Dentistry’s responsibility for sustainable practices
HEALTH MEDICINE AND NUTRITION
What every dentist needs to know about chocolate
ORTHODONTICS
Clear aligner therapy and symptoms of TMDs
Premium Plus Membership
Unlock the ultimate VIP experience and indulge in a membership crafted exclusively for YOU!
For an additional $199, you can receive the following:
• Free Early-Bird Scientific Session Registration
• Free CE Library PLUS 4 On-Demand Webinars of Your Choice
• 20% Discount on Fall Fellowship Review Course
• 20% Discount on Fellowship Study Guide
“Premium Plus was the obvious choice for me, as someone who wanted to take advantage of all that the scientific session offers plus additional education opportunities through AGD. It was a game changer when working toward my Fellowship.”
Rachel Malterud, DMD, MPH, FAGD Member since 2016 Learn more www.agd.org/membership
DEPARTMENTS
5 Editorial
Piloting our AGD for future success
6 Pharmacology
The confusing regulatory landscape of enteral sedation in the United States
12
Endodontics
Endodontic pathosis from multiple teeth: a diagnostic challenge
14 Public Health
If the next opioid overdose happens in your office, will you be ready?
17 Ethics
Dentistry’s ethical responsibility to patients’ overall health through sustainable practices and climate change awareness
78 Oral Diagnosis
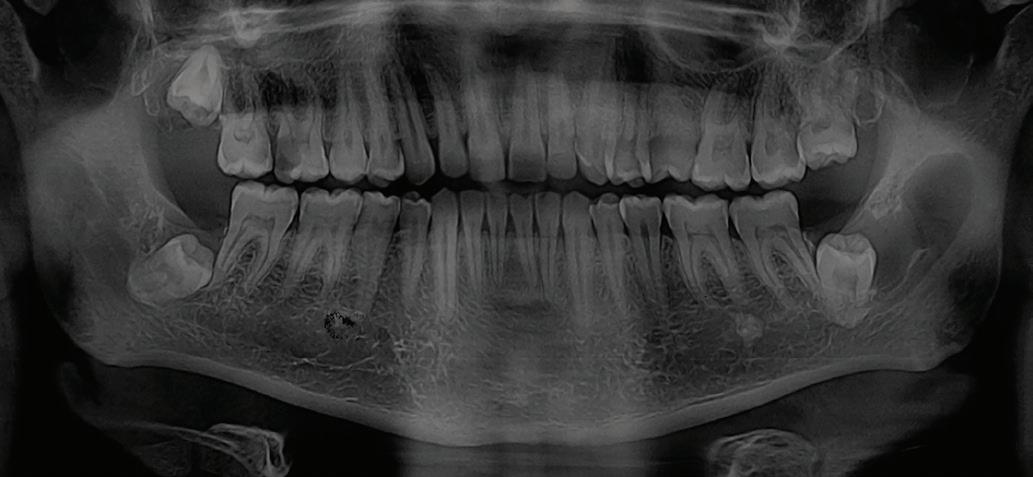
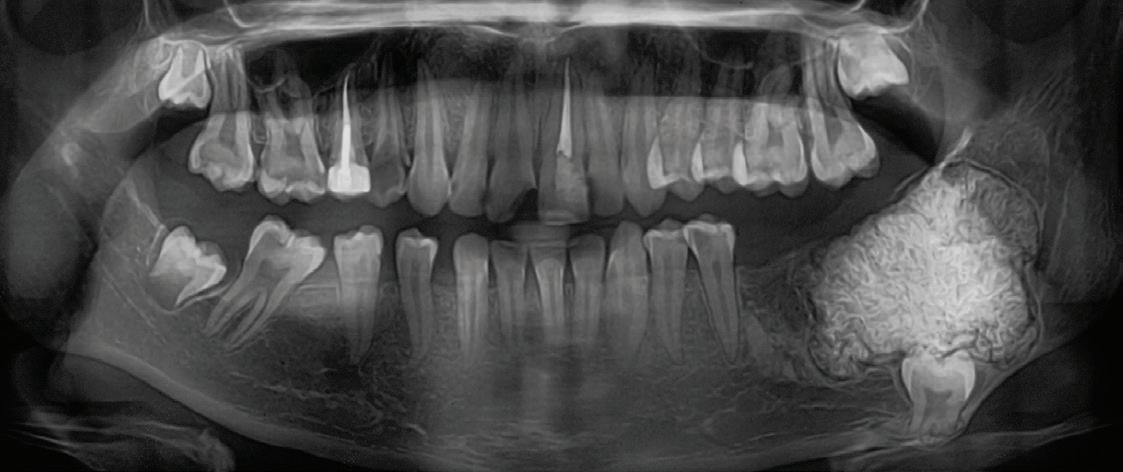
Bump on the gums and Inferior mandible radiolucency
79
Self-Instruction Answers
Exercises No. GD518, GD519, and GD520
CLINICAL ARTICLES
20 Basic Science
Evaluation of single-step self-etching ceramic primer and zirconia primer for bonding to zirconia-reinforced lithium silicate ceramic
Alfredo Estevam Llerena Icochea
Aliny Bisaia
Fabio Antonio Piola Rizzante
SELF-INSTRUCTION
27 Basic Science
Constantino Fernandes-Neto
Rafael Francisco Lia Mondelli
Adilson Yoshio Furuse
2 CE CREDITS, P. 25
Shear bond strength of resin cement to a CAD/CAM millable alloy subjected to various surface treatments
Mina Mohaghegh
Melika Hadadi
Maryam Firouzmandi
33 Oral Medicine, Oral Diagnosis, Oral Pathology
Pathologic jaw lesions associated with impacted teeth
Saede Atarbashi-Moghadam
Yaser Safi
38 Fixed Prosthodontics
Hosna Emamipour
Mitra Ghazizadeh Ahsaie
Comparison of flexural strength, marginal gap, and internal fit of milled and 3D-printed crown materials
Matthew Firestone
Robert Masterson
Christopher Raimondi
Eric Hu
Gen Paek
Wen Lien
SELF-INSTRUCTION EXERCISE GD537, 2 CE CREDITS, P. 46
47 Orthodontics
Clear aligner therapy and symptoms of temporomandibular disorders: a case report
Lina Sharab
Bushra Butul
Aqib Shafi
Jeffrey P. Okeson
SELF-INSTRUCTION EXERCISE GD538, 2 CE CREDITS, P. 53
54 Oral Medicine, Oral Diagnosis, Oral Pathology
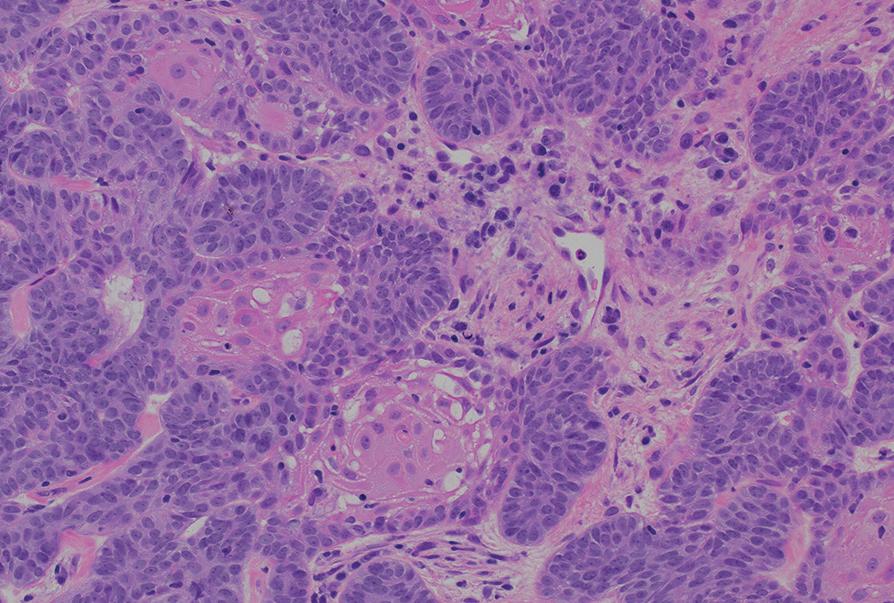
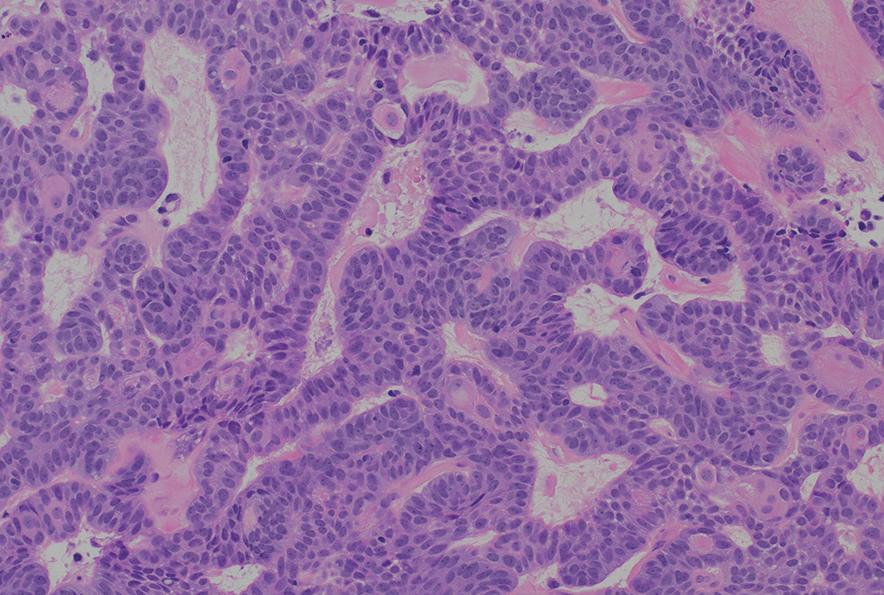
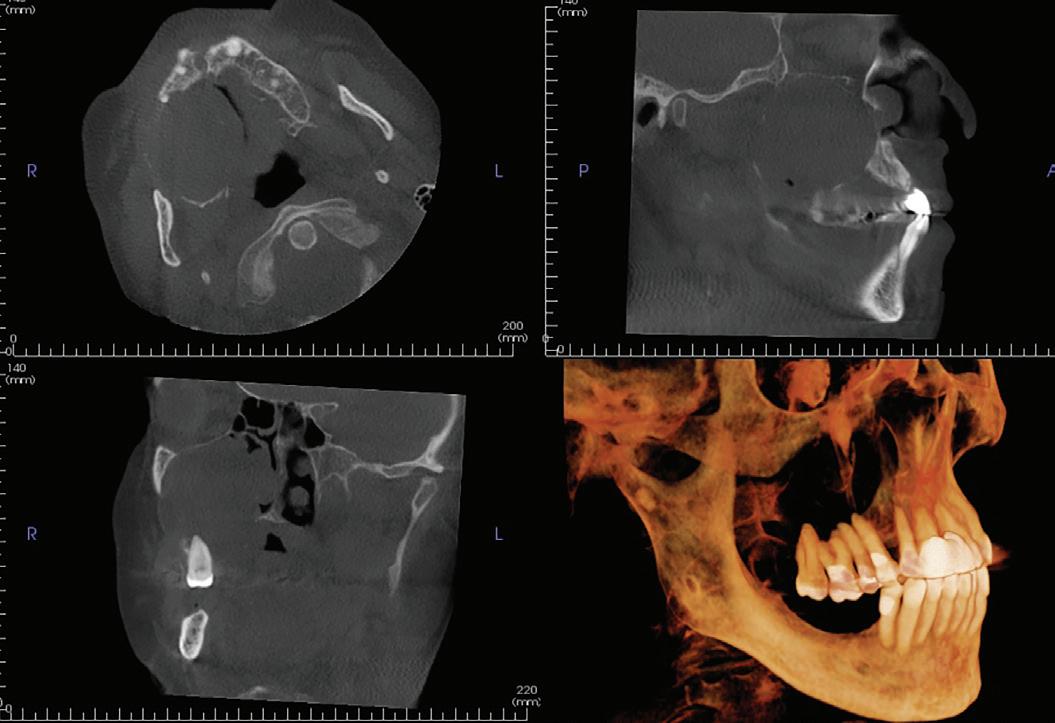
An unusual clinical and histopathologic presentation of a maxillofacial ameloblastoma: a literature review and case report
Pallavi Parashar
Clayton Davis
62 Fixed Prosthodontics
Salima Asifali Sawani
Camila Pacheco-Pereira
Minimizing excess cement around implant restorations: an in vitro study of cementation techniques
Hayleen Moran
68 Health Medicine and Nutrition
Nurit Bittner
What every dentist needs to know about chocolate
Emily M. D. Wieser
Christina L. Platia
72 Implants
Jeffery B. Price
Nasir Bashirelahi
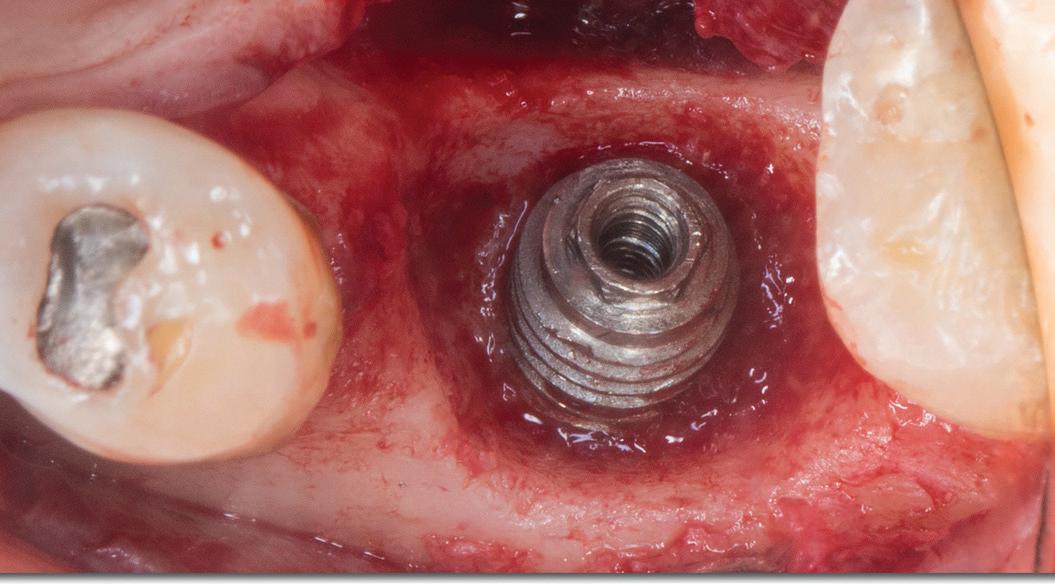
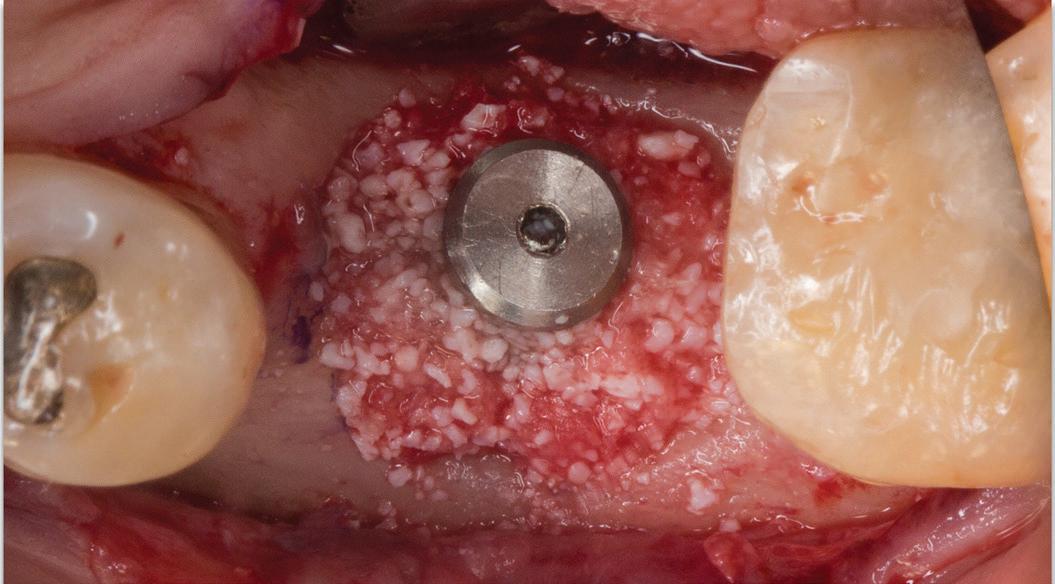
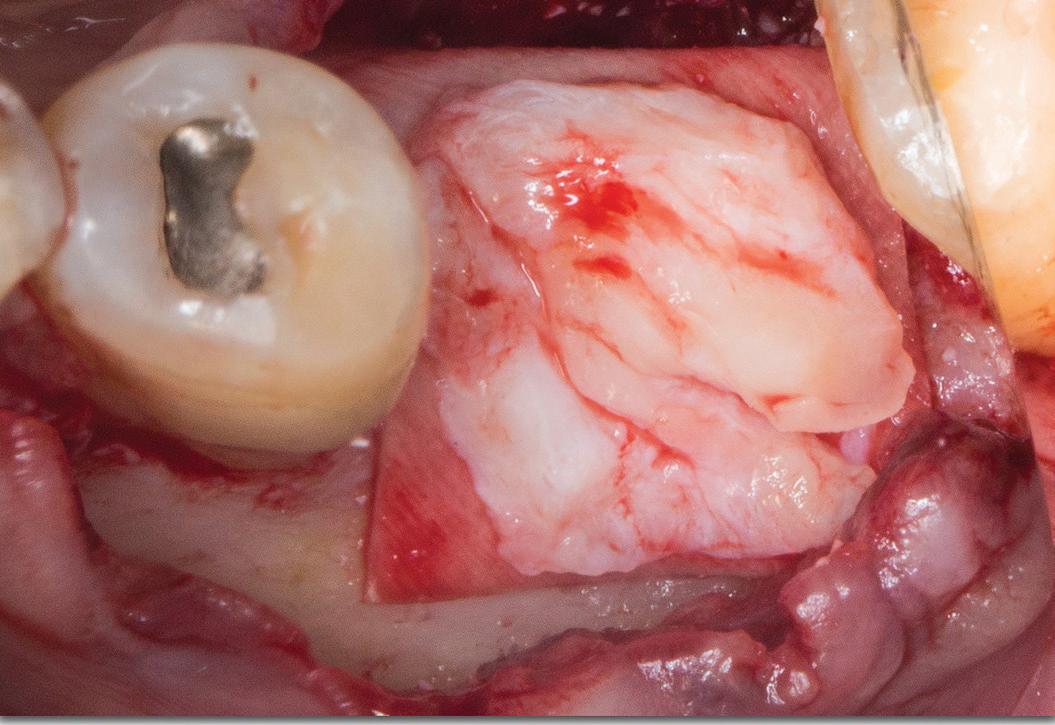
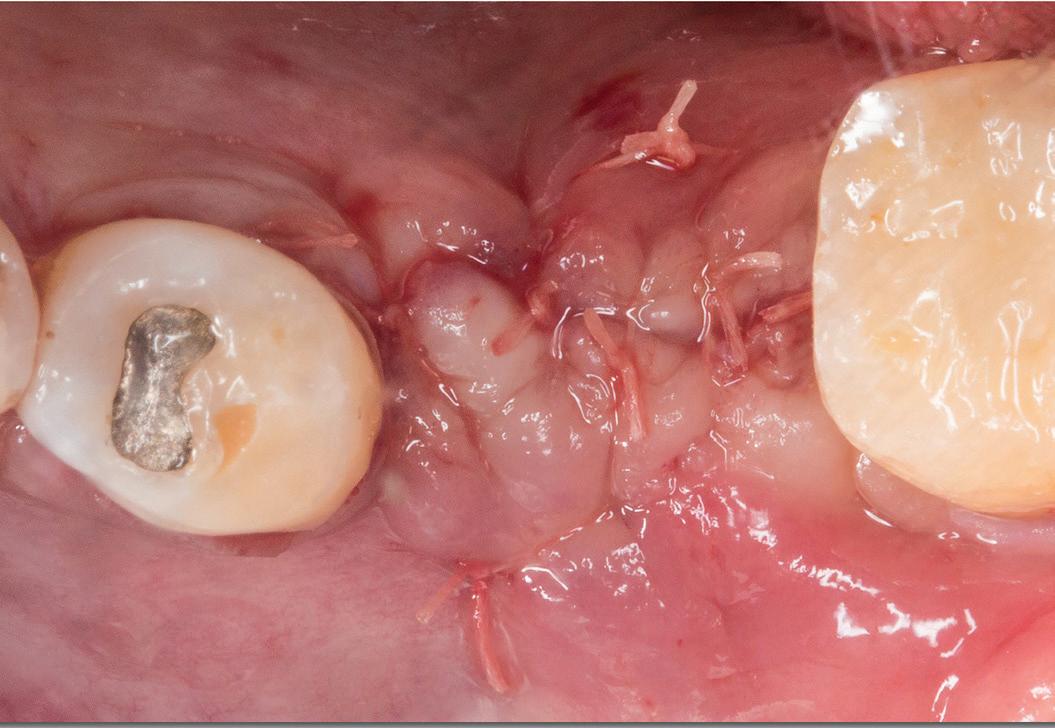
Surgical treatment of peri-implantitis via multiple decontamination procedures and a regenerative protocol: a case report with 6-year follow-up Ísis de Fátima Balderrama
Nicolas Nicchio
Elcio Marcantonio-Junior
Guilherme José Pimentel Lopes de Oliveira
Ana Carolina Monachini-Marcantonio
Cover image inspired by: Shear bond strength of resin cement to a CAD/ CAM millable alloy subjected to various surface treatments , on p. 27
Back Issues and Change of Address Members, call 888.243.3368 and ask for a Member Services representative.
Mailing Lists
For information about ordering AGD mailing lists, call 888.243.3368 ext. 4097 or email advertising@agd.org.
All materials subject to copying and appearing in General Dentistry may be photocopied for the noncommercial purposes of scientific or educational advancement. Reproduction of any portion of General Dentistry for commercial purposes is strictly prohibited unless the publisher’s written permission is obtained.
AGD does not necessarily endorse opinions or statements contained in essays or editorials published in General Dentistry. The publication of advertisements in General Dentistry does not indicate endorsement for products and services. AGD approval for continuing education courses or course sponsors will be clearly stated.
General Dentistry (ISSN 0363-6771) is published bimonthly in 2024 by the AGD, 560 W Lake St, Sixth Floor, Chicago, IL 60661-6600. AGD members receive GeneralDentistry as part of membership.
Periodicals postage paid at Chicago, IL and additional mailing office. POSTMASTER: Send address changes to General Dentistry, 560 W Lake St, Sixth Floor, Chicago, IL 60661-6600. Email: subscriptions@agd.org.
Canadian mailing information: IPM Agreement number 40047941. Change of address or undeliverable copies should be sent to: Station A, PO Box 54, Windsor, Ontario, N9A 6J5, Canada. Email: subscriptions@agd.org.
The nonmember individual subscription rate for General Dentistry is $120 for the print version, $120 for the online version, and $200 for print and online versions; the nonmember institution rate is $355 (add $5 for Canada). Single copies of General Dentistry are available to nonmember individuals for $22.50 and nonmember institutions for $27.
The question frequently raised by our AGD leadership team is: how can we continue to grow and excel as a professional organization? Our AGD provides so many valuable services, most notably advocacy and high-quality continuing education. However, many general dentists who are not members may be unaware of AGD’s existence or its benefits.
Although volunteer faculty in dental schools may introduce students to the Academy, these recruiting initiatives lack uniformity across regions. For some students, even nominal membership dues, offered at reduced rates to encourage involvement, can seem prohibitive as graduates face significant financial challenges and the burden of educational debt.
Established practitioners also feel the financial strain of running a dental practice and may allocate discretionary funds elsewhere. As dentists advance in their careers, their priorities evolve rapidly, and it is essential for each individual to assess what matters most to them. AGD competes with other organizations for members’ attention and must consistently demonstrate its value.
As volunteer leaders, our responsibility is to clearly articulate that value. We need to enhance participation by showcasing our exceptional speakers, who elevate clinical and business skills. The membership cost is not the issue when the perceived value is high.
To grow our organization, current members must promote the importance of AGD to nonmembers, guiding them toward our organization. Throughout my tenure, I’ve led various initiatives, sometimes with mixed results. I firmly believe that education is key to personal and professional success, and I share with others my confidence in AGD as a unique support—for both new graduates and experienced dentists—in the pursuit of continuous improvement and clinical excellence.
As AGD leaders, we must pilot our colleagues toward membership and a deeper understanding of our values. This
concept resonates with me, especially after conducting an implant training course at Washington AGD. I began the surgical segment by emphasizing the importance of the pilot bur in dental implant osteotomy. This initial step is crucial for evaluating the implant’s ideal position, much like guiding colleagues into their ideal position within the industry. The pilot bur helps determine not only the correct position but also the depth of the procedure, ensuring safety and efficacy. Similarly, seeking guidance from experienced dental pilots can illuminate the path toward achieving professional goals.
Understanding the right direction to take in surgery or in one’s career can be challenging, but once a direction is chosen, expanding one’s knowledge base is essential. Just as osteotomy burs widen a surgical site after establishing the correct position, enhancing one’s skill set opens new opportunities for financial and personal satisfaction in dentistry.
The complexities of implant dentistry extend beyond technique; they involve understanding anatomy, acknowledging the patient’s desires, and effectively communicating treatment options. Similarly, navigating a career in dentistry requires more than mastering clinical skills. It’s about integrating knowledge into a fulfilling lifestyle. Just as pilots steer planes safely to their destinations, we must ensure that prospective members know AGD will provide a smooth and successful journey through their career in general dentistry.
We may have some work to do in this endeavor, but I have complete confidence that we will meet our goals and provide a wonderful service—not only to the profession but to our communities at large.
Timothy F. Kosinski, DDS, MAGD Editor
PHARMACOLOGY
The confusing regulatory landscape of enteral sedation in the United States
Mark Donaldson, BSP, ACPR, PHARMD, FASHP, FACHE ¢ Jason H. Goodchild, DMD
Guidelines for the teaching and use of sedation and general anesthesia by oral healthcare providers (OHCPs) were first developed by the American Dental Association (ADA) in 1971 and have been updated 11 times since.1 The latest evolution of this document, adopted in 2016, was intended to add clarity and direction for OHCPs wishing to use these modalities and to further improve procedural sedation safety and efficacy.2,3 While the ADA produces guidelines, it is the purview of individual state dental boards to incorporate these guidelines into their regulations verbatim or develop entirely unique and customized rules for the use of sedation and general anesthesia to help fulfill their mandate of protecting the public. This creates the opportunity for up to 51 different iterations or interpretations of the ADA sedation guidelines, which can reduce their intended clarity and lead to confusion among OHCPs, especially clinicians who may practice in more than 1 state.
The intent of this column is to review the basic terminology and tenets of sedation and general anesthesia outlined in the ADA guidelines while drawing specific attention to the regulatory differences among dental boards pertaining to enteral sedation.2
Levels of sedation
Since the 2007 update, the ADA’s sedation and anesthesia guidelines
have defined 4 levels of consciousness: minimal sedation, moderate sedation, deep sedation, and general anesthesia . 4 Anxiolysis, the term previously used to define a technique for diminishing or eliminating anxiety, was replaced by minimal sedation. The term conscious sedation was eliminated from the guidelines entirely at that time.4 Table 1 presents the ADA’s definitions of the 4 levels of sedation and anesthesia, which are based on those of the American Society of Anesthesiologists (ASA). 2,5 It is important to recognize that in both minimal and moderate sedation, patients are conscious, can maintain their own airway without assistance, can respond appropriately to verbal and tactile stimulation, and maintain normal cardiovascular function. 6,7
Enteral sedation is the technique of medication administration in which the drug is absorbed across enteral membranes such as the gastrointestinal tract or oral mucosa (ie, oral, rectal, or sublingual).2 The intranasal route of drug delivery, while involving the nasal mucosa, is not considered enteral because it bypasses the gastrointestinal tract; intranasally delivered medications pass directly to the blood-brain barrier through the cribriform plate, allowing for faster onset of effects than enteral routes. 8 Anesthesia delivered intranasally and through other routes that bypass the gastrointestinal tract, including intravenous, intramuscular,
submucosal, and subcutaneous administration, is termed parenteral sedation.
The enteral route is the safest route for drug administration because it provides protection against foreign substances by the vomiting mechanism, first-pass elimination, and a muted anaphylactic response.9 The relatively slow absorption of enterally administered medication reduces distributional influences, allows the provider to recognize deleterious trends, and offers the opportunity to decrease further absorption. The enteral route eliminates the fear factor for patients who are afraid of needles and avoids local injury associated with needle puncture, venous irritation leading to thrombophlebitis, and ischemia resulting from intra-arterial injection.9 The disadvantages of enterally administered medications specific to sedation are the potential for slow and erratic absorption of the drug, the inability to easily titrate the dose to effect, and the lack of intravenous access.
The most common drug type used for dental enteral sedation in the United States is the benzodiazepines, including triazolam, lorazepam, midazolam, and diazepam. The benzodiazepine family of drugs has several advantages for enteral sedation, including the wide number of choices to match the right drug for the right patient, anxiolytic properties, anterograde amnesia, and their large margin of safety (little or no effects on
Terminology Definition
Minimal sedationa “A minimally depressed level of consciousness, produced by a pharmacological method, that retains the patient’s ability to independently and continuously maintain an airway and respond normally to tactile stimulation and verbal command. Although cognitive function and coordination may be modestly impaired, ventilatory and cardiovascular functions are unaffected.”
Moderate sedation “A drug-induced depression of consciousness during which patients respond purposefully to verbal commands, either alone or accompanied by light tactile stimulation. No interventions are required to maintain a patent airway, and spontaneous ventilation is adequate. Cardiovascular function is usually maintained.”
Deep sedation “A drug-induced depression of consciousness during which patients cannot be easily aroused but respond purposefully following repeated or painful stimulation. The ability to independently maintain ventilatory function may be impaired. Patients may require assistance in maintaining a patent airway, and spontaneous ventilation may be inadequate. Cardiovascular function is usually maintained.”
General anesthesia “A drug-induced loss of consciousness during which patients are not arousable, even by painful stimulation. The ability to independently maintain ventilatory function is often impaired. Patients often require assistance in maintaining a patent airway, and positive-pressure ventilation may be required because of depressed spontaneous ventilation or drug-induced depression of neuromuscular function. Cardiovascular function may be impaired.”
a Previously known as anxiolysis
respiratory and cardiovascular systems). They have a rapid onset, generally 1.0 to 1.5 hours, and are short acting, which makes them appropriate for in-office use. In addition, a reversal agent (flumazenil) is available.
The 2 levels of sedation appropriate for the use of enteral medications are minimal and moderate sedation. Minimal sedation may be achieved by the administration of a single enteral drug, in single or divided doses and with or without nitrous oxide–oxygen inhalation, to achieve the desired clinical effect. The cumulative dose of the enteral drug must not exceed the US Food and Drug Administration (FDA) maximum recommended dose (MRD) for unmonitored home use.2 Moderate enteral sedation may be viewed as a slightly deeper level of sedation compared to minimal sedation and may be achieved by administration of single or multiple enteral drugs with or without the use of nitrous oxide and oxygen. It is important to note that sedation and anesthesia are a continuum 2:
Repeated dosing of an agent before the effects of previous dosing can be fully appreciated may result in a greater alteration of the state of consciousness than is the intent of the dentist.
The confusing landscape of anxiolysis and minimal sedation
Table 2 reviews permit requirements for nitrous oxide–oxygen inhalation, minimal sedation, and enteral moderate sedation in the United States. As these complex regulations cannot be fully described in a summary, clinicians are encouraged to read the applicable rules for sedation and anesthesia in their state of practice and, if needed, contact the dental board for additional information.10-15 Currently, 10 states require a dentist to have a permit to use nitrous oxide and oxygen, and 15 states require a permit to administer minimal sedation. While 17 states have a specific permit for the use of enteral moderate sedation, 2 states allow the dentist to administer enteral minimal or moderate sedation without a permit. In the remaining 31 states and Washington, DC, OHCPs who wish to administer moderate sedation by any route must obtain a moderate sedation permit. This approach to regulating moderate sedation is consistent with the ADA guidelines2:
Level of sedation is entirely independent of the route of administration. Moderate and deep sedation or general anesthesia may be achieved via any route of administration and thus
an appropriately consistent level of training must be established.
All 51 dental boards in the United States require permits for the use of parenteral sedation and deep sedation/ general anesthesia.
Although the term anxiolysis was replaced by minimal sedation in the ADA guidelines almost 2 decades ago, current state dental board usage and rules pertaining to these terms are confusing and outdated. Furthermore, finding information and definitions for these terms on dental board websites is tedious and difficult. In some cases, these terms are used interchangeably; for example, the dental board rules of Wyoming clearly state, “ ‘Anxiolysis’ is minimal sedation.”14 In some cases, old and new terms are mingled, as in the regulations for Washington, DC15:
A dentist who administers anxiolysis shall maintain a margin of safety and a level of consciousness that does not approach moderate sedation and other deeper states of sedation and general anesthesia.
According to the administrative code of Florida, a licensed dentist can administer a single dose of a single enteral sedative up
Table 1. Levels of sedation and anesthesia. 2
Table 2. Summary of permits required for nitrous oxide–oxygen inhalation, minimal sedation, and enteral moderate sedation by state dental boards. a
Maine No No (patients ≥ 13 y) Yes (patients < 13 y)
Maryland No No
Massachusetts Yes Yes
Michigan No Yese
Minnesota No No
Mississippi No Yesf
Missouri No No Yes
Montana No No Yesb
Nebraska No Yes Yesb
Nevada No No Yesb
New Hampshire No Noc Yesb
New Jersey No No Yes
New Mexico Yes Yes Yesb
New York No No Yesb
to the MRD or a single narcotic analgesic medication appropriate for the unsupervised treatment of anxiety and pain with or without nitrous oxide and oxygen to achieve minimal sedation.16 In Nevada, licensed dentists are allowed to administer a single dose of a single enteral agent to achieve anxiolysis but cannot combine it with any other form of sedation, including nitrous oxide–oxygen inhalation.17
Deciphering the confusing the rules for anxiolysis and minimal sedation is
acutely important for OHCPs in states that require a minimal sedation permit. Clinicians may wonder what level of sedation an OHCP can provide based on their dental licensure and when an additional permit is required. Among
a All information is taken from the websites of the state dental boards. The information in this table is not a substitute for clinicians’ own review of the sedation and anesthesia rules of the state or states in which they practice. It is essential that clinicians read the applicable rules for sedation and anesthesia and, if needed, contact the dental board for additional information.
bThe state has no separate permit to provide moderate sedation by the enteral route specifically; a moderate sedation permit is required to provide moderate sedation by any route.
cThe state does not require a permit for minimal sedation, but there are specific rules for age-appropriate use of minimal sedation.
d Colorado: Minimal sedation pediatric designation is required for patients younger than 12 years of age. No minimal sedation permit is required if medication is prescribed or administered to nonpediatric patients ( ≥ 12 years), for the relief of anxiety or apprehension, with the following limitations: a dose of a single drug (up to the maximum recommended dose) with or without nitrous oxide (3 Colo Code Regs §709-1.14).10
e Michigan: Dentists are required to take a comprehensive training program in moderate sedation to administer minimal or moderate sedation (Mich Admin Code R §338.11602).11
f Mississippi: A licensed dentist without an advanced anesthesia permit can provide anxiolysis by nitrous oxide and oxygen; a single enteral agent not to exceed the maximum recommended dose; or nitrous oxide and oxygen with a single enteral agent in patients aged 8 years and older (30 Miss Code R. 2301-1.30).12
g North Carolina: A minimal conscious sedation permit is required. The North Carolina State Board of Examiners also defines anxiolysis as a “pharmacological reduction of anxiety through the administration of a single dose of a minor psychosedative, possibly in combination with nitrous oxide, to children (diazepam, diphenhydramine, hydroxyzine) or adults (e.g., alprazolam, diazepam, lorazepam) prior to commencement of treatment on the day of the appointment that allows for uninterrupted interactive ability in an awake patient with no compromise in the ability to maintain a patent airway independently and continuously. Nitrous oxide may be administered in addition to the minor psychosedative without constituting multiple dosing for purpose of these Rules” (21 NC Admin Code §16Q .0101).13
the most confusing examples of dental board rules are those in Colorado and Mississippi, which allow licensed dentists to administer anxiolysis and anxiety relief using an oral medication (a single drug, up to the MRD) with or without nitrous oxide–oxygen inhalation but still require a minimal sedation permit.10,12 This seeming contradiction may leave the licensed dentist in these states unclear about what clinically constitutes minimal sedation and when a permit is required. The distinction is clearer in a state such as Oregon, where a single enteral sedative for anxiolysis may be administered without a minimal sedation permit when used without nitrous oxide and oxygen.18 When an
Box. Best practices for minimal enteral sedation.
• Maintain Basic Life Support (BLS) for Healthcare Providers certification (dentist and team).
• Ensure the availability of an appropriate sedation team. The sedation team must include the dentist and at least one other person who has BLS certification (sometimes called an anesthesia monitor).
• Maintain a properly stocked medical emergency kit, including a vial of flumazenil and syringe (eg, 3-mL with 25-gauge 1-inch needle). Consider including a vial of naloxone or Narcan nasal spray.
• Certify that the patient is a good candidate for minimal sedation. Obtain a focused medical history by determining the patient’s American Society of Anesthesiologists (ASA) physical status classification, body mass index, STOP-Bang screening score (obstructive sleep apnea), Mallampati score (difficulty of endotracheal intubation), and history of adverse sedation experiences.
• Consider preprocedure dietary restrictions based on the sedation technique.
• Give verbal and written preoperative instructions to the patient, parent, escort, guardian, and/or caregiver.
• Document the intended level of sedation (ie, the minimal sedation provided).
• Take baseline vital signs (pulse, blood pressure, oxygen saturation) and document them in the patient record.
• Use a pulse oximeter continuously during the sedation appointment.
• Do not ever leave a sedated patient alone. The patient must be visually and verbally monitored at all times.
• Use a time-oriented sedation record to document the monitoring parameters and drugs used (including local anesthesia).
• Document the patient’s vital signs at discharge.
• Ensure that the patient satisfies the discharge criteria for dismissal (eg, vitals within 20% of normal; appropriate mental status and level of consciousness; ability to ambulate; acceptable pain level; minimal bleeding; absence of nausea or vomiting).
• Give verbal and written postoperative instructions to the patient, parent, escort, guardian, and/or caregiver.
• Ensure that the patient will be driven home from the appointment by an adult companion.
• Make a postoperative telephone call to remind the patient of postoperative instructions, including the importance of taking analgesics (ibuprofen + acetaminophen) on schedule and when to resume eating and drinking.
enteral medication and nitrous oxide–oxygen inhalation are combined, Oregon requires a minimal sedation permit. In North Carolina, the state dental board has defined a permit for minimal conscious sedation that appears to be a blending of minimal and moderate sedation rules.13 However, dentists can still administer a minor psychosedative to achieve anxiolysis, possibly in conjunction with nitrous oxide and oxygen, without an additional permit. The board has published 2 interpretative statements that help differentiate anxiolysis from minimal conscious sedation.19,20
A number of states have restrictions or special rules for the use of minimal
sedation based on the patient’s age. In California, no permit is required to administer minimal sedation to a patient 13 years of age or older, but a pediatric minimal sedation permit is required for patients under the age of 13 years.21 Even if the state does not have a permit requirement, it may still have rules for age-appropriate use of minimal sedation. For example, in Idaho, licensed dentists are allowed to administer minimal sedation to patients aged 16 years or older.22 The appropriate dose for sedation in this case is considered to be a single enteral drug administered in a dose that does not exceed the maximum FDA-recommended dose for unmonitored home use.
However, Idaho has established different rules for younger patients22:
In cases where the patient weighs less than one hundred (100) pounds, or is under the age of sixteen (16) years, minimal sedation may be administered without a permit by use of nitrous oxide, or with a single enteral dose of a sedative agent administered in the dental office.
Other states that have age-specific rules for minimal sedation include Alaska, Arkansas, Colorado, Georgia, Louisiana, Maine, Mississippi, New Hampshire, Ohio, and South Dakota. While the common understanding of the term minimal sedation is that it refers to administration of a single enteral medication given in a dose that does not exceed the FDA’s MRD, some states, such as Georgia, introduce an additional term, supplemental dosing23:
For adults, supplemental dosing that may be necessary for prolonged procedures should not exceed one-half of the initial drug dose and should not be administered until the dentist has determined that the clinical half-life of the initial dosing has passed. The total aggregate dose must not exceed 1.5× the MRD on the day of treatment.
