33 minute read
Health, Safety, Environment and Quality

By Prasenjit Mohanta
There was 03 recordable personal injury under LTI submitted Fleet Wide during March 2021.
Advertisement
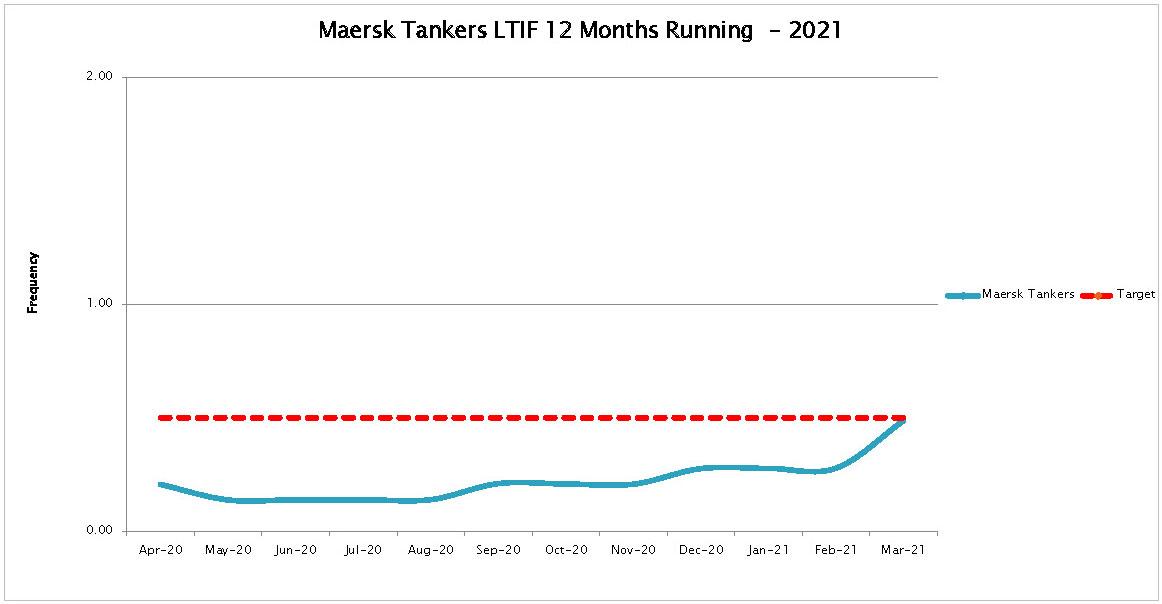
At the end of March 2021 MT safety performance (12 months rolling) was as follows:
12 months rolling YTD March 2021
LTIF 0.49 LTI 7 LTIF 1.08 LTI 4
TRCF 0.84 TRC 12 TRCF 1.90 TRC 7
During March 2021 - 5 external audits (ISM/ISPS/MLC) were conducted on board our fleet vessels.
Shore management vessel visits – as part of our commitment to visible leadership, we shall be publishing a list of vessels visited by shore management each month. Below virtual visits were undertaken during March 2021.
Umesh Shinde Maersk Caelum 02-Mar Madhav Kamath Maersk Stratus 08-Mar Madhav Kamath Roy Maersk 09-Mar Robert Elliot NightCrawler, Ex-Bro Designer 22-Mar Shashank Jahagirdar Robert Maersk 26-Mar Datharam Puttheguthu Eva Maersk 27-Mar Janus Auken Bro Nibe 31-Mar Peter Hawkin Maersk Mediterranean 31-Mar

Incidents
INC-8KQ-21-2 Bro Agnes 01/03/2021 Incidents Overboard pollution by yard / FERROL shipyard INC-O43-21-1 Maersk Erik 02/03/2021 Incidents RBD Palm oil on deck
ACC-O43-21-1 Maersk Erik 04/03/2021 Accident IP got hit by frame on the deck during darkness time and fell down on deck toward his left-hand side.
ACC-O46-21-1 Romoe Maersk 04/03/2021 Accident IP got hurt with twisted ankle during laying mooring lines.
INC-A5B-21-1 Maersk Capri 05/03/2021 Incidents Cargo Spill from Terminal at Tampico Mexico
ACC-U65-21-1 Maersk Kara 08/03/2021 Accident IP suffered injury in the area close to his right ear as he fainted in E/R workshop and hit his head.
INC-KB4-21-2 Maersk Maru 11/03/2021 Incidents
Windlass damage during anchoring operation in bad weather. ACC-KB4-21-1 Maersk Maru 12/03/2021 Accident IP got injured resulting to fractured wrist while working on the mooring winch for shifting of ropes. ACC-KH4-21-1 Henriette Maersk 14/03/2021 Accident IP while playing basketball twisted his knee.
ACC-4ZQ-21-1 Bro Nyborg 15/03/2021 Accident IP while climbing the ladder on a windy day hit his head against the mast ladder.
ACC-5Q8-21-4 Maersk Mediterranean 16/03/2021 Accident IP while preparing surface for painting stepped on coiled hose lost his balance and fell down.
ACC-198-21-1 Maersk Kate 16/03/2021 Accident
IP while making an attempt to stop the hatch from impact and tried to grab it but his hand got caught between the hatch and coming. INC-5ZQ-21-1 Bro Nibe 25/03/2021 Incidents Entering Danish Territorial Pilot Waters for anchoring without INC-L06-21-4 Hammerhead 30/03/2021 Incidents Port side Main engine (Azi pull) stopped suddenly.
BRO AGNES – 01ST MARCH 2021
Overboard pollution by yard / FERROL shipyard
Description/Sequence of events: At 12:05 on 1st March 2021 it was noticed that oil traces were there overboard (starboard side), same was immediately informed to the yard safety representative.
Investigation After investigation was discovered that yard workers open diesel line on deck and drain directly to the ship main deck 1-2 ltrs of diesel. Due to heavy rain all oil flow with rain overboard. The vessel protected by floating booms around all the time. The oil was contained by the oil fence rigged around the vessel and subsequently cleaned by Yard.
Underlaying / Root Cause: The shipyard personnel dismantled one pipe without informing the crew promptly. Language barrier could have played a role in this incident. Inadequate coordination between the shipyard personnel and the vessels crew. Shipyard personnel

