Australian and New Zealand College of Anaesthetists & Faculty of Pain Medicine
SPRING 2024
BEYOND CITY LIMITS Central Queensland’s scenic havens beckon
Medication errors
Look-alike ampoules still a cause for concern
Indigenous health Palm Island pain clinic is welcomed by locals
Dr Stephanie Giandzi
Get ready for National Anaesthesia Day!
An ANZCA initiative, National Anaesthesia Day is usually held each year on 16 October to mark the anniversary of the day in 1846 that ether anaesthesia was first demonstrated publicly.
This year’s theme “You’re in safe hands”, focuses on “real” anaesthetists with real stories that help the community understand what anaesthetists actually do, how well qualified they are and the essential role they play in the health system.
Join in the fun by using the hashtag #NAD24.
We’ve created resources including A3 posters and A4 posters that can be on display all year round, as well as video interviews with fellows across Australia and New Zealand. You can also download and print an activity sheet for kids.
Visit our website for more information.
ANZCA Bulletin
The Australian and New Zealand College of Anaesthetists (ANZCA) is the professional medical body in Australia and New Zealand that conducts education, training and continuing professional development of anaesthetists and specialist pain medicine physicians. ANZCA and FPM comprise about 8900 fellows and 1950 trainees. mainly in Australia and New Zealand. It serves the community by upholding the highest standards of patient safety.
Medical editor: Dr Kate McCrossin
Editor: Clea Hincks
Production editor: Liane Reynolds
Feature writer: Carolyn Jones
Advertising manager: Vivienne
Forbes
Designer: Michelle Nightingale
We encourage the submission of letters, news and feature stories. Please contact Bulletin editor Clea Hincks at chincks@ anzca.edu.au if you would like to contribute. Letters should be no more than 300 words and must contain your full name, address and telephone number. They may be edited for clarity and length. To advertise please contact communications@anzca.edu.au.
ANZCA may promote articles that appear in the Bulletin in other forums such as the ANZCA website and ANZCA social media platforms.
Contact us
ANZCA, 630 St Kilda Road, Melbourne Victoria 3004, Australia +61 3 9510 6299 communications@anzca.edu.au www.anzca.edu.au
Faculty of Pain Medicine +61 3 8517 5337 fpm@anzca.edu.au
The ANZCA Bulletin has been printed on FSC® certified paper using vegetable-based inks by Southern Impact under ISO14001environmental certification. It is fully recyclable.
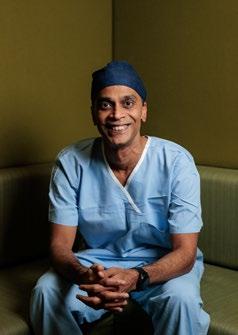
Senior staff specialist anaesthetist
Dr Suresh Singaravelu taking a break from his schedule at Mackay Base Hospital. Photo: Fiona Kroll.
SCAN TO FIND OUT MORE
Dr Yasmin Endlich FANZCA Specialist anaesthetist #InSafeHands
Most people will need an anaesthetist at some time in their lives.
19 Perioperative medicine
How one Queensland project is delivering patient-centred care to elective surgical patients.
16 The importance of open communication
Open discloure processes benefit patients, families and clinicians.
43 Avoid excessive opioid prescribing
Clinicians must take care when prescribing analgesic medications, particularly opioids, on discharge after surgery.
ANZCA research is not just about rats and RCTs
"It is better to light a candle than to curse the darkness."
- William L. Watkinson
Every anaesthetic is a research project with the hypothesis that, compared to other options, the approach I’m using is best for this patient. Health and medical research is a continuum that goes from discovery bench research through clinical trials to the newer sciences of health services and implementation research.
ANZCA fellows now research these ever-broadening areas including education and culture. To facilitate this research we have both clinical trials (Clinical Trial Network or CTN) and professional practice research networks (PPRN).
The key to all research is asking the right question(s). The question that started my doctoral thesis was: Why is normal saline acidic? The unexpected answer is at the end.
The best questions come from hypotheses rather than fishing expeditions.
In clinical trials this has the PICO formula: population, intervention, comparator, outcome. For example, from the ANZCA CTN-led RELIEF study (www.anzca.edu.au/profiles/ ctn-trials/published/relief-trial): In adults undergoing major abdominal surgery does a restrictive fluid regimen compared to a liberal fluid regimen lead to a lower rate of complications and a higher rate of disability-free survival?
Contrary to the hypothesis, the result was no difference in disability-free survival and an increase in acute kidney injury with restricted fluids. This strong evidence informs everyday clinical practice including ANZCA’s IV fluid advice during the current shortages (www.anzca.edu.au/news/iv-fluid-supplyupdate).
While some think otherwise, quality improvement should be treated with the same rigour as clinical trials. At least, the unreliability of answers from dodgy quality work should be recognised. Similarly, one of my more controversial mottos is: stop doing small crappy randomised trials! Instead start with feasibility and pilot studies1, including surveys, that ask the question: Can we do this research?
ANZCA doesn’t conduct research, rather we support those who do. Through the ANZCA Foundation, the ANZCA Research Committee allocates more than $A1.5 million per year in grants to fellows and their co-investigators with an ever-broadening range of research topics.
With some community input, the ANZCA Research Committee is a specialist committee of experienced researchers aiming to fund feasible research important to our specialties.
Increasingly the grants support early and mid-career researchers. ANZCA grants supporting pilot studies have been vital for subsequent success with government funding bodies in Australia, New Zealand, and Hong Kong. We can be proud that over the last 25 years ANZCA researchers have secured over $75 million in large grants predominately for clinical research. These trials are conducted in over 50 hospitals. A great return on investment.
The research team is one of the most important components after the research question.
A research team is like the movie Oceans 11; individuals with important skills add to the collective strength. Instead of explosives and cyber-hacking experts, research teams may have clinicians, trial co-coordinators, health economists, data base experts, statisticians, and increasingly consumers.
However, all researchers must be wary of the DunningKruger effect of overestimating our own abilities outside our areas of expertise. For example, many doctors did well in maths at school and assume they are a whiz with statistics. A senior statistician joked: “I wouldn’t read a first-aid book and say I’m a doctor.”
Having come from a 30-year career in quantitative physiological and clinical research I only now adequately appreciate qualitative research. Quantitative clinical studies can answer what is happening while qualitative research often aims to answer why it is happening, particularly in health services work.
The best of both worlds is mixed methods combining quantitative and qualitative. A good example of mixed methods researches the recent work by ANZCA fellows on women in the anaesthesia workforce.
Along with feasibility studies, survey research is a good place to start in research. Surveys are the only way to have a large-scale quantitative and often qualitative understanding of attitudes, knowledge, and practices. However, conducting
a good survey is harder than it looks. The ANZCA fellowship survey is an example of well-conducted survey research using mixed methods.
In my day job as an academic anaesthetist, I often have discussions with FANZCAs considering a PhD. One common misconception is that PhDs are primarily about new knowledge. Rather, that is the secondary aim; the primary aim is research training.
A PhD should be in an area that fascinates both the PhD student and their supervisors and can cover any area from pain receptors to frailty to simulation to cultural safety. ANZCA has specific research support for PhD students. Research isn’t for everyone, but if you think research might be your thing, start with your favourite hypotheses and consider your big questions. Ask questions that will get you out of bed in the morning. There are many fellows who can help you answer them.
Finally, why is normal saline acidic? The hypothesis was the effect of dissolved atmospheric carbon dioxide. However, that was about 10 per cent of the answer. The rest was complex acids from the plastic bags and ink on the outside of the bags.2
A definite surprise, and as often happens, a new set of questions.
Professor Dave Story ANZCA President
References
1. Story DA, Leslie K, French C. Feasibility and pilot studies: small steps before giant leaps. Anaesth Intensive Care. 2018 Jan;46(1):11-12.
2. Story DA, Thistlethwaite P, Bellomo R. The effect of PVC packaging on the acidity of 0.9% saline. Anaesth Intensive Care. 2000 Jun;28(3):287-92.
Workforce challenges continue
The Council of Presidents of Medical Colleges (CPMC) received a letter in September from Ahpra who was “pleased to confirm” they were on track to implement an expedited pathway for specialist international medical graduates (SIMGs).
ANZCA is less than pleased.
It means that SIMGs from the UK and Ireland will soon have open to them a different process that will allow them to bypass the medical colleges and be granted specialist registration to work in Australia more quickly.
The Australian Health Practitioner Regulation Agency (Ahpra) want this process to be in place for general practitioners in late October and for anaesthetists, obstetricians and gynaecologists, and psychiatrists in late December 2024. Other specialties will follow suit in 2025.
ANZCA and the CPMC have called for an immediate pause on the implementation of expedited pathways for SIMGs from the UK and Ireland and have sought clarity on how these SIMGs will be assessed to ensure patient safety.
We genuinely believe that patient safety in Australian hospitals is at risk and have called for an immediate pause on this short-sighted solution to the nation’s medical workforce problems.
We also believe that there is not enough focus on growing our own domestically trained doctors, a situation not helped by the relative stasis in university places for domestic medical student numbers over the past 10-15 years.
CPMC has formed an advocacy group, of which I am a member, to address some of the concerns about the push by government to become involved in roles that are traditionally the domain of the colleges.
Other areas of concern are scope of practice which threatens to blur critical professional boundaries without adequate safeguards, and new requirements for CPD homes (we are pushing for more clarity and an assurance of ongoing competence).
The lack of transparency, insufficient expert stakeholder consultation and potential overreach in decision-making processes is of concern to all of us.
But it is the SIMG expedited pathways issue – with deadlines fast approaching – that has become the most urgent.
We know that SIMGs play a vital role in our health system, and that to date, there has been a reliance on SIMGs to address workforce shortages, particularly in regional and rural settings where maldistribution of all medical specialists is an ongoing problem.
However, we are confident in our robust assessment processes that allow overseas trained doctors to work safely in our hospitals in a supportive environment. ANZCA exceeds the required timeframes in assessing SIMGs that seek specialist registration with Ahpra and ensures the competency of these specialists to meet required standards.
Certainly, we have always met and surpassed the standards set by government for processing applications quickly and effectively.
ANZCA and the CPMC have written to Ahpra with many questions about the new process, one of the recommendations of the so-called Kruk Report. Our primary concerns are:
The lack of targeted placements to ensure SIMGs are placed in areas of greatest need.
The risk of further concentration of specialists in urban areas or well-staffed specialties.
Insufficient long-term retention strategies to encourage SIMGs to remain in underserved areas or specialties.
The importance of efforts to train and retain domestically educated doctors.
The need for specialty-specific considerations for the unique challenges in different specialties and practice settings.
We are urging Ahpra to look at ways of addressing geographical maldistribution and specialty-specific shortages and to develop robust incentives and support systems for SIMGs in underserved areas and specialties.
Consultation with rural health stakeholders and specialtyspecific bodies is critical to this, as is the implementation of better monitoring and evaluation systems.
While concerned, we are committed to working collaboratively with the Medical Board of Australia, Ahpra, and other stakeholders to refine these pathways.
But this must not be at the expense of the high standards we enjoy in Australia and New Zealand.
Nigel Fidgeon ANZCA Chief Executive Officer
Make sure you’re not missing out on important information!
Keep your details up to date on the MyANZCA portal. We use the information on your MyANZCA profile for all of our official communications, including: Exam updates · Events and courses · Committee vacancies Safety alerts · Hospital rotations · Research opportunities
So please take a few minutes to check your personal details. It’s easy to do, and ensures you won’t miss out on important information.
1. Log into anzca.edu.au/portal
2. Click “Update my contact details”
3. Ensure your details are up-to-date and click “save”.
If you’re worried that you’re not receiving our emails, please check your junk and spam filters and, if necessary, add @anzca.edu.au or @anzca.org.nz to your address book.
Letters to the editor
NITROUS OXIDE LEAKS
Following the communication from Dr Akers and Dr Lightfoot in the Winter 2024 ANZCA Bulletin, I would like to highlight that most emissions from medical nitrous oxide are not related to its clinical use, but rather with the leak associated with reticulated nitrous oxide infrastructure.
Leaking nitrous oxide infrastructure has been repeatedly identified in hospitals.1-4 Whilst clinical use drives some demand, decreasing use of nitrous oxide is not necessarily associated with decreased emissions for a health service.5
Point of care nitrous oxide via cylinders can allow access to this useful drug while minimising waste at the cost of some inconvenience. Addressing leaked nitrous oxide has financial, societal, and environmental benefits. Supported by their colleges of anaesthetists and obstetricians the UK and Ireland are phasing out reticulated nitrous oxide manifolds by 2027.6
Is it possible to accomplish such a task for New Zealand and Australia?
Resources are available to help healthcare facilities transition to assist leak detection or transition to portable cylinder supply.7-8 This intervention should be simple in centres that anaesthetise mainly adults. The transition to point of care cylinders becomes a bit trickier, but not insurmountable, when a healthcare facility either has a birth suite or anaesthetises many paediatric cases.
The key is that nitrous oxide is supplied as a pressurised gas by a reticulated system that is prone to leakage. Large effort and expense above and beyond Australian standards would be required to keep the infrastructure leak free. The volumes clinically required in the modern era are already low and are dwarfed by the volumes purchased by healthcare facilities. We can and should do more to address nitrous oxide leak.
Whilst nitrous oxide leak is a significant driver of emissions, it is sensible to adopt less carbon intensive therapies, particularly when clinical equipoise exists.9
1. Chakera A, Mph B. Evidence-Based Policy Report: Reducing Environmental Emissions attributed to Piped Nitrous Oxide Products within NHS Hospitals. 2021;
2. Seglenieks R, Wong A, Pearson F, McGain F. Discrepancy between procurement and clinical use of nitrous oxide: waste not, want not. Vol. 128, British Journal of Anaesthesia. Elsevier Ltd; 2022. p. e32–4.
3. Gaff SJ, Chen VX, Kayak E. A weighing method for measuring nitrous oxide leakage from hospital manifold-pipeline networks. https:// doi.org/101177/0310057X231198123 [Internet]. 2023 Nov 25 [cited 2024 Apr 18];52(2):127–30. Available from: https://journals.sagepub.com/doi/ abs/10.1177/0310057X231198123?journalCode=aica
4. Skowno JJ, Kahlaee HR, Inglis AJ, McKinnon D, Asher K. Hospital-level flow measurement to detect nitrous oxide leakage. Anaesthesia [Internet]. 2024 Aug 1 [cited 2024 Jul 31];79(8):880–1. Available from: https://onlinelibrary.wiley. com/doi/full/10.1111/anae.16309
5. Hansen EE, Chiem JL, Righter-Foss K, Zha Y, Cockrell HC, Greenberg SLM, et al. Project SPRUCE: Saving Our Planet by Reducing Carbon Emissions, a Pediatric Anesthesia Sustainability Quality Improvement Initiative. Anesth Analg [Internet]. 2023 Jul 1 [cited 2024 Jul 12];137(1):98–107. Available from: https://journals.lww.com/anesthesiaanalgesia/fulltext/2023/07000/project_spruce__saving_ our_planet_by_reducing.11.aspx
6. Consensus Statement on the Removal of Pipeline Nitrous Oxide in the United Kingdom and Republic of Ireland Background. [cited 2024 Jul 31]; Available from: https://doi. org/10.1111/anae.16211
7. Chesebro B, Escalante J, Glass G, Hansen EE, Henkels G, Leigh J, et al. DISCONTINUING USE OF PIPED NITROUS OXIDE SYSTEMS IN HEALTHCARE FACILITIES [Internet]. 2024 [cited 2024 Apr 18]. Available from: https:// practicegreenhealth.org/sites/default/files/2024-03/ Cascaida%20Collaborative_Discontinuing%20N20%20 Playbook_V1.pdf
8. Kayak EEBJSCWJC, McGain F, Burch H, Dunne B, Gu Y, Davies J, et al. Detecting and reducing nitrous oxide leaks in healthcare facilities [Internet]. Canberra; 2024 Aug [cited 2024 Sep 5]. Available from: https://www.health.gov. au/resources/publications/detecting-and-reducing-leaksfrom-nitrous-oxide-in-healthcare-facilities-a-practicalguide?language=en
9. Peyton PJ, Leslie K. The safety of nitrous oxide: glass halffull or half-empty? Br J Anaesth [Internet]. 2024 [cited 2024 Jul 31]; Available from: https://pubmed.ncbi.nlm.nih. gov/38816332/
AMATEUR CLIMATOLOGISTS MISGUIDED
Two letters in the recent Winter ANZCA Bulletin discuss the imperative of maintaining diversity in the practice of anaesthesia.
Currently there is great threat to the practice and art of anaesthesia by the relentless momentum adversely narrowing the specialty, as a dictatorial, formulaic, colour by numbers, almost bullying approach to the provision of anaesthesia increasingly prevails.
If the only tool in the shed is a hammer, it follows that everything then looks like a nail.
The widescreen panorama of anaesthesia is being reduced to monochromatic total intravenous anaesthesia (TIVA) as the elimination of gaseous and volatile agents is deafeningly advocated by well meaning, environmentally concerned, often more recently qualified specialists, supported by hospitals with strong financial opposition to desflurane.
I object to colleagues attempting to dictate my anaesthetic palette.
Registrars come through the system with little experience of anything but TIVA, which is but one tool in the anaesthetic shed.
Nitrous oxide is a proven, invaluable anaesthetic agent.
The anaesthetic downside is minimal and the environmental impact slight.1 The delivery of nitrous oxide is the real problem.2 Desflurane is the perfect adjunct to nitrous oxide for relaxant general anaesthetics.
This combination used in parsimonious fashion for paediatric, bariatric, orthognathic and geriatric anaesthesia is unmatched and unmatchable.
Anecdotally there has been a cluster of awareness associated with TIVA in my locality, despite the use of electroencephalogram (EEG) monitoring.
Use of nitrous oxide, rather than air, greatly mitigates potential awareness and adding a volatile agent gives further security.
Anaesthetists wearing the cap of amateur climatologists decry desflurane and nitrous oxide environmentally.
But when a renowned international climatologist and her anaesthetist daughter in the UK publish a paper in the British Journal of Anaesthesia, 3 refuting the claims on desflurane’s environmental carnage, this is ignored, as it doesn’t fit prevailing enthusiastic, but very possibly misguided dogma.
As I write, I read an email from a major private hospital group in my locality, unbelievably announcing the environmentally irresponsible introduction of single use disposable theatre wear, despite the trumpeted removal of desflurane from this hospital group.
Dr Stuart Skyrme-Jones, FANZCA Richmond, Victoria
References
1. Gadani H and Vyas A. Anaesthetic gases and global warming. Potentials, prevention and future anaesthesia Anaesth Essays Res 2011;5(1)5-10
2. Smith E and Mitchell C. The importance of tackling leaks in nitrous oxide pipes. Autumn 2023 ANZCA Bulletin 2 p. 58-9
3. Slingo and Slingo. Climate impacts of Anaesthesia.
4. British Journal of Anaesthesia, vol 126 June 2021
ANAESTHESIA PRACTICE
In response to Dr Louis George’s letter in the Winter 2024 ANZCA Bulletin I appreciate that anaesthesia is a field where many varying practices exist, all of which are valid.
Providing a patient is comfortable during a procedure and experiences a post-operative period with minimal side effects, what does it matter how an anaesthetist chooses to use the drugs and skills in their armament to achieve the goals? While our drugs have varying costs, the highest cost to the system comes from adverse events. I would encourage anaesthetic practitioners to continue using vasopressors to maintain physiologic blood pressures if that complements their anaesthetic of choice.
It is not clear to me what Dr George’s specific concerns with the practice are? If it is cost, then although I have not done a strict cost analysis of desflurane versus sevoflurane anaesthesia, my memory was that desflurane is a more expensive per dollar amount to administer.
Discussing a need to give a drug to counter effects – my memory of using desflurane is that one always needed significantly more sympatholytic drugs such as opiates, alpha2 adrenergic agonists or short-acting beta-agonists (SABAs) to enable smooth induction and emergence. Despite this, I respect the choice of other practitioners to use it if they desire and have found satisfactory ways to maintain safe clinical practice using the drug. In exchange, I would hope they respect my educated choice to achieve the same result in a different way.
When talking to primary candidates about knowing about the widest variety of anaesthetic agents possible, I liken us to being mixologists in a cocktail bar. We are presented with ingredients and tools (medications, airways, monitoring), make an assessment of the customer in front of us (patients) and acknowledge the vibe of the bar overall (surgeons).
How we mix that cocktail combines artistry and science; it may vary between mixologists but we should learn and respect rather than criticise differences in practices.
Dr Claire Stewart, FANZCA Westmead, NSW
The views expressed by letter writers do not necessarily reflect those of ANZCA.
What we’re talking about
Facebook
STEUART HENDERSON AWARD
The most popular post on Facebook was a video with one of the 2024 Steuart Henderson Award recipients Dr Alex Konstantatos. This post reached 1867 people and had more than 260 post engagements (reactions, shares, comments and clicks). The award is presented to a fellow who has demonstrated excellence and provided outstanding contribution, scholarship and mentorship to medical education in the field of anaesthesia and/or pain medicine.
The video features Dr Konstantatos speaking about his background in medical education and what winning the award means to him.
Media
IV FLUID SHORTAGE
ANZCA President Professor Dave Story featured prominently in Australian media commenting on the Australian IV fluid shortage. He was interviewed for ABC Radio’s flagship AM program on 15 August, ABC Radio Sydney’s Afternoons program, ABC online and WIN TV News (syndicated to news feeds in Canberra, Hobart, Orange, Toowoomba, Rockhampton and Wagga Wagga).
Coverage also included an interview for ABC TV’s Afternoon Briefing program and segments from the interview were used in ABC nightly news bulletins in Sydney, Melbourne, Perth, Hobart, Brisbane and Canberra reaching more than two million people. Professor Story was interviewed by the Herald Sun for a page 1 article on Saturday 24 August. The article was syndicated to 14 other news sites.
NSW fellow Dr Mark Priestley of Westmead Hospital was also interviewed on ABC Radio Sydney’s Mornings program on 15 August for a 10 minute segment explaining why IV fluid solutions are used.
Instagram
ENVIRONMENTAL
SUSTAINABILITY
Our most popular post on Instagram was promoting the ANZCA Environmental Sustainability Network webinar “Clearing the air: Understanding and managing nitrous oxide”. The interactive discussion of identification and management of nitrous oxide leaks in healthcare services was held on 22 August.
Four expert speakers shared their knowledge and experiences and provided valuable perspectives and guidance on leak mitigation.
The Instagram post received 1412 impressions and 16 interactions.
X (formerly Twitter)
IV FLUID SUPPLY AND SURGERY
ANZCA councillor Associate Professor Stu Marshall featured in The Conversation on 19 August with an article “Australia’s IV fluids shortage will likely last all year. Here’s what that means for surgeries.”
ANZCA shared the article on X and it received 1000 impressions.
A/Prof Marshall noted that one way to work around the shortage “is to minimise how much IV fluid is used during the procedure. This can be achieved by ensuring those admitted to surgery are as well hydrated as possible.”
