We'd love to hear from you. Send us your ideas, stories, and comments. ACGMag@gi.org
CONTACT ACG American College of Gastroenterology 11333 Woodglen Drive, Suite 100 North Bethesda, MD 20852 (301) 263-9000 | gi.org
DIGITAL EDITIONS
American College of Gastroenterology is an organization with an international membership of over 20,000 individuals from 86 countries. The College's vision is to be the preeminent organization supporting health care professionals who provide compassionate, equitable, high-quality, state-of-the-art, and personalized care to promote digestive health. The mission of the College is to provide tools, services, and accelerate advances in patient care, education, research, advocacy, practice management, professional development, and clinician wellness, enabling our members to improve patients’ digestive health and to build personally fulfilling careers that foster wellbeing, meaning, and purpose.
CONTENTS
“With one tower, some imported supplies, and four buckets used to manually clean each scope, we completed more than 100 endoscopies—the large majority unsedated—and diagnosed gastric and colon cancers, recommended treatments for inflammation, and attempted to reassure worried patients.”
5
// MESSAGE FROM THE PRESIDENT
As her final President's Message coincides with this issue's cover story and with Women in Medicine Month, Dr. Amy Oxentenko reflects on her term & how fellow ACG women presidents have shaped her journey.
6
// NOVEL & NOTEWORTHY
ACG Trustee Dr. Vonda Reeves joins the ABIM GI board, Dr. Doug Drossman's retirement, Kennedy v. Braidwood, application periods for Leadership YOU and clinical research awards, and more.
8
// PATIENTS
Information for patients, parents, and caregivers on the diagnosis and management of eosinophilic esophagitis.
11
// ACG PERSPECTIVES
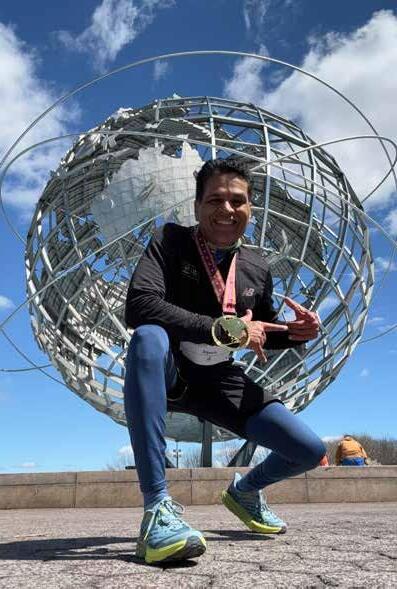
11 RUNNING THE WORLD
Dr. Sripathi Kethu—who has completed more than 100 full marathons—on how marathons help him stay balanced.
14 NORTH AMERICAN GI TRAINING GRANT
Dr. Dora Huang on her experience in Rwanda.
16 INNOVATION
Dr. Eric Shah details his constipation evaluation innovation and lessons learned.
18 // COVER STORY
TRAILBLAZERS & TORCHBEARERS
Dr. Katie Dunleavy speaks with ACG's women presidents about their experiences and journeys as leaders, mentors, and innovators.
29 // TRAINEE HUB
FIRST-YEAR GI FELLOW HANDBOOK
Dr. Clive Miranda shares universal lessons for thriving—not just surviving.
33 // GETTING IT RIGHT
LAW MIND
Ann Bittinger, Esq., delves into artificial intelligence and the standard of care in GI.
35 // INSIDE THE JOURNALS
AJG
ACG Clinical Guidelines on Ulcerative Colitis in Adults, Management of Crohn’s Disease in Adults, and Preventive Care in IBD.
CTG
Impact of Short Duration FODMAP
Restriction on Breath Gases and Gastrointestinal Symptoms by Pathipati, et al
ACGCRJ
Cracking the Code: A Practical Guide to Publishing in the ACG Case Reports Journal by Dr. Himesh Zaver, Dr. Daniyal Abbas, and Dr. Prateek Harne.
37 ACG GUIDELINE HIGHLIGHTS
Preventive Care in IBD (July 2025)
38 ACG GUIDELINE HIGHLIGHTS
Management of Crohn’s Disease in Adults (June 2025)
—DR. DORA HUANG: ACG NORTH AMERICAN GI TRAINING GRANT, PG 14
Dr. Dora Huang traveled to Butaro, a hilly, green region in the north
endoscopy unit.
Member Benefits!
Member Benefits!
Free Education from the Education Universe and the ACG Annual Scientific Meeting that keeps you current on treatment, therapy and management of key GI conditions and disorders
Free Education from the Education Universe and the ACG Annual Scientific Meeting that keeps you current on treatment, therapy and management of key GI conditions and disorders
Free subscriptions to The American Journal of Gastroenterology, Clinical and Translational Gastroenterology, EvidenceBased GI: An ACG Publication and the unique ACG Case Reports Journal
Free subscriptions to The American Journal of Gastroenterology, Clinical and Translational Gastroenterology, EvidenceBased GI: An ACG Publication and the unique ACG Case Reports Journal
Practice management tools that help you improve efficiency and increase profitability in your practice
Practice management tools that help you improve efficiency and increase profitability in your practice
Prior Authorization Letter Generator gives members access to custom letters with relevant data and research that payors are requesting
Prior Authorization Letter Generator gives members access to custom letters with relevant data and research that payors are requesting
Leadership Training offers members Leadership YOU a weekend that brings together a community of established and emerging leaders to cultivate core competencies that drive effectiveness and impact
Leadership Training offers members Leadership YOU a weekend that brings together a community of established and emerging leaders to cultivate core competencies that drive effectiveness and impact
CELEBRATING WOMEN IN MEDICINE MONTH
Amy S. Oxentenko, MD, FACG
IT FEELS ESPECIALLY FITTING
that my final President’s Message for ACG MAGAZINE coincides with September—Women in Medicine Month—and features interviews with the remarkable women who have served as presidents of the American College of Gastroenterology. What a powerful way to mark this moment.
Each of these trailblazing leaders has profoundly shaped my own journey in leadership and personal growth.
Dr. Amy Foxx-Orenstein appointed me to my first ACG committees during my first year as a GI fellow. I vividly remember the imposter syndrome I felt—sitting at those committee tables as the only trainee, one of few women, and visibly pregnant. Yet I was met with open arms and unwavering support. That experience opened the first door to opportunity within ACG for me, and I’ve carried a promise ever since: to do the same for others. From Dr. Foxx-Orenstein, I learned the true power of sponsorship.
Dr. Christina Surawicz has long been a role model of grace, compassion, and authenticity. I recall our time together at the first ACG Train-the-Trainers conference, where her humble and encouraging presence left a lasting impression. That evening, we went shopping together, and she shared her tradition of buying a purse after a tough day—a gesture of self-kindness. We both bought a purse that night, celebrating a day well spent rather than focusing on the day's challenges. After she passed the baton as Senior Associate Editor of The American Journal of Gastroenterology, she
signed her emails to me with “your greatest fan, Chris.” That sentiment is mutual. From Dr. Surawicz, I learned that small expressions of gratitude can have immeasurable impact.
Dr. Carol Burke has consistently used her voice to ensure women are not only present at the table—but heard. She has championed workplace environments that support women’s needs and shown that leadership and part-time work can coexist. Her love for family shines through. I remember her bringing her father to an American College of Physicians meeting in Orlando, where his pride in her was palpable. From Dr. Burke, I learned that personal and professional priorities should be considered with an “and,” not an “or.”
Dr. Susie Kane is a dynamic colleague and friend, full of delightful surprises. Her encyclopedic sports knowledge, love of fantasy football, and regular trips to Sturgis on her motorcycle are just the beginning. She’s also a gifted comedian, never hesitating to bring laughter to our Board of Trustees meetings or Grand Rounds. I often describe her as a pluripotent stem cell—capable of anything. Beyond her vibrant personality, she is a fierce advocate for her physician colleagues and a champion for women in ACG. From Dr. Kane, I’ve learned that Dot’s Pretzels are dangerously addictive—and that her door is always open to those in need of a listening ear.
I look forward to the day when the number of women ACG presidents
“I believe that our greatest achievements still lie ahead, and that if we continue to listen, learn, and lift one another up, we will accomplish even more.”
reaches double digits. It will take time, but we will get there. We’ve laid the foundation—raising awareness, creating opportunities, and fostering a culture of belonging. As efforts around diversity, equity, and inclusion face increasing scrutiny, I urge us all to stay the course. Let us continue to do what is right and ensure our leadership reflects the richness and diversity of our membership.
As my term as President of the American College of Gastroenterology comes to a close, I find myself filled with deep gratitude for the privilege of serving this extraordinary organization over the past year. It has been an honor to work alongside so many dedicated colleagues, to witness the passion and innovation that drive our field forward, and to contribute to the ongoing mission of advancing patient care, education, clinical research, and inclusion within gastroenterology. I am proud of the progress we’ve made together, yet there is still important work ahead. The challenges we face—funding cuts, workforce gaps, burnout, societal tensions, and administrative burden— require continued collaboration and commitment. As I prepare to hand over the baton to Dr. William Chey, I do so with full confidence in his vision, leadership, and unwavering dedication to our members and our mission. His thoughtful approach and tireless advocacy will serve ACG well in the year to come. I believe that our greatest achievements still lie ahead, and that if we continue to listen, learn, and lift one another up, we will accomplish even more. Thank you for the opportunity to serve, for the trust you’ve placed in me, and for the inspiration you provide every day. Together, we are shaping the future of gastroenterology—and I couldn’t be more hopeful for what’s to come.
Warmly, —Amy
& NOTEWORTHY
[GOVERNANCE]
DR.
VONDA REEVES JOINS ABIM GASTROENTEROLOGY
BOARD
The College congratulates ACG Trustee Vonda Reeves, MD, MBA, FACP, FACG, on being selected to serve as a member of the American Board of Internal Medicine's (ABIM) Gastroenterology Board.
Broadly, ABIM Specialty Boards have oversight of the approval committees and are responsible both for the broad definition of the discipline across Certification and Maintenance of Certification (MOC) and making Certification and MOC relevant vehicles in their discipline. The Gastroenterology Board is responsible for oversight of ABIM policy and assessment in gastroenterology.
Dr. Reeves, who practices at GI Associates Endoscopy Center in Flowood, MS, began her service on the Gastroenterology Board on July 1, 2025.
Read the ABIM announcement: bit.ly/abim-gi-board
[RETIREMENT]
The College congratulates DOUGLAS A. DROSSMAN, MD, MACG, on his recent retirement from clinical practice after 54 years of providing care for patients with disorders of gut-brain interaction and other GI conditions. Dr. Drossman will continue his work in the GI community through Drossman Care, where he contributes to educational programs and training, and in his role as CEO of the Rome Foundation.
[SHERMAN PRIZE] CONGRATULATIONS TO THE 2025 SHERMAN PRIZE WINNERS: Michael Kappelman, MD, MPH; Scott B. Snapper, MD, PhD; and Oriana Damas, MD. The Sherman Prize is awarded to IBD clinicians, surgeons, researchers, or academics with extraordinary track records of achievement, making exceptional and pioneering contributions that transform IBD care.
[LEARN TO LEAD] APPLY FOR ACG INSTITUTE’S LEADERSHIP YOU!
Choose the leadership program that fits your career stage! The ACG Institute’s Leadership YOU, will convene four leadership programs over one weekend, June 5-7, 2026, in Washington, DC, providing an opportunity for participants in all four cohorts to network and engage in shared learning sessions, in addition to cohort-specific professional development. The four leadership programs now accepting applications are the Emerging Leadership Program, Early Career Leadership Program, Advanced Leadership Program, and Clinical Research Leadership Program.
