Some Veterinarians Are Drawn to Oral Healthcare
AGD Impact April 2024, Vol. 52, No. 4 News for the General Dentist The Latest in Oral Cancer Research AGD2024 Course Overview
Animal Magnetism
 By William S. Bike
By William S. Bike

20 Oral Cancer: Updates from AGD and Around the World
As part of April as Oral Cancer Awareness Month, this issue of AGD Impact features an update from the AGD Foundation on its mission to bring awareness to oral cancer. It also includes the latest in oral cancer research from around the world.
22
Your Knowledge and Skills at AGD2024
Learn about all the featured speakers and subject areas at AGD’s latest scientific session.





agd.org/impact 1 2 Editor’s Note What Lasts a Lifetime? 4 AGD News 7 Financial Management Increase Cash Flow and Reduce Stress by Reducing PPO Exposure 9 Communications Transparency and Timing Are Key When Conveying Big Changes 11 Member Spotlight 2023 Humanitarian Award Winner Dedicates His Life’s Volunteerism to One Region 23 Testing the Tools
dental specialty allows a practitioner to perform a sinusotomy on a standing patient who happens to have 12 pounds of teeth or fix a tooth the patient broke by biting an antler? The answer is animal dentistry. 14 23
11 Contents
Magnetism Some Veterinarians Are Drawn to Oral Healthcare
What
7
Animal
Upgrade
What Lasts a Lifetime?
Iam sometimes asked while lecturing, “How long do dental implants last?” Patients also will ask how long a certain restorative result is supposed to remain functional. Sometimes it is presumed that our prescribed dental therapy is meant to last “a lifetime.” This may be an interesting dilemma for us practicing to the best of our abilities. Obviously, there are many considerations to be made prior to telling the patient what to expect. The quality and quantity of bone, the architectural design planned, function, and commitment to maintenance are all valuable indicators of longevity. Teeth were intended to last a “lifetime,” but, if they did, we would be out of business. Studies indicate that dental implants have a 90%–95% success rate over a 10-year period. This statistic may be misleading when determining whether the implants were placed in the maxilla or mandible, how many were placed, and how the prosthetics were designed. Also, what measure indicates success? Functional success may be different from esthetic success, especially with today’s visual expectations.

will be drivable depends too on scheduled maintenance and being aware of wear and tear. Most of our home appliances also have shelf lives. Dishwashers, washers/dryers and refrigerators may last 10 years. Furnaces may last 20, and roofs may last even longer. Proper maintenance can prolong these products’ lifespans, but eventually they’ll all need to be replaced.
So why do our patients presume lifetime dental restorations? It’s certainly true that materials, techniques, design and fabrication have allowed great strides in dentistry. CAD/CAM design, milling, high-quality materials and virtual design — and even artificial intelligence — have elevated our profession to incredible heights. Our treatments last a lot longer than they did a decade ago. But, as with cars, each patient’s mileage will vary.
Timothy
Associate
Bruce
Director,
Kristin
Executive
Tiffany
Managing
Associate
Let’s look at these questions from another angle. Conventional dental crown-and-bridge and dentures are said to also last about 10 years while in function. Esthetics may have a shorter lifespan as tissue and bone changes occur. Our orthopedic colleagues also routinely design and place implants in knees and hips. The average age of these patients is between 66 and 68 years old. Joints may last between 15 and 20 years, so I guess that could be considered a “lifetime” of use for those medical prosthetics.
Since I’m from Detroit, car analogies seem appropriate. A car today may last up to 200,000 miles or 12 years depending on your driving tendencies. Electric car batteries also are said to last for about 200,000 miles or 12–15 years. The length of time a vehicle
While clinical dentistry has advanced to unimaginable heights, our communication skills need to keep up. Clear, concise explanations on prognosis should be given, and the patient must be presented with a consent form illustrating the plan and potential immediate and future complications.
The mouth is a unique part of the body, open to the environment and functioning constantly, even in sleep. The constant stress and strain can be intense, more so than for orthopedic prostheses. Lasting a “lifetime” may be an impossible feat and cannot be assumed. We all need to do a better job explaining this to our patients.
 Timothy F. Kosinski, DDS, MAGD Editor
Timothy F. Kosinski, DDS, MAGD Editor
Periodical postage paid at Chicago, IL and additional mailing office.
*AGD members receive AGD Impact as part of membership; annual subscription rates for nonmembers are $70 to individuals/$90 to institutions (orders to Canada, add $15). Online-only subscriptions available outside U.S./Canada are $75 to individuals/$115 to organizations. Single copy rates are $17.50 to individuals/$20 to institutions (orders to Canada, add $2.50). All orders must be prepaid in U.S. dollars.
POSTMASTER: Send address changes to AGD Impact, 560 W. Lake St.,
2 AGD IMPACT APRIL 2024 Editorial Staff
Editor
F. Kosinski, DDS, MAGD
Editor
L.
Cassis, DDS, MAGD
Communications
S.
Gover, CAE
Editor
Nicole
Slade, MFA
Editor
Humbertson, MA
Leland
Editor
Davis
Production/Design
Henney
Designers
Ajami
Grawe Advertising advertising@agd.org Reprints scsreprints@sheridan.com How to Reach Us Academy of General Dentistry 560 W. Lake St., Sixth Floor Chicago, IL 60661-6600 agd.org impact@agd.org
312.335.3427 (fax) DISCLAIMER: The Academy of General Dentistry does not necessarily endorse opinions or statements contained in essays or editorials published in AGD Impact. The publication of advertisements in AGD Impact does not indicate endorsement for products and services. AGD approval for continuing education courses or course sponsors will be clearly stated. AGD Impact (ISSN 0194-729X) is published monthly by the Academy of General Dentistry, 560 W. Lake St., Sixth Floor, Chicago, IL 60661-6600. Canadian Mailing Information: IPM Agreement number 40047941. Change of address or undeliverable copies should be sent to: Station A, P.O. Box 54, Windsor, Ontario, N9A 6J5, Canada. Email: impact@agd.org.
Caitlin
Manager,
Tim
Graphic
Robert
Eric
888.243.3368
Sixth Floor, Chicago, IL 60661-6600. No portion of AGD Impact may be reproduced in any form without prior written permission from the AGD. Photocopying Information: The Item-Fee Code for this publication indicates that authorization to photocopy items for internal or personal use is granted by the copyright holder for libraries and other users registered with the Copyright Clearance Center (CCC). The appropriate remittance of $3 per article/10¢ per page is paid directly to the CCC, Inc., 222 Rosewood Drive, Danvers, MA 01923, USA. The copyright owner’s consent does not extend to copying for general distribution, for promotion, for creating new works, or for re-sale. Specific written permission must be obtained from the publisher for such copying. The Item-Fee Code for this publication is 0194-729X. Printed in U.S.A. © Copyright 2024, Academy of General Dentistry, Chicago, IL. Editor’s Note

Dental Practice
Dental Quality Alliance Offers Value to Dentistry
By Ralph A. Cooley, DDS, FAGD
Every now and then, other AGD members ask me about the Dental Quality Alliance (DQA). The most frequently asked questions are “What is the DQA?”, “What does the DQA contribute to dentistry?” and “Why is AGD involved in the DQA?”
In 2010, the American Dental Association (ADA) established the DQA in response to a federal mandate to incorporate quality measures into dental programs. The DQA’s original charge was to develop performance measures for oral healthcare, and the agency’s current efforts continue to be guided by its commitment “to improving patient care and safety through the collaborative development of oral healthcare measures.”
The DQA is an organization of major stakeholders in oral healthcare delivery who use a collaborative approach to develop these oral healthcare measures. AGD is one of 23 voting members and also maintains positions on the 11-member Executive Committee and the Education Subcommittee.
As AGD’s representative to the DQA, it was my honor to serve as DQA chair from 2022 to 2023. I’m pleased to share that there were many significant events that took place during that time. A few of the highlights, which were presented at the DQA’s November 2023 meeting, included:
• The biennial DQA Conference: The theme of the conference was “Moving Past Disruption to Improve Oral Healthcare.” The event was a success and had the highest in-person attendance (125 attendees) for any DQA conference since the inaugural meeting in 2013. The program successfully highlighted the various elements that comprise a quality improvement system — leadership, staff training, coding systems, evidence-based dentistry, medical-dental integration — and how they address value, cost and quality in the delivery of oral healthcare and impact patient outcomes. The DQA’s Education subcommittee, on which I participate, is currently exploring alternate educational program delivery options and venues instead of the traditional conference-style event.
• State Oral Healthcare Quality Dashboard: These data presentations can be viewed on the DQA website and currently offer reports on seven DQA pediatric measures involving Medicaid and the Children’s Health Insurance Program (CHIP) specific for all 50 states. The dashboard was updated with the successful release of new, dynamically generated reports and additional years of data.
Dental Practice
Vitamin K2: Is It Needed for Dental Health?
By Jeanie Kennedy, Manager, AGD Dental Practice & Policy
In 2011, the British Medical Journal published a study with the findings that women who supplemented with calcium were at higher risk of atherosclerosis, heart attack and stroke than those forgoing supplementation.1 Scientists have referred to the supplementation of calcium as a paradox. What they’re referring to is that calcium is needed for bone development and strengthening mineral density in the body but may end up depositing in blood vessels, causing potential calcification, heart disease and heart attacks.
• New quality measures: Two additional DQA measures were recommended for inclusion in the Centers for Medicare & Medicaid Services (CMS) core set for 2025. These measures represent the DQA’s first foray into addressing oral health among adults. The specific measures assess “Ambulatory Care Sensitive Emergency Department Visits for Non-Traumatic Dental Conditions in Adults” and “Oral Evaluation During Pregnancy.”
• Practice- and Clinician-Level Measure Development
Workgroup: This group has been meeting to explore what practice measures would be appropriate at the practice/clinician level. While this might be considered a controversial topic, the DQA is considering this measure in response to several third-party entities that have established such measures. The DQA has determined that many measures listed in reports are not appropriate for use in quality improvement programs at the practice/clinician level using claims data at this time. They’ve also sought input from various members on those measures. AGD was among the groups invited to provide input and, at the time this report was submitted, a response to the DQA on this issue was in development. The DQA will continue to consider public comments and see what measures might be appropriate in the future.
AGD continues to be the only professional association that exclusively represents the needs and interests of general dentists and advocates on our behalf. The organization is committed to representing our profession in all discussions that affect how dentistry is practiced in the United States. We will continue to be “at the table” voicing concerns and speaking out strongly as needed. It is an honor and a privilege to represent you as a fellow AGD member.
The next general meeting of the DQA will be June 14 at the ADA’s headquarters in Chicago. More information about the DQA, education, updates and detailed explanations about quality measurement in dentistry and how it can affect you in a positive way can be found on the DQA website: ada.org/resources/research/ dental-quality-alliance.
Ralph A. Cooley, DDS, FAGD, is the assistant dean of Admissions/ Student Services at UTHealth Houston School of Dentistry. He was previously in private practice for 34 years. He serves on AGD’s Legislative & Governmental Affairs Council and is AGD’s liaison to the DQA.
What Does Vitamin K2 Do?
Vitamin K2 activates certain proteins in the body, one of which is osteocalcin, which deposits calcium into bones and strengthens mineral density.2 Osteocalcin is also implicated as a critical nutrient to prevent type 2 diabetes. K2 activates the matrix Gla protein (MGP), which removes calcium from soft tissues such as arteries and veins.3 Additionally, vitamin K2 is associated with beneficial effects for many health conditions, including infertility, cancer and tooth decay.4
4 AGD IMPACT APRIL 2024 AGD News

