39 minute read
Infant Deaths in Utah, 1850-1939


Infant Deaths in Utah, 1850-1939
By LEE L. BEAN, KEN R. SMITH,GERALDINE P. MINEAU, ALISONFRASER, and DIANA LANE
Of all the health revolutions that have taken place in the United States since 1850, the reduction of infant mortality is arguably the most dramatic and far-reaching. Because of the incompleteness and unreliability of surviving vital records, we will probably never know precisely the rate of infant deaths a century ago. But an informed estimate would be that somewhere between 15 and 20 percent of all American infants born in the second half of the nineteenth century died before they could celebrate their first birthdays. It also seems probable that in some large cities and industrial towns, as well as in certain areas of the South, the rates were considerably higher, ranging upward to 30 percent. 1
The United States' records of births and deaths are certainly incomplete and unreliable for the last half of the nineteenth century and the first three decades of the twentieth century. Nevertheless, increasing evidence supports two conclusions: First, there was a continuous, yet erratic, decline in mortality rates beginning roughly in the mid-nineteenth century not only in the United States but in western Europe as well. This long-term decline of death rates and increase in life expectancy is often referred to as the mortality transition. Second, central to the mortality transition was the control of infant and child mortality. 2
Given the fact that the mortality transition was greatly influenced by reduced deaths among children, several historical demographers in the United States and Europe have undertaken studies to document more explicitly where and when infant and child mortality came under control. In the United States these studies include analyses of vital records from states, cities, and counties that maintained vital records prior to the development of a national registration system. 3 Similar types of records are being organized and analyzed in Europe. 4 Studies of changing mortality and especially changing infant mortality do not, however, depend exclusively on the availability of some form of vital registration. In Europe there are an increasing number of village demographic histories based on reconstitution, or collating and linking birth (or baptism) and death (or burial) records from parish registries, family histories, and genealogies. In North America somewhat similar historical data sets have been compiled in Quebec and Utah. 5
The Utah data set is identified as the Utah Population Database, UPDB. The structure of the database is described in more detail below. It includes, among other records, an unusually large and accurate set of individual records of births and deaths linked into families and pedigrees. The record of births and infant deaths among the UPDB population provides an opportunity to add to the increasing understanding of the infant mortality component of the mortality transition, making available data for an American region for which there are few complete and accurate late nineteenth- and early twentieth-century official records. UPDB records allow us to study the fate of many children born in Utah from 1850 to 1939, and the data make it possible to extend the study of infant mortality beyond the measures used in almost all historical demographic studies of infant mortality. 6
Infant mortality is measured by the number of deaths of children under the age of one divided by the number of births occurring during the same interval of time—a year or a combination of years—standardized for purposes of comparison for each 1,000 births. The infant mortality rate may be divided into two components. The neonatal mortality rate is the number of deaths in the first month of life (formally, the first twenty-eight days of life) divided by the number of births during the year. The second component is the post-neonatal mortality rate, in which the numerator is the number of deaths during the second through twelfth months of life. It is important to include an analysis of all three measures. These infant mortality rates are the standard measure and the basis for comparing the historical record of Utah with other reports.
Improvements in infant mortality rates reflect various interventions. Neonatal mortality is primarily due to premature births, birth trauma, or congenital anomalies, and improvements in these rates depend, in part, on improved prenatal care, delivery systems, and medical intervention. Post-neonatal mortality rates, on the other hand, are more often due to infectious and parasitic diseases; a decline in these rates is usually the result of improved public and family health measures. Consequently, there are differences in the rates of improvement in these two components of the infant mortality rate. For example, a 1912 report concludes, "In all quarters greater significance is being attached to the fact that the greatest reduction in infant mortality so far has been in the digestive and respiratory diseases and that little headway has been made in cutting down the appalling death rate in the first few weeks of life." 7
In addition to showing general trends of early child mortality the data available in the Utah Population Database (UPDB) provide the detail necessary to approach the history of child-loss in Utah from 1850 through 1939 from a different perspective. The traditional measures of infant mortality may have provided stimuli and guidelines for public health and medical programs, but these measures provide little information on the experiences of families. Was the loss of children common across many families or concentrated among a few? We address this question by looking at the changing proportion of mothers experiencing the loss of a child as well as calculating when multiple deaths among brothers and sisters occurred within a single year as a means of evaluating historical references to epidemics.
Because UPDB does not include a record of every individual birth and death in Utah, we begin with a summary of -what official records are available and subsequently compare the UPDB rates with those available from other sources. Second, we summarize our reading of family and county histories that reflect on the deaths of children in Utah. Third, we present the trends in infant, neonatal, and post-neonatal mortality followed by an analysis of the frequency of child loss and the temporal clustering of infant deaths among families. Finally, -we conclude by placing our analysis in a broader context of historical change.
