
15 minute read
CPD: Retrobulbar Injections in Filler-related Vision Loss

Miss Rachna Murthy and Professor Jonathan Roos explore the emergency management of filler-induced vision loss
Advertisement
Modern hyaluronic acid (HA) based dermal fillers have the power to change lives. Their popularity has grown,1 and with it the concern around complications.2 Although exceedingly rare, none is perhaps more feared than the onset of vision loss after an injection.2 Not surprisingly, a brief internet search will find many courses offering training in retrobulbar injection with hyaluronidase – the enzyme that can break down HA. However, is there evidence to suggest that it works? This article explains the latest evidence for the emergency management of filler-induced vision loss, why retrobulbar injections could compound the injury and why this approach is best avoided.
Understanding retrobulbar injections A retrobulbar hyaluronidase injection is often advocated as an emergency treatment following blindness caused by HA dermal filler injection. It involves passing a sharp 23 gauge bevelled needle behind the globe.3 It is passed either through skin or conjunctiva at the outer third of the orbit and advanced straight back for 15mm and parallel to the floor, before changing to point upwards and inwards, passing through into the muscle cone behind the eye. As shown in the larger central image in Figure 1, the globe itself is 23.5mm and the orbit 4.8mm – so a needle length of 38mm (red) is more likely to hit the optic nerve than 24mm (green). However, optic nerve damage is not the only potential danger. Needles can penetrate the globe, causing glaucoma, retinal detachment and eventual phthisis (an unsightly shrunken eye). Haemorrhages behind the eye can cause further damage to nerves and muscles and a painful compartment syndrome. Introduction of infection can spread back into the cavernous sinus with devastating consequences. In fact, there is even danger to the opposite unaffected eye; ocular trauma can reveal antigens normally hidden from the immune system and cause an autoimmune disease against the previously healthy eye.4 When blindness in one eye becomes blindness in both eyes, medicolegal questions will arise – particularly if the clinician is inexperienced in the technique.
Basic research evidence for retrobulbar hyaluronidase Given that there are courses available for teaching retrobulbar technique, one would have thought that there would be strong preclinical evidence for its use. Indeed, HA can be digested when a ligated cadaveric blood vessel filled with HA is suspended in a bath of hyaluronidase overnight.5 But when this experiment was repeated with living blood vessels the enzyme could not cross the wall into the lumen.6 The orbit and vasculature also have inhibitors of hyaluronidase activity which will deactivate any injected enzyme.7,8 Furthermore, the central retinal artery, which is blocked with filler in filler-related vision loss, enters inside the optic nerve and is covered with dura, pia and arachnoid mater layers preventing passive enzyme ingress.9,10 Despite the pre-clinical improbability – could retrobulbar hyaluronidase still work clinically?
Retinal detachment intraocular haemorrhage

Iris trauma cataract Damage to optic nerve Corneal opacity pthisis bulbi

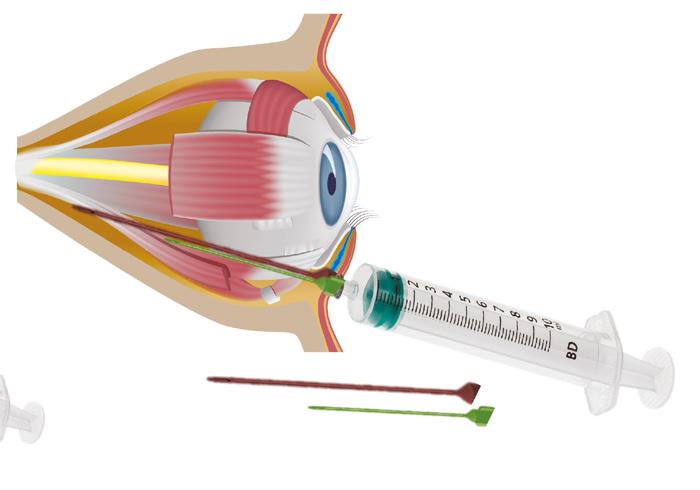
Retrobulbar haemorrhage damage to muscles
STEP 1: Confirm diagnosis
Record vision using written text/Snellen chart on smart phone/laptop.
Check pupil light reflex is direct and consensual and check for relative afferent pupil defect (RAPD).
Check and document eye movements in cardinal positions of gaze – preferably with video.
