19 minute read
The Effect of Education and Other Socioeconomic Factors on Smoking Status in Western Australia


Walter Chukwunonso Ikealumba PhD CHE, BEng ME (Hons), MIEAust, MIIMarEST walter.ikealumba@oum.edu.au
Abstract
Advertisement
Thehealth and economic consequences of tobacco use are drastic, with life expectancy of smokers reduced by 15 years due to tobacco-related illnesses. Few studies have addressed the effects of education and socioeconomic factors on smoking status in the Australian population. Thus, the aim of this study, is to examine the association between education and other socioeconomic factors with smoking status among Western Australian residents. In addition, the study will also examine if smoking within the Western Australian population fits the current global smoking epidemic.
The study consisted of a sample size of 78 participants. A questionnaire was utilized to collect information on demographics, why individuals smoke/started smoking, and why individuals quit smoking.
The results showed that prevalence of smoking was highest within 40 – 49 age group and lowest within the 50+ age group. The results also showed that as education levels increased, the total number of smokers decreased; in addition, the percentage of heavy smokers also decreased. The primary reason participants began smoking was peer pressure; and continue smoking because of stress. For those that did quit smoking, to avoid future health conditions, was the decisive factor.
This study showed that the age-related smoking status from a sample in Western Australia fits the global smoking epidemic trend. This study also illustrated the well-documented inverse association between education and smoking. Given the effect of peer pressure, stress and health concerns on smoking hab- its, preventative and cessation strategies should be aimed at subgroups; with the most crucial subgroup being young adolescents.
Introduction
Globally, 19.2% of adults are smokers with men at 32.7% and women at 5.8%. [1] Overall, there are more than one billion smokers in the world. [1] The health consequences of tobacco use are drastic. The life expectancy of smokers is reduced by 15 years due to tobacco-related illnesses. [2] Tobacco-use kills more than 8 million people per year and more than half of all lifetime users. [2] In Australia, the trend is slightly favourable with only 11.6% of adults being smokers, men at 12.8% and women at 10.4%. [3] However smoking is still the leading cause of preventable disease in Australia; and is linked to numerous diseases, which place a national financial burden of $136.9 billion. [4]
The global smoking paradigm can be broken into four stages. The first stage, 1900 – 1920, is when smoking was first introduced among men, especially those of a higher socioeconomic status, but was not very common among women. In the second stage, 1920 – 1950, smoking became a widespread middle class and working-class habit; as a result, smoking increased sharply with both men and women smoking. In the third stage, 1950 – 1980, smoking reached its peak, and slowly began to decline especially among those of high socioeconomic status. In the last stage, 1980 – 2000s, smoking declined to approximately 20%. [5]
Even though the global trend of smoking is on the decline, the impact it has on health and the economic system is still significant, which warrants the need to understand what causes people to smoke. Education is a social determinant of health, [6] and higher education has been linked with better mental health, longer life expectancy and better health related behaviour. [7] The knowledge of smoking and its risks is associated with education. [8] There is a strong inverse association between socioeconomic position, including education, and smoking. [9] Smoking is higher in groups with less education. [7,10] Other studies focused directly on the cognitive ability of individuals; those with low cognitive ability are more likely to take up smoking and less likely to quit, compared to those with higher childhood cognitive ability. [11] Interestingly, some studies pointed toward smoking as a coping strategy for poor educational performances and stress. [7,12] There is a clear inverse relationship between the level of education and smoking status and it is not surprising that within the global declining trend of smoking, this decline was noted more in those of higher education status. [10,13]
Even though numerous research point towards the link between low educational attainment and increased chances of smoking; some studies have concluded that low educational attainment not only increases the chances of smoking, but that smoking, can ultimately affect education status. [12,14] Its important to point out that education can be associated with whether individuals started smoking, but not whether they continued smoking. [11] This will be a crucial factor when targeting smoking cessation education and campaigns.
The socioeconomic position in young adolescent and early adulthood is the most important factors for determining the impact smoking will have on an individual’s life. [15] Initiation of smoking at this critical age group is associated with a large spectrum of personal and social disadvantage, with education being one of those disadvantages. [16] Smoking in this age group not only decreases the likelihood of enrolling into further education [12] but increases the likelihood of heavy smoking as the person ages. [7
Addressing smoking behaviours, therefore, should be focused on subgroups, [9] with prevention strategies aiming to reach young children during adolescence and continue to reinforce this into adulthood. [17] Smoking cessation, reduces mortality and doing so earlier in life, is associated with significant reductions in mortality. [18] However, it is important to determine why individuals continue smoking in the first place; studies have shown that they only stopped when there was a crucial reason or when they saw alternative ways of living. [19] other socioeconomic factors are identified. This will enable us to target at risk groups more accurately with correct preventative and cessation measures. Thus, the aim of this study, is to primarily examine the association between education and other socioeconomic factors with smoking status among Western Australian residents. In addition, the study will also examine if smoking within the Western Australian population fits the current global smoking levels.
