
7 minute read
Practices Monetized With Silent Partnerships

“I
Since COVID, some of the most valuable dental specialty practices have been Endodontic practices from coast to coast.
Advertisement
Timing Is Everything
In the last two years, at least eight “Endo Only” Invisible Dental Support Organizations (IDSO) have been formed. In addition, the multi-specialty IDSOs with dozens, or hundreds, of practices across the U.S. have joined the rush to invest in Endodontics. There are also several IDSOs which are eager to partner with Endo, Perio and OMS practices in the same areas.
over $600 million of transactions. Notably, over $100 million of our 2022 transactions were for doctors under 40.
A transaction involves monetizing part of your practice for cash now, remaining an owner for at least five years, and ultimately realizing a valuable exit strategy.

These are complex transactions with multiple moving parts of agreements and future partnership operations. Every word in an agreement matters, and doctor’s benefit from the advice of an expert.
These are complex transactions with multiple moving parts of agreements and future partnership operations. Every word in an agreement matters, and doctor’s benefit from the advice of an expert.
initial bid. A typical LPS Endodontic client
If you have a larger, growing practice, you will have multiple IDSO suitors. A spirited bidding contest among multiple eager partners always increases the value for doctors. The key is to meet with multiple partners and know which one is the best choice. It’s not always about the highest initial bid. A typical LPS Endodontic client will have six or more qualified IDSO partners to choose from resulting in higher values with the best partner fit for you.
CASH NOW, WEALTH LATER
Typically, an IDSO will silently invest in a great practice by purchasing 60% to 90% of a practice
Typically, an IDSO will silently invest in a great practice by purchasing 60% to 90% of a practice for cash. The doctor retains ownership of the balance, either at the practice or parent level, or both. With the right partner, the retained ownership portion can provide the doctor with significant future gains. There are many examples of doctors who became owners in IDSOs where their retained equity exceeded 3X, 5X and even 20X of the practice’s initial value.
Specialist Advisors Add Value At No Net Cost
LPS specializes in advising dental practices of all specialties and GP in partnership transactions with IDSOs nationally. In 2022, LPS completed
With the right advisor, you will find the best partner, at the highest value, in a smooth process, that actually closes. LPS is paid nothing unless a transaction is completed and only paid by doctors. The conflicted little advisors are paid by both the doctor and the IDSO.
With the right advisor, you will find the best partner, at the highest value, in a smooth process, that actually closes. LPS is paid nothing unless a transaction is completed and only paid by doctors. The conflicted little advisors are paid by both the doctor and the IDSO.
T He Process To Learn The Value Of Your Practice In An Idso Transaction
The Process To Learn The Value Of Your Practice In An Idso Transaction