Application Deadlines
• Early Career, Advanced, and Clinical Research Leadership Programs: November 14, 2025
• Emerging Leadership Program: November 24, 2025
Learn more and apply: gi.org/leadership-you
[SUPREME COURT RULING] SUPREME COURT UPHOLDS PREVENTIVE CARE ACCESS, BUT CONCERNS REMAIN
In June, the U.S. Supreme Court voted 6-3 in Kennedy v. Braidwood to uphold the U.S. Preventive Services Task Force’s (USPSTF) role in recommending which services must be covered with no cost sharing for patients under the Affordable Care Act (ACA)—a significant decision that ACG hopes will protect decades of colorectal cancer (CRC) screening progress.
“Gastroenterologists know firsthand that limiting access to colorectal cancer screening would have deadly consequences,” said ACG President Amy S. Oxentenko, MD, FACG. “We appreciate that the Supreme Court heard the College’s warning and urge the U.S. Department of Health and Human Services (HHS) to maintain the USPSTF’s essential role moving forward.”
In the spring, ACG represented the interests of GI providers and patients by submitting a “friend of the court” amicus brief. ACG championed the lifesaving benefits of CRC screening and alerted the court of the practical implications of eliminating the ACA's preventive services mandate.
The Supreme Court's ruling also affirmed the HHS Secretary's power to appoint or replace USPSTF members, as well as accept or reject their recommendations. In this context, ACG now urges Secretary Kennedy to maintain the integrity and independence of USPSTF members and the task force’s existing role within the ACA, ensuring its recommendations remain the gold standard for clinicians, patients, insurers, and policymakers.
Read more: bit.ly/braidwood-ruling
[RESEARCH FUNDING]
ACG 2026 GRANT PORTAL OPEN – APPLY NOW
The ACG Institute for Clinical Research & Education is pleased to announce the 2026 ACG Clinical Research opportunities! Last year, the Institute awarded $2.3 million in funding, bringing all-time ACG Institute funding to $34.2 million granted to 764 investigators.
Of note, the Clinical Research Award and Clinical Research Pilot Award amounts doubled this year! Learn more about this year’s awards and apply by December 1, 2025:
• Junior Faculty Development Award: $450K/3-year
• Established Investigator Bridge Award: $300K/2-year
*Note: New eligibility criteria and pre-qualification application due November 3: bit.ly/acg-bridge-form
• Leonidas Berry Health Equity Research Award: $75K ($50K year one, $25K year two, based on progress)
• ACG/ASGE Epidemiologic Research Award in Gastrointestinal Endoscopy: $50K/1-2 years
*Note: Submit request to GIQuIC for a letter of support by November 3.
• Clinical Research Awards: $100K/1-year
• Clinical Research Pilot Awards: $30K/1-year
• Medical Resident Clinical Research Award: $10K/1-year, plus travel to ACG 2026
• Medical Student Clinical Research Award: $5K/summer project 6-10 weeks, plus travel to ACG 2026
LEARN MORE: gi.org/research-awards
Diagnosis and Management of
EOSINOPHILIC ESOPHAGITIS
Information for Patients, Parents, and Caregivers: Understanding the ACG Clinical Guidelines
About
• The esophagus is the swallowing tube that connects the mouth to the stomach.
• Eosinophils are a type of white blood cell that are normally in the body, but not normally present in the esophagus.
• Eosinophilic esophagitis (abbreviated “EoE”) is a chronic allergic condition of the esophagus and can be thought of like “asthma of the esophagus.”
Symptoms: The most common symptoms in adults and adolescents are trouble swallowing and food getting stuck. While these can also happen in children, more common symptoms in children are poor growth, feeding difficulties, abdominal pain, and vomiting.
Warning Signs That Should Not Be Ignored: Trouble swallowing, choking on food, or getting food stuck is never normal and should be evaluated by a doctor. If food gets stuck and you can’t get it down or up (called a “food impaction”) you should go to the emergency room.
Diagnosis: EoE diagnosis requires having symptoms related to the esophagus and having increased levels of eosinophils in tissue samples of the esophagus (called “biopsies”). The tissue samples are obtained during an upper endoscopy, which is a procedure where you are asleep and a tube with a light and camera is placed through your mouth and into the esophagus. This also allows the esophagus lining to be examined for abnormal findings such as inflammation and scar tissue formation that can happen in EoE.
Treatment: The treatment types are diet elimination or medications. If there is scar tissue in the esophagus, dilation may also be necessary.
Diet Elimination: For many people, foods can trigger EoE. However, current allergy tests cannot tell what triggers EoE, and symptoms related to food also cannot tell you the triggers. However, we do know on average which foods are most likely to cause EoE, so a selection of these can be removed.
Medication Options
• Proton pump inhibitors
• Topical steroids
• Biologics
Esophageal Dilation: (stretching of the esophagus) is safe and effective to improve symptoms if there is scar tissue in the esophagus and if you have trouble swallowing. If dilation is done, you will still need a treatment to control the inflammation related to EoE, since dilation only stretches the scar tissue and does not treat the underlying EoE.
The Role of Endoscopy: After a new treatment is started or an existing treatment is changed, an endoscopy is needed to check the esophagus and collect biopsies. While you are on long-term treatment, you should follow-up with your provider regularly and an endoscopy could also be needed to check how things look.
Important Treatment Note: EoE is a chronic (long-term) condition that does not have a cure right now, so treatment and monitoring must be continued long-term. If treatments are stopped, EoE will flare up.
LEARN MORE
Questions for your Doctor
• Do I have EoE?
• Should I try an elimination diet or medication treatment for EoE?
• Can I work with a dietician or nutrition to help with the diet elimination treatment?
• What are the side effects of the medications for EoE?
• What should I expect during an endoscopy?
• What should I expect after the endoscopy if I have an esophageal dilation?
• How often will I need upper endoscopies?
• How often will I need clinic visits?
• Who will I work with in your office to help with medication approvals if the insurance denies the prescription?
• What is the most effective way to take the medication you are prescribing?
Eosinophilic Esophagitis in Pediatric and Adolescent Patients: gi.org/topics/eosinophilic-esophagitis-in-pediatric-andadolescent-patients
Author: Evan S. Dellon, MD, MPH, FACG
Read the ACG EoE Guideline Published January 2025 bit.ly/acg-eoe-2025
| American College of Gastroenterology: gi.org | Find a Gastroenterologist: gi.org/FindaGI
World Running the
How Marathons Help Me Stay Balanced as a Busy Gastroenterologist
By Sripathi Kethu, MD, FACG
I RAN MY FIRST FULL MARATHON IN 2016 in Dallas, TX. I still remember the moment I crossed the finish line—it wasn’t just the 26.2 miles that made it unforgettable, but the four months of focused training, the early mornings, and the realization that I had achieved something I once thought was impossible. It all started a year earlier with a half marathon, just to test the waters. Little did I know that this decision would evolve into one of the most transformative journeys of my life.
Fast forward to today: I have completed over 100 full marathons, including races on all seven continents. Yes, even Antarctica. I’ve run the six World Marathon Majors— Boston, New York, Chicago, Berlin, London, and Tokyo—and completed full marathons in all 50 U.S. states. It’s a journey that has taken me from the snow-covered tundras of Greenland to the sun-drenched trails of Hawaii. Each race has taught me something new about discipline, resilience, and joy.
HOW IT ALL BEGAN
My journey into running wasn’t planned—it began as a stress-relieving activity. Like many physicians, I needed a way to counterbalance the demands of a rigorous medical practice. Running gave me a sense of control, clarity, and space. It started as a simple, routine jog but gradually morphed into something much larger.
When I committed to my first marathon, I joined a local running group. Every Saturday morning, rain or shine, we met at 6:00 am for our long runs. During the weekdays, I trained four to five days, integrating speed workouts like fartleks, hill repeats, and strength training. I was never a natural-born runner, but consistency was the key. The group not only held me accountable but made the journey enjoyable.
THE DEMANDS OF TRAINING
Training for a marathon requires more than just logging miles. It requires intention. Each week typically involves one long run, tempo workouts, recovery runs, and cross-training days. Equally important are sleep, nutrition, and mental preparation.
As a gastroenterologist, my schedule is anything but predictable. Endoscopies, clinic visits, and hospital consults lead to my days filling up quickly. So, I learned to treat my training like any other professional commitment. Early morning runs before work became the norm. I kept my gear ready the night before, blocked time in my calendar, and learned to be flexible. Some days it meant running in the dark; other days, I squeezed in a short treadmill session in the evenings after work.
To help others—especially busy professionals—who want to start their own running journey, I recently wrote a detailed guide—Marathon Training Schedule for Doctors—which is available at docwealthhub.com/ marathon-training-schedule-fordoctors. It’s tailored for people juggling demanding careers who still want to pursue long-distance running.
WORK-LIFE INTEGRATION: IT’S ABOUT PRIORITIES
One question I get asked often is, “How do you find the time?” The truth is, we all have the same 24 hours in a day. It’s less about finding time and more about choosing how to use it. I prioritize activities that enhance both my mental and physical well-being. Running has become non-negotiable for me—not just for my body, but for my mind. It provides clarity, reduces stress, and helps me show up as a better physician, spouse, and friend.
To anyone struggling to find balance, I offer this: start by identifying what fuels you. It may not be running. It could be tennis, hiking, dancing, or working out in your home gym. Schedule it like you would a patient appointment. Make it part of your life, not an afterthought.
I also make time for family, social connections, and hobbies. A well-rounded life is a more sustainable one. You don’t have to do it all every day—balance happens over the week, not just the day.
A FEW MILESTONES THAT STAND OUT
Among the 104 marathons I’ve completed so far, several stand out for their uniqueness and challenge.
Greenland was undoubtedly the toughest. The majority of the course was covered in ice and snow. I ran about six miles on a pure ice sheet, which meant I needed to wear spikes on my shoes. The temperature was freezing, and any sweat turned to ice in seconds. I wore layers, yet still struggled to keep my hands warm. Removing gloves even briefly led to instant chill burns. It was both physically and mentally grueling—but also breathtakingly beautiful and deeply rewarding.
Running in Antarctica was surreal. Surrounded by glaciers and penguins, it was a reminder of the vastness of our planet—and the lengths one can go when committed to a goal. It wasn’t just a physical accomplishment—it was symbolic of how far I had come from when I hesitantly took on my first half marathon.
Completing the six World Marathon Majors and running in all 50 states were also proud moments. These goals took years of planning, training, and travel. As someone of Indian origin, I might be among the very few, if not the only one, to have completed all four—100+ marathons,
all 50 states, all six Marathon Majors, and all seven continents. This accomplishment is personal, but I hope it also serves as inspiration to others—especially those who believe their age, schedule, or background might hold them back.
WHAT RUNNING HAS GIVEN ME
Running has given me more than medals and memories. It has made me mentally resilient, physically stronger, and spiritually centered. In many ways, it mirrors the practice of medicine: every case is different, every patient is unique, and yet you show up every day committed to the process.
As physicians, we’re often the last to care for our own health. Running reminded me that self-care isn’t selfish—it’s necessary. I’ve become a better listener, more patient, and more empathetic in my clinical practice. And on a personal level, it has brought me lifelong friendships, countless sunrises, and an appreciation for nature and the human body that I never imagined.
SHARING THE JOURNEY: FROM CLINICS TO YOUTUBE
In August 2024, I launched a YouTube channel—Dr. Kethu, available at youtube.com/@DrKethu—to share what I’ve learned about gut health, running, fitness, and general wellness. I wanted to create a platform to educate the public, debunk common myths and misinformation on social media, and inspire others to live healthier lives. It has been one of the most rewarding extensions of my work.
Whether it’s explaining how fiber affects digestion, healthy eating, busting myths about probiotics, or talking about training plans for firsttime marathoners, the channel has helped me connect with a broader audience—people who may never see a gastroenterologist but are eager to learn how to take better care of themselves.
FINAL THOUGHTS: YOU CAN START TODAY
You don’t need to run 100 marathons to experience transformation. Start small. Walk around the block, jog for five minutes, or try a beginner
strength training video at home. The key is consistency and a mindset shift.
Aim for at least three workouts a week. Prioritize sleep. Eat well. Manage stress. Surround yourself with a supportive community. These are the foundations of a happy, healthy, and long life.
