Poor oral and systemic health: the sugar link theory
ORAL MEDICINE, ORAL DIAGNOSIS, ORAL PATHOLOGY
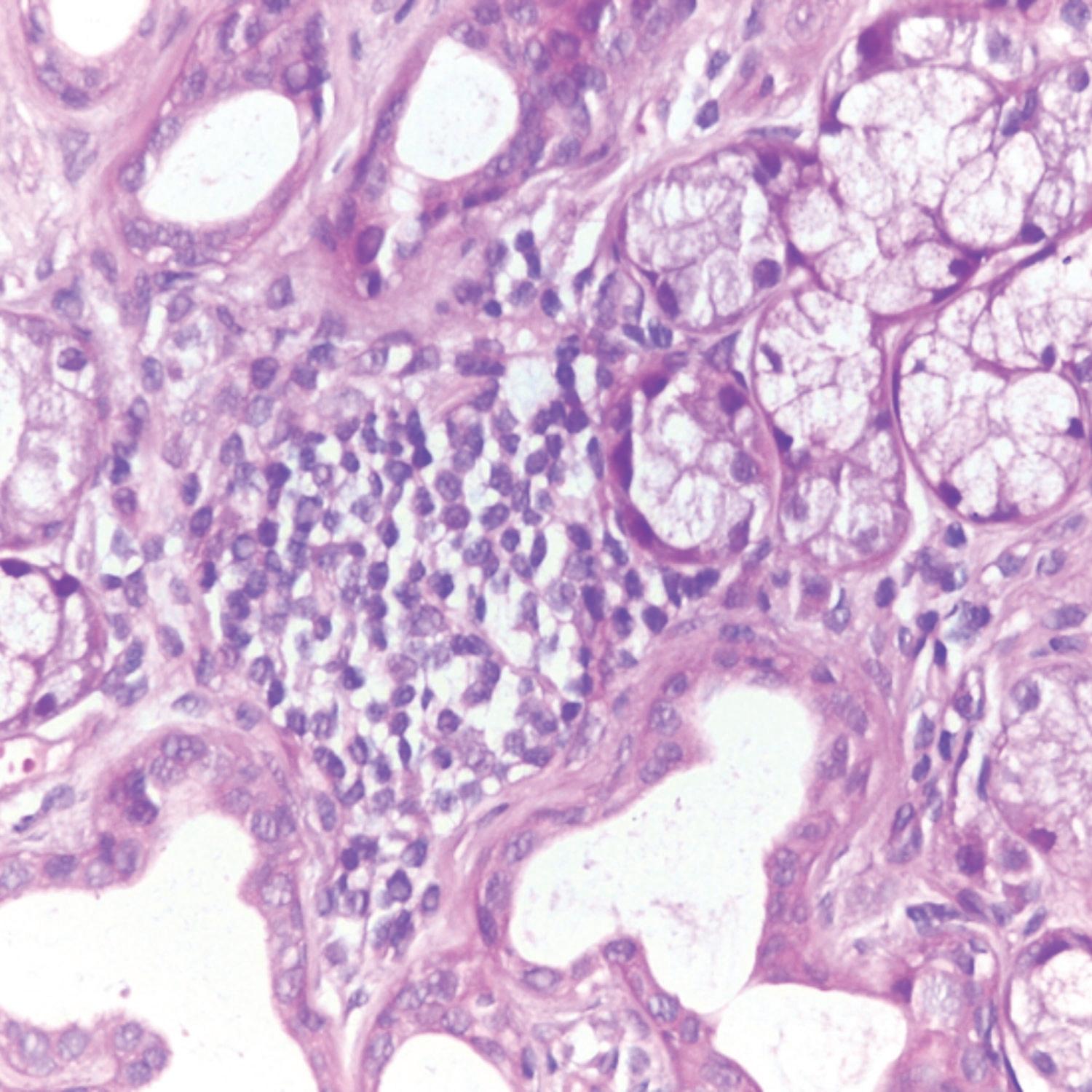
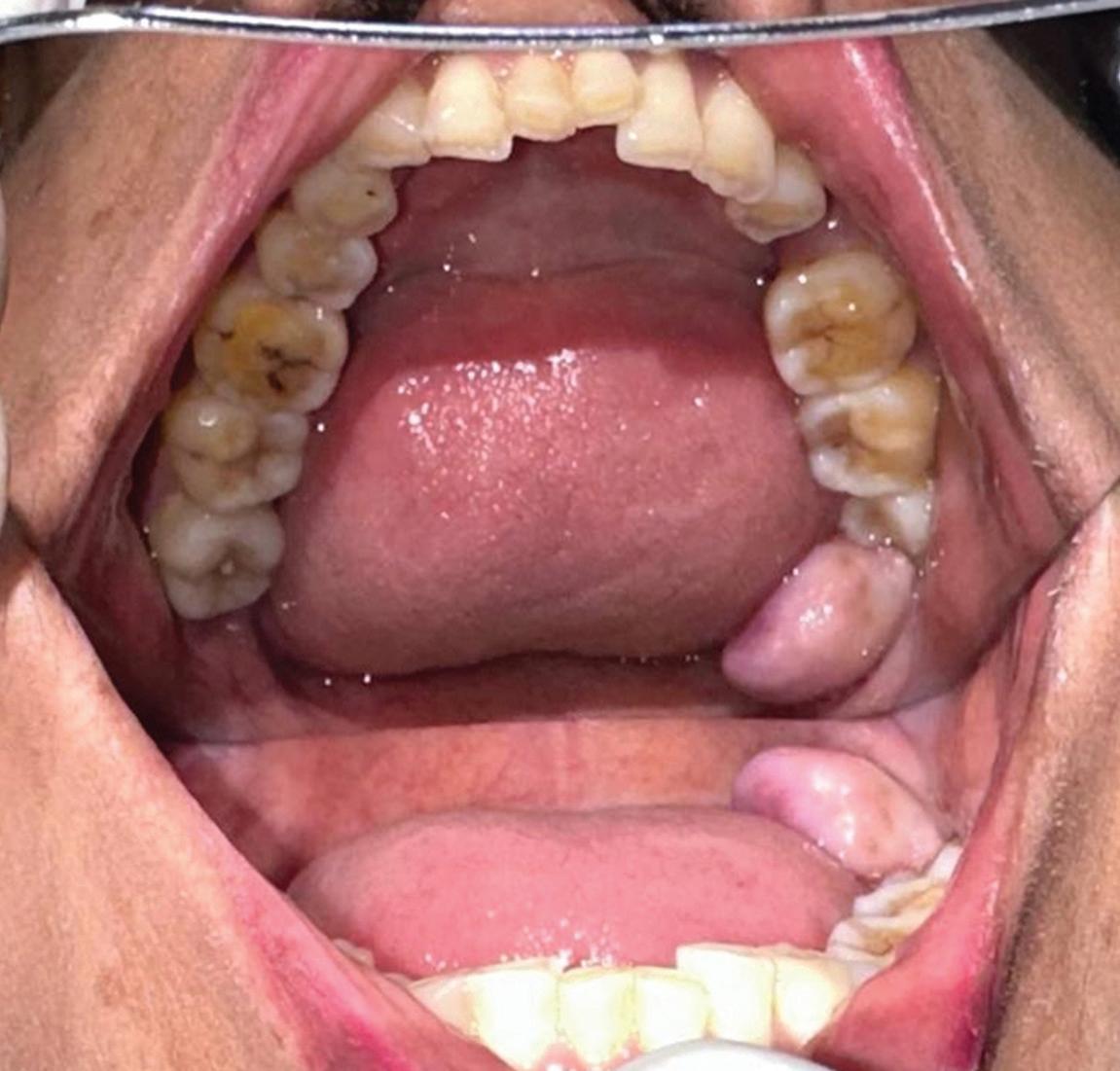
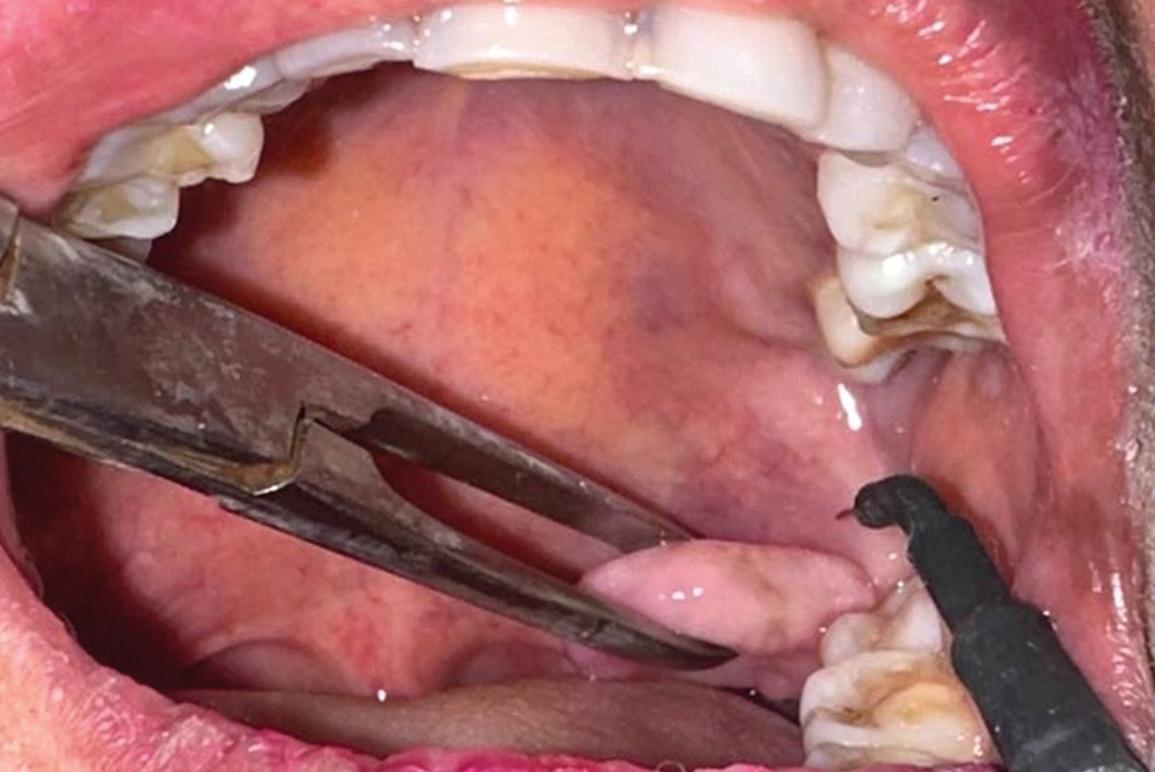
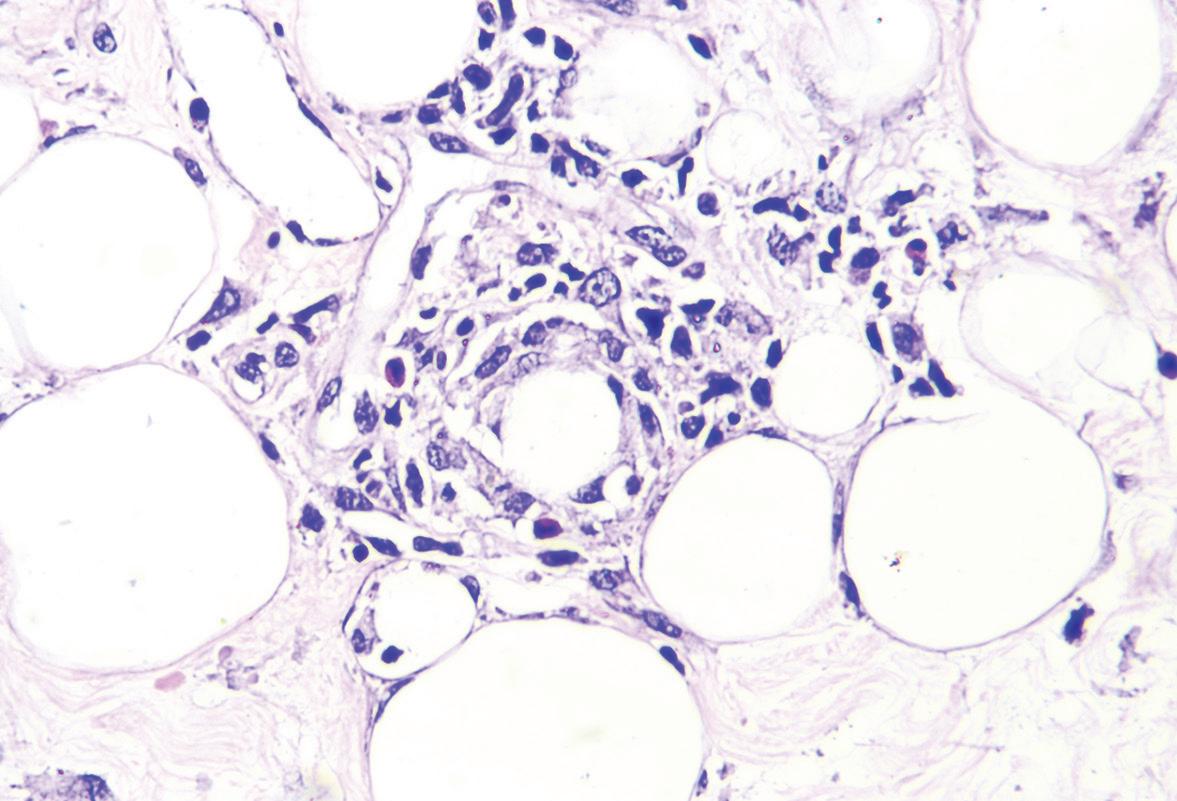
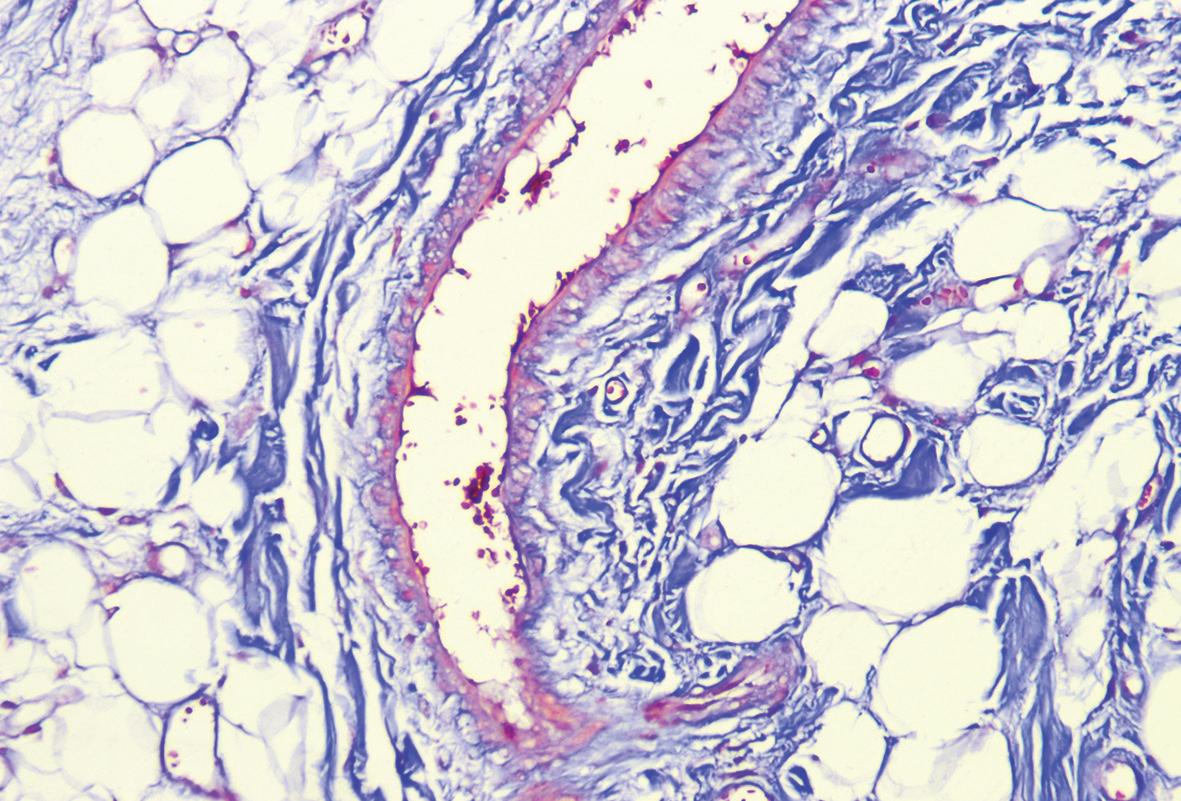
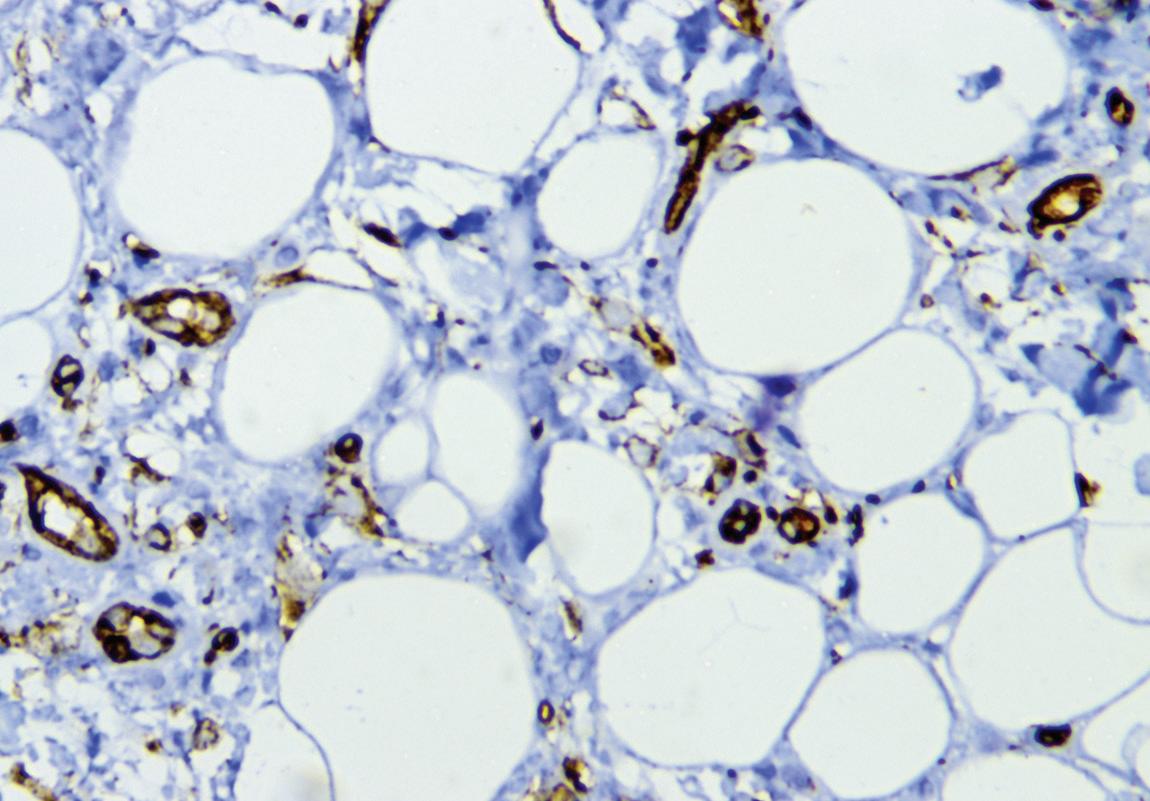
Rare angiofibrolipoma of the oral cavity
PHARMACOLOGY
Analgesic drug mechanisms of action
Deepening Your Knowledge
Experience a comprehensive selection of lecture courses designed to elevate your dental expertise.
Enhancing Your Career
Students and new dentists can take advantage of a range of resources designed to support early career growth.
Sharpening Your Skills
Explore hands-on participation courses that provide practical experience to refine your techniques.
Expanding Your Network
Take advantage of multiple networking opportunities to connect with peers, mentors and industry experts.
DEPARTMENTS
5 Editorial Stronger together
6 Implants
Tooth replacement from extraction to restoration.
2. Implant planning and placement
13 Pharmacology
Understanding analgesic drug mechanisms of action to aid in postoperative dental pain management
78 Oral Diagnosis
Circular radiolucency and Generalized rarefactions
79
Self-Instruction Answers
Exercises No. GD527, GD528, and GD529
CLINICAL ARTICLES
20 Fixed Prosthodontics
Surgical and prosthetic criteria for selecting prefabricated vs custom implant abutments
Gary Greenstein Sultan Albeshri
Ahmad Majeed-Saidan
SELF-INSTRUCTION EXERCISE
28 Restorative Dentistry
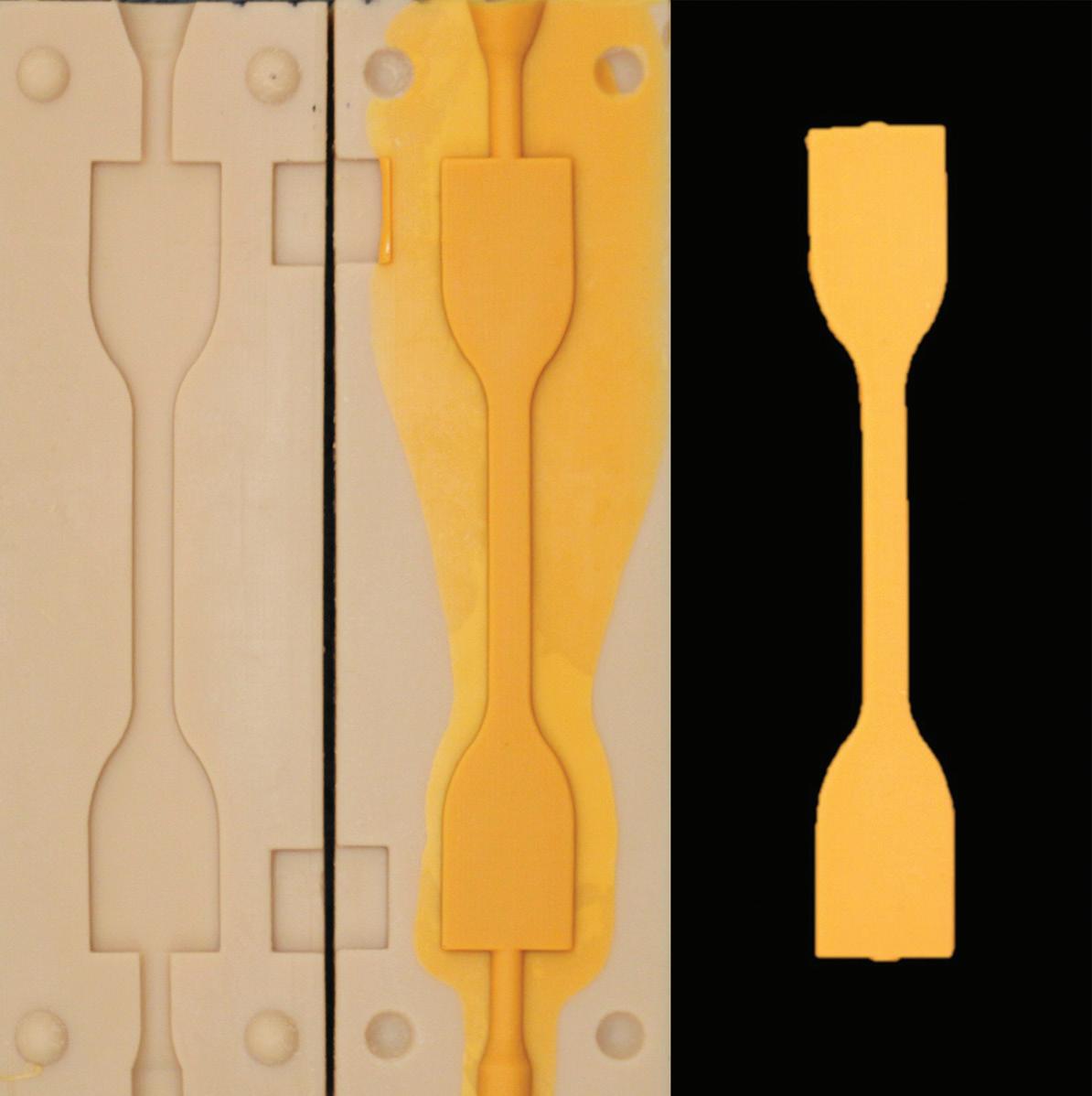
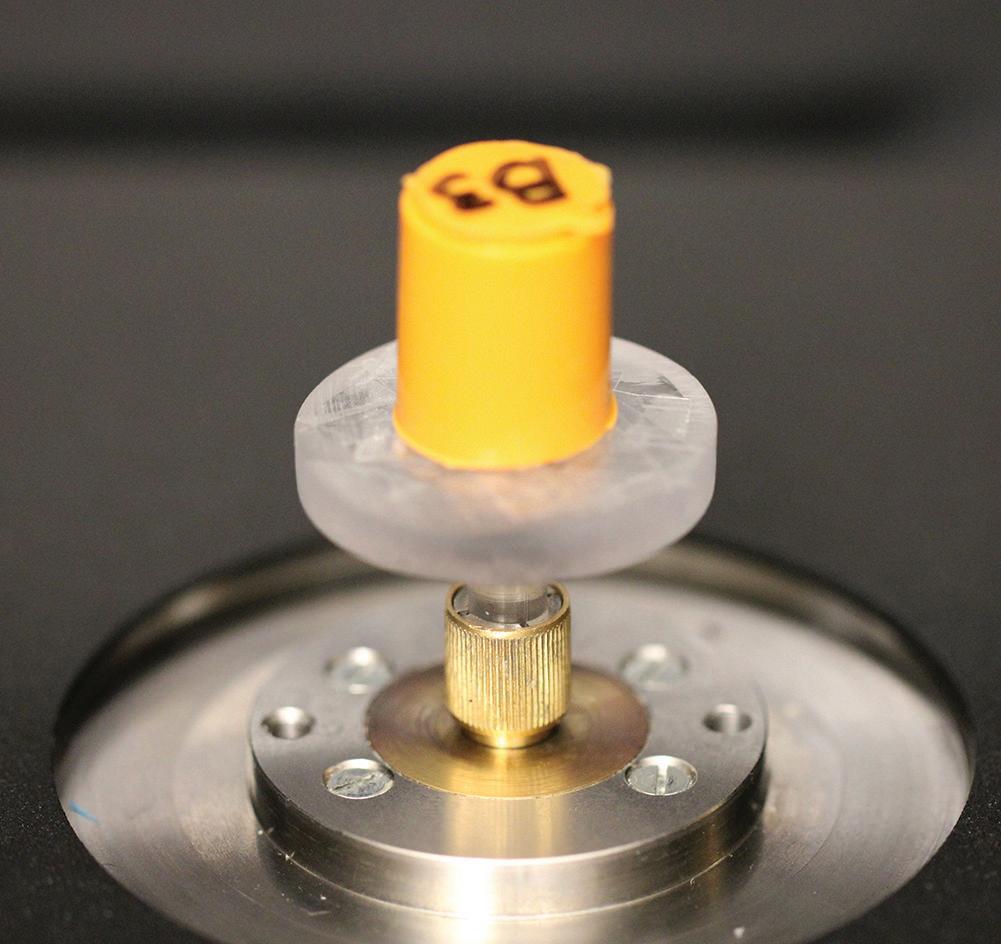
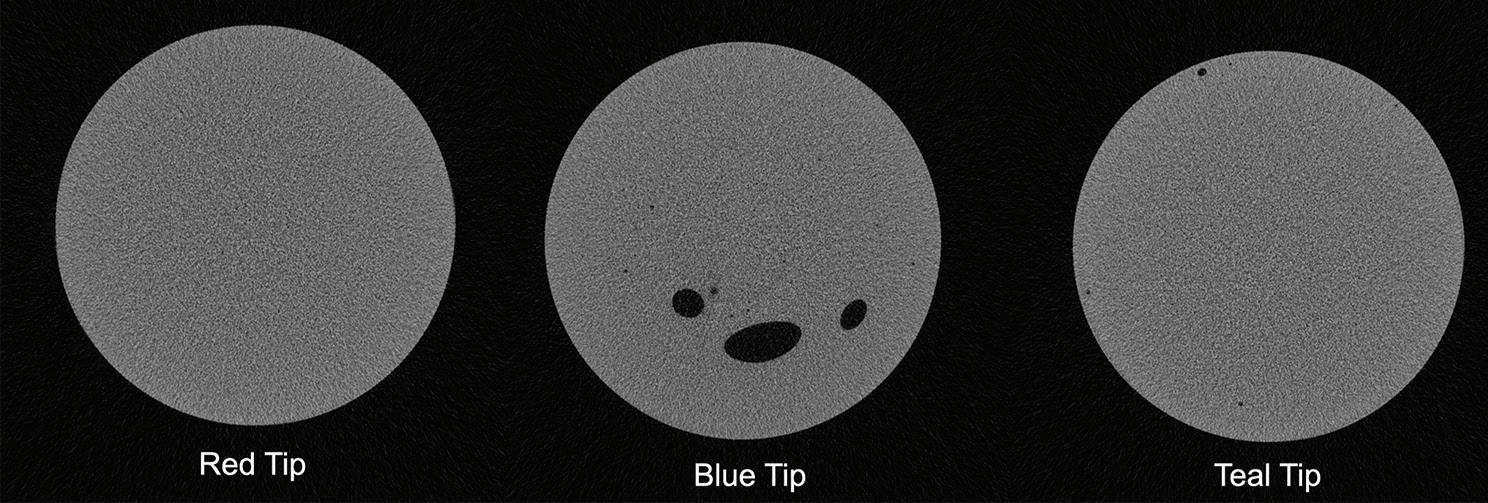
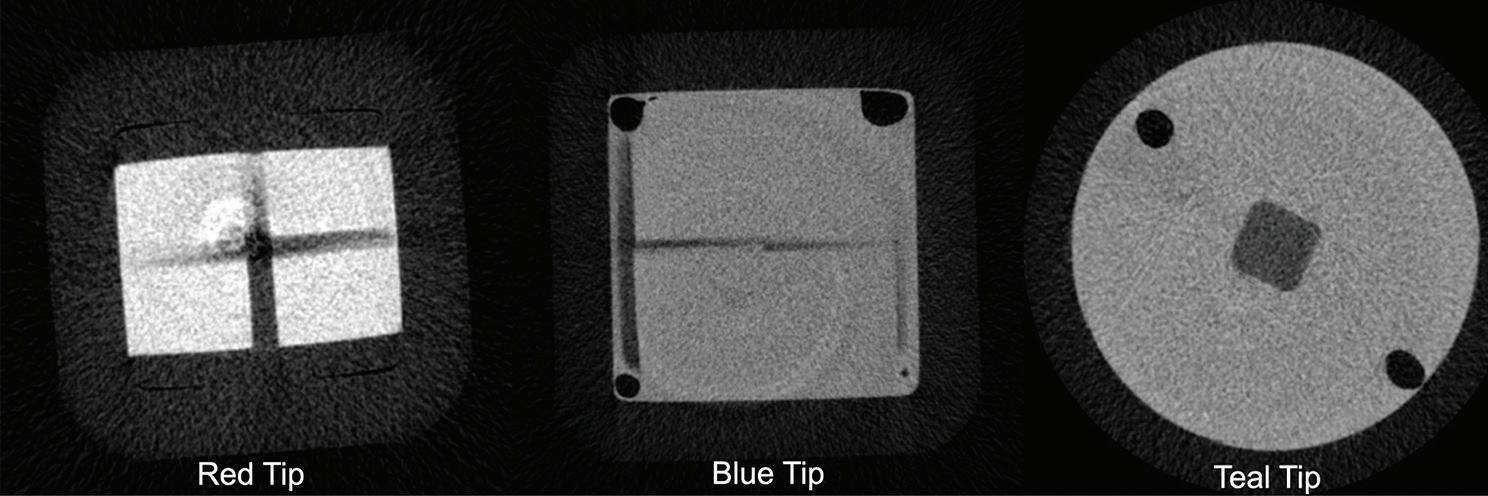
Effect of mixing tip design on the mechanical properties, porosity, and waste reduction of extra-light–body polyvinyl siloxane impression material
Kaisha T. Calvin
Robert Masterson
SELF-INSTRUCTION
Eric Hu
35 Oral Medicine, Oral Diagnosis, Oral Pathology
Evaluation of pulp stones in unerupted teeth and their correlation with principal biochemical factors using cone beam computed tomography
Zahra Javaheri
Nasim Jafari-Pozve
S. Marjan Arianezhad
Sogol Jafari-Pozve
Seyed Sasan Aryanezhad
42 Oral Medicine, Oral Diagnosis, Oral Pathology
A clinical guide to oral manifestations and diagnosis of limited systemic sclerosis: a case report
Vanessa Carvajal Soto
Helen Heloene Rosa
Marcelo Carlos Bortoluzzi
46 Sports Dentistry
Larissa Knysak Ranthum
Eduardo Bauml Campagnoli
What every dentist needs to know about electric scooters
John K. Brooks
Nasir Bashirelahi
SELF-INSTRUCTION
Youstina A. Hanna
51 Oral Medicine, Oral Diagnosis, Oral Pathology
Complementary examinations in the diagnosis of Sjögren syndrome: a report of 2 cases
Thaís Xavier Pereira da Silva
Adriana Dibo Cruz
Monica Ghislaine Oliveira Alves
Thaylla Núñez Amin Dick
Janete Dias Almeida
Geraldo Oliveira Silva-Júnior
56 Oral Medicine, Oral Diagnosis, Oral Pathology
Rare angiofibrolipoma of the oral cavity: a case report
Monika Nandan
Devender Singh Chauhan
60 Basic Science
Harmeet Singh
The connection between poor oral health and metabolic disease: the sugar link theory
Herman B. Dumbrigue
68 Pediatric Dentistry
Comparison of the clinical performance of pit and fissure sealants containing either fluoride or amorphous calcium phosphate on permanent first molars
Mahtab Memarpour
Azade Rafiee
73 Basic Science
Alireza Sharifinejad
Niloofar Mokhtari
Comparison of the antimicrobial effects of 0.2% curcumin mouthwash and chlorhexidine mouthwash on Streptococcus mutans in orthodontic patients: a randomized clinical trial
Tahura Etezadi
Hodis Ehsani
Amirreza Samaei
Ali Semnani
Hamid Reza Goli
Farhad Sobouti
Cover image inspired by: Effect of mixing tip design on the mechanical properties, porosity, and waste reduction of extra-light–body polyvinyl siloxane impression material, on p. 28
Members, call 888.243.3368 and ask for a Member Services representative.
Mailing Lists
For information about ordering AGD mailing lists, call 888.243.3368 ext. 4097 or email advertising@agd.org.
All materials subject to copying and appearing in General Dentistry may be photocopied for the noncommercial purposes of scientific or educational advancement. Reproduction of any portion of General Dentistry for commercial purposes is strictly prohibited unless the publisher’s written permission is obtained.
AGD does not necessarily endorse opinions or statements contained in essays or editorials published in General Dentistry. The publication of advertisements in General Dentistry does not indicate endorsement for products and services. AGD approval for continuing education courses or course sponsors will be clearly stated.
General Dentistry (ISSN 0363-6771) is published bimonthly in 2025 by the AGD, 560 W Lake St, Sixth Floor, Chicago, IL 60661-6600.
Periodicals postage paid at Chicago, IL and additional mailing office. POSTMASTER: Send address changes to General Dentistry, 560 W Lake St, Sixth Floor, Chicago, IL 60661-6600. Email: subscriptions@agd.org.
Canadian mailing information: IPM Agreement number 40047941. Change of address or undeliverable copies should be sent to: Station A, PO Box 54, Windsor, Ontario, N9A 6J5, Canada. Email: subscriptions@agd.org.
AGD members receive General Dentistry as part of membership; annual subscription rates for nonmembers are $135 for individuals and $255 for institutions. Online-only subscriptions are $120 for individuals and $230 for institutions. All orders must be prepaid in US dollars. Single copies are available upon request. Please contact our Membership Services Center at 888.243.3368 for more information.
The Academy of General Dentistry (AGD) was founded to promote high-quality dental education and advocacy. As dentistry constantly evolves, it is essential that we stay vigilant in upholding the values of our profession. AGD’s strength lies in the support system created by our leadership and team members, guiding us in this ever-changing field. Every benefit we enjoy—whether it’s our annual scientific session, webinars, podcasts, publications, or advocacy efforts—results from the hard work of many, supported by a network of sponsors. These generous partners are dedicated to advancing dentistry and our AGD, helping us become better-trained professionals and ultimately improving patient care.
It’s important to recognize that our sponsors do more than just provide financial support. They help drive initiatives that enable AGD to fulfill its mission, offering opportunities that are more cost-effective than if we were to seek them independently.
So, why should we as general dentists support the businesses that help us? Because doing so strengthens the cycle of success. When we engage with these sponsors, AGD can better provide highquality education and advocacy. As members, we sometimes overlook the infrastructure that supports our worldclass organization. I often say that AGD is the only organization that exclusively advocates for the general practitioner. AGD Impact keeps us informed in an easy-to-digest format, and General Dentistry is a high-quality, peer-reviewed journal that we should all be proud of.
Our sponsors help bridge the gap between education and the constant technological and clinical advances in dentistry. The exhibit hall at the scientific session is one example of how we can learn, connect, and refine our skills. With this help, our practices can grow and thrive.
AGD has always been a member-driven organization. Our leadership listens to those who invest in it, and together, we advance the profession. Staying current and relevant is a group effort.
So, what’s the return on investment (ROI) for AGD members? Your membership dues support clinical achievements, networking, and enhanced professionalism. Staying informed about trends and best practices ensures you provide optimal care to your patients. AGD offers numerous resources— these member benefits offer significant ROI and should be fully utilized. Engaging with our sponsors helps us stay at the forefront of innovations in healthcare.
Many issues affect dentists today, from legislative concerns to insurance challenges and regulations impacting our day-to-day practices. Advocacy is crucial in minimizing unfavorable policies and restrictions to the way we practice. By engaging with our sponsors, we strengthen our collective voice, ensuring that AGD can continue advocating on our behalf.
Our sponsors certainly benefit when we support them, but the relationship is mutually beneficial. By attending AGD events, taking advantage of member discounts, and exploring new products and services, we help sustain the programs that benefit our careers and practices. Without our engagement, many of these sponsors wouldn’t be able to continue supporting us.
Engaging with AGD sponsors helps sustain the resources that benefit us all.
Our support reinforces the value of these partnerships, ensuring AGD can continue providing high-level service and advocacy. Sponsorship is more than just funding—it’s also fostering a community where AGD, its members, and industry partners work together to elevate general dentistry.
The future of dentistry is bright, and AGD will continue to lead the way. The investments made through our sponsors are investments in all of us.
Timothy F. Kosinski, DDS, MAGD Editor
Tooth replacement from extraction to restoration. 2. Implant planning and placement
Marcus Cowan, DMD
The second part of a series on tooth replacement, this column discusses implant planning and placement.1 After successful socket preservation grafting, the proposed implant site is ready for implant placement. However, important planning and preparation steps must be completed before the patient’s surgical appointment. In addition, fabrication of a surgical guide can improve the efficiency and accuracy of implant placement and enhance operator confidence.
Implant planning
After tooth extraction and socket preservation, patients heal for at least 3 to 4 months. Once the healing process is complete, among the most important procedures for implant planning are cone beam computed tomographic (CBCT) and intraoral scans. The CBCT scan is a 3-dimensional (3D) radiograph that shows the patient’s bone in ways that cannot be seen on 2-dimensional images such as periapical, bitewing, or panoramic radiographs. The use of CBCT scans for implant cases is becoming common because of the important information provided, including bone height, bone width, and the location of arteries, veins, nerves, and other important anatomical features.2
In addition, CBCT images can be used to assess bone density. Bone density ranges from D1 to D4.3 The density is measured in a ratio of cortical-to-cancellous bone. Cortical bone, which makes
up the outer portion of the bone, is dense and has low vascularity. Cancellous bone, which makes up the inner portion of the bone, is not dense and has higher vascularity. D1 bone consists of a high percentage of highly dense cortical bone and minimal to no cancellous bone. D4 bone has a high percentage of low-density cancellous bone and little to no cortical bone. In bone that is more cortical and more dense, the clinician will generally make a larger osteotomy to reduce the stress put on the dense bone. In bone that is less dense and more trabecular, the clinician can make a more undersized osteotomy to ensure good primary stability of the implant. Depending on the type and density of bone found on the preoperative CBCT, the clinician can modify the implant placement technique to adjust for the findings. In my experience, the density of grafted sites is usually classified as D2, but this can vary depending on the type of graft used (Fig 1 and 2).
In addition to CBCT scanning, intraoral scanning is helpful. It captures the soft tissue volume so that the clinician can determine the gingival phenotype of the desired implant site as well as the tissue thickness at potential donor sites for connective tissue grafts or free gingival grafts. The intraoral scan can be aligned with the CBCT scan to create an accurate overlay that shows both bone and soft tissue. The anatomical crowns of teeth are the same on the CBCT and intraoral scans, so they can be used as references to align the jaws in the scans.
This is helpful because if there is any challenging anatomy, the clinician can plan accordingly to avoid it or work around it safely.
In grafted sites, it is preferable to obtain the CBCT scan at least 3 months after grafting to allow for a significant amount of hard and soft tissue healing at the site. Ideally, the intraoral scan is taken either at the same time as the CBCT or shortly afterward. This allows the treating clinician to evaluate the CBCT and to discuss the findings with patients when they come in for the intraoral scan. By the time the implant placement is scheduled, about 4 months will have elapsed since the socket preservation grafting, which is adequate healing time.
