Artificial intelligence in anaesthesia: Shaping the innovation pathway
Trasna na dTonnta: From UK to Rebel County
Quality Assurance: What is it and what does it mean for you?
The MyPreOp suite invites patients to complete their POA remotely, transforming capacity and capability. Book a demo
Honorary Digital Fellowship position now open hr@ultramed.co
www.ultramed.co
Welcome
As 2025 draws to a close, this issue of Anaesthesia News celebrates the variety, creativity, and spirit that make this specialty so rewarding.
We start with an incredible feature from a British Antarctic Survey doctor Katherine Ganly who spent 526 days in one of the most remote places on Earth, a story of resilience and medicine at the edge of the world. We also hear from Harriet Jenner and Makuo Ezenwa, sharing reflections from medical electives in the Philippines and Malaysia, and from Emily Bottle and Philip Barclay on the current state of undergraduate medical education.
Looking ahead, Joseph Harris and James Bowness explore AI in anaesthesia, while Matthew Bickerton considers its role in mentorship, with some lively responses. Elsewhere, you will find pieces on wellbeing and personal growth, from moving to Cork to finding meaning in everyday practice.
This issue also introduces our new Irish Standing Committee Convener, John Loughrey, and offers a fun read on pattern recognition in scans, plus insights into quality assurance across our educational work.
And before you sign off for the year, a reminder that the Winter Scientific Meeting 2026 is just around the corner! Join us in London this January for two packed days of learning, debate and networking, with over 30 hours of CPD on offer. It’s always a highlight of the year, and one not to be missed.
Thank you for reading, writing, and being part of our community throughout 2025. Wishing you all a restful festive season, and see you at WSM!
Francesca Cockshull Director, Publishing and Communications
Anaesthesia News
ISSN 0959-2962
Association of Anaesthetists
21 Portland Place, London W1B 1PY
Telephone: 020 7631 1650
Website: www.anaesthetists.org
Editor: Francesca Cockshull
Address for all correspondence, advertising or submissions:
Editorial Assistant: Erin Taylor Email: anaenews.editor@anaesthetists.org
Design: Chris Steer, Digital Designer Telephone: 020 7631 8803 Email: chris@anaesthetists.org
Copyright 2025
Association of Anaesthetists
The Association cannot be responsible for the statements or views of the contributors. No part of this magazine may be reproduced without prior permission. Advertisements are accepted in good faith. Readers are reminded that Anaesthesia News cannot be held responsible in any way for the quality or correctness of products or services offered in advertisements.
Join us today and become part of a vibrant and supportive community of over 10,000 anaesthetists
Since 1932 the Association of Anaesthetists has proudly represented the thousands of individuals who work in the life-changing, life-saving specialty of anaesthesia.
We independently support and advocate for our members in the UK, Ireland and internationally. Informing and inspiring them to achieve their full potential at every stage of their career.
Join our vibrant and supportive community today.
You can enjoy exclusive member benefits and services, and wellbeing support. Find out more: https://anaesthetists.org/ Home/Membership/Benefits-of-membership
Association of Anaesthetists Association of Anaesthetists @assocanaes.bsky.social
An anaesthetist in the Antarctic
It's October 2019, and I am on my way to receive handover in my new role as Medical Officer with the British Antarctic Survey. The usual apprehensions that come with a new appointment are amplified: this is a job unlike any other.
I’m travelling to South Georgia, a barren, mountainous sub-Antarctic island located in the South Atlantic, some 800 nautical miles from the nearest land mass. South Georgia is an island paradise, if your idea of paradise is the cold and very remote. Accessible only by ship, my commute takes four days from the Falkland Islands across the roughest seas in the world.
As the only doctor, I’ll need to be able to manage anything from a sore throat to a seal bite, along with any emergency that happens on my watch. To prepare, I’ve completed 6 months with the British Antarctic Survey Medical Unit (BASMU) prior to embarking on my journey south. Here I have been trained to process my own radiographs, perform a gram stain, carry out a tendon repair, and fill a tooth…or extract one, if required. I’m trained in powerboating and undertake a hairy sea survival course. A brilliant study weekend of baking skills is part of my polar preparations - we’ll be expected to make bread daily from scratch and I don’t want to be responsible for an unrisen loaf.
films, I can manipulate and plaster limbs, and we have a single-person recompression chamber for diving emergencies. The pharmacy is stocked with common and emergency drugs, enough to see us out until the following summer, providing resupply isn’t delayed.
Aside from a memorable encounter with a case of cold-induced angioedema (less than ideal when living in the ice), my clinical caseload largely falls under the remit of general practice and dentistry, and I refamiliarise myself with conditions not usually managed by an anaesthetist. This role requires excellent clinical skills. When a medevac takes ten days, the potential for the trivial becoming serious always needs to be considered.
Everything here is complicated by our isolation and remoteness.
My appendix comes on my journey with me — in modern times this doesn’t need excision prior to Antarctic deployment, though wisdom teeth might not survive screening and are often removed prior to polar travel.
The role of the medical officer in a place like no other
The island of South Georgia has no permanent population, my patients are my colleagues: the scientific, technical and managerial personnel based at King Edward Point Research Station. In the Antarctic summer we are busy: the station is abuzz with over 50 people living, working and sharing rooms on a spit of land only a few football pitches in size. Outside of the station, the remainder of the island is uninhabited and inhospitable.
Day-to-day clinical work is largely uncomplicated. The population is fit and medically screened. Summer work includes checking inventory, training staff in first aid, and running through emergency drills with the coldwater divers and heavy plant operators. My surgery, the Macklin Medical Centre, is well equipped. I can perform basic diagnostics including arterial blood gases, cardiac biomarkers and microscopy. I have an X-Ray machine and the equipment to process wet
Everything here is complicated by our isolation and remoteness.
Out with the medical, other tasks that fall under the remit of the doctor include conducting daily station safety checks. A rolling safety rota means once every nine days it’s an early rise in the dark and cold, an unpleasant task mitigated by the reward of surprising a waddle of penguins or huddle of seals. The doctor also assists science by piloting the small RIBs (Rigid Inflatable Boats) around the island to facilitate wildlifemonitoring projects and holds the dubious honour of being keyholder to the chocolate rationing for the year. All our food is brought in annually, and we need to make sure the sugar outlasts our winter for morale.
Winter
Our busy summer season ends early when a pandemic hits the rest of the world and we wave goodbye to the seasonal team, who return north before lockdown starts. Nine of us are left as winter crew.
Antarctic winter is tuition in self-sufficiency, teamwork and patience. Daily maintenance is ongoing, but the station becomes more relaxed. Everyone begins preparations for midwinter festivities — the Antarctic equivalent of Christmas, marking the halfway point before the days get longer and our relief returns. There is a week of festivities, a formal meal, a dip in the icy ocean and general celebration. We play darts via satphone with our sister station — a game entirely based on honestly reporting your score over a broken line. We win (honestly!). The highlight of the week is midwinter gift-giving, a Secret Santa-style exchange of homemade items the team has been secretly crafting for each other over months. My team produce pieces of carpentry, metalwork and art that could rival anything you’d buy in the UK.
Life is strange and beautiful over winter on this cold paradise isle. We spot leopard seals — the apex predator of our waters, alien and haunting — lounging in the bay. A king penguin hatches near my surgery, miles away from the nearest colony, and I watch in anxiety as his parents try in vain to keep him alive against the elements.
I arrange and rearrange the surgery, explore remnants of seasons passed, discover historical kit. I take a relic craniotome to burr a washed-up seal skull one quiet winter’s day through a mixture of boredom and curiosity.
Our spit of land feels very quiet with only eight other souls for company. A small error means our water system freezes, and we rally to melt ice and snow for 48 hours whilst the technicians repair the system. We are reminded how dependent we are on the team. When the International Space Station passes overhead, we calculate that at 250miles above, we are closer to the men in Space than we are to anyone else on Earth. Untouched by the drama unfolding in the rest of the world, we begin to feel like aliens ourselves.
Challenges
I pass my time reading papers about teamwork in ICE environments — the psychology of being in the Isolated, Confined and Extreme — and laugh when a ‘long’ isolation is described as six weeks. None of us had recognised Covid meant our winter would stretch to ten months. The role of a doctor in Antarctica comes with considerations not seen in conventional practice. The patient-doctor relationship, confidentiality, and professionalism all become challenging when living in such close quarters. My colleagues, friends, temporary Antarctic family get tired and fractious. Relationships form, break and reform. Things that seem trivial in the outside world become a big deal down here.
Winter progresses and I am keenly aware of skill fade: I practice mental drills, coming up with ever-more challenging scenarios and how I might manage should they occur. There is a background low-grade anxiety about being constantly ‘on call’. The stillness sometimes feels like it is waiting to trip you.
There are winter highs too — we discover a recording of Glastonbury 2000 in our library and dress up for a festival day, we create a golf course in the snow, and we direct our own film for the annual Antarctic film festival with much hilarity.
A high is the winter field trip — a chance to spend 5 days offstation in pairs. In the dead of Antarctic winter, my companion and I ‘holiday’ at St Andrews Bay amongst one of the biggest king penguin colonies in the world. We stay in a tiny field hut and survive by burning kerosene, eating ration packs and watching the birds. It is glorious isolation, and we have never been more at peace, despite the roar of the ocean and deafening kazoo calls of these remarkable birds.
Lessons learnt
As my season comes to an end, I reflect on what qualities are needed to succeed as a doctor in such an environment. For those considering this path, there are traits common to anaesthesia that will put you in good stead. Being comfortable with independent working clearly is essential, but other traits are also key: cultivating attention to detail, meticulous planning, and familiarity with various practical procedures and equipment; being a source of calm and control in an emergency and being able to direct those less skilled than yourself.
I board my ship home 526 days after arriving, finishing the longest on-call shift I’ll ever do.
Katharine Ganly Anaesthetics Resident, West of Scotland School of Anaesthesia
The state of undergraduate medical education in anaesthesia
The General Medical Council (GMC) provide recommendations and guide the curricula followed by medical students but there is no universal curriculum. Individual institutions have autonomy and flexibility to plan their programmes as they see fit. In the UK, the Royal College of Anaesthetists (RCoA) in conjunction with the Faculty of Intensive Care Medicine and the Faculty of Pain Medicine published a national framework in 2017 for undergraduate training (RCoA, 2017). Since this framework was introduced, there have been no published studies looking at undergraduate education in anaesthesia in the UK.
Anaesthesia was originally taught as an undergraduate subject from the 1880s as it was expected that house officers should be able to provide anaesthesia. It remained an undergraduate subject until anaesthesia evolved primarily into a post-graduate specialty and anaesthesia was removed from the compulsory undergraduate medical curriculum in 1947. It was not reinstated until 1980, when it was recognised that anaesthetists had many valuable skills to teach medical students outside of the remit of purely providing general anaesthesia, including cardio-pulmonary resuscitation, care of the critically ill patient, perioperative medicine, acute and chronic pain management, and applied physiology and pharmacology.
Historically, undergraduate education was focused on teaching factual information, but the focus of education has shifted to place more emphasis on competency-based skills including non-clinical skills such as communication, management and professionalism.
The practice of medicine requires a solid base of scientific knowledge together with the ability to activate and apply this knowledge in a specific context and transfer it into actions. Within an educational context, learners actively construct their understanding based upon previous experience, knowledge and perceptions of the world. A cyclical model is widely used in education, where a concrete experience is followed by reflective observation, abstract conceptualisation leading back to further concrete experience.
The GMC is responsible for setting standards in undergraduate and postgraduate education. In the 1990s, there was a significant curriculum change in both, with a move from factual learning towards practical on-the-job learning. This was also connected with the publication of ‘Tomorrow’s Doctors’ guidance in 1993, where it was argued that it was important that medical students have an ability to adapt to change to keep pace with rapid advances in medical science and technology. This has now been replaced by the ‘Promoting Excellence: standards for medical education and training’ document published in 2015.
In 2017, the RCoA published the framework guidance for undergraduate medical student training. This was based upon the GMC ‘Outcomes for graduates’ and ‘Tomorrow’s Doctors’.
It was deemed that 63 of the 103 GMC Outcomes could be facilitated by anaesthetists and intensivists. These were used to devise 8 domains of practice that enabled Outcomes for Graduates to be combined with the scope of clinical practice in anaesthesia and intensive care medicine.
1. Recognition and management of the acutely ill patient.
2. Applying basic sciences to clinical practice.
3. Supporting decision-making for optimal patient care, including end-of-life care.
4. Problem solving in clinical care.
5. Communication, collaboration, and negotiation.
6. Practical pharmacology.
7. Safe and effective practical procedures.
8. Understanding fallibility, managing risk.
Outcomes for Graduates also lists 32 practical procedures that new graduates were expected to be able to perform, with 11 judged to be achievable within anaesthesia and critical care and five of the general aspects were combined into one. In addition, the RCoA added airway maintenance* and cardiopulmonary resuscitation* as achievable skills during anaesthetic placements.
1. Airway Maintenance*
2. CPR*
3. Measuring body temperature, pulse rate, blood pressure and oxygen saturation
4. Venepuncture
5. Measuring blood glucose
6. Nutritional assessment
7. Peripheral venous cannulation
8. Making up drugs for parenteral administration
9. Dosage and administration of insulin
10. Subcutaneous and intramuscular injection
11. Blood transfusion
12. Use of local anaesthetics
13. Correct techniques for ‘moving and handling’
14. All five ‘general aspects of practical procedures’ (information and consent, handwashing, use of personal protective equipment (PPE), infection control and safe disposal of waste)
Despite national guidance from the GMC, the guidance from the RCoA is not prescriptive about how medical schools achieve this. This means anaesthetic curricula and placement schedules remain individualised and often tailored to services that are available in the locality.
Although the GMC set standards in medical education, there is no current facility for this to be robustly monitored. As a consequence, there is no available national data on medical schools’ individual curricula and there is no published data on the exposure of UK undergraduate medical students to training in anaesthetic practice and practical procedures.
Investigation
This was investigated by Emily Bottle as part of her master’s in medical education at University of Oxford in 2023. She carried out surveys and interviews with final year medical students at Imperial College London and University of Oxford to provide a qualitative and quantitative assessment of students' experience of their anaesthetic placement.
76% of the students had undergone a dedicated anaesthetics/ critical care placement, with most frequent duration 1 to 2 weeks. Of the 24% who didn’t, 100% stated that they would have liked to have had a dedicated placement.
Students were asked if they had the opportunity to practise 16 domains of clinical skills during their anaesthetic attachment.
All five ‘general aspects of practical procedures’ (information and consent, handwashing, use of personal protective equipment, infection control and safe disposal of waste)
None of the study participants had any experience of CPR (non-simulation) and nutritional assessment.
This correlated with answers about confidence with practical procedures where the commonest response was ‘very confident’:
• CPR (Simulation)
• Measuring body temperature, pulse rate, blood pressure and oxygen saturation
• Venepuncture
• Measuring blood glucose
• Peripheral venous cannulation
• All five ‘general aspects of practical procedures’ (information and consent, handwashing, use of personal protective equipment, infection control and safe disposal of waste)
Rating by students of ‘how useful do you feel your anaesthetic/critical care placement was’ varied hugely from ‘extremely useful’ to ‘slightly useful’.
The following themes emerged from analysis of structured interviews:
• Variability of experience and organisation, with some confusion about timetables and where to attend sessions
• Lack of continuity meant that you were often starting at square one with attachments to different consultants every day. When students did encounter continuity, they did find that to be very advantageous
• Students often found that the high pressure and acuity of anaesthetic attachments made it challenging to undertake practical skills, especially in unwell patients
What does an ideal anaesthetic placement look like?
• A designated clinical supervisor for the duration of the placement, which could be either an anaesthetic consultant or resident doctor
• Additional access to a dedicated teaching fellow in anaesthetics or critical care
• Introduction seminar on the first day of the placement including simulation training on anaesthetic emergencies and specialty-specific practical skills, such as airway maintenance, early in the student’s placement
• Regular small group seminars on anaesthetics-specific topics including pre-operative assessment, practical pharmacology, applied physiology, ventilators and anaesthetic equipment, and anaesthetic emergencies
• The opportunity to shadow the on-call anaesthetist, including out of hours, where appropriate
• The opportunity to attend pre-operative assessment clinics, chronic pain clinics and acute pain rounds
• Assessment should be formative, and students should compile a logbook of cases they have been involved with and practical procedures they have achieved throughout their placements.
