6 minute read
Healthcare design outlook


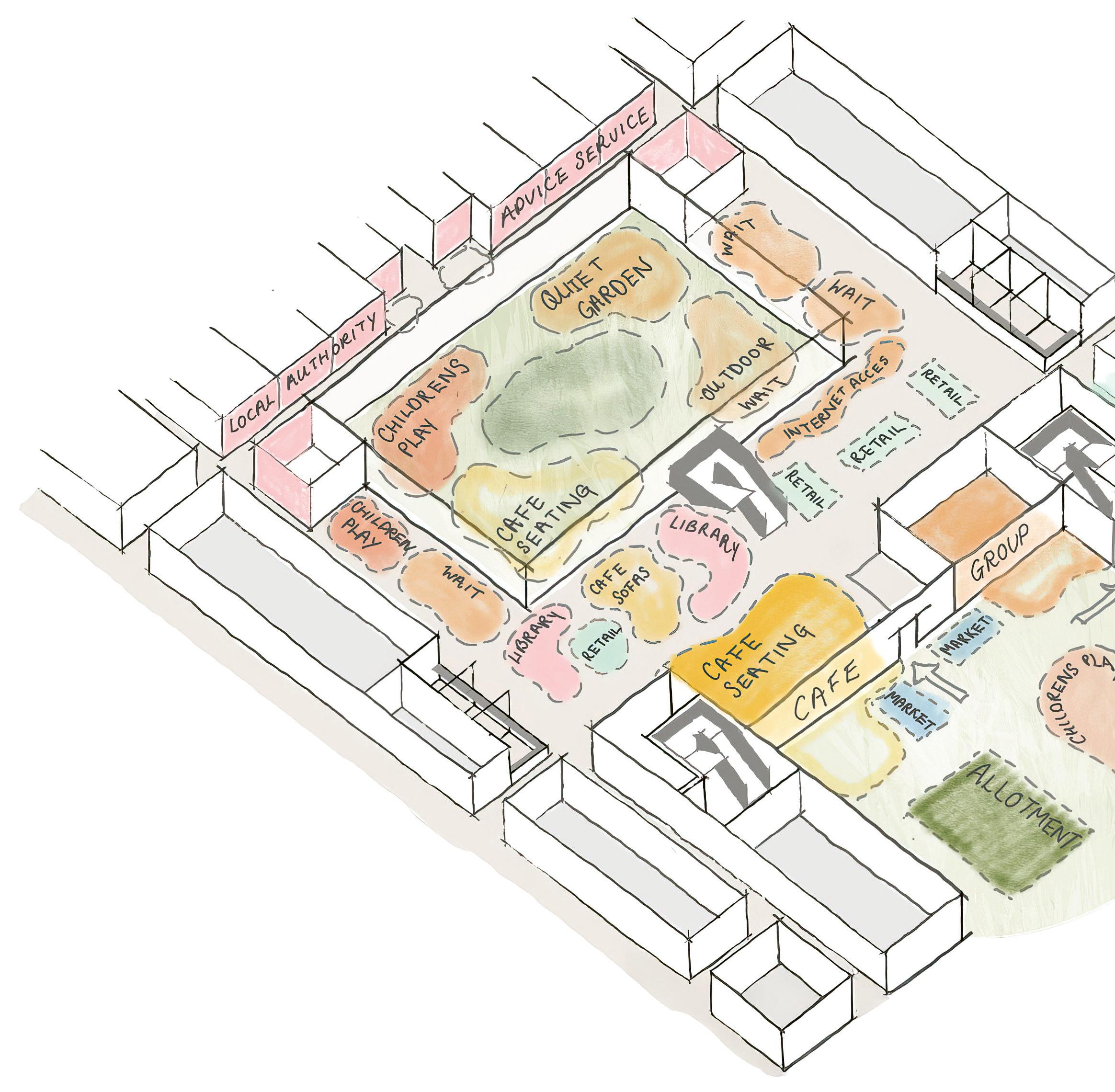
Cavell Community Health and Wellbeing Hub. © Medical Architecture
The relationship between architecture and landscape in healthcare design is long and enduring, with ever greater opportunities for an integrated approach.
Buildings battle to defy gravity and landscapes flow with gravity. If the enormous effort of raising a building is to be made, then it must at least be beautiful, and enable designers to acknowledge the former space and place that the new building now occupies – that expanse between earth and sky. It will also need to address any disturbed residual landscape that remains after such an intervention, providing a new context for future designers that is both healing and regenerative.
Healthcare buildings have historically been places of retreat, where concentrated resources of skilled professionals and medical equipment meet in one specialised facility, away from the front line of daily life. The caravanserai in the desert or the asylum on the edge of town are enduring examples of buildings offering excellent therapeutic recovery pathways using managed landscapes. More recently, healthcare buildings are frequently built in crowded city centres, embedded in these densely populated areas to provide dedicated space for emergency care. Their integration with the surrounding landscape is equally necessary for wellbeing, healing and recovery.