Discovery of K2
• Vitamin K2 was first discovered in the 1930s by Danish biochemist Henrik Dam. A decade later, an American researcher, Edward Doisy, isolated vitamin K as the coagulation nutrient.2 Dam and Doisy shared the Nobel Prize in physiology and medicine in 1943. However, both scientists recognized that vitamin K appeared in two forms: vitamin K1 and K2.
• In 1939, Dr. Weston A. Price published on “Activator X,” or menaquinone, which was later known to be vitamin K2. Price was a dentist and delved into the causes of dental cavities and chronic diseases.
• In 1975, Harvard Medical School researchers discovered that osteocalcin draws calcium into bones to prevent osteoporosis and dental cavities.5
• In 1997, vitamin K was discovered to be needed for depositing calcium into bones and preventing calcium deposits into soft tissue.6
• In 2007, vitamin K2 deficiency was found to have a major deleterious impact on human health.7
Vitamin K’s Nutritional Importance
Price was alarmed that his patients had many dental problems. In 1925, Price and his wife traveled to indigenous cultures to examine why some people are healthy and others are not. Price discovered that the more a population embraced modern eating habits and strayed from traditional diets, the more people were prone to deteriorating health.2 Dental health was the first symptom, followed by gum disease.
Price also found that teeth developed straight and uncrowded in dental arches with traditional diets. Notably, children raised on modern diets had teeth crowding and underdeveloped oral arches. Consumption of white flour, sugar, white rice, canned goods and other industrialized foods seemed to lead to more dental problems.8 Traditional diets contained more than 10 times the fat-soluble vitamins than modern fare. When the body lacks new sources of fat-soluble vitamins from consumption, calcium is pulled from the teeth, and bone loss can occur.
Price believed that healthy smiles were the product of heredity and prenatal nutrition. Later in his practice, Price began using highvitamin butter oil to treat cavities and drilled only in extreme cases.
Vitamins A and D act as hormones and catalyze proteins to enhance the absorption of nutrients. Other K vitamins are K3, K4, K5, K6 and K7. Research shows that vitamin K2, or menaquinone, deficiency can occur in as little as seven days.9 Menaquinone was once abundant in our diet but has diminished with the rise of processed foods. Important subtypes of K2 include MK4 and MK7.
Other Findings
• Vitamins K2 and D together better improve bone density and reduce fracture risk than either of the vitamins used alone.10
• Vitamin K2 shields brain cells from free radical damage.11
• Osteocalcin was found to have a major impact on the body’s production of and sensitivity to insulin.12
• In one study, menaquinone induced cell death for all types of leukemia included in the study.13
Testing for K2 Levels
Testing for vitamin K2 levels does not appear to be easily accomplished. Some researchers suggest that the under-carboxlylated osteocalcin (ucOC) test demonstrates more accurate readings for vitamin K2 deficiency.
How Much Vitamin K2 to Take, and When to Combine with Other Vitamins?
• Vitamin K2 works synergistically with vitamin A.
• MK7 is widely available in 120-microgram preparations.
• There is no USDA-recommended dosage for K2, but supplements are available in MK4 and MK7 preparations.
• Foods that contain vitamin K2 include liver, egg yolks, beef, chicken, fermented cheese, pork, and properly fermented natto (soybean product popular in Japan). Butter and fat from grass-fed animals also contains vitamin K2, but not from grain-fed animals.
References
1. Bolland, Mark J., et al. “Calcium Supplements With or Without Vitamin D and Risk of Cardiovascular Events: Reanalysis of the Women’s Health Initiative Limited Access Dataset and Meta-Analysis.” The BMJ, 19 April 2011, doi: 10.1136/bmj.d2040.
2. Rheaume-Blue, Kate. Vitamin K2 and the Calcium Paradox: How a Little-Known Vitamin Could Save Your Life. Collins, 2012.
3. Hariri, E., et al. “Vitamin K2—A Neglected Player in Cardiovascular Health: A Narrative Review.” Open Heart, 2021, doi: 10.1136/openhrt-2021-001715.
4. Burhenne, Mark. “Vitamin K2 Benefits for Dental Health.” Ask the Dentist, 19 Oct. 2018, askthedentist. com/vitamin-k2-benefits/.
5. Hauschka, Peter V., and Margaret L. Reid. “Vitamin K Dependence of a Calcium Binding Protein Containing Gammacarboxyglutamic Acid in Chicken Bone.” The Journal of Biological Chemistry, vol. 253, no. 24, 1978, pp. 9063-9068.
6. Booth, Sarah L. “Skeletal Functions of Vitamin K-Dependent Proteins: Not Just for Clotting Anymore.” Nutrition Reviews, vol. 55, no. 7, 1997, pp. 282-284.
7. Cranenburg, Ellen C. M., et al. “Vitamin K: The Coagulation Vitamin that Became Omnipotent.” Thrombosis and Haemostasis, vol. 98, no. 1, 2007, pp. 120-125.
8. Price, Weston A. Nutrition and Physical Degeneration, 8th ed. Price-Pottenger Nutrition Foundation, 2008
9. Human Vitamin and Mineral Requirements. Food and Agriculture Organization of the United Nations, 2001.
10. Ames, Bruce N. “Low Micronutrient Intake May Accelerate the Degenerative Diseases of Aging Through Allocation of Scarce Micronutrients by Triage.” Proceedings of the National Academy of Sciences of the United States of America, vol. 103, no. 47, pp. 17589-17594.
11. Li, Jianrong, et al. “Novel Role of Vitamin K in Preventing Oxidative Injury to Developing Oligodendrocytes and Neuron.” The Journal of Neuroscience, vol. 23, no. 13, 2003, pp. 5816-5826.
12. Sakamoto, N., et al. “Relationship Between Acute Insulin Response and Vitamin K Intake in Healthy Young Volunteers.” Diabetes, Nutrition & Metabolism, vol. 12, no. 1, 1999, pp. 37-41.
13. Yokoyama, Tomohisa, et al. “Vitamin K2 Induces Autophagy and Apoptosis Simultaneously in Leukemia Cells.” Autophagy, vol. 4, no. 5, 2008, pp. 629-640.
AGD Fact Sheets
Talking to Patients About Oral Cancer
AGD fact sheets provide your patients with all of the information they need to maintain their oral health. Fact sheets on more than 25 oral health topics are available for downloading online and can be customized to include your name and practice information. Download the fact sheet “What You Should Know About Oral Cancer” at agd.org/factsheets.
6 AGD IMPACT APRIL 2024 AGD News
Increase Cash Flow and Reduce Stress by Reducing PPO Exposure
By Wesley W. Lyon II, CPA, CFP®