Further
reading
General Medical Council. Outcomes for graduates, 2018.
One example of innovation in this area is the Immersive Anaesthesia Learning Team led by Professor Cliff Shelton (Lancaster University / Manchester University NHS Foundation Trust), which has introduced a simulation learning experience to orient year 3 medical students to the principles and practices of the induction of general anaesthesia. Scan QR code to find out more.
Conclusion
Not all UK undergraduates receive a dedicated placement in anaesthesia/critical care. Those who do, enjoy their experience in anaesthesia and feel that they have had good experiences and learning opportunities, particularly in performing practical procedures, although the content varies considerably.
The Association is keen to hear from anaesthetists involved in undergraduate medical education to collate ideas and best practice in teaching anaesthesia to medical students. Please email secretariat@anaesthetists.org if you wish to be involved.
Emily Bottle
Specialist Trainee in Anaesthesia (ST7), Imperial School of Anaesthesia
Philip Barclay
Consultant Anaesthetist, Chelsea and Westminster
Hospital Foundation Trust
Honorary Clinical Senior Lecturer, Imperial College
London Treasurer Elect, Association of Anaesthetists
Royal College of Anaesthetists. Science, skills and safety: A framework for medical student education in anaesthesia, intensive care, pain and perioperative medicine.
Bishop, M. J. How to make the most of your anaesthetics placement. BMJ, 2020; 369, m940.
Artificial intelligence in anaesthesia: Shaping the innovation pathway
The recent emergence of AI into almost all aspects of popular discourse means that most are now familiar with its powerful and disruptive potential. Within the domain of healthcare, AI continues to generate plenty of excitement, including among some ‘techno-optimists’ who view AI as a saviour to an NHS under unprecedented strain.[1]
In anaesthesia and perioperative medicine, accelerating digitisation alongside the widespread use of monitors, ventilators and ultrasound presents a huge opportunity to feed and train powerful, data-hungry AI algorithms. However, many across the frontlines of clinical medicine will feel that the much-vaunted wave of AI transformation is yet to be truly felt by healthcare providers in the UK, if at all. Given that the necessary conditions are seemingly present for an AI revolution, what explains this delay?
As the number of AI-driven devices on the market continues to increase,[2] adoption and impact remains limited due to the unique set of obstacles presented by complex healthcare systems: a lack of unified AI strategy, lengthy governance processes, data privacy concerns, poor interoperability of computer systems, and ethico-legal debates have all contributed to the slow pace of AI adoption into clinical workflows. A recent report into the barriers to NHS AI adoption in London examines these issues, reflecting an increasingly widespread recognition of the challenges ahead and a shift in posture to address them. [3] Fundamentally, however, the question remains about whether the technology- and commercially-led model of innovation may be stifling the transformation process.
The supply chain model of innovation
AI is predicted to accelerate exponentially over the coming years, and has generated a fiercely competitive arms race among industry players seeking to capitalise on a rapidly growing market.
This paradigm reflects the reality that it is easier to seek a clinical application for a capability than it is to engineer a solution to a complex clinical problem from the ground up. For instance, AI’s ability to construct highly accurate predictive models has led to a surge in research studying perioperative risk prediction. Examples include AI algorithms to predict perioperative mortality, neurological and cardiovascular complications, sepsis, acute kidney injury, venous thromboembolism, wound infections, delirium and post-op nausea and vomiting.[6] Studies examining the utility of these models are still in the feasibility stage and it remains to be seen whether these models have any bearing on clinical practice beyond conventional risk stratification tools — particularly in cases where surgery is already understood to be high risk, necessary and resource constrained. AI-based risk prediction algorithms also come with their own shortfalls and tradeoffs, many of which are underrecognised or understudied, such as the intensive use of computational resources, the compounding of existing biases in data, and a susceptibility to performance drift over time.[7]
Limited clinical involvement in the field of healthcare AI is a key factor hindering its impact, as it can result in the development of tools with low clinical utility or with poor fit into the clinical workflow. Commercial investment in AI is predicted to accelerate exponentially over the coming years,[4] and has generated a fiercely competitive arms race among industry players seeking to capitalise on a rapidly growing market. This model of AI development is based on technology-driven invention and commercial implementation, casting clinicians and healthcare organisations as consumers rather than partners in the development pathway. Without clinical metrics of success, a fixation on AI’s predictive accuracy and performance can overlook the complexities and realities of socio-technical healthcare environments, leading to poor clinical effectiveness. [5] Thus, the AI innovation pipeline often begins with devices and algorithms, created by software companies and academic labs, seeking a post-hoc practical and commercial fit for their products.
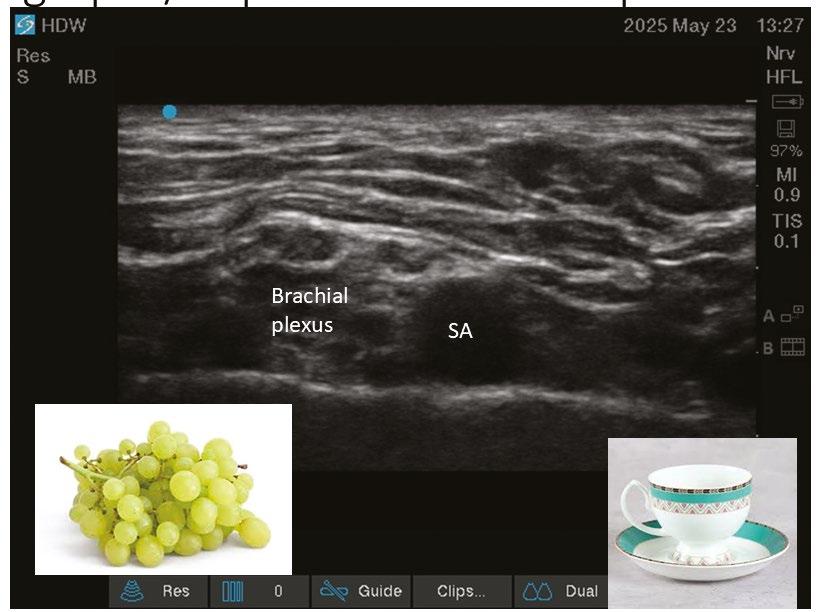
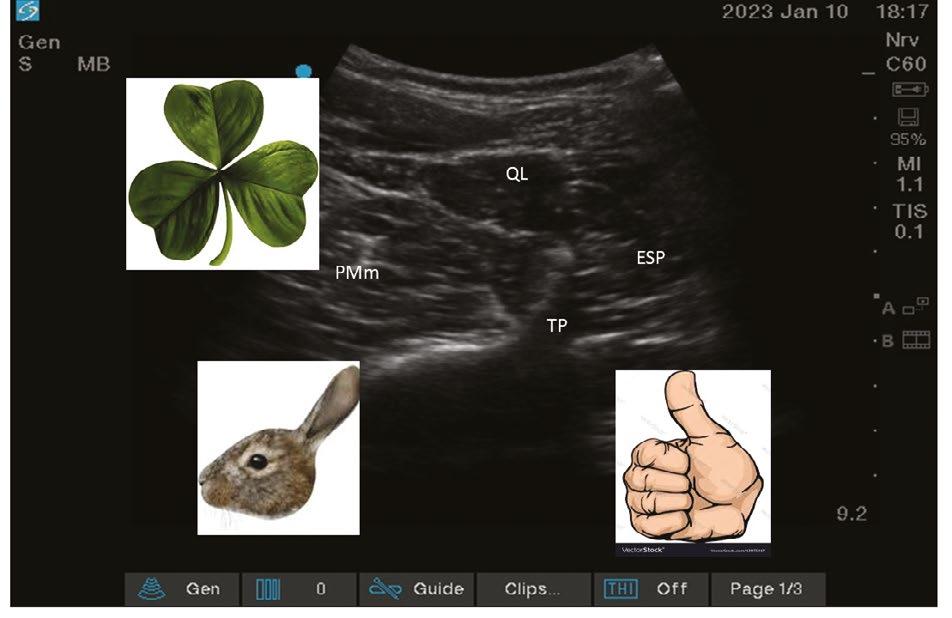
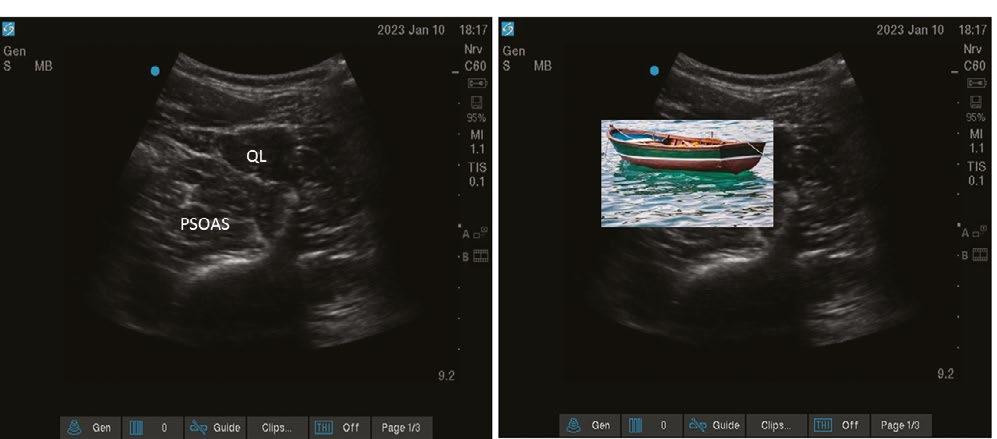
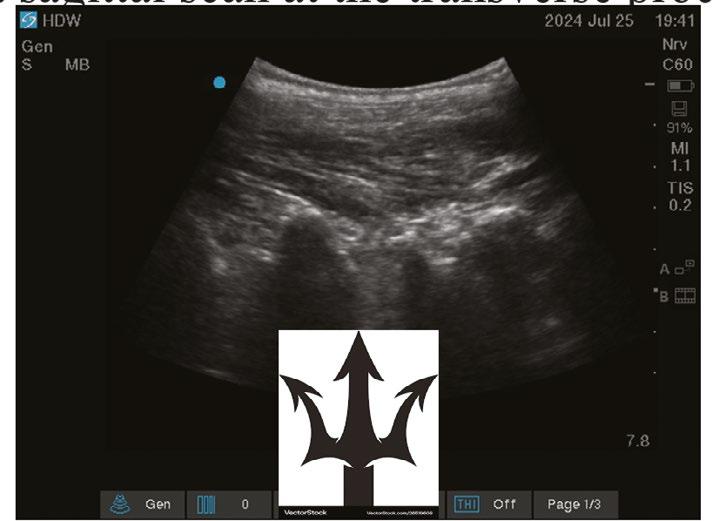
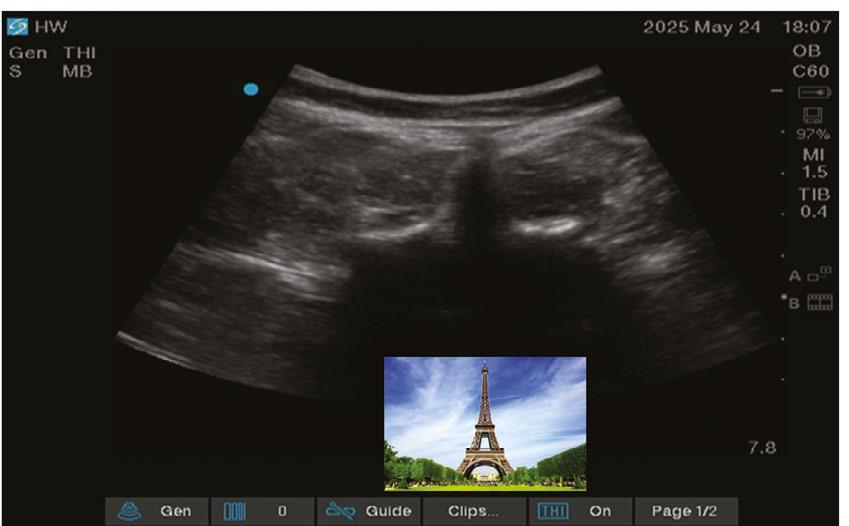
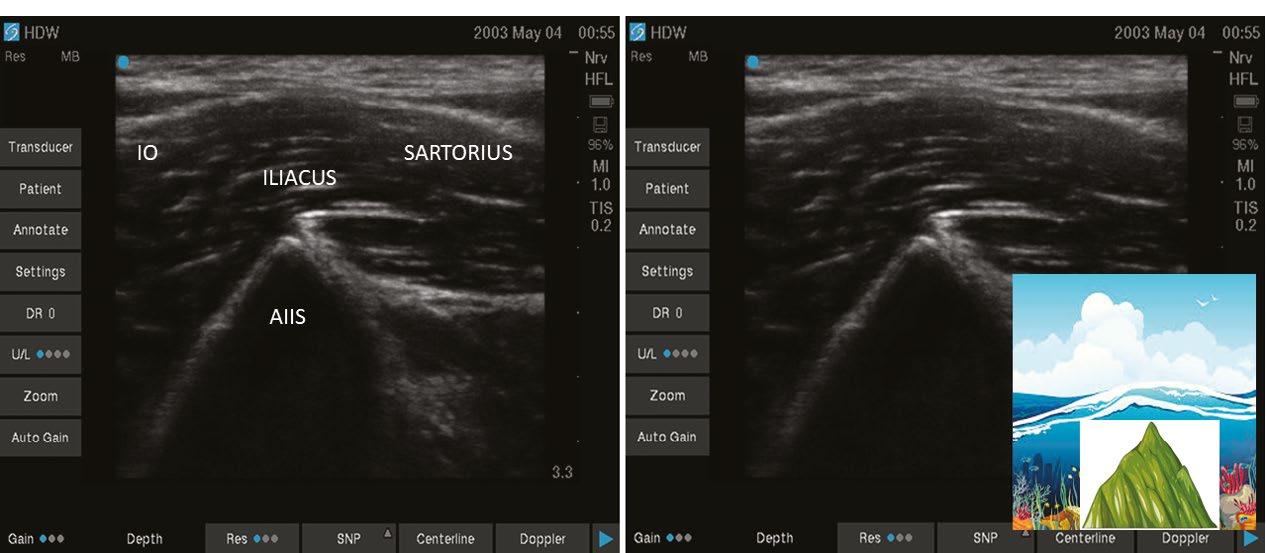
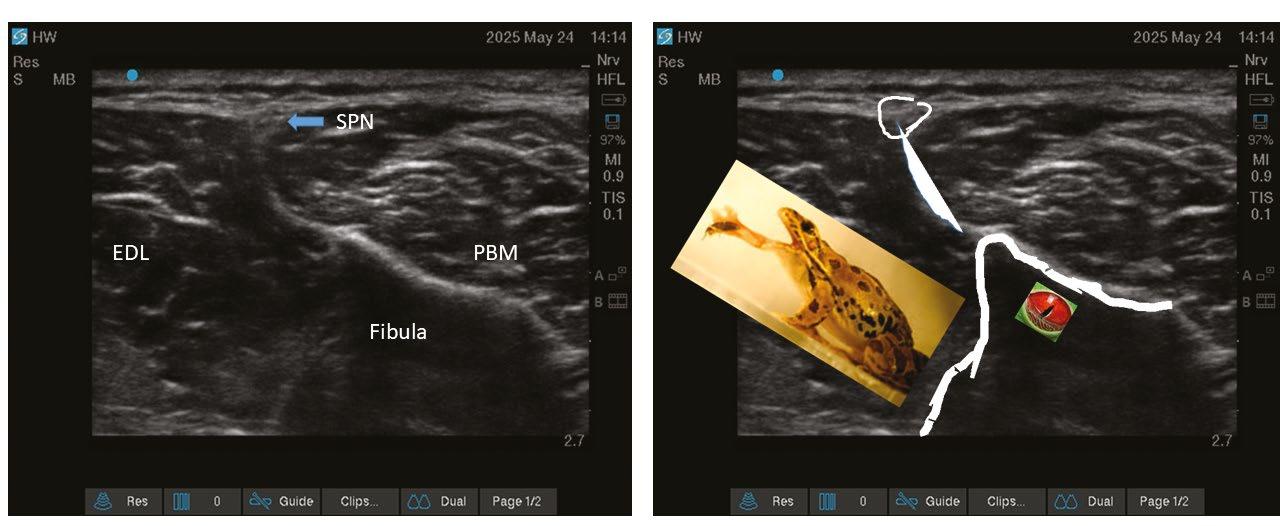
Another focus for AI in anaesthesia lies in real-time analysis of ultrasound scanning.[8] Multiple algorithms have been developed to segment and apply colour to greyscale ultrasound live images. Despite promising progress, the evidence base gathered to assess and appraise the utility of these various tools remains insufficient. Studies are too heterogenous, use differing performance metrics and ground truth definitions, or are simply not made public due to commercial sensitivity.[9]
So, despite promise, clinicians could be forgiven for wondering quite how, where, and when AI’s benefits might arrive at the clinical environment to make a difference to their patients.