The LPS process begins with a confidential, no obligation phone call between the doctor and an LPS principal to learn the general features of the practice and most importantly, the goals of the doctor(s). Doctors who are interested in learning the potential value of their practice execute a Non-Disclosure Agreement and provide three years of profit and loss statements. LPS analysts will review the data and schedule a call to learn more details. Once that call is complete, doctors have another call with an LPS principal to learn our view of the value of your practice and outline various transaction structure options available to you. If that value is of interest, doctors can engage LPS to represent them. LPS is only paid if and when a transaction is complete. Doctors have no risk or obligation.
The LPS process begins with a confidential, no obligation phone call between the doctor and an LPS principal to learn the general features of the practice and most importantly, the goals of the doctor(s). Doctors who are interested in learning the potential value of their practice execute a Non-Disclosure Agreement and provide three years of profit and loss statements. LPS analysts will review the data and schedule a call to learn more details. Once that call is complete, doctors have another call with an LPS principal to learn our view of the value of your practice and outline various transaction structure options available to you.If that value is of interest, doctors can engage LPS to represent them. LPS is only paid if and when a transaction is complete. Doctors have no risk or obligation.
877-437-3353
877-437-3353 www.FindMySilentPartner.com www.FindMySilentPartner.com
HeyJoe@LargePracticeSales.com
HeyJoe@LargePracticeSales.com
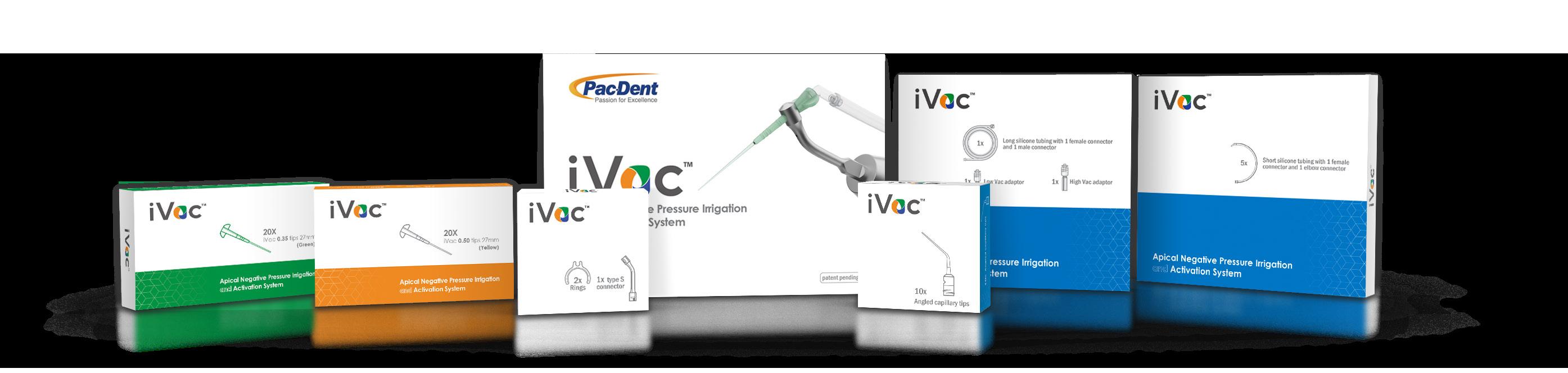
Apical Negative Pressure Irrigation and Activation System
Meet the True
All-in-One Irrigation System
DENTISTRY HAS SEEN SIGNIFICANT TECHNICAL DEVELOPMENT IN RECENT DECADES, and endodontics is no exception. Engine-driven NiTi files have seen prolific advances, showing more flexibility and fracture resistance. Nevertheless, while the highperformance file system advantageously shortened the operative time, it also reduced the time and volume of irrigating solution - mainly sodium hypochlorite - during the instrumentation phase. This imbalance is being observed in several published papers, emphasizing the importance of time, volume, activation, and renewal of the irrigating solution in the disinfection stage.
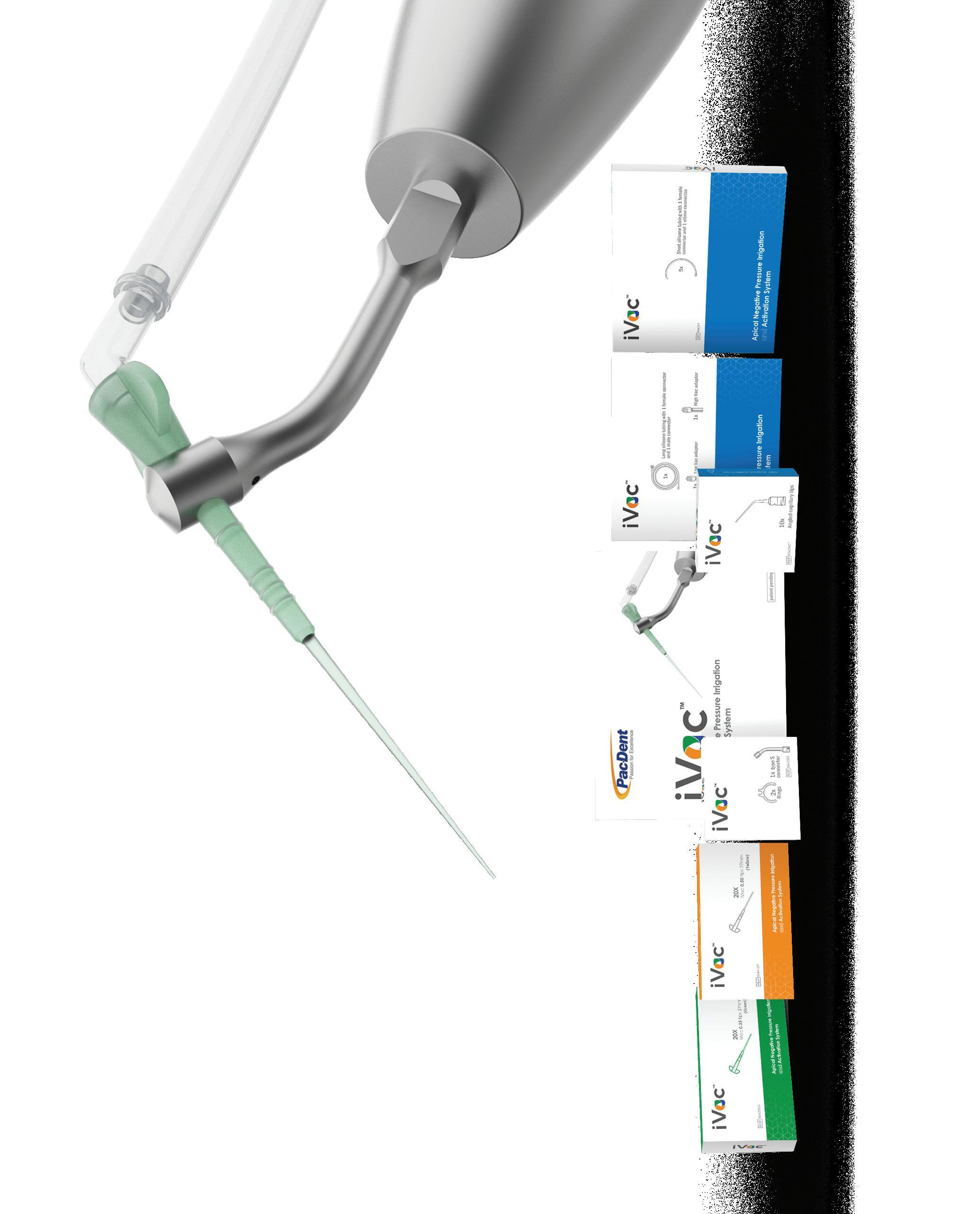
acting safely against the risk of liquid extrusion into the periapical tissue and activating the renewed fluid inside the canal. The system comprises an aspiration/ activation polymer cannula with two options of diameters, .35mm and .50mm. The iVac ultrasonic connector is designed to easily hold the cannula accurately while transmitting the vibration from the piezo ultrasonic handpiece. In addition, tubes and connections allow the ordinary vacuum outlet to be coupled, adding negative pressure to the system.
• Substantial less irrigant apical extrusion
• Concomitant irrigation leads to always using fresh liquid
• Allows the irrigating fluid to travel through the entire canal to the working length