did not inform the vessel crew and let the residual oil drain on deck.
Recommendation: Yard Manager assigned to the vessel must be present during coordination meeting and all plans for the day to be discussed in details. The scope of work on daily basis must be discussed on regular basis during the coordination meeting. Shipyard personnel on the other hand must notify the crew/officers if there is any pipe/or equipment to be dismantled. Extra ordinary meeting was held by the Master in the presence of all crew Officers emphasizing to be observant on the actions of the Yard personnel as obviously they are not keen on talking to crew likely due to language barrier.
MAERSK ERIK – 02ND MARCH 2021
RDB Palm oil spill on deck
Description and sequence of events. On March 02, 2021 while Discharging various grades of vegetable oil cargoes at Taman, Russia, Cargo of RBD Palm Oil spilled on deck from slop line drain valve.
Investigation The investigation into the incident has been conducted by the Master and the Marine Superintendent of the Maersk Erik. This has included a combination of review of near misses, document analysis, interviews and witness statements. Findings: The valve and hydrant cap of Slop Line drain were inadvertently opened and not checked. Failure to warn - There was no marking/stencil on the drain line indicating that it’s a drain for the cargo line.
Proper Risk Assessment and job plan for which all hydrants are to be opened and reported was missing. Inadequate compliance with company procedures. 06.404.01 - Cargo Operation Planning & Execution was not followed or executed, which states “Before, during and on completion of any cargo and deslopping operations, there are defined requirements for physical cross-checking of cargo system and line settings by at least two responsible deck officers. These checks shall include the settings of all valves, blanks, vents and over-boards; to verify their correct positioning according to the cargo plan;” Cargo system /
Valves settings were not checked prior to commencement of cargo operations.
Immediate cause Adverse weather conditions – As preparation for sub-zero conditions. Lines were to be drained, so as to avoid damage to ship’s equipment. However, wrong valve was opened. Failure to secure – Slop line cargo drain valve and hydrant cap were not secured. Inadequate warning system - There was no identification on the slop cargo line drain. Failure to follow rules and regulations – Cargo system / Valves were not checked prior to commencement cargo operations. Failure to follow rules and regulations – Two man check not completed.
Underlying and root cause: Inadequate Leadership and/ or supervision – Improper or insufficient delegation – Two Man check as required by 06.404.01 were not performed. Inadequate Leadership and /or supervision during adverse weather conditions – Risk Assessment and risk awareness that other valves and mitigation not done. Inadequate maintenance - There was no identification/ marking on the slop cargo line drain. Improper Motivation – Inadequate discipline- Cargo system / Valves were not checked prior to commencement cargo operations. Improper Motivation – Inadequate discipline – Two man check not completed. Recommendation: Extraordinary Safety Meeting was held discussing the incident. Drain valve was marked on deck and all other markings on the vessel to be checked to avoid any inadvertent opening of valves to avoid recurrence. Chief officer to prepare and share a detailed Risk Assessment for Winter precautions for review by Marine Superintendent. A Refresher training to be done and recorded for all deck-crew and the checklist of pre-cargo operation checks and contents of ShipNet ID 06.404.01 discussed.
Lesson learnt Risk awareness of inadvertent opening of wrong valves, while preparing the vessel for operation. Importance of marking/stencilling of equipment on deck. Importance of through 2-man check while lining up for vessel operations.
MAERSK ERIK – 04TH MARCH 2021
Personal Injury due to fall on deck
Description and sequence of events. On March 04, 2021 around 0500 Hrs Lt while Discharging cargo at Taman, Russia, IP fell on deck and suffered Comminuted fracture of the radius of the arm with displacement.
Investigation The investigation into the incident has been conducted by the Master and the Marine Superintendent of the Maersk Erik. This has included a combination of review of near misses, document analysis, interviews and witness statements.
Findings: IP went on deck, taking good initiative to check the progress of work and cargo parameters after his watch. However, the risk awareness was inadequate.

