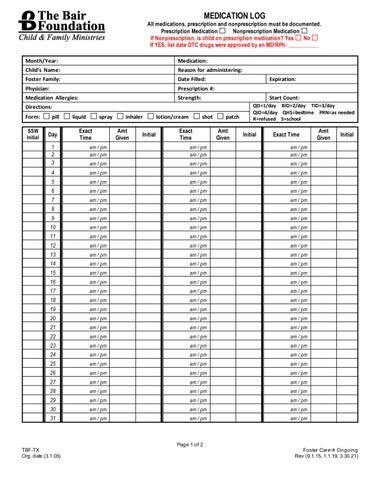
MEDICATION LOG
All medications, prescription and nonprescription must be documented. Prescription Medication Nonprescription Medication If Nonprescription, is child on prescription medication? Yes No If YES, list date OTC drugs were approved by an MD/RPh: ___________ Month/Year:
Medication:
Child’s Name:
Reason for administering:
Foster Family:
Date Filled:
Physician:
Prescription #:
Medication Allergies:
Strength:
Expiration: Start Count:
Directions: Form:
pill
SSW Initial
Day
liquid
spray
Exact Time
inhaler Amt Given
Initial
lotion/cream
shot
Exact Time
patch Amt Given
QD=1/day BID=2/day TID=3/day QID=4/day QHS=bedtime PRN=as needed R=refused S=school
Initial
Exact Time
1 2 3
am / pm am / pm
am / pm am / pm
am / pm am / pm
am / pm
am / pm
am / pm
4
am / pm
am / pm
am / pm
5
am / pm
am / pm
am / pm
6
am / pm
am / pm
am / pm
7
am / pm
am / pm
am / pm
8
am / pm
am / pm
am / pm
9
am / pm
am / pm
am / pm
10
am / pm
am / pm
am / pm
11
am / pm
am / pm
am / pm
12
am / pm
am / pm
am / pm
13
am / pm
am / pm
am / pm
14
am / pm
am / pm
am / pm
15
am / pm
am / pm
am / pm
16
am / pm
am / pm
am / pm
17
am / pm
am / pm
am / pm
18
am / pm
am / pm
am / pm
19
am / pm
am / pm
am / pm
20
am / pm
am / pm
am / pm
21
am / pm
am / pm
am / pm
22
am / pm
am / pm
am / pm
23
am / pm
am / pm
am / pm
24
am / pm
am / pm
am / pm
25
am / pm
am / pm
am / pm
26
am / pm
am / pm
am / pm
27
am / pm
am / pm
am / pm
28
am / pm
am / pm
am / pm
29
am / pm
am / pm
am / pm
30
am / pm
am / pm
am / pm
31
am / pm
am / pm
am / pm
TBF-TX Org. date (3.1.05)
Page 1 of 2
Amt Given
Initial
Foster Care→ Ongoing Rev (9.1.15, 1.1.19, 3.30.21)