12 minute read
Characteristics of Chronic Intestinal Failure in the United States

Adapted from Mundi MS, Mercer DF, Iyer K, et al. Characteristics of chronic intestinal failure in the USA based on analysis of claims data. J Parenter Enteral Nutr. 2022:1-9. doi 10.1002/ jpen.2426, with permission of the publisher.
How many people in the United States are living with chronic intestinal failure (CIF)* and requiring home parenteral (IV) nutrition (HPN)? How and where are they managed, and by whom? Information such as this could help focus research and resources where they can have the most impact, and help lessen the burden on patients with CIF on HPN and their caregivers. It would help in determining what works in caring for this population, and what doesn’t, and in validating some of the challenges we know they face—in part by listening to the people affected—so these, too, can be addressed.
Advertisement
Yet it has been difficult to find answers to these kinds of questions, and to get a picture of what CIF patients experience in the United States healthcare system. There is no central patient registry and no mandated reporting system. Two studies were conducted that helped establish how many people in the United States were on HPN, or the “prevalence” of HPN, in the 1990s and in 2013.
Using data from Medicare and the North American Home Parenteral and Enteral Nutrition Registry (which has long been defunct), Oley Foundation co-founder Dr. Lyn Howard and colleagues estimated that in the United States in 1992, 40,000 people (157 per million) received HPN (Howard L, Ament M, Fleming CR, Shike M, Steiger E. Current use and clinical outcome of home parenteral and enteral nutrition therapies in the United States, Gastroenterology. 1995;109[2]:355-365). More recently, Dr. Manpreet Mundi and his colleagues, using data from Medicare and from three of the largest durable medical equipment (DME) providers in the United States, estimated that in the United States in 2013, 25,011 people (70 per million) received HPN.
In this most recent study, Drs. Manpreet Mundi, David Mercer, Kishore Iyer, and others conducted an analysis of an open, deidentified insurance claims database to look at the current state of CIF management in the United States. Joan Bishop, then Oley Foundation Executive Director (and now Executive Director Emeritus), also contributed to this project.
Dr. Mundi et al looked at insurance claims from October 2012 to June 2022 and identified patients with “at least two PS [parenteral support] prescriptions within six [consecutive] months and a relevant diagnosis.” They then analyzed the “prevalence and characteristics of patients with CIF, their travel distance to receive PS prescriptions, and the distribution of PS providers and their prescribing history” (page 1). This article shares their findings, as presented in their paper, “Characteristics of Chronic Intestinal Failure in the USA Based on Analysis of Claims Data.” All quotes and citations used here are taken from this paper.
The Claims Database
“The IVD database is a national administrative open claims database consisting of longitudinal data of 290 million unique deidentified US patients regarding pharmacy claims, physician offices medical claims, and hospital claims, including patients with multiple years of PS claims. It covers all payment types, including…commercial plans, Medicare (including Medicare Advantage), Medicaid, cash, and assistance programs. It complies with the Health Insurance Portability and Accountability Act” (page 2).
Not all claims made in the United States are included in the IVD database. Mundi et al cite this as one of the limitations of the study, noting, “This may affect especially the Western region of the United States, as claims covered by one of the large insurers in the Western states are not included in the database” (page 7).
About the Patients with CIF
Dr. Mundi and his colleagues identified an estimated** 24,028 CIF patients, of all ages, in the database. Based on population estimates from 2012 to 2020, this translates to 75 CIF patients per million US inhabitants. This figure (75 per million) represents the estimated prevalence of CIF patients in the United States.
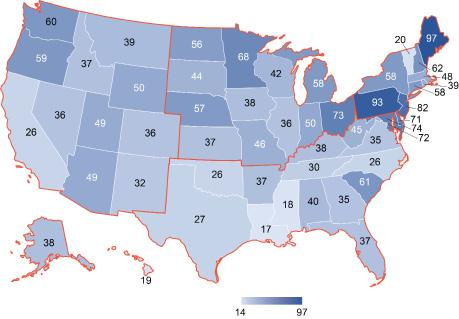
Figure 1 shows the number of CIF patients for each state per million individuals in the database. The states with the highest number of patients per capita were Maine, Pennsylvania, and New Jersey. The states with the lowest number were Vermont, Mississippi, and Louisiana.

