3 minute read
Polypharmacy


Other benefits of the CGA involve recognition of conditions that may interfere with cancer treatment, such as cognitive disorders, depression (especially subclinical depression), nutritional risk, polypharmacy, and absence of an adequate caregiver. Some of these conditions may be reversible, and others may be compensated for with proper intervention. For example, a patient with memory disorders may require the assignment of a caregiver prior to the start of chemotherapy; a patient unable to use transportation may need the designation of a driver.
While there is general agreement that a CGA is essential to the management of older cancer patients, controversy lingers over its execution. Several practises have adopted some form of screening test to identify patients who need a more “in-depth” assessment. In any case, the CGA involves a multidisciplinary team. While the initial evaluation of the patient, including functional assessment, is best performed by a nurse, a social worker is needed for assessing cognition, living conditions, and availability of a caregiver, a pharmacist for the assessment of polypharmacy, and a nutritionist for the assessment of nutrition and nutritional risk. Ideally, the team should also have access to other medical specialists including cardiologists, neurologists, endocrinologists, and nephrologists; to a minister of the appropriate faith trained for the recognition and management of spiritual and existential distress; and to a physical therapist.
Advertisement
The role of the team in the CGA is not limited to the estimate of functional age. It also involves the management of conditions that may compromise cancer treatment and may lead to functional dependence. This task will be described in the team function.
The prevalence of polypharmacy increases with age because, in part, of increased prevalence of comorbidity and, in part, the increased utilisation of over-the-counter medications and alternative medicine products by older individuals.
A definition of polypharmacy is wanted, but a number of issues are clear.
• Cancer patients 70 years and older take an average of 11 non-cancer- related medications per patient. • The risk of drug interactions increases geometrically for patients taking more than five medications on a single day. • For patients taking eight medications each day, the risk of drug inter- action is almost certain. • Polypharmacy is a major cause of iatrogenic morbidity and mortality.
In a study performed at our institution, the interaction between cancer- unrelated drugs was associated with an 80% increase in the risk of chemotherapy complications.
Several studies in elderly patients with and without cancer have shown that polypharmacy is best managed when a pharmacist is part of the treatment team. In this the pharmacist may be helped by a computer programme capable of identifying all potential drug interactions and by a number of criteria describing inappropriate prescriptions in the elderly. In addition to medication interactions, these include utilisation of medications that are partially contraindicated in older age such as benzodiazepines or nonsteroidal antiinflammatory agents.
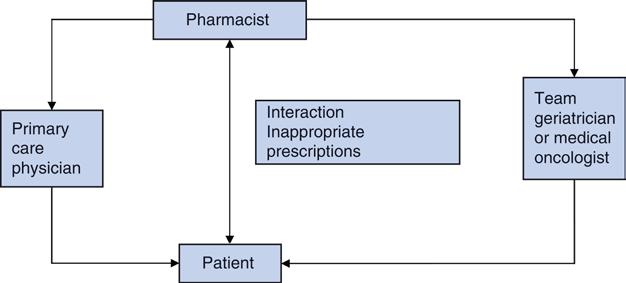
To estimate both risks and benefits of polypharmacy, it would be very helpful to have a physician with geriatric experience on the team. This is the case in some countries such as France where an ongoing cooperation of geriatricians and oncologists assures the safest and most effective treatment of older cancer patients. Alternatively, one should make sure that the older cancer patient may rely on a primary care physician to whom the team pharmacist should communicate all planned treatment changes. These alternative approaches are illustrated in Figure 2.
Figure 2 The pharmacist is central to identify inappropriate prescriptions. This information may be conveyed to the geriatrician or the oncologist on the team or to the patient’s primary physician.