“Monitoring of the supplies and ongoing honest and open dialogue between senior health managers and clinicians will be crucial in minimising the disruption to surgical services.”
For every intubation. Even the strange ones.
The HEINE visionPRO video laryngoscope.
For fast and reliable intubation, nothing is more important than the best view of the glottis. The HEINE visionPRO video laryngoscope provides just that with the one of a kind HEINE allBRIGHT display – even in very bright ambient light.
At the same time, the HEINE visionPRO is extremely robust, reliable and durable. To be as environmentally friendly as possible, we chose a rechargeable lithium battery and are the first to provide a blade made from upcycled material. More on heine.com
Scan here to request demonstration
VICTORIAN MINISTER VISITS
Professor Paul Myles, the founding chair of ANZCA CTN and Director of Research, Department of Anaesthesiology and Perioperative Medicine at The Alfred hospital and Monash University, recently hosted the Victorian Health Minister, Mary-Anne Thomas, on a recent visit to his research group at The Alfred in Melbourne.
The minister heard about perioperative clinical trials, how their conduct can be integrated into public hospitals and how they can inform current clinical practices.
ABOVE
From left: Health Minister Mary-Anne Thomas, Professor Paul Myles and research manager Sophie Wallace
ANZCA & government
We work with national, state and territory governments and their agencies to ensure we're appropriately consulted on decisions affecting our members; the health systems they work within; and their ability to provide every patient with safe, high-quality, and culturally competent care.
Progress update on workforce reform strategies
HEALTH MINISTERS MEETING
ANZCA President Professor Dave Story attended a faceto-face meeting with all nine Australian health ministers, specialist medical college presidents, the Australian Medical Council (AMC), the National Health Practitioner Ombudsman (NHPO), Medical Board of Australia (MBA) and the Australian Health Practitioner Regulation Agency (Ahpra) to discuss progress on reforms and improvements for the medical specialist workforce in Australia.
The discussion focused on improving training site accreditation processes and implementing the priorities of the so-called Kruk Review including establishing fast-track registration pathways and streamlined assessment processes for specialist international medical graduates (SIMGs). Ministers also explored ongoing challenges with medical workforce distribution across Australia as identified in the National Medical Workforce Strategy 2021-2031.
Attendees committed to continue working on strategies that would grow, distribute and sustain the workforce, supporting Australians to access the care they need, when and where they need it. Actions included:
• Specialist medical colleges will continue to work with jurisdictions, and other key stakeholders, on strategies to deliver the medical workforce in the right numbers and in the right locations (particularly in rural and regional areas) and to build the generalist capability of the medical workforce.
• Commitment to continue sharing workforce distribution, supply and demand data to provide an evidence base for national workforce planning.
• Specialist medical colleges, the AMC, Ahpra and MBA will continue to develop and implement expedited pathways for SIMGs, reducing the wait time to receive an outcome regarding their competency and ability to work in Australia’s health system.
TRAINING SITE ACCREDITATION FORUM
An Australian Medical Council (AMC) and Health Workforce Taskforce one-day accreditation forum was held recently to explore how medical colleges and health services can work together on concerns and complaints about accredited specialist medical training sites.
ANZCA representatives included President Professor Dave Story, Chief Executive Officer Mr Nigel Fidgeon, Training Accreditation Committee Chair Dr Mark Young and ANZCA Anaesthesia Training Program Manager Sharne Westlake.
A set of draft standards was developed with input from key stakeholders.
MEDICAL WORKFORCE ADVISORY COLLABORATION
The college attended the inaugural Medical Workforce Advisory Collaboration meeting as one of the five specialist medical college positions represented on this jurisdictional forum to advise federal, state and territory health ministers on medical workforce matters.
The group will oversee ongoing implementation and evaluation of the National Medical Workforce Strategy 20212031 and will seek to match medical workforce planning to community needs. The collaboration will attend an upcoming Council of Presidents of Medical Colleges meeting to talk about priority work including streamlining recruitment, selection criteria to increase rural and First Nations doctors, and building the generalist workforce.
ANAESTHETIST WORKFORCE MODELLING
The college attended a health workforce roundtable hosted by the Australian Society of Anaesthetists to launch the release of their Anaesthetist Workforce Modelling Final Report, providing a 10-year forecast and assessment of the sustainability of Australia’s anaesthetist workforce.
The launch was attended by colleges, peak bodies and parliamentary representatives. The meeting and report provided an assessment of the sustainability and shortage of Australia’s anaesthetist workforce and discussed the shared challenges of other specialties, particularly in regional, rural and remote communities.
EXPEDITED REGISTRATION PATHWAY FOR SPECIALIST INTERNATIONAL MEDICAL GRADUATES (SIMG s )
A key agenda driven by the federal government is the proposed expedited pathway for SIMGs. Anaesthesia is one of the four medical specialties that have been identified as a priority for implementation by the end of 2024. This pathway will bypass existing medical college assessment processes (for agreed qualifications) and Ahpra will conduct paper-based assessment of SIMGs and then approve them for specialist registration in Australia. The Medical Council of New Zealand is looking at a similar pathway, issuing a consultation request, to which ANZCA has provided a response.
ANZCA acknowledges that internationally qualified health practitioners play a vital role in our health system and are needed to supplement critical vacancies in the short term. However, we would like to continue to work with governments to increase local trainee numbers as a longerterm or large-scale strategy for specialist staffing recruitment. We recognise that any changes will significantly impact a key area of operation for the college and further, has potential adverse implications for anaesthesia training,
legal responsibility of clinicians, required cultural safety and community awareness, and training site accreditation into the future. ANZCA is continuing to engage with Ahpra through this process of development and advocate for the need for colleges to be involved in the assessment process. We will communicate known information via news items, newsletter updates and ANZCA Bulletin articles, as they become available.
NSW SPECIAL COMMISSION OF INQUIRY INTO HEALTHCARE FUNDING
Following ANZCA’s submission to the inquiry in late 2023, the college met with inquiry representatives in late May 2024 to discuss the topics in our submission. Representatives from our NSW Regional Committee provided the commissioners with a better understanding of evidence sought for the July and August hearings relating to workforce and training.
As part of the inquiry ANZCA have compiled and provided a response relating to training and accreditation policies and procedures as part of a “summons to produce documents” request, as well as a “witness statement” addressing a range of factual and evaluative questions.
Former NSW Regional Committee Chair Dr Michelle Moyle and current committee co-chair Dr Frances Page provided verbal evidence over three and a half hours at a hearing on 24 July 2024. The hearing covered the following key items:
• Role of the college in training and assessment and in advocacy.
• Overview of site accreditation process.
• Role of the college in safety and quality.
• Centralised recruitment.
• Workforce shortages and increases in service demand.
• Specialist Training Program (STP) and Integrated Rural Training Pipeline (IRTP) funding streams.
• Perioperative medicine.
• Award reform.
The second stage of the workforce hearings is expected in October 2024 and will focus on the identification and consideration of potential responses and solutions to the circumstances, issues and challenges identified during the first stage of the workforce hearings. The inquiry report is due to be delivered to the NSW government by late March 2025.
NEW ZEALAND HEALTH REFORM
In late July, following news of budget overspends, the board overseeing Health New Zealand/Te Whatu Ora was replaced by a single health minister-appointed commissioner, Dr Lester Levy, a former board member. He has since selected two deputy commissioners, Ken Whelan and Roger Jarrold.
Moves to configure the national hospital sector into four regions are continuing, but there is considerable uncertainty about progress with the formation of clinical networks, and health workforce.
Pressures within the service are acute in the primary care, aged and disability care sectors, with knock-on impact on emergency department hospital space for acute surgical admissions. There is also uncertainty about many major capital projects around the country, including hospital rebuilds.
While officially “no hiring freeze is in place”, clinicians on the frontline report difficulties advertising for vacancies, or even in some cases, completing recruitment processes for senior doctors even after job offers have been extended. Approvals for resident medical officer rotation recruitment, while slower this year than previously, now appear to have been made, relieving some of the uncertainty for trainees about their training pathways.
SUBMISSIONS
The college prepares submissions and makes representations to government and other stakeholders on a range of policy initiatives and inquiries, many of these in response to requests for college feedback and input. Our submissions to public inquiries are available on the college website following the inquiry closing date. Note that some inquiries and requests for college input are confidential. For a listing of recent submissions visit www.anzca.edu.au/safety-advocacy/advocacy.
Australia
• Department of Health and Aged Care: Independent Review of the National Registration and Accreditation Scheme.
• Health Workforce Taskforce: Assessment of communication protocol implementation.
• Medical Board of Australia: Draft revised registration standard: specialist registration.
• NSW Ministry of Health: Composition of health professional councils.
• Parliament of NSW : Special commission of inquiry into the funding of healthcare services provided in New South Wales summons to provide evidence.
• Parliament of NSW: Special commission of inquiry into the funding of healthcare services provided in New South Wales witness statement.
• SA Health: Anaesthesia and sedation in South Australia.
• SA Health: South Australian health climate change framework.
• Victorian Department of Health: Inquiry into women’s pain.
• Victorian Department of Health: Guideline for providers of liposuction.
New Zealand
• Health and Disability Commissioner/Te Toihau Hauora, Hauātanga: Review of the Health and Disability Commissioner Act 1994 and the Code of Health and Disability Services Consumers’ Rights.
• Medical Sciences Council of New Zealand/Te Kaunihera Pūtaiao Hauora O Aotearoa: Proposed changes to supervision of anaesthetic technicians.
• Medical Council of New Zealand/Te Kaunihera Rata o Aotearoa: Expedited pathway for registration in the provisional vocational scope of practice.
• Ministry of Health/Manatū Hauora: End of Life Choice Act review.
Become a locum anaesthetist and see Australia
Rural LAP has unique and rewarding opportunities for specialist and GP anaesthetists to provide quality healthcare in rural and remote communities throughout Australia.
As a locum, you will receive your salary, daily incentives and all your travel and accommodation provided.
Take advantage of this great opportunity and apply now
The importance of open communication
ANZCA’s Directors of Professional Affairs Policy, Dr Michelle Mulligan and Professor David A Scott, explain why an open disclosure process is so important for patient and clinician.
HOW CAN WE DO IT BETTER?
Adverse events and medical error remain a problem associated with the delivery of modern anaesthesia despite ongoing efforts to reduce them. In the past, clinicians and managers sometimes adopted a defensive approach to patient safety incidents. Even if a doctor wanted to apologise and felt that it was the right thing to do, they were not always advised to do so.
Patients and families were left feeling frustrated and angry when they were unable to get an explanation about what happened. Staff reported experiencing sadness, guilt and remorse because of not being able to provide information to patients and their families.
Full disclosure, apology, and open communication between doctors and patients has been shown to more effectively address the needs of patients and carers, clinicians and managers. Clinicians need not fear that their apologies, or other empathic words or gestures will later be used against them in formal proceedings. In fact, patients and their families have indicated that receiving a sincere apology was the most meaningful aspect of open disclosure.
At a minimum, an open disclosure process must include:
• An apology or expression of regret.
• A factual explanation of what occurred, including actual consequences.
• An opportunity for the affected patient to relate their experience.
• The steps taken to manage the event and prevent its recurrence.
An incident may be caused by several things. In anaesthesia practice it is most commonly because of something going wrong during the patient’s anaesthetic that was unplanned or unintended. It can also occur from a recognised risk inherent to treatment, for example, nerve damage following a nerve block. Or it can also occur because the patient did not receive their planned or expected treatment, for example, they did not receive their preoperative medication as ordered and required.
The objective of open disclosure is to provide information with sensitivity and empathy, including discussing arrangements for further support and ongoing care if required. Open disclosure may involve one discussion or may continue over a series of meetings. The duration will depend on the incident, the needs of the patient and/or their support person(s), how the investigation into the incident progresses, and whether there are ongoing health care
Adverse events may happen despite the best of care
needs because of the incident. There is not one standardised way to conduct open disclosure. Flexibility is required to meet specific circumstances and the needs of patients, their support person(s) and healthcare staff.
An expression of regret (“saying sorry”) is an important part of acknowledging the event and its impact. Done appropriately and sincerely it will not signify fault or expose the practitioner to potential blame.
The explanation of the event, and expression of regret, may need to be undertaken on more than one meeting with the patient and/or their family or carers. In anaesthesia it is not always easy to be available when such a meeting occurs, but it is important to make every attempt to be present and contribute. This reflects your empathy and concern as well as ensuring that accurate information is shared.
If a patient does not have the physical or mental ability (“capacity”) to participate in the disclosure discussion, their support person(s) must be notified and involved until the patient is able to fully participate and make decisions on their own behalf.
The five essential elements of open disclosure are an apology, a factual explanation of what happened, an opportunity for the patient to relate their experience, a discussion of the potential consequences, and an explanation of the steps being taken to manage the issues.
In addition to the essential elements above, effective open disclosure also includes:
• Acknowledging to the patient and/or their support person(s) when things go wrong.
• Listening and responding appropriately when the patient and/or their support person(s) relate their experiences, concerns and feelings
• The opportunity for the patient and/or their support person(s) to ask questions and to have those questions answered
• Providing support for patients and their support person(s) and health care staff to cope with the physical and psychological consequences of what happened.
• Providing information that reassures the patient that, wherever possible, steps will be taken to decrease the likelihood of such an event recurring.
“…nobody would acknowledge my account of what happened… the anaesthetist was freaking out and as white as a sheet... I’ve not been well since... The junior doctor was the only one who called me. They inferred I was being a princess and were quite dismissive… I’m worried about my family, this could happen to them too… No one is taking me seriously…”
(quote from a patient with an anaesthetic-specific complication under general anaesthesia).
While the event itself may not be foreseeable, actions taken at the time, including methods of communication, may be important to review and improve.
Ideally, disclosure should occur within 24 hours at a time that meets the needs of the patient and/or their support persons.
The Statutory Duty of Candour (SDC) has, in some jurisdictions, added additional legal requirements following a serious adverse event where significant patient harm occurred. This is modelled on the SDC process that was introduced in the UK National Health Service in response to findings of the 2013 Mid Staffordshire inquiry.
The SDC supports a culture of openness and transparency and also provides a level of objective scrutiny which can be used to identify and implement changes, if needed, to improve patient safety.
The SDC process is quite formal and includes notifying the health department and providing the patient with:
• A written account of the facts regarding the event.
• An apology for the harm suffered by the patient.
• A description of the health service entity’s response to the event.
• The steps that the health service entity has taken to prevent re-occurrence of the event.
• Further actions including conducting a SDC review meeting within 10 days of the event (a patient may elect not to participate if they so choose).
Every healthcare professional should know they might face many such events at any time during their career. Recognising that open discussion may not be an easy thing to do, discussion with a dependable trusted colleagues and seniors to analyse the adverse event conducted in a setting devoid of accusations and blame is a good idea.
ANZCA’s Supporting professionalism and performance – A guide for anaesthetists and pain medicine physicians (2024) provides guidance as a framework for understanding our professionalism and performance, including how we should communicate. Adverse events may happen despite the best of care, or as failings within the health service or delivery of care. How we respond to these events reflects our compassion and professionalism and can lead to improved outcomes for all concerned in the future.
Dr Michelle Mulligan, FANZCA and Professor David A Scott, FANZCA FFPMANZCA ANZCA Directors Professional Affairs, Policy
Acknowledgements:
www.cec.health.nsw.gov.au Open Disclosure Handbook https://www.safetyandquality.gov.au/sites/default/ files/2021-09/open-disclosure-principles-elements-andprocess_9.pdf
ANZCA's inaugural Course in Perioperative Medicine is in it's final trimester as we work towards developing a Chapter of Perioperative Medicine by the end of the year.
Private regional service tackles overwhelming demand
St Vincent’s Private Hospital Toowoomba (SVPHT) is a regional, private 190 bed hospital that performs 12,000 procedures/surgeries per year.
Our project was initiated because the pre-existing anaesthesia pre-assessment clinic was experiencing overwhelming demand. We created a comprehensive perioperative care service (PoCS) that allows for integrated nursing, medical and allied health communication, learning and collaborative care.
The clinic aligns with the mission and values by delivering person-centred care by ensuring the patients are informed and optimised for their anaesthesia and surgery. Our overarching objectives include enhancing patient flow, reducing cancellations, mitigating hospital acquired complications (HACs), and optimising the overall patient experience by leveraging evidence-informed approaches that are contextualised to patients.
METHOD/ACTIVITIES UNDERTAKEN
The former pre-anaesthetic clinic faced capacity challenges in 2019, serving about 600 patients annually with the support of four anaesthetist-intensivists. To address this, we introduced triage criteria to identify high-risk patients for our facility and defined what constitutes perioperative risk for SVPHT.
We then initiated a high-risk clinic for patients with the requirement that patients be seen before being given a
ABOVE
“Day-ofprocedure cancellations have become negligible, leading to improved patient flow.”
date for operation − a novel approach in private practice. The high-risk clinic serves as a platform for comprehensive risk assessment, shared decision-making, goals-of-care discussions, and advanced resuscitation planning, all of which are becoming ingrained in the culture of SVPHT.
Over the past two years we have expanded the PoCS clinics by engaging a visiting medical officer clinical lead and incorporating nursing, geriatrician, anaesthetist, anaesthetistintensivist, and physician clinics.
Increased administrative support has significantly reduced the burden on nursing staff allowing them to focus on nursing related tasks. We have also pursued allied health engagement.
Furthermore, we are developing evidence-based perioperative protocols and pathways to address common queries, resulting in decreased variability. These include a perioperative diabetic medication protocol and developing complex surgical pathways.
Continuous quality improvement is fostered through quarterly meetings where we address challenges, propose solutions, discuss morbidity and mortality, and explore ways to optimise service delivery, including the utilisation of information technology solutions (telehealth, Webpas, Microsoft Teams, messaging and artificial intelligence).
We are refining ways to collect data on patients’ journeys through the clinic and their surgical stays, including HACs, which enables us to monitor progress and identify areas for further improvement.
The perioperative care service (PoCS) team at St Vincent’s Private Hospital Toowoomba.
RESULTS
While we cannot say that all outcome variables shown here are directly attributable to the development of the PoCS service, the following data does demonstrate significant improvements in key quality indicators coincident with the establishment of the service and the culture change it has brought.
The PoCS service has witnessed a notable increase in patient volume, with the number of patients served rising from 600 to 922 in 2023 (a 50 per cent increase).
Notably, the high-risk clinic has experienced a doubling in referrals, illustrating growing acceptance and demand. Impressively, the high-risk clinic exhibits a decision to not pursue surgery at a rate of only 16 per cent, indicative of patients proceeding to operations following appropriate risk stratification, shared decision-making, and comprehensive discussions on goals of care and advanced resuscitation planning.
Furthermore, the service has successfully averted marginal benefit surgeries that would have posed a risk of significant perioperative complications and mortality risk. Day-ofprocedure cancellations have become negligible, leading to improved patient flow.
"The PoCS service has witnessed a notable increase in patient volume, with the number of patients served rising from 600 to 922 in 2023."
Additionally, elective surgical medical emergency team (MET) calls as a proportion of all surgical MET calls have decreased, as has unplanned intensive-care unit admissions for elective surgical patients. The latter is an important perioperative HAC which may well incur a hospital financial penalty in the future (figure 5 and 6).
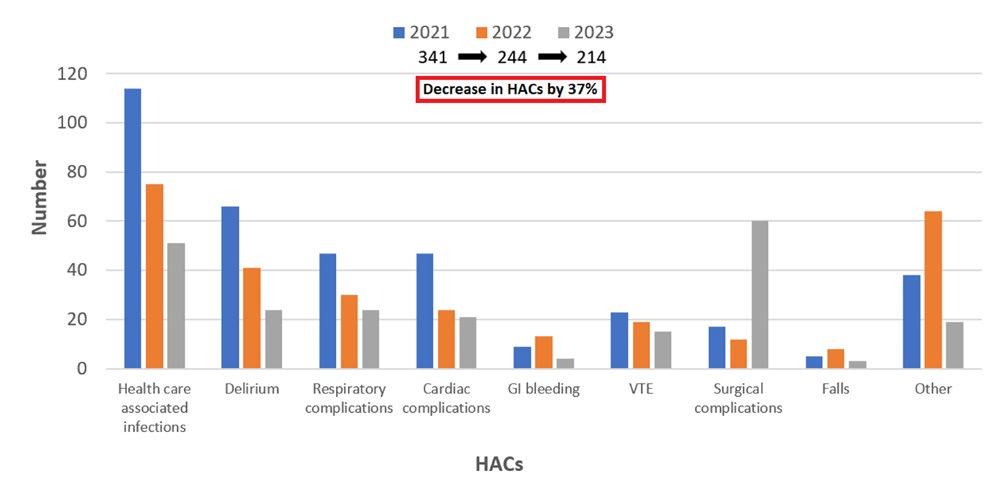
Across the board, our facility has decreased HACs by 37 per cent due to enhanced clinical documentation.
PoCS is likely to also have had an impact on this, as many HACs are related to surgery or a procedure (figure 7). Our efforts now target preventable surgical HACs, particularly delirium.
6 – Percentage of unplanned elective surgical admissions to ICU as a proportion of all surgical ICU admissions by year.
Figure 5 – Percentage of elective surgical MET calls as a proportion of all surgical MET calls by year
Figure
Figure 7 - How HACs have decreased over the last three financial years
Incorporating a patient feedback survey has yielded overwhelmingly positive responses in terms of our communication, usefulness and satisfaction with the service.
One of the most transformative changes observed at our regional private hospital is the gradual shift towards proactive decision-making concerning high-risk surgeries and at-risk patients.
CONCLUSION
The PoCS project is delivering contemporary, patientcentred care to elective surgical patients. It has contributed to improved surgical outcomes while considering the economic realities of working in the private medical environment.
Although we have made gains, we must remain dedicated to minimising HACs, continually enhancing patient outcomes, and reducing length of stay safely. Further efficiencies will come with comprehensive support for patients transitioning to home care through innovations such as tailored nurse navigation.
The project encountered various obstacles.
Initially, securing investment from the executive proved challenging, as this area of the hospital does not generate direct revenue. Nevertheless, the trust bestowed upon us by the executive have yielded positive outcomes.
We also recognise the necessity of acquiring higher-fidelity data concerning the economic impact of our service downstream. Overcoming the strong drivers towards early surgery and justification of a pause for appropriate risk stratification and optimisation have been other important aspects of our journey.
The project has helped establish collaborative decisionmaking and comprehensive patient optimisation within SVPHT.
“Continuous quality improvement is fostered through quarterly meetings where we address challenges, propose solutions, discuss morbidity and mortality, and explore ways to optimise service delivery.”
FUTURE DIRECTIONS
Moving forward, our focus is on establishing a self-sustaining system and continuing to decrease HACs and improve patient outcomes and their experience.
We are currently looking at ways to focus more attention on higher risk patients while streamlining lower-risk patient to surgery while minimising the touch points, they have with the service.