After the CBCT and intraoral scans are completed, it is time to begin the implant planning process using a restoratively driven protocol. This means that the implant-supported restoration is positioned in the ideal alignment in the arch, and the implant is positioned ideally beneath this restoration. The first step of the restoratively driven protocol is a digital wax-up of the missing tooth or teeth. This allows the clinician to determine the correct trajectory of the proposed implant in relation to the tooth and to plan for a screw-retained restoration with the access hole in the middle of the occlusal table. The long axis of the implant also has to be aligned with the proximal contacts because this will be the path of insertion for the prosthesis. If the long axis is parallel to the proximal
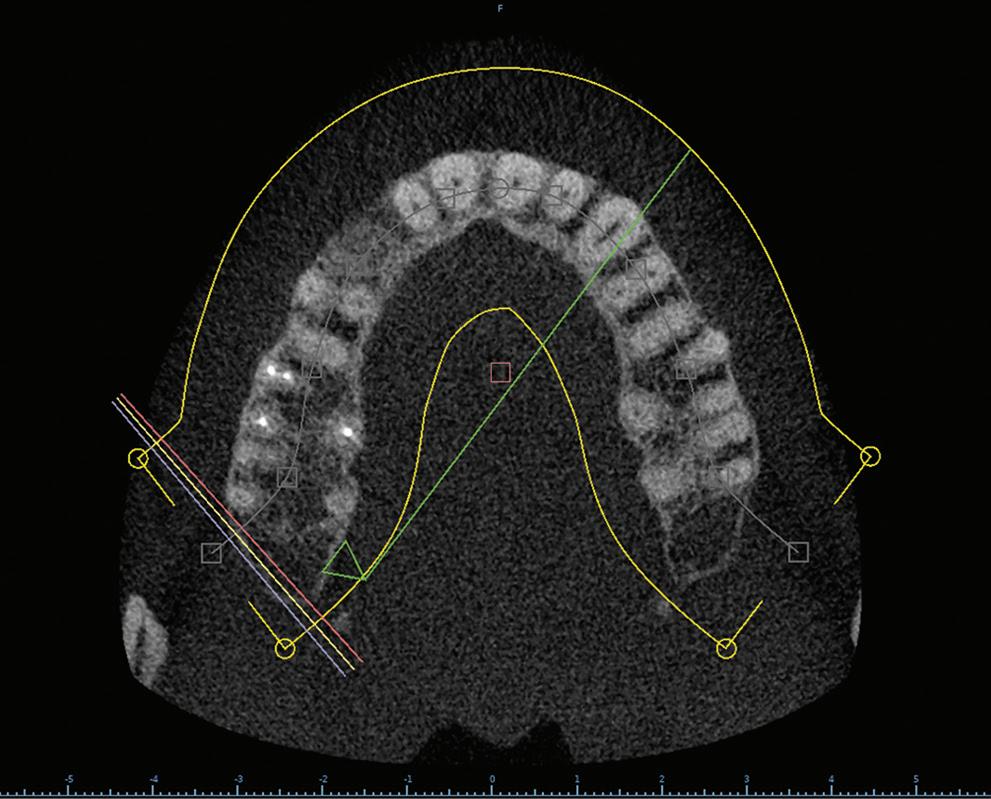
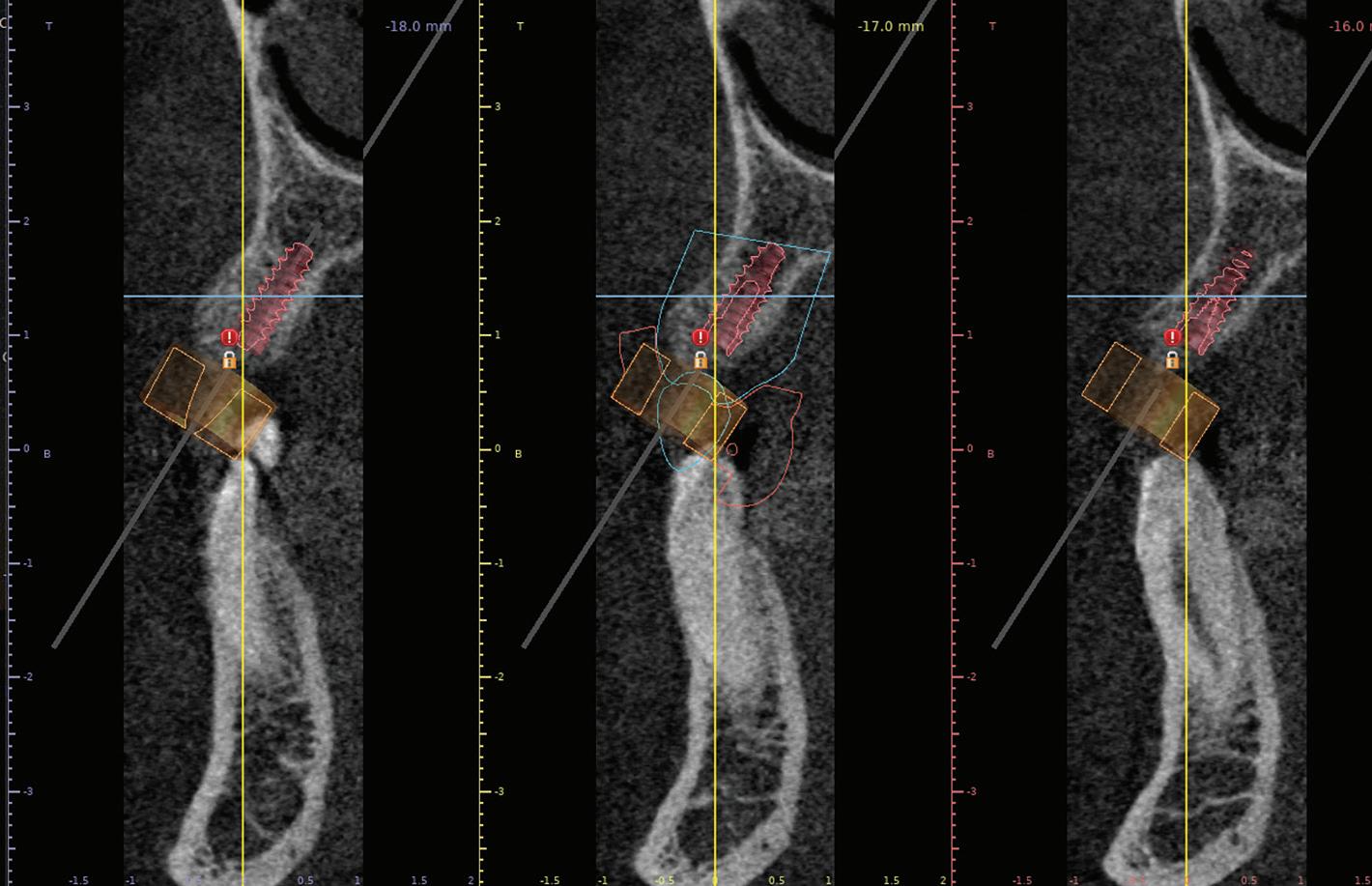
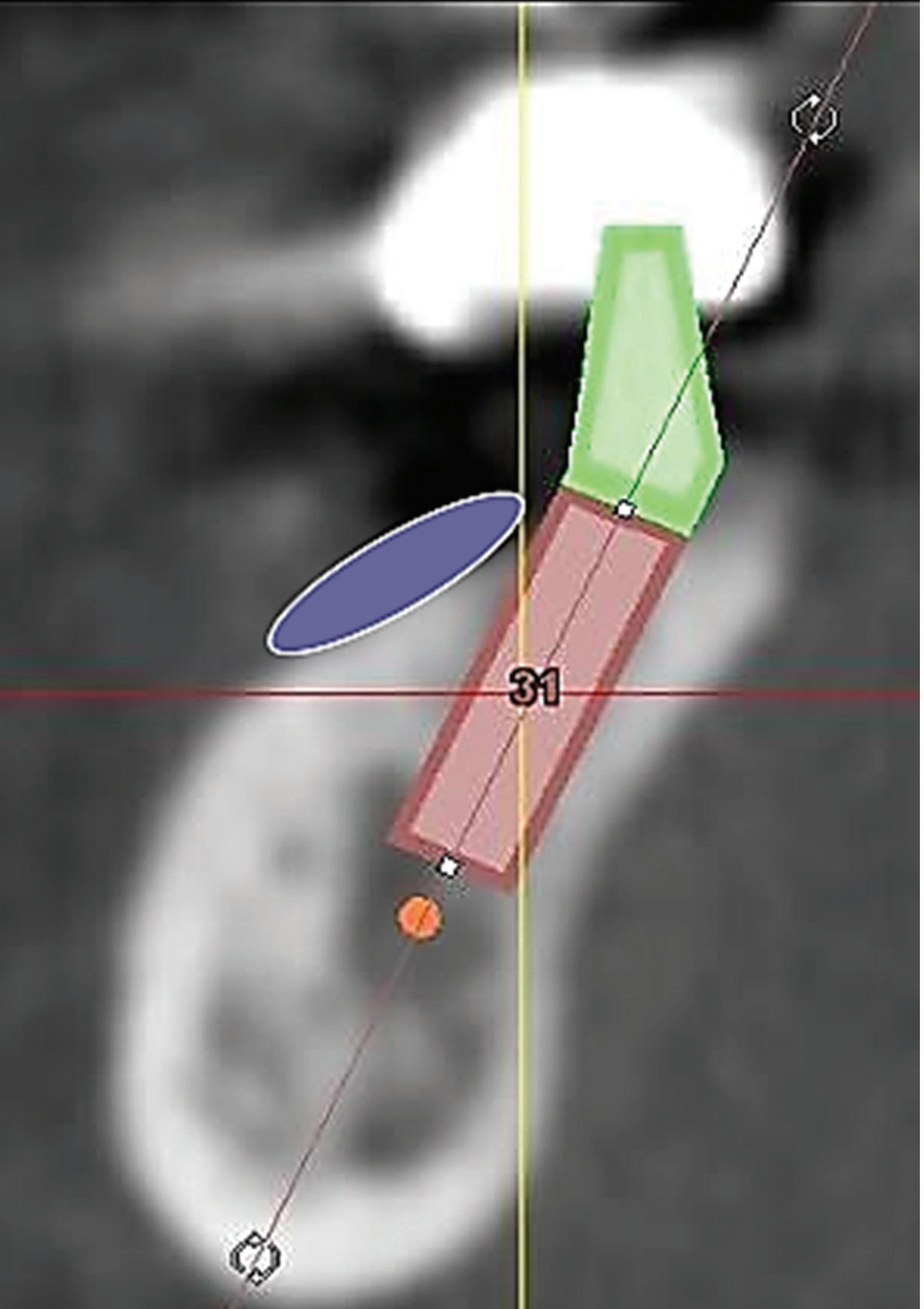
contacts, the restoration can be easily seated. When the long axis of the implant is not aligned with the proximal contacts of the adjacent teeth, it may not be possible to use a screw-retained restoration. In select cases, a cement-retained restoration may be necessary. Figure 3 shows implant planning performed using the CBCT images and intraoral scans. The proposed implant is placed in a biologically sound position, and the blue outline of the digital wax-up tooth can be seen. This angled positioning in the esthetic zone would have resulted in an access hole in the facial surface, which is unesthetic. This means that this case will need a cement-retained crown. Using the information from the CBCT and intraoral scans, we know this from the beginning of the case so the restorative portion of the case can be planned accordingly. If the position of the implant had been adjusted enough to place a screw-retained restoration, the result would have been a notable apical perforation, and several millimeters of the implant apex would be outside the bony housing. This would significantly complicate the case and require at least 1 additional grafting surgery, and grafting outside the bony housing is unpredictable. After taking all factors into consideration, it was decided to plan to restore with a cement-retained crown instead of undergoing further surgical procedures.
The amount of restorative space is an important factor in restoration planning and can impact implant depth. The space between the implant platform and the
opposing tooth must be at least 5 mm, and in cases involving minimal space, a screw-retained restoration will be necessary.3 If the restorative space is more than 15 mm, the chance of prosthetic complications such as screw loosening and breakage increases.4
To optimize the chance of achieving long-term stability of the bone and soft tissue around the implant, the clinician should aim for at least 2 mm of bone around the implant, especially on the buccal aspect.5 If there is not enough bone surrounding an ideally sized
implant, the clinician can consider performing bone augmentation procedures before or during implant placement. Another goal for promoting long-term stability is to have at least 2 mm of tissue thickness and 2 mm of keratinized tissue around the implant.6 Adequate tissue thickness helps maintain crestal bone around implants and mask the metal color, resulting in improved cosmetic outcomes. The aim for implant depth, according to the “zero bone loss concept,” is for the platform of the implant to be located 4 mm below the gingival margin.7
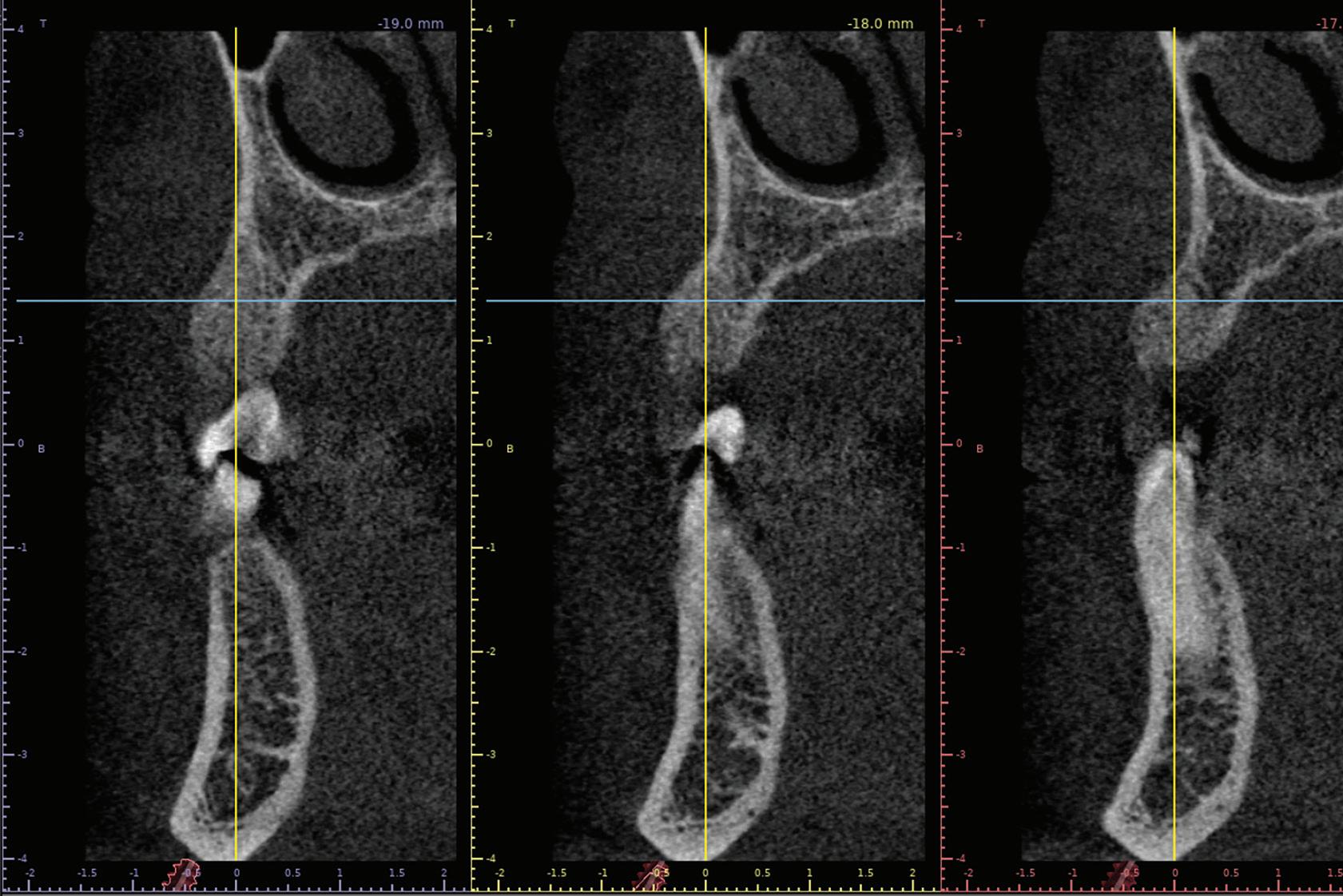
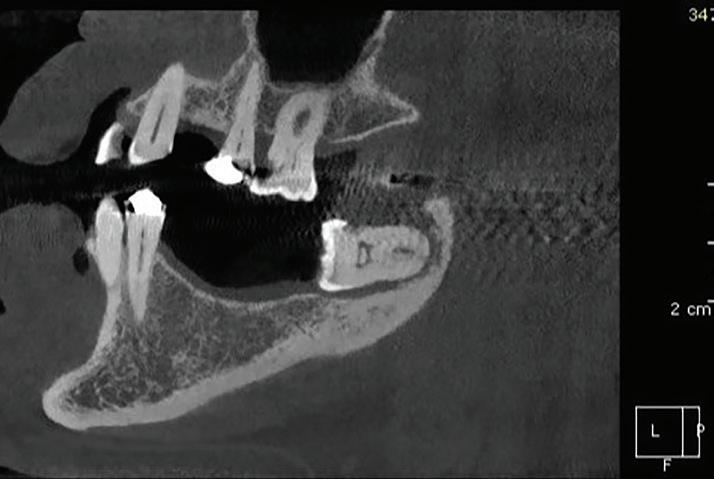
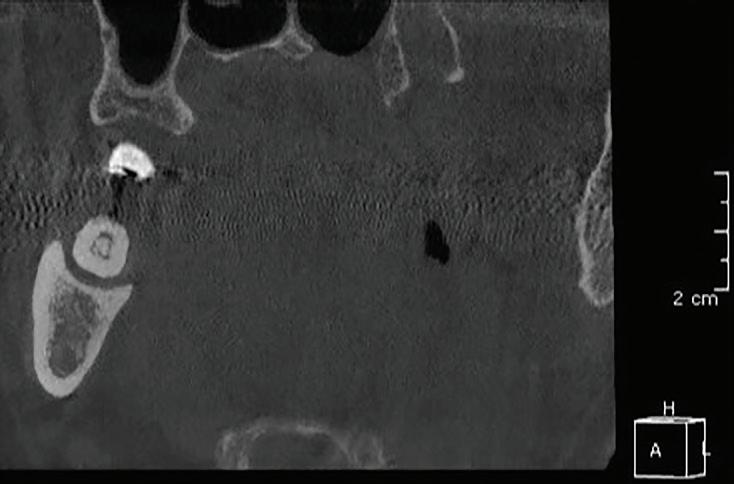
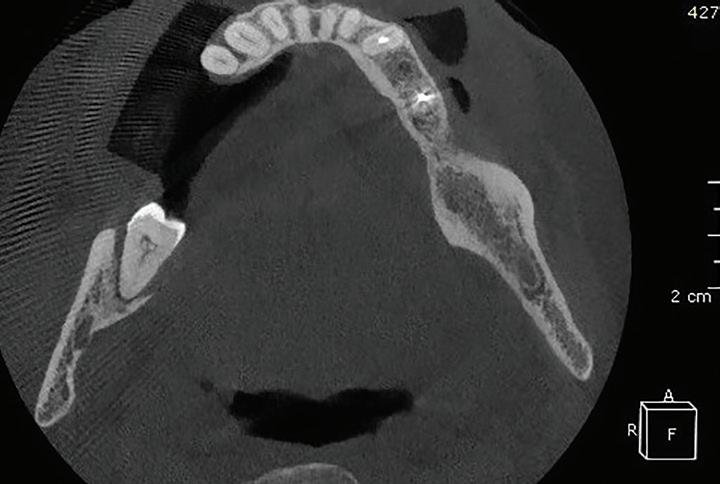
Fig 1. CBCT images confirm healing of the extraction site after grafting. Fig 2. An occlusal CBCT view reveals the density of the healed graft.
Fig 3. CBCT images of the proposed implant at the site. The digital wax-up can be seen outlined in blue. Placing the implant in a biologically sound position yields a restoration with facial screw access, making a screw-retained restoration an unesthetic option.
This allows room to establish biologic width, and implant biologic width is different from natural tooth biologic width.8 When placing implants, practitioners need to know the location of the inferior alveolar nerve and maxillary sinus in relation to the proposed implant site. Staying 2 mm away from these significant anatomical structures is a safe practice to avoid complications.9 However, this guideline is not set in stone; the case specifics and the practitioner’s experience are factors in deciding which parameters to use. The surgical plan must also account for the locations of other anatomical features such as lingual undercuts, arteries, and accessory nerves to avoid catastrophic surgical complications in what might otherwise be a routine case.
Surgical guide
Once all the surgical factors have been considered and the implant has been planned digitally, it is time to fabricate the surgical guide. There are a number of good software programs that can be used to fabricate a surgical guide at a reasonable cost. Practitioners should use whatever system they are comfortable using and that enables them to achieve predictable results. There also are commercial services that can do the planning for clinicians who do not want to do it themselves.
There are several types of surgical guides, which are classified from type 0 to type 4.10 A type 0 guide is actually no guide, or freehand placement. A type 1 guide involves the use of an imprecise aid such as a vacuum-formed (“suck-down”) stent to help visually approximate the position of the implant drill. This guide can be made from a suck-down stent on a stone cast and is not highly accurate by itself. Types 2, 3, and 4 guides are typically 3D printed and are usually accurate when used on their own. Type 2 is a pilot guide, which has a sleeve for a standard pilot drill. The remainder of the drilling and the implant placement are done freehand. A type 3 surgical guide has a sleeve designed to fit the pilot drill and all of the osteotomy burs, but the implant placement is performed freehand. A type 4 guide allows all of the drilling and the implant placement to be performed through the guide. My preference is a
type 3 guide, but all guides, types 1 to 4, offer benefits, especially for clinicians newer to implant surgery.
Some guides are designed to allow room for irrigation during drilling from the buccal or lingual aspect. In addition, some guides have windows, which are strategic holes that allow the clinician to ensure that the guide is fully seated. A surgical guide is not a substitute for adequate knowledge and training, but it is a tool that can help practitioners achieve great clinical results.
Implant placement
Prior to surgery, a 2-g loading dose of amoxicillin is given to the patient.11 The literature on the topic has mixed findings depending on the study, though there is enough positive evidence in my opinion to support the claim that preoperative antibiotics can be helpful in reducing the implant failure rate.11 If the patient is allergic to amoxicillin, alternative medications such as clindamycin can be used, but patients who are allergic to penicillin experience failure at a greater rate than do those who are not allergic.12 After the patient rinses with chlorhexidine, antiseptic is applied to the incision areas and then rinsed thoroughly. Although the mouth can never be sterile, these steps make the field as clean as possible for the surgery.
After antiseptic procedures, the surgical site is evaluated. In Fig 4, the site shows good hard and soft tissue volume consistent with that seen in the preoperative planning scans.
Anesthesia techniques for implant placement are similar to those used for tooth extraction.1 One difference is that in most cases, buccal and lingual local infiltration are sufficient for implant placement. The use of 4% articaine with 1:100,000 epinephrine for infiltration is preferred due to its increased efficacy compared with other common infiltration anesthetics.13
On rare occasions, some patients still experience discomfort once drilling in the mandible begins. If the case was planned digitally and one can be 100% certain of the location of the inferior alveolar nerve, it is acceptable to perform an inferior alveolar nerve block. Implant cases are typically planned to have a buffer zone of 2 mm from the nerve if
the anatomy allows. The guide drills are depth limiting, so the risk of damage to the nerve is almost nonexistent. Historically, practitioners performing freehand implant surgery would use only infiltration anesthesia in the mandible. If the drilling approached the inferior alveolar nerve, patients would be able to feel it and provide sensory feedback so clinicians would know not to drill any deeper. With a full digital work-up and guided implant placement, clinicians know exactly where the inferior alveolar nerve is in relation to the implant fixture. Clinicians doing guided surgery do not need any sensory feedback from the patient and can safely perform an inferior alveolar nerve block without any concern for complications.
After time is allowed for the initial anesthetic to sufficiently numb the surgical site, infiltration is performed at the crest of the ridge until the area blanches; the incision is made immediately thereafter. This infiltration hydraulically raises the periosteum from the bone slightly and makes flap reflection easier.
A size 15c scalpel blade is used to make the initial incision for the full-thickness mucoperiosteal flap. In most cases, I prefer to bury the implant for a 2-stage approach, so a crestal incision is made lingual to the middle of the crest. This approach means that the incision line is not located directly over the implant, thus decreasing the risk of a pinhole exposure over the implant. A pinhole exposure is a very small communication over the implant that allows bacteria to accumulate around the platform; this can result in early bone loss even though the implant has not yet been uncovered.
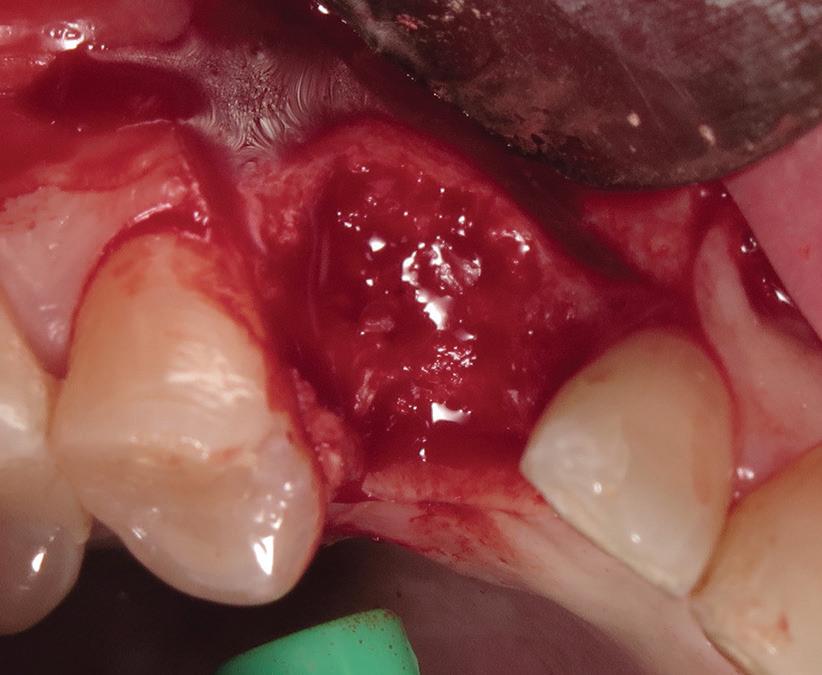
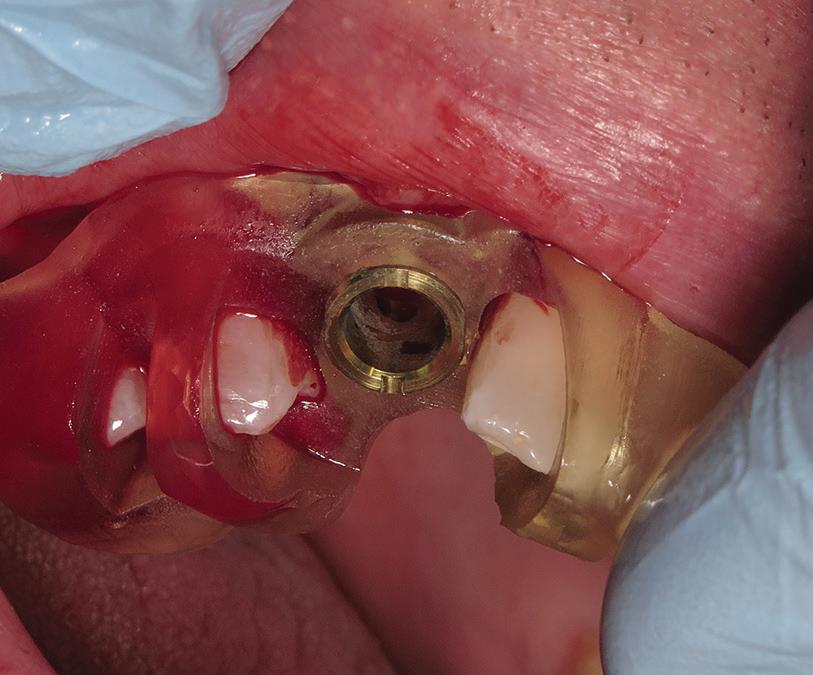
The flap design for implant cases usually extends to half a tooth beyond the surgical site in each direction. For example, for an implant at site 19, the flap is extended to the mesiofacial surfaces of teeth 18 and 20. It is also reflected at least 2 mm buccally and lingually to allow full visualization of the bone at the surgical site. The flap is raised with a Woodson elevator or a Molt No. 9 elevator, and the surgical site is examined (Fig 5). The surgical guide is tried on to ensure there are no issues with the fit or positioning of the guide (Fig 6). One benefit of using a surgical guide is that it holds the flap out of the way once it is
fully seated, freeing up the dentist’s or assistant’s hand.
Once the fit of the guide has been verified, it is time to begin the osteotomy. Each implant system can have different surgical kits, so clinicians need to confirm that they are using the correct one for the case at hand. Typically, implant systems have a freehand kit and a guided kit; if using the latter, the clinician needs to verify that the drills fit into the guide sleeve in the surgical guide. All implant systems have their own nuances, so dentists must familiarize themselves with the system being used.
When a surgical guide is used, the first drill used is the pilot drill. It is inserted into the guide and used to full depth of the guide per the digital planning. A periapical radiograph is taken to ensure that the orientation and depth are consistent with the preoperative planning. If everything looks aligned, the drill sequence is continued stepwise, sizing the osteotomy appropriately for the case. I have never used a guide that did not seat, but verification radiographs are still taken as a precaution. When implants are placed in a guided procedure, after the radiograph of the pilot drill at depth is taken, no other radiographs are taken until after the implant is placed.
If practitioners have limited experience placing implants or using a particular implant system, it is recommended that they follow the manufacturer’s recommendations with regard to drilling speeds and drilling protocol. With more experience, my technique has shifted to the use of biologic drilling.14,15 In this technique, the pilot drill is used to drill to depth at 1000 to 1500 rpm
under saline irrigation. After the pilot drill has been used, all subsequent drills are used at 50 rpm without irrigation. This technique offers a few advantages over traditional drilling. It allows for easier collection of autogenous bone in the flutes of the drill; the low-speed drilling eliminates the heat produced during high-speed drilling, so no irrigation is needed; drilling at slow speeds maintains the vitality of the osteoblasts in harvested bone and at the site; less pressure is applied to the bone of the osteotomy site; and the marks on the drill are easily visualized to verify the depth of the drill. In my opinion, it makes sense that drilling in a way that decreases trauma to the native bone would lead to faster bone healing and osseointegration; however, I have not conducted research on this topic to histologically verify these claims.
After the drilling is completed, the osteotomy is inspected prior to implant placement. Most kits include a ball probe,
which is used to explore all the walls of the osteotomy to ensure that only bone is felt. A soft spot signals a perforation. The soft area could be a buccal or lingual perforation, a nerve, the schneiderian membrane, or other nonbony anatomy. This needs to be investigated prior to implant placement and treated accordingly. Treatment of a perforation could be as simple as redirecting the osteotomy or as complicated as the need for nerve repair; the treatment depends on the extent and location of the perforation.
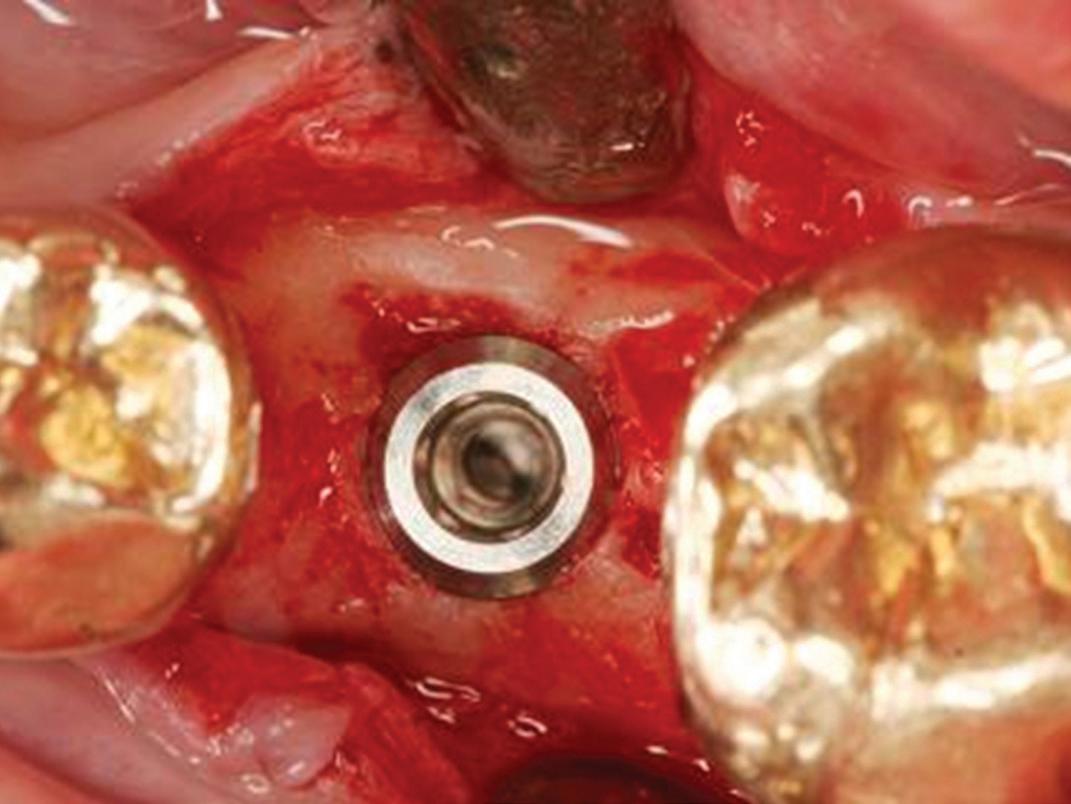
If no perforation is present, the implant is placed in the ideal positioning determined from the preoperative planning (Fig 7). The implant handpiece is preferred for placing the implant fixture because it provides a torque reading in real time as the implant is being placed. The implant motor is electively set to 35 N/cm, and the handpiece will stop advancing the implant once it reaches that reading. The hand driver is then used to finish fully seating the implant at
Fig 5. The reflected flap reveals bleeding vital bone and maintenance of ridge width.
Fig 4. The fully healed site is ready for implant placement.
Fig 6. The seated guide reveals an intimate fit with the dentition.
Fig 7. The implant positioning confirms excellent buccal bone width that will promote long-term stability.
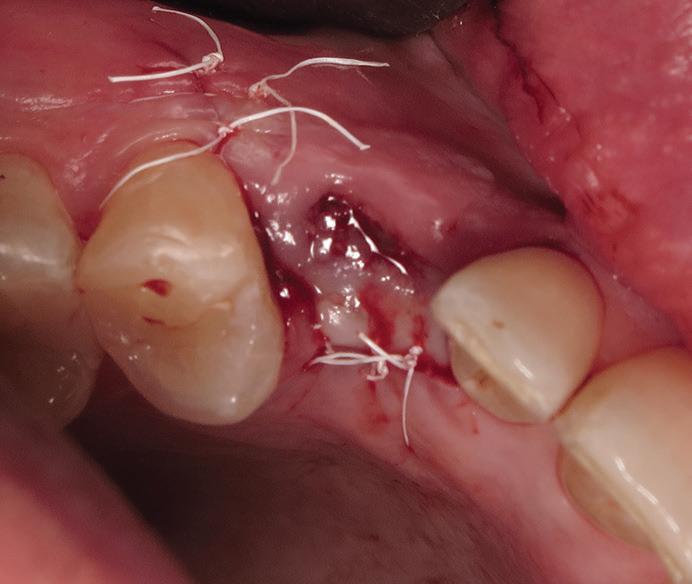
Fig 8. The implant site is closed with PTFE sutures in a 2-stage approach.
the surgical site. If the torque is high but the implant is at the desired depth, the clinician can back the implant out 1 to 2 counterrotations, and then reinsert the implant back to depth. This will decrease the torque without changing the implant positioning.
In some cases, the torque on the implant gets very high (above 75 N/cm) a few millimeters before it reaches the appropriate depth. In such cases, the hand driver is used to insert the implant farther, first driving it deeper by 3 or 4 rotations and then backing it out with 1 or 2 counterrotations. This is done repeatedly until the implant is at the desired depth and torque. If the implant reaches high torque value (≥ 75 N/cm) but the implant is only halfway to depth, the implant should be completely removed, and further drilling is needed.
If the clinician intends to place the implant in a 1-stage procedure, a primary stability of at least 35 N/cm torque is recommended. If it is a grafted site, my belief is that one should not aim for torque values higher than 35 N/cm to avoid excessive torque on the grafted bone.16 If the implant is placed mostly or entirely in native bone, the clinician can aim for 50 N/cm. During the healing phase, there is a decrease in stability due to bone turnover. That “stability dip” is generally considered to be the greatest at around the 4-week mark. The greater the primary stability, the more stable the implant will be during the stability dip. In addition, with good primary stability there is a lesser likelihood of micromovement during initial healing. Micromovement during early implant healing can lead to implant failure. Once the implant is placed to the appropriate depth and torque, the internal components of the implant should be irrigated with saline to ensure that no bone or blood is inside. After irrigation is complete, a healing abutment is placed, and a periapical radiograph is taken to ensure full seating of the component. The healing abutment can be a stock healing abutment, a stock anatomical healing abutment, or a custom healing abutment. After the healing abutment is confirmed to be seated, the flap is sutured closed around the healing abutment with a resorbable suture. Poliglecaprone 25 (PGCL) is a
good suture for closure around a healing abutment because it is a monofilament suture, and monofilament sutures harbor less plaque than braided sutures. It is also resorbable, so a second procedure for suture removal is not necessary. More on-site customization will be covered in part 3 of this series.
For a 2-stage procedure, I aim for 10 to 15 N/cm of torque so that minimal stress is placed on the bone. This range of torque is strong enough that the implant does not move when components are seated but light enough to exert minimal stress on the bone. The same technique described for 1-stage placement is used to place the implant to the appropriate depth and torque. Once the implant is placed to the appropriate depth and torque, I irrigate the internal components with saline to ensure that no bone or blood is inside the implant and then place the cover screw.
There is an additional optional step that can be done to help simplify the second-stage appointment. Prior to seating of the cover screw, a scan body is placed on the implant, and a periapical radiograph is taken to ensure that the scan body is fully seated. Even though the flap is still open, an intraoral scan of the site is taken. In this scan, the flap must be reflected so that it does not block the scan body. The scan body gives the exact positioning of the implant platform, so its full visibility during scanning is critical. This scan is then used to digitally design a custom healing abutment that can be 3D printed and ready to use at the secondstage appointment. Once the scan is complete, the scan body is removed, the internal components of the implant are irrigated to ensure no debris has accumulated, and the cover screw is placed.
A periapical radiograph is obtained to show the final implant position and to ensure that the cover screw is fully seated. The flap is then irrigated with saline to flush out any bone or debris under the flap and closed with sutures (Fig 8). Polytetrafluoroethylene (PTFE) sutures are preferred for closure as they are biologically inert and do not harbor plaque like braided sutures do. They are also nonresorbable, so when the patient returns to have them removed, I can assess the healing.17
Postoperatively, pain medications are given. Ibuprofen, acetaminophen, and hydrocodone are all options to alleviate postoperative discomfort and are administered on a case-by-case basis. An antibiotic is given postoperatively, and the ideal prescription is 500 mg amoxicillin 3 times a day for 7 days if the patient is able to tolerate the medication.11
For both 1-stage and 2-stage implant cases, the patient is seen 1 week, 1 month, and 3 months postoperatively. At the 1-week visit, the sutures are removed, if present. By the 1-month visit, the site should be well healed externally if there are no complications. At least 3 months are allowed for bone healing, after which the patient returns for either the implant uncovering and second-stage procedures in a 2-stage case or impressions in a 1-stage case. If significant grafting was performed at the time of tooth extraction or at the time of implant placement, additional healing time is preferred. The additional time could range from an additional 1 month up to an additional 6 months, depending on the size of the graft.
Author affiliation
Private practice, Hudson, Massachusetts.
Conflicts of interest
The author owns CowTech Dental Lab, Lithonia, Georgia, which produces surgical guides for implants.
References
1. Cowan M. Tooth replacement from extraction to restoration, 1: extraction and socket preservation. Gen Dent. 2025;73(1):6-9.
2. Gupta J, Ali SP. Cone beam computed tomography in oral implants. Natl J Maxillofac Surg. 2013;4(1):2-6. doi:10.4103/0975-5950.117811
4. Carpentieri J, Greenstein G, Cavallaro J. Hierarchy of restorative space required for different types of dental implant prostheses. J Am Dent Assoc. 2019;150(8):695706. doi:10.1016/j.adaj.2019.04.015
5. Cicciù M, Pratella U, Fiorillo L, et al. Influence of buccal and palatal bone thickness on post-surgical marginal bone changes around implants placed in posterior maxilla: a multi-centre prospective study. BMC Oral Health. 2023;23:309. doi:10.1186/s12903-023-02991-3
6. Jose EP, Paul P, Reche A. Soft tissue management around the dental implant: a comprehensive review. Cureus. 2023;15(10):e48042. doi:10.7759/cureus.48042
7. Linkevičius T. Zero Bone Loss Concepts. Quintessence Publishing; 2019.
8. Linkevicius T, Apse P. Biologic width around implants. An evidence-based review. Stomatologija. 2008;10(1):27-35. https://www.sbdmj.com/081/081-05.pdf
9. Tufekcioglu S, Delilbasi C, Gurler G, Dilaver E, Ozer N. Is 2 mm a safe distance from the inferior alveolar canal to avoid neurosensory complications in implant surgery? Niger J Clin Pract. 2017;20(3):274-277. doi:10.4103/1119-3077.183240
10. Stanley R. A comprehensive classification system for dental implant surgical guides. Dentistry Today. April 12, 2022. https://www.dentistrytoday.com/comprehensiveclassification-system-for-dental-implant-surgical-guides/
11. Torof E, Morrissey H, Ball PA. Antibiotic use in dental implant procedures: a systematic review and metaanalysis. Medicina (Kaunas). 2023;59(4):713. doi:10.3390/medicina59040713
12. Salgado-Peralvo AO, Peña-Cardelles JF, Kewalramani N, et al. Is penicillin allergy a risk factor for early dental
implant failure? A systematic review. Antibiotics (Basel). 2021;10(10):1227. doi:10.3390/antibiotics10101227
13. Martin E, Nimmo A, Lee A, Jennings E. Articaine in dentistry: an overview of the evidence and meta-analysis of the latest randomised controlled trials on articaine safety and efficacy compared to lidocaine for routine dental treatment. BDJ Open. 2021;7(1):27. doi:10.1038/ s41405-021-00082-5. Erratum: 2021;7(1):29. doi:10.1038/s41405-021-00085-2
14. Shetty SK, Shetty R, Sarfaraz H, Rauf RB, Thenukutty F, Dilip N. Biological drilling protocol in dental implantology—a review. Int J Adv Res. 2022;10(10):153-161. doi:10.21474/IJAR01/15474
15. Bernabeu-Mira JC, Peñarrocha-Diago M, Canullo L, Camacho-Alonso F, Cortes ARG, Peñarrocha-Oltra D.
Autologous bone harvested during implant bed preparation: a randomized clinical trial comparing high-speed drilling with irrigation versus low-speed drilling without irrigation. Clin Implant Dent Relat Res. 2024;26(4):724733. doi:10.1111/cid.13346
16. Javed F, Ahmed HB, Crespi R, Romanos GE. Role of primary stability for successful osseointegration of dental implants: factors of influence and evaluation. Interv Med Appl Sci. 2013;5(4):162-167. doi:10.1556/ IMAS.5.2013.4.3
17. Faris A, Khalid L, Hashim M, et al. Characteristics of suture materials used in oral surgery: systematic review. Int Dent J. 2022;72(3):278-287. doi:10.1016/j.identj.2022.02.005
Understanding analgesic drug mechanisms of action to aid in postoperative dental pain management
Jason H. Goodchild, DMD ¢ Mark Donaldson, BSP, ACPR, PHARMD, FASHP, FACHE
Dental pain is one of the most common types of pain, often resulting from conditions such as dentin hypersensitivity, pulpitis, periodontitis, infection, or postoperative dental procedures.1 Consensus among recent guidelines from the medical and dental literature can help practitioners select the most appropriate analgesics to keep patients comfor table 2-4 In 2022, the Centers for Disease Control (CDC) published the updated “CDC Clinical Practice Guideline for Prescribing Opioids for Pain — United States,” designed to serve as a clinical tool for primary care and other clinicians, including dentists, who provide pain management for patients ≥ 18 years with acute pain (< 1 month), subacute pain (1 to 3 months), and/or chronic pain (> 3 months). 2 These guidelines contain 12 recommendations for prescribing analgesics for outpatients with pain. The first 2 focus on whether to initiate opioids. Addressing acute pain specifically, the first recommendation of the CDC guideline states that nonopioid therapies are at least as effective as opioids for many types of acute pain, and clinicians should maximize nonopioid therapies unless the benefits of opioid therapy outweigh the risks. 2
Recently, the American Dental Association (ADA) released evidencebased clinical practice guidelines for
the pharmacologic management of acute dental pain in children, adolescents, adults, and older adults. These guidelines, along with the CDC’s recommendations, reinforce the importance of using nonopioid analgesics as first-line treatment for acute dental pain and emphasize the value of multimodal analgesia. 3,4 Multimodal analgesia incorporates around-the-clock nonopioid analgesics and nonpharmacologic therapies before considering systemic opioids. This opioid-sparing approach can be defined as the use of more than one pharmacologic class of medication, often targeting different receptors in the pain pathway, for the management of pain. 2,5 The combination of analgesics with different mechanisms of action often provides synergy or synergism: when 2 or more agents working in combination have an effect that is greater than the expected additive effect of either drug alone. 6 Using postoperative multimodal analgesic and synergistic approaches can help maximize the therapeutic effects of 2 or more medicines while also minimizing the potential adverse effects.7,8
This column explores the classes of oral analgesics commonly used in the management of dental pain, their mechanisms of action that may help to promote synergy, and the clinical implications of multimodal analgesia.
Mechanisms of action of oral analgesic drug classes
Acetaminophen
Acetaminophen is the most common drug ingredient in the United States and one of the most ubiquitous overthe-counter (OTC) medications used to treat pain and fever.9-13 Acetaminophen is thought to increase the pain threshold in the central nervous system (CNS) by inhibiting cyclooxygenase (COX), an enzyme involved in prostaglandin synthesis. Prostaglandins mediate pain, inflammation, and fever. Acetaminophen specifically inhibits both COX-1 and COX-2 in the CNS but does not affect prostaglandin synthesis in peripheral tissues, which explains its lack of peripheral anti-inflammatory effects.14,15 Despite advances in research, the exact mechanism of acetaminophen’s action remains unclear as of 2025. It may involve interaction with a unique COX isozyme (distinct from COX-3), serotonergic pathways, inhibition of nitric oxide synthesis, or modulation of cannabinoid receptors by an active metabolite—or possibly a combination of these mechanisms.16,17 Table 1 describes the different mechanisms of action of oral analgesics currently available in the United States for mild to moderate nociceptive pain, and Table 2 lists examples of how these analgesics can be utilized in a multimodal approach to manage postoperative dental pain.2-4,6,11 The accompanying Box
Table 1. Currently available oral analgesics in the United States for mild to moderate nociceptive pain.
Class and mechanism of action
Nonsteroidal anti-inflammatory drugs: Reversibly inhibit COX-1 and COX-2 enzymes, decreasing the formation of prostaglandin precursors and thereby resulting in antipyretic, analgesic, and anti-inflammatory properties
Subclass Generic (brand) name Usual adult dose Notes
Glucocorticoids: Decrease inflammation by suppression of neutrophil migration, decreased production of inflammatory mediators, and reversal of increased capillary permeability
Nonacidic agent Nabumetone (Relafen)
Oxicam Meloxicam (Mobic)
50-100 mg every 4 h
500 mg once, then 250 mg every 6 h
650 mg every 4-6 h or 1000 mg every 6-8 h
Inhibits prostaglandin synthesis primarily by decreasing activity of the COX-2 enzyme; does not appreciably inhibit COX-1 at therapeutic concentrations.
Mechanism of action is not fully elucidated but may include activation of descending serotonergic inhibitory pathways in the CNS.
500-750 mg every 8-12 h
7.5-15 mg/d
Oxicam Piroxicam (Feldene) 10-20 mg every 12-24 h
Propionic acid Naproxen (Naprosyn, Anaprox, Aleve) 250 mg every 6-8 h; 550 mg every 12 h; or 220 mg every 8-12 h
Salicylic acid derivative Diflunisal (Dolobid) 500 mg every 8-12 h
Atypical opioid: Binds to μ-opioid receptors in the CNS, inhibiting ascending pain pathways and thereby altering the perception of and response to pain; also inhibits the reuptake of norepinephrine and serotonin, which are neurotransmitters involved in the descending inhibitory pain pathway responsible for pain relief
Subclass Generic (brand) name Usual adult dose Notes
Synthetic opioid Tramadol (Ultram)
Opioids: Bind to opioid receptors in the CNS, altering the perception of and response to pain and producing generalized CNS depression
Available in fixed-dose combinations with acetaminophen or celecoxib.
Novel nonopioid analgesics
Selective blocker of the voltagegated sodium channel NaV1.8, which is expressed in peripheral sensory neurons such as dorsal root ganglion neurons
Humanized monoclonal antibodies that block NGF (anti-NGF) and reduce pain and inflammation
Antagonists of the TRPV1 receptor, which is expressed in subsets of nociceptive sensory neurons and plays a major role in both pain transmission and regulation
Semisynthetic opioid Hydromorphone (Dilaudid)
Synthetic opioid Meperidine (Demerol)
Natural opioid Morphine
15-60 mg every 4 h Available in fixed-dose combinations with acetaminophen.
10 mg every 12 h Immediate-release formulations only available in fixed-dose combinations with acetaminophen and ibuprofen.
2 mg every 6-8 h
50 mg every 3-4 h Use should be limited to 48 h or less.
10 mg every 4 h
Semisynthetic opioid Oxycodone (Roxicodone) 5-15 mg every 4-6 h Available in fixed-dose combinations with acetaminophen, aspirin, or ibuprofen.
Approved January 30, 2025, for moderate to severe acute pain in adults.42
Under investigation; these are intravenous therapies
Under investigation; these are intravenous therapies
Abbreviations: CNS, central nervous system; COX-1, cyclooxygenase 1; COX-2, cyclooxygenase 2; NGF, nerve growth factor; TRPV1, transient receptor potential subfamily V member 1.
a Biologic half-life is 8 to 12 hours.
b Biologic half-life is 12 to 36 hours.
cBiologic half-life is 36 to 72 hours.
Table 2. Examples of how these analgesics can be used in a tiered approach to postoperative pain management based on level of anticipated pain.