Running just happened to be my vehicle— but the destination is available to everyone.
Dr. Kethu is a gastroenterologist at Digestive Health Center of Plano, Plano, TX.
Clockwise from top right: Dr. Kethu participating in marathons in Australia, New York City, Hawaii, and Greenland, respectively.
ACG NORTH AMERICAN INTERNATIONAL GI TRAINING GRANT
By Dora Huang, MD
I WAS FORTUNATE TO TRAVEL TO RWANDA as part of the ACG North American International GI Training Grant. My original trip, planned to coincide with Rwanda Endoscopy Week (REW) and scheduled for November 2024, was delayed given the outbreak of Marburg virus in the country. Rwanda’s swift and successful response to the virus was exemplary, a demonstration of the growing capacity of the region, and REW was rescheduled for March 2025. Unfortunately, given an Ebola outbreak in Uganda, I was then unable to return to Mbarara for the second portion of my trip, though I have continued to work remotely.
I started my trip in Kigali, where I met with many of the GI clinicians and educators who have been partnering with REW and GI Rising over the past 10 years. Their services stretched throughout the city, from the academic
University Teaching Hospital of Kigali (CHUK) to the more private-based King Faisal Hospital, from the new Rwanda Military Hospital to the Charite Digestive Charity Clinic, the base of GI Rising’s operations. The impact of GI Rising on GI subspeciality care in Kigali cannot be overstated.
While in Kigali, we were able to observe clinic and endoscopy, the latter quite different when compared with the United States or even Uganda the year prior. Documentation, availability of sedation, and cleaning techniques differed— patients’ families were encouraged to record the endoscopy from a separate room, as patients’ access to online or digital records varied, and support staff manually processed scopes. Each hospital or clinic offered a different level of service, for example, as it related to advanced technique, sedation availability, colonoscopy with prep, etc. With other attendings and fellows in Kigali, we
delivered lectures and board review to current fellows and worked on the research arm of REW.
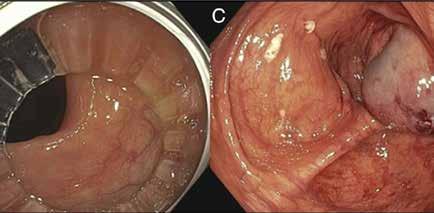
Our teams then dispersed to more than five different areas of the country, transporting rented scopes and supplies to set up endoscopy. With attending gastroenterologist Dr. Matt Smith, an endoscopy tech, and an emergency room nurse from the U.S., I traveled to Butaro, a hilly, green region in the north of Rwanda, closer to the Ugandan border. This was the second time a group from REW has visited this region, with the first time documented in a 2018 ACG MAGAZINE article by Katie Dunleavy, MB BCh BAO. Paired with the clinical director of Butaro Hospital and an operating room technician, we were given two empty rooms to open an endoscopy unit.
With one tower, some imported supplies, and four buckets used to manually clean each scope,
we completed more than 100 endoscopies—the large majority unsedated—and diagnosed gastric and colon cancers, recommended treatments for inflammation, and attempted to reassure worried patients. It changed my perspective on our “typical” requirements for anesthesia, nursing, and support staff. Across all the sites, the teams completed over 750 scopes, the impact of which is still being measured.
I hope to continue working with the research team at CHUK as they compile and analyze the data from this experience. Their IRB, which plans to look at patient outcomes after participating in these weeks, will quantify the impact of offering endoscopic care to the region, potentially encouraging more national and academic investment in GI subspecialty care.
My remote work in Uganda will also continue, as we work on our IRB to measure the impact of the newly formed GI clinic and endoscopy unit. Our work on characterizing patients diagnosed and treated with hepatocellular carcinoma is expanding as well.
I remain grateful for the partnerships that have formed across Boston and East Africa.
Dr. Huang is an attending gastroenterologist at the VA Pacific Islands Health Care System and completed her GI fellowship at Beth Israel Deaconess Medical Center in Boston, MA.
The views expressed in this article are those of the author and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
SPOTLIGHT ON INNOVATION:
REFRAMING CONSTIPATION EVALUATION WITH RED FOR GENERAL GASTROENTEROLOGY
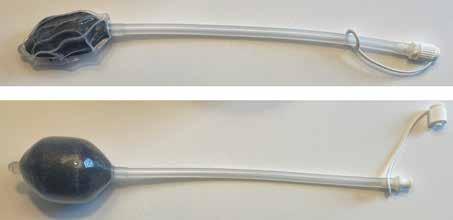
IN GASTROENTEROLOGY, meaningful innovation often emerges from the need to make diagnostic tools more accessible, efficient, and impactful in everyday practice. One such advancement is the Rectal Expulsion Device (RED). To explore this novel tool, we spoke with Dr. Eric Shah on behalf of the ACG Innovation & Technology Committee. Dr. Shah shared the inspiration, development process, and implementation strategies behind this disruptive technology.
Could you briefly describe what RED is and the clinical need it addresses?
RED—red4constipation.com—is a point-ofcare device designed to quickly identify pelvic floor dysfunction in patients with constipation at the time of their first GI visit. This device is used by inserting into a patient's rectum when they lay on their left side on an exam table, removing a cap to inflate the foam-filled balloon, asking the patient if they feel the urgent need to poop with the balloon inflated, and having the patient try to poop the balloon out without moving to a commode. RED can be done in separate, brief, back-to-back procedure visits just like a hemorrhoid banding clinic, or during the initial appointment itself
“The most important milestone is to choose the right teammates up front, which is usually more important than the idea itself.”
without disrupting workflow. RED is for patients seeing general gastroenterology who have constipation: some patients might have sensation of incomplete evacuation, overflow diarrhea, or hemorrhoids as part of their constipation, despite having soft, formed stool. RED predicts whether patients get better when they see a pelvic floor physical therapist. RED allows the provider to efficiently show the patient what pelvic floor physical therapy is all about. RED is designed to fit a fast-paced office visit or procedure appointment in the clinic.
What inspired you and your team to pursue this project, and how did the idea evolve from concept to implementation? The idea came from the fact that pelvic floor tests are traditionally used for patients at the end of the road, after failing other treatment options. Traditionally, comprehensive anorectal testing identifies treatment-refractory patients that respond to biofeedback in tertiary-level motility clinics for the small subset of patients needing that type of care. That paradigm is not designed to fit
A Conversation with Raseen Tariq, MD, MS, and Eric D. Shah, MD, MBA, FACG
“Meaningful innovation often emerges from the need to make diagnostic tools more accessible, efficient, and impactful in everyday practice.”
patients in general gastroenterology who just need daily laxatives or pelvic floor physical therapy. RED helps bring this type of testing to the front of the care pathway for patients in general gastroenterology, tied to pelvic floor physical therapy that is broadly available—pelvicrehab.com. Using RED allows an efficient conversation to inform patient selection, so as not to overwhelm pelvic floor physical therapists with patients who may not have significant pelvic floor problems or who might prefer other options after seeing what pelvic floor physical therapy entails.
What were some of the key milestones and challenges during development and clinical integration?
The biggest hurdle was the inertia to get started. The most important milestone is to choose the right teammates up front, which is usually more important than the idea itself.
How did collaboration or institutional partnerships play a role in the success of the initiative?
The University of Michigan played a critical role in the success of this project. Universities are often seen as a roadblock, but they can actually be a tremendous help. It is worth the deep
dive to understand the institutional policies, funding opportunities, and people around you that can help you get to the next step. There is no one-size-fits-all environment, and the right environment depends on the type of product you are developing. Many groundbreaking technologies arise from small practices outside of large universities.
What advice would you offer to clinicians or trainees interested in turning clinical observations into practical, scalable solutions?
Focus on the things around you and don't worry about having the right idea for the next big thing—hardly anyone ever does. Partner with the right people who have similar interests. Having the right partnerships leads to greater success. Avoid the goal of being "the innovator," as lightning is rarely going to hit twice. Enjoy the day job and advocating for patients and physician-owned practice.
How has your MD-MBA background shaped your approach to innovation in GI? Administrators see you as a physician, and physicians see you as an administrator. This skillset gives you the opportunity to find avenues for both sides to work together. While an MBA does not directly give you entrepreneurial skills, it can give you a sense of business management and the constructs of U.S. healthcare.
Are there specific ACG resources (e.g., mentorship, education, conferences) that helped support or influence this work?
ACG has robust offerings for fellows-in-training and early-career gastroenterologists. Beyond the ACG Annual Scientific Meeting, which offers tremendous value to fellows-in-training, I would also strongly encourage fellows to look into the ACG-FDA Visiting Fellowship Program when it returns, North American Conference of Gastroenterology Fellows (NACGF), and Early Career Leadership Program.
LESSONS LEARNED
1. Innovations don’t have to be complicated. Simplicity in design and workflow compatibility often make or break clinical adoption.
2. Trust the clinic as your lab. If a solution doesn’t fit into real-world practice, it likely won’t scale.
3. Institutional alignment is key. Understand your environment and engage champions early.
4. Start with the people, not the product. The right team determines the longevity and impact of any innovation.
5. Stay patient focused. RED was built to help providers and patients have better conversations, faster.
Dr. Shah is an Associate Professor in the Division of Gastroenterology and Hepatology at the University of Michigan who has expertise in esophageal motility, reflux disorders, and pelvic floor disorders. He serves as Innovation Champion for U-M Innovation Partnerships and is Director of the Michigan Medicine GI Physiology Laboratories.
Dr. Tariq is an Assistant Professor in the Division of Gastroenterology, Hepatology, and Nutrition at Virginia Commonwealth University who has expertise in inflammatory bowel diseases. She is a graduate of an NIH-sponsored T32 Gastroenterology fellowship at Mayo Clinic Rochester. She is a member of the ACG Innovation & Technology Committee.
TRAILBLAZERS TORCHBEARERS
& TRAILBLAZERS TORCHBEARERS
PRESIDENTS
THE LEGACY OF ACG WOMEN
Katie A. Dunleavy, MB BCh BAO
AAs a young woman at the start of my career in inflammatory bowel disease and gastroenterology, I’ve found inspiration and guidance in the leaders of the American College of Gastroenterology (ACG). Throughout my training and now in the early stages of my career, I’ve been fortunate to learn from and work alongside women gastroenterologists in prominent leadership roles, an opportunity that, not long ago, was far less common. In her 2023 The American Journal of Gastroenterology publication, "Women in Medicine: Honoring the Past and Bringing Women Further into the Scope of Gastroenterology,"1 ACG President Amy S. Oxentenko, MD, FACG, captured this evolution with clarity and depth, reminding us that today’s progress stands on decades of perseverance and advocacy.
I am honored to serve on the ACG Women in GI Committee. Since its inception in 1989, initially as an ad hoc group formed by then ACG President Jamie S. Barkin, MD, MACG, this committee has played a crucial role in advancing opportunities for women within the College. Its first chair, Robyn G. Karlstadt, MD, MACG, reflected on its origins with sincerity:
“I am very appreciative that the College took a chance comment of mine to establish a committee that has demonstrated its value to the organization many times over. The committee and the College have identified intelligent, passionate,
extremely capable women and helped develop them to become incredibly strong leaders in medicine/ GI today. You know my feelings toward the College. I am glad that I could be a part of this. Remember, I am old enough to have been told, ‘You will never succeed because you are a woman in gastroenterology. Who would want to see a woman physician?’ We’ve come a long way.”
Today, under the leadership of Chair Kara M. De Felice, MD, FACG, and Vice Chair Kathryn E. Hutchins, MD, FACG, the Women in GI Committee continues its mission of adapting, growing, and supporting the evolving needs of women in GI. Inspired by their efforts and the history of the committee, I felt compelled to learn more about the women who have led our organization in its highest role—as ACG President. To date, five exceptional women have served in this role, each helping to shape the direction of our field while breaking barriers for those who follow. I set out to learn from their experiences through interviews that highlight their journeys as leaders, mentors, and innovators. Dr. Foxx-Orenstein, who served as ACG President from 20072008, was not available to participate in this article. The responses here draw on a 2009 conversation Dr. Foxx-Orenstein had with Alvin M. Zfass, MD, MACG.
