
10 minute read
Language in Mind


Cerys Broad, 1st year
1. Introduction
Aphasia is a language disorder characterised by difficulties in speech production and communication. This can affect many aspects of language including phonology, morphology, syntax, and semantics (Code, 1989: 2). Aphasia is caused by damage to the brain, particularly in the left hemisphere as this is where speech and language production and processing is located (Sedivy, 2019: 69). A typical way in which the brain can be damaged resulting in language difficulties and more specifically aphasia is due to strokes. Damage to specific areas of the brain can result in different types of aphasia presenting varying severities and symptoms. The differences in symptoms for differing aphasia categories can be observed and used in diagnosing aphasia patients. This essay will define and characterise three types of aphasia, Broca’s, Wernicke’s, and Anomic aphasia. This information will then be applied to data from two aphasia patients, aiming to diagnose them with a specific type of aphasia.
2. Types of Aphasia
2.1 Broca’s Aphasia
One type of aphasia affecting speech and language production is Broca’s aphasia. Broca’s aphasia, also known as expressive aphasia, motor aphasia, syntactic aphasia or agrammatic aphasia (Berndt and Caramazza, 2008: 3) is a type of non-fluent aphasia and is caused by damage to the Broca’s area, located in the left frontal lobe of the brain (Code, 1989: 4). This type of aphasia is characterised by slow speech with frequent pausing and difficulty in choosing which words to use (Sedivy, 2019: 69). Broca’s aphasia can also be identified through shorter sentences/phrases, simplified syntax and a reduction in function words and functional morphemes (Cutler, 2005: 57).
2.2 Wernicke’s Aphasia
Another type of aphasia impacting language in patients is Wernicke’s aphasia. This is a fluent type of aphasia and is caused by damage to the Wernicke’s area, located in the left temporal lobe of the brain (Sedivy, 2019: 71). Similar to Broca’s, and most types of aphasia, patients with Wernicke’s aphasia have difficulties in finding the right words to use. Unlike Broca’s aphasia patients, they are able to speak fluently. This results in speech that is fluid and continuous but lacks substance and relevant meaning often resulting in nonsensical speech or what Pallickal and Hema (2020) refer to as “neologistic jargon” (p1140).
2.3 Anomic Aphasia
The final type of aphasia to be discussed is Anomic aphasia. This is another type of fluent aphasia and can be cause by damage to the left hemisphere of the brain. Anomic aphasia is characterised by the patient’s inability to retrieve lexical items from their lexicon (Andreetta et al, 2012). Despite difficulties in retrieving words and some instances of pausing throughout speech, anomic aphasia is still considered a fluent type of aphasia due to frequent production of full, coherent sentences without error (Bar-On et al., 2018: 884).
Unlike other types of aphasia, anomic patients often produce wellformed, grammatically correct, and relevant speech however there is a significant difficulty in finding the words to use which causes speech to be produced slower and less fluidly (Andreetta et al, 2012).
3. Data Analysis of Patients
In order to identify what type of aphasia a patient has a Mean Length of Utterance (MLU) must be calculated. This is the average number of words or morphemes that are uttered by patients at a given time (Sedivy, 2019: 207). To find the Mean Length of Utterance, the number of words or morphemes uttered are counted and divided by the total number of utterances. In this analysis, nonlexical utterances, fillers, and unintelligible utterances will not be counted and will not contribute to the Mean Length of Utterance. This includes utterances such as ‘mhm,’ ‘oh,’ ‘xxx,’ and ‘Au’.
These utterances do not carry significant meaning in what the patients are trying to articulate therefore omitting them from the analysis will clarify the data making the MLU calculation more reflective of the type of aphasia present in each patient. Utterance such as ‘yeah,’ ‘okay’ and ‘alright’ however, have been counted towards the MLU as these reflect more meaning in the patients’ speech. Repetition of the same words multiple times consecutively have also been discarded from the data and will be counted just once. For example, “Queen Queen Queen Queen” will be counted as “Queen” i.e., one utterance instead of four. It can be useful to investigate both patients’ data comparatively before analysing each of them individually. Below is a graph and table presenting the number of words and utterances spoken by each patient, followed by a graph presenting their respective MLU’s.