Method
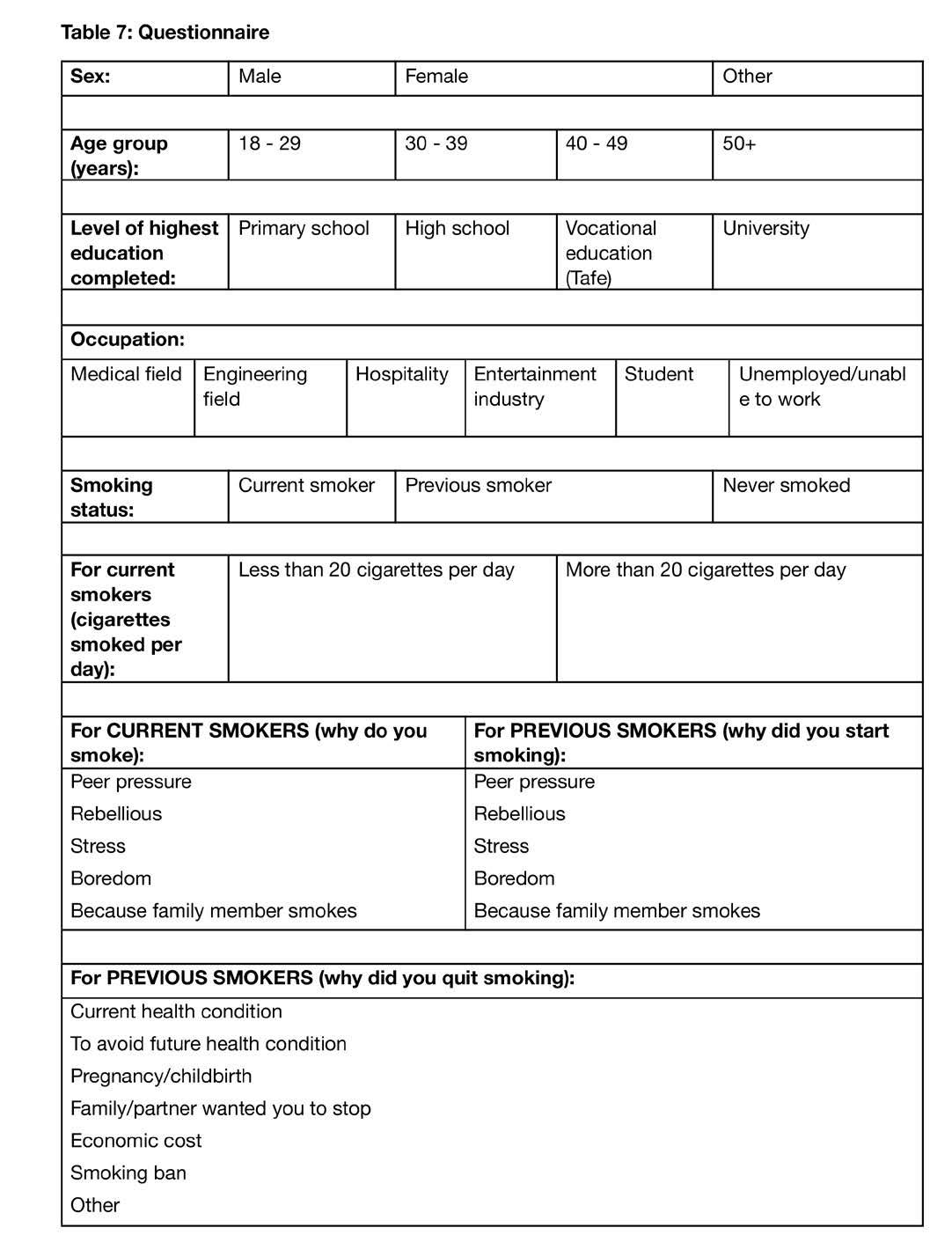
Thisis a preliminary study with a sample size of 78. Data was collected over a period of approximately 3 months starting from 21/09/2021, from Palm Springs Pharmacy using a questionnaire, with an age group of 18 years and above. The questionnaire collected information on sex, age, level of education attained, occupation, smoking status, why individuals smoke/started smoking, [20] and why individuals quit smoking. [21]
Age group brackets were distributed occupation, medical, engineering, hospitality, entertainment, student, unemployed/unable to work. The occupation options utilised in this study were selected to be all-encompassing of major industries, for example medial could include doctor, nurse, dentist, optometrist, pharmacy, and even receptionist within those establishments etc; engineering could include, engineers, mine workers, draftsmen, technicians, machinists etc; hospitality could include those in retail, restaurants etc; entertainment could include, musicians, actors and actresses, singers, night clubs, acrobats etc; students are those that are currently studying and not working; while unemployed/unable to work are those without any form of employment. There were three smoking status options either current smoker, previous smoker or never smoked. For current and previous smokers, reasons for starting smoking was analysed and includes some of the most common reasons people pick up smoking; [20] peer pressure, rebellious, stress, boredom or because family member smokes. For previous smokers, reasons for quitting was investigated and includes some of the most common reasons people quit smoking; [21] current health condition, to avoid future health condition, pregnancy related, family/ partner wanted you to stop, economic cost, smoking ban or other.