Are you struggling to increase your profit margin in a world of increased costs? Does your accountant recommend cutting expenses or having an expense reach a certain percent of your revenue? No matter how hard you try, the task may seem impossible. To make matters worse, some of your reimbursement rates may be declining. You’re not alone. My company meets with over 100 dentists each year struggling with similar issues.
Identifying the Problem
Often, the real cause is excessive preferred provider organization (PPO) write-offs, sometimes reaching more than 40% of gross production. Unfortunately, practices with excessive write-offs must rely on volume to survive. This adds undue stress to both the staff members and the doctors. With rising expenses and lower PPO reimbursements, now is the time to take action to increase your profits while decreasing your stress levels.
How could a dentist be unaware of such a large problem? Many dentists choose to hide from the problem by entering production under the PPO reimbursement schedule rather than their usual, customary and reasonable (UCR) fee. The first step to tackling this problem is to enter all fees under the UCR fee and enter write-offs separately as claims are paid. Thereafter, dentists should be able to review their write-offs regularly, even separating reports by dental insurance for a more precise look at the problem.
Developing a Game Plan
Once the write-offs are calculated, we can begin to create an outof-network wish list, ordering insurance providers by the expected impact to the practice. Each insurance plan should be listed along
with gross production, write-offs, write-off percentage and number of patients. Insurance plans with the highest write-off percentages and least amount of production or patients should be eliminated first. Let’s explore an example:
In this case, the dentist is feeling the most pain from Insurance A because $200,000 of income is being lost annually. While this may be true, the highest number of active patients and gross production can be attributed to Insurance A, so eliminating it could lead to much worse problems. Instead, the doctor should go out-of-network with Insurance C first. While write-offs were only $35,000, gross production was $70,000, leading to a 50% write-off percentage. This means that the doctor only has to keep 50% of these patients to break even (74 of them). Using the same logic, the dentist can focus on Insurance B next, even though the write-off percentage is actually lower than that of Insurance A.
Be Wary of Umbrella Networks Before Taking Action
In our example, we assumed the doctor is in-network with only three PPOs. Often, I discover that practices are in-network with almost all providers. This can lead to unintended consequences, including being entangled in a web of umbrella networks. An
agd.org/impact 7 Financial Management
Insurance Gross Production Active Patients Write-Offs Write-Off % A $700,000 1,288 $200,000 29% B $200,000 368 $40,000 20% C $70,000 147 $35,000 50%
umbrella network refers to insurance companies sharing networks or leasing their network to another insurance company.
Making a mistake while going out-of-network with umbrella networks can be a painful embarrassment to the doctor and staff. Since you will need to communicate these changes ahead of time to ensure a successful drop, the patient will be informed that you will no longer be in-network with their insurance at the next visit. When the next visit comes, it could surprise both the patient and doctor if the patient’s insurance comes back as in-network. This happens when the PPO that the doctor moved out-of-network with is picked up under an umbrella network with another provider. It is best to seek professional help to untangle any umbrella network webs prior to moving out-of-network to avoid confusion, staff frustration, and your patients perceiving your practice as disorganized or greedy.
Be Ready
Is your practice a candidate to reduce PPO exposure? Or do you have improvements to be made elsewhere? PPOs do serve a purpose in many practices, and that purpose is to provide patients. Prior to moving out-of-network, make sure your internal (i.e., patient referrals) and external (i.e., traditional) marketing programs are effective, as you’ll likely need to replace some patients who leave. For those practices busting at the seams, the time to take action is now.
Next, make sure to train your staff and create a game plan to communicate with your patients. I recommend involving a consultant to ensure a smooth transition. As a great first step, have a friend or colleague “secret shop” your practice by calling to set up an appointment, but be sure this secret shopper claims to
have an insurance that your practice is not in-network with. It still shocks me how many front desk employees will inform the patient that your practice does not accept their insurance. This couldn’t be further from the truth. Instead, you must retrain the staff to communicate that you work with all insurances, and the practice will file for benefits on their behalf. The front desk should be welcoming all patients to the practice rather than screening them. Staff can simply inform the patient to bring their insurance information with them to the initial appointment.
Execute the Game Plan
Begin by dropping an insurance that will have a very minimal impact on the practice (Insurance C in our example). This should be true in both production and number of patients. This gives the staff and you, the dentist, an opportunity to improve your business skills and comfort level. Begin dropping one PPO at a time, utilizing your drop sequence created earlier to choose which PPOs to go out-of-network with. Keep in mind, you may not succeed in leaving all of them behind, but it doesn’t mean you shouldn’t attack the low-hanging fruit. This past year, we helped a doctor increase his collections by over $50,000 per month by reducing PPO write-offs. He is still an in-network provider with a number of plans, but, by becoming more selective, he has been able to dramatically increase profits. ♦
Wesley W. Lyon II, CPA, CFP, is president and CEO of McGill and Lyon Dental Advisors. For more information on his firm’s comprehensive tax and business planning services for dentists and specialists, contact Janet Blair at 877.306.9780, or email consulting@mcgillhillgroup.com. To comment on this article, email impact@agd.org
8 AGD IMPACT APRIL 2024 Financial
Management
Transparency and Timing Are Key When Conveying Big Changes
By Gerard Scannell, DDS
With so much changing in the world, we, too, must adjust to keep our practices current. Communicating changes to our patients can be challenging, especially when those changes may affect their dental experience. But a lot of people don’t like change, especially older patients.
We can improve our practices in many ways, but three of the most common are price increases, changes in staff and new technology. These can be sensitive topics to discuss. How can you convey them in a way that is clear, respectful and reassuring? Here are some tips.
Price Increases
Handling communication about price increases is a delicate matter. The primary objective in sharing this information is to prevent any surprises. When patients encounter sudden price hikes without prior knowledge, they may feel exploited,
potentially eroding trust and loyalty. Therefore, transparency is key in navigating changes in pricing.
Clearly explain the reasons for the adjustment and provide a detailed breakdown of the revised pricing structure. Be honest about factors like increased costs of materials, equipment, labor or insurance. Additionally, you can highlight any enhancements or improvements planned for your practice, such as the incorporation of new technology, staff training or facility upgrades. This approach helps patients understand the necessity of the increase and enables them to make well-informed decisions about their dental care. To avoid negative reactions, proactively communicate any price changes, explain the reasons behind them, and emphasize the value of your services.
Effective communication about price increases involves forewarning patients. Notify patients no less than one month before new prices take effect. The more time patients have to adjust, the better. Use various channels, such as letters, emails, texts and/or flyers around the office. I recommend avoiding social media platforms to announce this change because it could be off-putting for potential future patients. Ensure that the communication includes the effective date of the change, the amount of the increase and details of the affected services.
Reinforce the value of your services during communication. Remind patients of the benefits, and emphasize the quality of care, convenience of your location, expertise of your staff or the variety of services offered. Highlight any discounts, promotions or payment plans available to help patients afford your services.
“Keeping patients well-informed is key to ensuring their comfort and confidence.”
Staff Changes
Changes in staff can have a profound impact on your patients, particularly if they are accustomed to a specific dentist or hygienist. To mitigate any negative sentiments, it is crucial to promptly notify your patients of any changes.
As much as possible, try to communicate this change in a positive light. This not only fosters a sense of comfort among patients but also builds trust with the incoming staff. Your staff plays a vital role in your practice, and it is essential to acknowledge the rapport and trust that patients have developed over time. Whether a staff member is departing or joining, patients may experience feelings of anxiety, confusion or disappointment.
Ensure that your patients are informed of staff changes well in advance, preferably before their next appointment. Unlike for fee increases, using social media to introduce a new staff member is a great way to create excitement and keep patients informed. Use multiple channels, including letters, emails and your website. Provide a comprehensive introduction, including their photo, bio, credentials and interests. Enlist the support of existing staff members to introduce and welcome the newcomers to patients, fostering a sense of community.
agd.org/impact 9 Communications
Expressing gratitude and appreciation for departing staff members is also a crucial step. Wish them well in their future endeavors, and encourage patients to do the same, either in person or by sending cards or email. Additionally, consider sharing positive feedback or testimonials from patients about the departing staff, creating a positive closure to their chapter at the practice.
New Technology
Introducing new technology is an exciting opportunity to enhance the patient experience. This may include a cone beam computed tomography machine, dental scanner, computer-aided design/computer-aided manufacturing system, more comfortable radiography sensors, transitioning from paper charts to electronic health records, or installing TVs in operatories. While these advancements significantly improve patient care, it’s crucial to recognize that they may seem intimidating to those unfamiliar with the technology. Therefore, keeping patients well-informed is key to ensuring their comfort and confidence.
This is also an excellent change to highlight on your social media platforms and website, setting your office apart from others in the community. Clearly articulate the benefits of the technology and offer insights into how it will be integrated into the practice.
While new technology enhances efficiency, quality and safety, it may pose challenges for patients, from unfamiliarity to perceived costs. To ensure a smoother transition, emphasize benefits such as reducing pain, discomfort or anxiety; improving diagnosis or treatment; and saving time and money.
Showcase the technology in action through in-person demonstrations, videos or brochures. If feasible, allow patients to experience it firsthand. Models, radiographs or images can effectively highlight the transformative differences between old and new technology.
When making changes, it’s important to inform your staff first. Your whole team needs to be on the same page and understand the importance of the changes you’re making. Many patients will ask our staff their thoughts before asking us dentists.
Communication is key when it comes to conveying changes in a dental office. By being transparent and keeping patients informed, you can help ensure a smooth transition and maintain patient trust. ♦
Gerard Scannell, DDS, is a general dentist practicing in his hometown of St. Petersburg, Florida. To comment on this article, email impact@agd.org


10 AGD IMPACT APRIL 2024
Communications
2023 Humanitarian Award Winner Dedicates His Life’s Volunteerism to One Region
Dr. Michael E. Lacey’s immersive, peoplefocused work shows the incredible impact long-term volunteerism can have on communities.
When Karen Lacey first heard Michael (“Mike”) E. Lacey, DMD, MAGD, speak about the genocide being committed against the Cambodian people during a speech class at Portland State University in 1978, she knew his passion for the people of that region and their suffering was genuine. “I saw the pain in Mike’s heart watching the entire world do nothing to stop the genocide,” she said.
It had been Mike’s dream for decades to be able to help the people of Cambodia, and the Laceys’ interest in and concern for issues throughout Asia was also strengthened by two of their
Background Information:
The Cambodian Genocide
The Cambodian genocide refers to the systematic killing of 1.5 to 2 million people — nearly a quarter of Cambodia’s population at the time — between 1975 and 1979 by dictator Pol Pot and the Khmer Rouge political party and its army. Some death toll estimates reach as high as 3 million, though 2 million is the most widely agreed upon number. The genocide began after the Khmer Rouge overthrew the democratic Khmer Republic after the Cambodian Civil War. Out of a desire to turn Cambodia into a self-sufficient agrarian society, Pol Pot employed ethnic cleansing to murder hundreds of thousands of people from ethnic minorities throughout Cambodia as well as political dissidents. Pol Pot’s administration banned the existence of more than 20 ethnic minorities, including ethnic Chinese and Vietnamese Cambodians, Muslim Chams, and Christian Cambodians. The Khmer Rouge created 189 execution prisons to house political dissidents; out of the estimated 14,000–17,000 people held in these execution centers, only 12 are known to have survived. Additionally, hundreds of thousands of Cambodian citizens who refused reeducation and assimilation were murdered by the Khmer Rouge in areas dubbed “Killing Fields” and dumped into mass graves. The Khmer Rouge administration was ousted from Cambodia in 1979 after Vietnam invaded Cambodia, though it and Pol Pot continued to fight a guerilla war against the Vietnamese