Figure 1: Both patient’s number of words and utterances
It is expected that patients with a lower Mean Length of Utterance will have non fluent aphasia i.e., Broca’s aphasia while patients with a higher MLU are expected to have a fluent type of aphasia i.e., Wernicke’s or Anomic aphasia.
Another useful tool when diagnosing aphasia patients is to look at the relevance of the patients’ responses to the prompts given by the investigator. It is likely that patients with Wernicke’s aphasia will have fewer relevant responses while responses from those with Broca’s or Anomic aphasia will be mostly relevant.
Relevant Responses to Questions/Prompts
Figure 4: Both patients’ Mean Length of Utterances
3.1 Data Analysis Patient A
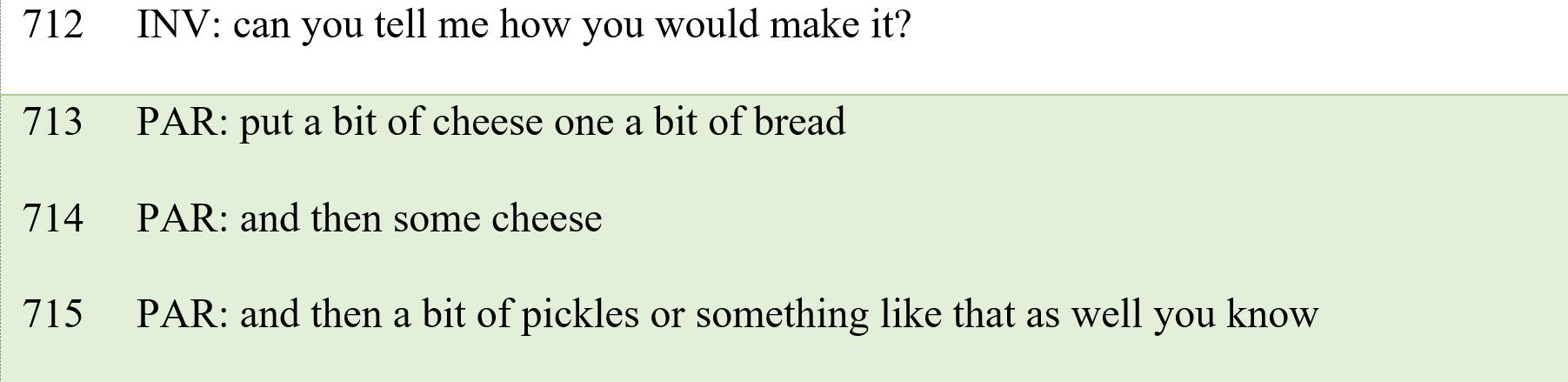
It is likely that patient A has anomic aphasia as they have an MLU of 7.54. This is evidence that they have a type of fluent aphasia e.g., Anomic or Wernicke’s as Broca’s aphasia patients tend to have lower MLUs. It is unlikely that they have Wernicke’s aphasia due to their score of 100% of relevant responses to the investigator’s prompts. This shows a level of comprehension that is only observed in patients with Broca’s and Anomic aphasia. Wernicke’s patients tend to experience disruptions in comprehension (Berndt and Caramazza, 2008: 249) meaning it would be unlikely for a Wernicke’s patient to produce 100% relevant responses. This can be found in the following example from the transcript when the investigator asks the patient to describe making a cheese and pickle sandwich.
Example 1
It is evident from this example that the patient is able to comprehend and understand the task given and produce a relevant response with accurate grammar which is common for patients with anomic aphasia (Andreetta et al, 2012: 1788).
Further evidence supporting the diagnosis of Patient A with anomic aphasia can be found in the analysis of the frequency of different word classes in their speech. Many functional word classes such as determiners, conjunctions, pronouns, and prepositions are retained in this patient’s speech. Bird et al (2002) note that anomic patients have a very high frequency of function words whereas a deficit in function words tends to be found in other types of aphasia. Below is a table and pie chart illustrating the frequency of content and function words in Patient A’s speech.
Figure 6: Patient A’s percentage use of content and function words
As illustrated by the pie chart, there is a roughly even split between the number of content and function words spoken with function words making up 44% of the patient’s speech. The use of function words can be observed in example 1 when the patient uses conjunctions, determiners, and prepositions. Deficits in function words tend to be found in agrammatical types of aphasia (Broca’s).