IP went on deck at hours of darkness and outside of catwalk/safety walkway without any personal communication or illumination device. Slippery deck – due to the presence of morning dew/condensation and possibly minor residue of palm oil cargo originating from the cargo tank squeezing activity two days prior to the incident.
Immediate cause Improper position of task - Improper use of catwalks/safety passages, not carrying personal illumination device during the hours of darkness. Environmental conditions – Presence of morning dew and condensation on deck, making it slippery.
Underlying and root cause: Inadequate mental/ psychological capability – Poor judgement. IP went on deck during the hours of darkness outside safety walkway and without personal illumination and communication device. Recommendation: Extraordinary Safety Meeting was held with the crew and the incident was discussed to avoid recurrence. IP completed the below safety refresher trainings, 0001 Personal Safety. 0002 Ship General Safety. Rapid Fleet Notification shared with the fleet vessels. Safety Alert on this accident will be shared with the fleet as part of Learning from Incidents.
Lesson learnt Hazard awareness and adequate attention to surroundings are key to prevent accidents Moving on deck with elevated longitudinal frames is unsafe, especially during the hours of darkness and should not be allowed Only safety walkways should be used for movement on deck, unless a particular tasks requires to go across decks.
ROMOE MAERSK – 04TH MARCH 2021
Personal injury while handling mooring ropes


Description and sequence of events. Personal injury with twisted ankle during laying mooring lines out on deck as part of arrival preparations for Port of Vitoria.

Immediate cause: A momentarily failure to observe surroundings before taking next step was identified as root cause.
Underlying and Root cause: Lack of awareness. Supervision in adequate. Latent hazard not identified not understood
Recommendations: To avoid recurrence, vessel has carried out a safety meeting and following was discussed with all crew to create awareness.
1. Discussed industry(Club/Class) documents on Slips trip falls with all crew members on board and also discussed safe methods to move about ship. 2. Few examples were discussed such as There could be particular challenges for example when tank cleaning veg oil tanks which may make the deck much more slippery than usual. A small thought during tool box meetings given to safe movement on board goes a long way to remind everyone to take care of their own safety. 3. It’s worth noting the comment at the end of one of attachments, “None of this is exactly ‘rocket science’; all might be thought of as simple seamanship and common sense, but the Club’s statistics confirm time and time again the absence of these precautions, and simple human carelessness, between them, really do cause enormous amounts of human misery and heavy claims.” 4. Briefed all crew about the important barriers (Tool box meeting, RA, briefing, PTW, company procedures, supervision, debriefing, etc) that should be used to avoid incidents accidents on board. 5. All crew were advised to follow safe working practices at all times and strictly comply to the company PPE requirements as per the PPE matrix. 6. Timely reporting of such occurrences/injury, etc during transit/travel during embarkation/disembarkation of the vessel or onboard so that appropriate corrective measures can be taken or arrange a doctor visit in cases of injury. 7. Continue Knowledge sharing & training during meetings/drills and exercises onboard about First aid, various injuries and its symptoms and actions to take. 8. Also please continue encouraging ship staff to observe various SMS safety tools to identify and report such issues.
MAERSK CAPRI – 05TH MARCH 2021
Cargo spill from terminal
Description and sequence of events. On March 05, 2021 around 0500 Hrs Lt while terminal personnel startd loosing nuts to remove blind from cargo arm. Same time Vessel personnel noted small dipping of cargo from the arm. After few second dipping stopped and Terminal personnel continue to release nuts to remove blind. Suddenly cargo start spraying around from loading arm, as blind was slack. Alarm sounded..
Immediate cause: According Pemex information, this spill was caused by an air bubble inside the loading arm.
Underlying and Root cause: The incident is purely due to shores fault and the vessel has no involvement to the cause of the spillage. Estimated amount of cargo spilled on terminal 2040ltrs

Recommendations: At every loading/discharging port, all draining of the loading arm will be suggested to be done at shore side or at drip tray onboard. It will be depressurized to make sure there is no pressure trapped on the line.
MAERSK KARA – 08TH MARCH 2021
Repairman fainted in ER workshop
Description and sequence of events. On 8th March 2021 at 09:30LT one of the engineer reported that Repairman fainted in E/R workshop and hit his head to the corner of the grinder's support frame. He suffered injury in the area close to his right ear. Immediately compresses applied to stop the bleeding. His face was washed with water and he become conscious. Injured person moved to ship's hospital where his wound was cleaned and bandage applied.
Immediate cause: Reason for fainting was unknown. it was just beginning of the day after rested weekend. Person was not showing any signs of alcohol or drug intoxication. Also, was not carrying out any heavy tasks/lifts. He was preparing to do some maintenance around the ER bottom platform, came up to the workshop to grab some tools and lost consciousness at that point.
Comments from marine assurance: Reason for fainting was unknown. it was just beginning of the day after rested weekend. Person was not showing any signs of alcohol or drug intoxication. Also, was not carrying out any heavy tasks/lifts. He was preparing to do some maintenance around the ER bottom platform, came up to the workshop to grab some tools and lost consciousness at that point. Condition including blood pressure and temperature was normal. First aid of cleaning and dressing the wound was done onbd. There was no requirement of radio medical advise or doctor visit.
On further queries, repairman responded as below: He had similar fainting at home once, but very long time ago (10 or 15 yrs ago). He is not taking any kind of medicines regularly for any known health issues.
As a precaution, condition was monitored for next few days. No abnormalities observed. The wound healed by first aid and continues to do normal tasks.
MAERSK MARU – 11TH MARCH 2021
Damage to the windlass
Description and sequence of events. Vessel was in ballast anchored at Rotterdam anchorage n5, at port anchor with 9 shackles on deck when she was called to proceed to pilot station Weather condition was rough, wind was 40kn and gusting above 50kn (Bf 8/9) Master took decision to heave up anchor based on his experience of anchoring in the same weather / winds conditions. Ch Off was called on bridge for toolbox meeting and risk assessment. It was noted that anchor team shall be ready to take on band brake and put crossbar down as soon as requested by Master or chain tension changed to long. For the reason of in time actions the team shall be positioned 1(Ch Off) Supervision, 1(AB) Windlass operator, 1(Pumpman) Band brake handling, 1(OS) Crossbar handling (Total 4 persons). On bridge was Master in conn, 3rd Off for OOW duties and AB at steering control. Ch Off was instructed to heave up anchor following the condition when the chain is moderate and going to slack and to apply bend brake when chain going to long. Vessel was moved by ME towards wind / anchor position (no time record) and at 0848LT start heaving anchor. By 0855 come 7sh on

