
6 minute read
Drug-Resistant Epilepsy: Potential Causes and Treatments

Rose Ludecke
Abstract:
One in three people with Epilepsy are nonresponsive to drugs attempting to suppress their epileptic episodes. This is known as Refractory Epilepsy and is defined as when a patient is unresponsive to two sufficient trials of anti-seizure medications (ASMs).1 A variety of treatments are possible, and further research looks more closely into potential mechanisms that may cause this condition.
Introduction to Epilepsy
Epilepsy is a condition that affects the Central Nervous System. Specifically, it is a neurological disorder in which the brain acts abnormally causing uncontrollable seizures, behaviors, sensations, and sometimes loss of awareness.2 The types of seizures or symptoms present among patients can vary in severity. Some will stare blankly, while others will twitch or seize uncontrollably.2 The brain operates through bursts of electricity between different neurons that work collectively to control thoughts, emotions, and movements. During an epileptic episode, something is disrupting this communication between the neurons, which can potentially cause a seizure to occur. There are two main categories for types of seizures: focal onset seizures and generalized onset. Focal onset seizures originally start in one specific area of the brain, and then spread across the brain. Patients with focal onset seizures usually have had some sort of trauma to a specific part of the brain that is now the origin of focal onset seizures, like a stroke or meningitis.3 Further, some patients can feel focal seizures start to occur before the symptoms become more intense. In generalized onset seizures, the activity occurs on both sides of the brain as opposed to originating in one specific part of the brain, and then spreading across the brain (Figure 1).
Figure 1: Generalized vs. Focal Seizures 4 Generalized onset seizures can be genetic, and usually start during childhood because of the brain’s inability to regulate the electricity between the neurons. Most patients who have epilepsy are able to be treated through medication. However, around 1/3 of the population with Epilepsy cannot be treated with medication, and instead have a form of Epilepsy known as Refractory Epilepsy.
Drug-Resistant Epilepsy
Drug-resistant Epilepsy is clinically defined as when a patient has been unable to stay seizure-free after two sufficient trials of antiseizure medications.1 This condition affects about 1/3 of all patients with epilepsy. The reasons for drug-resistance to Epilepsy vary and have different contributing factors from patient-to-patient due to different circumstances, and theoretically the action site of the medication being used.4
Potential Causes to Drug-Resistant Epilepsy
There is no consensus on the cause or causes of drug-resistant epilepsy. Simpler ideas put forth by doctors and scientists identify factors such as age, where older patients reported better results to the medication, and were more likely to be seizure-free.4
Multiple hypotheses have been put forth to attempt to explain the cause of Refractory Epilepsy. The target hypothesis, for example, puts forth the theory that the cause of this condition specifically related to how the anti-epileptic medication works. The theory is that the alteration of cellular targets causing the epileptic episodes by the medication leads to an eventual desensitization of the body to the treatment. As the patient continues to use the medication, the less effective it becomes. However, the target hypothesis presumes a total understanding of the mechanisms of antiepileptic drugs, which there is not. Additionally, there are people who are resistant to multiple types of epileptic drugs that have different actions, which the hypothesis does not account for. These are two relatively big problems for the target hypothesis. Another hypothesis currently being discussed is the transporter hypothesis, which postulates that, “drug resistance may be attributable to overexpression of multidrug efflux transporters at the epileptic focus.”4 One of the most studied efflux transporters is P-glyco-protein. The target hypothesis contends that while the transporter protein pumps normal amounts of xenobiotics from intracellular space back to the capillary lumen to maintain the integrity of the blood, the use of many medications used to regulate epileptic seizures alters the p-glyco-protein, causing the medication not to work because of the overexpression of these efflux transporters at the epileptic focus. This is consistent among many patients, found in resected samples of the brains of patients who had drug-resistant epilepsy. A conflicting explanation to this is that the gene that encodes the P-glycoprotein is the source of the poor response to the antiepileptic drugs. Another study was conducted that put forth reasoning behind resistance to a common anti-epileptic drug known as Carbamazepine. Carbamazepine works by blocking the fast-sodium current in dentate granule cells, but was lost in the hippocampus of patients who were drugresistant to carbamazepine. This wasn't found in a drug that has similar actions to carbamazepine, called lamotrigine. The resistance to these drugs (as well as ones that use sodium channels) could have been associated to polymorphisms (a discontinuous genetic variation resulting in the occurrence of several different forms or types of individuals among the members of a single species) of the SCN2A gene.4 While there are many hypotheses and theories surrounding potential causes of refractoryepilepsy, there is not yet a definitive consensus, which may be attributed to the variety in patients who have drug-resistant epilepsy.