These are their stories, trailblazers and torchbearers who have helped redefine what leadership looks like in gastroenterology.
Looking back on your presidency, was there a defining moment or initiative that captured the essence of your leadership? What about it still resonates with you today?
Amy S. Oxentenko, MD, FACG (2024-2025): Since joining the ACG Board and throughout my path to the presidency, I have remained committed to improving the representation of women and underrepresented groups in the College. It was clear to me from my first year on the Board that while important conversations were happening, the momentum for real action still needed a push, and I saw this as an opportunity and responsibility. As a former residency program director, I approached diversity in training programs with a similar lens. As I looked at guideline authorship, speaker lineups, and award nominations, I always asked the question, ‘Does this group of individuals represent the membership of our society?’ One of the small, but meaningful changes was the inclusion of the demographic breakdown of all meeting speakers to be reviewed during the planning process. I wanted to ensure that we were intentional about representation of qualified speakers. This past year has been challenging, as nationally we’ve taken steps backwards in the fight for equity and inclusion where we had started to make good progress. Despite this, the College remains committed to selecting expert faculty who represent the full breadth of its membership.
However, my vision for this year was a bit of a pivot and emerged from concerns raised at last year’s Board of Governors meeting around workforce shortages. While these shortages are certainly felt in academic settings, the impact is even more pronounced in private practices and endoscopy centers. It’s not just about the number of GI physicians. We’re seeing shortages across the board: anesthesiologists, CRNAs, endoscopy technicians, nursing staff, and allied professionals. At the same time, more nurse practitioners and physician assistants are entering GI, but we need to figure out how to integrate and support them meaningfully. The question became: What does the future of the GI workforce need to look like? The theme for any presidency must be one that resonates across the College and
its leadership, so that it becomes an investment in the long term. Therefore, the Workforce of the Future became the focus of my year, drawing on the needs of our members and my passion for training.
Also, attending ACG’s Advocacy Day on Capitol Hill was a pivotal moment. Not having come through the Governors’ path, it was eye-opening to see the crucial voice of healthcare professionals in driving policy change. Advocacy isn’t always popular but, now more than ever, it is essential. One of the most powerful and emotional experiences of my year was being in Washington, DC, for Colorectal Cancer Awareness Month, and standing on the National Mall among 27,400 blue flags, each representing someone under the age of 50 who is projected to be diagnosed with colorectal cancer by 2030. Hearing the stories of cancer survivors that day was incredibly impactful, and it empowered me to continue to do the hard work.
Sunanda V. Kane, MD, MSPH, MACG (2018-2019):
My legacy for my ACG presidential year was the creation of two work groups that later became the Innovation and Technology Committee and the Advanced Practice Provider (APP) Committee. I recognized early on that APPs play a critical role on the frontline of GI care. Despite their essential contributions, APPs weren’t being meaningfully represented in the College. At the Board level, there were conversations about the role of APPs in a historically physician-oriented organization and how to incorporate the full clinical team into the organization. I said, ‘We are the American College of Gastroenterology, and we are here to serve all providers.’ If we have industry partners and an FDA-Related Matters Committee, we should have dedicated space for the APP community.’ With the Board’s support, I launched the APP Committee by appointing an enthusiastic and respected senior APP, Mary S. Vetter, ANP-BC, who had long been a friend to the College, to serve as its inaugural chair. She took that opportunity and ran
with it, and today APPs have found a professional home in ACG. Similarly, the Innovation Committee has done amazing things, including the Endoscopy School, and I was happy to support their startup. These new initiatives did not emerge in isolation but were built on the foundation of other successful programs I helped champion throughout my years with ACG, including the North American Conference of GI Fellows (NACGF); the Navigating, Networking, and Negotiating Your First Job Workshop; and a focus on identifying strong leaders to head new initiatives. I like to joke that one of my small, but meaningful contributions was making ACG pins accessible for women’s clothing with magnet-backed pins. I even had my presidential ACG pin mounted into a necklace honoring this change.
Carol A. Burke, MD, MACG (2016-2017): There were two defining moments of my presidency. One was related to burnout and wellness in GI, and the other was concerning the ABIM Maintenance of Certification (MOC) program. Burnout was a looming epidemic in healthcare related to changes in models of reimbursement for clinical gastroenterologists, and the ABIM MOC program at the time was recognized by our members as an impractical, expensive, burdensome system, which had no convincing evidence to demonstrate that the program could judge or translate results on the quality of patient care delivered by, or practical, clinical important knowledge required of GI physicians in practice. I gathered a small group of ACG member collaborators—including ACG Past
President Dr. Chris Surawicz, who also had worked in burnout, and we devised a survey based on input from Dr. Tait Shanafelt, oncologist and burnout researcher, which was deployed to our ACG members in 2015-2016. When I presented the results during my presidency, it was the first inventory of burnout in GI and demonstrated burnout was prevalent (50%) in respondents and highlighted risk factors. That project spun off in future years to additional surveys the ACG deployed, which included GI fellows-in-training demonstrating similar results.2 Recognition of burnout and strategies for burnout mitigation are now well-recognized and incorporated in many programs and practices. The ABIM MOC program was a major factor contributing to stress and burnout in our membership who wanted change. The power of inspiration, collaboration, and creative force led to a substantial change in the ABIM program in GI, which now includes the longitudinal knowledge assessment and has rid us of other ABIM MOC requirements. What still resonates with me today is that we made palpable change to the practice of GI through both initiatives. Notably, during my presidency, all four major societies—ACG, AGA, ASGE, and AASLD—had women Presidents. At that time, I found [that the regular meetings among the societies] had more camaraderie and collegiality, and that having all women fostered a closer relationship.
“While change can be inspired by the vision of a single person, it requires a team of people from varied backgrounds, expertise, and diverse opinions to provide honest feedback and the skillset to turn vision into reality to propagate durable change.” — Dr. Burke
Amy E. Foxx-Orenstein, DO, MACG (2007-2008):
Under my ACG leadership, we had the opportunity to redo the Strategic Plan for the College, which was a monumental event. It had first been done in 2002 and [had not been] redone since then. The Strategic Plan for the ACG is the vision. What’s our mission? How are we going to get there? And we had to break it down into what areas the ACG should be most focused on. That was one event that I’m very proud of, because it really helped to shape the College for the next several years.
She reflected on another defining moment during her presidency:
The obesity initiative was another goal that I had. The prevalence of obesity has increased remarkably in the past 30 years, and it impacts every gastroenterology practice. We invited several different experts in the field, and we created materials from interactions amongst all those experts that [were] available on the website for physicians. That was a very important charge that I hoped to bring to the forefront of every gastroenterologist’s mindset.
Christina M. Surawicz, MD, MACG (1998-1999):
One of the first programs of my presidency was the Prescriptions for Success: Careers in Medicine and Science, which was held at Alhambra High School in Phoenix, during the Annual Meeting. As a parent of teenagers, I recognized that the pipeline for medicine and science cannot wait until college. This outreach program for disadvantaged and minority high school students happens each year during the ACG Annual Scientific Meeting, and I am grateful to the many ACG staff and members who continue this program today.
As one of the pioneering women to hold the highest office in ACG, what internal compass guided you through moments of resistance, complexity, or transformation, and how did those moments shape your legacy?
Dr. Surawicz: The ACG presidency is pivotal and collaborative. One cannot reach the presidency without working in the organization, for example as a committee member, a regional governor, trustee, and an officer. The committees are the little ‘hands and feet’ that move an organization forward
and rely on members and the always outstanding ACG staff and leadership. David Graham, MD, MACG, introduced me to the College and gave me early opportunities like chairing the annual Postgraduate Course, which gave me the freedom of choosing topics and speakers. I learned key leadership lessons from the first ACG Executive Director, Tom Fise, Esq., and later his successor, Brad Stillman, JD. For example, recognize that if you do not address conflict, you may not get change, so learn to embrace it. Tom pointed out that the saying that conflict is like a pancake, with two sides, is wrong; in fact, there are three sides: yours, mine, and the truth. Finally, I have been guided by the famous Maya Angelou quote: 'I’ve learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel.'
Dr. Foxx-Orenstein: Dr. Chris Surawicz was the Chair of the Women in GI Committee when I joined ACG, and Chris’ leadership style was remarkable. She opened my eyes to how a woman in this profession can make a real difference. She was succinct. She helped make subcommittees when the conversation went on too long. I wanted to emulate that pattern of leadership. I saw a level of organization coming from a woman who was strong, well-spoken, and could mix with any group, any gender, people of all races, and diverse individuals, and she seemed to have an impact. And I saw that there were things that I needed to learn to hopefully expose more people to the College.
Dr. Kane: I always return to my internal compass of asking myself: What is best for the constituents? For example, during my presidency, establishing an APP Committee felt essential. Visibility and connection were equally important, and I did this through handwritten notes to express appreciation to our members. At the end of the day, we were there to help others provide the best care possible to their patients. How do we do that? By offering amazing educational programs, publishing a journal with the best clinical papers, and investing in training programs that shape the future of GI.
I also didn’t realize how important it was for Congress to hear directly from us,
to understand what matters and why. During my year, they voted to eliminate surprise billing for colonoscopy, a win which reflected the power of advocacy. I reminded myself that I was only in this role for a year, and to remain humble and to do what I could to move the needle and have fun. That internal compass continues to guide me in my new role at Mayo Clinic as Chief Patient Experience Officer, where I work to understand the patients we serve by supporting the providers who care for them. It is very intertwined with the culture of safety, because if you don’t feel psychologically or physically safe coming to work, you can’t give the patient a good experience.
Dr. Burke: Authenticity, humility, and justice. While change can be inspired by the vision of a single person, it requires a team of people from varied backgrounds, expertise, and diverse opinions to provide honest feedback and the skillset to turn vision into reality to propagate durable change. Everyone’s voice is important, and justice, like authenticity, is about being open-minded to the assurance that we can provide the tools that everybody needs to be successful and feel valued in ACG. The College has been intentional about creating leadership development programs, research funding, [and] mentorship opportunities that help empower future leaders. I think curiosity is a key attribute of a leader. I am always curious about people, about what we do, and why things work or don’t. Curiosity drives growth.
Interestingly, it was never part of my plan to become the President of ACG. I’ve spoken to other women who have held this role in major GI societies, and they say the same. It was that we did a good job, we took good care, showed commitment, and over time, people noticed.
Dr. Oxentenko: When I was first nominated for this role, it wasn’t something I had envisioned for myself. I didn’t seek out the position, but I trusted that those who saw leadership potential in me felt I would carry that
into the presidency. As ACG President I remain true to who I am, but this role demands a level of responsibility, especially for women in GI, where we remain underrepresented in leadership roles. As a woman in leadership, I don’t just represent myself, but also the voices of other women and others who do not yet feel empowered to speak due to vulnerability or fear of retaliation. If I don’t speak up about something that allows all voices to be heard, then who will? I have always been mindful of how I deliver messages, especially those centered on diversity, equity, and inclusion. As I’ve come up in leadership in a maledominated society, I learned to read the room to understand how to address issues so more people will support important causes. This year is not about me, it’s about how you empower others—your committee chairs, governors, board members, and rising stars from emerging and advanced leaders. Our job is to prepare and lift up the next generation. I still remember my first ACG committee role was supported by Dr. Foxx-Orenstein, who nurtured my involvement in ACG. That opportunity opened a door that eventually led to where I am today. I am forever grateful.
In your view, how has the role and recognition of women in GI evolved over the course of your career, and what pivotal shifts still need to occur for true equity and inclusion to be realized?