Reshaping AI innovation by empowering demand
To invert the techno-centric approach to innovation, we must now ask: where are the key clinical pain points which may be addressable by an AI-based solution? And where would such tools meaningfully enhance anaesthetic practice to increase the provision of care or improve patient outcomes?
These questions form the basis of a new project, delivered in partnership with the Association of Anaesthetists and health innovation specialists UCLPartners. This research will be the first attempt to identify and explore the highest priority clinical problems across anaesthesia, perioperative medicine, and pain management which may be amenable to an AI-based solution. This process of clinician-led demand signalling will also seek expert input from stakeholders from across the healthcareindustry-academic network to ensure solutions are examined from all perspectives.
The study begins with an open survey inviting anaesthetists, perioperative medicine physicians, and pain specialists of all grades and subspecialties, to submit their highest priority clinical problems which could be alleviated by an AI-based solution. The second stage of this project will involve a consensus-generating process to prioritise these clinical problems, ultimately identifying a top 10.
A strong emphasis on a collaborative approach to AI development is central to creating the impactful AI of the future, starting at the earliest inception of each tool. In line with this, the prioritisation activities will integrate views of patients, NHS organisations, industry partners, academics, and policymakers. Finally, a series of roundtable discussions will be held, involving all of the above stakeholder groups, to further refine the proposed AI applications and explore the major realworld challenges and opportunities presented by them.
Impact and vision
By clearly signalling the demands of anaesthetists and affected stakeholders, this project will provide a mandate to guide innovation, strategy and investment towards AI-based interventions that will positively impact patients and clinicians. The solutions, produced through interdisciplinary dialogue, are more likely to be robust and resilient, having been formed in a setting which lays the foundation for long-term partnerships and collaboration.
A secondary consequence of this work is to empower clinicians to take greater leadership in the innovation space, including being the inventors or co-inventors of change. NHS Digital Transformation sets out a vision of collaborator ‘archetypes’ involved in AI development,[10] and while this provides a useful framework for thinking about the skills required to bring AI to market, we envisage a role for clinicians across all stages of development. This echoes existing calls to reframe clinicians not solely as users but as highly knowledgeable architects of technological innovation, to achieve solutions with maximal utility and commercial viability.[2]
Once established, the potential exists to scale this concept of clinically-orientated and stakeholder-informed demand signalling across different healthcare settings. Healthcare professionals are often siloed by designations and departments, yet in practice, shared environments and skills mean clinicians have common experiences, particularly in how they interface with medical technology. By considering the ways in which differing problems may converge, the opportunities for multi-specialty collaboration multiply.
To begin the first step on this exciting journey and reshape the innovation pipeline, we are calling on all anaesthetists to share their ideas for the future of artificial intelligence within the specialty, to collectively demand the changes we wish to see in the pursuit of more clinically-relevant AI.
Joseph Harris
Innovation Fellow in Anaesthesia, University College London
Hospitals NHS Foundation Trust
Honorary Research Fellow, University College London
James Bowness
Consultant Anaesthetist, University College London Hospitals NHS Foundation Trust Honorary Associate Professor of Anaesthesia, University College London
Kelly Lin UCL Partners
All Association of Anaesthetist members in the UK and Ireland are invited to share their ideas on the clinical pain points that AI could help address in anaesthesia, perioperative medicine, and acute pain management. The survey is now open and can be found using the QR code or link below.
www.bio.site/anaes.AI
References
1. Gerhold M. The Health Foundation (Blog), 2025. Available from: https:// www.health.org.uk/features-and-opinion/blogs/10-year-health-plan-weneed-to-move-from-techno-optimism-to-techno Accessed 20/8/2025.
2. Bowness JS, Kos S, Wiles MD. Artificial intelligence in healthcare: medical technology or technology medical? Anaesthesia 2025.
3. Lawrence A, Hardie T, Zapantis I, et al. AI in London healthcare: The reality behind the hype: UCL Partners, The Health Foundation, 2025 [Available from: https://s42140.pcdn.co/wp-content/uploads/UCLP-AIin-London-healthcare-03.25-final.pdf Accessed 16/8/25.
4. Lee NK, Kim JS. Status and Trends of the Digital Healthcare Industry. Healthc Inform Res. 2024; 30(3): 172-83.
5. Habli I, Sujan M, Lawton T. Moving beyond the AI sales pitchEmpowering clinicians to ask the right questions about clinical AI. Future Healthc J. 2024; 11(3): 100179.
6. van der Meijden S, Arbous M, Geerts B. Possibilities and challenges for artificial intelligence and machine learning in perioperative care. BJA education 2023; 23(8): 288-94.
7. Challen R, Denny J, Pitt M, et al. Artificial intelligence, bias and clinical safety. BMJ Qual Saf 2019; 28(3): 231-7.
8. Bowness J, El-Boghdadly K, Burckett-St Laurent D. Artificial intelligence for image interpretation in ultrasound-guided regional anaesthesia. Anaesthesia 2021; 76(5): 602-7.
9. Bowness JS, Metcalfe D, El-Boghdadly K, et al. Artificial intelligence for ultrasound scanning in regional anaesthesia: a scoping review of the evidence from multiple disciplines. Br J Anaesth. 2024; 132(5): 1049-62.
10. Developing healthcare workers’ confidence in artificial intelligence (AI): Workforce archetypes: NHS England Workforce Training and Education; 2023 [Available from: https://digital-transformation.hee.nhs.uk/buildinga-digital-workforce/dart-ed/horizon-scanning/developing-healthcareworkers-confidence-in-ai/chapter-2-workforce-archetypes/defining-thearchetypes [Accessed 25/9/25].
Two Monitoring Solutions in One Device
Flexibility to view the display of the EEG signal and spectrogram in different positions
Adjustable spectrogram colour scaling to aid with the interpretation
Optional trends in the spectrogram of Spectral Edge Frequencies SEF50 and SEF95
For questions or more information on Conox
References:
Conox® 2D is a non-invasive depth of anaesthesia monitor that aims to assess the hypnotic and analgesic effects of sedation and general anaesthesia through a single sensor that offers two monitoring solutions in one device. qCON index assesses the patient’s state of consciousness during sedation and general anaesthesia procedures1, while qNOX index provides the patient’s probability of response to noxious stimuli1,2. Additional features include Burst-Suppression Ratio (BSR) and Electromyography Index (EMG).
Marketing.Medtech@fresenius-kabi.com or scan the QR code
1.E.W. Jensen, J.F. Valencia, A. López, T. Anglada, M. Agustí, Y. Ramos, R. Serra, M. Jospin, P. Pineda and P. Gambús, “Monitoring hypnotic effect and nociception with two EEG-derived indices, qCON and qNOX, during general anesthesia”, Acta Anaesthesiologica Scandinavica, 58(8), 933-941, Sep 2014. 2.U. Melia, E. Gabarrón, M. Agustí, N. Souto, P. Pineda, J. Fontanet, M. Vallverdú, E.W. Jensen and P. Gambús, “Comparison of the qCON and qNOX indices for the assessment of unconsciousness level and noxious stimulation response during surgery”, Journal of Clinical Monitoring and Computing, 31 (6), 1273-1281, Oct 2016.
Reflection in the age of AI: Time to go back to basics?
Most of my friends and colleagues (resident anaesthetists, GPSTs, medics, all) are using ChatGPT to write reflections for their portfolio. With simple guidance it can quickly invent a scenario focused on the desired area of the curriculum, complete with learning points and ideas for future changes in practice. Writing a reflection used to take 30 minutes. Now it takes 30 seconds. The same approach can be used when sending SLEs and writing reports on quality improvement projects. I applaud their initiative.
Writing a reflection does not make a doctor reflective. Almost all of my colleagues are genuinely reflective and demonstrate it when discussing their cases, whether it’s over a coffee in the staff room, quietly in the corner of a pub after a shift, or in a rant to a partner on the drive home (sorry Nina!). The most valuable reflections happen with a mentor, but it’s increasingly difficult to access mentorship with rotational training. In the Northern deanery, we have a new educational supervisor (ES) every six months. In my experience, our infrequent meetings are focused on the portfolio rather than interesting/difficult cases and aspirations for the future. Perhaps this reflects some personal shortcoming – I know several trainees (incidentally all female) who can quickly form these meaningful relationships in new placements, sometimes even meeting outside of work to discuss careers. Many (I think most) of us however struggle to develop this sort of relationship quickly enough – before you know it the six months is up and we start again, trying to convince a new batch of trainers that we’re not complete numpties. This must be especially tricky in anaesthetics, where big departments, solo working and plenty of on-calls mean you might only have a couple of shifts with each consultant during a placement.
This is an excellent moment for the Association (and College) to embrace the future and improve our experience as
residents. In a few years, our portfolios will be full of AIgenerated nonsense that we’ve barely read, and that no one else will ever look at. It’s a waste of everyone’s time. Instead, why not mandate spending one hour a fortnight with a named mentor to discuss cases. With an email in advance of a placement, college tutors could pair residents with an ES/mentor who has similar interests. Fewer, higher-quality in-person learning events could be documented together, rather than a raft of half-hearted SLEs with the comment ‘great work, keep going’ attached. The College could recommend a minimum number of SLEs to suppress the ‘portfolio arms race’, where expectations on volume seem to rise year on year. Written reflections could be saved for serious events, and a comment on reflective practice could be added to the ESSR if needed. Universities and schools are moving back to in-person assessment to combat the negative impact of AI.
The Association should use this opportunity to trust its members, encourage mentorship and lobby the College to reduce the burden of paperwork that benefits no one and distracts from actual learning.
Matthew Bickerton
ST4 ICM/Anaesthetics, Northern School of Anaesthesia and Intensive Care Medicine
Responses:
Plus ça change… what exactly is training for?
I started my anaesthetic training in a pretty forward-thinking department in 2002. At that time, the department didn’t possess an ultrasound machine or a video laryngoscope. I learned the landmark technique for inserting central lines and nerve blocks using nerve stimulators and presented pieces of paper to consultants to tick to say I could do an epidural or a rapid sequence induction. The day-to-day business of developing as an anaesthetist was (mostly) enjoyable but the assessments felt like a tick-box procedure that didn’t capture how we were performing as doctors.
Over 20 years later and it feels like the discontent about training hasn’t changed all that much. The pieces of paper are gone, replaced with a doughnut that needs to be turned green on a website, and residents now need to prove their competence in techniques that I am still learning myself. Portfolio entries are supposed to help residents and their trainers shape a discussion about their development. The success of the endeavour depends a lot on the resident considering what they need to know and do to function as an autonomous anaesthetist in their chosen area and taking some responsibility for guiding themselves towards that, and the supervisor supporting that process. Reflection is a part of that – as trainers we are not looking for essays with the flourish that can be provided by ChatGPT, but for evidence that residents are thinking about how they work with patients and colleagues, and how they learn and develop from experience. This can be from conversation with a trusted colleague or by jotting notes down. We should bear in mind that entries in the portfolio are not privileged and may be discoverable in the event of legal or regulatory proceedings [1] – a subtlety that ChatGPT may not be able to parse.
Residents will have different needs at different stages of their career. This might include mentoring, coaching, exam practice or direct and immediate feedback in the clinical environment. There probably isn’t a one-size-fits-all approach that will solve current discontents. The problem of ‘half-hearted’ SLEs can be addressed by using tools such as LOAF/BREAD [2] checklists at the start and end of lists rather than abolishing them altogether.
Doing training properly takes time and effort. It is an investment in the future of the profession and the service, and units that do it well have better patient outcomes. The constant demand to increase throughput and reluctance of trusts to pay for supporting professional activities adds to the challenge of delivering high-quality training. The consultant body is reporting increasing levels of burnout and exhaustion. No one can train or be trained when they are struggling to keep up with the workload. We should look to the basics – providing doctors with the time, space and resources for training. We may find we don’t need to change anything else if we get that right.
Chloe Fairbairns
Consultant Anaesthetist, James Cook University Hospital
References
1. Williams, N. Gross negligence manslaughter in healthcare: The report of a rapid policy review, 2018.
2. The Educational Checklist, https://loafnbread.com/home/
Thank you for the opportunity to reply. This letter comes at a time when the use of AI in education, training and clinical practice is a hot topic within the NHS and royal colleges alike. Reflective practice by medical professionals is a lifelong requirement for revalidation with the GMC. As a consultant of 25 years, I wrote two reflections for my appraisal 1 month ago. It is not something that is going away nor something that has become less valid just because AI has provided a potential shortcut.
For residents, evidence of reflection remains an annual requirement for their ARCP. That said, as with many aspects of the new curriculum, it can be evidenced in a number of different ways. It can be written (a reflection on the year being reviewed or in response to a serious incident) or it can be done verbally with a mentor and documented in the ES report as having happened. The wording in the RCoA ARCP checklist is as follows and in my region that is what is recommended:
‘There is no requirement for a set number of reflections, but the trainee must provide their ES (and the ARCP panel) with evidence that they are a reflective practitioner, and they are able to learn from excellence as well as errors. This may be undertaken verbally.’
The benefits of debriefing (both formal and informal/social) have been well established. Mentorship is very much something we are supporting as a college. Dr Nancy Redfern, a long-standing advocate of the mentor programme, has been working with our network of College Tutors to provide training and to promote the role of the mentor. As this work expands there are already examples of good practice around the country with mentors being allocated in the North West by the Regional Adviser for residents post Final FRCA to help with navigating Stage 3 and to help with preparation for CCT. As a college we will continue to work with our training networks to spread good practice.
Sarah Thornton, Jon Chambers and Chris Carey RCoA VPs and Chair of Training Committee
Continued on next page >
AI-generated reflections: Missing the point
We read Bickerton’s thought-provoking article on the challenges that we face to ensure training and its regulation stay current with emerging technologies. The author raises an interesting point; how do we ensure individuals are maintaining reflective practice as AI becomes able to generate entries into the Lifelong Learning platform (LLP)? Perhaps, as the author outlines, the key is a more human approach; less volume, more detail and a better appreciation of the nuances in what we do.
Reflective writing in its current format can feel like an exercise solely designed to illustrate that the resident has fulfilled certain curriculum objectives, disregarding the true value in earnest reflection. The physical process of writing may allow many residents to articulate thoughts they struggle to express verbally. Alternatively, many find that candid discussions in the coffee room with colleagues or during a long case allow for contemplative reflection. Perhaps the key is flexibility, enabling residents to reflect in the manner most effective to them. Currently the curriculum does not facilitate or recognise this.
