This magazine is published by the Association of Salaried Medical Specialists and distributed by post and email to union members.
Executive Director: Sarah Dalton
Magazine Editor: Andrew Chick Journalist: Matt Shand Designer: Twofold Cover Image: Shutterstock
The Specialist is produced with the generous support of MAS.
WANT TO KNOW MORE?
Find our latest resources and information on the ASMS website asms.org.nz or follow us on Facebook and Twitter.
Also look out for our ASMS Direct email updates.
If you have any feedback on the magazine or contribution ideas, please get in touch at asms.org.nz
PREFER TO READ THE SPECIALIST ONLINE?
We have listened to your feedback and are aware that some members prefer not to receive hard copies of the magazine.
If you want to opt out of the hard copy, just email membership@asms.org.nz and we can let you know via email when the next issue is available to read online.
ISSN (Print) 1174-9261
ISSN (Online) 2324-2787
The Specialist is printed on Forestry Stewardship Council® (FSC®) certified paper.
The Specialist is printed on FSC certified environmentally responsible paper stocks manufactured under the environmental management system standard AS/NZS ISO 14001 using Elemental Chlorine Free (ECF) pulp sourced from sustainable well-managed forests. Processes for manufacture include use of vegetable-based inks and water-based sealants, with disposal and/or recycling of waste materials according to best business practices.
Printed by: City Print, Wellington, New Zealand
Leading
Newly appointed Te Whatu Ora National Chief Medical Officer Professor Dame Helen Stokes-Lampard speaks to The Specialist about her hopes and goals for her appointment in the health system.
PROFILE: DAVID SEYMOUR
Private conversation
For an Associate Minister of Health, David Seymour has some unusual ideas about the future role of private provision in our country’s health care system.
BROWN BAGGING IT
KATIE BEN, PRESIDENT
In February, Sarah Dalton and I were invited to the Beehive to meet the new Minister of Health, Simeon Brown.
The meeting started politely enough with discussions of where we felt the problems arose (lack of funding, lack of infrastructure, lack of junior support staff, lack of nursing and allied health staff), and what we thought the solutions were (improve terms and conditions, build better hospitals that are fit for purpose, improve conditions such that the junior doctors and our nursing and allied health colleagues want to stay in New Zealand).
From the outset he declared that he would not be able to discuss our current bargaining in any way. We still managed to inform him that the current ‘financial limitations’ to which Te Whatu Ora’s bargaining team were restricted would not allow us to achieve anything useful in terms of any of those issues.
Time and again we have been told that throwing more money at the problem is not the answer, and that we should be working smarter not harder (or in the case of most of us – both).
Imagine my interest when reading a recent press article that said the plans to partner with the private sector are the answer to all our problems and a “key part of [the] plans to deliver for Kiwis”.
The idea isn’t a new one; the UK has trialled public–private partnerships in health for some time. It results in limited success or abject failure, depending on whether you’re one of the lucky patients who gets their elective surgery
in the private sector, or whether you’re one of the doctors still working in the public sector who is faced with a high acuity workload containing all the patients deemed medically unfit for outsourcing.
Financially, the public sector is still on the hook for all the complications that occur in private hospitals, so the concept that private patients reduce the burden on the public health care system is not wholly accurate. Private health care firms are beholden to their shareholders and need to return a profit on their outlay. I do not and will not have private health insurance. I believe in a functioning public health system where patients will be given the care they need, at the right time, in the right place, and at the level of excellence that I know we strive for every day.
Bargaining is ongoing, and the team continues to advocate for better conditions for us all, to allow recruitment of new colleagues, and to try and keep our senior trainees in the country.
We are, as always, met with stonewalling across the table and with responses to our claims that they “must fall within our fiscal envelope”. We are going to need to ask you what you and
your colleagues are prepared to accept. There are key questions about what we are prepared to consider if we are to keep our health system publicly accessible, to keep our patients safe, and to strive towards equity in outcomes for our population.
Back to my chat with the Hon Simeon Brown. We finished on a less cordial note, with frank descriptions of overcrowding and beds in corridors, of patients having cancer surgery cancelled due to a lack of beds, of staff working illegal rosters or rosters with gaps that can’t be filled, of hospitals at night in the hands of very junior RMOs, and of patients that the health service is failing on a daily basis. To do him credit, he did sit there and make notes, and he has agreed to consider coming to conference this year, where I hope we can persuade him to keep our public health system 100 per cent public.
Minister Brown seems convinced that his targets will save lives. I’m more convinced that you and I and our colleagues throughout the health system are the ones saving the lives. We will continue to hold the Government to account to allow us to do so safely, equitably, and without sacrificing our own physical and mental health in the process.
The UK has trialled public–private partnerships in health for some time. It results in limited success or abject failure.”
THE ‘SIN’ OF OVERSTAFFING
SARAH DALTON, EXECUTIVE DIRECTOR
In my first months back at work this year, I have spent significant time attending events around the country to highlight the collapse of various health services.
First, I spent time in Palmerston North to talk with patients and whānau affected by the pause on surveillance colonoscopies. Then I spoke at the obstetric services hīkoi organised in Whakatāne following the temporary downgrade of their birthing service from secondary to primary.
Both these issues have a range of causes, but the most significant – and one common to both – is Te Whatu Ora’s refusal to maintain safe or sustainable levels of SMO and RMO staffing.
It is behaviour inherited from the DHBs and, as you will all know, is nothing new.
Our health leaders think the greater sin would be to overstaff! Imagine! The unwritten rule is to understaff and rely on the goodwill of whoever is in the building to hold things together.
Recently departed Te Whatu Ora Chief Executive Margie Apa told me late last year that the medical shortages listed in the 2023 workforce plan were not used to inform budgets. Take a moment to reflect on that.
Known shortages did not inform budget planning or decisions.
While shortages are being felt in all hospitals, our smaller and more remote hospitals are at the sharpest edge of this. They seldom have a deep RMO cohort, often relying on PGY1s and PGY2s, and the bulk of the work, including first call, is carried out by SMOs.
This is no way to staff a service, let along recruit!
Right now Malcolm Mulholland, the Chair of Patient Voice Aotearoa, will be carrying the Buller Declaration around the North Island seeking more signatures (see page 35).
Soon after, Art Nahill and Glenn Colquhoun will be driving a repurposed ambulance from Kaitāia to Wellington, holding a people’s inquiry into access to health care along the way (see page 12).
Where possible, I encourage you to engage in these projects – both focused on exposing the ways access to care is being limited, rationed and maldistributed in opposition to best advice from clinicians.
When speaking at these events, I find the public are sympathetic to the constraints faced by clinicians – they
understand that you didn’t undertake years of training and enter the public health system with a determination NOT to treat patients!
The public want to know what they can do to support a better funded, more accessible public health system –and they want to be able to discuss these issues with you.
I have also been talking to politicians from most of the political parties – Katie Ben and I met the new Health Minister last month; and I have also had discussions with health spokespeople from Labour, the Greens, and NZ First.
The Government’s singular focus on targets presents some real challenges in the immediate future. To date, they do so without an accompanying interest in the required staffing and resourcing to meet them.
We also face a real challenge to get a decent conversation going about improved community health services. Until these become a priority, hospitals will continue to struggle with the predictable outcomes of unmet need.
ASMS will be contributing directly to these debates from April with a new series of papers about health funding. We hope these will play a significant role in shaping the health funding debates and decisions – and will also be a platform for policy review as we head towards the general election in 2026.
This year’s annual conference will be built around these papers. So put 16–17 October in your diary now – it will be a really good one!
At the conference we will also be making some necessary constitutional amendments to ensure we are ready for the implementation of the Incorporated Societies Act in 2026.
We will also be sending out some ‘explainers’ about conference decision-making processes to ensure delegates are prepped and ready for conference discussions.
There is no doubt this will be a busy year. Remember that your union is here to support you – and to advocate for you – and we look forward to working together to fight for improved staffing, better health resourcing, and a more accessible health system.
Ngā mihi mahana ki a koutou.
LEADING HOPE
Newly appointed Te Whatu Ora National Chief Medical Officer Professor Dame Helen StokesLampard speaks to The Specialist about her hopes and goals for her appointment in the health system.
The biggest demotivator for clinicians is realising that they do not have sufficient numbers of colleagues to provide a safe service.”
The newly appointed National Chief Medical Officer says it is the front line that will have the answers to the health care system crisis, and she hopes to amplify clinicians’ voices across the health sector.
Originally from Wales, but based for many years in the Midlands of the United Kingdom, Dame Helen served as Chair of the Royal College of General Practitioners, then Chair of the Academy of Medical Colleges throughout the pandemic and as a professor of medical education at the University of Birmingham. She also established the National Academy for Social Prescribing.
“The United Kingdom is a bit further down the line in terms of some of the fiscal and workplace challenges in health care, and has had to make some difficult decisions,” she says.
“There is good and bad learning to be picked up on.”
As a GP herself, she will be practising medicine in New Zealand. She pushes back against the terminology of ‘productivity issues’ within the health system.
“Productivity in real life health care is a highly complex thing, but the current use of the phrase applies to a set of measures that clinicians tend not to recognise or value. So discussion of productivity without a clinical insight does not sit comfortably within frontline health care.
“We [clinicians] have a responsibility to do the best we can with the resources we have got, but you cannot do that if people do not feel valued.
“There is certainly measurable variation across the country in how many patients are treated by an FTE-equivalent clinician per day. What we as clinicians know is those differences are complex.
“One consultant might be dealing with a list containing highly complex, tertiary-level
patients while another might be dealing with straightforward ones. So, we know those kind of [productivity] measures are often very simplistic.”
“People have not felt able to take ownership of things they feel have been done to them by the system,” she says. “That is why clinical leadership is so very important. We are the interface between our patients and management.
“Things are perceived by clinicians as being turned into blame as opposed to creating incentives for doing the best for our patients and something that gives great clinical satisfaction.”
The top priority for Dame Helen is to finalise the permanent appointment of many of the district chief medical officers and introducing some stability into the workforce, which she says will empower the clinical voice.