Pac-Dent iVac™ irrigation system provides the synergistic e ect of negative pressure, continuous irrigation, and ultrasonic activation in one easy-to-use device.
Less irrigant extrusion compared with PUI and syringe irrigation
Concomitant irrigation always leads to the use of fresh liquid
Allows the irrigating fluid to travel through the entire canal to the working length
No build-up is necessary
Low cost per procedure
High debris removal capacity by ultrasonic fluid activation
Polymer cannula with high resistance and flexibility to curve canals challenge

Accurate control of the irrigation depth in open apices, regenerative, and foramen resorption cases
Easy and intuitive set-up
It avoids the vapor lock effect
It can be coupled to the most common types of piezo ultrasonic units (S and E-types)
Adaptable to the majority of final irrigation protocols
Additionally, the literature emphasizes three fundamental principles regarding irrigation delivery and physical action. The first principle attests that irrigation must reach the entire root canal system, particularly the apical third. The second would be the mechanical activation of the liquid, improving its interaction with the dentin walls. The third concerns the constant fluid renewal, ensuring that an active liquid continuously interacts with the root canal’s content.
Pac-Dent iVac™ Apical Negative Pressure Irrigation and Activation System was developed to fulfill the three mentioned irrigation mechanical aspects principles in a practical, efficient and safe way.
The iVac System is designed to be used during the irrigation/disinfection phase connected to a piezo ultrasonic handpiece. The first concept adopted is ultrasonic vibration, which acts as a chemical catalyst for irrigating solutions in conjunction with the transient cavitation and microstreaming effects. The second concept is true apical negative pressure, by which the irrigation fluid moves from the pulp chamber to the apical limit without extruding beyond the foramen. Additionally, concomitant irrigation, whereby the irrigating liquid is renewed continuously. The iVac united the three irrigation fundaments in a single device,