The 6 states that allow supplemental dosing during minimal sedation are Arizona, Arkansas, Georgia, Iowa, Montana, and Oregon. Oregon and Kentucky have also adopted a novel concept, presumptive sedation, for patients receiving nitrous oxide and minimal sedation.18,24 According to this principle, if the patient is concomitantly taking another substance with the potential to increase the sedative effects of the patient (eg, a chronic medication prescribed for a separate medical condition), additional permitting regulations may apply.
You want to administer sedation in the office: what should you do?
Any OHCP interested in providing inoffice sedation must first understand the state dental board rules that outline the training and permits that may be required. As noted previously, this
information is available online but not always easy to find or interpret. The rules help to define how these types of sedation should be provided: the appropriate sedation team, correct patient candidate, equipment needed, discharge criteria, and, in some cases, the drugs and doses to be used. Some state boards also have specific rules for continuing education for OHCPs who provide sedation. The Box presents several best practices for minimal sedation, based on the rules outlined in various states.
Conclusion
State dental boards may adopt ADA guidelines on the use of sedation and general anesthesia verbatim, but most have elected to customize the guidelines, creating a multitude of rules for minimal and moderate sedation across the United States. The disparate state rules, which are often hard to find and interpret, may confuse providers and hinder compliance. Nevertheless, as state dental board rules for sedation continue to evolve, it is incumbent on each OHCP who wishes to provide sedation services to review, understand, and abide by the applicable rules.
Author affiliations
Vizient Pharmacy Advisory Solutions, Irving, Texas (Donaldson); Skaggs School of Pharmacy, University of Montana, Missoula (Donaldson); School of Dentistry, Oregon Health & Sciences University, Portland (Donaldson); Faculty of Dentistry, University of British Columbia, Vancouver, Canada (Donaldson); Premier Dental Products Company, Plymouth Meeting, Pennsylvania (Goodchild); Department of Oral and Maxillofacial Surgery, Creighton University School of Dentistry, Omaha, Nebraska (Goodchild); Division of Oral Diagnosis, Department of Diagnostic Sciences, Rutgers School of Dental Medicine, Newark, New Jersey (Goodchild).
Conflicts of interest
None reported.
Disclaimer
The views expressed in this column are those of the authors and do not necessarily reflect those of Vizient, Premier Dental Products Company, Creighton University School of Dentistry, or Rutgers School of Dental Medicine.
References
1. American Dental Association, Council on Dental Education. Guidelines for Teaching the Comprehensive Control of Pain and Anxiety in Dentistry. American Dental Association; 1971.
2. American Dental Association. Guidelines for the Teaching and Use of Sedation and General Anesthesia. October 2016. Accessed September 3, 2024. https://www.ada.org/-/ media/project/ada-organization/ada/ada-org/files/ resources/research/ada_sedation_use_guidelines.pdf
3. Solana K. ADA House of Delegates adopts revisions in sedation, anesthesia guidelines. ADA News 2016;47(21):1, 15.
4. American Dental Association. Guidelines for the Use of Sedation and General Anesthesia by Dentists. October 2007. Accessed September 24, 2024. https://www.ada. org/-/media/project/ada-organization/ada/ada-org/ files/publications/cdt/anesthesia_guidelines.pdf
5. American Society of Anesthesiologists Committee on Quality Management and Departmental Administration. Continuum of depth of sedation: definition of general anesthesia and levels of sedation/analgesia. Last updated October 23, 2019. Accessed September 25, 2024. https:// www.asahq.org/standards-and-practice-parameters/ statement-on-continuum-of-depth-of-sedationdefinition-of-general-anesthesia-and-levels-of-sedationanalgesia
6. Goodchild JH, Feck AS, Silverman MD. Anxiolysis in general dental practice. Dent Today. 2003;22(3):106-111. https://www.dentistrytoday.com/anxiolysis-in-generaldental-practice/
7. Goodchild JH, Donaldson M, Chanpong B. The new dental anesthesiology specialty: implications for the general dentist. Gen Dent. 2019;67(4):12-15.
8. Donaldson M, Goodchild JH. Intranasal delivery of medications: opportunities for dentistry. Gen Dent 2023;71(4):10-14.
9. Dionne RA, Yagiela JA, Coté CJ, et al. Balancing efficacy and safety in the use of oral sedation in dental outpatients. J Am Dent Assoc. 2006;137(4):502-513. doi:10.14219/ jada.archive.2006.0223
10. Colorado Dental Board. Anesthesia. 3 Colo Code Regs §709-1.14. June 30, 2016. Accessed September 2, 2024. https://www.sos.state.co.us/CCR/GenerateRulePdf.do? ruleVersionId=11199&fileName=3%20CCR%20709-1
11. Michigan Board of Dentistry. Moderate or minimal sedation; requirements. Mich Admin Code R §338.11602. October 2, 2023. Accessed September 27, 2024. Mich Regist 2023;(19):41-42. https://www.michigan.gov/lara/-/ media/Project/Websites/lara/moahr/ARD/2023Michigan-Register/MR19_110123.pdf?rev=1a807f9e 176f4fc6bb121381d1353578&hash=12B8DCD116CC7 B1932AD334F6DF59D6E
12. Mississippi State Board of Dental Examiners. Board Regulation Number 30. Administration of Anesthesia. 30 Miss Code R 2310-1.30. May 19, 2020. Accessed September 2, 2024. https://www.dentalboard.ms.gov/sites/dentalboard/files/REG%2030%20FINAL%20FILING%20PDF.pdf
13. North Carolina Board of Dental Examiners. General Anesthesia and Sedation Definitions, 21 NC Admin Code 16Q .0101. June 1, 2017. Accessed September 3, 2024. http:// reports.oah.state.nc.us/ncac/title%2021%20-%20occupational%20licensing%20boards%20and%20commissions/ chapter%2016%20-%20dental%20examiners/subchapter%20q/subchapter%20q%20rules.pdf
14. Wyoming Board of Dental Examiners. Wyoming Administrative Rules. Chapter 5. Anesthesia Administration and Sedation Permit Procedures. Section 3. Definitions. May 29, 2024. Accessed September 2, 2024. https://rules.wyo. gov/Search.aspx?Agency=034#
15. District of Columbia Department of Health. Dentist and Dental Facility Certification to Administer Sedation or General Anesthesia. 17 DC Mun Regs §10701.6. July 17, 2020. Accessed September 3, 2024. https://dchealth. dc.gov/sites/default/files/dc/sites/doh/publication/ attachments/17%20DCMR%20%20Ch.%20107%20% 20Ch.%2042%20%20Dental%20Anesthesia.pdf
16. Board of Dentistry, Florida Department of Health. Training, Education, Certification, and Requirements for Issuance of Permits. Fla Admin Code Ann R 64B5-14.003. September 12, 2022. Accessed September 3, 2024. https://www. flrules.org/gateway/ruleno.asp?id=64B514.003&Section=0
17. Nevada State Board of Dental Examiners. Administration of General Anesthesia, Moderate Sedation or Deep Sedation. Scope. Nev Admin Code §631.2211. August 2019. Accessed September 3, 2024. https://www.leg.state. nv.us/Division/Legal/LawLibrary/NAC/NAC-631. html#NAC631Sec2211
18. Oregon Board of Dentistry. Chapter 818, Division 26. Anesthesia. Section 818-026-0000. January 1, 2020. Accessed September 3, 2024. https://secure.sos.state. or.us/oard/displayDivisionRules. action?selectedDivision=3691
19. North Carolina Board of Dental Examiners. Interpretive Statement Regarding Administration of Anxiolysis to Adult and Geriatric Patients. March 13, 2023. Accessed September 3, 2024. https://www.ncdentalboard.org/ PDF/Anxiolysis%20BODE%20Interpretive%20Statement% 203-13-23.pdf
20. North Carolina Board of Dental Examiners. Interpretive Statement Regarding Administration of Anxiolysis to Pediatric Patients. May 17, 2023. Accessed September 3, 2024. https://www.ncdentalboard.org/PDF/2023-0517%20Pediatric%20Anxiolysis%20Interpretive%20Statement.pdf
21. Dental Board of California. Article 5.1. Pediatric Minimal Sedation. 16 Cal Code Regs §1043.9.1. August 16, 2022. Accessed September 2, 2024. https://govt.westlaw.com/ calregs/Browse/Home/California/CaliforniaCodeof Regulations?guid=IE31A2B90224E11EDBD43BCE5C 41A44B1&originationContext=documenttoc&transition Type=Default&contextData=(sc.Default)
22. Idaho Board of Dentistry. Rules of the Idaho Board of Dentistry. Idaho Admin Code R 24.31.01 200.13. July 1, 2024. Accessed September 30, 2024. https://adminrules. idaho.gov/rules/current/24/243101.pdf
23. Georgia Board of Dentistry. Conscious Sedation Permits. Ga R Regs §150-13-.01. May 25, 2023. Accessed September 2, 2024. https://rules.sos.ga.gov/gac/150-13
24. Kentucky Board of Dentistry. Anesthesia and Sedation Related to Dentistry. 201 Ky Admin Regs 8:550. October 26, 2022. Accessed September 3, 2024. https://apps. legislature.ky.gov/law/kar/titles/201/008/550/
Endodontic pathosis from multiple teeth: a diagnostic challenge
Nathan Dinsbach, DDS, MSD, FAGD
Diagnosis is a foundational principle of modern endodontic therapy. Prior to performing treatment, a clinician must be sure that the tooth to be treated is the source of a patient’s pathosis. Sensibility tests, a thorough history, and dental radiographs all provide necessary clues to make a diagnosis. I try to replicate the symptoms of the patient’s chief complaint when I perform sensibility tests. Thus, a careful history must be taken regarding symptoms. Often a patient will report that cold drinks had caused significant pain, but follow-up questions reveal that cold drinks caused pain a month or so previously, and that in the days leading up to their appointment, cold stimulus no longer triggered their pain. The information gathered from the history should guide diagnostic tests.
Replicating the symptoms preoperatively is important, especially when a patient later reports continued pain following completion of endodontic therapy. An example is when there is continued pain in response to cold stimuli after I complete endodontic therapy. The first test I will perform is a cold test on the tooth I treated, which will not trigger any pain. I will remind the patient how painful that test was prior to treatment. Usually, the lack of response to cold is very surprising to the patient. I then explain that the source of their current pain is most likely a different tooth. I will then continue the cold tests until we locate the
source of their pain. Performing the tests in this manner helps the patient realize the tooth treated is not the source of their current pain.
The following case will highlight the importance of collecting a thorough dental history and repeatedly performing sensibility tests to guide treatment when the endodontic pathosis causing a patient’s symptoms emanates from more than 1 tooth.
Case report
A 55-year-old woman presented for diagnosis of pain in the maxillary left posterior quadrant. About 1 year prior to that date, another endodontist had performed endodontic therapy on tooth 15. She had continued symptoms in the area. The endodontist checked tooth 15 and did not believe that her symptoms were related to that tooth, but he did not diagnose the source of her symptoms. On the day of my consultation, if she pushed laterally on tooth 15 with her tongue, she could elicit moderately sharp pain. She also had a constant ache in the area.
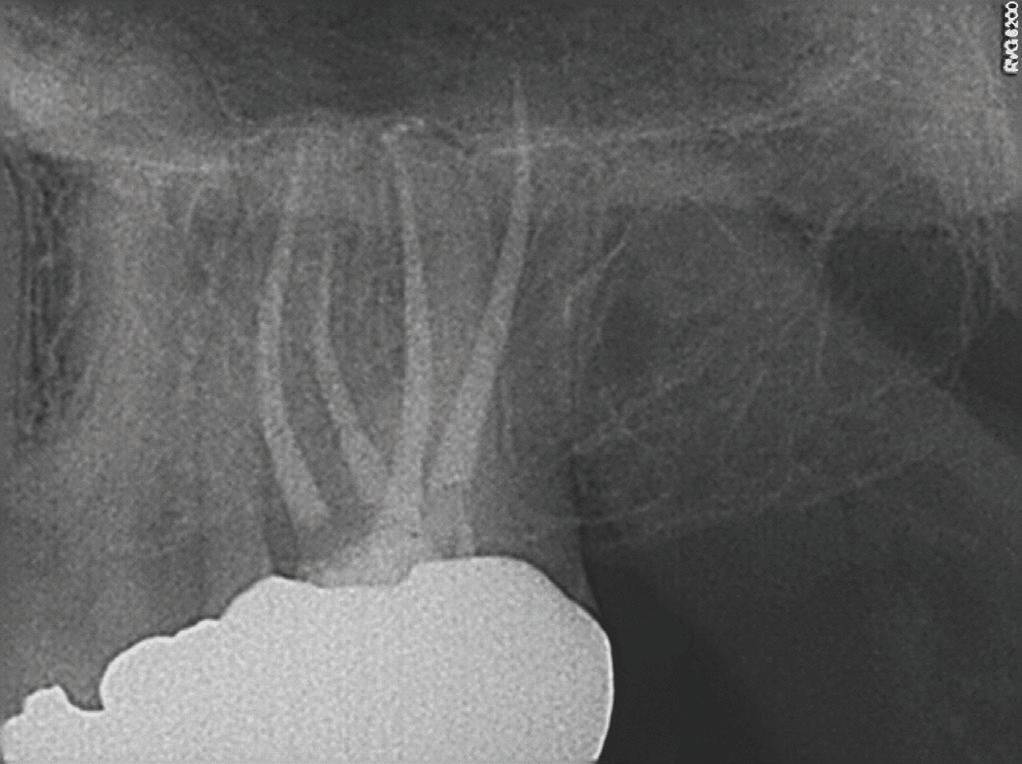
A periapical radiograph and a limitedfield-of-view cone beam computed tomogram of teeth 14 and 15 were taken, and no radiographic signs of apical periodontitis related to these teeth were noted that day (Fig 1). Sensibility tests were also performed. Tooth 15 responded normally to palpation and to bite and felt “different” on percussion (not painful, which is an important distinction to make). Tooth 14 responded
normally to palpation, percussion, and bite. Cold placed on tooth 14 triggered a significantly elevated, throbbing response that lingered more than 1 minute. Of all the tests performed, the cold on tooth 14 most closely replicated the pain of her chief complaint.
We reviewed treatment options, including no treatment. She elected to have endodontic therapy on tooth 14 performed that day. Local anesthetic was administered, and a dental dam was placed. This molar was slightly unusual in that I obtained patency in the palatal, distobuccal, and second mesiobuccal canals (MB2) that day, but the first mesiobuccal canal (MB1) was still not patent. Usually, it is MB2 that is the hardest to instrument. Calcium hydroxide medicament and a provisional restoration were placed. The patient was scheduled to return in 2 weeks for completion of endodontic therapy on tooth 14.
When she returned, I asked about her symptoms. The overall pain had reduced significantly, and the pain in tooth 15 with lateral pressure was gone, but there was still a deep ache in the area, now focused near tooth 15. She noticed a throbbing in the area with positional changes, such as sitting up and bending over. Sensibility tests were performed again. Tooth 14 responded normally to percussion, palpation, and bite. Tooth 15 responded normally to palpation, and percussion and bite elicited a moderately painful response (different from the results of the sensibility
tests performed preoperatively). We discussed the possible reasons for the pathosis related to tooth 15, including fracture. I recommended that if she desired to save the tooth, we should initiate retreatment of tooth 15 and place calcium hydroxide in the tooth. I would then see her a month later for a short consultation to check on her symptoms before obturating teeth 14 and 15. She agreed to this treatment plan.
Orthograde retreatment of tooth 15 was initiated that day in the usual manner, and calcium hydroxide was placed. At the follow-up appointment 1 month later, she was happy to report that
all her symptoms had resolved and that she had not needed to take ibuprofen or acetaminophen for more than 2 weeks. Both teeth were tested that day, and both responded normally to percussion, palpation, and bite. We then scheduled her for completion of treatment of both teeth.
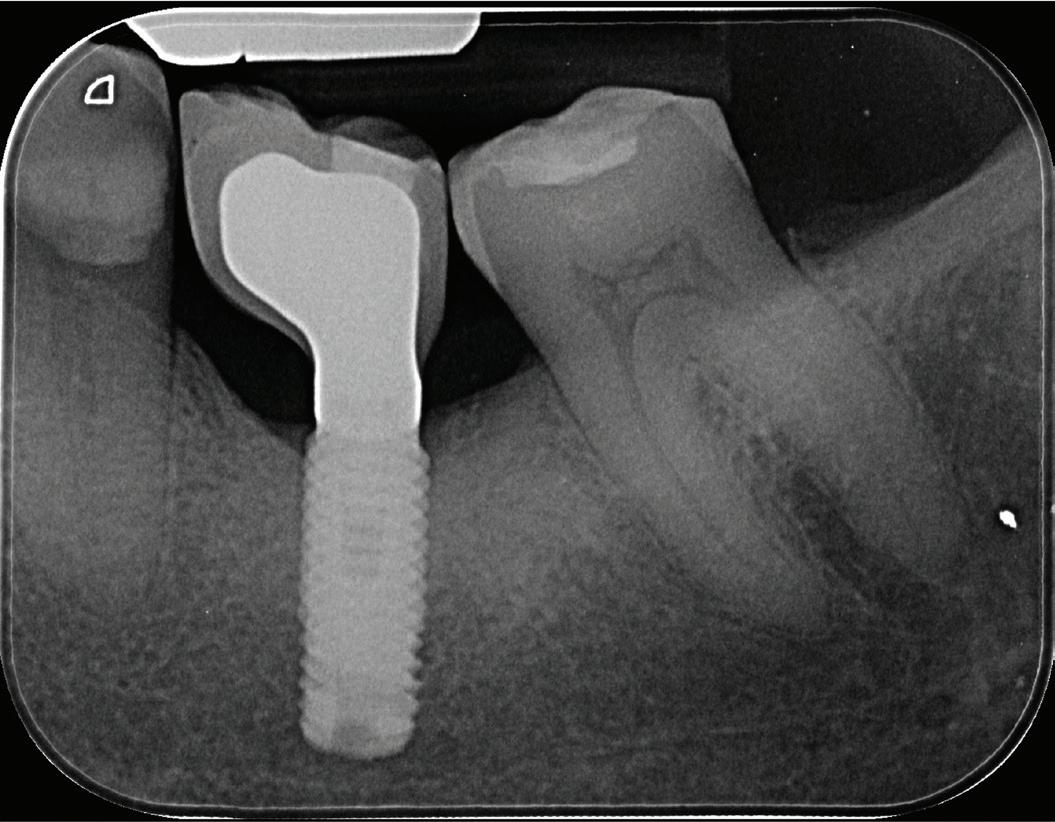
At our final appointment, I was able to fully instrument the MB1 canal. The final postoperative radiograph shows the curvature of the MB1 canal of tooth 14 (Fig 2). The teeth were closed with a medicated sponge and provisional material, and the patient was referred back to her general dentist for restoration of these teeth.
Conclusion
A careful dental history and radiographic assessment will guide sensibility tests to be performed when a patient presents with pain and symptoms. Preoperative tests can serve as a baseline recording for comparison if pain or symptoms continue during or after treatment. This is most helpful when a patient’s pain and symptoms result from more than 1 diseased tooth.
Author affiliation
Private practice, Utah.
Fig 2. Postoperative radiograph of teeth 14 and 15.
Fig 1. Preoperative radiographs. A. Tooth 14. B. Tooth 15.
If the next opioid overdose happens in your office, will you be ready?
Larry N. Williams, DDS, MPH
According to the Health Resources and Services Administration, more than 130 people in the United States die from opioid-related overdoses each day.1 That is nearly 4000 people per month. This level of loss led to the declaration of a public health emergency in the United States on Thursday, October 26, 2017.2 Numerous actions have taken place since this declaration to address this problem, and some of these involve dentistry. The purpose of this column is to look at various ways that our profession can be better prepared to address issues pertaining to opioid and substance misuse, which can lead to overdose and death.
Scope of the crisis
Some elements of the discussion surrounding opioids are widely understood. It is a given that dentists may prescribe opioids for moderate to severe pain. It is also a given that not all opioids come from reliable sources, and street opioids (eg, heroin or fentanyl) may be mixed with other substances. Opioids have an inherent risk of misuse, unknown use, and addiction. Anyone in your dental office, waiting room, or home may be an opioid user, abuser, or potential victim of overdose.
Opioid misuse
To increase awareness of and responsiveness to the opioid problem in this country, especially among youth, dentists must have a basic understanding of opioids that are prescribed
and used correctly, prescribed but used incorrectly, and street derived. Approximately 4% of youths between the ages of 12 and 17 years report having misused prescribed narcotic pain medications, and nearly 7% of young adults between 18 and 25 years old reported misusing opioids. 3
The signs of opioid misuse include drowsiness, constipation, nausea, dizziness, vomiting, dry mouth, headaches, sweating, mood changes, loss of appetite, and weakness.4 Signs of an opioid overdose include small, constricted pupils; falling asleep or loss of consciousness; slow, shallow breathing; choking or gurgling sounds; limp body; and discolored (bluish) skin, especially in the lips and nails.4 The timing between misuse and overdosing, or from consciousness to unconsciousness, is dependent on the type and dose of the drug ingested or injected, other additives, and length of opioid use. Opioids can also interact with other medication, alcohol, and certain health conditions.5
Fentanyl
The opioid with the most potent lethal dose is fentanyl, a synthetic opioid that is 100 times more potent than morphine.6 Fentanyl is lethal at a dose of 2 mg, the equivalent of 10 to 15 grains of salt, and many street drugs are being mixed with fentanyl.7 Drugs obtained through unofficial channels may contain a potentially lethal dose. As the Drug Enforcement Administration (DEA) notes, “Unless a drug is prescribed by a licensed medical
professional and dispensed by a legitimate pharmacy, you can’t know if it’s fake or legitimate.”6
Xylazine
Adding to the potential lethality of fentanyl is the addition of xylazine to the mix. Xylazine is a synthetic tranquilizer not approved for humans and not affected by emergency opioid-reversal medications like naloxone.8 According to the Centers for Disease Control and Prevention (CDC), xylazine is now found in many illicit medications and is linked to many overdose deaths.8
State efforts to address the crisis
Because of the rise in fentanyl use and resultant deaths, many states have initiated programs to educate residents about use of this drug. An example is the state of Georgia, which created a dedicated fentanyl information website.9 Many other states have similar resources. One key fact from Georgia’s site is that non-fentanyl–related opioid overdose deaths increased by 76% from 2019 to 2022, while fentanyl-related overdose deaths rose by 308% in the same time period.9 Georgia is one among many states that have enacted a medical amnesty law that encourages trained individuals to help address potential overdoses and protects both the overdose victim and bystanders who call for help from criminal charges. Illinois has enacted similar policies and introduced an effort to teach students about the
extreme danger of fentanyl.10,11 Ageappropriate education on the dangers of fentanyl is mandatory for Illinois 6th through 12th graders beginning in the current school year. Many other states are considering options to address the overdose potential of fentanyl and other combined drugs. Additionally, more than 20 states have added opioid training to continuing education requirements for dental license renewal.12
Federal efforts to address the crisis
At the federal level, 2 agencies, the DEA and Food and Drug Administration (FDA), made regulatory changes to help address the overdose public health emergency.
DEA licensure or renewal
As oral healthcare providers, we have become more aware of the opioid problem through dental school curriculum, continuing education, and hands-on training. Those of us who prescribe controlled substances are now subject to new opioid training to fulfill the requirements for the Medication Access and Training Expansion (MATE) Act. This training also fulfills the 1-time, 8-hour training needed to apply for or renew the DEA registrations necessary to prescribe Schedule II through V medications.13
The MATE Act offers 2 ways for oral healthcare providers to fulfill the 8-hour training requirement: (1) recent graduation (within 5 years of June 27, 2023) from a dental school with a curriculum that included training on opioid or other substance use disorders or (2) documented completion of 8 hours of approved training on the management of patients with substance use disorders, appropriate use of pain medications, management of pain, brief interventions, referral for substance use disorders, and recognizing risks of opioid use.14,15
FDA-approved naloxone status change
On March 29, 2023, the FDA approved 4-mg naloxone spray (Narcan) for over-the-counter (OTC) nonprescription use.16 Naloxone quickly reverses an overdose by blocking the effects of opioids.17,18 It can restore normal breathing within 2 to 3 minutes in a person whose
breath has slowed or even stopped as a result of opioid overdose. More than 1 dose of naloxone may be required when stronger opioids such as fentanyl are involved. Naloxone is easy to use and light to carry. This change to OTC status allows greater access to the medication, which can help ensure rapid reversal in overdose situations. Dentists should strongly consider including naloxone in their dental emergency kits.19
What can dentists do?
It is important for dentists to realize there is a vast drug culture out there populated by people who will readily use us as prescribers. In addition, we need to accept that even prescribed opioid use can lead to addictions that grow to include drugs like heroin and fentanyl. Dentists need to admit that if we overprescribe opioids for pain, we may be part of the problem. If we do prescribe opioids, we must prescribe low quantities for short periods of time.
We need to know our patients, beware of opioid shoppers, and consider offering nonnarcotic therapy first. By logging into the prescription drug monitoring program in their state (eg, Illinois, www. ilpmp.org), dentists can check the use of their DEA number by viewing the controlled substance prescriptions that they have written. Additionally, we must have confidence in the effectiveness of the nonopioid medicines we prescribe and not be swayed by patients’ requests for “something stronger” before they have tried the nonopioid approach.
In the event of a potential overdose, what should dentists do? Despite knowing the signs, it may be hard to tell if a person is under the influence of drugs or experiencing an overdose. If you are unsure, it is best to be cautious and treat the situation like an overdose; you could save a life. The CDC recommends the following actions20:
• Call 911 immediately.
• Administer naloxone if it is available.
• Try to keep the person awake and breathing.
• Lay the person on their side to prevent choking.
• Stay with the person until emergency workers arrive.
The effects of naloxone are temporary, and more than 1 dose may be required.20
The Substance Abuse and Mental Health Services Administration offers a free toolkit that not only discusses overdose prevention but also offers detailed information on reversal medications and guidance on responding to an overdose.21
In rural and remote areas where emergency services are not readily available, there are often first responders such as public safety officers or community volunteers who have been trained to treat overdoses and have access to naloxone. Remember that so-called Good Samaritan laws are in place in most states to protect overdosing individuals as well as anyone assisting them from arrest or criminal charges.4
If you have questions about how to respond in a potential overdose situation, contact your local health department to get training and save lives.
Author affiliation
Midwestern University College of Dental Medicine-Illinois, Downers Grove.
Conflicts of interest
None reported.
References
1. Health Resources & Services Administration. Opioid crisis. December 2023. Accessed August 8, 2024. https://www. hrsa.gov/opioids
2. Centers for Medicare & Medicaid Services. Ongoing emergencies & disasters. Updated September 10, 2024. Accessed October 1, 2024. https://www.cms.gov/aboutcms/what-we-do/emergency-response/currentemergencies/ongoing-emergencies
3. Opioids. Youth.gov. Accessed August 8, 2024. https:// Youth.gov/youth-topics/substance-abuse/opioids
4. Centers for Disease Control and Prevention. Signs of opioid misuse, opioid use disorder, and overdose. Accessed August 8, 2024. https://www.cdc.gov/ore/pdf/Signs-ofOpioid-Misuse-Opioid-Use-Order-and-Overdose_508.pdf
5. Office of Workers’ Compensation Programs. US Department of Labor. Risk factors for opioid misuse, addiction, and overdose. Accessed August 8, 2024. https://www. dol.gov/agencies/owcp/opioids/riskfactors
6. Drug Enforcement Administration. Facts about fentanyl. Accessed August 8, 2024. https://www.dea.gov/ resources/facts-about-fentanyl
7. Centers for Disease Control and Prevention. Fentanyl Facts. Accessed October 2, 2024. https://www.cdc.gov/ stop-overdose/caring/fentanyl-facts.html
8. Centers for Disease Control and Prevention. What you should know about xylazine. Accessed August 8, 2024. https://www.cdc.gov/overdose-prevention/about/whatyou-should-know-about-xylazine.html
9. Georgia Overdose Prevention. Fatal opioid overdoses are preventable with naloxone. 2024. Accessed August 8, 2024. https://georgiaoverdoseprevention.org
10. Illinois General Assembly. Emergency Medical Services Access Law. Public Act 097-0678. June 1, 2012. Accessed October 1, 2024. https://www.ilga.gov/legislation/publicacts/fulltext.asp?Name=097-0678
If the next opioid overdose happens in your office, will you be ready?
11. Illinois General Assembly. SCH CD-Fentanyl Education. Public Act 103-0810. August 9, 2024. Accessed October 1, 2024. https://www.ilga.gov/legislation/publicacts/fulltext.asp?Name=103-0810
12. Concord Seminars. State CE requirements for dentists. 2024. Accessed October 1, 2024. https://www.concordseminars.com/state-ce-requirements-for-dentists/
13. Substance Abuse and Mental Health Services Administration. Training requirements (MATE Act) resources. Accessed August 8, 2024. https://www.samhsa.gov/ medications-substance-use-disorders/training-requirements-mate-act-resources
14. Academy of General Dentistry. U.S. Drug Enforcement Administration (DEA) Medication Access and Training Expansion (MATE) Requirements. Accessed October 1,
15. US Department of Justice Drug Enforcement Administration. MATE training letter. March 27, 2023. Accessed August 8, 2024. https://www.deadiversion.usdoj.gov/ pubs/docs/MATE_Training_Letter_Final.pdf
16. Food and Drug Administration. FDA approves first overthe-counter naloxone nasal spray. News release. March 29, 2023. Accessed August 8, 2024. https://www.fda.gov/ news-events/press-announcements/fda-approves-firstover-counter-naloxone-nasal-spray
17. National Institute on Drug Abuse. Naloxone drug facts. January 2022. Accessed October 1, 2024. https://nida. nih.gov/publications/drugfacts/naloxone
18. Centers for Disease Control and Prevention. Reversing opioid overdoses with lifesaving naloxone. April 2024.
Accessed October 1, 2024. https://www.cdc.gov/stopoverdose/media/pdfs/2024/04/Naloxone-FactSheet-508.pdf
19. Drahos GL, Williams L. Addressing the emerging public health crisis of narcotic overdose. Gen Dent. 2017;65(5):7-9.
20. Centers for Disease Control and Prevention. How and when to use naloxone for an opioid overdose. April 2024. Accessed October 1, 2024. https://www.cdc.gov/overdose-prevention/media/pdfs/2024/04/FactSheet-Howand-When-to-Use-Naloxone.pdf
21. Substance Abuse and Mental Health Services Administration. SAMHSA Overdose Prevention and Response Toolkit. SAMHSA Publication No. PEP23-03-00-001. Revised January 2024. https://store.samhsa.gov/sites/default/files/ overdose-prevention-response-kit-pep23-03-00-001.pdf
Dentistry’s ethical responsibility to patients’ overall health through sustainable practices and climate change awareness
Toni M. Roucka, RN, DDS, MA
I have had the honor of writing the ethics column for this prestigious journal for more than 10 years. This is my last column as I transition to other personal and professional initiatives. For this last piece, I wanted to focus on a topic that I am passionate about and affects all of us. Thank you sincerely for your loyal readership over the years.
The dental profession is not only about ensuring that the oral cavity is healthy and smiles are bright. As healthcare providers, dentists bear a significant responsibility for their patients’ overall health and well-being. The oral-systemic connection cannot be denied. This responsibility extends beyond the immediate clinical outcomes of oral diagnosis and dental procedures; it includes providers’ duty to consider the long-term impacts of their practice on the environment and public health.1-3
It is undeniable that something is happening to our world’s climate, and it is well known that greenhouse gases from fossil fuels and other human activities are exacerbating the problem. As environmental degradation, plastic waste, and climate change become more widely acknowledged as serious dangers to global health, the dental and healthcare industries must embrace
more sustainable methods for delivering care. This is a duty and an opportunity to make positive change and inspire others to do the same. Sustainability simply aims to meet the needs of the present without compromising the ability of future generations to meet their needs.
The nexus between dentistry, health, and the environment
As do all healthcare providers, dentists operate within an ecosystem where their actions can have far-reaching effects. The materials they choose, the waste they generate, and the energy they consume all contribute to the healthcare sector’s larger environmental footprint. The interconnectedness of dentistry, health, and the environment is not just an idea but a reality that we must be acutely aware of and take responsibility for.
Have you ever visited the grocery store and consciously tried to avoid buying anything wrapped or packaged in some kind of plastic? It’s nearly impossible. The healthcare industry is even worse. Single-use plastics are ubiquitous and used to increase convenience and ensure patient safety through infection control. Plastics have now been found embedded in human tissues, including but not limited to the bloodstream and the brain.4 Since plastics are
man-made, this is a man-made problem. Although the long-term effects of these findings are not known, we must ask: Are we making ourselves sick in the name of safety and convenience?
Plastic waste in the ocean also kills hundreds of thousands of marine mammals and millions of fish and birds every year.5 Our planet’s oceans are central to reducing greenhouse gases and stabilizing the global climate, generating 50% of Earth’s oxygen and absorbing 25% of all carbon dioxide emissions.6 The great Pacific garbage patch, estimated to be 2 times the size of Texas and 3 times the size of France, is located between Japan and California and is composed almost entirely of plastics.7 Plastic is making our oceans sick as well.
Climate change exacerbates health issues such as respiratory, vector-driven, and cardiovascular diseases, which can be linked to environmental factors such as pollution and global warming.8 The healthcare industry annually contributes between 4.4% and 5.2% of greenhouse gas emissions worldwide.9 This is significant.
Environmental health is a branch of public health that focuses on the relationships between people and their environment, promotes human health and well-being, and fosters healthy and safe communities. Our colleagues in this field tell us what we know intuitively: that
people need to live in a clean and healthy environment to thrive and flourish. Flourishing people live a good, fulfilling life with a sense of purpose, unencumbered by unhealthy external factors. They are committed to good mental, physical, and social health in their lives and community. This includes family, work, education, ecosystem, politics, economics, and more. This is a basic human need—for everyone. Our overall health is interconnected with the planet’s health.
Ecological grief is also becoming a public health problem, especially among young people aged 18 to 35. This age group encompasses most of our dental student population and a good portion of our patient population. These young people are fearful for the planet’s health and future, and it’s taking a significant toll on their mental health. One study demonstrated that the majority of participants felt frustrated or embittered by indifference to environmental decline and the inaction of corporations and government agencies regarding climate change.10 Respondents were very worried about the environment, but their ecological grief left them feeling impotent to affect change. The same study found that when participants engaged in collective rather than individual action, they felt some capacity to protect themselves against depression.10 The study shows that when we provide young people with opportunities to engage in collective action, they can experience a restoration of hope. This allows them to identify goals and reclaim a sense of agency and connection on this issue.
In 2023, the American Dental Education Association (ADEA) House of Delegates passed resolution 4H-2023, Climate Change and Implications for Health, Oral Health, and Oral Health Education, acknowledging our responsibility to train future oral health professionals in sustainable practice.11 Putting words into action, ADEA has a new Special Interest Group (SIG) on
Sustainability in Dentistry. This growing SIG brings together like-minded faculty and staff to exchange ideas on best practices for including sustainability content in the curriculum and reducing waste in clinical operations while maintaining patient safety. Therefore, dental schools are beginning to incorporate sustainable dentistry education into the curriculum to teach students to make informed decisions for their future practices. Many universities are creating climate action plans to identify and implement sustainable solutions that decrease waste and energy consumption and educate future leaders on these issues.
Patients are becoming more knowledgeable about climate change and plastic waste issues as well. Incorporating sustainable practices into the office can be a practice builder, but most importantly, as stewards of health, dentists have an ethical responsibility to mitigate their contribution to environmental harm.
Touchpoints of sustainability in dental care
Sustainability is impacted at many levels along the dental care continuum. It begins with how raw materials used to make dental products are sourced. From there, manufacturing processes are a factor, particularly those that create plastic (a fossil fuel derivative). Packaging and distribution then play a role. Procurement is next, which then leads to actual patient care. When considering the environmental impact of patient care, we must also consider the transportation that patients, dental staff, and dentists take to and from the office. Transportation is the most significant contributor to greenhouse gas emissions in this continuum. Finally, waste management comes into play (Figure).
As you can see, the subject is complicated. However, the opportunities for increased sustainability are present at every level. More action is needed at each touchpoint in the process to make
a significant difference in greenhouse gas emissions in the long term. This includes the need for continued research on more sustainable dental materials, manufacturing processes, and packaging options. While the issue of climate change can seem overwhelming, if everyone makes small changes where they can, the impact will be magnified and make a real difference.
Making change now
The American Dental Association has excellent resources regarding sustainability in dental practice that are worth reviewing.12 If you are planning a building or remodeling project for your home or office, consider LEED (Leadership in Energy and Environmental Design).13 LEED aims to provide a framework for healthy, highly efficient, and cost-saving green buildings that offer environmental, social, and governance benefits. Below are some additional ideas for implementing eco-friendly options at each level of the sustainability continuum.
Materials and sourcing
Dentists can use eco-friendly and biocompatible materials such as non-BPA–containing resins; ceramics; autoclavable suction tips; cloth patient bibs and sterilization cassette wraps; metal bib clips; and bulk delivery systems (as opposed to unit doses), just to name a few. These items have a lower environmental impact than other choices. Prioritizing suppliers that utilize eco-friendly and fair-trade practices and offer sustainable options, such as recyclable packaging, can help reduce a practice’s carbon footprint.
Manufacturing
Dental practices can support reputable manufacturers that utilize environmentally sound practices. By opting for products made from renewable resources or those that have a smaller environmental impact during production (eg, less
Figure. The sustainability continuum in dentistry. Materials and sourcing Manufacturing
Packaging and distribution Procurement Patient care
management
plastic), dentists can encourage industry leaders to continue developing and refining greener manufacturing processes. More research and development are needed in this area.
Packaging and distribution
Practices can reduce waste by selecting suppliers that use minimal, recyclable, or biodegradable packaging. Supporting local suppliers can also reduce the carbon footprint associated with transportation.
Procurement
Dentists should establish procurement policies prioritizing sustainability, such as buying in bulk to reduce packaging waste. Additionally, consolidating orders to reduce the frequency of shipments can lower the carbon emissions associated with transportation.
Patient care
Dentists can promote preventive care and patient education to reduce the need for resource-intensive treatments. Thoughtful treatment planning processes also decrease the practice’s carbon footprint by maximizing patient care procedures at each appointment and decreasing patient transportation costs to and from the office. Training staff members to prepare carefully for each procedure limits the number of times they need to change personal protective equipment during appointments to run and get something. Overuse of disposable items leads to large amounts of medical waste, much of which ends up in landfills or the oceans. Using digital records and radiographs cuts down on waste. Opting for nontoxic and sustainable dental products and encouraging patients to choose eco-friendly dental care products at home are other ways to align patient care with environmental sustainability.
Energy consumption is another significant aspect of a dental practice’s environmental footprint. Dental equipment, lighting, heating, and cooling all require energy, which may come from nonrenewable sources, contributing to greenhouse gas emissions. One way to address this is to invest in energyefficient equipment when there is a
choice. Additionally, switching to LED lighting and optimizing the use of natural light can reduce energy consumption. Dentists can also consider installing renewable energy sources, such as solar panels or geothermal heating and cooling, to power their practices. While the upfront costs may be significant, the long-term benefits to the environment and the practice’s operating costs can be substantial.
Water conservation is another critical area where dentists can make a difference. Whether for patient care, rinsing and sterilizing instruments, or general cleaning, dental practices consume substantial amounts of water daily. Watersaving technologies and practices can help reduce this consumption, contributing to a more sustainable operation. Consider a dry vacuum instead of a wet vacuum system, for example.
Waste management
There are many opportunities to explore reducing overall waste generation through careful resource management. Implementing strict recycling protocols and minimizing single-use plastics and other materials can significantly reduce the waste a dental practice generates. Dental providers should also properly dispose of hazardous waste, such as biohazards, amalgam, and sharps, to prevent environmental contamination. It is important to be familiar with the local community’s recycling program opportunities, as these programs vary widely across the United States. Many dental suppliers also offer recycling programs.
Conclusion
Dentists’ ethical responsibility extends beyond the dental chair. As healthcare providers, dentists must consider the broader impact of their practices on their patients’ overall health and well-being, including the health of the environment and the mitigation of climate change, often described as the greatest public health challenge of the 21st century. By adopting sustainable practices, conserving resources, and reducing their environmental footprint, dentists can help protect public health in the face of climate change.
While transitioning to more sustainable practices may present challenges, the long-term environmental and public health benefits are clear. By embracing sustainability, dentists can fulfill their ethical obligations to their patients and contribute to a healthier, more sustainable future for all. Our choices today will shape the health of our patients, communities, and the planet for generations to come.
Author affiliation
Marquette University School of Dentistry, Milwaukee, Wisconsin.