Healthcare buildings have historically been places of retreat, where concentrated resources of skilled professionals and medical equipment meet in one specialised facility, away from the front line of daily life.
When an earthquake and fire destroyed much of San Fransisco in 1906, 40,000 people were sheltered and treated in a tent city set up in Golden Gate Park. The Park was an extensive managed landscape akin to Central Park in New York – providing a breathing space within the densely populated city sprawl. This temporary canvas city was remarkable in terms of the successful healing outcomes it produced, as measured at the time. Whether this was a result of the beautiful parkland setting or the military efficiency of a team of public health professionals is unclear. Regardless, the abundant beneficial effects of such an open, natural space within the heart of the city provides an illuminating, if unexpected, example of quality landscape in healthcare design.
Daylight and fresh air ventilation are the major pre-occupations of designers for healthcare. This is where the interrelationship of building and landscape has mainly been manifested through the inclusion of framed views and openable windows. The ‘Nightingale’ ward and the courtyard plan of the Nucleus template hospital, or the airing courts for patients in secure environments, are classic examples that recognise these fundamentals for health. Today, NHS Health Building Notes and Health Technical Memoranda offer guidance on standards to enable designers to engineer each type of healthcare environment in a more prescriptive way. BREEAM has also set much higher standards for the integration of landscape for health and wellbeing, and the Net Zero Carbon Building Standard has recently been mandated by the NHS for procurement of public buildings for healthcare. The climate emergency has also brought a much greater appreciation of the value of regenerative design.
Healthcare is often divided into sectors of primary, secondary and tertiary. Primary care GP practices, pharmacies and dental clinics tend to be of a domestic scale and distributed widely in residential and small town high streets. These facilities are modest and accessible and their relationship to the landscape tends to be similarly modest, perhaps with a front garden or some potted indoor planting.

There is a current trend by Integrated Care Boards to federate these services into health and wellbeing hubs that pull in certain secondary (community) minor surgery treatments and, in some cases, diagnostic imaging and therapy services. The aim is to keep people well, in their homes, and out of acute medicalised care situations for as long as possible. Such buildings become de facto neighbourhood community centres, presenting an opportunity for bolder integration of landscape and healthcare architecture. These facilities are welcoming and within walking distance for patients, perhaps with a café and gym, and social spaces that spill out to a garden for social prescribing activities. They might also be Passivhaus design accredited and flexibly occupied during their long lifespan. Key to their success is their appeal as both a destination and a place to work, with excellent air quality and visual delight provided by the landscape context, both external and internal.
Secondary care is in flux too, with district general hospitals being repurposed as treatment centres, perhaps losing their Accident and Emergency capability if another centre is within striking distance and providing elective and ambulatory care for minor injuries instead. They may also provide less critical care in favour of more rehabilitative or ‘step-down’ care. Longer stays and an increased risk of dementia as people live longer points to the need for less clinical and more therapeutic environments, with attractive views out and accessible outdoor space. Here there is an opportunity to recover lost courtyards and interstitial spaces to reinstate the garden lungs that were conceived in the older Nightingale or Nucleus models but were often infilled to provide clinical space.
Tertiary care requires specialist, highly bespoke facilities. Such buildings have tended to be deep plan and multistorey, within or near city centres, and well serviced by transport and energy infrastructure. Seen as acutely clinical and highly medicalised, their functional requirements have tended to override more therapeutic considerations. However, there is now a greater recognition that the feel of a place has significant value in terms of staff recruitment and private customer satisfaction. This has led to more emphasis being placed on designing excellent staff facilities with attractive outdoor breakout spaces and open views to nature where circadian rhythms can be reinforced.
Landscape opportunities are even greater for the design of mental health facilities. These range across primary, secondary and tertiary care, from small Child and Adolescents Mental Health Service (CAMHS) day centres to secure forensic psychiatric hospitals. When invited to participate in co-design sessions, patient advocates and service users often reflect on the value of accessible nature, both physically and visually, when they are unwell and at their most vulnerable.
Whether these gravity-defying healthcare buildings are densely urban, suburban, coastal or rural, their occupants will always benefit from a thoughtful and sustainable reintegration into the landscape or cityscape which they have disturbed.
Accessible gardens also relieve boredom for long-stay service users and allow opportunities for quiet reflection for staff and patients alike. Much has been written on the ways in which gardens nourish the mind and entertain all the senses, helping to reduce anxiety, improve sleep patterns and speed up recovery.
Whether these healthcare buildings are densely urban, suburban, coastal or rural, their occupants will always benefit from a thoughtful and sustainable reintegration into the landscape or cityscape which they have disturbed.
Bob Wills is a Director at Medical Architecture’s London studio. He has 30 years’ experience of healthcare design and has played a key role in the delivery of various large-scale mental health and acute health projects.