Check confrontation visual fields.
STEP 2: After diagnosis whilst other measures are being prepared
Demonstrate ocular massage to patient and commence .
Call local ophthalmology centre for help. Have their number readily available.
Hypercapnia: rebreathing into a paper bag, limited by symptoms of dizziness.
Consent patient for hyaluronidase treatment.
Have resuscitation equipment available as hyaluronidase has 0.1% risk of anaphylaxis.
Reconstitute 1500IU of hyaluronidase (Wockhardt) in 1ml bacteriostatic saline. To 0.5ml hyaluronidase solution add 0.5ml saline = 750 IU per ml. Ensure you and your staff know the location of your hyaluronidase.
Inject hyaluronidase into area where hyaluronic acid was originally injected and all around angiosome distribution of vessel supply by serial puncture including supratrochlear/supraorbital area (75IU in 0.1ml up to 1500IU for vessel distribution). Review reperfusion and repeat every 15 to 30 minutes.
If available: preferably IV rather than oral acetazolamide (Diamox) 500mg bolus and any topical ocular antihypertensives (e.g. beta blocker, iopidine, dorzolamide).
Prepare transfer to ophthalmology .
Send hyaluronidase with patient for ophthalmologist as they may not have any in stock.
STEP 3: Specialist ophthalmic interventions
Consider inferotemporal quadrant retrobulbar hyaluronidase injection 1500IU in 4ml saline with 25G retrobulbar needle.
Limbal paracentesis with removal of 0.1-0.2ml of aqueous from anterior chamber (remove the plunger on an insulin syringe to allow passive filling). Do not continue with ocular massage.
Repeat hyaluronidase to vascular territory hourly till capillary refill time (CRT) less than four seconds (up to six cycles per day).
Consider: 1. Repeat retrobulbar hyaluronidase 2. IV heparin/steroid if available 3. Hyperbaric oxygen if available 4. Scar management 5. Pain management according to analgesic ladder
STEP 4: Ophthalmic investigations (but not if delay treatment)
Consider neuroimaging with angiography.
Fundus fluorescein angiography.
Optical coherence tomography/ultrasound.
Table 1: Recommended interventions for visual loss after HA filler treatment as per Murthy et al. 19
Clinical evidence for retrobulbar hyaluronidase Unfortunately, here too the evidence is weak. Clinical certainty is elusive as our knowledge is gathered from sporadic case reports which differ in factors such as time of onset, delay to treatment, area affected, co-morbidities, and treatment type.11 A review of 44 cases has not found a single instance of successful retrobulbar treatment where the vision was objectively assessed before the intervention.12 Any successes have had multiple confounders preventing conclusions from being drawn.11 As retinal ganglion cells begin to progressively infarct after as little as 12-15 minutes of non-perfusion due to their high metabolic requirements,13 it is perhaps not surprising that there has been such little success in treating blindness. What is thought to perhaps help however, and much more safely, is pulsed hyaluronidase treatment into the affected vascular area, and in the area of the supraorbital artery, where there are anastomoses with the internal carotid circulation – some hyaluronidase may be injected intravascularly.14 There may, however, still exist a role for retrobulbar hyaluronidase. This is in the setting of orbital pain and changes in eye and lid position. Unlike the rapidly infracting retina, the muscles in the orbit are more resilient.15 The supplying vessels are not encased in dura and may be more amenable to treatment with prolonged ischaemia.10 Treating dermal filler blindness To date, there is no documented evidence of an intervention resulting in complete vision rescue after central retinal artery occlusion with HA.16 The matter is further complicated by a not insignificant rate of recorded spontaneous resolution (22-87%) after central retinal artery occlusion (CRAO) due to other emboli.17 The mechanism of filler-induced blindness is also debated; it can likely be caused not just by filler blocking the lumen (inside passage) of the vessel but also perhaps by external compression of a vessel, or a vessel being sent into spasm from filler. In 2019 the AIIVL Consensus group published guidelines recommending retrobulbar hyaluronidase be performed by an ophthalmologist within a 90-minute window.16 This is also recommended in current guidance by the Aesthetic Complication Expert (ACE) Group World.18 However, we recently contributed to an international consensus group including colleagues from California, France and the UK which looks at new evidence.19 Whilst acknowledging the difficulty in analysing case studies, we devised a protocol, representing our best advice based on the available clinical and in vitro evidence (Table 1). This advice includes taking into account the relative risk of the intervention causing harm.