Dr Jeremy Fernando, FANZCA Director of Intensive Care and Clinical Lead of the Perioperative Care Service
St Vincent’s Hospital, Toowoomba
Simulation training model a success for Queensland
An anaesthesia simulation training program that is unique to Queensland has just notched up a significant milestone.
The Rural Perioperative Team Training Program, an initiative of the Statewide Anaesthesia and Perioperative Care Clinical Network (SWAPNet), has been delivered 40 times across 26 hospital operating theatres in rural and remote communities since 2019.
The program enhances the skills and knowledge of healthcare professionals with hands-on skill development sessions and crisis management scenarios using a state of the art/life like manikin by a faculty team consisting of an anaesthetist, surgeon and perioperative nurse.
ANZCA councillor and SWAPNet co-chair, Queensland anaesthetist Associate Professor David Sturgess, says the two-day training program sessions have addressed an urgent and ever-increasing need for training for staff working in the perioperative environment in rural and remote Queensland.
“The program not only aligns well with ANZCA’s perioperative medicine model but also has a strong focus on simulation training in rural and regional sites, the areas of greatest need for workforce resourcing,” he explains.
Associate Professor Sturgess says SWAPNet principal project officer Karen Hamilton has played a key role in the success of the project which is now being eyed by other states as a possible training model.
“She organises 12 deliveries a year across Queensland and really is the ‘eyes and ears’ of the program.”
Ms Hamilton, who has managed the SWAPNet for more than 15 years, says the feedback from participants has been so positive with many highlighting the program as a catalyst for change in practice at their hospitals.
“In some hospitals, you can actually physically see a change in culture over the two days of training as the hierarchy breaks down and staff begin to feel more and more that they are now part of a supportive, cohesive team,” she explains.
“They’re empowered to speak up and as a team, identify opportunities for improvement. We had one case where the hospital’s theatre team and maternity team had not been able to agree on processes for three years and by the end of the two-day session they were working together well.”
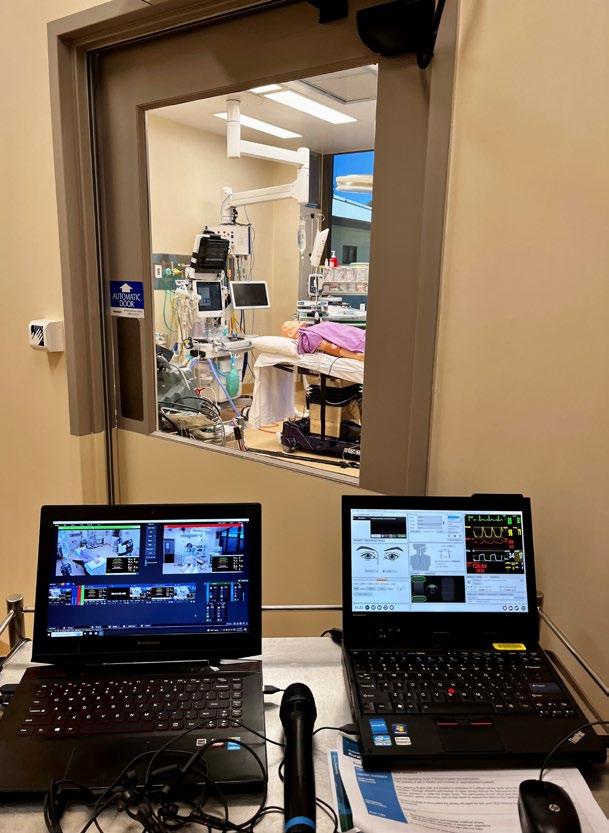
The training is conducted using a state-of-the-art manikin that has a pulse, blinks, breathes, speaks, bleeds and births a baby that cries.
“Real drugs are administered, operations are performed and the manikin accurately responds to the treatment provided at the time,” Ms Hamilton says.
“It’s as real as we can make it and we are constantly being told by participants that it is the best and most life like simulation they have ever experienced.”
ABOVE AND RIGHT
The simulation training program is conducted using a state of the art manakin that has a pulse, blinks, breaths, speaks, bleeds and births a baby that cries.
The scenarios are adapted to reflect local emergency cases, conditions and practice at each site.
The participants debrief after each scenario to identify what they did well and what could be changed/modified to ensure they are better prepared for real emergency situations.
She says the program has been a game changer for clinicians working in remote and regional hospitals.
“Previously, clinicians were expected to learn on the job under the guidance of a more senior staff member who more often than not, had limited capacity to train. The other alternatives for staff were to attend training off-site at regional and metropolitan facilities or train online.
“Staffing limitations in rural and remote locations meant that staff could not be backfilled to attend training off-site and when it was possible, the training environment in larger facilities was very different to their local rural environment and therefore transferability was a significant factor. Online training was also particularly limited, was not effective and did not deliver the training required.
“The success of the program can be attributed to its design which is based on what rural sites told us they needed, not what we thought they might want. We provide a safe, confidential, trusting environment where mistakes are embraced as opportunities for learning and training.
Participants remain in their day-to-day roles throughout the two days of training, there is no role playing.”
Associate Professor Sturgess believes the training program can have a long-lasting impact on staff retention.
“One of the things that I get a real sense of is the impact it can make on the retention of staff. If you can bring state of the art training to them and make it relevant it can make a difference. They have greater satisfaction in their roles and hopefully that translates to higher workforce retention rates.
“Staff tend to stay where they train so being able to deliver this to their local environment is a huge plus.”
Carolyn Jones Media Manager, ANZCA
Self matters
Kintsugi – the art of inner leadership
This edition focuses on how we might grow from our personal and professional experiences of loss.
It is a privilege to present Dr Olivia Ong’s piece on how she has reckoned with the physical and emotional impacts of an horrific accident. Her experiences have led her to support colleagues through coaching and mentoring. We all face an uncertain future. Any one of us might find ourselves on the other side of the healthcare equation – through trauma, illness, fertility-related intervention, ageing. Professional challenges also come to mind, especially those arising from the pandemic and our overstretched health systems. There is much to learn from Dr Ong about how to face and reframe life’s losses, and how this can lead to growth and healing.
As always, if you, or someone you know, has a wellbeing story you’d like to tell, please email me at bulletin@anzca.edu.au
Dr Lindy Roberts, AM FANZCA FFPMANZCA
On a fine spring day in 2008, my life changed forever. I was walking through the carpark of the hospital where I worked when suddenly I was hit by a car at high speed.
I landed with an earth-shattering thud.
I had a spinal cord injury and lost the ability to walk.
As I shared in the December 2021 edition of the Bulletin, 1 orthopaedic surgeons told me I would be in a wheelchair for the rest of my life.
My self-worth plummeted to rock bottom. I so badly needed to walk again. Not only because I wanted to be mobile, but because I wanted my identity back. Even an identity that lacked self-worth and self-confidence.
One day I heard about Project Walk, a centre for spinal cord injury recovery in San Diego in the US. At first, I thought the state-of-the-art technology was what was going to help me, but after three years there, I learned a far more powerful life lesson. This I discovered by myself in my time at Project Walk: kintsugi
Kintsugi is an ancient Japanese art that repairs broken ceramics with gold to make them stronger and more beautiful. In the 1400s, Japanese craftsmen started using precious metals to bond together pieces of pottery, thereby drawing attention to, rather than away from, the breaks. This made the break the most important part of the piece itself.
The first time I saw a piece of kintsugi, it was an epiphany. I realised that I too had been broken, but I was still here, repaired, proud of my experiences and my scars, and stronger than ever.
I share my experiences now because I believe kintsugi is a powerful metaphor for self-development. Like the golden fault lines running through the pottery, just as we are broken, we can be repaired – and the manner of that repair, the learning in that growth, becomes a strong and beautiful part of who we are.
When you come through a period of crisis — the loss of a job, a divorce, a serious illness — you can realise that the difficult times can be a powerful motive for change and the chance of a new, happier, more deeply lived life.
For healthcare professionals, kintsugi offers us the opportunity to reflect on the growth we might experience following difficult events, whether they are in the workplace or our personal lives. The Physician Wellness Task Force at McGill University in Canada used the concept of kintsugi to explore some of the ‘golden cracks’ physicians had found following the trauma of the COVID-19 pandemic.2 Physicians identified positive outcomes including accelerated research, increased collaboration across departments, and a greater focus on the mental health of healthcare professionals.
The gold used in kintsugi is significant – it’s strong but beautiful, and, most importantly, noticeable. It signifies the strength, confidence and value we can put into repairing our own breaks. As medical professionals, we can embrace these breaks to enrich our medical practice. For example, doctors who have personally experienced illness reported that it improved their ability to communicate and empathise with their patients.3
Kintsugi encourages us to live a full, rich authentic life, unafraid of the things that might break us. Both ceramics and life can break into a thousand pieces, but that’s no reason to stop living life intensely, working intensely and keeping all our hopes and dreams alive. Adversity is nothing more than a challenge; we just have to work out the right training to overcome it.
Kintsugi marks our progress. As we grow in strength, we also start to chart our own journey. Whether we have physical scars – I have a 20cm vertical scar on my upper and lower back from surgery to stabilise my spine – or mental ones, the golden joinery of kintsugi ensures we do not forget what led us to this point and what we have done to move forward. We shouldn’t conceal our repairs – they are proof of our strength.
References
Dr Olivia Ong, FFPMANZCA FAFRM Monash Health and Advance Healthcare, Victoria
1. Learning to walk again a catalyst for change. ANZCA Bulletin Summer 2021:68.
2. Dobkin PL. Kintsugi mind: How clinicians can be restored rather than broken by the pandemic. Can Fam Physician. 2022 Apr;68(4):252-254. doi: 10.46747/cfp.6804252.
3. Woolf, K., Cave, J., McManus, I.C. et al. 'It gives you an understanding you can't get from any book.' The relationship between medical students' and doctors' personal illness experiences and their performance: a qualitative and quantitative study. BMC Med Educ 7, 50 (2007). https://doi.org/10.1186/1472-6920-7-50
HELP IS ALSO AVAILABLE VIA THE
Doctors’ Health Advisory Services:
NSW and ACT 02 9437 6552
NT and SA 08 8366 0250
Queensland 07 3833 4352
Tasmania and Victoria 03 9280 8712
WA 08 9321 3098
Aotearoa New Zealand 0800 471 2654
Lifeline 13 11 14 beyondblue 1300 224 636
Free ANZCA Doctors’ Support Program
How to make an appointment:
To speak with a counsellor over the phone or make an appointment to see a consultant for a face-to-face session:
• Telephone 1300 687 327 in Australia or 0800 666 367 in New Zealand.
• Email eap@convergeintl.com.au.
• Identify yourself as an ANZCA/FPM fellow, trainee or SIMG (or a family member).
• Appointments are available from 8am to 6pm MondayFriday (excluding public holidays).
• 24/7 emergency telephone counselling is available.
WELLBEING HUBS
For Aboriginal and/or Torres Strait Islander Peoples Australian Indigenous HealthInfoNet. Connection. Strength. Resilience. Social and Emotional Wellbeing Resources at https://healthinfonet.ecu.edu.au/learn/ special-topics/voice-referendum-social-emotionalwellbeing-resources/
For Māori Kaupapa Māori wellbeing services at https://www.wellbeingsupport.health.nz/availablewellbeing-support/kaupapa-maori-wellbeing-services/ Te Aka Whai Ora website at https://www.teakawhaiora.nz/ our-work/advocating-for-change/rongoa/ Te Whare Tapa Whā at https://www.teakawhaiora.nz/ngarauemi-resources/te-whare-tapa-wha/
Four-legged friend is a hospital hit
Auckland City Hospital has a new staff member helping to treat patients with acute pain – and he’s cute, furry, and walks on all fours.
Gus is a two-year-old labrador/golden retriever cross, and is owned by consultant anaesthetist Lora Pencheva.
Dr Pencheva, who works for the hospital’s acute pain service, said the idea of using Gus for pet therapy came to her after she saw other therapy animals in the hospital.
“It all started when I saw some pets around the hospital, and I approached one of the handlers and they told me I could make my pet into a therapy dog.”
The hospital has recently completed a six-month trial with Gus visiting once a month to go on rounds with Dr Pencheva.
Before beginning the trial, Gus was assessed by Canine Friends Pet Therapy to ensure he was suited to the role of a therapy dog.
Being approved as a therapy dog was no easy task – among other tests, Gus’s ears and tail were pulled to gauge his patience, and he was also checked to see how he handled busy environments and whether he was distracted by unusual scents.
Additionally, Dr Pencheva needed Gus to be approved by the hospital’s charge nurses, who also indicated the patients who would most benefit from pet therapy.
The hospital’s communications team created posters of Gus to alert patients to his presence in the wards, and even made sure he had a hospital identity card.
Dr Pencheva said because of his popularity, Gus’s visits had to be tightly-controlled.
“We’d walk on the ward, and everyone was squealing, people were taking their phones out to take selfies – but we have to carefully select who sees him.
“The interaction has to be supervised and it has to be structured. It can’t just be ‘come and pat a dog’. You have to get the position right and see what the patient wants to do.
And the therapy itself is guided by the patient.”
The hospital followed the Canine Friends Pet Therapy welfare policy, ensuring Gus received adequate rest, and reward in the form of encouragement, treats, and time for play at the nearby Auckland Domain.
Dr Pencheva said the reaction to Gus had been overwhelmingly positive.
“Sometimes people just want to sit there and talk about their pet, or sometimes a pet that died many years ago.
“Some other people throw away their pain pumps and get themselves up from the bed, just so they can touch the dog.
“I just let the patients guide me and do the thing that works best for them.”
Gus has been good for the anaesthetists too – Dr Pencheva said her colleagues supported the initiative and even allowed Gus to spend time in the anaesthesia department office.
“This is important as pet therapy has been shown to mitigate burnout and increase resilience among medical staff.”
And it’s not just about cuddles and pats.
Dr Pencheva said international studies had established a connection between pet therapy and lower blood pressure and better cardiovascular outcomes. One study had even linked pet therapy to better pain scores for people recovering from knee surgery.
Now the trial has been completed, one of Dr Pencheva’s staff is carrying out a survey to gauge reaction to the therapy dog idea.
If the feedback is positive, Gus is likely to become a permanent fixture at the hospital – giving new hope for patients looking to find a way to ‘paws’ their pain.
Reon Suddaby Senior Communications Advisor New Zealand, ANZCA
LEFT
Dr Lora Pencheva has been joined at Auckland City Hospital by her two-year-old labrador/golden retriever cross Gus.
SHAPING
THE FUTURE TOGETHER
29 April – 1 May 2025
Thala Beach Nature Reserve, Port Douglas
Are you an emerging leader in anaesthesia or pain medicine?
Do you want to meet and learn from likeminded emerging leaders? Do you want to enhance your leadership within your workplace? Are you within five years of fellowship (taking into account career disruption)?
THEN APPLY NOW FOR THE 2025 ELC!
To apply, simply complete the online application form available on the meeting webpage (available via the QR code) and email a copy of your curriculum vitae to the meeting organiser (events@anzca.edu.au) by Wednesday 23 October 2024. Successful applicants will be notified in mid-December.
THINKING OF APPLYING FOR THE 2025 EMERGING LEADERS CONFERENCE?
Check out what a few of our 2024 delegates had to say about their experience.
We thoroughly enjoyed the opportunity to attend the 2024 ELC: “Breaking Barriers” in the picturesque Gold Coast hinterland. The dynamic presentations, small group reflection sessions and mentor groups provided us with the valuable opportunity to swap ideas, challenge our own biases and be inspired on our own leadership journeys. We all felt really privileged to have had the time with the incredible speakers, and to be allowed to see their vulnerability. Despite the full program the convenors did a wonderful job of promoting networking and facilitating introductions amongst delegates. We were all inspired to continue to embrace the challenges that come with effective leadership and to celebrate the new connections and global friendships. We would like to thank the Queensland Regional Committee for selecting us to attend and thank ANZCA for continuing to fund this exceptional conference.
Dr Thar Lwin FANZCA, Dr Anna Pietzsch FANZCA, Dr Hannah Bellwood FANZCA and Dr Georgie Cameron FANZCA
SCAN TO APPLY
Held in wonderful Wanggeriburra land (Mt Tamborine) the ELC was three days of challenging, thought-provoking and intellectual talks.
Nothing was off limits as our ANZCA leaders were asked challenging questions about First Nation representation in ANZCA, world political issues and the media’s portrayal of our specialty. The overarching theme of “what it means to be a leader” was underscored by intermittent round table discussions on topics such as unconscious bias, imposter syndrome and the ever quoted “falling” into the roles that so many of us find.
There were triggering times but for the most part it was an inspiring experience to talk with like-minded individuals about the future of our specialty and building networks to begin the process of improving it as best as we can.
Dr Angus McNally FANZCA
Attending the ANZCA Emerging Leaders Conference is a once in a career opportunity. I encourage you to apply if you are within five years of obtaining your fellowship (with allowances for time off for extended or parental leave) and have or are considering a leadership role.
I feel very fortunate to have attended the 2024 ELC against the beautiful backdrop of Cedar Creek Lodges, Mt Tamborine. I met an amazing and inspiring group of leaders from ANZCA and the broader medical and non-medical community and had the opportunity to listen to their journeys and words of wisdom. I also met an amazing and inspiring group of colleagues from many different backgrounds.
A recurring message during the ELC was to “Find your WHY” or “horizon” – to consider what inspires you, what you would like to achieve in future, how you might get there, what might block the view, and what may enhance it. It has led me to reflect since on my own WHY, personal attributes, strengths, and personal barriers.
Seize this opportunity. It is more than worth it.
Dr Rachel Sara FANZCA, FFPMANZCA
CPD cycle ending –what you need to do
All your CPD requirements must be completed by 31 December 2024, regardless of whether you have been selected for verification.
As the end of your 2024 continuing professional development (CPD) cycle is fast approaching, here’s what you need to know to prepare:
VERIFICATION (AUDIT) SELECTION
Each year, in line with regulatory requirements, 7 per cent of our fellowship is randomly selected for verification (audit).
This year’s audit marks the first verification since the introduction of the updated annual CPD program, as no audit was conducted in 2023. For the 2024 CPD cycle just over 500 fellows were chosen for verification and received email notification from the college in late August.
COMPLETING YOUR CPD REQUIREMENTS
All your CPD requirements must be completed by 31 December 2024, regardless of whether you have been selected for verification. Unfortunately, you won’t be able to use CPD activities completed in January 2025 to fulfill your 2024 CPD requirements.
If you have been selected for verification, you must also upload evidence of completion of your CPD activities. Any CPD activities that auto-populate to your online CPD portfolio, such as the ANZCA Annual Scientific Meeting, FPM Symposium or Learn@ANZCA courses, do not require evidence. However, any CPD activity entered manually will require evidence of completion. You must upload evidence by 31 December 2024.
You will only need to upload evidence of your minimum CPD requirements. You can check your minimum CPD requirements in the CPD handbook. If you have completed more than your minimum CPD requirements, you don’t need to provide evidence for all your activities/hours. Our CPD team needs to verify only your minimum CPD requirements.
TRANSITIONING TO THE 2025 CPD CYCLE
On 1 January 2025, if your 2024 CPD requirements have been successfully met, you will transition to the 2025 CPD cycle. If you’ve been selected for the audit, you will transition to the 2025 CPD cycle once your minimum CPD requirements for 2024 have been successfully verified.
If you’re unsure what CPD activities you can complete to fulfill your requirements, please consult the CPD activity guide and the CPD handbook.
CPD APP
We’ve had more than 4300 downloads of the new CPD app! If you have yet to download our new CPD app, you can do so via the Apple or Google stores.
The CPD app complements the CPD portfolio and allows you to record CPD activities and track your progress “on the go”. You can upload evidence for your activities by taking pictures and attaching documents. You can also review your completed activities and confirm your pending activities.
Recently released features:
• Generate a statement of participation and certificate of completion directly from the app.
• Add activities and evidence, even if offline.
• Rate your activities.
Features coming soon:
• Complete your CPD plan and evaluation from the app.
• In-app and push notifications.
Multi-factor authentication (MFA) is important for protecting your data and is now required to access your CPD portfolio or app.
MULTI-FACTOR AUTHENTICATION FOR ENHANCED DATA SECURITY
We’re committed to enhancing your user experience while ensuring the security of your personal and professional data.
If you haven’t set up MFA, when you log into your CPD portfolio or app, you will see a pop-up message prompting you to set up MFA using an authenticator app of your choice. Just follow the instructions and you will be signed up to MFA in no time.
If you need additional assistance, look at the step-by-step guide, video and troubleshooting information on the ANZCA website. You can also email us at cpd@anzca.edu.au and suggest a suitable time for a team member to call and talk you through the steps to set up MFA.
COLLEGE CLOSURE
Lastly, please consider contacting the CPD team (cpd@anzca.edu.au) well ahead of the end of the year as the college will close from Tuesday 24 December 2024 until Monday 6 January 2025.
Central Queensland a scenic haven for nature lovers
In the latest of our Beyond City Limits series we travelled to central Queensland to Rockhampton and Mackay to find out why anaesthetists are attracted to the region.
Dr Ryan Williams thinks nothing of planning a weekend of sailing, fishing and swimming on a tropical island off the central Queensland coast when he finishes work at Mackay Base Hospital’s department of anaesthesia.
A day spent on Brampton Island or St Bees Island is the perfect antidote to his work on the full-time roster as the hospital’s Specialist Training Program (STP) anaesthesia trainee.
In the year that he has been based in Mackay he has embraced the local lifestyle and believes he possibly has more opportunities to develop a broader range of specialty skills than at a larger metropolitan hospital. It was a 10-week rural rotation as a medical student in the small Western Downs Queensland town of Jandowae, with a population of 1000, that prompted Dr Williams to pursue rural and regional health placements.
“I started out as a rural generalist trainee in Brisbane and after experiencing clinical practice in anaesthesia there I knew I wanted to focus on anaesthesia as my specialty. It’s such a supportive department here as trainees and consultants have a much stronger working relationship which you often don’t get at larger metropolitan centre hospitals.”
He says the advantage of working in a large regional centre such as Mackay is that he gets exposed to a range of general and regional anaesthesia procedures early in his training.
“Mackay performs a high volume of regional nerve blocks and anaesthesia trainees get very good exposure in all peripheral nerve blocks.”
Dr Williams attends the nearby private hospital for supervised training in high volume ear, nose and throat, paediatrics and ophthalmology lists.
The anaesthesia departments at Mackay Base Hospital and, 335 km south, Rockhampton Hospital, are keen to showcase the benefits of living and working outside metropolitan centres. Attracting consultants can be challenging but the anaesthesia departments at both central Queensland hospitals hope they can convince other fellows, specialist international medical graduates (SIMGs) and trainees of the benefits of settling there.
Dr Williams’ trainee colleague, Dr Homya Bolla, was born in Mackay and attended the local high school before enrolling in medical school at James Cook University in Townsville. She is an introductory trainee on the Queensland Anaesthetic Rotational Training Scheme (QARTS).
“It’s such a supportive department here as trainees and consultants have a much stronger working relationship which you often don’t get at larger metropolitan centre hospitals.”
