5 minute read
Interdependence Helped by Integration

from Hospital Reports – Improving Operating Room Efficiency and the Role of Digital Technology – Barco

Peter Dunwell, Medical Correspondent
For successful surgery outcomes, people and technology have to work together and the technology needs to make the work more effective
In the two preceding articles, we have looked at some of the technology aspects of surgery and work in the operating theatre. But machines, even robots and guidance systems, are no more than tools. At the heart of any surgical procedure are people: the patient on whom the operation is being performed and the team who are carrying out the surgery. The comfort of the team, especially of the surgeon, will impact the way they work.
Human Factors in Surgery
As in any aspect of healthcare, in the operating theatre, patient safety is the foremost consideration and it is also a key driver of processes. As BMC explains in ‘Patient safety in surgery’16, “The surgical environment must be considered as HRO [High Reliability Organisation], therefore, it demands a high level of standardization and safety processes in place with redundant system to decrease errors and human mistakes.” For surgery, part of that safety consideration is addressed in the pre-operative assessment during which is, as ‘Teach Me Surgery’17 explains, “… an opportunity to identify co-morbidities that may lead to patient complications during the anaesthetic, surgical, or post-operative period.” continuing to add that imaging is an important part of the assessment which the surgeon will use during the procedure.
Given the complexity of almost any surgery, it will come as no surprise that stress is a factor affecting performance and outcomes. The American Journal of Surgery18 confirms, “Surgical adverse events persist despite several decades of system-based quality improvement efforts, suggesting the need for alternative strategies. Qualitative studies suggest stress-induced negative intraoperative interpersonal dynamics might contribute to performance errors and undesirable patient outcomes. Understanding the impact of intraoperative stressors may be critical to reducing adverse events and improving outcomes.” The causes of such stress will vary and are often the same as in any workplace as Europe PMC suggests in ‘Conflicts in operating room: Focus on causes and resolution’19 , “The operation theater (OT) environment is the most complex and volatile workplace where two coequal physicians share responsibility of one patient. Difference in information, opinion, values, experience and interests between a surgeon and anesthesiologist may arise while working in high-pressure environments like OT, which may trigger conflict.”
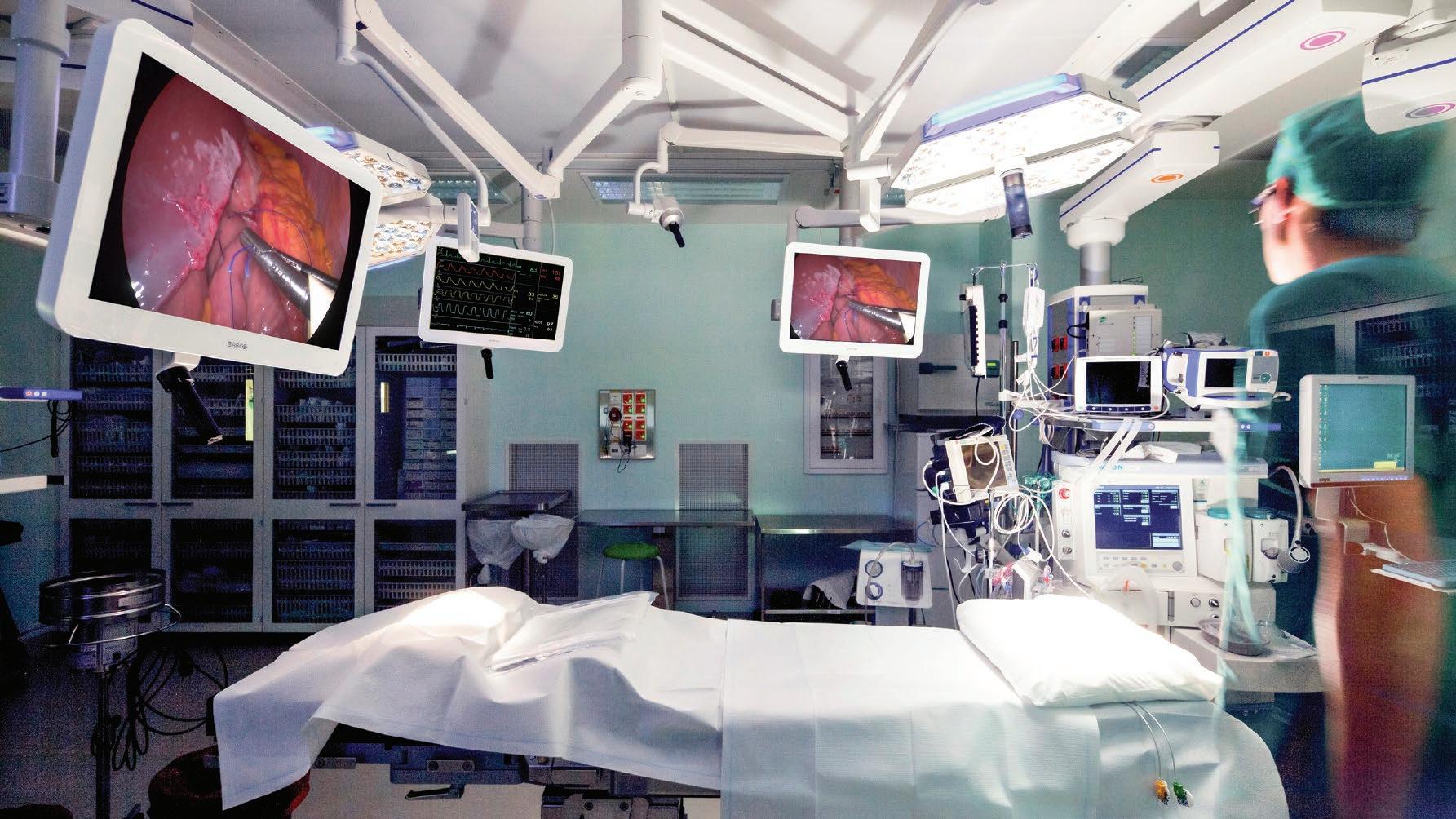
Stress in the operating theatre can also derive from factors specific to the equipment. We have mentioned in previous articles the problem of surgeons having to look up from their hands and the operation site in order to view instruments or images, and that can be both physically and mentally stressful.
Other human factors would include eye strain and eye fatigue which can often be caused by light quality; as obp20 points out, “One of the most notable effects of poor illumination on surgeons is eye strain and fatigue. Too much lighting is likely to fatigue the surgeon’s eyes and cause glare. Such adverse effects on the visual performance of the surgeon could lead to incorrect assessments and errors. Proper surgical lighting should provide the right amount of illumination and the correct patch size for surgery.” But it isn’t only lighting that can lead to eye strain for surgeons. NVision21 highlights a problem that is very much of our age, “Computer vision syndrome (CVS) is a condition caused by using digital displays – including computer monitors, laptops, tablets, e-readers, and smartphones – for too long without a break, without blinking enough, at an improper distance, or before sleep. Symptoms include dry eyes and headaches, along with other kinds of strain that lead to overall fatigue.” That is something with which every reader will be familiar but add to that the pressure of performing a complex and intricate procedure on the success of which a patient’s welfare depends and you can see how anything that can reduce the strain will be a very positive contribution to good outcomes.
Finally, the use of 2D imaging, while helpful, brings its own problems. Sage Journals22 explains, “Minimally invasive surgery (MIS) poses visual challenges to the surgeons. In MIS, binocular disparity is not freely available for surgeons, who are required to mentally rebuild the 3-dimensional (3D) patient anatomy from a limited number of monoscopic visual cues. The insufficient depth cues from the MIS environment could cause surgeons to misjudge spatial depth, which could lead to performance errors thus jeopardizing patient safety.” In other words, a 3D image will offer a lot more useful image with which a surgeon can work.