The Official Statistical Record
From 1850 through 1900, death records were collected at the time of each decennial census in the United States. These are valuable but incomplete resources because they depend on fallible retrospective reporting by community representatives, medical personnel, and family members. Early in the twentieth century, the federal government assigned responsibility to the Census Bureau to collect and summarize mortality records for states and cities that had in place an official registration system guaranteeing "at least a fair degree of completeness." Any state or city accepted into the system was identified as part of the Death Registration Area (DRA); initially, the DRA included only ten eastern states and the District of Columbia. 8 The Census Bureau became a permanent agency by act of Congress in 1902, and its first annual report of mortality statistics covered the period 1900-1904. These reports did not include Utah or Salt Lake City. Beginning in 1905 Salt Lake City was included as a DRA, but Utah at large was not included until 1910. 9 Utah began to collect death statistics statewide in 1904, but from 1904 through 1909 the state still did not meet the criterion of "reasonable completeness" in the registration of deaths.
Early official records, then, are sporadic, making comparisons over time difficult. In the case of Utah, there are mortality statistics associated with the censuses of 1850 through 1900 and then a set of annual records from 1910 onward. In the case of infant mortality—children dying in the first year of life per 1,000 births in the same year—accurate measures require complete counts of the number of infant deaths as well as the number of children born during a given year. However, information on births was not routinely collated and reported by the federal government until 1915, and Utah did not meet the "reasonable completeness" standard until 1917. 10
According to official records, Utah would seem to have had a lowerthan-average rate of infant mortality. Data collected in the decennial census of 1880 indicate that the infant mortality rate for the United States in that decade was 110.9 male deaths for every 1,000 male births and 90.5 female deaths for every 1,000 female births; for Utah, the rates were 87.2 for males and 71.6 for females. Using the Bureau of Census enumerations, Henry Hibbs calculated infant mortality rates for 1910 from the number of infant deaths relative to the number of children under age one counted in the 1910 census. He found that Utah had the lowest rate of infant deaths (82.3) among the twenty-two states reporting the number of infant deaths in 1910. 11 Of the states included in DRA in 1917, the records indicate that Utah again had the lowest infant mortality rate. By 1919, as other states were included in DRA, four had lower rates than Utah, but Utah's rate remained considerably lower than the national rate for the white population: 68 infant deaths per 1,000 births versus 91. These official records certainly suggest that mortality risks for infants and children may have been lower in Utah than in the earlier-settled, more densely populated areas of the eastern United States. However, these low rates conflict with historical references to frequent child deaths in Utah.
Historical References to Infant and Child Mortality
There have been a few remarkable community-level studies in Utah that give estimates of infant mortality for various periods in the nineteenth century using censuses, genealogies, and other records. Larry Logue used a variety of records to construct a life table for St. George, 1861—80. He writes, "Nearly 150 of each 1,000 newborns died before their first birthday, and mortality worsened in the next four years [of life]." Dean May employed an LDS church census of Kanab for 1874 and found an infant mortality rate of 10 percent, or about 100 deaths per 1,000 births. In addition, a 1985 analysis of the Utah Population Database using a variety of methods to adjust for missing deaths calculated a range of estimates of infant mortality rates for males born in 1880—89: 77.4 for the low and 104.4 for the high. These studies suggest higher infant mortality rates than those reported in either the 1880 or 1890 censuses. 12
More qualitative and individualized historical studies note the relative frequency of deaths among children. For example, Ed-ward A. Geary's history of Emery County reports that -when LDS apostle Francis M. Lyman visited the county in 1880, he was told that in one community there had been "but three deaths, and they were of children." Diphtheria epidemics appear to have taken a frightful toll on children, often resulting in the deaths of several children in the same family within hours or days of one another. Geary continues:
A family history from Davis County yields the same story of multiple deaths in the same family.
Among the volumes appearing in the recent Utah Centennial County History Series, diphtheria appears to be the second-most frequent epidemic after influenza. These county histories detail the spread of diphtheria throughout a wide range of counties, including Beaver, Carbon, Emery, Garfield, Kane, Millard, Morgan, Tooele, Uintah, Utah, and Wayne. Other sources identify diphtheria epidemics in Davis and Salt Lake counties, 15 and epidemics may have occurred in other areas as well.
The 1918—19 influenza epidemic is the most frequently cited epidemic in the county histories, but this epidemic disproportionally resulted in the deaths of young adults and especially males. 16 The histories also make references to other diseases typically associated with infant and child deaths. "Outbreaks of scarlet fever and smallpox also took a toll. Typhoid fever, usually contracted from polluted drinking water, was endemic in the county, claiming several lives each year. Pneumonia -was also a constant threat, especially to young children." 17 Throughout much of the state there was the problem of contaminated -water supplies, which resulted in the recurrence of typhoid and infant diarrheal diseases.
The negative picture of disease and early deaths noted in family and county histories corresponds to the high estimates of early infant mortality produced in the studies by Logue, May, and Lynch et al. Nevertheless, there may have been some advantage to living in Utah, away from the more densely settled eastern states where contagion was more likely, especially in the urban areas. In addition, there were some resources that may have reduced very early infant deaths. Many historical references indicate an extensive network of Utah midwives -whose reported record of mother and infant care is remarkable. For example, the daughter of Ellen Meeks Hoyt claims, "If my memory and those of others who live here serve, she never had a woman or a baby die out of the seven hundred cases she cared for." 18 In the case of Patty Bartlett Sessions, "of the 3,977 babies that she brought...[in only two] cases [did she have] cause to note any particular difficulty" 19 If the network of midwives was as successful as these two examples suggest, their work should be reflected in fewer deaths during the first month of life (neonatal mortality). The detailed data from the Utah Population Database allow for the analysis of neonatal mortality rates as well as post-neonatal mortality rates, although these measures did not become available in official statistics until 1920.