children, Mathew and Rachael, who were born in South Korea. “In 2009, when we were invited to Thailand to create our first dental hygiene clinic, Mike and I had no idea that this was our first step to serving the Cambodian people,” said Karen, who used her knowledge as a speech language pathologist to assist in the development and execution of the project.
invasion and retained an insurgent presence in Cambodia. The Khmer Rouge also retained Cambodia’s United Nations seat, along with much international support — including from the United States — as late as 1993.
During the genocide, hundreds of thousands of Cambodians fled to Thailand, where many remained for several years out of fear of returning to their country. A total of 260,000 Cambodian refugees were resettled, with more than 150,000 resettling in the United States. In 1991, a peace agreement was reached between the contending parties in Cambodia, with Vietnam withdrawing its military, and the United Nations facilitated the repatriation of 360,000 Cambodians from refugee camps in Thailand and border camps. In 1993, an independent Cambodian government was established, and the monarchy was also restored to a ceremonial position.
Sources
• “Cambodian genocide.” Britannica, britannica.com/event/Cambodian-Genocide.
• “What is Genocide: The Cambodian Genocide.” The Holocaust Explained, The Wiener Holocaust Library, theholocaustexplained.org/what-was-the-holocaust/what-was-genocide/the-cambodian-genocide/.
• González, Maya. “Experiencing Forced Displacement: Cambodia.” United States Holocaust Memorial Museum, 28 March 2022, ushmm.org/genocide-prevention/blog/experiencing-forced-displacementcambodia.
• “Cambodia.” College of Liberal Arts, Holocaust and Genocide Studies, University of Minnesota, cla.umn. edu/chgs/holocaust-genocide-education/resource-guides/cambodia.
• “Genocide in Cambodia.” Holocaust Museum Houston, hmh.org/library/research/genocide-in-cambodiaguide/.
• Ben, Kiernan. “The Survival of Cambodia’s Ethnic Minorities.” Cultural Survival, 2 March 2010, culturalsurvival.org/publications/cultural-survival-quarterly/survival-cambodias-ethnic-minorities.
agd.org 11 Member Spotlight
Mike at the dental trainer graduation ceremony with Gun (Hmong tribe), Sawalok (Ahka) and Napaporn (Hmong), in Chiang Kham, Thailand, January 2010.




At first, the focus of their project was to serve children from the hillside villages of Thailand where there were no local dentists. The rural mountainous areas of northern Thailand are mostly populated by minority ethnic groups — many of whom are indigenous to the region — referred to as the hill tribes of Thailand. Members of the hill tribes face many disadvantages due to their remote location as well as inequalities in their social and citizenship statuses within the country.
“On our second trip to Thailand,” Karen said, “we established a fully operational dental operatory at the Home of Blessing. On opening day, Mike was given 57 handwritten notes from every child who’d had dental pain. He was overwhelmed and saddened. Consequently, after reflection and prayer, we were inspired to change our focus to a preventive approach using older students as ‘dental trainers,’ who would then train the younger children in dental hygiene skills.”
“Ultimately, we were invited to develop three dental hygiene training programs for children,” said Mike. “The first was in Chiang Kham, Thailand, at the Home of Blessing; the second in Chiang Rai, Thailand, at Happy Homes; and the third at Poipet, Cambodia, at Mercy Ministries Foundation. At each training center, we trained primarily high school students to become dental trainers. These dental trainers would then be tasked with providing dental hygiene training clinics to other children at the training centers, other schools, other orphanages, their villages, and to adult leaders from other rural villages who would take that information back to provide dental hygiene training for the children of their villages. The project has gone from getting our feet wet in Thailand to moving into Cambodia, where the needs are astronomically greater than in even the remote rural villages of the hill tribes of Thailand. Our goal was to improve the conditions for the people of Cambodia, and that has been on our hearts for decades.”
Their method of incorporating and enmeshing the local community into their volunteerism has enabled the Laceys to have an exponential impact on the areas in which they have served. And, while the focus of the Laceys’ program was oral healthcare, their work had an equally impactful additional effect: youth development.
“The self-confidence that this program built in the young women and men who served as dental trainers was a positive impact we had not even considered when we initially created this concept,” said Karen. Additionally, dental trainers were given certificates acknowledging the training program they had completed and the work they had done, which opened up new job opportunities for them.
“Their enthusiastic, engaging and creative teaching methods captured the attention of and inspired thousands of children,” said Mike, who emphasized that their work would not be possible without the partnerships formed and investments from the dental trainers. “From never having a dental experience — or from having horrific dental experiences when they were younger — to having them want to become a part of our team — it was incredibly rewarding.”
The Laceys have been volunteering in Thailand since 2009 and Cambodia since 2014. Dedicating your volunteerism to one region the way the Laceys have over the decades necessitates a different approach than visiting different countries or regions
12 AGD IMPACT APRIL 2024 Member Spotlight
Patchaleeda and Muay applying flouride at a Chiang Rai, Thailand, orphanage.
Malee demonstrates brushing for a child.
Mike training Happy Homes dental trainers in Chiang Rai, Thailand.
Phachadela, a dental trainer, providing dental hygiene training in Chiang Saen, Thailand, in 2014. Dental trainers developed educational posters in their own languages.

of the world each trip, and it also changes the trajectory of what your impact can be.
The process of developing and sustaining a successful international project included learning about the Thai and Khmer cultures and required a vast group of experienced partners. It was a priority for the Laceys to show honor and respect for the Thai and Khmer people and their cultures.
Long-term impact requires long-term relationships and partnerships, and the Laceys worked extensively with local experts and organizations. Rather than going in with their own prescription, they listened first. “Prior to each trip, we learned to communicate extensively with the nongovernmental organizations (NGOs) that were requesting our services,” said Karen. “We spent considerable time learning how to best support their needs.”
Through their work, Mike has taught 75 young people to be dental trainers for their communities. Together, he and his dental trainers have hosted over a hundred dental clinics across Thailand and Cambodia and provided dental hygiene training to more than 5,000 children and adults. “Mike has a profound sense of joy and accomplishment from the training, nurturing and observing of the dental trainers he has taught,” Karen said. Additionally, the Laceys have sponsored two scholarships for past dental trainers from their program: Phatchari Loescher completed an RN program in 2021 and currently works full time as a nurse; Naowalak Pattipakdee earned a BA in English in 2016 and now lives in Minnesota. The
Laceys have spent over $250,000 of their personal funds to pursue their volunteer work. One year, the trip cost amounted to a third of the income from Mike’s solo dental practice.
“Over the last 18 trips, we faced countless challenges and hurdles — illnesses, equipment malfunctions, missing our family, team members cancelling, spontaneous changes to the schedule,” Karen said. “In reflection, we do believe that we experienced true miracles that allowed our project to flourish. One such miracle has been the recent improvement in access to care for the hill tribe people of Thailand. Our dear friend, Dr. Suchit Poolthong, president of the Thai Dental Council, has worked ambitiously with the Thai government to establish three new dental schools in northern Thailand.”
Though his work in Cambodia is far from over, Mike has already been honored with AGD’s Humanitarian Award for his selflessness and commitment to bettering the oral health of the communities in which he has served. In his acceptance speech during the 2023 AGD House of Delegates annual meeting, Mike gave his heartfelt thanks: “Thank you again, AGD, for recognizing this project in Southeast Asia. I joyfully accept this award on behalf of all of our dental trainers in Thailand and Cambodia who improved the dental health of thousands of underserved children. Ќhxbkhuņ māk, arkoun chraen — thank you very much.”
Watch Mike’s award acceptance speech video here: youtube. com/watch?v=3AuaFg8Huj0. ♦
agd.org 13
Children receiving dental hygiene training at Safe Haven primary school in Poipet, Cambodia, January 2020.

Animal Magnetism
Some Veterinarians Are Drawn to Oral Healthcare
By William S. Bike

What dental specialty allows a practitioner to perform a sinusotomy on a standing patient who happens to have 12 pounds of teeth or fix a tooth the patient broke by biting an antler? The answer is animal dentistry, which was not even considered a specialty until the late 1980s1 and is almost never performed by an individual holding a DDS or DMD degree.
Those who provide oral care for animals are all veterinarians, said Naomi Hoyer, DVM, assistant professor in dentistry and oral surgery at the College of Veterinary Medicine and Biomedical Sciences at Colorado State University
(CSU) and diplomate of the American Veterinary Dental College (AVDC).
“Human dentists cannot work on animal patients except in special cases, and then they must be directly supervised by a veterinarian,” she added. “All Board Certified Veterinary Dentists™” — a term trademarked by the AVDC — “are veterinarians.”
History
Animal dentistry was not always so organized. As early as 600 B.C., equine dentistry evolved in China due to the value of horses in both trade and everyday life. Full veterinary dental texts first appeared in the late 19th and early 20th
centuries and included techniques in small animal dentistry as well. 2
But it was not until 1976 that the American Veterinary Dental Society was formed, 1987 that the Academy of Veterinary Dentistry began (since merged with the Foundation for Veterinary Dentistry) and 1988 that the AVDC was granted provisional accreditation as a veterinary specialty college by the American Board of Veterinary Dentistry. 3,4
“There was not a lot of dental college and board certification in dentistry when I graduated,” said Travis Henry, DVM, who matriculated from the Michigan State College of Veterinary Medicine in
14 AGD IMPACT APRIL 2024
Stephen Juriga, DVM, performs root canal therapy on Whirl, a 16-year-old tiger, at Brookfield Zoo Chicago. Whirl is also pictured on the cover. (Credit: Jim Schulz/Brookfield Zoo.)