Dr. Burke: I have seen substantial increases of women in GI and for that matter, many medical specialties. Now more than 50% of GI fellows are female. Over the last 10-15
years, GI fellowship programs and practices have devised systems to accommodate their colleagues having children and created environments that are more flexible, such as parttime [work], job sharing, and work from home. These changes are not only enticing women into a practice but are family-friendly (maternity and paternity leave). In 1993 when I joined the Cleveland Clinic, I was the second woman in our group and the first subspecialist at the Cleveland Clinic working part time at 50%. The administration and my chairman did not understand how someone could work part time and provide good care to patients. I proved them wrong and have never worked full time for the last 34 years in practice. I am constantly asked by GI group managers if I know any women interested in looking at their practice. Female patients more often seek health care, direct the health care for their family, and request female providers than male patients [do]. Especially when it comes to colonoscopy and more-sensitive aspects of GI disorders that women may feel more comfortable discussing with a female provider. As former Chair of the Women in GI Committee, I worked with a group of women who published the results of a cohort of GI trainees over a decade and showed the gender disparities in the first 10 years of practice.3 The financial disparity still exists, but women and most trainees are becoming savvier in their business negotiations and these days ‘Women
Do Ask.’ Maybe because I have given out many copies of Linda Babcock and Sara Laschever’s books, Women Don’t Ask: The High Cost of Avoiding Negotiation and Positive Strategies for Change and Ask for It: How Women Can Use Negotiation to Get What They Really Want. Remember that what you need in the first five years is not always what you need later. Overall, women have and continue to make strides. We need to uplift medical trainees and gastroenterologists from underrepresented communities to foster a stronger workforce and enhance quality of care for our patients.
Dr. Oxentenko: Over time, we’ve had to create the environment and culture to make women and underrepresented groups feel supported in GI. By reaching trainees in medical school and residency, they can see role models who look like them and feel empowered to pursue any specialty
they choose. GI has really evolved in this space, and we are much more open to conversations that reflect a broad range of experiences and perspectives. The current generation of trainees and early-career physicians are very different from those nearing retirement. Some of those differences come from changes we as a profession helped implement, such as duty-hour limits and wellness/burnout initiatives. So, when this new generation enters their first job seeking flexibility and separation of work and life outside of work, it’s not a lack of dedication but rather a product of the culture we helped shape. It’s important that we don’t see these generational differences as shortcomings, but instead recognize that a workplace culture aligned with these values will be key to retaining the next generation of gastroenterologists. I am very lucky to have trained and worked in an environment that is very supportive of my personal and professional goals,
including starting a family and having flexibility early in my career when my children were young.
Dr. Kane: I don’t know that the role of women in GI has changed, but what certainly has is the recognition of women. Historically, GI has been a procedure-driven field, which means being on call and managing unpredictable hours. Similar to other specialties such as cardiology, there has been a culture shift in the United States, especially around roles within marriages and partnerships. That shift has opened a greater opportunity for women to participate in a procedural specialty because they have a true partner at home. My medical school class was the first that was 50% women—this was considered quite the milestone in the late 1980s. While interviewing for internal medicine residency, I did not feel that there was
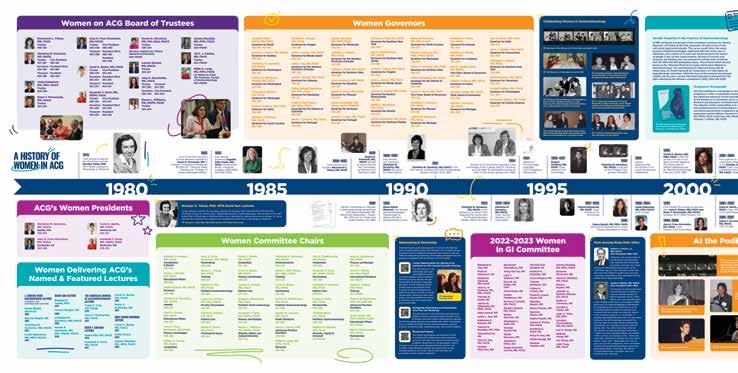
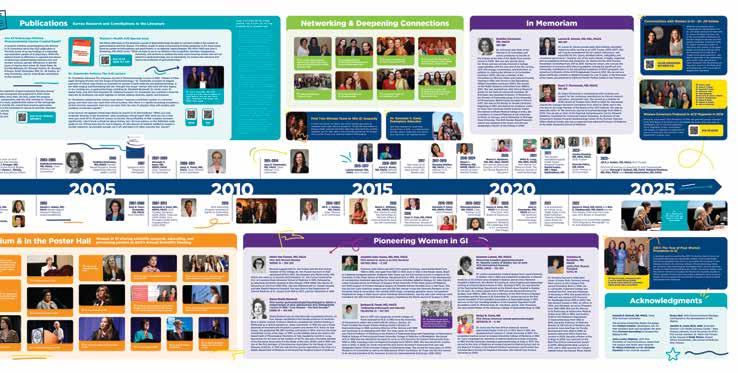
Celebrating Women in Gastroenterology Timeline
In 2023, the College marked the 30th anniversary of the ACG Women in GI Committee’s 1993-1994 transition from ad hoc to full committee status with a display, “Celebrating Women in Gastroenterology.” An archival project commemorating the founding of the committee and its many significant contributions to the life of the College and highlighting the role of women in gastroenterology and in ACG was presented at the Annual Scientific Meeting in Vancouver, BC, Canada. View a PDF of the ACG Women in Gastroenterology display at: bit.ly/acg-womens-history
any inequity or discrimination because of my sex. It was not until I went on interviews for GI did I realize how much some specialties of medicine were still very much a man’s world. I’ve always believed that women bring different and important skills to patient care. It is equally important as women in the field to serve as mentors and advisors, to champion and advocate for our qualified younger colleagues. The ACG also has a mentoring program, and I don’t think enough people take advantage of this [as mentors] and may not understand what can be gained from an enduring connection.
Dr. Foxx-Orenstein credited her initial interest in ACG to Dr. Zfass, who encouraged her to attend her first national meeting where she had the opportunity to meet the leadership of the Women in GI Committee right off the elevator. She reflects that, “it seemed to me, by that conversation, that this is an organization that really cares about the happenings of women in a profession that has otherwise not been very eyes-open to women.”
Dr. Surawicz: The role and recognition of women in medicine has greatly improved since my medical school
“...when this new generation enters their first job seeking flexibility and separation of work and life outside of work, it’s not a lack of dedication but rather a product of the culture we helped shape. It’s important that we don’t see these generational differences as shortcomings..." — Dr. Oxentenko
days at the University of Kentucky, where 10% of us were women (graduating class of 1973), but there is a long way still to go. We still fight bias, conscious and unconscious, institutional hurdles, and other obstacles. I urge you to listen to Dr. Oxentenko’s The American Journal of Gastroenterology Lecture at the 2021 ACG Annual Scientific Meeting.4 Later published, she sums it up better than I could today.
In a 2000 piece in The American Journal of Gastroenterology, Dr. Surawicz wrote: ...our [GI] societies need to be representative of our MD population. One of the benefits of specialty society membership is having a voice in making policy. Let’s encourage women to join the ACG, where they will reap the benefits of mutual support, development of leadership skills, ability to accomplish projects, and set policy on a rapid track, and learn new models for achievement and for meeting and becoming mentors.5
What philosophy or core value anchored your work as a mentor to emerging women leaders in GI, and how do you envision the next generation of women changing the future of this field?
Dr. Kane: If you think about it, although the first female ACG President wasn’t until Dr. Surawicz in 1998, in a relatively short period of time since then, there have been four incredible women who’ve been elevated to serve in the role. It took a long time, but the trajectory is positive, the bench is deep, and the future is extremely bright for women in GI. What we need to think about now is building the future of GI in a way that is agnostic of gender, sex, race, country of origin. If you are good, competent, thoughtful, kind, and humble, then you deserve a seat at the table. If you talk the talk and walk the walk, people will gravitate towards you.
“If you are true to your core values and consistent, then people will sponsor you for opportunities. If you don’t have a good reputation, you have nothing. It is important to communicate and advertise your core values. People want to have faith in their leader.” — Dr. Kane
If you are true to your core values and consistent, then people will sponsor you for opportunities. If you don’t have a good reputation, you have nothing. It is important to communicate and advertise your core values. People want to have faith in their leader. Even in fellowship, you’re already in a leadership position. It is your job to run the service, to be the leader who will manage difficult conversations, but know that there is always support. Nobody is without resources in a leadership role, and being an effective leader is knowing who you can turn to in your inner circle of advisors. That’s what’s so amazing about being an ACG President—there are very clear resources to help support us during the year to make the best decisions. Over my career, I have been so thrilled with how I have seen the number of women reflected in our classes of fellows and faculty, though we can still do better at the podium and in the highest leadership roles.
Dr. Burke: The core value that anchored my work as a mentor is sponsorship. Gastroenterology is a profession that
historically has been male-dominated. Over the last decade or so, the ranks of the profession have had the fortune to be joined by women and other traditionally underrepresented minorities. I believe that progress has been made by intentionality in supporting and sponsoring women in GI. In my opinion, women have arrived and are at the table. Our incredible female GI fellows are getting great jobs and negotiating strong contracts. Many female ACG members are becoming ACG fellows, leading ACG committees, serving as trustees, and furthermore institute heads and department chairs. I came into this field in an era when very few women were in GI. To a large degree, we had to figure things out on our own, develop strong connections through networking, and create or seize opportunities when available.
Moving forward our focus should continue to ensure a diverse workforce in gastroenterology and amplify others in our profession who still need to be empowered, emboldened, and supported. ACG, through its programming, has provided the scaffold to support a diverse community of providers in our field.
We cannot take our foot off the gas now, mentoring, coaching, allyship,
and sponsorship are key to our success. Both women and men must continue nominating, promoting, and championing one another—let’s give a platform to capable new voices!
The advice I want to give women is this: Give yourself permission to dream big, follow your dreams, and ask for what you want. Worst case scenario is you get a ‘no.’ For every door that closes, there is another one that opens. You can have the flexibility and authenticity to ask for what you want and go for it.
Dr. Oxentenko: I think we will continue to see more and more women entering GI. When we look at the percentage of women in GI fellowship programs, we are seeing growth, so the pipeline problem is going away—but we need to work to maintain it. When I look ahead, I would love to think that in 10-20 years, if currently 30% of our GI fellows are women, then that should be the representation of female GI leaders. To reach this goal, we can’t be complacent. I always challenge people to think about who they are sponsoring and supporting. For example, if a man reaches out to me to nominate them for an ACG award, I tell them I will consider nominating them if they consider nominating a woman or underrepresented individual for another award. If nothing else, it raises an awareness for that individual to be considerate of who they are nominating and how we are checking our biases. I have been proud of ACG because we are not losing sight of the work we need to do and continue to push forward.
Dr. Foxx-Orenstein: …one of [ACG’s] greatest strengths is its mission of working to enhance the practice of a clinical gastroenterologist with premier education and research opportunities. I represented a group which had not been represented on the podium much before. ACG utilizes the energy and the passion of the people that are in the College to move forward, to create ideas. It respects the members of the committees. It encourages all people to join committees and contribute to leadership different from
the other societies. When I came into the presidency, I had hoped to expose more women to the opportunity of the College, just like I felt Chris [Surawicz] had done for me, and [industry] was interested in supporting that goal. They initially provided financial support to develop a leadership program for women in gastroenterology, but I stepped back and said, ‘we should highlight [all] leaders everywhere.’ What we all hope for is that everyone should be equally recognized.
Dr. Surawicz: While work-life balance as a term has faded in favor of worklife integration, I still think of the helpful quote by mystery writer James Patterson, who wrote:
"Imagine life is a game in which you are juggling five balls. The balls are called work, family, health, friends, and integrity. And you’re keeping all of them in the air. But one day you finally come to understand that work is a rubber ball. If you drop it, it will bounce back. The other four balls... are made of glass. If you drop one of these, it will be irrevocably scuffed, nicked, perhaps even shattered."