Conflicts of interest
None reported.
References
1. Sustainability in dentistry. FDI World Dental Federation. 2024. Accessed August 26, 2024. https://www.fdiworlddental.org/sustainability-dentistry
2. Roucka T. Does dentistry have an ethical obligation to be more sustainable? Gen Dent. 2020;68(2):22-24.
3. American College of Dentists. Ethics Handbook for Dentistry. 2024. Accessed August 26, 2024. https://www. dentalethics.org/resources/ethics-handbook-for-dentistry/
4. Balch B. Microplastics are inside us all. What does that mean for our health? AAMC News. June 27, 2024. Accessed August 26, 2024. https://www.aamc.org/news/ microplastics-are-inside-us-all-what-does-mean-ourhealth
6. The ocean–the world’s greatest ally against climate change. United Nations Climate Action. Accessed August 26, 2024. https://www.un.org/en/climatechange/ science/climate-issues/ocean
7. Adkins F. Visualising the great pacific garbage patch. BBC. January 16, 2024. Accessed August 26, 2024. https:// www.bbc.com/future/article/20240115-visualising-thegreat-pacific-garbage-patch
8. Centers for Disease Control and Prevention. Impact of climate change on human health. U.S. Climate Resilience Toolkit. November 16, 2016. Accessed August 26, 2024. https://toolkit.climate.gov/image/505
9. Dutchen S. Confronting health care’s carbon footprint. Harvard Medicine. Autumn 2023. Accessed August 26, 2024. https://magazine.hms.harvard.edu/articles/ confronting-health-cares-carbon-footprint
10. Schwartz SE, Benoit L, Clayton S, Parnes MF, Swenson L, Lowe SR. Climate change anxiety and mental health: environmental activism as a buffer. Curr Psychol. 2022;1-14. doi:10.1007/s12144-022-02735-6
11. ADEA Reference Committee on Association Policy report. American Dental Education Association. March 12, 2023. Accessed September 11, 2024. https://www.adea.org/ WorkArea/DownloadAsset.aspx?id=46001
12. 80 ways to make your dental practice green. American Dental Association. Accessed September 11, 2024. https://www.ada.org/resources/practice/practicemanagement/office-design/80-ways-to-make-yourdental-practice-green
13. LEED rating system. U.S. Green Building Council. Accessed September 11, 2024. https://www.usgbc.org/leed
Evaluation of single-step self-etching ceramic primer and zirconia primer for bonding to zirconia-reinforced lithium silicate ceramic
The purpose of this study was to evaluate the influence of simplified ceramic surface treatments on the microshear bond strength (µSBS) of 2 resin cements to a zirconiareinforced lithium silicate (ZLS) material. Blocks of ZLS were sectioned to obtain a total of 90 specimens (1.5 mm thick), which were assigned to 9 different surface treatment protocols (n = 10). Either hydrofluoric acid (HF) surface conditioner or ammonium polyfluoride self-etching ceramic primer (Monobond Etch & Prime [MEP]) was used for surface treatment and then combined with different bonding strategies (Monobond N silane-based universal primer, Prosil silane coupling agent, Ambar Universal APS self-etching adhesive, and/or Signum Zirconia Bond methyl methacrylate–based bonding system [SZB]) and luting agents (Allcem or Multilink Automix dual-curing resin cement). Composite resin cylinders were bonded to ZLS with each of the cementation protocols, and the specimens were subjected to 6000 thermal cycles from 5°C to 55°C prior to the µSBS evaluation. The failure mode was analyzed with the aid of a stereoscopic loupe. Statistical analyses were performed with 1-way analysis of variance and Tukey HSD test (α = 0.05). The HF and MEP protocols resulted in significantly higher µSBS values (P < 0.001), while conditioning with SZB resulted in the lowest µSBS. Multilink Automix groups presented higher µSBS values than Allcem groups (P < 0.01). There was no statistically significant difference in the µSBS values of the MEP + Allcem groups based on whether or not an adhesive layer was applied. The failure mode was predominantly adhesive for all specimens. The results indicate that the ammonium polyfluoride–based material MEP may be used as a substitute for surface treatment with HF and silane, but the use of a zirconia primer alone is not advised for bonding to a ZLS ceramic material.
Monolithic zirconia-reinforced lithium silicate (ZLS) blocks intended for computer-aided design/ computer-aided manufacturing (CAD/CAM) purportedly combine the excellent optical properties of vitreous ceramics with reinforcement by zirconia particles, which are known for their good mechanical properties.1 Structurally, ZLS blocks are composed of lithium metasilicate and zirconium dioxide and are thus properly indicated for both anterior and posterior restorations.2 In addition to these characteristics, ZLS is an acid-sensitive ceramic due to its predominantly vitreous content, with 8% to 15% zirconia in its composition.3,4 Improvements in the chemical compositions of ceramics and the faster processing techniques available are accompanied by the need to ensure effective cementation protocols. Shortened and simplified clinical protocols that use ammonium polyfluoride–based materials, such as Monobond Etch & Prime (MEP; Ivoclar Vivadent), may save time by requiring fewer steps, focusing on the adhesive interactions among the ceramic, dental substrate, and luting agents.5
The reaction that takes place between hydrofluoric acid (HF) and the silica present in the glassy matrix of conditioned ceramic systems has been used to modify ceramic surfaces since the introduction of feldspathic ceramics. Application of HF results in a topographic alteration of the surface that promotes micromechanical retention of the luting agent. However, adequate HF concentration and etching time are important criteria for surface conditioning and may vary according to the percentage of the vitreous phase of the ceramic. Problems associated with an overconditioned surface also may have negative effects on the mechanical properties of the ceramic material, and HF exposure may have toxic systemic effects.6,7
Alternative materials are being studied to provide shortened clinical protocols for ceramic surface conditioning. Among these is the single-step, self-etching ceramic primer MEP, which is marketed as a substitute for HF and silane surface treatment. Such a material could offer a significant reduction in time during the cementation procedure in comparison with the conventional HF + silane + adhesive approach. In addition to the user-friendly protocol and minimization of steps, this material also reduces the potential toxic effects associated with HF.8
Further simplification protocols could in theory also be performed for ZLS, taking advantage of the 8% to 15% zirconia present in its composition. For instance, the use of zirconia
Material Code Type
Ambar Universal APS (FGM Dental Group)
Allcem (FGM Dental Group)
AU Self-etching adhesive
AC Dual-curing resin cement
Celtra Duo (Dentsply Sirona)
Signum Zirconia Bond (Kulzer)
Prosil (FGM Dental Group)
Condac Porcelana 10% (FGM Dental Group)
Monobond Etch & Prime (Ivoclar Vivadent)
Multilink Automix (Ivoclar Vivadent)
Monobond N (Ivoclar Vivadent)
ZLS
SZB
Zirconia-reinforced lithium silicate
Bonding system
S Silane coupling agent
HF
Hydrofluoric acid surface conditioner
MEP Self-etching ceramic primer
MA Dual-curing resin cement
MN Silane-based universal primer
Composition
Active ingredients: 10-methacryloxydecyl dihydrogen phosphate, methacrylic monomers, photoinitiators, coinitiators, stabilizers
primers such as Signum Zirconia Bond (Kulzer) and universal adhesives based on 10-methacryloxydecyl dihydrogen phosphate (10-MDP) is reported to have a positive effect on adhesion to conventional zirconia materials, as it is known that functional monomers are necessary for chemical bonding with polycrystalline materials.9-11
Thus, the aim of the present study was to evaluate the effects of different simplified surface treatment protocols on the bond strength between 2 resin cements and a ZLS ceramic. The study hypotheses were that (1) MEP alone could substitute for traditional bonding protocols with HF and silane; and (2) Signum Zirconia Bond (SZB; Kulzer) alone could substitute for traditional bonding protocols with HF and silane.
Methods
The materials tested in this study are described in Table 1. All materials were applied according to the manufacturer’s instructions.
Specimen preparation
ZLS blocks (Celtra Duo, Dentsply Sirona) were sectioned in a cutting machine (IsoMet 1000 Low Speed saw, Buehler) with a diamond disc (IsoMet 15LC diamond blade, No. 11-4254, Buehler) at a speed of 300 rpm under constant water cooling
to obtain 1.5-mm-thick slices. The slices were polished with 800-, 1000-, and 1200-grit sandpaper (K2000 polishing papers, Exakt Technologies) on a metallographic polishing machine (Exakt 400CS, Exakt Technologies) to standardize the ceramic surfaces. These slices were then cut into 4 equal parts with a diamond disc (Mono Face 7010, KG Sorensen) under constant water cooling. All specimens were sintered at a temperature of 840°C for 8 minutes in a ceramic oven (Programat P510, Ivoclar Vivadent), in accordance with the manufacturer’s protocol.
Composite resin cylinders (Vittra APS, FGM) were formed in surgical catheters with an internal diameter of 1.4 mm and 1.0-mm height. The material was cured with an LED device (VALO Cordless, Ultradent) operated in standard mode with an irradiance of 1000 mW/cm2. Ten minutes after light activation, the surgical catheters were removed with a No. 11 scalpel blade to expose the composite resin cylinders.
Surface treatment
After sintering, the specimens were randomly divided into 9 groups (n = 10), and the surface treatment protocol corresponding to each group was carried out according to the guidelines of each manufacturer (Table 2). The group treated with the conventional HF + silane + adhesive approach was designated as the control group.
Table 1. Composition of materials used in the study.
Group Surface treatment
HF + S + AU + AC Hydrofluoric acid + silane + Ambar Universal APS + Allcem
MEP + AU + AC Monobond Etch & Prime + Ambar Universal APS + Allcem
MEP + AC Monobond Etch & Prime + Allcem
SZB + AC Signum Zirconia Bond + Allcem
MEP + SZB + AC Monobond Etch & Prime + Signum Zirconia Bond + Allcem
HF + S + SZB + AC Hydrofluoric acid + silane + Signum Zirconia Bond + Allcem
MEP + MA Monobond Etch & Prime + Multilink Automix
MEP + MN + MA Monobond Etch & Prime + Monobond N + Multilink Automix
HF + MN + MA Hydrofluoric acid + Monobond N + Multilink Automix
In the groups conditioned with HF, Condac Porcelana 10% (FGM Dental Group) was applied for 20 seconds and then removed with copious water spray applied for 60 seconds. In the MEP groups, MEP was actively applied with a microbrush for 20 seconds and allowed to react on the surface for another 40 seconds. The product was then removed with copious air and water spray for 10 seconds.
After surface treatment, all ceramic surfaces received application of adhesive, silane (Prosil, FGM Dental Group), and/or zirconia primer. Subsequently, the resin cements were used to cement the ceramic to the composite resin cylinder.
Cementation and thermocycling
For each group, 1 of 2 resin cements, Allcem Dual (FGM Dental Group) or Multilink Automix (Ivoclar Vivadent), was used according to the manufacturer’s specifications to cement composite resin cylinders to the previously conditioned ceramic surfaces. In an attempt to simulate a realistic clinical scenario, a device was used to light activate the cement through the ceramics, as previously described.12 After removal of the excess cement with a brush, light activation was carried out using an LED device with an irradiance of 1000 mW/cm2.
After cementation, the specimens were stored for 48 hours in deionized water. Subsequently, all specimens were aged before bond strength testing by undergoing 6000 thermal cycles (5°C to 55°C) with a dwell time of 30 seconds at each temperature.
Bond strength evaluation
After thermocycling was completed, the microshear bond strength (μSBS) was evaluated on a universal testing machine (No. 3342, Instron). A 0.2-mm wire loop device was used to apply shear stress as close as possible to the bonding interface at a crosshead speed of 0.5 mm/min until fracture. The force measurement during the test was performed through a load
Table 3. Mean (SD) microshear bond strength of zirconia-reinforced lithium silicate ceramic to composite resin (n = 10 per group).
cell with a capacity of 50 kg (500 N). The bond strength was expressed in megapascals by dividing the maximum force in newtons by the bonding area in square millimeters.
After the μSBS evaluation, the surfaces of the specimens were analyzed with the aid of a stereoscopic loupe to determine the type of failure involved. The failures were classified as adhesive, cohesive, or mixed.
Statistical analysis
After verification of the normality and homogeneity of variance, data were analyzed using 1-way analysis of variance and the Tukey HSD test. The significance level was set at α = 0.05.
Results
There were statistically significant differences (P < 0.001) between groups in the (mean [SD]) bond strength values (Table 3; see Table 2 for definition of the groups). Multilink Automix groups presented higher µSBS values than Allcem groups (P < 0.01). The group that did not use HF treatment, MEP + MN + MA (29.5 [10.0] MPa), showed the highest µSBS and did not statistically differ from group HF + MN + MA (27.7 [5.3] MPa), which used conventional surface treatment with HF and silane-based universal primer. The application of SZB alone yielded the lowest µSBS. However, µSBS values similar to that of the HF + S + AU + AC control group (12.7 [6.1] MPa) were obtained when SZB was applied after MEP (8.6 [5.7] MPa) or after HF and silane (15.8 [7.3] MPa). Application of universal adhesive after MEP and before the resin cement Allcem (MEP + AU + AC) showed no statistical difference in µSBS when compared with MEP + AC.
Five pretesting failures were observed in the SZB + AC group and were considered as 0.0 MPa in the statistical analyses. The failure mode was predominantly adhesive in all groups.
Table 2. Groups and surface treatment protocols.
Discussion
The first hypothesis, that the µSBS of the simplified surface treatment with MEP could substitute for conventional HF and silane surface treatment, was not rejected. Groups that used the ammonium polyfluoride self-etching ceramic primer MEP showed mean µSBS values that did not differ from those that used HF and silane treatment, regardless of whether a 10-MDP bonding agent was applied.
In contrast, the hypothesis that SZB alone could substitute for the conventional bonding protocol with HF and silane was rejected, as a mean µSBS value close to 0.0 MPa was observed for the group SZB + AC. The protocols using the universal adhesive and SZB (groups HF + S + AU + AC; MEP + AU + AC; SZB + AC; MEP + SZB + AC; and HF + S + SZB + AC) aimed to provide bond strength through a possible interaction of the functional monomer 10-MDP with the polycrystalline part of the ZLS block. Previous studies have reported the chemical interaction of 10-MDP with yttria-stabilized tetragonal zirconia polycrystalline (Y-TZP) is well known.11,13,14 However, 10-MDP does not appear to interact in the same way with ZLS, possibly due to the higher amount of vitreous matrix in the composition of the ZLS block.
The mechanism by which HF acts on ceramic surfaces is detailed in the literature.15,16 HF reacts with silica and eliminates it selectively, thus achieving exposure of the ceramic crystalline structure. After the surface topography is modified, ceramics can be functionalized with silane and infiltrated with the bonding material.17,18 Nonetheless, the literature reports that use of conventional HF acid agents has detrimental effects, including high toxicity, corrosive potential, possible burns on skin contact, possible absorption into the bloodstream through interaction with skin and bone tissue, and irreversible damage if there is eye contact.7,19 In addition to the sensitivity of the technique, HF may also be detrimental to the mechanical properties of the material, with the effects depending on the acid agent concentration and the time of action on the ceramic surface.20-22
Although application of a bonding agent after silanization and prior to application of the resin cement is recommended, the μSBS results in the HF + MN + MA group suggest that the resin cement could be applied immediately after the application of the silane-based universal primer.15,17,22 This issue, however, demands further study.
The results of the present study suggest that MEP could be used as an alternative surface treatment to minimize the problems associated with HF technique sensitivity. MEP combines ammonium polyfluoride, which is a less aggressive acid agent, and silane (trimethoxypropyl methacrylate) in a single bottle, thus reducing the number of steps and the clinical time used in the conventional technique (HF + S).23,24 There are still few reports in the literature on the association of MEP and ZLS ceramics.16,25,26 Some studies have found encouraging results regarding the association of MEP with other ceramic materials and are in agreement with the results of the present study. Prado et al compared an HF + S protocol with MEP and concluded that there was no significant difference in the results produced by the 2 surface treatments on either lithium disilicate or feldspathic ceramic and that MEP specimens showed a more durable bond strength after aging
by thermocycling.26 El-Damanhoury and Gaintantzopoulou also concluded that MEP is efficient and its effects are material dependent, showing higher bond strength on IPS e.max CAD and Vita Enamic ceramics.25 Furthermore, Wille et al showed no significant differences in microtensile bond strengths obtained with the conventional method (HF + S) vs MEP on lithium disilicate.27
There are a few points about the methods employed in the present study that should be addressed. The cementation procedure was conducted indirectly, with the interposition of the ceramic thickness (1.5 mm) between the light source and the resin cement. For this purpose, a device containing an orange filter with a central hole of 2.0 mm in diameter was used to standardize the position of both the ceramic slice and the LED device underneath it, ensuring that polymerization of the resins occurred only through the ceramics.12 This approach simulated clinical conditions, where light activation of the resin cement occurs through the ceramic restoration. During preparation of the specimens, after the excess resin cement around the composite resin cylinders was removed, the tip of the LED device was positioned 2 mm below the ceramic slice so the light could pass through it. It is known that the presence of a ceramic material between the light source and the resin cement has the effect of decreasing the degree of conversion and the hardness of the resin agent.28,29
The study design also included a thermal aging protocol to age the adhesive interface 24 hours after the cementation procedure. The time of water storage seems to affect the bond strength produced by different surface treatment protocols, and exposure of the adhesive interface to an aggressive method is intended to simulate the conditions of the oral cavity. 30 Correct and sufficient exposure is necessary to achieve saturation of water for composite resin or resin cement; in the present study, 6000 thermocycles were programmed from 5°C to 55°C.
Since this study was designed to evaluate the bond strength resulting from different bonding strategies without the interference of surface roughness as a variable, specimens were polished with up to 1200-grit sandpaper. No sandblasting or other mechanical surface treatment was conducted. However, ZLS blocks are processed through milling with diamond burs in a CAD/CAM device. Thus, in a clinical scenario, higher bond strength values could be expected due to the increased roughness of the ceramic surface.
Pretesting failures were observed for the group SZB + AC, which did not receive any form of etching and relied only on the chemical interaction of the 10-MDP present in SZB and the polycrystalline content of ZLS. Therefore, it can be concluded that SZB alone did not interact well with the ceramic surface.
Future studies are necessary to characterize the chemical interactions on surfaces conditioned with the simplified MEP protocol as well as to understand interactions among MEP, different adhesives and primers, different types of resin cements, and other commercially available ceramics. Additional studies should also be performed to address the influences of different light activation devices, long-term water storage, longer thermocycling periods, and different mechanical stresses to assess the longevity of MEP.
Evaluation
Conclusion
A conventional pretreatment protocol with HF and silane and a shortened protocol with MEP seem to be equally effective in providing high bond strength to ZLS.
Author affiliations
Department of Operative Dentistry, Endodontics and Dental Materials, Bauru School of Dentistry, University of São Paulo, Bauru, Brazil (Icochea, Fernandes-Neto, Mondelli, Furuse); Department of Pediatric Dentistry, Bauru School of Dentistry, University of São Paulo, Bauru, Brazil (Bisaia); Department of Oral Rehabilitation, Medical University of South Carolina, Charleston (Rizzante).
1. Elsaka SE, Elnaghy AM. Mechanical properties of zirconia reinforced lithium silicate glassceramic. Dent Mater. 2016;32(7):908-914. doi:10.1016/j.dental.2016.03.013
2. Traini T, Sinjari B, Pascetta R, et al. The zirconia-reinforced lithium silicate ceramic: lights and shadows of a new material. Dent Mater J. 2016;35(5):748-755. doi:10.4012/dmj.2016-041
3. Bömicke W, Rammelsberg P, Krisam J, Rues S. The effects of surface conditioning and aging on the bond strength between composite cement and zirconia-reinforced lithium-silicate glass-ceramics. J Adhes Dent. 2019;21(6):567-576. doi:10.3290/j.jad.a43650
4. Barchetta NF, Amaral M, Prochnow C, et al. Strength of a zirconia-reinforced lithium silicate ceramic: acid-etching time and resin cement application effects. Int J Periodontics Restorative Dent. 2019;39(3):431-437. doi:10.11607/prd.4117
5. Silva LHD, Lima E, Miranda RBP, Favero SS, Lohbauer U, Cesar PF. Dental ceramics: a review of new materials and processing methods. Braz Oral Res. 2017;31(Suppl 1):e58. doi:10.1590/1807-3107BOR-2017.vol31.0058
6. Hoffmann S, Parikh P, Bohnenberger K. Dermal hydrofluoric acid toxicity case review: looks can be deceiving. J Emerg Nurs. 2021;47(1):28-32. doi:10.1016/j.jen.2020.08.005
7. Ozcan M, Allahbeickaraghi A, Dündar M. Possible hazardous effects of hydrofluoric acid and recommendations for treatment approach: a review. Clin Oral Investig. 2012;16(1):15-23. doi:10.1007/s00784-011-0636-6
8. Maier E, Bordihn V, Belli R, et al. New approaches in bonding to glass-ceramic: self-etch glass-ceramic primer and universal adhesives. J Adhes Dent. 2019;21(3):209-217. doi:10.3290/j.jad.a42546
9. Nagaoka N, Yoshihara K, Feitosa VP, et al. Chemical interaction mechanism of 10-MDP with zirconia. Sci Rep. 2017;7:45563. doi:10.1038/srep45563
10. Hanabusa M, Yoshihara K, Yoshida Y, et al. Interference of functional monomers with polymerization efficiency of adhesives. Eur J Oral Sci. 2016;124(2):204-209. doi:10.1111/ eos.12245
11. Llerena-Icochea AE, Costa RM, Borges A, Bombonatti J, Furuse AY. Bonding polycrystalline zirconia with 10-MDP-containing adhesives. Oper Dent. 2017;42(3):335-341. doi:10.2341/16-156-L
12. Mezarina-Kanashiro FN, Bronze-Uhle ES, Rizzante FAP, Lisboa-Filho PN, Borges AFS, Furuse AY. A new technique for incorporation of TiO2 nanotubes on a pre-sintered Y-TZP and
its effect on bond strength as compared to conventional air-borne particle abrasion and silicatization TiO2 nanotubes application on pre-sintered Y-TZP. Dent Mater. 2022;38(8):e220e230. doi:10.1016/j.dental.2022.06.015
13. Yoshida K, Tsuo Y, Atsuta M. Bonding of dual-cured resin cement to zirconia ceramic using phosphate acid ester monomer and zirconate coupler. J Biomed Mater Res B Appl Biomater. 2006;77(1):28-33. doi:10.1002/jbm.b.30424
14. Ozcan M, Nijhuis H, Valandro LF. Effect of various surface conditioning methods on the adhesion of dual-cure resin cement with MDP functional monomer to zirconia after thermal aging. Dent Mater J. 2008;27(1):99-104.
15. Prochnow C, Venturini AB, Grasel R, Gundel A, Bottino MC, Valandro LF. Adhesion to a lithium disilicate glass ceramic etched with hydrofluoric acid at distinct concentrations. Braz Dent J. 2018;29(5):492-499. doi:10.1590/0103-6440201802080
16. Vichi A, Fabian Fonzar R, Carrabba M, et al. Comparison between hydrofluoric acid and single-component primer as conditioners on resin cement adhesion to lithium silicate and lithium disilicate glass ceramics. Materials (Basel). 2021;14(22):6776. doi:10.3390/ ma14226776
17. Baratto SS, Spina DR, Gonzaga CC, et al. Silanated surface treatment: effects on the bond strength to lithium disilicate glass-ceramic. Braz Dent J. 2015;26(5):474-477. doi:10.1590/0103-6440201300354
18. Tian T, Tsoi JK, Matinlinna JP, Burrow MF. Aspects of bonding between resin luting cements and glass ceramic materials. Dent Mater. 2014;30(7):e147-e162. doi:10.1016/j. dental.2014.01.017
19. Blatz MB, Sadan A, Kern M. Resin-ceramic bonding: a review of the literature. J Prosthet Dent. 2003;89(3):268-274. doi:10.1067/mpr.2003.50
20. Menees TS, Lawson NC, Beck PR, Burgess JO. Influence of particle abrasion or hydrofluoric acid etching on lithium disilicate flexural strength. J Prosthet Dent. 2014;112(5):1164-1170. doi:10.1016/j.prosdent.2014.04.021
21. Zogheib LV, Bona AD, Kimpara ET, McCabe JF. Effect of hydrofluoric acid etching duration on the roughness and flexural strength of a lithium disilicate-based glass ceramic. Braz Dent J. 2011;22(1):45-50. doi:10.1590/s0103-64402011000100008
22. Hooshmand T, Parvizi S, Keshvad A. Effect of surface acid etching on the biaxial flexural strength of two hot-pressed glass ceramics. J Prosthodont. 2008;17(5):415-419. doi:10.1111/j.1532-849X.2008.00319.x
23. Román-Rodríguez JL, Perez-Barquero JA, Gonzalez-Angulo E, Fons-Font A, Bustos-Salvador JL. Bonding to silicate ceramics: conventional technique compared with a simplified technique. J Clin Exp Dent. 2017;9(3):e384-e386. doi:10.4317/jced.53570
24. Dapieve KS, Machry RV, Pilecco RO, et al. One-step ceramic primer as surface conditioner: effect on the load-bearing capacity under fatigue of bonded lithium disilicate ceramic simplified restorations. J Mech Behav Biomed Mater. 2020;104:103686. doi:10.1016/j. jmbbm.2020.103686
25. El-Damanhoury HM, Gaintantzopoulou MD. Self-etching ceramic primer versus hydrofluoric acid etching: etching efficacy and bonding performance. J Prosthodont Res. 2018;62(1):7583. doi:10.1016/j.jpor.2017.06.002
26. Prado M, Prochnow C, Marchionatti AME, Baldissara P, Valandro LF, Wandscher VF. Ceramic surface treatment with a single-component primer: resin adhesion to glass ceramics. J Adhes Dent. 2018;20(2):99-105. doi:10.3290/j.jad.a40303
27. Wille S, Lehmann F, Kern M. Durability of resin bonding to lithium disilicate and zirconia ceramic using a self-etching primer. J Adhes Dent. 2017;19(6):491-496. doi:10.3290/j.jad. a39545
28. Calgaro PA, Furuse AY, Correr GM, Ornaghi BP, Gonzaga CC. Influence of the interposition of ceramic spacers on the degree of conversion and the hardness of resin cements. Braz Oral Res. 2013;27(5):403-409. doi:10.1590/S1806-83242013000500004
29. Watanabe H, Kazama R, Asai T, et al. Efficiency of dual-cured resin cement polymerization induced by high-intensity LED curing units through ceramic material. Oper Dent. 2015;40(2):153-162. doi:10.2341/13-357-L
30. Morresi AL, D’Amario M, Capogreco M, et al. Thermal cycling for restorative materials: does a standardized protocol exist in laboratory testing? A literature review. J Mech Behav Biomed Mater. 2014;29:295-308. doi:10.1016/j.jmbbm.2013.09.013
GENERAL DENTISTRY SELF-INSTRUCTION
Exercise No. GD536, 2 CE Credits
Basic Science
Subject Code: 010
The 15 questions for this exercise are based on the article “Evaluation of single-step self-etching ceramic primer and zirconia primer for bonding to zirconia-reinforced lithium silicate ceramic” on pages 20-24. This exercise was developed by Jeffery B. Price, DDS, MS, MAGD, FICD, FACD, in association with the General Dentistry SelfInstruction committee.
1. Zirconia particles are mixed into lithium silicate ceramics to _____________.
A. provide additional strength
B. enhance cement adherence
C. improve gingival health
D. ensure greater patient acceptance
2. Which is the preferred location in the oral cavity for the use of zirconia-reinforced lithium silicate (ZLS) restorations?
A. anterior only
B. posterior only
C. anterior or posterior
D. neither location
3. Hydrofluoric acid (HF) is the preferred chemical for treating the zirconia substrate in ZLS restorations. The use of Monobond Etch & Prime (MEP) is expected to result in longer treatment protocols.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
4. MEP is marketed for which of the following bonding uses in restorative dentistry?
A. direct composite restorations
B. direct amalgam restorations
C. indirect ZLS restorations
D. indirect porcelain-fused-to-metal restorations
5. Which of the following is a study hypothesis?
A. To evaluate different surface treatment protocols on the bond strengths of 2 cements
B. MEP alone could substitute for traditional bonding protocols with HF and silane
C. Signum Zirconia Bond (SZB) alone could not substitute for traditional bonding protocols with HF and silane
D. To study bonding of resin cements to zirconia crowns under different clinical conditions
Reading the article and successfully completing this exercise will enable you to:
• understand the basics of bonding to zirconia-based ceramics;
• describe the differences between hydrofluoric acid and ammonium polyfluoride primers; and
• discuss the rationale for selection of an appropriate cementation protocol for use with zirconiabased crowns.
Answers must be submitted online at agd.org/self-instruction by October 31, 2025.
6. During testing preparation, the ZLS blocks were cut into ___-mm-thick slices for testing.
A. 0.5
B. 1.0
C. 1.5
D. 2.0
7. The irradiance energy of the LED curing wand was _____ mW/cm2.
A. 750
B. 1000
C. 1250
D. 1500
8. The specimens were divided into 9 groups of 10 specimens each. In the HF groups, HF was applied for 60 seconds and then removed with a 20-second water spray.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
9. The total application and surface cleansing time for the MEP group was ___ seconds.
A. 10
B. 20
C. 40
D. 70
10. The specimens were aged before the bond strength test by undergoing _____ thermal cycles with a dwell time of ___ seconds at each temperature.
A. 1000; 10
B. 2500; 25
C. 6000; 30
D. 7500; 55
11. All of the following are possible types of bonding failure except one. Which is the exception?
A. porosity
B. adhesive
C. mixed
D. cohesive
12. The statistical tests used to analyze the data were ___________.
A. paired t test and 2-way analysis of variance (ANOVA)
B. linear regression and 1-way ANOVA
C. 2-way ANOVA and Tukey HSD test
D. 1-way ANOVA and Tukey HSD test
13. Which of the following combinations of surface treatment protocols provided the 2 highest bond strengths?
A. MEP + MN + MA and HF + MN + MA
B. MEP + MN + MA and MEP + MA
C. HF + MN + MA and MEP + MA
D. SZB + AC and MEP + SZB + AC
14. Which of the following combinations of surface treatment protocols provided the weakest bond strength?
A. MEP + AC
B. SZB + AC
C. MEP + MA
D. MEP + SZB + AC
15. Bonding failure was predominantly ________.
A. homogenous
B. adhesive
C. mixed
D. cohesive
Refer a Colleague, Get Rewarded
AGD Referral Rewards Program
Refer your colleagues to join AGD now for 2025, and they’ll get the rest of 2024 for free.
You’ll both also earn $50 in Referral Rewards once they join!
Learn More agd.org/member-center
“AGD has been pivotal in shaping my career through their quality education and relationships amongst the members. I wouldn’t be where I am today without the AGD!”
Amanda Sonntag, DDS, MAGD Wyomissing, PA
Member Since 2014
Shear bond strength of resin cement to a CAD/CAM millable alloy subjected to various surface treatments
Resin cements are widely used to cement dental restorations; however, limited studies are available on the bond strength of these cements to computer-aided design/computer-aided manufacturing (CAD/CAM) base metal alloys. This study compared the shear bond strength between a self-etching resin cement (Panavia F 2.0) and a millable cobalt-chromium alloy (Ceramill Sintron) following various surface treatments. A total of 40 cylindrical alloy cores (6 mm in diameter × 8 mm in height) were milled and assigned to 1 of 5 groups for different surface treatments (n = 8): control (no surface treatment); sandblasting; metal primer; sandblasting + metal primer; or acid etching. Resin cement was then used to bond cylindrical composite resin specimens to the pretreated core surfaces. The specimens underwent a 1500-cycle thermocycling procedure and shear bond strength testing. The data were analyzed using 1-way analysis of variance, and P < 0.05 was considered statistically significant. The mean (SD) shear bond strength values in the different surface treatment groups were significantly different (P < 0.05): sandblasting, 16.59 (7.10) MPa; acid etching, 15.63 (2.94) MPa; sandblasting + metal primer, 13.28 (1.27) MPa; metal primer, 8.90 (2.08) MPa; and control, 8.86 (3.57) MPa. The mean differences in shear bond strength values were significant between the sandblasting and control groups (P = 0.003) and between the acid-etching and metal primer groups (P = 0.013). Surface roughening procedures—either sandblasting or acid etching of the alloy surface— improved the shear bond strength of resin cement to milled alloy surfaces. The use of metal primer between the alloy surface and resin cement did not significantly increase the bond strength.
Received: November 18, 2023
Accepted: February 2, 2024
Keywords: alloys, computer-aided design, metal primer, resin cements, shear bond strength, surface treatment
Metal-ceramic restorations are popular in fixed prosthodontics because they exhibit superb mechanical properties, are highly durable, and are less costly than all-ceramic restorations.1 Nickel-chromium (Ni-Cr) alloys are typically used to fabricate metal-ceramic prostheses, but 10% to 20% of the population is allergic to nickel-containing alloys.2 Cobalt-chromium (Co-Cr) alloys offer greater biocompatibility and corrosive resistance.3,4
Conventionally, the lost-wax technique is applied to fabricate the metal substructure for metal-ceramic restorations. However, this technique is lengthy and complex and therefore may result in varying quality and accuracy. Computer-aided design/computer-aided manufacturing (CAD/CAM) techniques have revolutionized design and fabrication methods for dental restorations, improving the quality of dental restorations and eliminating many shortcomings of the conventional lost-wax technique.5-7
Two approaches can be adopted to process base metal alloys in CAD/CAM protocols: additive manufacturing (laser sintering) and subtractive manufacturing (hard or soft machining). Subtractive manufacturing minimizes the development of defects and porosities in Co-Cr blocks during the casting process, but its drawbacks include the considerable hardness of the bulk blocks used for machining, increased wear of milling tools and the milling machine, and high maintenance costs. Soft machining of Co-Cr blocks was introduced to improve the fabrication and milling of these restorations. After design of the restoration, during the fabrication process, the blocks undergo a milling procedure in a CAD/CAM unit. The restoration then undergoes a sintering process to make it dense and hard.6,8
Adhesion of cement to the intaglio surfaces of metalceramic restorations provides retention and longevity, especially in restorations designed for short or overtapered abutments, where resin cements are the material of choice because they exhibit lower solubility, more viscosity, lower film thickness, and improved mechanical properties compared with conventional cements, including zinc phosphate and glass ionomer.2,9,10 However, the resin cement–metal alloy interface may not achieve a durable bond without surface treatment, since the luting agents exhibit a low chemical affinity for metal alloys. Different surface treatment options preceding cementation have been introduced to achieve micromechanical interlocking and a chemical bond to improve retention.
The proposed surface treatments of metals used for metalceramic restorations include sandblasting, acid etching, tin plating, silicoating, laser treatment, and the application of a metal primer. Sandblasting with aluminum oxide is the most
Panavia F 2.0 (Kuraray Noritake) 890066 Resin cement
Experimental (mixed for this study) NA Etchant gel
common method used to improve micromechanical retention because it is inexpensive and enhances the wettability of the cement by mechanically removing debris from the metal surface. Metal primers include active monomers such as 10-methacryloyloxydecyl dihydrogen phosphate (10-MDP), methacryloyloxyalkyl thiophosphate (MEPS), and 4-methacryloxyethyltrimellitate anhydride (4-META) as well as others that bind to metals and alloys through their affinity for metal oxides on metal surfaces. Etchant gels are applied easily and exhibit better efficacy than other micromechanical methods. Surface treatments such as tin plating, silicoating, and laser treatment are rarely used clinically due to their technique sensitivity and the need for additional equipment. However, combining such surface treatments might be useful for achieving micromechanical and chemical bonds. These combinations promote bonding mechanisms and enhance the metal-cement bond, but further investigations are necessary.9-11
A limited number of studies have investigated soft presintered alloys and their bond to resin cement. Therefore, the present study evaluated the shear bond strength of resin cement to a CAD/CAM millable presintered Co-Cr alloy after different surface treatments. The failure modes (within the cement or at the metal-cement interface) were also evaluated to help future studies.
The null hypothesis was that there would be no differences between different surface treatments with regard to their bond strength to resin cement or their failure pattern.
Methods
The protocol of this in vitro study was approved by the ethics committee of Shiraz University of Medical Sciences, Tehran, Iran (IR.SUMS.DENTAL.REC.1401.009).
Core preparation
Table 1 presents the materials used in this study. The study used 40 cylindrical cores of Ceramill Sintron (Amann Girrbach) with a diameter of 6 mm and a height of 8 mm as a millable presintered Co-Cr alloy.
Ceramill Sintron cores were designed by a CAD program (Ceramill Match 2, Amann Girrbach), and a milling machine (Ceramill Motion 2, Amann Girrbach) was used to process the presintered blocks. Following the manufacturer’s instructions, the cores were sintered at 1300°C in a sintering furnace under an argon gas atmosphere (Ceramill Argotherm, Amann Girrbach).
Surface treatment
The milled and sintered cores were assigned to 1 of 5 groups based on surface treatment (n = 8): control; sandblasting; metal primer; sandblasting + metal primer; or acid etching. The control group received no surface treatment. In the sandblasting group, the adhesive surface of the core was abraded with airborne 110-μm aluminum oxide particles (Basic classic, Renfert) under 0.2-MPa gas pressure for 10 seconds at a distance of 20 mm. The core was then placed in an ultrasonic bath (BioSonic UC300, Coltene) containing 95% methyl alcohol for 15 minutes and air dried. In the metal primer group, a single layer of Z-Prime Plus (Bisco) was applied to the adhesive surface of the metal with a micro brush and left to set in accordance with the manufacturer’s instructions. In the sandblasting + metal primer group, the adhesive surface of the core was sandblasted with 110-μm aluminum oxide particles and subsequently covered with a single layer of Z-Prime Plus. In the acidetching group, the adhesive surface of the core was etched with a 50-50 mixture of nitric acid and hydrochloric acid (mixed for this experiment) for 20 minutes and rinsed under running water for 1 minute. The core was subsequently cleaned ultrasonically with 96% ethanol (Bidestan) for 10 minutes and dried with air spray under 2-bar pressure for 10 seconds.
Cementation
Light-cured composite resin (Clearfil AP-X, Kuraray Noritake) was packed into silicone molds that were 3 mm in diameter and 3 mm in height. A glass slide was placed on each mold to create a uniform specimen surface, and then light curing (Heliolux DLX, Ivoclar Vivadent) was performed for 40 seconds on both sides. Subsequently, Panavia F 2.0 resin cement (Kuraray
Table 1. Compositions of the materials used in this study.
Noritake) was used to bond the cylindrical composite resin specimens to the pretreated core surfaces. After a 10-second initial light-curing procedure, excess cement on the margins was removed, an oxygen-inhibiting gel (Oxyguard II, Kuraray Noritake) was applied for 3 minutes, and final curing was performed from 4 directions for 40 seconds from each direction.
Shear bond strength testing
After the specimens were stored in distilled water at 37°C for 24 hours, they underwent a thermocycling procedure consisting of 1500 cycles at 5°C/55°C with a rest time of 20 seconds at each temperature. Shear load testing was undertaken in a universal testing machine (Z020, Zwick Roell). The specimens were fixed on the apparatus of the testing machine. A chisel applied a parallel shearing force to the cement-metal interface at a crosshead speed of 0.5-mm/min. The force at the resin cement–alloy surface bond failure was recorded in newtons (N) for each specimen, and the mean shear bond strength was determined in megapascals (MPa) using the following formula: S = T/A, where S is the shear bond strength, T is the tension (force) applied, and A is the bonded surface area.
The failure patterns were reviewed under a stereomicroscope (SMZ800, Nikon) at ×30 magnification (Figure). Failures were categorized as adhesive, indicating cement-metal bond failure; cohesive, indicating failure within the resin cement, with a thin layer of cement remaining on the metal; or mixed, indicating a mixture of the other modes, with some cement adhering to the metal.
Statistical analysis
Statistical analyses were performed with SPSS software (version 24, IBM) using the Kolmogorov-Smirnov test to analyze the distribution of data, 1-way analysis of variance (ANOVA) to compare the bond strengths of the 5 groups, post hoc Tukey tests to perform pairwise comparisons of the alloys regarding bond strength, and the chi-square test to analyze failure modes. For all tests, P < 0.05 was considered statistically significant.
Results
The Kolmogorov-Smirnov test showed a normal distribution of the bond strength data in all study groups. A 1-way ANOVA was applied to compare the effects of various surface treatment
modalities on the shear bond strength between the resin cement and base metal alloy. The results indicated significant differences in the mean bond strength values between groups (P < 0.05). Post hoc Tukey tests showed that the mean bond strength value was significantly higher in the sandblasting group than in both the control and metal primer groups (P < 0.05) (Table 2 and Chart).
The sandblasted surfaces exhibited no statistically significant differences in shear bond strength values compared with acidetched surfaces (P > 0.05). In addition, no statistically significant difference was observed between the sandblasting group and the sandblasting + metal primer group.