Approach Drug strategy
First-line therapy (mild to moderate anticipated pain) NSAID or acetaminophen
Consider Glucocorticoid
Second-line therapy (moderate anticipated pain)
Combination of NSAID and acetaminophen
Consider Glucocorticoid
Third-line therapy (moderate to severe anticipated pain)
Combination of NSAID and acetaminophen and glucocorticoid and immediate-release opioid (hydrocodone or oxycodone)
Examples
Ibuprofen 400 mg every 6 h, or naproxen sodium 220 mg every 8-12 h, or celecoxib 200 mg every 12 h or acetaminophen 325-1000 mg every 6-8 h
Consider Dexamethasone 4-8 mg SM or PO, perioperatively
Ibuprofen 400 mg every 6 h, or naproxen sodium 220 mg every 8-12 h, or celecoxib 200 mg every 12 h and acetaminophen 325-1000 mg every 6-8 h
Consider Dexamethasone 4-8 mg SM or PO, perioperatively
Ibuprofen 400 mg every 6 h, or naproxen sodium 220 mg every 8-12 h, or celecoxib 200 mg every 12 h and acetaminophen 325-1000 mg every 6-8 h and dexamethasone 4-8 mg SM or PO, perioperatively and hydrocodone 5 mg/acetaminophen 325 mg every 4-6 h, or oxycodone 5 mg every 4-6 h
provides examples of postoperative regimens for the different anticipated levels of pain: mild, moderate, and severe.2-4,6,11
Nonsteroidal anti-inflammatory drugs
The first nonsteroidal anti-inflammatory drug (NSAID), acetylsalicylic acid—or aspirin—was developed in 1853.18 Since then, many more NSAIDs have been synthesized, with ibuprofen, which was approved for use in the United States in 1974, among the most popular and widely used. All NSAIDs have the same mechanism of action for their therapeutic and adverse effects. They all competitively inhibit both COX-1 and COX-2 in the periphery by blocking arachidonic acid binding, resulting in analgesic, antipyretic, and anti-inflammatory pharmacologic effects.19 While all NSAIDs have the same mechanism of action, they are not created equally. There are very specific differences based on chemical structure and varying affinities for
different COX isoforms, which give some of these molecules distinct advantages in particular clinical situations.18
Glucocorticoids
All glucocorticoids have the same mechanism of action in preventing or suppressing inflammation and the immune response. They primarily exert their action on the CNS rather than at the site of injury or treatment.20-22 At the molecular level, unbound glucocorticoids readily cross cell membranes and bind with high affinity to specific cytoplasmic receptors. This binding triggers a response by altering transcription, which leads to the production of proteins that suppress inflammation and affect various metabolic processes, resulting in clinical benefits such as reduced pain and inflammation, management of inflammatory conditions, and prevention of postoperative nausea and vomiting. The degree of clinical effect is related to the dose administered. The anti-inflammatory actions
of glucocorticoids are thought to involve phospholipase A2 inhibitory proteins, collectively called lipocortins. Lipocortins, in turn, control the biosynthesis of potent mediators of inflammation, such as leukotrienes and prostaglandins, by inhibiting the release of the precursor molecule arachidonic acid.
Tramadol
According to the original product monograph, tramadol is a centrally acting analgesic agent that is a synthetic analog of codeine but has a relatively low affinity for opiate receptors.23 For this reason, it was originally marketed as a prescription medication but not classified as a controlled substance by the US Drug Enforcement Agency (DEA). Shortly after its market approval in 1995, however, diversion and abuse of the drug were reported, leading to changes in the product labeling by the US Food and Drug Administration (FDA) and the addition of warnings about its potential
for abuse.23-27 The product monograph now states: “[Tramadol] is an opioid agonist indicated in adults for the management of pain severe enough to require an opioid analgesic and for which alternative treatments are inadequate.”28 Further, the DEA states: “Tramadol is an opioid analgesic and opioid activity is the overriding contributor to its pharmacologic effects. Abuse and adverse events of tramadol are similar to those of other opioid analgesics.”23 As of 2014, tramadol is classified as a schedule IV medication under the Controlled Substances Act.24
Tramadol has a unique dual mechanism of pain relief.29 It has central opioid receptor agonist activity and exerts an analgesic effect through binding of the parent drug and the O-desmethyltramadol metabolite (M1) to μ-receptors.29-31 The relative analgesic contributions of tramadol and M1 are dependent on the plasma concentrations of each compound. The affinity of tramadol for μ-receptors is 10 times less than that of codeine, 60 times less than that of propoxyphene, and 6000 times less than that of morphine. The M1 metabolite has a 4- to 200-times greater affinity for the µ-receptor than tramadol.29-31
Tramadol also inhibits the reuptake of norepinephrine and serotonin, thus increasing the concentrations of these 2 neurotransmitters in the CNS.32 Since endogenous norepinephrine and serotonin are involved in pain modulation, they may also mediate the analgesic effect of tramadol.
Opioids
The 3 classic opioid receptor types, μ, δ, and κ, have been studied extensively.33 The more recently discovered N/OFQ receptor, initially called the opioid-receptor-like 1 (ORL-1) or orphan opioid receptor, has added a new dimension to the study of opioids.34 Each major opioid receptor has a unique anatomical distribution in the brain, spinal cord, and periphery, and these distinctive localization patterns suggest possible functions that have subsequently been investigated in pharmacologic and behavioral studies.34,35
Morphine and most other clinically used opioid agonists exert their CNS effects through μ-receptor stimulation. These drugs affect a wide range of
Box. Examples of postoperative regimens for mild, moderate, and severe levels of anticipated pain.
Mild
• Recommendation to the patient: 2 OTC 200-mg ibuprofen tablets or 2 OTC 325-mg acetaminophen tablets taken every 6 h around the clock.
• Inform the patient you will check on them via phone or text in 24 h to assess the pain control and to decide if any alterations to the analgesic plan are warranted.
• An alternative NSAID, such as naproxen sodium 220 mg, could be used. The directions would then be: take 2 tablets (440 mg) as soon as possible, then take 1 tablet (220 mg) every 12 h thereafter.
Moderate
• Immediately postoperative, before patient dismissal: Dexamethasone 4 mg injected submucosally into the previously anesthetized area. Oral dexamethasone could also be used at the same dose. Oral dexamethasone can be administered in the office, or a prescription can be written.
• Recommendation to the patient: 2 OTC 200-mg ibuprofen tablets and 2 OTC 325-mg acetaminophen tablets taken every 6 h around the clock.
• Inform the patient you will check on them via phone or text in 24 h to assess the pain control and to decide if any alterations to the analgesic plan are warranted.
Severe
• Immediately postoperative, before patient dismissal: Dexamethasone 4-8 mg injected submucosally into the previously anesthetized area. Oral dexamethasone could also be used at the same dose. Oral dexamethasone can be administered in the office, or a prescription can be written.
• Recommendation to the patient: 2-3 OTC 200-mg ibuprofen tablets and 2 OTC 500-mg acetaminophen tablets taken every 6 h around the clock.
• Prescribe hydrocodone 5 mg or oxycodone 5 mg every 6 h as needed for breakthrough pain.
• Inform the patient you will check on them via phone or text in 24 h to assess the pain control and to decide if any alterations to the analgesic plan are warranted.
Abbreviations: NSAID, nonsteroidal anti-inflammatory drug; OTC, over-the-counter. All examples assume the patient has no contraindications to ibuprofen, naproxen sodium, acetaminophen, or dexamethasone.
physiologic systems to produce analgesia, affect mood and reward behavior, and alter respiratory, cardiovascular, gastrointestinal, and neuroendocrine function.
The δ-receptor agonists are also potent analgesics in animals and in some cases have proved useful in humans.36Agonists selective for κ-receptors produce analgesia that, in animals, has been shown to be mediated primarily at spinal sites.37
Opioid analgesics provide symptomatic relief of pain, but unlike the mechanism of action of peripheral analgesics such as NSAIDs, the underlying disease remains. Because dental pain is primarily due to inflammation, opioids are not considered first-line agents in the management of dental pain since they do not directly
address the underlying pathophysiology. In addition, clinicians must weigh the benefits of opioid pain relief against any potential risk to the patient, including analgesic tolerance, respiratory depression, addiction and physical dependence, constipation, nausea and vomiting, and other adverse effects.38
Novel nonopioid analgesics
Emerging nonopioid pain management therapeutics focus on 3 promising classes of mechanism-specific therapeutics: selective sodium channel blockers, nerve growth factor (NGF) monoclonal antibodies, and transient receptor potential subfamily V member 1 (TRPV1) antagonists. 39
Selective sodium channel blockers
On January 30, 2025, the FDA approved suzetrigine (Journavx) for the treatment of moderate to severe acute pain in adults. Suzetrigine is an orally administered first-in-class selective antagonist of the Nav1.8 voltage-gated sodium channel that propagates pain signals.40,41 By inhibiting Nav1.8, found only in the peripheral nervous system, suzetrigine produces analgesia by blocking pain signal transmission to the CNS. In contrast to opioids, suzetrigine has not been shown to have the potential for dependency or addiction.
NGF monoclonal antibodies
NGF is a neurotrophic factor associated with pain signal transduction and nociceptor receptor gene expression.42 After tissue injury or inflammation, NGF is released and binds to tropomyosin receptor kinase (Trk) A, which can lead to central sensitization, induce the expression of peripheral– and central pain–related substances, and make adjacent pain-sensing neurons sensitive to inflammation, thereby mediating pain.43-45 The expression of NGF is significantly increased at the site of trauma and inflammation.46 Inhibition of NGF binding to its receptor can downregulate NGF expression, thus alleviating pain.
The efficacy and safety of anti-NGF monoclonal antibodies vs placebo in the treatment of osteoarthritis have been reported in systematic reviews, and the curative effect of anti-NGF monoclonal antibodies has been affirmed.47 However, a systematic review of the safety and efficacy of anti-NGF monoclonal antibodies compared to analgesic drugs such as NSAIDs and oxycodone is lacking. Whether anti-NGF monoclonal antibodies are superior to analgesic drugs is unknown. In addition, given the safety profile, the FDA has mandated that anti-NGF monoclonal antibodies and NSAIDs should not be used in combination and has called for more research on anti-NGF monoclonal antibodies at lower doses.48,49
TRPV1 antagonists
The TRPV1 receptor is expressed in subsets of nociceptive sensory neurons and plays a major role in both
pain transmission and regulation. 50 TRPV1 is predominantly expressed in the neurons of the peripheral nervous system in small- and medium-diameter nociceptive neurons in the dorsal root, nodose, sympathetic, and trigeminal ganglia. This receptor is involved in both inflammatory and neuropathic pain pathways, making it a key target in the development of novel pain therapies. One recent study on patients with knee inflammation found this to be a rational target to modulate activity at the origin of the pain pathway in knee osteoarthritis, and it may avoid the systemic side effects seen with currently available analgesics. 51
TRPV1 antagonists are being investigated across various formulations and pain management settings given their demonstrated ability to increase heat pain detection thresholds, reduce acid pain sensitivity, reduce postoperative ocular pain, and lessen the severity of dermatitis symptoms, all while maintaining a relatively favorable safety profile. However, despite these encouraging results, further phase III trials are needed to establish their long-term efficacy and safety in broader patient populations, such as the dental realm.
Clinical implications of multimodal analgesia therapy
The various classes of oral analgesics commonly used in dental pain management can be differentiated by their unique mechanisms of action, all of which target the underlying pathophysiology of dental pain. These mechanisms, with a shared target response, support the concept of a multimodal approach to pain management. The synergy created by combining analgesics with different mechanisms can produce effects greater than the expected additive effect of each drug alone. Synergism has additional clinical safety implications in multimodal analgesia therapy while maximizing the therapeutic effects of the medications involved. For example, using standard doses of ibuprofen and acetaminophen can enhance their combined effects while minimizing the potential adverse reactions found with high doses of either drug alone.
Conclusion
Effective pain management has long been hindered by the risks and limitations associated with opioid analgesics, necessitating the exploration of novel, nonopioid alternatives. According to recent pain guidelines published by the CDC and ADA, in most cases, nonnarcotic analgesic regimens potentially leveraging a multimodal approach to pharmacologic synergism (specifically ibuprofen and acetaminophen) should be considered first-line therapy for acute dental pain.2-4
While it is not explicitly covered in this column, clinicians should keep in mind that effective local anesthesia provides both perioperative and immediate postoperative pain relief. For procedures likely to cause moderate to severe pain, the use of long-acting local anesthetics, such as bupivacaine, is recommended in addition to the oral analgesic strategies mentioned in this column.
Three promising classes of mechanism-specific therapeutics may add to our armamentarium in the future: selective sodium channel blockers, NGF monoclonal antibodies, and TRPV1 antagonists. By targeting distinct pathways involved in pain sensation, these therapies aim to provide relief for various pain types, including chronic, inflammatory, and neuropathic pain, with potentially fewer side effects.
Author affiliations
Premier Dental Products Company, Plymouth Meeting, Pennsylvania; Department of Oral and Maxillofacial Surgery, Creighton University School of Dentistry, Omaha, Nebraska; and Division of Oral Diagnosis, Department of Diagnostic Sciences, Rutgers School of Dental Medicine, Newark, New Jersey (Goodchild); Kaufman Hall, a Vizient Company, Pharmacy Advisory Solutions, Irving, Texas; Skaggs School of Pharmacy, University of Montana, Missoula, Montana; School of Dentistry, Oregon Health & Sciences University, Portland, Oregon; and Faculty of Dentistry, University of British Columbia, Vancouver, Canada (Donaldson).
Conflicts of interest
None reported.
Disclaimer
The views expressed in this column are those of the authors and do not necessarily reflect those of their affiliated institutions.
References
1. Porporatti AL, Schroder ÂGD, Lebel A, et al. Prevalence of orofacial and head pain: an umbrella review of systematic reviews. J Oral Facial Pain Headache. 2024;38(3):1-14. doi:10.22514/jofph.2024.022
2. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC Clinical Practice Guideline for Prescribing Opioids for Pain – United States, 2022. MMWR Recomm Rep. 2022;71 (3):1-95. doi:10.15585/mmwr.rr7103a1
3. Carrasco-Labra A, Polk DE, Urquhart O, et al. Evidencebased clinical practice guideline for the pharmacologic management of acute dental pain in children: a report from the American Dental Association Science and Research Institute, the University of Pittsburgh School of Dental Medicine, and the Center for Integrative Global Oral Health at the University of Pennsylvania. J Am Dent Assoc. 2023;154(9): 814.e2-825.e2. doi:10.1016/j.adaj.2023.06.014
4. Carrasco-Labra A, Polk DE, Urquhart O, et al. Evidencebased clinical practice guideline for the pharmacologic management of acute dental pain in adolescents, adults, and older adults: a report from the American Dental Association Science and Research Institute, the University of Pittsburgh, and the University of Pennsylvania. J Am Dent Assoc. 2024;155(2):102.e9-117.e9. doi:10.1016/j. adaj.2023.10.009
5. Kianian S, Bansal J, Lee C, Zhang K, Bergese SD. Perioperative multimodal analgesia: a review of efficacy and safety of the treatment options. APS. 2024;2:9. doi:10.1007/ s44254-023-00043-1
6. Donaldson M, Goodchild JH. Utilizing synergism to maximize therapeutic effects of postoperative analgesics. Gen Dent. 2023;71(1):6-11.
7. Foucquier J, Guedj M. Analysis of drug combinations: current methodological landscape. Pharmacol Res Perspect. 2015;3(3):e00149. doi:10.1002/prp.2.149
8. Greco WR, Bravo G, Parsons JC. The search for synergy: a critical review from a response surface perspective. Pharmacol Rev. 1995;47(2):331-385.
9. Freo U, Ruocco C, Valerio A, Scagnol I, Nisoli E. Paracetamol: a review of guideline recommendations. J Clin Med. 2021;10(15):3420. doi:10.3390/jcm10153420
10. Blyth FM, Briggs AM, Schneider CH, Hoy DG, March LM. The global burden of musculoskeletal pain—where to from here? Am J Public Health. 2019;109(1):35-40. doi:10.2105/AJPH.2018.304747
11. Qaseem A, McLean RM, O’Gurek D, et al. Nonpharmacologic and pharmacologic management of acute pain from non-low back, musculoskeletal injuries in adults: a clinical guideline from the American College of Physicians and American Academy of Family Physicians. Ann Intern Med 2020;173(9):739-748. doi:10.7326/M19-3602
12. Wongrakpanich S, Wongrakpanich A, Melhado K, Rangaswami J. A comprehensive review of non-steroidal anti-inflammatory drug use in the elderly. Aging Dis 2018;9(1):143-150. doi:10.14336/AD.2017.0306
13. Donaldson M, Goodchild JH. Acetaminophen: how safe is it? Gen Dent. 2022;70(2):9-13.
14. Hashimoto R, Suto M, Tsuji M, et al. Use of antipyretics for preventing febrile seizure recurrence in children: a systematic review and meta-analysis. Eur J Pediatr 2021;180(4):987-997. doi:10.1007/s00431-020-03845-8
15. Moore RA, Moore N. Paracetamol and pain: the kiloton problem. Eur J Hosp Pharm. 2016;23(4):187-188. doi:10.1136/ejhpharm-2016-000952
In: Dowd FJ, Johnson BS, Mariotti AJ, eds. Pharmacology and Therapeutics for Dentistry. 7th ed. Mosby Elsevier; 2011:257-276.
17. Tylenol Professional. Resources. Accessed March 27, 2025. https://www.tylenolprofessional.com/resource-library
18. Donaldson M, Goodchild JH. Not all nonsteroidal antiinflammatory drugs are created equally. Gen Dent 2019;67(6):12-18.
19. Theken KN. Variability in analgesic response to non-steroidal anti-inflammatory drugs. Prostaglandins Other Lipid Mediat. 2018;139:63-70. doi:10.1016/j.prostaglandins.2018.10.005
20. Addison T. Anaemia—disease of the suprarenal capsules. London Med Gazette. 1849;43(8):517-518.
21. Schimmer BP, Funder JW. Adrenocorticotropic hormone; adrenocortical steroids and their synthetic analogs; inhibitors of the synthesis and actions of adrenocortical hormones. In: Brunton LL, Hilal-Dandan R, Knollmann BC, eds. Goodman & Gilman’s: The Pharmacological Basis of Therapeutics. 13th ed. McGraw-Hill Medical; 2018:15871612.
22. McKay LI, Cidlowski JA. Physiologic and pharmacologic effects of corticosteroids. In: Kufe DW, Pollock RE, Weichselbaum RR, et al, eds. Holland-Frei Cancer Medicine 6th ed. BC Decker; 2003.
23. Drug Enforcement Administration. Diversion Control Division. Drug & Chemical Evaluation Section. Tramadol (Trade Names: Ultram™, Ultracet™). March 2020. Accessed March 1, 2025. https://www.deadiversion.usdoj.gov/drug_ chem_info/tramadol.pdf
24. Drug Enforcement Administration, Department of Justice. Schedule of controlled substances: placement of tramadol into schedule IV. Final rule. Fed Regist 2014;79(127):37623-37630.
25. Liu ZM, Zhou WH, Lian Z, et al. Drug dependence and abuse potential of tramadol. Zhongguo Yao Li Xue Bao 1999;20(1):52-54.
27. Goeringer KE, Logan BK, Christian GD. Identification of tramadol and its metabolites in blood from drug-related deaths and drug-impaired drivers. J Anal Toxicol 1997;21(7):529-537. doi:10.1093/jat/21.7.529
28. Janssen Pharmaceuticals. Ultram. Highlights of prescribing information. Updated March 2021. Accessed March 27, 2025. https://www.accessdata.fda.gov/drugsatfda_docs/ label/2021/020281s048lbl.pdf
29. Raffa RB, Friderichs E, Reimann W, Shank RP, Codd EE, Vaught JL. Opioid and nonopioid components independently contribute to the mechanism of action of tramadol, an ‘atypical’ opioid analgesic. J Pharmacol Exp Ther 1992;260(1):275-285.
30. Dayer P, Collart L, Desmeules J. The pharmacology of tramadol. Drugs. 1994;47(Suppl 1):3-7.
doi:10.2165/00003495-199400471-00003
31. Kayser V, Besson JM, Guilbaud G. Evidence for a noradrenergic component in the antinociceptive effect of the analgesic agent tramadol in an animal model of clinical pain, the arthritic rat. Eur J Pharmacol. 1992;224(1):83-88. doi:10.1016/0014-2999(92)94822-d
32. Lee CR, McTavish D, Sorkin EM. Tramadol. A preliminary review of its pharmacodynamic and pharmacokinetic properties, and therapeutic potential in acute and chronic pain states. Drugs. 1993;46(2):313-340. doi:10.2165/00003495-199346020-00008
33. Waldhoer M, Bartlett SE, Whistler JL. Opioid receptors. Annu Rev Biochem. 2004;73:953-990. doi:10.1146/ annurev.biochem.73.011303.073940
34. Neal CR Jr, Mansour A, Reinscheid R, et al. Opioid receptorlike (ORL1) receptor distribution in the rat central nervous system: comparison of ORL1 receptor mRNA expression with (125)I-[(14)Tyr]-orphanin FQ binding. J Comp Neurol. 1999;412(4):563-605.
35. Mansour A, Khachaturian H, Lewis ME, Akil H, Watson SJ. Anatomy of CNS opioid receptors. Trends Neurosci 1988;11(7):308-314. doi:10.1016/0166-2236(88)90093-8
36. Moulin DE, Max MB, Kaiko RF, et al. The analgesic efficacy of intrathecal D-Ala2-D-Leu5-enkephalin in cancer patients with chronic pain. Pain. 1985;23(3):213-221. doi:10.1016/3959(85)90099-5
37. Pfeiffer A, Brantl V, Herz A, Emrich HM. Psychotomimesis mediated by kappa opiate receptors. Science 1986;233(4765):774-776. doi:10.1126/science.3016896
38. Paul AK, Smith CM, Rahmatullah M, et al. Opioid analgesia and opioid-induced adverse effects: a review. Pharmaceuticals (Basel). 2021;14(11):1091. doi:10.3390/ph14111091
39. Pulskamp TG, Johnson LM, Berlau DJ. Novel non-opioid analgesics in pain management. Pain Manag. 2024;14 (12):641-651. doi:10.1080/17581869.2024.2442292
40. Food and Drug Administration (FDA). FDA approves novel non-opioid treatment for moderate to severe acute pain. News release. January 30, 2025. Accessed March 27, 2025. https://www.fda.gov/news-events/press-announcements/ fda-approves-novel-non-opioid-treatment-moderatesevere-acute-pain
41. Osteen JD, Immani S, Tapley TL, et al. Pharmacology and mechanism of action of suzetrigine, a potent and selective Nav1.8 pain signal inhibitor for the treatment of moderate to severe pain. Pain Ther. 2025;14(2):655-674. doi:10.1007/s40122-024-00697-0
42. Mantyh PW, Koltzenburg M, Mendell LM, Tive L, Shelton DL. Antagonism of nerve growth factor-TrkA signaling and the relief of pain. Anesthesiology. 2011;115(1):189-204. doi:10.1097/ALN.0b013e31821b1ac5
43. Bannwarth B, Kostine M. Targeting nerve growth factor (NGF) for pain management: what does the future hold for NGF antagonists? Drugs. 2014;74(6):619-626. doi:10.1007/s40265-014-0208-6
44. Eskander MA, Ruparel S, Green DP, et al. Persistent nociception triggered by nerve growth factor (NGF) is mediated by TRPV1 and oxidative mechanisms. J Neurosci 2015;35(22):8593-8603. doi:10.1523/JNEUROSCI. 3993-14-2015
45. Cohen SP, Mao J. Neuropathic pain: mechanisms and their clinical implications. BMJ. 2014;348:f7656. doi:10.1136/ bmj.f7656. Erratum: 2014;348:g2323.
46. Hefti FF, Rosenthal A, Walicke PA, et al. Novel class of pain drugs based on antagonism of NGF. Trends Pharmacol Sci 2006;27(2):85-91. doi:10.1016/j.tips.2005.12.001
47. Zhao D, Zeng LF, Liang GH, et al. Does anti-nerve growth factor monoclonal antibody treatment have the potential to replace nonsteroidal anti-inflammatory drugs and opioids in treating hip or knee osteoarthritis? A systematic review of randomized controlled trials. EFORT Open Rev 2022;7(7):470-480. doi:10.1530/EOR-21-0103
49. Hochberg MC, Tive LA, Abramson SB, et al. When is osteonecrosis not osteonecrosis?: adjudication of reported serious adverse joint events in the tanezumab clinical development program. Arthritis Rheumatol. 2016;68(2):382-391. doi:10.1002/art.39492
50. Mickle AD, Shepherd AJ, Mohapatra DP. Sensory TRP channels: the key transducers of nociception and pain. Prog Mol Biol Transl Sci. 2015;131:73-118. doi:10.1016/ bs.pmbts.2015.01.002
51. Mobasheri A, Rannou F, Ivanavicius S, Conaghan PG. Targeting the TRPV1 pain pathway in osteoarthritis of the knee. Expert Opin Ther Targets. 2024;28(10):843-856. doi: 10.1080/14728222.2024.2416961
Surgical and prosthetic criteria for selecting prefabricated vs custom implant abutments
Gary Greenstein, DDS, MS ¢ Sultan Albeshri, BDS, MS, FRCD(C)
Ahmad Majeed-Saidan, BDS, MSD, FRCD(C), FACP
The abutment is an integral part of a prosthetic dental implant restoration. Both prefabricated and custom abutments aim to ensure proper gingival contours, maximum crown retention, proper emergence profiles, and the desired subgingival depth of the crown margins. To achieve good outcomes, abutment selection must be guided by biologic and prosthetic principles. In this narrative review, the dental literature was searched for articles addressing criteria used to select dental implant abutments. The literature indicates that both prefabricated and custom abutments can be used to enhance restorative therapy. A variety of clinical scenarios that cannot be resolved with prefabricated abutments (eg, excessive interocclusal space) can be managed with custom abutments. Technological advancements, such as computer-aided design/ computer-aided manufacturing, can help attain clinical benefits usually accomplished with traditionally made custom abutments. The review identified 15 surgical and prosthetic criteria that can be used to guide the selection of prefabricated vs custom dental implant abutments: implant position, implant angulation, sink depth, emergence profile, collar height, peri-implant crevicular depth, esthetics, restorative margin location, cement removal, running room, diameter parity or disparity, tissue sculpting, retention and resistance forms, interocclusal space, and gingival phenotype. Careful consideration of these factors will promote gingival health around a restoration, enhance esthetics, preclude food entrapment, and facilitate oral hygiene for the patient.
The dental implant abutment is a prosthetic component that links the implant to the restoration; it is the structural part of the implant prosthesis, providing retention, stability, support, and the optimal location for the implant restoration. The abutment is usually engaged by a screw, but other options for abutment retention include a locking taper or a 1-piece implant in which the abutment is part of the implant (often found with mini implants).1 In other cases, the abutment is incorporated in the crown, and this prosthetic construct is attached directly to the implant with a screw.
Different types of definitive implant abutments are available: prefabricated, custom, and computer-aided design/computeraided manufacturing (CAD/CAM) abutments. Prefabricated abutments are often referred to as stock abutments and are created by an implant manufacturer. In contrast, traditional custom abutments are designed and made in a dental laboratory to manage a variety of clinical scenarios for which stock abutments are not suitable (eg, excessive interocclusal space). Increasingly, CAD/CAM technology is used to fabricate custom abutments or to aid in customizing the emergence profile of titanium base abutments.2,3
In this review, CAD/CAM abutments will be considered custom made, although the fabrication processes are somewhat different from those of other custom abutments. In traditional fabrication of custom abutments, a master cast is generated and a wax-up of the abutment is performed, after which the abutment is produced by casting or copy milling. CAD/CAM production of abutments involves 3 consecutive steps: scanning (data acquisition), performed either intraorally or using the master cast; CAD modeling; and CAM production.4 The operator takes a virtual impression by using an optical camera to create a 3-dimensional image that is then imported into a software program. The software is used to produce a computer-generated cast, design the restoration, and guide milling of the abutment.5
CAD/CAM abutments provide the advantages of custom abutments but can be manufactured less expensively. Numerous CAD/CAM systems are available for this purpose, including NobelProcera (Nobel Biocare), BellaTek Encode (ZimVie), CARES (Straumann), and Atlantis (Dentsply Sirona).1
Both prefabricated and custom abutments have benefits and limitations (Box 1). Prefabricated abutments are less costly than custom abutments, can be modified to some extent, and come in a variety of specific heights and collar sizes. However, there are clinical situations that require custom abutments because the stock abutments available may not accommodate specific prosthetic requirements: if there is too much interocclusal space that cannot be managed with a prefabricated
Box 1. Benefits and limitations of prefabricated and custom abutments.
Prefabricated abutments
Benefits
• Can be ordered in advance
• Can be retained in inventory
• Can be used with a direct chairside procedure (prepared in mouth) or an indirect laboratory procedure (implantlevel master cast)
• Usually less costly
Limitations
• May not provide sizes and geometric shapes required in individual cases
• May increase the possibility of incomplete removal of excess cement
Custom abutmentsa
Benefit
• Offer greater availability of sizes and shapes
Limitations
• Increase the turnover time from dental laboratory or milling facility
• Are more costly
a Includes abutments fabricated via computer-aided design/computer-aided manufacturing.
Box 2. Criteria to consider during abutment selection.
• Implant position
• Implant angulation
• Sink depth
• Emergence profile
• Collar height
• Peri-implant crevicular depth
• Esthetics
• Restorative margin location
• Cement removal
• Running room
• Diameter parity or disparity
• Tissue sculpting
• Retention and resistance forms
• Interocclusal space
• Gingival phenotype
abutment; when an angulation correction greater than 25° is required; if a collar height that is greater than that available from the manufacturer is needed; or to create an emergence profile that reflects the cross-sectional profile of the prosthetic tooth.
Various materials can be used to fabricate permanent dental implant abutments, including titanium, nonprecious metals, gold, zirconia, and aluminum oxide–based ceramics.6,7 Abutments are typically made of titanium, but other materials, such as zirconia, may be more advantageous in the esthetic zone because they have a color similar to natural teeth and avoid the grayish gingival hue that may be caused by titanium abutments.6,8 Zirconia abutments often have a metal base to reduce stress fractures.9
Abutments can be characterized as permanent or temporary (provisional) prosthetic components. Temporary abutments, also called implant cylinders, are usually prefabricated and are made of plastic (polyetheretherketone) or metal (titanium).10 Temporary abutments include impression abutments (copings), healing abutments, and abutments used to support provisional prostheses. Healing abutments are employed to cover implant platforms after surgical implantation to preclude soft tissue growth onto the implant platforms. In addition, temporary abutments can be used to sculpt the soft tissues prior to definitive restoration placement.11
Abutments can connect to the implant platform with an internal or external connection. These antirotational features resist rotation between the abutment and the implant. External connections usually take the form of an external hexagon on the implant platform, whereas internal connections can be internal hexagons, internal octagons, or Morse taper connections.12 The osseointegrated implant and the prosthetic abutment are joined by a screw; therefore, this connection is called a screw joint. Both internal and external connections can be effectively used in prosthetic rehabilitation.13,14 However, internal connections are now employed more often because they have been found to reduce the incidence of prosthetic complications (eg, screw loosening).15
The various intersecting options for abutment design and fabrication demand a series of decisions during the treatment planning phase. To achieve good outcomes, abutment selection must be guided by biologic and prosthetic principles. Ultimately, abutment selection affects the gingival contour adjacent to the implant restoration, crown esthetics, the apical extent of the final prosthesis, the retention of the restoration, the occlusal relationship with the opposing dentition, and the cost of the prosthetic rehabilitation. This article reviews 15 surgical and prosthetic criteria that should be assessed during selection of prefabricated or custom abutments for cement- or screw-retained dental implant restorations (Box 2).
Criteria for selecting implant abutments
For this narrative literature review related to surgical and prosthetic criteria for selecting abutments, a literature search limited to English-language articles published from 1997 to 2024 was conducted in the PubMed, Ovid, Embase, Dentistry and Oral Sciences Source, and Cochrane Library databases. Articles of interest were identified using the search terms abutment, dental abutments, implant abutments, and dental implant-abutment design with respect to the 15 criteria listed in Box 2. Relevant articles were hand searched to determine whether additional articles could be included in this analysis.
Implant position
In the horizontal plane, the position of the implant platform in the bone is defined by its buccolingual and mesiodistal locations. An implant’s position may be central (in the middle of the future restoration), off-centered but within the body of the crown, or outside (peripheral to) the body of the planned restoration (Fig 1).16 The site of osteotomy development and implant placement can be guided by a surgical guide. The position of the implant needs to be considered when the clinician is choosing between a stock and a custom abutment. For instance, either prefabricated or custom abutments can be employed for centered implants, but implants that are off-centered or in the peripheral zones usually require custom abutments to compensate for positioning issues.
Five types of permanent abutments are commonly used: (1) titanium, which can be either conventional prefabricated abutments utilized with cement retention or prefabricated titanium base abutments used with cement or screw retention; (2) custom-milled or CAD/CAM–fabricated titanium; (3) custom cast titanium; (4) prefabricated zirconia; and (5) custom-milled or CAD/CAM–fabricated zirconia. Malpositioned implants usually require custom abutments. Titanium abutments are preferred if an abutment will be
Fig 2. Cross-sectional image of an implant well positioned in the mandibular right second molar site to avoid the submandibular fossa. The implant follows an angled trajectory to avoid the need for a bone graft in the area indicated by the blue oval.
Fig 1. Occlusal views of implant positions. A. Dental implant positioned within the central zone of the proposed restoration. B. Implant in the mandibular left second premolar site placed lingually (peripheral zone, outside the planned restorative dimensions of the premolar) to avoid injury to the mental nerve. This position will require alteration in the typical lingual dimension of the prosthetic tooth and utilization of a custom abutment.
subjected to strong occlusal forces due to implant malpositioning.17 These are custom milled or cast. Zirconia abutments are usually avoided in areas subjected to heavy occlusal stress because they are more prone to fracture than titanium abutments. However, as previously mentioned, in the esthetic zone, use of a zirconia abutment or a pink abutment may be considered to avoid discoloration of the peri-implant mucosa, particularly if the gingiva is thin.18,19
Implant angulation
Implant angulation is established by the course of the osteotomy and the path the implant takes when it is placed in the bone. An angled trajectory may be selected to avoid anatomical structures, such as dilacerated roots, or to ensure that an implant remains within the alveolar ridge (Fig 2).20 When an implant is placed at an angle due to anatomical considerations, a prefabricated, angulated, or custom abutment can be used to readjust the trajectory of the abutment to accommodate the patient’s occlusion.
Angulated abutments can be prefabricated or custom made in the case of minor (< 15°) or moderate (15° to 25°) angulations. If an extremely angulated abutment (> 25°) is required, then a custom abutment will usually be needed because suitable stock abutments are not available. A 15° angulated abutment can alter the occlusal aspect of a crown by 1.5 mm, and a 25° angled abutment can change the occlusal relationship by 2.5 mm.20 However, an angulated abutment does not alter the gingival position of a restoration.
The amount of angulation correction impacts the type of abutment that needs to be selected (prefabricated or custom) and the type of material that can be used to fabricate the abutment (usually titanium or zirconia). For example, a prefabricated
abutment can correct angulations up to approximately 25° if it is constructed of titanium and about 15° if it is made of zirconia.21
The sink depth defines the position of the implant platform in the vertical dimension.16 It is a surgical term that denotes the distance from the implant platform to the gingival margin. Prosthetically, the same distance is called the running room Both of these terms denote the space that is available to create a proper emergence profile for the restoration. The emergence profile is the axial contour of the abutment-restoration complex, beginning at the implant-abutment interface (implant platform) and terminating at the level of the restoration (crown margin). Importantly, the sink depth provides a method to compensate for implant misangulation and can be used to conceal prosthetic components. In other words, a deeper sink depth helps develop a better emergence profile for implants that were not ideally placed.
The sink depth will also affect the abutment collar height. The abutment collar is the polished portion at the implantabutment interface that ends at the restorative margin. Prefabricated abutments have collar heights and flares (contours) that are predetermined by the manufacturer (Fig 3). For example, straight abutments have a collar height of 1 to 3 mm.
A custom abutment with a larger collar height can be created to accommodate an implant with a deep sink depth. The collar height should be able to accommodate the esthetic needs, running room, and intrasulcular depth of the restoration.
When a restoration is cemented, the restorative margin coincides with the cement line. The quantity of residual
Fig 3. Prefabricated abutments. A. Abutment with 1-mm collar height (arrow). B. Abutment with 3-mm collar height (arrow).
Fig 4. Implant crown demonstrating correct usage of the available running room, resulting in a gradual and physiologic emergence profile of the restoration. The black line represents the osseous crest.
cement following cementation increases with increasing peri-crevicular depth of a restorative margin.22 Therefore, the sink depth should be as shallow as possible, but as deep as needed to achieve esthetic objectives and optimal crown form. Residual cement can contribute to mucositis and peri-implantitis.23,24
To prevent the cement line from being positioned too far apically, it is necessary to select a collar height that facilitates the desired peri-crevicular depths of the crown margins. In this regard, since prefabricated abutments only have collars with heights up to 3 mm, a sink depth of more than 4 mm will require a custom abutment with a tall collar, based on the premise that the restoration extends 1 mm into the sulcus. If a screw-retained restoration is used, the problem of cement retention is avoided.
Running room and diameter parity/disparity
From an anatomical perspective, the running room is the distance from the peri-implant soft tissue margin to the implant platform. Prosthetically, it is the space available to make the transition from the smaller circular form of the implant platform to the variable cross-sectional cervical shape of the tooth being restored.16 The running room allows for a gradual emergence profile and elimination of abrupt shape changes (Fig 4).
Table. Cross-sectional contours of natural teeth. 25
Tooth
Mandibular incisors
Maxillary incisors
Canines
Premolars
Molars
Shape
Circular or ovoid
Triangular or trapezoidal
Ovoid
Circular or ovoid
Trapezoidal or rectangular
Other terms can be used to describe differences in the crosssectional area between the implant platform and the tooth. Diameter parity indicates that an implant’s diameter is similar in size to that of the tooth being restored. In contrast, when there is diameter disparity, there is a geometric discrepancy between the implant and the tooth’s cross-sectional diameter at the level of the cementoenamel junction. For example, while implant platforms are circular, the cross-sectional shape of natural teeth can be circular, ovoid, triangular, or trapezoidal (Table).25 Thus, in the restorative phase of therapy, a transition is required from the shape of the implant to the larger geometric form of the restored tooth.
Often, a smooth transition from the implant-abutment interface to the margin of the restored tooth cannot be accomplished with a prefabricated implant abutment. If inappropriate prefabricated abutments are selected, the discrepancy in size between the implant and restoration will result in a deficient emergence profile. Therefore, the existence of a diameter disparity between the implant and the future restoration is a critical factor when a prosthesis is planned, and a custom abutment may be required to ensure the best emergence profile for a tooth.
Platform switching
Platform switching refers to the utilization of an abutment that is smaller in diameter than the implant platform.26 This approach results in less bone resorption (approximately 0.5 mm less than if platform switching is not used) because biologic width formation is initiated on the implant platform instead of starting at the level of the bone adjacent to the abutment-implant interface.
Tissue sculpting
Tissue sculpting is the use of pressure generated by the shape of a prosthetic component or prosthesis to modify the soft tissue and develop natural tooth tissue contours.11 Circular prefabricated abutments that are nonflared produce little or no change in the gingival contour coronal to the implant platform. In contrast, prefabricated abutments that are flared or modified (customized) by the clinician or technician facilitate the development of a larger circular soft tissue shape.
Traditionally, when a custom abutment is fabricated by a technician, an additive process is used. For example, custom cast abutments consist of a metal base with a plastic sleeve. The plastic sleeve is “waxed” to the desired cervical shape of
the tooth being restored. As part of this wax-up, collar height is developed, allowing the crown margin (cement line) to be moved to approximately 1.0 to 1.5 mm within the peri-implant crevice. When a custom abutment is needed to accomplish tissue sculpting, CAD/CAM technology offers easier fabrication processes than casting.
Retention and resistance forms
Retention form provides resistance to dislodgment parallel to the path of insertion. In contrast, resistance form refers to the capability to withstand displacement due to forces originating from all other directions (eg, biting and parafunctional forces).27 Every abutment, prefabricated or custom made, has retention and resistance forms that depend on the following factors: length, width, surface area, taper (convergence angle), antirotational flats, and the presence of boxes or grooves (Fig 5). The design of implant abutments can provide many advantages relating to retention and resistance. For example, the taper on a prefabricated or custom abutment is approximately 6°, which a clinician cannot routinely achieve when preparing a tooth.28 This slight, consistent taper of the abutment provides increased crown retention. If the height of an abutment is approximately 4 mm or greater and not overtapered, the retention will be adequate for a restoration. If the interocclusal space is limited and a short abutment is required, boxes or grooves that enhance retention and resistance forms can be incorporated into titanium abutments. When an abutment is less than 4 mm in height, it is necessary to use a screw-retained crown because this abutment size will not provide sufficient crown retention.
Interocclusal space
Interocclusal space is defined as the distance from the top of the implant platform to the tooth in the opposing arch. The dental literature specifies a hierarchy of restorative space needed for different types of implant constructs.29,30 The following are the minimum amounts of vertical space required for implant prostheses: screw-retained fixed prosthesis (implant level), 4 to 5 mm; screw-retained fixed prosthesis (abutment level), 7.5 mm; cement-retained fixed prosthesis, 7 to 8 mm; unsplinted overdenture, 7 mm; bar overdenture, 11 mm; and screw-retained fixed hybrid denture, 15 mm.29,30 Thus, the size of a dental abutment will be dictated by the amount of available restorative space.
The desired distance from the most coronal aspect of an abutment to an opposing tooth is 2 to 3 mm for a porcelain-fusedto-metal crown. This distance is needed to provide space for the crown metal (0.5 mm) and the porcelain (1.5 to 2.0 mm).31 Other materials require less interocclusal space. For example, monolithic zirconia or lithium disilicate crowns (pressed or CAD/ CAM fabricated) need as little as 1 mm of occlusal clearance because no space is needed for a metal understructure.32,33
A distinct disadvantage of prefabricated abutments is the limited selection of heights provided by manufacturers. If the distance from the most coronal aspect of the prefabricated abutment to the opposing arch is large (eg, 5 mm), it would result in excessive interocclusal clearance. In this situation, a custom abutment must be fabricated, because if a large
interocclusal space is filled with more than 2 mm of porcelain, the porcelain will be prone to fracture.32 The total height of CAD/CAM abutments is limited to 12 mm because this is the maximum size of titanium blocks available for milling. Custom cast abutments do not have this size limitation.
Gingival phenotype
The term gingival phenotype refers to the thickness and height of the gingival margins around a crown. Gingiva can also be described as flat or scalloped 34 In prefabricated implant abutments, the level of the circumferential collar that rests on the implant platform is manufactured as straight or contoured. For example, a contoured abutment can satisfy a scalloped gingival architecture without requiring the interproximal cement line to be placed too far subgingivally. A limitation of using prefabricated abutments is the small selection of contours provided by manufacturers. Modifications of straight and contoured abutment components are possible, but alterations must be made with subtractive methods, which restricts the scope of changes. When the abutment periphery requires a pronounced scallop, it is advisable to use a custom solution.
Custom abutments can be milled with the collar at any level. Usually, with custom abutments, the facial margin is placed within the peri-implant crevice (0.5 mm), the interproximal edges of the crown are more coronal, and the lingual margin is at the level of the peri-implant soft tissue.35 Information pertaining to the patient’s clinical situation is transferred to a technician or milling facility by means of a soft tissue master implant cast (analog protocol) or an intraoral scanning device. In general, if there is no gingival recession or alteration of the gingival architecture (interproximal tissue is usually coronal to the facial and lingual gingival margins), then contoured abutments (prefabricated or custom) are required to follow the differing heights of the soft tissue contours. Failure to use contoured abutments results in interproximal crown margins that are deeper into the sulcus than desired.
Proper selection of prefabricated or custom abutments can also avoid potential discoloration of the soft tissue, which is
Fig 5. Abutment modified with labial and distal boxes to enhance both the retention form and, in particular, the resistance form. This design will predictably retain a porcelain-fused-to-metal crown.
caused by metallic abutments. Historically, gingival deformities dictated the need to use pink porcelain to compensate for lack of gingival height, and additional costs were incurred because a custom abutment was needed and pink porcelain was baked into the cervical area. With CAD/CAM methodology, nonmetallic abutments (eg, zirconia) can be custom shaded in the cervical area, a useful asset to the restorative implant armamentarium.
Conclusion
This article reviewed criteria for abutment selection pertaining to implant prostheses and identified 15 factors that clinicians should evaluate when selecting an abutment. During treatment planning, dentists can ensure a well-fitting and esthetic restoration by considering implant position, implant angulation, sink depth, emergence profile, collar height, peri-implant crevicular depth, esthetics, restorative margin location, cement removal, running room, diameter parity, tissue sculpting, retention and resistance forms, interocclusal space, and gingival phenotype. Careful consideration of these factors will promote gingival health around a restoration, enhance esthetics, preclude food entrapment, and facilitate oral hygiene for the patient.
Author affiliations
Department of Periodontology, College of Dental Medicine, Columbia University, New York, New York (Greenstein); Private practice, Freehold, New Jersey (Greenstein); Department of Periodontics and Community Dentistry, College of Dentistry, King Saud University, Riyadh, Saudi Arabia (Albeshri); Private practice, Sijam Dental Clinic, Riyadh, Saudi Arabia (Majeed-Saidan).
Correspondence
Sultan Albeshri, BDS, MS, FRCD(C) (salbeshri@ksu.edu.sa).
Conflicts of interest
None reported.
References
1. Karunagaran S, Paprocki GJ, Wicks R, Markose S. A review of implant abutments—abutment classification to aid prosthetic selection. J Tenn Dent Assoc. 2013;93(2):18-23.
2. Abduo J, Lyons K. Rationale for the use of CAD/CAM technology in implant prosthodontics. Int J Dent. 2013;2013:768121. doi:10.1155/2013/768121
3. Al-Thobity AM. Titanium base abutments in implant prosthodontics: a literature review. Eur J Dent. 2022;16(1):49-55. doi:10.1055/s-0041-1735423
4. Lin WS, Harris BT, Zandinejad A, Morton D. Use of digital data acquisition and CAD/CAM technology for the fabrication of a fixed complete dental prosthesis on dental implants. J Prosthet Dent. 2014;111(1):1-5. doi:10.1016/j.prosdent.2013.04.010
5. Oen KT, Veitz-Keenan A, Spivakovsky S, Wong YJ, Bakarman E, Yip J. CAD/CAM versus traditional indirect methods in the fabrication of inlays, onlays, and crowns. Cochrane Database Syst Rev. 2014;4:CD011063. doi:10.1002/14651858.CD011063
6. Tramontana D. Custom Abutments for Dental Implants, Their Evolution and Uses: A Narrative Review. Master’s thesis. Porto, Portugual: Universidade Fernando Pessoa; 2022:5-6. https:// bdigital.ufp.pt/entities/publication/9d7f967d-48b5-49e1-8ef0-d83a4e7ad52c
7. Shah RM, Aras MA, Chitre V. Implant abutment selection: a literature review. Int J Oral Implantol Clin Res. 2014;5(2):43-49. doi:10.5005/jp-journals-10012-1114
8. Naveau A, Rignon-Bret C, Wulfman C. Zirconia abutments in the anterior region: a systematic review of mechanical and esthetic outcomes. J Prosthet Dent. 2019;121(5):775.e1-781.e1. doi:0.1016/j.prosdent.2018.08.005
9. Sailer I, Sailer T, Stawarczyk B, Jung RE, Hämmerle CH. In vitro study of the influence of the type of connection on the fracture load of zirconia abutments with internal and external implant-abutment connections. Int J Oral Maxillofac Implants. 2009;24(5):850-858.