deck and at 0900 was 6shackles on deck. At 0905 it was reported 4 shackles on deck and " not able to continue heaving" Next report was "gear wheel is broken"
Immediate cause: When big swell lifted bow out of water a strong hug made a downward force acted upon chain try pull chain into water. This strong force was transmitted to main gear wheel via chain gipsy / main shaft - same time hydraulic motor was locking/heaving it hence preventing this movement - at same time brake was disengaged and crossbar was lifted due to try heaving anchor home. Hence two opposite torsional forces acted upon main gear wheel which the wheel was not able to withstand, result it broke.
Underlying and Root cause: Heaving anchor in severe weather conditions. Effect of heavy swell was not considered in Risk Assessment. Readiness of crew to work in heavy weather condition was assessed incorrectly.
MAERSK MARU – 12TH MARCH 2021
Personal injury while handling mooring lines
Description and sequence of events. Vessel was at anchor in Rotterdam waiting for loading. On 11 March 2021 she was asked to proceed to Pilot station for berthing. While picking up her port anchor the big windlass gear just sheared off and whole gear wheel got collapsed. Vessel was not able to heave her anchor up. Later due to heavy weather condition and also commercial benefit in upcoming voyage it was decided to let go her port anchor from bitter end and proceed to repair yard to avoid delays with upcoming voyage. Vessel then proceeded to ROG repair berth for repairs. The big gear wheel for windlass was not available in Rotterdam or nearby areas; hence makers advised to use the wheel from one of the aft mooring winches and install on the port side forward windlass which was important to be fixed. Before the aft winch could be dismantled it was to be made free from the mooring line. The vessel was made fat to berth using all the aft mooring lines. In order to reel out STBD mooring line, the line had to be made fast on the bitt. Hence weight was taken on the stopper and then slacked line was secured on nearby mooring bitt. After the line was secured, the line was being continued to slack to reel out from the drum but the mooring line got caught in the gap plate between the storage and tension drum and then due to slight tension the line slipped out from the plate gap causing sudden upward movement which hit the 2/Off palm causing right hand wrist injury.
Immediate cause: Inadequate leadership and/or supervision – No work planning done, no toolbox, no risk assessment for repair job in the yard. Inadequate Problem detection / Situational Awareness by all involved. With crew complement onboard overlooked residual fatigue for the period of past seven days of operations.


Inadequate knowledge/experience – Painter was called to operate the winch. Same task was assigned twice causing double work and desire to complete the work asap. Mooring design flaw as mentioned in findings above not captured anywhere/RA for crew to be familiar with the arrangement.
Underlying and Root cause: Company Standards policies, or Administrative Controls (SPACs) not used – Enforcement issue Risk Assessment / toolbox meeting was not completed prior starting the task. Crew involved were not prepared for shipyard work neither mentally not physically while coming directly from incident scene to repair berth. Unauthorised person (Painter) was called to operate the winch. No rest hour planning / Fatigue management taken into account.
Recommendation: Extraordinary safety meeting conducted with all crew to discuss the incident and lessons learnt. Seagull training for Risk Assessment and Safe Mooring Practice to be completed by all crew. Risk assessment for mooring operation to be reviewed and necessary hazards pertaining to design flaw incorporated to prevent such accidents in future. Crew training to be carried out to ensure they are familiar with setup. Master & C/Eng to randomly take rounds of deck / engine room, also if possible, to attend/participate during Toolbox meeting to verify enforcement / compliance with company safety procedures. Further compliance to be verified during the next Internal Audit of the vessel by Shore
Superintendents. Vessel next Internal Audit to be carried out with add focus on implementation/compliance of company safety tools and procedures onboard.
Lesson Learnt: Crew to be mentally and physically prepared for shipyard work especially when this is unscheduled visit due to some incident or emergency. Rest hour planning/management to be done and any challenges should be immediately reported to shore management for support. Senior Management onboard should always discuss work planning /resources management with the repair yard team. Risk assessment and toolbox meeting should be conducted with all involved without fail. Always be situational aware of the surrounding work area.
BRO NYBORG – 15TH MARCH 2021
Injury on the head
Description and sequence of events. Officer had a head injury. His job was to climb the Radar Mast to take pictures for ELMT of the radar scanners name plate. While climbing up his helmet was taken by the wind and in the attempt to recover the helmet he hit his head against the mast ladder. The ladder is sharp metal and it caused a small scar. He has been given first aid and Radio Medical has been consulted. Weather: Wind force 5 and light rolling in the sea at anchor.
Underlying and Root cause: Helmet taken by the wind when climbing the radar mast ladder. Strong wind was not considered as hazard for the specific job.