1993. “They were just getting started, and, at that time, you worked on everything related to animal health.”
In 2020, the American Veterinary Medical Association Council on Education added dentistry to its accreditation standard on the curriculum.5
Hoyer noted that the “typical pathway” for those who are interested in animal dentistry starts with “a BA or BS, four years of veterinary school, one year of an internship, and three-to-four years of residency in veterinary dentistry.”
Focusing on Animal Dentistry
Veterinarians decide to focus on animal dentistry for the same reasons dentists decide to specialize — interest in and enjoyment of the topic plus a desire to help others.
Practicing in rural Wisconsin, Henry began to see horses with dental issues. “I just started researching what to do and how to treat them,” he said. “It became a passion over the next five years.” Once he sold his first practice in 2003, Henry decided he “was going to just do dentistry” and started Midwest Veterinary Dental Services in Elkhorn, Wisconsin, in 2003.
Because of his proficiency, Pfizer Animal Health (now Zoetis) asked him to go to different practices to teach horse diagnostics, techniques and tactics, which caught the attention of the University of California-Davis, where he worked in the university’s horse dentistry practice for seven years.
“I loved my time there and made a lot of professional friends,” Henry said.
Stephen Juriga, DVM, of the Veterinary Dental Center in Aurora, Illinois, chose to pursue a veterinary dental residency. “After 15 years in general practice, I found dentistry to be very rewarding,” he said. “The patients that received dental services had improved comfort and lived longer, healthier lives. Pet owners routinely said that their pets now acted five years younger.”
Specialties Within the Specialty
The AVDC provides Non-Species Specific Board Certified Veterinary Dentist™ and Board Certified Equine Veterinary Dentist™ board certifications, along with an Advanced Zoo and Wildlife Certification.6
“When they finish their training, residents submit their credentials package and then take a two-phase exam in order to become board-certified,” Hoyer said.
The Ross University School of Veterinary Medicine in St. Kitts, West Indies, calls it “one of the most difficult specialty examinations in veterinary medicine” with “a first-time pass rate of only 33%.”7
“Most of the veterinary dentists in the all-species category primarily treat dogs, cats and small mammals,” Juriga explained. “The equine specialists have advanced training in equine dentistry and oral surgery and are specially equipped to primarily treat horses.”
Juriga holds the Advanced Zoo and Wildlife Certification. Zoos do not have dentists on staff but instead consult with veterinary dentists or human dentists who have experience in treating zoo
animals. Juriga provides dental and oral surgical services to Brookfield Zoo Chicago in Brookfield, Illinois, and the Shedd Aquarium in Chicago. Henry is the rare veterinarian double-boarded in NonSpecies Specific and Equine dentistry.
“I think there are six of us,” he said. “We’re a pretty small group. But most veterinary dentists definitely specialize.”
Differences and Similarities
Among Human and Animal Teeth
Animal dentistry requires dentists to become familiar with the oral biology of dozens of animals, from mammals to fish and more.8
“Enamel, dentin and cementum make up any mammal’s tooth, whether you’re talking about a horse, cow, pig or human,” Henry said. “But there are different variations based on what we eat.”
Additionally, Juriga noted that, “there is quite a difference in function, occlusion and anatomy — and we are less concerned with esthetics [than human dentists]. We lack verbal feedback from our patients and depend on imaging and probing to diagnose conditions and treat disease. Therefore, cone beam computed tomography (CBCT) has become a standard of care.”
The differences between human teeth and those of our most common furry companions are easy to see and understand. “Dogs and cats are carnivores, and their teeth are sharp and interdigitate,” Juriga said. “Canine teeth are long and pointed, designed for grasping and holding prey. Their premolars and molars are pointed
agd.org/impact 15
Juriga irrigates the 73-mm root canal. The canal is obturated.
The restorative is light-cured.


and sharp and are designed to cut and shear meat from their prey, and they mainly swallow food in whole chunks. Whereas humans have flat crowns designed for grinding and chewing food.”
Meanwhile, the teeth of our barnyard friends have some surprising qualities. “Ruminants — horses, goats, sheep, rabbits — have fat molars designed for chewing coarse foods like hay, seeds and grasses, and these teeth continually erupt and wear throughout their lives,” Juriga added.
“The term ‘long in the tooth’ comes from what happens in herbivores because their teeth keep elongating and erupting out of the mouth all the time,” Henry noted.
“Reptiles, lizards, and many marine mammals — such as dolphins and seals — have sharp teeth that angle backward and are designed to hold food and move it into the oral cavity,” Juriga said.
“It really comes down to how good the anatomy of the mouth is to start,” Henry noted. “If you have a bunch of crooked teeth — whether you’re a horse, dog, cat or human — your teeth are not going to clean themselves through the chewing process. You’re going to have periodontal disease, which, when unchecked and untreated, ends up in tooth loss.”
Horse teeth, however, have an interesting distinction. “Horses are a little different because the only place on their teeth with enamel that’s exposed to the oral cavity is
right on the chewing surface, so they do a pretty good job of cleaning that,” Henry added. “But, if horses have bad anatomy, you can imagine what happens when hay is stuck between teeth and rotting and how much inflammation that can cause.”
Juriga noted that animal dentists often perform periodontal procedures, such as teeth cleaning, root planing and bone grafts. “Small-breed patients are more prone to bone loss, and many need extraction therapy,” he said.
Fractured teeth can be prevalent “in working or sporting breeds as well as many zoo animals, such as lions, tigers, bears, primates and gorillas,” Juriga said. “These are often treated with root canal therapy and crown therapy for working dogs.”
“This wave of giving your dog antlers to chew on is very good for our business and very bad for the dog’s teeth because it causes tooth fractures,” Henry said. “I’ve had people argue with me and say this is ‘natural,’ but, in the wild, animals don’t eat the skeleton unless they’re starving.”
Since animals may develop oral tumors, “CBCT imaging determines extent and directs our biopsies, and our biopsies are submitted to veterinary oral pathologists,” Juriga noted. “Tumor resections or maxillectomies/mandibulectomies are performed similarly to those performed by oral and maxillofacial surgeons in human dentistry.”
“We routinely perform partial mandibulectomies on dogs, and they go back to catching frisbees and hunting,” Henry said.
In addition, “facial trauma from falls, vehicle incidents or housemate animal bites can result in temporomandibular joint (TMJ) luxations and fractures of the maxilla and mandible,” Juriga explained. “We utilize interdental wire/composite bonding, interfragmentary wires or titanium plates to treat these patients.”
Pet, Zoo and Farm Dentistry
Whether their practices concentrate on pet, zoo or farm dentistry, veterinary dentists deal with a variety of species and must be versatile.
“There is no such thing as a typical day,” Hoyer explained. “At CSU, we might be traveling to one of our zoo partners, teaching students, performing surgery on TMJs or treating a cat with maxillofacial trauma.”
“Zoo veterinarians perform comprehensive examinations, including oral exams and imaging, allowing us to diagnose and provide care,” Juriga said. As a consulting veterinary dentist for the Shedd Aquarium, he also has treated sea otters and sea lions for fractured teeth.
“Zoo animals are tightly controlled and monitored, and zoos generally do a great job taking care of animals,” Henry said. “I couldn’t make a living just seeing zoo animals.”
16 AGD IMPACT APRIL 2024
Juriga examines a police dog. Juriga cleans the teeth of a sedated patient.
A challenge of pet dentistry is that often “our patients don’t exhibit signs or symptoms of oral pain or disease,” Juriga said. “Few pet owners look in their pets’ mouths, and it isn’t until we perform an exam under anesthesia with probing and imaging that we identify an issue.”
He explained that “70% of dogs and cats have gingivitis or periodontal disease, 50% of cats have tooth resorption, and 24% of dogs have tooth fractures, which often expose the pulp because the enamel in dogs is much thinner than in humans.”
He noted that, in the wild, if an animal has poor dentition, “something eats them, and they don’t pass that trait along to their offspring. Horses graze up to 18 hours per day, so they’re constantly salivating and bathing the teeth. But when you put an animal in confinement and feed them twice a day, they eat all their meals in a very short period of time and do nothing the rest of the day with their teeth. That causes problems.”
“Everyone asks, ‘Do dogs get braces?’” Juriga said. “The short answer is yes — we will provide orthodontic repositioning to correct a painful occlusion.”
Collaboration
“Some veterinary dentists collaborate individually with human dentists on cases,” said Hoyer. “But human dentists should not be practicing veterinary medicine.”
“In the early days, we learned a lot from human dentists and endodontists, but now we have our own research and more often collaborate with one of our own,” said Henry. “Veterinary dentists collaborate all the time.”
“Veterinary dentists and human dentists have gathered experience over the years and can serve as resources for each other, as they have purchased or created instruments and learned or developed treatment strategies to overcome challenges like long root canals,” Juriga noted, mentioning the example of kangaroos, wallabies and rhinoceroses not opening their mouths. “Therefore, we use a surgical approach through the cheek or long, specially designed elevators and luxators for intraoral procedures.”