Mentoring can be extremely valuable, and the Association has a free, nationwide scheme partnering trained mentors and mentees. This, in addition to local schemes which the author describes, can be a valuable source of reflection. Mandatory meetings with a designated individual come with potential concerns; the sessions may not facilitate the space to have honest and open discussions - being vulnerable with another colleague is difficult. We believe ‘unofficial’ conversations in the coffee room are no less reflective than formal meetings. The College should encourage meaningful conversation with supervisors in any format. Framed as a catch-up, a check-in, or a chance to discuss interesting cases, they may gently open the door to honest reflection. The Association's ‘Coffee and a Gas’ meetings may provide this outlet: a weekly meeting for residents to discuss their lives and reflect on challenging cases. The opportunity to be able to document attendance and engagement at meetings like this on LLP would be a step in the right direction.
As use of AI becomes more mainstream, we must review our training and its regulation. We believe engaging in regular reflective practice should be in the format most comfortable for the resident, and that to emerge with maximal benefit, one must engage with other human beings. True reflective practice is crucial to maintaining the humanity in medicine, and whilst AI will certainly have a future role, we must take care to ensure we do not lose the ability to improve our practice based on our own personal assessments.
Ashleah Mcculloch
Resident Doctor, NHS Greater Glasgow and Clyde
Andreas Sotiriou
ST6 Anaesthetic Resident Doctor, Guy’s and St Thomas’ NHS Foundation Trust, Department of Anaesthesia and Perioperative Medicine, London, United Kingdom
Written on behalf of the Association of Anaesthetists Resident Doctors Committee.
Soft, puffy if you're lucky foccacia bread
Top tip:
Oil your rosemary so that it doesn't burn or turn to charcoal!
Due to the unusually hot weather this year, we had a bumper harvest of tomatoes on our allotment.
Having exhausted ideas for dishes - we were finally at the 'we'll have to make tomato soup' stage!
We searched online and found some great Italian foccacia bread recipes to accompany our homemade soup. The following recipe is a tweaked, tried and 75% successful version of a multitude of versions that we made!
A simple, homemade classic Italian foccacia bread with fresh rosemary.
Serve with soup or as a side to pasta dishes.
Serves 12 (or 4 very hungry people!)
Prep: 25 mins
Proving time: 1 hr 45 mins
Bake: 20 mins
Chris Steer
Digital Designer, Association of Anaesthetists
Ingredients
500g strong bread flour (extra for dusting)
7g sachet of dried fast action yeast
2 tsp fine sea salt
340-380ml lukewarm water
5 tbsp olive oil
Sprinkle of good rock sea salt (for topping) A few sprigs of freshy picked rosemary
Method
1. Add the flour into a large mixing bowl, then mix the sachet of yeast into one side of the flour, and the fine salt onto the other side (separating prevents the salt from killing the yeast).
2. Mix everything together.
3. Next make a small well in the middle of the flour and add 2 tbsp olive oil and 340-380ml lukewarm water, add it gradually until the dough has a slightly sticky consistency.
4. Sprinkle some flour onto your worktop surface and then add the dough onto it. Knead for about 7 mins until your dough is soft and unsticky. Next put the dough into a clean bowl, cover with cling film or a tea towel and leave to prove for 1 hour until it (hopefully) doubles in size!
5. Add some greaseproof paper to a shallow rectangular baking tin (25 x 35cm) and brush with oil. Tip the dough into the tin and then stretch to fit. Cover with cling film or a tea towel and leave to prove for further 35-45 mins.
6. Preheat your oven to 220C/200C fan/gas 7. Poke your fingers into the dough to make lots of dimples.
7. Mix together 1½ tbsp olive oil, 1 tbsp water and drizzle over the bread. Add freshly cut rosemary, a sprinkle of rock salt into the dimples in the dough. You can also try adding alternatives like olives or tomatoes.
8. Bake for 20 mins until light golden brown. Whilst the bread is still hot, drizzle some olive oil, cut into squares and serve whilst still warm.
Irish Standing Committee news
The annual meeting organised by the committee takes place this year in a new venue – The Dublin Royal Convention Centre on 15 November. This is very central, right behind Dublin Castle and near The Chester Beatty Museum. As in past years it is held on a Saturday, the day following the National Anaesthesia Patient Safety Conference (NAPSAC). It is hoped delegates may combine the two educational activities. The NAPSAC meeting is being held in The Radisson Blu Hotel Golden Lane which is adjacent.
The Saturday programme includes the first oral presentation prize at this meeting for doctors in training. The topic in consideration is the future relationship of anaesthesiology and intensive care medicine. There are presentations on standardised national airway equipment, assessing neuraxial blocks and a session on workforce in Ireland. The workforce session includes Dr Michael Dockery the National Clinical Lead, Dr Emma Wain our SAS chair and Prof Anthony O’Regan, medical director of National Doctors Training and Planning in Ireland. The committee is finalising a briefing on anaesthesiology workforce in Ireland.
These combined meetings have often been referred to as the Winter Anaesthesia Weekend in Dublin. Winter, we hear you say –in November? The Met Office indeed defines winter as starting in December which aligns with the Gregorian calendar. In Celtic tradition however, winter begins in November following the festival of Samhain which marks the end of harvest season. A theme of Samhain was the belief that the barrier between the living and dead was at its weakest, allowing spirits to move between worlds. This formed the traditions around Halloween which were brought to North America by Irish and Scottish immigrants in the 19th century.
Following the September Annual Congress in Aberdeen, David Honan and Rory Page have finished their terms as convenor and hon secretary. Their contributions over many years as Irish Standing Committee members are gratefully acknowledged. John Loughrey and Sam Dawson have been appointed to the roles of Convenor and Hon Sec respectively for the next 3 years. We hope to welcome new committee members in 2026 and will be calling out for candidates.
Location: Dublin Royal Convention Centre, One Le Pole Square, Ship Street Great, Dublin, D08 E6PD, Ireland
Chairs: Prof David Honan, Convenor and Dr John Loughrey, incoming Convenor, Irish Standing Committee
Irish Standing Committee oral presentation prize
Irish medical students and trainees are invited to submit a 500-word synopsis of a presentation on the topic of Are anaesthesiology and critical care medicine headed for a messy divorce? This is the perfect opportunity to share your views with your peers, showcase your presenting skills, develop your portfolio and win cash prizes. Register your interest for the event to find out more.
100% of attendees to
Scan QR code to book now
Meet the new Irish Standing Committee officers
Where do you work?
What do you do in your leisure time?
I have been a consultant for 23 years. My primary hospital is the Rotunda Hospital in Dublin. It is the oldest working maternity hospital worldwide having been established in 1745. I also work at the Mater Misericordiae University Hospital and The Mater Private Hospital, both on Eccles Street in Dublin.
Why did you join the Association?
When I started anaesthesia back in the early 1990s, I joined within my first few months. I remember having to get several existing members to sign the application. It all felt very clubby, and I was very pleased see both the Anaesthesia journal and Anaesthesia News drop into my letterbox. I’ve gone paperless now, however. Direct debits are largely to thank for my annual renewal. The Association move to facilitating this from euro accounts was very wise. Having served as treasurer of The College of Anaesthesiologists I know the importance of debits! The professional support of the Association has been a reassuring presence over my career.
What motivated you to join the committee?
Having been a resident member in the late 1990s and subsequently a consultant member in the 2000s, I was aware of the role and importance of a voice for the specialty outside of the postgraduate training bodies and medical unions. It is a great honour to serve as convenor. There have been 10 individuals who have served in this role since our committee’s formation in 1988 and I have known all of them.
What are your goals for the committee?
I hope to hear what the membership residing in Ireland wish to see us achieving. The Sláintecare healthcare programme is changing the way the service is organised, and we need to ensure we advocate for high standards. We plan to update our Links network and improve communication pathways. The committee has always sought to advocate for those working in the private sector and I hope we can respond to current difficulties. We will of course continue to run educational events, member surveys and support our membership while focusing on patient safety.
I took up golf but never invested the time to practise. So, on many weekends a frustrated figure can be observed out in Dublin Bay on the Bull Island links. I also support Leinster Rugby who’ve enjoyed a talented squad these last few years. It won’t last forever.
Can you share a bit about your journey into anaesthesia, where you now work and what inspired you to choose this specialty?
Oddly, I started anaesthesia training in South Africa despite growing up in Northern Ireland (NI) and going to Queen’s University in Belfast. I was just married at the time, and we felt like some adventure. I was instantly hooked on the way deep physiology, pharmacology and physics meet exciting practical procedures and satisfying patient interactions. I completed the South African Diploma in Anaesthetics before deciding to return home. I then trained in NI and worked there as a consultant for five years before adventuring out West. I am now lucky enough to work as a consultant anaesthesiologist, with a fantastic team, in Sligo University Hospital.
Dr John Loughrey Convenor
Dr Sam Dawson Hon Secretary
What do you see as the biggest opportunity or challenge currently facing the field of anaesthesia in Ireland and the UK?
One of the biggest challenges for us as a specialty is the increased demand for our service. How do we accomplish this efficiently and safely in the context of inadequate resources and workforce? Navigating a way through the current difficulties surrounding the relationship between intensive care and anaesthesia training is difficult and delicate work. I’m hopeful all involved will find a solution that is good for patients and leads to the flourishing of our specialty. Patients languishing on long waiting lists for surgery are always on our minds. I think anaesthetists can play an incredible role in managing and overcoming this challenge. This leads me to think of the interaction between the public and private sectors in healthcare in Ireland and the UK. This is an area I am particularly interested in, and I would love to see reform of many of the aspects of anaesthesia in the private sector.
What motivated you to join the committee, and what do you hope to contribute or achieve during your time on it?
I think the Association has an important role to play. I love training and education and am aware of the resource the Association has always been to our specialty. I am committed to advocacy and fairness, both within our specialty, and in the areas it relates to the wider healthcare community. We are often one of the largest specialties in our hospitals, and one of the most dedicated and enthusiastic. Yet I sometimes feel we are overlooked and underappreciated. Maybe we make it look too easy! I would like our specialty to be as healthy and strong as possible so anaesthetists can have a greater influence in how healthcare is planned for and delivered in the UK and Ireland.
In what ways do you think the committee can make a tangible difference to practising anaesthetists and the wider medical community?
I think we all want a sufficient share of resources to provide better care for our patients. We want to maintain safe standards but would love to provide more efficient care so we can maximise our resources in the face of increasing demand. We want to be respected in our profession, listened to, and treated with a dignity that matches our own levels of professionalism. We want the time and resource to inspire our residents and imbue them with a love of our specialty. We want our specialty to receive the technological and electronic support it needs to provide an efficient and effective service. We want a seat at the table as the government works to reduce waiting times for surgery. We want clarity from our councils and colleges on the issues that destabilise our specialty. We want a private sector which provides the highest standards of safety, efficiency, transparency and fairness in anaesthesia. I think the committee has an important role to play in all of these areas and I certainly will be working hard to accomplish all I can to improve our specialty.
Outside of your clinical work, what do you enjoy doing or what keeps you grounded?
I suppose I often don’t notice or feel work as a stressful and pressured environment. It does leave me tired though at times and in need of rest. I find being outside and in nature one of the best ways to achieve this. I have challenges sitting still so tend not to be watching the sunset. I do love, however, to be out fishing, spearfishing, swimming, running, stalking, hiking and birdwatching. I also love binge-watching every Star Wars movie and series in the winter with my wife and three kids.
What advice would you give to young anaesthetists or trainees in Ireland who are just starting their journey?
Get your exams done. Then find the area that you love within the specialty and pursue it. And join the Association!
Medical elective in the Philippines
For my medical elective, I spent six weeks at a tertiary teaching hospital in Iloilo City, the Philippines. The hospital, with a capacity of approximately 300 beds, provides both public and private healthcare. My placement was split into two placements: three weeks in anaesthetics and three weeks rotating through the Intensive Care Unit (ICU) and Emergency Department (ED).
I chose the Philippines to gain insight into a healthcare system vastly different from the NHS, with the aim of broadening both my clinical knowledge and cultural understanding. The healthcare system in the Philippines is a mixed model, consisting of public and private providers. PhilHealth, a government-run health insurance scheme, aims to offer coverage for all Filipinos. However, access to healthcare remains inequitable, with many patients unable to afford even basic treatments. This often leads to late presentations and more severe disease pathology than typically seen in the UK.
Anaesthetics placement
During my anaesthetics placement, I observed several differences in clinical practice. Each procedure began with the patient secured in a crucifix position on the trolley, followed by a time-out and a spoken prayer. Religion, particularly Roman Catholicism, is deeply embedded in Filipino culture and healthcare practice. Crucifixes were present above each bed, and religious statues were commonly found throughout the hospital. This spiritual dimension also influenced patients' health beliefs, with some favouring non-medical, or faith-based interventions.
Batad Rice Terraces, North Luzon, Philippines - stock photo
Anaesthetic techniques were broadly similar to those in the UK, but with some notable differences. Spinal and epidural anaesthesia were preferred over general anaesthesia. This choice was driven by both cost considerations and the risks associated with general anaesthesia in a resource-limited setting. Total intravenous anaesthesia (TIVA) was rarely used; instead, Sevoflurane was the agent of choice for induction and maintenance, in addition to a propofol bolus for induction. Premedication typically included Midazolam and an opioid, with Suxamethonium and Rocuronium used interchangeably as muscle relaxants. Intravenous access was usually established during pre-operative assessment and care, but in difficult cases, venous cutdown was occasionally performed, a technique now rarely used in the UK.
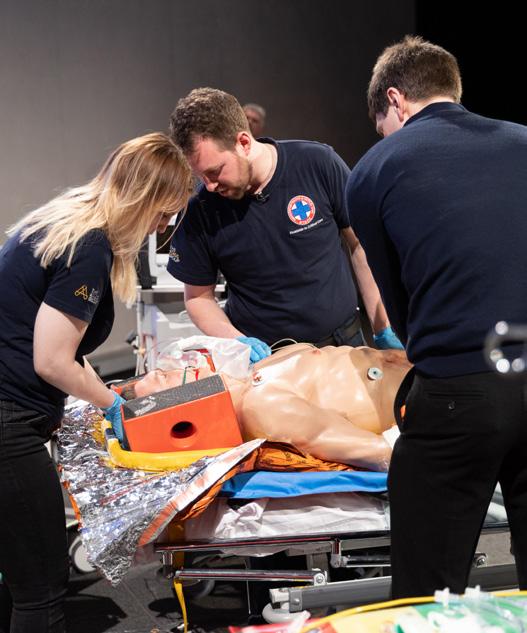
One particularly interesting case I saw was an Omphalocele repair in a 5-day-old neonate. For context, the patient was born via Caesarean section, normal for gestational age and born to a diabetic mother. In addition to an omphalocele, the baby had a cleft lip and palate, which further complicated anaesthesia and intubation. As a result, this case took meticulous planning, and 7 anaesthetists were present at the time of induction. Due to the size of the patient, manual ventilation was required throughout the procedure, as the anaesthetic machine could not deliver the required tidal volume at an appropriate airway pressure. The procedure was completed with no major complications, however, the patient did have episodes of low oxygen saturations due to bronchospasm and required Salbutamol.
ICU and ED
the patient is allocated, with seniors supervising. An interesting case I observed in the ICU was a female patient with toxic epidermal necrolysis (TEN) secondary to non-steroidal anti-inflammatory usage. She had the typical clinical findings of TEN with skin damage, resembling a severe burn, over her face and trunk, also involving her mucous membranes, including her eyes.
Each procedure began with the patient secured in a crucifix position on the trolley, followed by a timeout and a spoken prayer.
The ED is run quite differently to the UK as they do not have emergency doctors, and much like ICU, medical students run the shop floor and specialty doctors oversee them. The ED was overrun, hot and many patients were turned away due to lack of space and ability to fund treatment. In the ED, many patients were intubated without adequate sedation which was distressing to watch, and the indications were unclear. Common presentations included strokes secondary to untreated hypertension, with many patients presenting with a systolic blood pressure of over 200mmHg regularly. Other presentations included; diabetic foot infections, road traffic collisions, end-stage renal disease, pneumonia and tuberculosis. The comorbidities are similar to the UK, however, the main difference as I have already mentioned was the severity of disease and the time of presentation.
Overall, this elective broadened my clinical perspective, deepened my appreciation for the adaptability required in resource-limited settings, and reassured my interest in anaesthesia as a career choice. I am incredibly grateful to the Association of Anaesthetists for making this invaluable experience possible with their generous grant.