Current Available Treatments
One of the main underlying issues regarding the treatment of Refractory Epilepsy is pseudoresistance. In order to determine whether a drug treatment is effective or not, you have to make sure that the person was not misdiagnosed. There are many disorders that have effects similar to those of epilepsy, and patients are subsequently misdiagnosed with some form of drug-resistant epilepsy because they are not being given the right medication for what illness they have. Around 25% of people who are claimed to have drug resistant epilepsy actually have a different disorder.4 There are other potential causes such as the lifestyle of the patient (ex. abuse of drugs or alcohol, non-regulated use of medication or insufficient adherence to the medication) that can cause mistrials, and an eventual misdiagnosis of refractory epilepsy.
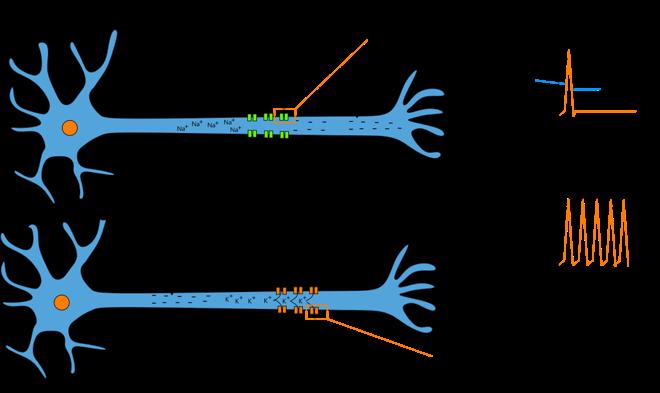
Figure 2: Nerve Cell Electrical Charge Movement
Once it is determined that the condition the patient has is, in fact, drug-resistant epilepsy, there are many ways potential treatment pathways. Patients should be evaluated early for the chance of a surgical remedy if they have conditions like unilateral hippocampal sclerosis or other lesions that can be resected. This decision should be weighed versus additional drug trials. In a randomized, controlled study, the prototype surgery of an anterior temporal lobectomy was shown to be better than medication in providing long-term relief from seizures in up to 70% of patients (adults) with Refractory Epilepsy.9 One issue with current antiepileptic drugs on the market is that they only focus on preventing seizures, and not necessarily at the right site. In some cases of epilepsy where there has not been an identified cause, there are autoantibodies involved in the neuronal excitation and inhibition that attack the ion channels, causing differences in positive and negative electricity in the cell (Figure 2). Patients who share this trait often do not respond to antiepileptic drugs, and immunotherapy trials have conflicting data surrounding their efficacy. Another possible treatment plan is the combination of multiple anti-epileptic drugs. Specifically, data from applied research of combination pharmaceutical therapy on animals suggests that the use of medication with two different modes of action, rather than multiple drugs with the same mode of action, could potentially help to cause patients to be seizure free, though highquality data supporting this theory is lacking. Those with refractory-epilepsy do not have one singular course of action to become seizure-free, however clinical trials are still underway to attempt to find a cure.
1 Epilepsy Foundation. 5 Oct. 2020, www.epilepsy.com/treatment/medicines/drdrresistant-epilepsy. Accessed 28 Apr. 2022 2 Mayo Clinic Staff. "Epilepsy." Mayo Clinic, 7 Oct. 2021, www.mayoclinic.org/diseasesconditions/epilepsy/symptoms-causes/syc-20350093. Accessed 28 Apr. 2022. 3 Johns Hopkins Staff, editor. "Types of Seizures." Johns Hopkins Medicine, Johns Hopkins, www.hopkinsmedicine.org/health/conditions-anddiseases/epilepsy/types-of-seizures. Accessed 1 May 2022 4 Kwan, Patrick, et al. "Drug-Resistant Epilepsy."