This patient clearly does not lack function words in their speech therefore the deduction can be made that they have anomic aphasia
3.2 Data Analysis Patient B
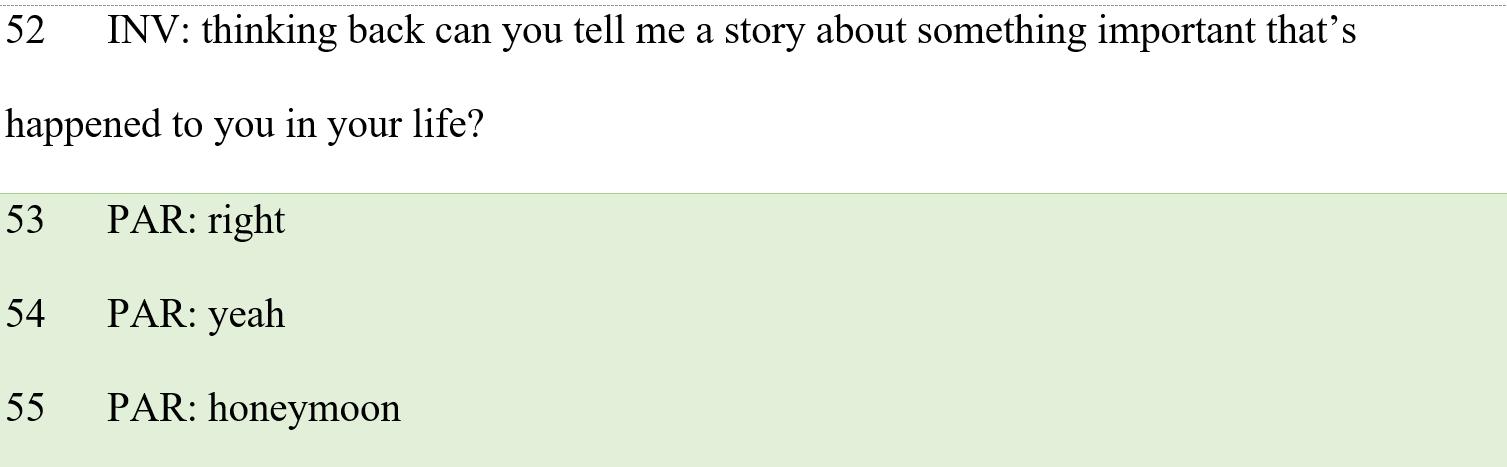
Patient B is likely a Broca’s patient. This can be deduced from the low MLU score of 1.85. A mean length of utterance this low indicates that the patient has a non-fluent type of aphasia i.e., Broca’s. The patient’s percentage of relevant responses also supports their diagnosis of Broca’s aphasia. 63% of Patient B’s responses to the investigator’s prompts were relevant. This level of comprehension is fairly common in Broca’s patients, auditory comprehension skills tend to be somewhat retained (Nielsen et al, 2019: 3) hence the lower percentage than that of the anomic patient but a higher one than that which would be observed in a Wernicke’s patient. An example of a relevant response from Patient B can be seen below.