Table 3 lists the fracture modes found in each group. The chi-square test indicated statistically significant differences in failure modes among the groups (P < 0.012). Stereomicroscopic evaluation of the failure modes showed that the majority of failures were mixed in the sandblasting, acid-etching, and sandblasting + metal primer groups. The predominant failure mode in the metal primer groups was adhesive. In the control group, adhesive and mixed failures were equally distributed. Notably, cohesive failure occurred in higher stress levels, and this type of failure was in the minority.
Discussion
The present study confirmed a significant effect of the surface treatment on the shear bond strength of resin cement to a base metal alloy and the resulting failure mode, rejecting the null hypothesis. Considering the effects of the resin cement–dental restoration bond on the severity of microleakage, relevant biologic complications, and restoration longevity, the bond strength in such restorations should be investigated comprehensively. Bonding between an alloy and a resin cement is achieved through micromechanical and chemical retention. Alloy surface roughening improves micromechanical retention, and a chemical reaction helps achieve a bond between the surface metal oxides and the acidic functional monomers of the metal primers and/or resin cements.12
The present study compared the effects of various surface treatments on the shear bond strength between a Co-Cr alloy and a resin cement, demonstrating that sandblasting and/or chemical etching of the Co-Cr alloy surface significantly improved the bond of the resin cement to the base metal alloy. Acid-etching solutions create micro-undercuts as a function
Figure. Examples of failure types. A. Adhesive. B. Cohesive. C. Mixed.
aStatistically significant differences in failure modes between groups (chi-square test).
of the acid concentration and the composition of the etched material. Sandblasting increases surface irregularities and the wettability of the cement by mechanically removing debris. Polymerization of resin in these undercuts creates a micromechanical bond, making the detachment of the cement from the metal more difficult. These methods are less technique sensitive and lower cost than other metal surface treatment modalities.13 Studies have reported similar findings with a Ni-Cr alloy after a sandblasting procedure using 50-μm alumina particles and chemical etching.14,15
Z-Prime Plus, which is applied as a surface treatment for zirconia, metals/alloys, composite resins, and alumina, improves the bond strength of composite resin cements to indirect restorative materials due to its unique chemical composition.13 The chemical composition of a resin adhesive or primer determines its clinical applications. Monomers are essential components of adhesives and primers. Panavia F 2.0, a dual-curing resin cement, and Z-Prime Plus include the monomer 10-MDP, a phosphate monomer with a hydrophilic phosphate terminal end that can form a chemical bond with the oxide layer on the metal surface. In addition, hydrophobic methacrylate terminal ends form a bond with the resin. Such a strong bond prevents water penetration into the adhesive interface, leading to decreased hydrolysis.13
Despite these reported effects, in the present study, application of a metal primer to the sandblasted surface of the metal alloy did not significantly increase the shear bond strength
when compared with sandblasting alone. Taira et al reported that the shear bond strength of Panavia 21 (Kuraray) to commercially pure titanium was not significantly different regardless of whether or not an alloy primer was applied after 24 hours of water storage and a thermo-cycling procedure.16 Abreu et al applied an alloy primer to the sandblasted surface of metal-ceramic copings cemented to minimally retentive preparations.17 No significant improvements in bond strength were reported compared with a sandblasting procedure with 50-μm alumina particles alone. Only the bond failure location was affected, consistent with the present study.17 In a study by Fonseca et al, Panavia F exhibited a higher bond strength to Ni-Cr alloy in specimens subjected to sandblasting than in those subjected to sandblasting + alloy primer.18
These findings might be explained by the impacts of metal primers on the sandblasted alloy surface. It is possible that the surface microporosities created by sandblasting are obstructed as a result of the copolymerization of the alloy primer monomers. Such surface changes adversely would affect the microundercuts formed within the metal, decreasing the access of resin materials to the surface area and thereby the interlocking between the resin cement and metal surface. However, Sadighpour et al concluded that a combination of sandblasting and applying a metal primer improved the bond strength significantly compared with sandblasting alone.12 The disparities in the results may be attributed to differences in the metal primers used and the experimental methods.
Chart. Mean shear bond strength of resin cement to a millable alloy, according to surface treatment (n = 8 per group).
Table 2. Mean (SD) shear bond strengths of the surface treatment groups (n = 8 per group).
Table 3. Failure modes observed under a stereomicroscope.
The present study found significantly lower shear bond strength values in the metal primer and control groups than in the other groups. These groups rely on the chemical bond between the metal and resin cement. In this study, the metal surfaces that were not treated with a method to roughen or form an oxide layer on the metal surface did not exhibit sufficient adhesion strength. According to Raeisosadat et al, a minimum bond strength of 10 to 13 MPa suffices for withstanding loads under oral conditions.9 In this respect, the bond strengths of the sandblasted and acid-etched groups were within the acceptable clinical range. Thermocycling was applied in the present study because it can accelerate the aging of polymeric materials, making it possible to evaluate the deterioration of metal adhesive systems over a shorter period than long-term immersion testing.19
The investigation of failure modes revealed that the highest numbers of mixed failures were in the sandblasting and acidetching groups, which also had higher shear bond strength values. According to previous studies, a high fracture rate within the substrate, in the form of cohesive or mixed failures, may indicate higher bond strength.20,21 In the present study, the groups with the lowest bond strengths (the control and metal primer groups) exhibited adhesive failure, consistent with studies by Al-Hana et al and Chung et al, who reported a high rate of adhesive failure in the groups with the lowest bond strength values.21,22 On the other hand, according to Armstrong et al, it might not be possible to attribute cohesive failure of the substrate in tensile or shear bond strength testing to a higher bond strength at the interface as opposed to the strength of the bonding agent itself.23
The present study has some limitations. Because only a single etching time and solution for the alloy were used, the most favorable etching conditions cannot be definitively stated. Further studies with different alloys, resin cements, and etching solutions are suggested to generalize the results. Because this was an in vitro study, the effects of long-term water aging and pH changes to simulate the oral environment were not evaluated. The effects of dynamic loading and the resulting fatigue on the longevity of the resin bond should be studied as well. Future long-term clinical research should substantiate the effectiveness of the tested systems in providing a reliable bond strength.
Conclusion
Within the limitations of this in vitro study, several conclusions may be drawn from the results. The shear bond strength of resin cement to Co-Cr alloy depended on the surface treatment, and roughening of the surface through sandblasting or acid etching of the alloy surface resulted in the highest bond strengths of the resin cement to the base metal alloy. Sandblasting significantly improved the bond strength of the resin cement to the base metal alloy. In addition, the data indicated that an effective bond can be achieved between resin cement and etched metal. The ease of the etching process and need for less equipment should encourage greater use of acidetching surface treatment. Application of a metal primer application did not improve the bond strength of the resin cement to the Co-Cr metal alloy.
Author affiliations
Biomaterial Research Center, Department of Prosthodontics, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran (Mohaghegh); Department of Operative Dentistry, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran (Firouzmandi); School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran (Hadadi).
This research was supported by the Vice-Chancellery of Research, Shiraz University of Medical Sciences (grant No. 24743).
Acknowledgments
The authors thank Dr Kamran Mirzaei of the Dental Research Development Center, Shiraz University of Medical Sciences, for the statistical analysis. This study was derived from an undergraduate thesis by Dr Melika Hadadi.
References
1. Wang H, Feng Q, Li N, Xu S. Evaluation of metal-ceramic bond characteristics of three dental Co-Cr alloys prepared with different fabrication techniques. J Prosthet Dent. 2016;116(6):916-923. doi:10.1016/j.prosdent.2016.06.002
2. Fonseca RG, Martins SB, de Oliveira Abi-Rached F, Dos Santos Cruz CA. Effect of different airborne-particle abrasion/bonding agent combinations on the bond strength of a resin cement to a base metal alloy. J Prosthet Dent. 2012;108(5):316-323. doi:10.1016/S00223913(12)60185-1
3. Park JK, Kim HY, Kim WC, Kim JH. Evaluation of the fit of metal ceramic restorations fabricated with a pre-sintered soft alloy. J Prosthet Dent. 2016;116(6):909-915. doi:10.1016/j. prosdent.2016.03.024
4. Lombardo GH, Nishioka RS, Souza RO, et al. Influence of surface treatment on the shear bond strength of ceramics fused to cobalt-chromium. J Prosthodont. 2010;19(2):103-111. doi:10.1111/j.1532-849X.2009.00546.x
5. Mohammadi Z, Mahabadi M, Tabbakhian G, Talaakoob M. Bond strength of porcelain to milled sintered and casting base metal alloys. J Dent (Shiraz). 2021;22(1):21-26. doi:10.30476/DENTJODS.2020.84347.1076
6. Izadi A, Vafaee F, Shishehian A, Roshanaei G, Fathi Afkari B. Evaluation of dimensional accuracy of dental bridges manufactured with conventional casting technique and CAD/CAM system with Ceramill Sintron blocks using CMM. J Dent Res Dent Clin Dent Prospects 2018;12(4):264-271. doi:10.15171/joddd.2018.041
7. Al Jabbari YS, Barmpagadaki X, Psarris I, Zinelis S. Microstructural, mechanical, ionic release and tarnish resistance characterization of porcelain fused to metal Co-Cr alloys manufactured via casting and three different CAD/CAM techniques. J Prosthodont Res. 2019;63(2):150156. doi:10.1016/j.jpor.2018.10.008
8. Stawarczyk B, Eichberger M, Hoffmann R, et al. A novel CAD/CAM base metal compared to conventional CoCrMo alloys: an in-vitro study of the long-term metal-ceramic bond strength. Oral Health Dent Manag. 2014;13(2):446-452.
9. Raeisosadat F, Ghavam M, Hasani Tabatabaei M, Arami S, Sedaghati M. Bond strength of resin cements to noble and base metal alloys with different surface treatments. J Dent (Tehran). 2014;11(5):596-603.
10. Di Francescantonio M, de Oliveira MT, Garcia RN, Romanini JC, da Silva NR, Giannini M. Bond strength of resin cements to Co-Cr and Ni-Cr metal alloys using adhesive primers. J Prosthodont. 2010;19(2):125-129. doi:10.1111/j.1532-849X.2009.00534.x
11. Ezoji F, Tabari K, Jaberi Ansari Z, Torabzadeh H, Kharrazi Fard MJ. Shear bond strength of a resin cement to different alloys subjected to various surface treatments. J Dent (Tehran). 2016;13(1):29-39.
12. Sadighpour L, Mostafavi AS, Pirmoradian M, Alipuryalda F. Comparison of bond strength in the different class of resin cements to cast and CAD/CAM Co-Cr alloys. Int J Dent. 2021;2021:7843979. doi:10.1155/2021/7843979
13. Jamel RS, Nayif MM, Abdulla MA. Influence of different surface treatments of nickel chrome metal alloy and types of metal primer monomers on the tensile bond strength of a resin cement. Saudi Dent J. 2019;31(3):343-349. doi:10.1016/j.sdentj.2019.03.006
14. Malek Nejad F, Ghavam Nasiri M. Effect of ultrasonic cleanser on base metal alloy to enamel bond strength after surface treatment by acid and sandblast. J Mashhad Dent Sch. 2003;27(1,2):57-66. doi:10.22038/JMDS.2003.1629
15. Isidor F, Hassna NM, Josephsen K, Kaaber S. Tensile bond strength of resin-bonded non-precious alloys with chemically and mechanically roughened surfaces. Dent Mater. 1991;7(4):225-229. doi:10.1016/S0109-5641(05)80019-3
16. Taira Y, Yanagida H, Matsumura H, Yoshida K, Atsuta M, Suzuki S. Adhesive bonding of titanium with a thione-phosphate dual functional primer and self-curing luting agents. Eur J Oral Sci. 2000;108(5):456-460. doi:10.1034/j.1600-0722.2000.108005456.x
17. Abreu A, Loza MA, Elias A, Mukhopadhyay S, Rueggeberg FA. Effect of metal type and surface treatment on in vitro tensile strength of copings cemented to minimally retentive preparations. J Prosthet Dent. 2007;98(3):199-207. doi:10.1016/S0022-3913(07)60056-0
18. Fonseca RG, de Almeida JG, Haneda IG, Adabo GL. Effect of metal primers on bond strength of resin cements to base metals. J Prosthet Dent. 2009;101(4):262-268. doi:10.1016/S00223913(09)60050-0
19. Matsumura H, Tanaka T, Taira Y, Atsuta M. Bonding of a cobalt-chromium alloy with acidic primers and tri-n-butylborane-initiated luting agents. J Prosthet Dent. 1996;76(2):194-199. doi:10.1016/s0022-3913(96)90306-6
20. Leloup G, D’Hoore W, Bouter D, Degrange M, Vreven J. Meta-analytical review of factors involved in dentin adherence. J Dent Res. 2001;80(7):1605-1614. doi:10.1177/ 00220345010800070301
21. Al-Hana DA, El-Messairy A, Shohayb F, Alhadainy H. Micro-shear bond strength of different composites and glass-ionomers used to reinforce root dentin. Tanta Dent J. 2013;10(2):58-66. doi:10.1016/j.tdj.2013.08.004
22. Chung CW, Yiu CK, King NM, Hiraishi N, Tay FR. Effect of saliva contamination on bond strength of resin luting cements to dentin. J Dent. 2009;37(12):923-931. doi:10.1016/ j.jdent.2009.07.007
23. Armstrong SR, Boyer DB, Keller JC. Microtensile bond strength testing and failure analysis of two dentin adhesives. Dent Mater. 1998;14(1):44-50. doi:10.1016/s0109-5641(98)00008-6
Pathologic jaw lesions associated with impacted teeth
The aim of this study was to evaluate the histopathologic diagnoses and radiographic characteristics of lesions associated with impacted teeth. In this retrospective study, 2624 biopsy reports were assessed. If the report was a record of a pericoronal lesion, the age and sex of the patient and the location, microscopic diagnosis, radiographic features, and size of the lesion were recorded. The Pearson chi-square, Kruskal-Wallis, and Fisher exact tests were used for statistical analysis. In total, 189 patients (7.2%) had lesions associated with impacted teeth. The mean (SD) age of affected patients was 25.91 (14.38) years, and 51.9% of patients with pericoronal lesions were male. The most common lesion sites were the posterior region of the maxilla (43.3%) and the posterior region of the mandible (38.0%).
Dentigerous cysts (DCs) constituted 64.6% of the lesions, and odontogenic keratocysts (OKCs) represented 18.5%. Radiographs were available in 153 cases, and most lesions were radiolucent (96.1%), had well-defined outlines (99.3%), and were unilocular (87.6%). Lesions larger than 2.0 cm were 5.5 times more likely than smaller lesions to be diagnosed as non-DC lesions (P = 0.001; Kruskal-Wallis test). Although most of the lesions associated with impacted teeth were DCs, there were other lesions with aggressive behavior, such as OKCs, ameloblastomas, and glandular odontogenic cysts, which require more extensive treatment. Lesions that were 2.0 cm or greater showed a higher probability of being non-DC lesions.
An impacted tooth is demarcated as a tooth that remains completely or incompletely embedded in the jaw or mucosa for more than 2 years following physiologic eruption time.1 Many odontogenic cysts and neoplasms are associated with impacted teeth.2 Impacted teeth in children and adolescents are infrequently associated with pathologic lesions, but the prevalence of complications increases in the following decades.3
The dentigerous cyst (DC) is the most common pericoronal lesion and develops through the accumulation of fluid between the reduced enamel epithelium and crown of the tooth.4 Other types of pericoronal lesion, including the odontogenic keratocyst (OKC) and ameloblastoma, can show radiographic features similar to DCs but require different treatment. Management of pericoronal lesions varies from enucleation of DCs to en bloc resection of ameloblastomas.
Most pericoronal lesions are detected incidentally on radiographic images, although some can cause swelling, pain, or functional disturbance. 2 Radiography is the first step in the diagnostic approach to jaw lesions, and the panoramic view is the primary imaging technique used to assess impacted teeth and associated lesions. 3 The DC classically displays as a well-defined unilocular radiolucency adjacent to the crown of an impacted tooth. The radiolucency surrounding the tooth crown should be at least 3 to 4 mm in diameter to differentiate it from the dental follicle. 3,4 Tooth displacement and root resorption may be present adjacent to the lesion. On radiographs, the OKC appears as a welldefined unilocular or multilocular radiolucent lesion with smooth or scalloped margins, which are often corticated. It tends to grow in an anteroposterior direction without causing significant expansion. The dominant radiographic feature of ameloblastoma is a multilocular pattern with coarse and curved septa. Mandibular lesions show well-defined and occasionally scalloped margins, while maxillary ameloblastomas display ill-defined margins. The ameloblastoma may be associated with root resorption, tooth displacement, bone expansion, and perforation. 3
The surgeon must make a correct differential diagnosis preoperatively by examining the radiographic features and clinical findings and providing appropriate treatment for the patient. The treatment of choice for pericoronal lesions larger than 2 cm is an excisional biopsy. Larger lesions may need incisional biopsy and supplementary surgical treatment after microscopic diagnosis.2
Several studies have focused their analysis only on the radiographic appearance of pericoronal pathologic lesions, and some have evaluated only the histopathologic reports.5-9 However, clinically, the combined evaluation of both types of findings can be more useful and reduce the possibility of diagnostic
error.2 The present study aimed to evaluate the histopathologic diagnoses and radiographic characteristics of lesions associated with impacted teeth and establish factors predictive of diagnosis in an Iranian population.
Methods
This study was approved by the ethics committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran (IR.SBMU. DRC.1400.110).
This retrospective study was based on the assessment of 2624 biopsy reports prepared in the years 2013 to 2022 at the Department of Oral and Maxillofacial Pathology, Shahid Beheshti University of Medical Sciences. The inclusion criteria were the files of patients with pericoronal jaw lesions. The exclusion criteria were files with unclear histopathologic or radiographic reports or without demographic information. For the cases included in the study, the age and sex of the patient as well as the location, microscopic diagnosis, radiographic features, and size (greatest dimension) of the lesion were recorded and categorized in tables. In addition, any available radiographs were evaluated and classified based on variables related to radiographic characteristics, including the size, internal structure, margins, and locularity as well as the effect of the lesion on surrounding structures. The microscopic slides of the selected cases were reexamined by an oral pathologist (S.A.-M.), and the diagnoses were confirmed.
Based on the findings of Caruso et al, the lesions were divided into 2 groups according to size (< 2.0 cm or ≥ 2.0 cm).2
The Pearson chi-square, Kruskal-Wallis, and Fisher exact tests were used for statistical analysis (SPSS, version 20, IBM), and statistical significance was set as α < 0.05.
Results
In total, 189 patients (7.2%) had lesions associated with impacted teeth. There were 98 male (51.9%) and 91 female (48.1%) patients, constituting a male to female ratio of 1.07/1. The lesions were most frequently identified in patients in the third and fourth decades of life (53.4%) and the mean (SD) age of patients with pericoronal lesions was 25.91 (14.38) years, with a range of 5 to 70 years.
There were 103 maxillary lesions and 86 mandibular lesions, and the most common site was the posterior region of the maxilla (n = 81; 43.3%). This was followed by posterior region of the mandible (n = 71; 38.0%), anterior region of the maxilla (n = 20; 10.7%), and anterior region of the mandible (n = 15; 8.0%). The exact location (anterior or posterior) of 2 maxillary lesions was unknown.
The review of the 189 microscopic diagnoses, based on an evaluation of biopsy reports and radiographs, identified 13 types of lesion: DC (n = 122; 64.6%), OKC (n = 35; 18.5%), solid ameloblastoma (n = 5; 2.6%), unicystic ameloblastoma (n = 5; 2.6%), glandular odontogenic cyst (n = 5; 2.6%),
Figure. Radiolucent pericoronal lesions. A. Dentigerous cyst. B. Odontogenic keratocyst. C. Solid ameloblastoma. D. Glandular odontogenic cyst. E. Odontoma.
Radiographic feature Lesions, n (%)
Internal structure
Radiolucent 147 (96.1)
Mixed 4 (2.6)
Radiopaque 2 (1.3)
Outline
Well-defined 152 (99.3)
Poorly defined 1 (0.7)
Margin
Scalloped 28 (18.3)
Nonscalloped 125 (81.7)
Locularity
Unilocular 134 (87.6)
Multilocular 19 (12.4)
Effect on surrounding area
Tooth displacement 35 (22.9)
Root resorption 8 (5.2)
Displacement and resorption 8 (5.2)
No effect 102 (66.7)
Table 2. Common pathologic diagnoses based on lesion size (n = 137).a
a Analysis of the 5 most common lesion types using cases with an available radiograph.
bLesions smaller than 2.0 cm were significantly more likely to be cysts (P = 0.041; Fisher exact test).
cDentigerous cysts were significantly smaller than odontogenic keratocysts (P = 0.000; Kruskal-Wallis test).
odontoma (n = 4; 2.1%), orthokeratinized odontogenic cyst (n = 3; 1.6%), myxoma (n = 2; 1.1%), ameloblastic fibroodontoma (n = 2; 1.1%), central giant cell granuloma (n = 2; 1.1%), adenomatoid odontogenic tumor (n = 2; 1.1%), DC associated with odontoma (n = 1; 0.5%), and DC associated with mucoepidermoid carcinoma (n = 1; 0.5%).
A majority of pericoronal lesions were odontogenic cysts (87.3%), and neoplasms comprised 12.7% of the lesions. A total of 153 radiographs were available for review. In most cases with available radiographs, the lesions were radiolucent (96.1%) (Figure). In addition, most lesions had well-defined outlines (99.3%) and were unilocular (87.6%) (Table 1). The effect on the surrounding area, classified as tooth displacement, root resorption, or both, was recorded for 51 lesions, or 33.3% of lesions with an available radiograph.
Statistical analysis was limited to lesion types represented by 5 cases or more in the sample: DC, OKC, solid ameloblastoma, unicystic ameloblastoma, and glandular odontogenic cyst. The lesion dimensions ranged from 0.5 to 9.0 cm (Table 2). The Kruskal-Wallis test indicated that DCs were significantly smaller than OKCs (P = 0.000). Lesions larger than 2.0 cm were 5.5 times more likely to be diagnosed as non-DCs (P = 0.001; Kruskal-Wallis test). According to the Fisher exact test, lesions smaller than 2.0 cm were significantly more likely to be cysts (P = 0.041).
The effect of the most common types of pericoronal lesion on surrounding structures was analyzed with the Fisher exact test (Table 3). No statistically significant relationship was found
between the frequency of different lesion types and the effect on surrounding structures (P > 0.05), although OKCs (3.6%) had a lesser tendency to cause root resorption than DCs (10.5%).
The Fisher exact test revealed a statistically significant relationship between the frequency of lesion types and their locularity (P = 0.000) (Table 4). Cysts were more likely to be unilocular than were tumors (P = 0.037). However, no statistically significant relationship was found between the frequency of different lesions and the type of margin.
There was a statistically significant relationship between the age of the patient and the presence of cyst versus a tumor (P = 0.006; Pearson chi-square test). The analysis revealed that cysts were found more frequently in individuals older than 18 years and tumors were found more frequently in patients aged 18 years or younger.
Discussion
In the present study, the overall frequency of pericoronal jaw lesions was 7.2%, which is in agreement with the findings of previous studies.2,10-14 The incidence of radiolucent pericoronal lesions in the general population is low (< 3%).2
Curran et al found that 9.32% of lesions around impacted teeth are significant pathologic lesions, and there was a strong relationship between increasing patient age and an increasing frequency of lesions around the crown.9 The present research showed a slight male predilection, which is in agreement with the findings of Al-Khateeb and Bataineh.7 In other studies, the male to female ratio was reported to be much higher.8,11
Table 1. Radiographic features of lesions associated with impacted teeth (n = 153).
a Analysis of the 5 most common lesion types using cases with an available radiograph. bNo statistically significant relationship was found between the frequency of different lesions and the effect on surrounding structures (P > 0.05; Fisher exact test).
Table 4. Marginal characteristics and locularity of the most common pericoronal lesions (n = 137).a
a Analysis of the 5 most common lesion types using cases with an available radiograph.
bNo statistically significant relationship was found between the frequency of different lesions and the type of margin (P > 0.05; Fisher exact test).
cCysts were more likely to be unilocular than were tumors (P = 0.037; Fisher exact test).
Contrary to these results, Yildirim et al reported that the frequency was higher in females.15 The mean age of affected patients in the present study was 25.9 years, tending to the third and fourth decades, which is consistent with the results of several previous studies.7,8,11,12,15
In the population in the present study, the majority of pericoronal lesions (87.3%) were cystic lesions. This finding is comparable to the results of other studies, which range from 78% to 93%.2,9,16,17 The most common type of lesion in the present population was the DC, followed by OKC and ameloblastoma (solid and unicystic), which is in line with the results of various studies in this field.2,9-11,15,16 However, in several studies, the frequency of ameloblastoma was reported to be greater than that of OKC.7,8,12,13
Another important finding in this study was the presence of mucoepidermoid carcinoma–like islands in the cyst wall of one DC in a 57-year-old woman. Other studies have also reported malignant lesions associated with impacted teeth, at rates ranging from 0.05% to 2%, and the most common microscopic report was squamous cell carcinoma. 2,8,9,12,13 It
has been mentioned that patients with malignant pericoronal lesions tend to be in their fifth decade or older, which suggests the possibility of malignant changes in the cyst wall with age. 2 Malignancies arising from cysts may show a benign radiographic appearance. 2 In the present study, 96.1% of the lesions were radiolucent, and the remaining 3.9% were related to lesions such as odontoma and ameloblastic fibroodontoma. About 87.6% of the lesions were unilocular; scalloped margins were observed in 18.3% of lesions, and 66.7% of lesions had no observable effect on the surrounding structures. According to Mortazavi et al, although various radiographic characteristics have been observed in pathologic lesions associated with the unerupted tooth, most initially appear as unilocular radiolucencies with the potential to change into multilocular lesions with well-defined margins, and some lesions show radiopaque foci. 3
In the present study, there was a significant relationship between different types of lesions in terms of locularity. For example, a greater percentage of ameloblastomas were multilocular, and a greater percentage of OKCs were unilocular.
Table 3. Effect of the most common pericoronal lesions on surrounding structures (n = 137). a
In contrast, Ariji et al observed no statistically significant difference in locularity between ameloblastomas and OKCs.18 In review of radiographs of DCs, OKCs, and ameloblastomas, Cardoso et al reported that ameloblastoma exhibited multilocularity more frequently than these 2 cysts and there was no difference between the characteristics of DCs and OKCs.19
In the present research, OKCs were significantly larger than DCs, but Cardoso et al found that ameloblastomas were significantly larger than OKCs and DCs.19 They also did not find a relationship between root resorption and the type of lesion.19 In contrast, in the present study, a higher percentage of DCs than OKCs were associated with root resorption, although the difference was not statistically significant. Caruso et al found that large size was predictive of non-DC pathologic diagnoses.2 Similarly in the present study, lesions larger than 2.0 cm were 5.5 times more likely to be diagnosed as non-DC lesions.
In the present study, DC was more common in the fourth decade of life. The relationship between age and microscopic diagnosis of radiolucent lesions has been previously investigated, and it has been observed that patients with non-DC lesions are usually in the first to third decades of life.20-22 Some studies have reported that DCs often occur when patients are in the second to third decades of life and the incidence decreases thereafter.9,23 However, other research has suggested that patients with DCs are generally in the fifth decade of life.2 Most DCs arise from third molars and grow slowly. Therefore, more time would be needed to develop a lesion of large size. In the general population, many of these diagnoses are likely to come from younger patients undergoing extraction of normal third molars with enlarged dental follicles.
Conclusion
In this Iranian population, most of the lesions associated with impacted teeth were DCs. However, there were also lesions that demonstrate aggressive behavior, such as OKC, ameloblastoma, and glandular odontogenic cyst, which require more extensive treatment. Lesions larger than 2.0 cm had a higher probability of being non-DC lesions. A combination of careful examination of radiographs and close review of histopathologic reports is vital to establishing a correct diagnosis and thereby ensuring appropriate treatment.
Author affiliations
Department of Oral and Maxillofacial Pathology, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran (Atarbashi-Moghadam); School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran (Emamipour); Department of Oral and Maxillofacial Radiology, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran (Safi, Ghazizadeh Ahsaie).
1. Zoubi H, Alharbi AA, Ferguson DJ, Zafar MS. Frequency of impacted teeth and categorization of impacted canines: a retrospective radiographic study using orthopantomograms. Eur J Dent. 2017;11(1):117–121. doi:10.4103/ejd.ejd_308_16
2. Caruso DP, Lee CC, Peacock ZS. What factors differentiate dentigerous cysts from other pericoronal lesions? Oral Surg Oral Med Oral Pathol Oral Radiol. 2022;133(1):8-14 doi:10.1016/j.oooo.2021.05.003
3. Mortazavi H, Baharvand M. Jaw lesions associated with impacted tooth: a radiographic diagnostic guide. Imaging Sci Dent. 2016;46(3):147-157. doi:10.5624/isd.2016.46.3.147.
4. Lotfi A, Shirkavand S, Mokhtari S, Zalani SS, Atarbashi-Moghadam S. Relative frequency of dentigerous cyst in Iranian population: a 20-year retrospective study. Indian J Dent Res 2019;30(5):751-754. doi:10.4103/ijdr.IJDR_392_17
5. van der Linden W, Cleaton-Jones P, Lownie M. Diseases and lesions associated with third molars: review of 1001 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;79(2):142-145. doi:10.1016/s1079-2104(05)80270-7
6. Santamaria J, Arteagoitia I. Radiologic variables of clinical significance in the extraction of impacted mandibular third molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;84(5):469-473. doi:10.1016/s1079-2104(97)90259-6
7. Al-Khateeb TH, Bataineh AB. Pathology associated with impacted mandibular third molars in a group of Jordanians. J Oral Maxillofac Surg. 2006;64(11):1598-1602. doi:10.1016/ j.joms.2005.11.102
8. Mohammed M, Mahomed F, Ngwenya S. A survey of pathology specimens associated with impacted teeth over a 21-year period. Med Oral Patol Oral Cir Bucal. 2019;24(5):e571-e576 doi:10.4317/medoral.22873
10. Karabas HC, Ozcan I, Tekkesin MS, Tasyapan SA, Guray B, Atapek MM. Evaluation of radiolucent lesions associated with impacted teeth: a retrospective study. Curr Med Imaging 2020;16(10):1332-1339 doi:10.2174/1573405616666200206115827
11. Shin SM, Choi EJ, Moon SY. Prevalence of pathologies related to impacted mandibular third molars. Springerplus. 2016;5(1):915 doi:10.1186/s40064-016-2640-4
12. Vigneswaran AT, Shilpa S. The incidence of cysts and tumors associated with impacted third molars. J Pharm Bioallied Sci. 2015;7(Suppl 1):S251-254 doi:10.4103/0975-7406.155940
13. Patil S, Halgatti V, Khandelwal S, Santosh BS, Maheshwari S. Prevalence of cysts and tumors around the retained and unerupted third molars in the Indian population. J Oral Biol Craniofac Res. 2014;4(2):82-87 doi:10.1016/j.jobcr.2014.07.003
14. Regezi JA, Kerr DA, Courtney RM. Odontogenic tumors: analysis of 706 cases. J Oral Surg. 1978;36(10):771-778
15. Yildirim G, Ataoğlu H, Mihmanli A, Kiziloğlu D, Avunduk MC. Pathologic changes in soft tissues associated with asymptomatic impacted third molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106(1):14-18. doi:10.1016/j.tripleo.2007.11.021
16. Stathopoulos P, Mezitis M, Kappatos C, Titsinides S, Stylogianni E. Cysts and tumors associated with impacted third molars: is prophylactic removal justified? J Oral Maxillofac Surg 2011;69(2):405-408. doi:10.1016/j.joms.2010.05.025
17. Güven O, Keskin A, Akal UK. The incidence of cysts and tumors around impacted third molars. Int J Oral Maxillofac Surg. 2000;29(2):131-135.
18. Ariji Y, Morita M, Katsumata A, et al. Imaging features contributing to the diagnosis of ameloblastomas and keratocystic odontogenic tumours: logistic regression analysis. Dentomaxillofac Radiol. 2011;40(3):133-140 doi:10.1259/dmfr/24726112
19. Cardoso LB, Lopes IA, Ikuta CRS, Capelozza ALA. Study between panoramic radiography and cone beam-computed tomography in the diagnosis of ameloblastoma, odontogenic keratocyst, and dentigerous cyst. J Craniofac Surg. 2020;31(6):1747-1752 doi:10.1097/ SCS.0000000000006538
20. Correa Pontes FS, Lacerda de Souza L, Paula de Paula L, de Melo Galvão Neto E, Silva Gonçalves PF, Rebelo Pontes HA. Central odontogenic fibroma: an updated systematic review of cases reported in the literature with emphasis on recurrence influencing factors. J Craniomaxillofac Surg. 2018;46(10):1753-1757 doi:10.1016/j.jcms.2018.07.025
22. Masthan KM, Anitha N, Krupaa J, Manikkam S. Ameloblastoma. J Pharm Bioallied Sci 2015;7(Suppl 1):S167-S170. doi:10.4103/0975-7406.155891
23. Daley TD, Wysocki GP. The small dentigerous cyst: a diagnostic dilemma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;79(1):77-81. doi:10.1016/s1079-2104(05)80078-2
Comparison of flexural strength, marginal gap, and internal fit of milled and 3D-printed crown materials
Matthew Firestone, DDS, MS ¢ Eric Hu, DMD, MS, FACP ¢ Robert Masterson, DDS, MS, ABGD
Gen Paek, DDS, FACP ¢ Christopher Raimondi, DDS, MS ¢ Wen Lien, MS, DMD, MS
The purpose of this study was to compare the flexural strength, Weibull modulus (reliability), marginal gap, and internal fit (internal gap) of 4 materials for milling or 3-dimensional (3D) printing of definitive and provisional crowns: IPS e.max CAD (IEC), Paradigm MZ100 Block (PMB), Permanent Crown Resin (PCR), and Temporary CB Resin (TCR). Flexural strength was tested by subjecting sectioned milling blocks (IEC and PMB) or 3D-printed bars (PCR and TCR) to a 3-point bending test in a universal testing machine (n = 15 per material). Crowns were milled or 3D printed, and the marginal gap and internal fit were measured using microcomputed tomography (n = 5 per material). The data were analyzed with a t test and compared using analysis of variance (ANOVA) with Tukey post hoc comparisons (α = 0.05). The groups demonstrated the following mean (SD) flexural strength values: IEC, 335.50 (28.97) MPa; PMB, 154.34 (21.03) MPa; PCR, 128.09 (7.30) MPa; and TCR, 126.29 (9.23) MPa. A 1-way ANOVA revealed significant differences in the flexural strengths of sectioned and 3D-printed bars (P < 0.001). The PMB group showed the lowest Weibull modulus (8.77), indicating its poor reliability. The IEC group showed the smallest marginal gap, 53.42 (31.99) µm; this value was significantly smaller than the gap in the TCR group (P < 0.001) but not the PCR or PMB group. The PMB group had the smallest internal fit discrepancy (87.44 [37.60] µm) but was not significantly different from PCR, while TCR had a significantly greater internal fit discrepancy (130.61 [65.16] µm) than IEC, PMB, and PCR (P < 0.001). The occlusal internal fit discrepancies of 3D-printed crowns were significantly greater than those of milled crowns (P < 0.001). There was no statistically significant difference in flexural strength between the 3D-printed definitive (PCR) and provisional (TCR) materials. When the data were combined according to manufacturing method, the marginal gap and internal fit of crowns fabricated with 3D printing were comparable to those of milled crowns, and all mean marginal gaps were within a clinically acceptable limit of less than 120 µm.
The use of additive manufacturing (AM), or 3-dimensional (3D) printing, has gained popularity in an everincreasing variety of industries, including dentistry.1
The International Organization for Standardization (ISO) defines AM as the “process of joining materials to make parts from 3D model data, usually layer upon layer, as opposed to subtractive manufacturing [SM] and formative manufacturing methodologies.”2 According to the ISO, there are 7 general types of AM: material extrusion, vat photopolymerization, powder bed fusion, material jetting, binder jetting, direct energy deposition, and sheet lamination.2,3 Stereolithography (SLA) is a type of vat photopolymerization that utilizes an ultraviolet laser to cure photosensitive resins layer by layer. Compared with SM, AM offers the benefits of less material waste, reduced cost, and the ability to manufacture intricate details and complex geometries. The limitations of AM include the potential for expensive start-up costs, the limited range of dental materials available for printing, and the requirement for more postprocessing time.
For more than 20 years, SM technology has been widely used for the fabrication of ceramic restorations. Two distinct advantages of SM compared with AM are the wider selection of materials available for milling and the requirement for less postprocessing treatment to produce a higher degree of surface finish. Nevertheless, SM technology has some inherent drawbacks. Examples include the need to replace worn tools, the generation of material waste, the risk that microcracks will be produced during milling, and limitations in the duplication of surface geometry based on characteristics of the CNC (computer numerical control) machine, such as its working axis and the size of milling tools.4 Some dentists leverage the advantages of both AM and SM, tailoring their approach to meet the unique needs of each patient.
Two novel 3D-printed definitive and provisional crown resins manufactured by BEGO (VarseoSmile Crown Plus and VarseoSmile Temp) are distributed by Formlabs for commercial use as Permanent Crown Resin and Temporary CB Resin. The manufacturers claim that these are the first tooth-colored, ceramic-filled resins for 3D printing.5,6 However, research comparing the strength, reliability, and accuracy of these new materials to those of existing dental milling materials is sparse.
The success of a fixed restoration is partially dependent on its mechanical properties and accurate fit of the material. One key measurement for assessing a material’s mechanical properties is the flexural strength test, which quantifies how well a material or crown resists bending deflection under high masticatory stress. The accuracy of the manufacturing process can be evaluated via assessment of the marginal gap (or
A2 Esterification products of 4,4’-isopropylidenediphenol, ethoxylated and 2-methylprop-2-enoic acid (50-75 wt%), silanized dental glass, diphenyl(2,4,6trimethylbenzoyl) phosphine oxide (< 3 wt%)17
A2 Esterification products of 4,4’-isopropylidenediphenol, ethoxylated and 2-methylprop-2-enoic acid (50-75 wt%), silanized dental glass, diphenyl(2,4,6trimethylbenzoyl) phosphine oxide (< 2.5 wt%)18
clinical gap) and internal fit (or internal gap) of crowns.7-9 An accurate marginal gap is essential to minimize cement dissolution, marginal discoloration, bacterial colonization, formation of secondary caries, and periodontal disease. A good internal fit benefits crown retention, but poor internal fit may affect marginal adaptation.7 While consensus on a clinically suitable value for marginal gap remains elusive, the literature commonly cites a reported acceptable threshold of 120 µm.10,11
Several techniques have been used to measure the marginal gap and internal fit of crowns, including the cross-sectional method, silicone replica technique, triple scan method, microcomputed tomography (μ CT), and optical coherence tomography.9 Many studies that evaluated marginal gap and internal fit have used direct observation with loupes or a stereomicroscope to assess the marginal gap.12 However, a μCT scanner produces high-resolution images that enable nondestructive measurement the marginal gaps and internal fit of crowns from any angle and position in space.9,13,14
The purposes of the present study were to evaluate and compare (1) the flexural strength of milled and 3D-printed crown materials; and (2) the marginal gap and internal fit of milled lithium disilicate crowns, milled composite resin crowns, and 3D-printed definitive and provisional crowns using μCT. The null hypothesis was that there would be no differences in the flexural strength, marginal gap, or internal fit of the milled and 3D-printed restorations.
Methods
The study was designed to compare 4 different resin materials and 2 different methods for crown fabrication. The materials IPS e.max CAD (IEC; Ivoclar Vivadent) and Paradigm MZ100 Block (PMB; 3M) were used for milling, and Permanent Crown Resin (PCR; Formlabs) and Temporary CB Resin (TCR; Formlabs) were used for 3D printing (Table 1).15-18
A total of 80 specimens were tested: 15 bars per material for flexural strength testing, and 5 crowns per material for marginal gap and internal fit analyses. The effect size was estimated from previous literature.7,19 All tooth preparation, specimen preparation, laboratory testing, and data collection in this study were performed by a comprehensive dentistry resident with 5 years of clinical experience (M.F.).
Flexural strength testing
Specimen preparation
To evaluate the PCR and TCR materials, a rectangular bar (1.3 × 4.0 × 18.0 mm) was digitally designed as recommended by ISO 6872:2015 using computer-aided design software (Meshmixer, version 3.4.35, Autodesk) and exported in standard tessellation language (STL) format.20 The STL file was used to print the PCR and TCR bars (n = 15 per material) on an SLA 3D printer (Form 3B, Formlabs). For each 3D-printing material, the STL file was loaded into a slicing software (PreForm, version 3.21.0, Formlabs), and the bars were printed in 50-µm-thick layers on a stainless steel build platform (BP-CBSS-02, Formlabs). Supports were automatically generated, and any supports located on or near the testing surface were repositioned (Fig 1).