The Utah Population Database
To provide another view of the levels and changes of infant mortality we return to the Utah Population Database. As stated, a 1985 study by Lynch, Mineau, and Anderton made use of the UPDB in an earlier form. 20 Since that original study, the database has been expanded in a number of ways. For example, the grant acknowledged in this paper provided funding to enter Utah death certificates dating from 1904 until the present into the database. These records eliminated many cases of unknown death dates.
UPDB contains approximately 1.5 million genealogy records of individuals among families identified on selected "family group sheets" from the Family History Library of the Church of Jesus Christ of Latter-day Saints (LDS). The family group sheets were selected if one or more family members experienced a demographic event—-birth or death—in Utah. Further details regarding the selection and quality of records have been described in a number of previous publications. 21 The representative nature of the genealogy file has been demonstrated in a variety of demographic studies that include fertility, 22 birth spacing, 23 adult mortality, 24 and households. 25 Since the analysis by Lynch, Mineau, and Anderton using the Utah Population Database, perhaps the most important extension of the database has been the entry and linking of Utah death certificates from 1904 to the present. 26 The files now more accurately confirm dates of death from 1904 onward and show which children born in the nineteenth century survived to older ages.
This study limits analysis to a subset of the files. In the first analysis, we restrict our study to infants born in Utah between 1850 and 1939 where the exact dates of birth and death were recorded. In the second two analyses—mothers'losses of children and the clustering of family deaths within a specific time interval—-we use data where children are linked to mothers. In these cases the analysis is restricted to mothers -who married only once, gave birth to at least two children, and survived in an intact marriage until the mother reached the age of fifty, typically the upper limit of the age of childbearing.
There are some data limitations. Because the original core data set of UPDB consisted of family group sheets from the LDS Family History Library, the records are more likely to represent members of this church, although they do contain substantial numbers of individuals with no affiliation with the church. In addition, place of death is often missing among children who died during the late nineteenth century, although place of birth is generally well recorded. Therefore our analysis is based on infant and child deaths among those who were born in Utah; some relatively small number may have died outside of Utah. Other constraints are also necessary in the analysis of the data, and as these affect a particular form of analysis they are detailed in the following sections as needed.
Neonatal, Post-neonatal, and Infant Mortality, 1850 to 1939
Table 1* presents estimates of neonatal, post-neonatal, and infant mortality rates for the period 1850 through 1939 in five-year groups. Table 1 also includes data from federal statistics-censuses and vital statistics-as the basis for identifying differences between these two sources of data for selected years. The UPDB data are combined into five-year intervals to "smooth" the minor year-to-year fluctuations. Therefore, comparisons with nineteenth-century federal estimates are approximate because the UPDP estimates represent five years of events, while the federal estimates are for a single census year.
The major difference between the federal and the UPDB estimates is for 1850. The census reports an infant mortality rate of 203.3, but UPDB reports 44.9 for 1850—54. This difference may well reflect the fact that our UPDB analysis is limited to infants who were both born and deceased in Utah. The federal statistics would include infant deaths among migrants after their arrival in Utah even though some of the children may have been born outside of Utah. Therefore, the number of births—the denominator of the rate—used in the calculation of the federal rate in Utah may be underestimated.
There are several reasons why the UPDB rates for 1850—54 and 1855—59 may be low. First, the low rates may represent inconsistent recording of both births and deaths during the difficult early years of settlement. Second, given the low population density, contagion may have been less of a problem than it would be later on. 27 Third, given the difficulties of migration as well as the high rates of mortality in the sites from "which the settlers migrated, the earliest settlers and their infants may represent a robust group of survivors. 28 Unfortunately there is no information allowing one to conclude that any one reason is more important than others, and indeed all three may, in combination, account for these low rates.
With the exception of 1850-54, UPDB rates for the last half of the nineteenth century are higher than the federal estimates, suggesting that the census collection procedures may have been incomplete. 29 In the twentieth century, federal counts of post-neonatal deaths are higher than the UPDB estimates. These lower UPDB rates in the twentieth century may be due to the fact that the UPDB population is dominated by members of the Church of Jesus Christ of Latter-day Saints. These mothers may have had access to more resources—church and community—to provide assistance in the case of childhood medical crises. In spite of the differences in levels, it is clear that there is a close correspondence between the two estimates in terms of trends.
There is an advantage gained from separating the neonatal from the post-neonatal mortality rates. As noted above, the post-neonatal mortality deaths (from age two months through twelve months) are generally due to infectious and parasitic diseases and especially diarrhea. Post-neonatal rates generally decline from 1865—69 onward, but it is not until the turn of the century that the post-neonatal death rate falls below the neonatal death rates. A decline in neonatal mortality generally depends on improved pre and post-neonatal care as well as medical intervention. These improvements apparently did not become widely available until the early decades of the twentieth century. Thus, the neonatal rate does not begin to drop until after World War I.