The layout of the ICU was similar to the UK; however they do not have ICU doctors. Instead, medical students look after the patients under the specific speciality
Harriet Jenner University of Exeter
The ClearLite™ anaesthetic face mask shows a 72% reduction in environmental impact compared to a standard PVC mask.1
The ClearLite™ anaesthetic face mask shows a 72% reduction in environmental impact compared to a standard PVC mask.1
The ClearLite™ anaesthetic face mask shows a 72% reduction in environmental impact compared to a standard PVC mask.1
A clear choice to reduce your impact on the environment
A clear choice to reduce your impact on the environment
A clear choice to reduce your impact on the environment
For further information please visit: www.intersurgical.co.uk/info/anaestheticfacemasks-singleuse
For further information please visit: www.intersurgical.co.uk/info/anaestheticfacemasks-singleuse
For further information please visit: www.intersurgical.co.uk/info/anaestheticfacemasks-singleuse
My anaesthetic elective in Kuala Lumpur, Malaysia
I was given the opportunity to spend my medical elective observing the anaesthetic team at University Malaya Medical Centre in Malaysia. During my time here I was able to gain valuable insight into the clinical and cultural practices and was exposed to many interesting cases. My time here was split between pre-operative clinics and operative theatres which provided insight into the varied responsibilities of anaesthetists.
Pre-op clinics
Whilst in pre-operative clinics I paid attention to optimising post-operative outcomes. The anaesthetists used multiple techniques to assess airway, such as neck range of motion, Mallampati scores, and thyromental distance. The use of multiple techniques was comprehensive and allowed the anaesthetists to make informed decisions regarding equipment for intubation e.g., standard vs video laryngoscope.
I performed blood tests to assess for anaemia and bleeding risk. This was particularly important in patients with clinical anaemia, haematological disease or those scheduled for procedures with blood loss >500mls. In cases of iron deficiency anaemia, to prevent cancellation of the patient’s operation, they would be brought back to clinic to receive IV iron. There was a strong focus here on patient blood management with the goal of optimising pre-operative anaemia prior to surgery to reduce the occurrence of post-operative complications and the need for blood transfusions.
The clinics also exposed me to just how diverse Malaysia’s population is. Malaysia is a beautiful blend of diverse cultures and languages. When patients came in, they were asked first their preferred language ensuring that patients can express themselves comfortably. The language barrier for me meant the use of respectful nods and greetings were essential.
Theatre time
My time in theatres exposed me to so many procedures. I witnessed everything from hysterectomies to paediatric cardiac procedures. The anaesthetists demonstrated how to use tidal volume, capnography, blood pressure and pulse to assess depth of anaesthesia. Over time, I gradually became more familiar with the anaesthetic monitoring machine and how to interpret it. In addition to standard anaesthetic monitoring there were cases that also used EEG/EMG monitoring. I initially had only seen intraoperative EEG/EMG monitoring during neurosurgery procedures, but here they were often used in elderly patients to assess depth of anaesthesia to reduce the risk of post-op delirium. This stood out to me as a meticulous way to prevent delirium in at-risk patients.
I had the opportunity to assist in bag-mask ventilation and laryngeal mask airway insertion and became more confident in my airway skills by the end of the elective. I saw the anaesthetists perform more challenging intubations such as a double-lumen intubation for a left-lung lobectomy case. This type of intubation was much less straightforward and involved the use of bronchoscopy to identify the bronchi and confirm the position of the endotracheal tube. I really admired the focus and skill needed to perform this.
Teaching
The anaesthetists I shadowed had a strong commitment to education and were keen to teach and involve me. I had the opportunity to join a simulation session with the Universiti Malaya students on transporting a critically ill patient. I learnt how to use the A-E model to identify which equipment is necessary for transfer and why. It was useful to understand how to calculate how much oxygen, fluids and medication a patient needs to be kept stable during transfer. It was also fun being able to practise how to physically transfer a patient.
I also joined a teaching session on airway management where we discussed different clinical scenarios and decided which airway device would be most suitable for each scenario. We then had the opportunity to practise administering oxygen using nasal cannula, a simple face mask, venturi mask and a non-rebreather mask. It was a fantastic opportunity to practise clinical reasoning.
Conclusion
Overall, I had an enjoyable experience, and the elective was an insightful learning opportunity that not only broadened my clinical understanding but also my understanding of how to deliver quality care to such a diverse population.
Makuochukwu Ezenwa University of Birmingham
The flavour of anaesthetics: A taster week
A ‘taster week’ is an opportunity given to UK Foundation Programme doctors to spend up to five days gaining experience in a specialty in which they have not previously worked. This is aimed at promoting career reflection and helping newly qualified doctors develop insight into the work and ‘lifestyles’ of different specialties.
I arranged a week working in the Anaesthesia Departments in the Royal Glamorgan and Prince Charles Hospitals, two district general hospitals in Cwm Taf Morgannwg University Health Board in South Wales. The week was arranged and shaped through a comprehensive timetable that would allow me exposure to different aspects of anaesthesia and provide topics for practical and academic learning, discussion and reflection.
With only limited exposure to anaesthesia in medical school, it remained much of an enigma to me. I was keen to have an immersive experience in the specialty. I hoped that by the end of my time there, I would have a greater sense of the depth and breadth of the specialty and whether it could offer me a satisfying and stimulating career choice.
Common folklore cites that all anaesthetists love cycling, crosswords and making coffee. The first morning of my taster week, there was not a shred of Lycra in sight and after formal introductions, I found myself in the anaesthetic room, eagerly awaiting the arrival of the first patient.
of course, a whole different matter. I quickly realised how nuanced and high-stakes the process is. Each intubation came with a brief pause and unspoken moment of focus as the anaesthetist visualised the epiglottis and guided the tube past the cords. Even in cases they had managed before, that moment carried weight.
Each anaesthetist had a particular approach to airway management, influenced by personal preference and patientspecific factors. I was particularly struck by the way the anaesthetists were constantly assessing risk to ensure their patients’ safety during surgery. It was clear that anaesthetic plans weren’t routine, they were personalised to each patient, underpinned by preparation for any eventuality.
What stood out was the calm precision in their work. Whether facing a difficult airway or responding to a monitor alert, the anaesthetist’s demeanour remained composed under pressure. The emphasis on pre-oxygenation, structured airway assessments, and clear escalation plans revealed a mindset rooted in anticipation rather than reaction.
Common folklore cites that all anaesthetists love cycling, crosswords and making coffee
Once the airway was secure, the focus became ventilation and vital signs. The monitors, which had once seemed like an overwhelming wall of cryptic numbers and alarms, started to make sense. I witnessed how the anaesthetists interpreted subtle changes in end-tidal CO2, heart rate, and blood pressure and observed how they converted this complex data into clear clinical decisions. Each decision and adjustment during surgery seemed small on its own but combined reflected a deep understanding and working expertise of physiology, pharmacology and a fundamental responsibility for keeping patients safe.
The week began with a focus on airway management. I had some basic knowledge of Guedels and LMAs, mainly from fighting them into a few poorly mannequins during medical school, but watching anaesthetists secure real airways was,
Anaesthesia brought physiology to life in a way I hadn’t fully appreciated before. In every case, I saw how a detailed understanding of cardiovascular and respiratory physiology guided each clinical decision. These weren’t abstract concepts from textbooks now, they were applied constantly, in real-time. This left me with a deep respect for the complexity within the specialty and a genuine curiosity to learn more.
Putting the patient under anaesthesia was just the starter, the main course was maintaining the right depth of anaesthesia intraoperatively. Tools like BIS and end-tidal monitoring weren’t just numbers on a screen — they were essential in protecting patients from awareness, especially when paralysed. I saw how the anaesthetist vigilantly fulfilled this duty to uphold the dignity, trust and safety of the patient.
One of the most memorable parts of the week was observing spinal anaesthesia for Caesarean sections in the obstetric unit. Analgesia sat beside haemodynamic control, whilst also managing the comfort and experience of the mother. There seemed to be a rhythm to anaesthetists’ practice across the board — recognising patterns early, preparing precisely, and acting decisively.
Anaesthesia is profoundly patient-focused, something that challenged some of the preconceptions I had. One consultant described anaesthesia as a series of chapters, where your sole focus is that patient, in that moment. That ability to give your undivided attention, even briefly, felt like a rare privilege in modern medicine. It felt closer to the version of care I aspired to when applying to medical school.
Alongside shadowing the consultants, I was fortunate to spend time with anaesthetic residents and gain a clearer picture of what life in training looks like. One resident described the relief of moving away from ward work and instead diverting their full attention to gaining new knowledge and skills whilst working closely with senior colleagues. The one-on-one time with consultants was something they all valued deeply, not just for procedural supervision, but for the opportunity to ask questions, reflect, and learn in real-time.
I also had candid conversations about the training pathway, changes and challenges to recruitment, portfolio development, and how to make the most of short-term exposure during foundation years. The guidance I received was motivating, especially in understanding how to proactively seek out opportunities in a specialty with limited time allocated in early training. The mix of routine and high-pressure emergency work, coupled with such a strong teaching culture, made a lasting impression on me.
The week gave me a broad view of the complexity of anaesthetic practice in both elective and emergency settings. I left with new practical skills and clinical knowledge, but also with an excitement and clearer understanding of the scope and variety anaesthesia offers as a career. It whetted my appetite to gain further experience and opportunity as I move forward in my foundation training.
Millicent Brown Foundation Year 1 Doctor Prince Philip Hospital, Llanelli, Wales, UK
The anaesthetists and residents I met were impressive, warm and engaging whilst maintaining the highest professional, clinical and intellectual standards. I was sad to end the week, and all that was left for me to do was grab my cycling helmet, hop on my bike and cycle home!
Trasna na dTonnta: From UK to Rebel
County
Blame the French, I usually say. It’s easy, traditional, and good sport. But on this occasion, it wasn’t entirely their fault. No, the true villain of the piece was that tiresome little affair known as Brexit.
You see, the original plan — devised in a rare fit of forward-thinking — was that once I’d obtained my CCT, my family and I would decamp to France. This wasn’t mere whimsy either, I’d married a Frenchwoman and had made a pinky-promise that we would settle in her homeland once my training was through.
Enter Brexit, stage right, brandishing a bureaucratic sabre. Overnight, my hard-won UK qualifications became about as useful in Europe as a Stanley knife is for playing the bodhrán. Recognition? Non. Equivalence? Pas du tout.
I sulked. I raged. I even considered becoming a poet. But then, during a mutual moan with a medically inclined friend, I caught wind of something called the Hocsmann Procedure — a name that sounded more like an East German colonoscopy than a career path. Still, beggars can’t be choosers, especially when the EU is involved. The gist was this: to get my qualifications rubber-stamped by the Continentals, I’d need to spend three years practising in an EU country.
After poring over the map of Ireland with the strategy of a Roman general on campaign, we settled on Cork. It had a nice ring — southern, coastal, Fastnet area on the shipping forecast. I mentioned this to an Irish acquaintance, expecting a nod of approval. Instead, he raised an eyebrow: “Cork, eh? You’re a brave Englishman, that’s Rebel County down there.”
directed to Fintan O’Toole’s book, We Don’t Know Ourselves, which gives a comprehensive account of the development of Ireland. Another reference worth looking at before visiting, is arethebritsatitagain.org, an excellent source which is updated daily.
Practicalities of living; well, the housing crisis is real, so accommodation is a challenge. Spots for childcare and preschools can also be difficult to come by. But one thing I would say, is that the sense of community over here is strong. People have been extremely welcoming and there are many activities for the kids that would not continue without the support of volunteers. It’s not long before you find yourself recruited, as an under-6s GAA assistant-coach, for example! The weather… well, the grass is definitely greener here. My favourite phrase over here is ‘you know when it’s summer in Ireland, because the rain is warmer!’
My favourite phrase over here is ‘you know when it’s summer in Ireland, because the rain is warmer!’
“Is í an Ghaeilge an ceol is ansa liom.” –
Willy Clancy
One of our more romantic ideas when moving to Ireland was giving our children the chance to learn Irish. It’s a beautiful language, musical, rich, and deeply tied to the country’s identity. Ask most Irish adults about it, though, and you’ll get glazed eyes and tales of reciting poems they didn’t understand and regrets that they didn’t keep up with it.
Professionally, the transition’s been smooth. I work at Cork University Hospital, surrounded by an excellent and supportive team. I’ve learned new techniques and approaches to clinical work — variations on a theme, like the subtle differences in crans and rolls that tell you whether a musician learned their trad tunes in Sligo or Sliabh Luachra.
And the politics? Uncannily familiar stuff: promises of increased funding, and initiatives that look suspiciously like the same ideas from a couple of decades ago; decentralisation to regional health authorities, primary care centres; all reminiscent of Tony Blair’s 1997 reforms in the NHS. The latest, a move toward a “7-day HSE”… sound familiar? For a more in-depth discussion on differences in NHS/HSE, probably easier to discuss it over a cup of Barry’s. However, one of the best sources of getting my head around the system here, was being
That said, things have changed. Irish language education today feels far more alive. We enrolled our daughter in the local Gaelscoil, imagining a gentle bilingual environment: some Irish, some English, a few folktales. A cultural toe-dip. A month in, I discovered the water was deeper than expected: Gaelscoileanna are full immersion. The entire day is conducted as Gaeilge. Lessons, announcements, playground squabbles — all of it.
I even get a buzz of the language just dropping my daughter off at school. A teacher stands at the gate with a warm “Maidin mhaith, a chairde!” and some more Irish that I have yet to figure out what it means. It has nudged me — gently but firmly — towards learning a few polite responses. My wife, with her flair for languages, has powered through Duolingo like a woman possessed. She now sits somewhere between level 50 and ready to move to a Gaeltacht, while I cling to my handful of rehearsed greetings at work, always worried I’ll accidentally insult someone’s grandmother.
Still, there’s something wonderful about it. The language isn’t just surviving — it’s thriving, in the most natural way possible: in children’s mouths, in music and play. Our daughter flits between English and Irish, sings carols as Gaeilge, and shows no signs of confusion — only mild embarrassment when she corrects my pronunciation when I join in with “Óró, sé do bheatha 'bhaile.”
“Never take your eyes off the ball, even when it’s in the referee’s pocket.” – Christy Ring
Perhaps the most unexpected highlight of moving to Ireland was my decision to take up what might be the greatest sport on Earth: hurling. I’d had a brush with it at university — enough to know it involved speed, violence, and a stick. Now, living in Cork, the sport was on my doorstep. The temptation proved too much.
Picture it: a 38-year-old man, turning up to his first training session with a hurley in hand and an accent that sounds suspiciously… not local. I hadn’t even stretched before a teammate asked, “Are you Australian?”
“Er… no. I’m English.” Cat amongst the pigeons? More like pigeon amongst cats.
It took the lads a while to work out what I was doing there. Curiosity? Liability? Probably both. But I stuck with it. A few sessions later, after taking (and giving) a few decent knocks,
I started to earn my place — if not in skill, then in stubbornness. Then came one of the proudest moments of my Irish life: I was selected for my local Junior B’s (also known as Hatchet Division) for the first match of the season. I even made the starting line-up — though this had more to do with our lack of subs than my dazzling talent.
Hurling is a tough, skilful game requiring fitness and hand-eye coordination that, ideally, begins with holding a hurley at birth. Halfway through my debut match, I was already contemplating retirement. But then, somehow, I scored my first goal (questionably a square ball). Out on the pitch, in the shadow of the hills, rain lashing down, hurley in hand, accent forgotten — I felt, if not quite like a local, then a little less of a blow-in.
As I sit down to write my next year’s PDP, the goals look increasingly non-clinical: 1) Sean-nós singing as Gaeilge 2) Master the pipes (it’s all about the bag) 3) Retire from hurling before I end up on my own trauma list.
Perhaps not quite what the CPD gods had in mind, but it undoubtedly complements the clinical work and helps me understand this place my family and I call home. Sin é
Matthew Day
Locum Consultant Anaesthetist, Cork University Hospital, Ireland
Two weeks after undertaking a total knee replacement, I was shocked to learn that my patient had died after developing bilateral DVTs and a pulmonary embolism.