• No build-ups are necessary
• Eliminates the vapor-lock effect
• Low cost per procedure
• Ultrasonic fluid activation
• Polymer cannula with the same resonance pattern as metal, high resistance, and flexibility to curve canals
• Easy and intuitive set-up
• It can be coupled to the most common types of piezo ultrasonic units
• Adaptable to the majority of final irrigation protocols.
The GentleWave® G4 System
BEYOND IRRIGATION. BEYOND CLEAN.
The GentleWave System takes you beyond canal complexity that can hinder thorough disinfection and debridement.

Inside the console the irrigant is thoroughly degassed, precisely diluted and continuously refreshed. Next, it enters the sealed, closed loop delivery system, where the system’s physics-accelerated chemistry becomes truly remarkable.
The GentleWave procedure is a more effective way of cleaning teeth, including hard-to-reach areas such as the apical thirds and complex anatomies of the root canal system:
• Predictably removes up to 99.9% of biofilm1
• Effectively disinfects and debrides undetected and intricate anato
• 4X - 8.5X greater penetration into dentinal tubules vs. ultrasonic systems4
This can lead to better outcomes for patients and deliver a more comfortable patient experience with reduced risk of complications:
• 96.6% of patients report mild to no pain within 48 hours5 of the procedure
• 97.7% 12-month healing rate6
• Preserves the structural integrity of the tooth
Experience a GentleWave G4 demonstration at AAE booth # 501 or visit https://gentlewave.com/doctor/contact?form_type=test_drive

The GentleWave System with CleanFlow™ Technology

CleanFlow is a procedure instrument custom-designed to simplify your procedures. The procedure instrument cleans and disinfects the entire root canal system without entering the tooth. CleanFlow is designed to be safe around critical anatomy. The unique design permits easier access inside the mouth and enables a one-handed procedure, making the patient experience even better.
Learn more at https://gentlewave.com/doctor/gentlewave-system
TDO® Software
THE DIGITAL OFFICE ® SOFTWARE BUILT FOR ENDODONTISTS https://wwww.tdo4endo.com/ doi: 10.1007/s00784-018-2515-x. Epub 2018 Jun

TDO Software is a full-suite practice management solution offering unparalleled imaging integration with key automations designed by endodontists for the most efficient endodontic workflow. Exceptional features include automated and custom referral doctor reports, at-home patient document completion, and workflow efficiencies that turn your waiting room into a welcome room, helping move patients more quickly into your operatory. TDO is trusted by endodontists across the world for the efficiencies it provides for offices of all sizes.
15. PMID: 29948281.
2. Molina B, Glickman G, Vandrangi P, Khakpour M. Evaluation of Root Canal Debridement of Human Molars Using the GentleWave System. J Endod. 2015 Oct;41(10):1701-5. doi: 10.1016/j.joen.2015.06.018. Epub 2015 Aug 12. PMID: 26275599.
3. Wang Z, Shen Y, Haapasalo M. Root Canal Wall Dentin Structure in Uninstrumented but Cleaned Human Premolars: A Scanning Electron Microscopic Study. J Endod. 2018 May;44(5):842-848. doi: 10.1016/j.joen.2018.01.014. Epub 2018 Mar 15. PMID: 29550004.
4. Vandrangi P (2016) Evaluating Penetration Depth of Treatment Fluids into Dentinal Tubules Using the GentleWave® System. Dentistry 6: 366. doi:10.4172/2161-1122.1000366
5. Data on file. Sonendo, Inc.
6. Sigurdsson A, Garland RW, Le KT & Rassoulian SA. Healing of Periapical Lesions After Endodontic Treatment with the GentleWave Procedure: A Prospective Multicenter Clinical Study. Journal of Endodontics. 2018;44(3):510-517.