Anesthesia
“In veterinary medicine, all our patients have to be anesthetized” for dental procedures, Hoyer said. But animals’ owners frequently object.
“There’s a whole camp of people talking about anesthesia-free dentistry in dogs and cats,” Henry said. “And the research has shown that it causes more harm than good. When people try to scale their own dog’s teeth or have the groomer do it, dogs will bite, squirm and try to jump off the table. Veterinary dentists need to get radiographs taken in the mouth to make diagnoses. So, small animals like dogs and cats go under general anesthesia.”
Anesthesia is delivered by “a team of one dental veterinarian and multiple veterinary dental nurses who have advanced training in anesthesia, which is performed with the same medications, monitoring and support that we humans receive at the hospital,” Juriga said. “We use individual anesthetic protocols based on the animal’s age, type of procedure and health status. We have protocols for pets with heart
disease, kidney disease, liver disease and diabetes.
“Veterinarians who educate with visual tools — models or photos — overcome pet owners’ fear of anesthesia” and “have the highest case acceptance,” he added.
For horses, the situation is a bit different. “You can sedate a horse,” Henry said. “They will sleep standing up and don’t have to lay down, so we can have them remain standing and do most of the work on them.”
Homecare
Homecare begins with prevention of oral disease in animals on the part of their owners. “Oral gels, sprays or water additives are not effective,” said Juriga. “We demonstrate how to provide daily plaque control with moist gauze or a toothbrush.” He noted that his team members encourage pet owners “to condition pets to accept touching the outsides of their teeth” by giving them a food reward, making it easier for the pet to accept toothbrushing, cleaning and polishing, and even a dental procedure. “Our goal is to have a cooperative pet,” Juriga said.
agd.org/impact 17
Juriga works on JoJo the gorilla at Brookfield Zoo Chicago.
“When clients ask me if they should brush their dogs’ teeth, I tell them, ‘Only the ones you want them to keep,’” Henry said.
“There are a few vets who have campers set up with the ability to do anesthesia at [the pet owner’s] place, but we like them to come in where we have a full lab, can do blood work, and can come up with an anesthetic protocol,” he noted.
Juriga also opts for in-office exams and treatment. “I do not know of any mobile
veterinary dentists, although quite a few provide services at multiple locations. Ultimately, over 90% of our patients require anesthesia, dental radiographs and CBCT. This requires a specially designed facility and support staff.”
For horses, however, “we do a lot of homecare,” Henry said. “We have a mobile rig, and we can unload a stockade to put the sedated horse in with a ‘horsey dental chair’ contraption that holds them so we can work
on them. Horses have 12 pounds of teeth. We can do a sinusotomy on a horse in a standing situation without full anesthesia.”
A Successful Journey
When Henry was in veterinary school, he learned that “horses had teeth and some people worked on them,” he said. “That was about the extent of our dental training. We’ve come a long way in 30 years. People can get dental work done on

Root Canals on Military Working Dogs
By Capt. Jennifer Keegan and Heidy Perry
In the military, about 1,600 working dogs are helping protect our nation.1 These working dogs perform a wide variety of jobs, including search and rescue, explosive detection and drug detection. Military dogs can also be trained as patrol dogs. Patrol dogs use their strong jaws and teeth to subdue would-be attackers. All U.S. military branches rely on working dogs; thus, it is essential that they are at optimal health. Optimal health in military dogs includes a balance of proper diet, exercise and routine visits with the veterinarian for regular checkups. A high-quality diet helps military dogs remain healthy as they deal with environmental and physical challenges. Their diet is a fixed formula that ensures consistency and helps avoid health problems caused by alteration in nutrition.2
If a military working dog is not at optimal health, they could be distracted from their duties, resulting in potential harm to their handler or even themselves. If a working dog has dental pain, they can be removed from their specific duties, either temporarily or permanently, depending on the severity of the dental condition. Since a military working dog is predicted to be worth up to $150,000, keeping them healthy and focused is crucial.3
Veterinarians are often the first line of defense when evaluating and treating dental disease in animals. The curriculum of veterinary schools includes training on various aspects of dentistry, such as diagnosis of dental disease and periodontal, orthodontic and endodontic treatment.4 However, if a veterinarian feels that the dental treatment needed is out of their scope of practice, they can consider referring the animal to a Board Certified Veterinary Dentist™, a specialty recognized by the American Veterinary Medical Association.5 Uniquely in the military, it is common to have a veterinary clinic partner with a military dental clinic for treatment of the condition.
The veterinarian clinic on Tinker Air Force Base (AFB) is responsible for the care of Transportation Security Administration (TSA) and military working dogs from both Texas and Oklahoma,
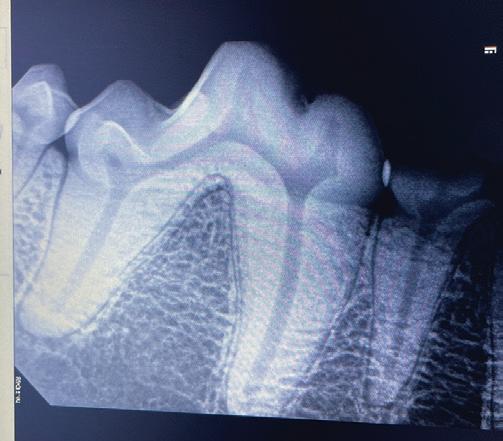

including Griff, a certified patrol dog that works at Altus AFB. During a bite work session 10 days prior, Griff started crying and spitting out the wrap used during training. Her handler noticed a slow worsening of behavior each session thereafter and decided to take Griff to see her veterinarian, Heather Cameron, DVM, at Tinker AFB. Cameron noticed a round 3 × 3 millimeter gingival abscess on the buccal gingiva between teeth Nos. 408 and 409 (the mandibular right molars). Radiographically, periapical radiolucencies were noted around both the mesial and distal roots of No. 408 and around the distal root of No. 409. Gutta percha was placed in the draining abscess and traced to the distal root apex of No. 409. The decision was made to proceed with root canals rather than extractions since both Nos. 408 and 409 are important teeth for Griff’s job as a certified patrol dog. In addition, extracting the two molars could lead to a greater chance of jaw fracture.
Griff was intubated and placed under general anesthesia by Cameron and her veterinarian team. Lt. Col. Ryan Gustafson, DDS, a general dentist; civilian Heidy Perry from the Tinker Dental Clinic; and myself, also a general dentist, completed endodontic treatment on Griff.
Both Nos. 408 and 409 had similar anatomy: three separate cusps with respective pulp horns connecting to two different
18 AGD IMPACT APRIL 2024
Pre-op radiographs of teeth Nos. 409 (left) and 408 (right).
animals by practitioners who are comfortable doing it and passionate about it.”
“There are not enough veterinary dentists,” Hoyer concluded, citing the high value placed on zoo and farm animals and people’s love of pets. There are only about 200 Board Certified Veterinary Dentists in the world.7 “So we are needed.” ♦
William S. Bike is a freelance writer and editor based in Chicago. He is a former director of

advancement communications for the University of Illinois Chicago College of Dentistry. To comment on this article, email impact@agd.org
References
1. Coffman, Curt R. “The Decade of Dentistry: Moving Veterinary Dentistry Forward.” DVM 360, 10 Feb. 2023, dvm360.com/view/thedecade-of-dentistry-moving-veterinary-dentistry-forward.
2. Easley, Kevin. “Veterinary Dentistry: Its Origin and Recent History.” Journal of the History of Dentistry, vol. 47, no. 2, July 1999, pp. 83-85.
3. Foundation for Veterinary Dentistry, veterinarydentistry.org. Accessed 14 Jan. 2024.

canals per tooth. Due to their unique morphology, access was made at all three cusps at tooth No. 409 and at two of three cusps at No. 408. The middle cusp on tooth No. 408 was not accessed due to concern that there would be too little tooth structure remaining after preparation. Dog apical morphology differs from humans, and research shows that adult dogs have a high prevalence of “apical delta” morphology, with what has been termed a “sprinkler-rose” anatomy demonstrating multiple pulpal pathways that radiate peripherally.6 The prevalence of an apical delta in dogs is estimated to be nearly 70%, with a greater incidence in mandibular teeth.7,8 An apical delta allows for a definite stop, which aids in cleaning, shaping and obturating the canal.
The initial apical file lengths were documented with periapical radiographs. Hand files were used up to the maximum size that the veterinary office had (a size 100 file is equivalent to 1 millimeter in tip diameter), and then a combination of rotary files (Lightspeed LSX size 90 and ProTaper Gold size F5) were used to clean and shape the canals. The canals were significantly wider than 100 (estimating close to 160–200 in size for the master apical file), so focus was put on taking the largest rotary files in the clinic and copious amounts of sodium hypochlorite to meticulously clean the walls of the chambers and canals. The canal spaces were cleaned, shaped and obturated with bioceramic sealer and warm gutta percha that
4. Bellows, Jan. “D Is for Dental Organizations.” DVM 360, 21 April 2023, dvm360.com/view/d-is-for-dental-organizations.
5. Fiala, Jennifer. “Dentistry Training May Be Required in U.S. Veterinary schools.” VIN News Service, Veterinary Information Network, 16 July 2020, news.vin.com/default.aspx?pid=210&Id= 9729066#update.
6. “Find a Board Certified Veterinary Dentist™.” American Veterinary Dental College, avdc.org/find-a-veterinary-specialist/. Accessed 14 Jan. 2024.
7. “What Is Animal Dentistry?” Ross University School of Veterinary Medicine, 23 June 2021, veterinary.rossu.edu/about/blog/what-isanimal-dentistry.
8. Newman, Elizabeth. “A Different Kind of Patient.” AGD Impact, vol. 40, no. 5, May 2012, pp. 40-44.