Once the bars were manufactured, they were placed in a resin washing station (Form Wash, Formlabs) filled with isopropyl alcohol (70%). After they were washed for 3 minutes, the bars were dried with compressed air until the surface appeared dry and lacked residual shine; they were then left to air dry for 30 minutes. The rafts, with supports still intact, were subsequently placed in the resin curing station (Form Cure, Formlabs) under dry conditions with the raft side down and cured at 60°C for 20 minutes. A handpiece with a cutting disc was used to separate the supports and the raft from the printed bars. The bars were
1. Restorative materials used in the study.
particle abraded with glass beads to remove residual coating at a maximum pressure of 1.5 bar for 10 seconds. Next, the bars were placed back in the curing station and postcured at 60°C for an additional 20 minutes, following the manufacturer’s instructions.18
To evaluate IEC and PMB materials, the blocks were sectioned into rectangular bars (1.3 × 4.0 × 18.0 mm) using a low-speed precision cutter (IsoMet, Buehler), as recommended by ISO 6872:2015. Any specimen with a visible defect was discarded. All specimens were carefully polished with 320and 600-grit silicon carbide abrasive paper (3M). The IEC bars were fired in a ceramic furnace (Programat P310, Ivoclar Vivadent) following the manufacturer’s instructions.21
Testing procedures
Flexural strength testing was completed in accordance with ISO 6872:2015.20 All specimens were tested in a universal testing machine (ElectroPuls 3000, Instron) with a crosshead speed of 1 mm/min, and data were recorded using a proprietary software (Bluehill, version 3, Instron).22 The flexural strength was obtained using the equation FS = 3Fl/(2 bd 2), where F is the loading force at the fracture point, l is the length of the support span (15 mm), b is the width of the beam specimen, and d is the depth. The parameters b and d were measured with electronic digital calipers (GA182, Grobet USA).
Weibull statistical analysis
Fifteen specimens were used for each group based on ISO 6872:2015. 20 The Weibull 2-parameter (σ 0 and m) distribution function is: (1),
where P f is the cumulative probability of failure, e is the natural exponent, σ (MPa) is the flexural strength, σ 0 (MPa) is the Weibull characteristic strength, and m is the Weibull modulus. The parameters σ 0 and m were calculated by using rank order statistics. For example, after the flexural strength (σ ) values for all 15 specimens were measured, the specimens were ranked in ascending order and assigned a P f value based on their ranking. This P f value was determined with the following equation:
where i represents 1, 2, 3, …, N of the i th datum in ascending order of the flexural strength (σi), and N is the total number of specimens tested. Next, equation 1 was rearranged into the following equation: (3),
where ln is the natural logarithm, m is the modulus, σi is the flexural strength, and σ0 is the Weibull characteristic strength.
The values derived from equation 3 were plotted on the ordinate axis of a graph against ln(σi) on the abscissa, from which a maximum likelihood estimation procedure was used to estimate the linear regression model. The slope and intercept of equation 3 yield m and m lnσ 0 , respectively. Then, σ 0 was solved from the intercept. When the characteristic strength is the strength value, P f = 63.2%.
The flexural data were analyzed with a t test and compared using 1-way analysis of variance (ANOVA) (α = 0.05).
Marginal gap and internal fit assessment
Specimen preparation
A mandibular left first molar typodont tooth (A5AN-200 tooth 19, Kilgore International) was mounted with adjacent teeth on a typodont and prepared for a full-coverage lithium disilicate crown following the manufacturer’s guidelines (circumferential 1.0-mm marginal width and 1.5-mm occlusal reduction). 23 The modified shoulder finish line was prepared with a modified, flat-end taper, fine diamond bur (NeoDiamond 847KR-016, Microcopy Dental).
After preparation, the typodont tooth was scanned with a chairside intraoral scanner (CEREC Primescan, Dentsply Sirona). The crown template was digitally designed with software (inLab, version 22.1, Dentsply Sirona). The cement space was set at 120 µm. The IEC and PMB crowns were manufactured with a 4-axis mill (CEREC MC XL, Dentsply Sirona). A new set of burs was installed prior to the milling of each material group. The IEC crowns were subjected to a crystallization firing procedure in a ceramic furnace (Programat P310) in accordance with the manufacturer’s instructions.21
(2),
Fig 1. Examples of 3D-printed crown and bar specimens. Fig 2. Microcomputed tomographic image showing points for measurement of marginal gap and internal fit. MG, marginal gap; AS, axial space; OS, occlusal space; CO, center occlusal.
Error bars represent the standard deviation. Means with the same letter are not significantly different (P > 0.05; 1-way ANOVA).
The 3D-printed crowns were fabricated using the same STL file used for the milled crowns. For each material, the STL file was loaded into the slicing software (PreForm 3.21.0), and the SLA printer (Form 3B) printed the crowns on a stainless steel build platform with the occlusal planes facing the platform. Supports were automatically generated, and any supports located on or near the margins were repositioned. Once the crowns were manufactured, they were postprocessed following the same method used for the 3D-printed bars used in flexural testing. The crowns were then cured with the occlusal plane facing upward. 24
Assessment procedures
The marginal gap and internal fit of each specimen were measured utilizing μCT (SkyScan 1172, Bruker). Each crown was stabilized on the typodont tooth preparation and then scanned 180 ° at a 0.4° rotational increment using a source voltage and current of 44 kV and 222 μA with a 0.5-mm Al filter and 8.31-μm image pixel size, resulting in 1048 × 2000 pixels per slice. The scanned images were reconstructed into 3D images using NRecon software (version 2.0, Bruker).
In each mesiodistal and buccolingual orientation, 5 vertical slices were assessed 100 slices apart. CTAn software (version 1.18, Bruker) was used to measure the marginal gap, axial space, occlusal space, and center occlusal size on each slice (Fig 2). Seven points of measurement were selected on each slice (2 for marginal gap, 2 for axial space, 2 for occlusal space, and 1 for center occlusal), resulting in a total of 70 points of measurements per crown.
The marginal gap was defined as the distance measured from the crown margin to the modified shoulder finish line.
Table 2. Comparison of the reliability parameters (Weibull modulus) among the 4 different materials (n = 15 per material).
The internal fit was measured as the closest 2 points from the intaglio of the crown to the axial and occlusal surfaces of the typodont tooth. The internal fit was defined as the combination of all axial space, occlusal space, and center occlusal measurements. The axial internal fit was determined by combining all axial space measurements, while the occlusal internal fit was defined as the combination of all occlusal space and center occlusal measurements.
Statistical analysis
The mean and SD values for marginal gaps and internal fit were captured for IEC, PMB, PCR, and TCR. The marginal gap and internal fit data were analyzed with a t test and compared using ANOVA with Tukey post hoc comparisons (α = 0.05).
Chart 1. Mean flexural strengths of milled and 3D-printed restorative materials (n = 15 per group).
Chart 2. Mean marginal gap and internal fit discrepancies of milled and 3D-printed crowns (n = 5 per group).
Error bars represent the standard deviation. Means with the same letter are not significantly different (P > 0.05; 3-way ANOVA with post hoc Tukey test).
Results
The highest (mean [SD]) flexural strength among all materials (335.52 [28.97] MPa), was demonstrated of the IEC group. Next highest was the PMB group (154.34 [21.03] MPa), followed by the PCR group (128.09 [7.30] MPa) and TCR group (126.29 [9.23] MPa). The ANOVA revealed statistically significant differences between the IEC and PMB groups as well as between both milled groups and the 3D-printed groups (F = 426.460; P < 0.001). The PCR group was not statistically significantly different from the TCR group (Chart 1). For the Weibull modulus, the PCR group (21.07) presented with the highest modulus, followed by the TCR group (16.52) and IEC group (13.70). The PMB group (8.77) showed the lowest modulus, indicating its poor reliability (Table 2).
According to the ANOVA, the IEC group (53.42 [31.99] µm) had statistically significantly smaller marginal gaps than TCR (72.27 [55.83] µm) (P < 0.001) but was not significantly different from the PCR (56.79 [43.04] µm) or PMB group (66.93 [61.23] µm) (Chart 2). The PMB group had the smallest internal fit discrepancy (87.44 [37.60] µm), but it was not significantly different from the internal fit of the PCR group (96.40 [54.23] µm), and the internal fit of the PCR group was not significantly different from that of the IEC group (104.92 [63.49] µm). No significant difference was found between the marginal gap of the TCR group and the internal fit of the PMB group. The greatest internal fit discrepancy was found in the TCR group (130.61 [65.16] µm), which was significantly greater than the discrepancies in the IEC, PMB, and PCR groups (P < 0.001).
The combined data of the milled specimens (IEC and PMB) and the combined data of the 3D-printed specimens (TCR and PCR) were analyzed to compare the marginal gap and internal
fit of milled vs 3D-printed restorations. The occlusal internal fit discrepancy of 3D-printed crowns (145.78 [51.30] µm) was significantly higher than that of milled crowns (124.54 [48.59] µm) (P < 0.001) (Chart 3). There was no statistically significant difference in marginal gap or axial internal fit between milled and 3D-printed crowns.
Discussion
The flexural strength and marginal gap data both showed statistically significant differences between the milled and 3D-printed definitive and provisional crown materials, so the null hypothesis was rejected. The flexural strength of IEC found in this study was comparable to values established in previous studies that utilized ISO 6872:2015 protocols.25,26 IEC was chosen to serve as a control in this study because it is a well-tested definitive crown material. PMB was chosen because it is commonly used by practitioners as a milled provisional material due to its physical properties, although it is marketed by the manufacturer as a definitive crown material. The flexural strength of PMB was found to be comparable to that reported in past studies.27,28 The flexural strength for TCR found in the literature (134 [17.51] MPa) was similar to the present findings.29 However, to the authors’ knowledge, no other literature has evaluated the permanent resin tested in the present study (PCR).
There was no statistically significant difference in the flexural strengths between the definitive and provisional resins for 3D printing (PCR and TCR). Both the permanent and temporary crown resins are composed of 4,4’-isopropylidenediphenol, also known as BPA, which is primarily used as a co-monomer in the production of polycarbonates.30
Error bars represent the standard deviation. Means with the same letter are not significantly different (P > 0.05; 3-way ANOVA with post hoc Tukey test).
2-Methylprop-2-enoic acid, also known as methacrylic acid, is widely used in the production of polymers, resins, and coatings as well as in the production of dental materials and adhesives.31 Silanized “dental glasses” are included for strength and esthetics, and diphenyl(2,4,6-trimethylbenzoyl) phosphine oxides are used as photoinitiators.5,17 However, the manufacturer has not released the exact percentages of the various components used in the material.18 Based on the results of this study, the similarity of the products could mean that a clinician would be able to achieve reasonably similar clinical results in terms of fracture resistance when using either the permanent or temporary 3D-printing resin.
In the present study, milled PMB exhibited higher flexural strength than 3D-printed PCR and TCR. This can be attributed to the method used to produce prefabricated resin blocks for computer-aided design/computer-aided manufacturing (CAD/ CAM) processes. Nguyen et al found that blocks fabricated with high-temperature/high-pressure polymerization showed a higher density and greater degree of cross-linking of the composite resin, which resulted in a significant increase in flexural strength, hardness, and density for CAD/CAM resin blocks, including the PMB material tested in the present study.27 A systematic review by Alzahrani et al concluded that milled materials fabricated under higher temperature and pressure contained a higher filler content, which resulted in lower porosity, voids, and residual monomer compared with 3D-printed resins.32 The Weibull outcomes of the present study suggested that the manufacturing process of the CAD/CAM blocks results in a less reliable reproducibility than 3D printing, but this is difficult to verify, since the manufacturing processes of the prefabricated blocks and printing resin are proprietary.
The flexural strength of all the definitive and provisional restorative materials used in the present study tested well above the minimum acceptable value of 50 MPa required by ISO 10477:2018 for polymer-based crown and veneering materials as well as the minimum acceptable value of 100 MPa required by ISO 6872:2015 for class 2 ceramics.20,32-35 Comparing the physical property values of these 3D-printed materials with the data reported in the literature is a complex task. Many preprocessing steps, such as variations in design, printing algorithms, supports, printing orientation, layer thickness, and testing procedures, can affect end values.33 Postprocessing factors such as postrinsing time, polishing methods, and storage can affect strength as well.33 The protocols used in the present study followed most of the manufacturer’s instructions, many of which have been supported by favorable findings in the literature, such as using a crown and bar build orientation in a 0° horizontal position, which maximizes flexural strength, and avoiding excessive rinsing, which can decrease flexural strength.33,36
The outcome data varied for marginal gap and internal fit analyses. For marginal gap, IEC performed the best, but its results were statistically similar to those of PMB and PCR. For internal fit, PMB produced the smallest discrepancy, which is consistent with studies showing that milled resins produce smoother marginal edges than milled ceramics.28 Yildirim et al found that resin blocks result in the smallest marginal deviation and internal fit when compared with glass ceramics and hybrid ceramics, which supports the finding that PMB had the smallest internal fit discrepancy in the present study.14
The (mean [SD]) marginal gap of the IEC group in the present study (53.42 [31.99] µm) was similar to the findings of SadidZadeh et al (77.2 [17] µm) but much smaller than that reported
Chart 3. Comparison of mean marginal gap and internal fit discrepancies in milled vs 3D-printed crowns (n = 10 per manufacturing method).
in other studies, such as the previously mentioned study by Yildirim et al (155.5 [33.0] µm).14,37 The smaller IEC marginal gap in the present study could be due to a smoother typodont tooth preparation, the use of a more advanced and accurate intraoral scanner, and improved software algorithms and milling strategies. The smaller marginal gap and internal fit values in the PCR group compared with the TCR group could be due to a difference in composition that leads to less polymerization shrinkage. It is worth noting that all mean marginal gap discrepancies of crown materials in the present study were less than the 120-μm threshold considered acceptable according to the literature, although CAD/CAM crowns have been creating margins well below this standard.10,11
No statistically significant differences were found in marginal gap or axial internal fit between milled and 3D-printed crowns. However, the occlusal internal fit discrepancy of 3D-printed crowns was significantly larger than that of milled restorations. This could be attributed to the manufacturing method, as 3D-printed crowns are made in a stepwise fashion that requires larger cement space. The manufacturer recommends 20 to 90 μm of cement gap for PCR and 10 to 70 μm of cement gap for TCR.24 However, Shin et al found that the smallest marginal gap (81.0 [35.7] µm), axio-occlusal gap (78.0 [27.6] µm), and occlusal gap (103.5 [27.6] µm) values of 3D-printed resin crowns were obtained with a 70-μm cement gap.38 There seems to be a lack of consensus for the ideal cement space for 3D-printed restorations due to wide variations in crown composition, scanning and printing technologies, and polymerization variations. Crown build orientation can also play a role; Khanlar et al found that a buccal placement (90°) print orientation had the smallest marginal gap and internal fit discrepancies and that occlusally oriented crowns had the largest marginal gap.19
One limitation of the present study is the isopropyl alcohol used. The manufacturer recommends washing both 3D-printed materials with at least a 90% concentration of isopropyl alcohol, but 70% isopropyl alcohol was used due to supply limitations. This could prevent the complete removal of excess resin from within the crown, which could alter the marginal gaps and internal fit of the crown. Another limitation is that the bar specimens used in flexural strength testing did not undergo thermocycling to simulate deterioration in the oral environment, and the literature has consistently shown lower values after this process. 34 It would be reasonable to assume that the flexural strengths of materials tested in this study would be lower after thermocycling but still fall within clinically acceptable limits.
Another limitation is the use of a single evaluator for marginal analysis. Each crown took about 90 minutes to prepare, including 45 minutes to scan in the μCT and another 45 minutes to mark all 70 measurements. Each point marked was subject to the operator’s perception, and evaluator fatigue over time could have led to varying results for marginal gap and internal fit measurements. A modern quantitative method for studying the accuracy of marginal gaps and internal fit of crowns to a tooth preparation is by calculating the root mean square of discrepancies between 2 STL files in 3D analysis software. 39-41 This would have been a less time-consuming method; however, miscalculations may result from inaccurate overlapping of the scanned
data, and there is no consensus in the literature on which method is the most accurate.9 El-Ashkar et al found no statistically significant difference between using 3D superimposition analysis and using a direct viewing method with a stereoscope to determine marginal gap.41
When utilizing 3D-printed materials for permanent restorations, providers need to verify that these materials possess attributes comparable to those of milled materials. Clinicians should be cautious if utilizing the newly introduced PCR as a definitive crown material with the manufacturer’s recommended minimum thickness (1.0 mm) in areas of high stress.18 Additional investigations are recommended to evaluate the impact of thermocycling on 3D-printed materials and the influences of different percentages of isopropyl alcohol, printing parameters, and printing orientation on the physical properties and marginal and internal adaptation of restorations. The effects of water sorption, wear characteristics, color stability, and failure modality must also be investigated to validate these materials for clinical practice.
Conclusion
Milled resins exhibited higher flexural strength than 3D-printed resins. There was no significant difference in flexural strength between the 3D-printed definitive and provisional crown resins. The marginal gap and internal fit of crowns fabricated with 3D printing were comparable to those of milled crowns, with all mean marginal gaps within the clinically acceptable limit of less than 120 μm
Author affiliations
2-Year Advanced Education in General Dentistry Residency Program, Fort Cavazos, Texas (Firestone, Hu, Masterson, Paek); Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University of the Health Sciences, Joint Base San Antonio–Fort Sam Houston (Firestone, Hu, Masterson, Paek); United States Air Force Dental Research & Consultation Service, Joint Base San Antonio–Fort Sam Houston, Texas (Raimondi, Lien).
Correspondence
Eric Hu, DMD, MS, FACP (eric.c.hu.mil@health.mil).
Conflicts of interest
None reported.
Funding
This study was funded in part by the Carl R. Darnall Army Medical Center, Fort Cavazos, Texas.
Disclaimer
The identification of specific products, scientific instrumentation, or organizations is considered an integral part of the scientific endeavor and does not constitute endorsement or implied endorsement on the part of the authors, US Department of Defense, or any component agency. The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Army, Department of the Air Force, Uniformed Services University
of the Health Sciences, Defense Health Agency, Department of Defense, or the United States government.
Acknowledgments
The authors thank Karl H. Wenger, PhD; Mathew Frazier, PT, DPT, MS, ATC; and Dawn Beaver, MS, for support with research protocol submissions.
Meeting presentation
This research was presented at the 2023 Carl R. Darnall Army Medical Center Research Day, May 18, 2023.
References
1. Methani MM, Revilla-León M, Zandinejad A. The potential of additive manufacturing technologies and their processing parameters for the fabrication of all-ceramic crowns: a review. J Esthet Restor Dent. 2020;32(2):182-192. doi:10.1111/jerd.12535
3. Revilla-León M, Özcan M. Additive manufacturing technologies used for processing polymers: current status and potential application in prosthetic dentistry. J Prosthodont. 2019;28(2):146158. doi:10.1111/jopr.12801
4. Al Hamad KQ, Al-Rashdan BA, Ayyad JQ, et al. Additive manufacturing of dental ceramics: a systematic review and meta-analysis. J Prosthodont. 2022;31(8):e67-e86. doi:10.1111/ jopr.13553
6. Formlabs. High-accuracy 3D printing materials for dental labs and practices. Accessed May 26, 2023. https://dental.formlabs.com/materials/
7. Marouki C, Shamon A, Svanborg P. Evaluation of fit and accuracy of single crowns fabricated from self-glazed zirconia compared with milled zirconia. J Prosthet Dent. 2024;131(6):11051110. doi:10.1016/j.prosdent.2023.02.016
8. Sanchez-Lara A, Hosney S, Lampraki E, et al. Evaluation of marginal and internal fit of single crowns manufactured with an analog workflow and three CAD-CAM systems: a prospective clinical study. J Prosthodont. 2023;32(8):689-696. doi:10.1111/jopr.13675
9. Son K, Lee S, Kang SH, et al. A comparison study of marginal and internal fit assessment methods for fixed dental prostheses. J Clin Med. 2019;8(6):785. doi:10.3390/jcm8060785
10. McLean JW, von Fraunhofer JA. The estimation of cement film thickness by an in vivo technique. Br Dent J. 1971;131(3):107-111. doi:10.1038/sj.bdj.4802708
11. Mitchell CA, Pintado MR, Douglas WH. Nondestructive, in vitro quantification of crown margins. J Prosthet Dent. 2001;85(6):575-584. doi:10.1067/mpr.2001.114268
12. Gold SA, Ferracane JL, da Costa J. Effect of crystallization firing on marginal gap of CAD/CAM fabricated lithium disilicate crowns. J Prosthodont. 2018;27(1):63-66. doi:10.1111/jopr.12638
13. Alfaro DP, Ruse ND, Carvalho RM, Wyatt CC. Assessment of the internal fit of lithium disilicate crowns using micro-CT. J Prosthodont. 2015;24(5):381-386. doi:10.1111/jopr.12274
14. Yildirim G, Uzun IH, Keles A. Evaluation of marginal and internal adaptation of hybrid and nanoceramic systems with microcomputed tomography: an in vitro study. J Prosthet Dent. 2017;118(2):200-207. doi:10.1016/j.prosdent.2016.11.005
15. Ivoclar Vivadent. IPS e.max CAD. Scientific documentation. March 2011. Accessed March 23, 2022. https://ivodent.hu/__docs/768_865d8476b1360c8ac461ae57f9c6b3c4.pdf
17. Formlabs. Permanent Crown. Safety data sheet. August 23, 2021. Accessed March 27, 2023. https://formlabs-media.formlabs.com/datasheets/ENUS_Safety_Data_Sheet_-_Permanent_ Crown.pdf
18. Formlabs. Temporary Crown. Safety data sheet. March 9, 2021 Accessed March 12, 2022. https://formlabs-media.formlabs.com/datasheets/2001437-SDS-ENUS-0.pdf
19. Khanlar LN, Francis C, Basir Barmak A, Rios ALS, Ashtiani RE, Zandinejad A. Effect of a new support design on the marginal and internal gap of additively manufactured interim crowns using direct light deposition technology. J Prosthodont. 2024;33(2):188-194. doi:10.1111/ jopr.13668
20. ISO. ISO 6872:2015. Dentistry—Ceramic Materials. ISO; 2015.
22. Lawson NC, Bansal R, Burgess JO. Wear, strength, modulus and hardness of CAD/CAM restorative materials. Dent Mater. 2016;32(11):e275-e283. doi:10.1016/j.dental.2016.08.222
23. Ivoclar Vivadent. IPS e.max CAD. Instructions for use. April 10, 2022. Accessed March 14, 2023. https://www.ivoclar.com/en_li/eifu?brand=IPS+e.max+CAD
24. Formlabs. 3D printing permanent crowns with the Form 3B. Application guide. Accessed August June 6, 2022. https://dental.formlabs.com/indications/permanent-crowns/guide/
25. Al-Thobity AM, Alsalman A. Flexural properties of three lithium disilicate materials: an in vitro evaluation. Saudi Dent J. 2021;33(7):620-627. doi:10.1016/j.sdentj.2020.07.004
26. Attar EA, Aldharrab A, Ajaj R. Flexural strength properties of five different monolithic computeraided design/computer-aided manufacturing ceramic materials: an in vitro study. Cureus. 2023;15(3):e36958. doi:10.7759/cureus.36958
28. Awada A, Nathanson D. Mechanical properties of resin-ceramic CAD/CAM restorative materials. J Prosthet Dent. 2015;114(4):587-593. doi:10.1016/j.prosdent.2015.04.016
29. Crenn MJ, Rohman G, Fromentin O, Benoit A. Polylactic acid as a biocompatible polymer for three-dimensional printing of interim prosthesis: mechanical characterization. Dent Mater. 2022;41(1):110-116. doi:10.4012/dmj.2021-151
30. Joint Research Centre: Institute for Health and Consumer Protection; Olsson H, Aschberger K, Munn S, et al, eds. Updated European Union risk assessment report: 4,4’-isopropylidenediphenol (bisphenol-A): environment addendum of February 2008. 2010. doi:10.2788/40195
31. 2-Methylprop-2-enoic acid;propane-1,3-diol. BenchChem.com. Accessed August May 26, 2023. www.benchchem.com/product/b1591248
32. Alzahrani SJ, Hajjaj MS, Azhari AA, Ahmed WM, Yeslam HE, Carvalho RM. Mechanical properties of three-dimensional printed provisional resin materials for crown and fixed dental prosthesis: a systematic review. Bioengineering (Basel). 2023;10(6):663. doi:10.3390/bioengineering10060663
33. Gad MM, Fouda SM. Factors affecting flexural strength of 3D-printed resins: a systematic review. J Prosthodont. 2023;32(S1):96-110. doi:10.1111/jopr.13640
34. Scherer M, Al-Haj Husain N, Barmak AB, Kois JC, Özcan M, Revilla-León M. Influence of the layer thickness on the flexural strength of aged and nonaged additively manufactured interim dental material. J Prosthodont. 2023;32(S1):68-73. doi:10.1111/jopr.13582
36. Al-Dulaijan YA, Alsulaimi L, Alotaibi R, et al. Effect of printing orientation and postcuring time on the flexural strength of 3D-printed resins. J Prosthodont. 2023;32(S1):45-52. doi:10.1111/ jopr.13572
37. Sadid-Zadeh R, Li R, Miller LM, Simon M. Effect of fabrication technique on the marginal discrepancy and resistance of lithium disilicate crowns: an in vitro study. J Prosthodont. 2019;28(9):1005-1010. doi:10.1111/jopr.13014
38. Shin H, Kang YJ, Kim H, Kim JH. Effect of cement space settings on the marginal and internal fit of 3D-printed definitive resin crowns. J Prosthet Dent. 2023;S0022-3913(23)00187-7. doi:10.1016/j.prosdent.2023.03.021
39. Lai YC, Yang CC, Levon JA, Chu TG, Morton D, Lin WS. The effects of additive manufacturing technologies and finish line designs on the trueness and dimensional stability of 3D-printed dies. J Prosthodont. 2023;32(6):519-526. doi:10.1111/jopr.13588
40. Yilmaz B, Donmez MB, Kahveci Ç, et al. Effect of printing layer thickness on the trueness and fit of additively manufactured removable dies. J Prosthet Dent. 2022;128(6):1318.e1-1318.e9. doi:10.1016/j.prosdent.2022.10.011
41. El-Ashkar A, Taymour M, El-Tannir A. Evaluation of the marginal and internal gaps of partially crystallized versus fully crystallized zirconia-reinforced lithium silicate CAD-CAM crowns: an in vitro comparison of the silicone replica technique, direct view, and 3-dimensional superimposition analysis. J Prosthet Dent. 2023;129(5):769-776. doi:10.1016/j.prosdent.2021.07.024
GENERAL DENTISTRY SELF-INSTRUCTION
Exercise No. GD537, 2 CE Credits
Fixed Prosthodontics
Subject Code: 610
The 15 questions for this exercise are based on the article “Comparison of flexural strength, marginal gap, and internal fit of milled and 3D-printed crown materials” on pages 38-45. This exercise was developed by Ralph Pruette, DDS, in association with the General Dentistry Self-Instruction committee.
1. Additive manufacturing is defined as the process of joining materials (usually layer upon layer) to make 3D objects from 2D model data. There are 7 general types of additive manufacturing.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
2. All of the following are benefits of additive manufacturing compared to subtractive manufacturing except one. Which is the exception?
A. less waste
B. reduced cost
C. wide range of materials
D. ability to manufacture intricate detail
3. Marginal gaps and internal fit were evaluated using ________.
A. loupes
B. stereomicroscopy
C. electron microscopy
D. microcomputed tomography
4. The 2 milled materials were ________ and ________.
A. IPS e.max CAD (IEC); Paradigm MZ100 Block (PMB)
B. IEC; Permanent Crown Resin (PCR)
C. PMB; PCR
D. PCR; Temporary CB Resin (TCR)
5. A total of ___ specimens were tested for flexural strength.
A. 20
B. 40
C. 60
D. 80
Reading the article and successfully completing this exercise will enable you to:
• understand the benefits and limitations of additive and subtractive manufacturing;
• know the comparative flexural strengths of milled and 3D-printed crowns; and
• know the comparative marginal gaps and internal fits of milled and 3D-printed crowns.
Answers must be submitted online at agd.org/self-instruction by October 31, 2025.
6. Marginal gap and internal fit analyses were conducted on ___ crowns per material.
A. 5
B. 6
C. 8
D. 10
7. For the marginal gap and internal fit analyses, a ________ typodont tooth was prepared.
A. maxillary right first molar
B. maxillary right first premolar
C. mandibular left first molar
D. mandibular left first premolar
8. The prepared typodont tooth was scanned using the ______ scanner.
A. iTero Element 5D
B. 3Shape Trios 3
C. CEREC Primescan
D. KaVo X 500
9. In each mesiodistal and buccolingual orientation, ___ vertical slices were assessed ____ slices apart.
A. 5; 100
B. 10; 200
C. 5; 70
D. 10; 140
10. The _____ group displayed the highest flexural strength among the materials.
A. IEC
B. PMB
C. PCR
D. TCR
11. The IEC group had a statistically significantly smaller mean marginal gap than the PMB group. The marginal gaps of the IEC and PCR groups were not significantly different.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second true.
D. Both statements are false.
12. The greatest internal fit discrepancy was found in the ____ group.
A. IEC
B. PMB
C. PCR
D. TCR
13. The ISO recommends a minimum flexural strength of ____ MPa for polymer-based crown and veneering materials.
A. 25
B. 50
C. 75
D. 100
14. _____ produced the smallest discrepancy for internal fit.
A. IEC
B. PMB
C. PCR
D. TCRF
15. The ____ and ____ groups had marginal gaps of less than 60 μm.
A. IEC; PCR
B. PMB; TCR
C. PCR; TCR
D. IEC; TCR
Clear aligner therapy and symptoms of temporomandibular disorders: a case report
The etiology of temporomandibular disorders (TMDs) is remarkably diverse. This case report highlights the use of clear aligners as a probable cofactor of TMD in an adult patient. A 56-year-old woman who presented with a chief concern of crowding was missing teeth in both arches and had generalized tooth wear, an indistinct history of temporomandibular joint musculoskeletal pain, and a self-reported history of clenching. Based on the patient’s preferences, clear aligner therapy (CAT) was initiated with a limited treatment goal of providing improved esthetics by reducing the overjet, expanding the arches, and aligning the anterior teeth. A few weeks into CAT, the patient developed acute masticatory facial pain. Therefore, the course of CAT was adjusted in favor of an individualized protocol to alleviate her occlusal symptoms until orthodontic treatment was completed. Dental providers must consider the potential contributory role of CAT in TMDs in patients who adapt poorly to occlusal changes and offer a patient-centered approach to manage the problem.
Temporomandibular disorders (TMDs) are a group of multifactorial conditions of the stomatognathic system that commonly manifest as pain or dysfunction of the masticatory muscles, temporomandibular joints (TMJs), and/ or associated structures. There is a long history of controversy regarding the relationship between occlusion and various TMD symptoms, and the relationship is still poorly understood. From a scientific standpoint, it is important to emphasize that a cause-effect relationship is far too simple to explain the etiology of a complex phenomenon such as TMD-related pain. Nevertheless, inadequate understanding of scientific research may lead the average dental provider to misinterpret the complex relationship between TMD symptoms such as orofacial pain and dental occlusion.
Although a cause-effect relationship alone cannot explain TMDs, possible interactions between existing cofactors should not be ignored. According to the National Institutes of Health, as many as 30 factors are reported to cause TMDs.1 Since these are multifactorial conditions, studying TMDs in a univariate model is not recommended. Rather, TMDs must be studied in a multivariate pattern to relate how multiple factors influence their etiology.2 The various etiologic and contributing factors include trauma (eg, whiplash injury, road traffic accidents, and endotracheal intubation); psychological factors (eg, alexithymia, mood or personality disorder, stress, and depression); genetic factors and heredity; systemic diseases; bruxism; and sex and advancing age (postmenopausal women aged 45 to 64 years are more susceptible). 3-11 Although the topic of TMDs has been extensively studied, consensus among dental providers regarding the etiology and other aspects is still lacking. Due to the complex multifactorial nature and the contributing factors, many aspects of TMDs are still unclear, which presents a clinical challenge.12
Clear aligner therapy (CAT) has been gaining popularity over the last decade because clear aligners make it easy to maintain good oral hygiene, are convenient, and, most importantly, are minimally visible to observers.13 CAT has offered an alternative treatment possibility that decreases patients’ pain levels and anxiety and improves their quality of life.1 It has been reported that there are no significant changes in occlusion or muscle activity during the shortterm retention period.14 To the authors’ knowledge, facial pain related to CAT has not been widely documented. This report describes a case in which the use of CAT exacerbated TMD symptoms. The orthodontic treatment with CAT was altered, thereby allowing the patient to continue orthodontic treatment while relieving symptoms of orofacial pain. Providers should be aware that in some patients, CAT may exacerbate factors leading to TMD symptoms. This
possibility should be explained to the patient at the time of consent, and the provider should be prepared to manage these symptoms if they occur.
Case report
A 56-year-old woman presented to the orthodontic clinic at the College of Dentistry, University of Kentucky, Lexington, for assessment of crowding in her maxillary and mandibular arches. The patient reported a history of clenching with no prior history of pain or other TMD symptoms. Her medical history was found to be noncontributory. When asked about her motivation for orthodontic treatment, she expressed being self-conscious of her smile. She was highly motivated for CAT and wanted to avoid traditional fixed appliances of all types.
Evaluation procedures
The soft tissue evaluation revealed a healthy thin biotype with root prominence, a normal profile with thin and retrusive lips, decreased facial convexity, and no signs or symptoms of muscle tenderness or TMJ-related issues. The intraoral examination revealed that the patient was missing her maxillary right lateral incisor and mandibular right canine, but she could not remember the history. She was also missing her mandibular left second molar, which had been extracted years ago, causing supraeruption of the maxillary left second molar. All third molars had been extracted due to impaction.
The patient had an end-on molar occlusion and excess overjet with a Bolton discrepancy of 2.6 mm of excess maxillary teeth. The Bolton discrepancy is caused by the difference in tooth mass between maxillary and mandibular anterior teeth as a result of missing teeth. The cephalometric radiograph revealed bimaxillary protrusion with a Class III tendency (Fig 1). Both the maxillary and mandibular teeth demonstrated mild anterior crowding, and there was a significant midline discrepancy of the midsagittal plane due to missing teeth. Both the maxillary and mandibular midlines were displaced to the right, with more severity in the maxillary arch. Generalized tooth wear was noted on the incisal edges and cusp tips, providing group function during eccentric movement. No functional shift was detected.
The panoramic radiograph revealed a flatter right condyle with no related TMJ pain or dysfunction (Fig 2). Figure 3 shows pretreatment intraoral scans.
Treatment
The patient was offered a comprehensive multidisciplinary orthodontic plan that aimed to correct all occlusal problems, including the midline discrepancy, supraerupted molar, and management of missing teeth. A second limited treatment option was presented that addressed her chief esthetic complaint. She selected the short treatment with no restorative options, in keeping with her initial treatment interest. The treatment objective was therefore limited to providing improved esthetics, given her preference for rapid, noninvasive treatment to align the anterior teeth but maintain good function and stability. CAT was planned to reduce the overjet, expand the arches, and align the anterior teeth.
Fig 1. Pretreatment cephalometric radiograph.
Fig 2. Pretreatment panoramic radiograph.
Fig 3. Pretreatment intraoral scans.
When CAT started, the patient was instructed to follow the recommended protocol of wearing each set of trays full time (except during meals) for 2 weeks. Initially, the patient was satisfied with the progress and complied with aligner wear. However, during the third week of treatment, the patient began to experience mild pain and soreness in the preauricular area of her face. The patient canceled her periodic orthodontic visit and visited an otolaryngologist, seeking pain relief. She was diagnosed with ear and sinus infections, and antibiotics were prescribed for her condition. When the symptoms did not resolve, she was referred to the orthodontic clinic.
The patient presented to her next orthodontic appointment and reported that she was experiencing pain in the masseter and preauricular areas. She rated the pain intensity as 7/10. She also reported that the pain intensified with jaw use and she had been aware of some increased clenching. The clinical examination revealed that she felt pain during palpation of the right masseter and temporalis muscles. The patient was referred to an orofacial pain specialist, and her pain was managed with routine home care, including relaxing exercises for the mandible, a softer diet, stress reduction, avoiding clenching, hot and cold compresses, and an over-the-counter anti-inflammatory pain medication.
A few months into the initial orthodontic treatment, the patient was following the established CAT protocol but continued to report orofacial pain symptoms that had not been resolved with routine home care. The patient was closely monitored with weekly orthodontic visits to investigate the source of the symptoms.
Over time, the patient became emotionally stressed due to the prolonged pain and poor sleep. She was also frustrated because the orthodontic treatment goals had not yet been accomplished. It was necessary to reprioritize and revise the original treatment goal. Symptom reduction became the primary treatment goal. The patient was first educated about the relationship between tooth clenching and emotional stress. The patient was informed that the disorder is benign and reversible and can be managed with some relatively simple behavioral changes. She was told that some patients have increased sensitivity to occlusal changes, and this may produce increased tension in the muscles, resulting in pain. This pain can lead to a protective muscle response, resulting in additional tension and pain. The increased pain can also increase emotional stress, prolonging the condition. The patient was encouraged to become more aware of the tension in the muscles, relax the jaw, and keep the teeth apart.
To obtain immediate pain relief, the patient was instructed to discontinue wearing the clear aligners for 1 week while she learned to reduce the tension in her jaw muscles. In 1 week, her pain was reduced to 2/10. The patient was then asked to resume CAT but only for nighttime use. For this patient, limiting the use of the aligners to nighttime allowed orthodontic tooth movement with minimum TMD symptoms.
A new scan was sent to the aligner manufacturer to create a new series of aligners that compensated for the lack of daytime wear. The forces of dental movements were increased in magnitude, while the adjustment intervals were extended to 3 to 4 weeks’ use for each set of aligners. Moreover, no attachments were placed, as they were a source of irritation for this patient.
The patient was closely monitored for TMD symptoms and orthodontic progress. The patient reported a favorable reduction of her symptoms when use of the aligners was limited to nighttime. She also indicated that learning about the relationships among muscle tension, emotional stress, and pain was beneficial, and she continued to utilize the skills she had acquired.
The patient continued to follow the new CAT protocol without experiencing TMD symptoms. After several months, the orthodontic treatment had fully accomplished the limited treatment objective, and the patient was satisfied with the results. Her functional occlusion was checked and found to be without interferences, and posttreatment scans and radiographs were taken (Fig 4). Superimposition of the pretreatment and posttreatment scans showed the successful but minor orthodontic changes (Fig 5).
Discussion
This case report demonstrates that common acute muscle TMD pain can occur in patients undergoing dental therapy. Despite the lack of evidence establishing a direct correlation between orofacial pain and occlusion, an enhanced critical thinking approach to such a case encourages the dental provider to help resolve the symptoms based on the available clinical evidence. A
Fig 4. Posttreatment intraoral scans.
Fig 5. Superimposition of pretreatment (blue) and posttreatment (white) scans showing arch expansion and minor alignment correction.
common factor that can initiate muscle symptoms is increased activity of the masticatory muscle secondary to various events. In some patients, this muscle response may be initiated by an acute change in the occlusal condition. This is commonly seen in the practice of general dentistry after the placement of a high crown; the muscles can experience protective co-contraction in an attempt to avoid a poorly fitting crown. This results in an increase in tonicity, which can lead to pain. Clear aligners are not initially designed to offer a stable occlusal condition, and this sudden change can initiate a similar protective response, leading to muscle pain. Patients who are also experiencing emotional stress and/or increased anxiety may be less tolerant of this change and more vulnerable to this increased muscle response. Once the pain has begun, the pain itself can reinitiate more protective co-contraction, leading to a self-perpetuating pain cycle.15
When a condition occurs secondary to the placement of a high crown, the patient will often immediately contact the dentist to report the problem. The dentist will adjust the tooth to fit proper occlusion, and the pain will resolve. The same condition is likely true when the acute change in occlusion is initiated by an aligner. However, a problem may arise if the clinician does not recognize the patient’s response to the treatment and allows the patient to continue with CAT based on the belief that occlusion and TMD symptoms are unrelated. This often results in a prolonged condition of local myalgia, where the pain becomes a self-sustaining cycle. At this point, the pain will contribute to an increase in the patient’s emotional stress and produce more anxiety. The clinician must recognize this muscle pain condition and effectively address it.
For the patient in this case report, the masticatory pain initially manifested as pain in the preauricular area and the ear. This is a very common pain referral pattern. The patient then independently sought treatment for ear pain, which was misdiagnosed as an ear infection. This is also a common scenario for TMD patients and unfortunately prolongs the pain, increasing stress and frustration for these patients.