Informed consent was obtained from the participants and anonymity was guaranteed. IRB approval was requested and approved by Oceania University of Medicine. Budget – There was a gift card given to the random participants of the survey.
Once data collection was completed, all analysis was conducted via Excel. Firstly, the prevalence of smoking within each age group will be analysed, which will assist in determining if smoking status among Western Australian residents fit the global smoking epidemic. Other demographic analysis such as comparing the incidence of smoking between different genders will also be conducted.
The effect of education on smoking will be investigated in addition to the occupation of the participants. It is important to determine the effect of occupation on smoking status, as there is a strong positive relationship between education and occupation. Those who smoke more than 20 cigarettes a day are considered heavy smokers and tend to have a shorter life expectancy. Therefore, it will be useful to identify the percentage of current smokers that fall into this category and the educational level of these smokers.
Finally, the analysis will be used to investigate the primary reasons underlying smoking, the continuation of smoking, and the cessation of smoking.
Statistical analysis – Not indicted for the proposed study.
Sample of the questionnaire is provided in the Table 7.
Results
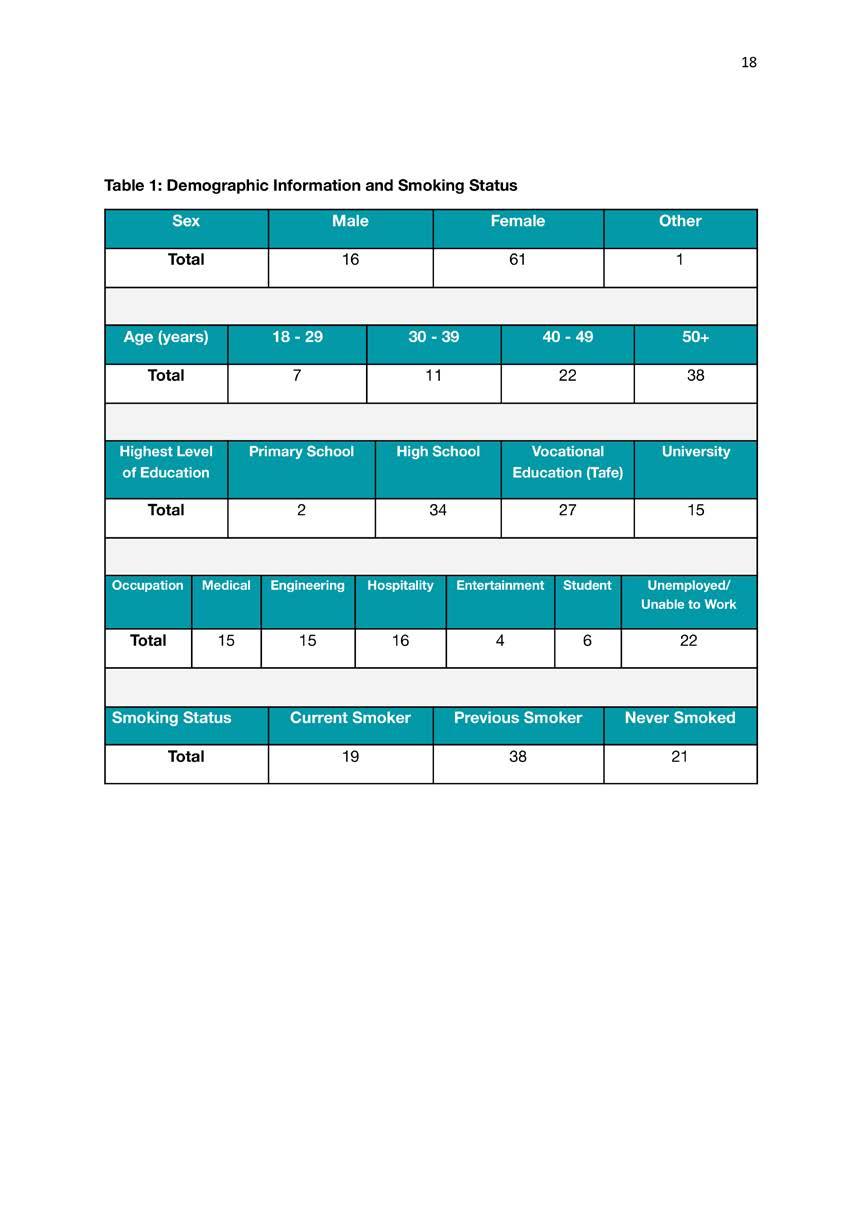
Table 1 summaries demographic characteristics of the study sample. Of the 78 participants, over 78% were female and approximately 77% were older than 40 years old. The highest level of education attained by participants was mainly high school, making up 43.6% of sample size, closely followed by vocational training at 34.6%. Unemployed/unable to work was the most frequent occupation, making up 28.2% of the sample size, however this was mainly due to a large portion of the participants being retired. Occupation across the medical, engineering and hospitality fields were relatively evenly distributed, at approximately 15%. Regarding smoking status of participants, approximately 48% were previous smokers, while current smokers and those who

Table 2 summaries information pertaining to current smokers. Of the 19 current smokers, 11 smoked less than 20 cigarettes per day, while eight were heavy smokers, smoking more than 20 cigarettes per day. Of these current smokers, 79% selected stress as the primary reason for smoking; while other reasons such as peer pressure, rebellious and boredom only make up small percentages. Whether a family member smokes, was not a reason for any of the current smokers to continue smoking.
