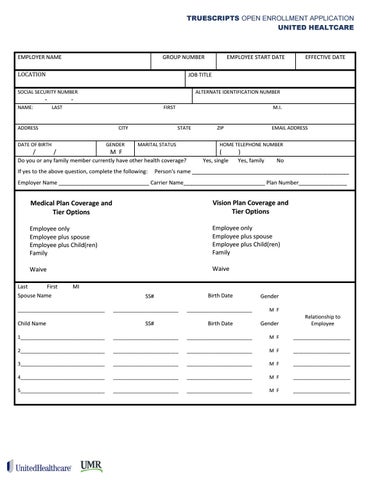
TRUESCRIPTS OPEN ENROLLMENT APPLICATION UNITED HEALTCARE
EMPLOYER NAME
GROUP NUMBER
SOCIAL SECURITY NUMBER NAME:
LAST
ALTERNATE IDENTIFICATION NUMBER
-
FIRST
ADDRESS DATE OF BIRTH
/
EFFECTIVE DATE
JOB TITLE
LOCATION
-
EMPLOYEE START DATE
CITY GENDER
/
M F
M.I. STATE
MARITAL STATUS
Do you or any family member currently have other health coverage? If yes to the above question, complete the following:
ZIP
EMAIL ADDRESS
HOME TELEPHONE NUMBER
(
Yes, single
)
Yes, family
No
Person's name ____________________________________________________
Employer Name ______________________________ Carrier Name___________________________ Plan Number________________
Medical Plan Coverage and Tier Options
Vision Plan Coverage and Tier Options
Employee only Employee plus spouse Employee plus Child(ren) Family
Employee only Employee plus spouse Employee plus Child(ren) Family
Waive
Waive
Last First Spouse Name
MI
________________________________
Child Name
SS# ________________________
SS#
Birth Date ________________________
Birth Date
Gender M F
Gender
Relationship to Employee
1_______________________________
________________________
________________________
M F
_____________________
2_______________________________
________________________
________________________
M F
_____________________
3_______________________________
________________________
________________________
M F
_____________________
4_______________________________
________________________
________________________
M F
_____________________
5_______________________________
________________________
________________________
M F
_____________________