4 minute read
Partnering with rural communities to prioritise population research


Over four decades of apartheid rule (1948 – 1990), South African Bantustans endured systemic, racist inequalities that resulted in ‘homelands’ for black South Africans that were least-resourced, received separate and inferior services, and lacked formal records of births and deaths.
From 1982, staff of Wits University’s Health Systems Development Unit (HSDU) were working in Gazankulu in the rural northeast of South Africa adjacent to the Kruger National Park and close to the border with Mozambique – their base was Tintswalo Hospital in Bushbuckridge, now a rural sub-district. In the early 1990s, anticipating approaching democratic change and deeply aware of the deficiencies in rural health services in the context of broader rural realities, the staff of the HSDU re-focused their approach to rural health systems development. They quickly learned that there was no reliable population information on which to base rational decision-making. Using first-hand experience of health and demographic surveillance systems (HDSS) visited in Bangladesh and Senegal, Steve Tollman and team set out to establish one in Agincourt, a remote area of Bushbuckridge far from tar roads and other infrastructure, save for a network of clinics and a community health centre. This would serve as a demonstration area in which to co-develop and model functioning district and sub-district health systems to inform district, provincial and national policy-makers. The undertaking began, in 1992, with producing Agincourt’s first maps (which were hand-drawn) and taking a baseline census of 20 villages – enumerating 58,000 people, including 15,000 Mozambican refugees displaced by the civil war. Over the ensuing years, the annual census, which tracks vital events (births, deaths and migrations) and indicators of socio-economic status amongst others, demonstrated rapid and profound health, population and social transitions. These were driven in large part by the devastating impact of the HIV/AIDS epidemic and impressive albeit late introduction of PMTCT and antiretroviral therapy – and alongside the predominance of HIV/AIDS, emerging noncommunicable diseases. By the late 1990s, work transitioned from designing and testing decentralised health systems to a populationbased research platform conducting work relevant to other transitioning rural communities in south and subSaharan Africa. By expanding its infrastructure, the Agincourt HDSS was able to “nest” studies along the life course, probe questions arising from the observed health and social transitions, establish cohorts, and trial interventions. In 2004, the Agincourt Health and Population Unit was officially recognised as a SAMRC and Wits University research unit, becoming the MRC/ Wits Rural Public Health and Health Transitions Research Unit (Agincourt). The surveillance area now includes 31 villages and some 120,000 people in 20,000 households From March 2020, the Unit’s longitudinal data platform and infrastructure (specifically an extended call centre) enabled a rapid response to the urgent challenges posed by the COVID-19 pandemic, repurposing existing studies and tackling new questions to serve the national response and contribute the rural component – often otherwise missing – to the national picture. Together with partners, the Unit’s COVID-19 response within the first few months included: health systems R&D; analyses of existing HDSS and other data to provide evidence for decision-making;
Advertisement
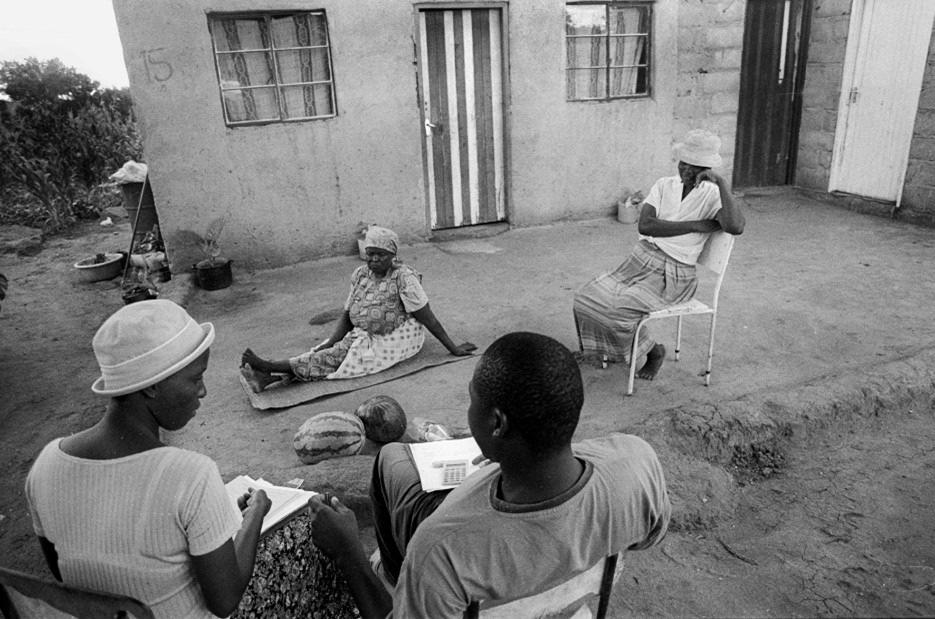
Figure 1. Fieldworkers collecting data for census. Photo by Paul Weinberg.

epidemiology on community burden and transmission dynamics of SARS-CoV-2 in a rural setting (with NICD); and social, behavioural and economic impacts during and post-lockdown to guide local and provincial programmes and national policy. Linkage of the population platform to clinic and hospital records enabled the introduction of “dashboards” as a basis for decision-making and resource deployment by clinical and service leadership. On the global front, the Agincourt Research Unit is leading a multinational Excess Mortality initiative to characterise all-cause and cause-specific mortality during COVID-19 times (using verbal autopsy data) in low- and middle-income settings. The initiative, funded by the Bill and Melinda Gates Foundation, capitalises on several population research networks namely, CHAMPS; ICDDR,B; INDEPTH; INSPIRE; and SAPRIN and involves 19 urban and rural population research platforms in East, West and Southern Africa, and South Asia. Leadership of the Agincourt Research Unit has been forward-thinking, having played a leading role in the establishment of the International Network for the Demographic Evaluation of Populations and Their Health (INDEPTH); supported the establishment of DIMAMO a rural HDSS linked to the University of Limpopo; and participated centrally in establishing the South African Population Research Infrastructure Network (SAPRIN). 2022 marks 30 years of the MRC/Wits-Agincourt Research Unit making it one of the longest running research centres of its kind in sub-Saharan Africa. The work is supported by close participation of the community and local government, dedicated staff, and a rich network of local and global partnerships and collaborations. The Agincourt Research Unit has been resilient to pressures and adaptable to change. The rapid and complex transitions experienced by our rural communities means that the Agincourt longitudinal research platform gains in value with increasing time, with the nested studies benefiting greatly from what it has to offer.


Figure 2. Access to potable water remains a priority issue impacting health and socioeconomic development. Photo by Jackie Roseleur.
Figure 3. Merga Agaa, Cho Kabudula (Agincourt Research Unit), and Gezahegn Negassa collaborating to clean and harmonize Kersa HDSS's dataset at an in-person data harmonisation workshop for the Excess Mortality initiative at Wits University in March 2022.