So, some advice: It’s OK to not have a five-year or 10-year plan, but do find your helpful colleagues at work, especially one you can turn to when things go wrong; identify those who may be mentors or sponsors as well, especially peer mentors. Learn when to say ‘yes’ and how to say ‘no.’ Recognize that lack of control at work is a huge driver of burnout. Being a mentor has been a privilege, but I cannot take credit for those successes—everyone must take full credit themselves. Professional relationships have been a rewarding part of my career, and I am thankful for the ACG, which has enriched my professional life.
“So, some advice: It’s OK to not have a five-year or 10-year plan, but do find your helpful colleagues at work, especially one you can turn to when things go wrong; identify those who may be mentors or sponsors as well, especially peer mentors. Learn when to say ‘yes’ and how to say ‘no.’” — Dr. Surawicz
The Future is Bright for Women in GI
As I reflect on the stories and insights shared by these remarkable women, I’m reminded that leadership is not just about holding a title, it’s about creating space for others, challenging outdated norms, and leaving the door open wider than it was found. Each of these ACG Presidents forged a path through a landscape that wasn’t always welcoming, yet they led with integrity, vision, and a deep commitment to our field.
Common threads among these women include a shared dedication to uplifting and giving voice to underrecognized groups within the College, from APPs and underserved medical students to early-career professionals and women in GI. Rather than advancing personal agendas, they worked to meet the greatest needs of the College’s diverse membership.
Viewed through a female perspective, their leadership emphasized collaboration, inclusion, and camaraderie, values that guided the formation of new partnerships and innovative programs. While each brought her own unique voice and vision, all honored the history of women in GI and contributed a lasting legacy that continues to shape the future of our profession.
Notably, none of these women set out with the goal of becoming ACG President. Leadership, for them, was not a destination but a result of consistently showing up, doing
the work, and staying committed to the mission. Their rise to the highest office in the College came from a place of service, care, and excellence that others recognized and elevated.
We still have ground to cover, but because of their courage and example, the path forward is brighter and more inclusive. It is both a privilege and a responsibility to carry the torch they lit, to lead, to serve, and to ensure that every voice in GI is seen, heard, and valued.
A Message from Dr. Dunleavy I extend my deepest thanks to the women ACG Presidents for speaking with me and sharing their experiences with such candor and grace. I’m also grateful to the incredible ACG MAGAZINE team, who allowed me to transform the “Trainee Hub” to reflect more voices of the College. Having passed the Trainee Hub baton to Natalie J. Wilson, MD, GI Fellow at the University of North Carolina, and her Associate Editors, I know you are in good hands. I can’t wait to see how the team continues this work, beginning with this issue! Thank you to my predecessor, Shifa Umar, MD, who first envisioned this voice for trainees and had faith in me to continue her work. While my training has been enriched by many mentors and friends of the College, I extend heartfelt thanks to ACG for helping me find my home in GI
Dr. Dunleavy practices at the Massachusetts General Hospital’s Crohn's and Colitis Center, Boston, MA.
1. Oxentenko, Amy S. MD, FACP, FACG, AGAF. Women in Medicine: Honoring the Past and Bringing Women Further Into the Scope of Gastroenterology. The American Journal of Gastroenterology 118(2):p 188-192, February 2023. | DOI: 10.14309/ajg.0000000000002163.
2. Anderson J, Bilal M, Burke CA, et al. Burnout among US gastroenterologists and fellows in training: Identifying contributing factors and offering solutions J Clin Gastroenterol. 2022 Oct 26. doi: 10.1097/ MCG.0000000000001781. PMID: 36477385.
3. Singh A, Burke CA, Larive B, Sastri SV; Women in Gastroenterology Committee of American College of Gastroenterology. Do gender disparities persist in gastroenterology after 10 years of practice? Am J Gastroenterol. 2008 Jul;103(7):1589-95. and Burke CA, Sastri SV, Jacobsen G, Arlow FL, Karlstadt RG, Raymond P. Gender disparity in the practice of gastroenterology: the first 5 years of a career. Am J Gastroenterol. 2005 Feb;100(2):259-64.
4. The video of Dr. Oxentenko’s lecture, Hidden in Plain Sight: Bringing Women into the Scope of Gastroenterology, can be accessed at: education.gi.org/presentations/universe_16236.
5. Surawicz CM. Scopes, Hopes, and Learning the Ropes. Am J Gastroenterol 2000; 95: 345–348.
For those readers interested in learning more about these topics, please consider these articles and books, many of which were recommended by our past ACG Presidents.
PRESIDENTIAL LECTURES
• Surawicz CM. Scopes, hopes, and learning the ropes. Am J Gastroenterol. 2000 Feb;95(2):345-8. doi: 10.1111/ j.1572-0241.2000.01818. x. PMID: 10685734.
• Foxx-Orenstein AE. ACG Presidential Address. Major changes: rising to face the challenges and opportunities for clinical gastroenterology. Am J Gastroenterol. 2009 Jan;104(1):5-8. doi: 10.1038/ ajg.2008.135. PMID: 19098839.
• Burke CA. 2017 ACG Presidential Address: Challenges in the Practice of Gastroenterology: Engaging with ACG for Positive Impact. Am J Gastroenterol. 2018 Feb;113(2):157-160. doi: 10.1038/ ajg.2017.478. PMID: 29467536.
• Kane SV. “On Becoming a Successful Leader: An Amazing Journey or the Road to Nowhere?” Gi.org, 2017, universe.gi.org/vow/14998.htm. Accessed 17 July 2025.
• Oxentenko AS. “'Think Outside the Box:' ACG President Aims to Address Workforce of the Future.” Healio. com, 17 Feb. 2025, healio.com/news/ gastroenterology/20250212/thinkoutside-the-box-acg-president-aimsto-address-workforce-of-the-future. Accessed 17 July 2025.
GENDER DISPARITY
• Burke CA, Sastri SV, Jacobsen G, Arlow FL, Karlstadt RG, Raymond P. Gender disparity in the practice of gastroenterology: the first 5 years of a career. Am J Gastroenterol. 2005 Feb;100(2):259-64. doi: 10.1111/j.15720241.2005.41005. x. PMID: 15667479.
• Singh A, Burke CA, Larive B, Sastri SV; Women in Gastroenterology Committee of American College of Gastroenterology. Do gender disparities persist in gastroenterology after 10 years of practice? Am J Gastroenterol. 2008 Jul;103(7):1589-95. doi: 10.1111/ j.1572-0241.2008.01976. x. PMID: 18691187.
• Travis AC, Katz PO, Kane SV. Mentoring in gastroenterology. Am J Gastroenterol. 2010 May;105(5):970-2. doi: 10.1038/ ajg.2010.19. PMID: 20445505.
• Lok A, Burke CA, Crowe SE, Woods KL. Society Leadership and Diversity: Hail to the Women! Am J Gastroenterol. 2017 Sep;112(9):1353-1355. doi: 10.1038/ ajg.2017.261. Epub 2017 Aug 15. PMID: 28809385.
• Bilal M, Balzora S, Pochapin MB, Oxentenko AS. The Need for Allyship in Achieving Gender Equity in Gastroenterology. Am J Gastroenterol. 2021 Dec 1;116(12):2321-2323. doi: 10.14309/ajg.0000000000001508. PMID: 34665160.
• Jansson-Knodell CL, Bhavsar-Burke I, Gayam S, Kothari S, Oxentenko AS. Visibility of Women at the American College of Gastroenterology Annual Meetings Increasing Over Time. Am J Gastroenterol. 2021 Oct 1;116(10):2149-2151. doi: 10.14309/ ajg.0000000000001345. PMID: 34114569.
• Shaukat A, Oxentenko AS. The Time Is Now to Understand and Address SexRelated Disparities in Gastroenterology and Hepatology. Am J Gastroenterol. 2021 Mar 1;116(3):441-443. doi: 10.14309/ ajg.0000000000001185. PMID: 33657032.
• Pawa S, Banerjee P, Kothari S, D’Souza SL, Martindale SL, Gaidos JKJ, Oxentenko AS, Burke CA; Women in Gastroenterology Committee of the American College of Gastroenterology. Are All Endoscopy-Related Musculoskeletal Injuries Created Equal? Results of a National Gender-Based Survey. Am J Gastroenterol. 2021 Mar 1;116(3):530-538. doi: 10.14309/ ajg.0000000000001136. PMID: 33560650.
• Oxentenko AS. Women in Medicine: Honoring the Past and Bringing Women Further Into the Scope of Gastroenterology. Am J Gastroenterol. 2023 Feb 1;118(2):188-192. doi: 10.14309/ ajg.0000000000002163. Epub 2022 Sep 21. PMID: 36574283.
• Allan JM, Brooks AK, Crusto C, Feld LD, Oxentenko AS, Spector ND, VerduzcoGutierrez M, Silver JK. Five Strategies Leaders in Academic Medicine Can Implement Now to Enhance Gender Equity. J Med Internet Res. 2023 Jun 13;25:e47933. doi: 10.2196/47933. PMID: 37310782; PMCID: PMC10337456.
BURNOUT AND WELLNESS
• Surawicz CM. J. Edward Berk distinguished lecture: avoiding burnout: finding balance between work and everything else. Am J Gastroenterol. 2014 Apr;109(4):511-4. doi: 10.1038/ajg.2014.44. Epub 2014 Mar 18. PMID: 24642578.
• Anderson JC, Bilal M, Burke CA, Gaidos JK, Lopez R, Oxentenko AS, Surawicz CM. Burnout Among US Gastroenterologists and Fellows in Training: Identifying Contributing Factors and Offering Solutions. J Clin Gastroenterol. 2023 Nov-Dec 01;57(10):1063-1069. doi: 10.1097/ MCG.0000000000001781. Epub 2022 Oct 26. PMID: 36477385.
• Lacy BE, Cangemi DJ, Burke CA. Burnout in Gastrointestinal Providers. Am J Gastroenterol. 2024 Feb 16. doi: 10.14309/ajg.0000000000002663. Epub ahead of print. PMID: 38235758.
NEGOTIATION
• Babcock L, Laschever S. Women Don’t Ask: The High Cost of Avoiding Negotiation—and Positive Steps for Change. New York: Bantam Books; 2007.
• Babcock L, Laschever S. Ask for It: How Women Can Use the Power of Negotiation to Get What They Really Want. New York: Bantam Dell; 2009.
PARENTAL LEAVE
• Riely CA, Jagiella V, Michaletz-Onody P, Roseman S, Schuman B, Surawicz C, Karlstadt R. Parental leave for trainees in gastroenterology. The Ad Hoc Committee for Women in Gastroenterology, The American College of Gastroenterology. Am J Gastroenterol. 1992 Oct;87(10):1368-71. PMID: 1415089.
• Feld LD, Oxentenko AS, Sears D, Charabaty A, Rabinowitz LG, Silver JK. Parental Leave and Return-toWork Policies: A Practical Model for Implementation in Gastroenterology. Clin Gastroenterol Hepatol. 2023 Oct;21(11):2709-2715. doi: 10.1016/j. cgh.2023.07.001. PMID: 37741653.
• Ali S, Chowdhury R, Bittner K, Oxentenko AS, Kothari S. Assessing Family Leave Policies and Pregnancy Outcomes Among Gastroenterologists: A Survey of Physicians in the American College of Gastroenterology. Am J Gastroenterol. 2023 Dec 1;118(12):2294-2300. doi: 10.14309/ ajg.0000000000002408. Epub 2023 Jul 19. PMID: 37463424.
TRAINEE HUB
The First-Year GI Fellow Handbook:
Lessons for Thriving (Not Just Surviving)
STARTING GASTROENTEROLOGY
FELLOWSHIP IS ONE OF THE MOST EXCITING—AND DAUNTING—CHAPTERS in a young physician’s journey. You’re no longer the general medicine resident; you’re the GI fellow, the "scope doctor." Everyone else expects you to know everything about gastroenterology on day one. The learning curve is steep, the responsibility is heavy, and the opportunities are endless. While every fellowship and institution is unique, there are universal challenges and lessons that all first-year GI fellows encounter. This handbook aims to distill practical pearls, mindset shifts, and survival strategies so you can not only get through the year, but grow, enjoy, and thrive.