The sharp increase in the rate of neonatal deaths from 1850—54 to 1865—69 may be due to the incorrect recording of early deaths as stillborns in the earlier years. The slight increase from 1865—69 through 1905—1909 may be the result of two factors -widely identified with increased risks of neonatal mortality. These are, first, the initiation of childbearing at relatively young ages and, second, relatively brief intervals between successive births. As we have shown elsewhere, there is a decline in the mean age of marriage across successive cohorts. Our earlier analysis of fertility change showed that, of those -women who eventually married, 48.4 percent of those born in 1835—39 married before age twenty and 58.2 percent of those women born in 1850—54 married before age twenty. These women -would have commenced childbearing approximately between 1850 and 1865. Women "who married before age twenty began childbearing early and gave birth, on average, to nine children. 30 In the absence of an unusually large number of multiple births (twins, triplets, etc.), an average of nine live births would suggest that the time between births would be relatively brief. Consequently, the increasing proportion of early marriages leading to early childbearing as well as successive short birth intervals may have increased the risk of neonatal mortality.
Examination of post-neonatal deaths suggests that there may have been a significant impact from diphtheria epidemics but little impact from the 1918 influenza epidemic. The post-neonatal deaths began to decline after 1865—69 but then increased during 1885—89 and 1890—94. This increase corresponds to several county history references to diphtheria. These include Beaver County in 1891, Carbon in 1891, Emery in 1886, Millard in 1889, Morgan in 1889, and Tooele in 1884. Diphtheria "was also reported at later dates in several counties, but it appears that the 1880s and 1890s represented crisis periods. If diphtheria itself did not actually increase postneonatal mortality, it may have slowed down the pace of improvement in infant mortality.
There is no evidence that the 1918—19 influenza epidemic disproportionately increased the number of post-neonatal deaths, but it does appear to have slowed the pace of improvement. The rates and numbers of post-neonatal deaths declined significantly from 1905—1909 to 1910—14. From 1910—14 to 1915—19 the numbers and rates continued to fall but at a slower pace. The 1918—19 influenza epidemic did not dramatically affect infant mortality because of the relationship between age and mortality unique to this particular flu epidemic; it was remarkable because of its great mortality among young adults and especially men. 31
Loss of Children in Families
UPDB provides opportunities to analyze data in ways not possible with vital statistics systems. These files, within "which husbands and wives are linked with children in a family unit, make it possible to answer questions of how many families experienced the loss of one or more children and when this trend changed. In this study we analyze sequential groups of mothers classified by the date of the mother's first childbirth in Utah. The data presented in Table 2* begin with mothers -whose first birth was in 1850-54 and end with mothers -who began childbearing in 1935-39. In Table 2 we summarize these data, looking at whether women lost one child, one or more, or two or more children. We also include a column with the average number of children born to mothers. To eliminate various confounding factors, -we limit the analysis to once-married women who gave birth to at least two children, who survived to age forty-nine, and whose husband did not die until after she reached age forty-nine.
Among the women who commenced childbearing in Utah during the period 1850 through 1854, more than 40 percent -would lose at least one infant. More than 25 percent lost one only, but 15 to 20 percent lost two or more infants. This high number of infant deaths coincided with a period when -women typically ended childbearing having given birth to an average of slightly more than nine children. This is not to suggest that the data indicate a causal connection between having many children and the death of infants. There is a relationship, but without further analysis one can only assume at this time that the more children at risk, the greater the likelihood of at least one (and perhaps more) dying. 32 The likelihood of experiencing multiple deaths (two or more) begins to fall after 1880; the chances of losing only one child begins to decline systematically only after 1890. The rate falls to approximately one in ten mothers losing one or more infants for those who began childbearing during 1935—39.