Challenges Need Solutions
So, we’ve managed to identify a number of challenges to the performance of surgeons and some of those challenges relate to the increasing amounts of equipment used in the operating theatre and the associated infrastructure (cables, connections, etc.) that it needs in order to operate and to deliver a range of information to the working surgeon. But what might be the solutions that can address those challenges? One new idea that promises much is to apply IP (Internet Protocol) solutions built on the IP network to improve the quality as well as the flexibility of the network. Whereas traditional AV solutions are fairly static and resistant to new video standards, IP solutions are extremely flexible. They require just one universal cable to distribute any audio, video and data signal.
As well as simplifying the physical complexity of the operating theatre, IP solutions can facilitate integration of services. Steris Healthcare23 explains, “An OR Integration System is designed to simplify and streamline the OR by consolidating data, access to video, and controls for all of these devices at a central command station, allowing the surgical staff to perform many of their tasks efficiently without needing to move around the OR. OR Integration also commonly involves suspending monitors and imaging modalities within the OR, removing trip-hazards caused by cabling and allowing for easy access and visibility to surgical video.” Keckler Medical24 sums up, “By putting comprehensive patient data into one efficient platform that works in existing environments and across multiple disciplines, Operating Rooms Audio/Video integration systems can help hospitals around the world lighten the load on surgical teams, improve Hybrid Operating Room workflow and decrease OR downtime.”
Over 70% of nurses surveyed said they preferred syringes where hands and fingers stay behind the needle area when activating the safety mechanism, and where the syringe is permanently disabled after the safety mechanism is activated