ABOVE
Rockhampton's Kershaw Gardens waterfall is a popular spot with tourists and locals. LEFT
The seaside town of Yeppoon has its own sparkling blue lagoon. Photo: Siobhan Spence
Dr Bolla’s partner is a doctor and she knows it can be difficult to commit to a location for years at a time, especially when both are working in medicine.
She had just helped complete a theatre list at the Mackay Base Hospital when the ANZCA Bulletin met her in the anaesthesia department.
“I was at medical school and was considering doing renal medicine but I did my first anaesthesia rotation here and loved it. The department is super supportive and I would love to stay on here after my training as I have already been given a lot of opportunities such as presenting posters for the Mackay Anaesthesia Community (MAC) conference that I might not have had access to in a larger metropolitan hospital.”
The department encourages its trainees to work on research and audit projects, and to participate in the annual Mackay conference.
Some non-Queensland fellows and trainees will be familiar with the MAC conference which is held as a three-day annual meeting as a joint event with the Anaesthesia Continuing Education Rural SIG meeting each year. This year’s meeting has been postponed but senior staff specialist anaesthetist Dr Suresh Singaravelu hopes it will return next year.
Dr Singaravelu moved to Mackay with his wife, a dentist, seven years ago from Liverpool in the UK where he had been practising as a consultant anaesthetist with the National Health Service.
“The reality is that we are in competition with the larger cities and centres for consultants and we’re hoping that will change over time.”
Research is a priority for the department, says Dr Singaravelu, with trainees encouraged to participate in studies and projects.
“We have established a reputation for punching above our weight in research projects under the leadership of clinical director Dr Danny Bartlett.”
Dr Singaravelu is principal investigator at Mackay Base Hospital for both the SNaPP (Sugammadex, Neostigmine and Postoperative Pulmonary Complication) and Vapor-C (Volatile Anaesthesia and Perioperative Outcomes Related to Cancer) clinical trials.
The central Queensland climate was one of the drawcards for the Singaravelu family’s move to the region along with the breadth of the clinical work for Dr Singaravelu at Mackay.
“The challenge is not about attracting trainees to the region as most of our trainees are from Queensland. The area is also popular with specialist international medical graduates (SIMGs) but we want to encourage more consultants from other states to settle here.
“The reality is that we are in competition with the larger cities and centres for consultants and we’re hoping that will change over time.”
Mackay Base Hospital has also carved out a reputation for its focus on teaching led by supervisor of training (SOT) Dr Alexander Cottle. Originally from Melbourne, Dr Cottle moved to Mackay a decade ago and has been the SOT for the last nine years. Dr Bolla and Dr Williams can’t praise him enough for the guidance and preparation he gives to trainees to prepare them for their anaesthesia exams.
Dedicated teaching time is set aside for one afternoon each week so Dr Cottle and the hospital’s anaesthesia trainees can meet for regular catch-up preparation sessions.
After completing his early postgraduate years in Ballarat in regional Victoria, Dr Cottle moved to north Queensland for his anaesthesia training. The region’s main appeal for him is the local climate, bush walking and minimal traffic.
The Eungella rain forest is about an hour’s drive from Mackay and platypus sightings are common. The Whitsundays are close by, whale watching is popular, Brisbane is just over an hour’s flight away and Airlie Beach is less than a two-hour drive.
“The SOT role doesn’t appeal to everyone but it was a natural progression for me. Even as a trainee I found myself helping others prepare for the primary exam with queries around pharmacology and physiology and short answer practice questions. I try to steer the trainees in the right direction and identify those who might need some extra guidance early on, usually about nine months out from the exam,” Dr Cottle explains.
LEFT
Mackay Base Hospital's anaesthesia trainees Dr Ryan Williams and Dr Homya Bolla.
Photo: Fiona Kroll
ABOVE
Rockhampton anaesthetists
Dr Thiago Moreira and Dr Sheila Kalashetty.
All four of Dr Cottle’s trainees sitting the primary exam last year passed, three of them on their first attempt.
“We are mindful not to just focus on the clinical work here,” he says. We have a nicely balanced set up here that also involves research and all our trainees are supported by structured mentoring and training.”
Nearly 350km south from Mackay, anaesthetists Dr Thiago Moreira and Dr Sheila Kalashetty explain what attracted them to the 300-bed Rockhampton Hospital that services the surrounding population of about 230,000 people. High risk maternity cases are transferred to Brisbane and the hospital covers similar surgery and procedures of other regional hospitals with the exception of bariatric surgery, neurolology, vascular or interventional radiology, and interventional cardiology.
Indigenous patients comprise between 25 and 30 per cent of the hospital’s patients, many of whom require ongoing treatment for type 1 diabetes and associated complications.
Mining and agriculture are the area’s main economic drivers.
Dr Kalashetty moved to Rockhampton two years ago as an SIMG with her family from the Midlands in the UK. Her twin daughters attend the local school and her home is a threeminute drive from the hospital.
As the SOT and obstetric lead at the hospital she ensures that the anaesthesia training program is given dedicated teaching time once a week on Thursday afternoons.
“This enables us to work with the trainees as they prepare for their exams,” she explains.
“This is a strong focus of our department as we want to ensure our trainees have the best opportunity to complete their training with the appropriate support.”
The smooth sands of Yeppoon beach with its adjacent lagoon are a pleasant 40-minute drive from Rockhampton. Fishing and swimming are popular pastimes in the Capricorn Coast town 30km northeast of Rockhampton and the local streets feature cafes, restaurants and shops and galleries showcasing local wares and handcrafts. Known as the gateway to the Great Barrier Reef and Heron Island, Rockhampton and its surrounds also attract visitors to the nearby Capricorn Caves and lush Kershaw Gardens.
Dr Moreira arrived in Rockhampton five years ago having completed his anaesthesia training in his homeland Brazil. Like Dr Kalashetty he and his family enjoy the Rockhampton lifestyle.
“My 14-year-old son and 12-year-old daughter are the main reasons why we love living here,” he explains.
“I walk to and from the hospital from home two to three times a week as we live in the same street as the hospital. The children have settled in well and compared to our previous home in Perth. Rockhampton is much more manageable. It’s the perfect ‘tripod’ of school, work and home.
“It’s a great place to work and such a welcoming group. We take care of each other and we’re more like friends than coworkers,” Dr Moreira explains.
“It can be challenging because of the lack of permanent staff as this means there is a flow on effect on our waiting lists. It can be hard to ‘sell’ regional areas to specialists when larger cities are also recruiting in Queensland – we’re competing with other centres such as Logan, Ipswich, Toowoomba, and the Sunshine Coast.”
Carolyn Jones Media Manager, ANZCA
DR IAN MACKAY
STP trainee, Rockhampton Hospital
“Rockhampton is a great training hospital and there is a lot of opportunity here.
“I’ve just come off night shift and had the usual emergency list to deal with – orthopaedics, a broken wrist and ankle, an epidural on the labour ward and an emergency caesarean. There’s a good range of clinical procedures and experience.
“I often have family and friends coming to visit because there are a lot of great camping spots.
“The team are very friendly here and we’ll often have dinner in the pub or go to a local trivia night. Carnarvon Gorge is great for camping and you can often catch concerts on Great Keppel Island.”
DR ELAYNE ANDERSON
Deputy director, Department of Anaesthesia, Mackay Base Hospital
“I work full-time and met my husband Dr Alex Cottle in Cairns in 2014. We have a three-year-old son and have settled in well here. Neither of us particularly like the hustle and bustle of big city life so it suits us here.
“It’s a small department but because of that we’re more like family with each other. We weren’t attracted to pursuing sub-specialty anaesthesia so the range of clinical work here ensures we get a bit of everything – emergency cases, hernia repairs, paediatric trauma cases.”
DR LEO LAM
Trainee, Rockhampton Hospital
“I was an STP-funded trainee in 2023 and I’m now preparing for the primary exam.
“Rockhampton is worlds apart from Canberra where I had my first hospital placement after my degree. The department here is very supportive and there is protected teaching time with consultants taking the time to help with viva practice and short answer questions.
“I’m interested in chronic pain and the hospital is looking at setting up a chronic pain service which would mean patients would not need to be referred to pain services in Townsville or Brisbane.
“I’ve joined the Badminton club and Yeppoon is just down the road. There’s also lots of local hikes, bush tracks and other social clubs depending on your interests.”
Palm Islanders benefit from new pain clinic
PALM ISLAND
Until early last year if Lex Wotton needed a chronic pain consultation he either had to take a two hour ferry trip, or a costly 20 minute plane ride from his Palm Island home to Townsville, and then a taxi ride onto the Townsville University Hospital to meet with a pain specialist.
Now, the Palm Island plumber is on his own country a few minutes’ drive from home talking to specialist pain medicine physician Dr Hannah Bennett at the persistent pain outreach clinic she runs in her role as joint clinical director of the North Queensland Persistent Pain Service.
After piloting the outreach service in 2023 with a grant from ANZCA’s Health Equity Projects Fund, Dr Bennett is a regular visitor to Palm Island with the clinic which not only treats patients, but also provides culturally safe and appropriate pain education five times a year. She and a Townsvillebased allied health team work on site at the Palm Island Community Company (PICC) Bwgcolman Healing Service with Aboriginal Health Workers employed by PICC.
The flight to Palm Island, 45 kilometres off the Queensland coast, takes 20 minutes from Townsville while a local ferry service from the town takes two hours.
Palm Islanders call themselves the Bwgcolman people which translates to “many tribes”. Bwgcolman are the historical owners on the land, whereas the traditional owners are known as the Manbarra people.
Palm Island is home to one of the largest Aboriginal communities in Australia with a population of about 3500, however during local events the population can grow to 4500.
For Mr Wotton and the estimated 2500 Palm Island locals who are active patients registered with PICC, the on-site
“Anyone needing treatment or a consultation would have had to previously go to the mainland, so this has been a huge change and of great benefit to the community.”
multi-disciplinary pain clinic provides a much-needed service that diagnoses, manages and treats their chronic pain.
A plumber for more than 30 years with a long medical history of injuries from his trade, Mr Wotton tells the ANZCA Bulletin that being able to meet with Dr Bennett on the island has made a big difference to how he manages his chronic pain.
“I know every manhole on the island but it took years for me to be diagnosed with a C5 problem on my spine. Twenty years ago a water pipe fell on me while I was working and I’ve also got carpal tunnel syndrome. I’ve had six reconstruction surgeries on my shoulder. I’m not as active as I used to be, but I know how important it is for us to understand our own bodies and to know when to seek help,” he explains.
“I’ve been doing a lot of things to try and understand the medical profession and understand what is happening to me. It took eight years for me to find out that a lot of my pain was caused by the problem with my C5.
“My whole life experience has prepared me in a lot of areas so I can deal with my pain and what I have learnt is that when pain affects you, you do need to try and find a solution that’s not always about medication,” Mr Wotton says.
“Every two months or so Dr Bennett and I get to see each other. I’m now tapering off some of my medication so I’m able to manage and learn to deal with my pain.”
Dr Bennett explains how while she and other colleagues from the Townsville University Hospital had been running a
ABOVE
Dr Hannah Bennett with patient Lex Wotton during a Palm Island consult.
medical outreach clinic on Palm Island since 2019 there was no dedicated multidisciplinary pain management clinic.
“It meant the community had to travel to Townsville for treatment − either by plane or ferry – and that was a barrier to being able to provide gold standard, multi-disciplinary pain treatment,” Dr Bennett explains.
“We worked with our local cultural practice co-ordinator in Townsville to help guide us on how we could develop an outreach clinic on the island and this extended to how we would phrase certain things. Simple language shifts are effective so that instead of talking to patients about their ‘persistent pain’ we talk to them about their ‘long lasting pain.’
“We also need to be flexible. We provide the same scope of care as in Townsville but the local community choose how and when they come to see us.”
“Palm Island patients receive an initial medical consultation so they can understand who we are, and we get to know them. We then work on developing a rapport and relationship before we move into the discussion about their pain, asking them what they understand about their pain and sharing pain management options with them. That has been a real shift in terms of the program being delivered here.
“Palm Island has a very long and complex history and there is a lot of multi-generational trauma. It has always been assumed that Indigenous communities have a very high pain threshold, but it’s more often the case that people living in remote communities haven’t felt empowered to seek pain relief. PICC has been a driving force behind the development of the program on Palm since 2020. Since then to now the program has further developed to onsite pain consultation and pain management.
“That power disparity within mainstream health systems often stops people from seeking medical care, so it is important that the community has a community controlled health centre here on their own land. The PICC-run Bwgcolman Healing Service provides a much safer space for the community, and the involvement of the local allied health workers means they have a relationship with people
“When pain affects you, you do need to try and find a solution that’s not always about medication.”
from the island and know how important it is to look after the mind, body and spirit.”
Dr Bennett says back pain is the most common cause of chronic pain consults on Palm Island along with knee pain, neuropathic pain, persistent chest pain and shoulder pain.
On the day the ANZCA Bulletin spent with Dr Bennett at the clinic she met with eight patients, including Mr Wotton.
Dr Bennett says the local Bwgcolman Healing Service health team plays a crucial role in the clinic, regularly meeting patients in their own homes and driving them to the clinic for their appointments.
Bwgcolman Healing team leader and Palm Island local Keira Blackley says the outreach pain clinic has been a positive move for the community.
“Anyone needing treatment or a consultation would have had to previously go to the mainland, so this has been a huge change and of great benefit to the community. One of our health workers can now go out to the patient on the island and have a little yarn with them so they can explain in their way. The health worker will then write notes for the doctor.
“Having our local health workers involved ensures cultural safety and making our community feel welcome and not maligned.
“Being a local myself I’ve had to go to Townsville for appointments so for others in the community who have limited education there can be a shame factor, particularly if they don’t have anyone to escort them. So having a service come here has been great for our community and very welcoming.
“They know they feel comfortable here when they come in and know that we support them as much as we can.”
Bwgcolman Healing GP Dr Alexander Pace has been travelling to the island for three days each week from Brisbane as part of the medical clinic team for the last two and a half years. He sees patients at the medical clinic and then refers them to the pain clinic if needed.
“Bringing services to Palm Island is important. There are often complex psychosocial issues at play for those with chronic
LEFT
The main beach on Bwgcolman (Palm Island).
pain, so being able to be treated within their own community helps break down the barriers to accessing care,” he explains.
“Noting that PICC has been operating a medical service on Palm Island since 2013, there has also been further changes to the services on Palm Island over the last four years with the main one being the move from the hospital as the main site of care for people to PICC transitioning to being a community controlled health organisation and taking over the main primary care service now known as the Bwgcolman Healing Service.
“A lot of people previously would have felt that the hospital system doesn’t look kindly on people with chronic pain. The fact that we are able to bridge that barrier has helped them feel their pain needs are met.
“It’s that wrap-around holistic care that we’re offering. The level of engagement with the pain clinic is high and that has a lot to do with cultural safety and the holistic approach we provide. Hannah is a great fit as a clinician for this environment and the opportunity for the community to know they can come here and yarn in a safe space if they need to is really important.”
The medical clinic is open from 8.30am-9pm Monday to Thursday, and from 8.30am to 4pm on Friday which enables locals to visit after work. The island also has a Queensland health department-run hospital with a 24-hour emergency department and a doctor on call at night.
Townsville physiotherapist Bede Ashley leads the North Queensland Persistent Pain Service’s team of allied health workers. They play a vital role in the Townsville University Hospital’s multi-disciplinary pain outreach services in Palm Island, Cairns, Mt Isa and Mackay.
The Townsville outreach clinic program receives funding through the Australian Government’s Department of Health’s “CheckUp” scheme which targets rural and remote medical services across Queensland. Recognising the benefits of allied health teams in medical programs such as the Palm Island pain clinic, the program recently extended the funding to include allied health practitioners.
“We’ve been able to send a multidisciplinary team to Palm Island three times so far and this includes myself as a physiotherapist, a psychologist, an occupational therapist and a nurse in addition to the doctor,” Mr Ashley explains.
“Anyone experiencing chronic pain has a story to tell but they often feel that they haven’t been fully listened to. On Palm Island we give patients time to tell their stories, often over several visits. Sometimes it can take multiple sessions or visits of storytelling before we can effectively start on a program with them. They need to feel understood and we need to develop trust. And that’s not just with the individual patients − building trust and rapport with the whole community is crucial.
“With Indigenous patients it can take a lot longer for them to feel comfortable talking to us about their pain. There is a lot of intergenerational trauma on the island so having that face to face interaction has made a difference. Telehealth services work well for some people but not all.
“Each time we go back to Palm Island we know that word of mouth is our strongest advocate.”
Carolyn Jones Media Manager, ANZCA
From top: Island locals regularly gather on the jetty; the Bwgcolman Healing Service plays a crucial role in the daily lives of locals; taking a quite stroll near the Healing Service; an information panel in the local library.
Photos: Siobhan Spence
Nominations for ANZCA Council Awards are now open
Award Title Criteria Eligibility
The highest award the college can bestow on its fellows. It recognises distinguished service to anaesthesia, perioperative medicine and/or pain medicine.
ANZCA Medal
ANZCA Council Citation
Recognises major contributions by fellows to the status of anaesthesia, intensive care, pain medicine or related specialties.
Awarded to an ANZCA fellow in recognition of significant contribution to a college project or ongoing college activities.
ANZCA Recognition Recognises significant contributions at a regional level to anaesthesia, perioperative medicine and/or pain medicine.
ANZCA Star
Awarded in recognition of those who make extraordinary and critically important contributions (clinical or non-clinical) in times of major disaster, conflict or in other circumstances outside the college.
It’s time to recognise the members of our college who make a difference to anaesthesia and pain medicine, with nominations for the 2024 ANZCA Council Awards now open.
ANZCA has a suite of awards that recognise the achievements and contributions of our fellows, trainees, specialist international medical graduates (SIMGs) and departments. The awards are a chance for our members to celebrate the contributions and outstanding achievements of individuals within their departments or communities.
For more information on the nomination process and selection criteria, visit the college website via www.anzca.edu.au/councilawards
Fellows of the college.
Fellows of the college.
Fellows, trainees and SIMGs of the college.
Fellow, trainee, SIMG of the college or department.
ENTRIES CLOSE ON FRIDAY 1 NOVEMBER 2024
The award recipients will be announced at the 2025 College Ceremony in Cairns as part of the 2025 ANZCA ASM on Saturday 3 May.
If you require assistance, please contact the membership services unit at membership@anzca.edu.au
close at 5pm AEDT on Friday 1 November.
Robert Orton Medal
Fellows of the college.
Submissions
Your Regional Organising Committee
Dr Andrew Potter, Convenor
Dr Daniel Foster, Scientific Co-convenor
Dr Danielle Volling-Geoghegan, Scientific Co-convenor
Dr Phuong Markman, Workshop Co-convenor
Dr Sonia Arwadi, Workshop Co-convenor
Dr Steve Durrant, ELC Co-convenor
Dr Monica Diczbalis, ELC Co-convenor
Dr James Sartain, Abstract and ePoster Convenor
Dr Nigel Thomson, Abstract and ePoster Convenor
Dr Hannah Bennett, FPM ASM Scientific Co-convenor
Dr Anju Tessa James, FPM ASM Scientific Co-convenor
Dr Aisha Bouhafs, Trainee Representative
A/Prof David Sturgess, ANZCA Councillor
A/Prof Stefan Dieleman, Scientific advisor
Call for abstracts now open
What’s more rewarding than showcasing your research at Australia and New Zealand’s premier anaesthesia and pain medicine meeting in front of more than 1800 engaged delegates? Join us for the 2025 ASM in Cairns, and submit your abstract for presentation now.
“We’re excited to be e-poster co-convenors for the 2025 ANZCA ASM and eagerly anticipate receiving abstracts on all aspects of anaesthesia and pain medicine from the operating room to the
Key dates
Program available
Late November 2024
ASM registrations open
Early December 2024
Abstract submissions close 19 January 2025 (11.59pm AEDT)
Abstract notification to authors
Early bird registration closes 11 March 2025 (11.59pm AEDT)
FPM Symposium 2 May 2025
ANZCA ASM 2-6 May 2025
Safety & quality
We're responsible for training, assessing and the continuing education of anaesthetists and specialist pain medicine physicians in Australia and New Zealand.
Avoiding excessive opioid prescribing on discharge
A recent publication by the TASMAN Collaborative1 highlights the importance of carefully considering the amount of analgesic medications, particularly opioids, prescribed on discharge after surgery.
This international prospective multicentre cohort study found that on average less than half of the opioid medication prescribed to adults on discharge after common surgical procedures was consumed within the first seven days.
Excessive and unnecessary opioid prescribing on discharge is associated with increased risk of individual and societal harms, including:
• Opioid-related adverse effects.
• Opioid-induced ventilatory impairment (OIVI).
• Persisting post-discharge opioid use (PPOU).
• Opioid misuse and diversion.
Post-surgical opioid prescribing is a significant contributor to the global opioid epidemic2.
Other findings from the study indicate that discharge prescribers are often poor at managing opioid-related adverse-effects and providing adequate patient information.
GENERAL PRINCIPLES FOR DISCHARGE OPIOID PRESCRIBING
1. Consider the amount of opioid used over the 24-48 hours prior to discharge.
2. If an opioid prescription is required, limit the prescription to a three to seven days’ supply.
3. Consider a prescription for laxatives and anti-emetics as required.
4. Avoid the prescription of modified-release opioids.
5. Ensure appropriate non-opioid analgesia has been optimised.
6. Provide patients with clear (preferably written) advice on:
• How to reduce and stop analgesic medications (starting with strong opioids) after discharge.
• How to safely store and dispose of excess medications.
• Non-pharmacological pain management and rehabilitation.
• Management of opioid related adverse effects.
• When and how to seek medical review if pain persists longer than expected or is increasing.
7. If you are concerned that a patient is at high risk of poor pain management or PPOU, consider verbal handover to their general practitioner or a transitional pain clinic.
Of those patients prescribed an opioid medication on discharge:
• Only 37 per cent received a prescription for a laxative.
• Only 22 per cent received a prescription for an antiemetic.
• Only 30.5 per cent received documented information on safe disposal of unused opioids.
Appendix 1 of ANZCA’s PS41(G) Position statement on acute pain management 20233 provides guidance on analgesic stewardship, including risk factors to be aware of for OIVI and PPOU; recommended approaches to opioid prescribing on discharge; recommendations for patient and carer communication and education; and recommendations for communication with primary healthcare.
More information on strategies that may be used to promote and introduce opioid stewardship can also be found in:
• The Australian Commission on Safety and Quality in Health Care Opioid Analgesic Stewardship in Acute Pain Clinical Care Standard (2022).
• The Resources for Opioid Stewardship Implementation (ROSI) available via the ANZCA website.
On
average, less than half of the opioid medication prescribed to adults on discharge after common surgical procedures was consumed within the first seven days.
The TASMAN collaborative has demonstrated the power of a worldwide frontline collective effort and I commend them for their valuable research.
They hope to contribute to procedure specific recommendations for post-discharge opioid prescribing in future.