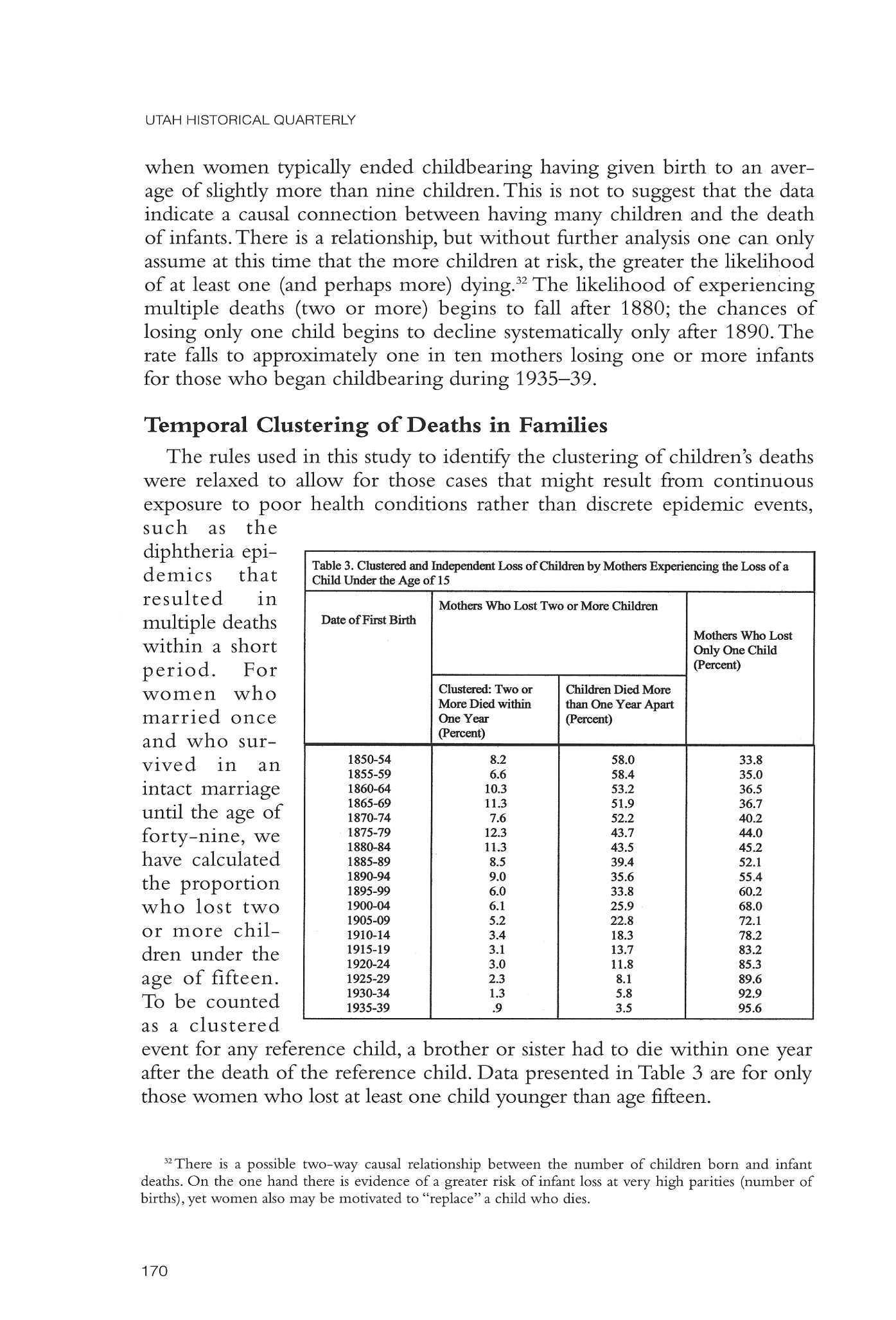
Temporal Clustering of Deaths in Families
The rules used in this study to identify the clustering of children's deaths were relaxed to allow for those cases that might result from continuous exposure to poor health conditions rather than discrete epidemic events, such as the diphtheria epidemics that resulted in multiple deaths within a short period. For women who married once and -who survived in an intact marriage until the age of forty-nine, we have calculated the proportion who lost two or more children under the age of fifteen. To be counted as a clustered event for any reference child, a brother or sister had to die within one year after the death of the reference child. Data presented in Table 3* are for only those women who lost at least one child younger than age fifteen.
Our data indicate that there is considerable variation in the percent of clustered cases among women who began childbearing during the period 1850 through 1894, but it is evident that clustering of deaths was not a rare event. More than 10 percent of the mothers beginning childbearing in 1860-64, 1865-69, 1875-79 and 1880-84 lost two or more children within a year. The numbers drop during the next two five-year intervals; nevertheless, roughly one of twelve mothers still lost two or more children within a brief period. The high rate of clustering also appears to coincide, approximately with the relatively early periods of settlement and the periods when highly contagious diphtheria was a major cause of death.
Summary and Conclusions
As Meckel stated in the paragraph quoted at the beginning of this article, our knowledge of the increasing control of infant and child mortality in the late nineteenth century and early twentieth century is incomplete because of the absence of reliable and accurate records. A number of recent efforts have provided better understanding of these changes through the development of historical data sets from census records, genealogies, parish records, and other sources. Complementing these sets of data specifically developed for demographic analysis is the Utah Population Database (UPDB), which was developed for purposes of medical research. UPDB provides detailed demographic information and the opportunity to study changes in infant and child mortality from the time of early settlement through the early decades of the twentieth century.
UPDB is not a completely accurate representation of changes in infant and child mortality in Utah, but it is certainly representative of trends. In the nineteenth century, UPDB shows infant mortality rates that were higher than those based on mortality statistics collected during the decennial censuses (with the exception of 1850). In the first half of the twentieth century, as more effective registration systems were developed state by state, the UPDB shows rates that are slightly lower than the vital statistics reports. Yet the trends remain the same.
Despite the many historical references to epidemics and catastrophic loss of young children, the "official" record indicates that infant mortality in Utah during the second half of the nineteenth century was lower than the national average. In both records, however, losses were high by today's standards. If epidemics -were responsible for heavy loss of children, our data indicate that it was essentially the diphtheria epidemics of the 1870s, 1880s, and early 1890s that either slowed down improvements in infant mortality or increased post-neonatal mortality rates. These periodic outbreaks of diphtheria also appear to account for increases in the loss of two or more children within the same family.
Post-neonatal mortality rates began to decline systematically around 1890—that is, near the time when diphtheria epidemics became less frequent, less widespread, and more responsive to methods of isolation and treatment. There is little basis in either UPDB or vital statistics to indicate that the great 1918 flu epidemic dramatically reversed the decline in infant mortality The decline in infant mortality from the late nineteenth century continuing through the immediate post-World War I period -was due almost entirely to a fall in post-neonatal deaths. Improvements in neonatal mortality did not occur until after World War I. Our data therefore suggest that, despite anecdotal evidence of their skill, the extensive network of midwives developed in the late nineteenth century had little or no impact on neonatal mortality rates.