was vertically condensed. The coronal aspects were finalized with amalgam restorations.
The endodontic procedures were successful in alleviating Griff’s pain, and she was returned to full duty.
The views and expressions in this article do not necessarily reflect policies or standpoints of the Department of the Air Force.
References
1. “Four-Legged Fighters.” U.S. Department of Defense, defense.gov/Multimedia/Experience/Four-LeggedFighters/.
2. Yanof, Susan, and Michelle Ross. “Readiness of Military Service Animals.” Scientific Advances in Animal Nutrition: Promise of the New Century, Committee on Animal Nutrition, Board on Agriculture and Natural Resources, Division on Earth and Life Studies, National Research Council, 2001, nap.nationalacademies. org/catalog/10299/scientific-advances-in-animal-nutrition-promise-for-the-new-century.
3. Green, Ranny. “What Do Military Working Dogs Do?” American Kennel Club, 1 Sept. 2021, akc.org/expertadvice/news/what-are-military-working-dogs/. Accessed 12 March 2024.
4. “Veterinary Dentistry.” American Veterinary Medical Association, avma.org/resources-tools/avma-policies/ veterinary-dentistry. Accessed 12 March 2024.
5. Dodd, Bert; American Veterinary Dental College. “Veterinary Dental Specialists.” Veterinary Medical Teaching Hospital, Texas A&M Hospital, vetmed.tamu.edu/vethospital/wp-content/uploads/sites/15/2023/02/ Dodd-Website.pdf. Accessed 5 February 2024.
6. Gao, Xianhua, et al. “Micro-CT Evaluation of Apical Delta Morphologies in Human Teeth.” Scientific Reports, vol. 6, no. 36501, 7 Nov. 2016, doi.org/10.1038/srep36501.
7. Gamm, David J. “The Incidence and Morphology of the Apical Delta in the Canine Tooth of the Dog.” Master’s Theses (1922-2009), Marquette University, 1990, epublications.marquette.edu/theses/5200.
8. Watanabe, Kazuhiro, et al. “The Formation of Apical Delta of the Permanent Teeth in Dogs.” Journal of Veterinary Medical Science, vol. 63, no. 7, 2001, pp. 789-795.
agd.org/impact 19
Left to right: Dr. Cameron, Lt. Col. Gustafson, Staff Sgt. Welsh, Capt. Park, Capt. Keegan, Stacey Freeman, Heidy Perry.
Griff under anesthesia.
Oral Cancer: Updates from AGD and Around the World
AGD Foundation Update Current Happenings and Future Goals
By James R. Keenan, DDS, MS, MAGD
2023 was a year of change, growth and rapid forward momentum for the AGD Foundation. We worked to expand awareness of oral and oropharyngeal cancers and improve access to education and screening.
Our accomplishments included:
• Creation of the AGD Foundation website (agdfoundation.org).
• Development of the AGD Foundation Oral Cancer Toolkit — a free comprehensive resource for patients and providers on our website.
• Development of a monthly e-newsletter, AGDF eBulletin.
• Creation of our own social media platforms on Facebook, LinkedIn and X (formerly known as Twitter), with Instagram coming in 2024.
• Achieving nearly 100% giving from our AGD regional constituencies at the 2023 House of Delegates.
• Expanding awareness of our grant program and funding six grants for 2024, totaling $21,300.
AGD Foundation 2024 grant recipients are:
Pennsylvania AGD
Oral screening day at the Capitol
(May 16, 2024)
Proposed number of patients served: 144
Grace Clinic, Washington
Oral cancer education for free clinic patients
(March 1, 2024 – Feb. 28, 2025)
Train 100 volunteer professionals and provide over 500 screenings
Midvale Community Building Community, Utah
Expanding oral cancer screening access in rural and underserved Utah (June 1, 2024 – Dec. 31, 2024)
Proposed number of patients served: 400
The Latest Oral Cancer Research Around the Globe
The battle against oral cancer is a long and gradual one. While major breakthroughs may be years away, scientists around the world are still making progress learning about the disease and the best treatments to recommend. AGD Impact has compiled some of these developments so that general dentists can stay abreast of developments around the globe.
UNITED STATES
Brush Biopsy Enables Early Detection of Oral Cancer Without Surgery
A new diagnostic kit, created and patented by researchers at the University of Illinois Chicago College of Dentistry, uses a small brush to collect cells from potentially cancerous lesions inside the mouth. The sample is then analyzed for genetic signals of oral squamous cell carcinoma, the ninth most prevalent cancer globally. This new screening method improves upon the
current diagnostic standard of surgical biopsies — an extra referral step that risks losing patients who sometimes don’t return until the cancer progresses to more advanced, hard-to-treat stages.
Source: “Brush Biopsy Enables Early Detection of Oral Cancer Without Surgery.” UIC Today, 17 Jan. 2024, today.uic.edu/brush-biopsy-enables-early-detectionof-oral-cancer-without-surgery/.
Researcher Developing Oral Rinse that Detects Mouth and Throat Cancers
A researcher at Sylvester Comprehensive Cancer Center, part of the University of Miami Miller School of Medicine, is leading the development of an oral rinse for detecting mouth and throat cancers.
Elizabeth J. Franzmann, MD, and her team have invented an inexpensive and noninvasive salivary screening test that uses a patented combination of three biomarkers to identify molecular features associated with cancers
Maryland State Dental Association (MSDA) Foundation
MSDA Foundation outreach: Bridging gaps in oral healthcare
Proposed number of patients served: 400
Floss Boss Care
Oral cancer awareness
(Full-day program, April 1, 2024)
Number of patients served: 150–300
West Virginia Health Right, Inc.
WVHR Mobile Dental Unit
(Jan. 1, 2024 – Dec. 31, 2024)
Number of patients served: 2,000
2024 Strategic Goals
In 2023, the AGD Foundation board convened to define its strategic goals for 2024 and beyond, including:
resulting from tobacco, alcohol and the human papillomavirus virus.
Source: Westlund, Richard. “Oral Rinse Detects Mouth and Throat Cancers.” University of Miami Miller School of Medicine News , 22 Nov. 2023, news.med.miami.edu/cancer-oral-rinse/.
UCLA
Dentistry–Led Team to
Use $5
Million Federal Grant to Develop Effective, Nonaddictive Synthetic Cannabinoid to Help People Manage
Oral Cancer Pain
Igor Spigelman, PhD, chair of the biosystems and function section at the University of California, Los Angeles School of Dentistry, has received a $5 million grant from the National Institute of Neurological Disorders and Stroke for research aimed at developing a nonaddictive cannabisbased pain medication for oral cancer patients. Synthetic cannabinoids — lab-developed chemicals intended as an alternative to
20 AGD IMPACT APRIL 2024
• Establishing the AGD Foundation as the trusted charitable arm of AGD.
• Creating a sound financial infrastructure.
• Expanding the reach of the foundation.
• Engaging larger and more diverse populations.
Our work to educate dentists and the general public about the importance of human papillomavirus (HPV) vaccination continues to be at the forefront of our efforts. Our oral cancer screening programs at the AGD scientific session and other venues remain a centerpiece of our efforts. We are in the planning stages of the oral cancer screening program that will be held at AGD2024 in Minneapolis this July. If you are interested in volunteering for this program, we encourage you to contact us directly at AGDF@ adgcommunications.com.
We are revamping and updating our annual silent auction. Many of you visited our booth at AGD2023 in Las Vegas. You suggested some items and brands you’d like to see available in future silent auctions — and we listened. In 2024, we are working hard to include new items that
appeal to our growing and increasingly diverse constituency. And we are bringing back some old favorites, too. We hope you will visit our booth at AGD2024 and come ready to bid! We will also reprise the online silent auction app so you can bid from anywhere.
Our educational print materials and public service announcements with compelling testimony from oral cancer survivors will be offered at the scientific session and House of Delegates annual meeting. If you are interested in receiving materials to distribute in your practice, please contact AGDF@adgcommunications.com. And ask about our #WeScreen campaign.
How Can I Support the Work of the AGD Foundation?
There are many ways you can support our work:
• Host an oral cancer screening event at your institution or practice.
• Donate to the AGD Foundation online by visiting agdfoundation.org/donation-form
• Make the AGD Foundation a beneficiary of your philanthropic legacy giving.
marijuana — target receptors outside the brain. Unlike traditional medicinal cannabis, which has shown efficacy in treating pain but is marred by significant side effects, these drug compounds can be created without addictive properties.
Source: Alkaly, Ben. “Can Cannabis-Based Meds Help People Manage Oral Cancer Pain?” UCLA Newsroom , 20 Oct. 2023, newsroom.ucla.edu/releases/cancannabis-based-meds-help-with-oral-cancer-pain.
Calcium Channel Drives Oral Cancer Pain and Growth
An essential protein that acts as a gatekeeper for calcium entering cells promotes the growth of oral cancer and generates pain, according to a study led by researchers at the New York University College of Dentistry.
Targeting this protein — the ORAI1 calcium channel — could provide a new approach to treating oral cancer, which causes persistent pain that worsens as it progresses.
Source: “‘Gates of Heaven’ Calcium Channel Drives Oral Cancer Pain and Growth.” NYU News Release , 5 Sept. 2023, nyu.edu/about/news-publications/ news/2023/september/gates-of-heaven-calciumchannel-oral-cancer.html.
Turmeric-Derived Drug Shows Promising Results in Combating Oral Cancer
Los Angeles Veterans Affairs scientists are experimenting with a nontoxic drug called APG-157. The drug is derived from turmeric and has shown promising results.
“The drug comes in the form of a gummy lozenge [and] has been given to newly diagnosed, locally advanced patients (stages 1-4) with oral or oropharyngeal (throat) cancer before other treatments. It has shown to reduce tumors, lessening the need for extensive surgery and intensive therapies,” said Marilene Wang, MD, one of the researchers. Source: Zick, Schirete. “VA Clinical Trial:











• Donate in-kind items to the electronic silent auction held during AGD2024 in Minneapolis.
• Get involved! Do you want to be part of the AGD Foundation governing body or volunteer on a committee? Contact us at AGDF@adgcommunications.com
• Follow us on social media. We have created pages on LinkedIn, Facebook and X.
We appreciate the support of our AGD members, sponsors and the larger dental community for more than 50 years, and we look forward to your continued support for 50 more. ♦
James R. Keenan, DDS, MS, MAGD, is president of the AGD Foundation. He is a clinical assistant professor, oral and maxillofacial pathology, radiology and medicine, at New York University. He is also a longtime member of AGD and a member of the AGD Foundation Board of Trustees. To comment on this article, email impact@agd.org
Promising Results in Combating Oral Cancer.” VA News , 26 April 2023, news.va.gov/118481/ clinical-trial-combating-oral-cancer/.
INDIA
Microbial Biomarkers May Help Detect Oral Cancer
Early detection of oral cancer may soon be possible with the assistance of oral microbial biomarkers. A new study by King George’s Medical University and IMTECH Chandigarh found that a significant group of microorganisms commonly in the mouth can undergo changes when cancer is present. The researchers are working now to develop a biomarker.
Source: “Microbial Biomarkers to Help Detect Oral Cancer Soon: Study.” The Times of India , 5 Feb. 2024, timesofindia.indiatimes.com/city/lucknow/microbialbiomarkers-to-help-detect-oral-cancer-soon-study/ articleshow/107412992.cms.
agd.org/impact 21
AGD2024
THE PREMIER MEETING FOR GENERAL DENTISTRY
Upgrade Your Knowledge and Skills at AGD2024
The best part of being a general dentist is that no two days are alike; one day, your schedule could start with routine preventive exams, lead to an afternoon of restorative procedures and then cap off with an emergency root canal just before dinnertime. Other days, you may get to sink your teeth into a full-mouth reconstruction with
AGD2024
July 17—20
Minneapolis, Minnesota Register now at agd2024.org
In addition to attending cutting-edge hands-on courses and lectures, network with colleagues, students and dental team members at the following special events:
President’s Reception
Exhibit Hall
Thursday, July 18: 5:45–7:30 p.m.
Speed Mentorship Event
New Dentist Lounge
Friday, July 19: 2:30–3:30 p.m.
Student & New Dentist Reception
New Dentist Lounge
Friday, July 19: 3:30–5 p.m.
Convocation Ceremony & Reception
Saturday, July 20: 4:30 p.m. (ticketed event)
an all-on-X procedure. But part of being a jack-of-all-trades is that you have a lot of trades to stay on top of. This summer, why not get yourself up to date on 20 different topics — all in one weekend?
AGD2024 has a dynamic schedule specifically crafted with general dentists’ education needs in mind.
Featured Speakers and Subject Areas
010 Basic Sciences
Brian B. Nový, DDS
070 Endodontics
Brett E. Gilbert, DDS
135 Laser Therapy/ Electrosurgery
Bruce L. Cassis, DDS, MAGD
Robert A. Convissar, DDS, FAGD
142 Medical Emergency Training & CPR
Eric Wong, DDS, MAGD
149 Multidisciplinary Topics
Fellowship Review Course
180 Occlusion
Van B. Haywood, DMD
250 Operative (Restorative) Dentistry
Lee Ann Brady, DMD
John Nosti, DMD, FAGD, FICOI
310 Oral and Maxillofacial Surgery
Bart W. Silverman, DMD
340 Anesthesia and Pain Management
Tom Viola, RPh, CCP
346 Opioid, Controlled Substances and Pain Management
Tom Viola, RPh, CCP
370 Orthodontics
Chung How Kau, BDS
430 Pediatric Dentistry
Robert A. Convissar, DDS, FAGD
Lance E. Kisby, DMD, FASDC, FAAPD, MAGD
490 Periodontics
Jim Grisdale, DDS
550 Practice Management and Human Relations
Mike Abernathy, DDS
Roger P. Levin, DDS
Melissa Turner, BASDH, RDHEP, EFDA
Ryan Vet, MBA
610 Fixed Prosthodontics
John Nosti, DMD, FAGD, FICOI
Amelia Orta, DMD, FACP
670 Removable Prosthodontics
John Nosti, DMD, FAGD, FICOI
690 Implants
Ian Erwood, BSc, DDS, FAGD, FICOI
Cory Glenn, DDS
Gene Peterson, MS, CDT
Randolph R. Resnik, DMD, MDS
Charles Schlesinger, DDS, FICOI
730 Oral Medicine, Oral Diagnosis, Oral Pathology
Jamison Spencer, DDS, MS
750 Special Patient Care
Mai-Ly Duong, DMD, MPH, MAEd, MAGD
Ronald R. Zentz, RPh, DDS, FAGD, CPHRM
780 Esthetics/Cosmetic Dentistry
Van B. Haywood, DMD
Gigi Meinecke, DMD, FAGD
22 AGD IMPACT APRIL 2024
JULY
20 AGD2024.ORG
MINNEAPOLIS, MN
17 -
Testing the Tools
By Ross Isbell, DMD, MBA
U Should Try the U-Shaped Brush
Autobrush®
tryautobrush.com


The traditional toothbrush head has always focused on single teeth as the target of cleaning, and it is the patient’s responsibility to ensure enough time is devoted to each tooth and each area. In contrast, the Autobrush® is a U-shaped tray boasting 58,000 bristles at about six different angles that surrounds teeth on all three sides. The trays are available as single or double arches. Autobrush offers a manual brush without a motor, a powered brush with a sonic vibration motor, and a version with a motor and a light kit. With any of the models, the patient uses a circular motion to move the trays and bristles to reach back to the molars toward the anterior, posterior, up and down. The motor handle produces a sonic vibration into the tray and bristles with three different modes. Personally, I couldn’t feel a significant difference in the modes, and the sonic pulses were not intense enough to clean effectively without manual motion. However, a 30-second routine with the full-mouth tray setup definitely feels as effective as two minutes with a regular brush. The light kit on the Sonic Pro model includes a blue light for antimicrobial care and whitening and a red light for near-infrared muscle relaxation and improved gingival blood flow. According to proprietary research, the Autobrush is 27 times as effective as a manual brush, which, to me, means it likely is as effective as the highend power brushes I normally prescribe. The large squarish handle is significantly easier to grip than a standard cylindrical shape. Using the Autobrush is simple enough that my twoyear-old could do it after two attempts, and he loves that the lion face on the handle plays a song for him to dance to while he brushes. This also would be a great tool for individuals with occupational therapy struggles, such as difficulty gripping a normal-size brush handle or rotating a brush head for modified Bass technique and 45-degree angulations as recommended by the American Dental Association. At a price point of around $100 for a handle, tray and foaming toothpaste, it is comparable to or cheaper than a standard power toothbrush.
For a Better Floss Flaus
goflaus.com


I tell my patients that there is no replacement for string floss when it comes to interproximal cleaning techniques, but that doesn’t stop me from trying to find other flashier options to keep them entertained and engaged in their comprehensive homecare routines. Many patients utilize simple flossers, but there are some options for upgrades. The Flaus sonic flosser has the same general design as more inexpensive flossers — two arms and a strand of floss suspended in between — but the rechargeable battery pack handle can produce up to 18,000 vibrations a minute with three intensity modes (I prefer the highest). The silky mint-flavored floss attached to the removable and recyclable heads slides easily into contacts and is shred-resistant so that it can be reused if the threads are cleaned and don’t stretch out. That means that the 45 heads that come with each pack can last for months. The battery can last for eight hours, which is about two months of normal use. When flossing and reaching the deepest area of the gingival sulcus, I typically move the flosser up and down while pressuring against a tooth for about five seconds to achieve the most biofilm disruption possible. If you decide after purchasing that this isn’t something you want to use as part of your homecare routine, the fingers of the flosser head can also function as an injection site distractor like a VibraJect®. My only complaint is that the flosser heads are only in one orientation, so it is better fitted for insertion into posterior contacts than anterior. If you are looking for an effective flossing aid that does more than just physical debridement, check out Flaus.
Ross Isbell, DMD, MBA, currently practices in Gadsden, Alabama, with his father, Gordon
Birmingham (UAB) School of Dentistry and completed a general practice residency at UAB Hospital. Isbell has confirmed to AGD that he has not received any remuneration from the manufacturers of the products reviewed or their affiliates for the past three years. All reviews are the opinions of the author and are not shared or endorsed by AGD Impact or AGD. To comment on this article, email impact@agd.org
agd.org/impact 23
Isbell, DMD, MAGD. He attended the University of Alabama at
Oral Care When You’re On the Go
Brushee brushee.com
Encouraging patients to practice constant oral hygiene sometimes feels like a losing battle. This is especially true for patients who are undergoing clear aligner therapy and need to have teeth cleaned quickly and frequently. For that purpose, the Brushee device combines a toothbrush with toothpaste, toothpick and flosser. The included toothpaste doesn’t have any bioactive ingredients but does freshen breath with a minty flavor, and the small brush head is surprisingly effective at cleaning interproximally. The toothpaste is substantial enough that it needs to be rinsed out, so plan for having water handy. Each Brushee is individually wrapped, so it can stay clean in a pocket or purse until use. This inexpensive but highly functional device is perfect for patients to keep with them on the go.

Look for the following articles in the March/April 2024 issue of AGD’s peer-reviewed journal, General Dentistry.
• Prosthetically driven robot-assisted implant surgery: turning a major failure into a simple case
• Oral manifestations of mpox (monkeypox)
• Possible dental implant failure attributed to embedded pencil graphite: first clinical report
Read these articles and more at agd.org/ generaldentistry.
In the May issue of AGD Impact:
• Dental Social Media Influencers
• AGD Constituencies with CE Centers

HAVE YOU MOVED?
If you have recently moved, or plan to in the near future, please make sure to update your AGD profile.
Log into the AGD website today!
We want to make sure you receive AGD publications and other important information from us! View or update your profile, check the status of your membership dues, manage your email subscriptions and change your password.
Please contact the AGD Membership Services Center with any questions at 888.243.3368 (toll-free) or 312.440.4300.
Our member representatives are available to assist you
Monday through Friday from 7:30 a.m. to 5:30 p.m. CST.
UPDATE YOUR PROFILE
agd.org/my-agd




24 AGD IMPACT APRIL 2024 Testing the Tools
Dental Marketing AGD Corporate Sponsors
Upcoming
ATTEND THE PREMIER MEETING FOR GENERAL DENTISTRY
Expand your knowledge and grow professionally with AGD2024’s numerous education offerings:
• Network with more than 2,500 fellow dentists and AGD members.
• Have the opportunity to earn more than 54 CE credits.
• Participate in interactive courses.
• Gain best practices from industry thought leaders.
• Attend free New Dentist Lounge lectures.
• Attend cutting-edge learning lab presentations.
Make the Most of Your Stay in Minneapolis
With its beautiful lakes, expansive park system, thriving arts scene, plentiful shopping and great food, Minneapolis offers a great backdrop for AGD2024 and is a great destination whether you plan on bringing guests or traveling solo.








AGD2024
MINNEAPOLIS, MN JULY 17 - 20 AGD2024.ORG
THE PREMIER MEETING FOR GENERAL DENTISTRY
General & Course Registration Is Now Open! agd2024.org Academy of General Dentistry Nationally Approved PACE Program Provider for FAGD/MAGD credit Approval does not imply acceptance by any regulatory authority or AGD endorsement 11/16/1990 to 5/31/2028 Provider ID# 216217