Le Bell et al studied the effects of adding an acute occlusal interference to 2 different asymptomatic patient groups.16 One group had never experienced any TMDs, and the other had a history of TMDs but was not experiencing symptoms at the time of the study. Both groups experienced mild TMD symptoms during the experimental period. Once the interference was eliminated, pain was quickly resolved in the group who had never experienced TMDs. However, the group that had a history of TMDs had a far longer period of recovery from the experimental interference. This suggests that some patients may be less adaptable than others regarding changes in their occlusal condition and may reflect the experience of the patient reported in the present case. Le Bell et al recommended future research to identify these “poor adaptors,” as their course of treatment may be more challenging.16
Li and Leung summarized all of the contributing factors related to TMD pain in their review of the condition and its management.17 They divided the etiology into 2 components, physical and psychosocial. Physical factors are myogenous (related to muscles) or arthrogenous (related to joints) in
origin, and psychosocial factors that contribute to the etiology of TMDs include depression and stress. Occlusal disturbances and bruxism are also considered etiologic factors for TMDs.18 Some studies suggest that traditional orthodontic treatment is not a pertinent factor in TMDs.19-21 Some dentists believe that CAT helps alleviate preexisting TMDs. One explanation for this belief is the inference that the aligners’ smooth surface and flexible material may help distribute forces and reduce the impact of grinding, acting as a temporary nightguard. Schupp et al stated that clear aligners (Invisalign) are comfortable, invisible, and a powerful instrument for treating craniomandibular disorders (including TMDs).22 However, a systematic review reported inconclusive evidence regarding the superiority of clear aligners in resolving TMJ symptoms when compared with conventional orthodontics due to differing opinions in various articles.23 Concerns about potential relationships between TMDs and orthodontics have opened conversations to differing opinions.24 Whether to address TMD pain before orthodontic treatment begins or to pause orthodontic treatment if the pain is still a dilemma for clinicians. It is reported that CAT is not associated with the sleep bruxism index but can reduce tonic contractions.25 In the present case, however, it appeared that CAT might have been a cofactor in lowering the threshold, leading to orofacial symptoms for this patient. These complex multifactorial phenomena cannot be explained by a simple cause-effect relationship; rather, it is an intricate interaction between factors as they coexist. The aim of this report is not to blame CAT therapy for causing TMD symptoms in this patient but rather to invite all providers to consider scientifically based practices when clear evidence is lacking.
Patients with active TMD symptoms should not receive any orthodontic treatment without clearance from an orofacial pain specialist. Managing TMDs often requires a multidisciplinary approach. The clinician should carefully assess the severity of TMD symptoms and consider a range of factors that might be contributing to the disorder. The multidisciplinary approach promotes an in-depth evaluation of contributing factors and holistic treatment approaches and improves treatment outcomes and patient satisfaction. Garrios-Pedros et al classified TMD treatment options for a multidisciplinary approach, or patient-centered care, into 4 categories: (1) odontology, consisting of intraoral orthopedic devices; (2) physiotherapy, including electrotherapy, manual therapy, exercise, brain exercise, and graded activity; (3) drugs and surgery, including corticosteroids, nonsteroidal anti-inflammatory drugs, arthrocentesis, arthroscopy, and open surgery; and (4) psychology, including relaxation techniques, cognitive behavioral therapy, and self-management.26 Patient education and management also play a role in the successful treatment of TMDs during orthodontic treatment.
The assumption that CAT should have positive effects on TMJs has no strong supporting evidence. As occlusal coverage of any kind can serve as a temporary balanced occlusion, care should be taken in treating any adult with clear aligners. CAT can be very attractive to dental practitioners as it simplifies the treatment flow for the provider and the patient. Limited treatment is a common goal for adult patients, as these
patients present with specific desires and variable constraints; as a result, limited records can be sufficient for establishing an initial diagnosis. However, the absence of a comprehensive clinical diagnosis can cause major issues in some cases, especially if a significant functional shift exists. As these shifts may not be visible in centric occlusion, clear aligners can function as a deprogramming device on the occlusion, unmasking a nonfunctional occlusion and/or introducing a factor that contributes to TMDs.
It is import for the dental provider to involve the patient in treatment choices. Persistent facial pain increases anxiety, and the patient’s motivation and attitude toward orthodontic treatment can change. This attitude shift can also affect the patient’s relationship and interactions with the provider, as, in the patient’s mind, this pain and suffering was introduced by the CAT and provider. When this occurs, the provider must show support and listen to the patient while maintaining objective and professional communication. Education to reduce the pain-anxiety loop and improve tolerance should be provided until the issue is resolved.
In the present case, the protocol for addressing TMD symptoms was a customized treatment designed to reduce pain without stopping the orthodontic tooth movement. The course of orthodontic treatment was altered, and basic behavioral education was introduced. The aligners may have also served as temporary nightguards that may have alleviated nighttime clenching while they advanced the orthodontic treatment goals. The protocol adjustment may differ for other patients based on their specific symptoms and contributing factors.
Proper patient education regarding TMDs and CAT is essential for patients with risk factors. Better treatment results are observed in patients who were provided with detailed information about their condition, which helped reduce anxiety, fear, and depression in patients with TMDs.27 Patients should be informed about the potential risks and benefits of CAT, and realistic expectations should be set.
Conclusion
Severe, acute orofacial pain may arise during orthodontic treatment that has simple and limited goals. In this context, CAT differs from fixed appliance therapy in having occlusal coverage that may initiate unpredictable responses for a subgroup of poorly adapting patients, especially adults. In the present case, a patient who opted for a limited treatment objective of improved esthetics developed acute masticatory facial pain several weeks into CAT. The TMD symptoms were addressed as soon as they were reported, the patient was monitored to investigate other contributing and etiologic factors, and the treatment plan was changed to address the patient’s needs. The adjusted protocol alleviated the patient’s occlusal symptoms, allowing satisfactory completion of orthodontic treatment.
Author affiliations
Division of Orthodontics, Department of Oral Health Science, College of Dentistry, University of Kentucky, Lexington (Sharab, Shafi, Butul); College of Dentistry, University of Kentucky, Lexington (Okeson).
Correspondence
Lina Sharab, DDS, MS, MSc (lina.sharab@uky.edu).
Conflicts of interest
None reported.
References
1. Gao M, Yan X, Zhao R, et al. Comparison of pain perception, anxiety, and impacts on oral health-related quality of life between patients receiving clear aligners and fixed appliances during the initial stage of orthodontic treatment. Eur J Orthod. 2021;43(3):353-359. doi:10.1093/ejo/cjaa037
2. Landi N, Manfredini D, Tognini F, Romagnoli M, Bosco M. Quantification of the relative risk of multiple occlusal variables for muscle disorders of the stomatognathic system. J Prosthet Dent. 2004;92(2):190-195. doi:10.1016/jprosdent.2004.05.013
3. Salé H, Isberg A. Delayed temporomandibular joint pain and dysfunction induced by whiplash trauma: a controlled prospective study. J Am Dent Assoc. 2007;138(8):1084-1091. doi:10.14219/jada.archive.2007.0320
4. Probert TC, Wiesenfeld D, Reade PC. Temporomandibular pain dysfunction disorder resulting from road traffic accidents—an Australian study. Int J Oral Maxillofac Surg. 1994;23(6 Pt 1): 338-341. doi:10.1016/s0901-5027(05)80049-9
5. Martin MD, Wilson KJ, Ross BK, Souter K. Intubation risk factors for temporomandibular joint/facial pain. Anesth Prog. 2007;54(3):109-114. doi:10.2344/0003-3006(2007) 54[109:IRFFTF]2.0.CO;2
6. Kight M, Gatchel RJ, Wesley L. Temporomandibular disorders: evidence for significant overlap with psychopathology. Health Psychol. 1999;18(2):177-182. doi:10.1037//02786133.18.2.177
7. Yap AU, Dworkin SF, Chua EK, List T, Tan KB, Tan HH. Prevalence of temporomandibular disorder subtypes, psychologic distress, and psychosocial dysfunction in Asian patients. J Orofac Pain. 2003;17(1):21-28.
8. Smith SB, Maixner DW, Greenspan JD, et al. Potential genetic risk factors for chronic TMD: genetic associations from the OPPERA case control study. J Pain. 2011;12(11 Suppl):T92T101. doi:10.1016/j.jpain.2011.08.005
9. Braido GVDV, Campi LB, Jordani PC, Fernandes G, GonÇalves DAG. Temporomandibular disorder, body pain and systemic diseases: assessing their associations in adolescents. J Appl Oral Sci. 2020;28:e20190608. doi:10.1590/1678-7757-2019-0608
10. Ohlmann B, Waldecker M, Leckel M, et al. Correlations between sleep bruxism and temporomandibular disorders. J Clin Med. 2020;9(2):611. doi:10.3390/jcm9020611
11. Lora VR, Canales Gde L, Gonçalves LM, Meloto CB, Barbosa CM. Prevalence of temporomandibular disorders in postmenopausal women and relationship with pain and HRT. Braz Oral Res. 2016;30(1):e100. doi:1590/1807-3107BOR-2016.vol30.0100
12. Manfredini D, Lombardo L, Siciliani G. Temporomandibular disorders and dental occlusion. A systematic review of association studies: end of an era? J Oral Rehabil. 2017;44(11):908-923. doi:10.1111/joor.12531
13. Galluccio G. Is the use of clear aligners a real critical change in oral health prevention and treatment. Clin Ter. 2021;172(2):113-115. doi:10.7417/CT.2021.2295
14. Kim KY, Choi JY, Oh SH, et al. Computerized assessment of occlusion and muscle activity during use of a multilayer clear retainer: a preliminary study. Sensors (Basel). 2021;21(2):541. doi:10.3390/s21020541
15. Okeson, JP. Management of Temporomandibular Disorders and Occlusion. 8th ed. Elsevier; 2020.
16. Le Bell Y, Niemi PM, Jämsä T, Kylmälä M, Alanen P. Subjective reactions to intervention with artificial interferences in subjects with and without a history of temporomandibular disorders. Acta Odontol Scand. 2006;64(1):59-63. doi:10.1080/00016350500419867
17. Li DTS, Leung YY. Temporomandibular disorders: current concepts and controversies in diagnosis and management. Diagnostics (Basel). 2021;11(3):459. doi:10.3390/diagnostics11030459
18. Commisso MS, Martínez-Reina J, Mayo J. A study of the temporomandibular joint during bruxism. Int J Oral Sci. 2014;6(2):116-123. doi:10.1038/ijos.2014.4
19. Conti A, Freitas M, Conti P, Henriques J, Janson G. Relationship between signs and symptoms of temporomandibular disorders and orthodontic treatment: a cross-sectional study. Angle Orthod. 2003;73(4):411-417. doi:10.1043/0003-3219(2003)073<0411:RBSASO>2.0.CO;2
20. Macfarlane TV, Kenealy P, Kingdon HA, et al. Twenty-year cohort study of health gain from orthodontic treatment: temporomandibular disorders. Am J Orthod Dentofacial Orthop 2009;135(6):692.e1-692.e8. doi:10.1016/j.ajodo.2008.10.017
21. Egermark I, Magnusson T, Carlsson GE. A 20-year follow-up of signs and symptoms of temporomandibular disorders and malocclusions in subjects with and without orthodontic treatment in childhood. Angle Orthod. 2003;73(2):109-115. doi:10.1043/00033219(2003)73<109:AYFOSA>2.0.CO;2
22. Schupp W, Haubrich J, Neumann I. Invisalign treatment of patients with craniomandibular disorders. Int Orthod. 2010;8(3):253-267. doi:10.1016/j.ortho.2010.07.010
23. Lu C. Evaluating clear aligners and conventional braces in treating TMJ and speech impediment. J Stud Res. 2022;11(4). doi:10.47611/jsrhs.v11i4.3688
24. Kandasamy S, Rinchuse DJ, Greene CS, Johnston LE Jr. Temporomandibular disorders and orthodontics: what have we learned from 1992-2022? Am J Orthod Dentofacial Orthop 2022;161(6):769-774. doi:10.1016/j.ajodo.2021.12.011
25. Bargellini A, Castroflorio T, Graziano V, Cugliari G, Deregibus A. Effects on sleep bruxism activity of three different oral appliances: one-year longitudinal cohort study. Curr Drug Deliv. 2023;21(8):1151-1159. doi:10.2174/1567201819666220519123754
26. Garrigós-Pedrón M, Elizagaray-García I, Domínguez-Gordillo AA, Del-Castillo-Pardo-de-Vera JL, Gil-Martínez A. Temporomandibular disorders: improving outcomes using a multidisciplinary approach. J Multidiscip Healthc. 2019;12:733-747. doi:10.2147/JMDH.S178507. Erratum: 2019;12:dccciii. doi:10.2147/JMDH.S230642
27. Pimentel G, Bonotto D, Hilgenberg-Sydney PB. Self-care, education, and awareness of the patient with temporomandibular disorder: a systematic review. Br J Pain. 2018;1(3):263269. doi:10.5935/2595-0118.20180050
GENERAL DENTISTRY SELF-INSTRUCTION
Exercise No. GD538, 2 CE Credits
Orthodontics
Subject Code: 370
The 15 questions for this exercise are based on the article “Clear aligner therapy and symptoms of temporomandibular disorders: a case report” on pages 47-52. This exercise was developed by Jeffery B. Price, DDS, MS, MAGD, FICD, FACD, in association with the General Dentistry SelfInstruction committee.
1. The relationship between occlusion and TMD symptoms is well understood. According to the National Institutes of Health, fewer than 15 factors are related to the etiology of TMDs.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
2. The case report describes ____________.
A. how to fabricate in-office CAT aligners
B. CAT that exacerbated TMD symptoms
C. orthodontic evaluation and diagnosis
D. management of Class III malocclusions
3. During which phase of CAT is the recommended time to discuss with patients the potential development of TMD symptoms?
A. at the time of consent
B. during the initial examination
C. while accepting payment
D. at posttreatment recall
4. Which of the following signs of occlusal habits was reported by the patient?
A. tooth grinding
B. clenching of teeth
C. chewing on pencils
D. biting fingernails
5. Which of the following describes the patient’s motivation for pursuing orthodontic treatment?
A. painful and sore temporomandibular joints (TMJs)
B. spaces between her teeth
C. trouble chewing food
D. self-consciousness about her smile
Reading the article and successfully completing this exercise will enable you to:
• understand some of the contributing factors for the development of temporomandibular disorders (TMDs);
• describe the advantages of clear aligner therapy (CAT) compared with fixed appliances for orthodontic therapy; and
• discuss potential management solutions for a patient who develops TMD pain symptoms after onset of CAT.
Answers must be submitted online at agd.org/self-instruction by October 31, 2025.
6. During the initial appointment, the TMJ examination revealed tenderness on palpation of the pterygoid muscles. The TMJ examination revealed no signs or symptoms of muscle- or TMJ-related issues.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
7. Which of the following statements best describes the clinical findings during the initial examination?
A. missing only third molars
B. midline discrepancies
C. moderate periodontitis
D. end-to-end incisor occlusion
8. The pattern of tooth wear on the incisal edges and cusp tips showed _________ during eccentric movement.
A. group function
B. an open bite
C. canine guidance
D. molar occlusion
9. Which of the following best describes the morphology of the condyles?
A. flattened right condyle
B. both condyles flattened
C. flattened left condyle
D. enlarged right condyle
10. The overall treatment objective for this case included a(n) ____________.
A. comprehensive, multidisciplinary plan
B. intermediate plan after periodontal therapy
C. limited plan to improve esthetics
D. fixed appliance plan before CAT
11. The CAT in this case included all of the following goals except one. Which is the exception?
A. reduce overjet
B. expand the arches
C. align the anterior teeth
D. intrude the maxillary left second molar
12. The patient began to experience pain and soreness in the preauricular region of the face during the ______ week of treatment.
A. first
B. second
C. third
D. fourth
13. The patient was diagnosed with which of the following conditions during an otolaryngologist visit?
A. tonsilitis and mastoiditis
B. ear and sinus infections
C. right masseter myositis
D. retrocapsular tendinitis
14. The orofacial pain specialist managed the patient’s symptoms with ________ and ________.
A. routine home care; over-the-counter (OTC) anti-inflammatory pain medication
B. routine home care; heated massage therapy 3 times a day
C. heated massage therapy 3 times a day; OTC anti-inflammatory pain medication
D. heated massage therapy 3 times a day; isometric jaw exercises 2 times a day
15. After becoming symptomatic, the patient was instructed to discontinue wearing the aligners for 1 week while she learned to reduce jaw muscle tension. After the patient began to wear the aligners only at night, tooth movement occurred with minimal TMD symptoms.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
An unusual clinical and histopathologic presentation of a maxillofacial ameloblastoma: a literature review and case report
The objectives of this article are to describe an unusual clinical and histopathologic presentation of an ameloblastoma affecting the right maxilla, maxillary sinus, and nasal cavity and to discuss the difficulty of establishing a clinical classification based on the most recent edition of Head and Neck Tumours in the WHO Classification of Tumours series (2022). A 74-year-old man presented with a 6 × 6-cm expansile, ulcerated mass on the right lateral palate. A clinical diagnosis of squamous cell carcinoma was rendered. A biopsy was performed, and the specimen showed multiple histologic patterns of ameloblastoma inconclusive of odontogenic or sinonasal origin. Cone beam computed tomographic imaging demonstrated a well-defined unilocular mass in the right maxilla extending up to the nasal cavity. A surgical resection was performed and confirmed the diagnosis of maxillary ameloblastoma with extension into the nasal cavity. This dilemma in delayed diagnosis led to a literature search for similar maxillary ameloblastoma cases with extension into vital structures. In 45 cases previously reported in the literature, the median age of patients with maxillary ameloblastoma was 50 years, and there was extensive involvement of adjacent vital structures. The nasal cavity/sinonasal region (24/45), orbit/orbital floor (12/45), multiple fossae (5/45), and base of the skull (4/45) were the most common extensions of maxillary ameloblastoma. Fifteen patients had lesions with multiple extensions, and 1 patient showed lung metastasis. The most common histologic presentation was the follicular pattern, followed by the plexiform pattern or mixed follicular and plexiform patterns. Surgical interventions were performed on most patients, with the majority undergoing maxillectomy. Differentiating primary sinonasal ameloblastoma from gnathic ameloblastoma with sinonasal extension is challenging, and this article discusses subtle radiographic criteria and symptoms that aid in the distinction of both types. The authors suggest that variants of maxillary ameloblastoma with extensive involvement of the sinonasal region, orbit, or base of the skull be classified with a clinical diagnosis of maxillofacial ameloblastoma, regardless of the tumor origin.
Ameloblastoma is a benign, slowly growing, locally destructive odontogenic tumor of the maxillofacial region with a high recurrence rate. In more than 80% of ameloblastomas, the posterior mandible and ramus areas are involved.1 However, maxillary ameloblastoma is more aggressive than mandibular ameloblastoma and can infiltrate the nasal, paranasal, and orbital structures.1
The classification of ameloblastoma has been modified over time, with various taxonomies based on histogenesis, the origin of differentiation, or biological behavior.2 In the first edition of the World Health Organization (WHO) classification of odontogenic tumors, published in 1971, ameloblastoma was classified simply as an odontogenic tumor.3 In the second edition, published in 1992, ameloblastoma was reclassified as an epithelial odontogenic tumor.4 In the third edition, published in 2005, ameloblastomas were further classified into benign and malignant tumors, depending on their biological behavior.5 The 2005 classification was not widely accepted, however, so a fourth edition of the classification (published in 2017) was developed to simplify the classification and terminology, clearly reflect the behavior and nature of the tumor, and encourage international acceptance.6 In 2022, WHO published a fifth edition, aiming to add diagnostic features for each entity and focus more on the molecular findings, which would help guide new treatment strategies.7
Despite the revisions, the recent classification still lacks clarification on the behavior of maxillary ameloblastoma and its involvement with adjacent and associated structures. Ameloblastomas may arise from odontogenic epithelial apparatus, including cell rests of the enamel organ, the epithelial lining of the odontogenic cyst, or basal cells of the oral mucosa. However, 2% to 10% of ameloblastomas have been reported in extragnathic sites, theoretically caused by an aberration in embryologic growth that results in ectopic seeding of odontogenic epithelium or subsequent odontogenesis in neighboring tissues.8 Sinonasal tract involvement, referred to as sinonasal ameloblastoma, is an example of an extragnathic site.9 It has been proposed that an abnormal differentiation of pluripotent stem cells of the sinonasal mucosa can lead to primary sinonasal ameloblastoma due to the proximity between the odontogenic apparatus and sinonasal cavity.10,11 It has also been hypothesized that chronic inflammation in the sinonasal mucosa can be a predisposing factor in the pathogenesis of ameloblastoma in the sinonasal tract.12
Unlike ameloblastoma arising from the jawbones, sinonasal ameloblastoma usually presents with rhinorrhea, epistaxis,
2. Hematoxylin-eosin staining of the biopsy specimens. A. Medium-power view demonstrating interlacing cords and strands of epithelium, with dyskeratotic cells and acanthomatous areas (original magnification × 20). B. High-power view demonstrating enhanced basaloid staining of the basal cells with acanthomatous areas (original magnification ×40). C. High-power view demonstrating reverse polarization of the palisaded basal cell (original magnification × 40).
facial swelling, headache, and paresthesia. The reported inconsistencies between the clinical and histologic presentations of maxillary ameloblastoma and those of sinonasal ameloblastoma usually lead to delayed diagnosis and increased morbidity.13 Additionally, the prognosis is based on the extension of the tumor into adjacent structures; therefore, it is clinically important to differentiate between maxillary ameloblastoma that is limited to the site of origin and maxillary ameloblastoma that extends to adjacent structures. Therefore, the objectives of this article are to describe an unusual clinical and histopathologic presentation of maxillary ameloblastoma affecting the right maxilla, maxillary sinus, and nasal cavity and to review the published literature on this entity, discussing the difficulty of establishing a clinical classification based on the 2022 WHO classification.7
Case report
Ethical approval for this case report and study was granted by the University of Alberta’s Alberta Research Information Services (ARISE) Board (No. Pro00119953).
A 74-year-old man was referred to the oral surgery clinic of the School of Dentistry, Faculty of Medicine & Dentistry, University of Alberta, Edmonton, Canada, for surgical management of a nonhealing palatal tumor. A 6 × 6-cm expansile, ulcerated mass was identified on the right lateral palate. The tumor extended from the maxillary right central incisor to the maxillary right tuberosity and medially toward the midline. The lesion was
3. CBCT images of the maxillary mass. A. Axial view. B. Sagittal view. C. Coronal view. D. Three-dimensional reconstruction.
ulcerated distal to the maxillary right second molar around the tuberosity and anterior soft palate. The tooth alignment was not affected. Palpation of the right buccal gingiva and sulcus revealed a mild expansion. The clinical features suggested that the lesion was an oral squamous cell carcinoma (Fig 1).
An incisional biopsy was acquired, and the histopathologic assessment of the biopsied specimen revealed multiple patterns,
Fig 1. Maxillary posterior palatal tumor.
Fig
Fig
An unusual clinical and histopathologic presentation of a maxillofacial ameloblastoma: a literature review and case report
Table. Summary of previous case reports on maxillary ameloblastoma (January 1971 through May 2024).
Patient Tumor characteristics
Study
Age, y Sex Clinical presentation
Histopathology
Fox and Dyson1 64 F Tumor in left maxilla FP
56 F Tumor in left maxilla FP
Guilemany et al27 68 M Mass extending outside nasal vestibule, nasal obstruction, rhinorrhea PP
Shahidi et al12 74 M Recurrent sinusitis, bony hard swelling in molar and premolar regions FP
Leibovitch et al28 60 M Recurrent maxillary ameloblastoma, decreased visual acuity in right eye, diplopia, headaches FP
Tranchina et al14 74 M Exophytic lesion, nasal obstruction, rhinorrhea, sinusitis FP, PP
Weissman and Wetli15 45 M Nosebleed, right nasal stuffiness, mass in right nasal chamber FP
73 M Recurrent maxillary ameloblastoma with diplopia, headaches PP
Friedrich and Zustin29 36 M Tumor in left maxillary sinus FP
Komisar16 63 M Tumor in posterior maxilla, preauricular pain, otalgia, nasal obstruction, foul-smelling oral discharge PP
Weiss et al17 72 M Soft tissue mass in maxillary antrum, blurred vision FP
Keay et al18
Pitak-Arnnop et al30 19 M Recurrent sinusitis and enlarging mass in right cheek Cystic spaces with ameloblastomatous epithelial lining
Jain et al31 43 F Mass in nasal cavity, nasal obstruction, recurrent epistaxis NR
76 F Nasal obstruction, purulent blood- stained catarrh, swelling in left maxilla FP, PP M Nasal polyp, headaches FP, PP
Bredenkamp et al19
37 F Swelling in right cheek FP
Herwig et al32 66 M History of ameloblastoma in left maxilla, new prominent mass on left side of face NR
Kochaji et al33 60 M Pain and swelling in left maxillary region FP
Scaccia et al20 Intranasal mass, nasal obstruction
16 F Postnasal discharge
Gupta et al34 14 M Swelling in left cheek FP, PP
Dentigerous cyst origin
Sakuntala et al35 63 F Swelling in right cheek NR
53 M Tumor in right maxillary alveolus
Agani et al36 16 M Swelling in right maxillary region Mural unicystic
36 F Postnasal discharge, sinus pain PP
Li et al37 4 F Swelling in right maxillary region NR
Sato et al21
Ono et al22
79 M Swelling in left maxillary region
60 M Large mass in left maxillary region, marked swelling in cheek PP
Lakshmi et al38 40 M Swelling in left maxillary region Hybrid de Menezes et al39 81 M Large mass in left maxillary region FP
Lovásová et al23
60 F Massive swelling in left side of face and neck
Faras et al40 56 F Swelling in left maxillary region FP
Jung et al41 27 M Nasal airway obstruction, perforated maxillary left second molar mucosa Acanthomatous
Schmidt et al24
81 F Swelling in left maxillary region
Biörklund et al42 67 M Pain and swelling in left maxilla FP, PP
Chebil et al43 54 F Ulceration of left alveolar process of maxilla FP
63 F Right-sided facial fullness, pain, nasal congestion, rhinorrhea
Chu44 35 M Swelling on left side of cheek FP,
Zwahlen and Grätz25 33 F Swelling in left maxillary region
Ferreira et al45 19 F Moderate headache, nausea, vomiting, left facial hypesthesia, low visual acuity FP, PP
26 F Painless swelling behind maxillary left first molar FP
42 M Swelling in left maxillary region
Karpal Singh et al46 24 M Massive swelling in right side of face FP
FP, PP
Pillai et al26
24 F Swelling in left maxillary anterior region
Table continued on pages 58-59.
including cords and strands of bilayered and interlacing columnar cells with evidence of reverse polarization; nests of epithelial islands with dyskeratotic cells; and scant mitotic activity. Given the wide diversity in the histologic presentation of the specimen, multiple types of odontogenic or sinonasal tumors were considered as the diagnosis (Fig 2). Upon immunohistochemical staining with cytokeratin (CK), lesional cells demonstrated uniform positivity for both CK19 and CK5/6, further supporting a diagnosis of maxillary ameloblastoma or sinonasal ameloblastoma. The tumor cells were negative for CK7 and CK20.
Cone beam computed tomographic (CBCT) images demonstrated a well-defined, unilocular, expansile, high-density mass located in the maxilla (Fig 3). The lesion extended into the right maxillary sinus and nasal fossa, reaching the nasal septum. Vertically, the mass extended from the alveolar bone at the level of the premolar and molar apices superiorly to the floor of the right orbit and from the medial wall of the nasal cavity to the
Desmoplastic
Linaburg et al47 50 F Massive swelling in left side of face Acanthomatous, FP
maxillary wall and tuberosity. The mass displayed a homogenous low-density internal content, and its periphery was partially corticated with areas of cortical interruption. The axial and sagittal CBCT views showed expansion and interruption of the right maxillary sinus walls and nasal cavity at the middle turbinate level. The mass caused the expansion of the buccal and palatal cortical plates of the maxilla and the resulting facial asymmetry. The floor of the right orbit showed mild superior displacement. The nasal septum was deviated to the left, and narrowing of the oropharyngeal space was noted at the uvula level, which could have been an effect of the lesion in the adjacent structures. The patient was referred to the head and neck surgery department for treatment. Prior to surgery, multidimensional computed tomographic imaging ruled out any soft tissue involvement. A right maxillectomy was performed, and analysis of the tumor further confirmed a histologic diagnosis of ameloblastoma.
Extension
Maxillary sinus
Maxillary sinus
Nasal cavity, orbital floor
Maxillary sinus, sinonasal region
Orbital area
Middle cranial fossa
Treatment
En bloc resection
Radical maxillectomy and reconstruction
Radiation and surgery
Radical left maxillectomy
Maxillectomy and radiotherapy
Endoscopic sinus surgery
Posterior choana, maxillary sinus
Left middle cranial fossa, temporal area, left orbit
Right partial maxillectomy
Neurosurgery and otolaryngology
Maxillary sinus, orbit, nasal cavity
Maxillary sinus
Maxillary sinus
Maxillary sinus, orbital floor
Maxillary sinus
Nasal cavity
Maxillary sinus
Nasopharynx, posterior pharyngeal wall, orbit, skull base
Intraorbital soft tissue, paranasal sinuses, skull base
Maxillary sinus
Orbital floor
Maxillary sinus
Maxillary sinus
Maxillary sinus
Maxillary sinus
Maxillary sinus
Maxillary sinus
Maxillary sinus
Orbital region, frontotemporal region
Maxillary sinus
Maxillary sinus, ethmoid sinus, orbital floor
Nasal cavity, maxillary sinus, orbital floor
Infratemporal fossa, temporal fossa
Maxillary sinus, orbital floor
Maxillary sinus, skull base
Orbital floor, ethmoid sinus
Maxillary sinus
Maxillary sinus
Left maxillary sinus, infratemporal fossa
Maxillary sinus
Maxillary sinus
Maxillary sinus
Skull base, cavernous sinus
Maxillary sinus, sphenoidal sinus, medial orbital wall
Brain and lung metastases
Maxillary sinus floor
Maxillary sinus, orbital floor
Review of the literature
Hemimaxillectomy
Surgery
Enucleation and curettage
Maxillectomy and local radiotherapy
Radical antrostomy
Transoral resection
Radical antrostomy
Partial maxillectomy and external beam radiation therapy
Maxillary sinus resection with left orbital exenteration
Medial maxillectomy, ethmoidectomy, and sphenoidotomy
Radical surgery
Partial left maxillectomy
Removal of cystic mass with right Caldwell-Luc approach
Right maxillary surgical resection
Right maxilloethmoidectomy
Surgical enucleation
Left maxilloethmoidectomy
Marsupialization and peripheral osteotomy
Maxillectomy and orbital exenteration
Hemimaxillectomy
Maxillectomy and reconstruction surgery
Curettage
Radical hemimandibulectomy with submandibular approach
Maxillectomy
Osteotomy
Left medial maxillectomy
Maxillectomy
Ethmoidectomy and maxillary antrostomy
Surgical resection
Hemimaxillectomy
Maxillectomy
Partial maxillectomy
Endoscopic resection
Left partial maxillectomy
Chemoradiotherapy
Partial maxillectomy and nonvascularized iliac bone graft
Left partial maxillectomy
A comprehensive literature search of the PubMed, MEDLINE, Scopus, Embase, and Google Scholar databases was performed for articles published from January 1971 through May 2024. The search terms were maxillary ameloblastoma, gnathic ameloblastoma, maxillary ameloblastoma with extension, and odontogenic tumors.
The search identified 45 published cases of maxillary ameloblastoma with an extension to the maxillary sinuses and associated structures (Table).1,12,14-47 The mean age of the patients was 50 years (range of 4 to 81 years), and there was no male or female predilection. The most common clinical presentation documented was a tumor in the maxillary region, nasal obstruction, or sinusitis. The nasal cavity/sinonasal region (24/45), orbit/orbital floor (12/45), multiple fossae (5/45), and base of the skull (4/45) were the most common extensions of maxillary ameloblastoma (Chart). Fifteen patients had lesions
with multiple extensions, and 1 patient showed lung metastasis. Histologically, the lesions most commonly presented with a follicular pattern, followed by a plexiform pattern. Surgical intervention was the treatment elected for the majority of patients, most of whom underwent maxillectomy.
Discussion
The diagnostic process for classifying maxillary ameloblastoma that extends into the maxillary sinus and paranasal structures is always challenging, as the origin is unclear. Maxillary ameloblastoma of gnathic origin is very invasive due to the structure of the maxillary bone and may involve the sinonasal region and other associated vital structures.48 The differential diagnosis of maxillary ameloblastoma with extension into adjacent structures includes acute and chronic sinusitis, inverted papilloma, squamous cell carcinoma, adenocarcinoma, angiofibroma, basal cell adenoma, and proliferation of craniopharyngioma.49
Table. Summary of previous case reports on maxillary ameloblastoma (January 1971 through May 2024) (continued).
Patient
Study
Guilemany et al27 68 M Mass extending outside nasal vestibule, nasal obstruction, rhinorrhea PP
Leibovitch et al28 60 M Recurrent maxillary ameloblastoma, decreased visual acuity in right eye, diplopia, headaches FP
73 M Recurrent maxillary ameloblastoma with diplopia, headaches PP
Friedrich and Zustin29 36 M Tumor in left maxillary sinus FP
Pitak-Arnnop et al30 19 M Recurrent sinusitis and enlarging mass in right cheek Cystic spaces with ameloblastomatous epithelial lining
Jain et al31 43 F Mass in nasal cavity, nasal obstruction, recurrent epistaxis NR
Herwig et al32 66 M History of ameloblastoma in left maxilla, new prominent mass on left side of face NR
Kochaji et al33 60 M Pain and swelling in left maxillary region FP
Gupta et al34 14 M Swelling in left cheek FP, PP
Sakuntala et al35 63 F Swelling in right cheek NR
Agani et al36 16 M Swelling in right maxillary region Mural unicystic
Li et al37 4 F Swelling in right maxillary region NR
Lakshmi et al38 40 M Swelling in left maxillary region Hybrid
de Menezes et al39 81 M Large mass in left maxillary region FP
Faras et al40 56 F Swelling in left maxillary region FP
Jung et al41 27 M Nasal airway obstruction, perforated maxillary left second molar mucosa Acanthomatous
Biörklund et al42 67 M Pain and swelling in left maxilla FP, PP
Chebil et al43 54 F Ulceration of left alveolar process of maxilla FP
Chu44 35 M Swelling on left side of cheek FP,
Ferreira et al45 19 F Moderate headache, nausea, vomiting, left facial hypesthesia, low visual acuity FP, PP
Sohal et al46 24 M Massive swelling in right side of face FP
Linaburg et al47 50 F Massive swelling in left side of face Acanthomatous, FP
Abbreviations: F, female; FP, follicular pattern; M, male; NR, not reported; PP, plexiform pattern.
Chart. Distribution of maxillary ameloblastoma with extension into associated vital structures (N = 45).
Ameloblastomas of the jaws are commonly diagnosed in the third decade of life, and there is no sex predilection. However, ameloblastomas involving the sinuses and nasal cavities are more common in older men, as in the present case.49
Diagnosis of ameloblastoma requires clinical, radiographic, and histopathologic examinations. Clinically, sinonasal ameloblastoma can be associated with nasal obliteration, sinusitis and/or epistaxis, and less common signs and symptoms of facial swelling, headache, and tearing.42 Radiographically, primary sinonasal lesions frequently appear as radiopaque, solid lesions that fill the nasal cavity or sinus. In contrast, ameloblastoma of gnathic origin commonly presents as a unicystic or multicystic entity.42 However, this radiographic difference cannot be appreciated if the tumor involves all the vital structures and presents as a single lesion involving the maxillofacial region of that site. Histologically, ameloblastoma of jaws and sinonasal ameloblastoma have a similar appearance, commonly
Extension
Nasal cavity, orbital floor
Orbital area
Left middle cranial fossa, temporal area, left orbit
Maxillary sinus
Maxillary sinus
Maxillary sinus
Intraorbital soft tissue, paranasal sinuses, skull base
Orbital floor
Maxillary sinus
Maxillary sinus
Maxillary sinus
Maxillary sinus
Maxillary sinus
Nasal cavity, maxillary sinus, orbital floor
Maxillary sinus, orbital floor
Maxillary sinus, skull base
Maxillary sinus
Left maxillary sinus, infratemporal fossa
Maxillary sinus
Skull base, cavernous sinus
Brain and lung metastases
Maxillary sinus, orbital floor
Treatment
Radiation and surgery
Maxillectomy and radiotherapy
Neurosurgery and otolaryngology
Surgery
Enucleation and curettage
Transoral resection
Maxillary sinus resection with left orbital exenteration
Radical surgery
Partial left maxillectomy
Right maxillary surgical resection
Surgical enucleation
Marsupialization and peripheral osteotomy
Hemimaxillectomy
Curettage
Maxillectomy
Osteotomy
Maxillectomy
Surgical resection
Maxillectomy
Endoscopic resection
Chemoradiotherapy
Left partial maxillectomy
presenting with a follicular or plexiform pattern, although multiple histologic forms can be found in a single specimen.42
The genomic analysis of ameloblastomas has shown oncogenic mutations in the hedgehog and mitogen-activated protein kinase pathways.50 Studies have documented that sequence variations in the SMO (smoothened, frizzled class receptor) gene are commonly observed in ameloblastomas of the maxilla, while variations in BRAF (B-Raf proto-oncogene) are predominant in tumors of the mandible.51 Notably, a specific SMO alteration, a leucine to phenylalanine substitution at amino acid 412 (p.Leu412Phe), has been identified as an activating mutation that can be inhibited effectively by arsenic trioxide, an antileukemia drug currently being investigated in clinical trials for its hedgehog-inhibitory activity. Similarly, ameloblastoma cells harboring an activating BRAF alteration that results in valine to glutamate substitution at amino acid 600 (p.Val600Glu) have been found to be responsive to treatment with the BRAF inhibitor
vemurafenib. These findings present a novel approach to the diagnostic classification and treatment of ameloblastomas.52
Surgery is the treatment of choice for either type of tumor. A protocol of radiographic follow-up examinations for at least 10 years after surgical management of maxillary ameloblastoma has been recommended because these lesions have a high recurrence rate, are clinically invasive, and can involve associated vital structures.48
Because maxillary ameloblastomas demonstrate slow and silent growth, patients usually present with an advanced and aggressive tumor associated with a poor prognosis.22 Therefore, the nomenclature corresponding to maxillary ameloblastoma involving extragnathic structures and associated vital structures must be revised. The authors propose classifying ameloblastoma with extensive involvement of the sinonasal region, orbit, or base of the skull as maxillofacial ameloblastoma, regardless of the tumor origin, when the WHO classification
of benign odontogenic tumors is revised in the future. This terminology would help pathologists and surgeons distinguish these challenging and morbid tumors from conventional ameloblastoma and, consequently, keep affected patients on a close radiographic monitoring and follow-up schedule.
Conclusion
The maxillary ameloblastoma has been occasionally reported to expand extensively into the paranasal sinuses and nasal cavity. However, primary sinonasal ameloblastomas with extension into the maxilla have also been reported. The present case report demonstrated the dilemma in appropriately classifying these clinical variants of ameloblastoma, as it was difficult to confidently identify the origin of the tumor as either conventional or extragnathic because it involved both the jawbone and paranasal structures. Regardless of the tumor origin, the term maxillofacial ameloblastoma is suggested as a more appropriate clinical diagnosis when there is extensive involvement of the sinonasal region and maxilla. The surgical management, however, remains unchanged.
Author affiliations
Mike Petryk School of Dentistry, Faculty of Medicine & Dentistry, University of Alberta, Edmonton, Canada.
The authors thank Dr Oualid Badri, a fellow of the TMJ/ Surgery Program, Mike Petryk School of Dentistry, Faculty of Medicine & Dentistry, University of Alberta, for the critical review of this article.
References
1. Fox J, Dyson D. Ameloblastoma of the maxilla: a report of two cases. Br Dent J 1975;138(2):61-64. doi:10.1038/sj.bdj.4803368
2. Soluk-Tekkeşin M, Wright JM. The World Health Organization classification of odontogenic lesions: a summary of the changes of the 2017 (4th) edition. Turk Patoloji Derg 2018;34(1):10.5146/tjpath.2017.01410. doi:10.5146/tjpath.2017.01410
3. Pindborg JJ, Kramer IRH, eds. Histological Typing of Odontogenic Tumours, Jaw Cysts, and Allied Lesions. International Histological Classification of Tumours: No. 5. World Health Organization; 1971
4. Kramer IRH, Pindborg JJ, Shear M, eds. Histological Typing of Odontogenic Tumors. 2nd ed World Health Organization International Histological Classification of Tumours. Springer; 1992.