Sum up: Safety meeting conducted the 16th March 2021 for all crew. Use of fall arrest demonstration conducted after this meeting and fall arrest equipment received check by chief officer and additional supplies will be on the next safety equipment PO nothing found to be needed urgent. Have made 1Q/2021 Safety Initiative improved helmet suggestion with 2 securing points for the chin strap on each side and mail forwarded the 22nd March 2021 with safety helmet options from the internet which would avoid helmets blow off by the wind.
MAERSK MEDITERRANEAN – 16TH MARCH 2021
Wrist injury due to trip / fall
Description and sequence of events. During paint preparation, deck flushed with fresh water and blown with air to remove salt formation. In this process painter step on coiled hose lost his balance and fell down. To avoid falling painter put his right arm in front of him on stiffener and he suffer wrist sprain. Weather conditions / Slight Sea / Wind SE x 4 Was the deck was slippery due to water / No Was the IP stepping on the deck longitudinals while moving on the deck / He tried to step over logitudinals Was vessel rolling at the time / No / Vessel at Houston outer anchorage PPE worn by the IP / As per Company Matrix.
Underlying and Root cause: Stepped on the coiled hose and lost balance. Lack of situational awareness. Arm position simulated at the time of fall
MAERSK KATE – 16TH MARCH 2021
IP Forearm Fracture while securing WBT hatch
Description and sequence of events. At 2000 Hrs on March 16th, 2021 while alongside at West Thurrock, UK; the IP was securing the Water Ballast Tank hatches prior to departure. The IP removed the securing pin to 1P WBT and the hinged hatch cover fell by gravity. The IP made attempt to stop the hatch from impact and tried to grab it, but his forearm got caught between the hatch cover and coming. Weight of the manhole lid caused a compression injury to his right forearm. IP was later found to have fractured forearm, and repatriated home.