10. Labban N. Use of temporary abutment to assess implant osseointegration before final impression: a case report. Clin Case Rep. 2021;9(12):e05159. doi:10.1002/ccr3.5159
11. Zamzok J. Nonsurgical soft tissue sculpting. Alpha Omegan. 1997;90(2):65-69.
12. Lemos CAA, Verri FR, Bonfante EA, Santiago Júnior JF, Pellizzer EP. Comparison of external and internal implant-abutment connections for implant supported prostheses. A systematic review and meta-analysis. J Dent. 2018;70:14-22. doi:10.1016/j.jdent.2017.12.001
13. Pera F, Menini M, Bagnasco F, Mussano F, Ambrogio G, Pesce P. Evaluation of internal and external hexagon connections in immediately loaded full-arch rehabilitations: a withinperson randomized split-mouth controlled trial with a 3-year follow-up. Clin Implant Dent Relat Res. 2021;23(4):562-567. doi:10.1111/cid.13029
14. Menini M, Pesce P, Bagnasco F, Carossa M, Mussano F, Pera F. Evaluation of internal and external hexagon connections in immediately loaded full-arch rehabilitations: a within-person randomised split-mouth controlled trial. Int J Oral Implantol (Berl). 2019;12(2):169-179.
15. Gracis S, Michalakis K, Vigolo P, von Steyern PV, Zwahlen M, Sailer I. Internal vs. external connections for abutments/reconstructions: a systematic review. Clin Oral Implants Res. 2012;23(Suppl 6):202-216. doi:10.1111/j.1600-0501.2012.02556.x
16. Cavallaro J, Greenstein G. Prosthodontic complications related to non-optimal dental implant placement. In: Froum S, ed. Dental Implant Complications: Etiology, Prevention, and Treatment. Wiley-Blackwell; 2010:156-171.
17. Zarauz C, Pitta J, Pradies G, Sailer I. Clinical recommendations for implant abutment selection for single-implant reconstructions: customized vs standardized ceramic and metallic solutions. Int J Periodontics Restorative Dent. 2020;40(1):31-37. doi:10.11607/prd.3913
18. Bittner N, Schulze-Späte U, Silva C, et al. Comparison of peri-implant soft tissue color with the use of pink-neck vs gray implants and abutments based on soft tissue thickness: a 6-month follow-up study. Int J Prosthodont. 2020;33(1):29-38. doi:10.11607/ijp.6205
19. Totou D, Naka O, Mehta SB, Banerji S. Esthetic, mechanical, and biological outcomes of various implant abutments for single-tooth replacement in the anterior region: a systematic review of the literature. Int J Implant Dent. 2021;7(1):85. doi:10.1186/s40729-021-00370-7
20. Cavallaro J Jr, Greenstein G. Angled implant abutments: a practical application of available knowledge. J Am Dent Assoc. 2011;142(2):150-158. doi:10.14219/jada.archive.2011.0057
21. Ellakwa A, Raj T, Deeb S, Ronaghi G, Martin FE, Klineberg I. Influence of implant abutment angulations on the fracture resistance of overlaying CAM-milled zirconia single crowns. Aust Dent J. 2011;56(2):132-140. doi:10.1111/j.1834-7819.2011.01314.x
22. Linkevicius T, Vindasiute E, Puisys A, Peciuliene V. The influence of margin location on the amount of undetected cement excess after delivery of cement-retained implant restorations. Clin Oral Implants Res. 2011;22(12):1379-1384. doi:10.1111/j.1600-0501.2010.02119.x
23. Wadhwani C, Rapoport D, La Rosa S, Hess T, Kretschmar S. Radiographic detection and characteristic patterns of residual excess cement associated with cement-retained implant restorations: a clinical report. J Prosthet Dent. 2012;107(3):151-157. doi:10.1016/s0022-3913(12)60046-8
24. Korsch M, Obst U, Walther W. Cement-associated peri-implantitis: a retrospective clinical observational study of fixed implant-supported restorations using a methacrylate cement. Clin Oral Implants Res. 2014;25(7):797-802. doi:10.1111/clr.12173
25. Crăciunescu EL, Negruţiu ML, Romînu M, et al. Dental anatomy and morphology of permanent teeth. In: Ardelean LC, Rusu LC, eds. Human Teeth—From Function to Esthetics. IntechOpen; 2023:chap 1. doi:10.5772/intechopen.110223
26. Atieh MA, Ibrahim HM, Atieh AH. Platform switching for marginal bone preservation around dental implants: a systematic review and meta-analysis. J Periodontol. 2010;81(10):13501366. doi:10.1902/jop.2010.100232
27. Owen CP. Factors influencing the retention and resistance of preparations for cast intracoronal restorations. J Prosthet Dent. 1986;55(6):674-677. doi:10.1016/0022-3913(86)90440-3
28. Emms M, Tredwin CJ, Setchell DJ, Moles DR. The effects of abutment wall height, platform size, and screw access channel filling method on resistance to dislodgement of cement-retained, implantsupported restorations. J Prosthodont. 2007;16(1):3-9. doi:10.1111/j.1532-849X.2006.00150.X
29. Carpentieri J, Greenstein G, Cavallaro J. Hierarchy of restorative space required for different types of dental implant prostheses. J Am Dent Assoc. 2019;150(8):695-706. doi:10.1016/j. adaj.2019.04.015
30. Sadowsky SJ. Treatment considerations for maxillary implant overdentures: a systematic review. J Prosthet Dent. 2007;97(6):340-348. doi:10.1016/S0022-3913(07)60022-5
31. Dozíc, A Kleverlaan CJ, Meegdes M, van der Zel J, Feilzer AJ. The influence of porcelain thickness on the final shade of ceramic restorations. J Prosthet Dent. 2003;90(6):563-570. doi:10.1016/s0022-3913(03)00517-1
32. Shirakura A, Lee H, Geminiani A, Ercoli C, Feng C. The influence of veneering porcelain thickness of all-ceramic and metal ceramic crowns on failure resistance after cyclic loading. J Prosthet Dent. 2009;101(2):119-127. doi:10.1016/S0022-3913(09)60006-8
33. Lan TH, Liu PH, Chou M, et al. Fracture resistance of monolithic zirconia crowns with different occlusal thicknesses in implant prostheses. J Prosthet Dent. 2016;115(1):76-83. doi:10.1016/j.prosdent.2015.06.021
34. De Rouck T, Eghbali R, Collys K, De Bruyn H, Cosyn J. The gingival biotype revisited: transparency of the periodontal probe through the gingival margin as a method to discriminate thin from thick gingiva. J Clin Periodontol. 2009;36(5):428-433. doi:10.1111/j.1600-051X.2009.01398.X
35. Schoenbaum TR. Implant prosthetics in the aesthetic zone: science, protocol, and technique. Webinar. April 17, 2015. Accessed March 20, 2025. http://kerncountyds.org/wp-content/ uploads/2015/04/The-Art-Science-of-Aesthetic-Implant-Restorations-Handout.pdf.
GENERAL DENTISTRY SELF-INSTRUCTION
Exercise No. GD545, 2 CE Credits
Fixed Prosthodontics
Subject Code: 610
The 15 questions for this exercise are based on the article “Surgical and prosthetic criteria for selecting prefabricated vs custom implant abutments” on pages 20-26. This exercise was developed by Daniel S. Geare, DMD, in association with the General Dentistry SelfInstruction Committee.
Reading the article and successfully completing this exercise will enable you to understand:
• the criteria for choosing a dental implant abutment;
• the different applications of prefabricated and custom abutments; and
• the restorative requirements for various implant designs.
Answers must be submitted online at agd.org/self-instruction by April 30, 2026.
1. The general objectives for abutments include all of the following except one. Which is the exception?
A. ensure proper gingival contours
B. maximize crown retention
C. ensure accurate interproximal contacts
D. establish proper emergence profiles
2. A dental implant abutment provides all of the following for a restoration except one. Which is the exception?
A. retention
B. stability
C. occlusion
D. support
3. Stock abutments are indicated for all of the following except one. Which is the exception?
A. excessive interocclusal space
B. cemented crowns
C. titanium crowns
D. increased occlusal stress
4. Computer-aided design/computer-aided manufacturing (CAD/CAM) of custom abutments includes all of the following steps except one. Which is the exception?
A. scanning
B. wax-up design of master cast
C. CAD modeling
D. CAM production
5. Prefabricated abutments are the same cost as custom abutments. Prefabricated abutments can be modified to some extent and come in a variety of specific heights and collar sizes.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
6. Antirotational shapes of internal connection implant abutments include ________.
A. parallel cylinders
B. pyramids
C. octagons
D. external hexagons
7. Implants that are placed in the peripheral zone require ________.
A. additional bone grafts
B. special stock abutments
C. custom abutments
D. additional healing time
8. A 15° angulated custom abutment can alter the occlusal aspect of a crown by ___________.
A. 1.5 mm
B. 2.5 mm
C. creating occlusal interferences
D. compromising the contact areas
9. Sink depth is defined as the ________.
A. distance of the platform to the bony crest
B. penetration depth of the pilot drill
C. distance the implant is placed in the preparation
D. distance from the platform to the gingival margin
10. The quantity of residual cement following cementation decreases with increasing pericrevicular depth. Therefore, sink depth should be as shallow as possible but as deep as needed to achieve esthetic objectives and optimal crown form.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
11. Platform switching refers to ________.
A. the use of an abutment diameter larger than the implant platform
B. results that generate more bone resorption
C. the use of an abutment diameter smaller than the implant platform
D. incorporation of 2 different implant systems
12. Retention and resistance forms depend on all of the following except one. Which is the exception?
A. length
B. placement
C. surface area
D. antirotational flats
13. The minimum interocclusal space needed for a screw-retained implant prosthesis at the level of the abutment is ___ mm.
A. 4 to 5
B. 7.5
C. 11
D. 15
14. The gingival ________ is the thickness and height of the gingiva around a crown.
A. phenotype
B. genotype
C. biotype
D. serotype
15. The facial margin of custom abutment collars is usually placed within the ________.
A. gingival crest
B. coronal margin
C. peri-implant crevice
D. free gingival margin
Effect of mixing tip design on the mechanical properties, porosity, and waste reduction of extra-light–body polyvinyl siloxane impression material
Kaisha T. Calvin, DDS, MS, ABGD ¢ Eric Hu, DMD, MS, FACP ¢ Robert Masterson, DDS, MS, ABGD
The purpose of this study was to compare the tensile strength, modulus of elasticity, porosity, and waste reduction of extra-light–body polyvinyl siloxane (PVS) impression material mixed with a helical impression tip or a new cartridge integrated system (NCIS) from the same manufacturer (Dentsply Sirona). The legacy teal tip (TT group) was compared with the NCIS red (RT group) and blue (BT group) mixing tips. Dumbbell-shaped specimens (TT, n = 17; RT, n = 15; and BT, n = 16) were prepared in accordance with German Institute for Standardization’s rubber testing standard (DIN 53504.2017) and tested in a universal testing machine for tensile strength and modulus of elasticity. Porosity was evaluated via microcomputed tomography of cylindrical specimens (TT, n = 7; RT, n = 6; and BT, n = 7). Waste reduction was evaluated by comparing the mass of the mixing tips before use and after polymerization of the PVS to determine the difference in weight, which represented the amount of retained material (n = 11 per group). Tensile strength was analyzed using 1-way analysis of variance (ANOVA). Modulus of elasticity was analyzed using 1-way ANOVA with Tukey HSD. Porosity and waste reduction were analyzed using Shapiro-Wilk, Kruskal-Wallis, and Steel-Dwass tests. The analyses revealed no differences in tensile strength between groups (P = 0.493). The TT group had a significantly higher modulus of elasticity than the RT and BT groups (P < 0.001). The BT group had the highest mean porosity, and the difference between BT and RT was statistically significant (P = 0.048). The RT group showed the least material waste. Supporting the claims of the manufacturer, the NCIS tips generated tensile strengths comparable to that of the legacy tip and produced less waste, achieving waste reductions of 62% (RT) and 21% (BT) compared with the legacy tip. However, the RT and BT groups had a lower modulus of elasticity than the TT group, and porosity was increased in the BT group.
Digital impressions have many advantages and are being increasingly utilized in the crown fabrication process. However, it is still important to understand and improve conventional impression materials and techniques. Even with advancements in impression materials, no material is 100% accurate.1 Elastomeric impression materials include polysulfides, condensation silicone, polyether, and polyvinyl siloxane (PVS).1 Since its introduction in 1975, PVS, also known as addition silicone, has been a top choice for clinicians for chairside use due to its excellent detail reproduction, elastic recovery from deformation, and polymerization shrinkage of less than 0.05%.2,3 Clinicians can choose PVS materials with less concern about the disadvantages of polyether or polysulfide materials, such as odor, allergic reactions, or locking into undercuts.1,4 PVS impression material comes in a 2-part system that includes a base paste and an accelerator paste containing a catalyst.1,4 A homogenous mixture of the 2 pastes is critical for capturing an accurate impression. There are 3 modes of mixing: hand mixing, static mixing, and dynamic mechanical mixing.4 Static mixing is the most commonly used mode and involves use of a mixing gun to push the pastes from the cartridge into a mixing tip to create a uniform mixture.4 Different sizes of mixing tips are available, and the size is selected based on the viscosity of the PVS and the amount of material needed for the impression.
Regardless of the mixing tip used, a mixture with ideal mechanical properties is desired. These mechanical properties include accuracy, elastic recovery, dimensional stability, hydrophilicity, flowability, viscosity, high tear energy, and tensile strength.5 Tensile strength evaluates the maximum stress the PVS can undergo before failure, while the modulus of elasticity evaluates the rigidity of the material. Both properties are critical in obtaining a deformation-free impression.6 To provide an accurate representation of the intraoral tissues and dentition, the PVS material should be able to withstand stresses from deformation and tearing when removed from the mouth or stone casts.7
While no set criteria for these mechanical properties have been established, the tensile strength of elastomeric impression materials ranged from 1 to 6 MPa in a study by Re et al, with light-body materials having lower tensile strength than medium- and heavy-body materials.7 In a study by Ud Din et al, the modulus of elasticity ranged from 2.6 to 3.5 MPa, while Papadogiannis et al reported a range of 1.8 to 6.5 MPa.8,9 The viscosity of impression materials has been shown in clinical studies to be the most critical consideration for attaining impressions with minimal voids.6 As extra-light–body PVS
materials are prone to an increased number of voids, evaluating the impact of different-size mixing tips can help determine which tip is better suited for materials with this viscosity.
In March 2022, the dental manufacturer Dentsply Sirona issued a news release announcing a new cartridge integrated system (NCIS), which purportedly would result in improved mix quality and a reduction in material waste.10 The manufacturer also stated that the NCIS requires the material to be bled only before the first use rather than before every impression. As a result, they found that waste could be reduced by 64% when comparing the NCIS red mixing tip to the legacy teal mixing tip.10
Few studies in the literature have evaluated the effects of various mixing tip designs and sizes on the resulting impression. The purpose of the present study was to compare the effects of the manufacturer’s legacy helical teal tip (TT) and the NCIS red tip (RT) and blue tip (BT) on the tensile strength, modulus of elasticity, porosity, and waste reduction of extralight–body PVS impression material. The null hypothesis was that there would be no statistically significant differences in tensile strength, modulus of elasticity, porosity, or waste reduction among PVS specimens prepared with these different mixing tips.
Methods
A single operator prepared all PVS specimens (K.T.C.). For all testing, a mixing gun (Dispensing Gun, Dentsply Sirona) was used to extrude extra-light–body PVS material (Aquasil Ultra+, XLV Regular Set, Dentsply Sirona) into the mixing tips. The size of the tips was analyzed as an adjunct to the waste reduction evaluation to identify all key product changes that could contribute to differences.
Testing of tensile strength and modulus of elasticity
A standard tessellation language (STL) file of a type S2 dumbbell-shaped specimen mold meeting the standards of the German Institute for Standardization (DIN 53504.2017-03) was
obtained via an open data repository (Zenodo).11,12 The file was opened, and supports were autogenerated in a print preparation software (PreForm version 3.21.0, Formlabs). A 3D printer (Form3B, Formlabs) was used to print 2 sets of molds on a stainless steel build platform using dental model resin (Model V3 Resin, Formlabs). Once printed, the molds were washed in a resin washing station (Form Wash, Formlabs) filled with 70% isopropyl alcohol for 10 minutes to remove excess resin. The molds were then dried with compressed air and placed in a resin curing station (Form Cure, Formlabs) for 5 minutes at 60°C, and supports were removed with flush cutters after processing was complete.
The molds were secured in a tabletop vise to maintain contact and then used to fabricate dumbbell-shaped specimens for each group via injection molding with the appropriate mixing tip (TT, n = 17; RT, n = 15; or BT, n = 16). The chambers of the NCIS red and blue tips are both cube shaped but have different dimensions, while the legacy teal tip has a helical mixing chamber (Fig 1).
Specimens were removed from the molds after a 7-minute setting time; 2 minutes were added to the 5 minutes recommended by the manufacturer to ensure complete polymerization at room temperature. After excess material was trimmed from the specimens, they were placed in a water bath. The specimens had a thickness of 2.0 ± 0.2 mm, a total length of 75.0 mm, and a bar that was 25.0 mm long (Fig 2). The heads were 12.5 mm wide, and the bar was 4.0 ± 0.5 mm wide.
Specimens were kept in an incubator (Forma Series II WaterJacketed CO2 Incubator, Thermo Fisher Scientific) for 24 hours at 36.9°C to prevent dehydration prior to testing.
At the time of testing, the width and thickness at the narrow portion of each dumbbell-shaped specimen were measured
Fig 1. Impression material mixing tips used in the study: red and blue tips from the new cartridge integrated system (left and center) and a teal tip from the legacy system (right).
Fig 2. Dumbbell-shaped specimen. A. After polymerization in the mold. B. After removal from the mold.
2 times with a digital caliper (EZ CAL IP54, iGaging), and the values were averaged. A stainless steel ruler was then used to mark 2 benchmarks equidistant from the center on each specimen, to indicate where it would be clamped for testing. Specimens were secured between pneumatic clamps in a universal testing machine (Alliance RT/5, MTS Systems) while care was taken to ensure the specimens were not in compression or tension.
The specimens were elongated until failure at a rate of 50 mm/min at 23°C and 50% relative humidity. The tensile strength data were recorded and the modulus of elasticity was calculated with computer software (TW Elite software, MTS Systems). Statistical analysis was completed using 1-way analysis of variance (ANOVA) for both tensile strength and elastic modulus data, with additional use of the Tukey HSD test for analysis of the modulus of elasticity (α = 0.05).
Testing of porosity
A multiwell plate with a flat bottom and lid (Falcon 24-well Clear Multiwell Plate, Corning) was used to make cylindrical specimens. The bottom of each well was removed to allow for easier removal of the specimen after polymerization. Specimens were made with the appropriate tip for each of the 3 groups: TT, n = 7; RT, n = 6; and BT, n = 7.
The PVS was injected into the mold while the mixing tip was held within the dispensed impression material as directed by the manufacturer.13 The lid and a 2-kg weight were placed on the plate, and specimens were removed after 7 minutes. The specimens were approximately 20 mm in height and 16 mm in diameter.
The porosity of the specimens was measured using microcomputed tomography (Skyscan 1172, control program version 1.5, Bruker). Images with a pixel size of 16.94 µm and a rotation step of 0.70° were obtained (Fig 3). The X-ray beam was set at 69 kV and an intensity of 144 µA. Reconstruction software (NRecon, version 2.0.0.5, Bruker) was used to create 900 crosssection slices, and porosity was evaluated using surface rendering and analysis software (CTAn, version 1.20.3.0, Bruker)
(Fig 4). The Shapiro-Wilk, Kruskal-Wallis, and Steel-Dwass tests were used for data analysis.
Testing of waste reduction
The mass (milligrams) of all mixing tips was measured on a scale (Balance XS105, Mettler Toledo) before and after use (n = 11 per group). The second measurement of mass was performed 7 minutes after use of the tip to ensure that polymerization of PVS was complete. The difference in mass before and after use was considered to represent the amount of PVS material retained within the impression tips, which was designated as wasted material. The mean values of the RT and BT groups were compared individually to the mean mass of the TT group to calculate the waste reduction of the NCIS tips.
The Shapiro-Wilk, Kruskal-Wallis, and Steel-Dwass tests were used for analysis of the waste reduction data.
Measurement of tip size
A digital caliper (Dental Digital Caliper, ProDent USA) was used to measure 1 each of the NCIS red and NCIS blue mixing tips, as the dimensions are proprietary and were not provided on request from the manufacturer. The dimensions of the legacy teal tip were obtained from the manufacturer (personal email correspondence, August 8, 2022).
Results
Tensile strength and modulus of elasticity
The groups demonstrated the following mean (SD) tensile strengths: TT, 4.07 (0.22) MPa; BT, 4.02 (0.38) MPa; and RT, 3.95 (0.25) MPa (Chart 1). No statistically significant difference in tensile strength was found among the TT, RT, and BT groups (P = 0.493). The mean (SD) modulus of elasticity values were TT, 3.50 (0.26) MPa; BT, 3.00 (0.09) MPa; and RT, 2.93 (0.13) MPa (Chart 2). The modulus of elasticity of the TT group was significantly higher than those of the RT and BT groups (P < 0.001), but no statistically significant difference was found between the RT and BT groups (P = 0.544).
Fig 3. Cylindrical specimen placed on the microcomputed tomography platform for porosity testing.
Fig 4. Microcomputed tomographic images. A. porosity specimens. B. Mixing tips with polymerized polyvinyl siloxane.
Error bars represent the standard deviation. There were no statistically significant differences between groups (P > 0.05; 1-way analysis of variance).
Porosity
Evaluation with microcomputed tomography revealed the following mean (SD) porosity values: BT, 0.43% (0.34%); TT, 0.22% (0.11%); and RT, 0.18% (0.10%) (Chart 3). The Shapiro-Wilk test indicated that the porosity data for RT (P = 0.435) and TT (P = 0.290) were normally distributed, but those for BT were not (P = 0.013); therefore, the Kruskal-Wallis test was used to determine if there were statistically significant differences between the groups. The Kruskal-Wallis test revealed a significant difference in porosity among the 3 groups (P = 0.031). The Steel-Dwass test was used for pairwise comparisons, and the results showed a significant difference in porosity between the RT and BT groups (P = 0.048) but no significant difference in porosity between the TT and BT groups (P = 0.131) or between the TT and RT groups (P = 0.799).
Waste reduction
Based on the weight of material retained in the tip after use, the mean (SD) material waste values were TT, 2689.41 (16.28) mg; BT, 2116.92 (46.41) mg; and RT, 1014.99 (15.84) mg. The Shapiro-Wilk test showed that the data were normally distributed for the RT (P = 0.066) and BT (P = 0.557) groups but not for the TT (P = 0.016) group; therefore, the Kruskal-Wallis test was performed to examine if there were statistically significant differences in mass among the different groups. After a significant difference was found (P < 0.001), the Steel-Dwass test was used for pairwise comparisons. The analysis showed statistically significant differences in mass between the RT and BT
cartridge integrated system;
Error bars represent the standard deviation. Groups with different letters are significantly different (P < 0.05; Tukey HSD test).
groups, the TT and BT groups, and the TT and RT groups (P < 0.001 for all comparisons) (Chart 4).
Tip size
The legacy teal tip has a mean (SD) diameter of 8.3 (0.20) mm (measured at the neck), an overall length of 88.5 (1.0) mm, and an orifice opening of 4.90 (0.15) mm. As the NCIS tips are cube shaped, the diagonal of the square was found by the following formula: √2 × the length of 1 side, measured at the neck above the wings. Based on a side length of 6.6 mm, the diagonal of the red tip was calculated to be 9.4 mm; the overall length of the tip was 59.5 mm, and the orifice opening was 4.4 mm. Based on a side length of 8.9 mm, the diagonal of the blue tip was calculated to be 12.6 mm; the overall length was 67.7 mm, and the orifice opening was 5.4 mm.
Discussion
This study evaluated the performance characteristics of an extra-light–body PVS used with a redesigned cartridge and NCIS mixing tips to explore the veracity of the manufacturer’s claims that these new tips save material, improve mix quality, and prevent cross contamination.10 The results were mixed, offering only partial support for these claims. The null hypothesis was partially rejected, as there were statistically significant differences in modulus of elasticity, porosity, and waste reduction between 2 different NCIS tips and a legacy helical tip. However, tensile strength was comparable among all 3 groups.
Chart 2. Mean modulus of elasticity of dispensed PVS according to mixing tip design.
Abbreviations: NCIS, new
PVS, polyvinyl siloxane.
Chart 1. Mean tensile strengths of dispensed PVS according to mixing tip design.
Abbreviations: NCIS, new cartridge integrated system; PVS, polyvinyl siloxane.
NCIS red tip NCIS blue tip Legacy teal tip (n = 15) (n = 16) (n = 17)
NCIS red tip NCIS blue tip Legacy teal tip (n = 15) (n = 16) (n = 17)
Abbreviations: NCIS, new cartridge integrated system; PVS, polyvinyl
Error bars represent the standard deviation. Groups with different letters are significantly different (P < 0.05; Steel-Dwass test).
The NCIS mixing cube technology is credited by the manufacturer with improving the mixing quality of the material. There was no significant difference in tensile strength between the groups, but there was a statistically significant difference in the modulus of elasticity between the TT and BT groups and between the TT and RT groups. All modulus of elasticity values were within an acceptable range, consistent with previous studies.8,9 The Glossary of Prosthodontic Terms defines the modulus of elasticity as “a ratio of stress to strain; as the modulus of elasticity rises, the material becomes more rigid.”14 The present study found that the TT group had a higher modulus of elasticity, making specimens in that group more rigid and possibly more able to withstand deformation. This may be due to the longer length of the TT, which could give the material more time to form its cross-linked network, contributing to a stiffer material.9
The results also showed that the BT group had the highest porosity and the RT group the lowest. The mixing cube technology could be introducing air to the mixture due to the larger lumen size on the BT and the low viscosity of the PVS used in the present study. Of note, the manufacturer of the NCIS Aquasil Ultra+ XLV cartridge does state that it should be used with an RT. However, clinicians may want to use a BT with XLV PVS for a monophase or putty-wash technique, where more impression material is needed and a larger tip would be more convenient and efficient. Increased porosity affects the accuracy of impressions and can result in the need for repeated impressions or additional prosthetic adjustments. It is possible that this increase in porosity was due to operator error, as all specimens were prepared by a single operator. However, air pockets could be clearly seen on the microcomputed tomographic images of the BT specimens.
Abbreviations: NCIS, new cartridge integrated system; PVS, polyvinyl siloxane.
The mass of PVS was considered to represent material waste. The percentages indicate the waste reduction in NCIS tips compared with the legacy tip.
Error bars represent the standard deviation. Groups with different lowercase letters are significantly different (P < 0.05; Steel-Dwass test).
The legacy TT was the longest tip (88.5 mm), while the NCIS BT was shorter (67.7 mm) but had the largest diameter (12.8 mm) and the widest orifice (5.38 mm). Despite being shorter, the NCIS tips have an internal cube design that seems to provide an increased surface area for mixing. The mixing mechanism of the NCIS tips also differs from that of conventional mixing tips. Although Xinial, the owner of the design used by Dentsply Sirona, did not disclose how the NCIS tips mix PVS, a similarly designed tip by Medmix, the MIXPAC T-Mixer, works by splitting, squeezing, folding, and stretching the PVS.15 In comparison, the conventional helical mixing tip mixes the pastes by alternating rotating elements, which repeatedly folds the pastes, resulting in a uniform mix.3,4,6,15 Maluly-Proni et al conducted a similar comparison between a helical tip and the new T-mixer tip.3 They found that the new T-Mixer design reduced material waste and resulted in more accurate detail reproduction over time compared with the conventional helical tip. The authors attributed these improvements to the T-mixer’s internal geometry and its ability to compress and elongate the PVS material evenly in a shorter tip.3
The 62% waste reduction of the RT group in the present study supports the manufacturer’s claim that the NCIS RT can reduce waste by up to 64% when compared with the legacy TT.10 Based on the results of the present study, the RT provided the best combination of strength, porosity, and material savings. The BT may perform better with higher-viscosity materials, as recommended by the manufacturer.16
Limitations of this study include its in vitro nature, which does not mimic intraoral conditions, as well as the fact that
Chart 4. Mean mass of PVS retained within the mixing tips after use.
Chart 3. Porosity of dispensed and polymerized PVS according to mixing tip design.
siloxane.
NCIS red tip NCIS blue tip Legacy teal tip (n = 6) (n = 7) (n = 7)
NCIS red tip NCIS blue tip Legacy teal tip (n = 11) (n = 11) (n = 11)
testing was performed by a single clinician. Another limitation was the unavailability of the legacy PVS cartridges, which can no longer be purchased from the manufacturer. This limited the ability to conduct multiple tests with various PVS viscosities for the legacy system.
Conclusion
Within the limitations of this study, the results showed that the tensile strengths of the legacy and NCIS mixing tips were comparable, but the legacy TT had the highest modulus of elasticity. The BT group showed an increase in porosity compared with the TT group, while the RT group demonstrated the least porosity. Both NCIS tips wasted less material than the legacy tip, supporting the claims of the manufacturer.
Author affiliations
2-Year Advanced Education in General Dentistry Residency Program, Fort Cavazos, Texas; Army Postgraduate Dental School, Uniformed Services University of the Health Sciences, San Antonio, Texas.
Correspondence
Eric Hu, DMD, MS, FACP (eric.c.hu.mil@health.mil).
Conflicts of interest
Dentsply Sirona provided the new mixing tips used in the study. The authors report no other potential conflicts of interest.
Funding
This study was funded in part by the Carl R. Darnall Army Medical Center, Fort Cavazos, Texas.
Disclaimer
The identification of specific products, scientific instrumentation, and/or organizations is considered an integral part of the scientific endeavor and does not constitute endorsement or implied endorsement on the part of the authors, Department of Defense, or any component agency. The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Army, Department of the Air Force, Uniformed Services University, Defense Health Agency, Department of Defense, or the US government.
Acknowledgments
The authors would like to thank Dr Fabian Huettig for providing the STL file for the dumbbell-shaped specimen mold; Wen Lien, MS, DMD, MS, and Christopher Raimondi, DDS, MS, MS, of the US Air Force Dental Research & Consultation Service, for assistance with research and data collection; Mathew Frazier, PT, DPT, MS, ATC, and Dawn Beaver, MS,
for support with research protocol submissions; and Ms Sarah Luehring, Dentsply Institutional Account Manager, for providing the new mixing tips for the study.
Meeting presentations
This research was presented as “Effect of mixing tip size on the tensile strength, modulus of elasticity, porosity and waste reduction of extra-light body polyvinyl siloxane impression material” at the 2023 Carl R. Darnall Army Medical Center Research Day on May 18, 2023, and as an e-poster at AGD2024, Minneapolis, on July 17, 2024.
References
1. Gupta R, Brizuela M. Dental impression materials. In: StatPearls. StatPearls Publishing; March 19, 2023. https://www.ncbi.nlm.nih.gov/books/NBK574496/
2. Vrbova R, Bradna P, Bartos M, Roubickova A. The effect of disinfectants on the accuracy, quality, and surface structure of impression materials and gypsum casts: a comparative study using light microscopy, scanning electron microscopy and micro computed tomography. Dent Mater J. 2020;39(3):500-508. doi:10.4012/dmj.2019-065
3. Maluly-Proni AT, Delben JA, Briso ALF, Marson FC, Dos Santos PH. Evaluation of material waste, dimensional stability, and detail reproduction of polyvinyl siloxane impression materials mixed with different mixing tips. J Prosthet Dent. 2022;127(5):759-764. doi:10.1016/j.prosdent.2020.11.024
5. Hamalian TA, Nasr E, Chidiac JJ. Impression materials in fixed prosthodontics: influence of choice on clinical procedure. J Prosthodont. 2011;20(2):153-160. doi:10.1111/j.1532849X.2010.00673.x
7. Re D, De Angelis F, Augusti G, et al. Mechanical properties of elastomeric impression materials: an in vitro comparison. Int J Dent. 2015;2015:428286. doi:10.1155/2015/428286
8. Ud Din S, Chaudhary FA, Ahmed B, et al. Comparison of the hardness of novel experimental vinyl poly siloxane (VPS) impression materials with commercially available ones. Biomed Res Int. 2022;2022:1703869. doi:10.1155/2022/1703869
9. Papadogiannis D, Lakes R, Palaghias G, Papadogiannis Y. Effect of storage time on the viscoelastic properties of elastomeric impression materials. J Prosthodont Res. 2012;56(1):11-18. doi:10.1016/j.jpor.2011.03.002
10. Dentsply Sirona. New cartridge and mixing tip: applying impression material efficiently and easily. News release. March 2022. Accessed March 19, 2025. https://www.dentsplysirona. com/en-us/company/news-and-press-release-detail-page.html/content/dam/master/ news/en/business-units/restorative/2022/new-cartridge-and-mixing-tip-system-applying-impression-materia
11. German Institute for Standardization. DIN 53504:2017-03, Testing of Rubber—Determination of Tensile Strength at Break, Tensile Stress at Yield, Elongation at Break and Stress Values in a Tensile Test. Deutsches Institut für Normung; 2017. doi:10.31030/2607941
12. Mutschler M, Huettig F. Injection-form for a S2 dumbell [sic] specimen acc. DIN 53504:2017 as STL. Version 1. May 14, 2021. Accessed March 19, 2025. https://zenodo.org/ records/4611959
16. Dentsply Sirona. Same great material. Accessed March 31, 2025. https://assets.dentsplysirona.com/master/product-procedure-brand-categories/restorative/product-categories/ indirect-restoration/impression-taking/silicones-vps/ncis-new-catridge-delivery-system/ RES-Insert-Impression-Material-Delivery-System-Change-EN-ML780101F.pdf
GENERAL DENTISTRY SELF-INSTRUCTION
Exercise No. GD546, 2 CE Credits
Restorative Dentistry
Subject Code: 250
The 15 questions for this exercise are based on the article “Effect of mixing tip design on the mechanical properties, porosity, and waste reduction of extra-light–body polyvinyl siloxane impression material” on pages 28-33. This exercise was developed by Millie K. Tannen, DDS, MAGD, in association with the General Dentistry Self-Instruction committee.
Reading the article and successfully completing this exercise will enable you to:
• understand the physical properties and advantages of polyvinyl siloxane (PVS) impression material;
• develop familiarity with the laboratory procedures used to evaluate impression materials; and
• make a scientifically informed decision about the use of the new cartridge integrated system (NCIS) in clinical practice.
Answers must be submitted online at agd.org/self-instruction by April 30, 2026.
1. Advantages of PVS impression material include all of the following except one. Which is the exception?
A. polymerization shrinkage less than 0.01%
B. elastic recovery from deformation
C. less concern for allergic reactions
D. excellent detail reproduction
2. The most common method of mixing PVS is ________ mixing.
A. hand
B. static
C. centrifugal
D. dynamic mechanical
3. The modulus of elasticity evaluates a material’s ________.
A. maximum stress
B. flowability
C. rigidity
D. dimensional stability
4. In a study by Re et al, the tensile strength of elastomeric impression materials ranged from ____ MPa.
A. 1 to 6
B. 2 to 7
C. 4 to 7
D. 6 to 9
5. Light-body elastomeric impression materials have ________ than medium- and heavy-body materials.
A. lower tensile strength
B. lower dimensional stability
C. higher tensile strength
D. higher dimensional stability
6. The most critical consideration for obtaining impressions with minimal voids is ________.
A. tensile strength
B. modulus of elasticity
C. viscosity
D. mode of mixing
7. The manufacturer’s claims for the NCIS include ________.
A. lower modulus of elasticity
B. greater waste reduction
C. fewer allergic reactions
D. improved taste and odor
8. The tensile strength and modulus of elasticity for each type of mixing tip were evaluated by creating ________-shaped specimens.
A. trapezoidal
B. full-arch
C. half-arch
D. dumbbell
9. To test tensile strength and modulus of elasticity, the specimens were elongated until failure at a rate of _____ mm/min.
A. 40
B. 50
C. 60
D. 70
10. To evaluate porosity, bar-shaped specimens were analyzed using microcomputed tomography. Reconstruction software was used to create 400 cross-section slices.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
11. This study demonstrated a statistically significant difference among the 3 mixing tips for all of the following properties except one. Which is the exception?
A. tensile strength
B. modulus of elasticity
C. waste reduction
D. porosity
12. The teal mixing tip resulted in a significantly higher _______ than the red and blue tips.
A. tensile strength
B. dimensional stability
C. viscosity
D. modulus of elasticity
13. The specimens mixed with the teal tip had a higher modulus of elasticity, making them less rigid. This may have been due to the longer length of the teal tip.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
14. The NCIS red and blue tips have a _______ internal design.
A. helical
B. cube-shaped
C. triangular
D. hexagonal
15. Use of the NCIS red tip resulted in a waste reduction of _____% compared with the legacy teal tip.
A. 38
B. 54
C. 62
D. 71
Evaluation of pulp stones in unerupted teeth and their correlation with principal biochemical factors using cone beam computed tomography
Seyed Sasan Aryanezhad, DDS, MSc ¢ S. Marjan Arianezhad, DDS, MSc
Pulp stones result from the calcification of dental pulp tissue. There is limited research on pulp stones in unerupted teeth, but they are more suitable for investigating the influence of systemic factors on pulp stone formation because they are not exposed to the conditions of the oral cavity. The objectives of this cross-sectional descriptive-analytical study were to use cone beam computed tomography (CBCT) to evaluate pulp stones in unerupted teeth and to be the first investigation to assess the correlation between pulp stones and blood levels of principal biochemical factors. The CBCT records of 90 patients were evaluated, and 3 groups were defined based on the size of pulp stones: small pulp stone (including total absence as well as minute particles with maximum diameter < 0.05 mm); moderatesized pulp stone (maximum diameter 0.05-1.59 mm); or large pulp stone (maximum diameter ≥ 1.60 mm). This was followed by assessment of the patients’ blood levels of 5 principal biochemical factors: fasting blood glucose (FBG), total cholesterol, triglycerides, high-density lipoprotein (HDL), and low-density lipoprotein (LDL). The data were analyzed by chi-square test, 1-way analysis of variance, and Kruskal-Wallis test, and values of P < 0.05 were considered statistically significant. Individuals with a large pulp stone were significantly older than individuals with a small pulp stone (P = 0.024). No statistically significant difference was found in the distribution of the sexes in the 3 pulp stone groups, nor was there any association between pulp stones in unerupted teeth and FBG, total cholesterol, triglycerides, HDL, or LDL level (P > 0.05). The prevalence of tooth types followed a consistent pattern across all 3 groups, with canines being the most commonly affected, followed by premolars. In the present study, confounding variables were minimized by using unerupted teeth. CBCT was found to be an accurate 3-dimensional imaging modality for evaluation of pulp stones. As people age, the likelihood of pulp stone formation increases. No statistically significant association was observed between the prevalence of pulp stones and patients’ sex or biochemical factor levels.
Pulp stones are calcified masses in the dental pulp of healthy, diseased, and even unerupted teeth.1 Dental pulp can form hard tissues in response to local and systemic irritation.2 Since pulp stones usually do not cause any disease or symptoms, it remains unclear whether they represent a pathologic condition or a biologic variation.1 The etiology of pulp calcification is not well understood.2-4 However, formation of pulp stones is mostly influenced by factors such as the individual’s age and sex as well as past dental treatment activities, the presence of chronic caries or periodontal disease, and the existence of systemic conditions secondary to calcium metabolism such as hyperkalemia, gout, and kidney stones.5,6 The formation of pulp stones increases as a result of local chronic irritation resulting from periodontal disease, caries, deep tooth restorations, and dental orthodontic movements.7-9
The appearance of stones on the radiographic view can be diverse; they may be round or oval and may be observed as a single dense mass or several small opacities within the pulp. The sizes of pulp stones can vary from microscopic particles to large masses that obscure the pulp chamber.2 For a pulp stone to be identified in 2-dimensional (2D) dental radiographs, its diameter must be greater than 20 µm.2,9 Another limitation of these imaging techniques is their inability to capture a 3-dimensional (3D) view. Cone beam computed tomography (CBCT) is used for complex dental procedures when standard 2D radiographs will not provide adequate information. CBCT is a cost-effective and easily accessible method for 3D evaluation and quantitative measurement of hard tissue. Its high-resolution images allow precise measurements and do not superimpose adjacent structures, making it a valuable and accurate tool for evaluating pulp stones.10,11
Studies have been conducted to investigate the relationship between levels of biochemical factors in the blood and calcification in other organs.12,13 Studies have also investigated the correlation between pulp stones and systemic diseases, but the results are controversial.1,12-14 In addition, understanding the precise correlation between pulp stones and systemic biochemical factors can help elucidate the exact mechanism of pulp stone formation.
There is limited research on the occurrence of pulp stones in unerupted teeth.14-16 Because fully unerupted teeth are not exposed to the environmental and functional conditions of the oral cavity, they are more suitable for investigating the influence of systemic factors on pulp stone formation. Therefore, the present study aimed to use CBCT imaging to
evaluate pulp stones in unerupted teeth and to be the first to investigate the relationship between pulp stones and the blood levels of 5 principal biochemical factors: fasting blood glucose (FBG), total cholesterol, triglycerides, high-density lipoprotein (HDL), and low-density lipoprotein (LDL).
Methods
The Ethics Committee of Islamic Azad University, Isfahan (Khorasgan) Branch, Iran, approved this cross-sectional descriptive-analytical study (IR.IAU.KHUISF.REC.1401.151). Consecutive subjects who were referred for dental treatment at the Department of Oral Medicine and Radiology, School of Dentistry, were considered for the study. The CBCT images evaluated in the study were made for the purpose of diagnosis and dental treatment. No additional radiation dose was imposed on any patient during the process.
Sample selection
The sample size (n) was calculated as 90 using the following formula:
n = 2σ 2 (Z 1- α/2 + Z 1 - β)2 = 90, δ2
where σ is the standard deviation; Z is the Z value, corresponding to the standard normal distribution; α is the type I error (set at 0.05); β is the type II error (set at 0.2); 1 − β is the power of the study (80%); and δ is the minimum detectable difference between the 2 means.
To minimize the effect of selection bias, 800 CBCT scans were assessed for eligibility, and 90 were selected according to the eligibility criteria. The inclusion criteria were dentate patients, aged 15 to 55 years, who underwent CBCT of the complete maxillary and mandibular arches during the period from January 2022 to January 2024.7,14,17 In addition, the selected patients had to have all permanent teeth, which could be impacted or developing, and at least 1 unerupted tooth with half of its root length formed. The CBCT images had to have adequate resolution, diagnostic quality, and field of view. Considering that biochemical changes in blood can occur relatively quickly, all patients included in the study had completed both an imaging examination and blood sample preparation within the span of 1 week.
Individuals older than 55 years were excluded from the study because the incidence of pulp stones increases with age.16 The other exclusion criteria were the presence of unerupted teeth with pathologic features; the presence of a syndromic condition,
because many syndromes can delay or inhibit the normal process of tooth eruption; the existence of any problem or disease that could affect the results of laboratory tests, such as anemia, polycythemia, leukemia, allergies, or rheumatoid arthritis; a history of periodontal disease with moderate to severe bone loss; a history of dental trauma, orthodontic treatment, or maxillomandibular surgery; a history of radiotherapy or chemotherapy; use of any medications (to eliminate potential confounding effects on biochemical factors and pulp stone formation, such as those associated with statins, corticosteroids, and bisphosphonates); the presence of impacted, developing, unerupted third molars; and low-quality CBCT images.14,18
CBCT evaluation
All images were obtained using a 7.5 × 14.5-cm CBCT unit (Soredex Scanora 3D, Dexis) operating at 90 kVp and 8 mA with a voxel size of 0.25 mm. The primary reconstruction of the raw data was restricted to the alveolar area. Curved planar (panoramic) reformation, multiplanar reconstructions (crosssections), and oblique planar reformation were reconstructed from tomographic sections.
For interpretation, real-time reconstruction was performed using OnDemand3D (version 1.0.10.6388, CyberMed), and the axial, coronal, and sagittal 2D multiplanar reformatted slices, parasagittal multiplanar reformatted images, and 3D images were provided to the examiners.
Opaque masses in the pulp chamber and inside the root, which were observed in all 3 planes (coronal, sagittal, and axial), were diagnosed as pulp stones (Figure).14 The examiners reviewed the CBCT images for the presence of pulp stones, viewing the records on a 22-inch flat-panel LED monitor (NEC, Sharp Imaging) with a resolution of 2048 × 1536 pixels and a screen refresh rate of 120 Hz. The software image processing tool was used to adjust the contrast and brightness of images, ensuring optimal visualization.
The records of each patient were analyzed independently by an oral and maxillofacial radiologist (S.M.A.) and an endodontist using a specific computer and monitor; any differences in interpretation were resolved by consensus. The examiners were blinded to the patients’ identities and case histories during all stages of image evaluation. To avoid examiner fatigue, the viewing sessions were split into several periods throughout the day. Additionally, the images were ordered randomly. After an interval of 15 days, 25% of the sample was reassessed in the same manner to assess the reproducibility of the method.
Figure. CBCT images showing a pulp stone (arrows) in an unerupted tooth of a single patient. A. Sagittal view. B. Coronal view. C. Axial view.
Sex, n (%) Male
Tooth type, n (%)
Incisors
Groups: small (including total absence as well as minute particles with maximum diameter < 0.05 mm); moderate-sized pulp stone (maximum diameter 0.05-1.59 mm); large pulp stone (maximum diameter ≥ 1.60 mm).
b No statistically significant difference (P > 0.05; chi-square test).
The maximum pulp stone size was measured by scrolling through the axial, coronal, and sagittal slices as well as parasagittal multiplanar reformatted images. Then, 3 groups were defined according to the presence and size of pulp stones: small pulp stone (including total absence as well as minute particles with maximum diameter < 0.05 mm); moderate-sized pulp stone (maximum diameter 0.05-1.59 mm); or large pulp stone (maximum diameter ≥ 1.60 mm).2
The final sample comprised 90 subjects, with 30 cases randomly selected from each pulp stone size after 800 CBCT images were assessed for eligibility to ensure balanced group sizes and minimize selection bias. The selection process aimed to minimize confounding factors by applying strict eligibility criteria.
Biochemical analysis
Each patient’s medical history, age, sex, and previously recorded principal blood factor levels were retrieved from the patient’s digital files. For laboratory testing, 2 mL of venous blood was collected and centrifuged to separate the serum. Principal biochemical factors—FBG, total cholesterol, triglycerides, HDL, and LDL—were evaluated using the Span BT-1000 fully automated package tester (TM Electronics). A single technician, who was blind to the CBCT scan results of the patients, performed all testing in the same laboratory using the same technique.
Statistical analysis
All data were entered into a database and analyzed using SPSS for Windows (version 22, IBM). The chi-square test, 1-way analysis of variance (ANOVA) with post hoc Bonferroni correction, and Kruskal-Wallis test were performed for statistical analysis. Values of P < 0.05 were considered to indicate statistically significant differences. The κ statistic was used to investigate the interobserver agreement in the evaluation of pulp stones.
Chart 1. Distribution of patients by study group and patient age (n = 30 per group).
Groups: small pulp stone (including total absence as well as minute particles with maximum diameter < 0.05 mm); moderate-sized pulp stone (maximum diameter 0.05-1.59 mm); large pulp stone (maximum diameter ≥ 1.60 mm).
Results
The intraobserver intraclass correlation coefficient was excellent (between 0.90 and 0.97) for all evaluations. The κ statistic for interobserver agreement ranged from 0.80 to 0.85, indicating substantial to almost perfect agreement.