Figure 2: Duplex ultrasonography can readily identify the supraorbital and dorsal nasal arteries. An ultrasound device such as the 18mHz Toshiba linear probe can be used to identify plane of injection and digital occlusion prior to injection.
What can we do to avoid filler-induced blindness? It is better to avoid complications than to treat them. We therefore also recommend employing the below prevention methods whenever possible.
1. Aspirate prior to injection when using a needle on bone. Blood in the syringe can suggest entry into a vessel lumen.20 Note that this method cannot be relied upon completely, depending on the filler rheology, needle diameter, fullness of syringe and aspiration time.
21
2. Perform micromovements when injecting in soft tissue. This ensures that any intravascular injection is only short-lived and of a small volume.22
3. Use ultrasound. This can reduce risk by detailing local vessel anatomy (Figure 2)2 before and during injection,24 and with digital compression of vessels using pressure with your fingers. Applying pressure over the orbital rim can reduce anastomotic passage of emboli into ophthalmic circulations and alter flow direction of any potential embolus.25,26 4. Choose needle or cannulas appropriately. Though a recent study has suggested that cannulas, being less sharp, are safer than needles this need not be the case in every situation.27 A fine bore cannula may act as a needle. When injecting onto bone, needles can allow cleaner penetration, while cannulas may be preferable when injecting into soft tissues. A limitation to many complication reports is whether a cannula or needle was used at the time of injection, complicating analysis. But evidently, complications can occur with either.
5. Use correct volumes and force. Even a very small volume can obstruct the CRAO when flow is reversed at a circulatory anastomosis.28 The evidence does not suggest a safe or dangerous volume, rather the correct volume to achieve the desired clinical effect should be given slowly and with as little force as possible. With higher forces, an HA embolus can be propelled against the arterial current before release of pressure allows it to flow forward and block the CRAO.29
If at all possible, injection pressure should not exceed pulse pressure.
Consider that ‘gentle and slow is the way to go’.
6. Choose the correct filler. There is no suggestion in the literature that a particular filler is more or less likely to cause occlusion and vision loss, but those with a higher cohesivity and cross-linking would be expected to be more likely to obstruct vessels. One should therefore use high G’ products where they are indicated, in areas for lift, and use the less cohesive products in the higher risk areas such as the tear troughs and orbit.
Aesthetics Clinical Advisory Board Lead, and co-author of the new hyaluronic acid related vision loss guidelines, Mr Dalvi Humzah says… Iatrogenic induced visual loss is devastating to the patient, and when faced with this complication it would arguably be difficult for the practitioner to remain calm and provide appropriate treatments. Retrobulbar injections of hyaluronidase have for some time been proposed as a treatment modality; when considering this it is important that we address both the practitioner’s competence and the evidence of effectiveness. In this article Miss Rachna Murthy and Professor Jonathan Roos present the compelling view that this procedure should only be considered in a specialist setting. For practitioners faced with this complication, this article provides an updated pathway that they can use in clinic and transfer patients onto specialists for further interventions. As noted in this article the evidence base for retrobulbar injections is confounded by many variables and when considering appropriate treatments, we should all be mindful of, and evaluate, the evidence base and anecdotal reports that are presented. There are several studies looking at alternative treatment protocols for visual loss and hopefully these will come to fruition in the near future. This is an essential read and provides practical advice for all practitioners in aesthetics.
More evidence is needed We believe the evidence for retrobulbar treatment is insufficient to advocate its use, particularly by those not routinely operating in or around the eye – a message that we, alongside the British Oculoplastic Surgery Society, are now trying to disseminate.30 The potential risks are significant, including to the other eye. Interventions depend not just on evidence but also a balance between their potential for benefit and harm. Weighing these up, we support ocular massage, rebreathing carbon dioxide, intraocular pressure lowering medication, as well as subcutaneous and supratrochlear hyaluronidase regardless of time of onset and delay to treatment.16 Only with further data can guidelines improve. We therefore urge practitioners who come across visual disturbance post filler, to ensure they inform the Medicines and Healthcare products Regulatory Agency (MHRA) through the Yellow Card System. Practitioners are also welcome, and encouraged, to assist in our further research on this topic by emailing FaceRestoration, so that we may help to inform further practice.