Dr Rachel Sara, FANZCA, FFPMANZCA Member, ANZCA Safety and Quality Committee Member, FPMANZCA Professional Affairs Executive Committee (PAEC) Middlemore Hospital, New Zealand
References:
1. TASMAN Collaborative. Patterns of opioid use after surgical discharge: a multicentre, prospective cohort study in 25 countries. Anaesthesia. 2024; 79: 924-936 https://doi. org/10.1111/anae.16297
2. Levy B, Paulozzi L, Mack KA, Jones CM. Trends in opioid analgesic-prescribing rates by specialty, U.S., 2007–2012. Am J Prev Med. 2015; 49: 409–13 https://doi.org/10.1016/j. amepre.2015.02.020
5. Levy, N., Quinlan, J., El-Boghdadly, K., Fawcett, W.J., Agarwal, V., Bastable, R.B., Cox, F.J., de Boer, H.D., Dowdy, S.C., Hattingh, K., Knaggs, R.D., Mariano, E.R., Pelosi, P., Scott, M.J., Lobo, D.N. and Macintyre, P.E. (2021), An international multidisciplinary consensus statement on the prevention of opioid-related harm in adult surgical patients. Anaesthesia. 2021; 76: 520-536 https://doi.org/10.1111/ anae.15262
Applications for the Dr Ray Hader Award for Pastoral Care are now open
The Dr Ray Hader Award for Pastoral Care acknowledges the significant contribution by an ANZCA fellow or trainee to the welfare of one or more ANZCA trainees. The nature of such a contribution may be direct, in the form of support and encouragement, or indirect through educational initiatives or other strategies.
The award is named after Dr Ray Hader, a Victorian ANZCA trainee who died of an accidental drug overdose in 1998 after a long struggle with addiction. Established in memory of Dr Hader by his friend Dr Brandon Carp, this award promotes compassion and a focus on the welfare of anaesthetists, other colleagues, patients and the community. In 2012, Dr Carp agreed to continue sponsorship of the award and to expand the criteria to recognise the pastoral care element of trainee supervision.
The winner of the award receives $A2000 to be used for training or educational purposes. Any ANZCA fellow and/or trainee can be nominated for this award. View the full nomination process and application forms on our website.
Nominations must be emailed to training@anzca.edu.au by Monday 28 October 2024.
A fluid situation
Toward the end of July, ANZCA became aware of supply issues that were affecting the ready availability of IV fluid products.
At the Safety and Quality Committee (SQC) meeting on 19 July some members noted that public hospitals in NSW had been instructed to conserve supply by switching to lower volume bags or consider alternative intravenous administration practices. Other members were unaware of supply constraints affecting their hospitals.
The following week the issue became mainstream news following reports published on the ABC News and The Guardian websites, and prompted the college to issue a safety alert for anaesthetists.
At the time, the only authoritative statement about the situation was in a medicine shortage alert from the Therapeutic Goods Administration, which said that the shortages were due to multiple factors including global supply limitations, unexpected increases in demand, and manufacturing issues.
Subsequent speculative chatter suggested that supplies manufactured outside Australia had been diverted to higherpaying international customers or that the US military was stockpiling in anticipation of an escalation in the Middle East.
Given the uncertainty and varying reports about the impact of the shortage on anaesthesia practice, Associate Professor Joanna Sutherland issued guidance on sparing of intravenous fluid use in her capacity as SQC chair. The guidance covered preoperative, intraoperative and postoperative considerations and highlighted “SipTilSend”.
It seems that clinical measures to conserve IV fluid products will be required throughout the remainder of 2024 such that usage is at about 80 per cent of that used in 2023.
Baxter Healthcare provided the college with a briefing document on 12 August stating that they were manufacturing IV fluid products above historical volumes and were at full capacity at their plant in NSW, that they had not experienced any manufacturing issues in their supply of sterile medical fluids, and that they were pursuing several actions to further increase supply volumes.
Australian health ministers met on 16 August and issued a joint statement on IV fluids that provided reassurance that supply challenges were being addressed and that health services were continuing.
A cross-jurisdictional response group was convened to identify additional procurement opportunities while supply remains constrained. ANZCA President Professor Dave Story was invited to participate in this group.
On the basis of better quantitative data and modelling presented to the group, it seems that clinical measures to conserve IV fluid products will be required throughout the remainder of 2024 such that usage is at about 80 per cent of that used in 2023.
Overall, Australia seems to be avoiding a crisis rather than managing a response to one.
Demand for IV fluid products is likely to be exceeding actual usage, exacerbated by ordering and stock piling behaviours and logistics choke points.
Professor Story will continue to provide feedback from the response group and the college will update advice to anaesthetists as required via safety alerts and website news items.
Anaesthesia-related deaths
Death of 45-year old patient following vascular surgery
The NSW Special Committee Investigating Deaths Under Anaesthesia (SCIDUA) has been reviewing deaths associated with anaesthesia and sedation since 1960. Example cases from the 2019 special report are being reproduced in the ANZCA Bulletin in an effort to enhance reporting back to the medical community.
CASE 10 – VASCULAR SURGERY
A 45-year-old female for superficialisation of left arm AV fistula.
Background history
• End stage renal failure secondary to diabetes.
• Super-morbid obesity (BMI 70).
• Obesity hypoventilation syndrome.
• Pulmonary embolism on warfarin.
• Recent lower respiratory tract infection.
ANAESTHETIC DETAILS
Local anaesthetic with sedation was used for the case.
The patient was commenced on high flow nasal prongs and sedated with dexmedetomidine. Loading dose (68 µg) and then an infusion (34 µg/hr).
Cephazolin 2g was given. The patient was prepped and surgery commenced.
About 30 minutes into the procedure the patient complained of feeling short of breath and hot, saturations began to fall and then the patient lost consciousness, which progressed to a cardiorespiratory arrest. 200mg of suxamethonium was given, the patient was intubated, and CPR started. For 30 minutes resuscitation continued with PEA.
During resuscitation:
• Lung ultrasound showed no evidence of pneumothorax.
• TOE showed no obvious PE.
• No rash noted.
• Adrenaline 7mg and intralipid given.
• For the entire surgical procedure 21mls of 1% xylocaine with adrenaline had been given.
Postmortem showed mild atherosclerosis of coronary vessels and a heart blood tryptase of 478 µg/L indicative of anaphylaxis.
LEARNING POINTS
• It is very challenging to sedate someone with obstructive sleep apnoea. There is a very fine line between patient comfort and obstruction in this population.
• Always suspect anaphylaxis in a patient with a sudden cardiorespiratory deterioration.
• Anaphylaxis caused the patient’s death in this case but to what substance remains unclear.
• Resuscitation in obese patients is always difficult. Despite superb resuscitation efforts in this case the patient still died.
Source:
Clinical Excellence Commission, 2021. Activities of the Special Committee Investigating Deaths Under Anaesthesia, 2019 Special Report. Sydney, Australia. SHPN: (CEC) 210176; ISBN: 978-1-76081-648-3.
Fellows are encouraged to read the SCIDUA report in its entirety. The detailed cases and data analysis presented are paving the way forward to a more informative and educational mortality analysis.
Safety alerts
Safety alerts appear in the “Safety and quality news” section of the ANZCA E-newsletter each month.
A full list is available on the ANZCA website: www.anzca.edu.au/safety-advocacy/safety-alerts.
Recent alerts:
• Australian impact of regional and global shortage of intravenous solutions (26 July 2024)
webAIRS
Look-alike ampoules: Inadvertent clonidine and glycopyrrolate substitution
BACKGROUND
Medication errors are a leading cause of patient harm in anaesthesia, with substitution being the second most common type of medication error in Australia.1
Look-alike errors occur when medications are visually similar in packaging, size, shape or colour2. This predisposes clinicians to inadvertent substitution errors, potentially resulting in adverse patient outcomes3
Clonidine and glycopyrrolate, two commonly used drugs in anaesthesia, are particularly prone to look-alike errors due to their similar ampoule appearance (Figure 1). Both ampoules have a nearly identical size, shape, and colour, with clear glass and black text labels without any background, reducing visual contrast. Additionally, text on the label is printed in a similar font and size, contributing to potential confusion.
One of the few distinguishing features is the drug name itself, which is printed in a small font size on the label. This subtle difference may be easily overlooked, especially if the ampoules are not carefully examined before administration.
Clonidine, an alpha-2 adrenergic agonist, is used for its sedative, analgesic, and anxiolytic properties4
Glycopyrrolate, an anticholinergic agent, is often used in combination with neostigmine to reverse neuromuscular blockade at the end of a surgical procedure5, or to counteract vagal tone, bradycardia or for its anti-sialagogue properties. The inadvertent substitution of clonidine for glycopyrrolate, or vice versa, can lead to significant clinical consequences.
Administering clonidine instead of glycopyrrolate may result in sedation, significant bradycardia, hypotension and when intended for use with neostigmine, the effects from the unopposed excess acetylcholine activity at muscarinic acetylcholine receptors such as nausea, vomiting, diarrhoea, involuntary urination, bronchospasm, excessive salivation and airway secretions.
Conversely, administering glycopyrrolate instead of clonidine may lead to undesired anticholinergic effects, such as tachycardia, dry mouth, and urinary retention.
Despite the potential for harm, the incidence and characteristics of look-alike medication errors involving clonidine and glycopyrrolate in the Australasian anaesthesia setting have not been well described.
This article aims to analyse incident reports from the webAIRS database to identify common themes, contributing factors, and potential strategies to mitigate the risk of these errors in anaesthesia practice.
Figure 1: Example of look-alike clonidine and glycopyrrolate ampoules
METHODS
We conducted a narrative search across all incidents reported to webAIRS from 2009 until April 2024 where “clonidi” AND “glyco” were mentioned. Two reviewers independently selected incident reports from the search where a drug error with clonidine and glycopyrrolate was mentioned in the narrative. These were subsequently analysed in our study.
Incident reports were initially read to identify themes described in the report. A single incident report could generate multiple themes. Common themes as identified by reporters, or as interpreted by analysers were then identified for discussion.
RESULTS
A total of 28 incident reports were initially identified and of these, 11 incident reports were analysed in further detail as they involved drug errors where either clonidine or glycopyrrolate had been used where the other had been other intended. Most of these incidents (n=7, 64%) resulted in no harm, or minor and temporary reported potential implications to the patient (despite one patient being administered a total of 600microg of clonidine in error). Four of those incidents (36%) were classified as near misses, with the error being detected before the drug reached the patient.
Of the remaining four incidents, one of three incidences with 300microg of clonidine instead of 400microg glycopyrrolate with neostigmine reversal, resulted in minor harm, necessitating a medical emergency team call overnight due to hypotension and bradycardia but no ongoing sequelae.
The second was admitted to the ward overnight for monitoring without issue and discharged the following day.
The third, which wasn’t recognised at the time and given additional actual glycopyrrolate, had sedation with delayed emergence, mild bradycardia and hypotension, and some vomiting/reflux (prior to extubation) without significant sequelae.
In the final case, glycopyrrolate was administered epidurally instead of clonidine during an emergency caesarean delivery, the patient later developed hypertension and neurological symptoms consistent with pre-eclampsia which required an intensive care unit stay as part of the hospital’s protocol. This patient had also been administered ergometrine for poor uterine tone, however the glycopyrrolate may have contributed to the clinical picture.
Several common themes emerged from the analysis.
The most prevalent causative factor was the similarity in appearance between clonidine and glycopyrrolate ampoules (n=11, 100%). Other contributing factors include the proximity of the two drugs in storage (n=6, 55%), failure to check the medication before administration (n=8, 73%), distraction (n=2, 18%), and the occurrence of the error during emergence (n=8, 73%).
Additional factors, such as the emergency nature of cases (n=5, 45%), errors occurring around handovers (for example, when relieving) (n=1, 9%), stocking errors where wrong drug ampoules were placed in the designated trolley space (n=3, 23.1%), not wearing reading glasses (n=1, 9%) and clinician fatigue (n=2, 15.4%) were also identified.
Table 1: Common themes identified in incident reports involving clonidine and glycopyrrolate errors (note: many incidents have multiple themes)
The high-stress environment of emergency cases and the presence of distractions, such as handovers and fatigue, may further contribute to the likelihood of medication errors.
AVOIDING CLONIDINE AND GLYCOPYRROLATE DRUG ERRORS
Suggested strategies to avoid clonidine and glycopyrrolate drug errors include:
Ensuring that clonidine and glycopyrrolate are not stored in the same drawer or compartment, and certainly not next to each other (ACSQHC Principle 8.10, ANZCA PG51(A) 5.2.4).
Considering the application of ancillary labels warning of look-alike medications, although the practicality of this may be limited due to the small size of ampoules (ACSQHC Principle 9.5, ANZCA PG51(A) 5.2.4).
Leaving clonidine and glycopyrrolate ampoules in their original cardboard packaging until just before use (ACSQHC Principle 9.7, ANZCA PG51(A) 5.2.6).
Implementing standardised trolley layouts, including anaesthesia trolleys in outside areas and theatres (ACSQHC Principle 9.6, ANZCA PG51(A) 5.2.2).
Encouraging the purchase and use of pre-mixed neostigmine/glycopyrrolate ampoules (ACSQHC Principles 13.2, 13.7, 14.1, ANZCA PG51(A) 5.1.6).
Consider alternative suppliers with clear labelling and packaging (ANZCA PG51(A) 5.1.3). (See Figure 2)
Communicating changes in drug packaging or labelling to the department (ANZCA PG51(A) 5.1.4).
Rechecking ampoules prior to drawing up or injection (ANZCA PG51(A) 5.4.2).
Implementing an independent second check for intrathecal drugs, as highlighted by the case where glycopyrrolate was given intrathecally instead of clonidine (ANZCA PG51(A) 5.4.6).
DISCUSSION
This study highlights the potential for look-alike medication errors involving clonidine and glycopyrrolate in anaesthesia practice.
The visual similarity between the ampoules of these two drugs was the primary causative factor in all reported incidents. This finding reinforces the importance of addressing the issue of look-alike medications in healthcare settings.
The human factors surrounding these errors are multifaceted and include issues such as inattention, failure to follow proper medication checking procedures, and the occurrence of errors during critical phases of anaesthesia, particularly emergence, where cognitive load may be higher.
The high-stress environment of emergency cases and the presence of distractions, such as handovers and fatigue, may further contribute to the likelihood of medication errors. Notably, several of these contributing factors, including look-alike medications and handovers were identified in the 2021 analysis of webAIRS reports, and they continue to be a concern.1
To mitigate the risk of look-alike medication errors, several strategies can be implemented, as outlined in the Australian Commission on Safety and Quality in Health Care’s principles for the safe selection and storage of medicines document6,7 and ANZCA’s PG51(A) Guideline for the safe management and use of medications in anaesthesia 2021.8 Global campaigns, like EZDrugID (https://ezdrugid.org/index.html), continue with initiatives and petitions to the relevant regulatory bodies to implement improvements to drug packaging.
CONCLUSION
This analysis demonstrates that drug errors continue to occur in anaesthetic practice.
There is a significant need for mindful medication preparation for administration as well as proactive measures to prevent look-alike medication errors involving clonidine and glycopyrrolate, and other medications which may have similar-looking ampoules at present or in the future.
Departments may consider strategic placement of drug ampoules in the anaesthesia trolley, additional labelling, or use of the original boxes.
Anaesthetists should exercise care in ensuring that they are administering the right medication, and frequent discussions should occur regarding medications with similar appearance in stock.
Nonetheless there is a need to continue to advocate for the healthcare and pharmaceutical industries to develop safer and clearer ampoule designs with standardised colourcoding to reduce the risk of look-alike errors.
Dr Shawn Chieh Loong Lee, Dr Tim Basevi and the ANZTADC Case Report Writing Group
Figure 2: Alternative supply of clonidine and glycopyrrolate with different labelling
Faculty of Pain Medicine
Established in 1998, the Faculty of Pain Medicine (FPM) is the first multidisciplinary medical academy in the world devoted to education and training in pain medicine.
FPM expertise across medicine
I am constantly reminded of the extent to which pain medicine finds roles in the management of many conditions. This is reflected in the depth and breadth of training required to achieve competency across our field. Our expertise can help patients in areas as diverse as diabetes, intractable angina and advanced neurological disease, to name but a few. Our diverse fellowship allows training and strategy development across this wide range of clinical environments. An example of this has been the recent development of PS15(PM) Statement on the clinical approach to persistent pelvic pain including endometriosis-associated pain. An expert document development group, including multiple fellows holding dual qualifications with FPM and the Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG), has produced a comprehensive review of the current evidence to support treatment in this area. A key aspect of the paper is its focus on a multidisciplinary approach to symptom management as opposed to a potentially reductionist view of lesion management. While this may seem relatively new in the pelvic pain setting, it covers general principles that are familiar to pain medicine physicians working across many other disciplines where the correlation between pathology and pain experience is often poor.
The statement has been generally well received by both health professionals and consumer bodies. While some critical responses have been forwarded these appear to be driven by a misunderstanding of the purpose and scope of the statement, particularly with respect to the role of surgical intervention. The faculty has produced a list of frequently asked questions on our website relating to the paper that fellows can consult to address concerns expressed by patients and health providers.
The pelvic pain statement has been published at a time when approaches from other colleges have highlighted the benefits of applying pain management principles to their
own professional domains. The faculty recently endorsed the position paper “Management of Perioperative Pain in Adults for Surgeons” developed by the Royal Australasian College of Surgeons (RACS) in association with the faculty. The paper emphasises the need to adopt an evidence-based approach to both perioperative pain management as well as emphasising the caution required in the surgical management of painful disease.
Separately, colleagues from RANZCOG have developed proposals for learning outcomes relating to pain management in a broad range of conditions occurring within their specialist field. This includes pain occurring across many areas of gynaecological practice. Importantly, there are also important references to pain management approaches suitable for pregnant women. The sociopsychobiomedical approach promoted throughout faculty training features strongly among the learning outcomes.
Further collaboration with our RANZCOG colleagues will be welcomed.
PAIN DEVICE IMPLANT REGISTRY
After an extraordinarily hectic three months, FPM, in conjunction with the Hunter Medical Research Institute and the Neuromodulation Society of Australia and New Zealand (NSANZ) submitted a detailed and fully-costed grant proposal to the Australian federal government’s Medical Future Fund (MRFF). The proposal is to support development of a registry of implanted spinal pain management devices to include detailed technical and outcomes data. The grant application was endorsed by multiple consumer, professional, industry and insurance groups. The grant application also acknowledges a substantial “in-kind” contribution from faculty fellows.
The grant proposal was overseen by our immediate past-dean, Dr Kieran Davis. Kieran committed substantial time and effort to the project and I am sure I speak for all of us in thanking him.
DEVELOPING FLEXIBLE ACCREDITATION PATHWAYS FOR RURAL SETTINGS
The "Developing flexible accreditation pathways for rural settings project" has progressed with a number of encouraging signs to date. The original survey saw nearly 50 responses from interested fellows with useful additional commentary being received through separate channels. The project consultants have set out a number of options for further development, based on the initial survey results together with analysis of activities undertaken by other medical colleges. The second stage of the project has seen information from focus groups and individual interviews being aggregated to guide further policy development.
The project has already identified a number of options for training away from large metro regions. It is also clear that work in rural and remote settings can offer many important learning opportunities that may not be found in the typical urban setting.
This is a valuable project and I urge fellows to remain engaged with it.
Dr Dilip Kapur
FPM Dean
FPM news update
2024 NATIONAL PAIN WEEK
The faculty supported National Pain Week, an initiative by Chronic Pain Australia which is dedicated to raising awareness and improving the management of chronic pain. The annual event (22-28 July) aims to break the cycle of stigma, isolation, and mental health challenges that often accompany chronic pain.
FPM Dean Dr Dilip Kapur participated in a National Pain Week event, "ABC Pain Factory Investigation: Giving Consumers Clarity on Chronic Pain Surgical Options". The panel discussion provided clear, trustworthy guidance on managing chronic pain and explored surgical and nonsurgical options.
Associate Professor Mick Vagg, Director of Professional Affairs (FPM), participated in a webinar “The State of Pain: Unpacking the 2024 National Pain Survey”.
The newly released 2024 National Pain Report has found that pain doesn’t just affect the person living with the condition; it affects our entire economy, health care system and society.
Key insights from the 2024 National Pain Survey include:
• Impact on productivity: Nearly half of those with chronic pain are in their prime earning years, significantly impacting national productivity. Nearly half of survey respondents had to stop working because of their pain, and almost 30 per cent have had to limit their hours.
• Strain on relationships: Two-thirds of respondents said their condition strains family relationships. More than 60 per cent reported reduced intimacy or a struggle to have sex as a result of their pain. Four in 10 struggle to pick up, carry, or play with their children.
• Stigma and barriers for young Australians: Reverse ageism creates stigma and barriers to care for younger Australians, with nine in 10 respondents aged 18 to 34 reporting being ignored or dismissed by health professionals. Significantly more in this age group have had thoughts of self-harm, taking their own life, or have attempted suicide.
• Medical misogyny: Nearly half of women report stigma from health professionals, and almost 40 per cent feel stigmatised by their GPs.
• LGBTQIA+ challenges: Respondents in this group are more likely to experience higher-than-average mental health issues, with pain affecting their sleep, ability to work, sexual intimacy, and independence.
• Slow diagnosis: 45 per cent of respondents said it took longer than three years to get a diagnosis. Women and non-binary respondents face even longer delays, with nearly half of women and almost 60 per cent of nonbinary respondents waiting more than three years.
• Potential for multidisciplinary care: Multidisciplinary (MDT) care, which treats chronic pain holistically in one location, in the heart of the community, has the potential to revolutionise treatment and improve the lives of those affected. Sadly, only 1 in 100 Australians can access MDT care.
The 2024 National Pain report is available on the Chronic Pain Australia website.
The Faculty of Pain Medicine has released a new position statement on persistent pelvic pain and endometriosis and has developed a series of answers to some commonly asked questions.
PS15(PM) Statement on pelvic pain and endometriosis is being piloted for six months until January 2025. We encourage feedback via fpm@anzca.edu.au which will be considered at the end of the six-month review period
Visit our website for some answers to questions we have already received in relation to PS15 and its background paper.
NEW FELLOWS
We congratulate the following doctors on their admission to FPM fellowship through completion of the training program:
• Dr David Boothman-Burrell, FRNZCGP, MRCPI, FFPMANZCA (New Zealand)
• Dr Nitin Chaudhary, FRACGP, FFPMANZCA (QLD)
• Dr Kin Ho Aaron Lee, FHKCA (Anaesthesiology), FFPMANZCA (Hong Kong)
• Dr Heshini De Silva, FAFRM (RACP), FFPMANZCA (QLD)
• Dr Slava Poel, FANZCA, FFPMANZCA (VIC)
• Dr Parul Sareen, DNB Anaesthesia, FFPMANZCA (Qld)
• Dr Behnood Shahi, FRACGP FFPMANZCA (Qld)
• Dr Michael Zhao, FRACGP, FFPMANZCA (NSW)
We also congratulate Dr Leigh James Edward Spurling, FRCA, FFPMANZCA (VIC) on his admission to FPM fellowship via the PM Specialist International Medical Graduate (SIMG) pathway.
