7 minute read
A Steady Hand


The use of robotic-assisted surgery has picked up quickly in recent years and the practice provides benefits to surgeons as well as patients
BY KAYLA PRASEK
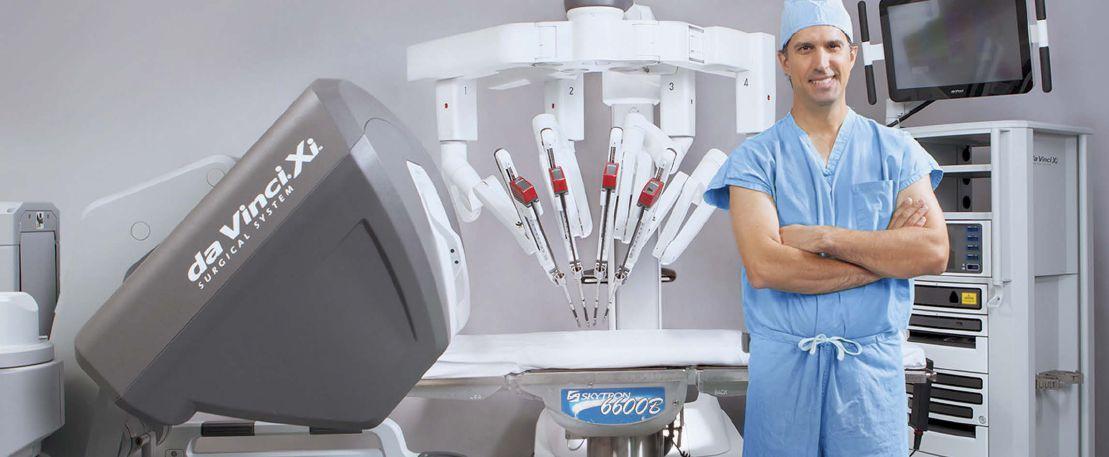
When Drs. Farhan Khan, Scott Johnson, Curtis Peery and David Maziarz head into the operating room, there’s a good chance they’ll be doing a robotic-assisted surgery. The da Vinci Surgical System — the system used nationwide for this type of surgery — was approved by the Food and Drug Administration in 2000, but its usage across various types of surgeries has increased considerably in the past year, the doctors say. The doctors also say the benefits of robotic-assisted surgery for both the surgeons and patients make it the preferred choice over laparoscopic and traditional open surgery.

The da Vinci robot is the only one approved for use in the U.S. and is used all over the world. To operate on a patient using the da Vinci, the patient is put under general anesthesia. The surgeon then makes three tiny incisions and preps the patient for surgery. The surgeon will complete the surgery sitting at a console, from which he or she controls the robot. A nurse practitioner stays next to the patient and the robot to switch out tools throughout the surgery. Khan, director of robotic surgery and a urological surgeon at Essentia Health West Region, says he is “away from the table but performing the surgery. The robot is the tool I use to perform the surgery.”
Avera Health, headquartered in Sioux Falls, S.D., introduced robotic-assisted surgery in 2009. Since then, it has “become one of the gold standards for safe surgery,” says Sandy King, director of operative services at Avera McKennan Hospital and University Health Center in Sioux Falls. “Most laparoscopic surgeries are now done robotically.” King says robotic-assisted surgery has reduced the trauma to the patient’s tissues and muscles, thus reducing healing and recovery time and blood loss. Patients also have considerably less postoperative pain and can get back to their normal, daily activities much more quickly. Patients also generally require fewer pain medications and are subject to lower risk of infection, King says.
“Over the last year, we’ve seen general surgery explode with the use of the robot,” King says. “It extends into almost every surgical specialty. This is the standard in training.” King says one in five surgeons in the U.S. are da Vinci-trained, but that jumps to 100 percent in colorectal surgeons.
Urology
When the FDA first approved the da Vinci, it was used primarily in urological surgeries, Khan says. “Urology has been at the forefront,” he says. Khan says any surgery that can be done laparoscopically can now be done robotically because the robot provides more magnification so the surgeon can see better and it allows the surgeon’s movements inside the abdomen to be more precise. “We’ve basically taken a step forward and made instruments that have a lot of movement. It allows me to be more stable, while the trauma the patient experiences is less.”