Miss Rachna Murthy is a Cambridge and Londonbased consultant oculoplastic and aesthetic surgeon and co-owns FaceRestoration. She is regarded as an authority on thyroid eye disease, eyelids, skin cancer and is on Allergan’s Faculty for filler complications. Miss Murthy trained in Melbourne, Chelsea and Moorfields, and sits on the RSM Eye Council and IMCAS Alert Board. Qual: BSc(Hons), MB, BS, FRCOphth
Professor Jonathan C P Roos is a Harvard, Cambridge and Moorfields-trained consultant oculoplastic surgeon and academic based in London at FaceRestoration. His work has been published in the world’s leading medical journals and he lectures internationally on aesthetics, eyelid diseases and thyroid eyes. With Miss Rachna Murthy, Professor Roos also runs a Cambridge dissection course for aesthetic filler safety called Aesthetic Clinical Training Academy. Qual: BA(Hons), MB BChir, MA PhD(Cantab), FRCOphth FEBO
Test your knowledge! Complete the multiple-choice questions below and go online to receive your CPD certificate!
Questions
1. The retinal ganglion cell survival time is…
2. Retrobulbar injections penetrating the eye can cause damage to the…
3. Which of the following manoeuvres can dislodge a hyaluronic acid retinal embolus…
4. Hypercapnia or rebreathing into a paper bag causes…
5. Which of these assessments are not necessary in the case of Hyaluronic
Acid Filler Embolus related vision loss?
Possible answers
a. 5 minutes b. 15 minutes c. 90 minutes d. 24 hours
a. Nasopharynx b. Frontalis muscle c. Facial nerve d. Other eye
a. Ocular massage b. Back massage c. Facial massage d. Lymphatic massage
a. Vasoconstriction b. Vasospasm c. Vasodilation d. Vasoproliferation
a. Check eye movements b. Check pupil reaction c. Check vision in each eye d. Check iris colour
Answers: 1. B, 2. D, 3. A. 4. C, 5. D
REFERENCES
1. International Society of Aesthetic Plastic Surgeons (ISAPS) International survey on aesthetic cosmetic procedures performed in 2018. ISAPS Global Survey Press Release. 3 Dec 2019. 2. Murthy R, Roos J, Goldberg R. Periocular hyaluronic acid fillers: Applications, implications, complications. Curr Opin Ophthalmol. 2019 Sep;30(5):395-400. 3. Fahmi A, Bowman R. Administering an eye anaesthetic: principles, techniques, and complications.
Community Eye Health. 2008;21(65):14-17. 4. Sympathetic ophthalmia. By: Chang GC, Young LH, Seminars in ophthalmology, 1744-5205, 2011
Jul-Sep, Vol. 26, Issue 4-5. 5. DeLorenzi C. Discussion: assessing retrobulbar hyaluronidase as a treatment for filler-induced blindness in a cadaver model. Plast Reconstr Surg 2019;144(2):321-324. 6. Hwang CJ, Mustak H, Gupta AA, Ramos RM, Goldberg RA, Duckwiler GR. Role of retrobulbar hyaluronidase in filler-associated blindness: evaluation of fundus perfusion and electroretinogram readings in an animal model. Ophthalmic Plast Reconstr Surg Jan/Feb 2019;35(1):33-37. 7. Fagien S, Carruthers J. Commentary on restoration of visual loss with retrobulbar hyaluronidase injection after hyaluronic acid filler. Dermatol Surg 2018;44(3):437-443. 8. Mio K, Carrette O, Maibach HI, Stern R. Evidence that the serum inhibitor of hyaluronidase may be a member of the inter-alpha-inhibitor family. J Biol Chem. 2000;275(42):32413-21. 9. Adulkar N, et al. An In Vitro Model Assessing the Penetration of Hyaluronidase through Optic
Nerve Dura for Management of Hyaluronic Acid Facial Filler Embolism. Plast Reconstr Surg. 2019
Jul;144(1):43e-47e. 10. Paap M, Milman T, Ugradar S, Silkiss R. Assessing Retrobulbar Hyaluronidase as a Treatment For