ASMS opposed the need to interview ‘interim’ CMOs and called for them to be confirmed in their roles once the review process found there would be no change to their roles.
“The system needs stability right now,” she says. “Nailing down those appointments will mean that the full tribe of 18 CMOs is confirmed, and we can move forward. There is a lot of work to do together.
“Over the next six months I will focus on workforce planning, working with the new leadership team and ministerial team to make the best of what we have right now. I believe there is a lot of potential in the clinical network structure and there is a massive challenge with morale across the profession.
“If I get the CMOs group enthused and working collaboratively across the country, then we can provide the inspirational leadership and leadership pipeline for the future, which in turn will have a positive benefit on morale.”
Asked about how morale can be improved, she said it is about getting more colleagues in post to allow safe service sizes to be enacted.
“The biggest demotivator for clinicians is realising that they do not have sufficient numbers of colleagues to provide a safe service,” she says.
“If we visibly improve the workforce, we can also start looking at how we help support morale. People need to feel valued. They need to feel their voices are heard. I understand people feel they have spoken out a lot in the past and have not had visible differences realised.”
The differences between the former DHBs and the diversity between hospitals in New Zealand has been a steep learning curve.
“I have been surprised that the health care system is so complex given the scale of the population,” she says, “and how different the challenges in the different districts are from each other as well as how things are done.
I never realised the variation would be so great.
“Almost invariably it is the people on the front line who have the answers. I want to use my experience to illustrate what is going on here and help draw out the solutions people find for themselves.”
In terms of what can be learned from her time in the UK, Stokes-Lampard says there are good and bad points but identifies more creative use of the workforce.
“The UK has been about expanding the workforce and using different health care professionals creatively,” she said.
“There have been some examples where that has worked well and there have been examples where things have not integrated well with other health care professionals. Places where supervision and regulation have lagged behind.
So, there is lots of learning in that space.”
“Only now are they regulating physician associates in the UK, and that’s 20 years after they were introduced. Whereas in New Zealand, regulation of the physician associate profession is under consideration by the Government.”
An editorial in the New Zealand Medical Journal in September last year (6 September 2024, Vol 137, No 1602) argued that a robust case has yet to be presented that physician associates are the solution to our medical workforce crisis.
Dame Helen says her relationship-building skills help her to hear concerns and find solutions from the front line to see what can be implemented as New Zealand cannot afford to lose more workforce.
“What makes people stay? Feeling valued. Feeling heard. Being able to do a good job. There are some areas where things are strong. New Zealand offers a strong employment contract to its doctors – both RMOs and SMOs.
“I was stunned at how much better it was than what I was used to in the United Kingdom. It’s the success of unions over the years that there is such a strong contract and people may not appreciate that until they go into an environment where that is not the case.”
Unfortunately, she does not see any fiscal improvement in the short term coming to assist clinicians.
“Global economics are pretty dire,” she says.
“Taxation-funded health care systems have borne the brunt of much of that, but there has been a lag for the impact to really hit home. We’re at the sharp end of it. You’ve seen the swing politically, as almost every government has experienced a swing. What does that mean for New Zealand? Well, you’ve got a shorter political cycle here than in most other countries, and I think that does have an impact. You’re likely to see the pendulum swing faster.
“I’m not seeing any sign that money’s appearing in the short term. So, I’m focused on helping people do the best with what we’ve got right now. And I won’t stand in the way of anyone who’s trying to campaign for anything different. Political cycles and targets are very short term. Those things can bring a conflict which needs to be resolved. While I do not have budgetary control, I do have influence, and I have the ability to create safe spaces for those difficult conversations to take place in a respectful manner.”
Overall, she wants to leave a message of hope for clinicians.
“I want you to know that I am a real clinician,” she says. “I get it. I am on a steep learning curve but do not be afraid to feed back to me. I want to listen and learn. The calibre of our clinicians out here is awesome, and we must use this talent to its best. I want to be an amplifier, and I want to be there for far greater control and for autonomy for clinicians. Because, as I said at the start, the solutions come from within the clinical workforce.”
I’m not seeing any sign that money’s appearing in the short term. So, I’m focused on helping people do the best with what we’ve got right now.”
– DAME HELEN STOKES-LAMPARD
DAME HELEN STOKES-LAMPARD AT THE 2024 ASMS CONFERENCE.
PIPING DOWN
ANDREW CHICK, JOURNALIST
There are three components to the so-called ‘workforce pipeline’ for medical specialists – retaining the doctors we have, training more doctors domestically and finding more from overseas. The final of those prongs has faced significant challenges and criticism in the last 12 months.
“If you look globally, over 50 per cent of that workforce are freelancers. They’re not permanent. New Zealand is in this little bubble where we feel like we need to hire permanent people.”
– CLAIRE MCGRORY
If there is one issue that unites SMOs across the country, it’s that they don’t have enough colleagues.
Organisationally, at least in its workforce plan, Te Whatu Ora agrees. The 2024 plan, eventually released in December last year, omits a current estimate of the doctor shortage (the 2023 version gave a very conservate number of 1,700 FTE) but does say they still need to find another 3,450 full-time doctors by 2033.
Claire McGrory is the Group Manager, International Recruitment at Te Whatu Ora. She, and a team of six, oversee international recruitment for the entire clinical workforce.
“Senior medical officers are probably our most challenging group,” she says.
McGrory says in last eight months their work has resulted in 230 new hires of SMOs and clinical fellows who will start with Te Whatu Ora over the next six months. Each week the same team identify around 130 new candidates for initial screening and evaluation.
But doctors on the ground are having a hard time seeing the results of that effort.
Alex Raines is a general medicine physician at Tairāwhiti and co-chair of the district’s SMO recruitment working group. Tairāwhiti currently has the highest vacancy rate of any district in the country – approximately 35 per cent.
Raines is concerned by how much of his time is taken up with recruitment and how much of that is taking away from his primary job – caring for patients.
“I currently spend about half my week on recruiting and admin tasks,” he says. “I am struggling to keep up with my clinical work because of the burden. As far as I am concerned, I should be involved only in the assessment of a candidate’s CV and references and in the interview process.”
Since October the district has had three different SMO recruiters and two different RMO recruiters.
“There have been candidates that have applied but not had their information passed on for us to review. There have been candidates that we reviewed and recommended for interview who have not had their interview scheduled before accepting a job offer somewhere else. We have had successful interviews where the candidate doesn’t receive the job offer for weeks, sometimes months, and they accept a job somewhere else or give up.”
ASMS Executive Director Sarah Dalton says Te Whatu Ora’s international recruitment efforts are simply not good enough.
“They are invisible. We don’t know what the international recruitment team are up to. We get constant notices of recruitment pause, or changes in process and delegation. Te Whatu Ora seem dead-set on undermining their own efforts.”
“Members find it infuriating when Te Whatu Ora tries to put the onus on them to solve the problem.”
“My international team is tiny,” McGrory says. “I have a team of six looking after all of those workforces. Nationally, it has more than halved in size in the last 12 months due to all of the change.”
McGrory hopes her team can grow back. “I’m woefully under-resourced. We have been out of market, so we haven’t been advertising for seven months.”
While they are now advertising again, and they still attend some international conferences for SMOs (last year they attended five), the most effective technique McGrory’s team currently use is direct contact.
“First my team uses online Boolean search and X-Ray search to target certain websites with certain keywords. It allows us to bring up specific names. Then we do direct engagement through email and phone call. It’s very time consuming.”
“But then it’s a recruiter 101 to ask ‘Who else do you know?’”
“You start hearing things that are going on in a particular hospital. At the moment, we’re really targeting Melbourne for an anaesthetist, because they’re all up in arms about their collective agreement.”
“Quite frankly, post and pray, as I call advertising, just doesn’t work in senior medical health care.”
“What’s made it more challenging for Health New Zealand is our brand. We have been so all over the place – we were Te Whatu Ora, then we were Health New Zealand, then we were Health New Zealand – Te Whatu Ora. We still have district health boards out there. When we’re talking to international candidates, almost the first question [they] ask is, ‘Who am I working for?’”
So, how effective does McGrory think their recruitment is?
“If we did some direct sourcing and campaigning and advertising on media – on a job board for example – for an anaesthetist, we might get five applicants. We find that our conversion from direct sourcing to application probably sits at around 40 per cent.”
It usually takes 12 and 18 months to actually get a doctor to New Zealand. McGrory sites the challenges that can come up with the Medical Council and, less so, immigration.
McGrory says it’s never going to be easy, but New Zealand does have advantages
“We recently recruited a psychiatrist – they are like hens’ teeth – I asked them to tell me why they came to New Zealand. Their response was, ‘I want my daughter to ride her bike without getting shot.’”
McGrory says we have a beautiful lifestyle story to tell. “The other thing is the model of care. You know, our senior medical officers get the opportunity to provide a much broader range of services.”
But she does concede we don’t pay as much here. “But if you work out the hourly rate in terms of what they work hours-wise here versus in the US...”
McGrory is also clear that Te Whatu Ora needs to accept SMOs working privately. “I just don’t think we should be trying to fight that. I’ve got my bosses saying hire permanent people full time, and I’m going, yeah, we might get them for a year, but let’s take a reality pill here. Let’s start pipelining for that 0.5 FTE now, as they land. Because we know that they’re going to go private at some stage.”
“I think we just have to put on our big girl pants and navigate a way through. If we can get them in the public sector for two, three days a week, and they go private for two, three days, then that’s okay.”
While agencies are still primarily responsible for Te Whatu Ora’s locum recruitment, McGrory thinks Te Whatu Ora should be more directly involved.
“[Locums] are the way the talent market is working. If you look globally, over 50 per cent of that workforce are freelancers. They’re not permanent. New Zealand is in this little bubble where we feel like we need to hire permanent people.”
“I was on a call with an old colleague. She’s the global talent acquisition manager for CVS, the largest pharmacy organisation in the US, and over 50 per cent of their pharmacists are freelancers. She said it means that they can
I’m woefully underresourced. We have been out of market, so we haven’t been advertising for seven months.”