In urology, the da Vinci can be used for prostate, kidney, bladder, adrenal and testicular cancer, lymph node removal and benign adrenal gland tumors. It can also be used to fix bladder and kidney reflux in children who are born with an obstruction in their kidneys. In rare cases, it is used to remove kidney stones in unusual locations.
“This is the trend moving forward,” Khan says. “We are moving away from laparoscopic surgery. In 99 percent of prostate cancer cases, surgery is done robotically. The robot makes the surgery even easier to do.” Those patients, who previously had two- or three-day hospital stays, now go home the next day.
Kidney surgery used to require large incisions but robotic-assisted surgery has changed that as well, Khan says. Khan is the only surgeon in North Dakota doing robotic partial nephrectomies in patients with kidney cancer. “We used to remove the whole kidney. Now, I can just take the tumor and leave the rest of the kidney. It must be done in 30 minutes, which makes it the ideal type of surgery for the robot.”
Gastric Bypass
Peery, a surgeon with Sanford Surgical Associates in Sioux Falls, S.D., mainly uses the da Vinci for bariatric and hernia surgery. He has been using the robotic system for more than 10 years.
“Ten years ago, no one could tell me how to use it, but I really believed in the technology,” he says. “I could see it could do the precise, delicate techniques you can’t do in laparoscopic surgery, so I found it most useful there.”
Peery says early stages of the da Vinci didn’t allow for a very wide range of surgeries, as the system was best for surgeries in a confined space. “Over the years, general surgery had less use for it because we do such a wide array of surgeries. The newer models are much more amenable to doing general surgery, so we’ve been able to catch up.”
In the early years of robotic-assisted surgery, general surgery saw few surgeons using the system because their surgeries were so varied, Peery says. “In the last year or so, we’ve seen a huge increase in general surgeons using the robot. In the Sioux Falls area, there’s been almost a four-fold increase in general and bariatric surgery using it. It took them longer to learn how to use it well and understand how it can be used.”

While Peery notes the main benefit is a speedier recovery time, he says the biggest change in his practice is in weight-loss surgery. “In 2013, I switched back to doing only robotic-assisted weight-loss surgery and increased my outcomes in every area. The number of my patients being admitted to the hospital and needing more surgeries is much lower.”
Gastric bypass, which was always considered the more complicated weight-loss surgery but also the surgery that provided the best results, is now the best option, Peery says. “There’s less pain, less blood loss and less scarring. In my patients, there are essentially no leaks. Those feared complications are so low that it’s a very safe surgery. In the past, patients would choose the other weight-loss surgeries because they were safer but not the best option for them. Now patients can feel more comfortable with the best option to lose more weight, resolve more health problems like diabetes and keep the weight off longer.”
IMAGE: AVERA HEALTH
Cardiac Surgery
Maziarz, a cardiothoracic vascular surgeon at Sanford Health in Sioux Falls, was first exposed to robotic-assisted surgery in 2001 and has been using the da Vinci in his own practice since 2007. He primarily uses the robotic system to fix specific blockages in the heart’s arteries in a less invasive surgery. He also uses it in bypass surgeries in the major arteries and in surgeries to reduce stroke risks.
“We no longer have to open the chest,” Maziarz says. “I can’t do every person with the robot, but it would be nice if we could.”
Maziarz is able to make smaller incisions and reduce the impact of cardiac surgery on his patients when using the robot. This allows his patients to make an earlier return to full activity, usually about six to eight weeks after surgery. “The robot has cut recovery time in half, while also decreasing pain and the number of patients needing blood transfusions.”
Maziarz says there is still a fairly small number of cardiac surgeons using the da Vinci. “As we’ve seen improvements in the system, it has become easier to reach certain parts of the heart.” While he uses the robot about once a month, Maziarz expects to utilize it more as it continues to progress. “As technology improves and there’s more integration with the robot and the software, I see even more use for it. I’m always looking to reduce the impact of surgery on my patients.”
Gynecology
Johnson, a gynecological surgeon and chief of the surgical procedural division at Essentia Health West Region in Fargo, N.D., says robotic-assisted surgery provides a third minimally invasive option for surgeons. “If at all possible, we want to do a minimally invasive surgery. In gynecology, that means vaginally, laparoscopically or robotically. All have benefits you’ll use at certain times.”
Johnson says the advantages of robotic-assisted gynecological surgery include being able to make very fine motions and details with tools in the patient and the ability to work around the organs more easily. Johnson, who has been using the da Vinci for more than six years, primarily uses the robotic system for hysterectomies, ovarian surgery and gynecologic cancer surgery.
“If we look nationally at hysterectomies, 50 percent are still done through incision,” Johnson says. “The robot has increased the number done minimally invasively. Ninety percent are done vaginally, laparoscopically and robotically. The robot has brought the number of patients with large incisions down and moved the bar in what we can do for patients.”
Johnson’s patients who have robotic-assisted surgery are usually able to go home the day of or day after surgery, have less blood loss, are able to return to work sooner and have less post-op pain. “We continue to push the bar for minimally invasive surgery so as many as possible can be done that way, and the robot is an important piece of that,” he says.
Future
While not every patient is a candidate for robotic-assisted surgery, King says Avera has a “very robust robotic team” and calls it “another hand in cancer care.” The surgeon determines if a patient is eligible for robotic-assisted surgery on a case-by-case basis.
“There will always be some surgeries done traditionally,” Khan says. “But they’re always trying to make the system better. They released a new model a year ago and even more surgeries can be done with it. As robotics get more advanced and efficient, they may replace all laparoscopic surgeries. Who knows where we’ll be in 10 years, because we never thought we’d be here.”
Peery sees a point where telemedicine and robotic-assisted surgery could become integrated. “In medicine, a lot of things are changing because of technology. I can see a point where telemedicine and robotic-assisted surgery will cross paths and will continue to change how we view medicine.” PB
Kayla Prasek Staff Writer, Prairie Business 701.780.1187