massachusetts. The suit alleges the dentist fired an employee for filing a health hazard complaint. According to the complaint filed in the U.S. District Court in Boston, the dentist discharged a dental assistant in November 2010 after the employee expressed concerns about a practice procedure that required employees to remove protective caps from contaminated needles prior to disposal. The lawsuit seeks the employee’s reinstatement and payment of lost wages, benefits, interest and compensatory and punitive damages.
An inspection resulted in the dentist being cited for eight alleged serious violations. The dentist contested those citations and the accompanying $26,400 in proposed fines to the independent Occupational Safety and Health Review Commission. Employers feel the impact of costs related to post-exposure management of health-care personnel ranging from $500 to $3,000 per incident.
Our goal as consultants is to promote safety. Remember, safety is not optional. Training, policy development, safer medical devices and engineering controls are important components in compliance. According to the US Organization for Safety, Asepsis and Prevention (OSAP), the application of four basic principles of infection control guides workers and patients in staying safe. These include:
• Take action to stay healthy;
• Avoid contact with blood and fluids;
• Limit the spread of blood and body fluid contamination; and
• Make objects safe for use.
In analysing the workplace, practices can easily achieve improvements by using an instrument cassette system such as IMS (Instrument Management System) by HuFriedy. Whether the practice is struggling with space or trying to achieve greater organisation and better time management, practices benefit from the system.
Beyond these benefits, practices promote safety by using cassettes. Injury to workers is significantly minimised when instrument handling is reduced. After use, the contaminated instruments are returned to the cassette and locked into place for transport to the instrument processing area. The cassette is then automatically cleaned in an ultrasonic cleaner or washer/disinfector, followed by drying, wrapping and steam sterilisation, all without removing instruments from the cassette. There is no more time consuming sorting into pouches or pulling sterile individual pouches to prep a tray.
Dental practices can minimise the risk of sharps injuries by avoiding the following safety hazards:
• Not having the proper procedures in place, including step-by-step instrument management and instrument processing protocols;
• Working in a high volume dental setting with insufficient time allotted for treatment room turnaround;
• Transporting loose instruments and sharps on trays through the office and risking bumping into another worker or patient. This is very dangerous and could lead to a sharps injury that could have been prevented through the use of cassettes. According to the US CDC, collision with a worker or a sharp represents 10% of the circumstances associated with needlestick injuries;
• Handling contaminated loose instruments with patient exam gloves in the sterilisation area rather than with heavy duty, utility gloves; and
• Improperly retrieving instruments and patient care items with contaminated gloved hands in cabinets and drawers. This is a common occurrence because many times there are necessary instruments missing from the tray and the assistant must get up during a procedure to retrieve them.
In analysing the investment versus the expense, IMS actually saves money through time management. Valuable clinical staff time is best devoted to patient care and infection control rather than sorting instruments into set-ups. Additionally, practices save money by preventing breakage of the instrument tips and loss of instruments as the cassette secures the instruments in place.
We interviewed a few practices that use IMS to get their input on how the cassettes integrate into their instrument processing and management program.
Olivia: Dr Cannon Doan of Family Dentistry in Cordova, Tennessee. Dr Doan, how long have you been using Hu-Friedy’s Instrument Management System?
Dr Doan: We’ve used the system since 1997. Implementing cassettes into our practice gave us the opportunity to keep up with the latest infection control and safety standards.
Olivia: What are your favourite features of the cassettes?
Dr Doan: There are many. We love the consistency of instrument set-up for each procedure type. We’ve observed fewer injuries caused by instrument sticks during instrument processing. Overall, the efficiencies gained in the central sterilisation area from using IMS leaves more time for the staff to spend with patients, which contributes to the practice’s quality of care and profitability.
Olivia: Dr Mao is a dentist in Springfield, Tennessee. Dr Mao and I discussed space issues in her central sterilisation area. She converted a house into a dental practice that features a beautiful reception area and spacious treatment rooms. We talked about the space issues of the small sterilisation area. Following an annual OSHA training, Dr Mao, the staff and I agreed that incorporating IMS would overcome the challenges of working in a small space. Three years later, they all agree it was a great decision. Dr Mao, what do you like best about Hu-Friedy IMS?