– CLAIRE MCGRORY
slice and dice their workforce at pace. If they’ve got new products coming through, they can elevate very quickly if they need to. Or, if they’re dropping products, they can reduce their workforce.”
I would have loved to go out to the UK preChristmas and said, ‘Hey guys, you’re about to go into the most horrible winter, come to New Zealand for six months and do your best work here.’ Even if we had them for six months. But we just don’t think that way.”
AN UNPRODUCTIVE INTERVIEW WITH LESTER LEVY
In a long-running saga, Commissioner of Heath Lester Levy has been avoiding questions from The Specialist since October 2024.
It started back in October 2024 when The Specialist sought interviews with the newly appointed Deputy Chief Executives of Health New Zealand, to introduce them to ASMS members and shed some light on their particular roles.
It ended up in a months-long saga of missing information, dodged questions and rescheduled interviews with Lester Levy.
While the sector has seen the high-profile departure of Te Whatu Ora Chief Executive Margie Apa and Director of Health Diana Safarti, there has been a need for visible leadership.
In the end, Commissioner Levy has not been able to confirm his desire to stay on as Commissioner after his initial term expires on 21 July.
His inability to schedule a quick phone interview and his failure to use the opportunity
to engage with and inform SMOs, appears to sit uncomfortably with his stated focus on “productivity issues” and “run-rate deficits”.
On 3 October last year The Specialist proposed to interview Te Whatu Ora’s four new Deputy Chief Executives (DCEs), asking questions such as “What is it you are aiming to do in the role?”, “What do you hope to bring to the position?” and “How will this improve things?”.
After no response, we followed up the request on 16 October and again on 11 November.
On 18 November Te Whatu Ora eventually replied that an interview would be possible, but Lester Levy would be best placed to speak for the DCEs.
“[The] Commissioner would be best placed to provide you with information on the topics below and we will provide you with some information
on each of the four regional DCEs that you can use as a breakout or spotlight on their priorities and work in each region.”
Each DCE is responsible for one Te Whatu Ora’s four regions and the healthcare provided within, but it appeared Levy judged them incapable of discussing that work publicly.
Despite misgivings, The Specialist agreed to an interview with Commissioner Levy on behalf of the four DCEs. But no date was given for the interview.
On 25 November there was still no date set, but we were told Dr Levy was travelling.
Then on November 26 we were given an interview date of December 6. This was past the copy deadline for the December issue of The Specialist (and we let Te Whatu Ora know this). But we agreed to the accommodation.
WHAT IS THE HEALTH ASSURANCE UNIT?
As Dr Levy has gone to ground, on 19 February new Health Minister Simeon Brown announced the creation of a six-person Health Assurance Unit within the Public Service Commission, led by Hamiora Bowkett.
The Unit was set up at the start of February and will run until the end of May. According
to the Public Service Commission, the Unit’s objective “is to advance the government’s health priorities”. The Unit is directly accountable to the Minister of Health to deliver this work.
Prompted for further clarification, the Commission confirmed the six roles have been seconded from across the public service, including the Ministry of Health. The priorities and targets in question are the priorities set out in the Government
Policy Statement on Health and the five Heath Targets announced by the Government in March 2024. The four-month timeframe is an “initial timeframe” only and the Unit will “engage with officials and health professionals across the system in order to inform and complete its work”.
The Commission were unable to provide any further information about specific areas the Unit would be focusing on or the tools they are going to use.
On December 5 Dr Levy cancelled the interview with no date to reschedule. Instead, his office did provide some brief pro-forma bios of the new DCEs taken from a website entry in July 2024.
The Specialist declined to print this content.
On 23 January, and again on 29 January, The Specialist reached out to try to secure an interview date with Dr Levy.
On 11 February 11 we tried yet again, stating, “With so much happening [in the health leadership space] we think it will be important to have any update from the Commissioner direct to SMOs. It is weak that we have tried to arrange a time since October 2024 and still no luck.”
This prompted an agreement that, rather than an interview, we would provide written questions for Dr Levy to answer. We sent the following questions:
• Will you be staying on as commissioner, or plan to stay on, past July 21 when the term expires?
What do you hope to achieve by July 21 in regards to the Health NZ reform? What cannot be done in that timeframe but should be?
• What do you hope the next two years, and five years looks like for Health NZ?
• When will the health plan to reset Health NZ be released? Why has this taken so long? We have been told it has had to be rewritten; can you confirm this detail?
• Is the productivity issue still present in Health NZ?
• Has the change of Minister affected the commissioner role?
• Do you think the budget restrictions placed on Health NZ are hampering its ability to recruit clinical staff where needed?
• Do you accept there are currently enough senior doctors in the workforce? If not, how short are we?
• Has the run-rate deficit improved during your tenure to date? Can you provide data and metrics to support this?
• Has the net number of clinical staff increased or decreased under your tenure? Can you provide data to support this?
• Does New Zealand have to increase private health provision to ease the public strain, what does this look like in your mind?
• How is Health New Zealand holding up against key health targets set by the Government? Can you supply current counts? What needs to be done to improve these target figures?
• Margie Apa has resigned, is this disappointing given you backed her once taking on the roll?
Should she have left immediate once you took over or served out her term?
• What sort of leadership does Health NZ need in your opinion? Should we be looking overseas?
• Job sizing remains an issue across many hospitals, we are seeing cracks in regional hospitals that are struggling to cope with short staffing (such as Tairāwhiti) – what initiatives will you implement to alleviate stress in regional and rural hospitals?
• Many are talking about a regional allowance or uplift – do you support this idea? Why/why not?
Two days later Te Whatu Ora confirmed Levy would answer the questions “next week”.
By 21 February there was still no response.
On 24 February a member of the Te Whatu Ora communications team wrote “I spoke to Lester late on Friday, he really wants to answer your questions as he thinks they’re important, but he’s just been hugely under the pump at the moment (which of course we can all understand) he will get something to you asap!”
On 25 February The Specialist followed up again. A spokesperson responded: “He asked to be able to send them through mid-week with the explanation, “I know it’s not ideal, but a reflection of the times.”
Already past our copy deadline for the March edition, we gave Dr Levy one last opportunity. That afternoon a communications staff member wrote back “He’s flat out, he thinks these are important questions and wants to be able to answer the ones he can properly. He will be happy to talk to you when he can find some time.”
ODE TO HEALTH
MATT SHAND, JOURNALIST
A living poem about the state of the public health system is being written by two doctors on an epic road trip.
Two doctors are driving across the North Island in an ‘arted-out’ ambulance to create a living poem about the state of the public health system.
Art Nahill and Glen Colquhoun have worked as doctors for more than 30 years but have become increasingly angered by the failure of successive governments to care for the public health system.
They have seen, and treated, patients who have fallen through the cracks as well as seen colleagues deal with stress and burnout. Now they are turning that anger into something positive by driving across the North Island to bring the voices of clinicians and patients to the steps of Parliament.
“For us, this is a way to turn art into action,” Nahill says. “It’s a way to channel our anger into something creative and something more positive. We’ve had our van painted up with the help of Nigel Brown, who is a veteran of lots of protests in his time, and he is someone well versed in using art to express anger and demonstrate the need for change.”
Their vehicle will leave Kaitāia on 26 April and travel to most major population centres in the North Island before arriving in Wellington on 8 May.
“Our van has been painted to look like a fanciful ambulance as a metaphor for the dire condition the health care system,” Nahill says.
“We’re advocating for a measured, data-driven, political redesign of the health care system to try and prevent people from becoming unwell.”
Nahill says that change will require a major rethink and a collaboration of ideas.
“As it stands, if you are unwell you go to your GP or, if there isn’t one, your emergency department,” Nahill says. “That’s where your health journey begins.
“There are lots of models internationally where workers in the community strive to maintain peoples’ health and do maintain it.
“We’ve seen that model work when we look at immunisations in Māori and Pacific communities.
And internationally, there are many models where a really active and robust community health engagement in the place where people live and work can pay lots of dividends in the long term.
“But part of the problem is that, because of our political cycle, we tend to not look in the long term. We tend to think of, okay, what’s the quick fix now? What can we do now? And while I’m all for training up more doctors and nurses, there’s nothing that’s going to change what draws them to Australia or draws them to the private system if we don’t change the public system.”
The team hopes to gather stories from patients, clinicians, nurses and anyone who has a view on what could improve the public health system.
“We want to hear from anybody who has a good story about their interactions with the health care system and, more importantly, gather their ideas as to what would make for a good health care system,” Nahill says.
“We don’t want to just gather gripes and grudges,
there are plenty of those to go around. We need to move the conversation a bit towards what are some viable, creative alternatives to what we have now.
“We must make it clear to politicians that there are ideas out there and that people do care about the state of the health care system. Ignore us at your own peril.”
Health has become a major political talking point in the lead up to next year’s election, with polling showing it a hotly contested issue. The hīkoi will be taking documentary footage and archiving the stories they hear as they go.
“All parties have failed to look after the health care system,” Nahill says. “We will be gathering footage and anticipate there will be a larger body of work to turn all the archival footage of our trip into something longer and something more in-depth.
“We are lucky to have two amazing young women, Oriwa and Emily, making the journey with us to collect and document the stories and suggestions,” Nahill says. They represent the ideas, passion and promise of young people and will work to capture their concerns.
The trip is being funded out of their own pockets and whatever donations the pair can scrounge together.
“If people want to get involved, they might help us out with a place to stay or some petrol, a cup of tea or a chat,” Nahil says.
More information can be found at healthreformnz.org
Tour stops
Day 1 Saturday, 26 April: Kaitāia (morning), Kerikeri (afternoon/evening)
Day 2 Sunday, 27 April: Whangārei
Day 3 Monday, 28 April: central Auckland (morning), south Auckland (afternoon/evening)
Day 4 Tuesday, 29 April: Hamilton (midday)
Day 5 Wednesday, 30 April: Rotorua (midday)
Day 6 And on the 6th day they rested!
Day 7 Friday, 2 May: Gisborne
Day 8 Saturday, 3 May: Hawke’s Bay
Day 9 A driving day (and some more rest!)