It was during the strikes, so I’d written the discharge letter myself. I omitted to provide low molecular weight heparin, and the ward pharmacist didn’t spot the error. Compounding this, against advice, the patient had not worn compression stockings at home.
After I received a complaint from my patient’s wife, my trust opened a Patient Safety Incident Investigation (PSII). This was followed by a coroner’s inquest –which the trust couldn’t support me with due to a conflict of interest. Then, because the coroner referenced my mistake in their conclusion, I faced a GMC investigation.
I can’t describe how awful that year was. Thankfully, my medicolegal consultant and solicitor from Medical Protection had a clear strategy that included legal rigour, supportive expert evidence, and early reflection and remediation. I was able to show that I’d learned from the experience, and to my immense relief the GMC closed the investigation with no further action.
Throughout it all, my Medical Protection team were there for me, not only as a doctor, but also as a human being. When you’re at rock bottom, that’s the most important thing of all.
Where personal and professional worlds collide
It wasn’t the Thursday morning I’d pictured back in July 2024. Back then it was all so simple – my friend C and I had been chatting casually a few days before around ideas for our usual summer getaway with our husbands, laughing over previous trips and promising to lock in the dates soon, looking forward to some time together.
Then came the call.
“M has collapsed. He’s being taken by ambulance to your hospital. Can you meet us there please?”
Details were scarce – just that paramedics were on the scene working hard and fast. There was no time for asking more questions, the urgency in her voice saying it all.
Unable to quite take in the words, time momentarily stood still but I dropped everything and drove to the hospital.
The journey to the hospital was a blur. “Collapsed”? It sounded vague, almost harmless – like a fainting spell or maybe a dizzy turn but that tone in her voice – tight and urgent – told me this was different. This was serious.
M was the picture of health and full of life. Since retiring he’d been more active than ever – jogging, cycling, playing golf and planning trips. He was healthy and strong. Thriving in his newfound freedom from work. But the moment I stepped into the hospital everything shifted. It felt surreal. These were the corridors I knew so well – places I walked every day. But today they felt unfamiliar. Cold and stark. And there C was, in the waiting room, my dear friend pale and trembling, barely able to form words. Her world crumbling and mine unravelling with hers. At that moment I realised that nothing in medical school training, or years as an anaesthetic consultant, had prepared me for this scenario. Fear and helplessness. We are trained to maintain professional boundaries, to offer clinical clarity in the face of emotional chaos, and to stand as pillars of strength when those around us are unwinding. But what happens when this person is such a close friend and you are watching the unimaginable with her?
M had had a cardiac arrest – the blockage in his main artery was cleared in the Cath lab, but he was now occupying a bed in ITU. The place that had always felt like a controlled environment – a world of protocols and predictable and recognisable patterns was now filled with unbearable uncertainty. Cold and sterile. I’d stood in this exact spot a hundred times before but never like this. Not with my friend’s husband lying there. Not with someone I loved hooked up to those machines that blinked and beeped steadily in the background. The rhythm of life. The familiar hum, once barely noticeable, now exacerbated, with every beep taking on an importance not previously realised. A signal of life. Of hope?
As a doctor I could understand every number, every change and I could anticipate what the next few hours and days would bring – how the downtime had been too long, how organ failure would progress and what scans would suggest. But as a friend all I could see was C’s face contorted with fear and grief, looking to me for answers that I wasn’t sure how to give. There was a mismatch between what I knew clinically and what I felt personally. Every instinct in me wanted to protect her, to soften the truth, to offer hope even where there was very little. But as a doctor I needed to be honest and clear when answering her questions. It was a line that was difficult to tread.
I found myself caught in the space where the personal and the professional collide. I wasn’t the doctor in charge, but I wasn’t just another visitor either. I understood too much and yet couldn’t explain why this was happening. The next few hours and days taught me that this was a situation I couldn’t ‘fix’ and I had to learn to stand by quietly, to listen carefully to what my colleagues were saying, not rushing in with a million questions, and to not compromise them by being present. I was overwhelmed with my own complex mix of emotions.
I felt uncomfortable and anxious as each day the ITU consultants would gently and thoughtfully convey updates with such care and compassion. The information needed to be repeated multiple times to the family. What they heard and what was actually said were often worlds apart. They clung to small positives not hearing the more difficult message. I worried constantly about giving them false hope even though I longed to feel that hope myself. Deep down I knew this was not going to end well and yet I had to maintain the same narrative, whilst gently, gradually, bit by bit offering the same information in small manageable pieces, giving them time to absorb the full weight of what was happening. All the time with them looking pleadingly for a different story.
I was both conflicted and confused as I wrestled constantly with whether I should step back completely, excusing myself, to allow the treating team to take full charge without my presence or to remain with the family as a source of comfort and translation. My professional knowledge, and the expectations placed on me because of it, clashed with my emotional loyalty to C as a friend.
As a mother of three myself, I could understand her desperate instinct to protect and shield her children from the harsh reality. It was heartbreaking to urge her towards being totally honest, knowing that even painful truths when shared in small pieces are better than the shock of a sudden unprepared blow.
The days became a relentless cycle of scans, conversations and deep sadness. As the family gradually became all too aware of the grim reality, they eventually asked the question that weighed heavily hanging in the air. Will M ever be the same again? Live a normal life? It broke my heart to confirm with them what the ITU consultants had been carefully guiding them towards. Each family member reacted differently –anger, tearful resignation, stoicism, stunned – but remarkably they were united about what the right course of action now was. Witnessing their immense courage and selflessness during such a traumatic time was humbling and a powerful reminder of the strength people can show in the face of extreme adversity.
I found myself caught in the space where the personal and the professional collide. I wasn’t the doctor in charge, but I wasn’t just another visitor either.
consultants are – not only in their clinical expertise but also their ability to convey upsetting information with such compassion, empathy and sensitivity. The support given to a grieving family was extraordinary and their equal support given to me was a blessing in the dark days. I was reminded of the quiet, unseen strength that underpins our specialty that often goes unnoticed and unappreciated. We must remember that our role as doctors impacts and extends beyond our clinical decision-making skills. It’s how we communicate, support and display those softer skills, whilst also bearing witness to such profound sadness that defines us.
All support was withdrawn, and nature was allowed to take its course. I had witnessed this moment many times before, standing beside other grieving families, but I could not have anticipated the sheer depth of this sadness. And then came the misplaced but real sense that somehow, I had ‘failed’ C. As doctors we are trained and driven to fix things, to intervene, to mend, to restore. Accepting that sometimes we can’t, especially for someone so close to you, felt like a personal shortcoming despite knowing intellectually that the outcome was never in my control.
Having been away from the specialised world of ITU, this episode provided a reminder of what immense skill and humanity are required in critical care. I had forgotten how exceptional these
Writing this piece has been deeply therapeutic – cathartic even. Reflecting and reliving the experience has provided a way of making sense of the numerous questions, emotions and uncertainties over the past year. The concept of ‘second victim’ is a phenomenon not much discussed amongst health care professionals, yet viewed through this lens, I’ve come to understand this journey. I would encourage, indeed urge, colleagues across all disciplines within medicine to be open about the emotional complexities that can arise from our everyday work. We must be aware of the psychological and physical symptoms that may surface, sometimes unexpectedly, and recognise the impact of them on oneself and the whole healthcare team. We must allow ourselves time to pause and reflect, to grieve and above all not forget that we are human too.
And finally, to my colleagues – you all know who you are – I will always be deeply grateful for your profound understanding, care and love shown to C and her family, but also to me personally. It will remain in my memory and will never be forgotten.
Siobhan Carroll Consultant Anaesthetist, Frimley Park Hospital
A Deeper Plane A Leaf, a Life and the Meaning Thereof
beyond the road curve ahead I do not know, we are still far and distant from winter snow, autumn has sprayed green leaves some yellow, some red, as they spiral and fall to their grassy bed.
these foliage tell tales of life and death, glory of existence and that final breath, when memories of life were all fresh and green, now strewn along the road is life that had been!
I stand on a bridge to view the flowing stream, silent it goes like a sequence in a dream, bearing on the surface, gatherings from trees, duty performed for nature, yearly with ease.
beauty all around is tribute to nature, meadow is still fresh, green is still the pasture, the demise of leaves is no reason for grief, future will bring new seasons! time is no thief!
A traveller will stop to admire the view, years and years from now when I have bid adieu, that day should not be any day for remorse, life always changes and flows and finds its course!
Krish Radhakrishna Consultant Anaesthetist, University Hospitals of Birmingham
After a walk along the Stratford upon Avon canal: 6km of my daily habitat.
A week of medicine, teaching, and community: Reflections from BKL Walawalkar Hospital
During a week-long medical education initiative at BKL Walawalkar Hospital in rural India, a multidisciplinary team of healthcare professionals from the UK delivered tailored sessions based on the specific learning needs of local staff and students. Through workshops, lectures, and clinical sessions, the programme focused on skill development, knowledge exchange, and fostering sustainable improvements in patient care and clinical education.
Nestled in the serene village of Dervan, halfway between the bustling metropolises of Mumbai and Goa, lies BKL Walawalkar Hospital. With 600 beds and an extensive campus that includes a nursing & medical college, a school, and a nearby temple, the hospital embodies a unique integration of spirituality, education, and modern healthcare. Established in 1995 by the Shree Janai Vinayak Charitable Trust (SJVC), the hospital's mission has always been clear: to deliver high-quality, affordable medical care to underserved populations in rural Maharashtra.
Since 2006, Dr Sanjay Deshpande has spearheaded an annual initiative known as the ‘UK Academic Camp.’ Each year, a group of multidisciplinary healthcare professionals from the UK travel to Dervan to collaborate with local medical teams, exchange knowledge, and deliver educational programmes. This year, I had the privilege of being part of this remarkable experience.
Reaching Dervan is no small feat. The journey involves a long-haul flight to Mumbai, a train ride to Chiplun, and a 30-minute drive through the lush Konkan countryside. This year, travel was especially challenging: due to extreme weather conditions in the UK, over half our team faced delays and had to reorganise their journeys at the last minute. Despite the obstacles, the moment our van rolled onto the hospital’s beautifully maintained campus, any fatigue quickly faded. We were greeted with warm smiles and a delicious home-cooked meal — an early sign of the incredible hospitality that would characterise the week.
After a much-needed evening of rest, we launched straight into a tightly scheduled programme. Our team included anaesthetists, surgeons, radiologists, ODPs and nurses, who conducted sessions driven specifically by host requirements. Some plans had to be adjusted to meet changing needs, but the team quickly adapted — brainstorming solutions, sharing resources, and designing practical, high-impact teaching sessions.
One of our major contributions was a regional anaesthesia workshop. We focused on using ultrasound rather than the landmark technique and taught the adductor canal block which was unfamiliar to the residents. The following day, these skills were applied during a total knee replacement case. Under our supervision, a resident performed the block using one of the hospital’s older ultrasound machines, due
to strict regulations on ultrasound use in India. The block was successful, eliminating the need for post-operative epidural top-ups. It was a powerful moment, exemplifying how skillssharing can translate directly into improved patient care. Educational initiatives extended across the hospital. We delivered lectures on neuroanaesthesia, preoperative optimisation and labour analgesia, a particularly novel concept in the region. The session on labour pain relief was attended by anaesthetists and obstetricians alike, sparking lively discussions about technique, cultural considerations, and patient outcomes. Small group sessions covered challenging clinical topics like difficult airway management and sedation strategies, as well as broader reflections on the differences between UK and Indian medical practices.
We also had the opportunity to engage with medical students, tailoring our sessions to suit their learning levels. We ran lectures on arterial blood gas interpretation and conducted Basic Life Support simulations, and even mock OSCEs), which we developed dynamically whilst on the trip, identifying specific needs and utilising all available resources. Initially unfamiliar with the format, the students were guided through what to expect, how to prepare, and how to maximise the experience. With local resident doctors helping to run the stations, by the third day the initiative had transformed into a peer-led activity, requiring minimal supervision from the UK team — a transformation that highlighted the enthusiasm and capability of local staff and students alike.
Over the years, the focus of the UK camp has evolved. Earlier trips involved more hands-on clinical care due to a lack of infrastructure and expertise. Today, the hospital is equipped to handle complex surgeries independently. Our role now centres on education by supporting advanced skill development, introducing new concepts, and fostering sustainable learning models.
Clinically, there were many fascinating contrasts to observe. While some practices differed from UK norms due to resource constraints, for example, the absence of end-tidal anaesthetic agent (etAA) monitoring, others were impressively innovative. Nasal prongs with built-in capnography, for example, were in routine use. Surgeries ranged from minor ENT cases to major hemiglossectomies (often necessitated by the prevalence of tobacco chewing). Even without high-end equipment like Wilson tables, the team displayed resourcefulness, for
example, using bolsters and padding creatively to ensure patient safety during prone positioning. Interestingly, there were no issues with medication shortages; India’s status as a major manufacturer of affordable pharmaceuticals ensures a steady and accessible supply, even in rural settings like Dervan.
One particularly memorable experience from the trip was a dissection session in the hospital's cadaveric anatomy lab. Collaborating with professionals from various disciplines — including anatomy, radiology, orthopaedics, and anaesthesia — we explored the hip and shoulder joints. These sessions not only deepened our understanding of anatomy from different clinical angles but also piloted the use of audiovisual teaching tools that could benefit future instruction.
Despite the intense schedule, the week was filled with moments of joy and cultural exchange. We were warmly welcomed into community celebrations such as a village baby shower and a school sports day. We played cricket and KhoKho with students, participated in a religious procession, and spent evenings bonding over quizzes and ice cream. The food was a particular highlight, fuelling us through long days of teaching and learning.
What made the experience truly special, however, was the spirit of collaboration and mutual respect. Although many of us had never met before the trip, we quickly found common ground, each bringing something unique to the table. We adapted to one another’s strengths, shared resources, and supported each other in delivering meaningful educational content. More importantly, we helped lay the groundwork for lasting improvements: setting up a shared drive for academic materials, initiating a journal club for residents, and auditing adherence to the WHO Surgical Safety Checklist.
This week at BKL Walawalkar Hospital was one of the most rewarding professional experiences of my career. It was a chance to contribute, to learn, and to be part of something
larger than ourselves through a shared mission to empower and uplift through education, medicine, and community. I left Dervan not just with memories, but with renewed purpose and the hope of returning again.
The placement at BKL Walawalkar is suitable both for those who have completed CT3 and for senior residents (ST6 and above). It has also been recognised by the RCoA as a suitable Out Of Programme Training (OOPT) experience.
Acknowledgements:
Mrs Suvarna Patil, Medical Director, BKL Walawalkar Hospital, India
Dr Leena Thakur, Consultant Anaesthetist, BKL Walawalkar Hospital, India
Dr Sanjay Deshpande, Consultant Anaesthetist, South Tyneside & Sunderland NHS Foundation Trust
Palbha Jain
ST5 Anaesthetist, Queen Victoria Hospital, East Grinstead, England
Anna Wilkinson
ST7 Anaesthetist, Glasgow Royal Infirmary, Scotland
Rewire the routine: Preventing hidden hazards in the operating theatre
The week began with energy: four joint cases on the list, a sharp and efficient surgeon at the helm, and a theatre team working in harmony. I took my usual position, threading myself through the familiar jungle of patient monitoring leads, cautery cables, and the towering presence of the surgical robot.
It was choreography — complex, precise, almost beautiful.
Until it wasn’t.
Just before noon, preparing for IV cannulation ahead of the third case, I stepped out of my tucked-away corner — what I half-jokingly call my ‘cage.’ Then, in an instant, it happened. I tripped over the worst cable I’ve ever seen. What I remember most vividly was the robotic cable. It felt alive, as if it had coiled around my foot and refused to let go. The crash came fast, a blur of motion. When I opened my eyes, it wasn’t pain that hit me, it was fear. Had I damaged my CABG? Miraculously, my head never hit the floor. Most of the impact struck my knees, especially the left.