Dr Mao: The organisation! It totally makes sense to use the cassettes to save time and maximise space. Our sterilisation area is very small; therefore organisation is key. Cassettes have eliminated
infection | CONTROL
the need to search through cabinets and drawers for instruments, which is very time consuming. From a safety perspective, we’re pleased to report a reduction in sharps injuries and potential cross contamination. The system gives me confidence that I’m doing everything I can to make the assistants’ and hygienists’ jobs easier and safer. In addition, our patients have an improved practice perception and sense of security knowing that the instruments are always organised and have been cleaned, packaged and sterilised.
Olivia: Dr John Stritikus is a paediatric dentist and co-owner of Dickson Pediatrics and Brentwood Pediatrics in Tennessee. How have the cassettes helped the efficiency of your practice?
Dr Stritikus: All instruments needed for a procedure are included in the cassette, sterilised and accessible. Less time is needed to set up for a procedure, which helps increase production, especially in our high-volume paediatric practice.
Olivia: Do you feel like parents notice?
Dr Stritikus: Anyone, parent or otherwise, can see that all cassettes are wrapped and marked with sterilisation tape to ensure safety. This safety component is a big part of our philosophy.
Olivia: Please elaborate on safety for your employees.
Dr Stritikus: All instruments are held within the cassette, which decreases the chances of injuries when handling instruments. It also helps ensure proper handling. Even in the worst case scenario, if the cassette is dropped, the instruments are still contained in the locked cassette.
Olivia: Can you compare using cassettes to not using cassettes?
Dr Stritikus: The initial cost was recouped through less time spent sorting instruments or workplace injuries; fewer
instruments have been replaced due to breakage compared to before using IMS; fewer mirror heads are scratched; we’re more likely to have the instruments we need in the set-up; the system is very simple to learn and new employees grasp the system from day one.
In summary, when implementing cassettes such as Hu-Friedy’s IMS, your practice can save time, money and best of all, promote safety among your clinical team members. Here are some timely reminders to close the gap in your practice’s safety program and minimise the risk of sharps injuries:
• Provide annual training for all your staff on correct infection control and safety procedures;
• Carefully review your sharps injury prevention program and have protocols in place if an injury occurs;
• Implement a post-exposure management plan and carefully review the protocol with your staff.
• Ensure that medical records for employees are current, including documentation on hepatitis B vaccine status, post-exposure reports and related documentation. Safety training does not have to be boring. Include the input from each team member whose perspective may provide valuable insight to the practice’s safety program. Remember to promote safety, day-to-day, to ensure you and your staff have long, healthy careers in dentistry.
Editor’s notes
This article was reprinted with permission from RDH Magazine. References to organisations such as the US Centers for Disease Control and Prevention (CDC), US Department of Labor and the Organization for Safety, Asepsis and Prevention (OSAP) have been retained for reader interest but have no regulatory influence in Australia or New Zealand.
About the author
Olivia Wann attended Tennessee Technology Center as an RDA and earned a bachelor of science degree in health-care administration from Saint Joseph’s College. She graduated from the Nashville School of Law with a doctorate in jurisprudence and is licensed to practice law in Tennessee. In 2000, she founded Modern Practice Solutions, which is dedicated to the compliance issues of dental practices.
Mastication – the threefold implications of chewing well for long enough
By Emeritus Professor Laurence J. Walsh AO
In clinical practice, we often have discussions with patients about their occlusal function and the need to ensure sufficient opposing pairs of natural teeth, or their relevant prosthetic replacements. We assume that patients understand the importance of proper chewing for effective eating.
Within dentistry, there is not a broad understanding of the benefits of chewing activities beyond the obvious connection to the mastication of food. The purpose of this article is to summarise recent concepts on the importance of chewing,
beginning with its obvious purpose in mastication and nutrition, then moving on to discuss the impact of chewing on appetite and finally, the impact of chewing on cerebral blood flow and the development of dementia.
Chewing food – using more cycles
Performing more chewing cycles before swallowing can provide a number of benefits. Using a greater number of chewing cycles helps to break the physical substrate of the food down further, enhancing subsequent digestion by facilitating the release of nutrients.1,2 This occurs because mastication increases the surface area to volume ratio of the food. It also reduces the maximum dimensions of the food and thus aids swallowing.