Infant mortality rates in Utah may have been lower than the national average, and this may reflect the more rural, more -widely dispersed population. In their analysis of 1900 census data, Preston and Haines showed that, after race, the most important discriminating variable in the explanation of difference in infant mortality was location—large cities versus all other communities. 33 Utah did not have large cities, and even in the most densely settled community, Salt Lake City, population density did not approach the levels found in eastern cities.
The 1890s fall in infant mortality in Utah preceded the development of effective public health programs, including the continuous disputatious efforts to improve water supplies and establish compulsory immunization. 34 It may have been at the level of the family that health measures were adopted, reducing the risk of infant mortality This argument is consistent with Preston and Haines, who cite the following as plausible reasons for infant mortality differences in the United States in 1900.
If a major reason for the decline in infant mortality was action in the home, parents had major stimuli to adopt health measures. The common loss of a child was one stimulus. Our data indicate that more than 40 percent of women surviving in an intact marriage to age forty-nine and beginning childbearing before 1895-99 would lose at least one infant. Multiple losses began to decline earlier, among women initiating childbearing in 1875—79, but the percent of women losing two or more children in infancy did not fall below 10 percent until the turn of the century. If the loss of children motivated women to take action to reduce the risk of infant mortality, what information resources were available? 36 The Society of Health was established in Salt Lake City in 1849 to teach principles of health, although at that time the prevalent thought was much influenced by Thomsonian medicine, -which emphasized the use of herbs and plants for the treatment of illness. Later, physicians created a short-lived publication, the Salt Lake Sanitarian (1888—90), which republished articles and letters dealing -with personal and public health. 37 Nineteenth-century midwives also became advocates for simple sanitary measures. Hannah Sorensen, a physician and convert from Denmark, began teaching her hygienic and obstetrics course in 1895. The course emphasized cleanliness, knowledge, and proper diet. For childbirth Sorensen stressed strict septic measures. Her course reportedly attracted midwives from throughout the state. 38 Mid-wives may have had little impact on neonatal mortality, but they probably contributed to the decline in post-neonatal mortality as they taught principles learned in such instructional programs.
As difficult as the process of settlement and colonization was for the Utah pioneers, in terms of infant mortality the population fared better than the population in the more densely settled eastern states. According to standard measurements, Utah in the nineteenth century had lower rates of infant mortality than populations elsewhere. Nevertheless, the population endured major epidemics such as diphtheria, resulting in the loss of many children and often multiple losses. A majority of mothers escaped the loss of an infant, but more than 40 percent did lose one or more children. These frequent losses may well have provided the stimulus to adopt procedures that produced improvement in infant mortality late in the nineteenth century. As important as public health programs -would prove to be in continuing the decline of infant mortality in Utah during the first decades of the twentieth century, initial improvements predated the formal organization of public health programs, including the initial appointment of a public health officer in Salt Lake City in the 1890s and the creation of the State Board of Health in 1898 and the Division of Child Hygiene in 1907. 39 Informal community programs and the adoption of early family health actions appear to have stimulated an early decline of infant mortality.
NOTES
* Tables can be viewed below as screen shots
Lee L. Bean is professor emeritus, Department of Sociology, University of Utah. Ken R. Smith is professor, Department of Family and Consumer Studies, University of Utah Geraldine P Mineau is a research professor, Department of Oncological Sciences, and director of Population Sciences, Huntsman Cancer Institute, University of Utah Dr Mineau is also director of the Pedigree and Population Research, which has the responsibility for maintaining the Utah Population Database Alison Fraser is the database manager, Utah Population Database, Huntsman Cancer Institute Diana Lane is a program manager and nosologist, Department of Family and Consumer Studies and the Department of Population Sciences, Huntsman Cancer Institute The authors wish to thank the Pedigree and Population Research, funded by the Huntsman Cancer Foundation, for providing the data and valuable computing support The work -was supported by National Institutes of Health grant AG 12748 (Kinship and Socio-Demographic Determinants of Mortality)
1 Richard A Meckel, Save the Babies: American Public Health Reform and the Prevention of Infant Mortality, 1850-1919 (Baltimore:Johns Hopkins University Press, 1990), 1
2 Schofield and Reher report, "It was not until the latter part of the nineteenth century that mortality once again declined sharply in most areas of Europe Child mortality, and somewhat later, infant mortality were responsible for much of this decline"; Roger Schofield and David Reher, "Introduction," in The Decline of Mortality in Europe, ed Roger Schofield, David Reher, and Alain Bideau (Oxford: Clarendon Press, 1991), 1 JaquesVallin, referring to a much earlier period, provides a more telling illustration:
"In pre-industrial Europe mortality during the early stages of life, infant mortality was very high, and had a considerable effect on life expectancy at birth Thus, in France in 1740—44, the chances of dying within the first five years of fife were nearly one-half (0.474) If this mortality could have been eliminated by the touch of a magic wand, life expectancy at birth would have immediately increased by 21 years from 24.2 to 45.7 years. The principal feature of the first stage of the mortality transition, therefore, was the reduction in mortality at early stages of life."JacquesVallin,"Mortality in Europe from 1720 to 1914: LongTerm Trends and Changes in Patterns by Age and Sex," in Schofield et al., The Decline of Mortality, 49
3 For an exhaustive summary of historical estimates of levels and changes in infant and child mortality in the United States, see Samuel H Preston and Michael R Haines, Fatal Years: Child Mortality in Late Nineteenth Century America (Princeton: Princeton University Press, 1991),52—57
4 See Alain Bideau, Bertrand Desjardins, and Hector Perez Brignoli, eds., Infant and Child Mortality in the Past (Oxford: Clarendon Press, 1997),91