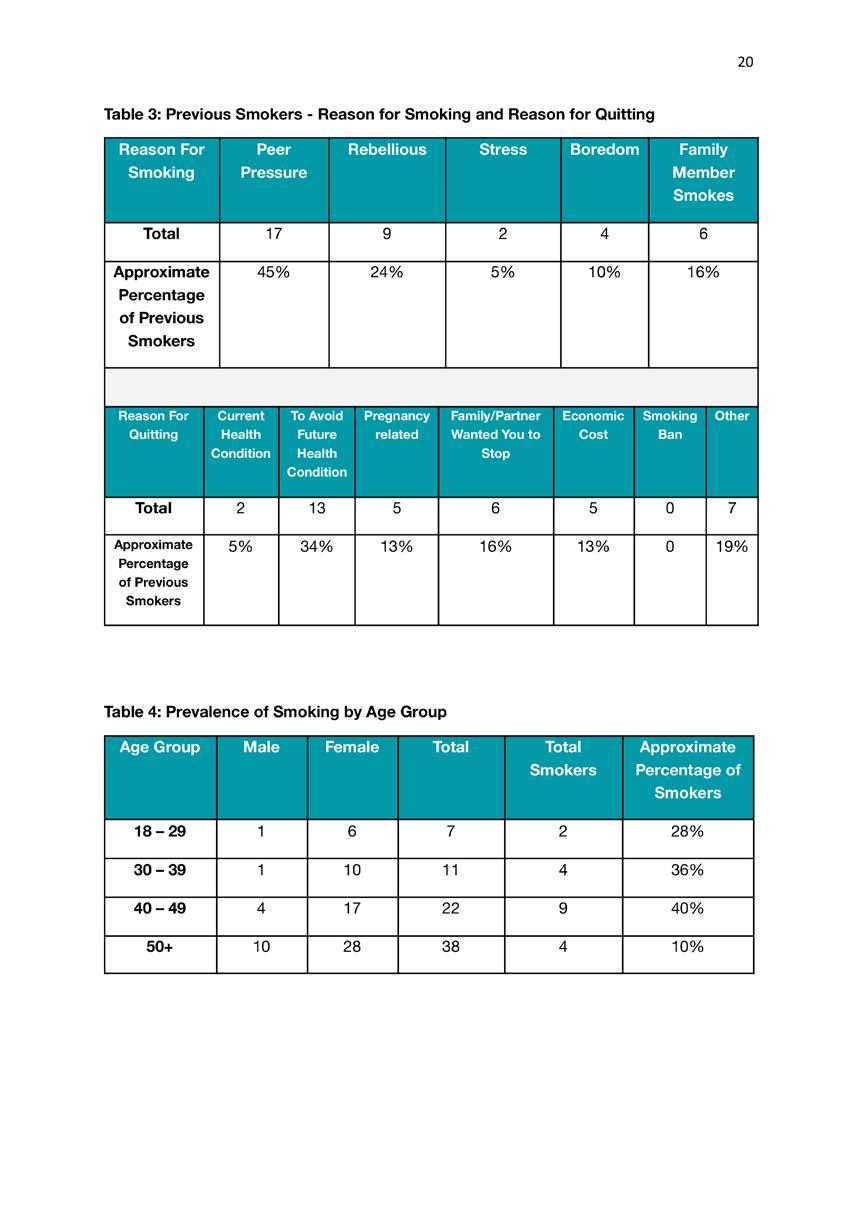
Table 3 summarises information concerning previous smokers. Of the 38 previous smokers, 45% had peer pressure as the predominant reason why they started smoking, followed by being rebellious at 24%. Interesting, 16% of previous smokers started smoking because family members smoke, showing the effect that family members can have on individuals picking up smoking. Stress, at 5%, was the least reason why previous smokers started smoking, which possibly points to stress not being the main reason people start smoking. While the main reason for quitting was to avoid future health condition, followed by the family member wanting the individual to quit. This shows the effect that health education and family members can have on individuals achieving their smoking cessation goals. Current health condition was the least reason, at 5%, why previous smokers quit smoking, which is thought-provok-
Table 4, was highest within the 40 – 49 age group. The percentage of smokers in this age group was 40%. The frequency of smoking was lowest in the 50+ age group, at 10%. The data shows that as age group increases, the prevalence of smoking increases up to the 40 – 49 age group, where it peaked and then started to decrease. Participants within the age groups of 18 – 29 are believed to be underrepresented, making up approximately 9% of the total sample size.