Day 10 Monday, 5 May: New Plymouth (morning), Whanganui (afternoon/evening)
Day 11 Tuesday, 6 May: Palmerston North (midday), Levin/Ōtaki (afternoon/evening)
Day 12 Preparation for our trip to Wellington –the final push!
Day 13 Thursday, 8 May: Wellington, Parliament grounds (midday)
We want to hear from anybody who has a good story about their interactions with the health care system and, more importantly, gather their ideas as to what would make for a good health care system.”
LEFT: ART NAHILL MIDDLE: NIGEL BROWN RIGHT: NIGEL BROWN.
The P-word
Private conversation Being extreme Survival medicine 20 16 23
Setting a new pace for medical research in New Zealand Is my patient fit to drive? 26 28 31
We have a largely private system, the part that is public is the commissioning, the organising. That’s the part where we need to ask ourselves, is it better if you had a choice…”
PRIVATE CONVERSATION
MATT SHAND, JOURNALIST
For an Associate Minister of Health, David Seymour has some unusual ideas about the future role of private provision in our country’s health care system.
ACT Party leader and Associate Minister of Health David Seymour wants New Zealand to have a conversation about wider privatisation of health care, but admits the country is not ready to have it. During his State of the Nation speech in January 2025, Seymour floated the idea of people being able to ‘opt out’ of the public health system and make their own arrangements.
While the concept was not fully fleshed out, the basic idea is for the state to provide a sum of money, about $6,000, for people to arrange private health care needs for themselves.
“I do feel the polarised debate that occurred after I mentioned the P word [privatisation] suggests maybe we are not ready for it,” he says. “On the other hand, I just look at the long-term future of health care and where the numbers go and I ask the other question – What is the consequence of not having these discussions?”
Outlining the problem
Seymour says the big problem with health care stems from the demographics of New Zealand.
“There are going to be more people over 80 with higher medical needs,” he says. “There are fewer children coming through, graduating and becoming doctors so there are two ways this can work. You can have more people migrate to look after older people and the other is to drastically increase the productivity or the effectiveness of medical care. That has been flat for a long time
in terms of measured productivity, it’s no slight on the people that work in the industry.
“I often say we have a first-world people in a third-world system. My sense is that there is just enormous waste because no one has the incentive to make things more efficient.”
Seymour says he has been called by surgeons who have had to cancel lists because staff members had not turned up, and these calls occur too often.
“Surely you would be working very hard to make sure that everybody shows up at the right place in the right time otherwise you are throwing money down the drain,” he says.
“Another example I have had is I have doctors tell me it takes a month to get a suspected skin cancer pathologised or analysed. I tried to fix this. I visited the lab and found out they were not very keen on doing this [the tests] because nobody had changed the price of a pathology test since like, 1997, or something and the price was not enough to justify them doing it.
“I think I probably wrote a letter to the Minister at the time but I thought that, even if I could fix this, there are a million other problems like that and there needs to be incentives to fix them. That’s the problem. Aging population, aging demographic, massive cost increases, massive waste and massive inefficiency. No one’s actually got responsibility of fixing it.
“I would say that Shane Reti would have been the most competent health minister in the world, certainly in New Zealand, and he couldn’t fix it. Having said that, Simeon Brown has been put there because he is one of the most dynamic and effective ministers in Government.”
How would your privatisation idea work?
“The fact is that a huge portion of health care in New Zealand is private,” Seymour says. “Hospitals are largely state-owned but there are some private hospitals. GPs are all private businesses, pharmacies and much of the allied health stuff.
“We have a largely private system, the part that is public is the commissioning, the organising. That’s the part where we need to ask ourselves, is it better if you had a choice of saying, well there’s a $30 billion health spend and 5 million people so that’s roughly where the $6,000 figure comes from.
“I would say, if you like your health care you can keep your health care. But if you would like to take that $6,000 up the road to say a Southern Cross or a nib they can accept your, for lack of a better term, token from the Government.
“There would be some rules. They must accept every patient who applies, they can never dump a patient, they can’t screen them and they must be responsible for the totality of that patient’s health care. Whatever they need or whatever
I would say that Shane Reti would have been the most competent health minister in the world, certainly in New Zealand, and he couldn’t fix it.”
– DAVID SEYMOUR
health care they receive must be compensated by that company.
“The flip side of that is they will start getting quite aggressive about how they manage their relationships with suppliers, and you know, if the pathology lab is too slow, they’re going to ask what they can do to solve that problem pretty quick. I think these guys will solve problems faster than we [the Government] do.”
Seymour gives the privatisation of mobile networks as an example where technical problems were solved through corporate pressure and profit-driven solutions.
He also says privatisation of health care could create incentives for public health measures from private providers like increasing the funding of GPs.
“I would argue that GPs are underfunded and the rest of the system is suffering as a result,” he says.
“We campaigned on but we could not get the Coalition to agree that we’re going to increase it. It’s a real shame. But that is a good point. At the moment you pretty much have to rely on someone going out, campaigning, winning an election to get the GP pricing right. In the system I am proposing if you are an insurance company now responsible for commissioning health for a patient you will have to think if we paid GPs a bit more then fewer patients might turn up to ED as a result and they wouldn’t have to pay [for ED treatment].”
Leaning on overseas models
Seymour points to other countries that have similar situations, such as a mixed, public–private system in Europe. “The UK is, you know, more
social than anywhere but they have one of the most lamented systems,” he says.
“You go across to France, Germany, Switzerland and they have a very mixed system where you can choose your insurer. Your insurer, chances are, will send you to a private provider most of the time, and for the most part, they have very good health care.”
Seymour says much of the English-speaking world uses the Beveridge health care system where the government provides health care for its citizens through income tax payments. Other countries, such as Germany, use the Bismark system where all residents are mandated to enrol in one of several publicly or privately managed insurance funds to ensure universal health care coverage.
“That system works much more like the one I am describing,” Seymour says. “Most of Europe has some sort of Bismark system with a network for private insurers and providers with the government sort of quarterback funding those people who cannot afford their own.
“There are criticisms of both methods. The Beveridge model reliant is on income tax, which can be adversely affected in times of crisis and by a rapid influx of patients. The Bismark model can leave people in poverty behind or leave them with limited coverage. Further, isolated townships often have little hospital coverage under the model.”
What about acute care?
The big question with private health care stems from what it cannot do. At the moment, acute care is left to the public system and there are ethical questions about ‘for profit’ emergency departments.
What happens in the case of a cardiac arrest or car accident in a privatised system?
“Hospitals have to accept all patients,” he says. “If you are injured you go to the nearest hospital, and there would need to be some rules to prevent discrimination. You would charge the same price to whoever the patient’s insurer was.”
Seymour did have some concerns about this leading to monopoly pricing in specialist areas and said there may need to be some rules introduced to counteract this. These could include special birthing units, children’s hospitals or other specialised care centres where it would make little sense to build multiple facilities in the same region.
What about rural and remote regions?
New Zealand is seeing its capability to deliver health care in remote locations erode due to a lack of commercial viability for private practices. This is leading to closures of GP clinics and further blockages, as GPs who remain are too overloaded to accept more patients. Would these areas ever appeal to private providers where income streams are not as robust?
“In those instances there is a question of should the state intervene and provide a service that won’t be provided. I mean the free market may not produce another Starship Hospital for example, so the government could do that,” Seymour says.
“That is really a separate question, the question is who should be the commissioner [of services]. You could have a remote area of Otago where you are insured and sometimes they will send you to private and sometimes they will take you public. If you are in an area where private is not viable,
then that is a problem for the current system and in the new system.”
Is the answer to provide more funding?
“Well… no,” Seymour says. “I think you know the fact we went from something like $18 billion in the late teens to upwards of $30 billion now. There has been inflation of course, but we’ve never spent more on health.
“I’ve come to the conclusion, if we went up another 50 per cent in five years getting up to $45 billion by 2030 people would still be as dissatisfied and we will still be short.
“One example during the peak of COVID was we needed more ICU beds. Somehow, despite having put amounts of money in that were just insane … there were fewer ICU beds then when we started. It’s a classic example of money still not getting the result.”
How has the privatisation debate gone?
Seymour says it is time New Zealand takes the debate of privatisation seriously. He uses the example of Hawke’s Bay where specialists set up their own health centre next to the hospital as an example of privatisation finding its own niche.
“I would say in a free society, people invent new institutions to achieve cooperatively what they cannot achieve individually. Really, this is about thinking how do we as society find new ways to cooperate to achieve things together.
“We should be more open minded about this.”
Seymour uses telecommunications services as an example of privatisation working, which, he says, has seen improvements in the last 30–40 years without government capital investment. “We’ve gone from zero to a situation where most
populated parts in New Zealand can switch on a phone, download a video and do whatever you want. This service costs almost nothing for what you get.
“Imagine if Health New Zealand had been responsible for introducing mobile phones to New Zealand,” he says. “We would still be using smoke signals. Second of all, imagine if we introduced the same sort of competition and dynamism that has, you know, brought in constantly improving quality of service at falling costs.
“Imagine if we use the same sort of approach to doing better with medicine.”
ASMS is constitutionally committed to “support the right of all New Zealanders to equal access to comprehensive quality public health care services”. This year ASMS will be publishing a series of research papers on health funding.
DAVID SEYMOUR WITH ACT PARTY LIST MP TODD STEPHENSON AND FORMER PHARMAC CHIEF EXECUTIVE SARAH FITT.
THE P-WORD
With the public health system under strain, the ‘P-word’ has started to make its way into the public discourse again. Is privatisation a means to increase supply of health services or is it just moving the deck chairs around?
The debate about privatisation of health care has sparked up again following comments from ACT Party Leader David Seymour in January stating that New Zealand needs to “get past the squeamishness” when it comes to the issue.
Newly appointed Minister of Health Simeon Brown has been visiting private hospitals and on 13 February attended the opening of an expansion to Wakefield Hospital in Wellington.
At the opening, Brown reiterated the Government’s key line that “targets save lives” and that improving the health system was the Government’s top priority.
Of note, he said achieving those targets will “require working in a more collaborative way, especially when it comes to reducing waitlists for electives”.