Immediate / Root cause: 1. The IP’s Ulnar fracture was caused by blunt force impact to the forearm by the steel hatch cover falling. The IP’s forearm was caught between the cover and the hatch coaming. 2. The IP had completed this same task many times. An element of job complacency was possible. 3. There was some coiled razor wire stowed within close proximity (70cm) of the hatch. The razor wire was not covered. The close proximity of this hazard likely caused the IP to assume poor bodily positioning for securing the hatch. 4. The IP was doing the task alone and did not have a second man assisting. 5. Inadequate design ergonomics of the hatch cover. There is a single handle placed on the centre of the hatch cover. Once the cover is open and locked in position, this handle is 1.48m height from the deck. For short statured persons to grasp the handle while closing the hatch would require raising their arms above shoulder height. 6. There was no risk assessment conducted by the vessel for opening/closing these hatches. 7. The IP had been onboard since June 2020 (10 months) and was due to sign-off and recently advised no reliever was available. Mentally he might have not had full presence of mind due to anticipated sign-off having been postponed.
Root cause: 1. Inadequate Task Planning a. No risk assessment had been conducted for the task b. No method / procedure had been developed for the task 2. Inadequate hatch design ergonomics a. Handle position unsuitable for short stature individuals
Recommendations: Vessel to conduct ship specific Risk Assessment for opening and securing WBT hatches. Vessel to develop ship specific procedure for operating the hatches which shall consider manpower and aids to assist with safely lowering the hatches such as rope tails which have been tested out. A safety sign/warning notice should be placed on each hatch of this construction type. Findings to be shared with all sister vessels. To be discussed next safety meeting onboard. Company Naval Architect to be consulted for potential design solutions.
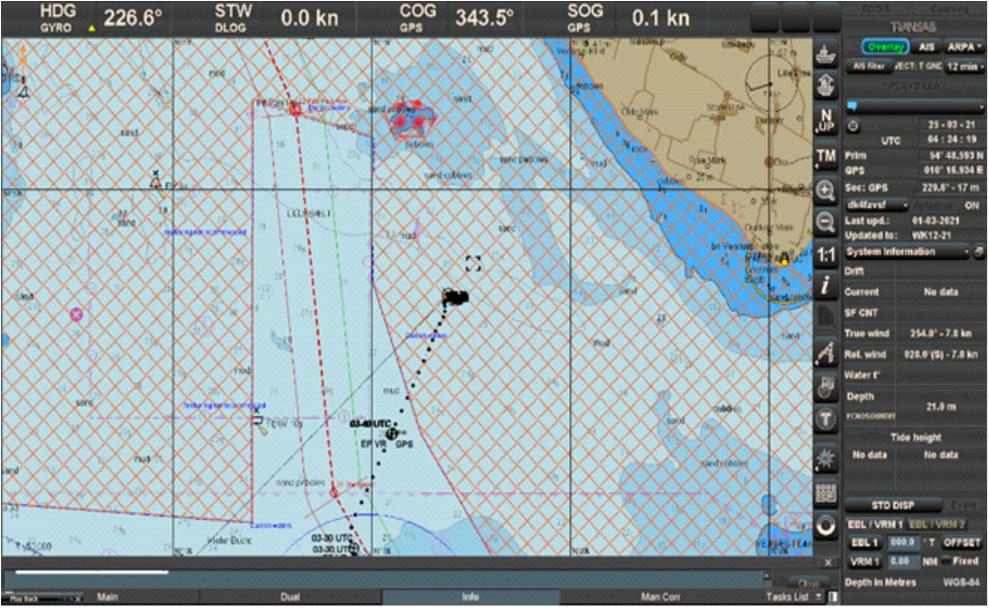
BRO NIBE – 24TH MARCH 2021
Entering Danish Territorial Waters without Pilot
Description and sequence of events. Vessel had departed from Saint Petersburg with a draught of 7,90m FWEK on March 22nd 2021, loaded with a cargo of 12534 mts of Vacuum Gas Oil for Charterer Litasco SA. Destination was Amsterdam for orders via Kiel Canal. Destination was later changed to Ensted Vaerket, Aabenraa, and upon entering the waters South of Langeland and Aeroe, the vessel crossed into the Danish Territorial Water Region and proceeded to drop anchor 3,5 nm from the Coast of Aeroe awaiting a vacant berth at Ensted Vaerket. This was done without employing a pilot, which was a violation of the Danish Pilotage Act – Section 4.
Immediate / Root cause: Basically poor voyage planning and poor preparation for the port call in the way that master was too quick to jump to the easy conclusions.
Root Cause: The root cause of the incident was identified as: Lack of time to reconsider all decisions. Final discharge orders arrived late PM at the end of a busy work day, where crew changes and Class attendance had been high on the agenda thus the new voyage plan and new port call arrangement
that had to be decided upon was not given the proper attention. Lack of proper planning.
The master should have paid much closer attention to the information in the chart, and studied the information in Admiralty Digital
Radio Signals 6 in more detail. Misunderstanding Operator’s Internal procedures. The wording: “You are therefore
NOT to order the pilot yourself but to forward your requirements to the agent for the specific port call” stopped any potential attempts at ordering a Dan Pilot from Great Belt South Pilot
Station. Wrong Interpretation of Agent’s information.
The words “Lodspligtig from Poels Rev” led to the belief that vessel could enter the area freely without a pilot on board. The agent failed to inform the vessel properly.
The pre-arrival information mail template sent out by the agent could have contained detailed information on the Danish Pilot Act and what that implies for the area in question.
Follow-up Corrective Action: The incident is to be shared with the Fleet high lighting the importance of Compliance and proper voyage planning.
Preventative Action: Maersk Tankers Order Letter and ShipNet Procedure 05.260.03 to be updated to explain in more detail, preferably with a map insert of Denmark and the Territorial waters to help guide mislead masters.
HAMMERHEAD – 30TH MARCH 2021
Port side Main engine (Azi pull) stopped suddenly
Description and sequence of events. On 30th March at the port of Falmouth, Port side engine (Azi pull) of Hammerhead stopped during maneuvering in Falmouth anchorage. Vessel still safely carried out operation and sailed to the discharge port with STBD engine.
Immediate cause:

Automatic shutdown by the monitoring system.
Root cause: Port side main engine suddenly stopped during maneuvering in Falmouth anchorage, Gear rim for starter and RPM monitoring shift from normal position. RPM monitoring sensors - 3 pcs damaged.
Action taken Vessel was safely maneouverred to Antwerp with one pod. Remote touble schooting was carrid out with the manufacturer. Emergency spares were connected to the vessel. Shore service team attended the vessel to rectify the situation.
Near misses and condition
Scenario 1 While making fast the loose rope aft , the rope stopper was used to take weight to make figure of 8 on the bollard close to the centre fairlead. during slacking the loose rope from the winch due to the less space between the stopper and fairlead, the stopper got stuck between the fairlead and the loose rope, the stopper couldnot be removed due to weight on the weight on the loose rope. This was due to the less space between the stopper and the centre fairlead which lead to this occurence. The stopper should have been taken at the further Bollard, which would have provided more space.
Scenario 2 During lifeboat drill, it was observed that the shackle arrangement for FPD on the lifeboat is in reverse position and the movement of the shackle is disabled. Quick reconnection of hooks while lowered in the water, Improper use of equipment, Under stress
Scenario 3 During routine rounds, engineer found LO metal pail bottom to be damaged and leaking to the floor, creating a slippery surface in LO store. The LO was transferred into another clean pail, and properly labeled. LO Store was cleaned of any traces of oil. The subject LO drum was one of the older stocks remaining, rest of the drums checked which are comparatively new, same received in New York.
Scenario 4 One of the fleet vessel experienced challenges while taking in ballast water via the BWTS during cargo operations where the water was noted to be dirty during the discharge operations in Quanzhou, China. The uptake was done with the BWTS by-passed. There after the vessel proceeded on a trans pacific voyage to Vancouver, BC and during the voyage carried out Ballast Water exchange without to use the Ballast Water Treatment System, not meeting the D-2 standards.