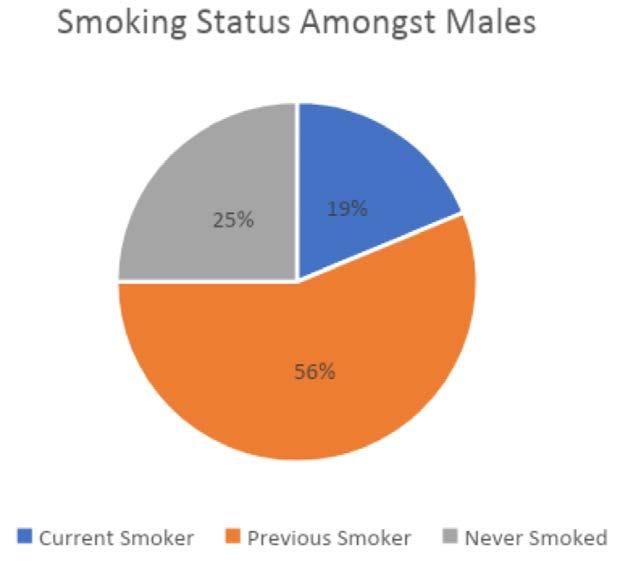
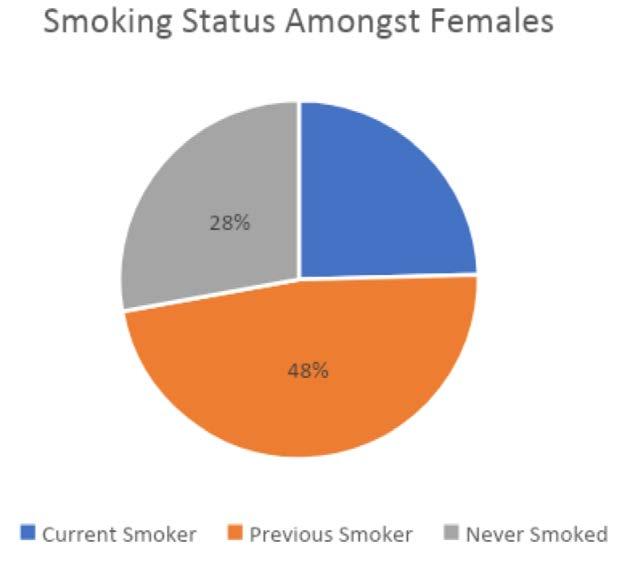
Figure 1 and Figure 2, show the smoking status of females and males respectively. The frequency of current smokers is higher in females compared to males, at 25% and 19% respectively. It’s interesting to note that in both genders approximately 50%, Figure 1 and Figure 2, are previous smokers. Whereas those who have never smoked is at approximately 25%.
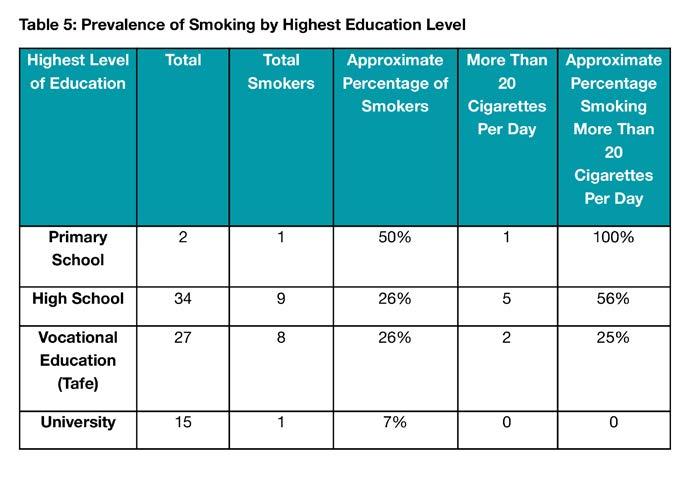
The prevalence of smoking, stratified against the highest level of education attained is presented in Table 5. Of those that completed university studies only 7% were smokers, compared to 26% amongst those that only completed high school or vocational education. For those that stopped schooling after primary school, the sample size of two participants, is believed to be insufficient, to accurately represent the predominance of smoking within this group. The percentage of heavy smokers was highest, at 56%, for those that only completed high school; 25% for those that completed vocation training and 0% for those that completed university.
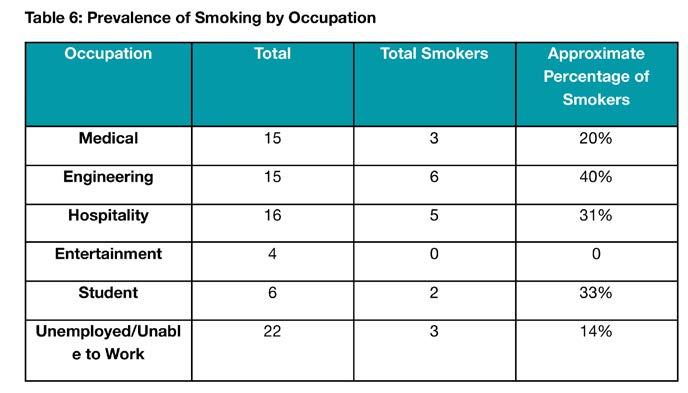
The prevalence of smoking by occupation is presented in Table 6. Participants unemployed or unable to work had the lowest rate of smoking, closely followed by those in the medical field, at 14% and 20% respectively. Engineering had the highest percentage of smokers, followed by those in the hospitality industry, 40% and 31% respectively. The sample size of students, including those in the entertainment industrial, as shown in Table 6, is believed to be insufficient, to accurately represent the smoking status within these groups.