Figure 1. Number of patients with CIF for each state per million individuals in the claims database.
Figures 1 and 2 from Mundi et al, Characteristics of chronic intestinal failure in the USA based on analysis of claims data. J Parenter Enteral Nutr. 2022:1-9, used with permission of the publisher.
The database included CIF patients of all ages (see table 1). Sixty percent of CIF patients in the adult age groups were women. “Medicare was the most important provider for patients 65 years or above and Medicaid was the second most important provider in the pediatric age group, as would be expected from the eligibility criteria of the two programs” (page 5). (See table 2.)

Table 1. Age ranges of CIF patients identified in database

Table 2. Health insurance coverage of CIF patients identified in database
Location data was available for 16,449 of the CIF patients identified in the database. Looking at the distribution of the average distance these patients “traveled outside of their ZIP3 area to receive PS prescriptions indicates that approximately half of the patients traveled between 10 and 100 miles for their PS prescriptions (55%), yet a notable proportion traveled between 100 and 1,000 miles (33%)….Of note, patients in the pediatric age group (0–17 years of age, n = 1,667) traveled further on average (median of 77 miles) than adult patients (n = 14,942, median of 62 miles)” (page 5).

Table 3. Geographical distribution of CIF patients identified in database
The distances traveled varied quite a bit depending on which region of the United States the patient lived in. Looking at median miles, patients living in the West traveled the furthest to receive their PS prescriptions. Those in the Northeast traveled the least. (See table 4.)

Table 4. Distance traveled by CIF patients identified in the database in the different regions of the US
The authors of this study note that they “used the center of the patients’ ZIP3 area code, which is not identical with the patients’ exact location. Furthermore, only the current location of the patient and physician were available, which is not necessarily their location at the time of the PS interaction….In addition, some of the PS interactions may have taken place via telehealth solutions instead of in person” (page 7). These are cited as limitations of the study.
About the PS Providers
Using the providers’ zip codes, Dr. Mundi et al created a map that shows the location of providers in the United States who prescribed PS for each of their patients for at least 12 months (see figure 2). There are many PS providers in the East, especially in the Northeast, “where hubs with providers prescribing for large patient populations were co-located with large population centers” (page 3). There were more providers, more densely located, in the Northeast than in any other part of the country.