Clive J. Miranda, DO, MSc, Creighton University School of Medicine, Omaha, NE
Mastering the Scope: The Art, Not the Race
One of the most transformative aspects of GI fellowship is developing your endoscopy skills. It’s important to remember—it’s not a race to the cecum.
Take your time during procedures. Understand why a finding is positive and equally why something might be negative. Learn to appreciate the nuances rather than rushing to finish.
Ergonomics matter more than you think. Early on, poor posture and awkward scope-handling can lead to aches in your fingers, forearms, shoulders, and even your back. Don’t ignore these small pains—they can become serious over time. Invest in good positioning habits from day one. Expect soreness, however; scoping is a new motor skill. Stress balls and occasional hand massages help, and the discomfort will fade as muscle memory develops.
Celebrate milestones—your first cecal intubation, your first polypectomy, your first variceal banding. These small victories boost confidence and remind you of your progress.
Above all, trust the process. Over time, you’ll learn the artistry of scoping, and one day, it will feel as natural as tying your shoes.
Build Smart, Sustainable Work and Study Habits
Fellowship is busy. Between consultations, scopes, clinics, and calls, studying often gets pushed to the back burner. But the knowledge base you build now forms the foundation for your future independent practice. Instead of cramming, study a little each day—even if it’s just one page or one question. Small, consistent efforts add up over the year. Use two to three solid resources along with a question bank rather than spreading yourself too thin. Some favorite resources among fellows include ACG’s Guide to the Guidelines, Gastroenterology
Clinical Focus, Liver Fellow Network, Practical Gastrointestinal Endoscopy, and Sleisenger and Fordtran’s Gastrointestinal and Liver Disease. The
ACG Postgraduate Course Self-Assessment
Test Questions are a top-rated question bank among fellows.
Set short-term, realistic goals. Rather than saying “I’ll read the entire guideline on IBD this month,” try “20 practice questions a week” or “one review article per month.” These achievable targets keep you motivated and accountable.
Consider pre-writing your clinic notes or scope H&Ps the night before. This makes the following day smoother and frees up mental energy for unexpected challenges. When possible, aim to finish tasks in one sitting. Dragging out notes or consult plans over several days only builds mental clutter.
Consults and Difficult People: Responding with Poise
One of the earliest lessons in fellowship is learning to handle the influx of consults, many of which may seem nonsensical or trivial. Remember—you’re at a teaching hospital. Primary teams often seek your help out of concern for the patient, not to annoy you. Rather than meeting these consults with frustration, use them as opportunities to educate residents and medical students. Being the fellow known for patience and teaching elevates your reputation and fosters better interdepartmental relationships.
You’ll encounter difficult personalities— ranging from pushy surgeons to anxious family members. Stay calm, be aware of your body language, and maintain a composed tone. Your demeanor reflects not just on you but on your entire division and program.
Stand firm in your medical opinions while remaining respectful. It’s okay to disagree with a proposed plan, but always approach discussions with curiosity and politeness rather than confrontation. Lastly, know your institution’s policies for addressing abusive or threatening behavior. You’re never alone—lean on your co-fellows and faculty when situations get tough.
Embrace the Field: Dive In and Network GI is an incredibly dynamic and welcoming specialty. Immersing yourself early will exponentially enrich your experience. Attend conferences such as ACG, DDW, AASLD, AIBD, and more. Apply to society-led courses like the ASGE
First-Year Fellows Course. These are prime opportunities to network with mentors, find research collaborators, and connect with like-minded peers. Consider joining society committees or interest groups. These roles expose you to leadership, advocacy, and community building within GI. They’re also fantastic platforms to advance your career and strengthen your CV. Personal branding isn’t just for influencers. Build your presence on platforms like Twitter/X or Instagram. Share educational pearls, reflections, and case discussions. You’ll develop communication skills, find mentors, and inspire others. Engage in research early—even if it’s just case reports or poster presentations. You don’t have to do everything at once. Pick projects that genuinely interest you and align with your future goals.
Adjusting to a New City: Embrace the Adventure Many fellows relocate for training, which brings both excitement and loneliness. Approach this as an adventure rather than a challenge. Follow local Instagram or TikTok accounts that highlight events, restaurants, and activities. Use apps like Meetup to find groups with similar interests. Visit public spaces—coffee shops, gyms, parks—to meet new people naturally.
Connect with your co-fellows and residents. Plan dinners, group outings, or attend local sports games together. Building a social network outside the hospital eases the transition and helps you fall in love with your new city. As the commonly used phrase goes, “It’s the people who make the place.” The more you explore and connect, the more quickly you’ll feel at home.
Night Call: Embrace the Chaos Night call is when everything feels magnified. Emergencies become your responsibility, and decisions carry weight. When in doubt, see the patient. No one will fault you for being overly cautious early on.
Familiarize yourself with common GI emergencies like variceal bleeding,
food impaction, cholangitis, and acute liver failure. Know your hospital’s protocols, have all important numbers saved, and understand how to set up endoscopy carts. Learn to triage consults efficiently. Notify your attending early about critical patients—communication is key to a smooth night. Build good relationships with on-call residents. Working as a team makes long nights much more bearable. And remember—every call shift eventually ends, no matter how rough.
Protect Your Wellbeing:
More Than Medicine Fellowship demands can easily overshadow your personal wellbeing. Protecting your health and happiness isn’t a luxury—it’s essential for sustainability and compassionate care. Prioritize fitness, nutrition, and sleep. Regular workouts and healthy meals keep your mind sharp and energy levels high.
Make time for hobbies, whether that’s playing an instrument, hiking, painting, or traveling. Staying connected to your passions prevents burnout and keeps your identity grounded beyond your professional role. Your support system—family, close friends, partners—deserves your attention too. Set aside dedicated time to nurture those relationships. In addition, start reflecting early on about what you want in a future job—practice type, lifestyle, research opportunities, and location. This foresight helps shape your fellowship
experience and long-term happiness. GI fellowship is as much about professional growth as it is about personal evolution. You’ll struggle, succeed, question yourself, and surprise yourself (often all in the same day). Trust that every difficult moment builds your resilience. Celebrate each small victory. Be kind to yourself and to those around you. Remember—it’s a privilege to be in this field and to care for patients in their most vulnerable moments. Enjoy the ride—scope by scope, consult by consult, day by day. You’ve got this!
TESTIMONIALS
“It’s easy to feel like you’re falling behind when you haven’t cracked open a book in weeks. Choose one solid resource per topic, protect small chunks of study time, and focus on quality over quantity.” —Hisham Wehbe, MD, Cleveland Clinic Foundation
“Learning the system early— knowing who to call, workflows, and resources—saves time and stress.” Talia Malik, MD, Medical College of Wisconsin
“Asking for help isn’t a weakness. Fellowship exists because we don’t know everything yet.” —Lauren Loeb, MD, Mayo Clinic Florida
“Build your professional identity through reliability, preparedness, and kindness. Your reputation starts on day one.” —Arjun Chatterjee, MD, Cleveland Clinic Foundation
“Celebrate milestones big and small, but resist comparing progress to your co-fellows. Everyone’s journey is unique.” —Luis Nieto, MD, Emory University School of Medicine
For a comprehensive list of resources for GI fellows, see @CarlKayMD’s “Useful Resources for GI Fellows" guide at cdn.me-qr.com/pdf/14096184.pdf or scan the QR code.
Dr. Clive Miranda is a GI fellow at Creighton University Medical Center in Omaha, NE. He currently serves on ACG’s Diversity, Equity, and Inclusion Committee and as a Social Media Ambassador for Evidence-Based GI
Sponsored by AbbVie
Telehealth IBD Psychotherapy Groups
A pilot program for patients with Crohn’s disease or ulcerative colitis
Do you have IBD patients in need of support from a gut-brain behavioral health professional? A telehealth psychotherapy group could be the right choice for them.
This program incorporates scientifically supported treatments designed to reduce stress, anxiety, inflammation, and flare frequency in people with Crohn’s disease or ulcerative colitis.
Treatments include:
• Cognitive behavioral therapy (CBT)
• Gut-directed hypnotherapy
Sessions are o ered for 75 minutes weekly for a total of eight weeks. Participants must be 18 years or older with a diagnosis of Crohn’s disease or ulcerative colitis (IBD), and access to a stable internet connection.
Conducted in partnership with
For more information about this program, including the group style, fees, and schedule, scan the code or visit gipsychology.com/ccf
GETTING IT Artificial Intelligence and the Standard of Care
By Ann Bittinger, Esq. LAW MIND
“DO PHYSICIANS RISK MALPRACTICE IF THEY USE CHATGPT?” I typed into the ChatGPT search box.
“Yes,” appeared after I hit enter. (At least AI is humble.)
As AI—short for Augmented Intelligence or Artificial Intelligence—has become ubiquitous, gastroenterologists face that simple question: am I at risk if I utilize this commonplace tool?
It’s often helpful to address complex situations with simple questions and simple answers: To be found liable for malpractice, a physician has to violate the standard of care.
WHAT IS THE STANDARD OF CARE?
The standard of care can be thought of as actions that are widely adopted; most of your peers do the same thing. It’s what a reasonably prudent and competent physician with similar resources and training would do in the situation.
The patient has to show that the physician violated the physician’s duty of care to the patient. That violation is often established by demonstrated deviation from the standard of care. If AI suggests that a physician does something outside the standard of care, and the physician relies on that, then the physician can be found liable for malpractice.
The plethora of information that goes into establishing AI’s knowledge base is massive. Yet AI is first to admit that its tools can generate what they call “hallucinations”—plausible but inaccurate responses.
The key to your risk assessment in using AI in your clinical practice is whether many of your peers are doing the same thing in using AI and how you are incorporating what you find into your clinical decision making.
In the gymnastics of a medical malpractice lawsuit, attorneys present their positions on the standard of care, most frequently by use of experts. In determining if AI equipment or tools are within the standard of care, look at who is using them, what research and publications have been shared on them, and who is writing those publications. Like animals in a safari, it’s best to move as a group.
Physicians must maintain independent clinical judgment. They can use AI as a supplement, not a substitute, for medical decision making.
DOCUMENTATION IS DEFENSIVE
Always document how medical decisions are made. If you use AI to help guide you to sources that help you make the decisions, document those sources and data points rather than relying solely on AI.
I cannot find any reported malpractice case against a physician for use of AI. (Even ChatGPT says there is no “notable” malpractice case
with AI.) So what’s the real risk? And what can an individual gastroenterologist use AI for?
First, never, ever enter PHI into any AI search. Doing so violates HIPAA, as an unauthorized release. Even if you don’t email or download anything, if you give identifiable health information in an AI search box, you made a disclosure in violation of HIPAA. Any information plugged in to an AI search must be deidentified within the meaning of HIPAA.
WHAT CAN YOU USE AI FOR?
Diagnosis. AI will emerge in diagnosis more in the form of specific equipment and tools that have AI tailored to specific uses. These are much different than opening something like ChatGPT on your PC and typing in some symptoms and a question. The FDA has approved more than 500 autonomous diagnosis machines for radiology, cardiology, and neurology. Those devices are very different from typical mass-available options like ChatGPT. Remember that what goes in must come out. Industry- and specialtyspecific, tailored databases designed with the input of gastroenterology experts will be the most reliable.
In gastroenterology in particular, you are seeing AI in endoscopy, particularly in polyp detection and characterization. The key here is that these are AI-powered tools used to help identify and classify polyps. They are tools that provide suggestions, not machines that provide diagnosis. It’s a difference with a very important distinguishing factor: documentation of medical decision making. The algorithms may produce results that take your
KEY TAKEAWAYS
1. To date, there are no reported malpractice cases due to physicians using AI.
2. Malpractice requires a breach of the standard of care.
3. There are no AI/gastroenterology standards established now.
4. AI may most safely take the form of features in new devices as opposed to a physician plugging in scenarios to ChatGPT.
breath away in terms of accuracy and swiftness, but you must be able to document the findings and your independent medical decision making. A good AI tool will tell you not only what it suggests, but the implications of that suggestion and the basis on which that finding was suggested.