A total of 90 patients (62 female and 28 male) aged 15 to 55 years were assessed for pulp stones in unerupted teeth. The 1-way ANOVA showed a statistically significant difference in the mean age among the individuals in the 3 groups (P = 0.024) (Table 1). According to a post hoc Bonferroni test, the mean age of patients with a large pulp stone was significantly higher than
Table 1. Distribution of pulp stones in the study groups (n = 30 per group).
Groups: small pulp stone (including total absence as well as minute particles with maximum diameter < 0.05 mm); moderatesized pulp stone (maximum diameter 0.05-1.59 mm); large pulp stone (maximum diameter ≥ 1.60 mm).
a No statistically significant difference (P > 0.05; 1-way ANOVA).
b No statistically significant difference (P > 0.05; Kruskal-Wallis test).
Groups: small pulp stone (including total absence as well as minute particles with maximum diameter < 0.05 mm); moderate-sized pulp stone (maximum diameter 0.05-1.59 mm); large pulp stone (maximum diameter ≥ 1.60 mm).
that of patients with a small pulp stone. Analysis of the pulp stone distribution according to patient age revealed that 83.3% of individuals with a small pulp stone, 63.3% of individuals with a moderate-sized pulp stone, and 46.7% of individuals with a large pulp stone were younger than 30 years (Chart 1).
The chi-square test identified no statistically significant difference in the distribution of sex among the individuals of the 3 groups (P = 0.147). The prevalence of tooth types followed a consistent pattern across all 3 groups, with canines being the most commonly affected, followed by premolars, molars, and incisors in descending order. The distribution of pulp stones
among the studied groups did not show a statistically significant difference within the maxillary (P = 0.750) or mandibular (P = 0.780) arches, suggesting that pulp stone formation is not significantly influenced by arch location.
Analysis of the mean value of blood factor levels measured in each group showed that there was no statistically significant difference in FBG, total cholesterol, triglycerides, HDL, or LDL between subjects with a small pulp stone, a moderate-sized pulp stone, or a large pulp stone (Table 2). The majority of individuals in all 3 groups were within the normal reference ranges for all of the principal blood factors that were measured (Chart 2).
Chart 2. Distribution of patients with biochemical factor levels in the normal reference ranges (n = 30 per group).
Table 2. Mean (SD) blood levels of biochemical factors in the study groups (n = 30 per group).
n Small pulp stone n Moderate-sized pulp stone n Large pulp stone
Groups: small pulp stone (including total absence as well as minute particles with maximum diameter < 0.05 mm); moderate-sized pulp stone (maximum diameter 0.05-1.59 mm); large pulp stone (maximum diameter ≥ 1.60 mm).
a No statistically significant difference (P > 0.05; 1-way ANOVA).
b No statistically significant difference (P > 0.05; Kruskal-Wallis test).
Statistical analyses were performed to compare blood factor levels among the study groups according to patient sex and age (Table 3). For the female patients, 1-way ANOVA tests revealed no statistically significant difference in FBG, total cholesterol, HDL, or LDL levels among the 3 pulp stone groups. In addition, the Kruskal-Wallis test found no significant difference in triglyceride levels. Similarly, for male patients, 1-way ANOVA tests showed no significant difference in FBG, total cholesterol, HDL, or LDL levels among the study groups, while the Kruskal-Wallis test showed no significant difference in triglycerides. In patients younger than 30 years, 1-way ANOVA tests showed no significant difference in FBG, total cholesterol, HDL, or LDL levels among the 3 groups. Similarly, 1-way ANOVA tests showed no significant difference in FBG, total
cholesterol, HDL, or LDL levels among the study groups in patients aged 30 years or older. In addition, the Kruskal-Wallis test showed no significant difference in triglyceride levels among the study group in either age category.
Discussion
There are noticeable discrepancies in the prevalence and risk factors reported in various studies of pulp stones.1,2,14,16 This disagreement may be due to exposure of erupted teeth to numerous confounding conditions within the oral cavity, potentially obscuring the true effects of the examined variables. Unerupted teeth, free of the environmental influences of the oral cavity, offer a more suitable material for investigating pulp stones, enabling a more accurate assessment of
Table 3. Comparison of mean (SD) blood factor levels among the study groups according to patient sex and age.
the relationship between pulp stone formation and systemic factors.14 Therefore, the present study aimed to use advanced imaging techniques to evaluate pulp stones in unerupted teeth. To the authors’ knowledge, no previous study has assessed the relationship between pulp stones in unerupted teeth and blood levels of principal biochemical factors.
The present study demonstrated that pulp stones can develop not only in erupted teeth exposed to the oral environment but also in unerupted teeth that have not yet been subjected to such conditions. This result is in line with that of Kaabi et al.14 In both the moderate-sized and large pulp stone groups, the unerupted canine was the most common type of tooth to have a pulp stone.
Among this patient sample, 83.3% of people with a small pulp stone, 63.3% of people with a moderate-sized pulp stone, and 46.7% of people with a large pulp stone were younger than 30 years, indicating that the likelihood of pulp stone formation grows as age increases. This result aligns with the findings of studies by Goga et al and Kaabi et al.2,14 It has been reported that factors such as caries, periodontal diseases, and the formation of tertiary dentin contribute to the increased prevalence of dental pulp stones with advancing age in erupted teeth.2 Similar to agerelated calcification in other organs, such as heart valves, coronary arteries, carotid arteries, and kidneys, the probability of pulp stones in unerupted teeth also rises.19,20 The present study also demonstrated an age-related increase in the prevalence of pulp stones in unerupted teeth. However, the findings suggest that their formation is likely influenced by additional mechanisms beyond these established factors. More research should be conducted to investigate the underlying mechanisms of pulp stone formation in both erupted and unerupted teeth.
Numerous studies have been conducted with dental 2D radiographs, which have several limitations in detecting pulp stones; for example, in panoramic images, due to superimposition of anatomical structures, lower resolution, magnification and distortion errors, lack of depth perception, and variability in beam angulation, such calcifications may be underidentified.9,21 The use of CBCT for imaging is a strength of the present study because it is the gold standard for angular and linear measurements and enables meticulous evaluation of pulp stones in 3D views.22
The present results showed no statistically significant difference between the sexes among the studied groups, a finding that is consistent with the study of Kaabi et al and contradicts the study of Ivanauskaitė et al.14,23 Ivanauskaitė et al concluded that women are more likely to experience pulp calcification due to bruxism.23 Bains et al also reported that pulp stones were more prevalent in women than in men, but this difference was not statistically significant.24 In the present study, as the examined teeth were unerupted, they were not subject to sex-specific risk factors in the oral environment that may influence pulp stone formation, including hormonal influences, differences in inflammatory responses, variations in mineral metabolism, and conditions such as bruxism and other stress-related factors, which are more prevalent in women.2,25 This enabled more precise evaluation of the intrinsic factors influencing pulp stone formation and their relationship with sex.
Puşcaşu et al found that pulp stones were more prevalent in people with type 2 diabetes, which was contrary to the results of the present study, where no significant association was observed between FBG level and the presence of pulp stones. 26 This discrepancy could be attributed to the fact that the study of Puşcaşu et al focused on erupted teeth, unlike this study. 26
In the present sample, there were no significant relationships between the presence or size of a pulp stone and the total cholesterol, LDL, HDL, and triglyceride levels. Sener et al found no relationship between pulp stones and history of cardiovascular diseases.1 Kaabi et al reported a significantly increased number of pulp stones in patients with systemic diseases.14 This discrepancy might be due to the different methods and eligibility criteria in these studies. The specific type of systemic disease was not considered in the study by Kaabi et al, while the present study measured principal biochemical factors in the blood.14
The present study has some limitations. First, the small sample size, a result of the strict eligibility criteria, may limit the potential to generalize the findings. Second, the scarcity of similar studies focusing on blood biochemical factors limited the availability of comparative data. Longitudinal studies would be beneficial to elucidate the etiologic factors involved in pulp stone formation and their complex relationship with biochemical factors. Additionally, comparison of systemic factors in patients with pulp stones in unerupted versus erupted teeth is recommended.
Conclusion
In this study, confounding factors were minimized by using unerupted teeth, which are not affected by the conditions of the oral environment, and accurate detection and 3D measurement of pulp stones were ensured by using CBCT. Pulp stones can be present in any type of unerupted tooth, but they were most commonly found in canines. As age increases, the likelihood of pulp stone formation also grows. There was no statistically significant difference in the prevalence of pulp stones in male and female patients. No association was found between pulp stones of any size and FBG, total cholesterol, triglyceride, HDL, or LDL levels.
Author affiliations
School of Dentistry, Isfahan (Khorasgan) Branch, Islamic Azad University, Isfahan, Iran (Javaheri, S. Jafari-Pozve); Department of Oral and Maxillofacial Radiology, School of Dentistry, Isfahan (Khorasgan) Branch, Islamic Azad University, Isfahan, Iran (N. Jafari-Pozve, Aryanezhad). Department of Oral and Maxillofacial Radiology, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran (Arianezhad).
Correspondence
S. Marjan Arianezhad, DDS, MSc (marjan.arianezhad@gmail.com).
Conflicts of interest
None reported.
References
1. Sener S, Cobankara FK, Akgünlü F. Calcifications of the pulp chamber: prevalence and implicated factors. Clin Oral Investig. 2009;13(2):209-215. doi:10.1007/s00784-008-0212-x
2. Goga R, Chandler NP, Oginni AO. Pulp stones: a review. Int Endod J. 2008;41(6):457-468. doi:10.1111/j.1365-2591.2008.01374.x
3. Inagaki Y, Yoshida K, Ohba H, et al. High glucose levels increase osteopontin production and pathologic calcification in rat dental pulp tissues. J Endod. 2010;36(6):1014-1020. doi:10.1016/j.joen.2010.03.018
4. Langeland K, Rodrigues H, Dowden W. Periodontal disease, bacteria, and pulpal histopathology. Oral Surg Oral Med Oral Pathol. 1974;37(2):257-270. doi:10.1016/00304220(74)90421-6
5. Hillmann G, Geurtsen W. Light-microscopical investigation of the distribution of extracellular matrix molecules and calcifications in human dental pulps of various ages. Cell Tissue Res. 1997;289(1):145-154. doi:10.1007/s004410050860
6. Mjör IA, Ferrari M. Pulp-dentin biology in restorative dentistry, 6: reactions to restorative materials, tooth-restoration interfaces, and adhesive techniques. Quintessence Int. 2002;33(1):35-63.
7. Edds AC, Walden JE, Scheetz JP, Goldsmith LJ, Drisko CL, Eleazer PD. Pilot study of correlation of pulp stones with cardiovascular disease. J Endod. 2005;31(7):504-506. doi:10.1097/01.don.0000168890.42903.2b
8. Ertas ET, Veli I, Akin M, Ertas H, Atici MY. Dental pulp stone formation during orthodontic treatment: a retrospective clinical follow-up study. Niger J Clin Pract. 2017;20(1):37-42. doi:10.4103/1119-3077.164357
9. Kannan S, Kannepady SK, Muthu K, Jeevan MB, Thapasum A. Radiographic assessment of the prevalence of pulp stones in Malaysians. J Endod. 2015;41(3):333-337. doi:10.1016/j. joen.2014.10.015
10. Vasegh Z, Safi Y, Azar MS, Ahsaie MG, Arianezhad SM. Assessment of bony changes in temporomandibular joint in patients using cone beam computed tomography—a cross sectional study. Head Face Med. 2023;19(1):47. doi:10.1186/s13005-023-00392-z
11. Pedram A, Aryanezhad SS, Jafari-Pozve N, Abrishami M, Arianezhad SM. Investigating the anatomy and location of the infraorbital canal in relation to the adjacent structures in cone beam computed tomography (CBCT) images. J Maxillofac Oral Surg. 2025;24(2):542-556. doi:10.1007/s12663-024-02191-8
12. Fernández-Palomeque C, Grau A, Perelló J, et al. Relationship between urinary level of phytate and valvular calcification in an elderly population: a cross-sectional study. PLoS One 2015;10(8):e0136560. doi:10.1371/journal.pone.0136560
13. Nayak M, Kumar J, Prasad LK. A radiographic correlation between systemic disorders and pulp stones. Indian J Dent Res. 2010;21(3):369-373. doi:10.4103/0970-9290.70806
14. Kaabi HH, Riyahi AM, Bakrman AK, Almutaw YA, Alrumayyan SF, Al-Maflehi NS. Pulp stones in unerupted teeth: a retrospective analysis using cone-beam computed tomography. BMC Oral Health. 2024;24(1):714. doi:10.1186/s12903-024-04503-3
15. Marwaha M, Chopra R, Chaudhuri P, Gupta A, Sachdev J. Multiple pulp stones in primary and developing permanent dentition: a report of 4 cases. Case Rep Dent. 2012;2012:408045. doi:10.1155/2012/408045
16. Jannati R, Afshari M, Moosazadeh M, Allahgholipour SZ, Eidy M, Hajihoseini M. Prevalence of pulp stones: a systematic review and meta-analysis. J Evid Based Med. 2019;12(2):133-139. doi:10.1111/jebm.12331
17. da Silva EJNL, Prado MC, Queiroz PM, et al. Assessing pulp stones by cone-beam computed tomography. Clin Oral Investig. 2017;21(7):2327-2333. doi:10.1007/s00784-016-2027-5
18. Altındağ A, Bahrilli S, Çelik Ö, Bayrakdar İŞ, Orhan K. The detection of pulp stones with automatic deep learning in panoramic radiographies: an AI pilot study. Diagnostics (Basel) 2024;14(9):890. doi:10.3390/diagnostics14090890
19. Diederichsen SZ, Grønhøj MH, Mickley H, et al. CT-detected growth of coronary artery calcification in asymptomatic middle-aged subjects and association with 15 biomarkers. JACC Cardiovasc Imaging. 2017;10(8):858-866. doi:10.1016/j.jcmg.2017.05.010. Erratum: 2017;10(9):1088-1089. doi:10.1016/j.jcmg.2017.08.003
20. Lee JS, Kim OS, Chung HJ, et al. The prevalence and correlation of carotid artery calcification on panoramic radiographs and peripheral arterial disease in a population from the Republic of Korea: the Dong-gu study. Dentomaxillofac Radiol. 2013;42(3):29725099. doi:10.1259/ dmfr/29725099
21. Tassoker M, Magat G, Sener S. A comparative study of cone-beam computed tomography and digital panoramic radiography for detecting pulp stones. Imaging Sci Dent 2018;48(3):201-212. doi:10.5624/isd.2018.48.3.201
22. Safi Y, Shamloo Mahmoudi N, Aghdasi MM, et al. Diagnostic accuracy of cone beam computed tomography, conventional and digital radiographs in detecting interproximal caries. J Med Life. 2015;8(Spec Issue 3):77-82.
23. Ivanauskaitė D, Kubiliūtė D, Janavičienė D, Brukienė V. Prevalence of pulp stones in molars based on bitewing and periapical radiographs. Stomatologija. 2021;23(1):9-15.
24. Bains SK, Bhatia A, Singh HP, Biswal SS, Kanth S, Nalla S. Prevalence of coronal pulp stones and its relation with systemic disorders in northern Indian central Punjabi population. ISRN Dent. 2014;2014:617590. doi:10.1155/2014/617590
A clinical guide to oral manifestations and diagnosis of limited systemic sclerosis: a case report
Vanessa Carvajal Soto, MS ¢ Larissa Knysak Ranthum, MS ¢ Helen Heloene Rosa, DDS
Eduardo Bauml Campagnoli, PhD ¢ Marcelo Carlos Bortoluzzi, PhD
Scleroderma is a rare connective tissue disease involving vascular injury and autoimmunity. It is characterized by the thickening, hardening, and tightening of connective tissues, leading to multifaceted complications.
Scleroderma is classified into 2 forms, localized scleroderma and systemic sclerosis (SSc). The systemic form is further subdivided into limited SSc (formerly known as CREST syndrome) or diffuse SSc. This report describes the case of a 41-year-old woman with gingival pain, temporomandibular joint pain, frequent fevers, night sweats, excessive thirst, hunger, frequent urination, and weight gain. Her medical history included Sjögren syndrome and Raynaud phenomenon. Physical examinations revealed petechiae on the palms, lips, tongue, and soft palate; hypochromia of the lips; fibrosis; dry mouth; and active periodontal disease. Serologic test results were positive for anticentromere and antinuclear antibodies and negative for anti-topoisomerase I antibody, confirming the diagnosis of limited SSc. The oral manifestations were critical to the early diagnosis of limited SSc. Telangiectasia, labial fibrosis, and xerostomia were key indicators. Interdisciplinary collaboration between oral healthcare professionals and rheumatologists is essential for optimal patient management. Further research is needed to understand the underlying mechanisms of SSc and refine the diagnostic criteria.
Scleroderma is a rare connective tissue disorder with a complex and unknown pathogenesis. It has 3 hallmarks: vascular injury, autoimmunity, and tissue fibrosis.1 The manifestations often overlap those of other rheumatologic or immunologic diseases, and the severity of presentation can vary, depending on the timing of diagnosis.2 Scleroderma can be divided into 2 primary forms, localized scleroderma and systemic sclerosis (SSc).1 Primarily affecting the skin and subcutaneous tissue, localized scleroderma is not associated with increased mortality and has specific clinical subtypes (morphea, linear scleroderma, and scleroderma en coup de sabre). Systemic disease can be further classified into 2 types based on clinical and serologic criteria: limited SSc (formerly known as CREST syndrome, characterized by calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia) and diffuse SSc. SSc primarily affects the skin, gastrointestinal tract, lungs, kidneys, skeletal muscles, and pericardium. Globally, the prevalence of SSc ranges from 38 to 341 cases per million people, while annual incidence rates vary between 8 and 56 new cases per million.1
The exact etiology of SSc is not fully understood, but both genetic and environmental factors are believed to contribute to its development. Genetic factors include familial clustering and the involvement of multiple autoimmune diseases within families, with genome-wide association studies highlighting the role of the major histocompatibility complex genetic region, specific human leukocyte antigens (HLA), and non-HLA loci such as PTPN22, NLRP1, STAT4, and IRF5. 1 Environmental factors linked to SSc include infectious agents such as cytomegalovirus, Epstein-Barr virus, and parvovirus B19 as well as exposure to silica dust, organic solvents, toluene, xylene, trichloroethylene, and polyvinyl chloride.1 Cigarette smoking is not a proven risk factor. Scleroderma-like disorders, distinct from SSc in clinical, histopathologic, and laboratory features, can arise from environmental exposures such as contaminated rapeseed cooking oil (toxic oil syndrome) and l-tryptophan (eosinophilia-myalgia syndrome), with certain drugs such as bleomycin and cocaine also implicated in the development of SSc-like illnesses.1
The aim of this case report was to investigate the diagnostic journey and clinical presentation of a patient with symptoms suggestive of systemic autoimmune disease. The importance of this case in dentistry lies in its exploration of the oral manifestations and diagnostic challenges associated with SSc. By detailing the patient’s symptoms, physical examination findings, and serologic test results, this report sheds light on the importance of recognizing and managing systemic autoimmune diseases in dental practice. Given the oral complications often
and
to
The surfaces of the lower lip mucosa, lateral border of the tongue, and soft palate are pale, and petechiae and areas of telangiectasia are present. The mucosa is tense and rigid.
accompanying SSc, such as fibrosis, dry mouth, and periodontal disease, dental professionals play a crucial role in early detection and referral for appropriate treatment.3-6 Thus, this case report serves as a valuable educational resource for dentists, emphasizing the need for interdisciplinary collaboration and vigilance in addressing systemic conditions impacting oral health.
Case report
The patient consented to the use and disclosure of her clinical data and images for academic and scientific purposes.
A 41-year-old woman sought treatment because of pain in the gingiva and temporomandibular joint. She reported that the pain began approximately 1.5 months earlier and improved with the application of warm compresses. Additionally, over the past 5 months, the patient had been experiencing frequent fevers and/or night sweats, excessive thirst, hunger, frequent urination, and significant weight gain. She also reported difficulty in opening her mouth and making lateral jaw movements; fatigue; muscle pain when chewing; headaches; neck pain; ear pain near the temporomandibular joint; and frequent joint noises. Her medical history included Sjögren syndrome and Raynaud phenomenon (both diagnosed about 8 years previously). In addition, she revealed a history of depression, fibromyalgia, carpal tunnel syndrome, seizures, fainting, headaches, numbness in the hands, fatigue, insomnia, and stress; she also experienced a stroke 3 years earlier. The patient reported taking several medications, including leflunomide and artificial saliva, which are not associated with dry mouth and have no relation to the signs and symptoms presented.
During the physical examination, petechiae were discovered on the palms of the hands, which exhibited rigid skin (Fig 1). Petechiae were also present on the lips, tongue, and soft palate (Fig 2). The patient reported that the petechiae had been present for approximately 18 months, without any prior diagnosis. On clinical examination, the lips exhibited hypochromia, accompanied by marked fibrosis and stiffness. Signs of dry mouth and active periodontal disease were also noted. The mucosa was tense and rigid, hindering clinical examination.
In the presence of clinical signs and symptoms such as telangiectasia in the oral cavity and on the palms, fibrosis and stiffness of the lip mucosa, and dry mouth, several conditions were considered in the differential diagnosis. These included systemic lupus erythematosus, Sjögren syndrome, rheumatoid arthritis, dermatomyositis/polymyositis and fibromyalgia, mixed connective tissue disease, and coagulopathy.
To narrow the diagnosis, a comprehensive series of serologic tests was conducted. These tests were ordered by the dental team as part of the patient’s diagnostic assessment. The complete blood count was within normal limits, indicating no signs of anemia or infection, and the platelet count was also normal. The erythrocyte sedimentation rate and C-reactive protein test results were within normal limits, suggesting the absence of significant systemic inflammation. Coagulation studies included the partial thromboplastin time and prothrombin time, the results of which ruled out the presence of hemostatic disorders. The blood glucose level was also within normal limits, eliminating hyperglycemia and diabetes as contributing factors.
Fig 1. The skin of the hands exhibits rigidity and tension. Petechiae and small areas of telangiectasia are present.
Fig 2. Oral signs and symptoms. A. The lips are hardened, sclerotic, and hypochromic,
the vermilion border is pale. B
D.
Table. Clinical characteristics and serologic differentiation of localized scleroderma and systemic sclerosis.
Systemic sclerosis
Findings Localized scleroderma
Clinical characteristics Morphea, linear scleroderma, and scleroderma en coup de sabre are specific clinical subtypes of localized scleroderma that primarily affect the skin and subcutaneous tissue; not associated with increased mortality
Anti-Scl-70–positive: predominantly observed, associated with diffuse cutaneous involvement, interstitial lung disease, and cardiac involvement; ARA-positive: linked to aggressive skin involvement, poor outcomes, and scleroderma renal crisis
Abbreviations: ACA, anticentromere antibody; ANA, antinuclear antibody; ARA, anti-RNA polymerase III antibody; anti-Scl-70, anti-topoisomerase I. Percentages represent the profile of autoantibody test results commonly observed in patients with localized or systemic forms of the disease.1
However, the serologic profile revealed crucial diagnostic markers. The result of the anticentromere antibody (ACA) test was positive, which is highly indicative of limited SSc. The anti-topoisomerase I (anti-Scl-70) antibody test result was negative, a finding that typically helps to differentiate limited SSc from diffuse forms of the disease. Additionally, the antinuclear antibody (ANA) test results were positive, with specific reactivity in the nucleus and chromosomal metaphase plate, but negative in the nuclear envelope, cytoplasm, and mitotic apparatus.
These serologic findings, combined with the patient’s distinct clinical manifestations, confirmed the diagnosis of limited SSc. The distinct subclassifications, clinical characteristics, and serologic differentiation of SSc are outlined in the Table.
Discussion
SSc is a complex autoimmune disease that affects multiple body systems, including the digestive and respiratory systems as well as the oral cavity. Systemically, SSc can cause esophageal scleroderma, resulting in gastroesophageal reflux and dysphagia; pulmonary fibrosis, leading to dyspnea and respiratory failure; pulmonary arterial hypertension; and scleroderma renal crisis.1 Orally, SSc manifests as microstomia, which complicates oral hygiene and eating; xerostomia, which predisposes the patient to caries and infections; telangiectasias in the oral mucosa; and gingival fibrosis, which causes bleeding and complicates dental treatments.6,7 In the clinical case presented here, the patient exhibited telangiectasias in the oral cavity and on the palms of the hands, fibrosis and stiffness of the labial mucosa, and xerostomia, all of which are characteristic symptoms of SSc.
Along with oral and systemic complications, SSc has a long list of clinical manifestations, making early and effective diagnosis challenging. The skin lesions and symptoms
caused by this condition can be mistaken for those of other dermatologic, rheumatologic, and/or immunologic diseases, such as lupus and rheumatoid arthritis, potentially leading to incorrect or delayed diagnoses. 8 The progression of SSc varies significantly among patients, ranging from rapid progression with failure of multiple organs to a slower course, further complicating disease monitoring and diagnosis. 9 In the present case, the patient’s oral and extraoral manifestations were crucial for reaching the diagnosis, which was confirmed by means of specific serologic tests. These tests revealed positive results for ACAs and ANAs and negative results for anti-Scl-70 antibodies, a typical serologic profile of limited SSc. 1
This case report demonstrates the importance of oral manifestations in the early diagnosis and treatment of patients with limited SSc. However, as this case study involved a single patient, there are limitations in generalizing the findings because interindividual variability raises the possibility of less pronounced or atypical manifestations in some cases. The involvement of dental professionals in the early identification of these oral manifestations is fundamental, reinforcing the need for an interdisciplinary approach to diagnosis and treatment.10
Conclusion
The present case highlights the pivotal role of oral manifestations in the early diagnosis of limited SSc. Telangiectasia, lip fibrosis, and xerostomia emerged as key clinical indicators of the disease in this patient. Interdisciplinary collaboration between oral healthcare professionals and rheumatologists is essential for optimal management of this disease. Further research is warranted to elucidate the pathophysiologic mechanisms underlying the oral manifestations of SSc and refine diagnostic criteria.
Author affiliations
Postgraduate Program in Dentistry, State University of Ponta Grossa (UEPG), Ponta Grossa, Brazil (Soto, Ranthum, Rosa, Bortoluzzi); Postgraduate Program in Health Sciences, State University of Ponta Grossa (UEPG), Ponta Grossa, Brazil (Campagnoli).
Correspondence
Marcelo Carlos Bortoluzzi, PhD (mbortoluzzi@uepg.br).
Conflicts of interest
None reported.
References
1. Adigun R, Goyal A, Hariz A. Systemic sclerosis (scleroderma). In: StatPearls. StatPearls Publishing; April 5, 2024. https://www.ncbi.nlm.nih.gov/books/NBK430875/
2. Zhou KY, Ye Q, Fang S. Nodular scleroderma partially controlled with tofacitinib. Letter. An Bras Dermatol. 2024;99(6):989-991. doi:10.1016/j.abd.2024.02.003
3. Ciurea A, Stanomir A, Șurlin P, et al. Insights into the relationship between periodontitis and systemic sclerosis based on the new periodontitis classification (2018): a cross-sectional study. Diagnostics (Basel). 2024;14(5):540. doi:10.3390/diagnostics14050540
4. Lefaan YM, Setiadhi R. Challenges in the management of oral manifestations in a patient with limited systemic sclerosis. Sci Dent J. 2021;5(3):148-154. doi:10.4103/sdj.sdj_93_21
5. Heyne S, Haufe E, Beissert S, Schmitt J, Günther C. Determinants of depressive symptoms, quality of life, subjective health status and physical limitation in patients with systemic sclerosis. Acta Derm Venereol. 2023;103:adv6502. doi:10.2340/actadv.v103.6502
6. Gagarine M, Cañedo-Ayala M, Cook V, et al. Oral health in systemic sclerosis: a scoping review. J Scleroderma Relat Disord. 2024;10(1):13-26. doi:10.1177/23971983241252899
7. Stanomir A, Micu IC, Soancă A, et al. The impact of systemic sclerosis on oral health. Ro J Stomatol. 2022;68(2):51-55. doi:10.37897/rjs.2022.2.1
8. Zhang S, Zhu J, Zhu Y, et al. Oral manifestations of patients with systemic sclerosis: a metaanalysis for case-controlled studies. BMC Oral Health. 2021;21(1):250. doi:10.1186/s12903021-01603-2
9. Puzio A, Przywara-Chowaniec B, Postek-Stefańska L, Mrówka-Kata K, Trzaska K. Systemic sclerosis and its oral health implications. Adv Clin Exp Med. 2019;28(4):547-554. doi:10.17219/acem/76847
10. Jerjen R, Nikpour M, Krieg T, Denton CP, Saracino AM. Systemic sclerosis in adults, I: clinical features and pathogenesis. J Am Acad Dermatol. 2022;87(5):937-954. doi:10.1016/j. jaad.2021.10.065
What every dentist needs to know about electric scooters
John K. Brooks, DDS ¢ Youstina A. Hanna, BS ¢ Nasir Bashirelahi, PhD
Somatic and craniofacial injuries from the use of electric scooters (e-scooters) have become a serious public health concern, affecting both riders and pedestrians. Accidents involving e-scooters pose a risk for bone fractures and significant injuries to the soft tissues and brain, and severe injuries may result in death. Oral healthcare providers should particularly be aware of the potential for injuries to the oral hard and soft tissues. Dentists have the opportunity to educate their patients on preventive measures to mitigate e-scooter injuries and to advocate the use of protective equipment, including a helmet, mouthguard, and elbow and knee pads.
Received: July 30, 2024
Accepted: October 8, 2024
Keywords: accidents, electric scooters, head and neck trauma, injury mitigation, public health
Electric motorized scooters (e-scooters) have become a popular and convenient mode of transportation in urban environments. They offer several consumer advantages, such as ease of use and cost-effectiveness, and they are considered environmentally friendly.1 Through 2024, it has been projected that the revenue from e-scooter ride-sharing will total $730 million in the United States.2 However, with the surge in e-scooter use, there has been a corresponding escalation in soft tissue and osseous injuries.
Self-propelled scooters have been in existence for more than 200 years. Use of scooters notably increased in the last decade, following technological enhancements to electric motors powered by lightweight lithium ion batteries and a self-operating business model utilizing global positioning technology. With the overall increase in consumer use, there has been a corresponding escalation in injuries, particularly among first-time riders.3 Numerous publications have substantiated the risk of bodily harm, literally from head to toe, following use of this alternative form of transportation.4
It is important for oral healthcare providers to become knowledgeable about newer fads, ethnic customs, and innovations, especially those that pose a risk for head and neck injuries.5-7 The aim of this article is to increase awareness of the scope of e-scooter–related injuries, with particular emphasis on those occurring in the craniofacial region. In addition, e-scooter–related safety gear, preventive measures, patient education, and regulations will be reviewed.
Injuries from e-scooter use
Patient demographics
The majority of individuals with reported e-scooter injuries are male, and patients have a mean age of 26 to 34.1 years (range of 4 to 78 years).8-10 Magee et al investigated a cohort of 11,452 pediatric e-scooter riders, noting that 26.7% were aged 6 to 7 years.11
Accident characteristics
Cicchino et al found that most e-scooter injuries occurred during daytime hours, with 13.5% taking place at night.3 Nearly 55% of injuries were sustained on weekdays.9 Approximately 61% of patients presented to the hospital emergency room as walk-ins, and 39.3% arrived via ambulance.9 Injuries varied by season, with 33.9% occurring in the summer, 26.2% in the autumn, 23.4% in the spring, and 16.5% in the winter.10 On average, inpatient hospitalization associated with e-scooter injuries extended nearly 4 days and exceeded $88,000 in costs.12
Sites of injury
Nonoral injuries
A systematic review of e-scooter accidents by Singh et al pooled data from 34 studies involving 5702 individuals, characterizing injuries that ranged from superficial to severe trauma.9
They found that 41.5% of e-scooter injuries occurred in the head and neck (27.4% in head/neck and 14.1% in the face), 33.5% in the upper extremities, 18.6% in the lower extremities, and 6.3% in the torso. Of note, 39.2% of all injuries were fractured bones, with 44.8% in the upper extremities, 24.9% in the lower extremities, 15.8% in the head and neck (12.6% in facial bones, 2.7% in the skull, and 0.5% in cervical structures), 3.5% in the abdomen, and 5.7% in unspecified locations. At least 28.5% of the injuries involved soft tissues, of which 19.1% were lacerations, abrasions, or contusions; 5.1% were sprains, strains, or dislocations; and 0.3% resulted in internal organ damage. One patient death was reported.9
Faraji et al characterized the distribution of craniofacial injuries among 188 e-scooter riders who sustained a total of 171 bone fractures.13 The most commonly fractured bones were the orbital complex (24.6%; n = 42) and maxilla (23.4%; n = 40); fractures occurred less frequently in the mandible (10.5%; n = 18), nasal bone (11.7%; n = 20), zygomatic bone (7.6%; n = 13), frontal sinus (5.8%; n = 10), sphenoid bone (5.3%; n = 9), temporal bone (4.4%; n = 7), parietal bone (1.8%; n = 3), occipital bone (1.2%, n = 2), and other facial bones (4.1%, n = 7). Soft tissue injuries of the head and neck were identified in 306 sites, with 34.6% (n = 106) involving the forehead, 11.8% (n = 35) scalp, 11.1% (n = 34) chin, 10.5% (n = 32) upper lip, 10.1% (n = 31) cheek, 8.2% (n = 25) nose, 8.2% (n = 25) eyelid, 4.6% (n = 14) lower lip, and 0.7% (n = 2) ear; the soft tissue sites were unspecified in 11.8% of cases (n = 36).
Yarmohammadi et al reported on 34 patients with facial trauma following an e-scooter collision, of which approximately 25% sustained orbital fractures (including 4 with bilateral fractures) and 21% experienced ocular injuries, consisting mainly of lid lacerations; there were single cases of retrobulbar or intraretinal hemorrhage associated with vision loss.14 Soliman et al described the clinical findings in 25 individuals with craniofacial trauma secondary to e-scooter accidents.15 Analysis of the injury types revealed that 28% of all patients had cutaneous lip lacerations, 20% had nasal lacerations, 20% involved the chin, 16% involved the forehead, and 8% involved the cheek.15 A limited number of cases of e-scooter injuries have involved the ear or resulted in facial foreign body implantation.13,16
An infrequent but concerning consequence of e-scooter usage is the risk of injuries to the central nervous system, with 8.6% to 19.1% of injuries involving a concussion, 11.0% involving traumatic brain injury, and 1.6% to 3.6% involving intracranial hemorrhage.9,17 Kim et al described 5 patients who presented with cerebrospinal leakage from skull base fractures following e-scooter–related trauma, including 1 patient with a “catastrophic injury not amenable to treatment.”18 Navarro et al estimated an overall yearly mortality rate of 6.7 patients among hospitalized e-scooter users.10 The predominant cause of death among e-scooter riders is head trauma.19
Oral injuries
Various intraoral injuries have been associated with e-scooter devices. Hennocq et al compiled data on the injuries found in 125 patients treated at 2 facial trauma centers.20 Facial injuries occurred in the chin (40%), lips (28%), supraorbital rim/forehead (18%), nose (11%), and cheek (3%). One patient sustained
a tongue injury. In addition, 55% (n = 66) of riders presented with mandibular fractures, of which 68% involved the condyle and 32% other gnathic sites. Dental injuries were noted in 44% of the total cohort, of whom 60% had crown fractures, 35% had tooth dislocations, and 5% had alveolar fractures; 80% of the involved teeth were incisors, and 20% were designated as “other teeth.” Kim et al evaluated e-scooter injuries among 256 patients and documented a 2.3% incidence of tooth avulsion, totaling 9 teeth.17 Faraji et al reported that 12.3% of 188 e-scooter patients incurred unspecified dental injuries.13
Lentzen et al performed a retrospective review of 52 patients with e-scooter–related mandibular osseous fractures.21 Of note, 45% of the injuries were purportedly associated with alcohol consumption. The data indicated that 48% (n = 25) of individuals had 2 sites of jawbone fractures, 29% (n = 15) had 1 fracture site, and 23% (n = 12) had more than 2 sites of fracture.21 While 67% (n = 35) of fractures occurred in the mandibular ramus, 58% (n = 30) occurred in the body, 33% (n = 17) at the angle, 12% (n = 6) at the symphysis, 8% (n = 4) at the condyle, and 1 in the alveolar process. In addition, 77% (n = 40) of individuals also experienced tooth fractures, and 18% developed traumatic brain injuries.21 Kim et al reported 5 maxillary and 5 mandibular fractures among 256 affected patients.17
Mechanisms of injury
With regard to the impact itself, 70.6% to 74.4% of patients were injured following a fall, 9.6% to 10.2% collided with a vehicle, 8.3% to 10.5% collided with an unspecified object, and 2.2% to 3.1% struck a pedestrian; infrequently, e-scooter injuries have involved collisions with cyclists or other e-scooter riders.3,9 Additionally, 48.5% of injuries occurred on the street, 26.2% occurred on the sidewalk, 19.9% were unspecified, and 5.5% were designated as “other.”9 Nearly 84% of collisions resulted in individuals being thrown from their e-scooter.10 Toofany et al reviewed the literature and identified 44 e-scooter accidents involving nonriders, finding that 59.1% (n = 26) of injuries resulted from being struck by an e-scooter and 29.5% (n = 13) from pedestrians tripping over a stationary e-scooter.22 Sikka et al reported a 60-year-old individual who was walking on the sidewalk and incurred an acute compression fracture of the lumbar vertebra following collision with an e-scooter rider.23 Several individuals have received serious thermal burns that resulted from exploding lithium ion batteries in standing e-scooters.24,25 Approximately 12% to 16% of e-scooter injuries have been attributed to device malfunction, usually to defective components (brakes, handlebars, steering mechanisms) or a sticky throttle.3,9 Riders of e-scooters with smaller wheels have a greater probability of losing control after running over objects and along uneven surfaces.18 Standing closer to the front wheel of the e-scooter while riding moves the center of gravity forward, increasing the stopping distance and the chance of collision, and conversely, riders who are positioned closer to the rear wheel shorten their stopping distance and have less risk of injury.26
Risk factors
Various factors contribute to an increased risk of e-scooter injuries. Epidemiologic studies have consistently identified that the greatest contributor to e-scooter injuries is underutilization
of protective equipment, principally the lack of helmet use as well as failure to wear elbow, wrist, and knee pads. Databases with cohorts of more than 1000 e-scooter riders indicate that the percentage of riders who wore helmets ranged from 5.2% to 38.3%, while 61.7% to 69.4% of riders had not worn a helmet.9,10 Although wearing a helmet while riding an e-scooter may attenuate the risk of traumatic brain injury, comparable to wearing a helmet for football or other contact sports, the construction of scooter helmets is deemed insufficient to completely eliminate this outcome.27 In addition, many of the commercial brands of helmets do not include a face shield component, which could reduce the risk of facial lacerations and dentoalveolar trauma.
Another important risk for e-scooter users is riding while chemically impaired. Most fundamentally, alcohol intoxication concurrent with e-scooter usage has ranged from 1.6% to 25.1% based on studies involving cohorts of more than 1000 riders.9,10 Faraji et al summarized the findings of 206 individuals with e-scooter injuries, noting that 54.2% of this cohort had been engaged in alcohol consumption.13 Rickelmann et al reported on 102 individuals with e-scooter injuries, 49% (n = 40) of whom were found with blood alcohol contents averaging 0.19%.28 State laws restrict the operation of vehicles when the driver has blood alcohol contents exceeding 0.08% to 0.10%.29 Injured e-scooter riders have also tested positive for recreational drugs at rates ranging from 6% to 20.3%.9,20
Other factors associated with e-scooter injuries include riding surface smoothness, with shorter braking (deceleration) distances along asphalt and concrete and the lowest on dirt pathways; traveling with multiple riders; decreased rider reaction time; distracted riders (eg, using a cell phone or listening to loud music); and riding during adverse visibility conditions (eg, nighttime, poor lighting, inclement weather).10,26,30,31 The speed at which the e-scooter is operated is another risk factor for injury, with greater velocity inherently associated with an increased force of impact and ensuing potential for greater trauma.31 Seemingly counterintuitive, Navarro et al noted that 60.0% of riders who had been admitted to the hospital were traveling < 20 mph, while 40.0% were traveling > 20 mph.10
Regulatory statutes
Laws regarding e-scooter usage vary by country, state, and local jurisdiction, with most communities permitting speeds no greater than 15 mph.26 Other regulations have involved helmet requirements; prohibitions on certain situations, such as additional passengers, ridership on sidewalks or within the public domain, or leaving e-scooters unattended on sidewalks; minimum age requirements; designated parking locations; and the need for mandatory insurance.32 In addition, e-scooter riders may be subject to financial liability if they cause injuries to other riders or pedestrians.23
Preventive measures
Oral healthcare providers should play an active role in advocating safe practices among e-scooter users, particularly emphasizing the importance of wearing helmets and other protective gear, refusing additional passengers, keeping both hands on the handlebars, obeying speed limits, slowing down on uneven
surfaces, and avoiding alcohol and recreational drug use when riding.
Conclusion
The increasing use of e-scooters has created an emerging public health concern. Oral healthcare providers should be aware of the potential severity of e-scooter injuries to the craniofacial region and somatic sites. Moreover, to reduce e-scooter injuries, clinicians may play a pivotal role in educating their patients on maintaining safe practices and preventive measures, including the use of protective equipment.
Author affiliations
Department of Oncology and Diagnostic Sciences, University of Maryland School of Dentistry, Baltimore, Maryland (Brooks, Bashirelahi); University of Maryland School of Dentistry, Baltimore, Maryland (Hanna).
Correspondence
John K. Brooks, DDS (jbrooks@umaryland.edu).
Conflicts of interest
None reported.
References
1. Badeau A, Carman C, Newman M, Steenblik J, Carlson M, Madsen T. Emergency department visits for electric scooter-related injuries after introduction of an urban rental program. Am J Emerg Med. 2019;37(8):1531-1533. doi:10.1016/j.ajem.2019.05.003
2. Statista. E-scooter-sharing - United States. Accessed March 20, 2025. https://www.statista. com/outlook/mmo/shared-mobility/e-scooter-sharing/united-states
4. Bentham MJ, Christopher HW, Borchert RJ, Thavakumar A, Riede P, Sadler TJ. Incidence and distribution of injuries associated with e-scooter use: a radiological perspective. Br J Radiol 2024;97(1155):567-573. doi:10.1093/bjr/tqad057
5. Brooks JK, Hooper KA, Reynolds MA. Formation of mucogingival defects associated with intraoral and perioral piercing: case reports. J Am Dent Assoc. 2003;134(7):837-843. doi:10.14219/jada.archive.2003.0281
6. Brooks JK, Reynolds MA. Ethnobotanical tattooing of the gingiva: literature review and report of a case. J Am Dent Assoc. 2007;138(8):1097-1101. doi:10.14219/jada.archive.2007.0322
8. Vernon N, Maddu K, Hanna TN, Chahine A, Leonard CE, Johnson JO. Emergency department visits resulting from electric scooter use in a major southeast metropolitan area. Emerg Radiol. 2020;27(5):469-475. doi:10.1007/s10140-020-01783-4
9. Singh P, Jami M, Geller J, Granger C, Geaney L, Aiyer A. The impact of e-scooter injuries: a systematic review of 34 studies. Bone Jt Open. 2022;3(9):674-683. doi:10.1302/26331462.39.BJO-2022-0096.R1
10. Navarro SM, Vakayil VR, Solaiman RH, et al. Risk of hospital admission related to scooter trauma injuries: a national emergency room database study. BMC Emerg Med 2022;22(1):150. doi:10.1186/s12873-022-00711-8
11. Magee LC, Chan C, Talwar D, Maguire KJ, Horn BD. A comparison of motorized and nonmotorized scooter injuries in pediatric patients seen in US emergency departments. Pediatr Emerg Care. 2022;38(6):e1314-e1319. doi:10.1097/PEC.0000000000002706
12. Hanna G, Mehra S, Haider SF, et al. Electric scooter sharing systems: an analysis of injury patterns associated with their introduction. Injury. 2023;54(7):110781. doi:10.1016/j. injury.2023.05.012
13. Faraji F, Lee JH, Faraji F, et al. Electric scooter craniofacial trauma. Laryngoscope Investig Otolaryngol. 2020;5(3):390-395. doi:10.1002/lio2.380
14. Yarmohammadi A, Baxter SL, Ediriwickrema LS, et al. Characterization of facial trauma associated with standing electric scooter injuries. Ophthalmology. 2020;127(7):988-990. doi:10.1016/j.ophtha.2020.02.007
15. Soliman L, Chang K, Sawicki N, et al. Craniofacial trauma from electronic scooter use. R I Med J (2013). 2023;106(6):42-46.