“Partnering with the private health sector is a key part of our plans to deliver for Kiwis,” he said.
“Aside from ensuring our public systems are working as effectively as possible, we also need to consider how we can make best use of the capacity and expertise the private health sector can offer.”
Some people would see the relationship between public and private health care as symbiotic,
others might describe it as more parasitic. But as workforce shortages continue to worsen, the balance of views might be changing.
As New Zealand’s population grows there are more people with private health insurance with about 30 per cent of the entire population of New Zealand having some form of private health care.
Health insurance sees surge in patients and cost
Southern Cross is responsible for about 71 per cent of all health insurance claims in New Zealand and has 60 per cent market share.
Chief medical officer Stephen Child says the net rate of people seeking private insurance is climbing but so too are the costs of providing it.
Southern Cross’ latest annual report showed it paid out $1.498 billion in health insurance claims over the last financial year. Compared to the total premiums it collected over the same time period, that left a deficit of $88.2 million, which the report described as due to “extraordinarily high demand for private healthcare from our members, particularly in the second half of the financial year”.
The annual report also noted the organisation faced significant price increases in medical supplies, and wage inflation in a tight labour market with shortages of medical professionals.
Child says the rising cost of delivering health care will likely result in premiums increasing.
“The way our premiums work, they are based on age and gender,” he says. “Basically, if you are a 56-year-old male, you basically pay the premiums of all 56-year-old males last year plus about 10 per cent.”
As patients get older, the premiums can increase, and so people can become unable to afford private health insurance, which creates an equity issue.
Child says each year about 60,000 people “churn” out of the system. “We lose that many a year.
“When you look at our surveys from 2019 to 2024, members’ concerns about the cost of living are rising even higher. They say they cannot afford the insurance, or they will drop to a lower level of cover.
“We have had growth, but it is not keeping up with the rising population of New Zealand.”
Child recognises the private health care system is not a standalone solution to workforce shortages.
MATT SHAND, JOURNALIST
ARTIST’S IMPRESSION OF NEW WAKEFIELD HOSPITAL IN WELLINGTON.
So private is an elephant when it comes to elective surgery, but a mouse when it comes to other health provision.”
– CHIEF MEDICAL OFFICER STEPHEN CHILD
“Public health care can do everything the private health care sector can do, but private health care cannot do everything the public health system does,” he says.
“About 70 per cent of all elective surgery is now done in private health care. So private is an elephant when it comes to elective surgery, but a mouse when it comes to other health provision.
“Private does not do chronic health conditions.
It does not do mental health. If you have a chest pain or faint or have a blood clot in your leg or a pneumonia – that is not covered in the private health care system.
“Private health care is procedure and surgery driven. It cannot stand alone. It is complementary to the public health care system.”
Child says the private health care system does offer some incentive to the public workforce and can, in some cases, be used to incentivise doctors staying in New Zealand.
“We wouldn’t have dermatologists in New Zealand if they were not able to top up their salaries in the private sector,” he says.
“Dollars are part of the driver, but it is also job satisfaction. The more autonomy a person has in their work the greater the satisfaction they can generate. Practising medicine in private, you have more choice and ability to influence what you do than in the public system. It must be soul destroying to be an orthopaedic consultant
working in public and seeing patients in pain but not being able to get them up the waiting list.”
Privatisation creep leads to for-profit hospitals
There has been gradual creep of privatisation in New Zealand and it does not appear to be slowing down.
Another for-profit hospital is set to open in the Wellington region in the next few years, with a developer gaining approval to build a sevenstory hospital in the suburb of Mount Cook (just down the road from the existing public hospital).
There have been conversations about other for-profit hospitals in more remote areas such as Wanaka. It seems business leaders have cottoned on to the need for more health care facilities and see a way to provide them – and a dividend.
But the rise in facilities is also tied to a rise in SMOs working in the private sector. Research completed by ASMS reveals between 2021 and 2024 there was a net growth in the number SMOs working in the private sector or other employment of 9.6 per cent, compared to the public hospital specialist’s workforce, which grew by just 4 per cent.
In the three years leading up to June 2024, 15 specialities saw a drop of 25.6 FTE in public hospitals, while those same specialties gained 177.9 FTE in the private workforce. Two of the biggest shifts were in anaesthesia and psychiatry.
ASMS policy and research lead Virginia Mills says the trends revealed in the research are worrying, particularly from an equity standpoint.
“The shift towards greater dependency on private secondary health services creates a double disadvantage for those who can’t afford health insurance or to self-fund their care. They are the same sections of the community – mostly Māori, Pacific Peoples and lower-income groups – who miss out in accessing private primary health services due to the costs and consequently have higher preventable hospitalisation rates,” she says.
“The cost barriers to primary care and the uneven distribution of general practices have prompted calls from health professionals and researchers for reform of primary health care services.
“This action would remove user charges and employ GPs like every other specialist working in a public hospital: on a salary, with regular benefits and paid continuing medical education, the right to collective bargaining, and most importantly, the ability to take care of all patients, regardless of income.”
Doctor Sanket Srinivasa will be the clinical lead when the for-profit Mount Cook hospital is built.
He says the project is being driven by unmet need, in particular the ability to conduct surgery. The hospital will feature operating theatres, endoscopy wards, radiology services and some other services such as a laboratory.
There will also be consultant rooms to allow physicians to practise out of the hospital.
“Public and private are often thought of as mutually exclusive things, but they are not,” he says.
“At a basic level, every single person who has got health insurance and access to private health care creates capacity for someone else to be treated in the public system.”
Does private just move deckchairs?
The issue with comments about increasing capacity is that it is not always that simple. At first glance, more surgery is more surgery. The question is who is performing that surgery.
In many places, the SMOs who will treat someone in private also work in public, which means theoretically there is an offset loss of potential time working in public when they work private.
It can also lead to equity issues when it becomes more and more like queue-jumping for those who can afford the money and cannot afford to wait.
One SMO who spoke to The Specialist said in their region, the anaesthetist and surgeon and most of the medical staff doing private surgery are the same ones from the hospital.
“The only difference is the way they are paid for it,” they said. “We can only do so many surgeries a day whether that is in public and private. We do private work in non-rostered hours. The workplace shortage of SMOs means that we cannot always covers shifts, so surgery lists get cancelled because they cannot fund cover, so there is not really a gain of people getting treated.
“If it was going to reduce wait lists, it would have already done it.”
Dr Renee Liang wrote in a column for North and South about the same issue. “We have a finite pool of doctors in this country,” she said.
“The same doctors who staff public hospitals also work in private, which means that the widespread belief that private health care is somehow ‘higher quality’ is also wrong, even if the waiting rooms have more expensive couches.
“Siphoning off those highly trained consultants to work in private affects public waiting lists, and most of those doctors would actually prefer to work in public if they were given the resources they needed to work effectively and efficiently.
“I know that ‘queue jumping’ is commonly discussed in patient forums – for example, if you pay to see a specialist in private you might get prioritised onto their public waitlist. Apart from this being unbelievably unsporting, it also bleeds resources from a public system which has been built on the principles of ‘the greatest good for the greatest number’.”
Ethical issues from monetisation
Child says there is an inherit ethical question when it comes to building private hospitals for profit, and clinicians have to walk a careful line.
“By definition, patients are vulnerable,” he says.
“It would not take me too long to convince someone that the slight discolouration on their left forehead there probably isn’t melanoma but for $1,000 I can take that off. I can probably get that $1,000 out of your pocket, and it is for that reason doctors have a sworn code of ethics.
“As doctors we are supposed to swear to the patients’ best interests, but in a business environment in which I have to maximise a return to shareholders there is always going to be a tension.
“I am personally concerned about corporate primary health care. One reason I work for Southern Cross is they walk the walk, with 93 per cent of all premiums being spent on purchasing health services.
“My code of ethics as a doctor says I am entitled to reasonable remuneration for health care services provided, but what is reasonable? What do shareholders expect for their return?
“The issue comes from unreasonable profit, and we need to have a discussion as a whole about what reasonable profit for health care is acceptable to society as a whole.”
That discussion will need to include the value from having a healthy population and not be just about dollars and cents.
ANOTHER VIEW OF THE NEW WAKEFIELD HOSPITAL EXTENSION.
BEING EXTREME
MATT SHAND, JOURNALIST
Some doctors are using their CME to learn about the limits of where you can practise medicine.
It is a change of mindset – what do you do when you do not have all your equipment around you. What is the priority. Is it treatment, evacuation or shelter?”
– AMY GREEN
Doctors wanting to see the world and challenge themselves in the process are finding opportunities through World Extreme Medicine, an organisation dedicated to upskilling medics so they can provide medical support for expeditions in extreme environments.
The organisation was founded in 2002 by former special forces group member Mark Hannaford.
“Mark quickly learned that when doctors were taken out of their usual setting, be that a hospital or surgery, they were not that confident in applying their skills in remote or austere environments,” education administrator Amy Green says.
“This could be impacted by the lack of nurses and other staff around, and so the course was born.
“The courses are designed to give health care professionals a realistic overview of what life is like being an expedition medic and what considerations you need to make for yourself to adapt to the environment you are heading into. It could be the desert in Oman, the jungles of Costa Rica, Everest Base Camp or arctic Norway.”
The organisation runs training courses to allow practical learning in harsh environments while having an adventure, Green says.
Green recently accompanied a training course in Oman for medics and says the course is wide
reaching and has practical applications when returning to hospital life.
“Our courses are not designed to teach people medicine,” she says. “Doctors already have those skills. It is more about teaching people to apply the skills they already have. It is a change of mindset – what do you do when you do not have all your equipment around you. What is the priority. Is it treatment, evacuation or shelter?”
“The big benefit for people on the courses is developing an ability to adjust to changing considerations quickly and adapt to the location.”
The courses feature medical training on environment-specific issues such as heat, cold and poisonous animals as well as a lot of non-practical training such as leadership, astral navigation, survival training and reading the weather conditions.
“When doctors are on expeditions these skills are essential,” Green says.
Each course includes a mini expedition, such as camping under the stars in the Oman desert. Because of this there are some physical requirements required of candidates.