The room froze. Colleagues rushed in, concern written all over their faces. I waved them off, rattled but standing. The surgeon approached, voice soft, urging me to rest. But I felt something heavier than pain — shame. I turned my focus back to the third patient. When I returned, I noticed something unsettling: the robot had quietly disappeared from the room. No fanfare. No discussion. And when the day ended, the debriefing was skipped altogether with a quiet nod. The case list was completed. The incident was erased. But I couldn’t shake the truth: we are sleepwalking into preventable disasters.
The hidden hazard
Operating theatres are littered with cables: monitoring leads, power cords, robotic lines. We step over them so often that we stop noticing them. Until one day, someone falls.
These cables are more than an untidy inconvenience. They are trap nets, hazards hiding in plain sight. And the cost of ignoring them is not just bruises or embarrassment. It could mean long-term injury for staff, a catastrophic delay in surgery, or harm to a patient.
The solution is simple
This isn’t a problem that needs a task force, a research grant, or another committee meeting. The solution already exists:
• Route all necessary cables just below the ceiling, secured and out of the way
• Use ceiling-mounted booms and overhead circular tracks to allow flexibility without cluttering the floor
• Many modern theatres are already designed this way. For those that aren’t, retrofitting is possible and worth it.
Why it matters
This isn’t about tidiness. It’s about safety, professionalism, and respect for the people who dedicate themselves to patient care. We cannot expect focus, precision, and excellence in surgery while tolerating basic hazards underfoot. Every fall is one fall too many. Let’s tidy up the jungle of wires before someone gets hurt.
Problem: Operating theatre floors are often cluttered with power cords, monitoring leads, and robotic cables. These create hidden hazards for staff and compromise workflow efficiency.
Please see instructions for authors on the Association's
Proposed solution: Implement cable-free floors by moving all major power supply and equipment connections overhead. I suggest a ceiling-mounted electrical supply: a series of modular ceiling ‘chandeliers’ or hubs, each equipped with multiple power outlets, gas ports, and data connections. Each hub could be designed to rotate or slide on ceiling-mounted tracks, ensuring machines and apparatus can be positioned conveniently on the right or left side of the patient as required. All cables and tubing would be suspended, leaving the floor completely clear for staff movement, equipment transfer, and emergency access.
Benefits:
• Eliminates tripping hazards and associated risks
• Enhances theatre efficiency by removing clutter
• Improves infection control by reducing floor-level obstructions
• Future-proofs theatres by accommodating both conventional and robotic surgical systems
Concept note
Hybrid ceiling-mounted electrical supply design
1. Central circle (Ventilation canopy integration)
• A large circular frame integrated around the theatre’s ventilation canopy
• Equipped with multiple sockets (electrical, gas, data)
• Symmetrically arranged for right- and left-sided use, supporting flexible positioning of machines and apparatus
2. Machine-specific circles (Satellite hubs)
• Smaller ceiling-mounted circles, each aligned with the location of its designated equipment:
• Anaesthesia hub: head end of the table
• Robotic hub: lateral docking zone
• X-ray/imaging hub: opposite side
• Each hub has its own dedicated connections, reducing overlap and confusion
3. Benefits
• Right- and left-sided sockets ensure adaptability for all surgical setups
• The modular circle system accommodates evolving surgical technology
Ahmed Amin Nasr Consultant Anaesthetist, Golden Jubilee National Hospital
My unusual posting in the South Seas
Back in the late 70s, I decided to specialise in tropical diseases and got a job in the Condominium of the New Hebrides, now Vanuatu, an archipelago of over 100 inhabited islands in the Western Pacific between New Caledonia and Fiji, uniquely administered since 1906 by Britain and France. (Imagine how that worked!)
Life in the New Hebrides had its own special confusion. There had been three different health services: the British, the French and the Condominium Health Service, the last to deal with public health. Its office was a wooden bungalow in the French residential quarter of Vila, the capital, with a French doctor in charge but nobody knew what went on there or, with Independence approaching in July 1980, the general French exodus and dissolution of the Condominium, what to do with it.
So, as the resident tropical public health expert, I was appointed Director of the Condominium Health Service. It felt good to be a director at such a tender age, with my own office and a secretary to type out my directives, even though she refused to speak a word of English. Then a cyclone blew the bungalow down so this orphaned branch of the health service was conveniently no more. But I kept the impressive rubber stamp for official documents like vaccination certificates. It is surely a collector’s item today.
I then needed another speciality, apart from medical island tours and sitting in outpatients, so before the country’s only anaesthetist departed, he gave me a crash course in anaesthesia and by this means I abandoned the tropical medicine career and became an anaesthetist instead. A couple of years later I returned to England, King’s College Hospital, to find out how it should be done.
Witchcraft
Confusion also means adventure. A chief on one of the islands had died in mysterious circumstances (‘leaf medicine’ = skulduggery). Witchcraft was suspected and the population was in turmoil. I was the doctor in charge, and it became my unpleasant duty to perform a postmortem examination of the 3-day-old exhumed body wearing three suits, brought to the island mission hospital by order of the new Minister of Health who thought Western medicine could settle this political problem. What could I possibly discover about ‘leaf medicine’ equipped with a knife, fork and a blunt bone saw, with the entire population (now called Ni-Vanuatu) of that end of the island, enthralled, crowding round every window blocking the light and air, a single 60-watt bulb powered by a spluttering generator and an assistant spraying Eau de Cologne in my face? The suits would not come off and one prick of the knife into the bloated corpse released several cubic metres of foul gas, so that counted for an abdominal examination. It was January 1980, the hottest on record according to ‘Voice of Vanuatu’, the local paper.
Twenty-five years later, we went back to Vanuatu and stayed in some tourist bungalows that turned out to be the enterprise of the same deceased chief’s son. He had been a teenager but remembered it all, including the removal of the top of his father’s skull. The hubbub had briefly quieted, then was broken by an authoritative voice: “Hemia nao: ples blong tingting!” (lit: ‘there now, that’s the brain’) followed by murmurs of approval. Luckily it was still there and was the sign we could call it an autopsy and go home. It has remained a mystery to me, to this day, where the brain goes when you die.
How does it get out?
I commiserated with the deceased’s son sitting next to me at the bungalows and apologised for removing his father’s skull, but I was just following orders. There was no discount offered on the accommodation for old-time’s sake or medical services rendered.
Tall tales from a distant island
Another proposed post-mortem, this time ordered by the police, proved more interesting. In November 1980, reports of the rape of two young girls and murder of one came from Futuna, the most remote island in the archipelago. The island has no radio and no airstrip, and being about 20 degrees south, the seas are often too rough for landing. Some recent arrivals from Futuna, speaking their own wan-tok via a Futunese policeman in Vila, reported the crime to a young British policeman, recently seconded to Vanuatu from London. Piecing all these little snippets together did not ring any alarm bells. It was long ago but today he is probably a Chief Constable somewhere so; to spare his blushes, I’ll call him Jones.
The story was that two girls aged 11 and 12 had been raped by four men. Both had become pregnant, and one fled to the neighbouring isle of Tanna on a boat but died on the trip, so the boat returned to Futuna, and she was buried. Jones was chortling and rubbing his hands with glee “unlawful carnal knowledge of a minor, mass rape. Suicide? Homicide?” Now, at last, he was policing wickedness in the islands, what he had been posted from London to do.
He had to have a corpse as evidence so that’s where I came in, having been nominated for the job by the Hospital Medical Superintendent.
Well, I had to go, I’d never get an offer like this again. We flew from Vila to Tanna in a special police charter which was half empty (“space to bring back suspects” said Jones) and were met by the Euphrosyne II, the former British Resident Commissioner’s touring boat which had been pulled from its previous duties, blowing up reefs with a New Zealand team, for this police investigation. The captain, Nassak, was none too pleased with an overnight sailing to Futuna. My role was to exhume the girl, who was buried a week ago, and perform an autopsy. I passed a restless night in the rolling and pitching boat thinking about the grisly task ahead and if my tools would do.
But it was great to go aboard the fine old vessel which I had not been on for a year, since before Independence. The Duke
and Queen Elizabeth had been removed but otherwise it was just the same. The cook, Stephen, promised his legendary breakfasts of orange juice, fried eggs, bacon, coffee and toast that taste so much better in a galley at sea with a view of the great Pacific Ocean on both sides.
I got up at 04:30 to see the dawn, always a great moment at sea. Approaching from the west, the 2,000-foot cliffs of Futuna were silhouetted right in front of us, surrounded by a black sea lashing the rocky and forbidding coastline. Not most people’s idea of a South Sea Island paradise. Unlike the rest of Vanuatu, the island is situated to the right of the so-called Buxton Line (famous to tropical medicine cognoscenti), to the east of which, from Fiji onwards through Polynesia, there are no anopheles mosquitos, no malaria.
We went around looking for a suitable place to ‘goasore’. The options were Mission Bay or Herald Bay; Nassak chose the former, on the east side.
So focused was I on the fearful business in hand that I made a serious error of judgement and jumped into the first boat ashore, missing breakfast. One should learn to always stand back and think before acting. The result was that I sat munching stale bread and drinking water in the dispensary for one hour waiting for the others to polish off my juice, bacon, eggs, toast and coffee. Nassak then upped anchor and circled the island to catch any murderers escaping by canoe.
Never mind, I got the story, such as it was, and had the satisfaction of seeing the expressions on the faces of Jones and his French No. 2 as I told them we had been well and truly had. It was a wild goose chase. There had been no rape, no one was or had been pregnant and of the two girls, one was standing next to me, smiling, fit and well, the other had gone on a boat to Tanna, had indeed died on the way but it was from natural causes, dysentery it sounded like. She was buried on the island and there was no indication to dig her up, praise The Lord.
The islanders weave the finest, most beautiful soft pandanus baskets in the whole of Vanuatu – we still have one hanging up at the back door – and they surely love their island, this rock in the middle of nowhere, taking occasional trips to neighbouring Tanna to get some culture shock from seeing the light bulb there. There was an interesting static bicycle-powered VHF radio. No one could make it work but that was 45 years ago. With the dispensary dresser as guide, we crossed over to Herald Bay via several fixed vertical bamboo ladders because the island is mostly high cliffs. There are numerous dogs that can climb these ladders faster than any human. I have never seen such a thing. There are two villages, one in each bay separated by this massive rocky middle. Rather than climb all the way back, Jones was persuaded to use his police dept. cash to hire the island speedboat round to the anchorage, with half the village on board as well for the ride and to study strange white people. We met the Euphrosyne coming the other way; Nassak had been told of the wasted trip but shouted across with reassurance that he had not decided to leave us on Futuna for the next six months as revenge.
I pulled a couple of teeth and left a box of medical supplies with the dresser, rifled from our pharmacy in Vila. Having done Futuna, I relaxed on deck, did some snorkelling round the boat and had a snooze in the sun. I’d been up early. Stephen produced a superb lunch, and then dinner, all washed down with some French wine that the No. 2 had brought along, and we discussed our rotten luck on the mission and what better things we could be doing... but no one could think of any. Jones’ Tours got a five-star rating.
Several Ni-Vanuatu were still ashore. We had to wait until midnight before they returned. The young Futunese policeman who had engineered the whole farce came on board, dead drunk, after hours of revelling in his home village that he had not seen for 7 years.
Oh, yes, we had been royally played. God knows what it all cost but that’s island life.
Paul Fenton
Retired
26 - 29 January 2026
A unique and truly multidisciplinary meeting of:
Anaesthesia, Critical Care & Pain
Dermatology • General Practice
Plastic Surgery • Radiology • Rheumatology
Trauma & Orthopaedics • Other Specialties
• Specialty specific sessions
• Multidisciplinary and satellite sessions
• Hands on workshops
• Contributions from allied professions
• Lifestyle medicine and wellbeing
• Innovation and AI in medicine
• Keynote lectures by invited speakers
The importance of medical leadership for anaesthetists
Medical leadership is a crucial aspect of modern healthcare. As specialists responsible for patient safety, perioperative care, and multidisciplinary collaboration, we are uniquely positioned to influence clinical outcomes and drive improvements across healthcare systems. Anaesthetists have a well-deserved reputation for being able to lead across traditional specialty boundaries.
Leadership skills have impact on patient care, team dynamics, professional development, and the broader healthcare environment and there is sound evidence that the most effective healthcare systems are led by doctors.
The Association’s new programme recognises this and is an important opportunity for gifted future leaders to get started.
Enhancing patient safety and quality of care
We are all familiar with the role of effective leadership in our core clinical work. Anaesthetists operate at the heart of patient safety, overseeing critical phases of care such as induction, maintenance, and emergence from anaesthesia. Our effective medical leadership ensures that safety protocols are meticulously followed, risks are anticipated and mitigated, and evidence-based practices are implemented consistently. As unit and system leaders, anaesthetists don’t just follow standards, we set standards, champion quality improvement initiatives, and foster a culture where patient safety is paramount. By guiding systems through complex or emergency situations, anaesthetic leaders help prevent strategic errors and ensure optimal outcomes and continuous improvement.
Facilitating multidisciplinary collaboration
Operating theatres, critical care and obstetric units and perioperative care settings are dynamic environments where anaesthetists work closely with surgeons, nurses, operating department practitioners, and other healthcare professionals. Strong medical leadership enables us to coordinate care, resolve conflicts, and communicate effectively across disciplines. By modelling collaborative behaviour and encouraging open dialogue, anaesthetic leaders promote seamless teamwork, which is essential for efficient, high-quality perioperative care. Our leadership helps bridge gaps between different specialties, leading to better patient experiences and more integrated healthcare delivery. Anaesthetic leaders enhance these skills further to develop pathways and strategies which will have an impact on patients before they reach the hospital front door – CPOC is a great example of this, and until very recently was led by an anaesthetist.
Driving change and innovation
Healthcare is continually evolving, with new technologies, techniques, and regulatory requirements emerging regularly. With well-developed leadership skills, we are well-placed to advocate for and implement positive change within our departments and systems. We can identify areas for improvement, champion the adoption of innovative practices, and lead the development of new protocols or pathways. By taking on leadership roles, anaesthetists become agents of change, helping our teams and the wider system adapt to advancements and maintain high standards of care in a rapidly changing environment.
Supporting professional development and wellbeing
Leadership in anaesthesia extends beyond clinical expertise; it encompasses mentorship, education, and the nurturing of future leaders. Anaesthetic leaders support the growth and development of junior colleagues, offering guidance, feedback, and opportunities for learning. This investment in professional development helps sustain the specialty, ensuring a pipeline of skilled practitioners are ready to meet future challenges. Moreover, effective leaders recognise the importance of wellbeing, advocating for healthy work-life balance, psychological safety, and supportive workplace cultures.
Advocacy and representation
Anaesthetists often serve as advocates for their patients and profession, both within the hospital and in broader healthcare policy discussions. Medical leadership development equips us with the skills to represent our specialty effectively, influencing decisions about resource allocation, service provision, and patient care standards. By engaging in leadership roles at local, regional, or national levels, anaesthetists help shape policies that affect clinical practice and patient outcomes, ensuring that the unique perspectives of our specialty are heard and valued.
Conclusion
Medical leadership is indispensable for anaesthetists, underpinning their ability to deliver safe, high-quality care, foster collaboration, drive innovation, and support the growth of the specialty. In an increasingly complex healthcare landscape, anaesthetists who embrace leadership are better equipped to navigate challenges, inspire their teams, and advocate for patients. The development and recognition of leadership skills among anaesthetists should therefore be a priority, benefiting individuals, teams, and the wider healthcare system alike.
The Future leaders in anaesthesia programme offers a stimulating blend of expert insight, lived experience, peer challenge and support and personal development to take participants’ concept and practice of leadership to a new level.
Emma Hosking
NHS Consultant Leadership Development
Future leaders in anaesthesia
We are excited to launch Future leaders in anaesthesia in partnership with Bayes Business School! This dynamic new programme is designed for resident doctors, SAS doctors/NCHDs, and earlycareer consultants looking to sharpen their leadership skills, drive positive change, and grow their influence within the NHS.
Places are limited to 21. The Association is pleased to offer funding for these places. Applications are now open and will close on Monday 8 December 2025.