Discussion
he prevalence of smoking, as seen in Table 4, was highest within the 40 –49 age group. The percentage of smokers in this age group was 40%. This finding fits the global smoking epidemic, as the in dividuals in the 40 – 49 age group would have been born around 1950 – 1980 when smoking reached its peak [5,22] and therefore could easily have picked up smoking compared to other age groups. The frequency of smoking was lowest in the 50+ age group, at 10%, Table 4. The lower prevalence of smoking in the 50+ age group, is perhaps due to increasing health concerns within this group due to their age. Cigarette smoking has declined significantly in most countries due to the awareness of the negative health impacts associated with smoking, including the implementation of smoke-free areas. This would have contributed to the decline of smoking also seen in this study as those in the 30 – 39 and 18 – 29 age groups showed reduced prevalence of smoking.
As presented in Table 1, of the 78 participants, 61 were females and only 16 were males. Globally and in Austra lia, the prevalent of smoking is highest amongst the male gender. [1,3] This was also illustrated in the global smoking ep idemic with men picking up smoking as a habit before females eventually started smoking; and percentage of male smokers always remained higher than that of fe males. [5,22] However, the results in this study opposed this finding, by showing that the frequency of smoking is high er in females compared to males, at 25% and 19% respectively, Figure 1 and Figure 2. This perhaps could be attributed to the disparity between the sample size of females to males. It’s interesting to note that in both genders approximately 50%, Figure 1 and Figure 2, are previous smok ers. We know that as individuals age, the likelihood to quit smoking due to health concerns increases; as is indicated in Ta ble 3, with ‘to avoid future health con ditions’ as the dominant reason. This correlates well with the age groups in this study, as majority of the male and female sample are in the 50+ age group, as shown in Table 4.
The strong inverse association between education and smoking is well-documented. [7,9-11,23] This association is also well represented in this study, as shown in Table 5. Higher educational attainment, resulted in reduced number of total smokers; with approximately 7% smokers amongst those that completed university level education, compared to rates in those with lower education levels. Several studies have also pointed towards less favourable psychosocial conditions in those with lower education, such as poor coping resources, lack of opportunities for alternative leisure, or elevated levels of socio-emotional distress. [12,25,26] Not only would these less favourable psychosocial conditions contribute to the higher smoking rates seen in those with lower educational levels, but it would also contribute to the lack of further educational attainment in these individuals. ly. However, a previous study pointed towards unemployment being a significant risk factor for smoking. [27] This opposes the results in our current study; however the results in this study were expected findings, as approximately 64% of the unemployed or unable to work, are individuals in the 50+ age bracket. As previously mentioned, the increasing health concerns within this age bracket results in a decreased percentage of smokers. As for those in the medical field, it is believed that their higher education levels, including their medical awareness of tobacco-related illnesses is the major deterrent to smoking. Interestingly, those within the engineering had the highest percentage of smokers, followed by those in the hospitality industry, 40% and 31% respectively. Stress seemed to be the major driver of smoking within the engineering and hospitality fields. Over 80% of smokers in the engineering field selected stress as the primary reason for smoking. This points towards the possibility that an occupation within the engineering field in Western Australia is stressful and/or other environmental factors contribute to making this occupation stressful. Overall, these results were consistent with a previous studies showing that those within hospitality, construction and mining had the highest rate of smoking; while those in medical and educational services had lower rates of smoking. [28] Also, despite the fact that engineering and hospitality have very educated professionals, they are obviously not as deeply informed about health issues as their medical counterparts. So these two professions, have the strange combination of factors where they can afford smoking and they are not as educated in their health as those in the medical profession. With those combinations they can smoke more than their medical profession counterparts.
Individuals that smoked more than 20 cigarettes per day are classified as heavy smokers, whereas those that smoked less than 20 cigarettes per day are classified as light smokers. As depicted in Table 2, 42% of the total smokers, a significant proportion, are heavy smokers. These individuals are at increased risk of tobacco-related illness and tend to have shorter life expectancy. The percentage of heavy smokers was less than that of light smok- ers, 42% and 58% respectively; and was anticipated because the global decreasing trend of smoking was likely to result in a decreased amount of smoking overall. By stratifying for educational attainment amongst the heavy smokers, Table 5, with increasing educational levels, from high school, vocational training (tafe) to university, the percentage of heavy smokers decreases, 56%, 25% and 0% respectively; again, supporting the strong inverse association between education and smoking status.