Variables such as the amount taken in one bite, the number of chews per bite and the rate of stimulated saliva production all influence the extent to which a food bolus is deformed, fragmented and lubricated with saliva during mastication. With longer chewing, the extended exposure to salivary amylase enzymes allows for greater breakdown of complex starches into simple carbohydrates, thus aiding digestion.
Longer chewing cycles and appetite suppression
Each individual has habitual masticatory processes and there are also inter-individual variations in bite force. Both the normal number of chewing cycles and the bite force applied can vary by a twofold range between different adults.3 Using more chewing cycles slows the pace of eating and provides more satisfaction from eating and a greater sense of satiety. As a result, less food is required to gain the same sense of fullness at mealtimes. This strategy reduces the intake of energy and so will aid in weight control and in the prevention of obesity. Following this logic, there is a compelling argument that extended mastication could be one simple strategy to reduce the risk of lifestyle-related diseases.3-5
At the end of a meal, the process that terminates eating is influenced by a range of feedback mechanisms and one of these is the duration of chewing. The literature shows a considerable influence of the number of chewing cycles on both the level of satisfaction with eating and the extent to which the sensation of hunger is suppressed. This leads to the conclusion that moderate chewing (e.g. 25 chewing cycles) is likely to be the most comfortable, with less than 10 cycles being insufficient and more than 40 chewing cycles being impractical.3-5 Eating at a slower rate with more chews per bite gives smaller particles to swallow, while eating at a faster rate is associated with larger bite sizes, a shorter mastication time and fewer chews per bite.5
As an example of these principles in action, chewing sugar-free gum increases the sensation of fullness and reduces the sensation of hunger and the desire to eat.3-5 Of note, this effect occurs even when the gum has no flavour, but the impact is enhanced when a suitably pleasant mint or fruit flavour is present in the gum. One explanation for this beneficial effect of chewing is that a greater number of chewing cycles is more likely to change the level of hormones, leading to increased levels of glucagon-like peptide (GLP-1) and insulin and suppressed levels of ghrelin.
Increased early insulin secretion is associated with better glucose absorption. The relationship between extended chewing and a stronger initial insulin response probably occurs because a longer chewing time extends the period for taste perception for the food. Ghrelin is the appetite hormone and is elevated in the blood between meals in the fasting state and then is reduced in response to food intake. Prolonged chewing suppresses the levels of ghrelin and thus reduces appetite.
As a simple, inexpensive and non-pharmacological approach, it seems difficult to argue against the benefits of using longer chewing cycles (Table 1). On the other hand, faster eating is often associated with poorer glucose tolerance and insulin responsiveness and an increased prevalence of metabolic syndrome.3-5
These types of beneficial relationships for prolonged chewing have been shown for chewing gum as well as for conventional foods such as pizza.3-5
For chewing gum, a period of chewing suppresses the return of hunger following a meal and reduces cravings for sweet and salty snacks between meals. For pizza, more chewing cycles can positively influence palatability. Of particular interest, prolonged chewing tends to dramatically reduce the intake of food in the parts of the meal which follow.
Some practical advice that follows from this is that patients could be advised to increase the number of chewing cycles for their food. The same advice could be given for sugar-free chewing gum, if they are using this. More chewing cycles per bite requires relatively little additional effort. Rather than counting individual chewing actions, it will be more practical to advise patients to chew each bite for 20 to 30 seconds before swallowing.
The advice on chewing must be tailor-made to the individual patient situation, since for some patients, implementing this as an approach may not be practical or appealing, e.g. because of a lack of suitable opposing teeth, mobile teeth, unstable prostheses, etc. As well, there can be considerable variations between one person in the next, since individuals have different expectations and habits around their eating practices. This means it is necessary to titrate in an individual patient the influence of chewing time when their end goal is to achieve a reduction in appetite or in food intake.
The variable of food texture
When giving advice about chewing for longer, one must take into account that the textures of different types of food can vary enormously. A ranking of foods by category is shown in Table 2, which incorporates descriptors from the International Dysphagia Diet Standardisation Initiative (IDDSI) Guidelines. The higher the category number, the greater the masticatory force and the number of chewing cycles that are required. Do not suggest to patients that they need to attempt to chew soup or other low viscosity or liquid foods. Softly textured foods require minimal chewing. On the other hand, foods with considerable hardness or a high viscosity have a microstructure which is more difficult to chew and this reduces the average bite size.1-3 Foods with thicker textures require longer processing in the mouth and this slows the eating rate. They also give higher than expected levels of fullness, meaning that the caloric intake is less overall. This is one of the obvious benefits of eating unprocessed fruit and raw vegetables.