5. Barnes L, Eveson JW, Reichart P, Sidransky D, eds. Pathology & Genetics of Head and Neck Tumours. WHO Classification of Tumours. 3rd ed. Vol 9. IARC Press; 2005.
6. El-Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg PJ, eds. WHO Classification of Head and Neck Tumours. WHO Classification of Tumours. 4th ed. Vol 9. International Agency for Research on Cancer; 2017.
7. WHO Classification of Tumours Editorial Board, eds. Head and Neck Tumours. Part A WHO Classification of Tumours. 5th ed. Vol 9. International Agency for Research on Cancer; 2022.
8. Prasad ML, Perez-Ordonez B. Nonsquamous lesions of the nasal cavity, paranasal sinuses, and nasopharynx. In: Gnepp DR, ed. Diagnostic Surgical Pathology of the Head and Neck 2nd ed. Saunders; 2009:111-189.
9. Guilemany JM, Ballesteros F, Alós L, et al. Plexiform ameloblastoma presenting as a sinonasal tumor. Eur Arch Otorhinolaryngol. 2004;261(6):304-306. doi:10.1007/s00405-003-0692-x
10. Leong SC, Karkos PD, Krajacevic J, Islam R, Kent SE. Ameloblastoma of the sinonasal tract: a case report. Ear Nose Throat J. 2010;89(2):70-71.
11. Schafer DR, Thompson LD, Smith BC, Wenig BM. Primary ameloblastoma of the sinonasal tract: a clinicopathologic study of 24 cases. Cancer. 1998;82(4):667-674. doi:10.1002/ (sici)1097-0142(19980215)82:4<667::aid-cncr8>3.0.co;2-i
12. Shahidi Sh, Bronoosh P, Daneshbod Y. Follicular ameloblastoma presenting as a sinonasal tumor. Iran Red Crescent Med J. 2012;14(2):113-116.
13. Mehta V, Sarode GS, Obulareddy VT, et al. Clinicopathologic profile, management and outcome of sinonasal ameloblastoma: a systematic review. J Clin Med. 2023;12(1):381. doi:10.3390/jcm12010381
14. Tranchina MG, Amico P, Galia A, Emmanuele C, Saita V, Fraggetta F. Ameloblastoma of the sinonasal tract: report of a case with clinicopathologic considerations. Case Rep Pathol 2012;2012:218156. doi:10.1155/2012/218156
15. Weissman BW, Wetli C. Ameloblastoma of the maxilla. South Med J. 1977;70(2):251-253. doi:10.1097/00007611-197702000-00043
16. Komisar A. Plexiform ameloblastoma of the maxilla with extension to the skull base. Head Neck Surg. 1984;7(2):172-175. doi:10.1002/hed.2890070213
17. Weiss JS, Bressler SB, Jacobs Jr EF, Shapiro J, Weber A, Albert DM. Maxillary ameloblastoma with orbital invasion: a clinicopathologic study. Ophthalmology. 1985;92(5):710-713. doi:10.1016/s0161-6420(85)33977-5
18. Keay DG, Small M, Kerr AI, McLaren K. Ameloblastoma presenting as nasal obstruction: case reports. J Laryngol Otol. 1988;102(6):530-533. doi:10.1017/s0022215100105560
20. Scaccia FJ, Strauss M, Arnold J, Maniglia AJ. Maxillary ameloblastoma: case report. Am J Otolaryngol. 1991;12(1):20-25. doi:10.1016/0196-0709(91)90069-r
21. Sato K, Sudo S, Fukuya Y, Sakuma H. Maxillary ameloblastoma with intracranial invasion— case report. Neurol Med Chir (Tokyo). 1994;34(10):704-707. doi:10.2176/nmc.34.704
22. Ono Y, Murakami-Yunoki J, Miyashita K, et al. An advanced primary ameloblastoma in the maxilla extending into the maxillary and ethmoid sinus tract: a case report. J Oral Maxillofac Surg Med Pathol. 2022;34(4):403-410. doi:10.1016/j.ajoms.2021.11.002.
23. Lovásová K, Borza B, Kizek P, Almaši M, Kachlík D, Hodorová I. A case of giant ameloblastoma: destructive effect on the facial skeleton and soft tissues of the head and neck. J Int Med Res. 2021;49(10):3000605211050185. doi:10.1177/03000605211050185
24. Schmidt R, Moses RL, Loggi D, et al. Unusual otolaryngic presentations of ameloblastoma. Otolaryngol Head Neck Surg. 1999;121(3):285-289. doi:10.1016/S0194-5998(99)70194-4
25. Zwahlen RA, Grätz KW. Maxillary ameloblastomas: a review of the literature and of a 15-year database. J Craniomaxillofac Surg. 2002;30(5):273-279. doi:10.1016/s10105182(02)90317-3.
26. Pillai R, Ongole R, Ahsan A, Radhakrishnan RA, Pai KM. Recurrent desmoplastic ameloblastoma of the maxilla: a case report. J Can Dent Assoc. 2004;70(2):100-104.
27. Guilemany JM, Ballesteros F, Alós L, et al. Plexiform ameloblastoma presenting as a sinonasal tumor. Eur Arch Otorhinolaryngol. 2004;261(6):304-306. doi:10.1007/s00405-003-0692-x.
28. Leibovitch I, Schwarcz RM, Modjtahedi S, Selva D, Goldberg RA. Orbital invasion by recurrent maxillary ameloblastoma. Ophthalmology. 2006;113(7):1227-1230. doi:10.1016/j. ophtha.2006.02.051.
29. Friedrich RE, Zustin J. Ameloblastoma of the maxillary sinus 11 years after extirpation of extensive dentigerous cysts and dystopic wisdom tooth. In Vivo. 2010;24(4):567-570.
30. Pitak-Arnnop P, Chaine A, Dhanuthai K, Bertrand JC, Bertolus C. Unicystic ameloblastoma of the maxillary sinus: pitfalls of diagnosis and management. Hippokratia. 2010;14(3):217-220.
31. Jain K, Hsu J, Goyal P. The utility of a combined endoscopic and transoral resection of maxillary ameloblastoma. Int Forum Allergy Rhinol. 2013;3(9):762-765. doi:10.1002/ alr.21167
32. Herwig MC, Fischer HP, Moore CE, et al. Orbital invasion of a maxillary ameloblastoma. Article in German. Ophthalmologe. 2013;110(3):251-254. doi:10.1007/s00347-012-2622-z
33. Kochaji N, Barbar R, Al-Assaf M, Barakat C. Extremely rare maxillary unicystic ameloblastoma causing double vision: first case report in the Middle East. Int J Surg Case Rep 2023;109:108485. doi:10.1016/j.ijscr.2023.108485
34. Gupta D, Gulati A, Khurana N, Patel S. Maxillary ameloblastoma—rare tumor in a child. Int J Pediatr Otorhinolaryngol Extra. 2015;10(1):1-3. doi:10.1016/j.pedex.2014.10.004
35. Sakuntala AA, Choirunisa E, Arini SS, Prajogo JK, Pahlevi MR. Follicular ameloblastoma of maxillary: a case report. Med Hosp. 2024;11(1):119-124. doi:10.36408/mhjcm.v11i1.1048
36. Agani Z, Hamiti-Krasniqi V, Recica J, Loxha MP, Kurshumliu F, Rexhepi A. Maxillary unicystic ameloblastoma: a case report. BMC Res Notes. 2016;9(1):469. doi:10.1186/s13104-0162260-7
37. Li L, Aladimi MT, Wang L, Gao N, Helal HHl. A rare case of maxillary ameloblastoma, unicystic type lesion in a 4-year-old child: case report. J Oral Maxillofac Surg Med Pathol. 2016;28(6): 578-580. doi:10.1016/j.ajoms.2016.07.008
38. Lakshmi CR, Bhavana SM, Nallamilli SM, Prabhat MP, Sarat G, Anuradha C. Hybrid ameloblastoma of the maxilla: a puzzling pathology. Iran J Med Sci. 2016;41(4):340-344.
39. de Menezes LM, de Souza Cruz EL, Carneiro JT Jr, Kataoka MSDS, Alves Júnior SDM, Pinhero JDJV. Maxillary ameloblastoma in an elderly patient: report of a surgical approach. Hum Pathol Case Rep. 2017;10:25-29. doi:10.1016/j.ehpc.2016.08.002
40. Faras F, Abo-Alhassan F, Israël Y, Hersant B, Meningaud JP. Multi-recurrent invasive ameloblastoma: a surgical challenge. Int J Surg Case Rep. 2017;30:43-45. doi:10.1016/j. ijscr.2016.11.039
41. Jung SP, Jee YJ, Kim HK, et al. Surgical treatment for a huge maxillary ameloblastoma via Le Fort I osteotomy: a case report. J Korean Dent Sci. 2018;11(2):86-91.
42. Biörklund A, Elner A, Snorradottir M. Ameloblastoma of the maxilla. Report of three cases. J Laryngol Otol. 1979;93(11):1105-1113. doi:10.1017/s0022215100088186
43. Chebil A, Hasnaoui M, Bhar S, Masmoudi M, Bellalah A, Mighri K. Asymptomatic ameloblastoma of the maxilla with infratemporal fossa involvement: a case report. Int J Surg Case Rep 2022;98:107457. doi:10.1016/j.ijscr.2022.107457
44. Chu YK. Maxillary ameloblastoma: a pictorial case report. Ann Case Rep. 2016;1(2):16-18. doi:10.29011/2574-7754/100006
45. Ferreira TSH, Pimentel IMF, Albuquerque LAF, Gondim JA. Pure endoscopic transsphenoidal treatment of skull base ameloblastoma with intracranial extension: case report and literature review. Surg Neurol Int. 2020;11:228. doi:10.25259/SNI_45_2020
46. Sohal KS, Mlaga S, Vuhahula EA. A rare case of maxillary ameloblastoma with lung metastasis: a case report. Research Square. Preprint posted online February 11, 2020. doi:10.21203/rs.2.23191/v1
47. Linaburg TJ, Araya J, Briceño CA. Maxillary ameloblastoma with local recurrence, orbital invasion, and systemic metastases: a case report and review of the literature. Case Rep Ophthalmol. 2024;15(1):238-245. doi:10.1159/000537707
48. Yang R, Liu Z, Gokavarapu S, Peng C, Ji T, Cao W. Recurrence and cancerization of ameloblastoma: multivariate analysis of 87 recurrent craniofacial ameloblastoma to assess risk factors associated with early recurrence and secondary ameloblastic carcinoma. Chin J Cancer Res 2017;29(3):189-195. doi:10.21147/j.issn.1000-9604.2017.03.04
49. Sehdev MK, Huvos AG, Strong EW, Gerold FP, Willis GW. Proceedings: ameloblastoma of maxilla and mandible. Cancer. 1974;33(2):324-333. doi:10.1002/10970142(197402)33:2<324::aid-cncr2820330205>3.0.co;2-u
50. Reichart PA, Philipsen HP, Sonner S. Ameloblastoma: biological profile of 3677 cases. EurJ Cancer B Oral Oncol. 1995;31B(2):86-99. doi:10.1016/0964-1955(94)00037-5
51. González-González R, López-Verdín S, Lavalle-Carrasco J, et al. Current concepts in ameloblastoma-targeted therapies in B-raf proto-oncogene serine/threonine kinase V600E mutation: systematic review. World J Clin Oncol. 2020;11(1):31-42. doi:10.5306/wjco.v11. i1.31
52. Sweeney R, McClary AC, Myers BR, et al. Identification of recurrent SMO and BRAF mutations in ameloblastomas. Nature Genet. 2014;46(7):722-725. Erratum: 2015;47(1):97. doi:10.1038/ng.2986
Minimizing excess cement around implant restorations: an in vitro study of cementation techniques
Hayleen Moran, DDS, MS ¢ Nurit Bittner, DDS, MS, FACP
Excess cement around cement-retained implant crowns is associated with a higher incidence of peri-implantitis, but there are limited data to indicate which cement application technique minimizes excess cement. The purpose of this in vitro study was to evaluate the amount of excess cement that resulted from different cement application techniques. Fifty identical titanium custom abutments and monolithic zirconia crowns were digitally designed and milled in the shape of a maxillary first molar. Ten crowns were cemented by applying temporary cement only to the intaglio coronal surface of the crown; these specimens were used as a control group to determine the amount of cement to be used in all other groups. Four different cement application methods were evaluated (n = 10): wall layer technique, in which cement was brushed on the intaglio axial walls of the crown; precementation technique, in which cement was applied to the intaglio coronal aspect of the crown, and the crown was precemented on an abutment replica, quickly removed, and then repositioned on the milled abutment; rim application, in which cement was applied to the cervical marginal rim of the crown; and increased cement space, in which the cement space was increased to 60 μm (compared with 40 μm in other groups) and cement was brushed on the intaglio coronal surface. Digital photographs of the cemented crowns were taken, and image editing software was used to measure the displacement of excess cement, that is, the distance that it traveled below the finish line on the mesial, distal, buccal, and lingual surfaces. Excess cement was then removed from each specimen and weighed. An analysis of variance test was used to evaluate the difference among groups, and each pair of groups was compared with the t test. Compared with all of the other experimental groups, specimens cemented with the wall layer technique showed a significantly smaller amount of cement excess in terms of both the distance traveled and weight (P < 0.05). Based on the findings, the wall layer cementation technique, in which cement is brushed on the intaglio walls of the crown, is recommended to reduce excess cement around implant crowns.
Considerations of esthetics, retrievability, retention, success, and complication rates play important roles in the design of the final implant restoration.1 Screwretained implant restorations have the advantages of predictable retrievability and the possibility of reducing interocclusal space. However, screw-retained implant restorations require precise, prosthetically driven implant placement based on the position of the screw access hole.2 The manufacturing process for screw-retained restorations is also more technique sensitive and more demanding than that for cement-retained restorations.3 In addition, a systematic review by Sailer et al showed that chipping of the veneering ceramic tended to occur more frequently at the screw-retained restorations.4
While cement-retained implant restorations may be easier to fabricate than screw-retained prostheses, determining the right amount of cement to apply can be challenging.2,5 The effectiveness of methods to limit excess cement largely depends on the volume of the cement used and predesigned cement space. Reducing the amount of cement can compromise the retention, but excess cement could be detrimental to the soft tissues.6 The most common problem associated with cement-retained implant restorations is the difficulty of achieving complete removal of excess cement, especially from subgingival margins (sulcus depth greater than 3 mm), where residual cement can lead to peri-implantitis.7 In a clinical study, Wilson evaluated cement-retained restorations with the aid of a dental endoscope over a 5-year period and concluded that cement excess was associated with signs of peri-implantitis.8 The relationship between excess cement and peri-implantitis was substantiated by the complete remission of disease soon after the excess cement was removed.8
Most of the cements currently used to cement implant crowns are not sufficiently radiopaque, which makes it difficult to observe the presence of excess cement on radiographs.9 When subgingival excess resin cement is identified, removal is difficult, and the use of stainless steel instruments can create scratches in the abutment surface, which can accelerate plaque accumulation and may jeopardize soft tissue health.10 It would be advantageous to prevent these kinds of complications by minimizing the amount of excess cement during cementation procedures.
Various techniques have been proposed to minimize excess cement when implant restorations are cemented. The most commonly used techniques are limiting application of the cement to the occlusal half of the intaglio surface of the crown; the precementation technique; applying a piece of rubber dam for isolation; incorporating a vent hole in the crown; the rim cementation technique; applying the cement to the walls of the crown with a brush (wall layer technique); and leaving a 2-mm
space in the screw access channel.7,11-15 There is, however, no consensus on which cement application technique produces the least amount of excess cement.7,11-16
Wadhwani et al studied cement application techniques and the quantity of cement commonly used by dentists to cement implant crowns.14 They determined that the most common cementation techniques were the brush application technique; the marginal application technique, where the cement was applied to the marginal rim of the intaglio surface of the crown; and the gross application technique, where the cement was applied with a spatula. The authors found no difference in the quantities of cement used in the brush and marginal application techniques, but gross application with a spatula resulted in an excessive amount of cement in comparison with the other techniques. They concluded that the appropriate quantity of cement to use for cement-retained implant restorations is still under debate and current methods for cementation and controlling excess cement are imprecise.14
There is limited published information on the amount of excess cement produced by different cementation techniques. Chee et al used 4 different cementation techniques to evaluate excess cement weight and found that the precementation technique resulted in the least amount of excess cement.16 However, they did not use a standardized amount of cement for all techniques or measure the distance traveled by the cement.16
The objective of the present study was to evaluate the effect of different cement application techniques on the amount of excess cement produced around implant restorations. The displacement (distance traveled below the finish line) and weight of cement excess were measured, and the null hypothesis was that the amounts of excess cement produced by the various application techniques would not differ in terms of displacement or weight.
Methods
Specimen fabrication
Fifty identical custom titanium abutments and monolithic zirconia crowns were digitally designed and milled (Prosthetic Design Center software, Stoneglass Industries) in the shape of a maxillary first molar.
The custom abutments were torqued to analogs (implant replica, NobelReplace RP, Nobel Biocare) at 35 N/cm and mounted in a custom-made plastic mount (Delrin acetal plastic, DuPont; milled at Stoneglass Industries). The access hole was filled with polytetrafluoroethylene film tape and sealed with packable composite resin (Filtek Supreme Ultra, 3M).
Cementation procedures
The specimens were divided into 5 groups of 10 crownabutment pairs each. The crowns in each group were cemented with a different technique: control group; group 1, wall layer technique; group 2, precementation technique; group 3, rim application; group 4, increased cement space. All crowns were cemented with the same temporary cement (Temp-Bond NE, Kerr), used according to the manufacturer’s specifications of 1.5 minutes for working time and 7.0 minutes for setting time.
All groups were cemented with the use of a surveyor (surveyorparallelometer, J.M. Ney). A 5-kg weight was applied to the top of the surveyor to mimic the amount of force exerted when a patient bites down during the crown cementation procedure. The 5-kg weight was maintained on top of the surveyor for a total of 7 minutes for each specimen to ensure that the cement was fully set.
Control group
The control group was used to determine the amount of cement to be used in the 4 experimental groups. Each crown in the control group was cemented with a different amount of cement, increasing in 1-mm increments from 3 to 12 mm. To control the amount of cement used for each specimen, lines were drawn on a sheet of grid paper at 1-mm intervals, and cement was dispensed to reach the top of the appropriate measuring line on the paper. The cement was applied to the paper using the dispenser tip provided with the cement to ensure that the thickness was consistent. A brush (Microbrush tube applicators, regular size, Microbrush International) was used to apply the premeasured cement to the crown. The cement was brushed on the intaglio coronal surface of the crowns (Fig 1). The crowns were then cemented to the titanium abutments.
In specimens 1 to 5, which had 3 to 7 mm of cement, no cement was extruded from the crowns on any surface (mesial, distal, facial, or lingual), indicating that the amount of cement was insufficient. Specimens 6 to 10, which corresponded to 8 to 12 mm of cement, had excess cement on all surfaces. It was determined that the excess cement extruded from specimen 6 of the control group (placed with 8 mm of cement) was sufficient to enable measurement of displacement and weight. Therefore, to standardize the specimens, 8 mm of cement was applied to all 4 experimental groups.
Group 1: wall layer technique
The preestablished amount of temporary cement was applied evenly to the intaglio axial walls of the crown with a brush (Fig 2).
Group 2: precementation technique
To provide room for the cement, the intaglio surface of the crown was coated with polytetrafluoroethylene tape. A fastsetting polyvinyl siloxane registration material (Blu-Mousse,
Fig 1. Application of cement in the control group.
Parkell) was placed inside the crown to copy its internal shape, creating a replica of the abutment. A Microbrush was inserted to form a handle and support the abutment replica (Fig 3). This abutment replica was later used as a precementation device.
To ensure that the precemented specimens in group 2 would retain sufficient cement to produce excess cement in amounts analogous to the other groups, a trial specimen was cemented to the abutment replica with 8 mm of temporary cement, as established for the other groups. This specimen was used to calculate how much cement was retained on the replica after the crown was removed and thereby determine how much cement, if any, should be added to the standardized amount. Temporary cement was applied with a brush to the intaglio coronal surface of the crown, the crown was manually seated on the replica, and extra cement was quickly removed from the crown margins (Fig 4). The crown was then removed from the replica, completing the precementation procedure. All of the cement retained on the replica was collected and weighed (Gemini-20 Precision Milligram Scale, American Weigh Scales), establishing that precementation
resulted in a loss of 0.008 mg of cement. After various amounts of cement were weighed and subsequently measured on the grid paper to determine the millimeter equivalent of 0.008 mg of cement, it was found that 2 mm of cement should be added to the standard amount.
All of the specimens in group 2 were precemented to the abutment replica as described for the trial specimen, with the exception that their coronal surfaces received 10 mm of temporary cement instead of 8 mm.
Group 3: rim application technique
A brush was used to apply 8 mm of temporary cement to the intaglio cervical marginal rim of the crown.
Group 4: increased cement space
The crowns for group 4 were designed with 60 μm of cement space, while the crowns in all other groups had 40 μm of cement space. The temporary cement was brushed only on the coronal intaglio aspect of the crown.
Fig 2. Application of cement in the wall layer group.
Fig 3. Abutment replica made with polyvinyl siloxane.
Fig 4. Removal of excess cement prior to cementation in the precementation group.
Fig 5. Ruler used to calibrate measurements of excess cement displacement.
Measurements
After crown cementation, digital photographs were taken of the mesial, distal, buccal, and lingual surfaces of each specimen to evaluate the displacement of excess cement, which was characterized as the distance it traveled below the finish line. A millimeter ruler with 0.5 mm-increments was included in each photograph for use as a reference and measurement device (Fig 5). A total of 200 photos were examined by a single evaluator (N.B.) using digital image editing software (Photoshop CS5 for Mac OS X, Adobe). Digital lines were drawn at the top and bottom of the excess cement, and extended to the ruler to be able to measure the distance (Fig 6). The presence of the ruler prevented errors that could result from unequal scale dimensions in the images. The greatest distance per surface was recorded.
After the digital photographs were taken, all excess cement was removed from the specimens and weighed with a digital scale (Gemini-20 Precision milligram scale, American weight scales, AWS). The scale was accurate to 1.0 mg.
Statistical analysis
All measurements obtained for the groups were analyzed with a 1-way analysis of variance (ANOVA), and each pair of groups was compared with the t test. Values of P < 0.05 were considered statistically significant (Stata, version 12, StataCorp).
Results
Table 1 presents the mean displacement value and weight of excess cement for each experimental group. Overall, excess cement traveled the shortest distance in the wall layer technique (group 1). For all groups, the least displacement occurred on the buccal surface. However, no statistically significant difference was observed in the distances traveled on the 4 surfaces within each group (ANOVA). When the distance that excess cement traveled on each surface was compared among groups, only the lingual and distal surfaces showed statistically significant differences (P < 0.001 and P = 0.035, respectively; ANOVA), with the shortest distance observed in group 1 and the longest in group 4 (increased cement space).
When t tests were used to compare groups in pairs, statistically significant differences in the distance of cement displacement were observed among several groups (Table 2). Statistically significant differences were observed between group 1 and all other experimental groups: 1 vs 2 (precementation technique), P < 0.001; 1 vs 3 (rim application technique), P = 0.0014; and 1 vs 4, P < 0.00001). Comparison between groups 3 and 4 also showed a statistically significant difference (P = 0.0024), with a shorter mean distance in group 3. No statistically significant difference was observed between groups 2 and 3 or groups 2 and 4.
Group 1 had the lowest mean weight of excess cement among the experimental groups. The weight was significantly different among all groups (P = 0.008; ANOVA). Comparison of the mean cement weights by pairs (t test) revealed statistically significant differences between group 1 and all other experimental groups: 1 vs 2, P = 0.0026; 1 vs 3, P = 0.024; and 1 vs 4, P =0.0038. No statistically significant differences were observed in any pairings of groups 2 to 4.
Discussion
Excess cement has a direct impact in the incidence of periimplantitis.8 Establishing not only the correct amount of cement but also the best cement application technique is crucial to preventing complications. However, cementation methods described in the literature lack uniformity and precision, and there is no consensus in the dental community regarding the appropriate quantity of cement or placement method for a cement-retained implant crown.14
The current study aimed to determine the best approach to reducing the amount of excess cement around implant crowns by assessing the 4 cement application techniques most commonly described in the literature. The null hypothesis, that the amounts of excess cement produced by the various application techniques would not differ in terms of displacement or weight, was rejected. Based on the results of the study, the technique that produced the least amount of excess cement, with the shortest distance traveled and lowest weight, was the wall layer technique, which involved brushing the cement evenly on the intaglio axial walls of the crown (group 1). The technique that resulted in the greatest amount of excess cement was an increase in the cement space and application of the cement on the intaglio coronal aspect of the crown (group 4).
The positive results obtained with the wall layer technique could be the result of a more uniform distribution of the cement on the intaglio surface of the crown. The negative results observed in the specimens with increased cement space could be the result of the cement application technique, rather than the increased space. Cement was brushed only on the intaglio coronal surface, which might have prevented even distribution.
The precementation technique evaluated in this study had limitations. The use of polytetrafluoroethylene tape as a cement spacer could have altered the results, since there could have been variability in its adaptation to the intaglio surface of the crown. It is also possible that the replica abutment was not accurate, allowing excess cement to remain in the crown before cementation to the final abutment. It could also be argued that the results were affected by the
Fig 6. Measurement of excess cement displacement using the blue lines that border the top and bottom of the excess cement and extend to the ruler.
Table
Measurement
Displacement, mma
Mesial
Distal
Buccal
excess cement around implant restorations according to cementation technique (n = 10 per group).
use of additional cement (2 mm) to compensate for the cement that remained on the abutment replica. However, other reports in the literature indicate that the precementation technique is not recommended because it significantly reduces crown retention.17 The lack of retention could be caused by an insufficient amount of cement, since a portion of the cement remains on the abutment replica. Adding cement could improve retention of the crown when this technique is used. It is also important to consider that the precementation technique would not be indicated for cementation of multiple units, since it would not be possible to complete the precementation of all units during the working time of most cements.
The results of the current study do not agree with the results reported by Chee et al, where the precementation technique showed the least amount of excess cement.16 One difference between the studies was that the present study used an anatomical abutment and crown in the shape of a molar, whereas Chee et al used a conical abutment, which could have affected the way the cement flowed.16 Bukhari et
al also reported favorable results for the precementation technique, but the fact that it is not applicable to multiunit restorations should also be taken into account.18
This study presents several limitations. It is difficult to completely replicate the clinical setting during in vitro experiments; however, a surveyor with a 5-kg load was used in an attempt to simulate occlusal forces during cementation of the specimens. Furthermore, this research was limited to the use of a maxillary crown, and additional research on a different type of tooth may be indicated. Another limitation of the study is the accuracy of the measuring devices. The scale used has an accuracy of 0.001 g. However, despite the fact that weights less than 0.001 g could not be accurately measured, statistically significant results were obtained for excess cement weights. In addition, the use of a metallic ruler to measure the distance that the cement traveled could result in inaccuracies; an alternative would have been to use transparent micrograph paper for measurement. However, the use of image editing software to extend a line digitally from the excess cement to the ruler helped to establish an accurate reading of the travel distance. Additional research evaluating the increased cement space approach may be beneficial. For this group, the cement was applied to the coronal aspect; however, since the wall layer technique showed the most positive results, using this technique in conjunction with increased cement space may be the ideal combination to reduce the excess cement to a minimum.
Conclusion
The present study evaluated the 4 most commonly used techniques for applying cement to cement-retained implant crowns to assess which method produced the least excess cement. The amount of excess cement was measured in terms of both displacement (distance that cement traveled) and weight, and the wall layer technique, in which the cement is brushed evenly on the intaglio axial walls of the crown, provided the best control over the amount of excess cement.
Table 2. Statistical (t test) comparisons between pair of groups (n = 10 per group).
1. Measurements of
Author affiliations
Private practice, New York, New York (Moran); Division of Prosthodontics, College of Dental Medicine, Nova Southeastern University, Fort Lauderdale, Florida (Bittner).
Correspondence
Nurit Bittner, DDS, MS, FACP (nbittner@nova.edu).
Conflicts of interest
None reported.
Funding
Stoneglass Industries provided the titanium milled abutments, all zirconia crowns, and the mount for the analog used in this study.
References
1. Lee A, Okayasu K, Wang HL. Screw- versus cement-retained implant restorations: current concepts. Implant Dent. 2010;19(1):8-15. doi:10.1097/ID.0b013e3181bb9033
2. Wittneben JG, Millen C, Brägger U. Clinical performance of screw- versus cement-retained fixed implant-supported reconstructions—a systematic review. Int J Oral Maxillofac Implants 2014;29(Suppl):84-98. doi:10.11607/jomi.2014suppl.g2.1
3. Michalakis KX, Hirayama H, Garefis PD. Cement-retained versus screw-retained implant restorations: a critical review. Int J Oral Maxillofac Implants. 2003;18(5):719-728.
4. Sailer I, Mühlemann S, Zwahlen M, Hämmerle CH, Schneider D. Cemented and screw-retained implant reconstructions: a systematic review of the survival and complication rates. Clin Oral Implants Res. 2012;23(Suppl 6):163-201. doi:10.1111/j.1600-0501.2012.02538.x
5. Hebel KS, Gajjar RC. Cement-retained versus screw-retained implant restorations: achieving optimal occlusion and esthetics in implant dentistry. J Prosthet Dent. 1997;77(1):28-35. doi:10.1016/s0022-3913(97)70203-8
6. Galván G, Kois JC, Chaiyabutr Y, Kois D. Cemented implant restoration: a technique for minimizing adverse biologic consequences. J Prosthet Dent. 2015;114(4):482-485. doi:10.1016/j.prosdent.2014.10.017
7. Kim HJ, Karasan D, Park K, Kwon HB, Han JS, Lee JH. Abutment margin levels and residual cement occurrence in cement-retained implant restorations: an observational study. Clin Oral Implants Res. 2023;34(1):33-41. doi:10.1111/clr.14015
8. Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontol. 1999;80:1388-92 2009;80(9):13881392. doi:10.1902/jop.2009.090115
9. Wadhwani C, Hess T, Faber T, Piñeyro A, Chen CS. A descriptive study of the radiographic density of implant restorative cements. J Prosthet Dent. 2010;103(5):295-302. doi:10.1016/ S0022-3913(10)60062-5
10. Agar JR, Cameron SM, Hughbanks JC, Parker MH. Cement removal from restorations luted to titanium abutments with simulated subgingival margins. J Prosthet Dent. 1997;78(1):43-47. doi:10.1016/s0022-3913(97)70086-6
11. Wadhwani C, Piñeyro A. Technique for controlling the cement for an implant crown. J Prosthet Dent. 2009;102(1):57-58. doi:10.1016/S0022-3913(09)60102-5
12. Seo CW, Seo JM. A technique for minimizing subgingival residual cement by using rubber dam for cement-retained implant crowns. J Prosthet Dent. 2017;117(2):327-328. doi:10.1016/j.prosdent.2016.08.024
13. Schwedhelm ER, Lepe X, Aw TC. A crown venting technique for the cementation of implantsupported crowns. J Prosthet Dent. 2003;89(1):89-90. doi:10.1067/mpr.2003.66
14. Wadhwani C, Hess T, Piñeyro A, Opler R, Chung KH. Cement application techniques in luting implant-supported crowns: a quantitative and qualitative survey. Int J Oral Maxillofac Implants. 2012;27(4):859-864.
15. Al Amri MD, Al-Johany SS, Al-Qarni MN, Al-Bakri AS, Al-Maflehi NS, Abualsaud HS. Influence of space size of abutment screw access channel on the amount of extruded excess cement and marginal accuracy of cement-retained single implant restorations. J Prosthet Dent. 2018;119(2):263-269. doi:10.1016/j.prosdent.2017.03.013
16. Chee WW, Duncan J, Afshar M, Moshaverinia A. Evaluation of the amount of excess cement around the margins of cement-retained dental implant restorations: the effect of the cement application method. J Prosthet Dent. 2013;109(4):216-221. doi:10.1016/S00223913(13)60047-5
17. Jimenez RA, Vargas-Koudriavtsev T. Effect of preseating, screw access opening, and vent holes on extrusion of excess cement at the crown-abutment margin and associated tensile force for cement-retained implant restorations. Int J Oral Maxillofac Implants. 2016;31(4):807-812. doi:10.11607/jomi.4143
18. Bukhari SA, AlHelal A, Kattadiyil MT, Wadhwani CPK, Taleb A, Dehom S. An in vitro investigation comparing methods of minimizing excess luting agent for cement-retained implantsupported fixed partial dentures. J Prosthet Dent. 2020;124(6):706-715. doi:10.1016/j. prosdent.2019.11.016
What every dentist needs to know about chocolate
Emily M. D. Wieser ¢ Jeffery B. Price, DDS, MS ¢ Christina L. Platia, DDS ¢ Nasir Bashirelahi, PhD
Chocolate is one of the most popular treats in the world. Debate over the potential benefits of its consumption has made chocolate a widely researched health topic. This article reviews the general health benefits of chocolate consumption, focusing on its involvement with the oral microbiota, caries development, and biofilm control, and discusses the potential negative consequences of excess chocolate consumption.
Chocolate can be traced back to as early as 1900 bce in Mesoamerica in the form of a bitter drink made from cocoa beans.1 Considered a gift from the gods, chocolate was used in healing practices and rituals such as weddings, baptisms, and funerals.1,2 Aztecs utilized cocoa beans as a natural treatment for more than 150 diseases. 3 During the 1500s, Spanish conquistadors brought chocolate from central America, where cocoa trees were first cultivated, to the European continent. The Spanish made modifications to the drink, including adding cane sugar and cinnamon, and it quickly became popular with the aristocratic and wealthy classes and a symbol of fortune and power.4,5
The worldwide popularity and consumption of chocolate was made possible by the invention of the cocoa press, which made chocolate cheaper to produce and more accessible to people of all social classes. In the 19th and early 20th centuries, driven by rising incomes, falling prices, and consumer preferences, chocolate became a mass produced and consumed product. 5 The popularity of chocolate has continued to grow and expand around the world, and the industry is now a billion dollar market. 6
Types of chocolate
Chocolate is classified into 3 categories: dark chocolate, milk chocolate, and white chocolate. The main differences in these categories are the quantity of cocoa bean solids and the presence of added ingredients (such as sugar, whole milk, or hazelnut).4 During chocolate production, cocoa beans are roasted and processed before other ingredients are added.7 Dark chocolate has the highest percentage of cocoa bean solids, ranging from 50% to 90%. Milk chocolate and gianduja chocolate (chocolate with hazelnut paste) have lower amounts of cocoa bean solids, ranging from 10% to 50%, but most commonly about 25%. White chocolate contains no cocoa bean solids and is primarily made from the cocoa butter produced during cocoa bean roasting and processing.4
The key chocolate components associated with its potential health benefits include flavanols (from the flavonoid family), methylxanthines (caffeine and theobromine), serotonin, tryptophan, β-phenylethylamine, magnesium, zinc, selenium, copper, potassium, riboflavin, and iron. 8 Flavanols are a polyphenolic compound and responsible for most of the health benefits associated with chocolate, demonstrating possible antioxidant and anti-inflammatory effects. The flavanol and general polyphenol levels in chocolate are directly associated with the percentage of cocoa bean solids. Therefore, since cocoa powder is simply ground cocoa bean solids, it is considered the most concentrated form of flavanols available in chocolate.9 Among the processed chocolates, dark chocolate contains the highest flavanol content, followed by milk chocolate and then white chocolate.10
Because dark chocolate has greater cocoa bean solid content and fewer added ingredients, researchers generally recommend consumption of dark chocolate for the best potential health benefits.9
Sugar-free vegan chocolate has been developed as a possible healthier alternative to milk chocolate. Instead of cocoa powder and sugar, this chocolate is made using carob powder and stevia. Carob powder is similar to cocoa powder in that it has a high polyphenol composition, but its naturally sweeter flavor allows for the addition of less sugar. Stevia is a naturally sweet sugar alternative derived from the plant Stevia rebaudiana . Studies have shown that stevia has antihypertensive, antioxidant, and antibacterial properties as well as other beneficial biologic effects. 3
Systemic benefits
Heart health
Polyphenols, specifically flavanols, act as antioxidants.11 Antioxidants protect the body from free radicals that cause oxidative stress, which can contribute to heart disease, cancers, and other health issues.12 The antioxidant properties of chocolate, especially dark chocolate, can decrease the risk of hypertension and other cardiovascular diseases.11 Studies have demonstrated that people who consume higher amounts of chocolate exhibit a lower risk of myocardial infarction and ischemic heart disease than those who consume lower amounts of chocolate.13 A study of 31,823 Swedish women aged 48 to 83 years old found that moderate consumption of chocolate (50 g per day, 7 servings per week) reduced the risk of heart failure.14 However, consuming more than 10 servings per week increased the risk of heart failure.14 The reduction in the risk of hypertension occurs because flavanols from the cocoa bean solids increase endothelial nitric oxide production, which in turn induces vasodilation, thereby reducing blood pressure.15
The polyphenolic compounds in chocolate also reduce the low-density lipoprotein oxidative effect and atherogenesis, resulting in decreased risk of coronary disease.16 While these trends have been observed in human subjects, more precise and accurate studies, such as randomized clinical trials, are needed to verify the cardiovascular benefits of chocolate.11
Plasma and urine metabolites
Chocolate also has a positive impact on metabolic processes in the body. Research has indicated that the active ingredients in dark chocolate have metabolic effects on the levels of gut microbial metabolites in urinary excretion.17 In patients with a high-stress profile, consuming dark chocolate resulted in a reduction of the stress hormone cortisol to levels found in patients with lower stress profiles. These patients also experienced a normalization of stress-related energy metabolism differences and gut microbial activities.17 The bioactive compounds of both dark chocolate rich in flavan-3-ol and standard dark chocolate were also shown to impact endogenous and colonic metabolic activity.18 These studies suggested that dark chocolate consumption may improve the body’s metabolic response to stress and may be associated with a reduction in mental and physical stress.17
Kidney health
The flavonoids found in chocolate may have an important role in reno-protective activity since they possess antiapoptotic and antifibrotic properties. Studies found that flavonoids reduced oxidative stress and inflammation in kidneys.19 For example, in rat and mouse models, flavonoids were observed to protect the kidneys from nephrotoxic compounds. Furthermore, studies have shown that flavonoids possess antitumor capabilities.19 In renal carcinoma cells, flavonoids induced cell cycle arrest and apoptosis, which inhibited cancer progression.
Other health benefits
A 100-g serving of dark chocolate is 600 calories and contains 50 g of carbohydrates and 35 g of fat, yet studies have shown higher consumption of any chocolate is associated with lower fat deposition.20 Chocolate’s polyphenols decrease intestinal absorption of lipids and carbohydrates, making it less likely to contribute to obesity.20 In addition, polyphenol-rich cocoa may act as a natural alternative treatment for diabetes by reducing insulin resistance.21 Studies have shown that polyphenol-containing foods increased insulin release and reduced blood glucose levels in diabetic rat models. Polyphenol-containing foods also controlled carbohydrate metabolism by restoring β-cells to improve insulin release and glucose metabolic activity.21
The anti-inflammatory effects of polyphenols also benefit the central nervous system by increasing cerebral blood flow.8 As a result, oxygen and glucose supply to the brain is improved and metabolic waste is discarded, thereby helping to protect against strokes. Studies have also suggested that the anti-inflammatory effects of polyphenols may limit progression of Parkinson and Alzheimer diseases.8
Chocolate consumption also can have a positive impact on the human gut microbiota by virtue of its prebiotic effects. Cocoa ingestion has been found to increase growth of Lactobacillus and Bifidobacterium spp, which play important roles in digestion and protection in the gut microbiota.22
The antioxidant and anti-inflammatory capabilities of chocolate also can contribute to skin health. By slowing down free radical activities, chocolate protects skin cells from potential damage and reverses signs of aging. Cocoa powder–based products have the potential to be used in products to treat sensitive or dry skin and protect against aging.3
Oral health benefits
Dark chocolate consumption may also contribute positively to oral health. Many of the essential nutrients in oral fluids that maintain antioxidant levels are not produced by the body and therefore must be consumed. Some of these important nutrients include polyphenols such as flavonoids. Polyphenols play a role in preventing cellular interactions with periodontal pathogens and the production of virulence factors. Flavonoids have antioxidant, anti-inflammatory, antiplatelet, and antitumor capabilities, which can help protect the oral microbiome.12 Dark chocolate is an especially excellent source of these compounds. Dark chocolate also contains unsaturated free fatty acids (eg, oleic and linoleic acids) that have antibacterial properties against Streptococcus mutans. Antibacterial properties are found more often in
dark chocolate than other types of chocolate because of its higher cocoa bean solid concentrations. 23
Cocoa has plaque-limiting capabilities because it contains inhibitors of the dextransucrase enzyme.24 Found in cacao plants, theobromine is an important compound in cocoa products that plays a role in limiting plaque formation. An in vitro study compared the effects of theobromine-based and traditional fluoride-based toothpastes.25 The theobromine-based toothpaste resulted in greater zones of inhibition for S mutans, Lactobacillus acidophilus, and Enterococcus faecalis than did fluoride-based toothpastes. Other studies have reported similar findings. One study reported a decrease in plaque scores after patients used a mouthrinse developed from the husks of cocoa beans.26 This reduction in plaque was attributed to the inhibition of the dextransucrase enzyme, which helps limit the formation of plaque.