“In general, if you can walk for several hours carrying a pack of about 15 kilograms you will
be fine,” Green says. “There is usually a bit of time to physically prepare before a course and we can help people who need it. Many courses qualify for use of CME as well, and there are courses with different levels of accreditation.”
Two doctors who went through one of the courses said it opened up a less conventional path for their medical careers.
Twins Lisa and Celeste Geertsema initially worked in New Zealand as locums on a fivemonth contract but ended up staying for 17 years working in the emergency departments and orthopaedics.
Now the pair are each pursuing a master’s degree in extreme medicine at the University of Exeter in the UK and are involved in a range of expeditions and adventure sports. They also work at ski resorts and worked at the FIFA World Cup.
“If you have an opportunity to do these courses,” Lisa says, “particularly as a young person, then you should just go for it. I took my annual leave to do the course and people asked why I was doing it. But I was like, ‘What else am I going to use it for?’”
The first course they attended was focused on core concepts. “It was a general course where you learned about teamwork and dealing with the outdoor environment,” Lisa says.
“Then we did a diving medicine course in Oman. It was three days in Oman diving and learning about dealing with incidents and diving-related illnesses. Then we did courses in Alta in the northern part of Norway and we learned to do cross-country skiing, pack and pull sleds behind us as well as about hypothermia, frostbite and exhaustion.”
These courses also included measures on how to build snow shelters and prevent medicines from freezing in cold environments.
“Then we did the alpine and mountain medicine course, which was the trek up to Everest Base Camp.”
The pair say the courses are the perfect combination of an activity, fun and learning.
“It was an activity holiday we would have done anyway and then combining that with medicine and the type of medicine we find really stimulating, so it was perfect. It was exciting to go on expeditions and develop interpersonal relations and figure out how to make stuff happen. I loved it.”
PARTICIPANTS AT A WORLD EXTREME MEDICINE ALPINE COURSE
SURVIVAL MEDICINE
MATT SHAND, JOURNALIST
From battlefields to Everest Base Camp, John Apps has travelled the world rendering medical aid and helping others. Now he gives back by awakening doctors’ joy of medicine through his training course in a bid to reduce burnout.
The word that doctor John Apps uses to describe the public health system is “relentless”.
“In my view this is starting to get worse and worse,” he says. “As a GP I was starting to think about how medicine is an all-consuming job. I felt a bit trapped in the health care system. I needed to take time to look after myself and learn how to say no.
“It also meant saying yes to doing more for my mental health and wellbeing.”
Apps says he funded himself for a three-month sabbatical, after hiring a locum to cover his shifts, and went off to find himself and reflect on his choice to enter medicine. He says more doctors, and health care professionals, need to find ways to reflect on what is important to them in order to combat the growing rates of burnout being seen in New Zealand.
Now, through his role instructing at World Extreme Medicine (WEM), Apps is giving back to a new generation of doctors who were feeling the effects of burnout just as he was.
“There are quite a few doctors in their early 20s and late 30s and so many of them are questioning what they are doing in medicine,” he says.
“The art of medicine has died. People are clicked into this idea of modern practice, which is more about box ticking and adherence to pathways or guidelines. We can teach doctors how to think outside the box and you see them come alive at the idea.
“Some doctors are uncomfortable with that, and in the world of extreme medicines there can be very limited evidence for some of the stuff we have to treat.
“It is also an uncontrolled environment. A lot of doctors are great within a controlled environment but put them on an ice cap or a mountain and they will struggle. You may not be able to do the full assessment or get the imaging you need. It may mean you need to think of logistics and shelter before treatment, which is invaluable training in pre-hospital or rural hospital settings.
“It changes the mindset, and this can provide a lot of confidence that doctors take back to their jobs in the cities or rural hospital settings.”
Apps says in a country where less and less per capita funding is being provided to health care the skills to cope in more extreme environments are becoming more and more valuable. In a way the city workspaces are starting to become more and more extreme.
“Sometimes the only way for doctors to get by is to cut corners,” he says. “There seems to be this refusal to accept that the health care system is woefully understaffed and under-resourced compared to other countries. What a shame. This country could have such a superb health service if it was properly resourced, and that would allow for retention rates. We need to look after our doctors better.”
Apps says doctors are incredibly good at pretending they are fine when things are going wrong and concealing illnesses from others. He sees this first hand in his WEM training, and it is a behaviour they focus on stopping.
“Doctors do not tell people they are suffering until things are pretty badly wrong with them,” he says. “We think we are immortal. Sometimes we must take time off, and that is hard for our patients, but
A lot of doctors are great within a controlled environment but put them on an ice cap or a mountain and they will struggle.”
sometimes the best thing we can do is accept that today is not a good day. Doctoring is one of the hardest jobs on the planet, but if you have lost concentration you have to take some time off for yourself.”
This is evidenced in high-altitude training where mathematics goes out the window. “You have to write things down in advance as you cannot make good calculations under stress. That’s how mistakes are made. At altitude you cannot do maths very well and make simple errors. That has parallels to the workplace.”
Apps says if doctors are feeling like they are stressed then the courses at WEM can be a good way to recharge the batteries and find new passion for medicine.
“There are a whole range of courses for whatever floats your boat,” he says. “There is exposure to a range of outdoor stuff with lectures thrown in, say, about altitude sickness or wound care. The environments range from jungle to desert to humanitarian disaster and it can open doors to MSF [Médecins Sans Frontières] and other agencies.
“More than that, you bring it back to work. It builds a whole new layer of resilience and problem solving. We get doctors who are jaded and switched off from the stress. But after a few hours the lights go on and they are engaged and interested in the practical, hands-on training.”
Apps has also worked and helped train people delivering medical care in Afghanistan and the Ukraine. He likens his time working in Afghanistan and Ukraine to the health care system, which he says gave him an important view on how the world treats people and the importance of looking after one’s wellbeing.
“You think, you know humans are doing terrible things to each other, and we are there trying to patch things up as best we can,” he says. “And I almost liken that to some of the working conditions in the health services. It is just this relentless flow of demand. And sometimes I think ... the only way to meet that demand is that you either work stupidly long hours or neglect yourself.”
Apps hopes more doctors take the time to find their why and rekindle their art of medicine whether through his courses or other means.
“You see them switched off when they come,” he says. “It’s great to see their faces light up as they get engaged and interested and remember why they practise medicine. It’s an absolute bonus for people and they bring all those skills back to work with a new mindset.
“Taking care of yourself should be a primary responsibility.”
DR JOHN APPS.
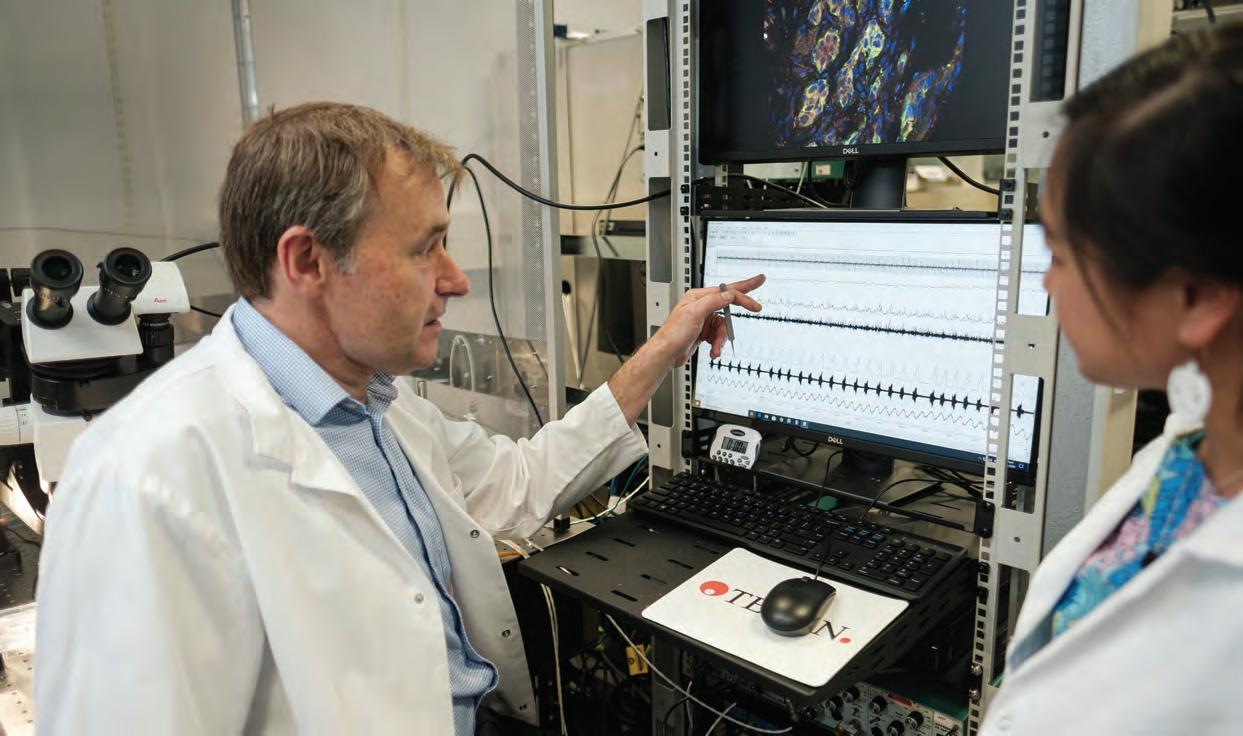
SETTING A NEW PACE FOR MEDICAL RESEARCH IN NEW ZEALAND
MATT SHAND, JOURNALIST
A pacemaker that re-establishes the heart’s variable rhythm has had its first human trials in New Zealand and could launch New Zealand into a billion-dollar medical technology industry.
For the past 15 years Dr Julian Paton has been developing a better pacemaker which uses the body’s in-built breathing rhythm to pace the heart, instead of a constant metronome.
The effect, trials have revealed, is an increase of cardiac output from patients more than 20 per cent.
“We know hearts are paced with the respiratory rhythm instead of a monotonic rhythm,” Paton says.