WHAT IS MY HOSPITAL USING?
Physicians should be aware of AI at use in hospitals where they work. If you walk into a surgical suite, you should know if a piece of equipment there is operating based on an algorithm. Hospitals may try to save staffing costs by automating patientfacing processes with AI, without the consent, never mind the knowledge, of the surgeons.
AI’s use in scanning massive amounts of patient data to identify risks and establish patterns and protocols on a large scale has been in existence in less-sophisticated forms for a decade or two. AI’s use in developing generic treatment plans and organizing them in a way to communicate with patients and other providers is useful and perhaps less risky if used as a starting point to be individually tailored.
JUST HOW UBIQUITOUS IS AI?
According to a recent survey by the American Medical Association, 66% of physicians surveyed in 2024 indicated they currently use AI in their practice, up significantly from 38% in 2023. They said the top area of opportunity for AI was “addressing administrative burden through automation.”
“…I know that AI is not going to replace doctors—but doctors who use AI will replace those who don’t,” the AMA quoted Jesse M. Ehrenfeld, MD, MPH, as saying.
Ann M. Bittinger, Esq., is a healthcare attorney with The Bittinger Law Firm and can be reached at ann@bittingerlaw.com
Inside the JOURNALS
PATIENT-CENTERED OUTCOMES
THE RED JOURNAL RECENTLY PUBLISHED THREE ACG CLINICAL GUIDELINES FOR IBD, providing key updates to reflect the surge of IBD therapies and management strategies that have emerged. The guidelines include expanded treatment options for induction of remission and maintenance therapy, as well as vaccine and health screening schedules for patients with IBD. A study by Pathipati, et al., in Clinical & Translational Gastroenterology examines the effect of a low-FODMAP diet on exhaled hydrogen and methane levels using at-home breath testing and meal and GI symptom tracking via an app. ACGCRJ shares a recent editorial by current and former Editorial Board members with helpful tips on getting published in the journal.
ACG CLINICAL GUIDELINE : Ulcerative Colitis in Adults
Rubin, et al.
This guideline update includes nine new FDA-approved therapies as well as updated recommendations for the positioning and sequencing of drug regimens, with two GRADE recommendations based on head-to-head trials. Two phenotypes were added to the guideline, distal colitis with a cecal patch and colitis associated with primary sclerosing cholangitis. Also new is the use of intestinal ultrasound to assess disease activity and response to therapy. The authors note that all medical options should be available based on physician recommendations and they do not support forced step therapy.
READ: bit.ly/acg-uc-2025
LISTEN: bit.ly/acg-uc-2025-podcast
SUMMARY: bit.ly/acg-uc-2025-highlights
ACG CLINICAL GUIDELINE: Management of Crohn’s Disease in Adults
Lichtenstein, et al
Notable updates to the Crohn’s disease guideline include recommended use of IL-23 inhibitors (i.e., mirikizumab, guselkumab, and risankizumab) for induction and maintenance of remission in patients with moderately to severely active Crohn’s disease. The guideline also recommends against use of azathioprine (at 1.5-2.5 mg/kg/day) or 6-mercaptopurine (at 0.75-1.5 mg/kg/day) to induce remission, instead noting their effectiveness as maintenance therapy, and against requiring failure of conventional treatment such as an immunomodulator before starting advanced therapy in patients with severely active disease.
READ: bit.ly/acg-crohns-2025
LISTEN: bit.ly/acg-crohns-2025-podcast
SUMMARY: bit.ly/acg-crohns-2025-highlights
ACG CLINICAL GUIDELINE: Preventive Care in Inflammatory Bowel Disease
Farraye, et al
The guideline on preventive care in IBD addresses vaccines, cancer screenings, bone health, and smoking cessation. Since the last update in 2017, new vaccines have been approved and age recommendations for the administration of pre-existing vaccines have been updated, and the new guideline reflects these changes. The authors also emphasize the significant role of the gastroenterologist in patients with IBD, with patients often viewing them as their primary care provider, particularly among younger patients. They highlight the value of a coordinated care approach and educating patients on the importance of vaccines and other preventive health measures.
READ: bit.ly/acg-ibd-preventive-2025
LISTEN: bit.ly/acg-ibd-preventive-podcast
SUMMARY: bit.ly/acg-ibd-preventive-highlights
[CLINICAL & TRANSLATIONAL GASTROENTEROLOGY]
Impact of Short Duration FODMAP Restriction on Breath Gases and Gastrointestinal Symptoms
Pathipati, et al
In this study, the authors aimed to better understand the accumulation of luminal gases following ingestion of fermentable carbohydrates (i.e. FODMAPs) and assess the effect of a low-FODMAP diet on hydrogen (H2) and methane (CH4) levels via breath testing. The study group consisted of 1,984 adults with active GI symptoms and were self-selected, without the requirement for a formal diagnosis of IBS or other GI conditions. After establishing a “baseline” week on their usual diet, they implemented a one-week lowFODMAP diet “reset.” Participants monitored breath H2 and CH4 levels using an at-home breath analysis device and recorded symptoms and meals in real time using the associated app. The study found that breath H2, CH4, and GI symptoms (such as bloating, abdominal pain, and flatulence) were significantly reduced following FODMAP restriction, suggesting that breath H2 and CH4 may be influenced by shortterm dietary changes and could be a useful biomarker of response to FODMAP restriction.
READ: bit.ly/ctg-fodmap-breath
[ACG CASE REPORTS JOURNAL]
Cracking the Code: A Practical Guide to Publishing in the ACGCaseReportsJournal
Himesh B. Zaver, MD; Daniyal Abbas, MD; Prateek S. Harne, MBBS, MD
This editorial provides a helpful resource to those interested in publishing cases in ACGCRJ The authors provide tips and best practices for crafting a strong case; clear, concise academic writing; high-quality figures and tables; navigating roles, responsibilities, and expectations with coauthors and mentors; and responding to reviewer comments.
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH
PATIENT GROUP INTERVAL
• PCV 20 or PCV 21 Vaccinations
If PCV naïve: PCV 21 or PCV 20
• H. pylori prevalence in North America is 30%-40%
19-49 years (immunocompromised)
• Typically acquired in childhood
PCV 21 or PCV 20
When to Test for H. pylori
If incomplete PCV: PCV 13 ≥1 y PCV 21 or PCV 20
If PCV naïve: PCV 21 or PCV 20
• More prevalent among non-White races or ethnicities, those living in crowded or poor sanitary conditions, and early generation immigrants from endemic regions.
50-64 years
≥65 years
Zoster ≥19 years
If incomplete PCV: PCV 13 + PPSV23 ≥5 y PCV 21 or PCV 20
Benign Conditions
• Dyspepsia if <60 years without alarm features (GI bleeding, vomiting, unexplained weight loss, iron deficiency)
COVID-19
• Dyspepsia if <50 years with high risk for gastric cancer
All adults
Rotavirus vaccine Infants exposed to biologics in-utero
• Endoscopy with biopsies if dyspepsia and alarm features, NSAID use, family history of gastric cancer, immigration from high incidence region
Influenza
Treatment for H. pylori
Maintenance
Abx = antibiotic
b.i.d. = twice a day
Examples of completed pneumonia vaccine regimens:
• PCV 13 and 2 doses of PPSV 23
• PCV 15 and PPSV 23
Premalignant and Malignant Conditions
If PCV naïve: PCV 21 or PCV 20
• Adult household members of H. pylori positive individuals
If incomplete PCV: ≥ 5 yrs since last PCV PCV 21 or PCV 20
Screen for depression and anxiety at baseline and annually. Refer for counseling/therapy.
6-MP = 6-mercaptopurine
HAV = hepatitis A virus
HPV = human papillomavirus
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH The American Journal of Gastroenterology 119(9):p 1730-1753, September 2024. | DOI: 10.14309/ ajg.0000000000002968
IBD= inflammatory bowel disease
JAK = janus kinase
NMSC = non-melanoma squamous cell cancer
PCV = pneumococcal conjugate vaccine
PPSV = pneumococcal polysaccharid vaccine
RSV= respiratory syncytial virus
S1P = sphingosine-1-phosphate
TDAP = tetanus, diptheria, and pertussis
TNF = tumor necrosis factor
Francis A. Farraye, MD, MSc, MACG; Gil Y. Melmed, MD, MPH, FACG; Gary R. Lichtenstein, MD, FACG; Edward Barnes, MD, MPH, FACG; Berkeley N. Limketkai, MD, PhD, FACG; Freddy Caldera, DO, PhD, FACG; Sunanda Kane, MD, MSPH, MACG The American Journal of Gastroenterology
DOI: 10.14309/ajg.0000000000003541
READ THE GUIDELINE: bit.ly/acg-ibd-preventive-2025
Concept and Content: Erica Duh, MD | Reviewers: William D. Chey, MD, FACG and Shailja C. Shah, MD, MPH
ACG GUIDELINE Highlights
Treatment of Helicobacter pylori Infection
Management of Crohn’s Disease in Adults
Concept and Content: Erica Duh, MD | Reviewer: Christina Y. Ha, MD, FACG
Diagnosis
Epidemiology
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH
Concept and Content: Erica Duh, MD | Reviewers: William D. Chey, MD, FACG and Shailja C. Shah, MD, MPH
• Consider clinical presentation as well as endoscopic, radiologic, histologic, and pathologic findings.
• Fecal calprotectin to differentiate inflammatory from noninflammatory (cutoff >50-100 ug/g)
• H. pylori prevalence in North America is 30%-40%
• Typically acquired in childhood
• Routine endoscopic surveillance for CRC is recommended for colonic CD Medical Management
When to Test for H. pylori
• More prevalent among non-White races or ethnicities, those living in crowded or poor sanitary conditions, and early generation immigrants from endemic regions.
The following are recommended:
Benign Conditions
• Infliximab
• Adalimumab
• Dyspepsia if <60 years without alarm features (GI bleeding, vomiting, unexplained weight loss, iron deficiency)
• Antibiotics
• Upadacitinib
• Adult household members of H. pylori positive individuals
• ITP
Premalignant and Malignant Conditions
• Vedolizumab
Treatment for H.
• Dyspepsia if <50 years with high risk for gastric cancer
• Ustekinumab Surgical and Postoperative Crohn’s Disease
• Unexplained IDA
• Recommend 6-12 month post-op colonoscopy to assess for early recurrent CD
• Current or prior history of PUD
• High risk gastric premalignant condition
- Atrophy, intestinal metaplasia, dysplasia
- Autoimmune gastritis
• MALT lymphoma
• Gastric epithelial polyps WHO recognizes H. pylori as a group I (definite) carcinogen
• Endoscopy with biopsies if dyspepsia and alarm features, NSAID use, family history of gastric cancer, immigration from high incidence region
• CD patients at high-risk for post-operative recurrence should consider starting advanced therapy shortly after resection.
• Chronically taking NSAID or starting daily aspirin therapies
- Family history of gastric cancer
- Foreign born with immigration from high incidence region
When to Refer to Surgery
- High risk race or ethnicity
• Intra-abdominal abscess >2 cm should be treated with drainage and antibiotics
• PPI b.i.d.
• Patients with symptomatic fibrostenotic strictures or abdominal abscesses should be considered for surgery Medical Management
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH The American Journal of Gastroenterology 119(9):p 1730-1753, September 2024. | DOI: 10.14309/ ajg.0000000000002968
Use limited to anti-TNF-experienced patients in the US.
Gary R. Lichtenstein, MD, FACG; Edward V. Loftus, MD, FACG; Anita Afzali, MD, MPH, MHCM, FACG; Millie D. Long, MD, MPH, FACG; Edward L. Barnes, MD, MPH, FACG; Kim L. Isaacs, MD, PhD, MACG; Christina Y. Ha, MD, FACG The American Journal of Gastroenterology
10.14309/ajg.0000000000003465
EARLY initiation of advanced therapy is KEY for optimal outcomes in CD