If you have further questions, email nicola@anaesthetists.org
Winter Scientific Meeting 2026: Two
days that will change your practice
Seventy speakers, three streams, 25 core topics and one unforgettable experience. Don’t miss WSM 2026 on 15-16 January at QEII Centre (London) or watch all three streams live online.
Winter Scientific Meeting (WSM) is the highlight of the Association’s education calendar. In January 2026 it returns to QEII Centre in London, bigger, brighter and more engaging than ever.
For two packed days, hundreds of anaesthesia professionals will come together to share knowledge, debate the future of the specialty, and enjoy the company of peers from across the UK and beyond.
With 70+ expert speakers, three concurrent lecture streams, a lively exhibition floor and meaningful networking opportunities, WSM is designed to give you new ideas, fresh perspectives, and connections that last well beyond the event.
“74% of 2025 delegates said they would change their practice after attending.”
What’s new this year?
• Core Topics Day: cover 25 essential subjects in just one day
• Live interviews with our speakers to gain fresh insights and hear behind-the-scenes perspectives
• All-new awards ceremony: recognising excellence across the specialty
• And, keep an eye out for some fun additions to the exhibition hall, giving you the opportunity to unwind
A programme shaped for you
Confirmed core topics sessions include: Cardiac surgery and co-morbidities; Haematology; Peri-operative care for the older patient; Bariatrics; Shared decision making; Blocks for trauma; ICU for the non-intensivist; Obstetrics and paediatrics.
Alongside these, delegates can also expect sessions on innovation, new guidelines, theatre efficiency, drug safety, and the ever-popular Anaesthesia Journal and Military sessions.
And don’t miss the e-poster presentations, showcasing cutting-edge research from colleagues across the profession.
View the programme online
Keynote highlight
Alan McEwen, an international air traffic controller with 25 years of experience in some of the busiest airspaces in the world, brings lessons from highpressure environments in his keynote: “Human factors and air traffic control: preventing planes from crashing.” His unique perspective will shed new light on risk, decision-making and teamwork under pressure.
Learn, connect, celebrate
WSM is not just about what happens in the lecture theatre. The event is designed to give you a full professional and social experience:
• Hear from world-renowned speakers
• Connect and network with hundreds of peers
• Explore the industry exhibition and inexhibition learning zones
• Relax and celebrate at the Networking Reception and Awards Presentation (included in ticket price)
Check out the latest in MedTech
We’re delighted to welcome our industry partners to Winter Scientific Meeting 2026, including Draeger Medical UK Ltd, GE HealthCare and Ambu who will be running sponsored symposium and demos in the in-exhibition Learning Hub (Lecture Theatre and Demo Zone).
Book now and save
Secure your place early and save: members benefit from discounts of up to £385 compared with the standard nonmember rate when booking before 23:59 on Thursday 4 December 2025.
Book your place now >
Quality Assurance:
What is it and what does it mean for you?
You may have noticed recently that booking pages for the Association’s educational events over the past year have been adorned with a ‘flash’ which says Quality Assured by the Association of Anaesthetists.
This article explains what that means for you, for us and for your CPD journey.
Last
year we decided to do more to bring our Quality Assurance (QA) activities to the attention of the membership and are continuing the drive this year.
At its core, we believe QA instils confidence. Confidence in the content delivered, the speakers engaged, and the overall experience of the attendees. For medical professionals like Association members, this confidence is paramount. It directly impacts patient care and professional development.
The Association has a fully developed, rigorous approach to QA of its educational output, summarised in four documents, and found on the Quality Assurance page of the website.
Why we feel our QA activities are important to you
• Each educational event is designed to meet the learning needs of the delegates. This includes selecting appropriate content, educational methods, and delivery strategies to ensure that delegates gain the knowledge and skills they need
• We collect feedback from delegates about their experience attending the event. This feedback is then used to improve future events and ensure that the needs of learners are being met
• Delegates can be sure that the CPD they have received from the Association is of the highest quality, due to our QA procedures
The Association’s QA framework
So, what does our QA process entail? It begins long before the event itself. We carefully select topics that are relevant and timely. Our speaker selection process is rigorous, ensuring expertise and credibility.
During an event, the talks are either filmed for later review or attended live by a QA assessor.
We also gather feedback, analyse data, and continuously strive to improve our events.
The Association has a QA lead, and a group that meets regularly. Once a year the Education Committee acts as the QA Board, and a selfassessment report tracks activities throughout the year. We consistently review our policies and procedures and go through a formal update of our policies and procedures every two years.
Our quality standards
Currently, we have the following quality standards for Association education/training in place, also found on our website:
1. Criteria for how the use of curricula, the mix of education topics and codes will be reviewed
2. Event programmes will be reviewed in advance
3. Where relevant, each activity will have a maximum of five learning objectives set
4. Presenter performance reviewed by delegates and by a QA person
5. A good mix of educational methods will be used, and the use of them measured
6. Promotion of reflective learning
7. Feedback to speakers is delivered, normally within a month of the delegate evaluation survey closing
8. A database of Association faculty will be maintained, recording event, talk title, feedback and QA results
How we ensure we meet the standards
To meet the standards above, we carry out these actions:
• We gather evaluation feedback from delegates and QA assessors and share with speakers, including whether learning objectives have been met
• Representatives of the Education Committee oversee the planning of events
• A QA assessor reviews either a live event, or a recording
• QA assessors will also scrutinise any lectures that have been videoed for use online
• Once a year the Association Education Committee and Education Team will conduct a quality audit/review and selfassessment/appraisal exercise to identify areas for improvement
QA self-assessment report
Each year we produce an annual report and QA action plan measuring our activities and performance out of a total of 10 points per event. We look at a range of areas, including delegate evaluation scores. The table shows how these have progressed over the years:
We also compare QA and delegate scores for each event type:
Actions the Association takes, and why
Update our policies every two years:
• The educational environment is constantly changing, including updates in technology, pedagogy, and curriculum
• The review provides an opportunity to identify areas for improvement and innovation
• Feedback from stakeholders, including delegates, faculty, and staff can be used to identify areas for improvement in the QA process
Quality assure each video prior to release on Learn@
Learn@ is our online learning portal, allowing you to record your CPD activities, as well as access our large library of educational videos. We review the videos before we release them onto Learn@ to:
• Ensure the videos accurately reflect what was presented during the event
• Provide our members with the most relevant and valuable videos when they are unable to attend in person. Allow the QA assessor to provide feedback on the videos, so we can improve them in future
Recruit QA assessors from the membership
Recruiting QA assessors from the membership and training them to quality assure educational videos has several benefits, including:
• Members of the Association who are recruited as QA assessors have a good understanding of the Association’s culture, values, and practices
• Training members of the Association to carry out QA can build capacity within the Association. This can enable the Association to become more self-sufficient in managing QA activities
Andrew Mortimore
e-Education Manager, Association of Anaesthetists
You can now join our panel of QA assessors
If you would like to join the panel of QA assessors, please email learn@anaesthetists.org explaining your reasons for signing up and telling us a bit about yourself.
All of our events are subject to our Quality Assurance process, ensuring that every educational event we deliver not only meets but exceeds the expectations of our attendees.
30 Member QA panel recruited from the membership – apply to join now
8 QA standards in our QA policy and procedure – all our events are measured against these QA group and a QA board to oversee our QA activity
86%
Average delegate score
87.6%
Average QA score
We produce an annual QA report about how well we meet our QA standards. We make a yearly QA action plan.
100%
Delegate feedback collected and delivered to speakers 100% of the time
Pattern recognition in USG
Ultrasound-guided (USG) regional anaesthesia has revolutionised how clinicians perform nerve blocks and fascial plane blocks. However, acquiring and interpreting high-quality ultrasound images remains a challenge, particularly for residents or those new to regional techniques. One solution lies in leveraging a fundamental function of the human brain: pattern recognition.
By linking sonographic images with familiar shapes, animals, or everyday objects, clinicians can improve recall, enhance image interpretation, and make anatomical landmarks easier to identify. Pattern recognition not only enhances learning but also ensures greater consistency and safety in regional anaesthesia practice. This use of pattern recognition helps anaesthetists using USG for regional anaesthetic techniques and in (Point of Care UltraSound) POCUS to acquire the desired and appropriate USG picture.
Pattern recognition: The brain’s natural tool
Pattern recognition is the cognitive process of identifying recurring forms, images, or configurations by matching new information with stored memory. It is an intuitive function, honed by repetition, that underpins how we learn and make decisions.
In the context of USG, pattern recognition allows anaesthetists to quickly identify complex anatomical structures by associating them with familiar shapes or visual metaphors. These mental models simplify sonoanatomy, breaking down complex images into digestible and memorable components.
Using familiar imagery in sonoanatomy
When sonoanatomical images are described using patterns already known to the mind, such as animals, objects, or scenes, the process of correlating and remembering them becomes significantly easier. Below and on the next few pages is a collection of commonly used and novel pattern descriptions used in USGguided regional anaesthesia, organised into two main categories: Animals/Birds and Objects/Scenes.
Pattern recognition is more than a learning tool, it can be an effective clinical strategy. By associating sonographic images with familiar forms, clinicians can demystify complex anatomy, reduce cognitive load, and streamline ultrasound-guided procedures.
Whether you are a resident beginning your USG journey or an experienced practitioner teaching others, embracing visual metaphors makes regional anaesthesia more accessible, memorable, and effective. Creating and sharing new patterns should be encouraged to promote a shared visual language in anaesthesia practice.
I. Animal and bird patterns in USG
Equal sign/Flying bat/Cats head level of the interspinous processes
Bat wing or cat head
• View: Transverse interspinous scan of the lumbar spine
• Description: The spinous process and laminae resemble bat wings or a cat’s head.
Horse head
• View: Parasagittal oblique scan at the lamina level of the lumbar spine
• Description: The bony lamina resembles a horse’s head profile.
Parasagittal scan Horse head sign at the lamina level
Parasagittal scan
Camel hump/saw tooth sign at the articular process
Camel hump
• View: Parasagittal oblique scan at the articular process level
• Description: The articular processes form two humps, reminiscent of a camel.
Rabbit head
• View: Shamrock view (QL block) at L3/L4
• Description: The transverse process and surrounding muscles resemble a rabbit's head.
II. Object and scene-based patterns
Traffic light at the interscalene block level
Traffic light or stop light
• View: Interscalene groove (C5, C6, C7 roots)
• Description: Nerve roots aligned in a vertical pattern resembling a traffic light.
Sunrise out of the mountains
• View: Dynamic scan of C5–C8 nerve roots
• Description: Nerve roots exiting the foramina resemble the sun rising over hills or the space between a thumb and finger.
U-turn sign
• View: T1 ventral root joining the C8 root
• Description: Appears as if taking a U-turn to form the inferior trunk.
•
Bunch of grapes/cup saucer at the supraclavicular level
• Description:
Cup and saucer
• View: Supraclavicular region
• Description: Neural elements of the brachial plexus sit above the first rib like a cup on a saucer.
Bunch of grapes
• View: Supraclavicular region, superolateral to subclavian artery
• Description: Brachial plexus elements resemble clustered grapes.
Shamrock
• View: Shamrock view at L3/L4
• Description: The transverse process, QL, erector spinae, and psoas major form a shamrock.
Thumbs up
• View: Modified shamrock view
• Description: Transverse process and vertebral body mimic a thumbs-up gesture.
Boat on water
• View: Shamrock view of QL and psoas muscle
• Description: QL appears like a boat floating on the psoas (water).
Bowtie
View: Suprainguinal fascia iliaca block
Internal oblique and sartorius muscles form a bowtie shape.
Bow tie sign in SIFI block
Boat on water - QL (Boat) on Psoas (Water)
Trident/Trishool sign
Parasagittal scan at the transverse process
Trident
• View: Parasagittal scan lateral to spine midline
• Description: Transverse processes form a three-pronged shape.
Tower sign-level of the spinous process
Tower
• View: Transverse scan at spinous process level
• Description: Vertebral architecture appears like a tower.
III. Author-created patterns for teaching and recall
The following visual metaphors are personal creations by the author to further aid learning and retention:
Harshal D Wagh
Consultant Anaesthetist, Kokilaben Ambani Hospital, Mumbai, India
References
• Water over the hill: Iliacus muscle flows over the pelvic brim in a SIFI block.
Superficial peroneal nerve - frog catching an insect Water flowing over a hill - in SIFI block
• Frog catching a fly: Superficial peroneal nerve scan with septal extension mimicking a frog’s tongue.
1. Børglum J, Moriggl B, Jensen K, Lønnqvist PA, Christensen AF, Sauter A, Bendtsen TF. Ultrasoundguided transmuscular quadratus lumborum blockade. British Journal of Anaesthesia 2013; 111 eLetters Supplement. https://doi. org/10.1093/bja/el_9919
2. Franco CD, Williams JM. Ultrasoundguided interscalene block: reevaluation of the “stoplight” sign and clinical implications. Regional Anesthesia & Pain Medicine 2016; 41(4): 452-9.
3. Areti A, Sivashanmugham T, Velraj J, Gajendran P. Sonographic corroborative dissection of C5-T1 ventral rami of brachial plexus with sonographic signs for identification. Turkish Journal of Anaesthesiology and Reanimation 2022; 50(6): 467468.
4. Nielsen TD, Moriggl B, Barckman J, Kølsen-Petersen JA, Søballe K, Børglum J, Bendtsen TF. The lateral femoral cutaneous nerve: Description of the sensory territory and a novel ultrasound-guided nerve block technique. Regional Anesthesia Pain Medicine 2018; 43(4) :357-366. doi: 10.1097/AAP.0000000000000737. PMID: 29381568.
Here, we present a selection of our best videos from our online learning platform Learn@.
VIDEOS
New Association Guidelines on Transfusion - what you need to know
Akshay Shah
Is Dural Puncture Epidural a “hole” lot better ?
Marc van de Velde
Tranexamic acid the wonder drug
Ian Roberts
Pre-op assessment in children
Shyamala Moganasundram
Ultrasound for neuraxial anaesthesia
Nhat Nguyen-Lu
Video recommendation
Anaesthesia and assessment: The Diploma in Anaesthesia and beyond
This November marks 90 years since the introduction of the Diploma in Anaesthetics (DA), a milestone in the formal recognition of anaesthesia as a medical specialty. Although the first recorded use of anaesthesia was in 1846, it wasn’t until 1935 that a formal qualification was established. Celebrate this important anniversary by tuning into Dr Rob Feneck’s recorded talk, where he explores the early days of anaesthesia and the origins and development of the DA.
PODCASTS
In this two-part episode, former ENT surgeon and current MP, Mr Peter Prinsley, talks about his career change before chatting with President of the Association, Dr Tim Meek, about how the Association advocates for its members.
Starting anaesthetics training can feel exciting, daunting, and everything in between. In this episode, the Coffee and a Gas hosts sit down with a resident doctor who has just completed Stage 1 to share what it’s really like — from first on-calls to tackling the Primary FRCA, managing the e-portfolio, and finding your feet in theatre. Packed with practical tips, honest reflections, and advice they wish they’d known on day one, this is your survival guide to navigating Stage 1 and setting yourself up to thrive. LISTEN NOW
Have you listened to a podcast or watched a video recently that stopped you in your tracks? Did it help you rethink your current practice or apply a new approach to your hobbies, wellbeing or life? If so, we want to hear about it! Please email anaenews.editor@anaesthetists.org with your name, affiliation, link to the podcast/video and 1-2 sentences about why you think others should take a listen or watch.
Winter Scientific Meeting 2026
Thursday 15 - Friday 16 January 2026
QEII Centre, London, UK
• 70+ speakers
• 3 streams
• 2 fantastic keynotes
• Latest guidelines, journal session and a lively debate
• Attend in person or online
• Bigger Winter Social than ever before including an awards ceremony
Confirmed Keynote
Alan McEwen (Air Traffic Controller)
Human factors and air traffic control: preventing planes from crashing
All 3 streams available online
New for 2026: Cover 25 core topics in anaesthesia in just one day
Book now Early discount rate ends 23:59, Thursday 4 December