Why individuals started smoking, why some still smoke, and why others quit will help us understand smoking habits within the Western Australia population. The primary reason individuals started smoking, Table 3, was shown to be peer pressure. Peer pressure is commonplace within the younger population and therefore smoking prevention strategies should be aiming to reach young children during adolescence. For those that do take up smoking, some quit along the way. To avoid future health conditions was the primary reason participants quit smoking and was an expected finding supported by previous studies. [29] We know that as individuals age, the likelihood to quit smoking due to health concerns increases and this correlates well with the age groups in this study, as majority of the sample is 40 years and older. Perhaps devising more effective strategies to educate the population about the future health related risk of smoking could help reduce the number of smokers. There were other reasons for quitting, family/partner wanting them to stop was another a common finding and demonstrates the power that family members have in supporting and guiding an individual through the process of quitting smoking. For those that continued smoking, Table 2, stress was the dominant factor making up 79% of the sample size. This was an expected result; the general stresses of life and occupation can keep individuals smoking; even students continue smoking due to poor educational performance and the surrounding stresses. Therefore, smoking preventative and cessation strategies should also find methods to educate people about stress and other coping methods for managing stress. This supports the finds in a previous study, showing the positive effect anger and stress coping skills have on smoking cessation. [30]
Limitations/Constraints
There were some limitations in this study including, 1) A prize was awarded for participation and therefore there is a chance that participants would falsify information, only to enter the prize draw; 2) The survey was both conducted online and via hardcopy, participants were given the privilege of completing the survey by themselves, there is no guarantee that information provided would be accurate; 3) The male population of Western Australia was underrepresented in this survey only making up about 20% of the total sample size; 4) Participants within the age groups of 18 – 29 were also underrepresented, making up approximately 9% of the total sample size; 5) The sample size of 78 was believed to be suitable for a preliminary study; however it did not allow for accurate representation of certain sub-groups within the study, such as those in the 18 – 29 age group, those with occupation of student or in the entertainment industry and those that stopped schooling after primary school.
Conclusion
The major strength of this study is, it is likely the first study investigating the effects of education and other socioeconomic factors on smoking status, conducted in Western Australia. In conclusion, the prevalence of smoking from a Western Australia sample, was highest within 40 – 49 age group, lowest within the 50+ age group, and fits the trend described in the global smoking epidemic. The results of this study, shows that smoking is higher in females compared to males, which did not fit the global trend. However, this could be attributed to the smaller sample size of males in this study. This study also illustrated the well-documented inverse association between education and smoking. As education level increased the total number of smokers decreased; in addition, the percentage of heavy smokers also decreased. Participants unemployed or unable to work had the lowest rate of smoking. The primary reason participants began smoking was because of peer pressure; and continue smoking because of stress. For those that did quit smoking, to avoid futter health conditions, was the decisive factor. Based on these findings, preventative strategies should be aimed at subgroups, with one crucial group being young adolescents. These strategies should not only educate all subgroups about the health consequences of tobacco use, but it should also encourage further general education especially within the younger population. Future studies should investigate the most effective smoking preventative and smoking cessation strategies; and consider using a larger sample size.
Acknowledgements
The author is grateful for David D’orazio from Palm Springs Pharmacy, Warnbro, Western Australia for providing access to their client database, through which the research questionnaire was distributed.
References
1. Organization WH: WHO Report on the Global Tobacco Epidemic, 2019: Offer help to quit tobacco use. 2019:209.
2. Tobacco Fact Sheet. (2020). Accessed: 5 May, 2021:https://www.who.int/newsroom/fact-sheets/detail/tobacco.
3. Tobacco smoking. (2020). Accessed: https://www.aihw.gov.au/reports/australias-health/tobacco-smoking.
4. Whetton S, Tait RJ, Scollo M, et al.: Identifying the social costs of tobacco use to Australia in 2015/16. Edited by Institute NDR, Sciences FoH, University C. Perth: National Drug Research Institute, Faculty of Health Sciences, Curtin University; 2019.
5. Lopez AD, Collishaw NE, Piha T: A descriptive model of the cigarette epidemic in developed countries. Tob Control. 1994, 3:242-247.
6. Braveman P, Gottlieb L: The social determinants of health: it's time to consider the causes of the causes. Public Health Rep. 2014, 129 Suppl 2:19-31. 10.1177/00333549141291S206
7. Setter C, Peter R, Siegrist J, Hort W: Impact of school and vocational education on smoking behaviour: results from a large-scale study on adolescents and young adults in Germany. Soz Praventivmed. 1998, 43:133-140. 10.1007/ bf01359721
8. Nishi N, Ogurii S, Onoda T, Nohara M, Inoue H, Okayama A: Knowledge of smoking-related risks and opinions on tobacco control by smoking status and education level in Japan. Nihon Koshu Eisei
Zasshi. 2005, 52:962-970.