16. Kappagantu A, Yaremchuk K, Tam S. Head and neck injuries and electronic scooter use in the United States. Laryngoscope. 2021;131(11):E2784-E2789. doi:10.1002/lary.29620
17. Kim M, Lee S, Ko DR, Kim DH, Huh JK, Kim JY. Craniofacial and dental injuries associated with stand-up electric scooters. Dent Traumatol. 2021;37(2):229-233. doi:10.1111/edt.12620
18. Kim JH, Ge M, Su P, Suh JD, Ference EH. CSF leaks due to electric scooter injury. Laryngoscope 2021;131(4):E1035-E1037. doi:10.1002/lary.29104
19. Hashavia E, Shimonovich S, Shopen N, Finkelstein A, Cohen N. Secular trends in the incidence and severity of injuries sustained by riders of electric bikes and powered scooters: the experience of a level 1 adult trauma center. Injury. 2024;55(5):111293. doi:10.1016/j. injury.2023.111293
20. Hennocq Q, Schouman T, Khonsari RH, et al. Evaluation of electric scooter head and neck injuries in Paris, 2017-2019. JAMA Netw Open. 2020;3(11):e2026698. doi:10.1001/ jamanetworkopen.2020.26698
21. Lentzen MP, Grandoch A, Buller J, Kreppel M, Zöller JE, Zirk M. Mandible fractures associated with the introduction of an e-scooter-sharing system. J Craniofac Surg. 2021;32(4):14051408. doi:10.1097/SCS.0000000000007518
22. Toofany M, Mohsenian S, Shum LK, Chan H, Brubacher JR. Injury patterns and circumstances associated with electric scooter collisions: a scoping review. Inj Prev. 2021;27(5):490-499. doi:10.1136/injuryprev-2020-044085
23. Sikka N, Vila C, Stratton M, Ghassemi M, Pourmand A. Sharing the sidewalk: a case of e-scooter related pedestrian injury. Am J Emerg Med. 2019;37(9):1807.e5-1807.e7. doi:10.1016/j.ajem.2019.06.017
24. Khor SN, Chong SJ, Tan KC. Electric scooter burns and the danger of personal mobility device battery. ANZ J Surg. 2018;88(3):250. doi:10.1111/ans.14391
25. Ragonez D, Mimoun M, Chaouat M, et al. Burns caused by exploding standing electric scooters (e-scooters): a new phenomenon. J Burn Care Res. 2021;42(2):348-349. doi:10.1093/jbcr/iraa201
26. Garman CMR, Como SG, Campbell IC, Wishart J, O’Brien K, McLean S. Micro-mobility vehicle dynamics and rider kinematics during electric scooter riding. SAE Technical Paper 2020-010935. SAE Mobilus; 2020. doi:10.4271/2020-01-0935
27. Daneshvar DH, Nair ES, Baucom ZH, et al. Leveraging football accelerometer data to quantify associations between repetitive head impacts and chronic traumatic encephalopathy in males. Nat Commun. 2023;14(1):3470. doi:10.1038/s41467-023-39183-0
28. Rickelmann AD, Nguyen TM, Martyak MT. Injury patterns associated with electronic scooter crashes: an institutional observational study. Am Surg. 2023;89(8):3505-3507. doi:10.1177/00031348231161716
29. Alcohol Policy Information System. National Institute on Alcohol Abuse and Alcoholism. Blood alcohol concentration limits. Accessed March 20, 2025. https://alcoholpolicy.niaaa.nih. gov/nhtsa-policy-topics/blood-alcohol-concentration-limits/49/changes-over-time
30. Tark J. Micromobility products-related deaths, injuries, and hazard patterns: 2017-2121. September 2022. Accessed March 20, 2025. https://www.cpsc.gov/s3fs-public/ Micromobility-Products-Related-Deaths-Injuries-and-Hazard-Patterns-2017-2021.pdf? VersionId=ZwIbrSm70AOuwb4de8hlVrn63Jx_SB.e
31. Pakarinen O, Kobylin A, Harjola VP, Castrén M, Vasara H. Speed and nighttime usage restrictions and the incidence of shared electric scooter injuries. JAMA Netw Open 2023;6(11):e2341194. doi:10.1001/jamanetworkopen.2023.41194
32. Serra GF, Fernandes FAO, Noronha E, de Sousa RJA. Head protection in electric micromobility: a critical review, recommendations, and future trends. Accid Anal Prev. 2021;163:106430. doi:10.1016/j.aap.2021.106430
GENERAL DENTISTRY SELF-INSTRUCTION
Exercise
No. GD547, 2 CE Credits
Sports Dentistry
Subject Code: 154
The 15 questions for this exercise are based on the article “What every dentist needs to know about electric scooters” on pages 46-49. This exercise was developed by Douglas P. Rockwood, DDS, MAGD, ABGD, in association with the General Dentistry Self-Instruction committee.
Reading the article and successfully completing this exercise will enable you to:
• appreciate the risks associated with electric scooter (e-scooter) operation;
• characterize the nature and extent of resulting craniofacial injuries; and
• promote preventive safety measures for e-scooter operation.
Answers must be submitted online at agd.org/self-instruction by April 30, 2026.
1. Self-propelled scooters have been in existence for more than 300 years. Widespread e-scooter usage is tied to the development of a business model utilizing global positioning technology.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
2. Most e-scooter injuries occurred during nighttime hours. Nearly 55% of injuries were sustained on weekends.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
3. The greatest frequency of bony fractures involved the ________.
A. head and neck
B. upper extremities
C. lower extremities
D. torso
4. Singh et al, characterizing e-scooter injuries in 5702 individuals, reported __ patient death(s).
A. 0
B. 1
C. 2
D. 3
5. Faraji et al reported that the greatest frequency of craniofacial bone fractures involved the _____________.
A. orbital complex
B. maxilla
C. mandible
D. zygomatic process
6. Traumatic brain injuries were reported in ____% of patients with e-scooter injuries.
A. 4.6
B. 7.1
C. 11.0
D. 13.9
7. Navarro et al estimated an overall yearly mortality rate of ____ patients among hospitalized e-scooter users.
A. 1.9
B. 3.5
C. 5.2
D. 6.7
8. In a review of 125 patients with e-scooter trauma, Hennocq et al reported that the incidence of dental injuries was ___%.
A. 21
B. 35
C. 44
D. 58
9. The most common dental injury reported by Hennocq et al was ________.
A. tooth dislocation
B. crown fracture of an incisor
C. crown fracture of other teeth
D. alveolar fracture
10. Lentzen et al found the most common location for mandibular fracture was the ________.
A. ramus
B. body
C. symphysis
D. condyle
11. With regard to the traumatic impact itself, the greatest percentage of e-scooter injuries occurred subsequent to ________.
A. a fall
B. collision with a vehicle
C. collision with an unspecified object
D. striking a pedestrian
12. Which of the following ranges describes the percentage of e-scooter injuries attributable to device malfunction?
A. less than 3%
B. 3% to 7%
C. 8% to 11%
D. 12% to 16%
13. Faraji et al reviewed e-scooter injuries in 206 individuals and found that ____% of the patients were engaged in alcohol consumption at the time of the incident.
A. 31.6
B. 46.1
C. 54.2
D. 63.1
14. The operating speed of e-scooters is another risk factor for injury. Navarro et al noted that 60.0% of riders were traveling more than 20 mph, while 40.0% were traveling less than 20 mph.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
15. Soliman et al reviewed 25 patients with cutaneous facial lacerations and found the most common site to be the ________.
A. forehead
B. chin
C. nose
D. lip
Complementary examinations in the diagnosis of Sjögren syndrome: a report of 2 cases
Sjӧgren syndrome (SS) is an autoimmune disorder characterized by lymphocytic infiltration of exocrine glands. Its clinical manifestations vary, ranging from sicca syndrome, which is characterized by xerostomia, xerophthalmia, and xeroderma, to the systemic involvement of organs. SS typically affects middle-aged women and may be associated with other autoimmune diseases. This article reports the diagnosis and treatment of SS in 2 women aged 58 and 56 years, highlighting the importance of proper disease management and complementary diagnostic tests. The patients reported xerostomia, xerophthalmia, and difficulty eating. Both had been previously diagnosed with other autoimmune diseases and exhibited unfavorable oral conditions. The diagnostic process comprised sialometry; anti-SSA, anti-SSB, and antinuclear antibody factor blood tests; ophthalmologic tests; biopsy of minor salivary glands; and ultrasound of major salivary glands. Results confirmed the diagnosis of SS in each patient. Subsequently, the patients received multidisciplinary treatment and support, but follow-up examinations showed no substantial improvement. Given the range of clinical manifestations that can mimic other diseases, delays in SS diagnosis are common and can lead to considerable patient morbidity. Healthcare professionals involved in the diagnosis of SS must possess knowledge about the necessary complementary tests and perform them when appropriate.
Received: July 30, 2024
Accepted: October 8, 2024
Keywords: diagnosis, diagnostic techniques and procedures, Sjӧgren syndrome
Autoimmune diseases are characterized by a dysregulated immune system that produces mechanisms to attack the body’s own structures, resulting in a chronic inflammatory response. Of the more than 50 types of autoimmune diseases that have been identified, Sjögren syndrome (SS) is the second most common.1
Epidemiologically, SS affects around 2.7% of the general population, especially middle-aged women, with a prevalence of 8 affected women for every affected man.2 SS is characterized by lymphocytic infiltration of the parenchyma of exocrine glands, resulting in dysfunction and destruction. Salivary and lacrimal glands are the tissues most commonly affected, and patients frequently complain of dry mouth (xerostomia) and dry eyes (xerophthalmia). The combination of xerostomia, xerophthalmia, and xeroderma (dryness of the skin) characterizes sicca syndrome.2-4
SS can occur in an isolated form (primary SS) or in association with other autoimmune diseases (secondary SS) such as systemic lupus erythematosus, scleroderma, and rheumatoid arthritis. A diagnosis of secondary SS requires the presence of a previously identified autoimmune disease in addition to the occurrence of oral symptoms, ocular symptoms, and other changes associated with SS.2,3
A diagnosis of SS involves exclusion of other conditions that can result in sicca syndrome as well as analysis of clinical, laboratory, and histopathologic findings. Various criteria for diagnosing SS have been proposed and evaluated since the 1970s. Currently, the most accepted set is that created by the American College of Rheumatology (ACR) together with the European Alliance of Associations for Rheumatology (EULAR; formerly the European League Against Rheumatism).5 The ACR-EULAR 2016 criteria for SS diagnosis consider 5 items: (1) positivity for anti-SSA (also known as anti-Ro) antibody is assigned 3 points; (2) ocular staining score ≥ 5 or van Bijsterveld score ≥ 4 (ocular surface damage) in at least 1 eye is assigned 1 point; (3) Schirmer test ≤ 5 mm/5 min (low tear production) in at least 1 eye is assigned 1 point; (4) unstimulated total salivary flow rate ≤ 0.1 mL/min is assigned 1 point; and (5) minor salivary gland with focal lymphocytic sialadenitis and focus score of ≥ 1 focus/4 mm2 is assigned 3 points.5 A score ≥ 4 points is considered a confirmed diagnosis of SS. Ultrasound evaluation of major salivary glands and the introduction of new biomarkers may enable the development of new diagnostic criteria.6,7
Since SS has different manifestations, management of the condition must be multidisciplinary, involving, for example, an ophthalmologist, a rheumatologist, and a dental surgeon.
Treatment aims at symptom control and immunosuppression when organs are involved, encompassing pharmacologic and nonpharmacologic strategies to preserve, replace, and stimulate glandular secretions, reducing local inflammation.6-9
Lack of knowledge on the part of professionals, compounded by the fact that SS is often associated with other diseases with similar manifestations, frequently results in delayed diagnosis or underdiagnosis that contributes to a significant worsening of patients’ quality of life. This article reports on 2 clinical cases of SS, emphasizing the importance of clinicians’ knowledge and appropriate performance of complementary tests during the diagnostic process.
Case reports
Both patients provided informed consent for their treatment and the use of their images and clinical data for this article.
Case 1
A 58-year-old woman attended a dental consultation following a referral from a rheumatologist for the investigation of sicca syndrome. The patient reported progression of xerostomia, difficulty eating, and xerophthalmia, with onset of symptoms 20 years earlier, in 2002, as well as recent positive results for anti-SSA antibody, anti-SSB (also known as anti-La) antibody, and antinuclear antibody (ANA).
She had a history of antineoplastic treatment for bowel cancer, toxoplasmosis in 2017, infarction in late 2021, Raynaud phenomenon, hypothyroidism, osteopenia, gastroesophageal reflux, and unstable angina. She had smoked for 15 years but quit smoking 20 years before she presented for examination. At the time, the patient took the following medications: clopidogrel, 75 mg; trimetazidine dihydrochloride, 80 mg; hidrosmin, 200 mg; domperidone/cinnarizine, 10 mg/25 mg; calcium/ vitamin D supplement, 600/400 mg; ezetimibe/simvastatin, 10/20 mg; enalapril, 20 mg; levothyroxine, 88 mg; and hydroxychloroquine, 400 mg.
Extraoral and intraoral clinical examinations revealed lip dryness, angular cheilitis, dehydrated mucous membranes, tongue coating, and an erythematous macule associated with
a 3-mm-diameter ulceration at the tip of the tongue, which the patient associated with episodes of pain (Fig 1). Diascopy resulted in lesion ischemia. Sclerotherapy with ethanolamine 0.05 g/mL diluted in sterile 0.9% saline solution (ratio of 1:2) was applied to the vascular tongue lesion in 2 sessions, with an interval of 7 days between sessions. To treat the angular cheilitis, miconazole oral gel, 200 mg, was prescribed for application on the lip commissures 3 times a day for 7 days. The patient was completely edentulous and used maxillary and mandibular dentures.
Given the clinical hypothesis of SS, sialometry was performed, and the results for unstimulated and stimulated salivary flow indicated severe hyposalivation (unstimulated flow = 0.0 mL/min). An opinion from a cardiologist, a complete blood count, and a coagulogram were requested. The patient was given guidelines for oral hygiene, prosthesis care, and salivary flow stimulation measures along with a prescription for artificial saliva for use as needed (composition: carboxymethylcellulose, 8.0 g; xylitol solution 70%, 4.3 g; potassium chloride, 0.96 g; sodium chloride, 0.67 g; magnesium chloride, 0.04 g; sodium fluoride, 0.2 g; calcium chloride, 0.12 g; potassium phosphate, 0.27 g; methylparaben, 0.01 g; propylparaben, 0.1 g; and distilled water).
Subsequently, the patient was evaluated by an ophthalmologist. The result of the Schirmer test was 2 mm in both eyes; the tear film breakup time was reduced in both eyes (< 5 seconds); and ocular staining revealed sparse punctate keratitis throughout the cornea in both eyes.
After the initial consultation, excisional biopsy of the minor salivary glands was performed. The procedure removed 5 minor salivary glands from the lower labial mucosa, and there were no adverse events during surgery. The sample was stored in a 10% formaldehyde solution and sent to the pathology laboratory for anatomopathologic examination. Results showed chronic sialadenitis, and there was microscopic visualization of predominantly focal lymphocytic infiltration, compatible with SS. Additionally, ultrasonography of the major salivary glands showed a reduction in volume and diffuse heterogenicity in the texture of glandular parenchyma, suggesting a chronic inflammatory process.
On confirmation of the SS diagnosis, the patient was informed about the disease, the need to continue the prescribed treatments of artificial saliva and salivary stimulation, the importance of maintaining oral hygiene habits and increasing water intake, the need to replace dentures over time, and the value of multidisciplinary follow-up (dentistry, rheumatology, and ophthalmology). The patient continues to attend follow-up appointments every 18 months and has thus far exhibited no change in symptoms or sialometric parameters.
Case 2
A 56-year-old woman presented with chief concerns of lack of saliva and difficulty eating. She mentioned that she had received a diagnosis of SS about 10 years prior and reported that the diagnosis was established through medical consultations and routine examinations, although she could not identify the specific tests performed. Since then, she had been observing considerable worsening of xerostomia and xerophthalmia.
Fig 1. Case 1. Initial clinical features: lip dryness, angular cheilitis, and a vascular lesion on the tip of the tongue.
She also reported generalized joint pain—undiagnosed thus far—and hypothyroidism that was under treatment. She used levothyroxine, 88 mg daily, and lubricating eye drops containing sodium hyaluronate and dexpanthenol, 2 mg/mL.
On extraoral and intraoral clinical examinations, the patient presented extreme lip dryness, angular cheilitis in the lip commissures, and depapillation of the dorsal surface of the tongue (Fig 2). She also had erythematous and dry mucous membranes and demonstrated poor oral hygiene, as evidenced by the presence of calculus, biofilm, and gingivitis. Several cervical carious lesions were observed. The patient exhibited some tooth loss but did not use prostheses.
The diagnostic hypotheses were SS or hypovitaminosis. Sialometry was performed, and the results of unstimulated and stimulated salivary flow tests were compatible with severe hyposalivation (unstimulated flow = 0.0 mL/min). Artificial saliva was prescribed for local lubrication, ketoconazole oral gel for application in the bilateral lip commissure (4 times a day for 14 days), and dexpanthenol for lip hydration.
Multiple tests were requested for a more comprehensive diagnostic investigation, including a complete blood count; ANA, anti-SSA, anti-SSB, and rheumatoid factor titers; coagulogram; and fasting glucose, serum iron, ferritin, vitamin B12, triiodothyronine (T3), thyroxine (T4), and thyrotropin levels. The patient was referred to an ophthalmologist to investigate the xerophthalmia.
The patient was reassessed after 21 days, and the angular cheilitis and lip dryness had decreased with use of the prescribed medications (Fig 3). Examination results showed positivity for anti-SSA, anti-SSB, and ANA. The patient was referred to a rheumatologist.
An excisional biopsy of minor salivary glands was performed in the lower labial mucosa. Microscopic findings revealed focal lymphocytic chronic sialadenitis compatible with SS (Fig 4). On confirmation of the SS diagnosis, the patient was referred
magnification ×20). The specimen shows a predominantly lymphoplasmacytic inflammatory infiltrate in 4 mm2 of glandular tissue, a finding that is characteristic of Sjögren syndrome.
for treatment to improve the health of the oral environment, including prophylaxis, scaling, caries removal, and restoration placement. She was also referred for ultrasonography of the major salivary glands, which exhibited hypoechogenicity in the parotid and submandibular glands. An ophthalmologist performed the Schirmer test, finding severe dry eye syndrome in both eyes (4 mm in each eye).
Fig 2. Case 2. Initial clinical features: extreme lip dryness, angular cheilitis in the lip commissures, and depapillation of the dorsal surface of the tongue.
Fig 3. Case 2. Reduction of angular cheilitis and lip dryness following 21 days of treatment.
Fig 4. Case 2. Minor salivary gland (hematoxylin and eosin stain; original
The patient continues to attend follow-up appointments and has reported reductions in xerostomia. Examinations have revealed decreased mucosal dryness but periodic recurrence of angular cheilitis. Repeat sialometry showed negligible stimulated or unstimulated salivary flow. Guidelines on increased water intake, lip hydration, permanent use of artificial saliva, and measures to stimulate salivary flow are reinforced at all follow-up appointments.
Discussion
The appropriate use of complementary tests was essential to the diagnosis of SS in both of the reported cases. The patients in cases 1 and 2 had scores of 8 and 7, respectively, according to the ACR-EULAR 2016 criteria.5 Both had the same scores for 4 of the 5 criteria: salivary lip gland with focal lymphocytic sialadenitis = 3; positive for anti-SSA/anti-Ro = 3; Schirmer test ≤ 5 mm/5 min in at least 1 eye = 1; and unstimulated total salivary flow rate ≤ 0.1 mL/min = 1. In addition, the patient in case 1 had an ocular staining score ≥ 5 in at least 1 eye = 1. The ophthalmologist did not perform an ocular staining test for the patient in case 2.
The incidence of SS is greater in women than in men. Research points to 8 affected women for every affected man.2 Most women manifest the first symptoms between 40 and 60 years of age.1,10-12 The patient in case 1, who was 58 years of age at the time of presentation, reported sicca syndrome approximately 20 years prior; thus, she could have received the SS diagnosis much earlier, at age 38 years. The patient in case 2 reported that she had received an SS diagnosis at the age of 46 years, 10 years before the initial consultation, but was unable to recall the tests that had been performed to reach that conclusion.
Over the years, various criteria have been established for precise detection of SS and differentiation between its primary and secondary forms. Currently, the most commonly used and accepted criteria are those defined by the ACR-EULAR in 2016, which assigns scores based on positive anti-SSA/anti-Ro titers, ocular staining, Schirmer test results, unstimulated total salivary flow rate, and presence of focal lymphocytic sialadenitis. A diagnosis of SS is confirmed when the sum of the items results in a score greater than or equal to 4.5,12-15
The main symptoms of SS are oral and ocular dryness. Approximately 90% of patients with SS have oral dryness, and 95% have ocular dryness.7,8,12
The reduction in salivary flow rates is associated with a decrease in salivary immunoglobulin A levels as well as loss of saliva lubricating and buffering capacity, which can result in eating difficulties, recurrent oral infections (eg, candidiasis), greater susceptibility to caries, early tooth loss, and mucosal atrophy.16 Reduced tear flow can result in a feeling of sand or a foreign body in the eyes, burning, and dry keratoconjunctivitis.8,14,17
Both patients exhibited angular cheilitis, a condition caused mainly by decreased vertical dimension of occlusion in association with the proliferation of microorganisms; atrophy of the mucous membranes; and difficulty eating. The patient in case 1 was completely edentulous and used dentures. The patient in case 2 was missing multiple teeth and had several carious
lesions, mostly cervical. Regarding ocular manifestations, both patients reported a burning sensation, and the patient in case 1 exhibited corneal lesions in both eyes.
The investigations of xerostomia and xerophthalmia begin with salivary flow testing and ophthalmologic tests. The ACREULAR 2016 criteria establish unstimulated sialometry (≤ 0.1 mL/min), Schirmer test (≤ 5 mm/5 min in at least 1 eye), and ocular staining test (≥ 5 in at least 1 eye) as the criteria for investigating such complaints.5 Evaluation of the patient in case 1 established an unstimulated salivary flow rate of 0.0 mL/min, Schirmer test results of 2 mm in each eye, and the presence of sparse punctate keratitis in both eyes (based on ocular staining), confirming the diagnoses of hyposalivation, severe dry eye syndrome, and corneal lesions resulting from low-quality tear film. The patient in case 2 presented with hyposalivation (unstimulated salivary flow rate of 0.0 mL/min) and dry eye syndrome (Schirmer test result of 4 mm in each eye).
Biomarkers are measurable indicators of the presence or severity of a disease and thus are important not only for obtaining a quick and accurate diagnosis but also for monitoring of the patient. Diagnostic investigation of SS should include specific biomarkers during test requests, such as rheumatoid factor, ANA, anti-SSA, and anti-SSB. Anti-SSA and anti-SSB autoantibodies are the markers most strongly associated with SS and can be detected in 70% to 100% and 35% to 70% of patients, respectively.2,18 Both patients in this case report were positive for anti-SSA, anti-SSB, and ANA.
The inflammatory target of SS is primarily the epithelium of the exocrine glands, especially the lacrimal and salivary glands. Thus, biopsy of the minor salivary glands followed by anatomopathologic examination is considered an important criterion for diagnosis. Microscopic evaluation should observe predominantly lymphocytic infiltrates around the gland epithelium, and a focal score ≥ 1 focus/4 mm2 is a specific characteristic of SS. This finding has a sensitivity of 82.4% and a specificity of 86.2% in SS diagnosis.9,14,19
Patients suffering from autoimmune diseases are at higher risk of developing other similar conditions. Secondary SS can be confirmed when there is an association with other autoimmune diseases, especially systemic lupus erythematosus, rheumatoid arthritis, or systemic sclerosis. Other less-reported conditions that are sometimes associated with SS include chronic autoimmune hepatitis, hypothyroidism, and Graves disease. The literature reports that 7% to 14% of patients with SS develop hypothyroidism.17 Raynaud phenomenon is a peripheral arterial disease that has an observed relationship with secondary SS associated with systemic lupus erythematosus.2,13,17 Both patients in the present case reports were diagnosed with hypothyroidism and were under the care of endocrinologists. Additionally, the patient in case 1 had Raynaud phenomenon.
Currently, imaging tests are not included as criteria for diagnosing SS in the global consensus. However, ultrasonography of the larger salivary glands can be a valuable option for analyzing additional alterations and is a noninvasive, cost-effective, and easily accessible test. Normal salivary glands present uniformly hyperechoic and homogenous tissue; when affected by SS, they may be hypoechoic, nonhomogenous, and reduced in size and
may have hypoechoic or anechoic foci. Some studies propose future replacement of biopsy of minor salivary glands with ultrasonography of major salivary glands.2,20,21 Delli et al conducted a meta-analysis of studies that examined the properties of ultrasonography of major salivary glands in diagnosing SS and showed that ultrasonography has a sensitivity, specificity, and diagnostic odds ratio of 69%, 92%, and 33.89%, respectively.19 Ultrasonography of the major salivary glands of the patient in case 1 found diffuse heterogeneity and a reduction in volume of the glandular parenchyma. Examination of the patient in case 2 revealed diffuse hypoechogenicity in the parenchyma of the parotid and submandibular glands.
The complexity of SS coupled with a lack of professional knowledge often delays diagnosis. Estimates show a delay of up to 10 years from the onset of signs and symptoms to confirmed diagnosis in many cases.1,2 Since early detection of SS results in improved quality of life and the prevention of complications, both dentists and physicians must be informed about the criteria and know how to accurately conduct complementary tests throughout the diagnostic process.1,2,10,11
Limitations of this case series and discussion include the scarcity of SS studies in dentistry and the availability of only 2 cases suggestive of SS, which were systematically diagnosed using the ACR-EULAR criteria.5 Nevertheless, clinical case series can contribute important data to advance the understanding of diagnostic criteria, thereby making the topic of SS increasingly accessible to health professionals and improving the specificity and sensitivity of diagnostic criteria.
Conclusion
Increased knowledge about SS and the existing classification criteria may reduce underdiagnosis, resulting in improved quality of life and prevention of complications for patients. Diagnosis of SS is often complex, requiring the involvement of several professionals. Complementary tests play a fundamental role and should be understood and used appropriately by the healthcare team.
Author affiliations
Department of Biosciences and Oral Diagnosis, Institute of Science and Technology, São Paulo State University (UNESP), São José dos Campos, Brazil (Silva, Almeida, Alves); Department of Pathology, School of Medicine, Fluminense Federal University (UFF), Niterói, Brazil (Dick); Department of Specific Training and Graduate Program in Dentistry, Nova Friburgo Health Institute, Fluminense Federal University (UFF), Nova Friburgo, Brazil (Cruz); Department of Diagnosis and Therapeutics, School of Dentistry, Rio de Janeiro State University (UERJ), Rio de Janeiro, Brazil (Silva-Júnior).
Correspondence
Thaís Xavier Pereira da Silva, DDS, MS (txp.silva@unesp.br).
Conflicts of interest
None reported.
References
1. Araújo CV, Silva NM, Souza PGVD. Pathophysiology of Sjӧgren’s syndrome and its diagnostic difficulty. Res Soc Dev. 2021;10(7):e41010716989. doi:10.33448/rsd-v10i7.16989
2. Jonsson R, Brokstad KA, Jonsson MV, Delaleu N, Skarstein K. Current concepts on Sjӧgren’s syndrome—classification criteria and biomarkers. Eur J Oral Sci. 2018;126(Suppl 1):37-48. doi:10.1111/eos.12536
3. Thorne I, Sutcliffe N. Sjӧgren’s syndrome. Br J Hosp Med (Lond). 2017;78(8):438-442. doi:10.12968/hmed.2017.78.8.438
4. Jensen MLN, Troldbord AM, Pfeiffer-Jensen M, Deleuran B. Sjӧgrens syndrome. Article in Danish. Ugeskr Læger. 2021;183(5):V04210309.
5. Shiboski CH, Shiboski SC, Seror R, et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjӧgren’s syndrome: a consensus and data-driven methodology involving three international patient cohorts. Arthritis Rheumatol. 2017;69(1):35-45. doi:10.1002/art.39859
6. Stefanski AL, Tomiak C, Pleyer U, Dietrich T, Burmester GR, Dӧrner T. The diagnosis and treatment of Sjӧgren’s syndrome. Dtsch Arztebl Int. 2017;114(20):354-361. doi:10.3238/ arztebl.2017.0354
7. Negrini S, Emmi G, Greco M, et al. Sjӧgren’s syndrome: a systemic autoimmune disease. Clin Exp Med 2022;22(1):9-25. doi:10.1007/s10238-021-00728-6
9. Cavalcante WS, Lourenço SV, Florezi GP, et al. Síndrome de Sjogren primária: aspectos relevantes para os dentistas. Clin Lab Res Den. 2017:1-11. doi:10.11606/issn.2357-8041. clrd.2017.137879
10. Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology. 4th ed. Elsevier; 2016:434-437.
11. Yura Y, Hamada M. Outline of salivary gland pathogenesis of Sjӧgren’s syndrome and current therapeutic approaches. Int J Mol Sci. 2023;24(13):11179. doi:10.3390/ijms241311179
12. Manfrè V, Cafaro G, Riccucci I, Zabotti A, et al. One year in review 2020: comorbidities, diagnosis and treatment of primary Sjӧgren’s syndrome. Clin Exp Rheumatol. 2020;38 (4 Suppl 126):10-22.
13. Stefanski AL, Tomiak C, Pleyer U, Dietrich T, Burmester GR, Dörner T. The diagnosis and treatment of Sjӧgren’s syndrome. Dtsch Arztebl Int. 2017;114(20):354-361. doi:10.3238/ arztebl.2017.0354
14. Patel R, Sharane A. The epidemiology of Sjӧgren’s syndrome. Clin Epidemiol. 2014;6:247255. doi:10.2147/CLEP.S47399
15. Cafaro G, Croia C, Argyropoulou OD, et al. One year in review 2019: Sjӧgren’s syndrome. Clin Exp Rheumatol. 2019;37(3 Suppl 118):3-15.
16. Epstein JB, Villines DC, Sroussi HY. Oral symptoms and oral function in people with Sjӧgren’s syndrome. Clin Exp Rheumatol. 2015;33(1):132-133.
18. Zhan Q, Zhang J, Lin Y, Chen W, Fan X, Zhang D. Pathogenesis and treatment of Sjogren’s syndrome: review and update. Front Immunol. 2023;14:1127417. doi:10.3389/ fimmu.2023.1127417
19. Delli K, Dijkstra1 PU, Stel AJ, Bootsma H, Vissink A, Spijkervet FKL. Diagnostic properties of ultrasound of major salivary glands in Sjӧgren’s syndrome: a meta-analysis. Oral Dis. 2015;21(6):792-800. doi:10.1111/odi.12349
20. Schäfer VS, Schmidt WA. Ultrasound diagnostics in Sjӧgren’s syndrome. Article in German. Z Rheumatol. 2017;76(7):589-594. doi:10.1007/s00393-017-0305-5
Angiofibrolipomas are one of the rarest variants of lipoma, a benign mesenchymal tumor composed of adipose tissue. Histologic examination of angiofibrolipomas reveals mature adipocytes, vascular tissue, and fibrous connective tissue. This case report describes an angiofibrolipoma in the oral cavity of a 40-yearold woman. A soft, painless, pedunculated mass was attached to the distolingual gingiva in the region of the mandibular third molar. The provisional diagnosis was pyogenic granuloma. The mass was excised using electrocautery, and the tissue was submitted for histologic examination. Histologic staining revealed mature adipose tissue, fibrous tissue, and numerous small blood vessels, consistent with a diagnosis of angiofibrolipoma. Further immunohistochemical analysis with CD34 biomarker was performed to rule out spindle cell carcinoma. At the 1-year follow-up examination, no recurrence was found. However, due to the rarity of these tumors, more data are needed to determine their recurrence rate.
Lipomas are benign mesenchymal tumors that consist of mature adipocytes surrounded by a thin capsule. Lipomas present as soft, painless masses and mostly occur on the trunk and upper extremities wherever adipocytes are present. In the head and neck region, the percentage of lipomas is 15% to 20%, and only 1% to 4% of these tumors occur in the oral cavity.1
The etiology of lipomas is unknown, although a correlation between trauma and lipoma formation has been described.2 Trauma at any site results in cytokine release, leading to differentiation and maturation of preadipocytes. Lipoma shows higher predilection in men between the fourth and sixth decades of life.2
Angiofibrolipoma is a rare histologic variant of lipoma. Histologic examination of these neoplasms reveals mature adipocytes, vascular tissue, and fibrous connective tissue.3 The present case report describes the diagnosis and treatment of an angiofibrolipoma attached to the distolingual gingiva in the region of the mandibular third molar. To the authors’ knowledge, there have been no previous reports in the literature of an angiofibrolipoma located on the attached or marginal gingiva in the third molar region.
Case report
A 40-year-old woman reported to the Department of Dental Surgery, Atal Bihari Vajpayee Institute of Medical Sciences and Dr. Ram Manohar Lohia Hospital, New Delhi, India, with a chief concern of swelling in the mandibular left posterior region. The mass, which had been present for 6 months, was initially small and then grew over the course of 4 months. In the prior 2 months, there had been no change in its size. No pain was associated with the mass; however, the patient reported difficulty in chewing and swallowing.
On examination, a mass measuring approximately 10 × 8 × 8 mm was observed near the distolingual marginal and attached gingiva in the third molar region (Fig 1). The pedunculated mass was attached near the distolingual gingival margin of the third molar. The size of the peduncle was approximately 5 mm, extending from the free gingival margin to the attached gingiva 4 mm below it. The reddish pink mass had a smooth, regular surface, and no inflammation or discharge was associated with it. On palpation, the swelling was nontender, nonpulsatile, and soft. The mandible did not show any expansion. The patient’s oral hygiene was satisfactory, although some small calculus deposits were observed near the marginal gingiva.
Based on the clinical presentation, a provisional diagnosis of pyogenic granuloma was made, and the treatment plan called for excision of the growth using electrocautery. Oral prophylaxis was performed, and the patient was instructed to rinse with 0.12% chlorhexidine gluconate mouthwash twice daily for 3 days until the scheduled surgery. Blood tests (complete blood
count and random blood glucose) were performed, and the values obtained were within normal ranges.
On the day of surgery, the patient provided informed consent for the surgical procedure. The patient was asked to rinse with chlorhexidine gluconate mouthwash. The local area was swabbed with povidone iodine, and 2% lidocaine was infiltrated around the area of the peduncle. An Allis tissue forceps was used to hold the mass, and the tip of the electrocautery device was used to excise the growth from the base of the peduncle (Fig 2). Bleeding was controlled with a pressure pack. The patient was advised to consume cold foods and beverages for the first 24 hours and then to gargle twice daily with 0.12% chlorhexidine gluconate mouthwash for 1 week. Nonsteroidal anti-inflammatory drugs were prescribed for 3 days. The
patient returned for follow-up the next day and 7 days after the procedure, and healing was found to progress satisfactorily.
The excised tissue was stored in 10% formaldehyde and sent for histologic examination (Fig 3). The microscopic examination revealed a tumor lining of stratified squamous epithelium and a subepithelium consisting of mature adipose tissue, fibrocollagenous tissue, and numerous small blood vessels (Fig 4). Immunohistochemical analysis using the CD34 biomarker highlighted the smooth muscle layer in blood vessels as well as interspersed fibroblasts (Fig 5). The CD34 marker was used to rule out spindle cell carcinoma. The mass was diagnosed as an angiofibrolipoma.
The patient returned for a follow-up examination 1 year after excision, and no lesion recurrence was found.
Fig 1. Soft, painless, pedunculated mass on the distolingual gingiva in the region of the third molar.
Fig 2. Removal of the soft tissue mass using electrocautery.
Fig 3. Specimen after excisional biopsy. A. Mediolateral view. B. Superoinferior view.
A B
4. Histologic findings. A. Mature adipose tissue and fibrocollagenous tissue are interspersed with blood vessels (hematoxylin and eosin stain; original magnification ×40). B. Collagen fibers are stained blue and smooth muscles of blood vessels are stained red (Masson trichrome stain; original magnification ×40).
Fig 5. Immunohistochemistry findings. CD34 staining highlights the smooth muscle layer (brown staining) in blood vessels and interspersed fibroblasts (original magnification ×40).
Discussion
Lipomas present as soft, often painless masses and are most commonly found on the trunk and upper extremities wherever adipocytes are present. They show higher predilection in men between the fourth and sixth decades of life.4 Oral lipoma was first described in 1848 by Roux, who called the lesion a yellow epulis. 5 The precise etiology of lipomas has not been documented. According to one theory, trauma leading to cytokine release and further differentiation and maturation of preadipocytes may be an etiologic factor.2
Angiofibrolipoma is one of the rarest variants of lipoma. The major significance of this case report is the rarity of the type and location of the tumor. To the best of the authors’ knowledge, none of the cases reported in the literature to date have described the presence of an angiofibrolipoma on the attached or marginal gingiva in the third molar region.
Very few cases of angiofibrolipoma in the maxillofacial region have been recorded to date, and even fewer have been
documented in the oral cavity. Agha-Hosseini and Moslemi observed an angiofibrolipoma in the retromolar pad region of a 63-year-old man.1 Brkić et al described an angiofibrolipoma in the buccal mucosa of a 59-year-old patient.6 Epivatianos et al reported a case of angiofibrolipoma in the alveolar mucosa near the maxillary left canine and premolar.7 Gyamtsho reported an angiofibrolipoma in the soft palate of an infant.8 Rare occurrences have also been observed in the larynx, pharynx, and tonsillar region.9-11 Extraoral occurrences of angiofibrolipoma in the head and neck region have been recorded in the ear canal and the intranasal area.12,13 Other reported sites for angiofibrolipomas are the kidney, greater omentum, transverse colon, and spermatic cord.14-17
Angiofibrolipomas have 3 components: blood vessels, adipocytes, and fibrous tissue. The histologic appearance reflects this triphasic pattern and aids in the differential diagnosis of the lesion from other variants of lipoma. The differential diagnosis of angiofibrolipoma includes vascular lipoma, fibrolipoma, angiomyolipoma, and infiltrating angiolipoma.3 The histologic analysis of the specimen in the present case revealed a lining of stratified squamous epithelium and a subepithelium containing proliferating blood vessels, mature adipocytes, and dense collagenous stroma, characteristic features of angiofibrolipoma.
Electrocautery was used for excision of the lesion, and a followup examination 1 year after the procedure showed no recurrence of the lesion. Due to the rarity of the lesion, more data are needed to determine the recurrence rate of these tumors.
Conclusion
Angiofibrolipomas are a rare variant of lipomas, and they are particularly uncommon in the head and neck region. Angiofibrolipomas consist of mature adipocytes, vascular tissue, and fibrous connective tissue, and histologic examination is required for confirmation of the diagnosis. The present case report contributes to the scientific literature about this tumor, describing an angiofibrolipoma located on the previously unreported location of the attached and marginal gingiva in the third molar region.
Fig
Author affiliations
Department of Dental Surgery, Atal Bihari Vajpayee Institute of Medical Sciences and Dr. Ram Manohar Lohia Hospital, New Delhi, India (Nandan, Singh); Department of Transfusion Medicine, Atal Bihari Vajpayee Institute of Medical Sciences and Dr. Ram Manohar Lohia Hospital, New Delhi, India (Chauhan).
1. Agha-Hosseini F, Moslemi E. Angiofibrolipoma of the retromolar pad region: case report. N Y State Dent J. 2014;80(4):33-37.
2. Aust MC, Spies M, Kall S, Jokuszies A, Gohritz A, Vogt P. Posttraumatic lipoma: fact or fiction? Skinmed. 2007;6(6):266-270. doi:10.1111/j.1540-9740.2007.06361.x
3. Kershisnik W, McCarthy DJ, O’Donnell E. Angiofibrolipoma. A histologic variant of the lipoma. J Am Podiatr Med Assoc. 1986;76(2):67-70. doi:10.7547/87507315-76-2-67
4. Johnson CN, Ha AS, Chen E, Davidson D. Lipomatous soft-tissue tumors. J Am Acad Orthop Surg. 2018;26(22):779-788. doi:10.5435/JAAOS-D-17-00045
5. Kumaraswamy S, Madan N, Keerthi R, Shakti S. Lipomas of oral cavity: case reports with review of literature. J Maxillofac Oral Surg. 2009;8(4):394-397. doi:10.1007/s12663-0090096-6
6. Brkić A, Ozçamur C, Gürkan-Köseoğlu B, Olgac V. Angiofibrolipoma of the buccal mucosa: a case report. J Oral Sci. 2010;52(1):173-176. doi:10.2334/josnusd.52.173
7. Epivatianos A, Kolokotronis A, Matiakis A, Poulopoulos A. Angiofibrolipoma of the oral cavity. J Investig Clin Dent. 2010;1(1):47-49. doi:10.1111/j.2041-1626.2010.00003.x
8. Gyamtsho S. Angiofibrolipoma of the soft palate: a very rare cause of upper air way obstruction in an infant. Bhutan Health J. 2020;6(1):45-48. doi:10.47811/bhj.99
9. Bochnia M, Grabowski K, Zalewska A, Morawska-Kochman M. Angiofibrolipoma of the larynx: case report and literature review. Head Neck. 2016;38(4):E81-E83. doi:10.1002/hed.24167
10. Alkheder A, Azar A, Mustafa A. Angiofibrolipoma in the head and neck region: a case report and literature review. Ear Nose Throat J. Published online November 16, 2024. doi:10.1177/01455613241301227
11. Krausen C, Becker K, Hamann KF. Angiofibrolipoma of the tonsil. Laryngol Rhinol Otol (Stuttg). 1986;65(6):355-356.
12. Jacob A, Kneile J, Welling DB. Angiofibrolipoma of the ear canal. Laryngoscope 2005;115(8):1461-1462. doi:10.1097/01.mlg.0000171053.44103.51
13. Çetin MA, İkincioğulları A, Göktürk UG, et al. Intranasal angiofibrolipoma. Kulak Burun Bogaz Ihtis Derg. 2013;23(5):291-294. doi:10.5606/kbbihtisas.2013.04695
14. Tóth C. Kidney angiofibrolipoma. Article in German. Z Urol Nephrol. 1975;68(4):279-282.
15. Pérez-Navarro JV, Flores-Cardoza A, Anaya-Prado R, González-Izquierdo J de J, Ramírez-Barba EJ. Angiofibrolipoma of the greater omentum: case report and literature review. Article in Spanish. Cir Cir. 2009;77(3):229-232.
16. Novozhilov VN, Dolidze UR, Degterev DB, Il’ina VA, Bakhtybaev DO. Angiofibrolipoma of the transverse colon. Article in Russian. Vestn Khir Im I I Grek. 2006;165(2):102-103.
17. Liu QL, Tian B, Zhang H, Qiao DS. Angiofibrolipoma of the spermatic cord. Asian J Androl 2009;11(6):746-747. doi:10.1038/aja.2009.57
The connection between poor oral health and metabolic disease: the sugar link theory
Herman B. Dumbrigue, DMD
The purpose of this narrative review is to explore the idea that habitual and excessive intake of sugar and ultraprocessed foods (UPFs) may be the link between poor oral health (specifically dental caries) and metabolic disease and the common upstream factor that explains the association between these conditions. This proposed sugar link theory posits a parallel between declines in oral health and systemic health, beginning with the detrimental impacts of sugar and UPFs on the oral and gut microbiomes (dysbiosis). The resulting ecologic shifts produce biochemical alterations that lead to oral and systemic disease. One way for dentists to mitigate the worldwide impact of dental caries and metabolic disease is to encourage their patients to avoid habitual and excessive intake of sugar and UPFs.
There is a significant association between poor oral health (caries, periodontal disease, and tooth loss) and metabolic disease (cardiovascular disease, diabetes, hypertension, cancer, and dementia) in adults and children.1-4 Periodontal disease and tooth loss have been reported to be good predictors of adverse cardiovascular outcomes, and early childhood caries and severe dental caries in adults were associated with obesity and a higher prevalence of metabolic disease in the populations studied.1-4 While the correlation between poor oral health and metabolic disease seems to be consistent, causality has not been established. Common risk factors and biologic mechanisms may explain the connection between oral health and systemic health.
In a review of the link between poor oral health and cardiovascular disease, Gianos et al proposed that the biologic mechanisms that link both conditions may include bacterial translocation, inflammatory mechanisms, and immune activation.4 Bacteremia from periodontal disease could lead to atherosclerosis through platelet activation, endothelium and plaque invasion, and oxidative stress. Periodontal disease may also be linked to atherosclerosis via inflammatory mediators (eg, interleukin 1, interleukin 6) acting on fibrinogen and C-reactive protein, as well as T-cell–mediated and lipoproteininduced immune responses.4
The mouth is inhabited by more than 700 species of oral microbes colonizing soft oral mucosal tissues and hard surfaces of teeth, and these microorganisms could be disseminated in systemic circulation.5 Varying degrees of bacteremia have been demonstrated immediately following scaling in patients with periodontal disease, oral microbes have been detected in atherosclerotic plaques, and thrombi from patients who suffered acute heart attacks were found to carry oral microbes, suggesting their involvement in atherosclerotic plaque inflammation and instability.6-8 Oral microbes from cavitated carious lesions may travel to the dental pulp and, if untreated, develop into chronic apical periodontitis. This may lead to an inflammatory response in endothelial coronary cells via increased production of matrix metalloproteinases.4,9 Kim et al evaluated coronary heart disease risk based on caries status in a large cohort of middle-aged patients and found that patients with severe dental caries had a significantly higher risk of coronary heart disease.10
Upstream of the biologic mechanisms described, there is a common risk factor that makes the association between poor oral health and metabolic disease more obvious and understandable, but the connection is not often recognized: habitual and excessive intake of sugar and ultraprocessed foods (UPFs). The addition of excessive amounts of sugar in the manufacturing of UPFs to make these products more palatable, desirable, and
Oral health
Excessive consumption of sugar and UPFs
Oral dysbiosis
Altered biochemistry (pH)
Tooth demineralization
Dental caries
Tooth loss
Abbreviation: UPFs, ultraprocessed foods.
Systemic health
Excessive consumption of sugar and UPFs
Gut dysbiosis
Altered biochemistry (hormones)
Insulin resistance
Metabolic disease
Early death
commercially successful has helped make dental caries the most prevalent chronic disease worldwide and a major global public health problem.11 Sugar has a detrimental effect on both the oral and gut microbiomes, leading to adverse local and systemic health consequences. Further, the removal of fiber from UPFs to prolong shelf life and facilitate storage and transport diminishes satiety and the feeling of fullness after these products are consumed, worsening the negative impact of carbohydrates on health.
The mouth serves as the entrance to the digestive system. Food enters the oral cavity and proceeds through the digestive tract, where digestion and absorption occur. Absorbed nutrients are then available to all cells in the body for utilization in metabolism, the biochemical processes within cells that transform food into the energy that allows the body to move, think, and grow. Diet has been implicated as a major contributor to metabolic disease, and it is plausible that the types of food that cause metabolic disease also cause the most common oral disease—dental caries.12 If this is the case, dental caries may be considered a harbinger of developing metabolic disease.
The purpose of this narrative review is to explore this idea and propose a parallelism between downward declines in both oral health and systemic health, beginning with the adverse effects of sugar and UPFs on the oral and gut microbiomes (ie, dysbiosis). These ecologic shifts lead to biochemical alterations that result in oral and systemic disease. In this proposed sugar link theory, a case will be made that habitual and excessive consumption of sugar and UPFs may be the link connecting poor oral health and metabolic disease and the common upstream factor explaining the associations between poor oral health and metabolic disease and between tooth loss and early death.1,2,4,10 In this review, dental caries will be used as a proxy for poor oral health, although many studies report a compelling association between sugar consumption and periodontal disease.13 The Chart illustrates the parallel declines in oral health and systemic health as theorized in the sugar link theory.
Ultraprocessed foods
UPFs represent 73% of the US food supply and account for nearly 60% to 80% of the calories consumed in the American diet.14-16 Almost all foods undergo some form of processing; in the NOVA classification system, which labels foods based on the degree and purpose of food processing, UPFs are described as items that are created with more than 5 ingredients, often including sugars, starches, oils, fats, and proteins, and retaining minimal, if any, intact food.17 Flavor enhancers, artificial sweeteners, food coloring or dyes, and other additives are also used to simulate the flavor, texture, and look of real food.17
Monteiro et al described UPFs as highly convenient, attractive, and profitable industrial products competing with freshly prepared real foods (like meats, vegetables, and fruits).17 Items classified as UPFs include, but are not limited to, infant formulas and other baby foods; sweet or salty packaged snacks; desserts and treats such as cookies, ice cream, chocolate, pastries, cakes, and candies; mass-produced breads and rolls; breakfast cereals; processed granola and energy bars; fruit yogurts with artificial sweeteners; sweetened beverages such as carbonated, energy, milk, fruit, and cocoa drinks; powdered meat extracts and instant sauces; instant soups and noodles; so-called healthy and diet products such as powdered or fortified meal substitutes; and most ready-to-heat products, including pasta, pizza, chicken nuggets, fish sticks, hot dogs, and other reconstituted meat products.17 These food products are intrinsically harmful to oral and systemic health.