On the other hand, foods which can be consumed very rapidly are associated with a greater overall intake of energy and consequently with adipose deposition and with higher body weight. Adding to this, individuals who eat very quickly not only consume more within a given meal, but they also tend to have greater consumption of snacks in the post meal period. They experience less of the sensation of fullness after the meal has finished.
The breakdown of food
Within the oral cavity, the food breakdown process is an interaction between time, the physical structure of the food and the degree of lubrication. Hence, foods with different characteristics have quite different breakdown dynamics. Foods that are physically large will take some time to chew to the point where the particles are below the threshold for size which is safe to swallow for that particular individual.
A further important consideration is that individuals vary greatly in terms of their ability to produce stimulated saliva when chewing. This causes variation in the number of cycles required. For hard foods with a low moisture content, those with very high production rates of stimulated saliva can reach the threshold where the food is suitable to swallow after a relatively small number of chewing cycles.
The reverse is true for those with salivary gland hypofunction who have a deficit in the production of stimulated saliva. The author refers to this as “Sao biscuit” test, where this particular hard dry biscuit is the challenge item that the patient must attempt to chew and then swallow, without taking any liquid.
Appetite suppression
One of the most interesting aspects of the literature on the topic of chewing is that forms of oral stimulation other than chewing can also lower the levels of ghrelin in the blood and suppress appetite.4-5
This effect has been explained in terms of vagal efferent nerve stimulation. It remains to be seen how such actions could be applied to practical protocols for oral stimulation that patients could perform themselves at home. Likewise, there could be an opportunity to alter the structure of chewing gum to enhance some of these effects on ghrelin.
An important limitation of the literature regarding the relationship between chewing cycles, appetite, food intake and hormone levels is that many studies have been done on individuals within the healthy weight range and relatively few studies have included individuals who are overweight.
A further issue is that it is not possible to have true blinding in such studies, as participants will be aware whether they have chewed or not, whether the gum is flavoured or not and how long they have chewed for.
A meta-analysis of the effect of chewing on self-reported hunger4 has identified that the longer the period of fasting, the greater the impact of prolonged chewing on satiety.
Enhanced salivary defences
As already mentioned, chewing is a powerful stimulus for the production of saliva from the major glands, particularly the parotid glands. As a consequence of this, as the flow increases and reabsorption of ions through the ductal structure of the saliva glands is altered, there is a dramatic elevation in the concentration of bicarbonate ions and therefore an increase in the pH. The pH can change from typically around 6.5 for saliva at rest, to 8.0-8.5 for stimulated saliva. This represents a 100-fold reduction in the concentration of hydrogen ions.
Stimulated saliva helps to create a favourable environment for remineralisation, since the isotherms which dictate the formation of various mineral species from calcium and phosphate ions are all driven to mineral formation under high pH (alkaline) conditions. Increased salivary flow also accelerates the clearance of substrates from the mouth and enhances the antimicrobial actions of saliva. These well-known benefits underpin the oral health benefits of chewing sugar-free gum.
Table 1. The rationale behind extended chewing
n Improved processing of food
n Smaller size and increased number and surface area of food bolus particles
n Extended contact with saliva
n Greater salivary amylase pre-digestion of starches
n Enhanced salivary clearance
n Enhanced initial insulin response
n Suppressed ghrelin levels, lowered appetite and decreased intake of food
n Increased glucagon-like peptide-1
n Increased satisfaction from eating
Table 2. A ranking for food texture according to the difficulty of mastication
0 Thin drinks (water, tea, coffee)
1 Slightly thick drinks (cream soup)
2 Mildly thick drinks (nectar)
3 Liquidised, moderately thick drinks or foods (honey)
4 Able to swallow without chewing; tines of a fork make a clear pattern on the surface; pureed foods and extremely thick drinks (purees, cooked cereals, mashed bananas, thick pudding)
5 Able to smash with the tongue; minced and moist foods; particles easily come through the tines of a fork (meat loaf, baked beans, casseroles)
6 Able to smash with edentulous ridges; soft and bite-sized foods; can be broken down with pressure from a fork (cheese, pizza, bagels)
7 Regular foods that are able to be chewed easily; can be broken down with pressure from a fork (muffins, tuna)
8 Hard and crunchy foods, tough raw fruits and vegetables
9 Dry and crusty breads, dry tough meats, hard nuts
Types 0-7 are designed for inclusion in the diets of people with dysphagia. Adapted from The International Dysphagia Diet Standardisation Initiative 2019 https://iddsi.org
As already mentioned, the salivary enzyme amylase plays a key role in hydrolysing the alpha bonds of starch and glycogen to release glucose. The concentration of salivary amylase varies widely between individuals, because of differences in the number of copies of the amylase gene. Higher numbers of gene copies are found in ethnic groups that historically were farmers rather than hunter gatherers, because of their greater reliance on starch-based foods as their primary energy source. Individuals who carry more copies of the amylase gene and who therefore have higher salivary amylase levels will be able to extract more energy from the same load of complex carbohydrates and will do so quite quickly after eating starchy foods.