9. Vedøy TF: The role of education for current, former and never-smoking among non-western immigrants in Norway. Does the pattern fit the model of the cigarette epidemic? Ethn Health. 2013, 18:190210. 10.1080/13557858.2012.700917
10. Hoebel J, Kuntz B, Kroll LE, et al.: Trends in Absolute and Relative Educational Inequalities in Adult Smoking Since the Early 2000s: The Case of Germany. Nicotine Tob Res. 2018, 20:295302. 10.1093/ntr/ntx087
11. Fawns-Ritchie C, Starr JM, Deary IJ: Health literacy, cognitive ability and smoking: a cross-sectional analysis of the English Longitudinal Study of Ageing. BMJ Open. 2018, 8:e023929. 10.1136/ bmjopen-2018-023929
12. Sabado MD, Haynie D, Gilman SE, Simons-Morton B, Choi K: High school cigarette smoking and post-secondary education enrollment: Longitudinal findings from the NEXT Generation Health Study. Prev Med. 2017, 105:250-256. 10.1016/j.ypmed.2017.09.025
13. de Graaf A, van den Putte B, Zebregs S, Lammers J, Neijens P: Smoking Education for Low-Educated Adolescents: Comparing Print and Audiovisual Messages. Health Promot Pract. 2016, 17:853861. 10.1177/1524839916660525
14. Latvala A, Rose RJ, Pulkkinen L, Dick DM, Korhonen T, Kaprio J: Drinking, smoking, and educational achievement: cross-lagged associations from adolescence to adulthood. Drug Alcohol Depend. 2014, 137:106-113. 10.1016/j.drugalcdep.2014.01.016
15. Tian J, Gall S, Patterson K, et al.: Socioeconomic position over the life course from childhood and smoking status in mid-adulthood: results from a 25-year follow-up study. BMC Public Health. 2019, 19:169. 10.1186/s12889-019-6483-0
16. Conwell LS, O'Callaghan MJ, Andersen MJ, Bor W, Najman JM, Williams GM: Early adolescent smoking and a web of personal and social disadvantage. J Paediatr Child Health. 2003, 39:580-585. 10.1046/j.1440-1754.2003.00240.x
17. Heris CL, Eades SJ, Lyons L, Chamberlain C, Thomas DP: Changes in the age young Aboriginal and Torres Strait Islander people start smoking, 20022015. Public Health Res Pract. 2020, 30. 10.17061/phrp29121906
18. Banks E, Joshy G, Weber MF, et al.: Tobacco smoking and all-cause mortality in a large Australian cohort study: findings from a mature epidemic with current low smoking prevalence. BMC Med. 2015, 13:38. 10.1186/s12916-015-0281-z
19. Wyndow P, Clifton E, Walker R: Improving Aboriginal Maternal Health by Strengthening Connection to Culture, Family and Community. Int J Environ Res Public Health. 2020, 17. 10.3390/ ijerph17249461
20. Folan P, Spatarella A, Jacobsen D, Farber HJ: Why Do I Smoke and Why Do I Keep Smoking? Am J Respir Crit Care Med. 2017, 196:P7-p8. 10.1164/rccm.1964P7
21. Gallus S, Muttarak R, Franchi M, et al.: Why do smokers quit? Eur J Cancer Prev. 2013, 22:96-101. 10.1097/CEJ.0b013e3283552da8
22. Ferrence RG: Deadly fashion : the rise and fall of cigarette smoking in North America / Roberta G. Ferrence. Garland, New York; 1989.
23. Schaap MM, Kunst AE, Leinsalu M, et al.: Female ever-smoking, education, emancipation and economic development in 19 European countries. Soc Sci Med. 2009, 68:1271-1278. 10.1016/j. socscimed.2009.01.007
24. Maralani V: Understanding the links between education and smoking. Soc Sci Res. 2014, 48:20-34. 10.1016/j.ssresearch.2014.05.007
25. McGee R, Williams S, Nada-Raja S, Olsson CA: Tobacco smoking in adolescence predicts maladaptive coping styles in adulthood. Nicotine Tob Res. 2013, 15:1971-1977. 10.1093/ntr/ntt081
26. Suhrcke M, Nieves CdP: The impact of health and health behaviours on educational outcomes in high-income countries: a review of the evidence. Edited by World Health Organization ROfE. 2011.
27. Jung Y, Oh J, Huh S, Kawachi I: The effects of employment conditions on smoking status and smoking intensity: the analysis of Korean labor & income panel 8(th)-10(th) wave. PLoS One. 2013, 8:e57109. 10.1371/journal. pone.0057109
28. Syamlal G, Mazurek JM, Hendricks SA, Jamal A: Cigarette smoking trends among U.S. working adult by industry and occupation: findings from the 2004-2012 National Health Interview Survey. Nicotine Tob Res. 2015, 17:599-606. 10.1093/ntr/ ntu185
29. McCaul KD, Hockemeyer JR, Johnson RJ, Zetocha K, Quinlan K, Glasgow RE: Motivation to quit using cigarettes: a review. Addict Behav. 2006, 31:42-56. 10.1016/j.addbeh.2005.04.004
30. Yalcin BM, Unal M, Pirdal H, Karahan TF: Effects of an anger management and stress control program on smoking cessation: a randomized controlled trial. J Am Board Fam Med. 2014, 27:645-660. 10.3122/jabfm.2014.05.140083