18-20 October 2024, Pullman Auckland, New Zealand
FPM celebrates 50 years of international pain congress
More than 30 FFPMANZCAs and FANZCAs from Australia, New Zealand, Singapore and Hong-Kong recently travelled to Amsterdam to commemorate 50 years of working together for pain relief at the International Association for the Study of Pain (IASP) 2024 World Congress on Pain.
FPM Board member and conference participant Dr Irina Hollington nominated her highlights of the August meeting:
• Speakers Dr Jane Ballantyne and Dr Allan Basbaum started the opening plenary with “It all began 50 years ago in Issaquah”, explaining how a group of physiologists, physicians, psychologists and philosophers met to nut out the basics of pain medicine on Dr John Bonica’s hobby farm in Washington State. Dr Ballantyne acknowledged the far-reaching influence of Dr Bonica’s inclusive mentorship which included our own giant of Australasian pain medicine, Professor Michael Cousins, who died earlier this year.
• Malaysian FFPMANZCA Dr Mary Cardosa received an honorary IASP membership for her outstanding contributions to advocacy. She emphasised the role of local partners, resources and assessment and follow-up and mentorship when starting chronic pain treatment in low-income countries.
• The latest version of the International Classification of Diseases (ICD-11) for chronic pain may become a game changer in coding pain diagnosis and treatment. Honorary IASP member Professor Detlef Treede displayed ICD-11 data from Germany highlighting how better coding data allowed for a change in funding model.
• Neural pre cursor cell (NPC) transplantation for spinal cord injury (SCI) is coming.
• Professor Masaya Nakasuya from Keino University showcased an exciting future cure for SCI. His group is now completing phase one studies in humans after replicating results from animal studies. They are transplanting pre cursor stem cells to spinal cord injury lesions where the cells penetrate the SCI scar lesions. Full results are due to be presented in 2025.
Finally, my pelvic pain buddy Karin Jones (Vic) and I met the fabulous Jilly Bond. To many pelvic pain practitioners Jill, a pelvic floor physiotherapist, is a well- known hero through her YouTube clips and online courses. Her practical research is now focussing on exploring graded motor imagery (GMI) for the pelvic floor.
The questions around best application of pre-clinical knowledge into the pain clinic remain unchanged. It is important to recognise that at that first meeting in Issaquah the pain medicine ground breakers weren’t to know how far their ideas, opinions and philosophies would contribute to the chronic pain care we provide today.
Dr Irina Hollington, FANZCA, FFPMANZCA FPM Board Member
ABOVE
Dr Irina Hollington and Dr Jonathan Newchurch (FPM trainee) at the Amsterdam meeting.
Procedures Endorsement Program
We’ve streamlined the application process for the Practice Assessment Pathway to alleviate the burden of paperwork. FPM fellows whose scope of practice includes pain procedures are encouraged to apply.
See anzca.edu.au for more information.
Scan the QR code or visit anzca.edu.au/news/beyond-city-limits-ebook
Training & education
We're responsible for training, assessing and the continuing education of anaesthetists and specialist pain medicine physicians in Australia and New Zealand.
Competency based medical education in the ANZCA training program
The Training Program Evolution project group was established in 2017 and comprises four streams of work: ANZCA educator skills, accreditation of the learning environment, trainee selection and competency based medical education (CBME). This article focusses on CBME, describing changes in introductory training (IT) and the theoretical and practical underpinnings of workplace-based assessment (WBA).
CHANGES PLANNED IN CBME IN 2025-26
The introduction of CBME will begin in 2025 with introductory training. Changes will continue to be rolled out in 2026 and beyond as implementation challenges are addressed and technology solutions are in place to adequately support CBME processes. Table 1 provides a summary of the changes, and the expected timelines.
Table 1. Intended changes in introductory training
Online multi-consultant feedback to support SOT decision-making Trainee e-portfolio for IT CUR
Group Decision Making at IT CUR
In 2025, an online multiple-choice question (MCQ) and an oral assessment with the supervisor of training (SOT) on specified emergency scenarios (SES) will replace the initial assessment of anaesthetic competence questions (IAACQ). SESs are mapped to six topics critical for patient safety. Each SES will be supported by a question and answer guide and a template for feedback. The online MCQ is an exciting new development – trainees will have unlimited access to a practice MCQ assessment where they receive a random selection of questions taken from the same bank as the MCQ assessment and get automatic feedback on any incorrect answers. When the trainee feels ready, they can complete the MCQ assessment. When a score of 80 per cent or higher is recorded the MCQ assessment is marked as complete in the Trainee Portfolio System (TPS). The assessment will drive trainees to learn the material, but with less stress and built-in feedback.
WBAs will change format in 2026. The main directions here are to simplify the form and its administration, ensure timely feedback, remove numbers from the ratings, provide a brief online module for supervisor training, and provide more specificity around the WBAs. At the IT core unit review
(CUR), the WBAs will demonstrate that the trainee can be entrusted with the care of ASA 1-2 patients for minor or moderate complexity surgery with distant supervision, that is, they are ready to progress to basic training (BT). Prompts for good questions for the feedback conversation will be incorporated into the WBA form. Extensive consultation on the minimum requirements for IT led to a modest increase in WBAs, hopefully offset by less time to complete. It is anticipated the new WBA form format will be used throughout the training program from 2026, but at this stage WBA types and numbers will remain unchanged beyond IT.
Group decision making (GDM), where the responsibility for the high-stakes decision on trainee progression at the CUR rests with more than one person is under consideration with a view to implement beyond 2026.
The main driver for CBME is to refocus progression decisions on observed competency in practice rather than assume that competency is achieved through time in practice. The following section explains some of the lessons learned about WBAs since their introduction to the curriculum in 2013 and how these have informed their evolution to the new format in 2025.
Specified WBAs and improved WBA forms
WBAS IN PRACTICE
WBAs are critically dependent on the willingness and engagement of workplace supervisors to provide feedback and their honest judgement on trainee ability. Incorporating WBAs into ANZCA training has been generally positive.1 Trainees have noted that WBAs can help with more structured feedback. But there’s room for improvement, including, clarifying the purpose of WBAs, maximising their value for learning and decisions on progression, and cutting down the admin.2
Trainees also observe that some supervisors are better at providing helpful feedback than others. Written WBA feedback in the TPS is often of limited quality and doesn’t guide the trainee on how to improve – only to ‘do more’ or ‘read more’. Trainees suggest some supervisors don’t use the entrustment scale as intended but use it as a traditional measure of 1=bad, 9=good. We note cases in the TPS where supervisors score BT as 9, that is, able to manage a complex neurosurgical case with distant supervision – surely this isn’t the case!
We also found that not all SOTs use WBAs to guide their progression decision at the CUR. Reasons given include difficulty accessing information, limited faith in WBA authenticity due to trainee ‘gaming’. Instead they use alternative ‘shadow’ systems of assessment.3 This leads to variability, and a lack of transparency for trainees.4 Feedback from trainees supports transparency of departmental assessment processes, making WBAs ‘count’, improving supervisor feedback and decreasing administration.5 These improvements are embedded in the new IT CUR and a planned TPS upgrade.
THE DUAL PURPOSE OF WBAS
Workplace assessments have a dual purpose. Late career anaesthetists grew up in a binary system of formative versus summative assessments, also referred to as low stakes versus
high stakes, that is, an assessment was for learning only, or it was for decision making only. Educational practice has moved on. In a workplace-based assessment, the supervisor is asked to do two things – firstly to support the trainee to learn from the case, and secondly to provide their judgement on the trainee’s need for supervision with a case like this. This dual purpose has been described as ‘assessment for learning and assessment of learning’ or a ‘continuum of stakes’ from low to high stakes.8 A single WBA is an opportunity for learning and is low stakes. Low stakes means that it is not a big deal for the trainee if they ‘fail’ it, because it is only one of many WBAs and importantly, they can learn from the WBA and repeat it. These supervisor judgements on individual WBAs contribute to a bigger picture of a trainee’s progress towards unsupervised practice. And at the core unit review, all the WBAs for that core unit together can provide information supporting progression to the next core unit, or suggesting the trainee is not yet ready to take on the work at the next phase of training. So, the whole collection of WBAs over a core unit becomes ‘high stakes’ in that it will affect progress of the trainee at the core unit review. Of interest, analysis of the many thousands of WBAs in the TPS showed that reliability is about the same as the final exams – both are good.6 A portfolio of 15 WBAs has a level of reliability acceptable for a high stakes decision such as progression at the CUR.7
ENTRUSTMENT
WBA reliability is partly due to the ‘entrustment’ scale. The original thinking around entrustment was that supervisors make daily decisions on how much they trust a trainee with a case every day, for example, going to the bathroom, leaving the operating department or not being in the hospital.9 These supervisor expert judgements on trainee supervision needs are based on their responsibility for the patient. This entrustment is many times more reliable than traditional scales of below average, average or above average. Furthermore, the entrustment scale can identify struggling
trainees, potentially addressing the failure to fail problem of traditional scales. The entrustment scale is used by ANZCA in WBAs for the anaesthesia training program.10
WHERE TO NEXT?
The anaesthesia training program is fundamental for ANZCA, recognised in the college’s commitment to continuous improvement. Through CBME we acknowledge that knowing and doing are not the same, and we want both for our graduates.
Our formal examinations ensure our trainees have the knowledge required to be an anaesthetist. CBME ensures that they can do the work required of them by the communities they serve.
Professor Jennifer Weller, FANZCA
Director of Professional Affairs Education, ANZCA
Head of Centre for Medical and Health Sciences Education, University of Auckland
Acknowledgements
The research on the ANZCA curriculum was funded by the ANZCA Research Foundation.
References
1. Weller JM, Jolly B, Misur MP, et al. Mini-clinical evaluation exercise in anaesthesia training. Br J Anaesth 2009;102(5):633-41.
2. Castanelli D, Jowsey T, Chen Y, et al. Perceptions of purpose, value, and process of the mini-Clinical Evaluation Exercise in anesthesia training. Can J Anaes 2016;63(12):1345–56.
3. Castanelli DJ, Weller JM, Molloy E, et al. Shadow systems in assessment: how supervisors make progress decisions in practice. Adv in Health Sci Educ 2020;25:131-47.
4. Weller JM, Coomber T, Chen Y, et al. Desire paths for workplace assessment in postgraduate anaesthesia training: analysing informal processes to inform assessment redesign. British Journal of Anaesthesia 2022;128(6):997-1005.
5. Weller J, Castanelli D, Chen Y. Desire paths in workplacebased assessment to improve feedback and decisions on progression in postgraduate anaesthesia training. . AMEE CBME Summit Basel Switzerland, 2024.
6. Weller J, Castanelli D, Chen Y, et al. Making robust assessments of specialist trainees’ workplace performance. Br J Anaes 2017;118(2):207-14.
7. Castanelli DJ, Moonen-van Loon JMW, Jolly B, et al. The reliability of a portfolio of workplace-based assessments in anesthesia training. Can J Anaesth 2019;66(2):193-200.
8. Schuwirth LW, Van der Vleuten CP. Programmatic assessment: From assessment of learning to assessment for learning. Med Teach 2011;33(6):478-85.
9. Crossley J, Johnson G, Booth J, et al. Good questions, good answers: construct alignment improves the performance of workplace-based assessment scales. Medical Education 2011;45(6):560-69.
10. Weller J, Misur M, Nicolson S, et al. Can I leave the theatre? A key to more reliable workplace-based assessment. Br J Anaesth 2014;112(6 ):1083-91
College bursaries
Did you know each year ANZCA offers a number of bursaries to trainees who are experiencing financial hardship?
Eligible trainees can receive up to a 50 per cent reduction in their annual training fees. All applicants will also receive an extension to the annual training fee due date.
Applications for 2025 will open in mid-November.
Applicants must be registered as a trainee with ANZCA or FPM.
Applications close on 31 January 2025.
For further information, please contact the ANZCA Training and Assessments team via email at training@anzca.edu.au or call +61 3 9510 6299.
Global development
We're committed to improving education and training capacity in anaesthesia and pain medicine in response to the needs of low- and middle-income countries.
PNG anaesthetist wraps up scholarship visit to South Australia
Port Moresby anaesthetist Dr Melany Werror has spent the past three months in Adelaide as the recipient of the ANZCA Global Development Committee’s new Pacific pain scholarship.
Through placements at the Royal Adelaide Hospital, Queen Elizabeth Hospital and the Women’s and Children’s Hospital she has seen at first-hand palliative care and acute and chronic pain management teams in action.
Originally from Madang on the north-coast of Papua New Guinea, Dr Werror works in the anaesthesia department at Port Moresby General Hospital.
Speaking to the ANZCA Bulletin in Adelaide as she neared the end of her visit, Dr Werror says being able to observe multi-disciplinary pain management and palliative care management teams has been a highlight of her time on hospital wards and clinics.
“I had never seen palliative care teams in action, including home-based services, until my visit,” she explains.
“In PNG we have palliative care management for cancer patients and it is on a much smaller scale. Here in Adelaide I could see how opioids are managed for pain relief and also how advanced care directives give patients autonomy over the care they want to receive.”
Dr Werror began her anaesthesia training in 2009 when she started her diploma of anaesthesia. Her first introduction to the specialty was as a resident in Madang where she joined the anaesthesia team headed by Dr Gertrude Marun, one of PNG’s first female anaesthetists.
“Gertrude had an enthusiastic anaesthesia team and she became a mentor to me. I had the option of either doing emergency medicine or obstetrics but after working with Gertude I was inspired to continue with anaesthesia training so I then started my Masters in Anaesthesiology in 2016.”
With her husband, an orthopaedic surgeon, and family, Dr Werror has moved between Madang, Lae and Port Moresby for much of her medical career. The number of anaesthetists in PNG is slowly increasing. Dr Werror is now one of about 30 anaesthetists in the country and they are supported by a team of anaesthetic scientific officers (ASOs), many of whom work in remote provincial hospitals.
“I appreciated being able to see the chronic pain teams manage their patients. For those patients who could not tolerate opioids they were instead given nerve blocks and I was able to go on home visits with the palliative care teams so they could see how their patients were coping, how they were managing their medication and whether their guardians or carers needed more help.’’
Dr Werror also spent three weeks at the Adelaide Women’s and Children’s Hospital with the “comfy kids” team who care for children with acute pain.
“I saw the important role played by the team’s nurses and the quality of care provided to the children by consultants. It really made me aware of the benefits of having a process in place to treat pain well and having a plan for each patient using pain guidelines for children.”
Dr Werror says she is now inspired to return to PNG armed with knowledge that she hopes could be used to establish an acute pain service at Port Moresby General Hospital.
“Learning about opioid stewardship, good control and regulation and how to use particular drugs has been very useful. It was the first time I had seen multi-disciplinary teams of physicians, paediatricians, psychologists and physiotherapists and I learnt how difficult it is to treat children with chronic pain.
“It has given me a lot of ideas and insights into what we could do back home. I’ve seen the benefit of the importance of the team approach to pain management to improve patient outcomes.
“It will take time but with the right advocacy, training and administrative support I’m hoping we could start making some small changes.”
*Dr Werror would like to thank ANZCA and FPM for supporting her visit, consultants and other staff in South Australia and the PNG Society of Anaesthetists and Intensivists and Port Moresby General Hospital for allowing her the time to undertake the observership.
Carolyn Jones Media Manager, ANZCA
ABOVE
Dr Melany Werror.
Supporting medical students, trainees and consultants in Madang
In June FANZCAs Dr Mark Trembath and Dr Stuart Andrews travelled to Madang in Papua New Guinea to take part in medical student teaching at Divine Word University (DWU) at the invitation of the medical school dean Dr Harry Aigeeleng. They also provided professional skills development training to trainees and consultants at Madang Hospital. Dr Trembath writes about his experience here.
DWU runs a five-year MBBS program which is still establishing itself in the PNG medical landscape. There were 29 students in the class, all from the northern side of PNG and the northern islands and representing a very different cohort from their colleagues at the University of PNG in Port Moresby.
A three-day teaching program comprised lectures, practical sessions and workshops. Feedback from students was very positive noting they enjoyed the interactive case discussions and describing the practical sessions as “the most fun they have had” in their course. There was a significant improvement in the post-course quiz (mean improvement of 26 per cent), highlighting that they had understood and retained core concepts from the week.
We delivered a clinical teaching session in the Madang Hospital operating theatre. This was attended by six local trainees, one rotating registrar, one resident, and one resident healthcare extension officer. Topics were undertaken at the request of Dr Aigeeleng and focused on practical application of theoretical knowledge in radiology, regional anaesthesia and ultrasound. There was no appropriate ultrasound machine available for teaching in Madang, but we were fortunate enough to borrow a Sonosite iViz unit from Port Moresby. This provided acceptable image quality, however, the machine overheated and needed to rest every 15 minutes!
The sessions were well received but were physically challenging as there was no power for most of our attempted sessions (the hospital’s generators did not have any backup fuel, so the entire hospital was devoid of power for almost the entire day). Participants found the radiology sessions challenging and were enthralled with the ultrasound training sessions, especially given they perform all blocks via landmark technique.
DWU’s MBBS program is looking to fill a vital role by meeting regional medical workforce needs. The challenges it faces are significant, operating in a resource poor setting and being understaffed. Despite these challenges, the exceptional and tireless work of local faculty have allowed the school to slowly grow over the past eight years.
Support from visiting FANZCAs contributes to the ongoing growth of the MBBS program providing potential generational benefit, providing students with additional high-quality education and giving local staff a well earnt break and morale boost. Similar arguments could be made regarding teaching at Madang Hospital where they are trying to attract and retain anaesthetic trainees and consultants, and where much of the departmental burden falls on only two consultants.
The Global Development Committee will continue to provide support to the DWU program and Madang Hospital anaesthetic services in response to requests from our PNG colleagues.
TRAINEE WINS MADANG SCHOLARSHIP
Dr Andrews travelled to Madang as a recipient of ANZCA’s Global Development Committee Trainee Scholarship and writes about his week there.
Developing a program for our time there was easy.
With input from Dr Aigeeleng and building upon Dr Trembath’s previous trip we were able to put together an appropriate ‘fit for purpose’ curriculum. Because we were able to organise this well in advance and with some knowledge of resources on the ground our goals were appropriate and attainable.
Once in Madang I found the week inspiring. The medical faculty are doing an exceptional job. They face the reputational issues that any new medical program does in a resource poor setting and are attempting to create a culture that is more open to teaching in surrounding hospitals.
Despite these challenges they remain optimistic and dedicated to their goal of providing PNG with top notch university graduates. The staff were always happy to help us in any way they could. Returning to Australia I will try and emulate their confidence, can do attitude and resilience.
The students are equally impressive. In addition to the challenge of studying medicine, they live away from home and 26 of the 29 students don’t speak English as their first language. I was happy that our pre- and post-course quizzes confirmed that while teaching had been a real pleasure they had also gained new knowledge.
There is room for improvement in teaching of medical officers at the hospitals. The power went out at 11am and the generators ran out of fuel. Despite our efforts, due to the heat (and the ultrasound overheating) we had to terminate the teaching in the early afternoon due to the austere conditions. What we were able to get through was very well received. One solution is to do the teaching at DWU – which the medical faculty would be happy to aid.
There is real potential for positive change in Madang and the Global Development Committee can become a significant catalyst for this. Madang and provincial PNG in general struggle to fill medical positions. The DWU medical school hopes to follow Australia’s experience with the success of regional universities encouraging graduates to remain local.
However, DWU struggles to attract medical specialists to educate their students, their medical staff work long hours and the medical school is still building its credibility in the country’s health sector.
Ongoing visits will help. The flow-on effect of a wellresourced and respected medical school in northern PNG could result in doctors who are more willing to fill roles outside of Port Moresby and who are also happier to return the teaching they received at medical school.
The aim should be to have medical students turned doctors become teachers of new medical students − a situation where the committee would no longer be needed in its current capacity in Madang.
Until then DWU and Madang Hospital will benefit from dedicated visits from representatives from the committee and in turn we can be confident that our efforts will lead to tangible benefits for the people of PNG.
Dr Mark Trembath, FANZCA Queensland Children’s Hospital
Dr Stuart Andrews, FANZCA Cairns Base Hospital
To support the work of the Global Development Committee through the ANZCA Foundation, please scan the QR code, or search ‘ANZCA GiftOptions’ to find the donation portal.
ABOVE
From left: Dr Gertrude Marun, Dr Mark Trembath, Dr Harry Aigeeleng, Dr Stuart Andrews. Dr Stuart Andrews discusses a case with anaesthetic registrar Dr Vanessa Soctine and Resident Health Extension Officer Mr John Oguro.
Supporting workforce training in PNG
BASIC LIFE SUPPORT TRAINING
The School of Medicine and Health Sciences (SMHS) at the University of Papua New Guinea was privileged to host its first-ever basic life support (BLS) training for the year in June.
The event was organised by Dr Pauline Wake and Dr Michelle Masta of the Department of Anaesthesia and Intensive Care at SMHS in collaboration with ANZCA. We were fortunate to have two members of the college’s Global Development Committee, Dr Yasmin Endlich and Dr Jessica Lim, in attendance who provided mentorship, training, and support during the three-day program.
The training was held in the nursing complex building at the university and was attended by hospital-based healthcare providers including doctors, health extension officers, anaesthetic technicians, nurses and community health workers.
To achieve the aims of Vision 2050 in ensuring institutional development and improving service delivery and health care for PNG, the Port Moresby General Hospital (PMGH) and the SMHS are fully committed to training and accreditation of all health care providers and non-medical personnel in BLS.
The three-day program began with a training of instructors session facilitated by Dr Lim and Dr Endlich. There were 13 participants in the instructor’s program from various disciplines and academic departments including rural medicine, obstetrics and gynaecology, dental, anaesthesia and intensive care and surgery.
The next two days of the workshop involved training a select number of hospital and university staff. These training sessions were organised and conducted by the newly trained instructors who were certified as trainers at the end of the program. Over these two days a total of 53 participants graduated with a certificate in BLS after successful completion of the course.
None of the wards in PMGH have a defibrillator and many participants were new to its use. A strong recommendation has been made to PMGH management for all wards to have a defibrillator to improve outcomes. It was also recommended to PMGH that they take ownership of the BLS training program and provide yearly refreshers and certification for all staff members.
Thanks to Dr Jessica Lim, Dr Yasmin Endlich (ANZCA), Dr Pauline Wake and Dr Michelle Masta- (Anaesthetic and ICU department PMGH and SMHS), Dr Carl Kingston and the emergency department (PMGH), SMHS and nursing division for the use of the lecture halls and tutorial rooms , PMGH for allowing staff to participate in the workshop and providing catering and all instructors and participants who took time off from their clinical and academic responsibilities to attend this training.
Dr Marilyn Morris
School of Medicine and Health Sciences, University of Papua New Guinea
ABOVE
Participants of the first basic life support training course held at the University of Papua New Guinea in June.