Example 2
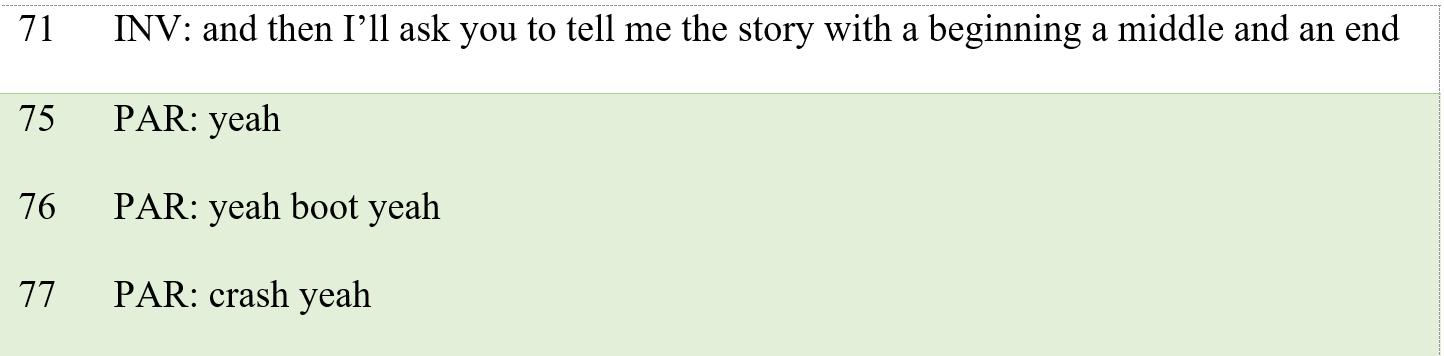
While this response is not very in-depth and consists of one-word utterances, it should be noted that it is relevant to the question asked therefore displaying comprehension skills in the patient. However, there are also examples of the patient giving answers that are not relevant to the prompt. Such as:
Example 3
The patient has once again given very short answers, which is common in Broca’s aphasia (Cutler, 2005: 57) and their answer is not necessarily relevant to the prompt given by the investigator. This shows a lack in their comprehension and understanding skills however, over half of their responses can be classed as relevant confirming that they have Broca’s aphasia as opposed to Wernicke’s. Patient B’s use of content and function words also support the diagnosis of Broca’s aphasia. Some function words are retained in their speech such as determiners, conjunctions and pronouns, however there are very few in comparison to Patient A and there is a noticeable lack of prepositions. Bird et al (2002) note that Broca’s patients tend to have difficulty retrieving function words while content words such as verbs, nouns, adjectives and adverbs can be retrieved more easily. The figures below show Patient B’s use of content and function words.
Figure 7: Number of content and function words spoken by Patient B
Patient B
Number of Function Words
21%
Number of Content Words
Number of Content Words
79%
Number of Function Words
Figure 8: Patient B’s percentage use of content and function words
The pie chart illustrates Patient B’s heavy favouring of content words over function words with function words making up just 21% of Patient B’s speech. No function words are found in the previously provided examples however they can be observed in lines such as “well everything anything yeah” and “them and them”. This patient’s lack of function words in their speech supports the diagnosis of Broca’s aphasia.
4. Conclusion
To conclude, out of the three types of aphasia discussed in this essay, distinct symptoms of each can be identified and applied to patients. It is clear that Patient A has anomic aphasia due to their high MLU score, high percentage of relevant responses and frequency of function words in their speech. It has also been deduced that Patient B has Broca’s aphasia highlighted by their very low MLU score, significant number of relevant responses to prompts and severe lack in function words.
Bibliography
Andreetta, S., Cantagallo, A., & Marini, A. (2012). Narrative discourse in anomic aphasia. Neuropsychologia, 50(8), 1787–1793.
https://doi.org/10.1016/j.neuropsychologia.2012.04.003
Bar-On, A., Ravid, D., & Dattner, E. (Eds.). (2018). Handbook of Communication Disorders: Theoretical Empirical, and Applied Linguistics Perspectives. De Gruyter, Inc.
Berndt, R. S., & Caramazza, A. (2008). A redefinition of the syndrome of Broca's aphasia: Implications for a neuropsychological model of language. Applied Psycholinguistics. 1(3). 225-278.
DOI: https://doi.org/10.1017/S0142716400000552 https://doi.org/10.1080/23273798.2019.1616104 https://doi.org/10.1080/02687038.2020.1739616
Bird, H., Franklin, S., & Howard, D. (2002). ‘Little Words’ – Not really: function and content words in normal speech and aphasic speech. Journal of Neurolinguistics. 15(3), 209237.
Code, C. (1989). The Characteristics of Aphasia. Taylor & Francis Group.
Culter, A. (2005). Twenty-First Century Psycholinguistics: Four Cornerstones. Taylor & Francis Group.
Nielsen, S, R., Boye, K., Bastiaanse, R., Lange, V, M. (2019). The production of grammatical and lexical determiners in Broca’s aphasia. Language, Cognition and Neuroscience. 34(8). University of Copenhagen.
Pallickal, M. & Hema, N. (2020). Discourse in Wernicke’s aphasia. Aphasiology. 34(9). 1138-1163.
Sedivy, J. (2019). Language in Mind (2nd Ed.). Oxford University Press.