UPFs are designed to be overconsumed—they are hyperpalatable, nonsatiating, and addictive. UPFs have been radically altered by manufacturers to last longer, taste better, and be more attractive to the consumer by subtracting nutrients and adding chemicals to enhance flavor, color, texture, and/or shelf life. The food processing alterations that make UPFs particularly harmful are the removal of insoluble fiber and the addition of excessive sugar.
Chart. Sugar link theory of the connection between poor oral health and metabolic disease.
Fiber is a complex carbohydrate (polysaccharide) that cannot be digested or absorbed by the body.18 Found in plant-based foods, fiber is considered an essential nutrient and must be consumed in the diet. Plants contain 2 types of fibers: soluble and insoluble. Both are needed in the diet for insulin sensitivity, modulation of digestive hormones, and other beneficial effects on markers underlying metabolism and inflammation.19 Soluble and insoluble dietary fibers behave differently as they course through the digestive tract. Soluble fiber turns into a gel-like substance when it combines with water, while insoluble fiber remains intact, serving as a matrix for the soluble fiber gel to be transported.19 Fiber is an essential dietary component due to its abilities to improve liver health and restore the physiologic balance of the gut microbiome.20 In UPFs, the insoluble fiber has been removed, depriving the gut microbiome of food and increasing the absorption of sugar.
The current recommendations for dietary fiber intake for adults are between 25 and 32 g for women and 30 and 35 g per day for men. The consumption of dietary fiber in the United States and in most European countries is around one-third below these recommended levels.21 Lack of dietary fiber has adverse effects on gut motility, insulin sensitivity, metabolic health, and gut microbiome ecology. Further, it has been associated with systemic chronic inflammation, depression, cardiovascular disease, colorectal carcinoma, and total mortality rates.22,23
The predominant dietary source of added sugars in the United States comes from sugar-sweetened beverages such as soda and fruit juice. While the American Heart Association recommends that women and men limit added sugar consumption to 6 and 9 tsp per day, respectively, the average daily consumption of added sugars in the United States is 22.2 tsp.24 Almost 90% of this sugar comes from UPFs.15
Sugar
Sugar is often regarded as empty calories, like the calories derived from starch. However, sugar is different because it carries the fructose molecule, which starch does not. Sugar (sucrose) contains 2 molecules: a single glucose molecule linked to a single fructose molecule. Fructose is the sweet molecule sought by taste buds and is associated with the onset of chronic metabolic disease.24 Sugar, despite being a carbohydrate, behaves as both a fat and a carbohydrate. Fructose is metabolized in the liver as fat, while glucose is metabolized as a carbohydrate.25 Cane sugar, brown sugar, beet sugar, fruit sugar, high-fructose corn syrup, maple syrup, agave, and honey all contain glucose and fructose.
Glucose is essential for life, but dietary glucose is not. Glucose is so important that the human body can produce it even if it is not included in the diet. Glucose that naturally exists unaccompanied by fructose is called starch. Consumption of glucose raises blood sugar levels and triggers the pancreas to release insulin, which drives glucose from the blood into fat cells for storage. Approximately 20% of the glucose consumed will enter the liver and be turned into glycogen; the remainder will be utilized by other organs. In the liver, excess glucose not utilized by the mitochondria will become triglycerides.26 High blood levels of triglycerides are linked to a higher occurrence of heart disease.27
Glucose is sticky and can bind to cellular proteins in vivo in a process called the Maillard (or browning) reaction, rendering proteins less flexible, accelerating aging, and disrupting organ function.28 Glycated hemoglobin (HbA1c), a measure of the percentage of hemoglobin in red blood cells bound to sugar over the previous 3-month period, is an example of the Maillard reaction.28 In addition, tissue damage can occur from the reactive oxygen species that are generated whenever protein binds to a glucose molecule.29
Fructose never exists alone in nature—it is always found with glucose. The Maillard reaction proceeds 7 times faster with fructose than it does with glucose, contributing to inflammatory responses implicated in the development of arthritis, asthma, and chronic bronchitis as well as vascular complications.30 Fructose is not converted into glycogen but rather metabolized in the liver like ethanol, causing nonalcoholic fatty liver disease and metabolic dysfunction.26,31 Glucose can be used by all organs for energy, but fructose is primarily metabolized in the liver, depleting liver cells of adenosine triphosphate and leading to uric acid production.32 Excess uric acid causes pain and swelling in the joints (gout) and inhibits nitric oxide production, affecting blood vessel elasticity and increasing blood pressure.32
Decline in oral health
Oral dysbiosis
The oral microbiome is an assortment of microorganisms that reside in the hard and soft tissues of the mouth and are organized in an ecologic system that provides important benefits to the host.33 Estimated to be between 500 and 700 species, these microbes are native residents of the oral cavity that may become pathogenic when their normal environment is disturbed by dietary alterations or when salivary flow is reduced. Disease development is not solely influenced by the existence of bacteria in the oral cavity. The dental biofilm, therefore, is necessary but not sufficient for caries to develop.34
Sugar-rich diets render dental biofilms cariogenic. The oral microbiome that resides in the dental biofilm efficiently metabolizes sugars into acids. As the biofilm becomes more acidic, a change in the microbial composition occurs, favoring bacteria that survive better in this acidic environment and inhibiting the growth of beneficial bacteria found naturally in dental plaque— a process called dysbiosis. 35 In an environment rich in sucrose and other fermentable carbohydrates, the ecologic balance moves toward an ecologic dysbiosis.36 These ecologic changes in bacterial composition within the dental biofilm, where less prevalent components increase in abundance and competitiveness, lead to disease.35,37-41 Patients with xerostomia are even more susceptible to dysbiosis because of reduced acid buffering and decreased acid removal rate from the tooth surface.35
Altered biochemistry (pH)
Dysbiosis renders the dental biofilm cariogenic, lowering pH and accumulating acids discharged within the dental biofilm fluid, thereby establishing and sustaining an acidic environment.42 Lingström et al investigated the pH changes of dental plaque in response to dietary sugar and showed decreasing pH values in response to increasing exposure times.43 In addition to the acid produced from fermentation of sugar by oral bacteria,
high acid content in many food and drink products lowers salivary pH and contributes to caries development.
Saliva helps to maintain the oral cavity at a pH level of about 6.75 to 7.25. The low intrinsic pH of sugar-sweetened beverages (2.04) decreases salivary pH from an average baseline level of 7.18 to 5.65 almost immediately after the drink is consumed.44 The sugar in a single 12-oz can of soda exceeds the American Heart Association’s recommended daily limits for sugar for both men and women.24 Prolonged and frequent consumption of sugar-sweetened beverages decreases salivary pH and leads to repeated episodes of low plaque pH from both the intrinsic acidity of the beverage and the fermentation of sugars by the oral microbiome, causing shifts in microbial flora and more acid production. A sustained acidic plaque environment breaks the mineral balance of the tooth surface. In this acidic environment, a change occurs in the equilibrium of the dental biofilm, transitioning from a net gain to a net loss in mineral content—that is, demineralization.37
Demineralization
Changes in pH will affect the chemical makeup of the biofilm fluid and its level of mineral saturation, thus affecting the chemical composition of the tooth surface. When acid attacks enamel and dentin, the organic and inorganic matrix components dissolve to a certain degree, so that the water contained within the enamel and dentin facilitates both the absorption of acid into the tooth and leaching of minerals from the tooth.45 The processes of demineralization and remineralization occur on the enamel surface at its interface with the biofilm in response to alterations in the surrounding pH; net mineral loss or gain occurs as a result of a range of ongoing events at any given point in time.45 Demineralization occurs when the pH of the dental biofilm decreases below the critical pH levels of 5.5 and 6.2 for enamel and dentin, respectively. Mineral loss is the beginning of the decalcification process and, if not interrupted, progresses to the early stages of carious lesion development.46
Dental caries
Diet influences and initiates the onset of dental caries.11 The World Health Organization states that dental caries is the world’s most prevalent chronic disease, and sugar is the essential dietary ingredient needed for caries to develop.47 Sheiham concluded that there is overwhelming evidence establishing sugar as the primary etiologic factor for dental caries.48 Without sugar, the prevalence of dental caries would be negligible.47-50
Dental caries was traditionally defined as an infectious and communicable disease and considered to be an infection of the enamel and dentin caused by specific bacteria.51-53 It was believed that infants acquired these bacteria from their mothers and only after primary tooth eruption.54 Dental caries is now understood as a noncommunicable disease (NCD).34,55,56 NCDs are a group of health conditions that have been exacerbated by modern diets and lifestyles and may be recognized by the analysis of demographic and epidemiologic transitions. NCDs are chronic diseases that have multiple common determinants that can account for their onset, which may include hereditary, physiologic, behavioral, and environmental factors.57 The current understanding of NCDs places dental caries
in the same category as cardiovascular disease, cancer, dementia, diabetes, and hypertension, providing opportunities to address risk factors and develop common strategies to prevent or mitigate the risk of acquiring these diseases.55,56
Tooth loss
Dental caries, if untreated, will progress and undermine tooth structure, which may lead to coronal fracture and, eventually, tooth loss. If the initial steps of patient education, prevention, and intervention fail, the dental profession has a final solution—tooth extraction. In the United States, approximately 2% of adults aged 20 to 64 years are edentulous.58 Among adults aged 65 or older, 26% have 8 or fewer teeth, and 17% have lost all of their teeth.58,59
Loss of teeth impairs chewing, nutrition, and quality of life. It turns out that tooth loss also affects quantity of life—that is, longevity. In exploring the hypothesis that risk factors common to both oral and systemic NCDs may increase the risk of both tooth loss and early death, Friedman and Lamster considered 2 questions.60 First, they asked, “Can we conclude that the number of teeth in aging humans can affect longevity and life expectancy?” Second, they asked, “Is tooth loss a predictor of shortened longevity?” They concluded that the answer to both questions was yes.60
Decline in systemic health
Gut dysbiosis
The gut microbiome is a complex collection of over 100 trillion microbes that affect human nutrition, metabolism, physiology, and immune response. Its composition is largely affected by environmental exposure to food and drugs as well as anthropometric features.61 UPFs that are high in sugar and lacking in fiber alter the bacterial composition in the gut environment. Gut dysbiosis has been implicated in obesity, chronic gastrointestinal diseases, metabolic disease, colorectal cancer, and impaired neurocognitive function.61-63
Fiber is food for gut bacteria, and when fiber is absent from the diet, the deprived microbiome starts to degrade the intestinal mucus layer. Fructose also contributes to the disruption of the intestinal barrier; excessive fructose metabolism in intestinal cells reduces the production of proteins that are important for maintaining gut barrier integrity. Gut dysbiosis leads to gut permeability and leakage of bacterial lipopolysaccharides into systemic circulation, leading to chronic inflammation and hormone imbalance.64 The “leaky gut” exposes the body to inflammatory mediators and reactive oxygen species, exacerbating insulin resistance and further increasing levels of insulin in the blood.65
Altered biochemistry (hormones)
Two of the hormones most impacted by excessive sugar consumption and the absence of dietary fiber are insulin and leptin. Insulin is an energy storage hormone. Carbohydrate-rich foods increase blood glucose levels, prompting insulin to be released from the pancreas according to the rise in the level of blood glucose. Insulin stimulates glycogen synthesis in the muscles and the liver and drives storage of excess fatty acids into fat cells, where they become triglycerides. Insulin generates fat, and the more insulin levels rise, the more fat is produced.66
Leptin is a protein produced and secreted by adipose tissue. It travels through the bloodstream and lets the hypothalamus know when enough energy has been stored in the fat cells. The fat cells, through leptin, tell the hypothalamus whether there is an energy surplus (obesity) or deficiency (starvation).67
The ventromedial hypothalamus (VMH) is the part of the brain that obtains information from the digestive tract through leptin and insulin, adjusts energy expenditure accordingly, and controls appetite.68 The VMH is continuously monitoring leptin signaling. When the leptin signal functions as it should, a person maintains energy balance—metabolizing energy normally. When the VMH is unable to detect leptin, the brain construes this deficient signal as starvation and signals the body to take any necessary action to replenish its energy supply.69
As it turns out, insulin inhibits leptin signaling. When insulin circulates in the blood unabated, the VMH cannot detect the leptin signal and thus fails to direct the body to stop eating, even in a state of energy surplus. Most people with obesity suffer from leptin resistance. They have plenty of leptin, but their brain cannot see it. Thus, the brain assumes a state of starvation and consequently attempts to increase the energy supply and decrease energy expenditure.68 The altered biochemistry drives the behaviors of overeating and lack of desire to exercise.
This biochemical alteration is driven by insulin, and excessive insulin is driven by excessive sugar consumption. In the absence of dietary fiber, sugar and starch are absorbed more readily in the gut, leading to increases in plasma insulin and triglyceride concentrations.70
Insulin resistance
The main driver of metabolic syndrome is insulin resistance. While there are many reasons a person may develop insulin resistance, excessive consumption of UPFs is one of the most common.71 Insulin resistance develops when muscles, fat, and liver cells are no longer able to respond appropriately to insulin. Glucose cannot enter the cells, so the cells starve and communicate to the pancreas to produce more insulin. Glucose builds up in the blood while the cells are starving, which leads to organ dysfunction. Insulin resistance is not due to low insulin levels but rather elevated levels (hyperinsulinemia) that develop because the cell is unable to respond to the insulin signal.72 Habitual and excessive consumption of sugar and UPFs increases insulin secretion and causes hyperinsulinemia. Insulin regulates its own sensitivity—continuous exposure to insulin causes a decrease in its cell receptors, resulting in insulin resistance.71,72 The body responds to excessively high levels of any substance by developing a diminished response to it; thus, chronically high levels of insulin cause insulin resistance. Cell dysfunction from chronically high insulin levels leads to metabolic disease, morbidity, and premature death.73
Metabolic disease
Metabolic syndrome is defined as “a cluster of metabolic dysregulations including insulin resistance, atherogenic dyslipidemia, central obesity, and hypertension,” as well as diabetes and cardiovascular disease.74 Each condition increases a person’s chance of early death. It is a spectrum of diseases, and not all
of the diseases affect each person diagnosed with metabolic syndrome. Obesity is one marker for metabolic disease, but even people of normal weight or who are underweight can have metabolic disease.
The lack of dietary fiber in UPFs raises the likelihood for metabolic disease, and the habitual and excessive consumption of sugar leads to metabolic disease both directly and indirectly—directly via impairment of the regulation of carbohydrate and lipid metabolic processes and indirectly via weight gain and increased adiposity, which lead to carbohydrate and lipid metabolic dysregulation.75,76
Early death
Globally, in 2019, 7 of the 10 leading causes of death were NCDs. NCDs were responsible for 74% of all deaths, with heart disease as the leading cause, followed by stroke.77 Obesity is also associated with decreased longevity. At a population level, people with obesity die younger. An actuarial analysis in 2003 demonstrated that life expectancy decreased significantly in obese younger adults. It was estimated that White men in their 20s with a body mass index of 45 or greater lost up to 13 years of life, while Black men in the same age group lost up to 20 years of life.78
However, people do not die of obesity—people die of diseases that accompany obesity, such as heart disease, hypertension, diabetes, cancer, and dementia, metabolic decompensations that link obesity to early death. The habitual and excessive consumption of UPFs and sugar not only directly and indirectly causes metabolic disease but also is significantly associated with premature deaths worldwide.79-82
Discussion
The etiology and pathogenesis of dental caries and systemic metabolic disease are multifactorial and complex, as are the possible links between both conditions. The proposed sugar link theory between poor oral health and metabolic disease is intended to highlight the parallelism in the downward declines in oral health and systemic health, with sugar and UPF consumption as a common primary upstream cause. Downstream of habitual sugar and UPF consumption, other proposed mechanisms (bacterial translocation, chronic inflammation, and immune activation) may play roles in common biologic processes of disease progression.4
The consumption of sugar and UPFs has increased globally, and both are ubiquitous in the current food environment. They occupy most of the square footage of most grocery stores, with real food (meats, fruits, and vegetables) relegated to either end of the floor plan—indeed, the shopper must travel through the UPF section to get from the meat to the produce section. As if that arrangement did not provide enough temptation, neatly packaged UPFs and drinks are attractively displayed at the checkout counters to break the customer’s last ounce of willpower. UPFs are delicious, cheap, addictive, and attractive, promoting the individual’s urge to consume them for pleasure even in the absence of physical hunger. This hedonic pathway of food reward subverts normal satiety cues to the brain. 24 The addicting quality of sugar and UPFs, as designed and manufactured by the food industry, makes it difficult for individuals to abstain
from them. Biochemistry drives behavior, and the altered hormones (eg, insulin and leptin) resulting from UPF consumption drive further the behaviors that interfere with healthy practices like eating a balanced diet and getting regular exercise.
68
UPF consumption alters the oral and gut microbiomes to the detriment of the host. The oral and gut bacteria outnumber human cells 10 to 1 and must be fed properly to maintain a healthy symbiotic relationship. Dietary fiber is food for gut bacteria, and its absence in UPFs forces the bacteria to feed on the intestinal mucus barrier instead, increasing the risk of gut permeability. From oral and gut microbial dysbiosis to alterations in biochemical processes to consequent metabolic changes, habitual and excessive consumption of sugar and UPFs ultimately leads to metabolic disease. It has been reported that only about 10% of metabolic diseases can be explained by genetics. 83 The other 90% are likely environmental, specifically, the quality and quantity of the diet.
84
Despite significant improvements in dental care and technology, dental caries is still the most prevalent oral disease globally. Of the $4.1 trillion in annual health expenditure in the United States, 90% is for treatment of NCDs. 85 Both modern dentistry and modern medicine prioritize spending and efforts on addressing downstream symptoms instead of tackling the underlying issues or upstream root causes. When dental caries is viewed and understood as a noncommunicable and behavioral disease similar to cardiovascular disease, cancer, dementia, diabetes, and hypertension, it becomes easier to recognize the link between poor oral health and metabolic disease— sugar and UPFs.
A proposed solution to mitigate the risk and control the progression of metabolic disease and dental caries is simple but difficult to accomplish: eat real food and avoid UPFs. 86 This solution requires controlling the food environment at home, school, and the workplace. UPFs and drinks should not be made available or easily accessible in these places, where people spend most of their lives. Instead, home-cooked meals using real food ingredients (meats, fish, fruits, nuts, and vegetables) should be encouraged and promoted. Real foods are healthy for the person and the microbiome, and a healthy microbiome is essential for metabolic health.
Healthy eating begins at the grocery store—what is bought and brought home will be eaten. If UPFs are in the pantry, they will be consumed. Behavioral change is difficult or impossible if UPF products are available in the immediate environment. Unfortunately, the popular adage “everything in moderation” does not work if the substance in question is addictive; for UPFs, a more appropriate saying would be “moderation kills.” They kill slowly—eroding years from life, and life from years. The goal of living to a ripe old age should not be expected to come with a dentition completely supported by implants and/or medicationcontrolled metabolic disease, a situation often seen today. Longevity is better enjoyed with an intact dentition and metabolic health.
Conclusion
The habitual and excessive consumption of sugar and UPFs may help explain the observed association between poor oral health and metabolic disease. As an upstream cause, consumption of sugar and UPFs leads to dysbiosis of the oral and gut microbiomes, altering biochemical processes, which in turn produces metabolic changes that negatively affect oral and systemic health. One way for dentists to mitigate the worldwide epidemic of dental caries and metabolic disease is to encourage their patients to avoid excessive consumption of sugar and UPFs and eat real food instead.
Author affiliation
Department of Comprehensive Dentistry, Texas A&M University College of Dentistry, Dallas.
Correspondence
Herman B. Dumbrigue, DMD (dumbrigue@tamu.edu).
Conflicts of interest
None reported.
References
1. Lee HJ, Choi EK, Park JB, Han KD, Oh S. Tooth loss predicts myocardial infarction, heart failure, stroke, and death. J Dent Res. 2019;98(2):164-170. doi:10.1177/0022034518814829
2. Cao X, Wang D, Zhou J, Yuan H, Chen Z. Relationship between dental caries and metabolic syndrome among 13998 middle-aged urban Chinese. J Diabetes. 2016;9(4):378-385. doi:10.1111/1753-0407.12424
3. Sabella FM, Feiria SNB, Ribeiro AA, et al. Exploring the interplay between oral diseases, microbiome, and chronic diseases driven by metabolic dysfunction in childhood. Front Dent Med. 2021;2:718441. doi:10.3389/fdmed.2021.718441
4. Gianos E, Jackson EA, Tejpal A, et al. Oral health and atherosclerotic cardiovascular disease: a review. Am J Prev Cardiol. 2021;7:100179. doi:10.1016/j.ajpc.2021.100179
5. Kilian M, Chapple ILC, Hannig M, et al. The oral microbiome—an update for oral healthcare professionals. Br Dent J. 2016;221(10): 657-666. doi:10.1038/sj.bdj.2016.865
6. Forner L, Larsen T, Kilian M, Holmstrup P. Incidence of bacteremia after chewing, tooth brushing and scaling in individuals with periodontal inflammation. J Clin Periodontol 2006; 33(6):401-407. doi:10.1111/j.1600-051X.2006.00924.x
7. Reyes L, Herrera D, Kozarov E, Roldán S, Progulske-Fox A. Periodontal bacterial invasion and infection: contribution to atherosclerotic pathology. J Clin Periodontol. 2013;40(14):S30-S50. doi:10.1111/jcpe.12079
8. Ohki T, Itabashi Y, Kohno T, et al. Detection of periodontal bacteria in thrombi of patients with acute myocardial infarction by polymerase chain reaction. Am Heart J. 2012;163(2):164-167. doi:10.1016/j.ahj.2011.10.012
9. Jain A, Bahuguna R. Role of matrix metalloproteinases in dental caries, pulp and periapical inflammation: an overview. J Oral Biol Craniofac Res. 2015;5(3):212-218. doi:10.1016/j. jobcr.2015.06.015
10. Kim K, Choi S, Chang J, et al. Severity of dental caries and risk of coronary heart disease in middle-aged men and women: a population-based cohort study of Korean adults, 2002-2013. Sci Rep. 2019;9(1):10491. doi:10.1038/s41598-019-47029-3
11. Moynihan P. Sugars and dental caries: evidence for setting a recommended threshold for intake. Adv Nutr. 2016;7(1):149-156. doi:10.3945/an.115.009365
12. Lutsey PL, Steffen LM, Stevens J. Dietary intake and the development of metabolic syndrome: the Atherosclerosis Risk in Communities Study. Circulation. 2008;117(6):754761. doi:10.1161/CIRCULATIONAHA.107.716159
13. Kusama T, Nakazawa N, Takeuchi K, Kiuchi S, Osaka K. Free sugar intake and periodontal diseases: a systematic review. Nutrients. 2022;14(21):4444. doi:10.3390/nu14214444
15. Martínez Steele E, Baraldi LG, Louzada MLDC, Moubarac JC, Mozaffarian D, Monteiro CA. Ultra-processed foods and added sugars in the US diet: evidence from a nationally representative cross-sectional study. BMJ Open. 2016;6(3):e009892. doi:10.1136/bmjopen2015-009892
16. Martini D, Godos J, Bonaccio M, Vitaglione P, Grosso G. Ultra-processed foods and nutritional dietary profile: a meta-analysis of nationally representative samples. Nutrients 2021;13(10):3390. doi:10.3390/nu13103390
17. Monteiro CA, Cannon G, Levy RB, et al. NOVA. The star shines bright. World Nutr. 2016;7(13):28-38.
18. Hijová E, Bertková I, Štofilová J. Dietary fibre as prebiotics in nutrition. Cent Eur J Public Health 2019;27(3):251-255. doi:10.21101/cejph.a5313
19. Weickert MO, Pfeiffer AFH. Metabolic effects of dietary fiber consumption and prevention of diabetes. J Nutr. 2008;138(3):439-442. doi:10.1093/jn/138.3.439
20. Pérez-Montes de Oca A, Julián MT, Ramos A, Puig-Domingo M, Alonso N. Microbiota, fiber, and NAFLD: is there any connection? Nutrients. 2020;12(10):3100. doi:10.3390/ nu12103100
21. Stephen AM, Champ MM, Cloran SJ, et al. Dietary fibre in Europe: current state of knowledge on definitions, sources, recommendations, intakes and relationships to health. Nutr Res Rev 2017;30(2):149-190. doi:10.1017/S095442241700004X
22. Barber TM, Kabisch S, Pfeiffer AFH, Weickert MO. The health benefits of dietary fibre. Nutrients. 2020;12(10):3209. doi:10.3390/nu12103209
23. Kim Y, Je Y. Dietary fiber intake and total mortality: a meta-analysis of prospective cohort studies. Am J Epidemiol. 2014;180(6):565-573. doi:10.1093/aje/kwu174
24. Johnson RK, Appel LJ, Brands M, et al. Dietary sugars intake and cardiovascular health: a scientific statement from the American Heart Association. Circulation. 2009;120(11):10111020. doi:10.1161/circulationaha.109.192627
25. Rippe JM, Kris Etherton PM. Fructose, sucrose, and high fructose corn syrup: modern scientific findings and health implications. Adv Nutr. 2012;3(5):739-740. doi:10.3945/ an.112.002600
26. Lustig RH. Fructose: it’s “alcohol without the buzz.” Adv Nutr. 2013;4(2):226-235. doi:10.3945/an.112.002998
27. Stauffer ME, Weisenfluh L, Morrison A. Association between triglycerides and cardiovascular events in primary populations: a meta-regression analysis and synthesis of evidence. Vasc Health Risk Manag. 2013;9:671-680. doi:10.2147/VHRM.S52713
28. Dills WL Jr. Protein fructosylation: fructose and the Maillard reaction. Am J Clin Nutr 1993;58(5 Suppl):779S-787S. doi:10.1093/ajcn/58.5.779S
29. Bonnefont-Rousselot D. Glucose and reactive oxygen species. Curr Opin Clin Nutr Metab Care. 2002;5(5):561-568. doi:10.1097/00075197-200209000-00016
30. Gugliucci A. Formation of fructose-mediated advanced glycation end products and their roles in metabolic and inflammatory diseases. Adv Nutr. 2017;8(1):54-62. doi:10.3945/ an.116.013912
31. Jensen T, Abdelmalek MF, Sullivan S, et al. Fructose and sugar: a major mediator of non-alcoholic fatty liver disease. J Hepatol. 2018;68(5):1063-1075. doi:10.1016/j. jhep.2018.01.019
32. Russo E, Leoncini G, Esposito P, Garibotto G, Pontremoli R, Viazzi F. Fructose and uric acid: major mediators of cardiovascular disease risk starting at pediatric age. Int J Mol Sci. 2020;21(12):4479. doi:10.3390/ijms21124479
33. Wade WG. The oral microbiome in health and disease. Pharmacol Res. 2013;69(1):137-143. doi:10.1016/j.phrs.2012.11.006
34. Giacaman RA, Fernández CE, Muñoz-Sandoval C, et al. Understanding dental caries as a non-communicable and behavioral disease: management implications. Front Oral Health 2022;3:764479. doi:10.3389/froh.2022.764479
35. Head D, Marsh P, Devine D, Tenuta LMA. In silico study of hyposalivation and sugar exposure on biofilm dysbiosis. JADA Found Sci. 2023;2:100019. doi:10.1016/j.jfscie.2022.100019
36. Marshall TA. Dietary implications for dental caries: a practical approach on dietary counseling. Dent Clin North Am. 2019;63(4):595-605. doi:10.1016/j.cden.2019.06.005
37. Takahashi N, Nyvad B. The role of bacteria in the caries process: ecological perspectives. J Dent Res. 2011;90(3):294-303. doi:10.1177/0022034510379602
38. Simón-Soro A, Mira A. Solving the etiology of dental caries. Trends Microbiol. 2015;23(2): 76-82. doi:10.1016/j.tim.2014.10.010
39. Lozano CP, Díaz-Garrido N, Kreth J, Giacaman RA. Streptococcus mutans and Streptococcus sanguinis expression of competition-related genes, under sucrose. J Caries Res 2019;53(2):194-203. doi:10.1159/000490950
40. Tanner AC, Kressirer CA, Faller LL. Understanding caries from the oral microbiome perspective. J Calif Dent Assoc. 2016;44(7):437-446.
41. Zhan L. Rebalancing the caries microbiome dysbiosis: targeted treatment and sugar alcohols. Adv Dent Res. 2018;29(1):110-116. doi:10.1177/0022034517736498
42. Takahashi N, Nyvad B. Caries ecology revisited: microbial dynamics and the caries process. Caries Res. 2008;42(6):409-418. doi:10.1159/000159604
43. Lingstrӧm P, van Ruyven FO, van Houte J, Kent R. The pH of dental plaque in its relation to early enamel caries and dental plaque flora in humans. J Dent Res. 2000;79(2):770-777. doi:10.1177/00220345000790021101
44. Hans R, Thomas S, Garla B, Dagli RJ, Hans MK. Effects of various sugary beverages on salivary pH, flow rate, and oral clearance rates amongst adults. Scientifica (Cairo) 2016;2016:5027283. doi:10.1155/2016/5027283
45. Fejerskov O, Nyvad B, Kidd EAM. Dental caries: what is it? In: Fejerskov O, Nyvad B, Kidd EAM, eds. Dental Caries: The Disease and Its Clinical Management. 3rd ed. Wiley Blackwell; 2015:7-10.
46. Bachand WR, Fraser OL, Park JN. The delicate balance of remineralization and demineralization. Decis Dent. 2022;8(9):32-35.
47. World Health Organization. Sugars and dental caries. November 9, 2017. Accessed March 10, 2025. https://www.who.int/news-room/fact-sheets/detail/sugars-and-dental-caries
48. Sheiham A. Dietary effects on dental diseases. Public Health Nutr. 2001;4(2B):569-591. doi:10.1079/phn2001142
49. Sheiham A, James WPT. Diet and dental caries: the pivotal role of free sugars reemphasized. J Dent Res. 2015;94(10):1341-1347. doi:10.1177/0022034515590377
50. Moynihan P, Petersen PE. Diet, nutrition and the prevention of dental diseases. Public Health Nutr. 2004;7(1A):201-226. doi:10.1079/phn2003589
51. Caufield PW, Li Y, Dasanayake A. Dental caries: an infectious and transmissible disease. Compend Cont Educ Dent. 2005;26(5 Suppl 1):10-16.
52. Anderson MH. Changing paradigms in caries management. Curr Opin Dent. 1992;2:157-162.
53. Loesche J. Role of Streptococcus mutans in human dental decay. Microbiol Rev 1986;50(4):353-380. doi:10.1128/mr.50.353-380.1986
54. Berkowitz RJ. Acquisition and transmission of mutans streptococci. J Calif Dent Assoc 2003;31(2):135-138.
55. Wolf TG, Cagetti MG, Fisher JM, Seeberger GK, Campus G. Non-communicable diseases and oral health: an overview. Front Oral Health. 2021;2:725460. doi:10.3389/froh.2021.725460
56. Pitts NB, Twetman S, Fisher J, Marsh PD. Understanding dental caries as a non-communicable disease. Br Dent J. 2021;231(12):749-753. doi:10.1038/s41415-021-3775-4
57. World Health Organization. Noncommunicable diseases. September 16, 2018. Accessed March 10, 2025. https://www.who.int/news-room/fact-sheets/detail/noncommunicablediseases
58. Centers for Disease Control and Prevention. Oral Health Surveillance Report: Trends in Dental Caries and Sealants, Tooth Retention, and Edentulism, United States, 1999–2004 to 2011–2016. Centers for Disease Control and Prevention, US Dept of Health and Human Services; 2019. https://stacks.cdc.gov/view/cdc/82756
59. Griffin SO, Griffin PM, Li CH, Bailey WD, Brunson D, Jones JA. Changes in older adults’ oral health and disparities: 1999 to 2004 and 2011 to 2016. J Am Geriatr Soc. 2019;67(6):11521157. doi:10.1111/jgs.15777
60. Friedman PK, Lamster IB. Tooth loss as a predictor of shortened longevity: exploring the hypothesis. Periodontol 2000. 2016;72(1):142-152. doi:10.1111/prd.12128
61. Valdes AM, Walter J, Segal E, Spector TD. Role of the gut microbiota in nutrition and health. BMJ. 2018;361:k2179. doi:10.1136/bmj.k2179
62. Kawano Y, Edwards M, Huang Y, et al. Microbiota imbalance induced by dietary sugar disrupts immune-mediated protection from metabolic syndrome. Cell. 2022;185(19):35013519.e20. doi:10.1016/j.cell.2022.08.005
63. Noble EE, Olson CA, Davis E, et al. Gut microbial taxa elevated by dietary sugar disrupt memory function. Transl Psychiatry. 2021;11(1):194. doi:10.1038/s41398-021-01309-7
64. Satokari R. High intake of sugar and the balance between pro- and anti-inflammatory gut bacteria. Nutrients. 2020;12(5):1348. doi:10.3390/nu12051348
65. Maersk M, Belza A, Stødkilde-Jørgensen H, et al. Sucrose-sweetened beverages increase fat storage in the liver, muscle, and visceral fat depot: a 6-mo randomized intervention study. Am J Clin Nutr. 2012;95(2):283-289. doi:10.3945/ajcn.111.022533
66. Ludwig DS, Ebbeling CB. The carbohydrate-insulin model of obesity: beyond “calories in, calories out.” JAMA Intern Med. 2018;178(8):1098-1103. doi:10.1001/jamainternmed.2018.2933
67. Flier JS. Clinical review 94: what’s in a name? In search of leptin’s physiologic role. J Clin Endocrinol Metab. 1998;83(5):1407-1413. doi:10.1210/jcem.83.5.4779
68. Morton GJ, Schwartz MW. Leptin and the central nervous system control of glucose metabolism. Physiol Rev. 2011;91(2):389-411. doi:10.1152/physrev.00007.2010
69. Leibel RL. The role of leptin in the control of body weight. Nutr Rev. 2002;60(10 Pt 2):S15S19. doi:10.1301/002966402320634788
70. Riccardi G, Rivellese AA. Effects of dietary fiber and carbohydrate on glucose and lipoprotein metabolism in diabetic patients. Diabetes Care. 1991;14(12):1115-1125. doi:10.2337/ diacare.14.12.1115
71. Lee GY, Lim JH, Joung H, Yoon D. Association between ultraprocessed food consumption and metabolic disorders in children and adolescents with obesity. Nutrients. 2024;16(20):3524. doi:10.3390/nu16203524
72. Shanick MH, Xu Y, Skrha J, Dankner R, Zick Y, Roth J. Insulin resistance and hyperinsulinemia: is hyperinsulinemia the cart or the horse? Diabetes Care. 2008;31(Suppl 2):S262-S268. doi:10.2337/dc08-s264
73. Janssen JAMJL. Hyperinsulinemia and its pivotal role in aging, obesity, type 2 diabetes, cardiovascular disease and cancer. Int J Mol Sci. 2021;22(15):7797. doi:10.3390/ ijms22157797
74. Fahed G, Aoun L, Zerdan MB, et al. Metabolic syndrome: updates on pathophysiology and management in 2021. Int J Mol Sci. 2022;23(2):786. doi:10.3390/ijms23020786
75. Chen JP, Chen GC, Wang XP, Qin L, Bai Y. Dietary fiber and metabolic syndrome: a metaanalysis and review of related mechanisms. Nutrients. 2018;10(1):24. doi:10.3390/ nu10010024
76. Stanhope KL. Sugar consumption, metabolic disease and obesity: the state of the controversy. Crit Rev Clin Lab Sci. 2016;53(1):52-67. doi:10.3109/10408363.2015.1084990
77. World Health Organization. The top 10 causes of death. August 7, 2024. Accessed March 10, 2025. https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death
78. Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB. Years of life lost due to obesity. JAMA. 2003;289(2):187-193. doi:10.1001/jama.289.2.187
79. Nilson EAF, Ferrari G, Louzada MLC, Levy RB, Monteiro CA, Rezende LFM. Premature deaths attributable to the consumption of ultraprocessed foods in Brazil. Am J Prev Med 2023;64(1):129-136. doi:10.1016/j.amepre.2022.08.013
80. Blanco-Rojo R, Sandoval-Insausti H, López-Garcia E, et al. Consumption of ultra-processed foods and mortality: a national prospective cohort in Spain. Mayo Clin Proc 2019;94(11):2178-2188. doi:10.1016/j.mayocp.2019.03.035
81. Schnabel L, Kesse-Guyot E, Allés B, et al. Association between ultraprocessed food consumption and risk of mortality among middle-aged adults in France. JAMA Intern Med. 2019;179(4):490-498. doi:10.1001/jamainternmed.2018.7289
82. Chang K, Gunter MJ, Rauber F, et al. Ultra-processed food consumption, cancer risk and cancer mortality: a large-scale prospective analysis within the UK Biobank. EClinicalMedicine 2023;56:101840. doi:10.1016/j.eclinm.2023.101840
83. Lusis AJ, Attie AD, Reue K. Metabolic syndrome: from epidemiology to systems biology. Nat Rev Genet. 2008;9(11):819-830. doi:10.1038/nrg2468
84. Bremer AA, Mietus-Snyder M, Lustig RH. Toward a unifying hypothesis of metabolic syndrome. Pediatrics. 2012;129(3):557-570. doi:10.1542/peds.2011-2912
85. Centers for Medicare & Medicaid Services. National health expenditure data: historical. December 15, 2021. Accessed March 10, 2025. https://www.cms.gov/data-research/statistics-trends-and-reports/national-health-expenditure-data/historical
86. Lustig RH. Metabolical: The Lure and the Lies of Processed Food, Nutrition, and Modern Medicine. Harper Collins; 2021:15-25.
Comparison of the clinical performance of pit and fissure sealants containing either fluoride or amorphous calcium phosphate on permanent first molars
The objective of this study was to compare the clinical performance of 2 types of pit and fissure sealants— containing either fluoride or amorphous calcium phosphate (ACP)—over a period of 24 months. In this retrospective split-mouth study, 36 fluoride-containing sealants (Clinpro) and 36 ACP-containing sealants (Aegis) were evaluated 24 months after placement in the permanent first molars of 30 children aged 6 to 7 years. The sealants were inspected for retention based on the criteria of Oulis and Berdouses, with scores of 0, 1, and 2 representing total retention, partial loss, and total loss, respectively. In addition, the sealants were assigned scores for marginal integrity, marginal discoloration, and anatomical form based on the criteria of Feigal et al. Differences between groups in the occurrences of each evaluation variable were compared using relative risk with its 95% CI as well as the chi-square or Fisher exact test. The level of significance was set at P = 0.05. The retention success rates of the fluoride and ACP sealants after 24 months were 66.6% and 61.1%, respectively, but the difference was not statistically significant (P > 0.05). The overall clinical success of the fluoride-containing sealant was slightly greater than that of the ACP-containing sealant in terms of marginal discoloration and anatomical form; however, these differences were not statistically significant (P > 0.05). The marginal integrity of the sealant with ACP nanofillers was greater than that of the fluoride-containing sealant, but the difference did not reach statistical significance (P > 0.05). After a 24-month follow-up period, no significant disparities in clinical performance were observed between fluorideand ACP-containing sealants in terms of retention rates, marginal integrity, marginal discoloration, or anatomical form. The clinical performance of both sealant types was found to be acceptable.
Received: May 4, 2024
Accepted: July 16, 2024
Keywords: amorphous calcium phosphate, caries, fluoride, pit and fissure sealant
The morphology of pits and fissures can make teeth susceptible to the formation of dental caries due to the accumulation of microbial plaque, and studies indicate that occlusal caries accounts for more than two-thirds of all dental caries.1,2 To counter this susceptibility, experts recommend the application of pit and fissure sealants as an effective modality for preventing occlusal caries.1 It has been reported that sealant application can decrease caries incidence by 76%.3
The effectiveness of fissure sealants is mainly determined by their composition and retention.4 Of the 2 main types of fissure sealants, resin based and glass ionomer based, the former has been reported as the superior choice in terms of retention and wear resistance.1 The resinous base may be derived from bisphenol A glycidyl methacrylate (Bis-GMA) or urethane dimethacrylate (UDMA), to which fillers or fluoride might have been added.5 Clinpro (3M), which is a fluoride-releasing, filler-free, Bis-GMA–based sealant, has been suggested for its durability and great benefits to the teeth.6,7
Aegis (Keystone Industries) is a UDMA-based fissure sealant embedded with amorphous calcium phosphate (ACP) nanofillers.2 The bioactive ACP nanofiller, incorporated within the polymerized methacrylate matrix, can gradually release calcium and phosphate ions in response to pH changes in the oral cavity.8,9 It is claimed that composite materials with up to 71% ACP fillers can remineralize the demineralized enamel.7 In addition, ACP-containing sealants are reported to preserve enamel mineral content.10,11
Both ACP- and fluoride-containing sealants have demonstrated the ability to inhibit demineralization and remineralize initial caries lesions.10,12 Delben et al reported that ACP prevented demineralization in the deeper areas of enamel, while fluoride showed a greater effect on the outer enamel.10 According to Alsaffar et al, Aegis was not superior to Clinpro fluoride-containing sealant in preserving enamel mineral content.13
The clinical efficacy of 3 resin-based sealants (Aegis; Helioseal with or without fluoride filler, Ivoclar Vivadent) placed in primary teeth was examined by Ünal et al.2 They found no statistically significant difference between the sealants in terms of retention, marginal discoloration, marginal adaptation, or the presence of caries 2 years after sealant placement. In a study by Khatri et al, Aegis and Embrace WetBond (Pulpdent), a moisture-resistant sealant, showed no difference in terms of retention 1 year after sealant placement.14 Fernández-Barrera
et al studied 2 fissure sealants, Clinpro and BeautiSealant (Shofu Dental), and both were effective in reducing the incidence of dental caries in schoolchildren during a 6-month follow-up.15 Clinpro showed the greatest effectiveness in terms of caries prevention and sealant retention.
Previous clinical studies evaluating the success of fissure sealants have mostly focused on their retention and caries prevention.1,14-17 However, other factors, such as marginal adaptation and discoloration, can also affect the clinical success of sealants.2,18 Therefore, the present study was aimed at comparing the 24-month clinical performance of 2 different types of resinbased sealants—containing fluoride or ACP—on permanent first molars in 6- to 7-year-old children.
Methods
This split-mouth retrospective cohort study was approved by the Ethics Review Committee of the School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran (IR.SUMS. DENTAL.REC.1400.106). Written informed consent for treatment was obtained from the patients’ guardians in accordance with the principles of the Declaration of Helsinki. Permission to use the collected data for research purposes was also obtained from the guardians.
Sample selection
Clinical information was collected from the dental records of patients who received treatment from a single pediatric dentist (M.M.) in the Department of Pediatric Dentistry, School of Dentistry, Shiraz University of Medical Sciences, during 2020. Patients were included in the study if they had at least 1 permanent first molar sealed with Clinpro and 1 sealed with Aegis during 2020; were aged 6 to 7 years old at the time of sealant placement; were identified as being at high risk for caries development and needing sealants on their permanent molars by a pediatric dentist during the initial clinical examination; were treated by a specialist in the Department of Pediatric Dentistry in accordance with standard procedures; participated in a follow-up examination 12 months after the sealant placement; and agreed to participate in the study examinations at a followup visit 24 months after the start of sealant therapy.
Patients were excluded from the study if they had a history of rampant caries, parafunctional habits, heavy occlusal contacts on sealed teeth, long-term use of medications affecting salivary flow or dietary habits, or physical or mental disabilities that would interfere with the examination process.19 Patients who had not participated in a follow-up examination 12 months after sealant application were also excluded from the study.
All patients’ files were reviewed thoroughly to select permanent first molars that met the study criteria. Based on this review, a total of 72 molars in 30 children were included in the study groups, which consisted of 36 teeth treated with Clinpro sealant and 36 teeth treated with Aegis sealant. Twenty-four patients received fissure sealants on 2 teeth each, and the remaining 6 individuals received sealants on 4 teeth each.
Sealant procedures
All treatments were started with dental prophylaxis, irrespective of the sealant type. Next, each sealant was placed based
on its manufacturer’s instructions. The enamel surface was etched with 37% phosphoric acid for 20 seconds, rinsed for 10 seconds, and air dried for 10 seconds. Then the resin-based sealant was placed and cured for 20 seconds with a halogen light-curing unit (Coltolux, Coltene) with an intensity of 550 mW/cm2. Moisture control during treatment was achieved with cotton rolls.
Sealant evaluations
To ensure consistency in the evaluation process, the research team was calibrated prior to the follow-up evaluations by examining 20 children, aged 8 years, who had previously received sealant treatment. In 2022, all children participating in the study were recalled for follow-up evaluations by 2 blinded, calibrated, and experienced evaluators (A.R. and A.S.) to assess sealant retention, marginal integrity, marginal discoloration, and anatomical form. If there was disagreement between the 2 evaluators, a third pediatric dentist (M.M.) made a final decision.
Because the dental records were coded before the examination by a single researcher (N.M.), the evaluators were unaware of the type of sealant used for each tooth. Furthermore, to prevent any previous information in the file from creating bias in the examiners, a new coded file sheet was used during the subsequent follow-up session.
The clinical examination included an evaluation of sealant retention based on the criteria described by Oulis and Berdouses.17 The retention of the sealants was categorized according to the following criteria: 0 (total retention), complete retention of sealant with no visible loss of the material; 1 (partial loss), loss of sealant material in some parts of the occlusal fissures; or 2 (total loss), absence of sealant material from the occlusal fissures. A score of 0 was considered to represent a successful seal, while a score of 1 or 2 was considered a failure.
The marginal integrity, marginal discoloration, and anatomical form of the sealants were evaluated based on the criteria described by Feigal et al.18 Marginal integrity was assessed according to the following criteria: 0, no loss of sealant material can be detected by an explorer; 1, margin is detectable with an explorer; 2, crevice with visible width and depth is detected along the margin; or 3, crevice formation has exposed the central fissure.
Marginal discoloration was evaluated based on the following criteria: 0, no color change is observed at the tooth-sealant interface; 1, marginal discoloration is visible at 1 point; 2, marginal discoloration is visible in multiple areas; or 3, severe marginal discoloration with evidence of microleakage and penetration is detectable.18
The anatomical form of the sealants was rated based on the following criteria: 0, the sealant material is in harmony with the occlusal form and structure; 1, a slight change in anatomical form is detected, but all fissures are covered; 2a, partial sealant loss in 1 or 2 pits or fissures without requiring reapplication or repair is detected; 2b, partial sealant loss in 1 or 2 pits or fissures requiring reapplication or repair is detected; 3, absence of sealant material on occlusal fissures (total loss) is evident; 7, partial loss of sealant due to occlusion is detected; or 9, an air bubble (not in contact with the margin) is detected.18
Table 1. Distribution of evaluation scores of the 2 types of fissure sealants.
Score
Sealant retention (Oulis and Berdousesa)
1 12 (33.4) 10 (27.8)
2 0 (0.0)
Marginal integrity (Feigal et alb)
Marginal discoloration (Feigal et alb)
(Feigal et alb)
Abbreviation: ACP, amorphous calcium phosphate.
a Oulis and Berdouses criteria: Score 0 indicates a successful seal. All other scores are considered sealant failures.17
b Feigal et al criteria: Scores of 0 and 1 for marginal integrity and marginal discoloration as well as scores of 0, 1, 2a, 7, 9 for anatomical form indicate successful seals. All other scores are considered sealant failures.18
Scores of 0 and 1 in the marginal integrity and marginal discoloration categories and scores of 0, 1, 2a, 7, and 9 in the anatomical form evaluation were considered to represent successful seals. A finding of any other score in any single evaluation category described by Feigal et al indicated treatment failure.18 Patients with any signs of treatment failure at the sealant evaluation session were scheduled to undergo sealant reapplication.