Filler-Induced Blindness in a Cadaver Midel. Plast Reconstr Surg. 2019 Aug;144(2):315-320. 11. Chestnut C. Restoration of visual loss with retrobulbar hyaluronidase injection after hyaluronic acid filler. Dermatol Surg Off Publi Am Soc Dermatol Surg 2018;44(3):435-437. 12. Kapoor et al (REF: Kapoor KM, Kapoor P, Heydenrych I, Bertossi D. Vision loss associated with
Hyaluronic Acid Fillers: A Systematic Review of Literature 2020 Jun;44(3):929-944). 13. Yu DY, Cringle SJ. Oxygen distribution and consumption within the retina in vascularised and avascular retinas and in animal models of retinal disease. Prog Retin Eye Res. 2001; 2:175-208. 14. Wibowo A, Kapoor KM, Philipp-Dormston WG. Reversal of post-filler vision loss and skin ischaemia with high-dose pulsed hyaluronidase injections. Aesthet Plast Surg. 2019 Oct;43(5):1337-1344. 15. Chen HY, et al. Proteomic Analysis of Various Rat Ocular Tissues after Ischemia-Reperfusion Injury and Possible Relevance to Acute Glaucoma. Int J Mol Sci. 2017;18(2):334. 16. Humzah MD, Ataullah S, Chiang C, Malhotra R, Goldberg R. The treatment of hyaluronic acid aesthetic interventional induced visual loss (AIIVL): A consensus on practical guidance. J Cosmet
Dermatol. 2019 Feb;18(1):71-76. 17. Hayreh SS. Central retinal artery occlusion. Indian J Ophthalmol. 2018 Dec;66(12):1684-1694. 18. Walker L, & King M, This month’s guideline: Visual Loss Secondary to Cosmetic Filler Injection, J Clin
Aesthet Dermatol. 2018 May; 11(5): E53–E55. 19. Murthy R, Ataullah S, Cartier H, Galatatoire O, Humzah D, Malhotra R, Goldberg R, Roos JCP.
Hyaluronic Acid Related Vision Loss: Pathophysiology, Prevention, & Emergency Interventions. (in submission). 20. van Loghem JAJ, Fouché JJ, thuis J. Sensitivity of aspiration as a safety test before injection of soft tissue fillers. Journal of Cosmetic Dermatology. 2018;17(1):39-46. 21. Kapoor KM, Murthy R, Hart SLA et al. Factors Influencing Pre-injection Aspiration for Hyaluronic Acid
Fillers: A Systematic Literature Review and Meta-analysis. Dermatol Ther. 2020 Oct 1;e14360. 22. Goodman GJ, Magnusson MR, Callan P, et al. A Consensus on Minimizing the Risk of Hyaluronic Acid
Embolic Visual Loss and Suggestions for Immediate Bedside Management. Aesthet Surg J. 2020
Aug 14;40(9):1009-1021. 23. Habib SM, Schelke LW, Velthuis PJ. Management of dermal filler (vascular) complications using duplex ultrasound. Dermatol Ther. 2020 Jul;33(4):e13461. 24. Loh KT, Chua JJ, Lee HM, et al. Prevention and management of vision loss relating to facial filler injections. Singapore Med J. 2016;57(8):438-443. 25. Tansatiti T, Moon HJ, Apinuntrum P et al. Verification of Embolic Channel Causing Blindness Following
Filler Injection. Aesthet Plast Surg. 2015 Feb;39(1):154-61. 26. Alam M, Kakar R, Dover JS, Harikumar V, Kang BY, Wan HT, Poon E, Jones DH. Rates of Vascular
Occlusion Associated With Using Needles vs Cannulas for Filler Injection. JAMA Dermatol. 2021;157(2):174-180. 27. Taylor G, Ian AO, Shoukath S, Gasgoine A, Corlett R, Ashtom M. The Functional Anatomy of the
Ophthalmic Angiosome and Its Implication in Blindness as a Complication of Cosmetic Facial Filler
Procedures. Plast Reconstr Surg 2020 Oct;146(4):745. 28. Cho K-H, dalla Pozza E, Toth G, Gharb BB, Zins JE. Pathophysiology Study of Filler-Induced Blindness.
Aesthet Surg J. 2019;39(1):96-106. 29. BOSS, Retrobulbar Hyaluronidase to reverse CRAO following injection of facial fillers, 24th February 2020. <https://www.bopss.co.uk/bopss/retrobulbar-hyaluronidase-to-reverse-crao-following-injectionof-facial-fillers/>