“What happens is the heart accelerates on inhilation and decelerates on exhalation. This variability is important. The more physically fit you are, the greater the amplitude in heart-rate variability you can produce. Patients with heart failure lose this ability.
“This is present in all animals. Our mathematical modeller says this behaviour would suggest it is a hard-wired energy-saving mechanism. This got us thinking about what would happen if we could pace hearts in patients with heart failure to each breath taken. Would we see better results because we are utilising this energysaving measure?”
The result is a pacemaker that is sent signals when the body breathes in and out to vary the pacing in the device. The pacemaker uses
analogue sensors to react to physical cues from the body and integrate into the respiratory cycle.
“No other pacemaker in the world can do what ours does,” Paton says.
Sheep trials show excellent results
To see if the pacemaker would make a difference to patients’ lives, the device was tested on sheep. “I’ve been a researcher for more than 40 years and I have not seen these types of results before,” Paton says. “It is incredible.”
Researchers induced a heart failure in sheep and used the pacemaker to measure cardiac output over a four-week period.
“We measure cardiac output on the ascending aorta and blood flow to the heart. After three or four days we started to see cardiac output come up. It continued to come up over the week, then plateau and hold for a few weeks. The fact that this was a delay meant this was not a hemodynamic effect. This was the pacing we were inducing that was causing changes in the gene expression that was affecting proteins to generate greater cardiac output.
“The cardiac output increased 23 per cent, which is three times or four times greater than
conventional therapy. You cannot ignore the magnitude of this effect.”
The study was repeated with the sheep given drugs similar to those that heart failure patients would receive.
“A human patient will be on diuretics, inhibitors, and beta blockers etc,” Paton says.
“We gave our sheep these heart failure drugs and started to pace them to see if we could increase their cardiac output. We saw the same per cent increase in cardiac output. This tells you that the mechanism that is driving this improvement in cardiac output is totally unique.
First in human trials begin
The first safety feasibility trials with humans have been undertaken, with a New Zealand patient at Waikato Hospital being the first to try the new technology. Further trials are taking place in Cardiff, Wales, and Melbourne, Australia.
The patients chosen have undergone coronary artery bypass surgery, with the new device connected to temporary pacemaker leads left exposed following the surgeries.
“This means we did not have to miniaturise our pacemaker to implant them,” Paton says.
The pacemaker market is worth billions and an investment in this design could see huge, huge return.”
– JULIAN PATON
“The first patient was a heart-rate variability pacer and the good news is there were no side effects or overt concerns from the patient.
“When asked how they felt they told me their breathing became lighter, which is a positive sign. We’ve seen in other patients quite dramatic increases in cardiac output, which we can measure with ultrasound. It is very encouraging, and it seems feasible to say that our chip is working to speed up the pacing during inhalation and slow it down during expiration. This is the first time this has been accomplished.”
Cardiologist at Waikato Hospital Martin Stiles was involved in connecting the pacemaker to the first patient.
“This could open the door to another therapeutic modality for patients with heart failure,” he says.
“Currently, patients with heart failure will get tablets and rehabilitation programmes, and a very small number of those will be pacemakers. We may find this will allow people with heart failure who don’t get a pacemaker to avail themselves of the technology.”
Stiles says tapping into the natural phenomena present in all animals that breathe is key to the success of the device.
“When I am giving a talk about the pacemaker, I tend to talk about the evolutionary preservation of respiratory variability,” Stiles says.
“Heart rate is linked to respiration, and this is present in animals, reptiles, even fish. It is something that is evolutionarily conserved –even with fish, in which we are talking about gills instead of lungs.
“Clearly there is a benefit to speeding up the heart during inhalation and slowing it during exhalation. But the benefit of doing so has never really been understood.”
Stiles says the ability for the heart to vary its beating is important for health. “We see this in young children,” he says. “They change their heart rate dramatically. As you get older, we lose this ability. The people that lose it the most are those who have heart failure. Losing heart rate variability is a sign of a sick heart. What we did not know is whether restoring heart rate variability improves heart health. We now have evidence, through this pacemaker, that it in fact does.”
Kiwi ingenuity hampered by shortsighted funding
Pacemaker manufacturing is a billion-dollar industry, with the United States and Europe leading the way.
Paton says New Zealand has the opportunity to set itself up as a manufacturer of devices and components in regard to medical innovations, such as the pacemaker.
JULIAN PATON.
“Another aspect,” Paton says. “Is the savings we can make in terms of health care costs because people live with heart failure for a very long time, and they need more and more health care as a result.
“People with heart failure become less and less able to work. The pacemaker we have developed could preserve patients’ ability to continue working, generate salary and pay taxes.”
The problem is funding. Even with a government commitment to boost scientific research, Paton says his project has been left behind, along with other medical technology developments.
Even with recent headlines about New Zealand increasing its scientific output to generate revenue, Paton’s pacemaker has been left on the shelf when it comes to funding.
“The pacemaker market is worth billions and an investment in this design could see huge, huge return,” he said. “But you have to wait for human trials to be done. Research has to be done robustly, carefully and safely, and that takes time. The feeling we are getting as fundamental discovery scientists is that the Government has turned it back on us. It is more interested in quick
return investments. We’ve applied for funding seven times and have been rejected every time.”
Paton says the result of underinvestment in medical technology could see a brain drain from our country’s leading research centres.
“The University of Auckland is the only place in the world that has at its disposal fantastic bio engineers, fantastic worldclass physiologists and an incredibly large preclinical animal research facility – you simply do not get that combination anywhere else in the world.
“But I tell you, it won’t last if we don’t get support, because we’ve spent years building teams, training people, and we’re likely to lose them. To start again and train them again would be very difficult.”
Stiles says it is likely the pacemaker technology will have to be sold to a large American company. “There are basically five large pacemaker manufacturers,” he says. “I think there are discussions with some to employ their algorithm into the pacemakers. It is a billion-dollar industry.”
ANIMAL TESTING
The University of Auckland is a signatory of the Openness Agreement on Animal Research and Teaching in New Zealand, developed by the Australia New Zealand Council for the Care of Animals in Research and Teaching (ANZCCART).
The Openness Agreement commits signatories to acknowledge, both internally and externally, that they and their members carry out, fund or support the use of animals in research and teaching. It also seeks to ensure that signatories are open about the use of these animals.
The University of Auckland supports the five commitments of the Openness Agreement:
• Be clear about why and how animals are used in research and teaching.
• Enhance communications with the media and the public about the use of animals in research and teaching.
• Enhance communications with tangata whenua about the use of animals in research and teaching.
• Be proactive in providing opportunities for the public to find out about research and teaching using animals.
• Report annually on progress and share experiences.
IS MY PATIENT FIT TO DRIVE?
DR LUCY GIBBERD, MEDICOLEGAL ADVISER, MEDICAL PROTECTION
The Medical Aspects of Fitness to Drive: A Guide for Health Practitioners (MAFTD) was updated in December 2024. Here’s what you need to know.
Many medical conditions and medications can affect a patient’s ability to drive. But that aspect of the patient’s life is not always foremost in our mind when we see a patient. In December last year an updated version of The Medical Aspects of Fitness to Drive: A Guide for Health Practitioners (MAFTD) was released by NZ Transport Agency Waka Kotahi (NZTA) and is now online only.
Clinicians have an ethical and legal responsibility to keep patients and the wider public safe by ensuring patients who are unfit to drive are aware and have been told to stop driving. In some situations clinicians may be required to report to NZTA.
Some of the changes NZTA has made are to align New Zealand guidance with Austroads guidance.
As a result, the physical document that is currently in use in our consultation rooms is no longer valid. Moving forward, NZTA will not be producing a hard copy version of the updated guide.
The core legal responsibilities that medical practitioners are subject to are unchanged with the new guide. They are set out in sections 18 and 19 of the Land Transport Act 1998 and clauses 41 and 44 of the Land Transport (Driver Licensing) Rule 1999:
1. That any medical examination done for the purpose of assessing medical fitness to drive must be carried out having regard to MAFTD.
2. To give NZTA medical reports as soon as practicable of persons unfit to drive, or who should only drive subject to conditions, and are likely to continue to drive after being advised not to.
3. When issuing a medical certificate, to give NZTA written notice as soon as practicable that the applicant isn’t medically fit to drive.
4. To do the required actions relating to patients subject to a Compulsory Inpatient Treatment Order (if you’re the person in charge of the hospital the patient is referred to or detained at).
These rules mean that medical practitioners have an obligation to use MAFTD when considering a patient’s fitness to drive.
They also clarify that, if you are seeing a patient for a matter other than assessing medical fitness to drive but are aware a patient is (or is likely to) drive against medical advice, you have a legal obligation to report this to NZTA.
If you think the patient will be compliant with advice not to drive, you are not obliged to notify NZTA. However, if the purpose of the consultation was to provide a medical certificate for driver licence (DL9) and you find the person is unfit to drive, you have an obligation to notify NZTA, whether or not you think the person is going to comply with your advice.
The updated MAFTD considers whether advances in medicine have made some conditions more manageable and whether the old stand-down periods are still appropriate.
It has also clarified the steps when advising a patient who is unfit to drive:
1. Tell the patient verbally and in writing that they are unfit to drive.
2. Give the patient the reasons they’re unfit to drive – verbally and in writing.
3. Tell the patient how soon they can expect to be fit to drive if applicable and if this will be subject to conditions.
4. Tell the patient if a medical review is needed before they can be fit to drive again.
5. Record the details around the decision.
There is a recommendation that patients are told they are not fit to drive and why, in writing. Doctors need to consider how they are practically going to achieve this in clinic, in the emergency department or at hospital discharge. If the information is added to an ‘Information for patients’ section on discharge summaries and a paper copy of this is given to the patient when discharging, it is likely this would be considered sufficient communication, if the patient has already been told verbally.
In GP clinics the situation is probably more onerous. Giving the advice in writing will require you to produce another document recording that you consider the patient is unfit to drive (although it would also be valid for this information to be sent via email/ Manage My Health).