Statistical analysis
Statistical software (SPSS, version 25.0, IBM) was used for data analysis. Data were reported as frequency and percentage. Differences between groups in the occurrences of each evaluation variable were compared using relative risk (RR) with its 95% CI as well as the chi-square or Fisher exact test. The level of significance was set at P < 0.05.
Results
The study population included 30 children (girls, 66.7%; boys 33.3%) with a total of 72 permanent first molars who had received at least 1 fluoride-containing sealant and 1
Table 2. Statistical comparison of evaluation scores of the 2 types of fissure sealants.
d RR could not be compared because the frequency in one cell was equal to zero.
ACP-containing sealant. The 2 groups comprised equal numbers of fluoride-containing and ACP-containing sealants (n = 36), and each group had 18 maxillary and 18 mandibular molars. The clinical evaluation of fissure sealants carried out after 24 months included inspection of the sealant retention, marginal integrity, marginal discoloration, and anatomical form based on previously described criteria (Table 1).17,18 Analysis of the outcomes at the 24-month follow-up revealed that fluoridecontaining Clinpro sealant demonstrated greater clinical success in retention than ACP-containing Aegis, but the difference was not statistically significant (P = 0.624) (Table 2). None of the teeth sealed with Clinpro showed total loss of the sealant, while the sealant was completely absent in 4 (11.1%) of the teeth treated with Aegis. In contrast, the presence of any sign of marginal disintegration (score ≥ 1) was slightly more frequent in the Clinpro group (22.2%) than in the Aegis group (16.7%). However, the difference between groups was not significantly different (RR = 1.33; 95% CI = 0.51-3.46; P = 0.551). Clinpro sealant demonstrated slightly greater clinical success in marginal discoloration and anatomical form scores, but neither difference was statistically significant (P = 0.493 and P = 0.151, respectively). Although no marginal discoloration was observed in the teeth treated with Clinpro, 2 (5.6%) of the teeth sealed with Aegis showed marginal discoloration at 1 point (score 1).
Discussion
The efficacy of pit and fissure sealants in preventing dental caries is determined by their physical ability to obstruct pits and fissures, which is contingent on their retention.17 Nonetheless, additional criteria have been utilized to assess
clinical efficacy.20 The criteria described by Feigal et al assess the marginal integrity, marginal discoloration, and anatomical form of fissure sealants.18 The current study evaluated the 24-month success rate of 2 different types of resin-based fissure sealants applied by a pediatric dentist.
In terms of retention, the present results revealed no obvious distinctions between Clinpro (an unfilled sealant) and Aegis (a filled sealant). This result was consistent with previous studies of sealant retention and caries development after 2 years.2,20-22 However, Reić et al reported that more of a filled resin-based sealant was retained than an unfilled sealant after 2 years on permanent teeth.23 During surface etching, resin sealants penetrate enamel microporosities.24 Despite the assumption that filled resin sealants with higher viscosity may penetrate more superficially than unfilled resin sealants, in vitro experiments have demonstrated no discernible difference between the bond strengths of filled and unfilled sealants.25
The 24-month retention rates of the fluoride-containing and ACP-containing sealants in the present study demonstrated acceptable results. In previous studies, all resin-based filled sealants (42.5% to 100.0%) and unfilled sealants (52.5% to 100.0%) showed comparable results 1 year after placement.21,23,26 Any differences between results may be attributed to the many factors that influence sealant retention. Some of these factors are fissure morphology, moisture control during placement, enamel conditioning, application techniques, specific material properties (such as viscosity and surface tension), adhesion (material penetration into the previously etched system of fissures), clinical performance, and evaluation methodologies.22
According to the evaluations in the present study, the marginal discoloration and marginal integrity of Clinpro and Aegis groups were not significantly different. Marginal discoloration refers to the development of discoloration or staining at the margins of a fissure sealant. Initial signs of marginal disintegration can be visualized as marginal discoloration.27 Marginal discoloration and loss of integrity can lead to further microleakage and the development of secondary caries. Ünal et al reported that the marginal integrity and discoloration of Aegis and a fluoride-releasing sealant (Helioseal F) were comparable, which is consistent with the present results.2
The anatomical form of a fissure sealant reflects its ability to conform to the surface of the tooth. In the present study, there was no significant difference between the groups in anatomical form. The number of teeth requiring reapplication of sealant was the same in both groups (6 of 36 teeth each). According to Simonsen et al, the choice between 2 fissure sealants can be influenced by additional factors, such as cost or ease of application.28
A split-mouth design was implemented in the present study to minimize the influence of patient-related factors such as dental habits, diet, and oral hygiene. In addition, oral hygiene education was provided to the parents of the patients, which may have affected the efficacy of the sealants. The teeth were isolated using cotton rolls. The technique was used because it has been reported that there is no discernible difference between using cotton rolls or a rubber dam to isolate the teeth during fissure sealant therapy.29 Additional clinical studies with more patients, longer follow-up periods, and the inclusion of permanent teeth with incipient caries are suggested.
Conclusion
After 24 months of follow-up, there were no statistically significant differences in clinical performance between an unfilled fluoride-containing Bis-GMA sealant and a filled ACPcontaining UDMA sealant in terms of retention rates, marginal integrity, marginal discoloration, or anatomical form on permanent first molars.
Author affiliations
Oral and Dental Disease Research Center, Department of Pediatric Dentistry, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran (Memarpour, Rafiee); Student Research Committee, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran (Sharifinejad, Mokhtari).
Correspondence
Azade Rafiee, DMD, MScD (arafiee@sums.ac.ir).
Conflicts of interest
None reported.
Funding
This research was supported by the Vice-Chancellery of Research, Shiraz University of Medical Sciences, Shiraz, Iran (grant No. 24345).
Acknowledgment
The authors thank Dr Mehrdad Vossoughi of the Center for Improvement, School of Dentistry, Shiraz University of Medical Sciences, for statistical analysis.
References
1. Alsabek L, Al-Nerabieah Z, Bshara N, Comisi JC. Retention and remineralization effect of moisture tolerant resin-based sealant and glass ionomer sealant on non-cavitated pit and fissure caries: randomized controlled clinical trial. J Dent. 2019;86:69-74. doi:10.1016/j. jdent.2019.05.027
2. Ünal M, Oznurhan F, Kapdan A, Dürer S. A comparative clinical study of three fissure sealants on primary teeth: 24-month results. J Clin Pediatr Dent. 2015;39(2):113-119. doi:10.17796/ jcpd.39.2.h247471176596757
3. Wright JT, Crall JJ, Fontana M, et al. Evidence-based clinical practice guideline for the use of pit-and-fissure sealants. Pediatr Dent. 2016;38(6):263-279.
4. Ramesh H, Ashok R, Rajan M, Balaji L, Ganesh A. Retention of pit and fissure sealants versus flowable composites in permanent teeth: a systematic review. Heliyon. 2020;6(9):e04964. doi:10.1016/j.heliyon.2020.e04964
5. Utneja S, Talwar S, Nawal RR, et al. Evaluation of remineralization potential and mechanical properties of pit and fissure sealants fortified with nano-hydroxyapatite and nanoamorphous calcium phosphate fillers: an in vitro study. J Conserv Dent. 2018;21(6):681-690. doi:10.4103/JCD.JCD_31_18
6. Ushimura S, Nakamura K, Matsuda Y, Minamikawa H, Abe S, Yawaka Y. Assessment of the inhibitory effects of fissure sealants on the demineralization of primary teeth using an automatic pH-cycling system. Dent Mater J. 2016;35(2):316-324. doi:10.4012/dmj.2015-297
7. Al Jawish A, Azzawy S, Al-Nerabieah Z. effectiveness of pit and fissure sealants containing amorphous calcium phosphate (ACP) and fluoride in the prevention of demineralization of adjacent enamel: in-vitro study. Int J Dent Oral Sci. 2021;8(2):1398-1403. doi:10.19070/2377-8075-21000311
8. Sears LM, Wu L, Morrow BR, Hollis W, Cagna DR, Hong L. Effects of NanoAg-ACP microparticles as bioactive fillers on the mechanical and remineralization properties of dental resin cement. J Prosthodont. 2022;31(8):705-713. doi:10.1111/jopr.13473
9. Bienek DR, Giuseppetti AA, Skrtic D. Amorphous calcium phosphate as bioactive filler in polymeric dental composites. In: Churchill D, Dutour Sikiric M, Čolović B, Füredi Milofer H, eds. Contemporary Topics About Phosphorus in Biology and Materials. IntechOpen; 2019:chap 8. doi:10.5772/intechopen.86640
10. Delben AC, Cannon M, Vieira AE, et al. Analysis of anticaries potential of pit and fissures sealants containing amorphous calcium phosphate using synchrotron microtomography. Oper Dent. 2015;40(2):218-223. doi:10.2341/13-325-L
11. Zawaideh FI, Owais AI, Kawaja W. Ability of pit and fissure sealant-containing amorphous calcium phosphate to inhibit enamel demineralization. Int J Clin Pediatr Dent. 2016;9(1):1014. doi:10.5005/jp-journals-10005-1325
12. Silva KG, Pedrini D, Delbem AC, Ferreira L, Cannon M. In situ evaluation of the remineralizing capacity of pit and fissure sealants containing amorphous calcium phosphate and/or fluoride. Acta Odontol Scand. 2010;68(1):11-18. doi:10.3109/00016350903260264
13. Alsaffar A, Tantbirojn D, Versluis A, Beiraghi S. Protective effect of pit and fissure sealants on demineralization of adjacent enamel. Pediatr Dent. 2011;33(7):491-495.
14. Khatri SG, Madan KA, Srinivasan SR, Acharya S. Retention of moisture-tolerant fluoridereleasing sealant and amorphous calcium phosphate-containing sealant in 6-9-year-old children: a randomized controlled trial. J Indian Soc Pedod Prev Dent. 2019;37(1):92-98. doi:10.4103/JISPPD.JISPPD_173_18
15. Fernández-Barrera MÁ, de Jesús Saucedo-Molina T, Scougall-Vilchis RJ, de Lourdes MárquezCorona M, Medina-Solís CE, Maupomé G. Comparison of two types of pit and fissure sealants in reducing the incidence of dental caries using a split-mouth design. Acta Stomatol Croat 2021;55(2):137-146. doi:10.15644/asc55/2/3
16. Althomali YM, Musa S, Manan NM, Nor NAM. Retention evaluation of fissure sealants applied using self-etch and conventional acid-etch techniques: a randomized control trial among schoolchildren. Pediatr Dent. 2022;44(4):249-254.
17. Oulis CJ, Berdouses ED. Fissure sealant retention and caries development after resealing on first permanent molars of children with low, moderate and high caries risk. Eur Arch Paediatr Dent. 2009;10(4):211-217. doi:10.1007/BF03262684
18. Feigal RJ, Musherure P, Gillespie B, Levy-Polack M, Quelhas I, Hebling J. Improved sealant retention with bonding agents: a clinical study of two-bottle and single-bottle systems. J Dent Res. 2000;79(11):1850-1856. doi:10.1177/00220345000790110601
19. Deshpande A, Sudani U, Bargale S, KS Poonacha, Kadam M, Joshi N. Six months clinical performance of self etch-self adhesive flowable composite and conventional pit-and-fissure sealants in 7 to 10 year old children. J Adv Med Dent Scie Res. 2016;4(1):38-43.
20. Ahovuo-Saloranta A, Forss H, Walsh T, Nordblad A, Mäkelä M, Worthington HV. Pit and fissure sealants for preventing dental decay in permanent teeth. Cochrane Database Syst Rev 2017;7(7):CD001830. doi:10.1002/14651858.CD001830.pub5
21. Bagheri E, Sarraf Shirazi A, Shekofteh K. comparison of the success rate of filled and unfilled resin-based fissure sealants: a systematic review and meta-analysis. Front Dent. 2022;19:10. doi:10.18502/fid.v19i10.8855
22. Reddy VR, Chowdhary N, Mukunda KS, Kiran NK, Kavyarani BS, Pradeep MC. Retention of resin-based filled and unfilled pit and fissure sealants: a comparative clinical study. Contemp Clin Dent. 2015;6(Suppl 1):S18-S23. doi:10.4103/0976-237X.152932
23. Reić T, Galić T, Negovetić Vranić D. Retention and caries-preventive effect of four different sealant materials: a 2-year prospective split-mouth study. Int J Paediatr Dent. 2022;32(4): 449-457. doi:10.1111/ipd.12924
24. Feigal RJ, Donly KJ. The use of pit and fissure sealants. Pediatr Dent. 2006;28(2):143-198.
25. Shingare PR, Chaugule V, Pankey N, Kakade P. Comparative evaluation of penetrative and adaptive properties of unfilled and filled resin-based sealants when placed using conventional acid etching, lasing, and fissurotomy bur technique of enamel preparation: an in vitro scanning electron microscope study. Contemp Clin Dent. 2022;13(4):349-355. doi:10.4103/ ccd.ccd_227_21
26. Baheti AS, Bhayya DP, Gupta S, Kumar P, Shyagali TR. Assessment of clinical success of three sealants: Embrace-Wetbond, Clinpro, and Helioseal-F in permanent molars: an in vivo study. J South Asian Assoc Pediatr Dent. 2020;3(1):7-13. doi:10.5005/jp-journals-10077-3035
27. Ninawe N, Ullal NA, Khandelwal V. A 1-year clinical evaluation of fissure sealants on permanent first molars. Contemp Clin Dent. 2012;3(1):54-59. doi:10.4103/0976-237X. 94547
28. Simonsen RJ, Neal RC. A review of the clinical application and performance of pit and fissure sealants. Aust Dent J. 2011;56(Suppl 1):45-58. doi:10.1111/j.1834-7819.2010.01295.x
29. Olegário IC, Moro BLP, Tedesco TK, et al. Use of rubber dam versus cotton roll isolation on composite resin restorations’ survival in primary molars: 2-year results from a non-inferiority clinical trial. BMC Oral Health. 2022;22(1):440. doi:10.1186/s12903-022-02449-y
Comparison of the antimicrobial effects of 0.2% curcumin mouthwash and chlorhexidine mouthwash on Streptococcus mutans in orthodontic patients: a randomized clinical trial
Tahura Etezadi, DDS, MS ¢ Ali Semnani ¢ Hodis Ehsani, DDS, MS ¢ Hamid Reza Goli, PhD
Amirreza Samaei, DDS ¢ Farhad Sobouti, DDS, MS
The use of mouthwash is a practical approach to decreasing bacteria during orthodontic treatment. This study aimed to investigate the antibacterial effect of 0.2% curcumin mouthwash on Streptococcus mutans in individuals undergoing fixed orthodontic treatment. For this double-blinded clinical study, 22 orthodontic patients aged 15 years or older with no systemic or periodontal diseases were selected and randomly divided into 2 groups of 11 individuals. One group received 0.2% curcumin mouthwash (intervention), while the other group received 0.2% chlorhexidine mouthwash (control) to use twice daily. Orthodontic elastics were collected from the patients’ mouth immediately before the first use of the mouthwash, immediately after the first use, and after 20 days of mouthwash use. The elastics were stored in normal saline, and the samples were transferred to a microbiology laboratory for serial dilution, plating, and incubation. After 48 hours, the number of colony-forming units (CFUs) of S mutans were counted and compared. The Friedman and Wilcoxon tests were used for statistical analysis of intragroup data, while the Mann-Whitney U test was used for intergroup comparisons. A difference of P < 0.05 was considered statistically significant. Both the curcumin and chlorhexidine groups demonstrated a statistically significant decrease in CFUs of S mutans immediately after the initial use as well as after 20 days’ use (P < 0.05). After the first use, there was no statistically significant difference between the groups in the reduction of CFUs (P = 0.071). However, after 20 consecutive days of mouthwash use, the curcumin group had a significantly greater decrease in CFUs of S mutans than the chlorhexidine group (P < 0.001). Both chlorhexidine and curcumin mouthwashes significantly reduced the number of S mutans colonies when used regularly. The results of the present study suggest that curcumin herbal mouthwash is a superior choice to chlorhexidine for orthodontic patients due to its long-term antibacterial properties.
Tooth decay is a chronic disease that results from the interaction of the host, environment, and bacteria, and bacterial plaque is a critical factor in the progression of this condition. Streptococcus mutans is a gram-positive bacterium that is mainly responsible for tooth caries. It produces acid from sugar metabolism, which erodes tooth structure over time.1,2
Any foreign body in the oral cavity, including unfinished dental restorations, dental prostheses, and orthodontic appliances, can lead to plaque accumulation.3-5 Elastics are components of orthodontic appliances that securely hold fixed orthodontic wires between brackets.6-10 These elastics are typically used for extended periods during orthodontic treatment. Conventional oral hygiene methods, such as toothbrushes and dental floss, may not be adequate for plaque elimination.11-13 Therefore, it is crucial to consider adjunctive treatments that can improve oral health.8
Multiple antimicrobial products are available to inhibit the growth of pathogenic oral microorganisms, and mouthwashes are considered among the most important of these measures.14-16 Chlorhexidine is a popular mouthwash and is widely regarded as the gold standard for comparison with other antiplaque agents.17 Several studies have demonstrated the effectiveness of chlorhexidine in controlling bacterial colonization, especially in preventing the formation of S mutans plaque.16 Chlorhexidine mouthwash may have some undesirable effects, including oral complications such as dryness, burning sensations, taste alteration, dental staining, and gingival desquamation as well as systemic adverse effects.18 The detrimental effects of chlorhexidine have led to increased use of herbal mouthwashes.19-21 In recent years, the herbal compound curcumin has become a subject of increasing interest. Curcumin is a bright orange crystalline substance that is obtained from the rhizome of turmeric (Curcuma longa) and other Curcuma species.22 Although curcumin mouthwash can produce temporary tooth staining, it can be easily removed with brushing.23,24 Several studies have suggested that curcumin is safe for human consumption, even at high doses. However, its therapeutic use is limited due to its low bioavailability. Many studies have investigated the local anti-inflammatory effects of curcumin in the form of gel or mouthwash for the treatment of gingivitis. Although the majority of these studies have been conducted on animals, a few have been performed on humans.20-22 Among these studies, only a limited number have compared the effects of 0.2% curcumin mouthwash with those
of chlorhexidine mouthwash on S mutans. The objective of the present study was to compare the effects of 0.2% curcumin and chlorhexidine mouthwashes on S mutans found on the elastics of orthodontic patients.
Methods
This double-blinded randomized clinical trial involved 22 patients referred to the Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran. The trial was approved by the university’s ethics committee (IR.MAZUMS.. REC.1401.15077). Patients provided written informed consent for the treatment protocol and use of their data for research and publication.
Sample and groups
All participants in the study were aged 15 years or older, had orthodontic brackets bonded for at least 2 months, and had no periodontitis or systemic diseases. Patients who exhibited poor compliance with treatment, had allergies to the components of the mouthwashes, were using corticosteroids, or had used any antibiotic or mouthwash for 10 consecutive days within the last 30 days were excluded from the study.
The study population of 22 participants was randomly divided into 2 groups of 11 patients each using Random Allocation Software (version 2.0, Informer Technologies). The intervention group received a mouthwash containing 0.2% curcumin, while the control group received 0.2% chlorhexidine mouthwash.25 To ensure blinding of both the observers and patients, the mouthwashes were placed in bottles of identical color and shape and delivered to the patients in a sealed condition, to be opened at home.
Rinsing protocol
Patients were educated on the horizontal scrub technique for oral hygiene and instructed to brush at least twice daily for 2 to 4 minutes per session. All patients were provided with the same toothbrush and toothpaste. They were instructed to rinse their mouth with 5 mL of the assigned mouthwash for 30 seconds twice daily (morning and night) for a period of 20 days. Patients were advised not to eat or drink for 1 hour after rinsing.25
To prepare the curcumin extract, 264 g of standard curcumin powder (C1386, Sigma-Aldrich) was dissolved in 5280 mL of sterile pure methanol. The mixture was stored in methanol solvent and underwent periodic magnetic stirring for 48 hours. Afterward, the solution was filtered using No. 4 Whatman filter paper (Cytiva), resulting in a 0.2% alcohol-water extract that was transferred into sterile 60-mL vials under hygienic conditions.26 The control group received a commercially available 0.2% chlorhexidine mouthwash (Irannajo).
Bacterial sampling
The patients were sampled at 3 points during the study. The first sampling (T1) was conducted just before patients rinsed with mouthwash for the first time. The elastics on the maxillary left canine and premolars were removed and placed in normal saline solution. The second sampling (T2) was performed at the same session, immediately after the patients rinsed with the mouthwash for 30 seconds and expectorated. This time,
the elastics on the maxillary right canine and premolars were immediately removed from the mouth and placed in normal saline solution. The third round of sampling (T3) was carried out 20 days after the first and second rounds. During this 20-day period, patients followed the instructions and continued to use their assigned mouthwash at home, including prior to the final sampling. At T3, the elastics on the maxillary right canine and premolars were taken off and placed in normal saline solution. All evaluations and elastic removal were performed by an orthodontist.
The samples were transferred to a microbiology laboratory in an ice-filled container within 4 hours of collection. The colonyforming units (CFUs) were counted to determine the effect of the mouthwashes on S mutans. This method involved serial dilution of the original samples and subsequent cultivation on mitis salivarius agar (Sigma-Aldrich) containing 20% sucrose (SigmaAldrich) and 200 U/L bacitracin (Sigma-Aldrich). The plates were incubated for 48 hours at 37°C and 10% carbon dioxide, and then the numbers of CFUs in the 2 groups were compared.
Statistical analysis
The data were analyzed using SPSS statistical software (version 23.0.0, IBM). The categorical variables of sex and age were compared with the Fisher exact test and independent t test, respectively, to determine differences between the groups. The Shapiro-Wilk test was conducted to check for normality of the data. The Friedman test was used for intragroup analysis, followed by the nonparametric Wilcoxon test. The MannWhitney U test was used for intergroup analysis. The significance threshold for all tests was set at P < 0.05.
Results
The sample included 11 female and 11 male patients. The mean (SD) ages of patients in the curcumin and chlorhexidine groups were 26.09 (8.56) and 21.82 (4.00) years, respectively. The groups had statistically similar sex and age distributions (P = 1.000 and P = 0.149, respectively), indicating their comparability.
Intragroup comparisons revealed that both the curcumin and chlorhexidine mouthwashes significantly reduced the CFUs of S mutans (Table 1). This decrease was observed after the first application of the mouthwashes and after use for 20 consecutive days (P < 0.05; Friedman test).
Intergroup comparisons showed no statistically significant difference between the curcumin and chlorhexidine groups in the reduction of S mutans colonies following the first application (Table 2). However, after 20 consecutive days of mouthwash use, the curcumin group demonstrated a significantly greater reduction in CFUs than the chlorhexidine group ( P < 0.0 01 ; Mann-Whitney U test).
Discussion
The presence of fixed orthodontic appliances is associated with elevated levels of plaque accumulation, so it is essential to have patients incorporate chemical plaque control strategies such as mouthrinses alongside mechanical methods of oral hygiene. Chlorhexidine is the most commonly used mouthwash and is regarded as the gold standard among antiplaque agents. The potential adverse effects of chlorhexidine have led to an
Table
in the curcumin and chlorhexidine mouthwash groups (n = 11 per group).
Group
Curcumin
Chlorhexidine
3818181.82 (2315952.58)
1263636.36 (1315501.98)
2827272.73 (2008029.34)
168454.55 (246836.53)
454545.45 (307777.96) 39909.09 (33437.87)
P < 0.001a T1 > T2 > T3 (P < 0.05b)
Abbreviations: CFUs, colony-forming units; T1, immediately prior to rinsing with mouthwash; T2, immediately after rinsing with mouthwash for 30 seconds; T3, 20 days after T1 and T2.
Table 2. Intergroup comparisons of Streptococcus mutans in the curcumin and chlorhexidine groups (n = 11 per group). Comparison
(452668.85)
(2187460.36)
(1858444.88)
Abbreviations: CFUs, colony-forming units; T1, immediately prior to rinsing with mouthwash; T2, immediately after rinsing with mouthwash for 30 seconds; T3, 20 days after T1 and T2.
a No statistically significant difference (Mann-Whitney U test).
bStatistically significant difference (Mann-Whitney U test).
increase in the use of herbal mouthrinses such as curcumin, which in recent years has become popular for its antimicrobial properties.27 Therefore, the present study aimed to investigate the effect of curcumin mouthwash on the number of S mutans colonies accumulating on patients’ orthodontic elastics.
The results of this study demonstrated that both curcumin and chlorhexidine mouthwashes significantly reduced the number of S mutans colonies after the initial use as well as after 20 days’ use. These results were in line with the findings of a systematic review conducted by Ehteshami et al, who evaluated the effect of curcumin in reducing the number of S mutans and its impact on reducing dental caries.28 They reported that curcumin resulted in statistically significant reductions in both the growth of S mutans and the incidence of dental caries. Fakheran et al conducted a systematic review and found that curcumin inhibits periodontal pathogens and stimulates the host response against them.29 Chatterjee et al studied the effect of 0.1% curcumin, 0.2% chlorhexidine, and placebo mouthwashes on gingivitis.8 Participants in all 3 groups were instructed to use their assigned mouthwash twice daily, and clinical parameters such as the plaque index, gingival index, and sulcus bleeding index were measured and recorded on days 0, 7, 14, and 28. The groups using curcumin and chlorhexidine mouthwashes had statistically significant improvements in all measured parameters
compared with the placebo group. Arunachalam et al found that rinsing with curcumin mouthwash significantly reduced signs of gingivitis compared with use of chlorhexidine mouthwash.17 According to a meta-analysis by Al-Maweri et al, curcumin, like chlorhexidine, has antiplaque, anti-inflammatory, and antibacterial effects.30 However, no statistically significant difference was observed between the effects of these 2 substances. Shirban et al concluded that curcumin mouthwash is a suitable herbal alternative to chlorhexidine mouthwash because it effectively reduces microbial colonization, plaque index, gingival index, and gingival bleeding index.31
A direct comparison between the results of the present study and those of previous investigations is impossible because previous studies did not specifically investigate the impact of mouthwashes on S mutans but instead relied on clinical measurements. However, because S mutans is known to play a significant role in the development of gingivitis and periodontitis, it is logical to assume that the findings of the current study are consistent with the results of the previous studies.32,33
The present study found no statistically significant difference between the curcumin and chlorhexidine groups in the reductions of S mutans CFUs after the first use. However, after using the mouthwash for 20 days, the curcumin group exhibited a significantly greater reduction of CFUs than the chlorhexidine
1. Intragroup comparisons of Streptococcus mutans counts
group. A systematic review compared the effectiveness of curcumin-containing products and chlorhexidine as adjunctive treatments for chronic periodontitis.34 In long-term evaluations (more than 3 weeks), local delivery of curcumin gel resulted in significantly greater reductions of probing depth than chlorhexidine but did not have a statistically significant effect on reducing the plaque index. However, short-term evaluations showed no statistically significant difference between the 2 substances.34 In another systematic review, Zhang et al compared the effectiveness of curcumin and chlorhexidine as adjuncts to scaling and root planing for the treatment of periodontitis.35 Their findings revealed no statistically significant difference between the 2 substances in terms of their ability to reduce probing depths, gingival index, or plaque index.
Suhag et al compared the efficacy of 1% curcumin, 0.2% chlorhexidine, and 0.9% normal saline for reducing periodontal probing depth, bleeding on probing, and gingival redness.36 Irrigation was performed immediately following scaling and root planing (day 0), daily for 5 consecutive days posttreatment, and on days 15 and 21. Clinical parameters were recorded on irrigation days and day 42. On day 5, the reductions in bleeding and redness were significantly greater in the curcumin group than in the chlorhexidine and normal saline groups. The mean reductions in probing depths were significantly greater in the curcumin group than the other groups at all recall visits.
Singhla et al compared the effectiveness of mouthwashes in reducing chronic periodontitis symptoms when used as an adjunct to scaling and root planing, investigating products containing 0.1% curcumin; meswak (or miswak), derived from Salvadora persica; and 0.2% chlorhexidine.37 They observed that all 3 types of mouthwash significantly improved clinical parameters (plaque index, gingival index, probing depth, and relative attachment level) and reduced microbial CFUs within 20 days. Curcumin resulted in a significantly greater reduction in the mean gingival index than the other 2 substances. However, chlorhexidine reduced the bacterial load more effectively than curcumin or meswak over the period of 21 days.
Studies by Siddharth et al and Anitha et al compared the efficacy of curcumin and chlorhexidine subgingival gels over short- and long-term periods.38,39 In both studies, curcumin gel was found to be significantly more effective than chlorhexidine gel in improving all clinical and microbiologic parameters. It can be challenging to compare these studies precisely to the present study because of variations in the concentrations and application methods of the substances. However, considering the overall performance of curcumin gel compared with chlorhexidine gel, the results of the present study are consistent with the findings of these previous studies.
The present study was able to achieve its objectives but has some limitations. First, the sample size was small. Second, some confounding variables, such as the participants’ dietary habits and normal oral microbial flora, could not be controlled. Fixed orthodontic treatments can alter oral microbial flora, leading to a rise in bacteria such as Aggregatibacter actinomycetemcomitans, Tannerella forsythia, and Streptococcus sobrinus in addition to S mutans. 40,41 While the present study focused on S mutans, additional studies are suggested to explore the potential effects of curcumin herbal mouthwash on other microbial species.
Conclusion
Short-term use of chlorhexidine or curcumin mouthwashes offers comparable effects in reducing the number of S mutans colonies. However, the results of the present study are consistent with previous research indicating that curcumin herbal mouthwash has superior antibacterial properties over the long term. Therefore, curcumin mouthwash represents a better choice, particularly for patients undergoing prolonged orthodontic treatment, who face potential adverse effects from extended use of chlorhexidine.
Author affiliations
Department of Orthodontics, Dental Research Center, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran (Etezadi, Sobouti); Students’ Research Committee, Dental Research Center, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran (Semnani, Samaei); Department of Periodontics, Dental Research Center, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran (Ehsani); Department of Medical Microbiology and Virology, Faculty of Medicine, Mazandaran University of Medical Sciences, Sari, Iran (Goli).
Correspondence
Hodis Ehsani, DDS, MS (Hodis.delyar@gmail.com).
Conflicts of interest
None reported.
References
1. Littlewood SJ, Mitchell L. An Introduction to Orthodontics. 5th ed. Oxford University Press; 2019. 2. Vijayakumar A, Sarveswari HB, Vasudevan S, Shanmugam K, Solomon AP, Neelakantan P. Baicalein inhibits Streptococcus mutans biofilms and dental caries-related virulence phenotypes. Antibiotics (Basel). 2021;10(2):215. doi:10.3390/antibiotics10020215
3. Klukowska M, Bader A, Erbe C, et al. Plaque levels of patients with fixed orthodontic appliances measured by digital plaque image analysis. Am J Orthod Dentofacial Orthop. 2011;139(5):e463-e470. doi:10.1016/j.ajodo.2010.05.019
4. Kurt A, Cilingir A, Bilmenoglu C, Topcuoglu N, Kulekci G. Effect of different polishing techniques for composite resin materials on surface properties and bacterial biofilm formation. J Dent. 2019;90:103199. doi:10.1016/j.jdent.2019.103199
5. Al-Anezi SA, Harradine NW. Quantifying plaque during orthodontic treatment: a systematic review. Angle Orthod. 2012;82(4):748-753. doi:10.2319/050111-312.1
6. Hewlings SJ, Kalman DS. Curcumin: a review of its effects on human health. Foods. 2017;6(10):92. doi:10.3390/foods6100092
7. Sharifi-Rad J, Rayess YE, Rizk AA, et al. Turmeric and its major compound curcumin on health: bioactive effects and safety profiles for food, pharmaceutical, biotechnological and medicinal applications. Front Pharmacol. 2020;11:01021. doi:10.3389/fphar.2020.01021
8. Chatterjee A, Debnath K, Rao NKH. A comparative evaluation of the efficacy of curcumin and chlorhexidine mouthrinses on clinical inflammatory parameters of gingivitis: a doubleblinded randomized controlled clinical study. J Indian Soc Periodontol. 2017;21(2):132-137. doi:10.4103/jisp.jisp_136_17
9. Bomdyal RS, Shah MU, Doshi YS, Shah VA, Khirade SP. Antibacterial activity of curcumin (turmeric) against periopathogens—an in vitro evaluation. J Adv Clin Res Insights. 2017;4(6):175-180. doi:10.15713/ins.jcri.188
10. Lim KS, Kam P. Chlorhexidine—pharmacology and clinical applications. Anaesth Intensive Care. 2008;36(4):502-512. doi:10.1177/0310057X0803600404
11. Dills SS, Olshan AM, Goldner S, Brogdon C. Comparison of the antimicrobial capability of an abrasive paste and chemical-soak denture cleaners. J Prosthet Dent. 1988;60(4):467-470. doi:10.1016/0022-3913(88)90250-8
12. Ousehal L, Lazrak L, Es-Said R, Hamdoune H, Elquars F, Khadija A. Evaluation of dental plaque control in patients wearing fixed orthodontic appliances: a clinical study. Int Orthod. 2011;9(1):140-155. doi:10.1016/j.ortho.2010.12.013
13. Mota SM, Enoki C, Ito IY, Elias AM, Matsumoto MA. Streptococcus mutans counts in plaque adjacent to orthodontic brackets bonded with resin-modified glass ionomer cement or resinbased composite. Braz Oral Res. 2008;22(1):55-60. doi:10.1590/s180683242008000100010
14. Davies GE, Francis J, Martin AR, Rose FL, Swain G. 1:6-Di-4’-chlorophenyldiguanidohexane (“hibitane”): laboratory investigation of a new antibacterial agent of high potency. Br J Pharmacol. 1954;9(2):192-196. doi:10.1111/j.1476-5381.1954.tb00840.x
15. Denton GW. Chlorhexidine. In: Block SS, ed. Disinfection, Sterilization, and Prevention. 5th ed. Lippincott, Williams and Wilkins; 2000:321-336.
16. Bernstein D, Schiff G, Echler G, Prince A, Feller M, Briner W. In vitro virucidal effectiveness of a 0.12%-chlorhexidine gluconate mouthrinse. J Dent Res. 1990;69(3):874-876. doi:10.1177/ 00220345900690030901
17. Arunachalam LT, Sudhakar U, Vasanth J, Khumukchum S, Selvam VV. Comparison of antiplaque and anti-gingivitis effect of curcumin and chlorhexidine mouth rinse in the treatment of gingivitis: a clinical and biochemical study. J Indian Soc Periodontol. 2017;21(6):478-483. doi:10.4103/jisp.jisp_116_17
18. Ferretti GA, Raybould TP, Brown AT, et al. Chlorhexidine prophylaxis for chemotherapy- and radiotherapy-induced stomatitis: a randomized double-blind trial. Oral Surg Oral Med Oral Pathol. 1990;69(3):331-338. doi:10.1016/0030-4220(90)90295-4
19. Aghili H, Nadoushan AA, Herandi V. Antimicrobial effect of Zataria multiflora extract in comparison with chlorhexidine mouthwash on experimentally contaminated orthodontic elastomeric ligatures. J Dent (Tehran). 2015;12(1):1-10.
20. Sari E, Birinci I. Microbiological evaluation of 0.2% chlorhexidine gluconate mouth rinse in orthodontic patients. Angle Orthod. 2007;77(5):881-884. doi:10.2319/080506-320.1
21. Simões Moraes R, Modesto A, Regina Netto dos Santos K, Drake D. The effect of 1% chlorhexidine varnish and 40% xylitol solution on Streptococcus mutans and plaque accumulation in children. Pediatr Dent. 2011;33(7):484-490.
22. Lee SM, Yoo SY, Kim HS, et al. Prevalence of putative periodontopathogens in subgingival dental plaques from gingivitis lesions in Korean orthodontic patients. J Microbiol. 2005;43(3):260-265.
23. Sugito H, Eguchi T, Tanaka R, Haruyama A, Muramatsu T. The effects of dietary pH changes on tooth staining of the enamel surface. Oper Dent Endodontol Periodontol. 2023;3(1):8085. doi:10.11471/odep.2023-009
24. Maciel CRO, Amorim AA, Oliveira RFL, Vivanco RG, Pires-de-Souza FCP. Whitening efficacy of popular natural products on dental enamel. Braz Dent J. 2022;33(3):55-66. doi:10.1590/0103-6440202204863
25. Salehi P, Momeni Danaie S. Comparison of the antibacterial effects of persica mouthwash with chlorhexidine on Streptococcus mutans in orthodontic patients. DARU J Pharm Sci. 2006;14(4):178-182.
26. Sheinizadeh-Emadi S, Ehsani P, Dahanzadeh S, Haghighizadeh M. Comparison evaluation of curcumin (Curcuma longa extract) with the application of expressed breast milk in the treatment of nipple cracks in lactating primiparous women: a randomized clinical trial. Article in Persian. J Clin Nurs Midwifery. 2015;4(2):11-19.
27. Ambili R, Ramadas K, Nair LM, et al. Efficacy of a herbal mouthwash for management of periodontitis and radiation-induced mucositis—a consolidated report of two randomized controlled clinical trials. J Ayurveda Integr Med. 2023;14(6):100791. doi:10.1016/j. jaim.2023.100791
28. Ehteshami A, Shirban F, Gharibpour F, Bagherniya M, Sathyapalan T, Sahebkar A. Does curcumin have an anticaries effect? A systematic review of in vitro studies. Adv Exp Med Biol. 2021;1291:213-227. doi:10.1007/978-3-030-56153-6_12
29. Fakheran O, Khademi A, Bagherniya M, Dehghannejad M, Sathyapalan T, Sahebkar A. Antibacterial activity of curcumin against periodontal pathogens: a systematic review. Adv Exp Med Biol. 2021;1291:239-249. doi:10.1007/978-3-030-56153-6_14
30. Al-Maweri SA, Alhajj MN, Deshisha EA, et al. Curcumin mouthwashes versus chlorhexidine in controlling plaque and gingivitis: a systematic review and meta-analysis. Int J Dent Hyg. 2022;20(1):53-61. doi:10.1111/idh.12518
31. Shirban F, Gharibpour F, Ehteshami A, Bagherniya M, Sathyapalan T, Sahebkar A. The effects of curcumin in the treatment of gingivitis: a systematic review of clinical trials. Adv Exp Med Biol. 2021;1291:179-211. doi:10.1007/978-3-030-56153-6_11
32. Contardo M, Díaz N, Lobos O, Padilla C, Giacaman R. Oral colonization by Streptococcus mutans and its association with the severity of periodontal disease in adults. Rev Clin Periodoncia Implantol Rehabil Oral. 2011;4(1):9-12. doi:10.1016/S0718-5391(11)70058-1
33. Dani S, Prabhu A, Chaitra K, Desai N, Patil SR, Rajeev R. Assessment of Streptococcus mutans in healthy versus gingivitis and chronic periodontitis: a clinico-microbiological study. Contemp Clin Dent. 2016;7(4):529-534. doi:10.4103/0976-237X.194114
34. Terby S, Shereef M, Ramanarayanan V, Balakrishnan B. The effect of curcumin as an adjunct in the treatment of chronic periodontitis: a systematic review and meta-analysis. Saudi Dent J. 2021;33(7):375-385. doi:10.1016/j.sdentj.2021.07.008
35. Zhang Y, Huang L, Mazurel D, Zheng H, Yang J, Deng D. Clinical efficacy of curcumin versus chlorhexidine as an adjunct to scaling and root planing for the treatment of periodontitis: a systematic review and meta-analysis. Phytother Res. 2021;35(11):5980-5991. doi:10.1002/ ptr.7208
36. Suhag A, Dixit J, Dhan P. Role of curcumin as a subgingival irrigant: a pilot study. Perio. 2007;4(2):115-121.
37. Singhla R, Tevatia S, Chaudhry S, Vaish S, Dodwad V. Comparative evaluation of the efficacy of locally delivered 0.1% curcumin irrigation, meswak irrigation and 0.2% CHX irrigation in management chronic periodontitis patients. J Dent Specialities. 2017;5(1):53-57.
38. Siddharth M, Singh P, Gupta R, Sinha A, Shree S, Sharma K. A comparative evaluation of subgingivally delivered 2% curcumin and 0.2% chlorhexidine gel adjunctive to scaling and root planing in chronic periodontitis. J Contemp Dent Pract. 2020;21(5):494-499.
39. Anitha V, Rajesh P, Shanmugam M, Priya BM, Prabhu S, Shivakumar V. Comparative evaluation of natural curcumin and synthetic chlorhexidine in the management of chronic periodontitis as a local drug delivery: a clinical and microbiological study. Indian J Dent Res. 2015;26(1):53-56. doi:10.4103/0970-9290.156806
40. Papageorgiou SN, Xavier GM, Cobourne MT, Eliades T. Effect of orthodontic treatment on the subgingival microbiota: a systematic review and meta-analysis. Orthod Craniofac Res. 2018;21(4):175-185. doi:10.1111/ocr.12237
41. Tang X, Sensat M, Stoltenberg JL. The antimicrobial effect of chlorhexidine varnish on mutans streptococci in patients with fixed orthodontic appliances: a systematic review of clinical efficacy. Int J Dent Hyg. 2016;14(1):53-61. doi:10.1111/idh.12163
Galal Omami, BDS, MSc, MDentSc, FRCD(C)
Circular radiolucency
A 55-year-old man presented with a well-circumscribed unilocular radiolucent lesion in the mandibular left first molar extraction site, which was incidentally discovered on routine radiographic
Figure. Panoramic image shows a thinly corticated unilocular radiolucency in the extraction site of the mandibular left first molar. Note the inferior displacement of the mandibular canal.
Generalized rarefactions
An 80-year-old White woman presented to the dental clinic seeking treatment for her carious teeth. The patient’s past medical history was remarkable for hypertension,
Figure. Panoramic image shows generalized loss of the normal cortical thickness and trabecular bone density.
imaging (Figure). The patient denied having any discomfort. Clinical examination revealed a slight nontender swelling of the affected area. The overlying mucosa was normal.
Which of the following is the most appropriate diagnosis?
A. odontogenic keratocyst
B. residual radicular cyst
C. simple bone cyst
D. unicystic ameloblastoma
Diagnosis is on page 80.
rheumatoid arthritis, and peptic ulcer. A panoramic radiograph showed generalized loss of the normal thickness and density of the jaws (Figure).
Which of the following is the most appropriate diagnosis?
A. hyperparathyroidism
B. multiple myeloma
C. osteomalacia
D. osteoporosis
Diagnosis is on page 80.
Author affiliation Department of Oral Health Practice, University of Kentucky College of Dentistry, Lexington.
GENERAL DENTISTRY SELF-INSTRUCTION ANSWERS
Exercise No. GD527 May/June 2024, p. 33
1. B 2. C
3. C
4. D
5. D 6. B 7. A 8. B 9. C 10. A 11. B 12. C 13. D 14. A 15. B
Exercise No. GD528 May/June 2024, p. 41
1. B
2. D
3. A
4. B
5. C 6. A 7. C 8. D 9. C 10. B 11. D 12. C 13. B 14. A 15. B
Exercise No. GD529 May/June 2024, p. 49
1. D
2. D
3. B 4. C 5. C 6. A 7. C 8. A 9. D 10. B 11. A 12. C 13.
Look for these articles and more in the July/August 2025 issue of General Dentistry:
• Tooth wear rehabilitation using a digital workflow and tabletop restorations
• Trueness of CAD/CAM custom milled post and cores
• Effects of abutment screw channel angle on removal torque of ball-end Torx screws
In the May issue of AGD Impact
• Navigating Implant Success with Photogrammetry
• What Makes a New Graduate Employable?
In the June issue of AGD Impact
• Regenerative Dentistry: Current Research and Upcoming Advances
• Competing Dental and Dental Hygienist Compacts: What Dental Professionals Need to Know
HAVE YOU MOVED?
If you have recently moved, or plan to in the near future, please make sure to update your AGD profile.
Log into the AGD website today! We want to make sure you receive AGD publications and other important information from us! View or update your profile, check the status of your membership dues, manage your email subscriptions and change your password.
Please contact the AGD Membership Services Center with any questions at 888.243.3368 (toll-free) or 312.440.4300. Our member representatives are available to assist you Monday through Friday from 7:30 a.m. to 5:30 p.m. CST. UPDATE YOUR PROFILE agd.org/my-agd
Circular radiolucency
Diagnosis
B. residual radicular cyst
A residual radicular cyst is a radicular (periapical) cyst that remains in the jaw after extraction of the associated tooth. Most lesions are asymptomatic and discovered on routine radiographs. These cysts are usually filled with clear, strawcolored fluid that contains cholesterol products. Pain may occur when the cyst becomes secondarily infected.
Radiographically, the residual radicular cyst appears as a well-defined and -corticated, round-to-ovoid unilocular radiolucency that is centered in the former apical region of a previous extraction site. If the cyst becomes secondarily infected,
Generalized rarefactions
Diagnosis
D. osteoporosis
Osteoporosis is a skeletal disorder characterized by low mineral bone density and structural changes of bone, resulting in increased bone fragility. Although osteoporosis is an aging phenomenon, it also may occur secondary to an underlying condition, such as nutritional deficiency, lack of physical activity, hormonal changes, or corticosteroid therapy. White postmenopausal women are particularly at risk. Patients may develop pathologic fracture with resulting pain and deformity. The most common fracture sites are the proximal femur, distal radius, and spine.
Radiographically, osteoporotic changes of the jaws are more pronounced in the mandible and include generalized thinning of the cortical boundaries and reduction of
it may lose its peripheral cortex. Dystrophic calcification may develop within long-standing cysts. The lesion may cause displacement or resorption of the adjacent teeth or expansion of the outer cortical plates.
A residual radicular cyst is treated by surgical enucleation, and the lesion should not recur.
Reference
White SC, Pharoah MJ, eds. Oral Radiology: Principles and Interpretation. 7th ed. Mosby; 2014:336-338.
the trabecular volume. The marrow spaces may become enlarged, and the residual trabeculae appear fewer, coarser, and hypodense. The teeth may stand out in contrast to the generally radiolucent jaws. The dentist may be the first health professional to observe this condition on routine dental imaging. The diagnosis of osteoporosis is made primarily by a bone density test, known as a DEXA (dualenergy X-ray absorptiometry) scan. Osteoporosis is treated by bisphosphonate medications to maintain bone mass and reduce bone remodeling.
Reference
White SC, Pharoah MJ, eds. Oral Radiology: Principles and Interpretation. 7th ed. Mosby; 2014:460-461.
Refer a Colleague, Get Rewarded
AGD Referral Rewards Program
Refer your colleagues to join AGD and you’ll both earn $50 in Referral Rewards once they join!
Learn More
“AGD has been pivotal in shaping my career through its quality education and relationships among the members. I wouldn’t be where I am today without AGD!”