Figure 2. Geographic location associated with PS providers in the US. The color represents the number of patients each provider had PS interactions with that were at least 12 months apart. Each dot represents one physician who signed orders for PS prescriptions at the respective geographical loca- tion associated with their ZIP code. Providers with higher patient counts took priority over providers with lower patient counts at each ZIP location.
Figures 1 and 2 from Mundi et al, Characteristics of chronic intestinal failure in the USA based on analysis of claims data. J Parenter Enteral Nutr. 2022:1-9, used with permission of the publisher.
Many of the providers in the Midwest, South, and West managed fewer numbers of PS patients (1 to 4). The exceptions were in “high prescriber hubs,” such as Rapid City, South Dakota, and Salt Lake City, Utah, where there was at least one provider writing prescriptions for 20 or more CIF patients.
Looking at how many PS orders providers signed for different time periods of up to 12 months showed that “the number of physicians who had PS interactions with their patients generally decreased over time, irrespective of the number of patients they were managing. There was a relatively high number of physicians (n = 21,004) who signed orders for at least two PS prescriptions for a small number of patients with CIF (1 to 4 patients) over a relatively short period of time (i.e., 2 months). This number dropped by 47% over 12 months, indicating that only a little over half (n = 11,205) of physicians still prescribed PSfor their individual patient or small patient group after 1 year.
“Considerably fewer physicians signed orders for at least two PS prescriptions over at least 2 months for 5–9 patients with CIF (n = 648) and even fewer for 10–19 and 20 or more patients with CIF (n = 176 and n = 83, respectively). …After 12 months, only 37% of physicians with 5–9 patients (n = 237), 44% of physicians with 10–19 patients (n = 78), and 33% of physicians with >20 patients (n = 28) still prescribed PS for their patient pool.”
A large percentage of providers signed PS prescriptions for one or a small group of patients over a short period of time. “Often, these prescriptions are being guided by DME [durable medical equipment or home care company] providers who are delivering PS to patients, as many PS prescriptions have the ability to have DME providers actively manage PS. Although the DME providers may be managing PS for a significant number of patients, they are not able to provide wholistic CIF care for individual patients.” Only a few physicians (n = 28) signed PS orders for 20 or more patients long term (for 12 months), "presumably indicating more stable patient populations at well-established medical centers specializing in the care of patients with CIF” (pages 5–6).
"Even though PS orders were signed by providers who managed a small number of patients, presumed to be primary care providers, patients still traveled up to 100 miles to receive their PS prescriptions. This indicates that, although patients were able to have their PS orders filled locally, they often had to travel considerable distances to visit with the provider who wrote the original PS prescription. A large proportion of patients traveled >100 miles, indicating a substantial inequality in healthcare coverage throughout the country….There was less coverage in the rural areas of the Midwest, South, and West, where the majority of providers prescribe PS for individual patients or small patient groups. For this reason, patients in rural areas presumably had to travel considerably longer distances to receive PS prescriptions than their urban counterparts” (pages 6–7).
Traveling with CIF can be difficult. In addition to having to travel with supplies necessary for the administration of PS, patients with CIF often have frequent need to use a restroom, and would have to find public restrooms along the way. Also, traveling longer distances means more time away from work and other responsibilities, and higher out-of-pocket expenses.
Conclusion
Mundi et al state, “Despite advances in the management of CIF, including dietary interventions, oral rehydration solutions, antimotility agents, and novel drugs targeting intestinal mucosal growth, the fragmentation of care for CIF in the United States seems to be worsening over time” (page 7). From 2012 to 2020, they noted a decrease in the number of doctors with long-term prescribing history.
They suggest that the following factors may be contributing to this decline:
• Fewer providers developing an expertise in the management of CIF. It is possible, too, they note, that primary care providers may sign the initial PS prescription, then refer the patient elsewhere as their condition progresses or stabilizes.
• A lack of physicians developing an expertise in nutrition. They note, too, that in medical schools and residency programs, there is a decline in nutritionfocused education, with fewer programs requiring a dedicated nutrition course.
• The current reimbursement model for healthcare. Under the current system, health insurance plans “often reimburse significantly more for surgical interventions or procedures, such as endoscopy, than for office visits focusing on disease prevention. In this reimbursement model, many physicians tend to focus their practice on management of acute issues rather than chronic care, especially oversight of PS prescription” (page 7).
• The lack of a dedicated CIF code in the two commonly used collections of standardized codes representing medical procedures, supplies, products and services (HCPCS, the Healthcare Common Procedures Coding System, and ICD, International Standard Classification of Diseases and Related Health Problems). “Over decades, this situation has complicated clinical practice and forced healthcare providers to use a variety of other diagnostic and treatment codes for their patients with CIF. Appropriate codes for intestinal failure and short bowel syndrome have been added to the 2022 release of the ICD-11 and are under discussion for the ICD-10-CM for use in the United States as well. [Dr. Mundi and the other authors of the paper] hope that future iterations of the ICD and HCPCS applicable in the United States will include these codes to facilitate management of, and reimbursement for, patients with CIF. The lack of a uniform coding system to date has not only limited an assessment of the true prevalence of CIF in the United States, it has also hampered analysis of healthcare resource utilization and other characteristics associated with CIF, which would enable the establishment of appropriate regulations and frameworks for its management” (page 7).
Dr. Mundi et al conclude, “Healthcare disparities for patients with CIF have likely been obscured by the lack of CIF-specific diagnostic and procedure codes, obliging providers to code [to record a diagnosis for insurance purposes] for their patients under other codes. Effective policy changes, including centralized care, revision of reimbursement models, and expansion of nutrition-focused education in addition to the newly introduced International Classification of Diseases codes, are needed to provide the best care for patients" (page 1).
*Chronic intestinal failure (CIF) has recently been defined as a “reduction of gut function below the minimum necessary for the absorption of macronutrients and/or water and electrolytes, such that intravenous supplementation is required to maintain health and/or growth.” “Intravenous (IV) supplementation,” or PS, refers to IV fluids and/or parenteral nutrition. (Pironi L, Arends J, Bozztti F, et al. Home Artificial Nutrition & Chronic Intestinal Failure Special Interest Group of ESPEN. ESPEN guidelines on chronic intestinal failure in adults. Clin Nutr 2016;35(2):247-307)
**The number is an estimate because the claims database contains duplications. If a patient moves from one state to another or changes their name, for example, data about that patient could show up twice. This is considered one of the limitations of the study.