Works in 3 mins Material compatibility1,2
Removes+ 99.9% of odour-causing bacteria*3-5
Lifts stains, removes discolouration6,7
Helps keep appliances looking clear1,2
Compatible with common dental appliance material1,2
Retainers
Aligners
Night Guards Mouthguards
For more information, visit www. haleonhealthpartner.com/enau/, www.haleonhealthpartner. com/en-nz/ or scan the QR code
Teeth for the lifespan
There is evidence that the loss of teeth is associated with cognitive decline in the later years of life, with a gradient dose-response effect for missing teeth and the risk of cognitive decline. This effect has been seen in population studies in South America and in North America.6,7
Tooth loss is positively associated with an increased risk of dementia in adults.8
Conversely, having more remaining teeth is associated with having a lower risk of dementia in later life.9
There is accumulating evidence that tooth loss and occlusal dysfunction may affect brain function and trigger the onset of dementia.10
This could mean that poor oral function could be a contributing factor to the onset of dementia.
While part of any such connection between tooth loss and dementia could be due to periodontitis and ongoing chronic subclinical inflammation, it is also possible that a decline in chewing due to edentulism could contribute.
The reason for this is that chewing increases cerebral blood flow bilaterally, which in turn positively affects cognitive function.11-13 Following this line of argument, there is an active discussion in the recent geriatric dentistry literature of the ben-
efits of effective and prolonged chewing to ensure sufficient activation of masticatory muscles, as well as for the proper mastication of food, whether that chewing involves natural teeth, dental implants or dental prostheses.
Appropriate and sufficiently long chewing then enhances cerebral blood flow and activates specific brain areas. Together, these prevent amyloid-beta plaque formation, which is an essential event in the development of neurodegenerative diseases.14-16
Conclusions
The most recent concepts around the importance of chewing stress that all the components of the masticatory system must work together in order to ensure adequate nutrition, appropriately regulate the desire for food and preserve cognitive function.
Dental professionals can make powerful arguments around the importance of maintaining teeth for their chewing function. Hopefully the recent evidence summarised in this article provides a steppingstone for people to explore the sizeable literature which has accumulated around the importance of chewing in the maintenance of health.
References
1. Witt T, Stokes JR. Physics of food structure breakdown and bolus formation during oral processing of hard and soft solids, Curr Opin Food Sci. 2015;3:110-117.
2. Prinz JF, Lucas PW. An optimization model for mastication and swallowing in mammals, Proc Roy Soc London B 1997;264:1715-1721.
3. Robinson E, Almiron-Roig E, Rutters F, de Graa CF, et al. A systematic review and meta-analysis examining the effect of eating rate on energy intake and hunger. Am J Clin Nutr. 2014;100(1):123-151.
4. Miquel-Kergoat S, Azais-Braesco V, Burton-Freeman B, Hetherington MM. Effects of chewing on appetite, food intake and gut hormones: A systematic review and meta-analysis. Physiol Behav. 2015;151:88-96.
5. Forde CG, Stieger M. Metabolic Impacts of food oral processing. Food Chemistry, Function and Analysis No. 30. Oral Processing and Consumer Perception: Biophysics, Food Microstructures and Health. Eds. Wolf B, Bakalis S, Chen J. The Royal Society of Chemistry, 2022. London. Pp. 137-186.