5 George Alter, "Infant Mortality in the United States and Canada," in Bideau et al., Infant and Child Mortality, 91.
6 The development of UPDB began in 1974 Initially the project involved the selection and data entry of family group sheets These in turn were to be linked with the computerized records of the Utah Tumor Registry consisting of diagnosed cases of cancer primarily in Utah The basic purpose was to identify the clustering of specific forms of cancers within families For a summary of the development of UPDB see Mark Skolnick,"The Utah genealogical data base:A resource for genetic epidemiology," in Banbury Report No. 4: Cancer Incidence in Defined Population, ed. J. Cairns (New York: Cold Spring Harbor Laboratory, 1980), 285-97 and Mark Skolnick, Lee L. Bean, Sue M. Dintelman, and Geraldine P. Mineau, A Computerized Family History Data Base," Sociology and Social Research 63 (Fall 1979), 601-19
7 Report of the Executive Secretary, Transactions of the American Association for Study and Prevention of Infant Mortality, 1912 (Baltimore:AASPIM, 1913), quoted in Meckel, Save the Babies, 160
8 Department of Commerce and Labor, Bureau of the Census, Mortality Statistics, 1908 (Washington, D.C: Government Printing Office, 1910), 9.The Death Registration Area had come into being before the turn of the century Therefore, some volumes of the 1900 census report mortality rates for the initial group of DRA states.
9 Salt Lake City created a vital statistics reporting system in 1895, preceding the state system by nine years The earlier establishment of the Salt Lake City system allowed the city to meet the "reasonably complete" standard earlier than the state as a whole Therefore, Salt Lake City mortality data are included in the federal DRA reports from 1905 onward. See, for example, Department of Commerce and Labor, Bureau of the Census, Special Reports: Mortality Statistics 1900 to 1904 (Washington, D.C: Government Printing Office, 1906), and Department of Commerce and Labor, Bureau of the Census, Mortality Statistics, 1908 (Washington, D.C: Government Printing Office, 1910)
10 Department of Commerce, Bureau of the Census, Birth Statistics for the Registration Area of the United States: 1915. First Annual Report (Washington, D.C: Government Printing Office, 1917); Department of Commerce, Bureau of the Census, Birth Statistics for the Registration Area of the United States: 1911 (Washington, D.C: Government Printing Office, 1917)
11 In 1910 the calculation for Utah was based on the number of children under the age of one enumerated in the 1910 census The result is quite different from the procedure that uses the number of births as the denominator Using the enumerated children under age one results in an "infant mortality rate" for Utah of 82.3, or a rate higher than the 1900 and 1920 rates. In only seven states and two cities were births accurately recorded, allowing for computation of the infant mortality rate using both procedures The differences are, in some cases, substantial The traditional computation yields a rate of 127 for Connecticut, but using the number of enumerated children under the age of one as the denominator yields a rate of 143.7 See Henry H Hibbs, Jr., Infant Mortality: Its Relation to Social and Industrial Conditions (New York: Russell Sage Foundation, 1916; reprint New York and London: Garland Publishing, 1987),4—5
12 Larry M. Logue, A Sermon in the Desert: Belief and Behavior in Early St. George, Utah (Urbana and Chicago: University of Illinois Press, 1988): 94; Dean L May, "People on the Mormon Frontier: Kanab's Families of 1874," Journal of Family History 1 (1976): 183; Katherine A Lynch, Geraldine P Mineau, and Douglas L Anderton, "Estimates of Infant Mortality on the Western Frontier: The Use of Genealogical Data," Historical Methods 18 (Fall 1985): 155-64
13 Edward A Geary, A History of Emery County (Salt Lake City: Utah State Historical Society and Emery County Commission, 1996), 151,153.
14Ardelle Hogan Mills, ed., The Knud Nelson Family from Denmark to America (Bountiful, Utah: Carr Printing Company, 1962), 239
15 Dr Ralph T Richards analyzed data from various sources, including hospitals, cemeteries, and the Salt Lake City Board of Health to estimate the numbers of deaths from various types of diseases in Salt Lake City Records from the Salt Lake City and Mt Olivet cemeteries between 1848 and 1894 indicate the burials of 2,715 children under age two for which the recorded cause of death was diarrheal disease From 1895 to 1948 there were 1,550 deaths from diarrheal diseases recorded by the Salt Lake City Board of Health Dr Richards's examination of city cemetery books finds 1,240 deaths between 1863 and 1894 attributed to diphtheria, with especially heavy concentrations in 1878, 1879, 1880, and 1891 See Ralph T Richards, Of Medicine, Hospitals, and Doctors (Salt Lake City: University of Utah Press, 1953).