The pre-arrival Ballast water report was sent out to the Canadian Authorities and same was acknowledged without any additional comments by the authorities. However, during the PSC inspection in Vancouver, the visiting PSCO highlighted non-use of BWTS and issued a deficiency. Though, after discussion, the vessel was permitted to discharge the ballast on board via the BWTS, this could have also led to vessel being not permitted to discharge the ballast at the port, leading to other implications.
Scenario 5 Another fleet vessel experienced challenges while taking in ballast water via the BWTS during cargo operations where the water was noted to be dirty during the discharge operations in New Orleans, USA. The uptake was done with the BWTS by-passed. During the voyage, vessel was instructed by the office to carry out Ballast Water exchange using the Ballast Water Treatment System, as vessel crew were not aware of action required to be taken due to the lack of familiarity with relevant section of the BWMP. As per Class approved BWM Plan, vessel is permitted to by-pass the BWMS in places with challenging water quality, (highlighted below, section quoted from vessel’s BWMP). However, the exchange needs to be done via the BWTS, which was also not done in Scenario-1 .
Basis above cases, following recommended:
Ensure strict compliance with the D-1/ D-2 standards as required by your Int. Ballast Water Management
Certificate. Pls inform office and authorities in case there are any challenges and/ or possible noncompliance immediately for assistance. Relevant entries to be made in the Ballast Water
Record book and vessel’s Deck log. Ensure that the BWTS is well maintained and filters cleaned prior to arrival into ports where the water is expected to be dirty/muddy to ensure that vessel has done the due diligence. Familiarization of responsible crew i.e. those involved with BW management on-board vessel with the contingency measures within the BWMP. Please convene a management meeting to discuss above and reiterate the contingency measure as per BWMP if BWTS is not functioning as required.
Scenario 6 The accommodation stair case have antipiracy grills which are held in open position with bolts. This bolt is so badly corroded, if it breaks and the grill falls on somebody, they will be severely injured.
Scenario 7 While normal monthly testing of Engine Room local water mist fire fighting system, it was noticed that the water mist was not released in any of the sections. It was observed that after activating a particular section of water mist system, the isolation valve for that particular section was opening. The mist release alarm was sounding, but the water mist pump was not starting, thereby not possible to actually activate the water spray for fighting the fire of particular area. On further investigation it was found all concerned relays were operating, but the water pump starting signal was not available at the pump starting panel.
Scenario 8 During loading operations in Swinoujscie the 2 P/S cargo tanks were loaded to about 96 % (final ullages: 1.05 m and 1.07 m) . The 95% HLA did not activate, though this was expected to happen at a corresponding ullage of 1.18 m. Upon completion of the discharge the 2 P/S high level alarms were removed from position and probes inspected, cleaned and


tested. No physical damages were found. A test was carried out by submersing the alarm probes into a bucket of water and the alarms came. Further into the investigation it was noticed that the above mentioned HLA were engraved with 1P and 1S and corresponding serial numbers. The engravings on some other cargo tanks HLA were checked and found: for 1P Drain Tank , 1S 5P , 4S Slop P etc.
Scenario 9 On routine safety rounds, It was observed hissing (air leakage) sound coming near engine room ventilation fan no. 1, On investigation found copper tube union thread gave away leaking air. This copper tube carry air for damper closing from remote in case of emergency. Air leaking from copper tube pipeline leading to damper closing arrangement. Ermeto coupling thread gave away due to vibration. Thread worn out due to age/vibration. Female hexagonal cap slipped from union as thread worn out.
Damper can be closed remotely by activating solenoid valve for damper closing arrangement. Due to leakage not full air pressure available at inlet of the piston. It Can lead to ambiguous situation damper might close or can remain open in case of critical emergency situation demanding closing of all air flaps and opening to ER.
Scenario 10 During life testing of Rescue Boat engine in open sea was noticed too low cooling water flow , thus giving high temperature alarm on the engine. After investigation it was found that the water pump impeller broke down and was blocking the flow of water to the motor. As possible reason, testing motor without cooling water. Dirty cooling media with abrasive substance. Age of rubber impeller. Scenario 11 During routine deck inspection, fall protection chains on the forecastle were found completely rusty and in very poor condition. Weather and sprays of sea water influence.
Scenario 11 During routine checks it was noticed that several mesh for accommodation drains were in advanced corroded condition and some were completely missing. If not rectified in time this could have led to clogged drain pipes and personnel injury if one would have stepped wrongly above the drain holes. Possible weather condition has led to the advanced corrosion condition; insufficient maintenance and overlooking the poor condition of the drains mesh.