Follow us on social media
Wherever you go to for information, events, news, and networking, we’ve got you covered! Follow us…
@ANZCA | @ANZCA_FPM | @GKMuseum
@the_anzca | @gkmuseum
@ANZCA1992
Australian and New Zealand College of Anaesthetists
Australian and New Zealand College of Anaesthetists
Faculty of Pain Medicine
Australasian Anaesthesia submissions
We’re seeking expressions of interest for contributions to the next edition of Australasian Anaesthesia (the Blue Book).
Before starting your article, we ask you to submit a form to the editorial team for review. This is intended to avoid unintentional duplication of submissions, and ensure the topic and format proposed are appropriate for the scope of the Blue Book.
This form must be completed, with the topic approved and an editor assigned, prior to an article being submitted for review. Please send the completed form to bluebook@anzca.edu.au
Visit anzca.edu.au for more information and the form.
Call for better recognition of pain services in New Zealand
“What I’m looking at is how we optimise outcomes for patients across the whole perioperative process"
The ANZCA Invited Speaker at this year’s Aotearoa NZ Anaesthesia Annual Scientific Meeting (ASM) is calling for greater support for pain services in New Zealand – and citing the example set by an anaesthesia and pain medicine legend as a possible way forward.
Associate Professor Michal Kluger will speak at the ASM, held from 7-9 November in Auckland, on the concept of a transition pain model of care, the background and context of the service within the ANZCA framework, as well as potential challenges for anaesthesia as a medical specialty.
A/Prof Kluger says boosting the profile and funding of chronic pain services in New Zealand is vital.
“In the bigger picture, chronic pain in New Zealand is funded terribly, it’s got no profile, it’s not sexy and it doesn’t win votes, it never appears on the election manifesto, it never appears when the Minister of Health is talking about outcomes, and as a construct it’s not going to take priority.
“You ask jurisdictions around the world, it’s an international problem. I think New Zealand is such a small country…if we got one or two high-profile centres in New Zealand that were really nationally known leaders in pain management that were given media coverage and profile, that’s the way to do it.
“It happened in Australia with Professor Michael Cousins – he was an absolute legend in Australia, and he went from Sydney to Adelaide, and created a research centre that no one had seen anywhere in the world. Professor Cousins’ team undertook basic science laboratory work, world-leading clinical research and led the world in pain management from an innovative, yet comparatively small hospital – Flinders Medical Centre in Adelaide.
“Looking at New Zealand, that’s what we need, we need a couple of flagship areas to be developed to create centres
of excellence, whether that’s through private funding, a benefactor that’s had a relative that’s been involved with chronic pain, or academic and public hospital joint ventures –that’s the sort of thing that might be useful.”
Professor Cousins, regarded as a doyen of Australian anaesthesia and pain medicine and the internationally bestknown ANZCA fellow, died earlier this year. He founded the Faculty of Pain Medicine within ANZCA and became its first dean.
A/Prof Kluger, who is currently involved in setting up a transition pain model of care at Waitematā Health New Zealand, says transition pain care is an integral part of perioperative medicine.
“What I’m looking at is how we optimise outcomes for patients across the whole perioperative process, of which anaesthesiologists are central, and we’re certainly a group that’s got a huge interest and expertise in this area.”
Rather than create new silos within a currently stretched health system, A/Prof Kluger’s hope is that the transition pain model of care is integrated within existing perioperative pathways, extending the role of anaesthetists.
He says this may be a future challenge for the specialty of anaesthesia and ANZCA, where training, education and placement focus to a greater extent on out-of-operating-room locations, rather than the traditional base within the confines of a theatre.
A/Prof Kluger says while the transition pain model originated in Canada as a response to issues with opioid use in North America, the situation is different in New Zealand.
He says problematic opioid prescribing, along with inappropriate pharmacological management of postoperative pain are ongoing issues in New Zealand, but persistent post-surgical pain and delayed functionality were also key outcomes that needed to be addressed.
“My push here is that we look at that but with the emphasis really on optimising functional outcome from surgery, and anaesthesia is a part of that.
“The role of a transition pain model of care within the current perioperative process, and combining this with other innovative models of care such as advanced recovery room care from Professor Guy Ludbrook’s research in Adelaide, will hopefully lead to important patient-centred healthcare utilisation and fiscal improvements.
“That’s why I got into looking at transition pain models of care and research, discussing with innovators such as Toronto General Hospital, going to various centres around the world such as Johns Hopkins Medicine and Duke Medical Center, and looking at how we can bring this back to New Zealand to make it cost-efficient, cost-effective, and realistic in the current financial climate.”
Reon Suddaby
Senior
Communications Advisor New Zealand, ANZCA
WORKING TOGETHER AOTEAROA NZ ANAESTHESIA ASM 2024
Prof Ki Jinn Chin Department of Anesthesiology and Pain Medicine University of Toronto Canada
Prof Bobbie Jean Sweitzer Systems Director, Preoperative Practices Inova Health Virginia, USA
A/Prof Joyce Yeung Associate Clinical Professor in Anaesthesia and Critical Care. University of Warwick, UK
AUCKLAND TĀMAKI MAKAURAU
Associate Professor Michal Kluger.
Foundation update
FOUNDATION ESTABLISHES THE W. JOHN RUSSELL ANZCA RESEARCH AWARD
Thanks to the generosity of Mrs Jan Russell, the foundation has received the unanimous approval of the ANZCA Research Committee for the new W. John Russell ANZCA Research Award.
The new award will run for at least two years and be awarded at the committee’s discretion to encourage highquality studies in anaesthetic engineering or equipment, patient safety or teaching.
The ANZCA Foundation named research award will honour the outstanding career and contributions to the practice and teaching of anaesthetics by ANZCA Robert Orton medallist, Adelaide’s Dr W. John Russell, in the above areas of clinical and academic anaesthesia.
GLOBAL AND INDIGENOUS HEALTH
Anaesthesia registrar teaching delivered in Samoa Foundation donors continue to support ANZCA fellow volunteers’ vital training and education visits to improve access to anaesthetic care and pain medicine in lower income countries where there are fewer specialists and facilities.
In June, Dr Megan Walmsley from Royal Darwin Hospital was funded by an ANZCA Foundation Health Equity Program grant to conduct an anaesthesia registrar teaching visit to Tupua Tamasese Meaole Hospital, the tertiary referral centre for Samoa, in Apia.
Samoa has a population of 200,000 and four qualified anaesthetists for operating theatre and intensive care unit services, compared to the recommended five anaesthetists per 100,000 people.
The primary purpose of Dr Walmsley’s visit was to provide clinical supervision for Dr Esjae Sesega, one of two anaesthesia registrars in the department (staff levels in Samoa mean level one supervision is rare), and tutorials on chosen topics. The secondary objective was to support the two recently graduated Samoan consultants responsible for the department and supervising a masters trainee.
The visit covered in-theatre supervision during spinal surgery, septics, orthopaedics and general surgery lists, registrar and medical student teaching on a wide range of clinical topics nominated by the local team, team discussions, and support for Dr Sesega’s research planning and study strategies.
In his feedback, Dr Sesega said “Thank you for all your help the past two weeks, for the teachings, my research proposal planning and for helping me with study strategies. I feel a lot more relieved, less stressed and somewhat excited about working on the research”.
MELBOURNE WINTER ANAESTHETIC MEETING RESEARCH AWARDS
At the 2024 Melbourne Winter Anaesthetic Meeting on 27 July, Dr Ned Douglas received the ANZCA Melbourne Anaesthesia Emerging Researcher Award from foundation governor patron Dr Peter Lowe, for the study “A pilot trial of midodrine, atomoxetine or placebo to prevent ward hypotension after major non-cardiac surgery”.
Dr Lowe also presented the ANZCA Melbourne Emerging Researcher Scholarship’, to Dr Luke Fletcher for his PhD based on the study “Haemodynamics and assessment in realtime of left atrial pressure (PHARLAP)”.
Dr Lowe provides $A15,000 for the award and $A25,000 for the scholarship every year to support new emerging academic anaesthetist researchers.
FELLOW RECEIVES NATIONAL AMA AWARD
Brisbane anaesthetist, researcher, and teacher Professor Andre Van Zundert, FANZCA, received the Australian Medical Association’s Excellence in Healthcare Award for 2024 at the annual meeting of the Australian Medical Association in August.
Presenting the award, AMA president Dr Steve Robson said, “Professor Van Zundert’s efforts in healthcare are exemplary, and they are matched equally by his efforts in many other fields.”
The foundation congratulates Professor Van Zundert, a longstanding member of the ANZCA Research Committee.
BLOOD PRESSURE MEASUREMENT IN OBESE PATIENTS
Eighteen final reports were received in 2023 for ANZCA Foundation-funded studies, which have generated a wide range of publications in leading peer-reviewed medical journals, and many presentations at international scientific meetings.
The Academic Enhancement Grant report from Professor Victoria Eley (Royal Brisbane and Women’s Hospital) was a highlight, outlining a program of work including five studies related to perioperative blood pressure measurement in obese patients.
A sub-study was included to measure renin and aldosterone levels in the blood and mineralocorticoid receptor (MR) expression in the adipose tissue, and compare concentration of inflammatory markers in the blood and adipose tissue of patients with a body mass index (BMI) of more than r 35 kg/ m2.
Professor Eley’s team aimed to deliver outcomes to help improve care of obese patients, for whom inaccurate blood pressure measurements are known to compromise quality. The team identified that available finger cuff technology did not fit the target population and was not sufficiently accurate to replace invasive arterial monitoring.
After realising anaesthetists are frequently unaware of postdischarge complications of arterial lines the team developed a health services evaluation project “Perioperative arterial catheterisation: a prospective evaluation of ultrasound, infection and patient-focused outcomes”, and a local flow-chart for patients with symptoms following arterial catheterisation.
The RBWH team of ten, including seven FANZCAs and one provisional fellow, have been shortlisted for the ‘Metro North Research Excellence Awards’ for their work “optimising the perioperative care of patients with obesity.”
CONTACT AND SUPPORT
To donate, please use the 2024 subscriptions form, search ‘GiftOptions –ANZCA’ in your browser, or scan the QR code.
For queries, contact:
Rob Packer, General Manager – ANZCA Foundation, +61 (0)409 481 295, or at rpacker@anzca.edu.au
Research grants program:
Susan Collins, Research and Administration Co-ordinator, scollins@anzca.edu.au
From top: Dr Walmsley working with Dr Esjae Sesega in OT at TTMH.
Bottom: Samoan medical students learning spinal anaesthesia (photo taken with consent).
ANZCA CTN Workshop
The ANZCA Clinical Trials Network (CTN) workshop recently held in Sydney was a tremendous success, drawing more than 180 delegates. The event set the stage for fruitful exchanges on advancing clinical trials.
Fostering innovation and collaboration
Ahead of the workshop, the Anaesthesia Research Coordinators Network (ARCN) came together for their annual networking event. New research coordinators had the opportunity to learn about the CTN and meet their regional mentor.
The formal program opened with a moderated poster session featuring five investigators, including three trainees, who presented their novel research. This intimate setting was designed to ignite collaboration among new and emerging investigators ahead of the weekend’s activities.
Morning workshop sessions included the presentation of several new research proposals. Dr Liz Ryan from Monash University delivered keynotes on Bayesian statistics and adaptive platform trials, highlighting the CTN’s focus on improving trial efficiency and resourcing. Dr Marlena Klaic from the University of Melbourne emphasised the importance of planning for successful implementation of results.
The first day continued with interactive workshops on safety endpoint reporting led by Dr Tanya Symons and consumer engagement in both adult and paediatric research by CTN teams. The day concluded with trial updates and a panel discussion on overcoming trial complexities to ensure feasibility and timely completion within an increasingly challenging clinical trials landscape.
Strategic focus and regional engagement
The second day featured the ARCN and CTN business meeting, which outlined the strategic directions and ongoing work of the network. Mr Rob Packer and Professor Britta Regli-von Ungern-Sternberg discussed the vital role of the ANZCA Foundation in supporting research by fellows and trainees, including available grant opportunities.
A session on rural and regional engagement followed with Grampians Health showcasing their impressive departmental growth over the past decade and their impact
on making trials more accessible and equitable for rural and regional communities. Presentations from the NSW Rural, Regional and Remote Clinical Trials Enabling Program and the Australian Teletrial Program introduced new opportunities to enhance trial accessibility in these areas. Dr Ruth Griffiths from the Department of Health and Aged Care informed delegates about the latest Medical Research Future Fund (MRFF) grant opportunities, particularly for rural and regional-led research.
The day concluded with discussions on how research departments can recruit Māori, Pacific Islander, Aboriginal, and Torres Strait Islander people into trials. The theme was on building sustainable research departments and fostering collaborative opportunities with other research networks, including obstetrics, paediatrics, and pain medicine. The session featured a workshop on stakeholder engagement and overcoming challenges when getting buy-in for clinical trials. The day wrapped up with the DECIDE start-up meeting, marking the launch of the latest NHMRC-funded trial and a conference dinner at Coogee Surf Life Saving Club.
Practical insights and future directions
The final day featured a trial feasibility workshop which guided delegates through key considerations for ensuring trials are feasible at their respective sites. The sessions also covered adaptive platform trials and the development of an adaptive platform trial as a resource which CTN researchers can access. The day ended with talks on emerging technologies.
This year’s workshop was notable for the high turnout of first-time delegates, with significant contributions from trainees and research coordinators. The high level of engagement, combined with innovative sessions and strategic discussions, ensures that the pipeline of world-class clinical trials will continue to grow and thrive in our network.
ABOVE
From left: Ms Natasha Brice from Grampians Health, Vic. Dr Greg Henderson, Ms Natasha Brice, Dr Ruth Griffiths, Dr Jo Youd, Ms Anne O'Neill, Dr Suresh Singaravelu, Associate Professor Nicole Phillips, Professor Phillip Peyton. Professor Tomás Corcoran, Dr Marlena Klaic.
What’s new in the library
EXPANDED RESOURCE SUPPORT FOR THE ANZCA AND FPM CPD PROGRAM
The ANZCA Library, in conjunction with the ANZCA and FPM CPD Program, has launched a revised and expanded guide for ANZCA and FPM CPD Program Resources.
The expanded guide now covers all 56 activities in our CPD program and provides information, suggestions and resource support for the entire program. You’ll find numerous ideas and great inspiration on how to meet your CPD requirements in a way that supports your learning needs and scope of practice.
This expanded guide joins the recently launched CPD for Clinical Support Roles guide for fellows and other CPD participants working in clinical support roles and/or without direct patient care.
What you’ll find inside:
• Participation suggestions for each activity.
• Additional support resources including new guides and e-books.
• Links to recommended external resources, courses and sites.
• Shortcuts to all related ANZCA and FPM resources and documentation.
• Course suggestions.
So if you’re interested in learning more about critical reflection activities, completing a practice audit, claiming time spent reading articles via Read by QxMD or being a peer reviewer then the ANZCA and FPM CPD Program Resources guide is a great place to start.
ANZCA LIBRARY AT THE 2024 ASA NSC
As part of the launch of the updated ANZCA and FPM CPD Program Resources guide, ANZCA Library Manager John Prentice recently attended the 2024 ASA National Scientific Conference in Darwin.
Latest books
For the latest updates and a complete list of new titles check out the library news page: libguides.anzca.edu.au/news
The meeting provided an invaluable opportunity to promote the guide to new and existing fellows and CPD participants, as well showcase the many other library services and resources available to help support college fellows and trainees. This included hands-on demonstrations of LibKey Nomad and the BrowZine app, and taking the many trainees in attendance through the recently updated Primary Exam Recommended Reading list and Anaesthesia Training Resources guide.
As part of this trip, John was also able to complete library orientation sessions with anaesthesia staff and registrars at the Caboolture Hospital in NSW and Royal Darwin Hospital in the Northern Territory. The trip also offered an invaluable opportunity to meet with NT Health staff to discuss resourcing for the in-development cultural safety toolkit.
In November, John will be attending the Aotearoa NZ Anaesthesia ASM 2024 in Auckland where he can be found at the ANZCA booth.
HELP THE LIBRARY KEEP OUR GUIDES UP TO DATE – AND EARN CPD HOURS!
Did you know that the college library maintains over 100 resource guides to help support our training, CPD and research programs?
These guides are maintained by library staff who regularly add new and exciting content covering the anaesthesia, pain medicine, and perioperative medicine specialties.
We are assisted in this task with expert contributions from fellows, trainees, staff and external consultants. Our liaisons help ensure the content is kept relevant, accurate and current, and – just as importantly – are able to claim CPD hours for their contributions.
If you’ve got some “big ideas” you’d like to see realised in our guides, then contact the ANZCA Library for more information: library@anzca.edu.au.
Dr Philip Byth died peacefully at home surrounded by his family on 5 July following a 12-year battle with recurrent relapsing non-Hodgkin’s lymphoma.
Phil was the leader whose energy and tenacity built the foundations of the strong departments of intensive care, anaesthesia and pain management that exist today at the John Hunter Hospital. His leadership was defined by a strong moral compass and the ability to take on tough issues.
The benefit of his work stretches across communities not just in Newcastle and the Hunter region but extends from the central coast of NSW to the Queensland border and includes the trauma and retrieval services which he was instrumental in establishing.
Phil grew up in Graceville Brisbane and attended Brisbane Grammar. At school he excelled academically and in sport. He played in the first XV rugby team and was the Great Public Schools’ Association’s 800 and 1500 metre champion. Phil’s lifelong passion for tennis started on his home tennis court and he remained a very competitive player over recent years, despite his illness.
He graduated from the University of Queensland medical school in 1975 with first class honours and completed his junior medical officer years at The Alfred hospital in Melbourne. He returned to Brisbane and trained in anaesthesia and intensive care medicine at Royal Brisbane Hospital, completing his FFARACS. This lead to him taking a job as a senior registrar at St Vincent’s Hospital in Sydney to further his ICU training.
He moved to Newcastle in 1984 and took up a job as a staff specialist in anaesthesia and intensive care at the Royal Newcastle Hospital. Following the opening of the John Hunter Hospital in 1991, Phil was appointed as the inaugural
director of intensive care, and subsequently chair of the division of anaesthesia, intensive care and pain management. While managing the leadership roles, he remained a gifted and empathic clinician. During this period he was also very involved with the Australian and New Zealand Intensive Care Society as the honorary secretary, and then serving as president from 1991 to 1993.
A reorganisation of the clinical divisions at John Hunter Hospital moved anaesthesia and pain management into the division of surgical services. Phil took up the role of leading that combined service, which was very challenging. His success in directing surgeons owed much to his tenacity and willingness to confront difficult issues, and also to his ability to hold respectful conversations with colleagues that placed the patient at the centre.
Phil was also a great teacher and mentor. He firmly believed that the best way ahead for a non-capital city hospital was to train your own future specialists. He was instrumental in recruiting the late Professor Geoff Cutfield to Newcastle to revitalise the training program.
When he stepped down from his role as head of surgical services in 2010, Phil returned to being a clinical anaesthetist and took up the role as the ANZCA supervisor of training until he retired due to ill health in 2014. He enjoyed helping trainees and having a coffee bought by Phil was a common introduction to a future career in anaesthesia and intensive care.
A clear picture of Phil is not complete without his family. Phil was a family man who loved and was loved by Tracy his wife, and his five children − three from his first marriage − and six grandchildren.
He was a great support to Tracy as she progressed through her medical training, obtained her PhD and became a professor in genetics, ultimately to be awarded the Order of Australia. After his retirement he enjoyed running a wellorganised and loving home for his whole family.
If he wasn’t playing tennis Phil loved walking, his favourite places being Merewether Beach (often with a coffee) and the coast around Hawks Nest in NSW, especially Dark Point.
Phil faced his illness with great determination and despite its relapsing nature, maintained a positive outlook. It was a difficult 12-year journey but he was able to support his family and watch them grow as they supported him during his difficult times.
He will be remembered as a man who achieved the rare combination of being a competent and empathic clinician, leading a complex health service and maintaining a loving home life. He is missed, we were enriched by knowing him and poorer for his passing.
Dr Patrick T Farrell, FANZCA
NSW
Jenny Henry
1965 – 2024
Dr Jenny Henry died suddenly on 20 June following a catastrophic brain haemorrhage.
Jenny was an international anaesthetist who had made Northland, New Zealand her home for the past 20 years, and will be sorely missed by the medical and wider community of this beautiful and close-knit place.
Jenny spent much of her early childhood in Africa, then undertook her secondary and medical school education and anaesthesia training in the UK.
During her anaesthesia training, she developed a lifelong passion for the ocean and took up a consultant post in Plymouth, on the Devon/Cornwall border of the south coast of England.
She later relocated to New Zealand with her young family, having secured a specialist anaesthetist role in Whangārei. She rapidly integrated into work and life in the small coastal city, where she remained until her untimely death.
Jenny was a huge asset to the anaesthesia department and Whangārei Hospital community. She was hard-working, practical and pragmatic, and was highly regarded for her clinical judgement and well-timed declarations of commonsense.
She led the department from 2012 to 2015, and held many other roles, including leading roles in sustainability and union activities. Her experience and wisdom, together with her caring attitude and passion for high quality but lowwaste healthcare were valued by the whole perioperative team.
Jenny was a strong advocate for equity in healthcare. In recent years, she was a key contributor to the anaesthesia service at Kaitaia Hospital, a small rural hospital which serves some of the most isolated and deprived members of the community.
Outside work, Jenny’s passion for the environment led her to become involved with marine conservation both locally and further afield, taking her as far as Antarctica in her quest to help clean up the ocean and preserve precious marine flora and fauna.
Those wishing to remember Jenny should consider a contribution to Project Jonah – see www.projectjonah.org.nz for further details.
Jenny is survived by her two young adult children, Dougie and Pippa, of whom she was fiercely proud. She had suffered the loss of her long-term partner in 2023, and, at the time of her death, was planning to have a year in the UK to spend time with her sister and her son.
At the time of her death she was on the Gold Coast with her daughter, and in keeping with her wishes, she was able to donate organs to eight recipients, a last act of giving in a life filled with adventure, passion and caring.
She achieved so much in her 58 years on the planet and will be remembered and missed by so many.
Dr Jo Coates, FANZCA Whangārei Hospital, NZ
John “Fred” “Ted” Eugene Gilligan, AO OStJ
1936 – 2024
John to his brothers, Ted to his family and Fred to his medical colleagues.
Fred was born on 17 December 1936 in Adelaide and attended Rostrevor College. He was talented academically and loved learning anatomy from a St John’s first aid manual. He attended medical school at the University of Adelaide.
He started his medical career at the Royal Adelaide Hospital (RAH) in 1961 and undertook specialist training in anaesthesia, qualifying in 1967. In the 1970s he became the first director of the RAH intensive care unit – a position he held until 1991 when he became the first RAH director of retrieval and resuscitation. He held this position until his retirement in 2002.