16The 1918 flu epidemic had an age-related mortality pattern different from any other influenza epidemic Recent studies report that in contrast to the traditional "U" shaped curve with high mortality among the young and old, the 1918 flu epidemic followed a "W" curve with especially high levels of mortality among young adults and especially males; see Gina B Kolata, The Story of the Great Influenza Pandemic of 1918 and the Search for the Virus that Caused It (New York: Farrar, Straus, and Giroux, 1999); Andrew Noymer and Michel Garenne, "The 1918 Influenza Epidemic's Effects on Sex Differentials in Mortality in the United States," Population and Development Review 26 (September 2000): 565—81 Referring to a family history, Lyman and Newell quote in reference to the flu,'"Most of those who have fallen victim have been big, hearty men, with the best part of life ahead of them'"; Edward Leo Lyman and Linda King Newell, A History of Millard County (Salt Lake City: Utah Historical Society and Millard County Commission, 1991), 253
17 Geary, A History of Emery County, 153.
18 Claire Noall,"Mormon Midwives," Utah Historical Quarterly 10 (1942): 125
19 Ibid., 109
20 Lynch et al.,"Estimates of Infant Mortality."
21 See, for instance, Lee L Bean, Geraldine P Mineau, and Douglas L Anderton, Fertility Change on the American Frontier (Berkeley: University of California Press, 1990) The selection involved a review of all family group sheets in the "Patron" section in 1975-76 Additional sheets were added following a review of the "Main" section in 1978-79
22 Ibid., 109-138
23 Douglas L Anderton and Lee L Bean, "Birth Spacing and Fertility Limitation: a Behavioral Analysis of a Nineteenth Century Frontier Population," Demography 22 (May 1985): 169-83
24 Lee L. Bean, Geraldine P.Mineau, and Ken R. Smith, "The Effect of Pioneer Life on the Longevity of Married Couples," in Nearly Everything Imaginable: The Everyday Life of Utah's Mormon Pioneers, ed Ronald Walker and Doris Dant (Provo:BrighamYoung University Press, 1999), 386-403
25 Geraldine P.Mineau, Lee L. Bean, and Douglas L.Anderton, "Description and Evaluation of Linkage of the 1880 Census to Family Genealogies: Implications for Utah Fertility Research," Historical Methods 22 (1989): 144-57
26 Most demographic analysis of UPDB has focused on fertility change The recent addition and linkage of the death certificates to the genealogies provide new opportunities to study mortality in Utah. See, for example, Ken R Smith and Geraldine P Mineau, "Effects of Childbearing Patterns on Parental Mortality for Marriages during 1860-1919," paper presented at the 1996 annual meetings of the Population Association of America; and Geraldine P Mineau, Ken R Smith, and Lee L Bean, "Historical Trends of Survival amongWidows and Widowers," Social Science and Medicine, 54 (2002): 245-54
27 Morrell notes, "Diseases were relatively rare in the early days of the settlement because the country was uncontaminated Refuse had not had time to accumulate As time went on and contamination increased, the population also become more dense, disease became more prevalent"; Joseph R Morrell, Utah's Health andYou:A History of Utah's Public Health (Salt Lake City: Deseret Book Company, 1956), 32
28 Richards believed that while early migrants may have been infected with diphtheria, the disease ran its course over the time it took to migrate from the Midwest to Utah The surviving migrants were thus "disease-free." Consequently the first death attributed to diphtheria among the Salt Lake City Cemetery burials was not recorded until 1863; see Richards, Of Medicine, Hospitals, and Doctors, 151
29 In our judgment the UPDB is more likely to reflect the actual level of infant mortality The census procedure of sending retrospective questions and questionnaires to medical practitioners—with a low response rate—appears to yield incomplete counts Questions regarding the accuracy of the census have a long history.
30 Bean, Mineau, and Anderton, Fertility Change on the American Frontier, 125—32
31 In 1918 only 5.1 percent of the 926 deaths of children under the age of one was attributed to flu. In the age group twenty to twenty-nine, 49 percent of the 955 deaths were due to flu, and in the age group thirty to thirty-nine, 45 percent of the 892 deaths were due to flu; Department of Commerce, Bureau of the Census, Mortality Statistics, 1918 (Washington, D.C : Government Printing Office, 1920),Table 8, 411
32 There is a possible two-way causal relationship between the number of children born and infant deaths On the one hand there is evidence of a greater risk of infant loss at very high parities (number of births), yet women also may be motivated to "replace" a child who dies
33 Preston and Haines, Fatal Years, 97—102
34 Morrell, Utah's Health and You, 45-46, 100-101
35 Preston and Haines, FatalYears, 209
36 Preston and Haines argue that "lack of know-how rather than lack of resources was principally responsible for foreshortening life in the United States in the 1890s"; ibid., 209
37Morrell, Utah's Health andYou, 49
38 Miriam B. Murphy, A History of Wayne County (Salt Lake City: Utah State Historical Society and Wayne County Commission,
39Morrell, Utah's Health andYou, 78, 92-93.