HIGH POTENTIAL (HIPO NEAR MISS)
During the review of the Oil Record Book Part II on board it was noted that inappropriate entries were made for the period 03rd – 05th March 2021. The master informed the company of his findings. Vessel was instructed with corrective actions, regarding appropriate entries into the ORB and vessel`s flag administration informed.
Intermediate and Root Cause:
A. Inadequate compliance with company procedures Intermediate Cause – Excessive Action Requirements (During hand over / take over). Root Cause - Company Standards, Policies or Administrative Controls (SPACs) Not Used – Enforcement issue
B. Inadequate knowledge of requirements Intermediate Cause – Knowledge-based decision required. Root Cause – Company Standards, Policies or Administrative Controls (SPACS) Not Used – Unaware of SPACs
KNOWLEDGE SHARING
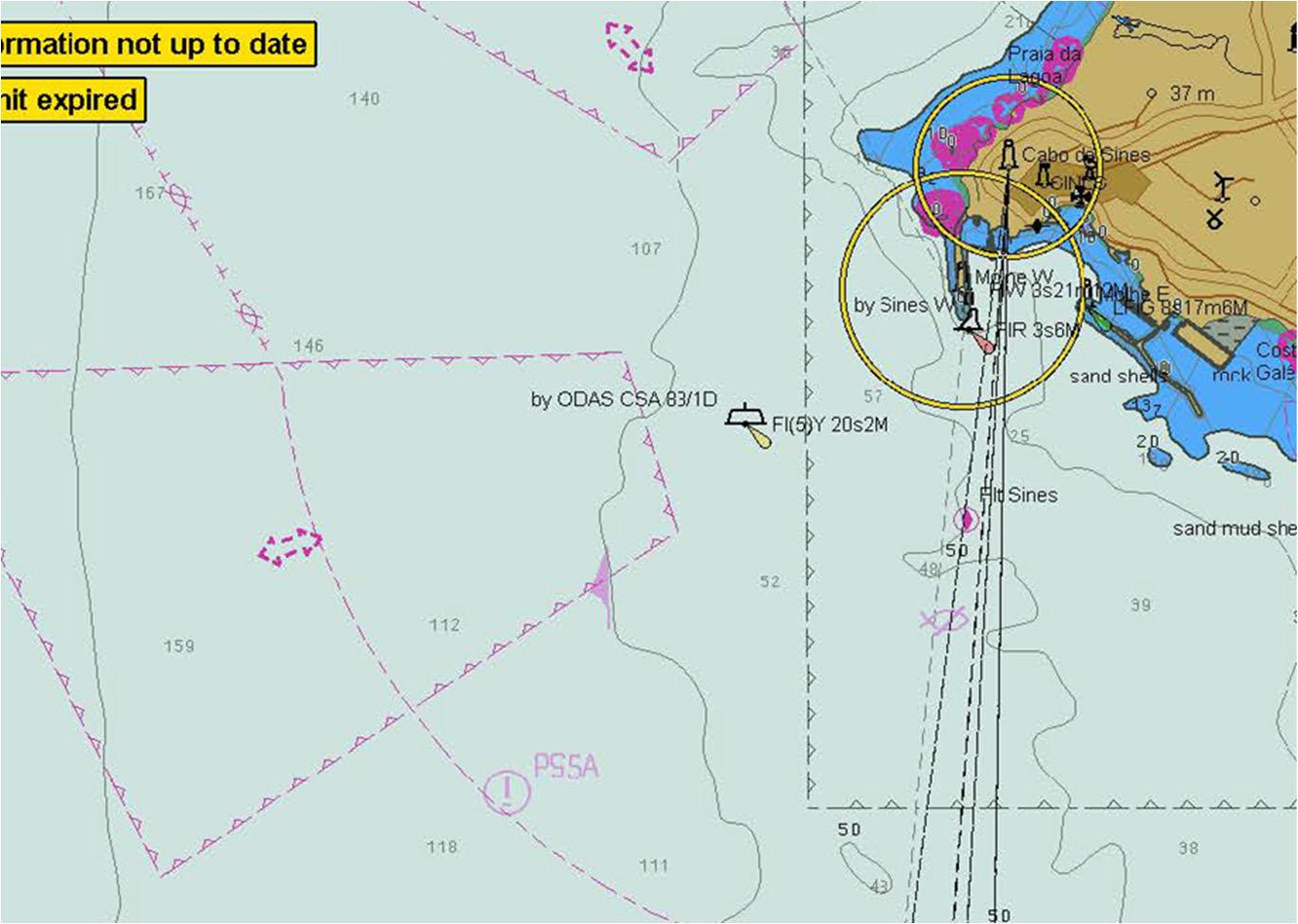
PORT OF SINES, Portugal Port of Sines is located along the North Atlantic coast of Portugal and is exposed to the long ocean swell. It is an artificial port not guarded by breakwater. Due to swell ships often experience surging movement whilst moored alongside berth. Over the last few years our ships have reported Incidents / Near Misses during this port call resulting in parted or damaged mooring ropes, damaged gangway, parted tug’s line, and evacuation from berth. Implementing control measures to reduce the risks to ALARP level can assist with making the port call safer and occurrence free.
Local weather forecast, port contingency plan, availability, procedure & timeline required for tugs, pilot, mooring crew etc, shall be verified during Master-Pilot information exchange as well as pre-transfer key meeting with the terminal representatives & local agent.
Masters shall use their professional judgment to assess the risks on site and make the decision to depart from a berth in ample time or to deploy additional moorings and have tugs assisting her to remain alongside. Mooring lines deployed shall be as long as possible, with chafe guard and preferably maintained equal and slightly slack to allow the vessel to ‘play’ taking into consideration tolerance for cargo hose/arm. For vessels equipped with wire ropes, longer 22m tails should be considered. SN procedure 06.203.01, Mooring Equipment Guidelines and OCIMF Effective Mooring should be consulted for further guidance regarding mitigating swell or surge alongside. Technical and Commercial departments should be updated if facing issues.