MAFTD suggests that if the patient is not competent to understand your advice, you should consider telling the next of kin. This may have privacy implications in some cases – you may wish to discuss your options with Medical Protection or your indemnifier.
The new guide clarifies the difference between an occupational therapist driving assessment and an on-road safety test and points out that the on-road safety test is not a medical assessment and should not be used if you have concerns around the patient’s physical and cognitive ability to drive safely.
This is a good point to consider the changes introduced by the Land Transport (Drug Driving) Amendment Act 2022, which came into effect in March 2023. The Act includes 25 listed qualifying drugs that may impair driving and outlines high-risk and tolerance blood concentration levels for these drugs.
You can see the feature in the March 2024 issue of The Specialist for more details about that law change.
However, one responsibility outlined in the new MAFTD may raise issues for clinicians.
It states, “Always advise your patient about the impact their medical condition, disability or treatment, may have on their ability to drive. Give this advice to them in writing as well as verbally.”
The word ‘always’ allows for very little wiggle room; this guidance is essentially saying that if your patient has any health condition, disability or treatment that could affect their driving, you have a responsibility to talk to them about that and provide advice about it in writing. This is above and beyond when you consider a patient is actually unfit to drive but applies to any condition or treatment that may affect driving ability.
From a legal point of view, MAFTD only applies to consultations where driving certification is being considered. The concern is that if a patient has a road accident and the issue is raised with the coroner or with the Health and Disability Commissioner, those authorities are likely to look to MAFTD as proving the standard of care.
We are aware that these concerns are being raised with NZTA and, hopefully, they can ensure that this expectation does not become a standard of care, where doctors are criticised if it does not occur.”
If a doctor did not talk to the patient about the effect their condition might have on their driving and/or did not give that advice in writing, it is possible they will be criticised. Further, there is, in theory, a possible route to civil liability where a doctor negligently gives (or fails to give) advice to someone about driving and that person then suffers a financial loss (for example, by crashing their vehicle).
A plaintiff could refer to the MAFTD as setting the standard of reasonable, competent conduct. An obvious concern is that this advice to ‘always’ give advice in writing creates an unrealistic and unattainable standard. In a severely resource-constrained environment, clinicians may be struggling to find time to provide the necessary verbal advice and record that in the notes, let alone also providing patients with written advice.
We are aware that these concerns are being raised with NZTA and, hopefully, they can ensure that this expectation does not become a standard of care, where doctors are criticised if it does not occur.
If you have any questions about a specific case or scenario, and you are a member of the Medical Protection Society (MPS), please contact our advice line for individualised advice on 0800 2255677 or email us on advice@medicalprotection.org
To access the up-to-date version of the MAFTD, visit www.nzta.govt.nz/assets/resources/medical-aspects/ Medical-aspects-of-fitness-to-drive-a-guide-for-healthpractitioners.pdf
A summary of the changes to the MAFTD is available at www.nzta.govt.nz/assets/resources/medical-aspects/ medical-aspects-of-fitness-to-drive-a-guide-for-healthpractitioners-summary-of-changes-december-2024.pdf
Private lab workers take action
Patient Voice
Aotearoa brings Buller Declaration to the North Island
I didn’t want to smile
Kāpiti Coast example highlights health and safety issues
APEX MEMBERS RALLY IN WELLINGTON.
IN BRIEF
NEWS FROM AROUND THE MOTU
PRIVATE LAB WORKERS TAKE ACTION
More industrial action is on the cards for APEX private medical laboratory workers as pay negotiations remain deadlocked following the rejection of their bid for pay parity with lab workers employed directly by Te Whatu Ora.
APEX is negotiating a multi-employer collective agreement with three private providers: Awanui Labs, Pathlab Limited and Medlab Central/TLab.
Lab workers employed in these labs are paid 28 to 32 per cent less than their Te Whatu Ora counterparts, but are performing exactly the same work.
The union called two 24-hour strikes either side of Waitangi Day on 5 and 7 February.
APEX members are campaigning on the message of “same work, same pay”. APEX has raised a claim for pay parity to rectify significant wage rate disadvantage, and in turn, enable the rebuilding of these struggling medical laboratory services.
APEX bargaining advocate Denise Tairua said following the strikes a further pay offer was made but was only a 2.2 per cent uplift and was “a slap in the face”.
“We are looking at a four-day strike unless things change. That is likely to occur near the end of March,” she said.
PATIENT VOICE AOTEAROA BRINGS BULLER DECLARATION TO THE NORTH ISLAND
Patient advocacy group Patient Voice Aotearoa is staging a series of public meetings across the North Island to talk about the dire state of the New Zealand health care system.
The group is making an open invitation to local mayors, iwi leaders and the community to come along and talk about the state of our health system and – most importantly – look to find solutions.
Patient Voice Aotearoa will also be inviting those who attend to sign the Buller Declaration. The Declaration toured the South Island in the second half of 2024. The Declaration asserts:
1. Aotearoa New Zealand’s health system is in a state of crisis.
2. The Government must act urgently to address that crisis.
3. Rural, Māori and low-income populations are disproportionately impacted by the crisis.
4. The Government must act urgently to meet its obligations under Te Tiriti o Waitangi and protect Māori health, in consultation with iwi and hapū.
5. The Government must allocate additional resources to train, recruit and retain more nurses, doctors and specialists.
A culmination of all the signatures will be presented at Parliament on 18 November 2025.
Meeting venues are still being confirmed, but dates for the roadshow are listed below, with more information available at facebook.com/ patientvoiceaotearoa
health system that is well-resourced and consistent with Te Tiriti o Waitangi.
You can download a copy of the report at www.dentalforall.nz/research
THE DATES FOR THE MEETINGS ARE:
9 April
9 April
10 April
10 April
11 April
12 April
13 April
15 April
16 April
17 April Kaitāia 18 April
1 May Gisborne 2 May Levin 6 May
THE LAUNCH OF THE BULLER DECLARATION.
I DIDN’T WANT TO SMILE
The Dental for All coalition has released a new report – I Didn’t Want to Smile – recounting the challenging oral health care experiences of 10 varied New Zealanders.
Written by Kayli Taylor, the report brings human stories to the numbers outlined in ASMS’ 2023 report Tooth Be Told
“Everyone has a story to tell about problems accessing dental services,” says Taylor.
“What people want is simple – to smile and live a life without shame.”
The stories cover people from different stages of life and all corners of the country.
Student Mac tells of facing at $530 bill for an X-ray and clean. He couldn’t afford it. He remembers, “While I waited to get the tooth done, I was in pain … I lived with a big gross pimple in my mouth that leaked pus and blood every now and then.”
Moana tells the story of having to pay for two root canals using a Q Card. “Q card isn’t a payment plan; it is a credit card with a standard
Following pressure from ASMS members, Te Whatu Ora has come round to replacing an outdated X-ray machine in the catheterisation lab.
In January tests showed the X-ray equipment was exposing staff to a heightened level of radiation. Due to its age, the machine was also no longer producing images of an acceptable quality.
Industrial Officer Helen Kissell met with members and together they organised a joint letter outlining concerns for staff and patients in continuing to use the outdated equipment.
interest rate of 30% per annum … I paid it off – but because of the high interest rate I paid off an extra $1,200.”
Aroha relied on MSD grants to address major dental problems, including rotting teeth. “They charged $3,000 for a plate, fillings, and extraction. I paid the money back to them but I should have paid the money back to MSD. The dentist took the money, and MSD didn’t waive the debt –so I remain in debt to MSD for money I have already paid back to the dentist.”
Later in the year, Dental for All is planning a national roadshow to bring local attention to the limitations of current private dental care and promote the group’s call for free and universal oral health care in Aotearoa, as part of a public health system that is well-resourced and consistent with Te Tiriti o Waitangi.
You can download a copy of the report at www.dentalforall.nz/research
CANTERBURY MEMBERS STAND TOGETHER OVER CATH LAB
In the letter members laid down an ultimatum that they would have to stop using the lab beyond 24 February if the equipment was not replaced.
Within a week Te Whatu Ora released a statement saying the machine would be upgraded.
“It shouldn’t have gotten to this stage,” said Kissell.
“Te Whatu Ora’s decision to run the gear so far beyond its recommended life is emblematic of their failure to invest. Equally, the late decision to replace it will still mean six to eight weeks of disruption before a new machine is installed.”
But Kissell also says the result shows the power of collective action.
“I’d like to thank the 15 doctors who stood together and put their names to the letter,” she said.
“In these difficult times, it’s a good reminder that we’re strongest when we’re working collectively. It’s also important that there is visibility of safety concerns at the district and regional level.”
INDUSTRIAL OFFICER HELEN KISSELL.
THE OLD PARKSIDE BUILDING WHERE THE CATH LAB IS LOCATED.
ASMS SERVICES TO MEMBERS
As a professional association, we promote:
• the right of equal access for all New Zealanders to high quality health services professional interests of salaried doctors and dentists
• policies sought in legislation and government by salaried doctors and dentists.
As a union of professionals, we:
• provide advice to salaried doctors and dentists who receive a job offer from a New Zealand employer
• negotiate effective and enforceable collective employment agreements with employers. This includes the collective agreement (MECA) covering employment of senior medical and dental staff in DHBs, which ensures minimum terms and conditions for more than 5,000 doctors and dentists, nearly 90% of this workforce
• advise and represent members when necessary
• support workplace empowerment and clinical leadership.
ASMS JOB VACANCIES ONLINE
Check out jobs.asms.org.nz a comprehensive source of job vacancies for senior medical and dental specialists/consultants within New Zealand hospitals and health services.
CONTACT US
Association of Salaried Medical Specialists
Level 9, The Bayleys Building, 36 Brandon St, Wellington Postal address: PO Box 10763, The Terrace, Wellington 6140
P 04 499 1271
E asms@asms.org.nz
W www.asms.org.nz
FOLLOW US /asms.nz /ASMSNZ
Have you changed address or phone number recently? Please email any changes to your contact details to: asms@asms.org.nz
If you have reason or need to seek a reduction or waiver to your annual subscription, please write to us. Our constitution allows for this in certain circumstances. Emails should be addressed to sarah.dalton@asms.org.nz