
2 minute read
Iliac side branch devices show promise in tortuous aortoiliac anatomy



Gianmarco de Donato (University of Siena, Siena, Italy) uses a case example to highlight the benefits of Artivion/Jotec’s iliac branch device portfolio in the treatment of tortuous aortoiliac aneurysms.
A 75-YEAR-OLD WOMAN presenting with a 5.5cm abdominal aortic aneurysm with ectatic common iliac arteries underwent endovascular aneurysm repair (EVAR) with a trimodular stent graft (Ovation iX [Endologix]: main body 26/80mm; right iliac limb 22/100mm; left iliac limb 18/100mm).
Regular follow-up was performed, with computed tomography angiography (CTA) at one month, and duplex ultrasound (DUS) at six, 12 and 24 months after implantation revealing good aneurysm sealing with sac shrinkage of 0.4cm. At three-year follow-up, a high-flow endoleak associated with sac increase of 0.7cm was suspected at DUS, and confirmed at CTA as a type 1b bilateral endoleak (Figure 1). Due to degeneration of the distal sealing zones, both iliac limbs were migrated a few centimetres into the aneurysmal sac, while the proximal sealing was still optimal.


We looked for an endovascular rescue intervention and planned a relining with a right iliac branch device with a dedicated bridging stent to the previous stent graft main body, and a limb extension at the level of the left common iliac artery. Additional anatomical challenges were represented by the tortuosity of the first portion of the right external iliac artery, and the presence of some severe eccentric calcifications (Figure 2)
Through a common femoral artery access, a 13/13x50mm E-tegra bridging stent graft (Artivion/Jotec) and a 14/10 E-liac branch device (Artivion/Jotec) were implanted (Figure 3a), while the hypogastric component was delivered through the left brachial access (7Fr, 90cm sheath plus Advanta balloon-expandable stent graft [Getinge] 10/59mm; Figure 3b).
As an adjunctive manoeuvre, we performed pre-dilation with a 12mm compliant balloon of the right main body gate in order to reduce any potential friction or conflict during the tracking of the new components for the relining (Figure 4). This resulted in a very smooth transition of the iliac bridge and iliac branch device, and an easy orientation of the E-marker to cannulate the hypogastric ostium. The delivery of the balloon-expandable covered stent from the brachial access was performed with synchronous inflation of a 10mm compliant balloon in the external iliac portion of the iliac branch device to stabilise the implantation and avoid any conflict at the level of bifurcation.
A further relining was performed at the level of the left common iliac with a 18/100mm Ovation extension.
A CTA at 45 days after relining revealed complete aneurysm sealing, with excellent patency of the iliac components (Figure 5). In particular, it is evident how the bifurcation stent with the dedicated design allowed a flexible orientation of the side
Figure 1. High-flow endoleak associated with sac increase of 0.7cm confirmed at CTA as a type 1b bilateral endoleak
Figure 2. Additional anatomical challenges were represented by the tortuosity of the first portion of the right external iliac artery, and the presence of some severe eccentric calcifications
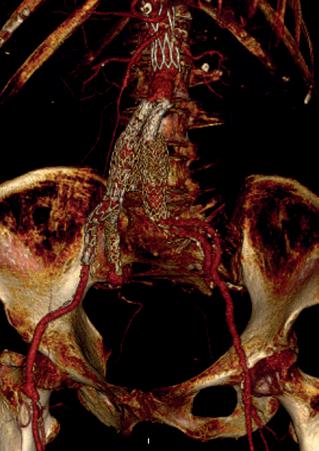
Figure 3a. Through a common femoral artery access, a 13/13x50mm E-tegra bridging stent graft and a 14/10–100mm E-liac iliac branch device were implanted
Figure 3b. The hypogastric component was delivered through the left brachial access
Figure 4. Pre-dilation with a 12mm compliant balloon of the right main body gate branch; the E-liac appears nicely seated on the hypogastric bifurcation (Figure 6), the hypogastric bridging stent is securely connected thanks to the compression stent shape, while the asymmetrical spring of the external iliac segment offers good adaptability even in the presence of calcium and vessel angulation.
The 24-month DUS after iliac branch device implantation showed no endoleak and sac shrinkage of 0.5cm.

Despite meticulous initial selection, some patients will experience degeneration of the proximal and/or distal sealing zones after initial EVAR. Where feasible, the preservation of the hypogastric artery with an iliac branch device to assure antegrade flow is worthwhile in the management of aortoiliac aneurysms.
Gianmarco de Donato is a full professor of vascular surgery at the University of Siena in Siena, Italy.