While Dr Tom Allen is credited with the first road medical retrieval in South Australia in 1958, Fred became increasingly concerned that acutely unwell patients were suffering, not only in Adelaide’s private hospitals (that did not have ICUs at that stage) but also in the rural sector. Fred was a medical pioneer in medical retrieval in Australia.
With increasing demand the SA retrieval services grew to involve all modes of transport and extend beyond the major teaching hospitals in Adelaide and rural SA to become a worldwide service known as “RAH Mediflight”. Road ambulances, helicopters, fixed-wing aircraft, executive jets and commercial aircraft were incorporated into a complex system that saved many lives. Many rural GPs appreciated the critical care phone assistance and rapid in-person support on these most stressful days.
The service became a mobile intensive care unit with specialist intensive care doctors and intensive care nurses. They carried the required blood products and intensive care equipment necessary to resuscitate and transport critically ill and injured patients over both short and long distances. This included establishing contracts with the Australian government and mining companies for critical care support around Australia. Whoever thought an RAH ICU team would fly into Asia for a gunshot politician?
Fred collaborated with a range of people from many organisations including the Royal Flying Doctor Service, all the emergency services and the city and rural hospitals to achieve system change. One of Fred’s achievements was educating politicians on the need for financial investment in a very expensive industry. The first helipad at RAH was one of these fine achievements. It became affectionately known as Gilligan’s Island.
Fred wrote many articles on the activity of the SA retrieval services including a review of interstate retrievals with a neurosurgeon for emergency neurosurgery in Mildura (Vic), Broken Hill (NSW), Alice Springs and Darwin (NT). In the early years, none of these centres had intensive care facilities hence the need for such long-range retrievals back to the RAH ICU.
The longest executive jet retrieval was from the Seychelles to Sydney while Qantas 747s supported the service worldwide in very complicated and expensive long-haul repatriations. The planning was 24/7 and Fred was known to answer calls at any time.
All those who worked with Fred would recall his signature opening words “Do you have a minute?”. It was not uncommon for Fred to hear a helicopter fly over his house at 4am resulting in a call to the ICU to find out what was going on and whether assistance was required.
Fred was also instrumental in establishing the hyperbaric service at the RAH. Before 1985 the treatment of divers with decompressive and gas embolic illnesses was severely lacking in SA.
Frequent presentation of severely ill abalone divers, plus the occasional iatrogenic cerebral gas embolic incidents were, on occasion, treated at a private multi-person chamber outside the RAH. However, within the RAH any such cases could only be treated in small, single person hyperbaric oxygen “chambers” used in early days to enhance radiotherapy effectiveness.
There was no ability to effectively ventilate or intervene when needed in this dangerous 100 per cent compressed oxygen environment. Fred saw the opportunity to introduce a safe multi-person hyperbaric chamber with full intensive care medical/nursing capability. Initially, this was achieved in association with the National Safety Council Victorian division) before its demise. This association provided highly experienced technical chamber operational staff, the initial fixed chamber, and a transportable hyperbaric chamber used to transport critically ill patients. The RAH transportable and fixed chambers were used for Victorian cases until a new chamber became operational at The Alfred hospital.
Appropriately, Fred opened the multi-compartment chamber at the new RAH.
Fred exuded calmness, particularly in a crisis. These features, together with his gentleness with patients and their families deservedly achieved confidence with all people involved, be they the givers or those on the receiving end of patient care. Fred was liked by all, especially the retrieval and equipment nurses. The nurses spent many hours sorting equipment in preparation for many retrieval teams to be out simultaneously day or night. Fred also kept terrible work hours, however, the family recalled his dedication to the family unit.
A true gentleman, Fred saw the best in people, believed in social equity and was never angry at anyone. He held the medical profession in high regard. Almost always Fred was dressed in a tie – even at a roadside crash resuscitating a patient with his retrieval overalls on top!
He was a kind teacher and doctor and appreciated by thousands. He always had time to educate and speak to the
ambulance paramedics. He treated all in the field with respect and valued their input. Fred was active in rural education, spending many days touring the rural sector as supported by the South Australian Post-Graduate Medical Association.
Fred received many awards including the Australian Medical Association’s SA service to medicine in 1994 and was awarded the rank of Officer in the Order of Australia (AO) in 1999 for his contribution to intensive care medicine, especially the conduct of airborne intensive care activities.
Despite his dedication to his work, Fred was fortunate to have met Jan whom he married in 1962. Together Fred and Jan displayed their enduring love story and remained the ideal couple for 62 years. Their three children, Chris, Simon, and Sarah, and four grandchildren completed the close-knit family. A lover of music and the piano in particular, Fred was also fond of Japanese whiskey.
Fred died peacefully on 13 May surrounded by family after a short farewell stay at the new RAH ICU with his favourite dog “Eddie” on his lap.
Dr Peter Sharley OAM, FANZCA, FCICM
Patrick Desmond Lynch
1938 – 2024
Patrick was born on 28 March 1938 in Lismore, NSW where his father worked for the postmaster-general. He was the youngest of four children − an elder sister Geraldine and two older brothers Barry and John. The family soon moved to Bathurst where they lived for six years before moving to Broken Hill and then on to Sydney.
Pat’s grandfather loved to play the violin and for his sixth birthday one of Pat’s aunts gave him a violin she no longer used. He learned to play the violin and piano at the local convent. After 12 months of learning both instruments one of the nuns decided he should either play one or the other. Pat chose the violin because she would not hit him across the knuckles if he made a mistake.
Pat went to high school at Marist Brothers Strathfield in Sydney and continued to have violin lessons. At one stage he was playing so well he considered becoming a professional musician. He played classical violin for many years in a quartet.
Pat enrolled in medicine at Sydney University, graduating in 1962. After an internship at Lewisham Hospital he commenced training in anaesthesia at Concord Hospital. After gaining his FFARACS he was appointed staff specialist at Concord, a position he held until his retirement in the mid1990s. He was a founding member of the Concord Hospital pain clinic having gained experience in this field while travelling to Europe and Japan.
He also made his mark in the industrial relations field. He was for several years the federal secretary of the Repatriation Department Medical Officers Association and played a major role in a case that won better pay and conditions for staff specialists and medical officers. This experience resulted
in his appointment to the Administrative Appeals Tribunal (AAT) where he would be involved in providing fair and independent reviews of administrative decisions involving Commonwealth employees who had grievances against the government.
Pat became an Army Reserve officer where he reached the rank of Lieutenant Colonel and was specialist anaesthetist to both the Reserve, and regular, Army as well as to the 4RAAF Hospital Butterworth, Malaysia (1968-1992). He was Commanding Officer of First Field Ambulance and enjoyed regular war games with other nations’ forces.
Everyone who met Pat noticed his distinctive laugh and sense of humour. He never took himself too seriously and always had a joke or funny anecdote to entertain a social gathering of family or friends. He had recorded many Goon Show episodes and friends were not only entertained by the goons, but by watching Pat’s enjoyment of them. His jokes and stories came to the fore in the operating theatre where, as the anaesthetist, he took on the role of raconteur and entertainer.
One of Pat’s admirable traits was his sense of fairness. This might have been an early life lesson as a red-headed violin playing son of the postmaster in a mining town or perhaps instilled by his parents with an Irish sense of local justice. He was never one to put on airs and graces; he always put everyone at ease, whatever their background or status, a quality he instilled in his children.
Pat had a great love of history and he undertook a Masters of Australian History course as an external student at Armidale University for two years preparing a thesis.
His other interests included fine red wines, opera and occasional philosophical discussions. He loved being physically active, whether it was surfing or working on his five acres at Dural, driving the tractor or building dry stone walls. He loved nothing more than having his family and friends over for a BBQ surrounded by children and dogs.
His most enduring and passionate love was his wife Anne who sadly died from myeloma after 50 years of marriage.
Pat is survived by six children and five grandchildren.
Dr Michael Harpur, FANCZA
*This obituary was written with assistance from Pat’s family.
Donald Norman Stewart
1944 – 2024
Donald Norman Stewart was born on 3 January 1944 and grew up with both parents, an older sister and later a younger brother. He was educated at Perth College and then Guildford Grammar School, WA, from 1952 to 1960. He received a state secondary school scholarship, the FA Moss Engineering Scholarship at Guildford, and then a Commonwealth scholarship to study medicine at the University of Western Australia. He worked at Narrogin District Hospital between high school and university and during every university long vacation. Don was grateful to the Narrogin GPs for providing a strong foundation for his future career.
Don attended the University of Western Australia’s School of Medicine from 1961-67 and was active in the WA Medical Students’ Society. He was awarded the Carnation Company Prize in Infant Health in 1966 and decided to become a rural GP.
In 1968 Don started as a resident at the Royal Perth Hospital (RPH). He gave 36 years of interrupted service to RPH before his retirement 46 years later. He had started a three-year program for general practice at Royal Perth Hospital with secondments to Perth’s women’s and children’s hospitals. During his rotation to King Edward Memorial Hospital for Women he participated in the inaugural examination for the diploma in obstetrics for the Royal College of Obstetricians and Gynaecologists. He studied and passed the diploma in obstetrics. But he came to realise that the standards required for country general practice were too high and his thoughts turned to emergency medicine. In 1969 he spoke with Dr Ted Hudson, head of anaesthesia at RPH, about spending time in the department to become skilled in resuscitation in the emergency department. The rest is history as he enjoyed the anaesthesia rotation so much.
He became a registrar in anaesthesia in 1971 although there was no formal training program in WA. Two years later he moved to the UK to gain further experience. He was a registrar in anaesthesia at Chelmsford and Essex Hospital during 1973-75 and then at Luton and Dunstable University Hospitals during 1975-76. During this time, he obtained the diploma in anaesthesia in 1974, then passed the final FFARCS exam in 1976. He also won the Chelmsford Medical Staff Prize for “high standards of his work and other contributions to the medical atmosphere of the district”.
Don returned to Perth and resumed his RPH service as a senior registrar in anaesthesia in 1977. Not long after Dr Bob Wong asked the head of the department, Dr Ted Hudson, if Don could join the small and overworked cardiac anaesthesia group of Terry McAuliffe, Peter Beahan and Bob Wong. In 1978, Don joined the staff of RPH’s department of anaesthesia as a specialist anaesthetist. Between 1978 and 1999 Don’s entire workload was cardiothoracic anaesthesia and medical perfusion. Don was a foundation member of the Cardiac Anaesthetists’ Group and was the anaesthetist in charge of the group for almost 14 years. He was part of the bypass discussion group and a foundation member of the RPH anaesthesia executive group. In 2006 he moved to noncardiac anaesthesia, and then to the preoperative assessment clinic. His medical history-taking was legendary and without equal. In 2002 he received his 30-year long service award. He retired from RPH and anaesthesia practice in August 2014 at the age of 71. And although Don’s contribution to cardiothoracic anaesthesia was extraordinary, it was his commitment to anaesthesia education that stood out.
Don made a long-term contribution to the education of anaesthesia technicians, nurses, ambulance officers, medical students and post-graduate anaesthesia trainees (especially cardiac anaesthesia registrars). There are too many roles and positions to list, but I will emphasise his role in UWA medical student anaesthesia education and examinations that lasted more than 20 years.
In 2001 Don received the ANZCA Citation in recognition of his outstanding contributions to undergraduate anaesthesia training and education in Western Australia. In 2010 Don was honoured to deliver the Bunny Wilson Oration. In 2010 Dr Peter Mcloughlin introduced the Don Stewart Annual Prize for the best anaesthesia technician during their clinical placement. In 2019 he was appointed as Emeritus Consultant, Department of Anaesthesia and Pain Medicine.
Don passed on 6 May after a three-and-a-half-year battle with cancer and is survived by his wife Laurel and his children from his first marriage, Annabelle and Jeremy. He was besotted with Annabelle’s twins and would have loved to see them grow older.
There are so many stories and anecdotes attesting to Don’s strength of character, his advocacy for our specialty, his commitment to excellence, and loyalty to Royal Perth Hospital.
On behalf of all your colleagues, Don, thank you for being a champion for anaesthesia.
Dr Richard Riley, FANZCA Royal Perth Hospital, WA
Ian Pearson
1945 – 2024
Dr Ian Young Pearson, a pioneer in Australian intensive care medicine (ICM), passed away on 22 April 2024.
Born in South Africa, his early experiences in Durban shaped his dedication to mastering a broad range of medical skills. Witnessing a patient’s death due to limited expertise and resources in 1971 became a turning point, driving him to pursue a career in ICU long before it was a recognised specialty.
Dr Pearson’s training was pivotal. His anaesthesia training at the Glasgow Royal Infirmary exposed him to the UK’s first purpose-built ICU, and his subsequent fellowship at Royal Perth Hospital in Western Australia allowed him to gain experience in advanced medical practices in coronary care and post cardiac surgery management. Here, he worked under Dr Geoff Clarke, widely regarded as one of the fathers of intensive care in Australia.
In 1979, Dr Pearson became the inaugural director of intensive care at the new Westmead Hospital. He faced numerous challenges. Building strong relationships with nurses and registrars, he introduced crucial changes, establishing best practices and protocols for patient management. However, gaining recognition for the ICU’s expertise from other specialists required persistent effort.
He advocated for intensivists, specialists with expertise in critical care, to play a leading role in patient management. This initially created friction with some who preferred the traditional system.
In the early stages of development of the unit, Ian collaborated with Dr George Skowronski, one of Australia’s first ICU fellows, to establish a solid foundation for patient care. Together, they championed evidence-based practices and collaboration between intensivists and referring physicians.
Dr Pearson’s leadership extended beyond his unit. He chaired the Australian and New Zealand Intensive Care Society Committee on organ donation, helping to establish standardised brain death diagnostic protocols and procedures and making Westmead ICU a leading provider of organs in NSW.
In 1990, a Westmead hospital executive decision to rotate ICU administration between the specialties of anaesthesia, surgery and medicine led to budget cuts and staffing reductions.
Finding this untenable, Dr Pearson resigned and shortly after was invited to undertake a prestigious visiting professorship in neuroanesthesia at Johns Hopkins University Hospital in Baltimore. Upon returning to Australia, he applied his expertise at the Royal Melbourne and Prince of Wales Hospitals for the last ten years of his career.
Dr Pearson’s legacy is profound. The countless clinicians trained under his guidance made significant contributions to critical care in Australia. Many became ICU directors in Australia and overseas. Some, like Fran Smith, made significant contributions to the establishment of the Careflight medical retrieval system. Neil Soni went on to become director of ICU at the Chelsea and Westminster hospital in London.
Philip Cumpston, specialist in intensive care and anaesthesia, went on to become director of intensive care at the Royal Canberra Hospital and was a founding member and examiner of the Australasian College for Emergency Medicine.
Felicity Hawker became director of ICU at Cabrini Melbourne, and was the first dean of the Joint Faculty of Intensive Care Medicine.
Dr Pearson›s unwavering dedication to establishing ICU as a distinct specialty not only helped save countless lives, but also paved the way for future generations of intensivists.
Dr Philip Cumpston, MBBS (SYD), FANZCA, FCICM, FFACEM, MSc (IT)
Dr John Morris Founding Head Department of Neurology Westmead Hospital
My father knew from the age of six that he wanted to be a doctor. Born in South Africa into a working-class family and as one of four children, he often described the numerous vibrant challenges in achieving this goal. Thankfully, as a very bright child with steady guidance from his strong mother and elder sister, he was able secure a place at a selective school followed by Cape Town University under full scholarship. He later moved to Scotland and then to Australia, where he continued to study throughout his career.
He was devoted to his patients, some of whom he retained friendships with until late in life, such was his impact on their and their family’s lives. One of those friends described him as “never giving up” whilst she was in the ICU as a young teenager, in and out of consciousness for many months. “He always made sure to say goodbye to me everyday, no matter how late he worked, I survived, now I’m married with two children who’ve played sport for Australia at a national level”.
We heard many stories around the dinner table about his passion to change a system. It is not until now, as we hear the wonderful words from his valued colleagues and friends that we appreciate what he achieved.
Ian was a gentle man. He was a lover of rugby, classical music, an avid reader and a talented ballroom dancer. As a Sydney Coogee resident for many years, he spent much of his time in his later career and then in his retirement, walking the coastline and enjoying nature. A devoted friend, father and grandfather, he is deeply missed.
Denny-Lyn Pearson
Daughter of Dr Ian Pearson
Bruce Lindsay Taylor
1955 – 2024
Bruce Lindsay Taylor was born on 14 April 1955 at Broughty Ferry, Scotland and educated at the universities of St Andrews and Manchester. Between 1981 and 1989 he trained in anaesthesia and intensive care in the UK in Gloucester, Southampton, Cambridge, Exeter and Bristol. He travelled to Australia in May 1985 to work as registrar in anaesthetics in Brisbane and medical practitioner to the Queensland Flying Surgeon Service. While there, Bruce gained his pilot’s licence.
Bruce was impressed by Australia’s structured intensive care medicine (ICM) training and returned in February 1989 as registrar in intensive care at Melbourne’s Royal Children’s Hospital and, later, locum staff specialist in intensive care in Brisbane. In 1990, he was awarded fellowship of the Australia and New Zealand College of Anaesthetists (FANZCA) and fellowship of the Joint Faculty of Intensive Care Medicine (FJFICM), subsequently becoming a foundation member of the College of Intensive Care Medicine of Australia and New Zealand.
Returning to the UK in 1990, Bruce took up a consultant post in anaesthesia and intensive care in Portsmouth, initially working primarily in the intensive care unit (ICU) at St Mary’s Hospital. Inevitably, because of his paediatric intensive care expertise, the unit’s reputation for caring for critically ill children grew, and it was often referred patients from surrounding hospitals. Bruce was then invited to serve on national groups working to structure paediatric intensive care services around the UK.
Bruce was an excellent and resourceful clinician, and a consummate problem-solver. His practice was founded on a vast clinical knowledge, outstanding practical and communication skills, empathy for patients and their families, and, above all, extreme kindness. His approach was to always do the simple things well, attend to the details and ensure that patients were safe.
In March 2005 Bruce raised national awareness that the UK’s draft pandemic influenza contingency plan had predicted more than 50,000 UK deaths yet contained no mention of ICU requirements. He was invited to chair the UK Department of Health’s Critical Care Contingency Planning Group and joined several other national bodies considering emergency preparedness.
Bruce was a motivating and enthusiastic teacher, always keen to pass on knowledge, skills and practical tips. He developed two multi-professional courses to teach non-paediatric staff the basics of caring for sick children – paediatric emergency and resuscitation seminars (PEARS) and surgical paediatric emergency and resuscitation seminars (SPEARS). He was also examiner in critical care and applied physiology at the Royal College of Surgeons. He later used his experience of the Australian ICM training system to benefit the UK’s own program as a member of both the board of the UK Faculty of ICM (FICM) and the UK Intercollegiate Board for Training in Paediatric ICM. Bruce was awarded fellowship of the UK Faculty of Intensive Care Medicine at its creation in 2011.
Bruce was a humble Scotsman who failed to recognise the magnitude of his influence on medicine. He often felt an imposter on committees, even those he chaired, and expressed surprise that he could hold his own with those he regarded as superior intellects. Nevertheless, he held several major positions in the UK Intensive Care Society (ICS) – council member; chair of the ICS Standards, Safety and Quality Committee; editor of the Journal of the ICS; ICS honorary secretary and ICS president. In 2012, his contributions to medicine were recognised with the award of a NHS Consultants’ Clinical Excellence Gold Award, honorary fellowship of The Royal College of Physicians and honorary membership of the Intensive Care Society.
Bruce was an accomplished musician, playing violin, guitar and, perhaps inevitably, didgeridoo. He played bass guitar in the band EMD – Emergency Manoeuvres in the Dark –and relished writing material for and participating in hospital revues – his tour de force being a rewriting of Paul Simon’s The Sound of Silence as The Sound of Suction.
Bruce met Claire Rogers, an ICU nurse, in 1986. They married in 1994 and had two sons, Alex and Christopher, and a daughter, Lily.
Cruelly, much of the family’s life, especially the children’s upbringing and memories of their father, was scarred by his development of the symptoms of frontotemporal dementia, finally diagnosed in 2012 as Semantic Variant Primary Progressive Aphasia. Eventually, this robbed Bruce of many of the essential components of his personality – his dry, witty humour, eloquence, originality and ability to comprehend.
After many years of slow deterioration, Bruce died of pneumonia at St Magnus Hospital, Haslemere, UK on 22 January 2024. Posthumously he was awarded the FICM’s Gold Medal in recognition of his exceptional contributions to ICM.
Dr Gary B Smith FRCA, FRCP Retired Intensive Care Medicine consultant
Member benefits
Your membership gives you access to a wide range of resources, opportunities, and services specially designed to support you professionally and personally throughout your career and into retirement.
Exclusive use of our world-recognised post-nominals
Fellowship of ANZCA and FPM are internationally recognised hallmarks that indicate specialists of the highest professional standing. Only members can use the post-nominals FANZCA or FFPMANZCA. Access print and electronic versions of the FANZCA and FFPMANZCA logos for use on your professional communications and marketing collateral via our website.
Supporting your lifelong learning
Unlimited 24/7 access to our world-leading online continuing professional development (CPD) program is included in your membership. It has been specially designed to make sure you meet your mandatory requirements for clinical practice and fellowship. CPD opportunities are available online and in person through a broad series of curated events, courses and meetings.
Helping you to connect and collaborate
No one can understand the passion you have for your profession better than your peers, which is why we’re constantly creating new opportunities for you to connect and collaborate with colleagues across our countries and around the world. As a member, you get priority access to our program of events, courses, and workshops.
Advocating for you and your specialty
We're your voice in the community. We work closely with governments, peak health agencies, and the community to provide advice on clinical practice and advocate for the issues that matter to you, including patient care, clinical standards and doctors’ welfare.
Setting standards
We’re proud to be a leader in patient safety. Our professional documents, guidelines and safety alerts support you in your clinical practice, ensuring the safest and most advanced care in the world.
Providing a safe, healthy, inclusive college culture
Training and practising as a specialist doctor can be tough. We’ve developed a range of resources and services to support you throughout your career, and made inclusion and diversity and doctors' health and wellbeing core components of our training curriculums, CPD, events, governance, and advocacy work.
A world-class medical library at your fingertips
ANZCA library provides access to a wide range of print and online resources, including books, journals, guides and databases, as well as specialist services to suit the clinical information needs of ANZCA and FPM fellows and trainees.
Expert research support
Our Research Consultation Service provides support through literature searching, publishing advice, and the research lifecycle to facilitate the translation of research-based evidence about anaesthesia, pain medicine and perioperative medicine into policy and practice.
Access to research funding
Every year, we make grant funding available to fellows who are novice, emerging or established researchers, for studies in anaesthesia, intensive care, pain or perioperative medicine.
College publications
Your membership entitles you to copies of popular inhouse publications including Australasian Anaesthesia (the Blue Book), Acute Pain Management: Scientific Evidence, the quarterly ANZCA Bulletin.
Recognising excellence
Our awards, prizes and medals recognise achievements in areas such as the advancement and promotion of specialist medicine; exam performance; clinical research; education; and pastoral care.