6. Peres MA, Bastos JL, Watt RG, Xavier AJ, Barbato PR, D’Orsi E. Tooth loss is associated with severe cognitive impairment among older people: findings from a population-based study in Brazil. Aging Ment Health. 2015;19(10):876-84.
7. Galindo-Moreno P, Lopez-Chaichio L, Padial-Molina M, Avila-Ortiz G, O’Valle F, Ravida A, Catena A. The impact of tooth loss on cognitive function. Clin Oral Investig. 2022;26(4):3493-3500.
8. Fang WL, Jiang MJ, Gu BB, Wei YM, Fan SN, Liao W, Zheng YQ, Liao SW, Xiong Y, Li Y, Xiao SH, Liu J. Tooth loss as a risk factor for dementia: systematic review and meta-analysis of 21 observational studies. BMC Psychiatry. 2018;18(1):345.
9. Oh B, Han DH, Han KT, Liu X, Ukken J, Chang C, Dounis K, Yoo JW. Association between residual teeth number in later life and incidence of dementia: A systematic review and meta-analysis. BMC Geriatr. 2018;18(1):48.
10. Nakamura T, Zou K, Shibuya Y, Michikawa M. Oral dysfunctions and cognitive impairment/dementia. J Neurosci Res. 2021;99(2):518-528.
11. Hasegawa Y, Ono T, Hori K, Nokubi T. Influence of human jaw movement on cerebral blood flow. J Dent Res. 2007;86(1):64-8.
12. Ono T, Hasegawa Y, Hori K, Nokubi T, Hamasaki T. Task-induced activation and hemispheric dominance in cerebral circulation during gum chewing. J Neurol. 2007;254(10):1427-32.
13. Hasegawa Y, Tachibana Y, Sakagami J, Zhang M, Urade M, Ono T. FlavorEnhanced Modulation of Cerebral Blood Flow during Gum Chewing. PLoS One. 2013;8(6):e66313.
14. Miquel S, Aspiras M, Day JEL. Does reduced mastication influence cognitive and systemic health during aging? Physiol Behav. 2018;188:239-250.
15. Lopez-Chaichio L, Padial-Molina M, O’Valle F, Gil-Montoya JA, Catena A, Galindo-Moreno P. Oral health and healthy chewing for healthy cognitive ageing: A comprehensive narrative review. Gerodontology. 2021;38(2):126-135.
16. Da Silva JD, Ni SC, Lee C, Elani H, Ho K, Thomas C, Kuwajima Y, Ishida Y, Kobayashi T, Ishikawa-Nagai S. Association between cognitive health and masticatory conditions: a descriptive study of the national database of the universal healthcare system in Japan. Aging 2021;13(6):7943-7952.
About the author
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology.
Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 400 journal papers, with a citation count of over 20,000 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
Clean. Disinfect. Lubricate. Purge. Dry. In 12 minutes.
Disinfect. Lubricate. Purge. Dry. In 12 minutes. Replace Manual with Mechanical. Clean. Disinfect. Lubricate. Purge. Dry. In 12 minutes. Replace Manual with Clean. Disinfect. Lubricate. Purge. Dry. In 12 minutes. Replace Manual with Mechanical.
Replace Manual with Mechanical.
UP TO
BETTER* REPAIR^ FOR SENSITIVE TEETH
NovaMin delivers superior* coverage of exposed dentine tubules1, with a reparative^ layer that is 50% harder than natural dentine.2
To find out more and order free samples, scan the QR code or visit at www.haleonhealthpartner.com/en-au/ or www.haleonhealthpartner.com/en-nz/ NZ AU
ALWAYS READ THE LABEL AND FOLLOW THE DIRECTIONS FOR USE.
*In lab testing vs stannous fluoride toothpaste.1
^Forms a protective layer over the sensitive areas of the teeth. Brush twice a day for lasting sensitivity protection.
1. Cambridge, 2013. Haleon Data on File: Surface coverage and tubule occlusion of dentine treated with competitor products after 12 hrs immersion in AS. Richard Langford, Cambridge University, July 2023. 2. Parkinson, C. R. and Willson, R. J. (2011) ‘A comparative in vitro study investigating the occlusion and mineralization properties of commercial toothpastes in a four-day dentin disc model’, J Clin Dent, 22(3), pp. 74-81.