Dark chocolate also contains properties that help reduce the loss of tooth structure and protect enamel and dentin.23 Theobromine has also been found to protect teeth from caries better than fluoride.25 In addition, theobromine is nontoxic, unlike fluoride. Higher theobromine concentrations are found in foods with a content of higher cocoa bean solids, such as dark chocolate. Therefore, dark chocolate may contribute to an increase in the hardness of enamel and dentin as a result of the increased cocoa concentration.25
Finally, increased use of cocoa products has been linked to lower serum levels of tumor necrosis factor α (TNF-α), an inflammatory cytokine that can cause pulpal inflammation, periodontitis, and oral pain when overexpressed. 27,28 A study analyzing adult patients with slight or moderate chronic periodontitis found that increased salivary TNF-α levels corresponded to deeper periodontal probing depths and clinical attachment levels greater than 5 mm. 29 The flavonoid content of chocolate offers a possible treatment option for TNF-α overexpression. A study observed the effects of using cocoa in the treatment of periodontitis that was induced in an animal model. 30 Animals that were treated with cocoa had lower serum TNF-α levels than animals not treated with cocoa. While the authors recommended further research be completed on the cocoa diet and its effects, they also suggested that there is a connection between a cocoa-enriched diet and decreased TNF-α levels. 30 The flavonoid content of chocolate is also believed to prevent synthesis of prostaglandin E2 and matrix metalloproteinases—major factors in gingival inflammation and tooth degradation—thereby inhibiting progression of periodontitis. 27
Chocolate alternatives containing carob powder and stevia have similar positive oral implications. The high polyphenol content present in carob powder is similar to the antioxidant and protective capabilities found in polyphenols in regular chocolate. Stevia leaves have anticariogenic and antibacterial activities against S mutans, Streptococcus sobrinus, and L acidophilus, all of which can cause dental plaque formation.3
Negative effects of chocolate
While chocolate is associated with many health benefits, it has some notable negative effects as well. Although dark chocolate is associated with the majority of the health benefits described,
milk chocolate is the predominant form of chocolate consumed in the United States. Milk chocolate contains lower amounts of beneficial polyphenols and higher amounts of sugar.31 Every 44-g serving of milk chocolate contains 22.7 g of sugar, which is the source of many of the negative effects of chocolate.32 Sugar consumption activates the dopamine-response reward center of the brain, which is associated with addictive tendencies, pushing people toward overconsumption.33 Increased sugar consumption is also associated with an increased risk of developing diabetes.34
In terms of oral health, sugar consumption is linked to the development of dental caries.35 A study on sugar consumption in university students found that suboptimal toothbrushing and dental caries were more common in students eating chocolate, candy, or chips.36 Self-reporting by the students demonstrated that frequent consumption of chocolate or candy was also linked to the presence of carious lesions as well as more toothaches. A survey on children’s dental health found a higher rate of caries in children who consumed sweets and chocolate.37 While toothbrushing lessened the negative impacts of consuming sweets and chocolate, the results suggested that the best option for reducing caries is a combination of decreased sugar consumption and increased toothbrushing. Since the dental health data were based on parental recall, additional prospective studies are needed to explore the link between chocolate and candy consumption and dental caries.37
Conclusion
Chocolate continues to be one of the most popular sweet treats around the world. Recent studies evaluating the potential health benefits of chocolate consumption have indicated that the polyphenol contents of chocolate, dark chocolate in particular, have antioxidant and anti-inflammatory effects and protect against dental caries and plaque formation. While the overconsumption of chocolate, especially milk chocolate, has negative health effects due to its sugar content, additional research should be done to explore the potential benefits of incorporating chocolate into the diet as well as its effects on oral health.
Author affiliations
University of Maryland, College Park, Maryland (Wieser); Department of Oncology and Diagnostic Sciences, University of Maryland School of Dentistry, Baltimore, Maryland (Price, Bashirelahi); Department of Comprehensive Dentistry, Division of General Practice, University of Maryland School of Dentistry, Baltimore, Maryland (Platia).
1. Mozdy M. Chocolate: its origins. Natural History Museum of Utah. August 14, 2016. Accessed May 5, 2024. https://nhmu.utah.edu/articles/2023/05/chocolate-its-origins
2. Lippi D. Sin and pleasure: the history of chocolate in medicine. J Agric Food Chem. 2015;63(45):9936-9941. doi:10.1021/acs.jafc.5b00829
3. Dumbrava D, Popescu LA, Soica CM, et al. Nutritional, antioxidant, antimicrobial, and toxicological profile of two innovative types of vegan, sugar-free chocolate. Foods 2020;9(12):1844. https://doi.org/10.3390/foods9121844
4. Montagna MT, Diella G, Triggiano F, et al. Chocolate, “food of the gods”: history, science, and human health. Int J Environ Res Public Health. 2019;16(24):4960. doi:10.3390/ ijerph16244960
5. Poelmans E, Swinnen J. A brief economic history of chocolate. In: Squicciarini MP, Swinnen J, eds. The Economics of Chocolate. Oxford University Press; 2016:11-46.
6. Klein C. Chocolate’s sweet history: from elite treat to food for the masses. History.com. Updated May 16, 2023. Accessed May 5, 2024. https://www.history.com/news/the-sweethistory-of-chocolate
7. Claims about cocoa: can chocolate really be good for you? NIH News in Health. August 2011. Accessed May 5, 2024. https://newsinhealth.nih.gov/2011/08/claims-about-cocoa
8. Nowaczewska M, Winciński M, Kaźmierczak W, Kaźmierczak H. To eat or not to eat: a review of the relationship between chocolate and migraines. Nutrients. 2020;12(3):608. doi:10.3390/nu12030608
9. A healthy way to show your love? Tufts Health & Nutrition Letter. 2024;41(12):1,7.
10. Pimentel FA, Nitzke JA, Klipel CB, de Jong EV. Chocolate and red wine—a comparison between flavonoids content. Food Chem. 2010;120(1):109-112. doi:10.1016/j.foodchem. 2009.09.078
11. Garcia JP, Santana A, Baruqui DL, Suraci N. The cardiovascular effects of chocolate. Rev Cardiovasc Med. 2018;19(4):123-127. doi:10.31083/j.rcm.2018.04.3187
12. Kaur G, Kathariya R, Bansal S, Singh A, Shahakar D. Dietary antioxidants and their indispensable role in periodontal health. J Food Drug Anal. 2016;24(2):239-246. doi:10.1016/j.jfda. 2015.11.003
13. Yuan S, Li X, Jin Y, Lu J. Chocolate consumption and risk of coronary heart disease, stroke, and diabetes: a meta-analysis of prospective studies. Nutrients. 2017;9(7):688. doi:10.3390/ nu9070688
14. Gong F, Yao S, Wan J, Gan X. Chocolate consumption and risk of heart failure: a metaanalysis of prospective studies. Nutrients. 2017;9(4):402. doi:10.3390/nu9040402
15. Persson IA, Persson K, Hägg S, Andersson RG. Effects of cocoa extract and dark chocolate on angiotensin-converting enzyme and nitric oxide in human endothelial cells and healthy volunteers—a nutrigenomics perspective. J Cardiovasc Pharmacol. 2011;57(1):44-50. doi:10.1097/FJC.0b013e3181fe62e3
16. Baba S, Osakabe N, Kato Y, et al. Continuous intake of polyphenolic compounds containing cocoa powder reduces LDL oxidative susceptibility and has beneficial effects on plasma HDL-cholesterol concentrations in humans. Am J Clin Nutr. 2007;85(3):709-717. doi:10.1093/ajcn/85.3.709
17. Martin FP, Rezzi S, Peré-Trepat E, et al. Metabolic effects of dark chocolate consumption on energy, gut microbiota, and stress-related metabolism in free-living subjects. J Proteome Res. 2009;8(12):5568-5579. doi:10.1021/pr900607v
18. Ostertag L, Philo M, Colquhoun IJ, et al. Acute consumption of flavan-3-ol-enriched dark chocolate affects human endogenous metabolism. J Proteome Res. 2017;16(7):2516-2526. doi:10.1021/acs.jproteome.7b00089
19. Vargas F, Romecín P, García-Guillén AI, et al. Flavonoids in kidney health and disease. Front Physiol. 2018;9:394. doi:10.3389/fphys.2018.00394
20. Cuenca-García M, Ruiz JR, Ortega FB, Castillo MJ; HELENA Study Group. Association between chocolate consumption and fatness in European adolescents. Nutrition. 2014;30(2):236-239. doi:10.1016/j.nut.2013.07.011
21. Solayman M, Ali Y, Alam F, et al. Polyphenols: potential future arsenals in the treatment of diabetes. Curr Pharm Des. 2016;22(5):549-565. doi:10.2174/1381612822666151125001111
22. Martin MÁ, Ramos S. Impact of cocoa flavanols on human health. Food Chem Toxicol. 2021;151:112121. doi:10.1016/j.fct.2021.112121
23. Hamasaeed NH, Toma IS, Abdullah AO, Kadir SK. Assessing the impact of varied dark chocolate concentrations on enamel and dentine microhardness. Appl Sci. 2024;14(1):382. https://doi.org/10.3390/app14010382
24. Andújar I, Recio MC, Giner RM, Ríos JL. Cocoa polyphenols and their potential benefits for human health. Oxid Med Cell Long. 2012;2012:906252. https://doi.org/10.1155/2012/ 906252
25. Lakshmi A, Vishnurekha C, Baghkomeh PN. Effect of theobromine in antimicrobial activity: an in vitro study. Dent Res J (Isfahan). 2019;16(2):76-80.
26. Srikanth RK, Shashikiran ND, Subba Reddy VV. Chocolate mouth rinse: effect on plaque accumulation and mutans streptococci counts when used by children. J Indian Soc Pedod Prev Dent. 2008;26(2):67-70. doi:10.4103/0970-4388.41619
27. Fideles SOM, Ortiz AC, Reis CHB, Buchaim DV, Buchaim RL. Biological properties and antimicrobial potential of cocoa and its effects on systemic and oral health. Nutrients 2023;15(18):3927. doi:10.3390/nu15183927
28. Hall BE, Zhang L, Sun ZJ, et al. Conditional TNF-α overexpression in the tooth and alveolar bone results in pulpitis and osteitis. J Dent Res. 2016;95(2):188-195. doi:10.1177/ 0022034515612022
29. Kibune R, Muraoka K, Morishita M, Ariyoshi W, Awano S. Relationship between dynamics of TNF-α and its soluble receptors in saliva and periodontal health state. Dent J (Basel) 2022;10(2):25. doi:10.3390/dj10020025
30. Tomofuji T, Ekuni D, Irie K, et al. Preventive effects of a cocoa-enriched diet on gingival oxidative stress in experimental periodontitis. J Periodontol. 2009;80(11):1799-1808. doi:10.1902/jop.2009.090270
31. Vinson JA, Proch J, Zubik L. Phenol antioxidant quantity and quality in foods: cocoa, dark chocolate, and milk chocolate. J Agric Food Chem. 1999;47(12):4821-4824. doi:10.1021/ jf990312p
32. Candies, milk chocolate. FoodData Central Search Results. April 1, 2019. Accessed May 5, 2024. US Department of Agriculture. https://fdc.nal.usda.gov/fdc-app.html#/fooddetails/167587/nutrients
33. Why do we overeat? Tufts Health & Nutrition Letter. 2019;37(7):4:5.
34. Basu S, Yoffe P, Hills N, Lustig RH. The relationship of sugar to population-level diabetes prevalence: an econometric analysis of repeated cross-sectional data. PLoS One 2013;8(2):e57873. doi:10.1371/journal.pone.0057873
35. Chi DL, Scott JM. Added sugar and dental caries in children: a scientific update and future steps. Dent Clin North Am. 2019;63(1):17-33. doi:10.1016/j.cden.2018.08.003
36. Peltzer K, Pengpid S. Dental health status and oral health behavior among university students from five ASEAN countries. Nagoya J Med Sci. 2017;79(2):123-133. doi:10.18999/ nagjms.79.2.123
37. Skafida V, Chambers S. Positive association between sugar consumption and dental decay prevalence independent of oral hygiene in pre-school children: a longitudinal prospective study. J Public Health (Oxf). 2018;40(3):e275-e283. doi:10.1093/pubmed/fdx184
Surgical treatment of peri-implantitis via multiple decontamination procedures and a regenerative protocol: a case report with 6-year follow-up
Ísis de Fátima Balderrama, DDS, MSc, PhD ¢ Guilherme José Pimentel Lopes de Oliveira, DDS, MSc, PhD
Nicolas Nicchio, DDS, MSc ¢ Ana Carolina Monachini-Marcantonio, DDS, MSc, PhD
Elcio Marcantonio-Junior, DDS, MSc, PhD
Peri-implantitis is an inflammatory disease around dental implants that induces progressive bone resorption. Several procedures for decontaminating the implant surface and promoting bone growth have been established to treat this condition. The purpose of the present case report was to describe the decontamination method used to achieve peri-implant health in a 60-year-old man who had a single implant that had been in function in the mandibular left molar region for 10 years. The implant, in the region of the first molar, was osseointegrated and showed radiographic bone loss associated with a probing depth of 8 mm and bleeding on probing. The diagnosis was peri-implantitis, and a surgical treatment approach was selected to enable decontamination of the area with a combination of mechanical debridement, tetracycline hydrochloride (500 mg/mL), and photodynamic therapy. After the decontamination process, a sodium bicarbonate spray device was used, and a guided bone regeneration protocol with a xenogeneic graft and collagen membrane was performed to reestablish the peri-implant bone height. A connective tissue graft was placed to obtain a better biological seal and increase the peri-implant keratinized mucosa. Follow-up examinations performed 30 days, 5 months, 3 years, and 6 years after the surgical procedure revealed new bone formation and progressively reduced probing depths. The successful outcome in this case suggests that combining different decontamination procedures and a bone regeneration protocol could be an effective approach to inducing bone formation around dental implants in patients with peri-implantitis.
Peri-implantitis, a pathologic condition that occurs around an osseointegrated implant in function, is characterized clinically by inflammation of the peri-implant tissue associated with progressive bone loss.1 The treatment of peri-implantitis is focused on the removal of bacterial biofilm and subsequent implant surface decontamination to create conditions that will promote reosseointegration of the implant.2-4 Several approaches to decontamination of dental implants diagnosed with peri-implantitis have been described in the literature.3 Decontamination can be performed by mechanical or chemical methods used with nonsurgical or surgical approaches. The mechanical methods include manual instrumentation with metal or plastic curettes or titanium brushes; ultrasonic scaling; air-powder abrasion; and laser or photodynamic therapy.4-6 However, no specific protocol has been established as a gold standard decontamination method.7,8 In addition, different nonsurgical and surgical approaches have been proposed to control peri-implantitis.9
Peri-implantitis is characterized by bone loss, and the goal of treatment is to restore and stabilize tissue support for the implant through reconstructive techniques that fill the defects with newly formed bone.10 To add to the body of scientific evidence about long-term outcomes of treatment for periimplantitis, the present case report describes the surgical treatment of an implant affected by peri-implantitis after 10 years of loading. Mechanical and chemical decontamination methods were combined with guided regenerative surgery to promote bone formation around the implant.
Case report
A 60-year-old man who was a nonsmoker and in good general health presented at the Araraquara School of Dentistry, São Paulo State University, for routine evaluation of a dental implant that had been in function for 10 years. The patient’s chief concern was pain around the implant, which was located in the region corresponding to the mandibular left first molar. A dentist in a different private clinic had attempted to treat the periimplantitis through a surgical procedure about 5 to 6 months previously but with unsatisfactory results. That dentist had already removed the prosthetic crown and placed a cover screw.
The implant demonstrated no mobility during the clinical examination, but the examination revealed the presence of bleeding on probing, a lack of keratinized peri-implant mucosa,
and probing depths greater than 8 mm (Fig 1). A radiographic examination revealed that the implant was 13 mm long and had an external hexagon connection (Fig 2). There was evidence of bone loss around the implant. According to the definitions outlined in the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions, the results of the clinical and radiographic examinations indicated a diagnosis of peri-implantitis.1
As the first step in treatment, nonsurgical periodontal supportive therapy was performed to reduce inflammation, and the patient was instructed in regular oral hygiene procedures with emphasis on the area of the implant. The surgical treatment was performed 2 weeks after initial therapy. The surgical procedure started with administration of 4% articaine with 1:100,000 epinephrine for local anesthesia. After anesthesia was established, a crestal incision was made and a full-thickness flap was raised on both the buccal and lingual aspects to provide good visualization of the bone defect.
To initiate the decontamination procedures, the granulation tissue around the implant was removed. The implant surface was then mechanically debrided with plastic curettes to remove residual granulation tissue and biofilm (Fig 3).
Chemical decontamination was performed through topical application of 500 mg/mL of tetracycline hydrochloride. The agent was left in place for 3 minutes, and then the implant and surrounding tissues were irrigated with a sterile physiologic saline solution.
Photodynamic therapy was performed using a hand-held diode laser (Therapy XT, DMC Equipamentos) with a red light wavelength of 660 nm and power rating of 100 mW and 5 J. After
application of 1% methylene blue to the site as a photosensitizer, the laser was applied in contact with the mucosa. The laser was applied for 30 seconds using continuous vertical movements from the bottom of the sulcus to the cervical area. A sodium bicarbonate spray device (Vitally Pro) was also used for 1 minute to clean the implant surface.
After the decontamination procedures were completed, guided bone regeneration procedures were performed to reestablish bone height around the implant. The bone defect around the implant was filled with xenogeneic particles (Bio-Oss Collagen, Geistlich Pharma North America), and a cover screw was placed (Fig 4). The site was then covered with an absorbable collagen membrane (Bio-Gide Membrane, Geistlich Pharma North America), and a subepithelial connective tissue graft was placed to create a better biological seal and increase the peri-implant keratinized mucosa (Fig 5). The flap was sutured with 4-0 absorbable silk threads (Fig 6).
The postoperative medications prescribed for the patient included a 0.12% chlorhexidine rinse, twice daily for 2 weeks; 500 mg of amoxicillin, 3 times a day for 7 days; 100 mg of nimesulide, 2 times a day for 3 days; and 800 mg of paracetamol, as needed for pain. The patient was also reminded about oral hygiene techniques, and regular follow-up examinations were scheduled.
The follow-up examination 30 days after surgery revealed the cessation of the infectious process and reestablishment of peri-implant tissue health. At the 5-month follow-up examination, intraoral radiography revealed increased radiopacity and complete fill of the defect with newly formed mineralized bone at the site of the implant. A new prosthetic crown was placed at that time.
Fig 1. Initial clinical appearance.
Fig 3. Clinical appearance after defect preparation.
Fig 4. Bone defect filled with xenogeneic collagen particles.
Fig 2. Initial panoramic view showing bone loss (arrow) around the implant in the site of the mandibular left first molar.
Surgical treatment of peri-implantitis via multiple decontamination procedures and a regenerative protocol: a case report with 6-year follow-up
Fig 5. Adaptation of the subepithelial connective tissue graft over the surgical site.
Fig 6. Immediate postsurgical appearance.
Fig 7. Clinical appearance at the 3-year postsurgical follow-up examination.
Fig 8. Radiographic appearance at the 3-year postsurgical followup examination.
Fig 9. Clinical appearance at the 6-year postsurgical follow-up examination.
Fig 10. Radiographic appearance at the 6-year postsurgical follow-up examination.
The patient underwent regular professional oral hygiene procedures every 6 months postsurgery, and a recall examination was conducted at least once a year for 6 years. After 3 years, no bleeding on probing could be detected, and the probing depth was reduced to 2 mm (Fig 7). Bone formation was observed on the periapical radiograph 3 years postsurgery (Fig 8).
At the clinical examination 6 years postsurgery, no bleeding on probing was detected, and the probing depth was maintained at 2 mm (Fig 9). Continued bone formation was observed (Fig 10). The combined decontamination and regenerative procedures resulted in restoration of healthy periimplant tissue architecture, and the patient reported satisfaction with the favorable outcome.
Discussion
In the present case, a combination of different decontamination methods was performed in an attempt to preserve the implant. The literature lacks scientific evidence and consensus on an efficient treatment protocol for decontaminating implant surfaces, and peri-implantitis treatment is still a controversial topic. Based on the currently available evidence, nonsurgical mechanical debridement alone has limited efficacy for the treatment of peri-implantitis.11 Chemical methods that use antibacterial agents for implant surface decontamination are more efficient when used as an adjunct to surgical treatment of peri-implantitis.12 Tetracycline, which originally was used in periodontal regeneration procedures, has been adopted as a treatment for peri-implantitis; it has a positive antimicrobial effect when locally delivered.13-15 When tetracycline decontamination is associated with guided bone regeneration procedures, it may enable the repair of the periimplant tissues via formation of new bone.
Other protocols for treatment of peri-implantitis have also been assessed, including the use of photodynamic therapy. Some studies have demonstrated that the combination of a methylene blue sensitizing agent, diode laser, and mechanical debridement significantly decreased the bacterial load at the infected site, resulting in reductions in probing depth, bleeding on probing, and plaque index.16-18 Photodynamic therapy cannot be recommended as a replacement for mechanical treatment but may be indicated as an additional tool for maintenance therapy.19 In the present case, the diode laser was applied using a protocol that was based on clinical practice at São Paulo State University; however, as no standard protocols are described in the literature, it could be difficult to interpret the present results and compare them with outcomes reported in other studies.
A surgical approach to treating peri-implantitis enables better visualization of the infected implant site and facilitates mechanical debridement to remove the decontamination on implant threads. In addition, use of a guided bone regeneration protocol has been proposed because it promotes significant reconstruction of intraosseous peri-implantitis defects, resulting in an improvement of all clinical parameters.20
Soft tissue grafting of implant sites affected by peri-implantitis can be performed to transform the gingival phenotype from thin to thick to obtain greater tissue stability and treat defects such as the apical migration of the gingival margin and the absence of keratinized tissue.21
Some studies have demonstrated that soft tissue augmentation—with either a xenogeneic collagen matrix or connective tissue graft—used in conjunction with regenerative surgical treatment may stabilize the peri-implant tissue and enable the patient to perform plaque control procedures more efficiently.21,22 The importance of keratinized mucosa around the dental implants has been previously reported. The presence of a keratinized mucosa width of more than 2 mm has a positive effect, reducing marginal bone loss, plaque accumulation, tissue inflammation, and brushing discomfort.23-25
A lack of compliance with supportive implant therapy can be harmful to dental implant treatment. 26 One of the major reasons that patients cite for failing to comply with supportive peri-implant maintenance therapy is a lack of information and motivation; an improved educational effort during implant therapy could increase patient compliance with recommended maintenance therapy protocols. 27
Conclusion
This case report described treatment of peri-implantitis with a combination protocol that provided a successful outcome that was maintained over a 6-year follow-up period. Mechanical debridement, tetracycline hydrochloride, photodynamic therapy, and a sodium bicarbonate spray device were used for decontamination; a guided bone regeneration protocol with a xenogeneic graft and collagen membrane was performed to reestablish the peri-implant bone height; and a connective tissue graft was placed to increase the peri-implant keratinized mucosa. The treatment protocol used in this case effectively decontaminated the implant surface and promoted bone formation around the implant, resulting in long-term positive effects on clinical and radiographic assessment parameters. However, randomized controlled clinical trials with longer periods of follow-up should be conducted to compare the effectiveness of this approach to treatment of peri-implantitis.
Author affiliations
Department of Diagnosis and Surgery, Araraquara School of Dentistry, São Paulo State University (UNESP), Araraquara, São Paulo, Brazil (Balderrama, Nicchio, Monachini-Marcantonio, and Marcantonio-Junior); Department of Periodontology/ Implantology, Dental School, Federal University of Uberlândia (UFU), Uberlândia, Brazil (Oliveira).
This work was supported by grants from the Department of Diagnosis and Surgery, Araraquara School of Dentistry, UNESP, and the Coordination for the Improvement of Higher Education Personnel (CAPES), Brazilian Ministry of Education.
Surgical treatment of peri-implantitis via multiple decontamination procedures and a regenerative protocol: a case report with 6-year follow-up
References
1. Schwarz F, Derks J, Monje A, Wang HL. Peri-implantitis. J Clin Periodontol. 2018;45(Suppl 20):S246-S266. doi:10.1111/jcpe.12954
2. Singh P. Understanding peri-implantitis: a strategic review. J Oral Implantol. 2011;37(5):622626. doi:10.1563/AAID-JOI-D-10-00134
3. Claffey N, Clarke E, Polyzois I, Renvert S. Surgical treatment of peri-implantitis. J Clin Periodontol. 2008;35(8 Suppl):316-332. doi:10.1111/j.1600-051X.2008.01277.x
4. Schwarz F, Sahm N, Iglhaut G, Becker J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of periimplantitis: a randomized controlled clinical study. J Clin Periodontol. 2011;38(3):276-284. doi:10.1111/j.1600-051X.2010.01690.x
5. Schwarz F, Bieling K, Nuesry E, Sculean A, Becker J. Clinical and histological healing pattern of peri-implantitis lesions following non-surgical treatment with an Er:YAG laser. Lasers Surg Med. 2006;38(7):663-671. doi:10.1002/lsm.20347
6. Mellado-Valero A, Buitrago-Vera P, Sola-Ruiz MF, Ferrer-Garcia JC. Decontamination of dental implant surface in peri-implantitis treatment: a literature review. Med Oral Patol Oral Cir Bucal. 2013;18(6):e869-e876. doi:10.4317/medoral.19420
7. Gosau M, Hahnel S, Schwarz F, Gerlach T, Reichert TE, Burgers R. Effect of six different periimplantitis disinfection methods on in vivo human oral biofilm. Clin Oral Implants Res 2010;21(8):866-872. doi:10.1111/j.1600-0501.2009.01908.x
8. Ramanauskaite A, Daugela P, Faria de Almeida R, Saulacic N. Surgical non-regenerative treatments for peri-implantitis: a systematic review. J Oral Maxillofac Res. 2016;7(3):e14. doi:10.5037/jomr.2016.7314
9. Roos-Jansaker AM, Renvert S, Egelberg J. Treatment of peri-implant infections: a literature review. J Clin Periodontol. 2003;30(6):467-485. doi:10.1034/j.1600-051x.2003.00296.x
10. Almohandes A, Carcuac O, Abrahamsson I, Lund H, Berglundh T. Re-osseointegration following reconstructive surgical therapy of experimental peri-implantitis: a pre-clinical in vivo study. Clin Oral Implants Res. 2019;30(5):447-456. doi:10.1111/clr.13430
11. Schwarz F, Becker K, Sager M. Efficacy of professionally administered plaque removal with or without adjunctive measures for the treatment of peri-implant mucositis: a systematic review and meta-analysis. J Clin Periodontol. 2015;42(Suppl 16):S202-213. doi:10.1111/ jcpe.12349
12. Rokaya D, Srimaneepong V, Wisitrasameewon W, Humagain M, Thunyakitpisal P. Periimplantitis update: risk indicators, diagnosis, and treatment. Eur J Dent. 2020;14(4):672682. doi:10.1055/s-0040-1715779
13. Mombelli A, Feloutzis A, Bragger U, Lang NP. Treatment of peri-implantitis by local delivery of tetracycline: clinical, microbiological and radiological results. Clin Oral Implants Res 2001;12(4):287-294. doi:10.1034/j.1600-0501.2001.012004287.x
14. Park JB. Treatment of peri-implantitis with deproteinised bovine bone and tetracycline: a case report. Gerodontology. 2012;29(2):145-149. doi:10.1111/j.1741-2358.2011.00470.x
15. Mariotti A. Efficacy of chemical root surface modifiers in the treatment of periodontal disease: a systematic review. Ann Periodontol. 2003;8(1):205-226. doi:10.1902/ annals.2003.8.1.205
16. Lopez MA, Passarelli PC, Marra M, et al. Antimicrobial efficacy of photodynamic therapy (PDT) in periodontitis and peri-implantitis: a systematic review. J Biol Regul Homeost Agents. 2020;34(5 Suppl 3):59-65.
17. Alqahtani F, Alqhtani N, Alkhtani F, Divakar DD, Al-Kheraif AA, Javed F. Efficacy of mechanical debridement with and without adjunct antimicrobial photodynamic therapy in the treatment of peri-implantitis among moderate cigarette-smokers and waterpipe-users. Photodiagnosis Photodyn Ther. 2019;28:153-158. doi:10.1016/j.pdpdt.2019.09.003
18. Derikvand N, Ghasemi SS, Safiaghdam H, Piriaei H, Chiniforush N. Antimicrobial photodynamic therapy with diode laser and methylene blue as an adjunct to scaling and root planning: a clinical trial. Photodiagnosis Photodyn Ther. 2020;31:101818. doi:10.1016/ j.pdpdt.2020.101818
19. Sculean A, Deppe H, Miron R, Schwarz F, Romanos G, Cosgarea R. Effectiveness of photodynamic therapy in the treatment of periodontal and peri-implant diseases. Monogr Oral Sci 2021;29:133-143. doi:10.1159/000510189
20. Wen SC, Barootchi S, Huang WX, Wang HL. Surgical reconstructive treatment for infraosseous peri-implantitis defects with a submerged healing approach: a prospective controlled study. J Periodontol. 2022;93(2):195-207. doi:10.1002/JPER.21-0161
21. Sculean A, Romanos G, Schwarz F, et al. Soft-tissue management as part of the surgical treatment of periimplantitis: a narrative review. Implant Dent. 2019;28(2):210-216. doi:10.1097/ID.0000000000000870
22. Schwarz F, Sahm N, Becker J. Combined surgical therapy of advanced peri-implantitis lesions with concomitant soft tissue volume augmentation: a case series. Clin Oral Implants Res 2014;25(1):132-136. doi:10.1111/clr.12103
23. Perussolo J, Souza AB, Matarazzo F, Oliveira RP, Araujo MG. Influence of the keratinized mucosa on the stability of peri-implant tissues and brushing discomfort: a 4-year follow-up study. Clin Oral Implants Res. 2018;29(12):1177-1185. doi:10.1111/clr.13381
24. Roccuzzo M, Grasso G, Dalmasso P. Keratinized mucosa around implants in partially edentulous posterior mandible: 10-year results of a prospective comparative study. Clin Oral Implants Res. 2016;27(4):491-496. doi:10.1111/clr.12563
25. Bouri A Jr, Bissada N, Al-Zahrani MS, Faddoul F, Nouneh I. Width of keratinized gingiva and the health status of the supporting tissues around dental implants. Int J Oral Maxillofac Implants. 2008;23(2):323-326.
27. Amerio E, Mainas G, Petrova D, Giner Tarrida L, Nart J, Monje A. Compliance with supportive periodontal/peri-implant therapy: a systematic review. J Clin Periodontol. 2020;47(1):81100. doi:10.1111/jcpe.13204
Earn CE at Your Convenience with Self-Instruction
Now is the time to take advantage of AGD’s Self-Instruction program that includes exercises based on AGD Impact articles. These exercises contain 10 questions and are worth 1 CE credit. It’s the perfect complement to General Dentistry
AGD Impact
1 exercise = $15
2 exercises = $25 (save $5)
4 exercises = $50 (save $10)
Learn More agd.org/self-instruction
General Dentistry
1 exercise = $30
3 exercises = $70 (save $20)
6 exercises = $120 (save $60)
12 exercises = $180 (save $180)
ORAL DIAGNOSIS
Tanya M. Gibson, DDS
Bump on the gums
(Case courtesy of Dr Abbey Allen, Atchison, Kansas.)
A 29-year-old pregnant woman in her third trimester initially presented with erythematous, papular, hyperplastic tissue of the interdental papilla, associated with teeth 27 and 28 (Fig 1). In a 3-week time span, the lesion rapidly progressed into an erythematous, ulcerated, smooth, pedunculated nodule covering portions of the clinical crowns of teeth 27
Fig 1. Erythematous, papular, hyperplastic tissue of the interdental papilla associated with teeth 27 and 28.
and 28 (Fig 2). The patient reported excessive bleeding in the area with minimal pain. A differential diagnosis was established, and a biopsy was subsequently performed. Histologic findings included sections of ulcerated hyperplastic surface epithelium overlying a vascular proliferation with a mixed inflammatory cell infiltrate.
Fig 2. Erythematous, ulcerated, smooth, pedunculated nodule covering portions of the clinical crowns of teeth 27 and 28.
Inferior mandible radiolucency
(Case courtesy of Dr Conrad Journée, Kansas City, Missouri.)
A 68-year-old man presented for a new patient examination. A panoramic radiograph revealed a well-defined, corticated, unilocular radiolucent area located in the right
Which of the following is the most appropriate diagnosis?
A. peripheral giant cell granuloma
B. peripheral ossifying fibroma
C. pyogenic granuloma
D. pleomorphic adenoma
Diagnosis is on page 80.
antegonial region, below the right inferior alveolar canal (Figure). The patient was aware that he had a “growth” in his jawbone.
Figure. Well-defined, corticated, unilocular radiolucent area located in the right antegonial region, below the right inferior alveolar canal.
Which of the following is the most appropriate diagnosis?
A. aneurysmal bone cyst
B. antral pseudocyst
C. static bone cyst
D. traumatic bone cyst
Diagnosis is on page 80.
Author affiliation
Department of Oral Pathology, Radiology and Medicine, School of Dentistry and School of Graduate Studies, University of Missouri – Kansas City.
GENERAL DENTISTRY SELF-INSTRUCTION ANSWERS
Exercise No. GD518
November/December 2023, p. 31
1. B
2. D
3. D
4. D
5. A
6. C 7. B 8. A 9. C 10. A 11. C 12. B 13. A 14. A 15. D
Exercise No. GD519
November/December 2023, p. 41
1. A
2. D
3. A
4. C
5. D
6. B 7. C 8. A 9. A 10. D 11. A 12. A 13. B 14. C 15. D
Exercise No. GD520
November/December 2023, p. 47
1. C
2. C
3. B
4. B
5. A 6. A 7. B 8. C 9. A 10. C 11. B 12. C 13. A 14. B 15. D
HAVE YOU MOVED?
If you have recently moved, or plan to in the near future, please make sure to update your AGD profile. Log into the AGD website today! We want to make sure you receive AGD publications and other important information from us! View or update your profile, check the status of your membership dues, manage your email subscriptions and change your password.
Please contact the AGD Membership Services Center with any questions at 888.243.3368 (toll-free) or 312.440.4300. Our member representatives are available to assist you Monday through Friday from 7:30 a.m. to 5:30 p.m. CST.
UPDATE YOUR PROFILE agd.org/my-agd
Coming next
issue
Look for these articles and more in the January/February 2025 issue of General Dentistry:
• Esthetic treatment of molar-incisor hypomineralization from microinvasive to restorative procedures: a case report
• Dietary beta carotene hyperpigmentation of the oral mucosa
• Multimodal management of persistent labial hemangioma: a case report
In the November issue of AGD Impact
• Exploring Nonclinical Career Paths
• U.S. Air Force International Health Specialist Program
In the December issue of AGD Impact
• Tech Tool: Artificial Intelligence Chatbots Play Increasing Role in Dentistry
• Balancing Intuition and Technology: Ethical Considerations for AI in Dental Practice
Bimonthly
or
Business Office of Publisher: Same as above Names and Mailing Addresses of Publisher, Editor, and Executive Editor: Publisher: Academy of General Dentistry, 560 W Lake St, Sixth Floor, Chicago, IL, 606616600 Editor: Timothy F. Kosinski, DDS, MAGD, address same as above Executive Editor: Tiffany Nicole Slade, address same as above Owner: Academy of General Dentistry, address same as above Known Bondholders, Mortgagees, and Other Security Holders: None Tax Status: Has not changed during preceding 12 months Issue Date for Circulation Data Below: 09/01/2024.
Publication of Statement of Ownership: November/December 2024 issue Signature and Title: Tiffany Nicole Slade, Executive Editor Date: 09-24-2024
Extent and Nature of Circulation
Bump on the gums
Diagnosis
C. pyogenic granuloma
Pyogenic granuloma is a reactive nodular proliferation of granulation tissue that can occur on any mucosal or cutaneous surface. This tumor-like condition most often occurs in children or young adults and has a female predilection.1 The etiology of a pyogenic granuloma is believed to result from local irritation, poor oral hygiene, or hormonal factors.1 Due to the vascularity of pyogenic granuloma, bleeding is a common clinical feature, and it may be associated with mild pain.
This reactive lesion commonly develops during pregnancy and is often referred to as a pregnancy tumor or granuloma gravidarum. Lesions can present during the first trimester of pregnancy; however, the incidence increases through the seventh month of pregnancy.1 Of the pyogenic granulomas that occur on the gingiva, 75% to 85% occur on the anterior maxillary facial gingiva.1
When pyogenic granulomas occur on the gingiva, peripheral giant cell granuloma and peripheral ossifying fibroma should be included in the differential diagnosis. This triad is often referred to as the 3 Ps. Clinicians should be mindful that other more serious pathologic entities can mimic their clinical appearance, necessitating the need for a biopsy with histologic analysis. The pyogenic granuloma’s histology exhibits a vascular proliferation reminiscent of granulation tissue.
Peripheral giant cell granuloma is a reactive lesion that often presents as a reddish or bluish-gray nodular mass. It
Inferior mandible radiolucency
Diagnosis
C. static bone cyst
The aneurysmal bone cyst, antral pseudocyst, static bone cyst, and traumatic bone cyst are all classified as pseudocysts. As pseudocysts, all of these pathologic entities lack the histopathologic finding of having an epithelial lining. Additionally, they also have distinct clinical or radiologic features.
Static bone cyst, commonly referred to as a Stafne defect, is a developmental lesion in which a portion of the submandibular gland becomes entrapped in the mandible. They are most often found in the posterior mandible below the inferior alveolar nerve canal, located between the molars and angle of the mandible.1
Radiographically, it presents as well-defined, corticated, unilocular radiolucency and is identified as an incidental finding on routine radiographic examination. It is estimated that Stafne defects are identified on 0.8% to 0.48% of all panoramic radiographs, with 80% to 90% occurring in men.1 Surgical intervention is not indicated; however, normal submandibular salivary gland tissue is expected to be identified on histologic analysis.
The aneurysmal bone cyst presents as a rapidly expansile tumorlike growth. Many occur following a blunt trauma. Radiographically, it presents as a unilocular or multilocular
is exclusively found on the gingiva or alveolar mucosa. The peripheral giant cell granuloma’s histology is characterized by plump mesenchymal cells intermixed with multinucleated giant cells.
Peripheral ossifying fibroma is a reactive lesion that often presents as a mucosa-colored nodular mass that may or may not be ulcerated. It is exclusively found on the gingiva or alveolar mucosa. Its histology is characterized by a proliferation of fibrous connective tissue with the formation of mineralized product. Complete surgical excision is the recommended treatment for the 3 Ps. Recurrence of these lesions is common.
Pleomorphic adenoma is the most common salivary gland neoplasm. When it occurs in association with the minor salivary glands, it usually presents as a mucosa-colored submucosal mass. Pain is not expected unless it is secondarily traumatized. The gingival tissue does not contain salivary gland tissue; therefore, it is not a site where salivary gland lesions would occur. Complete surgical excision is the recommended treatment for a pleomorphic adenoma, and histologic analysis is required for a definitive diagnosis.
Reference
1. Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology. 5th ed. Elsevier; 2024:525-527.
radiolucency. The lesional tissue is often described as a bloodsoaked sponge. A biopsy is required for definitive diagnosis. An antral pseudocyst occurs exclusively in the maxillary sinus and presents radiographically as a grayish, dome-shaped swelling with smooth borders. It results from an accumulation of an inflammatory exudate underneath the sinus epithelium. These lesions are typically an incidental finding and require no treatment. Because of the characteristic radiographic presentation, a biopsy is generally not indicated.
A traumatic bone cyst is of unknown etiology. It often presents as a mandibular radiolucency. At the time of biopsy, the surgeon often reports the presence of an “empty” cavity. A thorough curetting of the cavity walls during the biopsy procedure stimulates bleeding, which promotes the healing process. A biopsy is indicated to rule out other intraosseous pathologic entities.
Reference
1. Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology. 5th ed. St. Louis Elsevier, 2024:23-25.